chronic disease program planning in public health: what's the evidence
TRANSCRIPT
Welcome! This webinar has been made possible with support from the
Canadian Institutes of Health Research
Chronic Disease Program Planning:
Discussing Review-Level Evidence
You will be placed on hold until the webinar begins. The webinar will begin shortly, please remain on the line.

What’s the evidence? Booth, M., O’Brodovich, H., Finegood, D. (2004). Addressing
childhood obesity: The evidence for action. Ottawa, ON: Canadian Institutes of Health Research, Institute of Nutrition, Metabolism and Diabetes.
Shiell, A., Spilchak, P., Ladhani, N., Hawe, P., Lorenzetti, D. (2008). A systematic review of population health approaches to prevent type II diabetes: Report to the Public Health Agency of Canada. Calgary, AB: Population Health Intervention Research Centre (PHIRC).
O’Brien, K., Nixon, S., Tynan, A.M., Glazier, R.H. (2010). Aerobic exercise interventions for adults living with HIV/AIDS. Cochrane Database of Systematic Reviews, Issue 8, Art. No.: CD001796.
Farmer, A.P., Legare, F., Grimshaw, J., Harvey, E., McGowan, J.L., et al. (2008). Printed educational materials: Effects on professional practice and health care outcomes. Cochrane Database of Systematic Reviews, Issue 3, Art. No.: CD004398.
Housekeeping Connection issues Recommend you use a wired Internet
connection rather than wireless, to help prevent connection challenges
Please contact the WebEx 24/7 help line:
1-866-229-3239

Housekeeping How to post comments/questions
during the webinar To write in CHAT or Q&A
• Address questions to all panelists
• Raise hand using the ‘hand’ icon (indicated on the right)
• Respond to general comments using the feedback icon
To talk: • If have a head set, you can ask to
be passed the mic (mic request icon on right)
Hand icon Mic request
Chat
Q&A
Side Panel in WebEx
Feedback icon
Welcome! This webinar has been made possible with support from the
Canadian Institutes of Health Research
Chronic Disease Program Planning:
Discussing Review-Level Evidence
You will be placed on hold until the webinar begins. The webinar will begin shortly, please remain on the line.

Maureen Dobbins Scientific Director Tel: 905 525-9140 ext 22481 E-mail: [email protected]
Kara DeCorby Administrative Director Tel: (905) 525-9140 ext. 20461 E-mail: [email protected]
Lori Greco Knowledge Broker
Daiva Tirilis Research Coordinator Tel: (905) 525-9140 ext. 20460 E-mail: [email protected]
Lyndsey McRae Research Assistant
Robyn Traynor Research Coordinator
The Health Evidence Team
Heather Husson Project Manager

What is www.health-evidence.ca?
Evidence
Decision Making
inform
Why use www.health-evidence.ca?
1. Saves you time
2. Relevant & current evidence
3. Transparent process
4. Supports for EIDM available
5. Easy to use

Meetings, Planning & Dissemination Project
CIHR Funded MOP-238541

CIHR-Funded Reviews Booth, M., O’Brodovich, H., Finegood, D. (2004). Addressing
childhood obesity: The evidence for action. Ottawa, ON: Canadian Institutes of Health Research, Institute of Nutrition, Metabolism and Diabetes.
Shiell, A., Spilchak, P., Ladhani, N., Hawe, P., Lorenzetti, D. (2008). A systematic review of population health approaches to prevent type II diabetes: Report to the Public Health Agency of Canada. Calgary, AB: Population Health Intervention Research Centre (PHIRC).
O’Brien, K., Nixon, S., Tynan, A.M., Glazier, R.H. (2010). Aerobic exercise interventions for adults living with HIV/AIDS. Cochrane Database of Systematic Reviews, Issue 8, Art. No.: CD001796.
Farmer, A.P., Legare, F., Grimshaw, J., Harvey, E., McGowan, J.L., et al. (2008). Printed educational materials: Effects on professional practice and health care outcomes. Cochrane Database of Systematic Reviews, Issue 3, Art. No.: CD004398.
Evaluation
Please check your email for the evaluation survey link after the webinar.
It take 5 minutes to complete!
If you’ve been watching with someone else and did not personally register for the webinar, please
e-mail Jennifer McGugan at [email protected] to be sent the survey.

Questions?

