chronic pain management in general and hospital practice
TRANSCRIPT
123
Koki Shimoji Antoun Nader Wolfgang HamannEditors
Chronic Pain Management in General and Hospital Practice

Chronic Pain Management in General and Hospital Practice

Koki Shimoji • Antoun Nader Wolfgang HamannEditors
Chronic Pain Management in General and Hospital Practice

ISBN 978-981-15-2932-0 ISBN 978-981-15-2933-7 (eBook)https://doi.org/10.1007/978-981-15-2933-7
© Springer Nature Singapore Pte Ltd. 2021This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed.The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use.The publisher, the authors, and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, expressed or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This Springer imprint is published by the registered company Springer Nature Singapore Pte Ltd.The registered company address is: 152 Beach Road, #21-01/04 Gateway East, Singapore 189721, Singapore
EditorsKoki ShimojiPain Control InstituteShinjyukuTokyoJapan
Wolfgang HamannGuy’s and St Thomas’ Hospital, Pain Management CentreLondonUK
Antoun NaderFeinberg School of MedicineNorthwestern University Feinberg School of MedicineChicagoILUSA

v
Contents
Part I Basic Considerations
1 History of Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3W. Hamann
2 Theories of Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Koki Shimoji and Yoshiyuki Yokota
3 Anatomical Physiology of Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Koki Shimoji and Satoshi Kurokawa
4 Pathophysiology of Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43W. Hamann
5 Pharmacology of Analgesics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55Koki Shimoji and Hitoshi Fujioka
6 Investigation of the Chronic Pain Patient . . . . . . . . . . . . . . . . . . . . . . . 87Nicholas Padfield
7 Interventional Treatment of Chronic Pain . . . . . . . . . . . . . . . . . . . . . . 113Thomas E. Smith
8 Nerve Blocks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 129Ryan Zaglama and Antoun Nader
9 Other Methods: Minimally Invasive Techniques in Pain Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141Koki Shimoji and Tatsuhiko Kano
10 Pain Measurements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173Koki Shimoji and Sumihisa Aida

vi
Part II Pain Management Techniques
11 Back Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203Pierluigi di Vadi
12 Postherpetic Neuralgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219Christine El-Yahchouchi and Antoun Nader
13 Neuropathic Pain: Complex Regional Pain Syndrome (CRPS) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 225Mansoor M. Aman, Ammar Mahmoud, and Taruna Waghray-Penmetcha
14 Neuropathic Pain Syndrome: Diabetic and Other Neuropathies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 249Atsushi Sawada and Michiaki Yamakage
15 Phantom Limb Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 261Luminita M. Tureanu and Ljuba Stojiljkovic
16 Neuropathic Pain Syndromes. 5: Other Neurological Conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 279Soshi Iwasaki and Michiaki Yamakage
17 Psychological and Psychiatric Pain Conditions . . . . . . . . . . . . . . . . . . 291Yukari Shindo and Michiaki Yamakage
18 Headache . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303Oluseyi Fadayomi and Antoun Nader
19 Trigeminal Neuralgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 323Kim Nguyen
20 Orofacial Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 341Maxim S. Eckmann and Antoun Nader
21 Myofascial Pain Syndrome and Fibromyalgia . . . . . . . . . . . . . . . . . . . 355Maria M. Cristancho, Gunar B. Subieta, and Maria L. Torres
22 Urogenital Pain Including Pelvic Pain . . . . . . . . . . . . . . . . . . . . . . . . . 373Maged Mina, Jonathan Benfield, Sylvia Botros-Brey, and Cyril Mina
23 Chest Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 389Ju Mizuno and Kazuo Hanaoka
24 Upper Abdominal Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 425Ju Mizuno and Kazuo Hanaoka
25 Central Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 443Marc Korn, Mary Leemputte, and Dost Khan
Contents

vii
26 Management of Cancer Pain in Primary, Secondary, and Palliative Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 455Emma Whitehouse and Nick Dando
27 Arthritis Pain; Rheumatoid Arthritis, Osteoarthritis, and Fibromyalgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 483Afsha Khan, João Calinas Correia, and David Andrew Walsh
28 Vascular Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 517Kellie Gates and Pegah Safaeian
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 535
Contents

Part IBasic Considerations

3© Springer Nature Singapore Pte Ltd. 2021K. Shimoji et al. (eds.), Chronic Pain Management in General and Hospital Practice, https://doi.org/10.1007/978-981-15-2933-7_1
Chapter 1History of Pain
W. Hamann
This summary of the history of pain focusses on its relevance to pain management. It is self-restricting, aiming to tease out the development of the subject pain towards the present situation of the history of medicine.
At the beginning, it is worthwhile to summarize our current understanding of the pain pathway, and then go through history bearing in mind what research tools were actually available to clinicians and researchers at particular points in times, and what relevant religious faiths and philosophies influenced the thinking about the nature of pain. One also needs to be aware that pathology can occur at any level of the pain pathway from peripheral receptors right up to relevant connections in the brain. Central pain, e.g., which may be excruciatingly debilitating, occurs without any peripheral origin but may be projected to peripheral parts of the body.
Rey [1] emphasizes the importance of discriminating between perception of pain and the ensuing suffering. Both aspects are of course therapeutic targets for the pain physician. Without alleviation of suffering there can be no effective pain manage-ment. It is therefore now generally accepted that pain management has to be holistic.
Historically, pain medicine concentrated on acute pain conditions. This may par-tially be due to the much shorter life expectancy in historic times. Many people did not live long enough to experience the full effects of degenerative diseases. Among the Graeco-Roman minor deities there are many gods specifically concerned with acute pain conditions and hardly any focussed on chronic pain. Similarly, among the catholic saints, there are only Milian, Saint Marcus and James the Great, whose remit is rheumatism. There are many more saints one can appeal to for help with acute pain.
Every civilization does have its own medicine experts with specific views on the significance of pain and how to deal with it. Commonly, sophisticated systems of
W. Hamann (*) Guy’s and St Thomas’ Hospital, Pain Management Centre, London, UKe-mail: [email protected]

