chronic kidney disease: beyond nephrology
TRANSCRIPT

David C Wheeler
Chronic Kidney Disease: Beyond Nephrology
Advanced Medicine 2017
16th February 2017
RCP London

Kidney dysfunction: terminology
Acute kidney injury (AKI) (formerly known as acute renal failure)
• Sudden deterioration in renal function with potential to recover.
Chronic kidney disease (CKD) (formally known at chronic renal failure)
• Slow irreversible deterioration of kidney function over time usually without symptoms until damage is advanced.
The history of CKD in the UK
• 2005 Renal National Service Framework
• 2007 Standardisation of creatinine measurements
• 2007 Mandatory eGFR reporting
• 2008 NICE CKD Guideline
• 2008 Quality Outcomes Framework
• 2010 Quality Outcomes Framework update
• 2014 NICE CKD Guideline updated
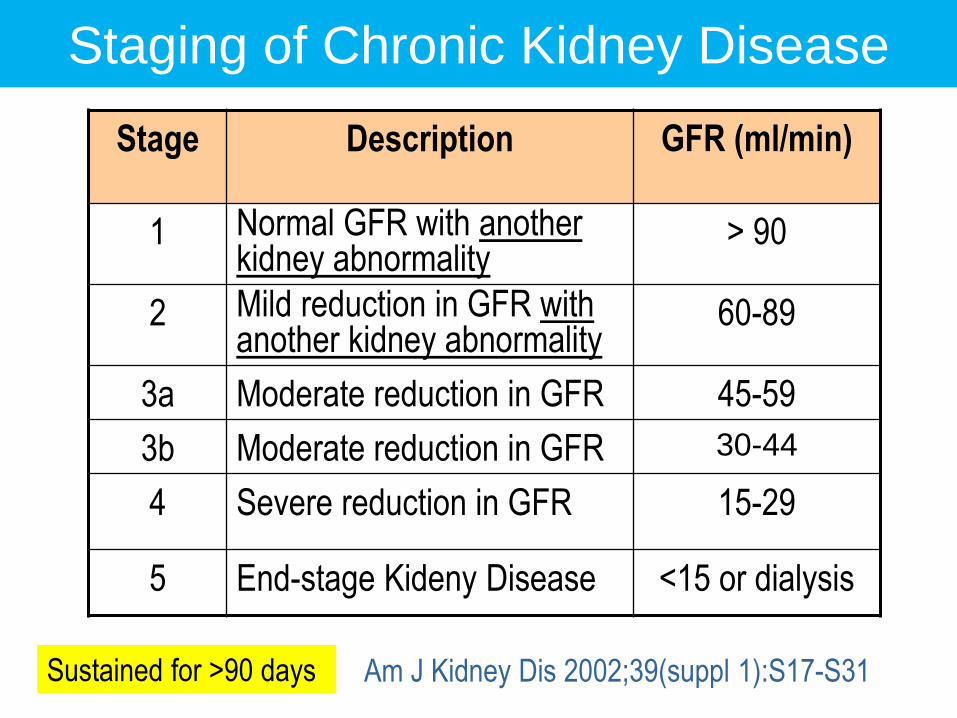
Stage Description GFR (ml/min)
1 Normal GFR with another kidney abnormality
> 90
2 Mild reduction in GFR with another kidney abnormality
60-89
3a Moderate reduction in GFR 45-59
3b Moderate reduction in GFR 30-44
4 Severe reduction in GFR 15-29
