cinacalcet treatment in advanced ckd - is it justified? · goce spasovski erbp advisory board ......
TRANSCRIPT

October 21, 2017, Antalya
Cinacalcet treatment in
advanced CKD - is it justified?
Goce Spasovski
ERBP Advisory Board member
University of Skopje, R. Macedonia
TSN Congress

Session Objectives
From ROD to CKD-MBD in CKD patients
General issues
Guidelines
Controversies conference (updates)
Bone quality / Clinical outcome data
Cinacalcet treatment – new evidence
Efficacy - cost related evidence
When to treat – rationale
Monitoring frequency
Summary
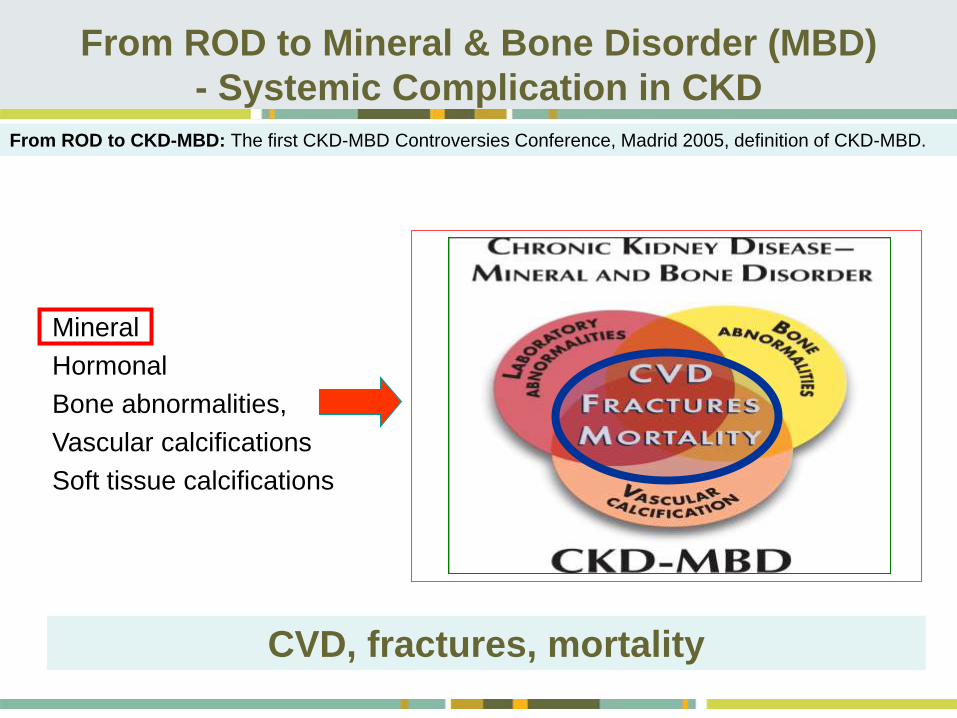
From ROD to Mineral & Bone Disorder (MBD)
- Systemic Complication in CKD
• Mineral
• Hormonal
• Bone abnormalities,
• Vascular calcifications
• Soft tissue calcifications
CVD, fractures, mortality
From ROD to CKD-MBD: The first CKD-MBD Controversies Conference, Madrid 2005, definition of CKD-MBD.

Bone, P & Ca Management guidelines
K-DOQI Guidelines
GB Renal Association Guidelines
EDTA Guidelines
KDIGO Guidelines

Publishing the CKD-MBD Guideline
The first KDIGO clinical
practice guideline on
CKD-MBD was published
in August 2009.

After the publication…

The term traditionally used to describe the abnormalities in
bone morphology that develop in patients with CKD1
Bone abnormalities are common complications of CKD and
are found in almost all patients with stage 5 CKD
(glomerular filtration rate below 15 mL/1.73 m2/min)2
Evaluation and definitive diagnosis of renal osteodystrophy
requires a bone biopsy1
Histomorphometry is not essential for clinical diagnosis, but
should be performed in research studies1
1Moe S, et al. KI, 2006;69:1945-53; 2Malluche HH, et al. JBMR. 2011;26:1368-76; 3 KDIGO CKD-MBD WG. KI. 2009; 76 (Suppl 113):S1-130.
Renal osteodystrophy
2009 KDIGO® Definition of Renal Osteodystrophy3
• Renal osteodystrophy is an alteration of bone morphology in patients
with CKD
• It is one measure of the skeletal component of the systemic disorder of
CKD-MBD that is quantifiable by histomorphometry of bone biopsy