4
herbal medicine were part of the treatments employed, and frequently, the same plants were used for similar indications.
This summary focusses on a few major instalments in the history of medicine preceding and during the recent scientific approach to pain and its management of pain.
The earliest written records mentioning opium date back 3000 years, on Sumerian clay tablets [2]. It is not clear whether this document refers to the use of the drug for pain control or as a narcotic. Thompson [2] also reported on Assyrian clay tablets recommending the use of ointments containing mandrake together with the use of charms for the control of toothache.
In parallel, medicine developed separately in Egypt, China, the Indian subconti-nent in the form of Ayurvedic medicine and later further west in the Greco-Roman- Arabic sphere. Many aspects of pain management originating from these cultures have survived either in mainstream practice or in the form of alternative medicine.
Egyptian pain treatment was often combined with a Charm [3]. The Ebers Papyrus [3] reports use of the yeast of the opium drink, the willow tree, poppy plant, berries and seeds accompanied by chanting of a charm for pain control.
In Indian (Ayurveda) and Chinese (Tao) medicines an individual’s good health was dependent on complying with conditions maintaining well-balanced relation-ship and heaven and earth.
The authoritative historical reference to Chinese medicine is the Yellow emper-ors Huang Ti’s Classic of Internal Medicine (Nei Ching) dated 2697 B.C. which catalogues the knowledge current at his time. However, over the years the original information will have been added to. Analysis of style of the text available now indicates that the present text was written approximately at 1000 B.C.
The Nei Ching is a Chinese philosophical compendium on preventative medi-cine. It is not a medical textbook in the modern sense. It quotes the old sages [4] as saying that “they will not treat those who were already ill; they instructed those who were not ill”.
Tao, which means “the way”, expresses itself in the human body through the opposing concepts of Yin and Yang, which need to be kept in balance for good health and longevity. Diagnosis and treatment is based on a structured system around the five viscera, five elements as well as the seasons. Severe pain ensues when the spirit is hurt [4].
Acupuncture was introduced as a technique that can control the flow of vital forces including Yin and Yang.
It is surprising that surgical techniques do not figure highly in the Nei Ching. For this, Veith [4] gives two reasons. Firstly, the very high esteem for Chinese internal medicine hindered the development of surgery. Secondly, because of the Confucian tenet of the sacredness of the human body surgery appeared an inappropriate form of treatment.
However, two surgeons Pien Ch’iao and Hua T’o achieved prominence around 190 A.D. [4]. Apart from excellent surgical skills their success was based on the introduction of effective anaesthesia. All Hua T’o’s records were unfortunately burned, and no record exists today of either his or Pien’s methods of pain control.
W. Hamann

5
Four Sanskrit Vedas (Rigveda, Samaveda, Yajurveda and Atharvaveda) date back to between 4500 and 1600 B.C. [5]. They form the basis of the Indian Ayurveda medical practice.
The Egyptian compendium of medicine, the Ebers Papyrus [6] was written about 1500 B.C. and refers back to data collected as early as 3500 B.C.
Historic approaches to medicine and by implication pain management were often holistic in one way or another. They went beyond solely targeting the assumed somatic mechanism. Treatment of the assumed pathology was complemented by a psychological or spiritual component. Plato [7] succinctly expressed this as follows “For this is the greatest error of our day; in the treatment of the human body the physicians first separate the soul from the body”.
During Antiquity important strives were made in the development of medicine. The Hippocratic collection [1], mostly written between 430 and 380 B.C. is a col-lection of medical knowledge and thought available at that time. It drew both on practices at the Cosian as well as Cnidian school. Although it subscribed to the concept of humorism (black bile, yellow bile, phlegm and blood), it introduced the concept of rationalization in medicine. Hippocrates furthermore postulated the sep-aration of medical doctrine from philosophy. At his time, medical doctrines were most or part based on philosophy about nature’s origin and composition. Pain itself had no utility, but nevertheless needed to be controlled.
In the text of Epidermis V it is recommended to match like with like. One pain may calm another simultaneous one, anticipating the diffuse non-specific inhibitory control (DNIC) described by Le Bar in 1979 [8].
For gynaecological pains, the use of mandrake, a nightshade and poppy is recommended.
Alexandria with its large library was a centre for medical research in the third century B.C. Eristrasus [1] described motor and sensory nerves using vivisection on criminals, which was later forbidden by the authorities.
Roman medicine was built on the foundation of Greek knowledge and experi-ence. In his book De Re Medicinae written about 30 A.D., Celsus [9] who was prob-ably not a doctor himself, stated that pain was mainly useful for prognostic purposes, and that seasonal aspects, different periods in life, individual temperament and gen-der were important factors affecting the presentation of pain. Pain itself had no conceivable positive value. In terms of medical methodology, he discriminated between diagnosticians who tried to understand the pathophysiology of a condition, empiricists who relied on their clinical experience and methodists who were relying on common traits evident between specific disorders.
The most prominent physician during Roman times living in the second century was Galen [vide ref 1] a real celebrity physician. The emperors Marcus Aurelius, Commodus and Septimius Severus were among his patients. He published some 500 titles. For him, pain was important as a symptom to be treated, but also helpful for the understanding of the pathophysiology and prognosis of a condition. Dissection was for him an important tool for the understanding of underlying mech-anisms of a disease. Pain was regarded as excessive mechanical stimulation in anal-ogy to excessive brightness harming vision and sound that is too loud damaging
1 History of Pain

6
hearing. Galen’s pathophysiological model about good health depending on balance between black bile, yellow bile, phlegm and blood was finally abandoned only dur-ing the nineteenth century.
Galen’s writings, the Hippocratic corpus and De Materia Medica by Dioscorides [10] have remained required reading for doctors until the mid-nineteenth century. The Materia Medica is a compendium of 800 plants described to very high botanical standards. Side effects and efficacy are described in detailed terms. The book men-tions opium poppy, field poppy, lettuce, belladonna, hyoscine and black nightshade for pain control.
As part of these developments, herbal medicine advanced on an empirical basis with the detailed Materia Medica by Dioscorides surviving [10]. Willow bark as an analgesic reminds us that the first known non-steroidal anti-inflammatory has been in use for a very long time.
During medieval times in Europe, the understanding of medical matters was strongly interwoven with religious thought.
The concept of pain as punishment by God for the original sin or other sins often entailed that pain had to be endured. Consequently, there was little advance in pain management during this time. The power of a strong faith in controlling the sensa-tion of pain is well documented by the absence of signs of suffering in artwork of the time depicting torture of saints.
Many of the Greek manuscripts only survived in Arabic translation.With the advent of the age of Enlightenment in Europe, modern scientific method
established itself gradually, and has since remained the driving force for development.Based on anatomical knowledge, Descartes [11] proposed a dualistic system for
the perception of pain that separated the sensing of pain from its emotive compo-nent. This deviated from the holistic approach towards pain management that had prevailed hitherto. The impact of his model of pain perception on the one hand had a stimulating effect on further scientific research. On the other hand, it engendered a somewhat mechanistic approach towards perception and control of pain, which has only been overcome recently with the introduction of cognitive behavioural treatment into pain management and more recently with the emphasis on mindful-ness. It is significant that early modern pain centres often called themselves pain relief clinics. Unfortunately, pain relief is not always attainable in chronic pain con-ditions. Most pain clinics have since redefined themselves as pain management establishments.
In conclusion, over the centuries and millennia pain management has been shaped by the prevailing understanding of the underlying mechanisms as well as by culture and religion.
During the middle ages, between 500 and 1500 A.D., the concepts about the meaning and control of pain understanding of pain diverged between Europe on one side and Arabia and Persia on the other. The latter two areas became centres of high learning, building on the knowledge of Greek and Roman experts and translations of their writings.
In Europe, the largely scholastic approach towards medicine precluded any fur-ther development in the understanding of the physiology of pain. In addition,
W. Hamann
7
religion had a profound effect on the appreciation and contemporary meaning of pain. Either as a divine punishment by God or as redemption by suffering in a way Christ did were probably important ways to accept pain as deserving. Pain was sanctified, because it brought sufferers closer to the pain experienced by Christ [1]. For non- believers this type of reasoning is difficult to agree with. Indirectly, the religious understanding of pain amplified the inhibition of development inherent in the scholastic approach.
Renaissance and the age of enlightenment brought a change towards a more scientific approach towards medicine and biology.
In 1586 Fernel [vide Rey 1] applied Galen’s concept of overstimulation to the understanding of pain. He introduced tissue damage as the common denominator for the sensation of pain. However, perception of pain was only caused by the sub-sequent appreciation of the injury.
During the middle of the seventeenth century, Descartes developed the dualistic system of sensory perception [12]. He accepted phantom limb pain in an arm ampu-tee as a real phenomenon and not as an aberration of the mind. His model of nervous conduction was that of a mechanical pulley, which could be tugged at any position on its course to the brain. Interpretation of the message took place in the soul, which was supposed to reside in the pineal gland.
During the eighteenth and nineteenth century, although not universally accepted, views were held that the sentience for pain was a function of the perceived level of civilization as well as cultural and intellectual development of an individual. It was this type of thinking that led to the appalling conditions associated with slavery [13].
During the nineteenth century, there were major advances in anaesthesia and analgesia. In parallel, hypotheses and theories and factual observations about the organization of the pain pathway became increasingly detailed. Perl has provided a comprehensive time line of the development during the nineteenth and twentieth centuries [14].
Based on the study of cross-sectional spinal lesions in patients, Brown-Sequard [15] established the contralateral anterolateral tract in man as essential for the transmission of nociceptive information.
Anatomically, Edinger [16] identified the spinothalamic tract in 1890.At the beginning of the nineteenth century Johannes Mueller [17] developed the
concept of specific peripheral receptors for each individual sense, a concept previ-ously held by Avicenna. Muellers law of “law of specific nerve energies” stated that there were specific receptors for each of the senses. However, he attributed their sensitivity to unique Vitalism based qualities of energy in the afferent nerve fibres. He came to this conclusion, because specific sensory experiences could be elicited by non-physiological excitation with electrical stimuli or, e.g., excessive pressure on the eyeball. It was Adrian’s discovery of the action potential as the uniform mode of nervous conduction which disproved the hypothesis of a unique sense specific to nervous energy in primary afferent fibres.
On the basis of finely discriminating sensory testing of the skin in combination with histological investigations, von Frey [18] developed the specificity hypothesis of the senses. The test of this theory ultimately depended on electrophysiological
1 History of Pain

