chronic myelogenous leukemia: disease biology and current...
TRANSCRIPT

90 American Society of Hematology
Chronic Myelogenous Leukemia: Disease Biology andCurrent and Future Therapeutic Strategies
Hagop Kantarjian (Chair), Junia V. Melo, Sante Tura, Sergio Giralt, and Moshe Talpaz
Over the last 2 decades, four major therapeuticapproaches have drastically changed the progno-sis in chronic myelogenous leukemia (CML): 1)allogeneic stem cell transplant (SCT); 2) interferonalpha (IFN-�����) based regimens; 3) donor lymphocyteinfusions (DLI); and 4) and the revolutionary BCR-ABL tyrosine kinase inhibitors such as STI571(signal transduction inhibitor 571). Each modalityhas exploited and targeted different aspects of CMLbiology, and is associated with different risk-benefitratios.
In Section I of this review, Dr. Melo reviews themolecular pathophysiology of CML and potentialnew targets for therapy including anti-sensestrategies to disrupt the BCR-ABL gene andinhibition of the BCR-ABL tyrosine kinase activity.
In Section II, Dr. Tura, addresses importantquestions in the use of IFN-� � � � � for the treatment ofCML, including the mechanism of action and thedevelopment of resistance, the optimal dose andduration of therapy and the prediction of responsebased on clinical features. An approach to thechoice of therapy based on the predicted mortalityis presented.
In Section III Dr. Giralt presents an update onthe results of unrelated donor transplantion, donorlymphocyte infusions (DLI) and non-ablative stemcell transplantation (NST) in CML. The roles of CD8-depletion, dose escalation and the transduction of
suicide genes in treatment with DLI are addressed.Early results of NST in CML show that it is feasibleand can result in long-term disease control.
In Section IV Drs. Kantarjian and Talpaz reviewthe results of IFN-����� plus low-dose cytosine arabino-side and other promising modalities for CMLincluding homoharringtonine, decitabine, andpolyethylene glycol-interferon. In Section V theypresent an update on the recent experience withSTI571. Objective but transient responses havebeen seen in 40% to 50% of patients in CML blasticphase. In accelerated phase, the response rate withSTI571 exceeds 70%, and these responses aredurable. In chronic phase CML, STI571 at 300 mgdaily in patients who failed IFN-����� produces acomplete hematologic response (CHR) in over 90%of patients. Early results suggest cytogeneticresponse rates of approximately 50%, which may bemajor in approximately 30%. The maturing resultswith STI571 may soon change current recommen-dations regarding the relative roles of establishedmodalities such as allogeneic SCT and IFN-�����.Important questions include 1) whether STI571therapy alone may be sufficient to induce long-termsurvival and event-free survival in CML, or whetherit needs to be combined simultaneously or sequen-tially with IFN-����� and cytosine arabinoside; and 2)what should the indications for frontline allogeneicSCT be in relation to STI571 therapy.
* Department of Hematology–RPMS, Hammersmith Hospital,Ducane Road, London W12 0NN, UK
I. CML: MOLECULAR PATHOPHYSIOLOGY AND
POTENTIAL NEW TARGETS FOR THERAPY
Junia V. Melo, M.D., Ph.D.*
CML was the first neoplastic process to be linked to aconsistent acquired genetic abnormality, and it is by nowthe best studied molecular model of leukemia. Thisknowledge, together with the availability of sophisticatedbiochemical and biophysical technology, offers a uniqueopportunity to develop rational molecularly targetedtherapies for this leukemia.
The Molecular Pathophysiology of CMLThe crucial genetic event in CML is the generation of at(9;22)(q34;q11) reciprocal chromosomal translocationin a hematopoietic stem cell. This translocation createstwo new genes, BCR-ABL on the 22q- or Ph chromo-some, and the reciprocal ABL-BCR on the derivative 9q+.The latter gene, although transcriptionally active,1 does notappear to have any functional role in the disease.
Hematology 2000 91
tional analyses have identified several features or domainsin the Bcr-Abl fusion protein that are essential for cellu-lar transformation. In the Abl moiety they include theSH1 (tyrosine kinase), SH2 and actin-binding domains,and in the Bcr portion a coiled-coil oligomerization do-main contained in amino acids (aa) 1–63, the tyrosine atposition 177 and phosphoserine/threonine rich sequencesbetween aa 192–242 and 298–413.
A large number of substrates can be phosphorylatedby Bcr-Abl (Figure 2). Due to autophosphorylation thereis a marked increase of phosphotyrosine on Bcr-Abl it-self, which creates binding sites for the SH2 domains ofother proteins. Generally, substrates of Bcr-Abl can begrouped according to their physiological role into adap-tor molecules (such as Grb-2, Crkl and Dok), proteinsassociated with the organization of the cytoskeleton andthe cell membrane (such as paxillin, talin and Fak) and athird group of proteins with catalytic function (such asthe non-receptor tyrosine kinase Fes, PI-3 kinase and thephosphatase Syp). The choice of substrates depends onthe cellular context. For example, Crkl is the major ty-rosine phosphorylated protein in CML neutrophils,whereas phosphorylated Dok is predominantly found inearly progenitor cells.
The signalling network controlled by Bcr-Abl is com-plex and highly redundant (Figure 2). The sum of theseprotein interactions translates into the altered phenotypeof CML cells, which consists of constitutively activemitogenic signalling, defective adherence to stromal cellsand extracellular matrix, and reduced response to apopto-sis-inducing stimuli. ‘Correction’ of any of these defectsby a rationally designed therapeutic tool would very likelytip the balance towards the re-establishment of normalhematopoiesis.
Possible Levels of Intervention
Prevention of CMLPrevention of CML would be better than cure. Unfortu-nately, except for its association with previous exposureto high-dose ionizing radiation, no significant risk factorhas been associated with the development of CML. Re-cent studies on the mechanisms of leukemia-associatedchromosomal translocations have shown that BCR-ABL,as well as other transcriptionally functional genes, is gen-erated spontaneously in hematopoietic cell lines in cul-ture9 and, even more importantly, in circulating normalleukocytes from healthy adults.10,11 This low level of back-ground translocations is part of the intrinsic instability ofthe human genome, and is not currently preventable.
In theory, one could prevent the development of CMLby attempting to increase the immunological surveillanceagainst BCR-ABL-containing cells through vaccinationwith Bcr-Abl peptides (see below). Because of the low
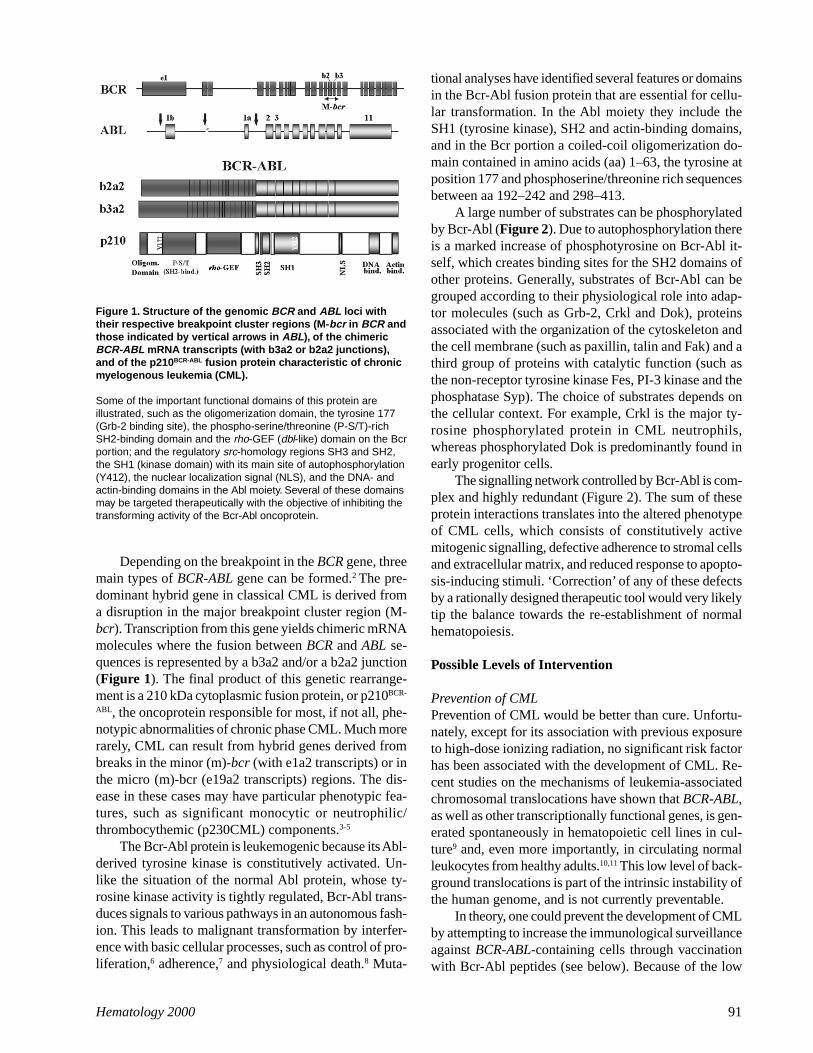
Depending on the breakpoint in the BCR gene, threemain types of BCR-ABL gene can be formed.2 The pre-dominant hybrid gene in classical CML is derived froma disruption in the major breakpoint cluster region (M-bcr). Transcription from this gene yields chimeric mRNAmolecules where the fusion between BCR and ABL se-quences is represented by a b3a2 and/or a b2a2 junction(Figure 1). The final product of this genetic rearrange-ment is a 210 kDa cytoplasmic fusion protein, or p210BCR-
ABL, the oncoprotein responsible for most, if not all, phe-notypic abnormalities of chronic phase CML. Much morerarely, CML can result from hybrid genes derived frombreaks in the minor (m)-bcr (with e1a2 transcripts) or inthe micro (m)-bcr (e19a2 transcripts) regions. The dis-ease in these cases may have particular phenotypic fea-tures, such as significant monocytic or neutrophilic/thrombocythemic (p230CML) components.3-5
The Bcr-Abl protein is leukemogenic because its Abl-derived tyrosine kinase is constitutively activated. Un-like the situation of the normal Abl protein, whose ty-rosine kinase activity is tightly regulated, Bcr-Abl trans-duces signals to various pathways in an autonomous fash-ion. This leads to malignant transformation by interfer-ence with basic cellular processes, such as control of pro-liferation,6 adherence,7 and physiological death.8 Muta-
Figure 1. Structure of the genomic BCR and ABL loci withtheir respective breakpoint cluster regions (M-bcr in BCR andthose indicated by vertical arrows in ABL), of the chimericBCR-ABL mRNA transcripts (with b3a2 or b2a2 junctions),and of the p210BCR-ABL fusion protein characteristic of chronicmyelogenous leukemia (CML).
Some of the important functional domains of this protein areillustrated, such as the oligomerization domain, the tyrosine 177(Grb-2 binding site), the phospho-serine/threonine (P-S/T)-richSH2-binding domain and the rho-GEF (dbl-like) domain on the Bcrportion; and the regulatory src-homology regions SH3 and SH2,the SH1 (kinase domain) with its main site of autophosphorylation(Y412), the nuclear localization signal (NLS), and the DNA- andactin-binding domains in the Abl moiety. Several of these domainsmay be targeted therapeutically with the objective of inhibiting thetransforming activity of the Bcr-Abl oncoprotein.

92 American Society of Hematology
frequency of CML, the cost-effectiveness of such under-taking would be unacceptable, unless a specific group ofindividuals at higher risk of developing CML could beidentified.
Disruption of BCR-ABLOnce a ‘successful’ t(9;22) is perpetuated in an expand-ing clone of hematopoietic cells, chronic phase CMLdevelops. At this stage, the only known identified geneticabnormality is the BCR-ABL gene itself, although otheras yet unidentified mutation(s) may have preceded andfacilitated the emergence of the BCR-ABL-containingclone. The BCR-ABL gene and its cognate mRNA andfusion protein are in principle ideal targets for disruptionin an attempt to remove the neoplastic machinery of theleukemia cells. Strategies aimed at blocking BCR-ABLat different levels of expression are at the forefront ofcurrent investigations.
Disruption of the Bcr-Abl-associated pathwayAn alternative to neutralizing Bcr-Abl would be to targetproteins that are directly or indirectly modulated by Bcr-
Abl in its various oncogenic pathways. Since the effectsof Bcr-Abl are multifactorial, inhibition of one pathwaymay not be sufficient to abrogate effectively the malig-nant phenotype.
Molecularly Designed StrategiesMolecularly designed strategies, which are based on ourcurrent knowledge of the molecular and cell biology ofCML, have concentrated on three main areas: (a) inhibi-tion of gene expression at the translational level by‘antisense’ strategies; (b) modulation of protein functionby specific signal transduction inhibitors; and (c) stimu-lation of the immune system’s capacity to recognize anddestroy the leukemic cells.
Antisense strategiesAntisense RNA and DNA oligonucleotides (ODNs) tar-geted against nuclear genomic DNA or cytoplasmicmRNA, synthetic DNA transcription factor ‘decoys,’ribozymes (catalytic RNA molecules)12 and DNA-bind-ing proteins have all been employed as tools for target-ing genetic defects in CML cells.13 In the traditional ap-
Figure 2. Pathways involved in Bcr-Abl signalling.
A large number of Bcr-Abl substrates and associated proteins have been identified, a selection of which are shown here. For some ofthese both the active (solid) and the inactive (punctuated) forms are illustrated. Inhibition of individual pathways by targeting proteinsdownstream of Bcr-Abl (e.g. Grb-2, Ras, PI-3 kinase) may be effective to suppress individual aspects of the CML cell phenotype, althoughthe redundancy of the system may work against the therapeutic success of such strategies.

