chronic obstructive pulmonary disease … · clinical pathway checklist process ... if patient co 2...
TRANSCRIPT

VOIDED
DISCUSSION BEGUN RE: CODE STATUS OR LIMITS TO INTERVENTIONS
DISCHARGED PATIENT HAS CCAC REFERRAL, WITH PERMISSION
ER TRANSFER SIGNATURE:
DISCHARGED PATIENT UNDERSTANDS THE NEED FOR SPIROMETRY
APPOINTMENT FOR FOLLOW-UP, IF NO PREVIOUS RESULTS
ER ADMISSION SIGNATURE:
CHRONIC OBSTRUCTIVE
PULMONARY DISEASE
CXR ABG's ECG
DISCHARGED PATIENT HAS BLUE COPD FOLDER WHICH INCLUDES THE
PLAN OF ACTION ON WHEN TO RETURN TO ER IF NECESSARY
OTHER:
BEST MEDICINE RECONCILIATON BEFORE DISHCARGE TO ASSESS FOR
PATIENT ADMINISTRATION KNOWLEDGE
DISCHARGED PATIENT UNDERSTANDS TO FOLLOW-UP WITH PRIMARY
PRACTITIONER WITHIN 1 WEEK
ABLE TO MOBILIZE SHORT DISTANCE BEFORE DISCHARE (e.g.. 6 MINUTE
WALK TEST) TO CONSIDER FOR DISCHARGED PATIENTS
MEDICATIONS
ANTIBIOTIC GIVEN WITHIN ONE HOUR OF PRESENTATION
VTE ASSESSMENT COMPLETED FOR ADMISSION
MOBILITY/
ACTIVITY
OTHER:
CAM TOOL COMPLETED
LABORATORY /
DIAGNOSTICS
ABNORMAL BLOOD WORK RESULTS REPORTED
(CBC, ELECTROLYTES, UREA, CREATININE, GLUCOSE)
CULTURE SPUTUM:
DISCHARGE
FROM ER
SATS ORDERED TO BE MAINTAINED: � > 92% � 88% - 92%
Notify physician if oxygen requirement exceeds 50%
DOCUMENT NOTIFICATION TIME OF PHYSICIAN FOR DYSPNEA SCALE >
7, TEMPERATURE > 38.5 SIGNS OF HYPO/HYPERTENSION, SATS < 88%
REPORTED TO
INPUT UNIT
ASSESSMENT
INITIAL VITAL SIGNS INCLUDE O2 SATS & TEMPERATURE BEFORE
LEAVING DEPARTMENT
* CHEST ASSESSMENT - RATE, COUGH, PRODUCTIVE (COLOUR NOTED),
EFFORT & HYPOVENTILATION
* BRONCHODILATOR EFFECT PRE & POST DOSE(S) DOCUMENTED