8
primary afferent and postsynaptic single unit recordings. Initially only few nocicep-tor primary afferents were identified by Zottermann [19] the A delta fibres and by Iggo [20] among C-fibres.
During the nineteenth and twentieth century, several hypotheses were proposed discussing the issue whether pain is a specific or non-specific sensation gaining its unique properties not on the basis of specific receptors in the periphery, but solely by central nervous processing.
The debate became even more intense after it became possible to record from single postsynaptic cells in the spinal cord. Initially, only wide dynamic range units were encountered, receiving excitatory input from a wide range of nociceptive as well as non-nociceptive primary afferents. It was not clear, how the nervous system could disentangle such messages. On the basis of the electrophysiological evidence available in 1965, Melzack and Wall [21] developed the gate theory, postulating that the gate to the perception of pain was opened by discharge in primary afferent C-fibres and that it was under control of descending and segmental modulation.
Since then electrophysiological recording techniques have improved. A large proportion of primary afferent C-fibres does not subserve nociception [22], how-ever, many do. Postsynaptically, there are neurones solely responsive to noxious stimuli [23].
In 1897, Sherrington [24] introduced the concept of the synapse into neurophysi-ology, allowing for modulation of information along the pathway from the periph-ery to the brain. The concept of integration along sensory pathways from the periphery to the ultimate termination in the brain was a considerable advancement on Descartes’ “bell pulley” mechanism eliciting the sensation of pain in the soul. It was also more specific than the forces of vitalism to which Mueller still subscribed. In modern medicine, artificial activation of segmental and descending inhibition is activated by transcutaneous nerve stimulators, acupuncture, spinal cord stimulators and peripheral nerve stimulators.
Mersky’s 1979 [25] definition of “Pain as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” was adopted by the International Association for the study of pain. This definition clearly differentiates between the perceived sensory event and its emotional impact.
Until sometime during the nineteenth century, Western clinicians still discrimi-nated between personality types on the basis of the Hippocratic philosophy of the predominant effect of one of the four humours (phlegm, black bile, yellow bile and blood). According to this classification, there were phlegmatics, cholerics, melan-cholics and sanguins. Pain was experienced according to one’s type of personality.
Since the nineteenth century, in parallel with sensory neurophysiology, clinical and behavioural observations have served as influential tools investigating the whole breadth of pain perception as outlined in Mersky’s definition.
Clinical and behavioural hypotheses and theories were reported in depth by Bourke [13]. Observations by Leriche [vide 13] during World War 1 and Beecher [26] during World War 2 described substantial injuries being sustained by soldiers without any pain being reported.
W. Hamann

9
Among civilians, pain sentience was said to depend on race, personal character-istics or traits shared by individuals grouped according to class or occupation [13]. Phrenology was also of some importance. Organs of destructiveness, and an organ for fighting were supposedly identified, the location of these centres can still be found in phrenology maps sometimes sold in curiosity shops.
Whilst much of this evidence is anecdotal or of prejudicial nature, it points towards differences between individuals in central nervous processing of painful events. In other words, it became clear that there must be modulation on the passage of messages along the pain pathway.
During the second half of the twentieth century, psychological techniques of pain management became increasingly Important. In the first wave, operant conditioning based on the concept of Pavlovian reflexes were tried for a variety of medical condi-tions. The second wave in the form of cognitive behavioural treatment (CBT) was introduced to many pain management establishments. Courses were either residen-tial or on an out- patient basis. They consisted of a combination between explana-tions of the current medical understanding of patient’s pain conditions, reduction in medication and fitness training, often resulting in improvement in quality of life that mattered. More recently, the third phase has become widely accepted in the form of mindfulness training Kabat-Zinn [27], which is in essence a form of meditation without the teachings of Buddhism.
References
1. Rey R. History of pain. Paris: Editions La Decouverte; 1993. p. 11. ISBN 2-7071-2256-4, Ibid pp. 26–32, Ibid pp. 32–35, Ibid pp. 60–66, Ibid p. 72, ref 27.
2. Thompson. Proc. Roy. Soc. Med. Sect. Hist. Med. 1926;19:69–78. Quoted from Sigchrist HE. Primitive and archaic medicine. Oxford Univ. Press; 1967.
3. Ebers G. The Papyrus Ebers: translated from the German version by Cyril P. Brian. London: Geoffrey Bles; 1930. p. 24–30.
4. Veith I. The Yellow Emperor’s classic of internal medicine. Berkeley: University of California Press; 1970. p. 2–3. ISBN 0-520-01296-8, p.53, Ibid p 117, Ibid p 3, Ibid.
5. Mishra LC. Scientific basis for Ayurvedic therapies. Boca Raton: CRC Press; 2004. 0-8493-1366-X. Introduction.
6. The Ebers Papyrus (trans: Ryan CP). Letchworth: The Garden City Press LTD; 1930. Royal Soc Med.
7. Stempsey WE. Plato and holistic medicine. Med Health Care Philos. 2001;4(2):201–9. 8. Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls (DNIC). I. Effects
on dorsal horn convergent neurones in the rat. Pain. 1979;6:283–304. 9. Celsus De Re Medicinae AD. 30 (quoted from Douglas Guthrie. Edinburgh: Thomas Nelson
and Sons LTD; 1958. p. 72–75). Ibid pp. 74–82. 10. De Materia Medica D. Being an herbal with many other medicinal materials (trans: Osbaldeston
TA). Johannesburg: Ibidis Press; 2000. 11. Descartes R. Dioptrique, Discourse Quatrieme. In: Oevres et lettres. Paris, Gallimard; 1637.
[La Pleiade (1953) p. 203]. 12. Descartes R. Principia Philosophica. Amsterdam: Lois Elzevir; 1644. 13. Bourke J. The story of pain. Oxford: Oxford University Press; 2014. p. 195.
ISBN978-0-19-96843-9. Ibid pp. 193–268, Ibid p. 224, Ibid. p. 209.
1 History of Pain

