ckd-mbd for dallas dietitians 2 24-15
TRANSCRIPT

CKD-MBD
05/2015 Dallas Area Dietitians
Jorge Roman-Latorre MDDNA

Following reflects only my personal opinion today
It does not represents DNA or Fresenius
Considers current guidelines
Does not necessarily follow any one protocol
Complex subject : changing fast
We do not have all answers!!!
CKD Ca PO4 PTH
1937 Donahue : CKD Rats had increased Calcium in kidney tissue, proportional to parathyroid weight. Parathyroidectomy prevented Ca deposition in Kidneys
1978 Ibels : Rats subtotal Nephrectomy on either low Phosphorus diet or regular chow + Al(OH)3 : Less uremia , Normal K ; controls had interstitial nephritis, not controlled for protein intake
Man made disease
not noticeable without dialysis
2011 > 2.2M dialysis + .6 M grafted
Rare before chronic dialysis ( 1960 Seattle )
Focus has changed last 35-40 years
From Renal Rickets to a silent common disorder often fatal
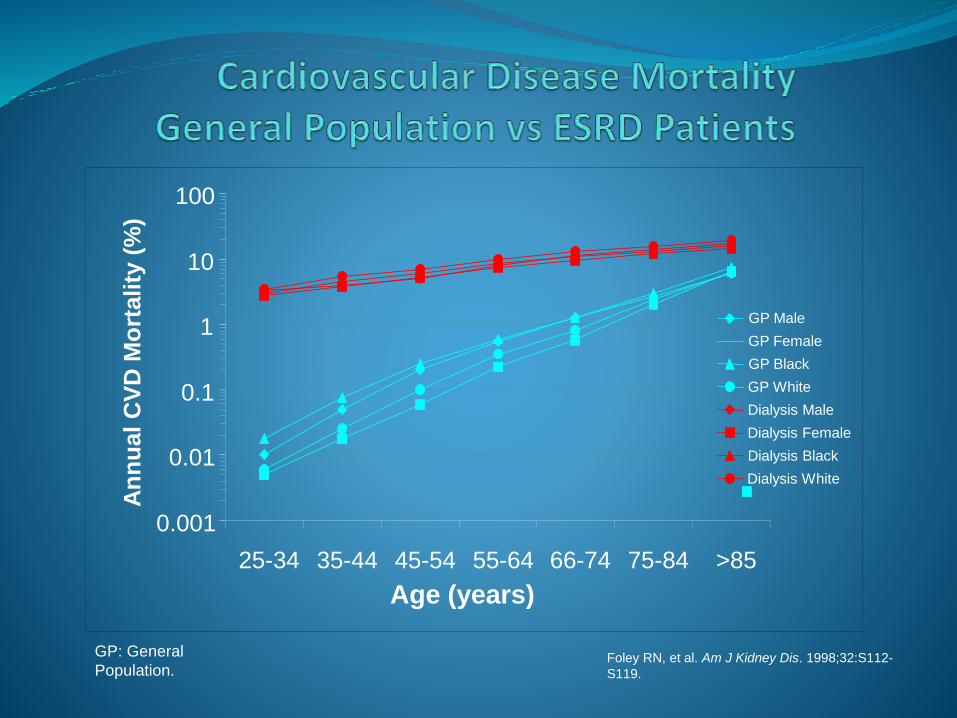
Foley RN, et al. Am J Kidney Dis. 1998;32:S112-
S119.
GP: General
Population.
0.001
0.01
0.1
1
10
100
25-34 35-44 45-54 55-64 66-74 75-84 >85
GP Male
GP Female
GP Black
GP White
Dialysis Male
Dialysis Female
Dialysis Black
Dialysis White
Age (years)
An
nu
al
CV
D M
ort
ali
ty (
%)