Summary Statement: Booth (2004)
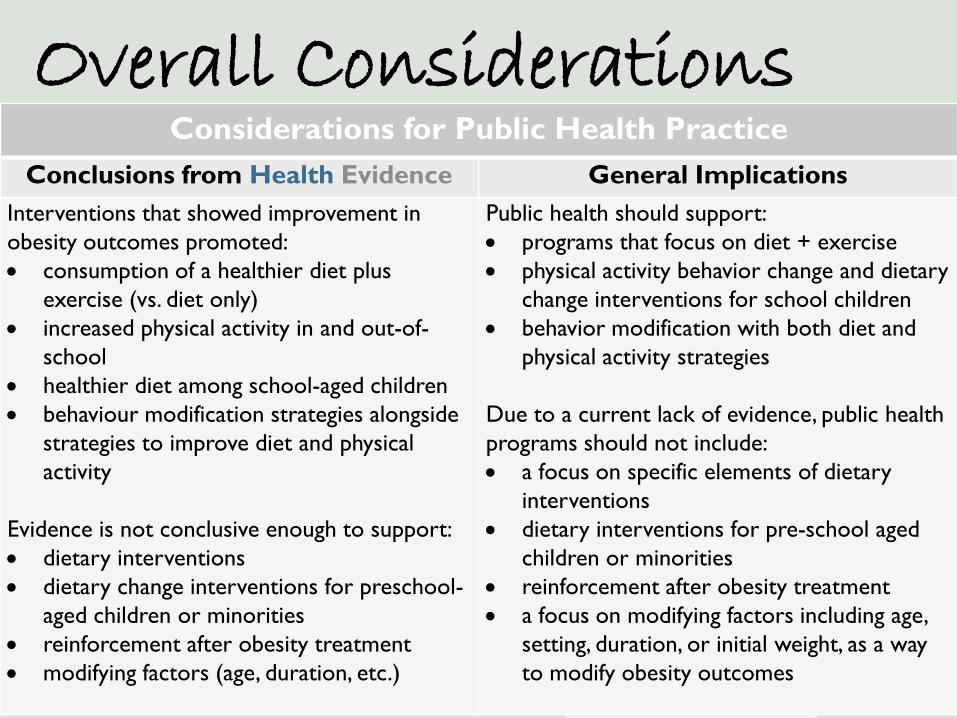
Overall Considerations
Considerations for Public Health Practice Conclusions from Health Evidence General Implications
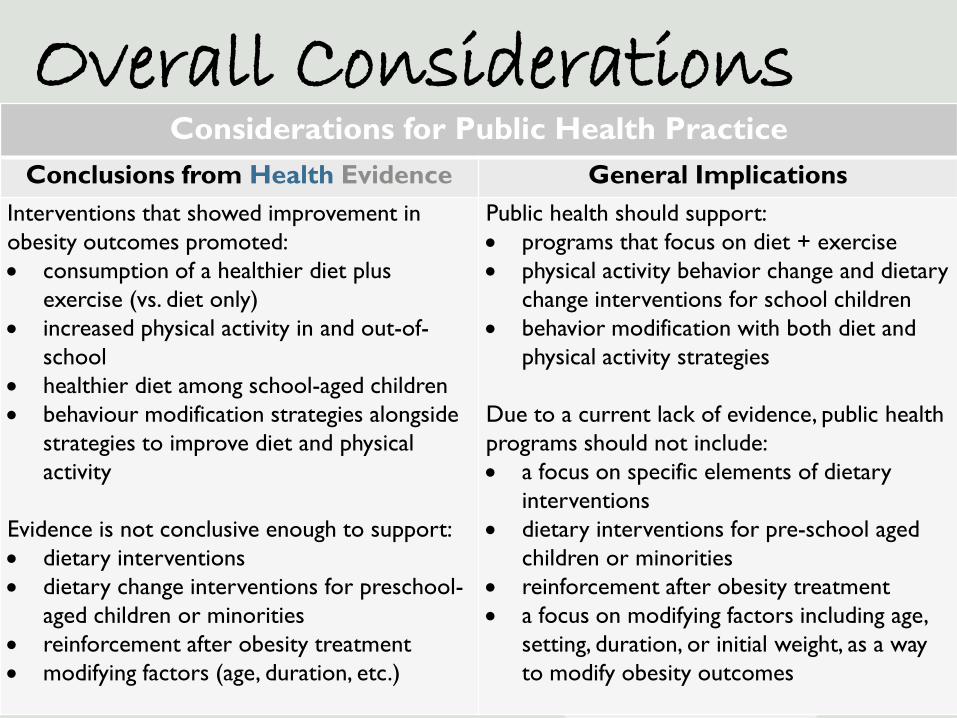
Interventions that showed improvement in obesity outcomes promoted: • consumption of a healthier diet plus
exercise (vs. diet only) • increased physical activity in and out-of-
school • healthier diet among school-aged children • behaviour modification strategies alongside
strategies to improve diet and physical activity
Evidence is not conclusive enough to support: • dietary interventions • dietary change interventions for preschool-
aged children or minorities • reinforcement after obesity treatment • modifying factors (age, duration, etc.)
Public health should support: • programs that focus on diet + exercise • physical activity behavior change and dietary
change interventions for school children • behavior modification with both diet and
physical activity strategies
Due to a current lack of evidence, public health programs should not include: • a focus on specific elements of dietary
interventions • dietary interventions for pre-school aged
children or minorities • reinforcement after obesity treatment • a focus on modifying factors including age,
setting, duration, or initial weight, as a way to modify obesity outcomes
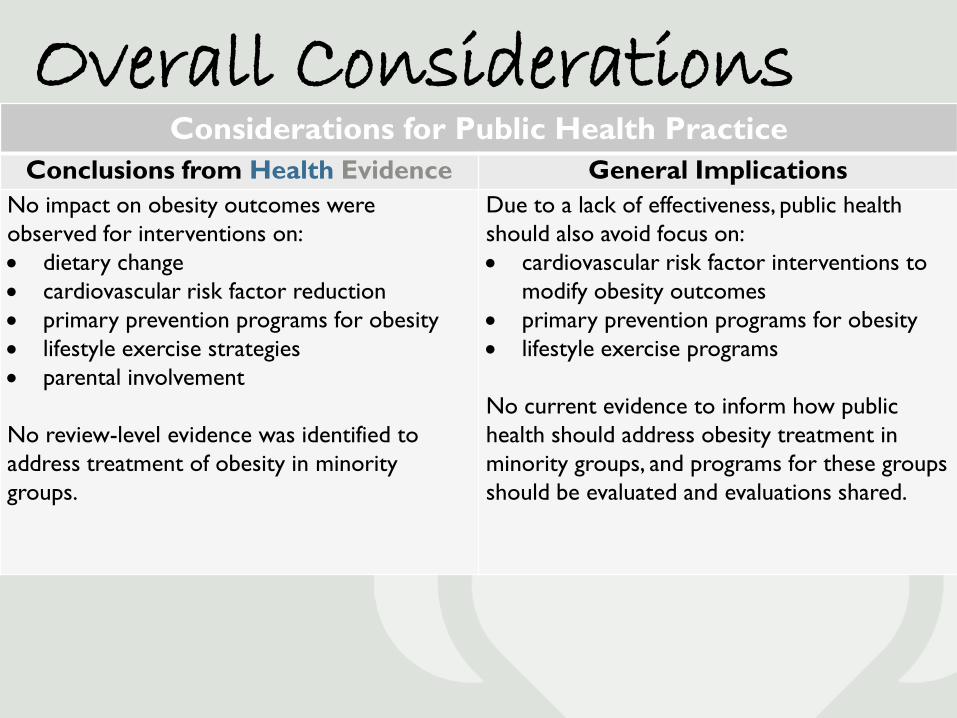
Overall Considerations Considerations for Public Health Practice
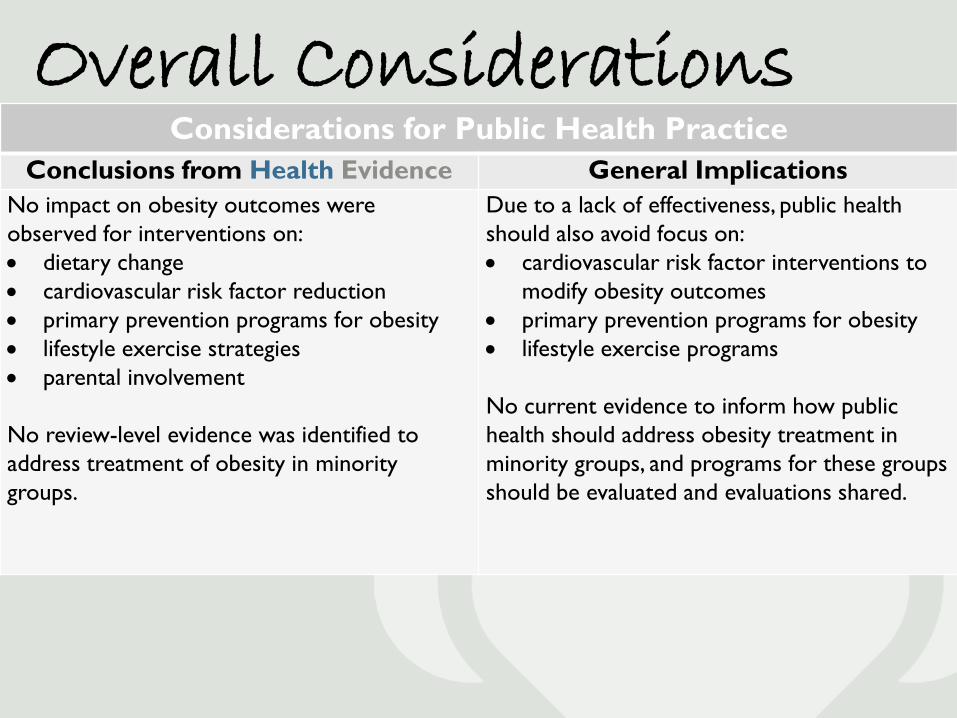
Conclusions from Health Evidence General Implications No impact on obesity outcomes were observed for interventions on: • dietary change • cardiovascular risk factor reduction • primary prevention programs for obesity • lifestyle exercise strategies • parental involvement
No review-level evidence was identified to address treatment of obesity in minority groups.
Due to a lack of effectiveness, public health should also avoid focus on: • cardiovascular risk factor interventions to
modify obesity outcomes • primary prevention programs for obesity • lifestyle exercise programs No current evidence to inform how public health should address obesity treatment in minority groups, and programs for these groups should be evaluated and evaluations shared.

