chronic pain services - royal national orthopaedic hospital · nhs england in relation to...
TRANSCRIPT

Chronic Pain Centre 2015
Royal National
Orthopaedic Hospital
Chronic Pain Centre
Annual Report 2015 - 16
Financial Year 2015 / 2016
Authors: Roxaneh Zarnegar (Clinical Lead)
Tacson Fernandez (Neuromodulation Section)
Tajinder Manic (Data Collection & Research Officer)

Chronic Pain Centre 2015
Contents
Introduction 3
Key Achievements in 2014 – 15 Current Constraints & Limitations
Chronic Pain Service Structure 4
Definitions & Abbreviations 5
Service Provision 6
18 Week Waiting times
Referral Pathways
Case Load 7
Case Load in Adult Pain Clinics Case Load in Paediatric Pain Clinic Admission s for Residential Pain Management Rehabilitation Programs
Case Load 10
Case Load in Neuromodulation Clinics
Patient Related Outcome Measures Data
General information on PROMs data collection 11 Outcomes Data for Adult Pain Clinics (EQ5D-5L BPI, HEALTH VAS, PGIC,SE,PDI,PHQ-2,GIC)
Neuromodulation GP Satisfaction Survey 2014 – 2015 TF 25
Friends and Family Test for the Chronic Pain Service 28
Education & Training 29
Clinical Audit and Quality Improvement 30
Research Publications and Conference Abstracts 31

Chronic Pain Centre 2015
Introduction This is the second annual report for the RNOH Chronic Pain Centre (RNOH CPC). It should be considered in conjunction with the first report (2014-15).
Key Achievements in 2015 – 16
Appointment of a fourth substantive consultant, Dr Mihaylov
Commencement of formal Complex Case, Incidents & Risks Meetings
Presentation of the service at the RNOH Clinical Audit Meeting: “The chronic pain service,
benchmarking against the National Pain Audit and patient feedback on outcomes data
collection.”
Organisation of Evening Meetings on Chronic Pain for GPs in late 2015
Chronic Pain Centre Website updated including a section on the Neuromodulation Service
Improvements to POD data collection of electronic Patient Reported Outcome Measures
(PROMs) system.
Updating RNOH website for Chronic Pain & Neuromodulation completed
Personal Pages for Pain Consultants set up
Video for Neuromodulation “Patient care for Neuromodulation” uploaded to RNOH website.
GP Satisfaction Survey commenced 2015 – 16 in review
Commencement of Patient satisfaction Survey commenced 2015 – 16
The procurement of a new dashboard for POD to streamline service reporting
Current Constraints & Limitations
Over the course of the year, the Chronic Pain Service has been engaged in discussions with
NHS England in relation to recognition as a specialised centre for delivering care for patients
with complex musculoskeletal and neuropathic pain conditions. These discussions are on-
going although initial responses to the bid have been positive.
Demand for the RNOH Chronic Pain Service has continued to rise dramatically and meeting
the 18 week target has at times been difficult. Limited supply of space for clinical activity
continues to be a significant challenge to much needed expansion.

Chronic Pain Centre 2015
Chronic Pain Service Structure
Consultants in CP Roxaneh Zarnegar (Lead Consultant)
Rebecca Berman
Tacson Fernandez
Dan Mihaylov
Consultants in Psychiatry George Ikkos
Sara McNally
Clinical Nurse Specialists Julia Sach
Faustina Aikins
Michelle Lilley
Service Manager Rob Emmins
Secretarial & Administrative Sarah Jason
Victoria Brodie Smith
Sonia Brito
Data Collection & Research Tajinder Manic
Trainees
Advanced Pain Training Anthony Gubbay (Aug 15 – Feb 16)
Nicolas Varela (Feb 16 – current)
The service is supported by:
Specialist Physio- and Occupational Therapists in CP and Rehabilitation
Rehabilitation and Pain Specialist Psychology Service
Gill Thurlow, Nurse Consultant in Rehabilitation
RNOH Central Bookings Office particularly Ethal Sangasinha & Nadine Bourne
Pharmacy services particularly Drumita Pindora, Pain Management Specialist
Pharmacist