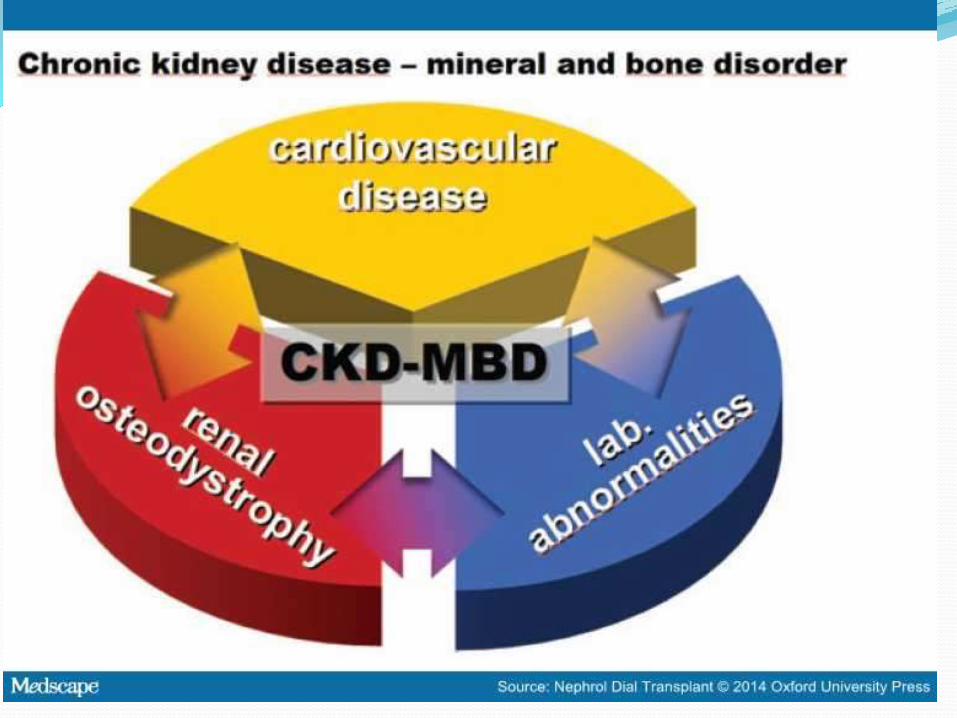

Definition of CKD-Mineral and Bone Disorder
A systemic disorder of mineral and bone metabolism due to CKD manifested by either one or a combination of the following:
Abnormalities of calcium, phosphorus, PTH, or vitamin D metabolism
Abnormalities in bone turnover, mineralization, volume, linear growth, or strength
Vascular or other soft tissue calcification
Moe S, et al. Kidney Int 69: 1945, 2006
Excess Mortality (previous slide)
excess Fractures 20% excess Block G.A. CJASN 8:2132-2140 2013
More Kidney Damage = CKD Progression
Renal Osteodystrophy ( a very mixed bag)
Stiff Vessels; Media Calcification; abnormal pulse wave velocity , abnormal medial thickness
Coronary scores :Calcified heart valves
Excess Atrial Arrythmias?
Lungs, soft tissue calcification; pruritus
Sexual Dysfunction
CVA’s?
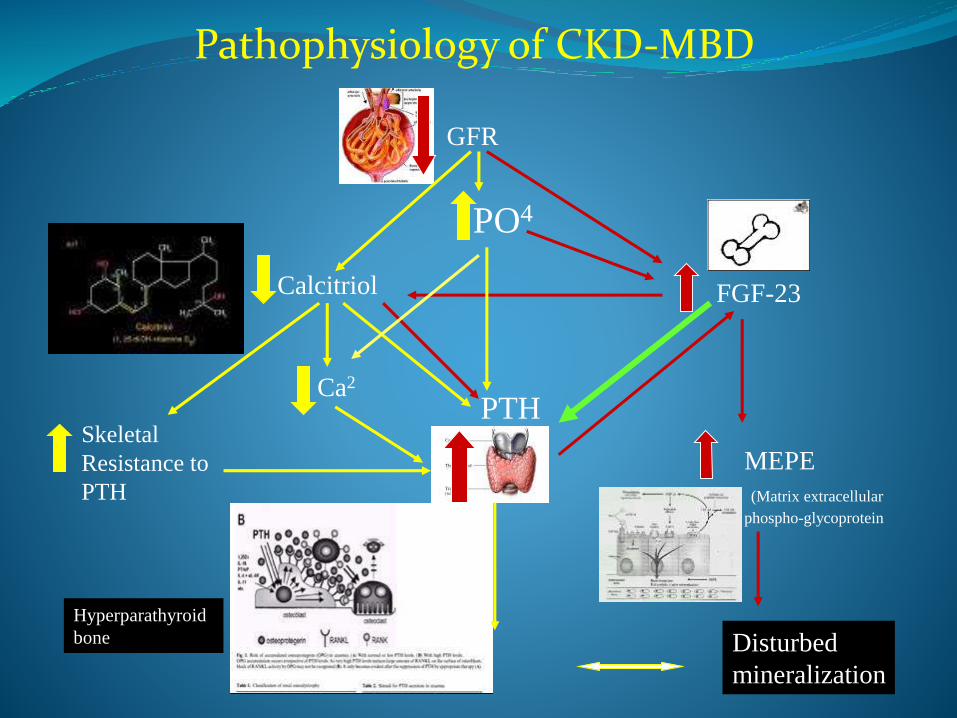
Pathophysiology of CKD-MBD
PO4
Skeletal
Resistance to
PTH
GFR
PTHCa2
FGF-23
Disturbed
mineralization
Calcitriol
MEPE
(Matrix extracellular
phospho-glycoprotein
Hyperparathyroid
bone

