cigarette smoking, n-acetyltransferases 1and 2, breast cancer … · 2005-07-30 · multivariate...
TRANSCRIPT

Vol. 7. 371-378, May 1998 Cancer Epidemiology, Biomarkers & Prevention 371
Cigarette Smoking, N-Acetyltransferases 1 and 2, andBreast Cancer Risk1
Robert C. Millikan,2 Gary S. Pittman, Beth Newman,Chiu-Kit J. Tse, Ornella Selmin, Beverly Rockhill,David Savitz, Patricia G. Moorman, and Douglas A. Bell
Department of Epidemiology, School of Public Health and LinebergerComprehensive Cancer Center, School of Medicine, University of North
Carolina, Chapel Hill, North Carolina 27599-7400 [R. C. M., B. N., C-K. J. T.,D. 5.1; National Institute of Environmental Health Sciences, Research Triangle
Park, North Carolina 27709 [G. S. P., D. A. B., 0. 5.]; School of Public
Health, Harvard University, Boston, Massachusetts 021 15 [B. Ri; and
Department of Epidemiology and Public Health, Yale University, New Haven,
Connecticut 06510 [P. G. M.]
AbstractTo examine the effects of smoking and N-acetylationgenetics on breast cancer risk, we analyzed data from anongoing, population-based, case-control study of invasivebreast cancer in North Carolina. The study populationconsisted of 498 cases and 473 controls, withapproximately equal numbers of African-American andwhite women, and women under the age of 50 and age 50years or older. Among premenopausal women, there wasno association between current smoking [odds ratio (OR),0.9; 95% confidence interval (CI), 0.5-1.5] or pastsmoking (OR, 1.0; 95% CI, 0.6-1.6) and breast cancerrisk. Among postmenopausal women, there was also noassociation with current smoking (OR, 1.2; 95% CI, 0.7-2.0); however, a small increase in risk was observed for
past smoking (OR, 1.5; 95% CI, 1.0-2.4). Forpostmenopausal women who smoked in the past, Oilsand 95% CIs were 3.4 (1.4-8.1) for smoking within thepast 3 years, 3.0 (1.3-6.7) for smoking 4-9 years ago, and0.6 (0.3-1.4) for smoking 10-19 years ago. Neither N-
acetyltransferase 1 (NA Ti) nor N-acetyltransferase 2(NAT2) genotype alone was associated with increased
breast cancer risk.There was little evidence for modification of smoking
effects according to genotype, except amongpostmenopausal women. Among postmenopausal women,Oils for smoking within the past 3 years were greater forwomen with the NATi*iO genotype (OR, 9.0; 95% CI,1.9-41.8) than NATi�non*1O (OR, 2.5; 95% CI, 0.9-7.2)and greater for NAT2-rapid genotype (OR, 7.4; 95% CI,1.6-32.6) than NAT2-slow (OR, 2.8; 95% CI, 0.4-8.0).
Received 10/10/97; revised 2/18/98; accepted 3/1/98.
The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked advertisement in
accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
i Supported by the Specialized Program of Research Excellence in Breast Cancer,
NIH/NC! P50-CA58223; Pesticides and Breast Cancer in North Carolina, NIH!
NIEHS ROl -ESO7 128; Environment and Breast Cancer Program, R2 1-CA66201;
and National Action Plan on Breast Cancer, DWH 00014.
2 To whom requests for reprints should be addressed, at Department of Epide-
miology, CB #7400, School of Public Health, University of North Carolina at
Chapel Hill, NC 27599-7400.
Future studies of NAT genotypes and breast cancershould investigate the effects of environmental tobaccosmoke, diet, and other exposures.
Introduction
The relationship between cigarette smoking and breast cancer
has been examined in numerous epidemiological studies. Mostdemonstrate a weak positive association or no association,
whereas a few suggest a weak inverse association (1). Amongpositive studies, greater risk for longer duration of smoking isreported more consistently than a dose-response relationship
based on the number of cigarettes smoked (1). In the largestcase-control study to date, Baron et a!. (2) found no association
between current smoking and breast cancer risk and a slightlyincreased risk of breast cancer for past smoking. In anotherrecent case-control study, Morabia et al. (3) included informa-tion on exposure to ETS.3 After excluding women exposed toETS (at home, at work, and during leisure time) from thereferent group, the authors observed strong positive associa-
tions for active smoking (current and past), and risk of breastcancer increased with the number of cigarettes smoked. In-creased risk also was observed among women exposed only to
ETS.Two recent epidemiological studies examined whether
polymorphisms in the NAT2 gene increase susceptibility to the
effects of tobacco smoke and thereby increase risk of breast
cancer (4, 5). N-Acetylation represents a metabolic detoxifica-tion pathway for arylamines, a group of potentially carcino-genic compounds that includes 4-aminobiphenyl and other con-stituents of cigarette smoke (6-9). Approximately 50% ofwhites and a lower proportion of African-Americans inherit a
polymorphism in the NAT2 gene that leads to decreased acet-ylator activity (i.e., NAT2-”slow” genotype; Refs. 10 and I 1).Ambrosone et a!. (4) found that postmenopausal women with
the NAT2-slow genotype exhibited strong positive dose-re-sponse relationships between breast cancer risk and the numberof cigarettes smoked 2 and 20 years ago, as well as cumulative
pack-years of smoking. No association between smoking andbreast cancer was observed ignoring NAT2 genotype. Recentresults from a case-control study nested within the Nurse’s
Health Study cohort (5) suggested that current smoking wasassociated with a only a slight increase in breast cancer riskamong women with the NAT2-slow genotype. Althoughslightly stronger in postmenopausal women, this increase wasnot statistically significant. The authors also noted a slight (butstatistically nonsignificant) increase in risk associated with pastsmoking among women with the NAT2 rapid genotype.
Neither Ambrosone et a!. (4) nor Hunter et a!. (5) exam-
3 The abbreviations used are: ETS, environmental tobacco smoke: CBCS. Caro-
lina Breast Cancer Study; NAT!, N-acetyltransferase I ; NAT2, N-acetyltransferase
2; OR, odds ratio; CI, confidence interval.
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

372 Cigarette Smoking and Breast Cancer Risk
med the effect of NAT2*14, a low-activity allele found mainlyin individuals with African ancestry (10). In addition, no breastcancer study to date has investigated the role of newly discov-ered polymorphisms in the NATJ gene. The NAT1 enzyme
participates in N-acetylation of a variety of carcinogenicarylamines (6, 12) and is expressed in breast tissue (13). NAT]
alleles exhibit variable acetylator activity (14-17). Severalstudies suggested that the NATJ*1O allele is associated with
elevated N-acetyltransferase activity (reviewed in Ref. 18).However, the link between NAT] alleles and enzyme function
has not been directly established, and further investigations arepresently being conducted to clarify the functional significanceofNATJ gene variants (18-20).
As part of a population-based, case-control study con-ducted among African-American and white women in NorthCarolina, we examined the effects of active smoking as well as
ETS on breast cancer risk and addressed the role of polymor-
phisms at both NAT] and NAT2.