If patient CO2 retainer, consider compressed air for nebulization.
GREY BRUCE HEALTH NETWORK
CLINICAL PATHWAY CHECKLIST
PROCESS
ER DISCHARGE/ADMISSION CHECKLIST DATE/TIME DATE/TIME
���� = Done/Yes ���� = Not Done/No N/A = Not Applicable
* requires descriptive charting in progress notes ER DISCHARGE
Updated Apr 2013© 2006 - 2013 Grey Bruce Health Network 1
Review Apr 2016
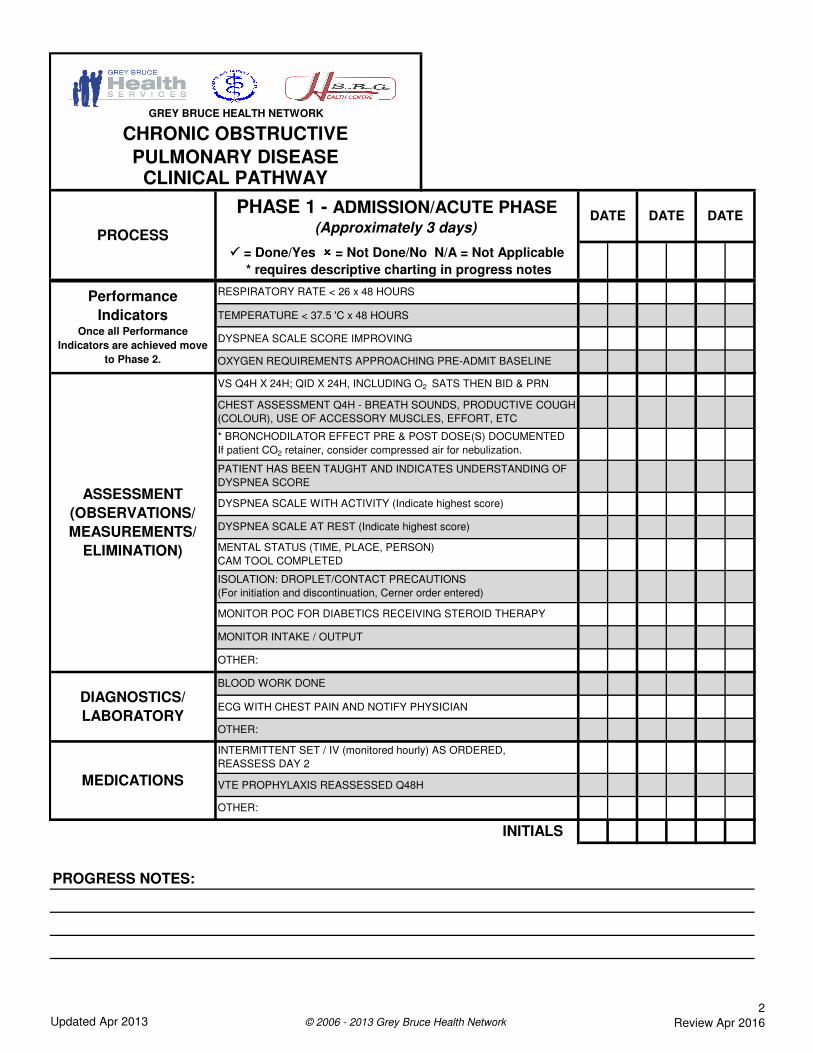
TEMPERATURE < 37.5 'C x 48 HOURS
DYSPNEA SCALE SCORE IMPROVING
ECG WITH CHEST PAIN AND NOTIFY PHYSICIAN
VTE PROPHYLAXIS REASSESSED Q48H
PROGRESS NOTES:
OXYGEN REQUIREMENTS APPROACHING PRE-ADMIT BASELINE
DIAGNOSTICS/
LABORATORY
BLOOD WORK DONE
OTHER:
MEDICATIONS
INTERMITTENT SET / IV (monitored hourly) AS ORDERED,
REASSESS DAY 2
OTHER:
DYSPNEA SCALE AT REST (Indicate highest score)
MENTAL STATUS (TIME, PLACE, PERSON)
CAM TOOL COMPLETED
ISOLATION: DROPLET/CONTACT PRECAUTIONS
(For initiation and discontinuation, Cerner order entered)
MONITOR POC FOR DIABETICS RECEIVING STEROID THERAPY
MONITOR INTAKE / OUTPUT
OTHER:
DATE
���� = Done/Yes ���� = Not Done/No N/A = Not Applicable
* requires descriptive charting in progress notes
Performance
IndicatorsOnce all Performance
Indicators are achieved move
to Phase 2.
RESPIRATORY RATE < 26 x 48 HOURS
ASSESSMENT
(OBSERVATIONS/
MEASUREMENTS/
ELIMINATION)
VS Q4H X 24H; QID X 24H, INCLUDING O2 SATS THEN BID & PRN
CHEST ASSESSMENT Q4H - BREATH SOUNDS, PRODUCTIVE COUGH
(COLOUR), USE OF ACCESSORY MUSCLES, EFFORT, ETC
* BRONCHODILATOR EFFECT PRE & POST DOSE(S) DOCUMENTED
If patient CO2 retainer, consider compressed air for nebulization.