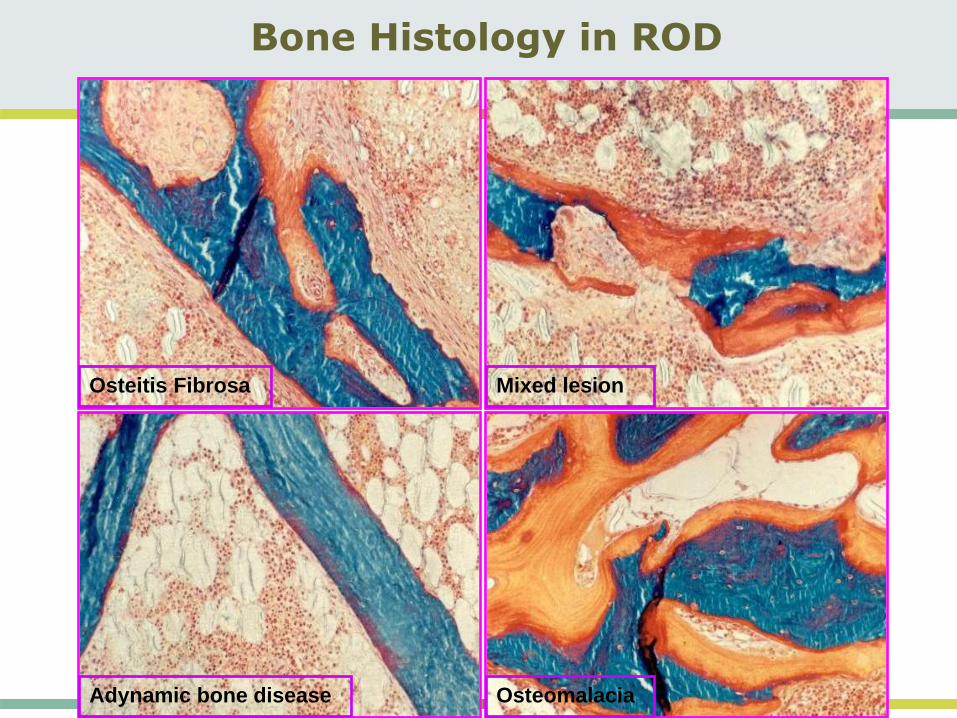
Bone Histology in ROD
Mixed lesion
Osteomalacia
Osteitis Fibrosa
Adynamic bone disease

Pi
PTH Secretion
Parathyroid Cell Growth
Increased CaxP & risk of
metastatic calcifications
Morbidity &
Mortality
Ca++
PTH resistance
Calcitriol
Calcitriol resistance
Consequences of Elevated Serum
Phosphorus
Treatment ABDHPTH
Spasovski G et al. Semin Dial 2009; 22(4): 357-362

GB Spasovski et al. Nephrol Dial Transpl 2003; 18: 1159-66
Normal bone38%
Mixed lesion18%
Hyperpara9%
Adynamic bone23%
Osteomalacia12%
• Prospective,• Non-randomized,
Macedonian Population• N = 84 patients• Histomorphometric criteria
according to:Salusky et al., Kidney Int.,33,1988 Parfitt et al., Calcif Tissue Int 42, 1988
N = 84
Ch
ang
ing
sp
ectr
um
of
rena
l o
ste
od
ystr
op
hy
Spectrum of Renal Bone Disease in patients with
end-stage renal bone disease not yet in dialysis

Down regulation of
PTH receptor
Insufficient PTH levels
Osteoblastic dysfunction
Uremic toxins
Decreased BFR
Relative
hypopara-
thyroidism
Al + Fe Vit.D
cinacalcet
VDR poly-
morphism
Better Pi
control
Diabetes
Older age
Malnour-
ishment
Ca receptor
expression
Extracellular Ca++
Ca load: Ca based binders
HD & CAPD dialysis fluid Ca conc.
Diabetes
Older age
Male gender
Growth factors
Al + Fe
Vit.D treatment
VDR expression
Mg++
Physiopathology of Adynamic Bone

Association in CKD patients between:MBD (abnormal mineral metabolism & bone health)
&
Fractures – decreased quality of life
VC – most important cause of morbidity
CVD – significant mortality
Clinical Relevance and Consequences
Bone health and vascular calcification relationship in chronic kidney disease
Spasovski G. Int Urol Nephrol 2007;39:1209–1216

CKD - MBD: Bone lose & fracture
United States Renal Data System data (300,000 patients)
- The relative risk for hip fracture in dialysed patients is 4.4
times (men and women) that of age-matched controls.Alem A et al. Kidney Int 2000, 58: 396-9