Subjects and Methods
Case and Control Selection
The CBCS is an ongoing, population-based, case-control study
of breast cancer in North Carolina (21). Women with a firstdiagnosis of histologically confirmed, invasive breast cancer
were identified through a rapid ascertainment system with thehelp of the North Carolina Central Cancer Registry (22). Con-trols were selected from lists provided by the North CarolinaDivision of Motor Vehicles (women ages 20-64) and the
United States Health Care Financing Administration (womenages 65-74). Randomized recruitment (23) was used to identifyapproximately equal numbers of African-American and white
women as well as equal numbers of women younger than age50 and age 50 or older, among cases and controls. During Phase
1 of the CBCS (May 1993-December 1996), 889 cases and 841controls were enrolled. Among eligible and locatable women,interviews were completed for 77% of cases and 68% of con-trols. For the present study of NAT genotype and smoking,sampling was based solely on timing: we included the first 498
cases and 473 controls who agreed to a home interview and
provided a blood sample, in order of enrollment in the CBCS.
Data Collection
In-person interviews were conducted in participants’ homes by
trained nurse-interviewers and included reproductive history,diet, and lifestyle factors, a detailed family history, and occu-pation history. Approximately 98% of participants who wereinterviewed agreed to give a 30-ml blood sample at the time of
interview. Informed consent to obtain germ-line DNA wassought using a form approved by the Institutional ReviewBoard of the University of North Carolina School of Medicine.
Variable Definitions
Race was classified according to self-report. For the presentanalysis, we classified women as African-American and white.Among whites, we included seven American-Indians, three
Asian-Americans, and three women who listed their race as“multiracial.”
With regard to smoking, women were asked about current
and past smoking status, age at initiation of smoking, number of
cigarettes smoked, and whether they had ever lived with some-one who smoked. A reference date of the date of diagnosis (for
cases) or selection (for controls) was used to define exposurestatus for all study participants. Participants who had smoked at
least 100 cigarettes in their lifetime and were smoking on thereferent date were considered current smokers. Those who hadsmoked at least 100 cigarettes in their lifetimes but ceasedsmoking prior to the referent date were considered former
smokers. Former smokers were further categorized according totime since quitting, calculated as the interval between the date
of smoking cessation and the referent date. Duration of smok-ing was determined by asking, “Keeping in mind that you may
have stopped and started several times, overall how many years
did you smoke regularly?” Women were classified as exposedto ETS if they reported living with a smoker when they were 18
years of age or older. Women also were asked about pipesmoking and snuff use, but there were too few positive respon-dents for meaningful analysis.
Laboratory Methods
Germ-line DNA was extracted from peripheral blood leuko-
cytes according to standard methods (24) and stored for futureuse.
NATJ Genotyping. Four variants in the 3’ region of NAT]
near the polyadenylation signal were genotyped according tomethods published previously (15). Terminology for NAT al-
leles follows the recommendations of Vatsis et al. (25). Thealleles detected were NATJ*4, NAT]*3, and NAT]*]], all ofwhich contain the consensus mRNA polyadenylation signal
(nucleotides 1086-1092) of “T” at nucleotide 1088, andNAT]*]O, which contains “A” at nucleotide 1088, resulting ina shift of the polyadenylation signal. PCR was used to amplify100 ng of DNA, followed by restriction enzyme digestion,
agarose gel electrophoresis, and RFLP analysis, as describedpreviously (15).
Individuals were classified as NAT]*]O if they possessed
one or two copies of the NATJ*]O allele; otherwise, they wereclassified as NAT]�non*]O. Preliminary evidence suggests thatthe presence of one or more copies of the NATJ*]O allele is
associated with increased enzymatic activity, but a direct rela-tionship between genotype and phenotype has not been firmly
established (18). For the purposes of the present analysis, wegrouped individuals on the basis of the presence or absence ofthe consensus mRNA polyadenylation sequence: the NAT]*1O
allele contains a shift in the m.RNA polyadenylation signal,whereas the remaining alleles (NAT]*4, NAT]*3, andNAT]*]]) contain the consensus signal. The NAT] assay was
unreadable for 6 cases and 5 controls; thus, NAT] results arepresented for 492 cases and 468 controls.
NAT2 Genotyping. PCR-RFLP methods were used to identifythe five most common functional and low-activity NAT2 alle-les, as described previously (10). The alleles detected were:
NAT2*4 (wild-type or functional allele); and the low-activityalleles, NAT2*5 (Ml: KpnI polymorphism, C481T), NAT2*6(M2: TaqI polymorphism, G590A), NAT2*7 (M3: BamHI poly-morphism, G857A), and NAT2*14 (M4: MspI polymorphism,
GI91A).Individuals homozygous for the functional NAT2*4 allele
were classified as NAT2 rapid. Individuals heterozygous forNAT2*4 in combination with a low-activity allele (NAT2*5,
NAT2*6, NAT2*7, or NAT2*]4) were classified as NAT2 in-termediate. Individuals with any combination of the low-activ-
ity alleles (i.e., those who did not inherit NAT2*4) were clas-sified as NAT2-slow. To calculate ORs for NAT2, we combinedwomen with NAT2-rapid and -intermediate genotypes and com-
pared them with NAT2-slow, as performed by Ambrosone et a!.
(4). ORs were nearly identical when we combined women withNAT2-slow and intermediate genotypes and compared with
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 373
NAT2-rapid. The NAfl assay was unreadable for 10 cases and1 control; thus, NAT2 results are presented for 488 cases and472 controls.
Statistical Methods
Adjusted ORs and 95% CIs from unconditional logistic regres-sion models were used as the measure of association (26).
PROC GENMOD of the software package SAS (version 6. 1 1;SAS Institute, Cary, NC) was used to incorporate offsets de-rived from the sampling probabilities used to identify eligible
participants (23) and to adjust for race (as a two-level categor-ical variable) and age (as an 1 1-level ordinal variable that
reflected 5-year age categories).For analyses of active smoking effects, a common referent
group of women who had smoked fewer than 100 cigarettes intheir lifetime (“never smokers”) was used. When we excludedwomen with exposure to ETS from the referent group, ORs for
active smoking were unchanged or slightly attenuated. Thus,results for active smoking are presented ignoring ETS. Analy-
ses of ETS were conducted among women who never smoked
themselves (“never smokers”), using as a referent group womenexposed to neither active smoking nor ETS.
Multivariate logistic models were used to adjust for po-
tential confounding factors (26). Covariates included age atmenarche (continuous), age at first full-term pregnancy (threecategories), parity (three categories), lactation (ever/never),
family history of breast cancer (yes/no for first-degree relative),and benign breast biopsy (yes/no). In this population, relatively
few women consumed large amounts of alcohol; thus, analysesof this variable are based upon a dichotomous (ever/never)categorization only. Participants with missing values for any ofthe variables in a regression model were not included in such
analyses. Stratified analyses were used to investigate the effectsof menopausal status. For the present analysis, menopausal
status was defined using criteria identical to those used by
Ambrosone et a!. (4): for women under the age of 50 years,postmenopausal status was assigned to women who had under-
gone natural menopause, bilateral oophorectomy, or irradiationto the ovaries; in women aged 50 years or older, menopausal
status was assigned on the basis of cessation of menstruation.For NAT] and NAT2, tests for Hardy-Weinberg equilib-
rium were performed by comparing observed and expectedgenotype frequencies using a f test (27), as implemented inSAS. We estimated the main effects for NAT genotypes using
ORs. We investigated additive and multiplicative interactionbetween NAT] and NAT2 (gene-gene interaction) by conduct-ing stratified analyses classifying individuals with the combi-
nation of NAT]*]O and NAT2 rapid genotypes as a commonreferent group and calculating ORs for the remaining combi-
nations of NAT] and NAT2 genotypes. To further investigatemultiplicative interaction, we included both genotypes in mul-tivariate models and used P for the interaction term as a test forstatistical significance (28). We investigated modification ofsmoking effects by NAT] and NAT2 genotype status (gene-environment interaction) using stratified analyses (29). Testsfor trend were conducted by calculating Ps for the f3 coefficientin a logistic regression model with the exposure coded as anordinal variable (28).