PATIENT HAS BEEN TAUGHT AND INDICATES UNDERSTANDING OF
DYSPNEA SCORE
DYSPNEA SCALE WITH ACTIVITY (Indicate highest score)
INITIALS
GREY BRUCE HEALTH NETWORK
CHRONIC OBSTRUCTIVE
PULMONARY DISEASECLINICAL PATHWAY
PROCESS
PHASE 1 - ADMISSION/ACUTE PHASE (Approximately 3 days)
DATE DATE
Updated Apr 2013 © 2006 - 2013 Grey Bruce Health Network
2
Review Apr 2016

DNR WISHES DISCUSSION ADDRESSED AND RECORDED
OTHER:
OTHER:
SMOKING CESSATION INFO HAS BEEN GIVEN / REINFORCED
OTHER:
PROGRESS NOTES:
CCAC REFERRAL ON ALL COPD DIAGNOSED PATIENTS, WITH
PERMISSION
OTHER:
DISCHARGE
PLANNING
GREY BRUCE HEALTH NETWORK
CHRONIC OBSTRUCTIVE
PULMONARY DISEASECLINICAL PATHWAY
MOBILITY/ACTIVITY
ASSIST PERSONAL HYGIENE
PSYCHOSOCIAL
SUPPORT
ASSESS ANXIETY AND INTERVENE
EDUCATION
REVIEW PATIENT PATHWAY
START AND CONTINUE WITH TEACHING CHECKLIST
ASSESS DISCHARGE CRITERIA DAILY
BRPs WITH ASSISTANCE, INCREASE TO AAT
WALK IN HALLWAY DAILY WITH GOAL OF 9 METERS QSHIFT
BEFORE DISCHARGE
PROCESS
PHASE 1 - ADMISSION/ACUTE PHASE (Approximately 3 days)
NUTRITION
REGULAR DIET OR SPECIAL DIET ____________________________,
NUTRITION INTAKE A - Adequate IN - INadequate
ENCOURAGE FLUIDS 2 - 3 LITRES/DAY
DATE
���� = Done/Yes ���� = Not Done/No N/A = Not Applicable
* requires descriptive charting in progress notes
DATE DATE
INITIALS
Updated Apr 2013 © 2006 - 2013 Grey Bruce Health Network
3
Review Apr 2016

PROGRESS NOTES:
RESPIRATORY CONSULT
SOCIAL WORK CONSULT
SPEECH THERAPY / SWALLOWING CONSULT
WOUND CLINICIAN CONSULT
OTHER:
OTHER:
MULTIDICIPLINARY CONSULTS
CCAC CONSULT
CLINICAL NUTRITION CONSULE
OCCUPATIONAL THERAPY CONSULT
PHARMACY CONSULT
PHYSIOTHERAPY CONSULT
DATE OF
ASSESSMENT /
SIGNATURE
DATE OF
CONSULT
ASSESS SUPPORT SYSTEMS FOR PATIEN (FAMILY, FRIENDS, FINANCES, ETC) AND ENGAGE
MULTIDISCIPLINARY TEAM AS NEEDED (PHYSICIAN ORDER REQUIRED FOR TREATMENT)
GREY BRUCE HEALTH NETWORK
CHRONIC OBSTRUCTIVE
PULMONARY DISEASECLINICAL PATHWAY
Updated Apr 2013 © 2006 - 2013 Grey Bruce Health Network
4
Review Apr 2016

GREY BRUCE HEALTH NETWORK
CHRONIC OBSTRUCTIVE
PULMONARY DISEASE
CHEST ASSESSMENT DOCUMENTATION PAGE
DATE: ____________ TIME: __________ INITIAL: _______
DYSPNEA SCORE: Activity _______ Rest _______
DATE: ____________ TIME: __________ INITIAL: _______
DYSPNEA SCORE: Activity _______ Rest _______
PATIENT ID
DATE: ____________ TIME: __________ INITIAL: _______
DYSPNEA SCORE: Activity _______ Rest _______
DATE: ____________ TIME: __________ INITIAL: _______
DYSPNEA SCORE: Activity _______ Rest _______
DATE: ____________ TIME: __________ INITIAL: _______
DYSPNEA SCORE: Activity _______ Rest _______
DATE: ____________ TIME: __________ INITIAL: _______
DYSPNEA SCORE: Activity _______ Rest _______
Updated Apr 2013© 2006 - 2013 Grey Bruce Health Network 5
Review Apr 2016

All rights reserved. No part of this document may be reproduced or transmitted,
in any form or by any means, without the prior permission of the copyright owner.