CKD-MBD Where can we act? Nutritional Vit D (Calcidiol level 50-100)
PO4 poisoning: Limit inorganic intake
binders
Proton Poisoning (acidosis)
Ca++ not needed !!
PTH Phosphaturic toxin
FGF 23

My Pill will fix it!!!

Vit Ds and VDRA’s Steroid Hormones (Seco Steroids)
Not true vitamins : skin can make it (naked in sun)
Receptors in multiple cells and tissues
All Vit D’s can activate receptor at different doses
Activation in Steps Liver 25-OH
Kidneys and multiple tissues 1-OH
1,25-OH Endocrine, Paracrine, Autocrine effects
1,25-OH circulating levels = little meaning
Physiology different from Pharmacological !!

Zehnder D J (2001 ) Clin Endocrinol Metab. Feb;86(2):888-94
• skin (basal keratinocytes
• hair follicles)
• lymph nodes (granulomata)
• colon (epithelial cells and parasympathetic ganglia)
• pancreas (islets)
• adrenal medulla
• brain (cerebellum and cerebral cortex),
• placenta (decidual and trophoblastic cells).
Extrarenal distribution of 1 alpha-hydroxylase
Vit D Receptors :Vitamin D receptor (VDR) is a member of the nuclear
receptor superfamily of ligand-activated transcription factors
RARs (retinoic acid receptors)
TRs (thyroid hormone receptors)
GRs (glucocorticoid receptors)
ERs and PRs (estrogen and progesterone receptors)
PPARs (peroxisome proliferator-activated receptors)
*RXRs (retinoid X receptors)
McDonnell DP, Science. 235:1214-1217, 1987.Baker, et al. Proc Natl Acad Sci U S A. 85 (10): 3294–3298, 1988.

System Tissue
Gastrointestinal Esophagus, stomach, small intestine, large intestine, colon
Arterial Vessels Vascular smooth muscle cells
Hepatic Liver parenchyma cells
Renal Proximal and distal tubules, collecting duct
Endocrine Parathyroid, pancreatic b-cells, thyroid C-cells
Exocrine Parotid gland, sebaceous gland
Reproductive Testis, ovary, placenta, uterus, endometrium, yolk sac,
Immune Thymus, bone marrow, B cells, T cells
Respiratory Lung alveolar cells
Musculoskeletal Osteoblasts, osteocytes, chondrocytes, striated muscle
Epidermis/appendage Skin, breast, hair follicles
Central nervous system Brain neurons
Connective tissue Fibroblasts, stroma
Vitamin D Receptor Distribution
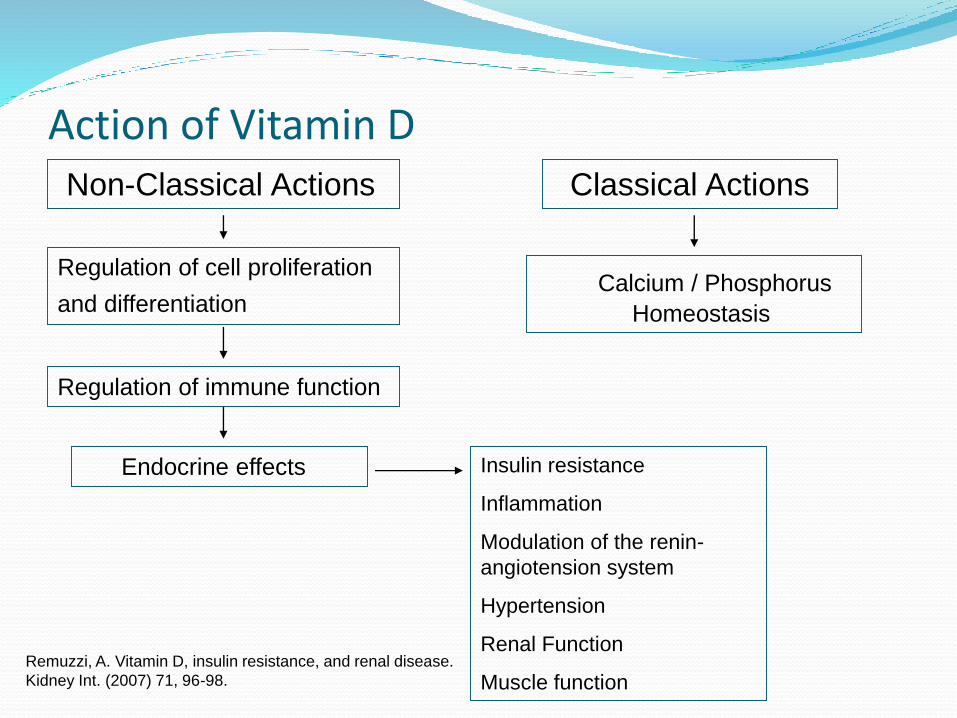
Action of Vitamin DClassical Actions
Calcium / Phosphorus
Homeostasis
Non-Classical Actions
Regulation of cell proliferation
and differentiation
Regulation of immune function
Endocrine effects Insulin resistance
Inflammation
Modulation of the renin-
angiotension system
Hypertension
Renal Function
Muscle functionRemuzzi, A. Vitamin D, insulin resistance, and renal disease.
Kidney Int. (2007) 71, 96-98.