5 End-stage Kideny Disease <15 or dialysis
Am J Kidney Dis 2002;39(suppl 1):S17-S31
Staging of Chronic Kidney Disease
Sustained for >90 days
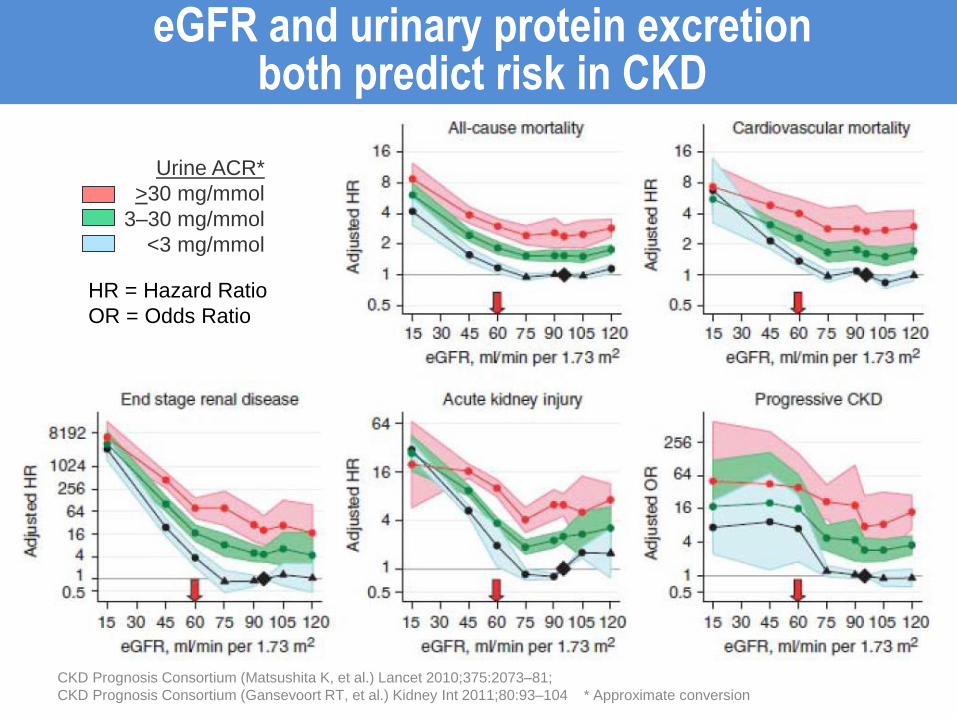
eGFR and urinary protein excretion both predict risk in CKD
Urine ACR*
>30 mg/mmol
3–30 mg/mmol
<3 mg/mmol
CKD Prognosis Consortium (Matsushita K, et al.) Lancet 2010;375:2073–81;
CKD Prognosis Consortium (Gansevoort RT, et al.) Kidney Int 2011;80:93–104 * Approximate conversion
HR = Hazard Ratio
OR = Odds Ratio
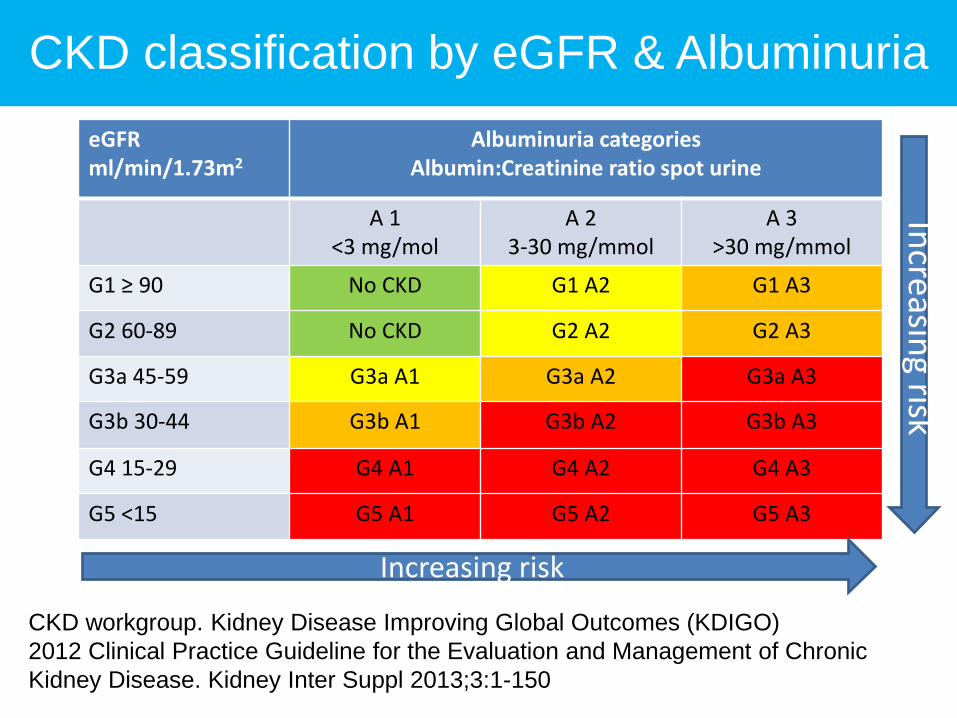
CKD classification by eGFR & Albuminuria
eGFR ml/min/1.73m2
Albuminuria categories Albumin:Creatinine ratio spot urine
A 1 <3 mg/mol
A 2 3-30 mg/mmol
A 3 >30 mg/mmol
G1 ≥ 90 No CKD G1 A2 G1 A3
G2 60-89 No CKD G2 A2 G2 A3
G3a 45-59 G3a A1 G3a A2 G3a A3
G3b 30-44 G3b A1 G3b A2 G3b A3
G4 15-29 G4 A1 G4 A2 G4 A3
G5 <15 G5 A1 G5 A2 G5 A3
CKD workgroup. Kidney Disease Improving Global Outcomes (KDIGO)
2012 Clinical Practice Guideline for the Evaluation and Management of Chronic
Kidney Disease. Kidney Inter Suppl 2013;3:1-150
Increasing risk
Increasin
g risk