10
14. Perl E. Ideas about pain, a historical view. Nat Rev Neurosci. 2007;8:71–80. 15. Brown-Sequard CE. Course of lectures on the physiology and pathology of the central nervous
system. Philadelphia: Collins; 1860. 16. Edinger L. Zwolf Vorlesungen uber den Bau der Nervosen Centralorgane Fur Arzte and
Studierende. Leipzig: F.C.W. Vogel; 1892. p. 150–3. 17. Müller J. Handbuch der Physiologie des Menschen fur Vorlesungen, vol. 2. Coblenz: Verlag
von J. Holscher; 1837–1840. 18. von Frey M. Beitrage zur Sinnesphysiologie der Haut. Dritte Mitteilung, Konigl Sachs Ges
Wiss Math Phys, Classe 48; 1895. p. 166–184. 19. Zottermann Y. Touch Pain and Tickling and electrophysiological investigation on cutaneous
sensory nerves. J Physiol. 1939;95:1–28. 20. Iggo A. Cutaneous heat and cold receptors with slowly conducting © afferent fibres. Quart J
Exp Physiol. 1959;44:362–70. 21. Melzack R, Wall PD. Pain mechanisms a new theory. Science. 1965;150:971–9. 22. Walker SC, Trotter PD, Swaney WT, Marshall A, Mcglone FP. C-tactile afferents: cutane-
ous mediators of oxytocin release during affiliative tactile interactions? Neuropeptides. 2017;64:27–38.
23. Christensen BN, Perl ER. Spinal neurons specifically excited noxious or thermal stimuli: mar-ginal zone of the dorsal horn. J Neurophysiol. 1970;33:293–307.
24. Sherrington CS. The integrative action of the nervous system. New York: Charles Scribner’s Sons; 1906.
25. Mersky H, Bogduk N. Classification of chronic pain. Seattle: IASP Press; 1994. 26. Beecher HK. Pain in man wounded in battle. Ann Surg. 1946;123(1):96–105. 27. Kabat-Zinn J. Mindfulness with Jon Kabat-Zinn. 2007. YouTube. https://www.youtube.com/
watch?v=3nwwKbM_vJc.
W. Hamann

11© Springer Nature Singapore Pte Ltd. 2021K. Shimoji et al. (eds.), Chronic Pain Management in General and Hospital Practice, https://doi.org/10.1007/978-981-15-2933-7_2
Chapter 2Theories of Pain
Koki Shimoji and Yoshiyuki Yokota
2.1 Specificity Theory
Specific theory of pain states that each modality of sense, touch or pain, is encoded in separate pathways. For instance, touch and pain stimuli are received by special-ized sense organs. Impulses of each sensory modality are conducted along the distinct pathways and projected to the touch and pain centers in the brain, respec-tively. Thus, its fundamental thought is that each sense of modality has a specific receptor and associated sensory fiber sensitive to only one specific stimulus [1].
Aelius Galen, a prominent Greek physician, demonstrated that spinal cord sec-tion caused sensory (including pain) as well as motor deficits cited by Ochs [2, 3]. Vesalius, Belgium anatomist, in the middle of seventeenth century, also confirmed the findings by Galen [2, 3].
Descartes was believed to be the first philosopher who described the hypothesis on pain pathway in man in 1662 (Fig. 2.1). He described pain as a perception that exists in the brain and is distinct difference between neuronal phenomenon of sensory transduction and the perception of pain. Descartes perceived the nerves as hollow tubules that conduct both sensory and motor activities.
Descartes claimed that the heat of flame near the foot activates a fiber within the nerve tubule that travels up to the leg, to the spinal cord, and finally to the brain center. Descartes postulated proverbial bells which are the pores lining along the cord and brain ventricles. When pores open in response to the sensory stimulus “the
K. Shimoji (*) Niigata University Graduate School of Medicine, Niigata, Japan
Pain Control Institute, Tokyo, Japane-mail: [email protected]
Y. Yokota Department of Anesthesiology, Ariake Hospital, Cancer Foundation, Koto City, Japane-mail: [email protected]

12
animal spirits” were thought to flow through the tubule and elicit the motor responses.
Like turning the head and eyes to recognize the flame, raising the hands and moving the body away from the flame occur to protect from burn (Fig. 2.1).
Modern concept of pain pathway was described by Bell and Shaw in 1868 [4]. They postulated that the brain is not the common sensorium as suggested by Descartes, but the brain is a heterogeneous structure as suggested by Willis in the seventeenth century [5, 6]. They suggested that nerves are constructed by heteroge-neous neurons playing specialized functions. Thus, Bell and Shaw believed that different sensory neurons play for different types of motor neurons and “vital neu-rons” that are connected to the mind rather than the brain.
Thus, fundamental idea of specific theory of pain suggests that a pathway spe-cific to pain exists (Fig. 2.2).
Bernard and Magendie in 1856 [7] reiterated Bell’s findings and described the motor and sensory nerves having separate paths to and from the spinal cord (cited by Stahnisch [8].
The discovery of cutaneous touch receptors, such as Pacinian corpuscles [9], Meissner’s corpuscles [10], Merkel’s discs [11], and Ruffini’s end-organs [12] gave further evidence that each specific sense is encoded by specific nerve fibers (cited by Ochs) [2, 3]. However, a specific end organ dedicated to pain sense had not yet been found.
a b
Fig. 2.1 (a) Portrait of René Descartes (b) Descartes’ pain pathway: “Particles of heat” (A) acti-vate a spot of skin (B) attached by a fine thread (cc) to a valve in the brain (de) where this activity opens the valve, allowing the animal spirits to flow from a cavity (F) into the muscles causing them to flinch from the stimulus, turn the head and eyes toward the affected body part, and move the hand and turn the body protectively [2, 3]. [Descartes et al. (1664), out of copyright; translated by M. Moayedi]
K. Shimoji and Y. Yokota