Disordered bone remodelling can induce
vascular calcification
High bone turnover
Low bone turnover
Phosphate
Calcium
Precipitation
in vessels and
soft tissues
Calcification
London et al. J Am Soc Nephrol 2004;15:1943–1951; Spasovski G. Int Urol Nephrol 2007;39:1209–1216
High bone turnover leads to release of Ca + P from bone. Low bone turnover hinders
their emplacement in bone. Result is cardiovascular and soft tissue calcification.
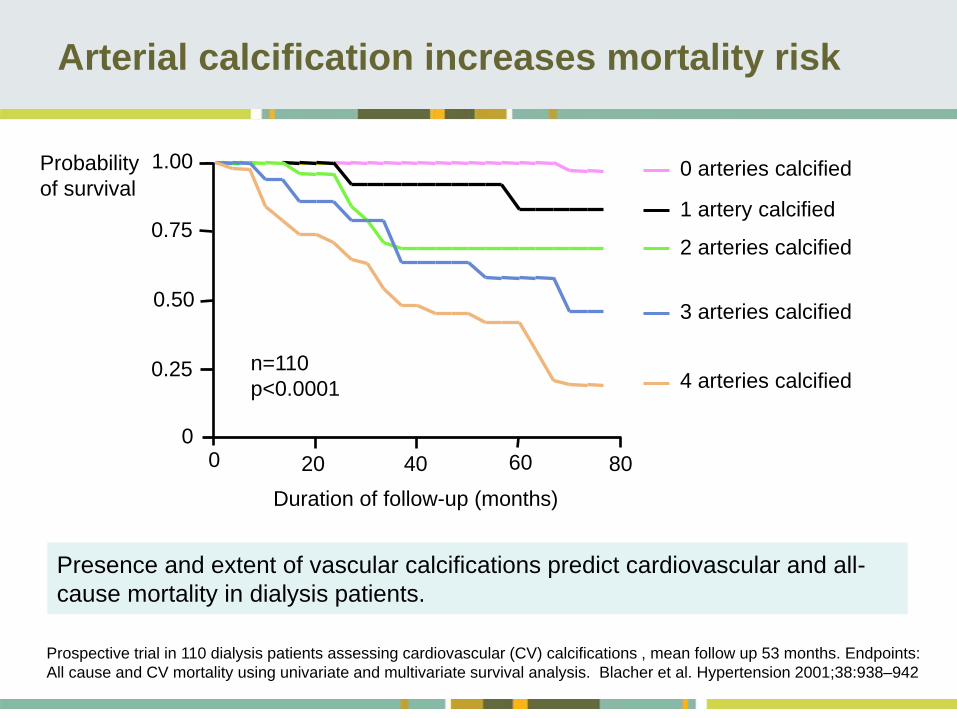
Arterial calcification increases mortality risk
0 arteries calcified
1 artery calcified
2 arteries calcified
3 arteries calcified
4 arteries calcified
Prospective trial in 110 dialysis patients assessing cardiovascular (CV) calcifications , mean follow up 53 months. Endpoints:
All cause and CV mortality using univariate and multivariate survival analysis. Blacher et al. Hypertension 2001;38:938–942
Presence and extent of vascular calcifications predict cardiovascular and all-
cause mortality in dialysis patients.
Probability
of survival
n=110
p<0.0001
1.00
Duration of follow-up (months)
0
0.25
0.50
0.75
0 20 40 60 80

PREVENTION OF
COMPLICATIONS OF THERAPY
. . .
OF HYPERPHOSPHATEMIA
&
MBD & ROD & VC
IN CKD PATIENTS
THERAPEUTIC APPROACH
PREVENTION OF
COMPLICATIONS OF THERAPY

• INDIVIDUALIZED COMBINATION
• Dose of Ca carbonate/acetate ”As much as needed” (AMAN)
• Non Ca-based P binders in pts at risk for VC & CVD
• Vitamin D (AMAN)
• Use Low Calcium dialysate - always
• Use aluminum (small amount, shortly)
• Vit. D analogs – upon indication
• Calcimimetics – upon indication
New Strategies in Treatment of MBD and AssociatedCardiovascular Disease in Patients with CKD - HPTH
Spasovski G, Recent Patents on Cardiovascular Drug Discovery, 2008; 3(3):222-8

Thadhani et al, JAMA 2012; 15;307(7):674-84
• At 48 weeks, the change in left ventricular mass index did not differ
between treatment groups.
• Doppler measures of diastolic function also did not differ.
• Episodes of hypercalcemia were more frequent in the paricalcitol
group compared with the placebo group.
Vitamin D therapy and cardiac structure and
function in patients with CKD: the PRIMO RCT