Hematology 2000 93
proach, the exogenous nucleotide sequence hybridizesto the target mRNA creating a duplex that in effect formsa ‘jam’ that prevents the ribosomal complex from read-ing along the message. The antisense strategies receivedmuch attention in the last decade but, due to a number oftechnical problems, have in general failed to fulfill theirtheoretical promises (recently reviewed in reference 14).New modifications to the system, however, such as theuse of BCR-ABL junction-specific catalytic subunits ofRNase P may revitalise the field.15
Although BCR-ABL may in theory be the most at-tractive target for antisense therapy, the long half life (inexcess of 24 hours) of its protein poses a significant ob-stacle. This led some investigators to investigate antisenseODNs against downstream targets of Bcr-Abl, such asMYC, CRKL, GRB2, KIT, VAV and MYB. Of these, onlyanti-MYB ODNs have been tested in clinical trials, butlong-term follow-up results of these trials have not beenreported.16
Signal transduction inhibitorsIf translation of Bcr-Abl and related proteins cannot beadequately halted by an antisense technology, the nextlevel for molecular intervention is to block protein func-tion. Preventing a protein from exerting its role in theoncogenic pathway should ultimately lead to eliminationof the leukemic phenotype.
The development of signal transduction inhibitors(STIs) has evolved in close parallel to the unravelling ofthe biochemical properties of proteins involved in the sig-nalling network in hematopoietic cells. These inhibitorsusually target a specific functional domain of a protein.As with the antisense technology, the ideal STI for thetreatment of CML should be able to block the Bcr-Ablfusion protein itself, as this would limit its ‘damaging’effects (e.g. anti-proliferative, pro-apoptotic, enhance-ment of cell adherence) to the cell clone that needs to be‘damaged.’ In practice, though, inhibition of selected Bcr-Abl-associated proteins may be just as effective in dis-rupting the oncogenic process in the leukemia cell, withlittle or no adverse consequence to the normal tissueswhere the given protein is expressed under physiologicalcontrol.
a) Inhibitors of the Bcr-Abl fusion protein: Since themain transforming property of Bcr-Abl is exerted throughits constitutive tyrosine kinase activity, direct inhibitionof such activity seems to be the most logical means of‘silencing’ the oncoprotein. To this effect, several tyrosinekinase inhibitors have been evaluated for their potentialto modify the phenotype of CML cells. The first to betested were compounds isolated from natural sources,such as the isoflavonoid genistein and the antibioticherbimycin A.17 Later, synthetic compounds known astyrphostins were developed through a rational design of
chemical structures capable of competing with the ATPor the substrate for the binding site in the catalytic centerof the kinase.18
One of these tyrphostins (AG1112), genistein, andherbimycin A were variably reported to inhibit thep210BCR-ABL tyrosine kinase, to induce differentiation ofthe K562 CML cell line and to inhibit the in vitro growthof some BCR-ABL-positive cell lines. Genistein has alsobeen shown to exert a strong anti-proliferative effect onCML colony-forming progenitor cells, whereas AG957was observed to restore �1-integrin-mediated adhesionand inhibitory signalling in CML progenitors.
So far, the most successful of the molecularly de-signed ATP competitors is the 2-phenylaminopyrimidineSTI571 (previously known as CGP57418B), fromNovartis Pharma (Basel, Switzerland), which specificallyinhibits Abl tyrosine kinase at submicromolar concen-trations.19 Inhibition of the Bcr-Abl kinase activity by thiscompound results in transcriptional modulation of vari-ous genes involved in the control of the cell cycle, celladhesion and cytoskeletal organization, leading the Ph-positive cell to an apoptotic death.20 STI571 selectivelysuppresses the growth of CML primary cells and cell linesboth in vitro and in mice.21-23 As described later in thisreview, this compound is now being tested in several clini-cal trials, with exceptionally good results.
To anticipate and possibly overcome CML resistanceto STI571, investigators have generated murine and/orhuman BCR-ABL-positive cell lines resistant to STI571.These have shown that the most frequent mechanism ofresistance is amplification and overexpression of the BCR-ABL gene.24 Overexpression of the Pgp glycoprotein, theproduct of the multidrug resistance (MDR) gene, mayalso contribute to the resistant phenotype. However,STI571-resistant clones from some cell lines, e.g. KCL22,do not show either of these resistance phenotypes, sug-gesting that resistance to STI571 may evolve by multiplemechanisms. Patients in lymphoid blast crisis have a rapidand significant response to treatment with STI571 butrelapse after a median time of 10.5 weeks. It will be im-portant to study the causes of resistance in these primaryCML cells, in order to design modifications to the treat-ment. It is possible that combinations of STI571 withother drugs such as interferon-� (IFN-�), daunorubicinor cytosine arabinoside (ara-C) may be more effectivethan STI571 alone, as suggested by in vitro studies ofcell lines and primary CML cells.25
Two possible molecular side effects of Abl tyrosinekinase inhibitors should be kept in mind. The first are theconsequences of inhibition of the normal Abl kinase ac-tivity, which may be related to the regulation of cell pro-liferation and lymphoid development and, if suppressed,may diminish cellular immunity. Bcr-Abl/Abl tyrosinekinase inhibitors may also inhibit other tyrosine kinases,

94 American Society of Hematology
namely the PDGF receptor and the steel factor receptor(c-kit), potentially interfering with normal cellular func-tions. The negligible degree of side effects observed inthe STI571 clinical trials so far suggests that if suppres-sion of the normal Abl and other tyrosine kinases occurs,it may be compensated by activation of alternative path-ways.
In addition to the tyrosine kinase, inhibition of otherrelevant domains of p210BCR-ABL may have a negative ef-fect on the survival and proliferative potential of Ph-posi-tive cells. Candidates for manipulation are the Bcr oligo-merization domain and the Abl SH2 and actin-bindingdomains. Inhibitors being tested are short peptides de-signed to be homologous to all or part of a given domain,which compete with p210BCR-ABL for ligands or substratesimportant for the transforming capacity of the full-lengthprotein. These inhibitors are administered to the cell ei-ther via transfection of a recombinant expression vectorencoding the designed peptide, or as a synthetic drugacting as a peptidomimetic.26 Arlinghaus and co-work-ers27 have shown that adenovirus-mediated transfer of amutant Bcr 64-413 (containing the first exon minus theoligomerization domain) into the K562 and BV173 CMLcell lines inhibited Bcr-Abl kinase activity and colonyformation. Introduction of this Bcr fragment into bonemarrow cells from a CML patient suppressed their prolif-eration in suspension culture and promoted their adhesionto the culture flask, suggesting that this treatment may cor-rect some aspects of the CML phenotype.
b) Inhibitors of other signal transduction proteins:The use of farnesyl transferase inhibitors (FTIs) againstBCR-ABL-induced leukemias is starting to gain momen-tum. The rationale for this strategy was again based onthe notion that Bcr-Abl signals via activation of the Ras/MAPK pathway. In order to be activated, the Ras proteinhas to be anchored to the cytoplasmic face of the plasmamembrane through a covalently attached prenyl (usuallya farnesyl) group. FTIs inhibit the 3-hydroxymethyl-glutaryl-coenzyme A reductase, an early and rate-limit-ing enzyme in the sterol synthesis pathway, thus deplet-ing the cell of farnesyl pyrophosphate. Although it wasinitially thought that the anti-proliferative capacity ofsome FTIs was due to reduced post-translationalfarnesylation of Ras and consequent prevention of itsmembrane localization, it appears that other mechanisms,such as the gain of geranylgeranylated Rho-B, are alsoinvolved. It should be emphasized that current FTIs maynot inhibit farnesylation of ras, or ras itself, although theymay inhibit CML proliferation through other potentialmechanisms. Encouraging preliminary results have beenreported on inhibition of in vitro proliferation of ALLand juvenile myelomonocytic leukemia cells by thesecompounds.28 Investigations on the effect of FTIs in BCR-ABL-positive cells are warranted.
Another promising approach is the use of PI-3 ki-nase inhibitors. PI-3 kinase functions downstream of Bcr-Abl may involve both apoptosis and control of cytoskel-eton organization. Treatment of BCR-ABL transfected celllines with wortmannin, a potent PI-3 kinase inhibitor,normalizes their pattern of stress fibers and focal adhe-sion contacts and decreases their excessive spontaneousmotility. When tested on CML cell lines and primary bonemarrow CD34+ cells, wortmannin led to suppression ofcolony formation, with apparently no effect on colonyformation by normal CD34+ cells.29 The next step is totest the efficacy and in vivo toxicity of the PI-3 kinaseinhibitors in animal models of CML.
Immunological stimulationThe capacity of donor lymphocyte infusions (DLI) toinduce complete remission, without cytotoxic chemo-therapy, in a high proportion of patients who relapse af-ter SCT is probably the best evidence for the role of theimmunological pathway in CML. The mechanism is likelyto be, at least in part, related to cytotoxic T cell lympho-cytes (CTLs) that recognise CML targets. Major effortshave been devoted for the past 5 years to establishing anefficient strategy to enhance CML-specific T cell-medi-ated immunity.
In the post-allogeneic stem cell transplant setting,CTLs of donor origin can be generated in vitro whenmixed with the recipient’s leukemic cells.30 The stimu-lant in this case is either a leukemia-associated antigen(e.g. a product of the p210BCR-ABL or a proteinase 3 pep-tide)31 or minor histocompatibility antigens.32 Whateverthe antigenic specificity, CTLs recognize targets in thecontext of major histocompatibility complex (MHC). Themain obstacles in the development of CTL clinical pro-tocols are the difficulties in generating specific lines orclones that can be expanded in vitro to the large quanti-ties needed for effective therapy. Furthermore, the require-ment for CTLs to be self-MHC restricted implies thatnot all patients would be eligible for this form of treat-ment.
An ingenious strategy has been recently tested forraising CTL against the Wilms’ tumor (WT1) antigen,which is reported to be preferentially expressed in CML,as compared to normal CD34+ cells.33 In this case, WT1peptide-specific CTL clones isolated from HLA-A0201-or HLA-A24-negative donors were able to kill leukemiccell progenitors from the respective HLA-A-positivecounterpart patients, suggesting that selection of suchlymphocytes for CTL adoptive immunotherapy may beused in a one-locus HLA-mismatch transplant protocol.
It is not yet clear how easily CTLs can be raised inthe autologous setting. The fact that a clone of BCR-ABL-positive cells was allowed to expand and produce the dis-ease in the first place suggests that some form of toler-