Chronic Pain Centre 2015
Definitions & Abbreviations
BPI: British Pain Inventory CP: Chronic Pain
IASP: International Association for the Study of Pain MDT: Multidisciplinary Team NPA: National Pain Audit PMP: Pain Management Programme
PROMs: Patient Reported Outcome Measures SCS: Spinal Cord Stimulation
Chronic Pain Centre 2015
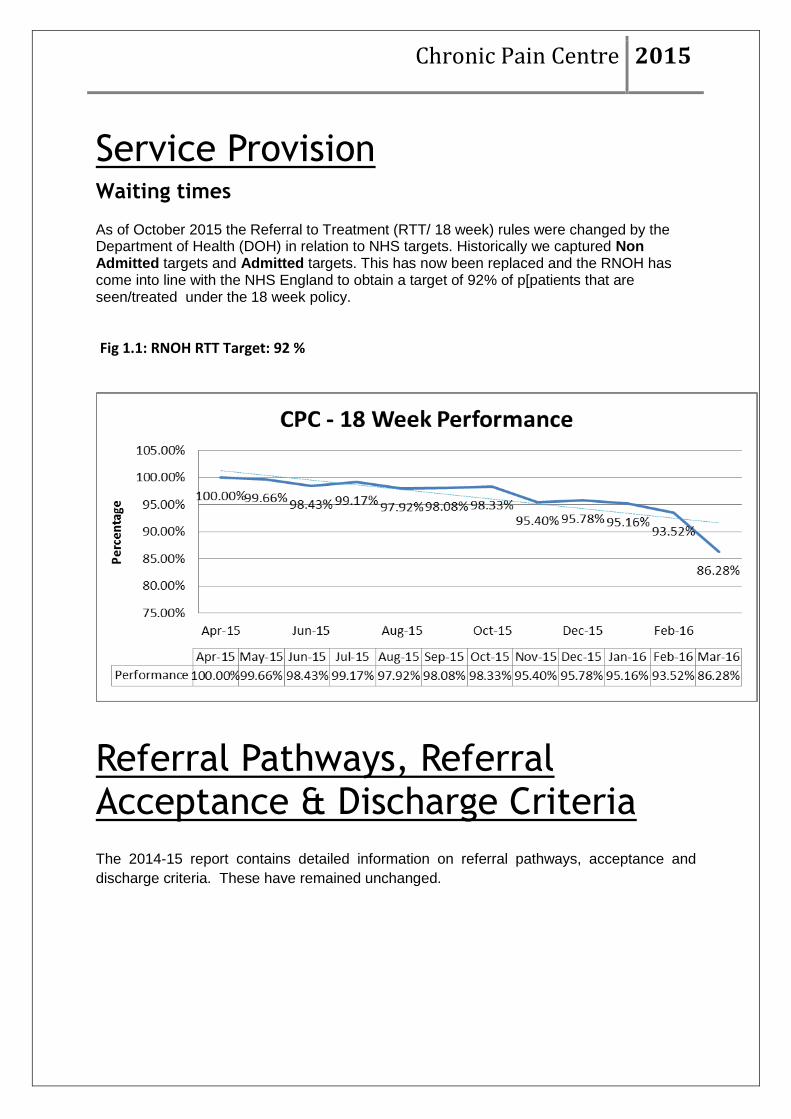
Service Provision Waiting times
As of October 2015 the Referral to Treatment (RTT/ 18 week) rules were changed by the Department of Health (DOH) in relation to NHS targets. Historically we captured Non Admitted targets and Admitted targets. This has now been replaced and the RNOH has come into line with the NHS England to obtain a target of 92% of p[patients that are seen/treated under the 18 week policy.
Fig 1.1: RNOH RTT Target: 92 %
Referral Pathways, Referral Acceptance & Discharge Criteria
The 2014-15 report contains detailed information on referral pathways, acceptance and
discharge criteria. These have remained unchanged.
Chronic Pain Centre 2015
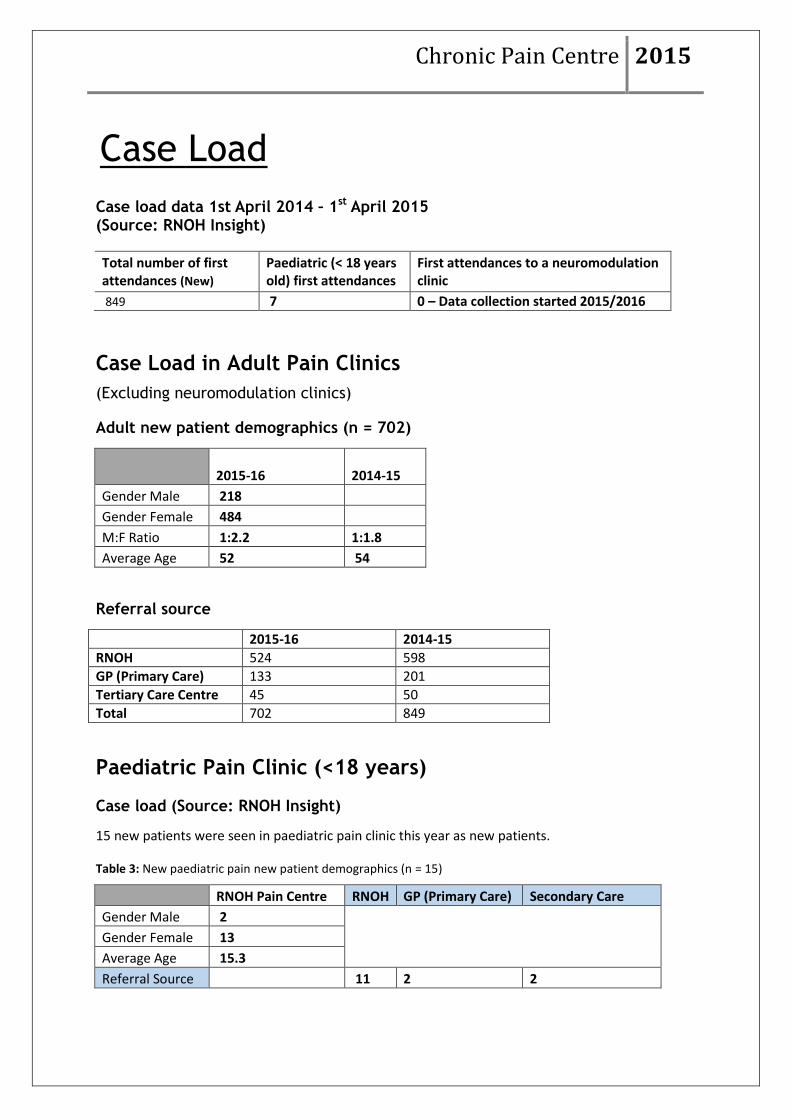
Case Load
Case load data 1st April 2014 – 1st April 2015 (Source: RNOH Insight)
Total number of first attendances (New)
Paediatric (< 18 years old) first attendances
First attendances to a neuromodulation clinic
849 7 0 – Data collection started 2015/2016
Case Load in Adult Pain Clinics
(Excluding neuromodulation clinics)
Adult new patient demographics (n = 702)
2015-16 2014-15
Gender Male 218
Gender Female 484
M:F Ratio 1:2.2 1:1.8
Average Age 52 54
Referral source
2015-16 2014-15
RNOH 524 598
GP (Primary Care) 133 201
Tertiary Care Centre 45 50
Total 702 849
Paediatric Pain Clinic (<18 years)
Case load (Source: RNOH Insight)
15 new patients were seen in paediatric pain clinic this year as new patients.
Table 3: New paediatric pain new patient demographics (n = 15)
RNOH Pain Centre RNOH GP (Primary Care) Secondary Care
Gender Male 2
Gender Female 13
Average Age 15.3
Referral Source 11 2 2