A success in the fight against renal failure
“An eGFR will now become as much part of the GP’s medical check as a patient’s haemoglobin, blood count, blood sugar, cholesterol levels and, of course, their blood pressure.”
24 July 2006
THE TIMES

Who looks after CKD patients (UK)?
Primary Care Nephrology Other
secondary
care
CKD 3 84.6 1.6 13.9
CKD 4 57.2 28.8 14.0
CKD 5 19.8 70.0 10.1
% of total by stage
Data from NHS England

Points Payment
Stages
A register of patients aged 18 and
older with CKD stages 3-5
6
Percentage of patients with a record
of blood pressure in the previous 15
months
6 40-90%
Percentage of patients with BP of
140/85 mmHg or less
11 40-70%
Percentage of patients who are
treated with an ACEi or ARB
4 40-80%
The CKD domain of the Quality Outcomes Framework (QOF)
NHS Information Centre

Impact of eGFR Reporting on Referrals:
Lincolnshire Primary Care Trust
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Patient num
bers
10
20
30
40
50
60
70
80
90
eGFR reporting
2004 2006 2005

May 11th, 2006
GPs Shoulder the Burden of CKD

NICE 2014: Referral to Kidney Doctors
• eGFR < 30ml/min with or without diabetes. • ACR 70 mg/mmol or more, unless known to be caused
by diabetes and already appropriately treated. • Sustained ↓ GFR of 25% or more and a change in GFR
category or sustained ↓ GFR of 15 ml/min/1.73 m² or more.
• ↓ eGFR of >25% after starting ACEi or ARB. • Hypertension that remains poorly controlled despite
the use of at least 4 antihypertensive drugs at therapeutic doses.
• Known or suspected rare or genetic causes of CKD • Complications of CKD • Suspected renal artery stenosis.

NICE 2014: Suggested Frequency of monitoring
GFR Category
GFR mL/min/1.73m2
GFR Description
Frequency of monitoring eGFR (times per year)
A1 A2 A3
G1 ≥90 Normal or high ≤ 1 1 ≥1
G2 60-89 Mildly decreased ≤ 1 1 ≥1
G3a 45-59 Mildly to Moderately decreased
1 1 2
G3b 30-44 Moderately to severely decreased
≤ 2 2 ≥2
G4 15-29 Severely decreased 2 2 3
G5 <15 Kidney failure 4 ≥ 4 ≥ 4
ACR Categories: A1 (normal to mildly increased) < 3 mg/mmol, A2 (moderately increased) 3-30 mg/mmol, A3 (severely increased) > 30 mg/mmol

Stage GFR Test frequency
Tests required
1 >90 12/12 U&E, Creatinine, UACR
2 60-89 12/12 U&E, Creatinine, UACR
3 30-59 6/12 U&E, Cr, UACR, FBC, PTH
4 15-29 3/12 U&E, Cr, UACR,
bicarbonate, Ca, PO4, FBC,
PTH 5 <15 3/12
http://www.renal.org/eGFR/eguide.html
Monitoring CKD

Case history 1
• 68 year old female with osteoporosis
• BP 140/80 mmHg on Irbesartan 75 mg od
• Urea 5.5 mmol/l, Creatinine 120 mmol/l
• eGFR = 46 ml/min/1.73m2

• 48 year old afrocaribbean male
• History of hypertension and haematuria
• Presents in pulmonary oedema
• eGFR <15 ml/min/1.73m2
• Urinary albumin:creatinine ratio 320 mg/mmol
• 8.5 cm right kidneys on ultrasound scan
• Central line and emergency dialysis
Case History 2
So what use are nephrologists in management of patients with CKD?
• Diagnosis of cause of CKD
• Management of complications of CKD
• Preparation for dialysis
• Preparation for kidney transplantation
• Palliative care for end-stage chronic kidney disease
Case history 3
• 27 year old male (82 kg)
• Ankle swelling, BP 130/80 mmHg
• Urea 4.5 mmol/l, Creatinine 84 mmol/l
• eGFR = 116 ml/min
• Dipstix positive for protein +++
• ACR 1024 mg/mmol