Interpreting the Evidence
Prevention of obesity (6 SR including 34 studies + 6 narrative reviews; mostly low to moderate quality)
What’s the evidence? Implications for practice & policy
No impact of obesity OR cardiovascular prevention interventions on adiposity • Systematic review evidence (4 reviews for
which citation analysis was possible): does not support obesity prevention programs (i.e. several school-based) for the reduction of adiposity. (7/26 studies identified a reduction in adiposity)
• Systematic review evidence (1 review – 16 studies): Cardiovascular prevention programs were not effective in decreasing adiposity (7/77 showed a positive impact).
• Narrative review evidence (6 reviews): insufficient evidence for obesity prevention as an adiposity reduction measure.
• Public health decision makers should not rely on either obesity prevention or cardiovascular prevention programs for decreasing adiposity, given the current evidence from both systematic and narrative reviews.

Interpreting the Evidence
Diet vs. Diet and Exercise (5 reviews)
What’s the evidence? Implications for practice & policy
• Exercise programs combined with a dietary intervention offered some improvement in adiposity (6 of 10 studies); however the extent to which benefits are sustained in long term is unclear)
• Public Health decision makers should promote diet and exercise together (as opposed to diet alone) for the secondary prevention of obesity, and evaluate whether long-term benefits are realized.
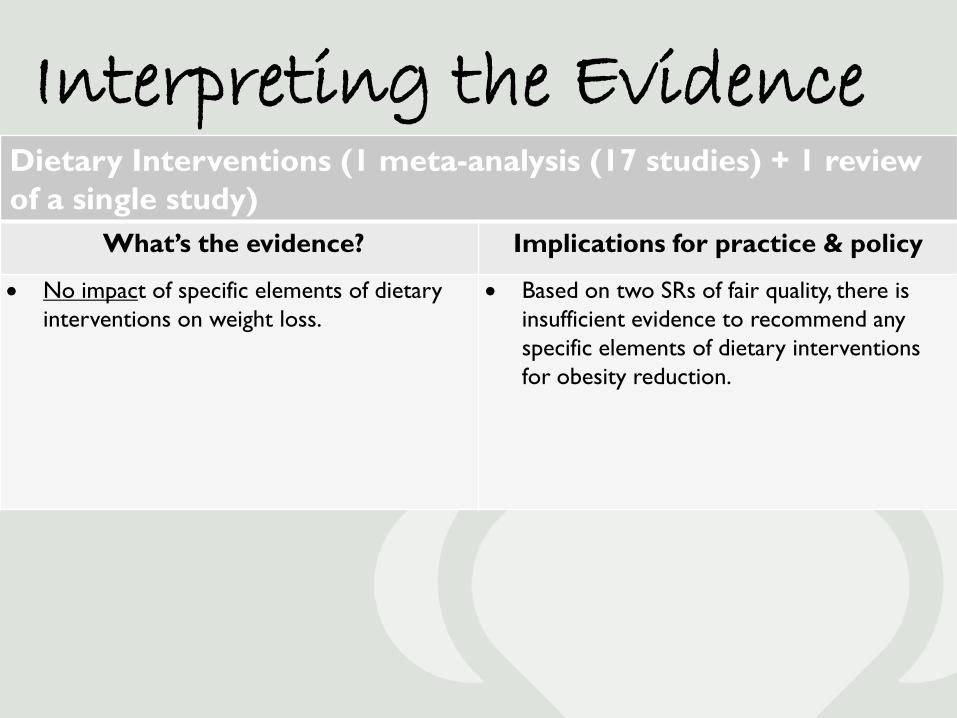
Interpreting the Evidence
Dietary Interventions (1 meta-analysis (17 studies) + 1 review of a single study)
What’s the evidence? Implications for practice & policy
• No impact of specific elements of dietary interventions on weight loss.
• Based on two SRs of fair quality, there is insufficient evidence to recommend any specific elements of dietary interventions for obesity reduction.

Interpreting the Evidence
Physical Activity (PA) Behaviour Change (8 reviews)
What’s the evidence? Implications for practice & policy
• PA during school hours – high quality review evidence (4 reviews) shows that school-based interventions are effective in increasing PA during school hours.
• PA outside school hours – there is some (mixed) evidence that school-based interventions increase PA outside school hours.
• Public health should promote PA behaviour change interventions to increase PA during school hours. Programs should be evaluated to determine whether PA outside school hours is increased.
• Evaluations conducted by public health should ideally include long-term follow up into adulthood.

Interpreting the Evidence
Strategies to promote dietary change (7 SR + 5 narrative reviews; analysis according to behaviour change model)
What’s the evidence? Implications for practice & policy
• Preschool children: 7/10 studies in 2 SRs offer mixed evidence that does not conclusively support specific behavioural or knowledge-based strategies to change food-related behaviour (e.g. touch/smell/taste new foods, modeling, repeated exposures)
• School-based: 42/59 studies in 6 reviews showed some improvement in dietary behaviour that was more closely attributed to behaviourally-based approaches rather than knowledge-based approaches. Descriptions of strategies are not provided.
• Minority Populations: 1 low-quality review offered no definitive conclusions that dietary interventions are effective.
• Public health should not rely on either behavioural or knowledge-based approaches to improve preschool children’s dietary behaviour.
• Public health should use and evaluate behaviourally-based approaches to improve dietary behaviour in school-based programs.
• Public health should evaluate efforts to improve dietary behaviour in minority populations in order to contribute to the evidence base available.