13
On the other hand, there were arguments that pain was different from other senses in the way that it causes unpleasantness [13, 14].
Further evidence of specific theory was reflected on Charles-Edouard Brown- Sequard’s observations that sensory fibers decussate in the spinal cord [14–16]. Further, Schiff and Woroschiroff established the presence of two pathways by observations of effect of incisions at different levels of the spinal cord, anterolateral pathway for pain and temperature and the posterior bundles for tactile sense (cited by Ray) [5]. Goldscheider in1894 reported the sensory spots which elicit a specific sense such as warmth, cold, pressure, or pain, and supported the specific theory [5, 16, 17].
Max von Frey further advanced the specific theory by carrying out the experi-ments by developing the well-known von Frey’s hairs to measure the pressure required to elicit a sensation at each skin spot identified by Blix and Goldscheider (cited by Forster and Handwerker) [18] (Fig. 2.2). Von Frey found that the distribu-tion of pressure points was related to the distribution of Meissner’s corpuscles, whereas the pain points were related to the distribution of the free nerve endings in the skin (Fig. 2.3).
Although Sherrington [19] supported the specificity theory addressed by von Frey, he also found that the behaviors of animals showed the temporal and spatial pattern of activity resulting from these four specific neurons demonstrated by von Frey. Burgess and Perl [20] discovered the primary afferent fibers that responded only to noxious mechanical stimulations, and then Besson and Perl [21] discovered nociceptive unmyelinated afferent fibers, polymodal nociceptors, and high- threshold mechanoreceptors.
Fig. 2.2 A set of von Frey hair, a type of esthesiometer designed in 1896 by Maximilian von Frey. Von Frey filaments rely on the principle that an elastic column, in compression, will buckle elastically at a specific force, dependent on the length, diameter, and modulus of the material. Once buckled, the force imparted by the column is fairly constant, irrespective of the degree of buckling. The filaments may therefore be used to provide a range of forces to the skin of a test subject, in order to find the force at which the subject reacts because the sensation is painful. This type of test is called a mechanical nociceptive threshold test. Sets of filaments are normally made of nylon hairs, all the same length, but of varying diameter so as to provide a range of forces, typically from 0.008 g force up to 300 g force. Von Frey filaments are, therefore a diagnostic, research, and screening tool, used both in human and animal medicine
2 Theories of Pain

14
Specificity theorya
c d
b
Innocuous
Innocuous
Innocuous
Impu
lses
Impu
lses
Impu
lses
Noxious
Noxious
Cell 1
Cell 1
Cell 2
Centralcontrol
Actionsystem
Gate control system
TSG
A-fibres
C-fibres
Cell 2
Cell 3
Cell 3
Noxious
Noxiousstimulus
Noxiousstimulus
Noxiousstimulus
Intensity
Intensity
Intensity
Skin
Skin
SkinDRG
nociceptors
DRGneurons
Dorsal hornnociceptive
neurons
Dorsal hornneurons
Intensity theory
Innocuousstimulus
Innocuousstimulus
Low thresholdDRG neurons WDR dorsal
horn projectionneurons
Pattern theory Gate control theory
Fig. 2.3 Schematic diagrams of pain theories. (a) Based on the Specificity Theory of Pain; each modality (touch and pain) is encoded in separate pathways. Touch and pain stimuli are encoded by specialized sense organs. Impulses for each modality are transmitted along distinct pathways, which project to touch and pain centers in the brain, respectively. DRG, dorsal root ganglion. (b) based on the Intensity Theory of Pain; there are no distinct pathways for low- and high-threshold stimuli. Rather, the number of impulses in neurons determines the intensity of a stimulus. The primary afferent neurons synapse onto wide-dynamic range (WDR) second-order neurons in the dorsal horn of the spinal cord, where low levels of activity encode innocuous stimuli, and higher levels of activity encode noxious stimuli. (c) The Pattern Theory of Pain posits that somatic sense organs respond to a dynamic range of stimulus intensities. Different sense organs have different levels of responsivity to stimuli. A population code or the pattern of activity of different neurons encodes the modality and location of the stimulus. (d) The Gate Control Theory of Pain proposes that both large (A-fibers) and small (C-fibers) synapse onto cells in the substantia gelatinosa (SG) and the first central transmission (T) cells. The inhibitory effect exerted by SG cells onto the pri-mary afferent fiber terminals at the T cells is increased by activity in A-fibers and decreased by activity in C-fibers. The central control trigger is represented by a line running from the A-fiber system to the central control mechanisms; these mechanisms, in turn, project back to the Gate Control system. The T cells project to the entry cells of the action system. +, excitation; −, inhibi-tion. (Figure is reproduced with permission from Dr. Perl ER: Ideas about pain, a historical view, Nature Reviews Neuroscience, 2007)
K. Shimoji and Y. Yokota

15
Recently, Hu et al. reported that chronic post-surgical pain is related to the hepa-tocyte growth factor [22]. This report may support in part the specific theory in terms of gene encoding.
2.2 Intensity Theory
On the other hand, intensity theory of pain claims that there are no distinct pathways for touch or pain perception. The theory defines pain not as a unique sensory experi-ence but as an emotion that occurs when stimulus is too strong.
Erasmus Darwin supported the idea advanced in Plato’s Timaeus that pain is not a unique sensory modality, but an emotional state produced by stronger than normal stimuli such as intense light, pressure, or temperature [23]. Wilhelm Erb, a German neurologist also argued in 1874 that pain can be generated by any sensory stimulus, provided it is intense enough, and his formulation of the hypothesis became known as the intensive theory (cited by Moayedi and Davis, and Jost) [6, 23].
Naunyn in 1889 [24] found that repeated innocuous stimulations including elec-trical stimulations produced unbearable pain in patients with syphilis, and con-cluded that some form of summation occurs in these pathological conditions.
William Kenneth Livingston advanced a summation theory in 1943, proposing that high intensity signals, arriving at the spinal cord from damage to nerve or tis-sue, set up a reverberating, self-exciting loop of activity in a pool of interneurons, and once a threshold of activity is crossed, these interneurons then activate “trans-mission” cells which carry the signal to the brain’s pain mechanism; that the rever-berating interneuron activity also spreads to spinal cord cells that trigger a sympathetic nervous system and somatic motor system response; and these responses, as well as fear and other emotions elicited by pain, feed into and perpetu-ate the reverberating interneuron activity (cited by Moayedi and Davis [6].
Thus, the number of impulses of other neurons determines the intensity of stim-uli. The primary afferent neurons synapse onto the wide-dynamic range second neu-rons (WDR) in the dorsal horn of the spinal cord.
The low threshold or low intensity impulses encode innocuous stimuli, whereas high levels of impulses encode noxious or pain stimuli (Fig. 2.3b) [6].
2.3 Pattern Theory
Pattern theory of pain postulates that sense organs respond to wide and dynamic range of stimuli. Different sense organs have different levels for responsivity to stimuli. The pattern of activity of different neurons encodes the modality and loca-tion of the stimuli. (Fig. 2.3c).
Pattern theory proposes that there is no separate system for perceiving pain, and the receptors for pain are shared with other senses, such as of touch. This theory considers that peripheral sensory receptors, responding to touch, warmth, and other
2 Theories of Pain