Current data associates vitamin D deficiency with
multiple disorders (25-OH = Calcidiol deficit)
Cancer
Albuminuria CKD progression
Insulin Resistance
Secondary Hyperparathyroidism
Cardiovascular Disease Carotid thickening
Hypertension
Early mortality Plain/Dialysis
Define Deficiency when PTH elevated??

Vitamin D Deficiency/Insufficiency Rickets Targets
25(OH)D serum levels For Bones only
< 15 ng/mL Deficiency < 37.5 nmol/L
>15, <30 Insufficiency 37.5 -75
≥ 30 ng/mL Replete ≥ 75 nmol/L
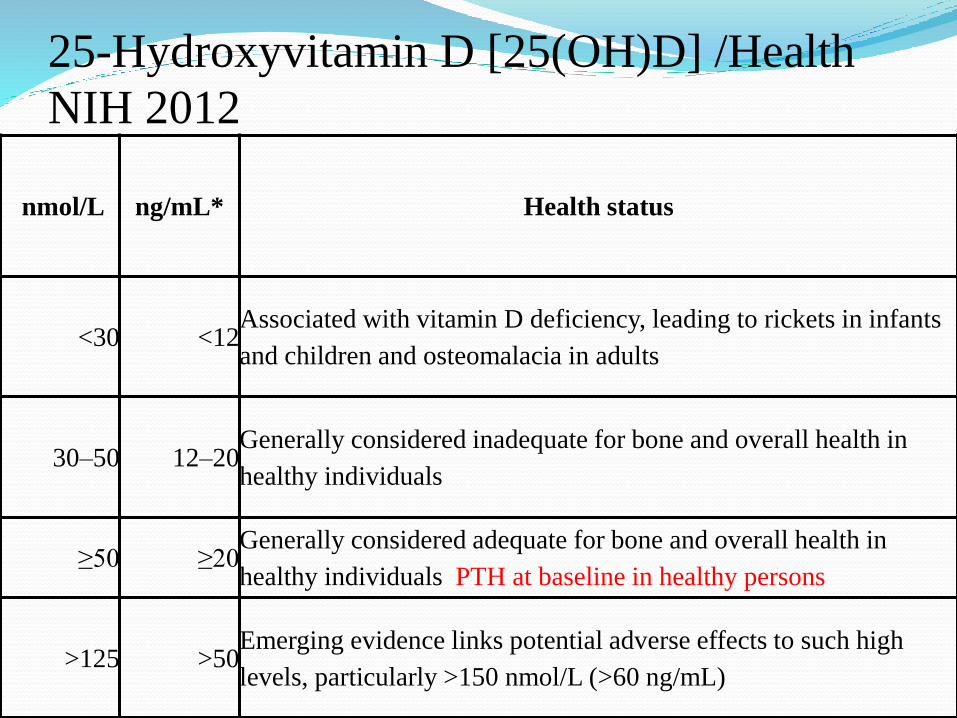
25-Hydroxyvitamin D [25(OH)D] /Health
NIH 2012
nmol/L ng/mL* Health status
<30 <12Associated with vitamin D deficiency, leading to rickets in infants
and children and osteomalacia in adults
30–50 12–20Generally considered inadequate for bone and overall health in
healthy individuals
≥50 ≥20Generally considered adequate for bone and overall health in
healthy individuals PTH at baseline in healthy persons
>125 >50Emerging evidence links potential adverse effects to such high
levels, particularly >150 nmol/L (>60 ng/mL)
Who When Supplement Vit D
Everyone Blindly or 25-OH = Calcidiol 50-100Regardless PTHNot as Rx; as Basic nourishmentVDRA’s not enough!!!!Different from Rx VDRA’sRecommended not proven yet
http://drholick.com
Phosphorus as Poison Normal and vital ion
Linked to Protein in food but added
CKDII+ : body keeps balance without high level but at a price : PTH ; tissue deposition
Ca x PO4 = active process like osteogenesis
Remain “Normal” range until late CKDIV
Normophosphemia in CKD NOT ENOUGH
TRP FEPO4 needs monitoring !!!