Results
Characteristics of Cases and Controls. Characteristics ofbreast cancer cases and controls are presented in Table I.
Participants in the present analysis did not differ appreciably
from the entire CBCS.
Table I Characteristics of breast ca ncer cases and controls
Cases Controls
n498 ,i473
,i ((4.) n (‘5�)
Age
20-29
30-39
40-49
50-59
60-69
>70
Race
African-American
White
Menopausal status
Premenopausal
Postmenopausal
Age at menarche (yr)
<12
�l2
Missing
Age at first full-term pregnancy (yr)
Nulliparous
<26
�26
Missing
No. of children
Nulliparous
Missing
Breastfeeding
Never
Ever
Missing
Breast cancer in first-degree relative
No
Yes
Missing
Breast biopsy
No
Yes
Missing
Alcohol consumption
Never
Ever
Missing
13
75
193
75
176
41
(2.6)
(15.1)
(38.8)
(15.1)
(20.3)
(8.2)
4
56
179
99
92
43
(1.0)
(11.8)
(37.8)
(20.9)
(19.5)
(9.0)
202
296
(40.6)
(59.4)
198
275
(41.9)
(58.1)
241
257
(48.4)
(51.6)
217
256
(45.9)
(54.1)
117
381
0
(23.5)
(76.5)
102
370
1
(21.6)
(78.4)
75
318
102
3
(15.2)
(64.2)
(20.6)
51
317
103
2
(10.8)
(67.3)
(21.9)
75
97
326
0
(15.1)
(19.5)
(65.4)
51
80
342
0
(10.8)
(16.9)
(72.3)
333
165
0
(66.9)
(33.1)
267
206
0
(56.5)
(43.5)
408
78
12
(84.0)
(16.0)
402
53
18
(88.4)
(11.6)
409
86
3
(82.6)
(17.4)
394
77
2
(83.7)
(16.3)
146
352
0
(29.3)
(70.7)
140
332
1
(30.0)
(70.0)
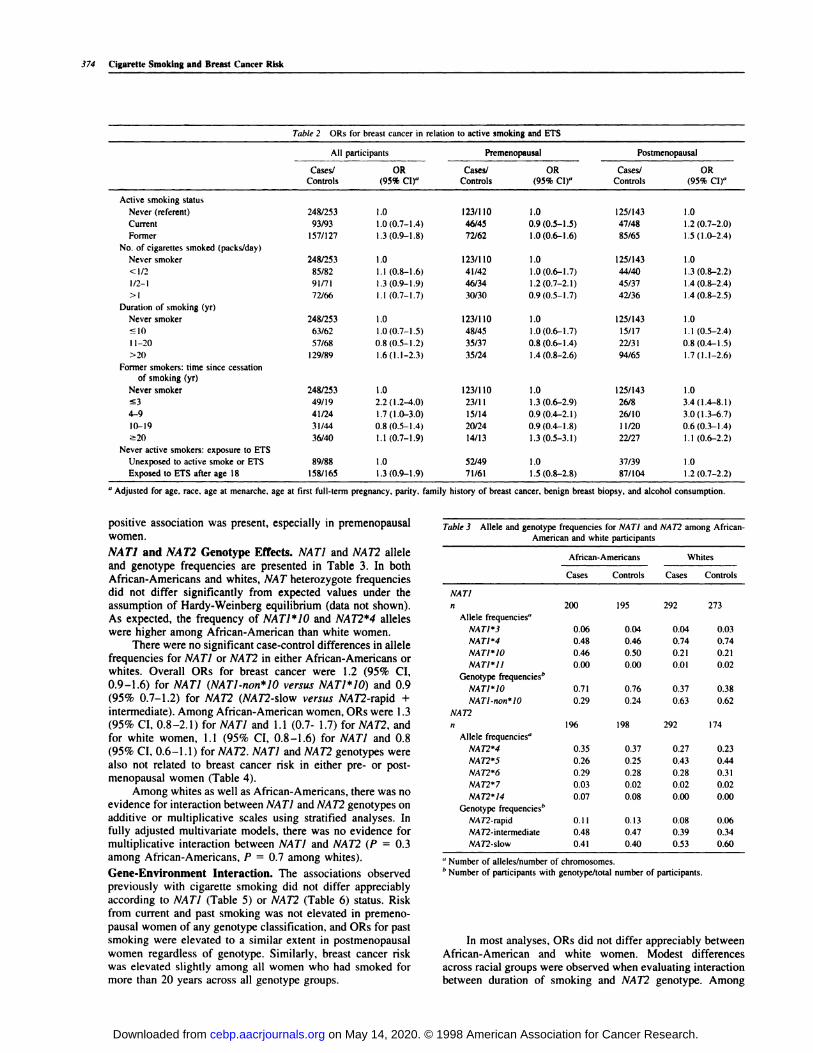
Active Smoking. Current smoking was not associated with
breast cancer risk (Table 2). Among postmenopausal women, apositive association was observed for former smokers corn-
pared with never smokers (OR, 1.5; 95% CI, 1 .0-2.4). Therewas no relationship between number of cigarettes smoked perday and breast cancer risk. However, smoking for 20 years orlonger was associated with a slight increase in risk among both
pre- and postmenopausal women (Table 2). These results wereconsistent across racial groups.
Because risk of breast cancer was elevated among formersmokers, we evaluated the association between risk and time
since quitting smoking. No relationship was observed amongpremenopausal women, but among postmenopausal women,risk appeared to decline with time since last smoked (Table 2).We did not observe marked differences in risk according to age
at initiation of smoking (data not shown).