16
non-damaging as well as to damaging stimuli, give rise to non-painful or painful experiences as a result of differences in the patterns and in time of the signals sent through the nervous system [6].
Thus, according to this theory, people feel pain when certain patterns of neural activity occur, such as when appropriate types of activity reach excessively high levels in the brain. These patterns occur only with intense stimulation. Because strong and mild stimuli of the same sense modality produce different patterns of neural activity, being hit hard feels painful, but being caressed does not. It suggested that all cutaneous qualities are produced by spatial and temporal patterns of nerve impulses rather than by separate, modality specific transmission routes.
Central summation theory by Livingstone [25], the fourth theory of pain [26], and sensory interaction theory [27] might be all involved in this category [6].
Central summation theory proposed that the intense stimulation resulting from the nerve and tissue damage activates fibers that project to internuncial neuron pools within the spinal cord creating abnormal reverberating circuits with self-activating neurons. Prolonged abnormal activity bombards cells in the spinal cord, and infor-mation is projected to the brain for pain perception.
The fourth theory of pain stated that pain was composed of two components: the perception of pain and the reaction one has towards it. The reaction was described as a complex physiopsychological process involving cognition, past experience, culture, and various psychological factors which influence pain perception.
Sensory interaction theory describes two systems involving transmission of pain: fast and slow system. The latter presumed to conduct somatic and visceral afferents whereas the former was considered to inhibit transmission of the small fibers [5, 6, 28].
2.4 Gate Control Theory
Melzack and Wall in 1965 [29] proposed a new theory, gate control theory of pain, which supported in part both specificity and pattern theories of pain.
The gate control theory of pain proposes that large A-fibers and small C-fibers synapse onto the substance gelatinosa cells (SG cells) and the first central trans-mission cells (T cells) in the dorsal horn of the spinal cord. Their model proposed that the signals in the primary afferents by stimulation of skin were transmitted to the three regions in the spinal cord, (1) the substance gelatinosa (SG), (2) the dorsal column, (3) a groups of cells which they called transmission cells (Fig. 2.3d). They proposed that the gate in the spinal cord situates in the SG which modulates the sensory transmission of sensory information from the primary afferent neurons to transmission cells (T cells) in the cord. This gating mechanism is controlled by activity of both large and small fibers. Large fiber activity inhibits (or closes) the gate, whereas small fiber activity facilitates (opens) the gate. Activity from descending fibers from supraspinal structures could also modulate
K. Shimoji and Y. Yokota

17
this gate. The inhibitory activity exerted by the SG cells on to the primary afferent fiber terminals (both A-fibers and C-fibers) which synapse onto the T cells is increased by activity of A-fibers and decreased by activity of C-fibers. The inhibi-tory activity exerted by the SG cells or other interneurons onto the primary affer-ent terminals can be recorded as primary afferent depolarization (PAD) from the dorsal part of the spinal cord in animals [30] and even in human [31]. The T cells enter to the action system of central nervous system (CNS) including brain, and the impulses from A-fibers also activate the CNS where, in turn, impulses project back to the gate control system. Thus, the gate control theory in fact may help to reconcile the differences between the specificity and pattern theories of pain (Fig. 2.3d).
2.5 Consideration for Chronic Pain
Although the specificity theory appropriately described sensory receptors which respond only to suprathreshold stimuli, there have been no neurons in the brain which respond to both non-nociceptive and nociceptive stimuli such as wide- dynamic range neurons (WDR neurons). Although WDR neurons are well documented, their detailed functions in pain perception have to be determined.
Thus, none of these theories adequately explains the complexity of the pain sys-tem. Further, these theories focus on cutaneous pain but do not address deep-tissue, visceral, or muscular pains. Additionally, these models are focused on acute pain and may not explain mechanisms of persistent pain or chronic pain. Although the mechanisms of persistent and chronic pain are still not fully understood, it is now clear that peripheral and central plasticity can develop following repeated nocicep-tive stimulation even in healthy subjects [32] and in chronic pain [33]. Recent work has also demonstrated that plasticity is not only limited to changes in neurons but can also involve changes in glial cells [34]. Glial cells are thought to be related to the maintenance of persistent and chronic pain [35].
For instance, underlying mechanisms of complex regional pain syndrome (CRPS) are so complex, involving significant autonomic features. Both peripheral and central nervous system mechanisms are involved for its etiology. These include peripheral and central sensitization, inflammation, altered sympathetic and cate-cholaminergic function, altered somatosensory representation in the brain, genetic factors, and psychophysiological interactions [36]. Relative contributions of the mechanisms underlying CRPS may even differ across patients and even within a patient over time, particularly in the transition from “acute CRPS” to “chronic CRPS.” Recently, even sex differences have been advocated in pathogenesis for development of CRPS [37]. Although nociceptive hypersensitivity in CRPS has been studied in different pain models, the underlying molecular and cellular mecha-nisms remain elusive.
2 Theories of Pain

18
Although there have been a variety of treatments with demonstrated effective-ness for the management of CRPS, pain clinicians are unsure what treatments would be most effective for individual clients [38].
Enhanced knowledge regarding the pathophysiology of CRPS increases the pos-sibility of eventually achieving the goal of mechanism-based CRPS diagnosis and treatment [39].
References
1. Dubner R, Sessle BJ, Storey AT. The neural basis of oral and facial function. New York: Plenum; 1978.
2. Descartes R. De Homine Figuris et Latinitate Donatus a Florentio Schuyl. Leiden: Franciscum Moyardum & Petrum Leffen; 1662.
3. Ochs S. A history of nerve functions: from animal spirits to molecular mechanisms. Cambridge: Cambridge University Press; 2004.
4. Bell C, Shaw A. Reprint of the “idea of a new anatomy of the brain,” with letters, & c. J Anat Physiol. 1868;3:147–82.
5. Rey R. The history of pain. Cambridge: Harvard University Press; 1995. 6. Moayedi M, Davis KD. Theories of pain: from specificity to gate control. J Neurophysiol.
2013;109:5–12. 7. Bernard C, Magendie F. Leçon d’ouverture du Cours de Médecine du Collège de France. Paris:
Baillière; 1856. 8. Stahnisch FW. Francois Magendie (1783–1855). J Neurol. 2009;256:1950–2. 9. Pacini F. Sopra un Particolar Genere di Piccoli Corpi Globulosi Scoperti Nel Corpo Umano da
Filippo Pacini Alunno Interno Degli Spedali Riunti di Pistoia. (Letter to Accademia Medico- Fisica di Firenze.); 1835.
10. Meissner G. Beitraege zur Anatomie und Physiologie der Haut. Leipzig: Leopold Voss; 1853. 11. Merkel F. Tastzellen und Tastkörperchen bei den Hausthieren und beim Menschen. Arch Mikr
Anat EntwMech. 1875;11:636–52. 12. Ruffini A. Sur un nouvel organe nerveux terminal et sur la presence des corpuscules Golgi-
Mazzoni dens le conjonctif souscutané de la pulpe des doigts de l’homme. Mémoires de l’Academie Royale. Roma: LAccademia Nazionale dei Lincei Lincei; 1893. p. 249–65.
13. Boring EG. Sensation and perception in the history of experimental psychology. New York: D. Appleton-Century; 1942.
14. Dallenbach KM. Pain: history and present status. Am J Psychol. 1939;52:331–47. 15. Aminoff MJ. Historical perspective Brown-Sequard and his work on the spinal cord. Spine
(Phila Pa 1976). 1996;21:133–40. 16. Goldscheider A. Ueber den Schmerz in Physiologischer und Klinischer Hinsicht: Nach einem
Vortrage in der Berliner Militärärztlichen Gesellschaft. Ann Arbor: University of Michigan Library; 1894.
17. Norrsell U, Finger S, Lajonchere C. Cutaneous sensory spots and the “law of specific nerve energies”: history and development of ideas. Brain Res Bull. 1999;15(48):457–65.
18. Forster C, Handwerker HO. Central nervous processing of itch and pain. In: Carstens E, Akiyama T, editors. Itch: mechanisms and treatment. Boca Raton: CRC Press/Taylor & Francis; 2014. Chapter 24.
19. Sherrington CS. The integrative action of the nervous system. Cambridge: Cambridge University Press; 1947.
20. Burgess PR, Perl ER. Myelinated afferent fibres responding specifically to noxious stimulation of the skin. J Physiol. 1967;190:541–62.
K. Shimoji and Y. Yokota