Interpreting the Evidence
Strategies Lifestyle Exercise Strategies (3 reviews citing the same 3 studies + 1 meta-analysis)
What’s the evidence? Implications for practice & policy
• Lifestyle exercise was distinct from other exercise programs in that it (1) includes activities of daily living, (2) includes caloric expenditure in small increments throughout the day, and (3) no prescribed intensity.
• No impact on childhood obesity compared to either no exercise or other exercise, based on the meta-analysis incorporating the widest range of evidence.
• Public Health decision makers should not rely on lifestyle exercise to decrease childhood obesity. However, public health should consider other possible benefits to be derived from the promotion of lifestyle exercise.

Interpreting the Evidence
Parental Involvement (4 reviews (13 studies) + 1 meta-analysis)
What’s the evidence? Implications for practice & policy
• Parental involvement interventions varied, with only one study directed solely at parents. A range of interventions were aimed at both children and parents to varying degrees. Intervention elements are not well described; but tend to be family-oriented and include homework assignments, and parents motivating their children.
• No impact on childhood obesity treatment, even though there is good evidence in this topic area
• Public health should not focus on parental involvement strategies as a way to improve childhood obesity treatment.

Interpreting the Evidence
Behaviour Modification Strategies (2 reviews of 9 studies + 1 meta-analysis)
What’s the evidence? Implications for practice & policy
• Little information provided regarding the nature of behaviour modification strategies used.
• Improvement in obesity status when behaviour modification strategies were used with dietary and physical activity strategies in the short-term. Behaviour modification, dietary AND physical activity strategies together demonstrated greater treatment effect than behaviour modification and either dietary or PA.
• No impact of additional or “add-on” self-control training on obesity status.
• Behaviour modification strategies should be considered for use with dietary and physical activity interventions, and ideally with all three strategies combined, in aiming to improve obesity status.
• Public health should not focus on self-control training as an additional strategy for reducing obesity in children.

Interpreting the Evidence
Reinforcement (1 review)
What’s the evidence? Implications for practice & policy
• A single, small (15 subjects) study of fair quality in one review showed that periodic reinforcement after obesity treatment enhanced weight loss
• There is limited evidence at this time to support the provision of reinforcement following obesity treatment programs

Interpreting the Evidence
Factors Influencing Obesity Prevention
What’s the evidence? Implications for practice & policy
• There is a very limited evidence examining the effect of setting, duration of treatment and initial weight status upon which to assess the impact on obesity outcomes.
• Based on evidence available at this time, public health should not focus on modifying factors such as: setting, duration of treatment, age, and initial weight status to improve obesity outcomes. It is possible that relationships between these factors and obesity may exist; however, they are unclear at this time.
Overall Considerations
Considerations for Public Health Practice Conclusions from Health Evidence General Implications
Interventions that showed improvement in obesity outcomes promoted: • consumption of a healthier diet plus
exercise (vs. diet only) • increased physical activity in and out-of-
school • healthier diet among school-aged children • behaviour modification strategies alongside
strategies to improve diet and physical activity
Evidence is not conclusive enough to support: • dietary interventions • dietary change interventions for preschool-
aged children or minorities • reinforcement after obesity treatment • modifying factors (age, duration, etc.)
Public health should support: • programs that focus on diet + exercise • physical activity behavior change and dietary
change interventions for school children • behavior modification with both diet and
physical activity strategies
Due to a current lack of evidence, public health programs should not include: • a focus on specific elements of dietary
interventions • dietary interventions for pre-school aged
children or minorities • reinforcement after obesity treatment • a focus on modifying factors including age,
setting, duration, or initial weight, as a way to modify obesity outcomes
Overall Considerations Considerations for Public Health Practice
Conclusions from Health Evidence General Implications No impact on obesity outcomes were observed for interventions on: • dietary change • cardiovascular risk factor reduction • primary prevention programs for obesity • lifestyle exercise strategies • parental involvement
No review-level evidence was identified to address treatment of obesity in minority groups.
Due to a lack of effectiveness, public health should also avoid focus on: • cardiovascular risk factor interventions to
modify obesity outcomes • primary prevention programs for obesity • lifestyle exercise programs No current evidence to inform how public health should address obesity treatment in minority groups, and programs for these groups should be evaluated and evaluations shared.

Questions?
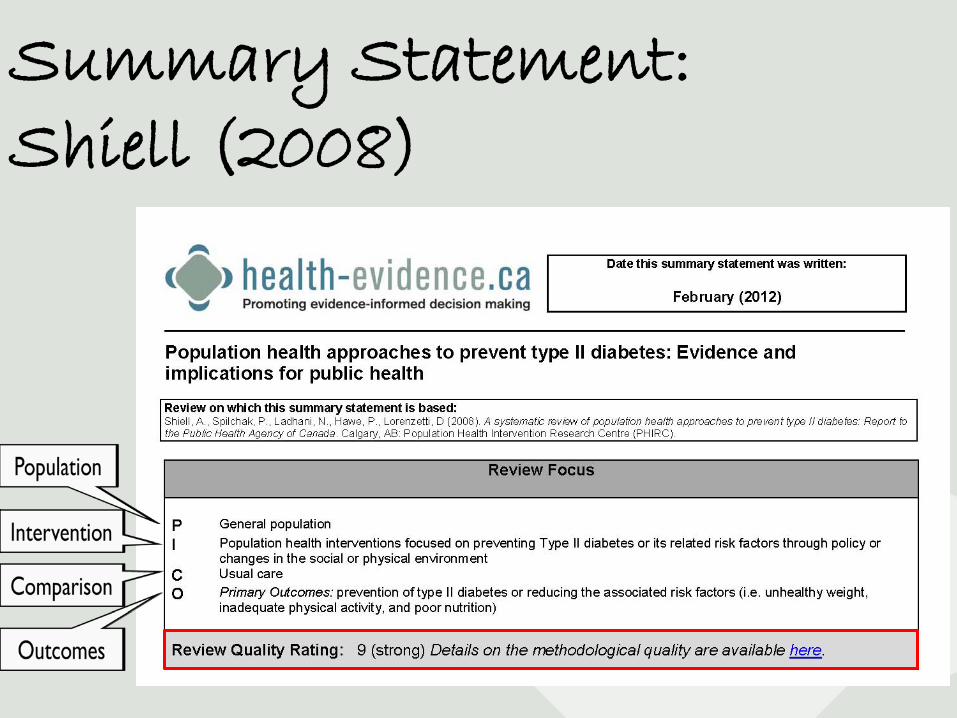
Summary Statement: Shiell (2008)