PhosphorusVery Common 1% weight;
< 0.03 % dialyzableConstituent/chelated/inorganicIntake 800-2700 mg/day (added)Absorption Passive + activeRegulated?Excretion : Renal Regulated by Phosphatonins PTH, FGF23 othersIs there safe limit? MDR?
Phosphorus Additives Dicalcium Phosphate
Hexametaphosphate
Monocalcium Phosphate
Phosphoric Acid
Pyrophosphate
Sodium Acid Pyrophosphate
Sodium Aluminum Phosphate
Sodium Phosphate
Sodium Tripolyphosphate
Tricalcium Phosphate
Why PO4 additivesWorldwide use ; USA 4x increase Leavening • pH Contrrol • Suspension/dispersion agent • Anti caking • Decrease cooking time • Emulsifier • Stabilizer • Moisture binding • Improve texture • Maintain color or firmness • Flavor enhancer
PO4 Absorption is active : Na/PO4 Cotransporter
Inhibiting decreases Na & PO4 absorption Dream pill 2/day
Binders crank up CoTransporter = Do not skip!!
Niacin alone or plus Laropiprant (antiflushing)
Phosphonoformic Acid (Foscarnet)
Others under research
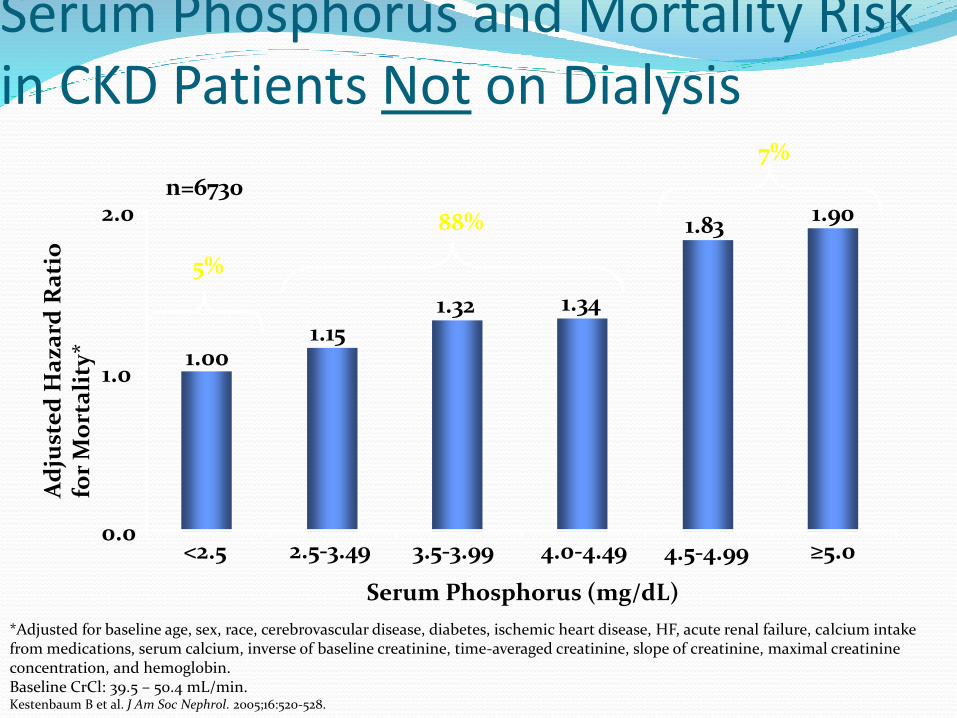