Hematology 2000 95
ance to the abnormal cells or immunosuppression mustoccur in these patients.
A new approach to induce a CTL response is to pulseaccessory cells with exogenous 8-25 aa-long peptidesderived from the b3a2 or b2a2 junctional regions ofp210BCR-ABL. This approach was pioneered by Scheinberget al, who conducted a phase I clinical trial in which thesafety and immunogenicity of a multidose, multivalentb3a2 peptide vaccine were evaluated in 12 patients withCML in chronic phase. No significant adverse effects wereseen. Three out of six patients treated at the two highestdose levels of vaccine generated peptide-specific T cellproliferative responses ex vivo and/or delayed type hy-persensitivity responses, lasting up to 5 months after vac-cination, although CTLs were not identified.34 The over-all results suggest that a Bcr-Abl-derived peptide vac-cine can be safely administered to CML patients and canelicit a specific immune response. It remains to be seenwhether this type of vaccination will result in significantclinical benefit. Combining such molecularly orientedtherapies (e.g. STI571 and FTIs) may synergize anti-CMLefficacy and allow successful strategies in CML outsidethe setting of allogeneic SCT.
Summary and ConclusionsThe considerable expansion of our knowledge of themolecular pathophysiology of CML has provided impor-tant new insights into targeting the treatment of patientsto specific molecular defects. The ideal candidate for dis-ruption should be the BCR-ABL gene and encoded fu-sion protein, since these are the molecules that areuniquely present in the CML cells. Thus, various strate-gies aim at neutralizing BCR-ABL proper, such as anti-sense ODNs or ribozymes against the junctional se-quences, inhibition of Bcr-Abl tyrosine kinase activityby STIs, or enhancement of an immune response to BCR-ABL-containing cells. Alternative approaches are de-signed to block molecules that are constitutively activatedby Bcr-Abl (e.g. Ras, PI-3 kinase, Grb2, Crkl). The on-going search for proteins and pathways associated withthe abnormal phenotype of the CML cell will surely un-cover new molecular targets for a rational therapy of CMLin the near future.
II. IMPORTANT QUESTIONS RELATED TO INTERFERON-�����THERAPY IN CHRONIC MYELOID LEUKEMIA
Sante Tura, M.D.*
IFN-� has become the treatment of choice in patientswith Ph-positive CML who are not candidates for allo-geneic stem cell transplant (SCT). It induces durable cy-togenetic responses and prolongs duration of chronicphase and survival compared with conventional chemo-therapy.35-41 Questions regarding IFN-� include a) the
mechanisms of action of IFN-�; b) the best IFN-� doseschedule and duration of treatment; c) the optimal IFN-�combinations; d) the long-term outcome of patients onIFN-� therapy; e) the relationships between features ofCML and probability of response to IFN-� and expectedbenefits; and f) definitions of clinical and biological tar-gets of treatment, including the concept of cure.
The molecular and biologic bases of the mechanismsof action of IFN-� are poorly understood.35,42 The effectof IFN-� may be a direct anti-proliferative effect or anindirect one on the immune system through non-specificenhancement of anti-leukemic cell-mediated response.IFN-� may increase HLA molecule expression on Ph-positive cells, so that the HLA-linked leukemic peptidecan be recognized more efficiently by antigen presentingcells and by T-lymphocytes.43,44 Binding of IFN-� to itsmembrane receptor activates a number of signalling path-ways that eventually modulate the transcription of sev-eral genes.42 Many of these pathways are shared withthose that are constitutively activated by the leukemia-specific BCR-ABL tyrosine-kinase oncoprotein p210.One important difference is ICSBP, which may be down-regulated in BCR-ABL-expressing cells and up-regulatedby IFN-�. Mice lacking ICSBP expression develop a my-eloproliferative syndrome resembling chronic phaseCML. Why some Ph-positive cells are or become resis-tant to IFN-� is unknown. An indirect answer to the ques-tion is provided by the clinical observation that the thera-peutic effect of IFN-� decreases with time, since it ismuch greater in early than in late chronic phase and isminimal with progression from chronic to accelerated orblastic phases.35,36 This implies the development of othergenomic abnormalities that make the cells more resistantto IFN-� and perhaps to other modalities, including allo-geneic SCT, homoharringtonine (HHT) and STI571. Sen-sitivity to IFN-� may be primarily dependent on p210amount.45 The identification of other genomic abnormali-ties may provide a basis for a more rational use of IFN-�, either alone or in combination.
IFN-� was initially administered at a dose of about5 million units (MU)/m2/daily, although most studies ul-timately deliver a dose of 5 MU daily or less. The opti-mal IFN-� dose, particularly in combinations, is underinvestigation. Arguments regarding IFN-� dose are notalways based on biologic and pharmacokinetic data, buton the fact that IFN-� is expensive, that its side effectsare dose related (especially in the elderly), and that somepatients respond well to lower doses of IFN-�. Two pro-spective studies in the UK and in the Netherlands arenow comparing low-dose (3 MU five times a week) ver-sus high-dose (5 MU/m2 daily). These studies address
* University of Bologna, Inst. of Hematology and Oncology, ViaG. Massarenti, 9, 40138 Bologna, Italy

96 American Society of Hematology
treatment toxicity and cost-effectiveness, not improvedefficacy, which is the major drawback of IFN-�. The ac-tivity of low-dose IFN-� may provide important infor-mation for the combination of IFN-� with other agents.
A third important question is whether IFN-� therapycan cure CML. Cure in CML can be considered clinical,(i.e. resulting in durable hematologic and cytogenetic re-missions) or biological (resulting in molecular evidenceabsent of very limited residual disease).46-48 Current mo-lecular techniques can identify as few as 30 or 40 mol-ecules of bcr-abl transcript and detect one Ph-positivecell in a million cells. The concept of cure in CML andthe role of molecular biology in providing guidelines fortreatment have been discussed extensively.49,50 Data onpatients who achieve a complete cytogenetic (CG) re-sponse (CG CR) may provide valuable information. Sincethe frequency of CG CR ranges between less than 10%and 35%, European investigators have gathered cases ofPh-positive CML who had achieved a CG CR at leastonce on IFN-� alone. This registry of CG CR includesnow 317 cases, seen between 1983 and 1997, for an ob-servation time ranging between 2 and 15 years (median6.5 years). Their median age is 49 years (range 9 to 73years). The percentage of low-risk patients is 62% usingSokal’s risk criteria51 and 58% using the new Euro riskcriteria.52 At last follow-up, 212/316 patients (67%) werestill in CG CR, 36 (11%) were in major or partial cytoge-netic response, 30 (9%) had lost their cytogenetic responsebut were still in hematologic remission, 5 (2%) had diedin chronic phase, 5 (2%) had undergone transplantation,and only 28 (9%) had progressed to accelerated or blas-tic phase. The 10-year projected survival was more than80% from diagnosis and more than 70% from date of fistCG CR. The projected 10-year survival was more than90% for low-risk patients, 75% for intermediate-risk pa-tients, and only 50% for high-risk patients. This suggeststhat long-term survival (potential cure) is possible in low-risk patients.
Two recent analyses compared cohorts of patientstreated with IFN-� versus allogeneic SCT.54,57 In the Ital-ian experience comparing IFN-� versus allogeneic SCTin CML, the authors concluded that initial allogeneic SCTmay be superior among younger patients (age < 32 years)and those with higher risk disease, while initial IFN-�therapy may be superior among older patients and thosewith low-risk disease.54 When patients were cross tabu-lated into four categories by age (32 years or youngerversus older) and risk group (higher versus low), onlypatients who were 32 years old or younger and who hadhigher-risk disease (61/422 = 14% of total) had a signifi-cant 10-year survival benefit with allogeneic SCT versusIFN-� (10-year survival rate 65% versus 14%, p = .008).Patients older than 32 years with higher risk diseaseshowed a similar trend (10-year survival rate 47% versus
17%; p = .50), which was perhaps not significant becauseonly 32 patients had undergone allogeneic SCT while130 had received IFN-�. However, in low-risk patients(219/422 = 52% of total), there was no survival advan-tage for one modality over another. Hehlmann et al com-pared the outcome of allogeneic SCT versus IFN-� basedon “genetic randomization,” i.e. patients were allocatedaccording to eligibility for transplant and then receivedallogeneic SCT if available. Of 901 patients, 524 weregenetically randomized: 165 (18% of total) for SCT and389 for IFN-� therapy. Median observation time was 639days. During the first 4 years of observation survival wasbetter with IFN-� (p = 0.014), but the survival curveswere expected to cross at 5 years. Early mortality fromSCT was 25% from unrelated donors and 30% from re-lated donors. While the authors suggest that SCT out-come will be more favorable with longer follow-up amongintermediate-high risk patients, this is not observed forlow-risk patients, although they speculate it may occurwith much longer follow-up.57
The long-term observations of patients who achievedCG CR with IFN-� alone and of the outcome of IFN-�versus allogeneic SCT provide some guidelines for thetreatment of CML with IFN-� based on response andrisk.53,54 Low-risk patients constitute about 50% of thoseless than 55 years old and about 30% of older patients. Aguideline is shown in Table 1. Patients younger than 30years should be considered for frontline allogeneic SCT,regardless of risk group. Among older patients, low riskpatients are likely to respond to IFN-� and those whoachieve a CG CR can survive for prolonged periods oftime. They are the best candidate for IFN-� treatment. Incontrast, non-low risk patients may respond to IFN-� andsurvive longer, but their survival is not prolonged indefi-nitely. For the patients who are less than 55 years old, thecontroversial question of IFN-� therapy versus allogeneicSCT upfront depends on the probability of cure and therisk of transplant-associated mortality53-55 (Table 2).
These guidelines are based on the results of IFN-�therapy alone and on the current accepted risks of trans-plant in different patient subsets (based on age, relatedversus unrelated donors, degree of mismatching, and pa-tient selection). These guidelines, including the roles offrontline allogeneic SCT and of IFN-� therapy, shouldbe re-evaluated as data with STI571 matures.21-23,56 Fu-ture investigations of STI571 alone or combined withIFN-�, ara-C, HHT, decitabine, or other molecular strat-egies (e.g. FTIs) may provide superior survival and du-rable complete and major cytogenetic responses. Guide-lines would then be based, not on the comparative resultsof allogeneic SCT versus IFN-�, but on the SCT-associ-ated mortality (i.e. the acceptable upfront risk for an es-tablished curative modality). A reasonable approachwould be as follows:

Hematology 2000 97
III. UPDATES ON UNRELATED DONOR TRANSPLANTATION,DONOR LYMPHOCYTE INFUSIONS, AND NON-ABLATIVE
STEM CELL TRANSPLANTATION
Sergio Giralt, M.D.*
Unrelated Donor TransplantationOnly 35% of patients with CML under the age of 55 ac-tually undergo an allogeneic transplant, primarily due tothe lack of an appropriate tissue-compatible related do-nor.58 Alternative progenitor cell sources such as cordblood, mismatched related transplants or matched unre-lated donor transplants have been extensively exploredas treatment options for patients with CML. CML is themost common indication for unrelated donor transplantsand represents 35% of all unrelated donor transplants donein the United States.59 With the increasing number andsize of volunteer donor registries, the median time foridentification of a suitable donor has decreased from 6.9months to 5.5 months; however, only one of four searchesactually culminates in transplantation.60 Results of thelargest series of unrelated donor transplantation for CMLare summarized in Table 3.59,61-63
Acute graft-versus-host disease (GVHD) and infec-tious complications remain the most important causes ofmorbidity and mortality of unrelated donor transplanta-tion.9-64 The single most important prognostic factor fordevelopment of acute GVHD is degree of histocompat-ibility. Serologic typing underestimates the degree ofmismatching in a large proportion of donor-recipient
Table 1. The guidelines for the treatment of chronicmyelogenous leukemia (CML) with interferon-����� (IFN-�����) orallogeneic stem cell transplantation (SCT) are based on risk,age and the availability of a suitable marrow donor.
Testing for IFN sensitivity may help decide between IFN-� andallogeneic SCT. Testing for IFN-� sensitivity may require sometime, but treatment of low-risk patients is never urgent. In thetable, the term investigational treatment encompasses a numberof procedures (e.g. intensified chemotherapy with autologousstem cell rescue, allogeneic SCT from mismatched donors or inthe elderly) and novel agents. However, the first-line investiga-tional option to be considered should be the BCR-ABL tyrosine-kinase inhibitor STI571, either alone or in combination.
Age < 30 years, any risk• First-line option is allogeneic SCT, from any matched donor.
Age 30-55 years, low risk• Test for IFN-� sensitivity. If test is positive, first-line option is IFN-
�. The surrogate target for long survival is achieving a majorcytogenetic response in 1 year and a complete cytogeneticresponse in 2 years.
• If test is negative, first-line option is allogeneic SCT from anHLA-identical sibling or an HLA-matched unrelated donor.
• If a suitable donor is not available, investigational treatment.
Age 30–55 years, non-low risk• First-line option is allogeneic SCT from an HLA-identical sibling
or an HLA-matched unrelated donor.• If a suitable donor is not available, investigational treatment.
Age > 55 years, low risk• Test for IFN-� sensitivity. If test is positive, first-line option is IFN-
� as for younger patients.• If test is negative or IFN-� is not tolerated, investigational
treatment.
Age > 55, non-low risk• First-line treatment is investigational.• If investigational treatment is not feasible or not tolerated,
second line is hydroxyurea.
1. If SCT-associated one-year mortality is below 20%(younger patients with matched-related donors), alloge-neic SCT is the frontline treatment option.
2. If mortality is between 20% to 40% (older pa-tients up to 50 years of age with related donors, or youngpatients with matched unrelated donors), only patientswho fail therapy (lack of cytogenetic response after oneyear of therapy, subsequent loss of cytogenetic response)are offered allogeneic SCT in chronic phase.
3. If mortality is estimated to exceed 40%, investi-gational options are offered in chronic phase (HHT,decitabine, tyrosine kinase inhibitors) and allogeneic SCTproposed if signs of disease transformation appear. Pa-tients may then survive many years in chronic phase.Furthermore, the transplant-related mortality in acceler-ated phase is not sufficiently higher in these patients tojustify the upfront high risk of transplant mortality inchronic phase.
Table 2. Proposed risk classification for allogeneic stem celltransplantation (SCT).55
Risk factors are donor type (0 for HLA-identical sibling donor, 1 fora matched unrelated donor); disease stage (0 for first chronicphase, 1 for accelerated phase, and 2 for blast crisis or higherchronic phase); age of recipient (0 for < 20 years, 1 for 20–40years, and 2 for > 40 years); sex combination (0 for all, except 1for male recipient/female donor); and time from diagnosis to SCT(0 for < 12 months, 1 for > 12 months)
Results at 5 years% of Leukemia- Transplant-
Risk Patients with Free RelatedFactors Risk Factors Survival (%) Mortality (%)
0 2 60 201 18 60 232 28 47 313 28 37 464 15 35 515 7 19 71
6-7 2 16 73
Adapted from Gratwohl et al.55
* M.D. Anderson Cancer Center, 1515 Holcombe Boulevard, Box65, Houston TX 77030-4009