LEGEND:
W - WHEEZES
C - CRACKLES
A - ABSENT BREATH SOUNDS
0 - Nothing at allNOTIFY PHYSICIAN IF NOT RESOLVED WITH
BRONCHODILATOR:
1 - Very slight 7 - Very severe
DYSPNEA SCALE
3 - Moderate NOTIFY PHYSICIAN IMMEDIATELY IF:
4 - Somewhat severe 9 - Very, very severe (almost maximal)
Maintain Sats Between:
6 -
5 - Severe 10 - Maximal
SAMPLE
POSTERIOR VIEW (LEFT/RIGHT)
2 - Slight 8 -
Baseline Oxygen Requirements:
INSTRUCTIONS FOR CHEST ASSESSMENT DOCUMENTATION PAGE:
On the diagram, record the various lung sounds heard using a series of legend-identified symbols.
WW
C C
C C
C C
C C
L R
Updated Apr 2013 © 2006 - 2013 Grey Bruce Health Network Review Apr 2016

OTHER:
INITIALS
PROGRESS NOTES:
PROCESS
OFF SUPPLEMENTAL OXYGEN OR ON USUAL HOME O2
DATE
LABORATORY /
DIAGNOSTIC
CXR IF NOT IMPROVING
OTHER:
CONSULTS
VS BID ONCE STABLE & PRN, INCLUDING O2 SATS
HOME O2 THERAPY AS NEEDED (ABG RESULTS REQUIRED)
DYSPNEA SCALE AT REST
CAM TOOL
OTHER:
ABG’s
DYSPNEA SCALE WITH ACTIVITY
ISOLATION DISCONTINUED & ORDER ENTERED IN CERNER
CHEST ASSESSMENT (BREATH SOUNDS, PRODUCTIVE COUGH)
PHASE 2 - MAINTENANCE PHASE(Approximately 2 days)
DATE
PATIENT INDICATES KNOWLEDGE OF CHRONIC DISEASE MANAGEMENT
AND DISCHARGE PLAN
���� = Done/Yes ���� = Not Done/No N/A = Not Applicable
* requires descriptive charting in progress notes
DATE
ASSESSMENT
(OBSERVATIONS/
MEASUREMENTS/
ELIMINATION)
GREY BRUCE HEALTH NETWORK
CHRONIC OBSTRUCTIVE
PULMONARY DISEASECLINICAL PATHWAY
DYSPNEA SCALE SCORE < 5
ACTIVITY LEVEL AS PER PREADMISSION
USUAL MENTAL STATUS
TEMPERATURE LESS THAN 37.5° C
PERFORMANCE
INDICATORS (DISCHARGE READINESS)
Updated Apr 2013© 2006 - 2013 Grey Bruce Health Network 7
Review Apr 2016

ASSESS PROPER USE OF INHALERS
INITIALS
PROGRESS NOTES:
DATE
���� = Done/Yes ���� = Not Done/No N/A = Not Applicable
* requires descriptive charting in progress notes
PATIENT OWNED PORTABLE OXYGEN AVAILABLE FOR DISCHARGE
BRONCHODILATOR TREATMENT EFFECTIVE AND ASSESSED QSHIFT