Overall Considerations
Considerations for Public Health Practice Conclusions from Health Evidence General Implications
School-based interventions led to: • no effects on physical activity, nutrition, BMI,
fruit and vegetable intake, energy from fat, total serum cholesterol, and VO2 Max (rigorous studies)
• improvements in triglycerides, physical activity, systolic and diastolic blood pressure, percentage body fat, smaller increase in BMI, and waist circumference among boys
Community-based interventions led to: • increase in self-reported physical activity
Worksite-based interventions led to: • increase in smoking cessation rates
The most current, rigorous evidence does not support school-based interventions to reduce Type II diabetes or its risk factors. Findings from less rigorous studies do support the use of school-based interventions. Community-based interventions are currently recommended for increasing physical activity. Worksite-based interventions are suggested for increasing smoking cessation rates. There is limited, good quality evidence. Results should be applied cautiously to public health practice, and any associated public health programs need to evaluate the impact of these interventions.
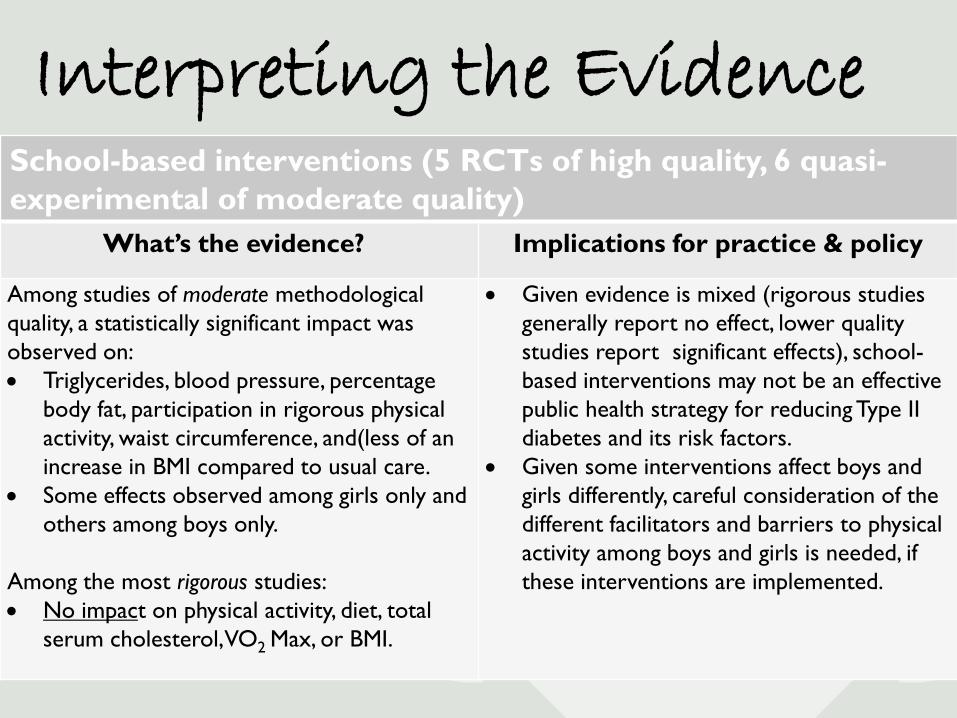
School-based interventions (5 RCTs of high quality, 6 quasi-experimental of moderate quality)
What’s the evidence? Implications for practice & policy
Among studies of moderate methodological quality, a statistically significant impact was observed on: • Triglycerides, blood pressure, percentage
body fat, participation in rigorous physical activity, waist circumference, and(less of an increase in BMI compared to usual care.
• Some effects observed among girls only and others among boys only.
Among the most rigorous studies: • No impact on physical activity, diet, total
serum cholesterol, VO2 Max, or BMI.
• Given evidence is mixed (rigorous studies generally report no effect, lower quality studies report significant effects), school-based interventions may not be an effective public health strategy for reducing Type II diabetes and its risk factors.
• Given some interventions affect boys and girls differently, careful consideration of the different facilitators and barriers to physical activity among boys and girls is needed, if these interventions are implemented.
Interpreting the Evidence
Community-based interventions (1 study; moderate quality)
What’s the evidence? Implications for practice & policy
• One studies of moderate methodological quality, statistically significant impact was observed on self-reported physical activity.
• Community-based interventions are supported for increasing physical activity. Results should be interpreted cautiously as physical activity was measured through self-report, which may overestimate the true treatment effect.
• These findings must be re-evaluated as more rigorous evidence emerges.
Interpreting the Evidence
Worksite-based interventions (1 study; moderate quality)
What’s the evidence? Implications for practice & policy
• One study of moderate methodological quality found a statistically significant increase in smoking cessation rate (OR 1.38; 95% CI 1.05-1.81).
• Worksite-based interventions are recommended for increasing smoking cessation rates.
• These findings must be re-evaluated as more rigorous evidence emerges.
Interpreting the Evidence

Overall Considerations
Considerations for Public Health Practice Conclusions from Health Evidence General Implications
School-based interventions led to: • no effects on physical activity, nutrition, BMI,
fruit and vegetable intake, energy from fat, total serum cholesterol, and VO2 Max (rigorous studies)
• improvements in triglycerides, physical activity, systolic and diastolic blood pressure, percentage body fat, smaller increase in BMI, and waist circumference among boys
Community-based interventions led to: • increase in self-reported physical activity
Worksite-based interventions led to: • increase in smoking cessation rates
The most current, rigorous evidence does not support school-based interventions to reduce Type II diabetes or its risk factors. Findings from less rigorous studies do support the use of school-based interventions. Community-based interventions are currently recommended for increasing physical activity. Worksite-based interventions are suggested for increasing smoking cessation rates. There is limited, good quality evidence. Results should be applied cautiously to public health practice, and any associated public health programs need to evaluate the impact of these interventions.

Questions?

Summary Statement: O’Brien (2010)