98 American Society of Hematology
pairs. Modern molecular techniques have demonstratedthat molecular mismatches in serologically matched do-nor-recipient pairs are common and correlate with trans-plant outcomes.65-67 In the Seattle study, young patientswith CML (less than 50 years of age), who receive a fullymolecular matched unrelated donor and are transplantedwithin 1 year of diagnosis have an estimated 5-year sur-vival rate of 74%, indistinguishable from recipients offully matched sibling donor transplants.62 The impact ofrelevant pre-treatment variables on outcome of unrelateddonor transplants in CML is summarized in Table 4.
The approach to patients with CML who lack anHLA-identical sibling donor has become increasinglydifficult. On one hand the availability of non-transplantstrategies that can effectively achieve cytogenetic remis-sions, such as interferon and more recently STI571, of-fers the possibility of long-term disease control for somepatients without allogeneic transplantation.68 On the otherhand, the increasing size and number of volunteer donorregistries as well as improvements in tissue typing andsupportive care have improved the outcomes of unrelateddonor transplantation. The current challenge for physi-cians and patients is how to incorporate these strategiesin each individual case and how to decide who shouldundergo unrelated donor transplantation as primarytherapy or as salvage therapy for their disease. Trans-plant and non-transplant options should be viewed ascomplementary strategies in the treatment of CML, thegoal being to obtain complete cytogenetic remissions inas many patients as possible with the minimum toxicitynecessary for each patient.
Donor Lymphocyte InfusionsDLI are an effective therapeutic strategy for patients withCML who have relapsed after allogeneic hematopoietictransplantation.69,70 DLI is limited by the occurrence ofacute and chronic GVHD in up to 60% of patients, whichhas been associated with significant morbidity and a
mortality of approximately 20%. Current strategies toimprove the results of DLI in CML have concentrated ondecreasing the risk of GVHD after infusion, and fall intoone of the following categories:• Selective depletion of lymphocyte subsets.• Incremental doses of donor lymphocytes.• Gene-modified DLI
CD8-depleted donor lymphocyte infusionsDepletion of CD8+ cells from DLI has resulted in a re-duction of the incidence of GVHD without compromis-ing response.71 Remissions after CD8-depleted DLI aredurable and the factors that predict outcome are similarto those after unmanipulated DLI and are summarized inTable 5.
At the University of Texas M.D. Anderson CancerCenter, 26 patients with CML who relapsed after an allo-geneic transplant have been treated with CD8-depletedDLI. CD8+ depletion with immunomagnetic or panningtechniques resulted in a mean depletion of 2.6 log ofCD8+ lymphocytes. The median CD4+ cell dose infusedwith the first DLI was 39.8 x 106 cells/kg, and the me-dian CD8+ dose was 0.3 x 106 cells/kg. Fourteen patientsachieved complete cytogenetic and molecular remissionsfollowing DLI. The stage of the disease at the time ofDLI was the most important prognostic factor for re-sponse. Thirteen of the 15 (87%) patients who were incytogenetic or chronic phase relapse at the time of DLIresponded. Actuarial rate was 8% (95 CI, 3-13%) for acuteGVHD. Chronic GVHD occurred in 4 patients and wasextensive in two patients. Actuarial risk for chronicGVHD was 22%.
The median follow-up of the 15 patients relapsing innon-transformed phases was 3.5 years (range, 1-6.5): 13are still alive, 10 in complete remission; the estimated 5-year survival rate is 87%, and estimated 5-year disease-free survival rate 65% (Figure 3). This experience, aswell as studies performed at the Dana-Farber Institute,(72)
Table 3. Results of representative studies of unrelated donortransplantation for chronic myelogenous leukemia (CML).
% % %Median Survival GVHD GVHD %
N Age (at x yr) II-IV III-IV Relapse
McGlave59 1423 35 37 (3) 43 33 8
Spencer61 115 33 46 (3) 24 23
Hansen62 196 35 57 (5) 77 35 10
Drobyski63 27 32 52 (3) 39 8 9
Table 4. Variables that affect outcomes of unrelated donortransplants in chronic myelogenous leukemia (CML).
OutcomeVariable (Reference) GVHD Survival
Chronic phase status at time of SCT(59,62) – +
Serologic mismatch Class I or II(59,61,65) + 0
Molecular mismatch(62,66,67) + –
Older age(59,62) 0 –
Transplant < 12 months from diagnosis(59,62) 0 +
CMV positivity(59,61) 0 –
T-cell depletion(59) – 0
Abbreviations: GVHD, graft-versus-host disease; –, negativeeffect; +, positive effect; 0, no significant effect

Hematology 2000 99
demonstrate that CD8-depleted DLI is effective in in-ducing remissions in post-transplant CML relapse, andreducing the risk of GVHD. These results are currentlybeing tested in a prospective randomized trial.
Dose-escalated donor lymphocyte infusionsThe incidence of GVHD increases with the number ofcells infused, but there may be a different threshold forGVHD and graft-versus-leukemia (GVL). One approachis to administer escalating doses of donor lymphocytesstarting with a relatively low dose and escalating the doseon subsequent infusions, infused in non-responders atpredetermined intervals. Investigators at the Hammer-smith Hospital have compared an escalating dose regi-men, starting with 1 x 107 CD3+ cell/kg (1 x 106 for DLIfrom unrelated donors), to a single larger dose DLI (me-dian dose 1.5 x 108 CD3+ cells/kg). The escalating doseregimen resulted in similar response rate but a lower in-cidence of acute and chronic GVHD, despite the infu-sion of an equivalent total number of lymphocytes withthe multiple infusions.74
Transduction of donor lymphocytes with suicide genesTransduction of donor cells with a suicide gene, such asthe herpes simplex virus thymidine kinase, which con-
Table 5. Predictors of outcome post donor lymphocyteinfusion (DLI) in chronic myelogenous leukemia (CML)relapse following allogeneic stem cell transplantation (SCT).Results compare presence vs absence of the variable inquestion.
Study(Reference)/ % % %Variables Response GVHD AplasiaVariable P A P A P A
Kolb(69)
CP at DLI 80 2No GVHD with BMT 84 64IFN treatment 73 51 52 24Hematologic relapse 68 45 49 12
Collins(70)
CP at DLI 81 44No GVHD with BMT 64 86 72 91Caucasian 64 85 72 94IFN treatment 74 81
Shimoni(71)
CP at DLI 87 9Time to relapse 23 85 < 12 monthsSibling donor 40 100
Dazzi(74)
Bulk DLI 67 91 44 10
Abbreviations: P, presence; A, absence; CP, chronic phase; DLI,donor lymphocyte infusion; GVHD, graft-versus-host disease;BMT, bone marrow transplantation; IFN, interferon
Figure 3. Overall survival of CML patients receiving CD8-depleted donor lymphocyte infusions (DLI) for relapse afterallograft according to disease status at the time of DLI.
fers sensitivity to ganciclovir, has also been explored asa means of increasing the safety of DLI. If the patientdevelops GVHD, it can be abrogated by ganciclovir treat-ment.75 In a recent update of this strategy Bonini et alreported a response rate of 60%; three patients devel-oped > grade 2 GVHD, of which two responded to ganci-clovir therapy. However, in a multicenter study of TK-transduced DLI, Champlin et al reported only two re-sponses in 14 patients with CML and no GVHD. Thissuggests that transduction techniques may affect thealloreactivity of the donor lymphocytes.76
Non-Ablative Stem Cell TransplantationThe anti-leukemia responses observed after DLIs in CMLpatients who relapsed after an allogeneic progenitor celltransplant represent direct evidence of the GVL effectmediated by lymphocytes. This observation also demon-strated that very effective GVL effects can be seen inCML without the need for the intense myeloablation pro-vided by the preparative regimen. This finding paved theroad for the concept of non-ablative stem cell transplan-tation (NST).77 NST has been proposed as a strategy thatwould allow the “harnessing” of the GVL effect in pa-tients considered poor candidates for myeloablative thera-pies either because of their age or concurrent medicalconditions.
CML represents an ideal candidate for therapy withNST for the following reasons: a) relatively stable natu-ral history that will allow time for induction of a GVLeffect; b) high response rate to immune-modulatory ma-neuvers (DLI, IFN); and c) lack of therapies that canchange the natural course of the disease if failure of front-line therapy (usually IFN-based therapy) occurs.
CML patients also present particular challenges forNST due to their relatively conserved immune compe-tence, which could increase the risk of rejection, and thepresence of splenomegaly in some patients, which may
Time in Years
Cum
ulat
ive
Pro
port
ion
Sur
vivi
ng

100 American Society of Hematology
affect engraftment.Trials of non-ablative stem cell transplantation in
CML are still immature and have only a small number ofpatients. At the M.D. Anderson Cancer Center, a total of43 patients with CML have received either a true non-ablative stem cell transplant with fludarabine/idarubicin/cytarabine combinations or a reduced-intensity condition-ing with melphalan/purine analog combinations. Patientcharacteristics are summarized in Table 6.
Of the 10 patients who received fludarabine/idarubi-cin/cytarabine followed by infusion of donor progenitorcells, all had neutrophil and platelet recovery at a medianof 13 days and 14 days respectively. All patients showedevidence of donor cell engraftment except the two re-cipients of unrelated donor cells. Bone marrow on day30 revealed complete cytogenetic remission in four pa-tients and major cytogenetic remission in another two
patients. All five patients transplanted in advanced CMLphases had cytogenetic progression during the first 6months after transplant, and failed to respond to subse-quent salvage therapy. Three of the five patients trans-planted in chronic phase CML have relapsed. One pa-tient achieved a subsequent complete cytogenetic remis-sion with a donor lymphocyte infusion; the other two havefailed to respond to this therapeutic maneuver. Survivaland disease-free survival are depicted in Figure 4.
McSweeney et al, using 200 cGy of TBI, reportedthat four of eight patients with CML achieved completecytogenetic remissions, with little toxicity, but graft fail-ure rate was 20%, which has prompted the addition offludarabine to the preparative regimen. More patients andlonger follow-up will be needed to assess the true impactof non-ablative preparative regimens in the control of thisdisease.78
The initial results with fludarabine, idarubicin andara-C combinations suggested that this strategy is noteffective in CML in blast transformation and is notimmuno-suppressive enough to allow engraftment of cellsfrom unrelated or mismatched donors. Therefore, thedevelopment of reduced intensity conditioning, whichmay be more intense than truly non-ablative regimensbut still better tolerated than conventional myeloablativeregimens, was necessary. Melphalan in combination withpurine analogs was thus developed as the new condition-ing regimen in our studies.
Thirty-three patients with CML have undergone al-logeneic transplants at M.D. Anderson Cancer Centerafter reduced intensity conditioning with fludarabine/melphalan combinations. More than half of these patientsreceived bone marrow from unrelated donors, and onlyeight patients were in first chronic phase. Thirty-two of33 patients achieved neutrophil recovery within a me-dian of 14 days, and 24 achieved platelet transfusion in-dependence at a median of 20.5 days. At the time of firstmarrow, the median percentage of donor cell engraftmentas determined by cytogenetics or molecular techniqueswas 100% for recipients of sibling transplants (range, 80–100) and for recipients of unrelated donor bone marrow(range, 0–100). Only three recipients of unrelated donorbone marrow had less than 50% donor cells at the timeof first marrow, one of whom became a full donor chi-mera over a period of 3 months. Other important trans-plant outcomes are summarized in Table 7 and depictedgraphically in Figure 5.
In summary, NST and reduced intensity condition-ing are feasible in CML and can result in long-term dis-ease control. Their role in the therapy of CML remainsto be established, in relation to the therapeutic alterna-tives of interferon-based therapy, STI571, and conven-tional myeloablative transplantation. Preliminary resultssuggest that NST should be further investigated as an
Figure 4. Current disease-free survival and overall survivalfor patients with chronic myelogenous leukemia (CML)undergoing non-ablative stem cell transplantation (Flag-Ida)at M.D. Anderson Cancer Center according to disease stageat transplant.
Table 6. Characteristics of chronic myelogenous leukemia(CML) patients rndergoing non-ablative stem celltransplantation (Flag-Ida) or reduced intensity conditioning(fludarabine/melphalan) at M.D. Anderson Cancer Center.
Fludarabine/Parameter Flag-Ida Melphalan
Number 10 33Median age, (range) 57 (42-72) 52 (24-70)Median time to BMT in months,
(range) 29 (13-11) 29 (3-220)Stage at BMT
first chronic 5 8phase transformed 5 25
Donor typesibling 8 15unrelated 2 18
Comorbid conditionsage > 55 year 6 13extensive prior therapy 0 23infection/organ function/PS = 2 3 6none 1 6
Cum
ulat
ive
Pro
port
ion
Dis
ease
Fre
e at
Fol
low
-Up
Time in Months