Effect of Cinacalcet on CVD in Pts Undergoing D
The EVOLVE Trial Investigators*
COST-EFFECTIVENESS OF THE TREATMENT WITH CINACALCET
AND VITAMIN D ANALOGS?
N Engl J Med. 2012; 367(26): 2482-94

The treatment of CKD-MBD - improvement in biochemical
parameters of the disease, hard clinical end points or
surrogate end points studies are limited.
PRIMO & EVOLVE study – negative end points (change in
left ventricular mass index and death, myocardial
infarction, unstable angina, heart failure or peripheral
vascular disease)
The results of these two randomized controlled trials with
negative primary end points require physicians to
individualize therapies for the treatment of secondary
hyperparathyroidism.
Moe & Thadhiani, 2012
Treatment of CKD-MBD after PRIMO & EVOLVE
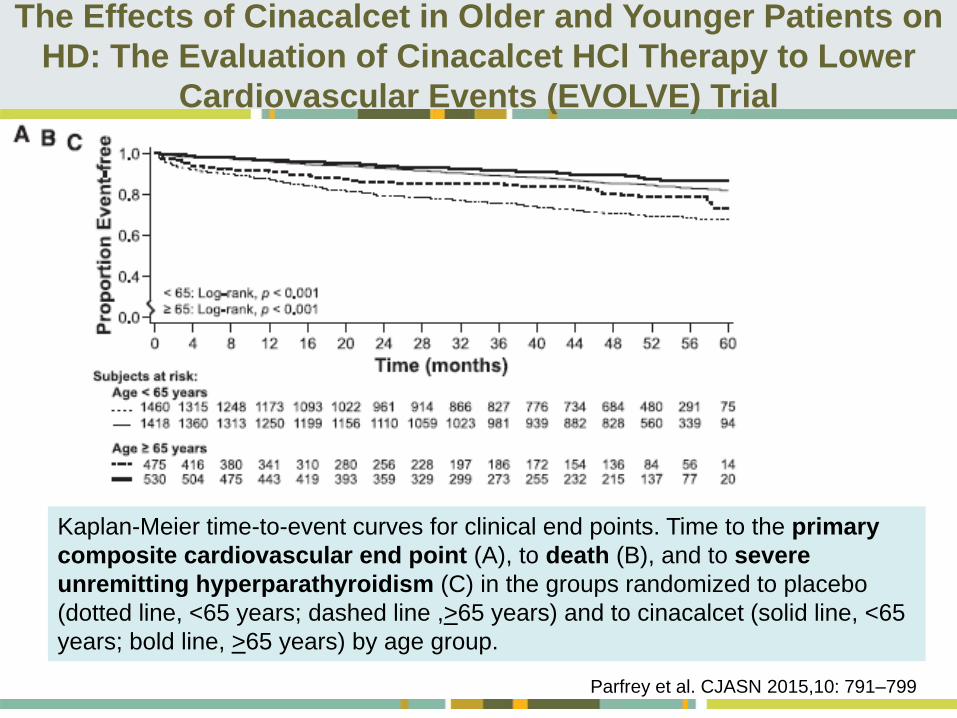
Kaplan-Meier time-to-event curves for clinical end points. Time to the primary
composite cardiovascular end point (A), to death (B), and to severe
unremitting hyperparathyroidism (C) in the groups randomized to placebo
(dotted line, <65 years; dashed line ,>65 years) and to cinacalcet (solid line, <65
years; bold line, >65 years) by age group.
The Effects of Cinacalcet in Older and Younger Patients on
HD: The Evaluation of Cinacalcet HCl Therapy to Lower
Cardiovascular Events (EVOLVE) Trial
Parfrey et al. CJASN 2015,10: 791–799

Relative hazard (HR) of achieving a ≥30% reduction in FGF23 from baseline to
week 20 vs not achieving such a reduction on clinical outcomes (patients
randomized to cinacalcet from FGF23 cohort).
Cinacalcet, FGF-23, and CVD in HD (EVOLVE) Trial
Reduction in FGF23 Is Associated With Reduced
CVD Mortality and Morbidity
Moe et al, Circululation 2015; 132:27-39

Relative hazard (HR) of achieving a ≥50% reduction in FGF23 from baseline to
week 20 vs not achieving such a reduction on clinical outcomes (patients
randomized to cinacalcet from FGF23 cohort).
Cinacalcet, FGF-23, and CVD in HD (EVOLVE) Trial
Reduction in FGF23 Is Associated With Reduced
CVD Mortality and Morbidity
Moe et al, Circululation 2015; 132:27-39