Chronic Pain Centre 2015
Waiting times
Paediatric referrals are prioritised by the service. The mean waiting time from referral to first appointment has
been 7.8 weeks in 2015-16 (median 7 weeks, range 3-18 weeks).
An analysis of paediatric referrals from April 2013 - end March 2016
Referral sources n
RNOH Spinal Surgery 11
PNI Unit 4
Shoulder & Elbow Unit 3
Paediatric Surgery 3
Joint Replacement Unit 1
GP or Community Paediatrics 3
GOS for transition 2
Total 27
Principle chronic pain problem
n
Musculoskeletal MSK axial 13
(MSK) MSK PWP* 1
MSK joint 5
MSK axial & radicular 3
MSK other 1
Neuropathic CRPS I 0
CRPS II 1
Peripheral neuropathic 3
Total 27 *PWP = Persistent Widespread Pain
Four of the above patients had persistent post-surgical pain, and five had an inherited or birth acquired MSK
condition that predisposed to the pain problem.
Treatments recommended* n Not used
Local measures TENS 15 2
Topical treatments 6
Versatis (Lidocaine 5%) 5
Medication advice Medication additions 14 2
Medication reduction 11 1
Therapy services 15
Pain procedure 5
RNOH Psychiatry** 2
Prepared for adult PMP 2
GOS referral for PMP 2
Total 27 *All patients are offered a variety of multimodal treatment options
**Patients already receiving successful treatment with CAHMS not included

