chronic intestinal dysmotility a growing problem · chronic intestinal dysmotility a growing...
TRANSCRIPT

Chronic intestinal dysmotility A growing problem Dr Simon Gabe Consultant Gastroenterologist St Mark’s Hospital

Chronic intestinal pseudo-obstruction Definition
A severe digestive syndrome characterized by derangement of gut propulsive motility in the absence of a mechanical obstruction
Antonucci et al, World J Gastroenterol 2008;14(19):2953–2961


Conditions that mimic or contribute to the presentation
Organic obstruction Transition point
Opiates Opiate withdrawal & chronic opiate usage (both manifest as abdominal pain)
Psychosocial problems
Functional GI disorders (severe IBS) Anorexia nervosa Atypical eating disorders

Chronic intestinal pseudoobstruction
Primary
Myopathy
Neuropathy
Mesenchymopathy
Secondary
Autonomic or enteric nerves
Collagen diseases (eg Elhers Danlos)
Endocrine & metabolic
Other

INTESTINAL DYSMOTILITY
Obstruction Psychosocial Narcotic Bowel Syndrome Anorexia nervosa
IBS SMA syndrome
Opiates Undernutrition
Primary Hollow visceral myopathy
Jejunal diverticulosis
Secondary Systemic sclerosis
Amyloid Irradiation
Muscular diseases
Primary Hirsprung’s Autoimune
Infective
Secondary General neurological disease
Paraneoplastic Drugs
Myopathy Neuropathy
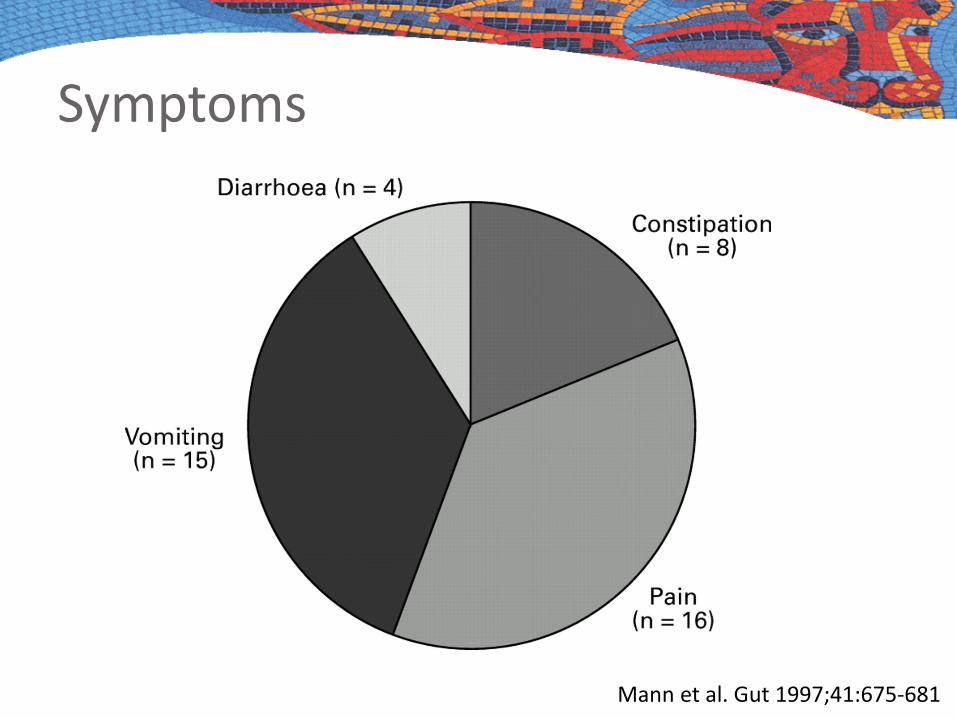
Symptoms
Mann et al. Gut 1997;41:675-681

Age of onset of symptoms
Mann et al. Gut 1997;41:675-681

Investigations
Exclude mechanical causes
BaFT, OGD, colonoscopy
CT, CTE, MRE

Investigations Motility studies Histology
Gastric emptying Whole gut transit EGG SB manometry Oesophageal manometry
Full thickness biopsy Dilated & non-dilated SB Fix in formalin & liquid
nitrogen Skeletal muscle biopsy
If MNGIE suspected
Essential to perform functional studies off opiates