19
21. Bessou P, Perl ER. Response of cutaneous sensory units with unmyelinated fibers to noxious stimuli. J Neurophysiol. 1969;32:1025–43.
22. Hu C, Lu Y, Chen X, Wu Z, Zhang Q. Gene transfer of a naked plasmid (pUDK-HGF) encod-ing human hepatocyte growth factor attenuates skin/muscle incision and retraction-induced chronic post-surgical pain in rats. Eur J Pain. 2018;22(5):961–72.
23. Jost WH. A tribute to Wilhelm H. Erb. J Neurol. 2006;253(Suppl 1):I1–2. 24. Naunyn B. Ueber die Auslösung von Schmerzempfindung durch Summation sich zeitlich fol-
gender sensibler Erregungen. Naunyn Schmiedeberg’s Arch Pharmacol. 1889;25:272–305. Access Volume 45, Issue 1 January 2001, pp. 134–135
25. Livingston WK. In: Fields HL, editor. Pain and suffering. Seattle: IASP Press; 1998. p. xvii, 250.
26. Noordenbos W. On the specificity of sensory events. Psichiatr Neurol Neurochir. 1960;63: 298–306.
27. Hardy JD, Wolf HG, Goodell H. Studies on pain. A new method for measuring pain threshold: observations of spatial summation of pain. J Clin Invest. 1940;19:649–57.
28. Perl ER. Ideas about pain, a historical view. Nat Rev Neurosci. 2007;8:71–80. 29. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150:971–9. 30. Lidierth M, Wall PD. Dorsal horn cells connected to the Lissauer tract and their relation to the
dorsal root potential in the rat. J Neurophysiol. 1998;80:667–79. 31. Shimoji K, Higashi H, Kano T. Epidural recording of spinal electrogram in man.
Electroencephalogr Clin Neurophysiol. 1971;30:236–9. 32. Bingel U, Herken W, Teutsch S, May A. Habituation to painful stimulation involves the anti-
nociceptive system—a 1-year follow-up of 10 participants. Pain. 2008;140:393–4. 33. Davis KD, Moayedi M. Central mechanisms of pain revealed through functional and structural
MRI. J Neuroimmune Pharmacol. 2013;8:518–34. 34. Eroglu C, Barres BA. Regulation of synaptic connectivity by glia. Nature. 2010;468:223–31. 35. Zhuo M, Wu G, Wu LJ. Neuronal and microglial mechanisms of neuropathic pain. Mol Brain.
2011;4:31. 36. Bäckryd E. Pain as the perception of someone: an analysis of the interface between pain medi-
cine and philosophy. Health Care Anal. 2019;27:13–25. 37. Tang C, Li J, Tai WL, et al. Sex differences in complex regional pain syndrome type I (CRPS-I)
in mice. J Pain Res. 2017;10:1811–9. 38. Packham T, Holly J. Mechanism-specific rehabilitation management of complex regional
pain syndrome: proposed recommendations from evidence synthesis. J Hand Ther. 2018;31(2):238–49.
39. Bruehl S. An update on the pathophysiology of complex regional pain syndrome. Anesthesiology. 2010;113:713–25.
2 Theories of Pain

21© Springer Nature Singapore Pte Ltd. 2021K. Shimoji et al. (eds.), Chronic Pain Management in General and Hospital Practice, https://doi.org/10.1007/978-981-15-2933-7_3
Chapter 3Anatomical Physiology of Pain
Koki Shimoji and Satoshi Kurokawa
3.1 What Is Pain?
The widely accepted definition of pain was addressed by a taxonomy task force of the International Association for the Study of Pain: Pain is an unpleasant sensory and emotional experience that is associated with actual or potential tissue damage or described in such terms [1]. Thus, a key feature of this definition is that pain is a sub-jective sensation. When we observe the patients with pain, we should always be cau-tious about the patient’s complaints modified by their own past and recent experiences to interpret and comment on what they perceive as pain, discomfort, distress, and anxi-ety. Training and experience in studying and observing patient’s behavior are required to interpret what the patients are complaining of and how severe the patient’s pain is.
3.2 Peripheral Mechanisms
Skin, muscle, bone, and other tissues have thousands of nerve endings within a single millimeter. When stimulated these nerves generate electrical signals, action potentials, which travel at various speeds along (afferents) nerve fibers to the spinal cord and brain. It can take from a few milliseconds to a few seconds for these signals to generate an experience of pain or to produce an appropriate physiological and/or behavioral response.
K. Shimoji (*) Niigata University Graduate School of Medicine, Niigata, Japan
Pain Control Institute, Tokyo, Japane-mail: [email protected]
S. Kurokawa Department of Anesthesiology, Tokyo Women’s Medical School, Tokyo, Japane-mail: [email protected]

22
Noxious stimulation is detected by nociceptors, which are located on free nerve endings of thin, myelinated (Aδ) and unmyelinated (C) nerve fibers, in various tissues.
Pain receptors, nociceptors, respond to high intensity mechanical (pricking, stretching), high intensity thermal (heat, cold), and intense chemical stimuli (K+, H+, prostaglandins, cytokines, etc.). These chemicals may be released as a result of damage to tissues by trauma, inflammation, or ischemia. Nociceptors are also stim-ulated and/or sensitized by chemicals released during inflammatory responses to infectious, toxic, or allergenic agents. The release or action of some of these chemi-cals can be reduced or stopped by common analgesic and anti-inflammatory treat-ments such as non-steroidal anti-inflammatory drugs (NSAIDS) and/or steroids.
When a nociceptor fiber detects a pain stimulus on the skin or in an internal organ, the pain signal is transmitted to the spinal cord and then on to the brain by neural pathways different from those of other skin sense (Fig. 3.1).
At each of the synapses along this pain pathway, several neurotransmitters are involved in carrying the nociceptive message. Two major groups are identified: clas-sical neurotransmitters and neuropeptides [2, 3].
Examples of classical neurotransmitters include glutamate, aspartate, and sero-tonin. At least 20 neuropeptides involved in transmitting pain impulses have been identified, including substance P, vasoactive intestinal peptide, calcitonin gene- related peptide, somatostatin, and cholecystokinin. By contrast, ACTH, the enkeph-alins, a large family of peptides, exert an inhibitory effect on the descending control pathways.
Mast cell
CGRP
CGRPSubstance P
K+Prostaglandin
5-HT
BradykininHistamine
Substance P
Dorsal rootganglion neuron
Bloodvessel
Spinal cord
Lesion
Fig. 3.1 Chemicals produced by damaged tissues and/or mast cells (K+, bradykinine,5-HT, pros-taglandin, histamine, etc.) and neuropeptides (substance P, calcitonin gene-related peptide, neuro-peptide- Y, etc.) are attached to the free nerve terminals to produce the signals which are sent to the spinal cord by A-delta or C fibers and then the brain through the spinal tract (Barrett KE et al.: Ganong’s Review of Medical Physiology,25th Ed. www.accessmedicine.com Copyright McGraw- Hill Education)
K. Shimoji and S. Kurokawa