• The ADVANCE and EVOLVE trial comparing cinacalcet vs
standard treatment on sHPTH failed to demonstrate a
significant effect on the primary end points but showed
positive signals concerning some predefined secondary
end points.
Ketteler et al. KI 2015 Mar;87(3):502-28

Should patients with CKD stage 5D & biochemical
evidence of sHPTH be prescribed calcimimetic therapy?
An ERA-EDTA position statement
What do the guidelines say?
No guidelines on this subject (KDOQI, CARI, RA, NICE) have
been produced on this topics since the release of the EVOLVE
results.
Recommendations ERBP
1. We do not recommend routine use of calcimimetic therapy to
improve survival in patients with CKD stage 5D and
biochemical evidence of secondary hyperparathyroidism (1A).
2. There is insufficient evidence whether parathyroidectomy or
medical intervention with cinacalcet or standard care or a
combination thereof should be preferred to control secondary
hyperparathyroidism in patients with CKD stage 5D.
Goldsmith et al. NDT; 2015; 30: 698–700

Topic #3: Bone Quality
3.2.1 In patients with CKD stages 3–5D, it is reasonable
to perform a bone biopsy in various settings including,
but not limited to: unexplained fractures, persistent
bone pain, unexplained hypercalcemia, unexplained
hypophosphatemia, possible aluminum toxicity, and
prior to therapy with bisphosphonates in patients with
CKD–MBD (not graded)
Argument:
Secondary analyses in osteoporosis trials
New therapies – denosumab and teriparatide
Revision Yes No

Bone histomorphometry before and after long-term
treatment with cinacalcet in dialysis patients with sHPT
• Cinacalcet is indicated for lowering parathyroid hormone
(PTH) in dialysis patients with sHPT, but its effects on bone
remain unclear.
• The effect of cinacalcet on renal bone disease among
patients undergoing dialysis has yet to be characterized
adequately
• The multicenter, single-arm BONAFIDE study characterized
the skeletal response to cinacalcet in adult dialysis patients
with plasma PTH ≥300 pg/mL, serum calcium ≥8.4 mg/dL
(2.1 mmol/L), bone-specific alkaline phosphatase (BALP)
>20.9 ng/mL and biopsy-proven high-turnover bone disease.
Behets, Spasovski et al. Kidney International; 2015;87(4):846-56

Study design and treatment schema
146 adult dialysis patients with plasma PTH (PTH) ≥300 pg/mL, serum
calcium ≥8.4 mg/dL, and bone-specific alkaline phosphatase (BALP)
>20.9 ng/mL underwent bone biopsy during screening.
Behets, Spasovski et al. Kidney International; 2015;87(4):846-56

Comparison of PTH level at baseline and
end of study (median-IQR-range)
The median (interquartile
range; IQR) PTH at
baseline was 985 (674,
1621) pg/mL, and values
decreased nominally to 480
(268, 798) pg/mL, or by a
median (IQR) percent
change of -48.3% (-68.8%, -
26.5%), after treatment with
cinacalcet, p<0.001
BFR – same pattern!
Behets, Spasovski et al. Kidney International; 2015;87(4):846-56
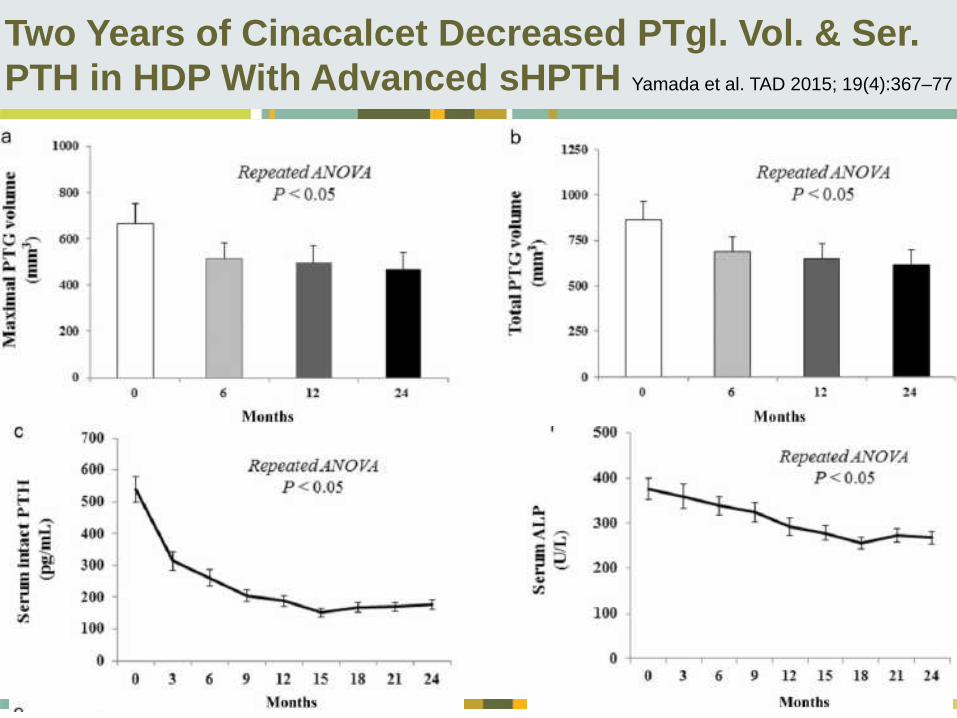
Two Years of Cinacalcet Decreased PTgl. Vol. & Ser.
PTH in HDP With Advanced sHPTH Yamada et al. TAD 2015; 19(4):367–77