Hematology 2000 101
IV. INTERFERON-����� PLUS LOW-DOSE CYTARABINE AND
OTHER PROMISING TREATMENT MODALITIES FOR
CHRONIC MYELOGENOUS LEUKEMIA
Hagop M. Kantarjian, M.D.* and Moshe Talpaz, M.D.**
Investigational strategies in CML have aimed at suppres-sion of Ph-positive CML cells (78,79) and more recently atsuppression of the molecular consequences of the BCR-ABL abnormality or associated molecular events, as dis-cussed earlier. Evidence supporting this approach include1) the causal association between the BCR-ABL abnor-mality and development of CML, as demonstrated by theinduction of CML-like disease by transfection of Ph-as-sociated BCR-ABL molecular abnormalities in animalmodels80,81; 2) the suppression of CML disease achievedin preclinical models through interference with the BCR-ABL abnormalities82,83; and 3) the association betweenthe achievement of minimal residual disease (completehematologic response, cytogenetic response) and im-proved survival in CML.37-41,84
Large-scale studies with IFN-�, including those atM.D. Anderson, have reported a complete hematologicresponse (CHR) rate of 50–80% and a cytogenetic re-sponse rate of 20–60%.35-41,84,85 Patients achieving a ma-jor cytogenetic response have the greatest survival advan-tage; hence, strategies to improve this rate are warranted.
IFN-����� and Low-Dose Cytarabine in Chronic PhaseCML
The rationale behind the combination of IFN-� and low-dose cytarabine was based on 1) the selective in-vitrosuppression of CML cells with cytarabine86; 2) the clini-
Figure 5. Current disease-free survival of patients withchronic myelogenous leukemia (CML) undergoing reducedintensity conditioning with fludarabine/melphalan accordingto disease status at the time of transplant and donor type.
Table 7. Outcomes of non-ablative and reduced conditioningregimens for chronic myelogenous leukemia (CML) at M.D.Anderson Cancer Center.
Fludarabine/Parameter Flag-Ida Melphalan
Number 10 33
Donor cell engraftment 8 32
Graft failure 2 2
Relapse 6 8
GVHD > 2 1 14
Responses after relapse 2 1
2-yr survival CP1:80% CP1:63%
Other:20% Other:33%
2-yr DFS CP1:40% CP1:63%
Other:0% Other:30%
alternative for patients in chronic phase ineligible forconventional transplant techniques, but that it may beineffective in advanced phase CML.
Future Issues in Progenitor Cell Transplantation forCML
The main challenge for physicians and patients with CMLis how to decide among existing therapeutic options.Current therapies should be viewed as complementary.Physicians and patients should develop treatment plansand algorithms from the time of diagnosis, decidingwhether transplantation is appropriate as initial therapyor whether it will be used as salvage if initial non-trans-plant therapies fail to achieve complete cytogenetic re-missions.
NST and reduced intensity conditioning have in-creased the pool of possible transplant candidates. How-ever, GVHD, loss of donor cell engraftment, and diseaserecurrence are major causes of treatment failure. The in-corporation of STI571 and/or IFN needs to be studied inthe post-transplant setting as a means of reducing dis-ease recurrence, particularly in patients who undergo pro-genitor cell transplantation in advanced phase CML.
* M.D. Anderson Cancer Center, Hematology Department, 1515Holcombe Boulevard, Box 61, Houston TX 77030-4009** M.D. Anderson Cancer Center, 1515 Holcombe Boulevard, Box302, Houston TX 77030-4009
Cum
ulat
ive
Pro
port
ion
Sur
vivi
ng D
isea
se F
ree
Cum
ulat
ive
Pro
port
ion
Sur
vivi
ng D
isea
se F
ree
Time in Months
Time in Months

102 American Society of Hematology
cal experience with single-agent low-dose cytarabineshowing cytogenetic responses in seven of nine pa-tients87,88; and 3) the positive results from pilot studies inlate chronic phase CML, which established the safety andefficacy of the combination.89
IFN-� and daily low-dose cytarabine in single-armtrials90-93
Experience with different schedules of the combinationof IFN-� and low-dose ara-C have been reported in sev-eral single-arm studies in CML by the M.D. AndersonCancer Center group90 (Tables 8 and 9), Arthur et al fromAustralia,91 Thaler et al from Austria,92 and Silver et alfor the CALGB Study.93 These studies demonstratedtrends for higher response rates with the combinationcompared with IFN-� alone (Table 10). Table 11 com-putes the cumulative rates of CHR and cytogenetic re-sponses reported from nine studies of IFN-� alone, aswell as seven studies of IFN-� plus low-dose ara-C. Inthe MD Anderson studies, daily low-dose ara-C was moreeffective than intermittent low-dose ara-C (Table 8). In-termittent low-dose ara-C (20mg/m2 daily x 10 everymonths) may be associated with significant gastrointes-tinal complications (mucositis, diarrhea), and with fre-quent treatment interruptions due to myelosuppression.
Randomized trials of IFN-� and low-dose cytarabineversus IFN-� aloneIn a French multicenter trial in CML, Guilhot et al ran-domized patients to IFN-� 5 MU/m2 daily alone (N =361) or IFN-� plus low-dose cytarabine 20 mg/m2 dailyfor 10 days every month (N = 360).94 IFN-� plus ara-Cwas associated with a significantly higher CHR rate at 6months (66% versus 55%, p < .01), and a higher cytoge-netic response rate at 12 months, overall (61% versus50%) and major (38% versus 26%, p < .0.01) (Table 12).With a median follow-up of 43 months, IFN-� and cytar-
Table 9. Prognosis by patient risk group with interferon-�����(IFN-�����) plus daily low-dose cytarabine therapy.
% % Cytogenetic ResponseRisk Group No. CHR Any Major CR
Good 61 95 82 61 43
Intermediate 37 95 73 49 24
Poor 17 82 53 29 18
P value .17 .05 .045 .06
Abbreviations: CHR, complete hematologic response
Table 8. Percent response to interferon-����� (IFN-�����) plus dailyara-C, IFN-����� plus intermittent ara-C, and IFN-����� alone.90
IFN-����� +IFN-����� + Daily Intermittent
low-Dose Low-Dose IFN-�����Cytarabine Cytarbine Alone P
Response [N=134] [N=45] [N=274] Value
Complete hematologic 92 84 80 .01
Cytogenetic overall 74 73 58 .003
Complete response 31 20 26 .06
50% 38% 38%
Partial response 19 18 12
Minor response 24 33 20
Table 10. Single-arm studies of interferon-� � � � � (IFN-�����) plus low-dose cytarbine.
Study No. % %Cytogenetic Response(reference) Treated CHR Complete Major
MDACC(89)
daily cytarabine 134 92 31 50intermittent cytarabine 54 84 20 38
Arthur(91) 30 93 30 53
Thaler(92) 84 54 18 25
Silver(93) 88 72 15 51
Abbreviations: CHR, complete hematologic response; MDACC,M.D. Anderson Cancer Center
Table 11. Cumulative data on response with IFN-����� with andwithout ara-C in CML
IFN-����� +Parameter IFN-����� low-dose ara-C
No. treated 1632 700
No. studies 9 6
%CHR 60 72
% cytogenetic response
major 22 42
complete 14 24
Table 12. French CML 91 study results.
IFN-� � � � � + PParameter Cytarabine IFN-����� Value
No. analyzed 360 361
% CHR at 6 months 66 55 < .01
% cytogenetic response at 12 months
- overall response 61 50
- complete response 15 10
38% 26%
- partial response 23 16 <.001
% 5-year survival 70 60 .02
Abbreviations: IFN-�, interferon-�; CHR, complete hematologicresponse

Hematology 2000 103
abine was associated with a significantly better survival(5-year rate 70% versus 60%; p = .02), which was con-firmed by multivariate analysis. A landmark analysis bycytogenetic response at 2 years showed an association ofcytogenetic response with survival: the 7-year survivalrate was 85% for patients achieving complete or partialcytogenetic response, 62% for those with minor cytoge-netic response, and 25% for others. Cytogenetic response,whether obtained with IFN-� alone or with IFN-� plusara-C, was associated with significant prolongation ofsurvival. These results continued to be confirmed withlonger follow-up.95
The Italian Cooperative Study Group on CML(ICSG-CML) conducted a randomized trial similar to theFrench study. The ICSG-CML study used similar sched-ules of IFN-� plus cytarabine versus IFN-�. Five hun-dred forty evaluable patients were randomized; 275 re-ceived IFN-� and cytarabine, and 265 received IFN-�alone. In an update of the study in 1999, the mean obser-vation time was 24 months. The combination of IFN-� plusara-C was demonstrating superior results.96 At 6 months,the CHR rates were 87% versus 80%. IFN-� plus ara-Cwas associated with higher cytogenetic response rates(48% versus 44%), and with higher rates of major cyto-genetic response (28% versus 19%, p = .01), and of com-plete cytogenetic response (14% versus 7%) comparedwith IFN-� alone. The 3-year survival rate was also higherwith IFN-� plus ara-C compared with IFN-� alone (85%versus 80%, p = .03). However, these results need to beconfirmed with longer follow-up and more mature analy-sis before a final assessment of the potential benefit ofadding ara-C can be made (S. Tura, personal communi-cation).
HomoharringtonineHomoharringtonine (HHT) is a semi-synthetic plant al-kaloid derived from the Cephalotaxus fortuneii tree. Ini-tial studies from China suggested activity of HHT in acutemyelogenous leukemia (AML) and acute promyelocyticleukemia. In fact, many frontline studies in AML use thecombination of HHT and cytarabine with or withoutanthracyclines.
Phase I–II studies in the United States confirmedmodest activity of HHT in AML and myelodysplasticsyndrome. However, at HHT doses of 5 to 9 mg/m2 dailyfor 5 to 7 days, severe cardiovascular and hypotensivecomplications occurred, discouraging further investiga-tions of HHT. At M.D. Anderson Cancer Center, a lower-dose longer exposure schedule of HHT (2.5 mg/m2 bycontinuous infusion daily for 14 to 21 days) reduced sig-nificantly the cardiovascular problems. HHT alone (2.5mg/m2 daily x 14 days for induction, then x 7 days everymonth for maintenance)97 was then compared to HHT +ara-C (HHT 2.5 mg/m2 daily x 5 and ara-C 15 mg/m2
daily x 5, every month) in late chronic phase CML.Among 173 patients treated, the CHR and cytogeneticresponse rates were identical with either regimen (Table13). However, survival was significantly longer with HHT+ ara-C, even after accounting for risk groups and bymultivariate analysis (Kantarjian, submitted).
In subsequent studies, HHT was investigated in earlychronic phase CML. HHT was then given for six cyclesas remission induction followed by IFN-� maintenance.CHR rate was 92% and cytogenetic response rate was68%.98 Results after 6 months appeared to favor HHTover IFN-� in relation to response, suggesting that HHTmay be a valuable addition to our future frontline thera-pies, which could include IFN-�, ara-C, STI571 and oth-ers. HHT is certainly superior to low-dose ara-C alone,with which one could not achieve the impressive resultsof HHT in patients in late chronic phase CML who failedIFN-� therapy.
After establishing the baseline efficacy of single-agent HHT for 6 months in frontline therapy of CML (tocompare it with IFN-�), combination studies of HHT,IFN-� and ara-C, and of HHT + IFN-� in older patientswere developed. So far, about 100 patients in early chronicphase have received the triple regimen. The CHR ratewas 98%; with a median follow-up 11 months, the cyto-genetic response rate was 77% (major 43%). Because ofthe short follow-up, the 6-month results of HHT + IFN-� + ara-C, compared with IFN-� + ara-C, or IFN-� alone
Table 13. Results with homoharringtonine (HHT) alone or withcytosine arabinoside (ara-C) in late chronic phase chronicmyelogenous leukemia (CML) (p = .02).
Parameter HHT HHT plus ara-C
No. treated 73 100
%CHR 67 72
% cytogenetic response 30 32
- major 15 15
- complete 5 5
% 4-year survival 38 58
Abbreviations: CHR, complete hematologic response
Table 14. Six-month response rates with homoharringtonine(HHT) + cytosine arabinoside (ara-C) + interferon-� � � � � (IFN-�����).
6-Month HHT + IFN-����� IFN-����� +Response + Ara-C Ara-C IFN-�����
No. patients 42 148 274
% CHR 98 70 67
% cytogenetic response
- major response 67 49 39
- complete response 33 18 12
Abbreviations: CHR, complete hematologic response