*Adjusted for baseline age, sex, race, cerebrovascular disease, diabetes, ischemic heart disease, HF, acute renal failure, calcium intake from medications, serum calcium, inverse of baseline creatinine, time-averaged creatinine, slope of creatinine, maximal creatinine concentration, and hemoglobin. Baseline CrCl: 39.5 – 50.4 mL/min.Kestenbaum B et al. J Am Soc Nephrol. 2005;16:520-528.
Serum Phosphorus and Mortality Risk in CKD Patients Not on Dialysis
1.001.15
1.32 1.34
1.90
Serum Phosphorus (mg/dL)
5%
88%
7%
1.83
n=6730
1.0
0.0<2.5 2.5-3.49 3.5-3.99 4.0-4.49
Ad
just
ed
Ha
za
rd R
ati
ofo
r M
ort
ali
ty*
4.5-4.99 ≥5.0
2.0
50 40 30 20 1060
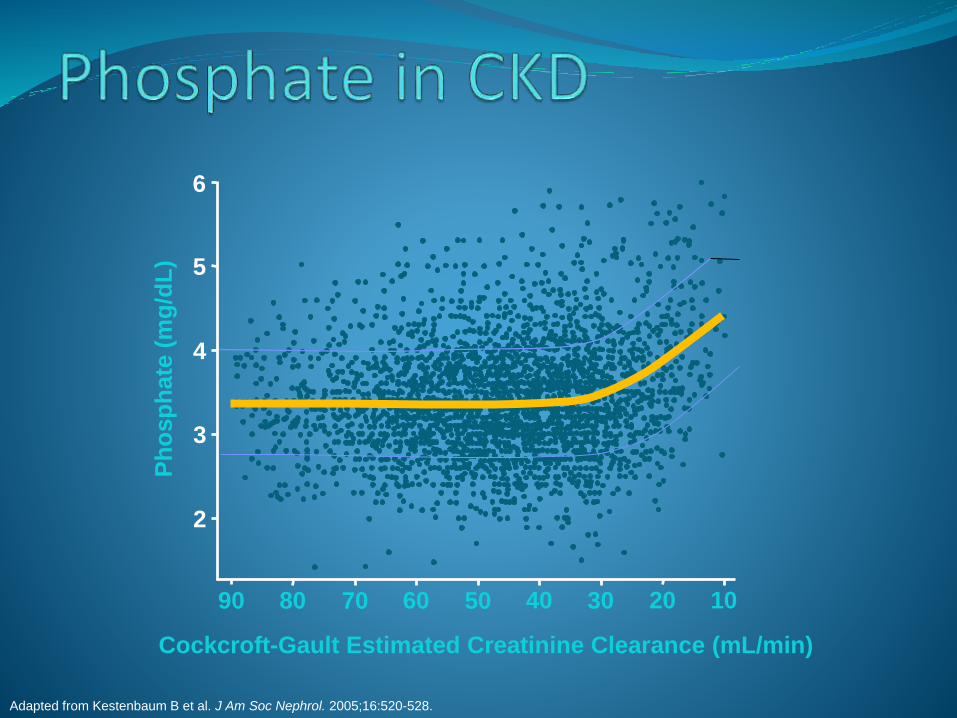
Adapted from Kestenbaum B et al. J Am Soc Nephrol. 2005;16:520-528.
Ph
osp
ha
te (
mg
/dL
)
2
3
4
5
6
90 80 70
Cockcroft-Gault Estimated Creatinine Clearance (mL/min)
Trade Off Hypothesis In CKD < V hyperphosphemia rare
Filtered load decreases with decreasing GFR
Diet/ Absorption unchanged:
FEPO4 must increase (TRP decrease)
Phosphatonins (Hormones to pee PO4):
PTH’s
FGF 23
Others under study and synthesis (MEPE)