Diameter of PT gl Measured by CT as an Indicator
for Response to Cinacalcet in HDP with SHPTH
Hong et al. Kidney Blood Press Res 2015;40:277-287
Measurement of parathyroid gland (PTG) volume and diameter on high-resolution US and PTG
diameter on CT before cinacalcet therapy. Study 1 - cutoff values of imaging parameters; study
2, we reevaluated the clinical and radiologic risk factors for response of cinacalcet treatment.
A, B: Parathyroid gland volume and diameter measured by US. The PTG was diffusely
hypoechoic and hypervascularized on color Doppler US.
C: Measurement of parathyroid gland diameter by CT.

Hong et al. Kidney Blood Press Res 2015;40:277-287
Comparison of clinical and biochemical parameters between responders and non-
responders to cinacalcet treatment in a single center (1)
Diameter of PT gl Measured by CT as an Indicator
for Response to Cinacalcet in HDP with SHPTH

Hong et al. Kidney Blood Press Res 2015;40:277-287
Clinical factors influencing the response to cinacalcet treatment in SHPT in a multicenter study (2)
Diameter of PT gl Meas. by CT - Indicator for Response to Cinacalcet in SHPTH
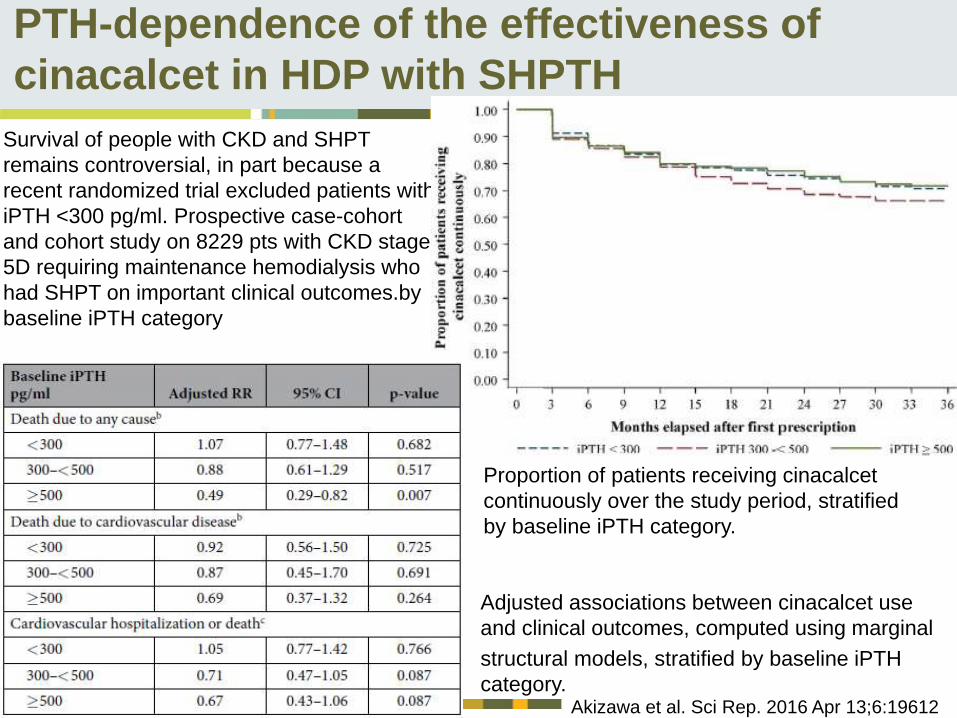
PTH-dependence of the effectiveness of
cinacalcet in HDP with SHPTH
Akizawa et al. Sci Rep. 2016 Apr 13;6:19612
Survival of people with CKD and SHPT
remains controversial, in part because a
recent randomized trial excluded patients with
iPTH <300 pg/ml. Prospective case-cohort
and cohort study on 8229 pts with CKD stage
5D requiring maintenance hemodialysis who
had SHPT on important clinical outcomes.by
baseline iPTH category
Adjusted associations between cinacalcet use
and clinical outcomes, computed using marginal
structural models, stratified by baseline iPTH
category.
Proportion of patients receiving cinacalcet
continuously over the study period, stratified
by baseline iPTH category.