Overall Considerations
Considerations for Public Health Practice Conclusions from Health Evidence General Implications
Immunologic/virologic • significant impact on CD4 count (interval
aerobic exercisers) • no impact: CD4 count, CD4%, and viral
load (all other types of exercise) Cardiopulmonary • improvement in VO2 Max • no impact: max. heart rate or exercise time Strength • improvements in strength (exercisers) Weight and Body composition • decrease in body fat (aerobic exercisers) • increased change in leg muscle (aerobic
exercise plus progressive resistive training) • no change in body weight, BMI, waist or hip
circumference, waist-to-hip ratio, fat mass Psychological • improvement in depression-dejection
The overall findings suggest that: • the promotion of aerobic exercise, while
resulting in improvements for a small number of outcomes, does not positively impact most outcomes, and may not be an effective public health strategy for this population.
• various formats of aerobic exercise did not positively and significantly impact immunologic/virologic outcomes, most cardiopulmonary outcomes, and strength measures
• given improvements on VO2 Max, percent body fat, and depression in HIV patients, promotion of exercise may be supported
If implemented, the impact of aerobic exercise promotion on this population should be evaluated within the local context.
Interpreting the Evidence
Immunologic/Virologic Outcomes (14 RCTs)
What’s the evidence? Implications for practice & policy
• A statistically significant impact on CD4 count was observed in the interval aerobic group compared to non-exercisers (69.58 cell/mm3, 95% CI, 14.08 – 125.09, P=0.01) (2 studies).
• No impact on change in CD4 count, CD4%, and viral load for all other combinations of exercise versus no exercise.
• Generally the evidence does not support public health allocating resources to promote aerobic exercise among HIV populations for the purpose of improving CD4 count, CD4%, or viral load.
Interpreting the Evidence
Cardiopulmonary (14 RCTs)
What’s the evidence? Implications for practice & policy
• A statistically significant improvement in VO2 Max was observed among aerobic exercisers vs. non-exercisers (2.63 Ml/kg/min, 95% CI, 1.19 – 4.07); constant aerobic exercisers vs. non-exercisers (2.40 Ml/kg/min, 95% CI 0.82-3.99); heavy intensity vs. moderate intensity (4.30 Ml/kg/min, 95% CI 0.67 – 7.98).
• No impact on maximum heart rate or exercise time.
• Exercise promotion is supported as a public health intervention among HIV populations if improvements in VO2 Max are of greatest interest.
• However, improvements in maximum heart rate and exercise time should not be expected.
Interpreting the Evidence
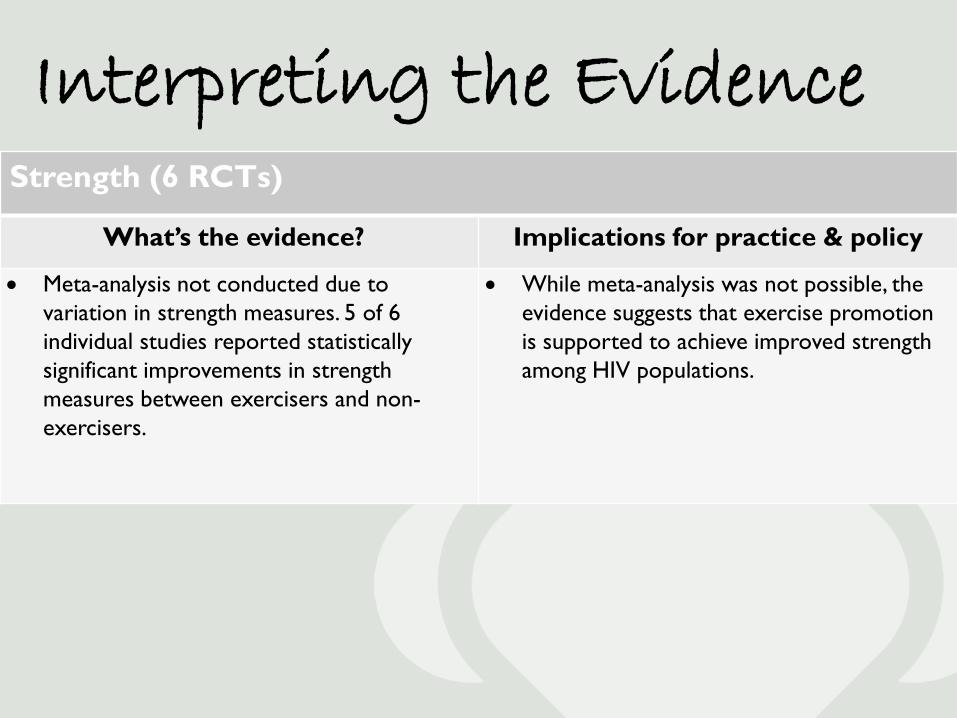
Strength (6 RCTs)
What’s the evidence? Implications for practice & policy
• Meta-analysis not conducted due to variation in strength measures. 5 of 6 individual studies reported statistically significant improvements in strength measures between exercisers and non-exercisers.
• While meta-analysis was not possible, the evidence suggests that exercise promotion is supported to achieve improved strength among HIV populations.
Interpreting the Evidence
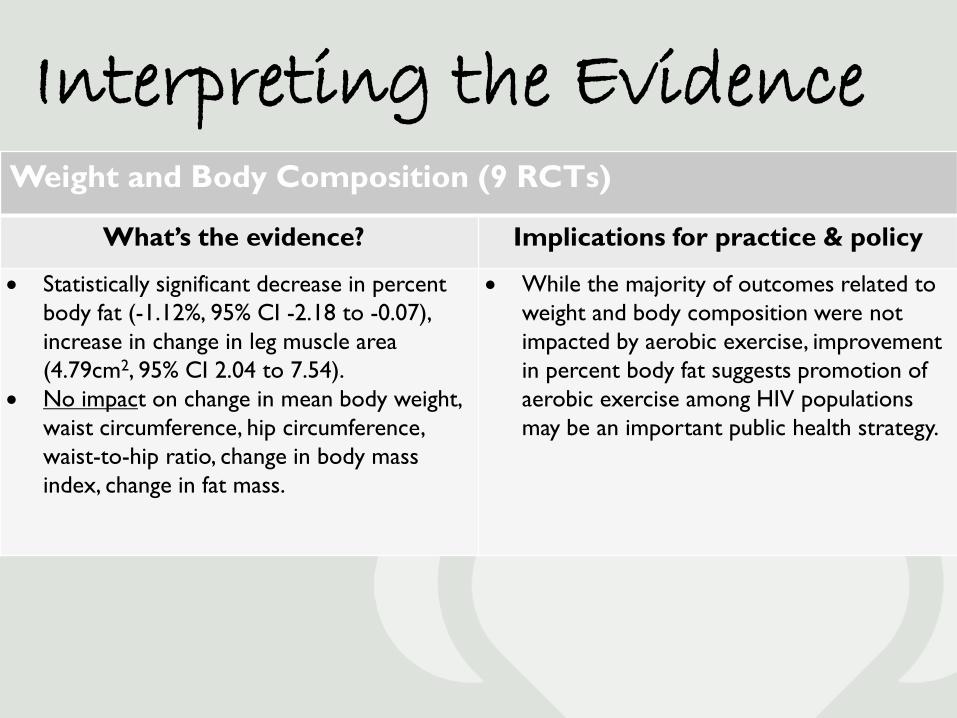
Weight and Body Composition (9 RCTs)
What’s the evidence? Implications for practice & policy
• Statistically significant decrease in percent body fat (-1.12%, 95% CI -2.18 to -0.07), increase in change in leg muscle area (4.79cm2, 95% CI 2.04 to 7.54).
• No impact on change in mean body weight, waist circumference, hip circumference, waist-to-hip ratio, change in body mass index, change in fat mass.
• While the majority of outcomes related to weight and body composition were not impacted by aerobic exercise, improvement in percent body fat suggests promotion of aerobic exercise among HIV populations may be an important public health strategy.

Interpreting the Evidence
Psychological (9 RCTs)
What’s the evidence? Implications for practice & policy
• Statistically significant improvement in depression-dejection scale in exercisers vs. non-exercisers (7.68, 95% CI -13.47 to -1.90).
• The evidence suggests the promotion of aerobic exercise among HIV populations for improving depression-dejection measure.