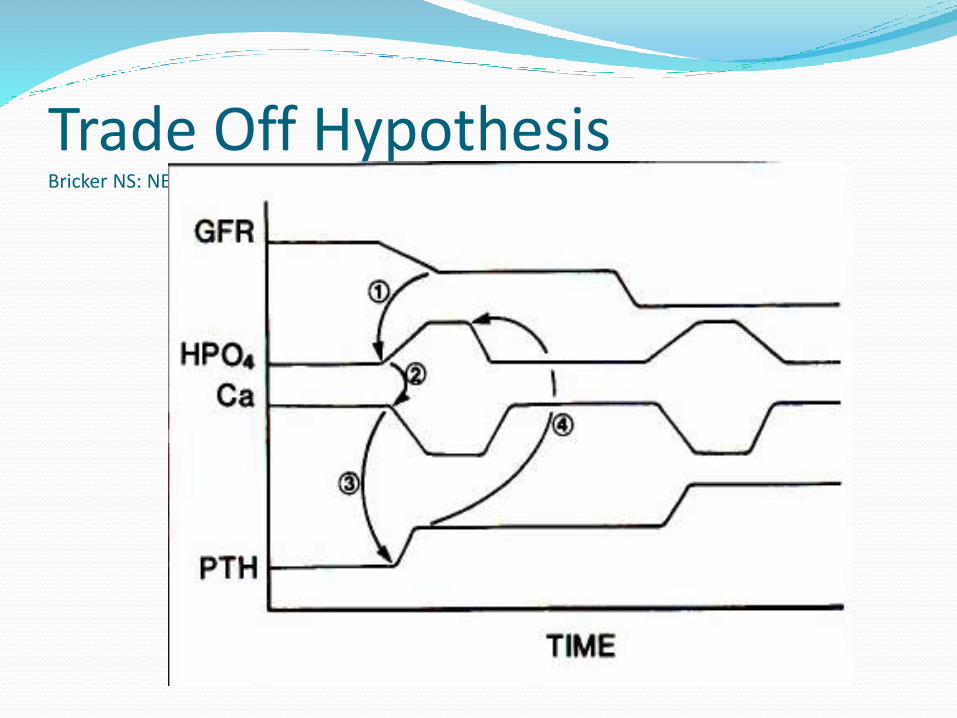
Trade Off HypothesisBricker NS: NEJM 286: 1093-1099, 1972
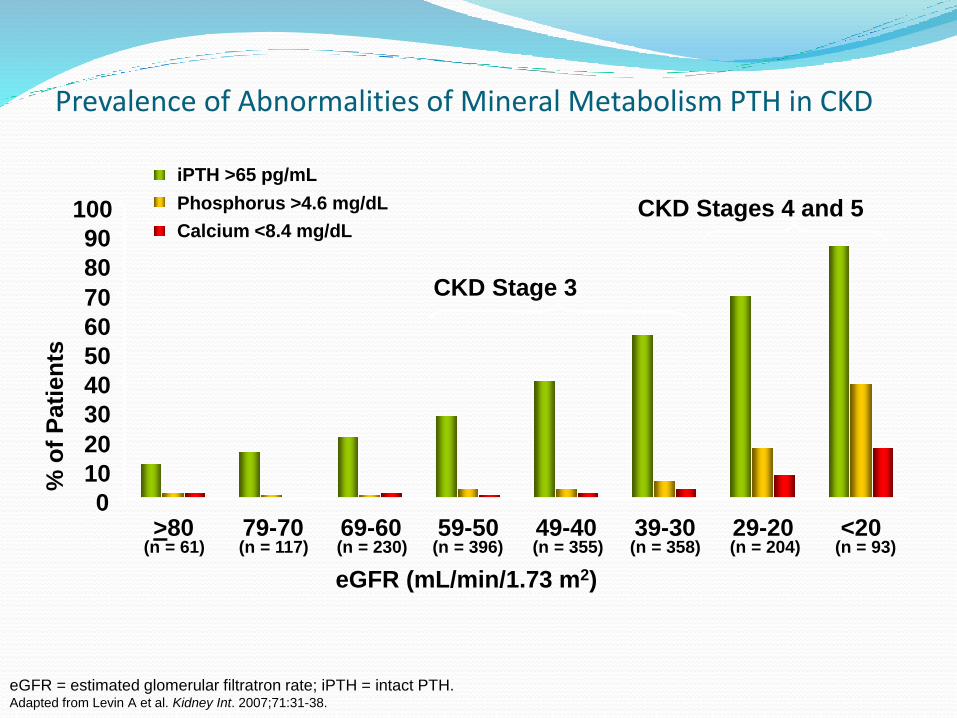
Prevalence of Abnormalities of Mineral Metabolism PTH in CKD
(n = 61) (n = 117) (n = 230) (n = 396) (n = 355) (n = 358) (n = 204) (n = 93)
CKD Stage 3
CKD Stages 4 and 5
% o
f P
ati
en
ts
eGFR (mL/min/1.73 m2)
0
10
20
30
40
50
60
70
80
90
100
79-70 69-60 59-50 49-40 39-30 29-20 <20
iPTH >65 pg/mL
Phosphorus >4.6 mg/dL
Calcium <8.4 mg/dL
eGFR = estimated glomerular filtratron rate; iPTH = intact PTH.Adapted from Levin A et al. Kidney Int. 2007;71:31-38.
>80
CV Risk = even non- CKD PO4 correlates
Impaired endothelial function
Renal Interstitial fibrosis / CKD progression
Accelerated Vascular calcification
Phosphatonins can be toxic PTH : Bone , CV, Neuropathy ; associated incr.
Mortality
FGF 23 : LVH, Vascular ; associated incr. Mortality
Others : Not clearly identified
Arterial Calcification is active cell mediated process resembling Osteogenesis; not simply CaxPO4
Which are Calcification mediators??