PTH-dependence of the effectiveness of
cinacalcet in HDP with SHPTH
Akizawa et al. Sci Rep. 2016 Apr 13;6:19612
Survival of people with CKD and SHPT
remains controversial, in part because a
recent randomized trial excluded patients with
iPTH <300 pg/ml. Prospective case-cohort
and cohort study on 8229 pts with CKD stage
5D requiring maintenance hemodialysis who
had SHPT on important clinical outcomes.by
baseline iPTH category
Adjusted associations between cinacalcet use
and clinical outcomes, computed using marginal
structural models, stratified by baseline iPTH
category.
When analyses were restricted to patients
with iPTH levels ≥ 300 pg/ml (an inclusion
criterion of the EVOLVE study), cinacalcet
initiation was associated with a lower
incidence of cardiovascular hospitalization
or death due to any cause (adjusted RR
0.71, 95% CI 0.53–0.94).

Etelcalcetide vs Cinacalcet on PTH in HDP
With sHPTH A Randomized Clinical Trial
Etelcalcetide IV & oral
placebo (n = 340) or oral
cinacalcet and IV placebo
(n = 343) for 26 weeks.
The IV study drug was
administered 3 times
weekly with hemodialysis;
the oral study drug was
administered daily.
Among patients receiving
HD with moderate to
severe sHPTH, the use of
etelcalcetide was not
inferior to cinacalcet
in reducing serum PTH
concentrations over 26
weeks.
Block et al. JAMA. 2017;317(2):156-164
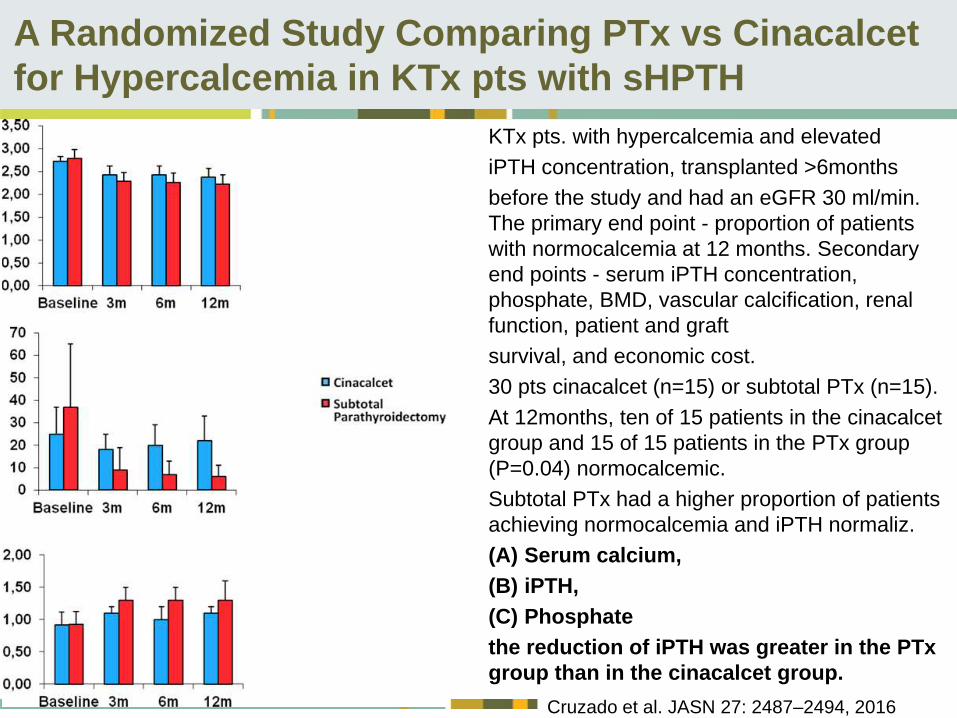
A Randomized Study Comparing PTx vs Cinacalcet
for Hypercalcemia in KTx pts with sHPTH
Cruzado et al. JASN 27: 2487–2494, 2016
KTx pts. with hypercalcemia and elevated
iPTH concentration, transplanted >6months
before the study and had an eGFR 30 ml/min.
The primary end point - proportion of patients
with normocalcemia at 12 months. Secondary
end points - serum iPTH concentration,
phosphate, BMD, vascular calcification, renal
function, patient and graft
survival, and economic cost.
30 pts cinacalcet (n=15) or subtotal PTx (n=15).
At 12months, ten of 15 patients in the cinacalcet
group and 15 of 15 patients in the PTx group
(P=0.04) normocalcemic.
Subtotal PTx had a higher proportion of patients
achieving normocalcemia and iPTH normaliz.
(A) Serum calcium,
(B) iPTH,
(C) Phosphate
the reduction of iPTH was greater in the PTx
group than in the cinacalcet group.