PATIENT ABLE TO AMBULATE AS TOLERATED
CHRONIC OBSTRUCTIVE
PULMONARY DISEASE
ADEQUATE DIET INTAKE AND ENCOURAGE FLUIDS 2 - 3 LITRES/DAY
DIET SUPPLEMENTS IF INADEQUATE NUTRITION
MOBILITY /
ACTIVITY
PATIENT ABLE TO COMPLETE ADL'S WITH MINIMAL ASSISTANCE
TRANSPORTATION ARRANGED FOR PENDING DISCHARGE
REVIEW DISCHARGE PLANS WITH PATIENT
CCAC ENGAGED AND EQUIPMENT AND SUPPORTS IDENTIFIED PRE-
DISCHARGE
REINFORCE SMOKING CESSATION EDUCATION
NUTRITION
DISCHARGE
READINESS
PROCESS
PHASE 2 - MAINTENANCE PHASE(Approximately 2 days)
START AND CONTINUE WITH TEACHING CHECKLIST
OTHER: TREATMENTS/
INTERVENTIONSOTHER:
REVIEW PATIENT PATHWAY
EDUCATION
GREY BRUCE HEALTH NETWORK
CLINICAL PATHWAY
DATE DATE
Updated Apr 2013© 2006 - 2013 Grey Bruce Health Network 8
Review Apr 2016
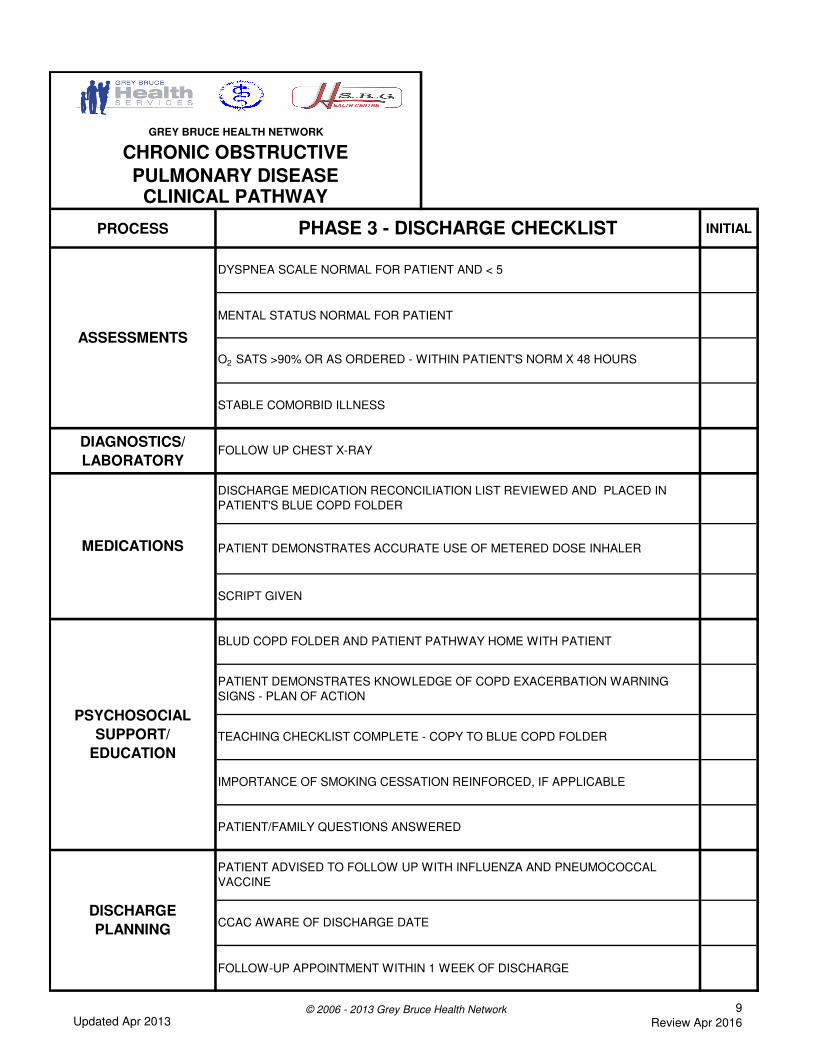
PROCESS INITIAL
MENTAL STATUS NORMAL FOR PATIENT
DIAGNOSTICS/
LABORATORY
FOLLOW-UP APPOINTMENT WITHIN 1 WEEK OF DISCHARGE
FOLLOW UP CHEST X-RAY
PHASE 3 - DISCHARGE CHECKLIST
DISCHARGE MEDICATION RECONCILIATION LIST REVIEWED AND PLACED IN
PATIENT'S BLUE COPD FOLDER
CCAC AWARE OF DISCHARGE DATE
PATIENT ADVISED TO FOLLOW UP WITH INFLUENZA AND PNEUMOCOCCAL
VACCINE
ASSESSMENTS
PSYCHOSOCIAL
SUPPORT/
EDUCATION
GREY BRUCE HEALTH NETWORK
CHRONIC OBSTRUCTIVE
PULMONARY DISEASECLINICAL PATHWAY
BLUD COPD FOLDER AND PATIENT PATHWAY HOME WITH PATIENT
O2 SATS >90% OR AS ORDERED - WITHIN PATIENT'S NORM X 48 HOURS
DYSPNEA SCALE NORMAL FOR PATIENT AND < 5
STABLE COMORBID ILLNESS
DISCHARGE
PLANNING
SCRIPT GIVEN
PATIENT/FAMILY QUESTIONS ANSWERED
IMPORTANCE OF SMOKING CESSATION REINFORCED, IF APPLICABLE
MEDICATIONS PATIENT DEMONSTRATES ACCURATE USE OF METERED DOSE INHALER
TEACHING CHECKLIST COMPLETE - COPY TO BLUE COPD FOLDER
PATIENT DEMONSTRATES KNOWLEDGE OF COPD EXACERBATION WARNING
SIGNS - PLAN OF ACTION
Updated Apr 2013© 2006 - 2013 Grey Bruce Health Network 9
Review Apr 2016

DATE INITIALNEEDS
REINFORCEMENT
What is COPD?