Chronic Pain Centre 2015
Admissions for Residential Pain Self-Management Rehabilitation Programs (PMP)
1st April 2015 – 1st April 2016. This data does not include admissions under rheumatology and rehabilitation services
Number of admissions for pain rehabilitation: 69
Hotel programme: 34 Rehabilitation ward: 35 PMP patient demographics
RNOH Pain Centre
Gender Male 21
Gender Female 48
Ratio M:F 1:2.3
Average Age 49

Chronic Pain Centre 2015
Case Load in Neuro-modulation Clinics
Neuromodulation Activity April 2015 – April 2016
43 New patients referred to the Neuromodulation clinic.
17 were selcted for 2nd
stage full implant.
RNOH Pain Centre
New Patients 19
Number of Trials 19
Number of patient who have completed 1st Stage awaiting 2nd stage 17
Number of implants 2nd Stage 17
Number of implants 2nd Stage that completed POD outcomes 7
New Patients Fully Implanted 2015 – 2016 (n = 17)
RNOH Pain Centre
Gender Male 8
Gender Female 11
M:F Ratio 1.1.4
Average Age 50
Median Age 50
Note: 7 patients filled out Pre assessment and Post assessment Neuromodulation questionnaires.
{6 patients forgot to fill out there pre assessment from & 4 patients did not fill any from out.} The Neuromodulation
Service is moving from paper based questioners to electronic during 2016/2017 RNOH service to lower the impact of
missing outcomes for service reporting.
Age group (Average age)

Chronic Pain Centre 2015
Outcomes Data (Neuromodulation) 1st April 2015– 31st March 2016 (inclusive)
First Visit PROMS Data for Neuromodulation Clinics
A) EuroQol 5D-5L – Neuromodulation patients with SCS/PNS insertion (17)
Table: Data on Pre-Op visit to RNOH Pain Clinic (n = 7 of the 17 patients who completed proms)
EQ5D-5L health state Mobility (%)
Self-care (%)
Usual activities (%)
Pain (%) Anxiety/depression
(%)
No problems (1) 0(0%) 2(28.6) 0(0%) 0(0%) 0(0%)
Some impact (2) 0(0%) 1(14.3) 1(14.3) 0(0%) 1(14.3)
Moderate (3) 1(14.3) 3(42.9) 0(0%) 0(0%) 4(57.1)
Severe impact (4) 5(71.4) 1(14.3) 5(71.4) 3(42.9) 1(14.3)
Extreme impact/unable to do activity at all (5) 1(14.3) 0(0%) 1(14.3) 4(57.1) 1(14.3)
Table: Data on Post –Op visit to RNOH Pain Clinic (n = 7 of the 17 patients who completed proms)
EQ5D-5L health state Mobility (%)
Self-care (%)
Usual activities (%)
Pain (%) Anxiety/depression
(%)
No problems (1) 1(14.3) 3(42.9) 0(0%) 0(0%) 2(28.6)
Some impact (2) 0(0%) 2(28.6) 1(14.3) 1(14.3) 1(14.3)
Moderate (3) 1(14.3) 1(14.3) 1(14.3) 3(42.9) 2(28.6)
Severe impact (4) 4(57.1) 1(14.3) 5(71.4) 1(14.3) 2(28.6)
Extreme impact/unable to do activity at all (5) 1(14.3) 0(0%) 0(0%) 2(28.6) 0(0%)
Figure 6: EQ 5D-5L comparative profiles for before & after implantation in neuromodulation patients

Chronic Pain Centre 2015
(Smaller value indicates higher health status)

Chronic Pain Centre 2015
Table 7: EuroQol Index Value of Health Status Pre & Post implantation for neuromodulation.
(n = 7 of the 17 patients who completed proms)
Average (Mean)
Pre Implantation (n = 7) 3.7 Post Implantation (n = 7) 4.9
Table 8: EuroQol Health VAS Scores on Pre & Post implantation for neuromodulation
(n = 7 of the 17 patients who completed proms)
Median Mean
Interquartile range
Pre Implantation (n = 7) 40 45 61 – 70 Post Implantation (n = 7) 85 79 12 -18