23
A single nociceptive fiber can contain a variety of different peptides and neu-rotransmitters, and their respective roles remain largely undetermined. It is also hard to establish any correlations between the kinds of peptides that the various nociceptive pathways contain and their electrophysiological properties.
It is known, however, that glutamate and substance P are thought to be the sub-stances most involved in the transmission of pain. For example, substance P binds to specific receptors, called neurokinine-1 (NK1) receptors, that are located on the nociceptive neurons of the dorsal horn of the spinal cord.
In general, substance P has been associated with relatively slow excitatory con-nections, and hence with the persistent, chronic pain sensations transmitted by C fibers, whereas glutamate is involved in the rapid neurotransmission of acute pain associated with A-delta fibers. The receptors for glutamate and substance P can be distributed in different populations of neurons that preserve their own specific char-acteristics. But the two types of receptors can also coexist on the same neurons, as has been observed in several different parts of the central nervous system.
3.2.1 Transduction of Pain
Transduction begins when the nociceptors of C fibers and A-delta fibers of primary afferent neurons respond to noxious stimuli. Nociceptors are exposed to noxious stimuli when tissue damage and inflammation occurs as a result of trauma, surgery, inflammation, infection, and/or ischemia.
The nociceptors are distributed in the somatic structures (skin, muscles, connec-tive tissue, bones, joints) and visceral structures (visceral organs such as liver, gastro- intestinal tract).
There are three principal kinds of nociceptors: (1) Aδ mechanical nociceptors, (2) C-polymodal nociceptors, and (3) silent nociceptors.
The A-delta and C fibers are associated with different qualities of pain as listed in Table 3.1.
3.2.2 Noxious Stimuli and Responses
Harmful stimuli to the skin or subcutaneous tissue, such as joints or muscle, activate several classes of nociceptor terminals, the peripheral endings of primary sensory neurons whose cell bodies are located in the dorsal root ganglia and trigeminal gan-glia. Three major classes of nociceptors are considered: thermal, mechanical, and polymodal as well as a class termed silent nociceptors.
Thermal nociceptors are activated by extreme temperatures (>45 °C or <5 °C). They have small-diameter, thinly myelinated Aδ fibers that conduct signals at about 5–30 m/s. Mechanical nociceptors are activated by intensive pressure applied to the skin. They also have thinly myelinated Aδ fibers conducting at 5–30 m/s. Polymodal nociceptors are activated by high intensity mechanical, chemical, or thermal (both
3 Anatomical Physiology of Pain

24
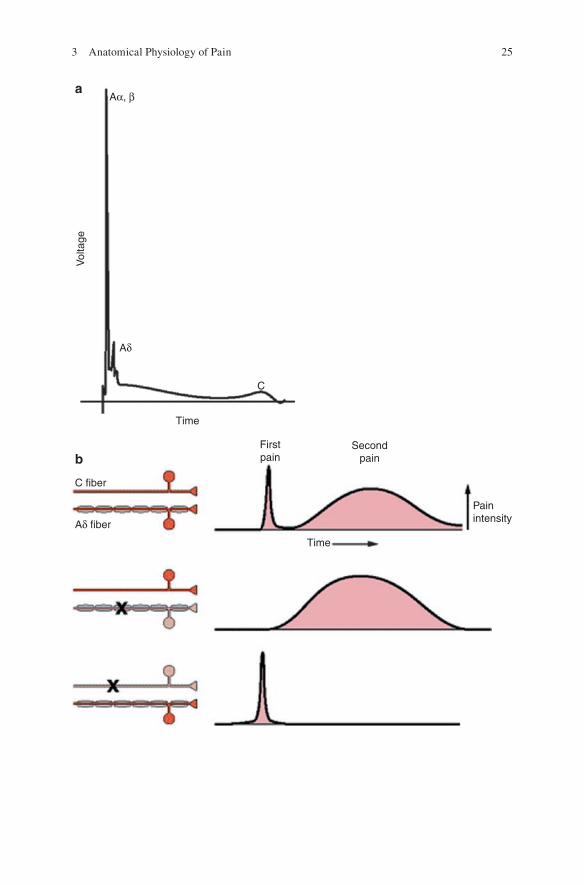
hot and cold) stimuli. These nociceptors have small-diameter, nonmyelinated C fibers that conduct slowly, generally at velocities of 0.5–2.0 m/s (Table 3.1).
The cause of stimulation may be internal, such as pressure exerted by a tumor or external excessive stimuli such as trauma or burn. These noxious stimulations cause a release of chemical mediators from the damaged cells including: prostaglandin, bradykinin, serotonin, substance P, potassium, histamine, etc. (Fig. 3.1).
These chemical mediators activate and/or sensitize the nociceptors to the nox-ious stimuli. In order for a pain impulse to be generated, an exchange of sodium and potassium ions (depolarization and repolarization) occurs at the cell membranes. This results in an action potential and generation of a pain impulse (Fig. 3.2).
Table 3.1 Characteristics and functions of A-delta and C fibers
A-delta fibers C fibers
Characteristics
• Primary afferent fibers • Primary afferent fibers • Larger diameter • Small diameter • Myelinated • Unmyelinated • Fast conducting • Slow conductingReceptor type
• High-threshold mechanoreceptors responding to mechanical stimuli over a certain intensity
• Polymodal receptor responding to more than one type of noxious stimuli:
• Thermal • Chemical • Mechanical
Pain quality
• Well-localized • Diffuse • Sharp • Dull • Stinging • Burning • Pricking • Aching • Referred to as fast or first pain • Referred to as slow or second pain
Fig. 3.2 Propagation of action potentials in sensory fibers results in the perception of pain. (Modified from Fields HL, Basbaum AI, Heinricher MM, 2005) [3]. (a) This electrical recording from a whole nerve shows a compound action potential representing the summated action poten-tials of all the component axons in the nerve. Even though the nerve contains mostly nonmyelin-ated axons, the major voltage deflections are produced by the relatively small number of myelinated axons. This is because action potentials in the population of more slowly conducting axons are dispersed in time, and the extracellular current generated by an action potential in a nonmyelinated axon is smaller than the current generated in myelinated axons. (b) First and second pain are car-ried by two different primary afferent axons. First pain is abolished by selective blockade of Aδ myelinated axons (middle) and second pain by blocking C fibers (bottom)
K. Shimoji and S. Kurokawa
25
Time
Painintensity
C fiber
Aδ fiber
Time
Vol
tage
Aδ
Aα, β
C
Firstpain
Secondpain
a
b
3 Anatomical Physiology of Pain