Managing COPD
Breathing Techniques
Know Your Medications
How To Use Puffers
(Inhaler-Spacer Teaching Checklist)
Smoking Cessation
(Journey 2 Quit)
Vaccinations
Home O2
(O2 Manufactures Information)
Follow Up With Doctor / Tests
Recognizing Flare Ups
Action Plan
All rights reserved. No part of this document may be reproduced or transmitted
in any form or by any means, without the prior permissin of the copyright owner.
� COPD Flare-Ups, The Lung Association � The BreathworksTM Plan Booklet
� Canadian Respiratory Guidelines - Plan of Action � COPD Patient Pathway - EBC Program
� Journey 2 Quit - Smoking Cessation Book, The Lung Association
COMMENTS: (i.e. patient understanding)
GREY-BRUCE HEALTH NETWORK
CHRONIC OBSTRUCTIVE
PULMONARY DISEASE (COPD)
TEACHING CHECKLIST
Resources:
� COPD - Circle of Care Booklet, The Lung Association � Inhaler-Spacer Teaching Checklist
Updated May 2013 © 2003 -2013 Grey Bruce Health Network Review May 2016

GREY BRUCE HEALTH NETWORK
EVIDENCE-BASED CARE PROGRAM
CHRONIC OBSTRUCTIVE
PULMONARY DISEASE
PATIENT PATHWAY
NOTE: Grey Bruce Health Network is starting to use computer patient charts to record the care that has been given to you
by hospital staff. Using the computer lets us have quick access to your patient chart and keeps us up-to-date with important
information about your health. This helps us to give you the best care where and when you need it. This Electronic Patient
Record is part of the Ontario wide plan to make your Electronic Health Record complete with records from other health
care people like your Family Physician, etc.
Your personal health information is password protected to keep it private and confidential. This allows for each one of your
health care team to see only the information they need to treat you.
Updated May 2013 Review May 2016
© 2006-2013 Grey Bruce Health Network

PROCESS
PATIENT RESPONSIBILITIES
ASSESSMENT
TESTS
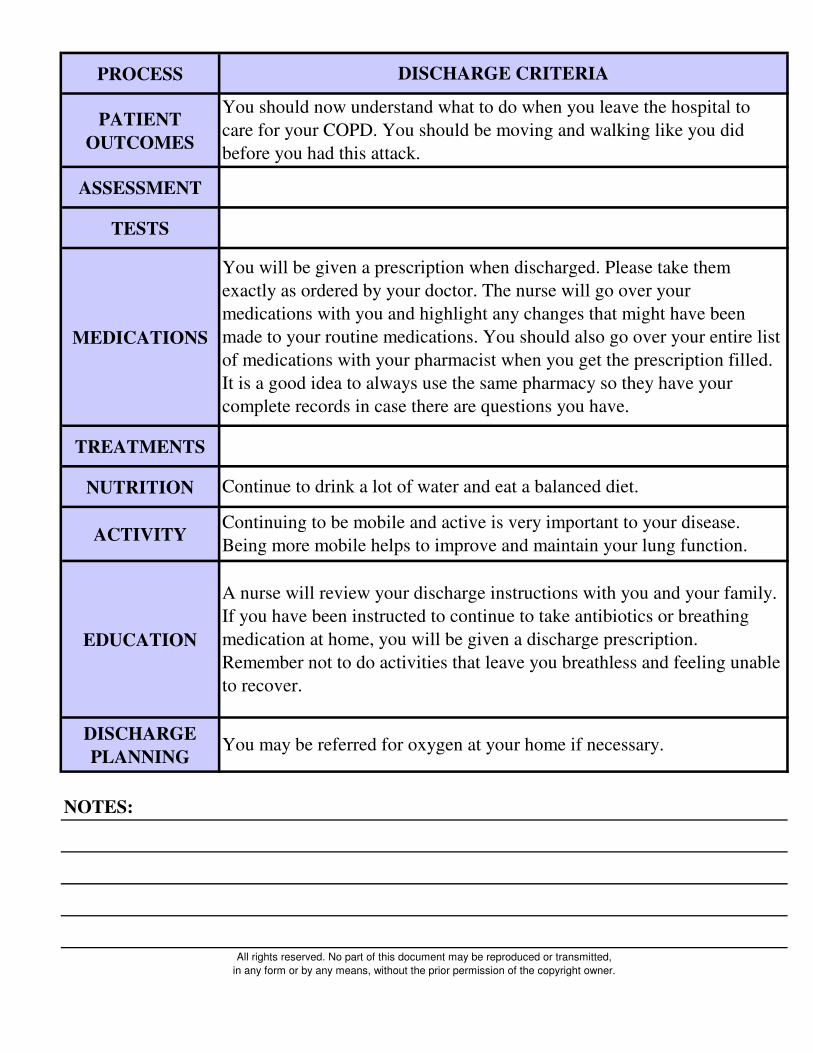
MEDICATIONS
NOTES:
ADMISSION
It is important that all patients with COPD understand how they can help
themselves get better and how they can stay healthy for as long as
possible. This can be done by learning about your disease. The hospital
staff will help you understand the information you are given and if you do
not understand some of it, or have questions, please ask the people
providing your care.
Your temperature, pulse, breathing and blood pressure will be checked.
Different healthcare providers will listen to your chest and assess your