Chronic Pain Centre 2015
(Higher value indicates Higher health status)

Chronic Pain Centre 2015
B) Brief pain inventory – Total patients (12)
Table 9: BPI – Pain severity score at Pre & Post implantation for neuromodulation
Pain ratings Pre Pain average Post Pain average
Minimum 0 0
1st quartile 61 27
Median 64 56
Mean 65.6 63.6
3rd quartile 70 59
Maximum 10 10
Table 10: BPI – Pain severity score at Pre & Post implantation for neuromodulation
(Smaller value indicates higher health status)
Table 11: BPI – Pain interference profile at Pre Assessment visit to RNOH Neuro-mod Clinic
ITEM
Statistic General activity Mood
Walking ability
Normal work past 7 days
Relationships with other people Sleep
Enjoyment of life
BPI interference (mean)
Minimum 0 0 0 0 0 0 0 0
1st quartile 8 9 8 8 9 9 9 9.8
Median 10 10 10 10 9 10 10 10
Mean 9.3 9.6 9.4 9.3 9 9.4 9.6 9.4
3rd quartile 10 10 10 10 10 10 10 10
Maximum 10 10 10 10 10 10 10 10
Mean average pain severity
Pre Implantation (n = 7) 65.6 Post Implantation (n = 7) 45.4

Chronic Pain Centre 2015
Table 11: BPI – Pain interference profile at Post Assessment visit to RNOH Neuro-mod Clinic
ITEM
Statistic General activity Mood
Walking ability
Normal work past 7 days
Relationships with other people Sleep
Enjoyment of life
BPI interference (mean)
Minimum 0 0 0 0 0 0 0 0
1st quartile 4 4 3 4 3 5 3 3.7
Median 8 8 8 8 5 8 8 7.8
Mean 6.4 7 6.6 6.6 5.7 6.9 6.3 6.5
3rd quartile 9 9 10 9 8 9 8 8.9
Maximum 10 10 10 10 10 10 10 10
Table 12: Direct comparison of Pre & Post implantation for neuromodulation
(n = 7 of the 17 patients who completed proms)
BPI median average pain
Pre Implantation (n = 7)
9.4
Post Implantation (n = 7)
6.5
(Smaller value indicates higher health status)

Chronic Pain Centre 2015
E) S-E Questionnaire – (Self-Assessment)
Table 12: Direct comparison of Pre & Post implantation for neuromodulation
(n = 7 of the 17 patients who completed proms)
Questions Average
Pre Average
Post
Still enjoy things, despite pain 6.7 2.9
I can still do most of household chores despite pain 5.5 3.3
I socialise with friends/family despite pain 6 3.3
I can cope with pain in most situations 5.5 3.7
I can do some sort of work 6.7 4
I can still do my many hobbies despite the pain 15 5.5
I can cope with my pain without medication 7.5 4.6
I can accomplish most of my goals despite the pain 7.5 4.6
I can still live a normal life despite the pain 7.5 4
I can gradually become more active despite the pain 10 3.5
(Pain scores are out of a total of 60 – Higher number indicates lower health /confidence
status.)

Chronic Pain Centre 2015

Chronic Pain Centre 2015
F) PDI (Pain disability Index)
Table 12: Direct comparison of Pre & Post implantation for neuromodulation
(n = 7 of the 17 patients who completed proms)
Questions Average
Pre Average
Post
Family Home Responsibility 1.1 1.4
Recreation 1.1 1.4
Social Activity 1.2 1.5
Occupation 1.3 1.6
Sexual Behaviour 1.3 2.3
Self-Care 1.6 2.3
Life Support Activity 1.9 2.6
(Pain scores are out of a total of 70 – Lower number indicates lower health /confidence
status.)