Kidney Biopsy

Case history 4
• 67 year old male
• Smoker, overweight, type 2 diabetes 10 years
• Breathless on exertion
• 3/52 ankle swelling
• Creatinine 210 mmol/l
• eGFR 28 ml/min/1.73m2 (NR>90)
Case history 4
• 67 year old male
• Smoker, overweight, type 2 diabetes 10 years
• Breathless on exertion
• 3/52 ankle swelling
• Creatinine 210 mmol/l
• eGFR 28 ml/min/1.73m2 (NR>90)
• Previous biochemical tests
• HbA1c, Blood pressure
• Dipstix: protein ++
• Urine test: ACR 24 mg/mmol (NR<3)
• Renal tract ultrasound scan
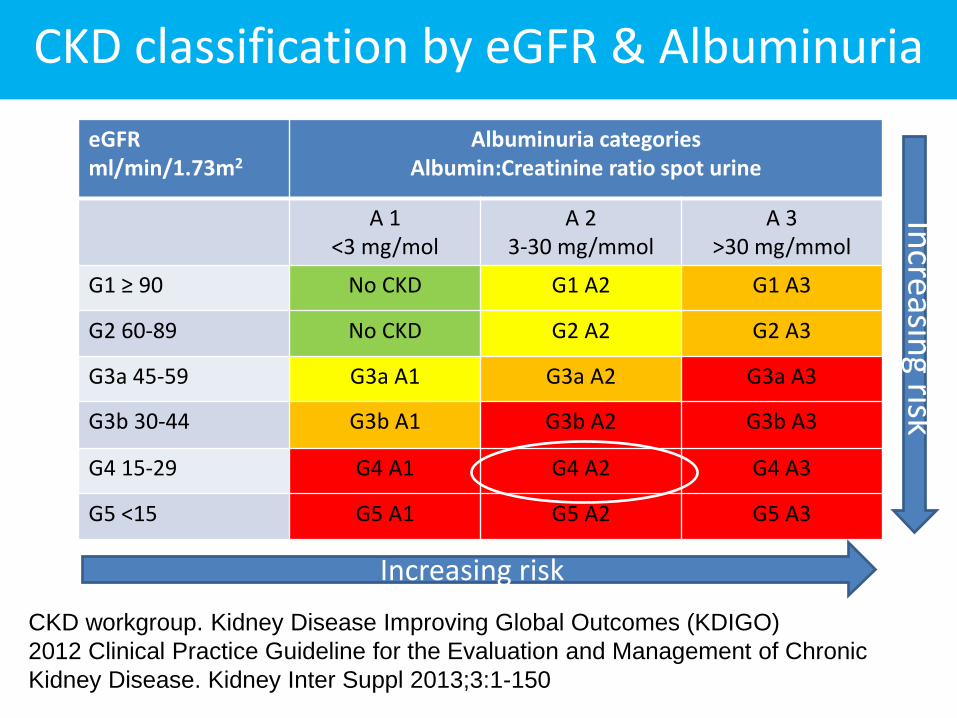
CKD classification by eGFR & Albuminuria
eGFR ml/min/1.73m2
Albuminuria categories Albumin:Creatinine ratio spot urine
A 1 <3 mg/mol
A 2 3-30 mg/mmol
A 3 >30 mg/mmol
G1 ≥ 90 No CKD G1 A2 G1 A3
G2 60-89 No CKD G2 A2 G2 A3
G3a 45-59 G3a A1 G3a A2 G3a A3
G3b 30-44 G3b A1 G3b A2 G3b A3
G4 15-29 G4 A1 G4 A2 G4 A3
G5 <15 G5 A1 G5 A2 G5 A3
CKD workgroup. Kidney Disease Improving Global Outcomes (KDIGO)
2012 Clinical Practice Guideline for the Evaluation and Management of Chronic
Kidney Disease. Kidney Inter Suppl 2013;3:1-150
Increasing risk
Increasin
g risk

Causes of Chronic Kidney Disease
• Diabetes Mellitus
• Idiopathic glomerulonephritis
– Focal segmental glomerulosclerosis
– IgA nephropathy
– Membranous nephropathy
• Ischaemic Nephropathy
• Renal dysplasia/Urosepsis
• Systemic diseases (SLE, Vasculitis)
• Genetic Diseases (ADPKD, Alport’s)
• Unknown cause

High blood pressure and CKD
“Hypertension” in usually the consequence of CKD, not the cause
Why does CKD cause hypertension? • Fluid retention • Activation of renin-angiotensin system • Increase sympathetic activity • Endogenous toxins