breathing. They will ask you questions about your shortness of breath and
provide you with a scale to help you rate it.
You should let the nurse know if you are not making as much urine as you
normally do at home, especially when you are trying to drink more while
in hospital.
You will have some blood tests done and a chest x-ray taken.
Swabbing of the nose and anus on admission is necessary on all patients
admitted to the hospital. You may need to be put in isolation until the
results of those tests are known. This is a precaution to protect all of the
other patients as well as yourself.
Drugs will be given to you as ordered by your doctor. These will probably
include antibiotic(s) and medication to help with your breathing.
Once you have been placed on the right medication and you are ready to
go home, a complete list of your medications will be given to you as well
as a prescription. The medication may need to be adjusted from time to
time until the right combination is found.

PROCESS
TREATMENTS
NUTRITION
ACTIVITY
EDUCATION
DISCHARGE
PLANNING
NOTES:
ADMISSION
You will be given oxygen through a face mask or small prongs in your
nose if necessary.
Medications in the form of a mist are sometimes used with a mask to help
with your breathing.
You may eat or drink as you like, unless you require a special diet.
It is important that you drink a lot of fluids.
You will be encouraged to move as much as possible. Staff will assist you
as needed.
Reading your printed material given, asking questions about things you
don't understand, and communicating with your healthcare providers is the
key to getting you better and home as quickly and safely as possible.
A team of people are already working on getting you ready for home.
Please let your healthcare provider know if you have been having some
problems doing some of the activities at home.
Maybe we will be able to help you with some of those things to make it
easier for you to breathe once you arrive there.

PROCESS
PATIENT
OUTCOMES
ASSESSMENT
TESTS
MEDICATIONS
TREATMENTS
NUTRITION
ACTIVITY
NOTES:
PHASE 1 (AT ABOUT 2 DAYS)
You are now starting to breathe easier.
You should have no fever.
Your temperature, pulse, breathing and blood pressure will be checked
less often, but still when you need it.
Different healthcare providers will listen to your chest and assess your
breathing and continue to ask you about the breathing scale and how short
of breath you feel.
