circulation through special regions 1
TRANSCRIPT

Circulation through special regions
Prof. Vajira Weerasinghe
Professor of Physiology

Objectives Explain the special features of the following regional
circulations with respect to their functions; A. Coronary
B. Cutaneous
C. Cerebral
D. Skeletal muscle
E. Splanchnic (including liver)
F. Renal

Coronary circulation Heart receives blood supply from two coronary
arteries Left coronary artery
Left anterior descending branch Circumflex branch
Right coronary artery
Dominance Right in 50% Left in 20% Equal in 30%

Basic facts High resting blood flow of 84 ml/100g/min
(4.7% of cardiac output) At maximal cardiac work: 300-400 ml/100g/min
High capillary density (3000-5000 mm2, about one capillary per myocyte)
Large surface area Short diffusion distances (9μm)


Coronary flow

Coronary blood flow Flow in the subendocardial vessels of the left ventricle occurs
only during diastole Because diastole is shorter when the heart rate is high, left
ventricular coronary flow is reduced during tachycardia Subendocardial portion of the left ventricle is more prone to
ischemic damage and is the most common site of myocardial infarction
Blood flow to the left ventricle is decreased in patients with stenotic aortic valves
Therefore patients with aortic stenosis are more prone to develop myocardial ischaemia
Increased venous pressure in congestive heart failure reduces coronary flow because it decreases effective coronary perfusion pressure

Myocardial blood flow is characterized by almost complete oxygen extraction (70-80%) from the blood across the coronary capillaries
Therefore, blood flow must increase to increase oxygen delivery to the heart
Myocardial oxygen delivery is FLOW LIMITED Aortic pressure provides driving force for
coronary blood flow

Regulation of blood flow Metabolic (Functional) Hyperemia
Reactive Hyperemia
Autoregulation

Metabolic (Functional) Hyperemia Primary determinant of coronary blood flow is
myocardial oxygen consumption which is dependent on metabolic activity
Myocardial oxygen consumption is influenced by Cardiac pressure development Wall tension Heart rate Cardiac output Inotropic state Afterload Preload


The exact means by which increased oxygen consumption causes coronary circulation not known
Possible mechanism Hypoxia -> vasodilator substances to be released from cardiac muscle
cells Adenosine is the main vasodilator substance Adenosine produced in myocytes from the metabolism of ATP Stimulates nitric oxide release from endothelium Nitric oxide is a potent vasodilator
Other factors K+, H+, CO2, bradykinin, prostaglandins, lactate

Reactive hyperaemia Brief occlusion of coronary vessel is followed
by a transient increase in coronary blood flow Occlusion results in the accumulation of
vasodilator metabolites in the interstitium Magnitude and duration of extra flow dependent
on the duration of the occlusion

Reactive hyperaemia

Autoregulation Blood flow is relatively constant at perfusion
pressures from 60 mmHg to 150 mmHg Metabolic and myogenic mechanisms involved Curve resets upward at elevated O2 such as
during exercise Autoregulatory capacity is important in
maintaining coronary flow when vessels are partially obstructed

Autoregulation

Neural factors Heart contain sympathetic
b1 receptors which cause positive inotropic and positive chronotropic effects
a1 receptors (direct effect is to cause vasoconstriction)
However the net effect of sympathetic stimulation of the heart is to increase coronary blood flow due to increase in the production of metabolic vasodilators with increased oxygen consumption

Parasympathetic cholinergic fibers direct effect is to vasodilate coronary resistance
vessels via endothelial release of nitric oxide net effect of parasympathetic stimulation of the
heart may actually be reduced coronary blood flow resulting from decreased heart rate and oxygen consumption

When the systemic BP falls The overall effect of increase in noradrenergic
discharge is increased coronary blood flow due to metabolic changes
Increased noradrenergic discharge will cause vasoconstriction of cutaneous, renal and splanchnic vessels
This may protect the heart

CAD (Coronary artery disease) Coronary artery disease (CAD) (or
atherosclerotic heart disease) is the end result of the accumulation of atheromatous plaques within the walls of the coronary arteries that supply the myocardium
Is the leading cause of death worldwide

CAD (Coronary artery disease) CAD causes
Angina pectoris, commonly known as angina is severe chest pain due to ischemia (a lack of blood and hence oxygen supply) of the heart muscle, generally due to obstruction of the coronary arteries
Myocardial infarction (MI) commonly known as a heart attack is the interruption of blood supply to part of the heart causing some heart cells to die

Coronary angiography

Cutaneous circulation Primary role is regulation of internal
temperature It protect against the environment it is also involved in blood pressure control
Average: 12.8 ml/100g/min (8.6% cardiac output)
Range from 1 to 150 ml/100g/min due to shunting blood through anastomosis

Arterioles Located in non-acral skin - limbs, trunk, scalp High density of alpha-1 adrenergic receptors Sympathetic nervous system vasoconstrictor innervation - little
activity at normal core temperature Sympathetic nervous system cholinergic (vasodilator)
innervation is prominent to sweat glands Bradykinin mediates “active” vasodilatation Arterioles exhibit
autoregulation reactive hyperemia basal tone (myogenic)