ETS. ORs for exposure to ETS are presented in Table 2,restricted to women who were never active smokers. A weak
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
374 Cigarette Smoking and Breast Cancer Risk
Table 2 ORs for breast cancer in relation to active smoking and ETS
All participants Premenopausal Postmenopausal
Cases! OR Cases! OR Cases/ ORControls (95% CI)” Controls (95% CI)” Controls (95% CI)”
Active smoking status
Never (referent) 248/253 1.0 123/1 10 1.0 125/143 1.0
Current 93/93 1 .0 (0.7-1 .4) 46/45 0.9 (0.5-1 .5) 47/48 1 .2 (0.7-2.0)
Former 157/127 1.3 (0.9-1.8) 72/62 1.0 (0.6-1.6) 85/65 1.5(1.0-2.4)
No. of cigarettes smoked (packs/day)
Never smoker 2481253 1 .0 123/1 10 1 .0 125/143 1.0
<1/2 85/82 1.1 (0.8-1.6) 41/42 1.0(0.6-1.7) 44/40 1.3 (0.8-2.2)
1/2-I 91/71 1.3 (0.9-1.9) 46/34 1.2 (0.7-2.1) 45/37 1.4(0.8-2.4)
> I 72/66 l.l (0.7-1.7) 30/30 0.9 (0.5-1.7) 42/36 1.4(0.8-2.5)
Duration of smoking (yr)
Never smoker 248/253 1 .0 123/1 10 1 .0 125/143 1.0
10 63/62 1.0 (0.7-1 .5) 48/45 1 .0 (0.6-1 .7) 15/17 1 . I (0.5-2.4)
I 1-20 57/68 0.8 (0.5-1.2) 35/37 0.8 (0.6-1.4) 22/31 0.8 (0.4-1.5)
>20 129/89 1.6(1.1-2.3) 35/24 1.4(0.8-2.6) 94/65 1.7(1.1-2.6)
Former smokers: time since cessation
of smoking (yr)
Never smoker 248/253 1.0 123/1 10 1.0 125/143 1.0
�3 49/19 2.2(1.2-4.0) 23/11 1.3(0.6-2.9) 26/8 3.4(1.4-8.1)
4-9 41/24 1.7(1.0-3.0) 15/14 0.9(0.4-2.1) 26/10 3.0(1.3-6.7)
10-19 31/44 0.8(0.5-1.4) 20/24 0.9(0.4-1.8) 11/20 0.6(0.3-1.4)
�20 36/40 1.1 (0.7-1.9) 14/13 1.3 (0.5-3.1) 22/27 1.1 (0.6-2.2)
Never active smokers: exposure to ETS
Unexposed to active smoke or ETS 89/88 1 .0 52/49 1 .0 37/39 1.0
Exposed to ETS after age 18 158/165 1.3 (0.9-1.9) 71/61 1.5 (0.8-2.8) 87/104 1.2 (0.7-2.2)
a Adjusted for age. race, age at menarche. ag e at first full-term pregnancy, parity, family history of breast cancer, benign breast biopsy, and alcohol consumption.
positive association was present, especially in premenopausalwomen.
NATJ and NAT2 Genotype Effects. NAT! and NAT2 allele
and genotype frequencies are presented in Table 3. In bothAfrican-Americans and whites, NAT heterozygote frequenciesdid not differ significantly from expected values under the
assumption of Hardy-Weinberg equilibrium (data not shown).As expected, the frequency of NATJ*1O and NAT2*4 alleleswere higher among African-American than white women.
There were no significant case-control differences in allelefrequencies for NAT] or NAT2 in either African-Americans orwhites. Overall ORs for breast cancer were 1.2 (95% CI,0.9-1.6) for NAT] (NATI.non*]O versus NAT]*lO) and 0.9(95% 0.7-1.2) for NAT2 (NAT2-slow versus NAT2-rapid +
intermediate). Among African-American women, ORs were I .3(95% CI, 0.8-2.1) for NAT] and 1.1 (0.7- 1.7) for NAT2, andfor white women, 1.1 (95% CI, 0.8-1.6) for NATJ and 0.8
(95% Cl, 0.6-1.1) for NAT2. NAT] and NAT2 genotypes werealso not related to breast cancer risk in either pre- or post-menopausal women (Table 4).
Among whites as well as African-Americans, there was noevidence for interaction between NAT] and NAT2 genotypes onadditive or multiplicative scales using stratified analyses. Infully adjusted multivariate models, there was no evidence formultiplicative interaction between NAT] and NAT2 (P = 0.3among African-Americans, P = 0.7 among whites).
Gene-Environment Interaction. The associations observedpreviously with cigarette smoking did not differ appreciablyaccording to NAT] (Table 5) or NAT2 (Table 6) status. Risk
from current and past smoking was not elevated in premeno-
pausal women of any genotype classification, and ORs for pastsmoking were elevated to a similar extent in postmenopausal
women regardless of genotype. Similarly, breast cancer riskwas elevated slightly among all women who had smoked formore than 20 years across all genotype groups.
Table 3 Allele and genotype frequencies for NATI and NAT2 among African-
American and white participants
African-Americans Whites
Cases Controls Cases Controls
NATI
n 200 195 292 273
Allele frequencies”
NATI”3 0.06 0.04 0.04 0.03
NATI”4 0.48 0.46 0.74 0.74
NATI*10 0.46 0.50 0.21 0.21
NATJ”I1 0.00 0.00 0.01 0.02
Genotype frequenciesb
NATI*10 0.71 0.76 0.37 0.38
NATJ.non”l0 0.29 0.24 0.63 0.62
NAT2
n 196 198 292 174
Allele frequencies”
NAT2*4 0.35 0.37 0.27 0.23
NAT2*5 0.26 0.25 0.43 0.44
NAT2”6 0.29 0.28 0.28 0.31
NAT2*7 0.03 0.02 0.02 0.02
NAT2*14 0.07 0.08 0.00 0.00
Genotype frequencies”
NAT2-rapid 0.1 1 0.13 0.08 0.06
NAT2-intermediate 0.48 0.47 0.39 0.34
NAS2-slow 0.41 0.40 0.53 0.60
a Number of alleles/number of chromosomes.b Number of participants with genotype/total number of participants.
In most analyses, ORs did not differ appreciably between
African-American and white women. Modest differencesacross racial groups were observed when evaluating interactionbetween duration of smoking and NAT2 genotype. Among
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 375
As part of an on-going, population-based, case-control study ofinvasive breast cancer in North Carolina, we investigated the
Table 4ORs for breast cancer in relation to NAT! and NAT2 genotypes
Genotype
Premenopausal Postmenopausal
Cases ControlsOR
(95% CI)”Cases Controls
OR
(95% Cl”
NATI”10
NATI.non*I0
NAT2-rapid
NAT2-slow
n239
114
125
n236
112
124
n2l3
112
101
n216
106
1 10
1.0
1.2(0.8-1.8)
1.0
1.1 (0.7-1.6)
n253
137
116
n=252
139
1 13
n255
138
117
rs=256
122
134
1.0
1.0(0.7-1.5)
1.0
0.7 (0.5-1.0)
a Adjusted for age, race, ag e at menarche. age at first full-term pregnancy , parity, family history of breast cancer. beni gn breast biopsy, and alc ohol consumption.
premenopausal African-American women, ORs for duration of
smoking (:� 10, 1 1-20, and >20 years, compared with never
smokers) were: 0.6 (0.1-2.2), 1.5 (0.5-4.5), and 1.5 (0.4-5.1)for individuals with NAT2-rapid genotype; and 2.6 (0.7-10.2),1.7 (0.3-9.5), and 3.0 (0.6-14.3) for NAT2-slow. Among pre-menopausal white women, ORs were: 0.8 (0.4-2.0), 1.4 (0.7-
3.9), and 2.3 (0.5-9.7) for NAT2-rapid; and 0.8 (0.4-1 .8), 0.5
(0. 1-1 .3) and 1 .2 (0.5-3.0) for NA72-slow. Among postmeno-pausal African-American women, ORs were: 0.8 (0.1-5.4), 0.6(0.2-1.2), and 2.1 (0.9-5.4) for NAT2-rapid; and 0.6 (0.1-2.8),
0.4 (0.1-4.2), and 2.3 (0.8-6.3) for NAT2-slow. Among post-menopausal white women, ORs were: 0.9 (0.2-3.7), 1.6 (0.6-4.5), and 1.8 (0.8-3.5) forNAT2-rapid; and 3.2 (0.7-13.5), 0.5
(0.2-1.7), and 1.7 (0.8-3.5) for NAT2-slow.The effects of time since cessation of smoking varied
slightly according to genotype. Among postmenopausal
women, there was a suggestion of greater risk for smoking inthe recent past among women with NAT]*]O (Table 5) and
NAT2 rapid (Table 6) genotypes. However, there was consid-
erable overlap in CIs, which were wide due to small numbersof women in each genotype-exposure category.