You should be doing to the bathroom normally.
There may be more tests depending on how you are doing.
You will continue taking drugs to help you breathe.
The medication with the mist may be changed to a puffer with a "spacer"
attached, if it hasn't already.
You may still have the medication in the mist, but you will need to let the
nurses know that you require it BEFORE you are very short of breath.
If you have a puffer that is kept at your bedside, you need to let the nurse
know EVERY TIME you use it and how much you use.
You will continue to receive oxygen if necessary.
Your oxygen needs should be approaching what is normal for you when
you are well at home.
You will be encouraged to drink extra fluids.
You will be encouraged to sit in a chair and walk short distances today.
Staff will assist you as needed.
This is very important to the speed of your recovery.
DO NOT do exercises that make you very short of breath so that you feel
like you cannot recover easily.

PROCESS
EDUCATION
DISCHARGE
PLANNING
NOTES:
PHASE 1 (AT ABOUT 2 DAYS)
Education is very important in helping you manage your disease and stay
healthy longer.
You will be given a booklet that will help you to understand what COPD
is and what support is available to help.
The folder you have been given is yours to keep. It has basic information
about your disease. more information can be given to you if you want to
learn more about certain subjects.
You can also find a lot of information on The Lung Association website at
www.on.lung.ca and look under the tab "Lung Health".
You are to take this folder with you to your healthcare practitioner when
you see them after discharge and they will provide you with additional
education when there.
A Community Care Access Centre Case Manager may talk with you, with
your permission, if needed, to plan for your discharge from hospital.

PROCESS
PATIENT
OUTCOMES
ASSESSMENT
TESTS
MEDICATIONS
TREATMENTS
NUTRITION
ACTIVITY
EDUCATION
DISCHARGE
PLANNING
NOTES:
PHASE 2 (AT ABOUT 2 - 5 DAYS)
You are now preparing for discharge.
Your breathing should be back to normal and you should be off oxygen by
the time you are discharged, if you normally do not use oxygen at home.
If you used oxygen at home before admission you should have someone
bring your portable tank to be available for your day of discharge.
Your temperature, pulse, breathing and blood pressure will be checked.
Different healthcare providers will listen to your chest and assess your
breathing.
You may have some blood work done.
You will continue taking drugs to help your breathing. Let the nurse know
if you are having difficulty breathing.
Your need for oxygen will be reassessed.
Continue deep breathing and coughing exercises.
You should continue to drink extra fluids.
You will be encouraged to continue moving and walking as much as
possible, increasing your activity level each day in preparation for
returning home.
Different healthcare providers will review the booklet on COPD with you.
You will receive instructions to help you prepare for discharge, including
reasons to call your doctor.
A pharmacist/nurse may see you if the drugs you took at home before
coming to the hospital have changed a great deal.
A Community Care Access Centre Case Manager may talk with you, with
your permission, if needed.
You may be discharged if your breathing is improving.
PROCESS
PATIENT
OUTCOMES
ASSESSMENT
TESTS
MEDICATIONS
TREATMENTS
NUTRITION
ACTIVITY
EDUCATION
DISCHARGE
PLANNING
NOTES:
DISCHARGE CRITERIA
You should now understand what to do when you leave the hospital to
care for your COPD. You should be moving and walking like you did
before you had this attack.
You may be referred for oxygen at your home if necessary.
All rights reserved. No part of this document may be reproduced or transmitted,
in any form or by any means, without the prior permission of the copyright owner.
You will be given a prescription when discharged. Please take them
exactly as ordered by your doctor. The nurse will go over your
medications with you and highlight any changes that might have been
made to your routine medications. You should also go over your entire list
of medications with your pharmacist when you get the prescription filled.
It is a good idea to always use the same pharmacy so they have your
complete records in case there are questions you have.
Continue to drink a lot of water and eat a balanced diet.
Continuing to be mobile and active is very important to your disease.
Being more mobile helps to improve and maintain your lung function.
A nurse will review your discharge instructions with you and your family.
If you have been instructed to continue to take antibiotics or breathing
medication at home, you will be given a discharge prescription.
Remember not to do activities that leave you breathless and feeling unable
to recover.