Diagnoses prior to identification of correct diagnosis
Initial diagnosis No of patients (%) Mechanical bowel obstruction 9 (45) Constipation 4 (20) Idiopathic megarectum or megacolon and constipation 3 (15) Sigmoid volvulus 1 (5) Pseudo-obstruction 1 (5) Vesico-ureteric distension and acute renal failure 1 (5) Abdominal migraine/periodic syndrome 1 (5)
Mann et al. Gut 1997;41:675-681

How to manage CIP Ensure no mechanical cause Manage symptoms Manage nutrition & fluid balance Address psychological issues Avoid opiates Avoid parenteral addictive medication Avoid surgery

Gastroparesis Common in neuropathic & myopathic CIPO
De Georgio et al, Gastroenterol Clin North Am 2011;40:787-807

Gastric pacemakers Diabetic gastroparesis
Used to be the main indication No longer funded by the NHS
Dysmotility patients Gastroparesis unlikely to occur
without small bowel involvement
Not a modality that we currently recommend

Venting PEG / gastrostomy Can be very helpful for symptom minimisation Trial of venting NG before placing a PEG But, there are some common issues Drainage dependent on
Tube factors (tube gauge, male Luer connection) Position of the tube in the stomach Place low in the body of the stomach Siting can be a challenge

We need better venting PEG tubes - Currently designed for feeding - Need to develop the ideal tube

Jejunal feeding
NJ PEGJ
Surgical jejunostomy Direct PEJ

Surgical or endoscopic? Surgical jejunostomy Direct PEJ
Laparoscopic possible More invasive Surgical procedure to
remove Tube has more limited
lifespan
Endoscopic procedure under GA
Less invasive Can be removed
endoscopically Tube lasts longer

Click to edit Master title style Do not place a Foley catheter!

There is a need for better jejunal feeding tubes to be developed

Psychology
There are almost always significant past issues Childhood abuse Disturbed childhood or young adult life Trauma: PTSD
If you only deal with the physical problems you are only dealing with half the issues WILL FAIL

Nutrition support Patients are often malnourished Cause: inadequate food intake > malabsorption
Oral nutrition
• Low fat & low fibre diet
• Liquid diet
Enteral nutrition
• NG trial • NJ trial • PEGJ (medium term) • Jejunostomy (long term)
Parenteral nutrition
• Usually supportive (IVN) • allows patients to eat
as tolerated • Occasionally exclusive
(TPN)

IV nutrition Helpful to overcome nutritional consequences Rarely helpful for symptoms Tell patients Their symptoms will be the same IVN will only address the undernutrition Significant risk of infection, especially if on opiates
Beware Underlying eating disorders (can become more apparent when trying to give IVN)

BAPEN: data from BANS
Patients 2000 2005 2010 2011 2012 2013 Numbers 32 66 79 87 137 152 % 9.1 10.4 15.1 14.2 15.4 14.0
% New registrations % Point prevalence 2000 2013 2000 2013
Crohns 25.0 16.1 34.3 22.3 Ulcerative colitis 3.4 2.1 2.9 3.3 Ischaemia* 14.8 10.4 17.7 15.0 Radiation enteritis 5.7 2.8 5.1 2.6 Pseudo-obstruction 4.5 10.0 9.1 14.0 Cancer 17.0 24.6 5.7 11.2
IF due to dysmotility is on the increase

Summary tips Work as a team
Be patient, listen and try your best to help
Boundaries can be essential Make the boundaries clear Can compromise on some issues
Involve the psychologists/psychiatrists Just as important for you as for the patient!

Intestinal transplantation Indications Refer / discuss
Irreversible IF, and
Liver disease Fibrotic liver disease Progressive IFALD
Severe sepsis Life threatening (>1) Life threatening (1)
Loss of venous access
Limited to 3 major sites Limited to 4 major sites
Poor QOL Correctable by transplantation
Correctable by transplantation
Partial or complete evisceration Evisceration requiring MVTx (eg desmoid)
Strategies to minimise surgical resection
Need for other abdominal organ transplant
eg renal When transplant being considered