Arteriovenous anastomosis Coiled, thick-walled vessels Direct connections between dermal arterioles and veins Provide low resistance shunt pathways to feed dermal venous plexus Little basal tone (myogenic) Little metabolic control - no autoregulation or reactive hyperemia Sympathetic nervous system vasoconstrictor innervation has almost
exclusive control Tonic activity Located in “acral skin”: areas of high surface area/volume - fingers, toes,
palms, soles, lips, nose, ears Passive vasodilatation due to reduced sympathetic nervous system activity


Venous plexus Contains greatest cutaneous blood volume - Acts as a reservoir Important for heat transfer Sympathetic nervous system vasoconstrictor
innervation

Control of blood flow Sympathetic Nervous System
to conserve heat SNS activity increases causing vasoconstriction and reducing heat transfer to the environment
to lose heat SNS activity is reduced causing vasodilatation and enhanced heat transfer to the environment

Local warming will produce local vasodilatation and sweating
Local cooling will produce local vasoconstriction due to increased affinity of alpha2-adrenergic receptors for norepinephrine
Intensity controlled by central brain temperature centers
Cutting spinal cord results in extremely poor temperature regulation

Effects of local heating and cooling

Cold causes cutaneous vasoconstriction But severe cold causes vasodilatation
Cold-Induced vasodilatation When temperature falls, smooth muscle becomes
paralyzed and vasodilatation occurs Physical compression (e.g. sitting)
ischemia accumulation of metabolites stimulates nociceptors casing pain shift weight reactive hyperemia

Hormones epinephrine constriction angiotensin II constriction vasopressin constriction
Role in Blood Pressure Control Hypotension increased sympathetic nervous system activity AVA, arteriolar and venous constriction TPR and mobilization of blood to support venous pressure
During exercise enhanced blood flow to the cutaneous circulation is necessary for
dissipating heat reduces venous return to the heart arterial pressure falls

White reaction When a pointed object is drawn across the skin Stroke lines becomes pale Called white reaction
Due to mechanical stimulus initiating contraction of the precapillary sphincters and blood drains out of the capillaries and small veins
Response appears in about 15 s

Triple response When the skin is stroked more strongly triple
response occurs
1. Red reaction (within about 10 s) Capillary dilatation (direct effect)
2. Wheal (swelling) Increased capillary permeability of the capillaries
3. Flare (redness spreading out from injury) Arteriolar dilatation (due to axon reflex)
Persists after sympathectomy Neurotransmitters: substance P, CGRP
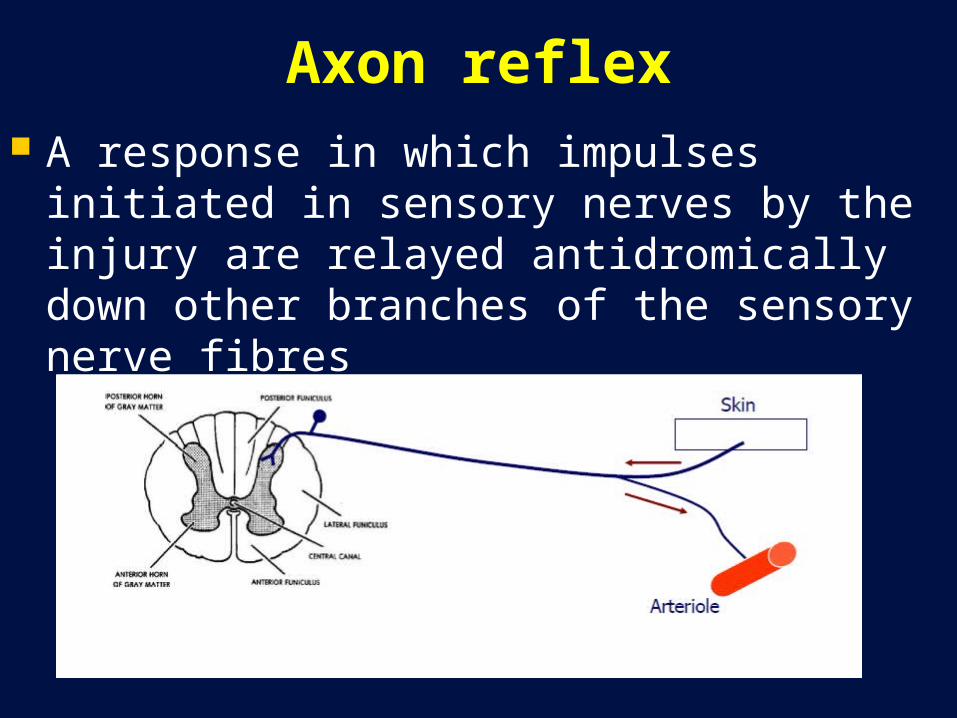
Axon reflex A response in which impulses initiated in
sensory nerves by the injury are relayed antidromically down other branches of the sensory nerve fibres

Reactive hyperaemia Brief occlusion of blood flow is followed by a
transient increase in flow When the blood supply to a limb is occluded,
the cutaneous arterioles below the occlusion dilate. When the circulation is reestablished, blood flowing into the dilated vessels makes the skin become fiery red
Arteriolar dilation is probably due to a local effect of hypoxia
Noradrenergic nerve stimulation and circulating epinephrine and norepinephrine constrict cutaneous blood vessels
No known vasodilator nerve fibers extend to the cutaneous vessels, and thus vasodilatation is brought about by a decrease in constrictor tone as well as the local production of vasodilator metabolites