Chronic Pain Centre 2015
Chronic Pain Centre 2015
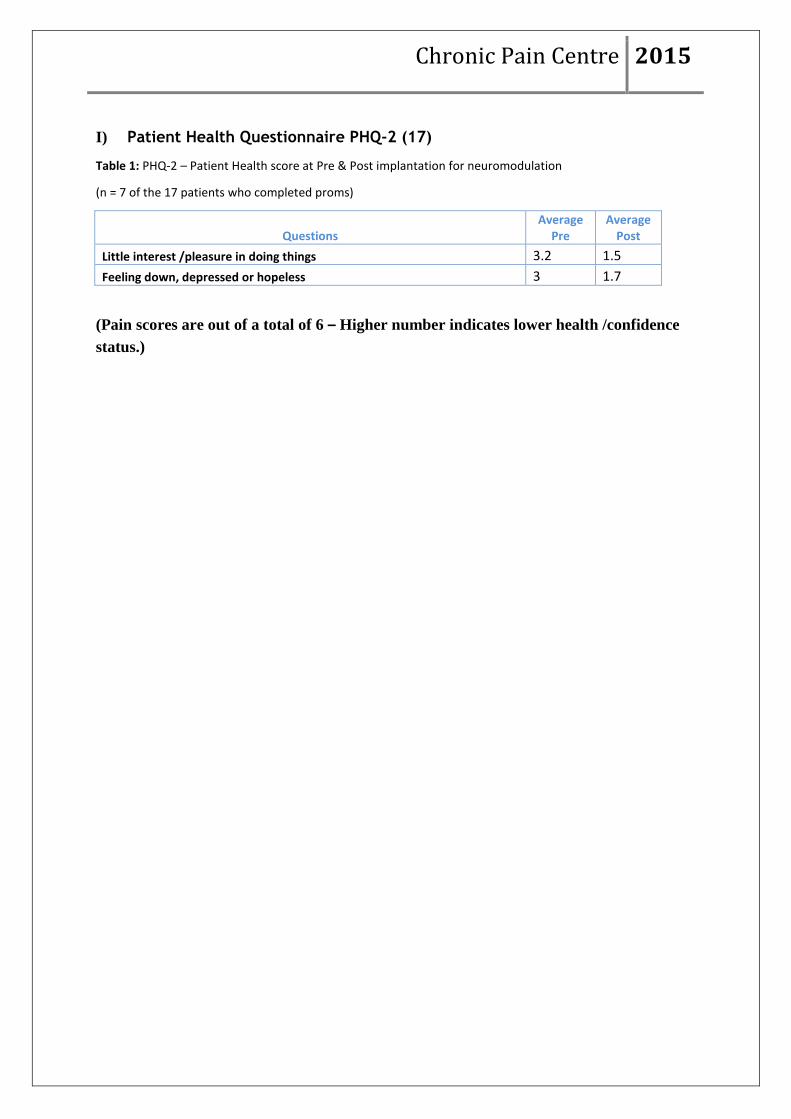
I) Patient Health Questionnaire PHQ-2 (17)
Table 1: PHQ-2 – Patient Health score at Pre & Post implantation for neuromodulation
(n = 7 of the 17 patients who completed proms)
Questions Average
Pre Average
Post
Little interest /pleasure in doing things 3.2 1.5
Feeling down, depressed or hopeless 3 1.7
(Pain scores are out of a total of 6 – Higher number indicates lower health /confidence
status.)

Chronic Pain Centre 2015

Chronic Pain Centre 2015
K) Global impression of change Questionnaire – Total patients (17)
The GIC is broken down into 2 scales: Severity scaling & Improvement scaling.
GIC - Severity scales & Improvement scaling at Pre & Post implantation for neuromodulation.
(n = 7 of the 17 patients who completed proms)
Questions Average
Pre Average
Post
How bad is overall pain 6 4.3
Compare your health from admission to today, how has it changed. 5 2.4
(Pain scores are out of a total of 14 – Higher number indicates lower health /confidence
status.)

Chronic Pain Centre 2015

Chronic Pain Centre 2015
Neuromodulation GP Satisfaction
Survey 2014 – 2015 TF
Chronic Pain Centre 2015