104 American Society of Hematology
were evaluated. These show improved cytogenetic re-sponse rates (Table 14). In addition lower doses of IFN-� (median 2MU daily), ara-C (median 5 mg Tiw), andHHT (median 2 days/month) were required to achievethe results. Anemia appeared to be a significant cumula-tive side effect, which required dose reduction and couldbe improved with weekly erythropoietin injections.99
Similar encouraging results were obtained with HHT +IFN-�, mostly in older patients.100
Ernst et al also combined HHT + ara-C in early andlate chronic phase CML. Among 44 patients treated, 41(93%) achieved CHR, including 14/14 (100%) receivinginitial therapy. Among 14 patients treated with HHT +ara-C as initial therapy, 11 (84%) had a major cytoge-netic response. In their studies, the CHR and cytogeneticresponse rates were higher than those reported in our stud-ies, which may be due to the difference in treatment sched-ules or study group characteristics.101
We are currently investigating alternate routes of HHTdelivery (e.g. subcutaneous or oral schedules), and possiblemodifications to the HHT structure, which could improvethe efficacy: toxicity profile of HHT (Jean-Pierre Robin,personal communication). This could lead to investigationof HHT as an agent for treatment of other hematologic can-cers such as myelodysplastic syndrome, AML maintenance,acute promyelocytic leukemia or others.
5-Aza-2'-DeoxycytidineGeneral and site-specific DNA methylation is character-istic of disease progression and resistance in many tu-mors, including solid cancers as well as hematologicmalignancies such as myelodysplastic syndrome, acuteleukemia, and CML. There is now major interest in strat-egies that suppress DNA methylation as a method to treatcancers or even non-malignant conditions such as sicklecell disease and thalassemia. 5-azacytidine and 5-aza-2'-deoxyazacytidine (decitabine) are cytidine analoguescapable of inducing hypomethylation through inhibitionof DNA methyltransferase enzyme. Both agents have al-ready demonstrated significant activity in myelodysplasticsyndrome, which is thought to be partly due to inhibitionof methylation of p15INK4b. In CML, disease progressionis associated with hypermethylation of the Pa promoterregion within BCR-ABL.102,103 This led to our interest inusing decitabine in CML. The initial studies useddecitabine at 100 mg/m2 over 6 hours every 12 hours for10 doses (5 days) every 4–8 weeks (1000 mg/m2/course),based on the previous European experience. This wasassociated with delayed myelosuppression and dose re-ductions of 50%, i.e. 50 mg/m2 per dose (500 mg/m2/course). Decitabine produced response rates of 25% inblastic phase and 53% in accelerated phase disease.104
Compared with intensive chemotherapy as initial therapyfor CML blastic phase, decitabine was associated with
significantly better survival among patients 50 years orolder (p < .01). By multivariate analysis, decitabinetherapy remained an independent favorable prognosticfactor for survival (p = .047) after accounting for pre-treatment prognostic factors.105 We are currently investi-gating lower dose schedules of decitabine (e.g. 5 to 10mg/m2 daily for 10 to 20 days) to target hypomethylationas the molecular endpoint and correlate it with response.This may provide a less myelosuppressive, and perhapsequally effective regimen. Investigations of decitabine incombination with busulfan and cyclophosphamide as partof a preparative regimen for allogeneic stem cell trans-plantation and as salvage therapy with stem cell rescueafter relapse from allogeneic transplant are also inprogress.106
Polyethylene Glycol (PEG) InterferonPolyethylene glycol (PEG) interferon is a modified IFN-� molecule that is covalently attached to polyethyleneglycol. PEG interferon has a longer half-life than the par-ent compound and is given once weekly instead of daily.In a phase I study, 21 patients with CML in chronic phasewere treated with escalating doses of PEG interferon (In-tron). The starting dose of PEG-Intron was 0.75 µg/kgweekly. The presumed equivalent dose of regular IFN-� 3to 5 MU/m2 daily (i.e. 21 to 35 MU/m2 weekly) is a weeklydose of PEG Intron 1.2 to 1.5 µg/kg. The maximum toler-ated dose in the study was 7.5 µg/kg weekly, and the dosechosen for phase II studies of PEG-Intron was 6 µg/kgweekly(presumably equivalent to regular IFN-� 180 MUweekly = 15 MU/m2 daily). Dose-limiting toxicities wereneurotoxicity, thrombocytopenia, fatigue, and liver func-tion abnormalities, similar to IFN-�, but occurring athigher doses than with IFN-�. In addition to a better side-effect profile of PEG interferon, 9/27 patients improvedtheir responses, including three complete and three par-tial cytogenetic responses. All six patients intolerant toIFN-� were able to receive Peg-Intron. Preliminary re-sults with PEG interferon are promising since it appearsto be easier to deliver (once weekly), less toxic, and pos-sibly more effective than IFN-�. Current studies are in-vestigating the two different formulations of PEG inter-feron, PEG-Intron and Pegasys (PEG-Roferon) alone andin combination with ara-C in early chronic phase CML.PEG-Roferon has a larger molecular weight and may haveless CNS penetration but more hepatic uptake. It is likelythat PEG interferon preparations will replace IFN-� infuture standard of care because of the easier route of de-livery, if the favorable efficacy:toxicity profile is con-firmed with longer follow-up.

Hematology 2000 105
V. STI571 IN CHRONIC MYELOGENOUS LEUKEMIA
Hagop M. Kantarjian, M.D., and Moshe Talpaz, M.D.
STI571 represents a major therapeutic advance in themanagement of CML. The experience with STI571 pro-vides the most dramatic example of how understandingdisease biology and pathophysiology can result in ex-tremely successful molecular-targeted approaches. CMLis an ideal disease for such advances, since the molecu-lar target is unique, highly expressed in most patients,and disease specific. STI571 may provide a model appli-cable to many other tumors in the future.
General Overview of BCR-ABL SignalTransduction Inhibitors
As discussed previously, several naturally occurring com-pounds manifest inhibitory activity against protein ty-rosine kinases, including the isoflavinoid genistein, herbi-mycin A (an antibiotic), the flavinoid quercetin, anderbstatin.108,109 Later, synthetic compounds known as tyr-phostins were rationally designed to complete with ATPor substrate for the binding site in the catalytic center ofthe kinase.18,110,111 These were the first compounds to dis-play specificity for tyrosine kinases.112 Scientists atNovartis identified kinase inhibitors by screening a largelibrary of compounds. Optimization of a lead compoundagainst specific targets led to the development of STI571.
Preclinical Experience with STI571STI571 inhibits the ABL tyrosine kinases at very low con-centrations (0.025 micromolar), including p210BCR-ABL,p185BCR-ABL, V-ABL, and c-ABL. In addition, STI571 in-hibits the c-kit and platelet-derived growth factor recep-tor (PDGFR) tyrosine kinases at similar concentra-tions.21,23,113
This is of interest for several reasons:a) The submicromolar concentrations were easily
achievable in the clinical trials. Once the STI571 dose inphase I studies reached 300 mg orally daily, serum levelsof STI571 of > 1 micromolar were achieved and corre-lated with high response rates.
b) STI571 has activity in both p210 and p190 Bcr-Abl-positive leukemias.
c) The therapeutic activity of STI571 may extendbeyond Ph-positive leukemias to c-kit and PDGFR-posi-tive disorders including AML, myeloproliferative disor-ders, prostate cancer, brain tumors, sarcomas and others.
Preclinical studies have confirmed the selective in-hibitory effects of STI571 against p210BCR-ABL andp190BCR-ABL,20,21 with minimal inhibition of normal he-matopoiesis. Inhibitory activity results in apoptosis. Ef-ficacy was also demonstrated in syngeneic or nude miceinjected with BCR-ABL-expressing cells and then treatedwith STI571.23,114
Animal toxicology studies with oral STI571 demon-strated progressive hepatic toxicity at the highest dose of100 mg/kg. Other toxicities were vomiting, diarrhea, andmyelosuppression (anemia, neutropenia).
Update of the Clinical Experience with STI571 inCML
STI571 has undergone relatively rapid evaluations inphase I and phase II pivotal trials for the purpose of FDAapproval. The pivotal trials targeted the three phases ofCML, chronic, accelerated and blastic. The studies openedin December 1999, and patient accrual was completedby May 2000.
The phase I dose escalation study used STI571 at astarting daily dose of 25 mg orally and reached a highestdose of 1000 mg. Common side effects were nausea, skinrashes, muscle cramps and bone aches; these were mostlymild and responsive to supportive care. Myelosuppres-sion with anemia, granulocytopenia and thrombocytope-nia were also observed. Hepatotoxicity was rare. At thehigher doses, edema (periorbital, leg) and fluid retentionwere more prominent, but there were no clear-cut maxi-mally tolerated dose (MTD) or dose-limiting toxicity(DLT). The phase I study continues with lower doses ofSTI571 in combination with low-dose ara-C.
The phase I study included both chronic and blasticphase patients. The results in chronic phase CML pa-tients who had failed IFN-� therapy were recently up-dated.115 At daily oral STI571 doses of 300 mg or more,the CHR rate was 100% and cytogenetic responses wereobserved 53% of patients with complete cytogenetic re-missions in 13%. Most of these responses are maintainedwith ongoing therapy.
The results of the phase I study in blastic phase werealso recently reported at ASCO.116 A total of 51 patientswere treated with STI571 at doses of 300 to 800 mg orallydaily, and 48 were evaluable. Their median age was 53years (range 26 to 76 years); 33 had myeloid blastic phase,seven had lymphoid blastic phase, and eight had Ph-posi-tive ALL. Responses were defined as complete response(classical definition), complete response without recov-ery of peripheral counts (i.e. marrow CR), and partialresponses (marrow blasts reduction to < 15%). The re-
Table 15. Results of STI571 in chronic myelogenous leukemia(CML) blastic phase.
No. (%)Lymphoid and
Ph-positiveParameter Myeloid ALL Total
No. treated 33 15 48
Complete response 4 (12) 3 (20) 7 (15)
Marrow complete response 5 (15) 6 (40) 11 (23)
Partial response 15 (45) 2 (13) 17 (35)