To compare our NAT2 results with those of Ambrosone et
a!. (4), we conducted trend tests for dose and duration ofsmoking (Table 6). Among postmenopausal women withNAT2-slow genotype, there was a suggestion of increasing risk
with increasing number of cigareues smoked per day, but the
test for trend was nonsignificant (P = 0. 1). ORs also wereelevated among postmenopausal women with NAT2-rapid gen-otype. Among premenopausal women, there was a suggestionof stronger effects of dose and duration of smoking among
women with NAT2-rapid genotype (Table 6), but tests for trendwere nonsignificant.
ORs for genotype-smoking interactions did not differ sig-nificantly according to race. Adjustment for additional covari-
ates did not alter point estimates appreciably, but CIs foradjusted estimates were wide due to small sample sizes. Thus,ORs for active smoking are presented after adjustment for age
and race only in Tables 5 and 6.The effects of NAT genotype on exposure to ETS are
presented in Table 5 (NAT]) and Table 6 (NAT2). Point esti-mates differed slightly after controlling for additional covari-
ates; therefore, fully adjusted estimates are presented for ETS.There did not appear to be an influence of NAT genotype,
except among postmenopausal women, where the NAT2-slow
genotype appeared to confer a slightly greater risk than the
NAT2-rapid (Table 6).
Discussion
relationship of cigarette smoking and breast cancer. We did not
observe a dose-response relationship between the number ofcigarettes smoked and breast cancer risk, but we found that long
duration of smoking (20 years or more) was associated with a
modest elevation in risk in pre- as well as postmenopausal
women. These results are compatible with many previous stud-ies, suggesting that heavy smokers or women who smoked forlong periods of time are at slightly increased risk of breast
cancer (1). We observed a modest increase in risk associatedwith past smoking among postmenopausal women (OR, I .5;
95% CI, 1.0-2.4). Associations with past but not current smok-ing have been reported previously (30, 31). As observed in our
study, Baron et a!. (2) found that smoking within the past 3
years was associated with increased breast cancer risk among
postmenopausal women, and risk declined with years since
cessation of smoking.
An important methodological issue in studying the health
effects of smoking is the choice of a proper referent group.
Kuller et a!. (32) and Wells (33) suggest that a “truly non-exposed” referent group be used to examine the effects of active
smoking and cancer. Morabia et a!. (3) found that excludingwomen with exposure to ETS from the referent group resultedin stronger associations between cigarette smoking and breast
cancer. In our study, ORs for active smoking were unchangedor even slightly attenuated after women exposed to ETS were
excluded from the referent group. However, because we did notmeasure exposure to ETS at work or during leisure time, we
could not exclude women with such exposure from the referent
group. Among nonsmokers, there appeared to be a slight in-crease in risk for women who had lived with a smoker after the
age of 18 (OR, 1.3; 95% CI, 0.9-1.9). Morabia et a!. (3)
reported an OR of 2.0 (95% CI, 1 . 1-3.7) comparing nonsmok-
ing women ever married to a spouse who smoked versus
nonsmoking women never married to such a spouse. Prior to
Morabia et a!. (3), only two studies examined risk of breastcancer associated with ETS (34, 35). Both found moderateelevations in risk among nonsmoking women who were mar-
ried to smokers.
One of the primary goals of this study was to determine
whether the effects of smoking were modified by NAT] andNAT2 genotypes. Allele frequencies for NAT] and NAT2 have
not been published previously for a large, multiracial popula-
tion, and we confirm that the NAT]*]O and NAT2*4 alleles are
more common among African-Americans. Neither NAT] norNAT2 genotype was related to breast cancer risk, overall or in
subgroups defined by race and menopausal status. Ambrosoneet a!. (3) and Hunter et a!. (4) also found no association between
NAT2 genotype and breast cancer risk.In our study, the relationship between smoking and breast
cancer risk was not modified strongly by NAT! or NAT2 gen-
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Table 5 Effect of NAT! genotype on ORs for active smoking, ETS. and breast cancer by menopausal status
Premenopausal Postmenopausal
NAT!*!0 NAT!.non* /0 NAT!”!0 NAT! .non”!0
Cases! OR Cases! OR Cases! OR Cases! OR
Controls (95% Cl) Controls (95% CI) Controls (95% CI) Controls (95% CI)
Active smoking status”
Never 60/57 1.0 62/52 1.0 71/82 1.0 53/60 1.0
Current 22/21 1.0 (0.5-2.1) 24/23 0.9 (0.5-1.8) 22/26 1.1 (0.6-2.2) 24/22 1.2 (0.6-2.4)
Former 32/34 1.0(0.5-1.9) 39/26 1.2(0.6-2.3) 43/30 1.8(1.0-3.1) 39/35 1.4(0.8-2.6)
No. of cigarettes smoked (packs/day)”
Never 60/57 1 .0 62/52 1 .0 7 1/82 1 .0 53/60 1.0
<1/2 20/26 0.7(0.3-1.4) 21/14 1.2(0.6-2.6) 25/22 1.4(0.7-2.7) 19/18 1.2(0.6-2.6)
1/2-I 22/15 1.6 (0.8-3.4) 23/19 1.0 (0.5-2.1) 21/18 1.4 (0.7-2.9) 21/19 1.4(0.7-2.9)
>1 11/13 0.9(0.4-2.2) 19/16 1.0(0.5-2.2) 19/16 1.4(0.6-3.0) 23/20 1.4(0.7-2.9)
Trend test P = 0.7 P = 0.9 P 0.2 P 0.3
Duration of smoking (yr)”
Never smoker 60/57 1.0 62/52 1.0 71/82 1.0 53/60 1.0
�I0 20/26 0.7 (0.3-1.4) 27/18 1.2 (0.6-2.5) 7/1 1 0.8 (0.3-2.2) 7/6 1.4(0.4-4.5)
11-20 19/19 1.1 (0.5-2.3) 16/17 0.8(0.4-1.8) 12/12 1.1 (0.5-2.6) 9/19 0.5 (0.2-1.2)
>20 15/9 1.9 (0.8-4.8) 20/14 1.2 (0.6-2.6)
P=0.3 P=0.9
46/33 1.7 (1.0-3.0)
P=0.07
47/32 1.8(1.0-3.3)
P=0.1
Former smokers: time since cessation (yr)”
Never smoker 60/57 1.0 62/52 1.0 71/82 1.0 53/60 1.0
�3 12/7 1.6(0.6-4.5) 1 1/4 2.1 (0.6-7.2) 13/2 9.0(1.9-41.8) 13/6 2.5 (0.9-7.2)
4-9 5/5 0.8 (0.2-3.0) 9/9 0.8 (0.3-2.2) 17/3 7.0 (2.0-25.2) 817 1.5 (0.5-4.5)
10-19 10/13 0.9(0.4-2.3) 10/9 1.0(0.4-2.7) 5/9 0.6(0.2-1.9) 6/lI 0.6(0.2-1.8)
�20 5/9 0.6 (0.2-1.9) 9/4 1.7 (0.5-6.2) 9/16 0.6 (0.2-1.5) 12/1 1 1.7 (0.7-4.3)
Never active smokers: exposure to ETS”
Unexposed to active smoke or ETS 26/24 1.0 26/24 1.0 21/23 1.0 15/16 1.0
Exposed to ETS after age 18 34/33 1.7 (0.7-4.3) 36/28 1.3 (0.5-3.2) 49/59 1.2 (0.6-2.6) 38/44 1.3 (0.5-3.6)
376 Cigarette Smoking and Breast Cancer Risk
a Adjusted for age and race.