Chronic Pain Centre 2015
Selection of comments received:
‘Patient reports excellent experience’
‘The only drawback was the travel distance’
‘You are offering an excellent service’
‘Excellent result’
‘Continue to maintain the excellent standards of care provided’
Chronic Pain Centre 2015
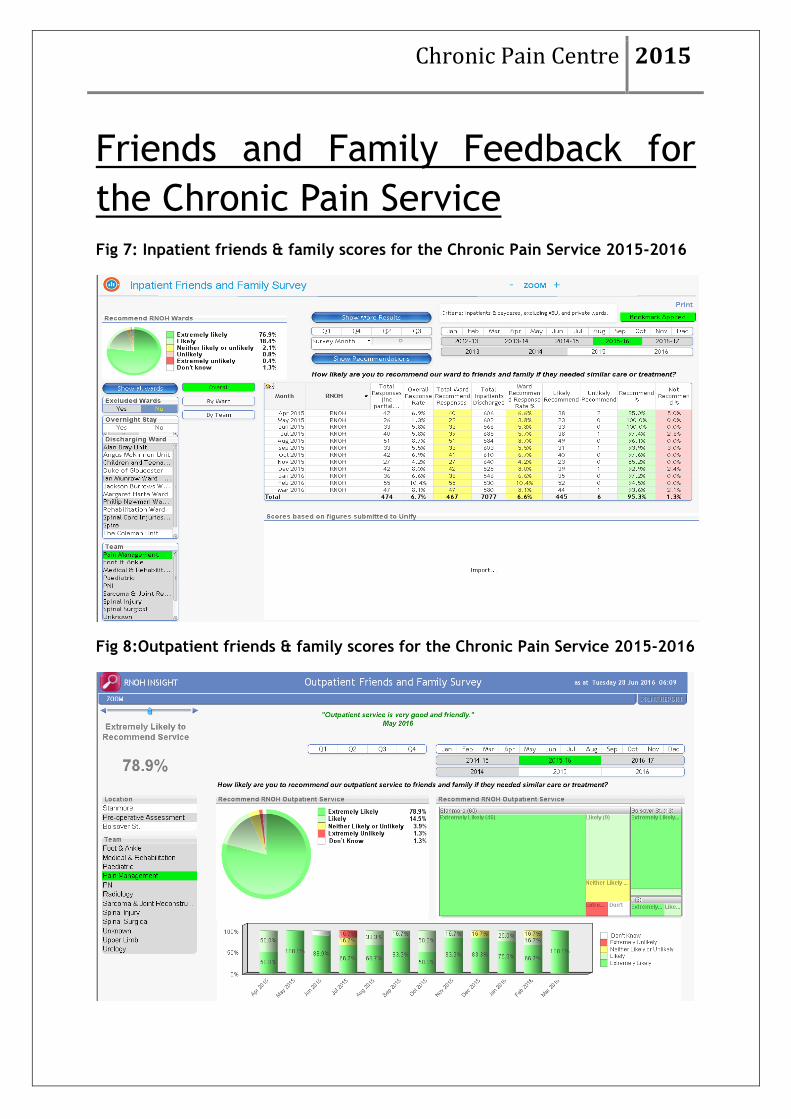
Friends and Family Feedback for
the Chronic Pain Service
Fig 7: Inpatient friends & family scores for the Chronic Pain Service 2015-2016
Fig 8:Outpatient friends & family scores for the Chronic Pain Service 2015-2016

Chronic Pain Centre 2015
Education & Training
Advanced pain training
Written by Dr Nicolas Valera, Advanced Trainee, February 2016 for six months
RNOH is a nationwide center of excellence for the care of orthopaedic patients.
There is also a growing chronic pain service that currently has an advanced pain
trainee (APT) post. This is a 1 year post, with six months at RNOH and 6 months
take at National Hospital for Neurology and Neurosurgery (UCL).
As an APT my clinical duties included outpatients clinics (2 days each week),
interventional lists (between 2 and 2.5 days each week), inpatients review, MDT’s
and administrative time. All of my work was supervised, whether directly or
indirectly, and I had an excellent consultant support. It is to be noted that as
RNOH is a very specialised center, the patients seen in our clinics usually have
complex orthopaedic pathology (extreme scoliosis, multiple surgeries, etc.) and
are therefore challenging from a pain treatment point of view. Nevertheless, this
was much easier thanks to the fact that the consultants and Clinical Specialist
Nurses are always there to help the fellow.
The work at RNOH is intense, and throughout this six months I have seen almost
600 patients in clinic or theatre. Nevertheless this has not had a negative impact in
the teaching as I was encourage to attend different meetings with other
departments (Spine MDT, radiology MDT, psychiatry MDT) as well as clinics with
other specialists. The Advanced Pain Trainee attends one neuromodulation whole
day theatre list every other week, and at the end of the 6 months that means more
than 20 procedures (implants and trials).
Finally, I can’t finish without saying a word about the people that work here at
RNOH. During this six months everybody has been very pleasant as well as very
professional. This makes work much easier and there hasn’t been one single issue
with the rest of the people that work here. This is a huge help for the trainee who
will feel very confident since the very beginning. I have no doubt that I would
truly recommend this post to any trainee wanting to follow the pain medicine
pathway.
RNOH Pain Management Evening Educational Sessions – 17th November 2015, 24th November 2015
This was started as a new initiative in 2015 and organized primarily by Dr Mihaylov
with support from the RNOH Teaching Centre and collaboration with the RNOH