106 American Society of Hematology
sults are summarized in Table 15. Most responses weretransient, lasting for a median of 3 months; few com-plete responses from myeloid blastic phase are ongoingafter one year. Three patients had complete cytogeneticresponses.
The pivotal trials have accrued over 500 patients inchronic phase and over 200 patients in accelerated phase.Updated results of the STI571 studies will be presentedat the ASH meeting.
STI571 is currently being compared to IFN-� plusara-C in a randomized trial of newly-diagnosed patients.Combinations of STI571 with low-dose ara-C and withIFN-� are in progress or planned. For CML in blasticphase and Ph-positive ALL, combinations of STI571 withstandard anti-leukemic agents warrant study. Other po-tential applications of STI571 to treat minimal residualdisease (post SCT or IFN-�), for in vitro purging, and incombinations with other agents are under evaluation.More time is needed to evaluate the drug’s effect on sur-vival and potential cure of CML. Finally, ongoing stud-ies are assessing mechanisms of drug resistance.
VI. SUMMARY AND FUTURE DIRECTIONS
Major breakthroughs have recently occurred in under-standing the pathophysiology of CML, and in its treat-ment. Of the four main therapeutic breakthroughs—allogeneic SCT, DLI, IFN-� regimens, and STI571—STI571 may have the most significant impact on patientprognosis.
It is clear that many of our current practical and in-vestigational strategies in CML will evolve aroundSTI571-based regimens. Rapid evaluations of STI571alone and in combination are needed in newly diagnosedCML patients, in advanced phase CML and in Ph-posi-tive ALL. Other molecularly targeted strategies (e.g. FTIs)and immunomodulatory approaches (cellular, vaccines)need to be evaluated. Patients failing STI571 and whohave received or are not candidates for SCT or IFN-aregimens need to undergo investigational approachesdesigned specifically for STI571 failure, aimed at revers-ing the mechanisms of resistance or at using alternatestrategies (e.g. HHT, decitabine). Finally the role and tim-ing of allogeneic SCT and IFN-� regimens need to bere-evaluated frequently as the STI571 results continue tomature.
REFERENCES
1. Melo JV, Gordon DE, Cross NC, Goldman JM. The ABL-BCRfusion gene is expressed in chronic myeloid leukemia. Blood.1993;81:158-165.
2. Melo JV. The diversity of BCR-ABL fusion proteins and theirrelationship to leukemia phenotype [editorial]. Blood.1996;88:2375-2384.
3. Melo JV, Myint H, Galton DA, Goldman JM. P190BCR-ABL
chronic myeloid leukaemia: the missing link with chronicmyelomonocytic leukaemia? [see comments]. Leukemia.1994;8:208-211.
4. Ravandi F, Cortes J, Albitar M, et al. Chronic myelogenousleukaemia with p185(BCR/ABL) expression: characteristics andclinical significance. Br.J.Haematol. 1999;107:581-586.
5. Mittre H, Leymarie P, Macro M, Leporrier M. A new case ofchronic myeloid leukemia with c3/a2 BCR/ABL junction. Is itreally a distinct disease? [letter]. Blood. 1997;89:4239-4241.
6. Puil L, Liu J, Gish G, et al. Bcr-Abl oncoproteins bind directlyto activators of the Ras signalling pathway. EMBO J.1994;13:764-773.
7. Gordon MY, Dowding CR, Riley GP, Goldman JM, GreavesMF. Altered adhesive interactions with marrow stroma ofhaematopoietic progenitor cells in chronic myeloid leukaemia.Nature. 1987;328:342-344.
8. Cortez D, Kadlec L, Pendergast AM. Structural and signalingrequirements for BCR-ABL-mediated transformation andinhibition of apoptosis. Mol Cell Biol. 1995;15:5531-5541.
9. Deininger MW, Bose S, Gora TJ, Yan XH, Goldman JM, MeloJV. Selective induction of leukemia-associated fusion genes byhigh-dose ionizing radiation. Cancer Res. 1998;58:421-425.
10. Biernaux C, Loos M, Sels A, Huez G, Stryckmans P. Detectionof major bcr-abl gene expression at a very low level in bloodcells of some healthy individuals. Blood. 1995;86:3118-3122.
11. Bose S, Deininger M, Gora TJ, Goldman JM, Melo JV. Thepresence of typical and atypical BCR ABL fusion genes inleukocytes of normal individuals: biologic significance andimplications for the assessment of minimal residual disease.Blood. 1998;92:3362-3367.
12. James HA, Gibson I. The therapeutic potential of ribozymes.Blood. 1998;91:371-382.
13. Gewirtz AM, Sokol DL, Ratajczak MZ. Nucleic acid therapeu-tics: state of the art and future prospects. Blood. 1998;92:712-736.
14. Clark RE. Antisense therapeutics in chronic myeloid leukaemia:the promise, the progress and the problems. Leukemia.2000;14:347-355.
15. Cobaleda C, Sanchez-Garcia I. In vivo inhibition by a site-specific catalytic RNA subunit of RNase P designed against theBCR-ABL oncogenic products: a novel approach for cancertreatment. Blood. 2000;95:731-737.
16. Gewirtz AM, Luger SM, Sokol DL, et al. Oligodeoxynucleotidetherapeutics for human myelogenous leukaemia: interim results.Blood. 1996;88:270a. (abstr)
17. Boutin JA. Tyrosine protein kinase inhibition and cancer. Int JBiochem. 1994;26:1203-1226.
18. Levitzki A, Gazit A. Tyrosine kinase inhibition: an approach todrug development. Science. 1995;267:1782-1788.
19. Buchdunger E, Zimmermann J, Mett H, et al. Inhibition of theAbl protein-tyrosine kinase in vitro and in vivo by a 2-phenylaminopyrimidine derivative. Cancer Res. 1996;56:100-104.
20. Deininger MW, Vieira S, Mendiola R, Schultheis B, GoldmanJM, Melo JV. BCR-ABL tyrosine kinase activity regulates theexpression of multiple genes implicated in the pathogenesis ofchronic myeloid leukemia. Cancer Res. 2000;60:2049-2055.
21. Druker BJ, Tamura S, Buchdunger E, et al. Effects of a selectiveinhibitor of the Abl tyrosine kinase on the growth of Bcr-Ablpositive cells. Nat Med. 1996;2:561-566.
22. Deininger MWN, Goldman JM, Lydon NB, Melo JV. Thetyrosine kinase inhibitor CGP57148B selectively inhibits thegrowth of BCR-ABL positive cells. Blood. 1997;90:3691-3698.
23. Beran M, Cao X, Estrov Z, et al. Selective inhibition of cellproliferation and BCR-ABL phosphorylation in acute lympho-blastic leukemia cells expressing Mr 190,000 BCR-ABLproteinby a tyrosine kinase inhibitor (CGP-57184). Clin Cancer Res.

Hematology 2000 107
1998;4:1661.24. le Coutre P, Tassi E, Varella-Garcia M, et al. Induction of
resistance to the Abelson inhibitor STI571 in human leukemiccells through gene amplification. Blood. 2000;95:1758-1766.
25. Thiesing JT, Ohno-Jones S, Kolibaba K, Druker BJ. Efficacy ofan Abl tyrosine kinase inhibitor in conjunction with other anti-neoplastic agents against Bcr-Abl positive cells. Blood.1999;94:100-101a. (abstr)
26. Deisseroth A, Wang T, Guo XYD, et al. Use of computationaland combinatorial chemistry to develop chemical inhibitors ofthe Abl kinase and the Ras G proteins for treatment of chronicmyelogenous leukemia. Blood. 2000;94:101a. (abstr)
27. Liu J, Yang Y, Wu Y, Estrov Z, Talpaz M, Arlinghaus R.Induction of cell adhesion and inhibition of cell growth in CMLcell lines by expression of BCR(64-413) using a recombinantadenovirus. Blood. 1998;90:91a. (abstr)
28. Emanuel PD, Snyder RC, Wiley T, Gopurala B, Castleberry RP.Inhibition of juvenile myelomonocytic leukemia cell growth invitro by farnesyltransferase inhibitors. Blood. 2000;95:639-645.
29. Skorski T, Kanakaraj P, Nieborowska SM, et al.Phosphatidylinositaol-kinase activity is regulated by BCR/ABLand is required for the growth of Philadelphia chromosome-positive cells. Blood 1995;86:726-736.
30. Falkenburg JH, Wafelman AR, Joosten P, et al. Completeremission of accelerated phase chronic myeloid leukemia bytreatment with leukemia-reactive cytotoxic T lymphocytes.Blood. 1999;94:1201-1208.
31. Molldrem JJ, Clave E, Jiang YZ, et al. Cytotoxic T lymphocytesspecific for a nonpolymorphic proteinase 3 peptide preferen-tially inhibit chronic myeloid leukemia colony-forming units.Blood. 1997;90:2529-2534.
32. Warren EH, Gavin M, Greenberg PD, Riddell SR. Minorhistocompatibility antigens as targets for T-cell therapy afterbone marrow transplantation. Curr Opin Hematol. 1998;5:429-433.
33. Ohminami H, Yasukawa M, Fujita S. HLA class I-restrictedlysis of leukemia cells by a CD8(+) cytotoxic T- lymphocyteclone specific for WT1 peptide. Blood. 2000;95:286-293.
34. Pinilla-Ibarz J, Cathcart K, Korontsvit T, et al. Vaccination ofpatients with chronic myelogenous leukemia with bcr-abloncogene breakpoint fusion peptides generates specific immuneresponses. Blood. 2000; 95:1781-1787.
35. Faderl S, Talpaz M, Estrov Z, Kantarjian HM. Chronicmyelogenous leukemia: biology and therapy. Ann Intern Med.1999;131:207.
36. Talpaz M, Kantarjian H, Kurzrock R, et al. Interferon-alphaproduces sustained cytogenetic responses in chronic myelog-enous leukemia. Ann Intern Med. 1991;114:532.
37. Italian Cooperative Study Group on Chronic Myeloid Leukemia.Interferon Alfa-2a compared with conventional chemotherapyfor the treatment of chronic myeloid leukemia. N Engl J Med.1994;330:820.
38. Hehlmann R, Heimpel H, Hasford J, et al. Randomizedcomparison of Interferon-a with busulfan and hydroxyurea inchronic myelogenous leukemia. Blood. 1994;84:4064.
39. Allan NC, Richards SM, Shepherd PCA, et al.: UK MedicalResearch Council randomised, multicentre trial of interferon-an1for chronic myeloid leukaemia: improved survival irrespectiveof cytogenetic response. Lancet. 1995;345:1392.
40. The Italian Cooperative Study Group on Chronic MyeloidLeukemia; Long-term follow-up of the Italian trial of Interferon-a versus conventional chemotherapy in chronic myeloidleukemia. Blood. 1998;92:1541.
41. Chronic Myeloid Leukemia Trialists’ Collaborative Group:Interferon alfa versus chemotherapy for chronic myeloidleukemia: a meta-analysis of seven randomized trials. J NatlCancer Inst. 89:1616, 1997
42. Platanias LC, Fish EN. Signaling pathways activated byinterferons. Exp Hematol. 1999;27:1583.
43. Bocchia M, Korontsvit T, Xu Q, et al. Specific human cellularimmunity to bcr-abl oncogene-derived peptides. Blood.1996;87:3587.
44. Ten Bosch GJA, Kessler JH, Joosten AM, et al. A BCR-ABLoncoprotein p210b2a2 fusion region sequence is recognized byHLA-DR2a restricted cytotoxic T lymphocytes and presented byHLA-DR matched cells transfected with an Iib2a2 construct.Blood. 1999;94:1038.
45. Pane F, Mostarda I, Selleri C, et al. BCR/ABL mRNA and theP210BCR/ABL protein are downmodulated by interferon-� inchronic myeloid leukemia patients. Blood. 1999;94:2200.
46. Mahon FX, Faberes C, Pueyo S, et al. Response at three monthsis a good predictive factor for newly diagnosed chronic myeloidleukemia patients treated by recombinant interferon-�. Blood.1998;11:4059.
47. Chomel JC, Briward F, Veinstein A, et al. Persistence of BCR/ABL genomic rearrangement in chronic myeloid leukemiapatients in complete and sustained cytogenetic remission afterinterferon-� therapy or allogeneic bone marrow transplantation.Blood. 2000;95:404.
48. Hochhaus A, Reiter A, SauBele S, et al. Molecular heterogeneityin complete cytogenetic responders after interferon-� therapyfor chronic myelogenous leukemia: low levels of minimalresidual disease are associated with continuing remission.Blood. 2000;95:62.
49. Faderl S, Talpaz M, Kantarjian HM, Estrov Z. Should poly-merase chain reaction analysis to detect minimal residual diseasein patients with chronic myelogenous leukemia be used inclinical decision making? Blood. 1999;93:2755.
50. Goldman JM, Kaeda JS, Cross NCP, et al. Clinical decisionmaking in chronic myeloid leukemia based on polymerase chainreaction analysis of minimal residual disease (Letter). Blood.1999;94:1484.
- Lion T. Monitoring of residual disease in chronic myelogenousleukemia by quantitative polymerase chain reaction and clinicaldecision making (Letter) Blood. 1999;94:1486.
- Faderl S, Talpaz M, Kantarjian H, Estrov Z. Should polymerasechain reaction analysis to detect minimal residual disease inpatients with chronic myelogenous leukemia be used in clinicalmaking? (Letter, response) Blood. 1999;94:1487.
51. Sokal JE, Cox EB, Baccarani M, et al. Prognostic discriminationin “good-risk” chronic granulocytic leukemia. Blood.1984;63:789.
52. Hasford J, Pfirrmann M, Hehlmann R, et al. (Writing Commit-tee for the Collaborative CML Prognostic Factors ProjectGroup): A new prognostic score for survival of patients withchronic myeloid leukemia treated with Interferon alfa. J NatlCancer Inst. 1998;90:850.
53. Italian Cooperative Study Group on Chronic Myeloid Leukemiaand Italian Group for Bone Marrow Transplantation. Monitoringtreatment and survival in chronic myeloid leukemia. J ClinOncol. 1999;17:1858.
54. Tura S. �-Interferon versus allogeneic stem cell transplantationin early chronic phase chronic myelogenous leukemia: strategiesby age and risk group. In Schechter GP, Hoffman R, Schrier S,eds. Hematology 1999 American Society of HematologyEducation Program Book. New Orleans, LA; 1999:156-159.
55. Gratwohl A, Hermans J, Goldman JM, et al. Risk assessment forpatients with chronic myeloid leukaemia before allogeneic bloodor marrow transplantation. Lancet. 1998;352:1087.
56. Le Coutre P, Mologni L, Cleris L, et al. In vivo eradication ofhuman BCR/ABL-positive leukemia cells with an ABL kinaseinhibitor. J Natl Cancer Inst. 1999;91:163.
57. Hehlmann R, Berger U, Hochhaus A, et al. Randomizedcomparison of allogeneic bone marrow transplantation and IFN