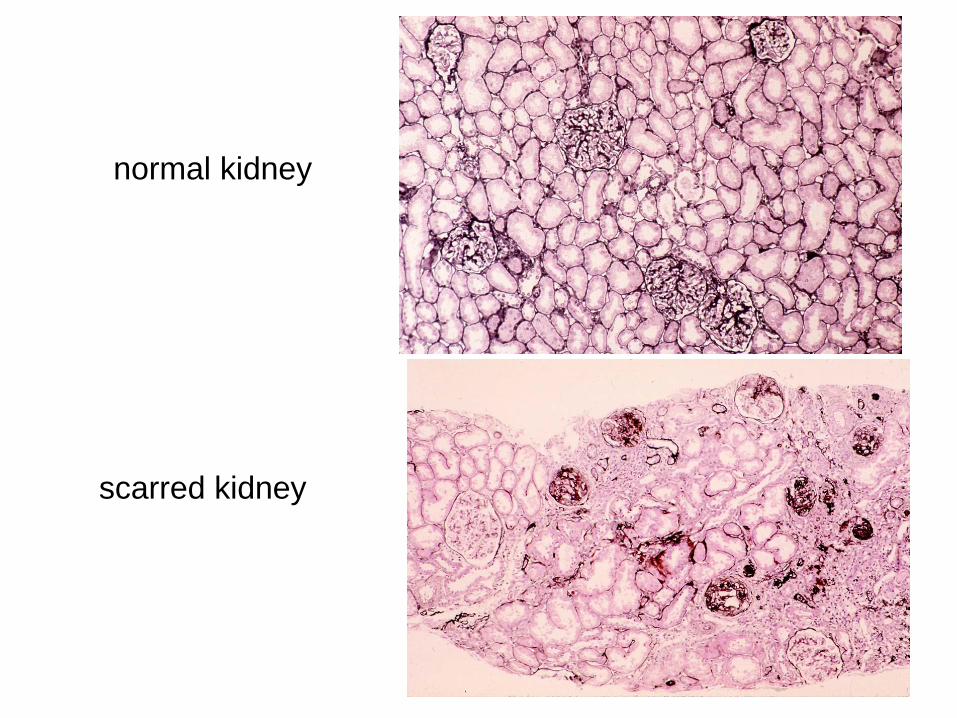
normal kidney
scarred kidney
Tests for unexplained CKD
• Renal tract ultrasound scan
• Prostatic specific antigen
• Protein electrophoresis + serum light chains
• Viral screen (HIV, Hep C)
• Autoantibody screen (dsDNA, ANCA, anti-
glomerular basement membrane)
• Bone disease
Complications of Chronic Kidney Disease
• Fluid retention
• Metabolic acidosis
• High blood pressure
• Normochromic Normocytic Anaemia
• Secondary Hyperparathyroidism
• Bone disease

Medical Management of Chronic Kidney Disease
• Diuretic therapy
• Antihypertensive medication
• Oral sodium bicarbonate
• Phosphate binders
• Active vitamin D analogues (alfacaclcidol)
• Calcimimetics
• Erythropoiesis stimulating agents (ESAs)

End-Stage
Kidney
Disease
Kidney Biopsy
US Scans
Immunotherapy
Chronic
Kidney
Disease
(CKD)
Stage 1 to
Stage 4
CKD
Conservative/
Palliative care
Renal replacement
therapy (RRT)*
Haemodialysis*
Peritoneal
dialysis*
Transplantation*
Chronic Kidney Disease: The Patient Journey
Blood Pressure
Fistula
Cardiac Tests
Live donor workup
Anaemia
Acidosis
Death with chronic kidney disease

Framework for understanding the patient with kidney disease.
• What is the eGFR and the ACR
• Is the cause of chronic kidney disease known and can it be treated?
• Where is the patient on their journey?
• If CKD is progressing is blood pressure controlled?
• If albuminuria present, is patient on ACE/ARB?
• Is it time to prepare patients for renal replacement therapy of palliative management of end-stage kidney disease?

• CKD is a common syndrome with a prevalence of
approximately 5% in primary care
• Classified by both eGFR and urinary Alb:Cr ratio
• Underlying causes should be considered but a
histological diagnosis is rarely required
• Blood pressure control is the mainstay of therapy
• ACE/ARBs preferred if albuminuria
• Patients should be offered statins and vaccinations
• If progression, early referral improves prognosis
http://www.renal.org/eGFR/eguide.html
Take home messages