/� Adjusted for age, race, age at menarche. age at first full-term pregnancy,
otype, except among subgroups of postmenopausal women.Among postmenopausal women who were former smokers, theeffects of smoking within the past 3 years tended to be stronger
among women with NAT]*iO and NAT2-rapid genotypes. OurNAT2 results differ from Ambrosone et a!. (4), who observed
elevated risk of breast cancer among postmenopausal womenwho smoked and inherited the slow NAT2 genotype. Am-brosone et a!. (4) reported a slightly stronger effect of NAT2
genotype on dose (number of cigarettes smoked) than pack-
years among postmenopausal women. We evaluated dose andduration of smoking separately and did not find differences foreither variable according to NAT2 genotype.
Our results for past smoking are more compatible with theresults of Hunter et a!. (5), who found a slight increase in risk
associated with smoking 10 years prior to diagnosis (as well asprior to first pregnancy) among women with the NAT2 rapidgenotype. Among premenopausal women, we observed thatlonger duration of smoking was associated with slightly greater
risk among women with NATI*]O and NAT2 rapid genotypes,the latter consistent with Ambrosone et a!. (4). However, tests
for trend were nonsignificant in both studies.Several authors suggest that the effects of carcinogen
metabolism genes, such as NAT] and NAT2, are most likely tobe observed at low levels of environmental exposure (36, 37).
We did not observe an effect for NAT genotype at low levels ofactive smoking or for exposure to ETS. However, our infor-mation on ETS exposure was limited to exposure at home.Further study of ETS is warranted (33, 38, 39) and shouldinclude exposure at home, at work, and during leisure time (3,40). However, such exposure history is difficult to obtain (39,40), and large numbers of participants would be needed forreliable estimates of interaction with NAT genotype (41).
parity, family history of breast cancer. benign breast biopsy. and alcohol consumption.
We addressed a number of issues raised by previous stud-ies. Some authors suggest that positive associations betweensmoking and breast cancer might result from high refusal rates(for interviews and/or blood draws) among controls who are
smokers, leading to a false lower prevalence of smoking in
controls ( 1). In our study, the prevalence of smoking in ourcontrols was 20%, similar to a recent survey conducted amongNorth Carolina women (21%).� In addition, NAT] and NAT2
allele and genotype frequencies among controls were similar to
a sample collected previously from persons in North Carolina,5further evidence that our controls are representative of womenin the study area. We explored the impact of using as a referentgroup women unexposed to ETS, as suggested by Morabia et
a!. (3). Finally, we included information on NAT] genotype: theNAT! enzyme exhibits higher activity than NAT2 in the breast(13) and other tissues (16) and may have more relevance forcarcinogenesis.
Our study had sufficient power to detect strong interac-tions between NAT] or NAT2 genotype and smoking. For
example, our study had over 80% power to detect OR ofinteraction of 4.0 or more (41) for NAT2 and past smoking
among postmenopausal women, the magnitude of the OR re-
ported by Ambrosone et a!. (4) for the highest levels of smokingamong NAT2-slow acetylators. Our study had less poweramong white women only, but we did not observe substantialdifferences in smoking or genotype effects across racial groups.
Because most of our observed associations are weak,
4 North Carolina Department of Environment, Health and Natural Resources,
Behavioral Risk Factor Surveillance System. unpublished findings, 1996.
5 D. Bell, unpublished observations.
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 377
Table 6 Effec t of NAT2 genotype on ORs for active smoking, ETS, and br east cancer by menopausal status
.
Smoking status
Premenopausal Postmenopausal
NA72-rapid NA72-slow NAT2-rapid�
NA72-slow�
Cases! ORCases! OR Cases/ OR Cases! ORControls (95% CI) Controls (95% Cl) Controls (95% Cl) Controls (959t� Cl)
Active smoking status”
Never 56/55 1.0 64/55 1.0 71/71 1.0 51/72 1.0
Current 21/20 1.1 (0.5-2.3) 25/25 0.8 (0.4-1.6) 23/20 1.4 (0.7-2.8) 24/28 1.1 (0.6-2.2)
Former 35/31 1.1 (0.6-2.1) 35/30 1.0 (0.5-1.9) 44/31 1.6 (0.9-2.9) 38/34 l.8 (1.0-3.3)
No. of cigarettes smoked (packs/day)”
Never smoker 56/55 1 .0 64/55 1 .0 7 117 1 1 .0 5 1172 I .0
<l!2pack/day 20/24 0.8(0.4-1.6) 21/18 0.9(0.4-1.9) 24/18 1.5(0.7-3.0) 19/22 l.2(0.6-2.5
1/2-1 pack/thy 21/17 1.2(0.6-2.6) 24/17 1.2(0.6-2.5) 24/18 1.5(0.7-3.0) 20/19 1.5 (0.7-3.2)
I pack/day 14/10 1.3(0.5-3.3) 15/19 0.7(0.3-1.5) 19/15 l.4(0.6-3.0 23/21 1.7 (0.8-3.5)
Trend test P = 0.5 P = 0.6 P 0.2 P 0. I
Duration of smoking (yr)”
Never smoker 56/55 1.0 64/55 1.0 71/71 1.0 51172 1.0
�I0 19/23 0.7 (0.3-1.5) 27/22 1.0 (0.5-2.0) 6/8 0.8 (0.3-2.5) 9/9 1.4 (0.7-3.8)
1 1-20 22/17 1.4 (0.7-3.0) 13/19 0.6 (0.3-1.3) 16/16 1.1 (0.5-2.4) 6/15 0.5 (0.2-1.4)
>20 15/10 1.7 (0.7-4.2) 20/14 1.3 (0.6-2.8) 45/27 1.8 (1.0-3.2) 47/38 1.9 (0.7-5.5)
Trend test P = 0.3 P = 0.9 P = 0.06 P = 0.08
Former smokers: time since cessation
(yr)”
Never smoker 56/55 1 .0 64/55 1 .0 7 1/7 1 1 .0 5 1/72 1.0
rt3 14/8 1.5 (0.6-4.0) 7/3 1.9 (0.5-7.9) 13/2 7.4 (1.6-32.6) 12/6 2.8(0.4-8.0)
4-9 5/8 0.5(0.2-1.7) 10/5 1.7(0.5-5.4) 15/4 4.1(1.3-13.1) 11/6 2.7W.9-7.9(
10-19 12/10 1.3 (0.5-3.3) 8/14 0.5 (0.2-1.3) 5/10 0.6 (0.2-1.9) 6/10 0.9 (0.3-2.7)
�20 4/5 0.8(0.3-3.2) 10/8 1.1 (0.4-3.1) 12/15 0.8(0.3-1.9) 9/12 1.4 (0.5-3.7)
Never active smokers: exposure to ETSb
Unexposed to active smoke or ETS 23/25 1 .0 28/24 1 .0 23/1 9 1 .0 12/20 I .0
Exposed to ETS after age 18 33/30 2.3 (0.9-6.2) 36/31 1.2 (0.5-2.8) 47/52 0.8 (0.4-1.8) 39/52 1.9 (0.7-5.2)
a Adjusted for age and race.h Adjusted for age, race, age at menarche, age at first full-term pregnancy, parity, family history of breast cancer, benign breast biopsy. and alcohol consumption.