108 American Society of Hematology
based drug treatment in CML. Proc ASCO. 1999;19:10.58. Silberman G, Crosse MG, Peterson EA, et al. Availability and
appropriateness of allogeneic bone marrow transplantation forchronic myeloid leukemia in 10 countries. N Engl J Med.1994;331:1063.
59. McGlave PB, Ou SX, Wanqing W, et al. Unrelated donormarrow transplantation for chronic myelogenous leukemia: 9years’ experience of the National Marrow Donor Program.Blood. 2000;95:2219.
60. Beatty PG, Clift RA, Mickelson EM, et al. Marrow transplanta-tion from related donors other than HLA identical siblings. NEngl J Med. 1985;313:765.
61. Spencer A, Szydlo R, Brookes PA, et al. Bone marrowtransplantation for chronic myeloid leukemia with volunteerunrelated donors using ex-vivo or in-vivo T-cell depletion: majorprognostic impact of HLA class I identity between donor andrecipient. Blood. 1995;86:3590.
62. Hansen JA, Gooley TA, Martin P, et al. Bone marrow transplantswith unrelated donors for patients with chronic myeloidleukemia. N Engl J Med. 1998;338:962.
63. Drobyski WR, Ash RC, Casper JT, et al. Effect of T celldepletion as graft-versus-host disease prophylaxis on engraft-ment, relapse, and disease free survival in unrelated marrowtransplantation for chronic myelogenous leukemia Blood.1994;83:1980.
64. Ochs L, Ou Shu X, Miller J, et al. Late infections afterallogeneic bone marrow transplantation: comparison ofincidence in related and unrelated donor transplant recipients.Blood. 1996;86:3979.
65. Beatty PG, Anasetti C, Hansen JA, et al. Marrow transplantationfrom unrelated donors for treatment of hematologic malignan-cies: effect of mismatching for one HLA locus. Blood.1993;81:249.
66. Petersdorf EW, Gooley TA, Anasetti C, et al. Optimizingoutcome after unrelated marrow transplantation by comprehen-sive matching of HLA class I and II alleles in the donor andrecipient. Blood. 1998;92:3515.
67. Sasazuki T, Juji T, Morishima Y, et al. Effect of matching ofclass I HLA alleles on clinical outcome after transplantation ofhematopoietic stem cell donors from an unrelated donor. N EnglJ Med. 1998;339:1177.
68. Kantarjian H, Melo J, Talpaz M, Tura S, Kolb HJ, Druker B.Chronic myelogenous leukemia. In Schechter GP, Hoffman R,Schrier S, eds. Hematology 1999 American Society of Hematol-ogy Education Program Book. New Orleans, LA; 1999:143.
69. Kolb HJ, Schttenberg A, Goldman JM, et al. Graft-versus-leukemia effect of donor lymphocye transfusions in marrowgrafted patients. Blood. 1995;86:2041.
70. Collins RH, Shpilberg O, Drobyski WR, et al. Donor leukocyteinfusions in 140 patients with relapsed malignancy afterallogeneic bone marrow transplantation. J Clin Oncol.1997;15:433.
71. Shimoni A, Anderlini P, Andersson B, et al. CD8-depleted donorlymphocyte (DLI) for the treatment of CML relapse afterallogeneic transplant: long term follow up and factors predictingof outcome. Blood. 1999;94(Suppl 1):160a.
72. Alyea E, Soiffer RJ, Canning C, et al. Toxicity and efficacy ofdefined doses of CD4+ donor lymphocytes for treatment ofrelapse after allogeneic bone marrow transplant. Blood.1998;91:3671.
73. MacKinnon S, Papadopoulos EB, Carabasi MH, Reich L,Collins NH, O’Reilly RJ. Adoptive immunotherapy using donorleukocytes following bone marrow transplantation for chronicmyeloid leukemia: is T cell dose important in determiningbiological response? Bone Marrow Transplant. 1995;15:591-4.
74. Dazzi F, Szydlo M, Craddock C, et al. Comparison of single-dose and escalating-dose regimens of donor lymphocyte
infusion for relapse after allografting for chronic myeloidleukemia. Blood. 2000;95:67.
75. Bonini C, Marktel S, Zappone E, et al. Long term follow up in30 patients receiving HSV-TK transduced donor lymphocytesafter allo-BMT. Blood 1999;94(Suppl 1):668a.
76. Champlin R, Bensinger W, Henslee-Downey J, et al. Phase I/IIstudy of thymidine kinase (TK)-transduced donor lymphocyteinfusions (DLI) in patients with hematologic malignancies.Blood. 1999;94(Suppl 1):324a.
77. Champlin R, Khouri I, Kornblau S, Molldrem J, Giralt S.Reinventing bone marrow transplantation. Nonmyeloablativepreparative regimens and induction of graft vs malignancyeffect. Oncology. 1999;13:621.
78. McSweeney P, Niederwieser D, Shizuru J, et al. Outpatientallografting with minimally myelosuppressive conditioning oflow-dose TBI and postgrafting cyclosporine (CSA) andmycophenolate mofetil (MMF). Blood. 1999;94(Suppl 1):393a.
79. Kantarjian HM, O’Brien S, Anderlini P, Talpaz M. Treatment ofchronic myelogneous leukemia: Current status and investiga-tional options. Blood. 1996;87:3069-1081.
80. Daley GQ, Van Etten RA, Baltimore D. Induction of chronicmyelogenous leukemia in mice by the P210BCR/ABL gene ofthe Philadelphia chromosome. Science. 1990;274:824-830.
81. Kelliher MA, McLaughlin J, Witte ON, Rosenberg N. Inductionof a chronic myelogenous leukemia-like syndrome in mice withv-abl and bcr/abl. Proc Natl Acad Sci USA. 1990;87:6659-6653.
82. Carroll M, Ohno-Jones S, Tamura S, et al. CGP 47148, atyrosine kinase inhibitor, inhibits the growth of cells expressingBCR-ABL, TEL-ABL and TEL-PDGFR fusion proteins. Blood.1997;90:4947.
83. Le Courtre P, Mologni L, Cleris L, et al. Eradication of humanBCR/ABL positive leukemia cells with an ABL kinase inhibitor.J Natl Cancer Inst. 1999;91:163-168.
84. Kantarjian HM, Smith TL, O’Brien S, et al. Prolonged survivalin chronic myelogenous leukemia after cytogenetic response tointerferon-� therapy. Ann Intern Med. 1996;122:254-261.
85. Kurzrock R, Estrov Z, Kantarjian H, et al. Conversion ofinterferon-induced, long-term cytogenetic remissions in chronicmyelogenous leukemia to polymerase chain reaction negativity.J Clin Oncol. 1998;16:1526-1531.
86. Sokal J. Leong S, Gomez G. Preferential inhibition bycytarabine of CFR-GM from patients with chronic granulocyticleukemia. Cancer. 1987;59:197-202.
87. Sokal J, Beinger SH. Low-dose cytosine arabinoside bysubcutaneous infusion in early and advanced chronic granulo-cytic leukemia. Blood. 1986;68:233a. (abstr)
88. Robertson MJ, Tantravahi R, Griffin JD, Canellos GP, CannistraSA. Hematologic remission and cytogenetic improvement aftertreatment of stable-phase chronic myelogenous leukemia withcontinuous infusion of low-dose cytarabine. Am J Hematol.1993;43:95-102.
89. Kantarjian H, Keating M, Estey E, et al. Treatment of advancedPhiladelphia chromosome-positive chronic myelogenousleukemia with interferon-� and low-dose cytarabine. J ClinOncol. 1992;10:772-778.
90. Kantarjian HM, O’Brien S, Smith TL, et al. Treatment ofPhiladelphia chromosome-positive early chronic phase chronicmyelogenous leukemia with daily doses of interferon alpha andlow-dose cytarabine. J Clin Oncol. 1999;17:284-292.
91. Arthur CK, Ma DFF. Combined interferon alpha-2a andcytosine arabinoside as first-line treatment for chronic myeloidleukemia. Acta Haematol. 1993;89(Suppl 1):15-21.
92. Thaler J, Hilbe W, Apfelbeck U, et al. Interferon-alpha-2c andlow-dose ara-C for the treatment of patients with CML: resultsof the Austrian multi-center phase study. Leukemia Res.1997;21:75.
93. Silver R, Szatrowski T, Peterson B, et al. Combined �-interferon

Hematology 2000 109
and low-dose cytosine arabinoside for Ph+ chronic phasemyeloid leukemia. Blood. 1996;88(Suppl 1):638a.
94. Guilhot F, Chastang C, Michallet M, et al. Interferon alfa-2bcombined with cytarabine versus interferon alone in chronicmyelogenous leukemia. N Engl J Med. 1997;337:223-229.
95. Guilhot F, Maloisel F, Guyotat D, et al. Significant survivalimprovement with a combination of interferon alpha 2b andcytarabine in chronic myeloid leukemia. Update of a random-ized trial. Proc ASCO. 1999;18:7a.
96. Rosti G, Bonifazi F, De Vivo A, et al. Cytarabine increaseskaryotypic response and survival in �IFN treated chronicmyelogenous leukemia patients: Results of a national prospec-tive randomized trial of the Italian Cooperative Study Group onCML. Blood. 1999;94:2669.
97. O’Brien SM, Kantarjian H, Keating M, et al. Homoharrring-tonine therapy induces responses in patients with chronicmyelogenous leukemia in late chronic phase. Blood.1995;86:3322-6.
98. O’Brien S, Kantarjian H, Koller C, et al. Sequentialhomoharringtonine and interferon-� in the treatment of earlychronic myelogenous leukemia. Blood. 1999;93:4149-4153.
99. Kantarjian HM, Talpaz M, Cortes J, et al. Triple combinationtherapy with interferon-alpha, low-dose cytarabine andhomoharringtonine in Philadelphia chromosome-positivechronic myelogenous leukemia in early chronic phase. Blood.1999;94(Suppl 1):4440.
100. O’Brien S, Talpaz M, Giles FJ, et al. Simultaneous interferonalpha and homoharringtonine is an effective in Philadelphiachromosome (Ph)-positive chronic myelogenous leukemia.Blood. 1999;94(Suppl 1):278b.
101. Ernst TJ, Vance E, Alyea E, III, Soiffer R, Quartulli M, Ritz J.Homoharringtonine and low-dose ara-C is a highly effectivecombination for the treatment of CML in chronic phase. Blood.1997;90(Suppl 1):571a. (abstr)
102. Ben-Yehuda D, Krichevsky S, Rachmilewitz EA, et al.Molecular follow-up of disease progression and interferontherapy in chronic myelocytic leukemia. Blood. 1997;90:4918.
103. Issa J-P, Kantarjian H, Mohan A, et al. Methylation of theABLI promoter in chronic myelogenous leukemia: lack ofprognostic significance. Blood. 1999;93:2075-2080.
104. Kantarjian HM, O’Brien SM, Keating M, et al: Results ofdecitabine therapy in the accelerated and blastic phase ofchronic myelogenous leukemia. Leukemia. 1997;11:1617-20.
105. Sacchi S, Kantarjian HM, O’Brien S, et al. Chronic myelog-enous leukemia in non-lymphoid blastic phase: analysis of theresults of first salvage therapy with three different treatmentapproaches in 162 patients. Cancer. 1999;86:2632-41.
106. Kantarjian HM, O’Brien SM, Estey E, et al. Decitabine studiesin chronic and acute myelogenous leukemia. Leukemia1997;11(Suppl 1):S35-36.
107. Talpaz M, Cortes J, O’Brien S, et al. Phase I study ofpolyethylene glycol interferon alpha-2b in CML patients(abstract]. Blood. 1998;92(Suppl 1):251.
108. Carlo Stella C, Dotti G, Mangoni L, et al. Selection of myeloidprogenitors lacking BCR/ABL mRNA in chronic myelogenousleukemia patients after in vitro treatment with the tyrosinekinase inhibitor genistein. Blood. 1996;88:3091-3100.
109. Okabe M, Uehara Y, Miyagishima T, et al. Effect ofherbimycin A, an antagonist of tyrosine kinase, on bcr/abloncoprotein-associated cell proliferations: abrogative effect onthe transformation of murine hematopoietic cells by transfec-tion of a retroviral vector expressing oncoprotein P210bcr/abland preferential inhibition on Ph1-positive leukemia cellgrowth. Blood. 1992;80:1330-1338.
110. Anafi M, Gazit A, Zehavi A, Ben NY, Levitzki A. Tyrphostin-induced inhibition of p210bcr-abl tyrosine kinase activityinduces K562 to differentiate. Blood. 1993;82:3524-3529.
111. Bhatia R, Munthe HA, Verfaillie CM. Tyrphostin AG957, atyrosine kinase inhibitor with anti-BCR/ABL tyrosine kinaseactivity restores beta1 integrin-mediated adhesion andinhibitory signaling in chronic myelogenous leukemiahematopoietic progenitors. Leukemia. 1998;12:1708-1717.
112. Yaish P, Gazit A, Gilon C, Levitzki A, et al. Blocking of EGF-dependent cell proliferation by EGF receptor kinase inhibitors.Science 242:933, 1988.
113. Carroll M, Ohno-Jones S, Tamura S, et al. CGP 57148, atyrosine kinase inhibitor, inhibits the growth of cells expressingBCR-ABL, TEL-ABL and TEL-PDGFR fusion proteins.Blood. 90:4947, 1997.
114. le Coutre P, Mologni L, Cleris L, et al. In vivo eradication ofhuman BCR/ABL positive leukemia cells with an ABL kinaseinhibitor. J Natl Cancer Inst. 1999;91:163-168.
115. Druker BJ, Talpaz M, Resta D, et al. Clinical efficacy andsafety of an ABL specific tyrosine kinase inhibitor as targetedtherapy for chronic myelogenous leukemia. Blood. 19(Suppl1):368a, 1999.
116. Talpaz M, Sawyers CL, Kantarjian H, et al. Activity of an ABLspecific tyrosine kinase inhibitor in patients with BCR-ABLpositive acute leukemias, including chronic myelogenousleukemia in blast crisis. Proc ASCO. 19:4a, 2000.