Chronic Pain Centre 2015
Rheumatology Department. The sessions were aimed mainly at GPs. Four sessions
were organized in two evening on 17th And 24th November:
‘Pain Management Programmes’, Dr R Zarnegar ‘Fibromyalgia: diagnosis & management’, Dr H Cohen ‘Inflammatory spondyloarthropathy: diagnosis & management’, Dr Gayatri Mittal ‘Opioids for persistent non – malignant pain’, Dr D Mihaylov Over 30 people attended the sessions and 26 feedback forms were collected.
Feedback from the sessions was very positive with all talks rated as good or very
good by all the participants in the categories of presentation content, speakers’
skills and general organization of the evenings. Further evenings are planned in
2016.
Clinical Audit & Quality
Improvement
The RNOH VTE Risk Assessment Audit
All admissions under the care of a CPC consultant are risk assessed for VTE on admission. The Trust’s performance in this area is steadily improving. The vast majority of our patients who are admitted for day case interventional procedures are not expected to have any reduction in mobility compared to their normal state and therefore do not need any prophylactic measures. Rehabilitation admissions usually have greater mobility than usual. Mechanical prophylaxis measures are used for patients who need more extensive procedures such as insertion of neuro-stimulator.
Audit of Referral Triage 2015-16
R Zarnegar
Referrals to the RNOH CPC are triaged by the service clinical lead according to the referral
acceptance criteria for the centre. During 2015-16, 92 referrals were sent back. Most were GP
referrals (70), 19 were from RNOH clinicians and 3 were from other sources.
The commonest reason for a referral not to be accepted is that the case is suitable for a local
secondary care service (52 cases). In 20 cases, referral to another service (not pain clinic) would
have been more suitable and in 4 cases another more suitable tertiary centre was suggested to the
GP, the reasons for the letter may have been geographical or clinical. Eleven letters were sent back
because there was insufficient information for triage. A number of these would subsequently be re-
referred and may or may not have got an appointment.
Overall 11% of referrals are sent back. Referrals from RNOH clinicians are in patients with more
complex physical or psychosocial problems and are less likely not to receive an appointment.

Chronic Pain Centre 2015
Policies & Procedures
In 2015, the following CPC documents were updated:
Patient information for nerve root injections (R Zarnegar & J Sach)
Research Publications, & Abstracts
Kalsi P, Turkistani W, Sykes C, Lucas A, Zarnegar R. "Work is a beautiful
thing...." Exploring attitudes towards employment in chronic pain (CP) patients
attending a pain management programme (PMP). Journal of Vocational
Rehabilitation 2015 44:97-107. DOI:10.3233/JVR-150783
Zarnegar R, Brown M D R, Henley M, Tidman V, Pathmanathan A. Patient
perceptions and recall of consent for regional anaesthesia compared with
consent for surgery. Journal of the Royal Society of Medicine 2015 108:451-456.
DOI: 10.1177/0141076815604494
Zarnegar R, Rajapakse D, Finch J. Managing Children’s Pain; Pharmacology and
Prescribing in Paediatric Pain Management. Pain management eLearning for
Royal College of Paediatrics and Child Health, 2015.
Ikkos, G., Psychiatric Expertise in 100 words. BJPsych 2015 207(5): 399
Carol Smyth, Marcantonio M Spada, Katherine Coultry-Keane & George Ikkos (2016): The Stanmore Nursing Assessment of Psychological Status:
Understanding the emotions of patients with spinal cord injury, The Journal of Spinal Cord Medicine, DOI: 10.1080/10790268.2016.1163809 Published 8 April 2016
Conference Presentations Prof G Ikkos: Key note speaker IASP Special Interest Group for CRPS International Congress, title of talk “Psychiatry and CRPS: From Somatisation to
Health Anxiety and beyond” Zurich, 1 Sept 2015
Prof G Ikkos: British Pain Society Conference Plenary Lecture: 21/22/23 Title of talk : "Pain and Psychiatry: body, brain, mind, self and clinical practice" Glasgow, April 2015