Overall Considerations
Considerations for Public Health Practice Conclusions from Health Evidence General Implications
Immunologic/virologic • significant impact on CD4 count (interval
aerobic exercisers) • no impact: CD4 count, CD4%, and viral
load (all other types of exercise) Cardiopulmonary • improvement in VO2 Max • no impact: max. heart rate or exercise time Strength • improvements in strength (exercisers) Weight and Body composition • decrease in body fat (aerobic exercisers) • increased change in leg muscle (aerobic
exercise plus progressive resistive training) • no change in body weight, BMI, waist or hip
circumference, waist-to-hip ratio, fat mass Psychological • improvement in depression-dejection
The overall findings suggest that: • the promotion of aerobic exercise, while
resulting in improvements for a small number of outcomes, does not positively impact most outcomes, and may not be an effective public health strategy for this population.
• various formats of aerobic exercise did not positively and significantly impact immunologic/virologic outcomes, most cardiopulmonary outcomes, and strength measures
• given improvements on VO2 Max, percent body fat, and depression in HIV patients, promotion of exercise may be supported
If implemented, the impact of aerobic exercise promotion on this population should be evaluated within the local context.

Questions?
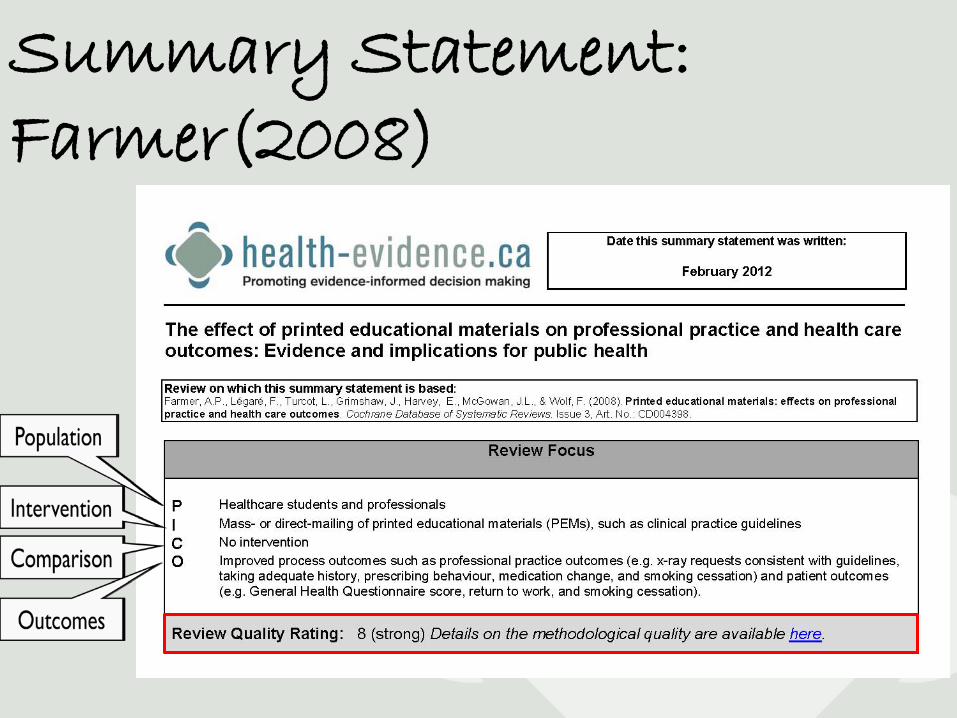
Summary Statement: Farmer(2008)
Overall Considerations
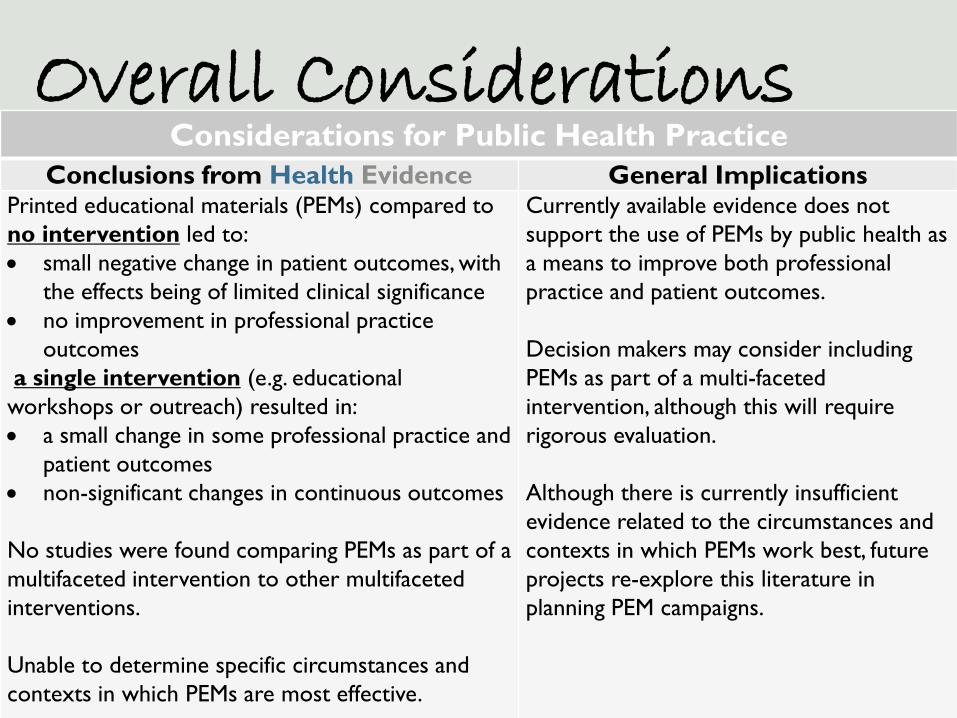
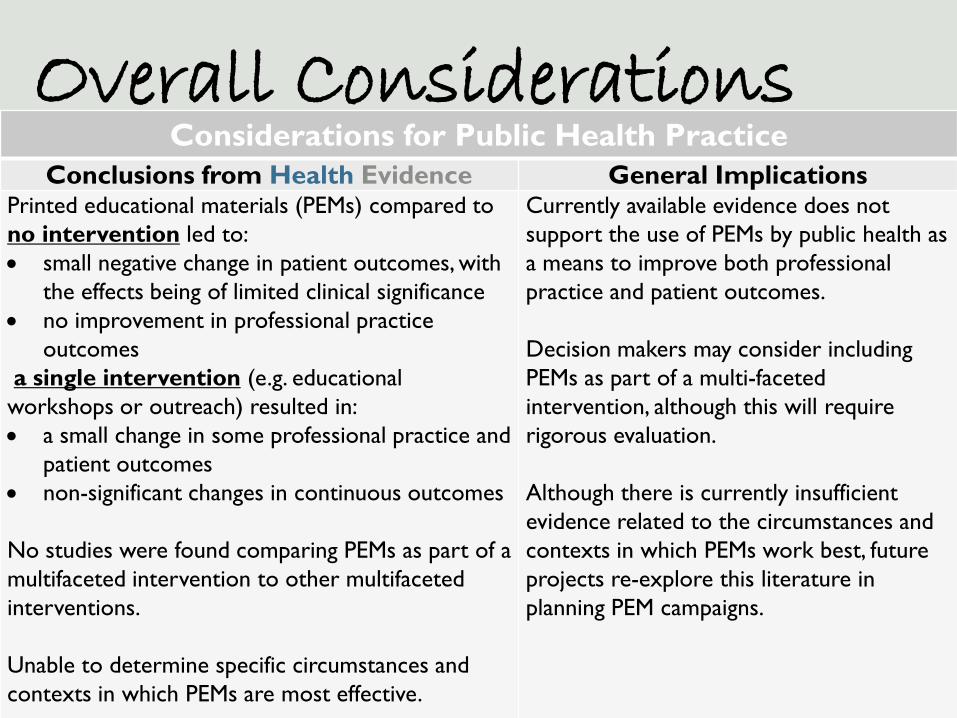
Considerations for Public Health Practice Conclusions from Health Evidence General Implications
Printed educational materials (PEMs) compared to no intervention led to: • small negative change in patient outcomes, with
the effects being of limited clinical significance • no improvement in professional practice
outcomes a single intervention (e.g. educational workshops or outreach) resulted in: • a small change in some professional practice and
patient outcomes • non-significant changes in continuous outcomes
No studies were found comparing PEMs as part of a multifaceted intervention to other multifaceted interventions. Unable to determine specific circumstances and contexts in which PEMs are most effective.
Currently available evidence does not support the use of PEMs by public health as a means to improve both professional practice and patient outcomes. Decision makers may consider including PEMs as part of a multi-faceted intervention, although this will require rigorous evaluation. Although there is currently insufficient evidence related to the circumstances and contexts in which PEMs work best, future projects re-explore this literature in planning PEM campaigns.
Interpreting the Evidence
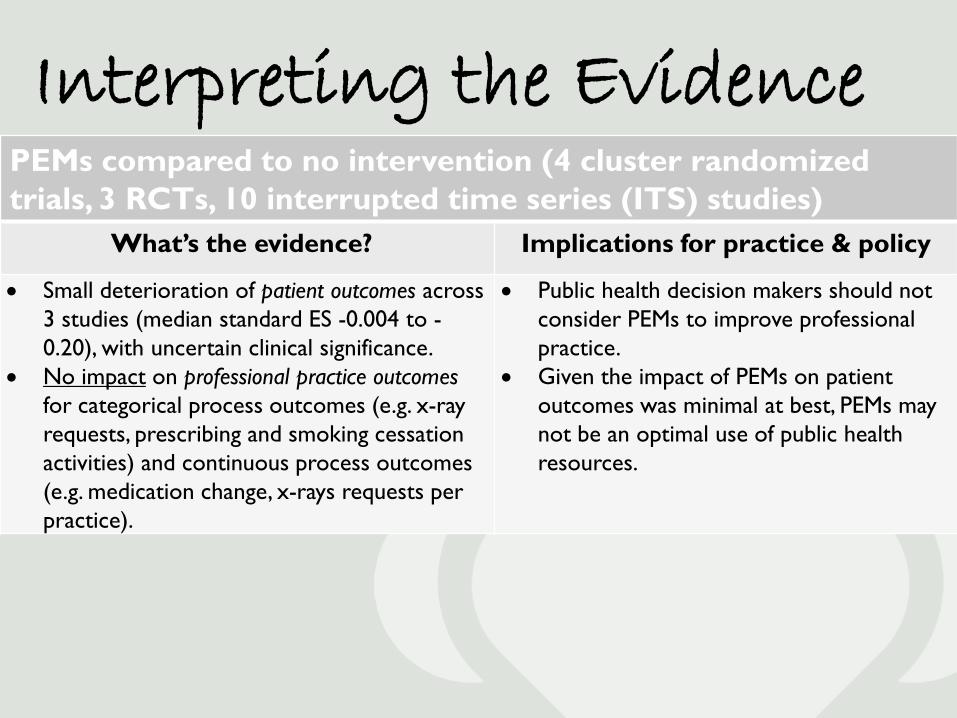
PEMs compared to no intervention (4 cluster randomized trials, 3 RCTs, 10 interrupted time series (ITS) studies)
What’s the evidence? Implications for practice & policy
• Small deterioration of patient outcomes across 3 studies (median standard ES -0.004 to -0.20), with uncertain clinical significance.
• No impact on professional practice outcomes for categorical process outcomes (e.g. x-ray requests, prescribing and smoking cessation activities) and continuous process outcomes (e.g. medication change, x-rays requests per practice).
• Public health decision makers should not consider PEMs to improve professional practice.
• Given the impact of PEMs on patient outcomes was minimal at best, PEMs may not be an optimal use of public health resources.