chance findings or confounding by unmeasured exposures can-not be ruled out. We controlled for breast cancer risk factors
reported previously to be associated with active smoking orexposure to ETS in the National Health and Nutrition Exami-nation Survey (42) and other studies. However, the etiology of
breast cancer is largely unknown (43); therefore, residual con-
founding by unmeasured risk factors must be considered. Thepositive associations observed with past smoking could haveresulted from overreporting of smoking by cases. However, therelationship of smoking and breast cancer is not well estab-
lished, and no relationship was observed between current smok-ing and breast cancer risk. Furthermore, the association withpast smoking was observed to diminish with time since quit-ting. The latter results are compatible with some but not all
previous studies and suggest that there may be some benefitfrom smoking cessation.
Although our results for modification of smoking by gen-
otype were largely negative, current knowledge of the metab-
olism of constituents of tobacco smoke within the breast isincomplete. Enzyme kinetics for NAT activity in breast tissue
have been investigated only recently (13, 44). It is possible thatacetylation enzymes, particularly NAT1, catalyze both activa-
tion and detoxification of tobacco-derived arylamines in thebreast, making differences in risk associated with genotypedifficult to detect. Additional sources of arylamine exposure(e.g., occupational solvents) as well as heterocyclic amines in
cooked meats (13) might be considered in future studies ofNAT and breast cancer. For these studies to proceed, additionalinvestigation of the functional significance of allelic variation at
NAT] and NAT2 is needed ( 18), especially in large multiracial
populations. As suggested by Aragaki et a!. (45), hierarchicalmodeling ofNATgenotype effects may be useful for addressingdata sparseness and incomplete knowledge of the biologicalbasis for gene-environment interaction.
Acknowledgments
We thank Dr. Peter Shields. Dr. David Hunter. and Barbara Parker for helpfulcomments. We also acknowledge the important contributions of the nurse inter-viewers for the Carolina Breast Cancer Study: Carolyn Dunmore. Dianne Mat-
tingly, Theresa Nalevaiko, Patricia Plummer, and Cheryl Robinson.
References
1 . Palmer, J., and Rosenberg, L. Cigarette smoking and breast cancer. Epidemiol.
Rev., !5: 145-162, 1993.
2. Baron. J., Newcomb, P., Longnecker, M., Mittendorf, R., Storer, B.. Clapp. R..
Bogdan, G., and Yuen. J. Cigarette smoking and breast cancer. Cancer Epidemiol.
Biomark. Prey., 5.� 399-405, 1996.
3. Morabia, A., Bernstein, M., Heritier, S., and Khatchatrian, N. Relation of
breast cancer with passive and active exposure to tobacco smoke. Am. J. Epide-
miol., !43: 918-28, 1996.
4. Ambrosone, C., Freudenheim, J., Graham, S., Marshall, J.. Vena. J.. Brasure.
J., Michalck, A., Laughlin, R., Nemoto, T., Gillenwater. K., Hamngton. A.. and
Shields, P. Cigarette smoking. N-acetyltransferase 2 genetic polymorphisms and
breast cancer risk. J. Am. Med. Assoc.. 276: 1494-1501. 1996.
5. Hunter, D., Hankinson, S., Hough, H., Gertig, D., Garcia-Closas, M..
Spiegelman, D., Mattson, J., Coldit.z, G., Willet, W., Spcizer. F.. and Kelsey. K.A prospective study ofNAT2 acetylation genotype. cigarette smoking and risk ofbreast cancer. Carcinogenesis (Land.), !8: 2127-2132, 1997.
6. Hem, D.. Doll, M., Rustan, T., Gray, K., Feng. Y., Ferguson, R.. and Grant,D. Metabolic activation and deactivation of arylamine carcinogens by recombi-nant human NAT1 and polymorphic NAT2 acetyltransferases. Carcinogenesis
(Lond.). /4: 1633-1638, 1993.
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

378 Cigarette Smoking and Breast Cancer Risk
7. Smith, G., Stanley, L., Sim, E., Strange. R., and Wolf, C. Metabolic polymor-
phisms and cancer susceptibility. Cancer Surv., 25: 27-55, 1996.
8. D’Emco, A., Taioli, E., Chen, S., and Vineis, P. Genetic polymorphisms andthe risk of cancer: a review of the literature. Biomarkers, !: 149-173, 1996.
9. Nebert, D. Polymorphisms in drug-metabolism enzymes: what is their clinical
relevance and why do they exist? Am. J. Hum. Genet., 60: 265-271, 1997.
10. Bell, D., Taylor, J., Butler, M., Stephens, E., Wiest, J., Brubaker, L,
Kadlubar. F., and Lucier, G. Genotype/phenotype discordance for human NAfl
reveals a new slow-acetylator allele common in African-Americans. Carcinogen-
esis (Land.), !4: 1689-1692, 1993.
I I . Lin, H. Smokers and breast cancer: ‘chemical individuality” and cancer
predisposition. J. Am. Med. Assoc., 276: 151 1-1512, 1996.
12. Badawi, A., Hirvonen, A., Bell, D., Lang, N., and Kadlubar, N. Role of
aromatic amine acetyltransferases, NAT! and NA72, in carcinogen-DNA adduct
formation in the human urinary bladder. Cancer Res., 55: 5230-5237, 1995.
13. Sadrieh, N., Davis, C., and Snyderwine, E. N-Acetyltransferase expression
and metabolic activation of the food-derived heterocyclic amines in the human
mammary gland. Cancer Res.. 56: 2683-2687, 1996.
14. Vatsis, K.. and Weber, W. Structural heterogeneity of Caucasian N-acetyl-
transferase at the NAT! gene locus. Arch. Biochem. Biophys., 30!: 71-76, 1993.