Frequency of monitoring CKD-MBD in sHPTH pts:
assoc. with achievements and adjusted therapy
Japanese multicenter cohort study on 3276 HDP with sHPTH.
Yokoyama et al. NDT 2017: Epub ahead of print
Conclusion: increasing frequency of measurements is helpful when serum marker levels exceed
the target range, partially via adjustment in the therapeutic regimen.
No evidence that frequent measurements helps if mineral levels are already within target ranges.
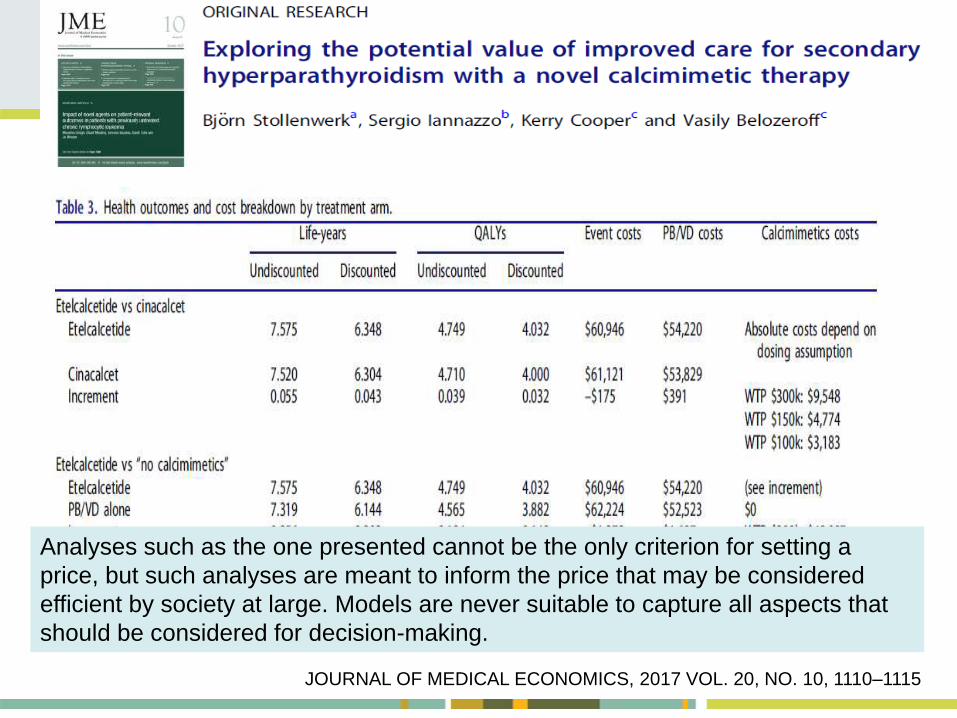
JOURNAL OF MEDICAL ECONOMICS, 2017 VOL. 20, NO. 10, 1110–1115
Analyses such as the one presented cannot be the only criterion for setting a
price, but such analyses are meant to inform the price that may be considered
efficient by society at large. Models are never suitable to capture all aspects that
should be considered for decision-making.

Kidney Int. 2017 Jul;92(1):26-36

Summary - Research Recommandations -
sHPTH
Parathyroidectomy remains a valid treatment option
especially in cases when PTH lowering therapies fail,
Recom. 4.2.5 from 2009 KDIGO-CKD-MBD guideline
Placebo controlled trials with calcimimetics versus
standard therapy for the treatment of SHPT in patients
with CKD stage 5D with emphasis on those at greatest
risk (e.g. older, CVD)
Prospective pts-centered RCTs with the new parenteral
calcimimetics (etelcalcitide) surrogate outcomes (primary
endpoints: mortality, cardiovascular events; secondary
endpoints: FGF23, LVH progression, calcification)
RCTs evaluating Calcimimetic vs vitamin D therapies on
the specific reduction of FGF23 as a therapeutic endpoint
Increasing freq. of CKD-MBD parameters measurements
Even the best treatment option are not perfect
“Do no harm and prevent complications”