Interpreting the Evidence
PEMs as one component of any intervention compared to a single intervention (1 RCT)
What’s the evidence? Implications for practice & policy
• A single RCT showed a small positive impact on professional practice outcomes (median absolute risk difference 0.5 in favour of PEMs), with the 2 other trials reporting non-significant effects.
• A single RCT showed a small positive impact on categorical patient outcomes for smoking cessation (median standardized effect -0.2%).
• No impact on continuous patient outcomes (e.g. screening, return to work, quit smoking).
• When using PEMs as one component of a larger intervention, public health decision makers should not invest heavily in PEMs to improve professional practice OR patient outcomes. However, the currently-available evidence is limited.
Overall Considerations
Considerations for Public Health Practice Conclusions from Health Evidence General Implications
Printed educational materials (PEMs) compared to no intervention led to: • small negative change in patient outcomes, with
the effects being of limited clinical significance • no improvement in professional practice
outcomes a single intervention (e.g. educational workshops or outreach) resulted in: • a small change in some professional practice and
patient outcomes • non-significant changes in continuous outcomes
No studies were found comparing PEMs as part of a multifaceted intervention to other multifaceted interventions. Unable to determine specific circumstances and contexts in which PEMs are most effective.
Currently available evidence does not support the use of PEMs by public health as a means to improve both professional practice and patient outcomes. Decision makers may consider including PEMs as part of a multi-faceted intervention, although this will require rigorous evaluation. Although there is currently insufficient evidence related to the circumstances and contexts in which PEMs work best, future projects re-explore this literature in planning PEM campaigns.

Questions?

Discussion Forum Please continue to discuss this topic and other
topics on our discussion forum. www.health-evidence.ca/forum/
Login with your health-evidence username and password or register if you aren’t a member yet.
Join us for a LIVE on Monday, February 27 at 1:00 pm EST to have your questions answered in real time!
Evaluation Please check your email for the evaluation
link. It take 5 minutes to complete! If you’ve been watching with someone else and did
not personally register for the webinar, please e-mail Jennifer McGugan at
[email protected] to be sent the survey.
Thank you for your participation!