15. Bell, D., Stephens. E., Castranio, T., Umbach, D., Watson, M., Deakin, M.,
Elder, J., Hendrickse, D., Duncan, H., and Strange, R. Polyadenylation polymor-
phism in the acetyltransferase 1 gene (NAT!) increases risk of colorectal cancer.
Cancer Res., 55: 3537-3542, 1995.
16. Bell, D., Badawi, A., Lang, N., Ilett, K., Kadlubar, F., and Hirvonen, A.Polymorphism in the NAT! polyadenylation signal: association 0fNAT!”!0 allele
with higher N-acetylation activity in bladder and colon tissue samples. Cancer
Res., 55: 5226-5229, 1995.
17. Doll. M., Jiang, W., Deitz, A., Rustan, T., and Hem, D. Identification of a
novel allele at the human NAT! acetyltransferase locus. Biochem. Biophys. Res.
Commun., 233: 584-591, 1997.
18. Grant. D., Hughes, N., Janezic, S., Goodfellow, G., Chen, H., Gaedigk, A.,Yu, V., and Grewal, R. Human acetyltransferase polymorphisms. Mut. Res., 376:
61-70, 1997.
19. Hughes, N., McQueen, K., Janezic, S., Jewett, M., Castranio, T., Bell, D., and
Grant, D. Identification and characterization of variant alleles of human acetyl-
transferase NAT! with defective functions using p-aminosalicylate as an in vivo/invitro probe. Pharmacogenetics, in press, 1998.
20. Deitz, A., Doll, M., and Hem, D. A restriction fragment polymorphism assay
that differentiates nine human N-acetyltransferase I (NAT!) alleles. Anal. Bio-chem., 253: 219-224, 1997.
21. Newman, B., Moorman, P., Millikan, R., Qaqish, B., Geradts, J., Aldrich, T.,and Liu, E. The Carolina Breast Cancer Study: integrating population-based
epidemiology and molecular biology. Breast Cancer Res. Treat., 34: 51-60, 1995.
22. Aldrich, T., Vann, D., Moorman, P., and Newman, B. Rapid reporting of
cancer incidence in a population-based study of breast cancer: one constructive
use of a central cancer registry. Breast Cancer Res. Treat., 35: 61-64, 1995.
23. Weinberg, C., and SandIer, D. Randomized recruitment in case-control
studies. Am. J. Epidemiol., /34: 421-432, 1991.
24. Sambrook, J., Maniatis, T., and Fritsch, F. Molecular Cloning: A Laboratory
Manual, Ed. 2. Cold Spring Harbor, NY: Cold Spring Harbor Laboratory, 1988.
25. Vatsis, K., Weber, W., Bell, D., Dupret, J-M., Evans, D., Grant, D., Hem, D.,Lin, H., Meyer. U.. Relling, M., Sim, E., Suzuki, T., and Yamazoc, Y. Nomen-
clature for N-acetyltransferases. Pharmacogenetics, 5: 1-9, 1995.
26. Breslow, N., and Day, N. Statistical methods in cancer research: the analysis
of case-control studies. Lyon: IARC, 1980.
27. Cavalli-Sforza, L., and Bodmer, W. The Genetics of Human Populations. San
Francisco: W. H. Freeman, 1971.
28. Kleinbaum, D., Kupper, L., and Morgenstern, H. Epidemiologic Research:
Principles and Quantitative Methods. New York: Van Nostrand Reinhold, 1982.
29. Khoury, M., and Beatty, T. Applications of the case-control method in
genetic epidemiology. Epidemiol. Rev., !6: 134-150, 1994.
30. Brownson, R., Blackwell, C., Pearson, D., Reynolds, D, Richens, J., andPapermaster, B. Risk of breast cancer in relation to cigarette smoking. Arch. Int.
Med., !48: 140-144, 1988.
31 . Rohan, T., and Baron, J. Cigarette smoking and breast cancer. Am. J.
Epidemiol., /29: 36-42, 1989.
32. Kuller, L., Garfinkel, L., Correa, P., Haley, N., Hoffman, D., Preston-Martin,
S., and SandIer, D. Contribution of passive smoking to respiratory cancer.Environ. Health Perspect., 70: 57-69, 1986.
33. Wells, A. Breast cancer, cigarette smoking, and passive smoking. Am. J.
Epidemiol., /33: 208-210, 1991.
34. Sandler, D., Everson, R., and Wilcox, A. Cigarette smoking and breast
cancer. Am. J. Epidemiol., !23: 370-371, 1986.
35. Hirayama, T. Cancer mortality in nonsmoking women with smoking hus-
bands based on large-scale cohort study in Japan. Prey. Med., !3: 680-690, 1984.
36. Vineis, P., Bartsch, H., Caporaso, N., Harrington, A., Kadlubar, F., LandI,M., Malaveille, C., Shields, P., Skipper, P., Talaska, G., and Tannenbaum, G.
Genetically based N-acetyltransferase metabolic polymorphism and low-level
environmental exposure to carcinogens. Nature (Lond.), 369: 154-156, 1994.
37. Vineis, P., and Martone, T. Genetic-environmental interaction and low-level
exposure to carcinogens. Epidemiology, 6: 454-457, 1995.
38. Burns, D. Environmental tobacco smoke: the price of scientific certainty.
J. Natl. Cancer Inst., 84: 1387-1388, 1992.
39. Kabat, G., Steelman, S., and Wynder, E. Relation between exposure to
environmental tobacco smoke and lung cancer in lifetime nonsmokers. Am. J.
Epidemiol., /42: 141-148, 1995.
40. Kawachi, I., and Colditz, G. Confounding, measurement error, and publica-
tion bias in studies of passive smoking. Am. J. Epidemiol., !44: 909-915, 1996.
41. Hwang, S-i., Beaty. T., Liang, K-Y., Coresh, J., and Khoury, M. Minimum
sample size estimation to detect gene-environment interaction in case-control
designs. Am. J. Epidemiol., /40: 1029-1037, 1994.
42. Matanoski, G., Kanchanaraksa, S., Lantry, D., and Chang, Y. Characteristics
of non-smoking women in NHANES 1 and NHANES 1 Epidemiologic Follow-up
Study with exposure to spouses who smoke. Am. J. Epidemiol., !42: 149-157,
1995.
43. Kelsey, J., and Horn-Ross, P. Breast cancer epidemiology: summary and
future directions. Epidemiol. Rev., !5: 256-263, 1993.
44. Lee, J., Chung, J., Lal, J., Levy, G., and Weber, W. Kinetics of arylamine
N-acetyltransferase in tissues from human breast cancer. Cancer Lett., !!!:
39-50, 1997.
45. Aragaki, C., Greenland, S., Probst-Hensch, N., and Haile, R. Hierarchicalmodeling of gene-environment interactions: estimating NAT2” genotype-specific
dietary effects on adenomatous polyps. Cancer Epidemiol. Biomark. Prey., 6:
307-314, 1997.
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1998;7:371-378. Cancer Epidemiol Biomarkers Prev R C Millikan, G S Pittman, B Newman, et al. cancer risk.Cigarette smoking, N-acetyltransferases 1 and 2, and breast
Updated version
http://cebp.aacrjournals.org/content/7/5/371
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/7/5/371To request permission to re-use all or part of this article, use this link
on May 14, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from