Dialysis removal PO4 poor Inorganic PO4 added to diet : well absorbed
Constituent Organic PO4 or Chelated (phytate ) little bioavability
Diet restriction should center inorganic added
Binders needed until absorption blockers out

Binders Aluminum Aluminum Hydroxide, Sucralfate
Strongest binders; Constipation
Al+3 Toxicity : Bone , Bone Marrow, Brain
Levels > 50-100 warn; slow > 2-3 years
All toxicity occurred before levels could be measured
Most came from dialysis water with Aluminum
Most nephrologists do not use them but there is role
Binders : Calcium Ca Acetate (Not Citrate) 667 = 169 mg;
Carbonate .5 = 199.6 mg
Rather effective but Silent toxicity
Hypercalcemia rare
Maximum dose ? 3-4 pills day TOTAL Old limits CaAc 9 CaCarb 5 pills
MDR for CKD undefined : very low!!
Do not use if tCa++ > 9.5- 10; PTH< 300; Ion product > 65-70
Interactions : Quinolones, Vit D’s , Thyroid, CCB’s, Tetracyclins

Probability of All-Cause Survival According to Calcification Status
*Comparison Between Curves Was Highly Significant (x2=42.66, P<0.0001)
Blacher A, et al. Hypertension: Vol 38, pp 938-942, October 2001
0 Arteries Calcified
1 Artery Calcified
2 Arteries Calcified
3 Arteries Calcified
4 Arteries Calcified
Pro
babili
ty o
f S
urv
ival
0.00
0.25
0.50
0.75
1.00
Duration of Follow-Up (Months)
0 20 40 60 80
P<0.0001
n = 110
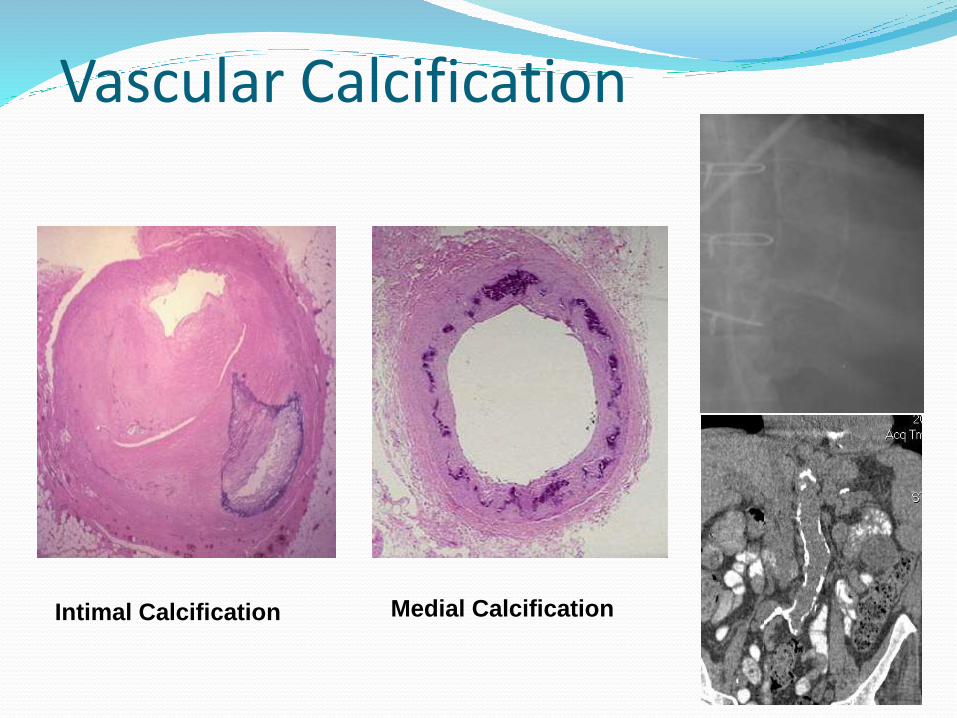
Medial CalcificationIntimal Calcification
Vascular Calcification

Binders: Magnesium Mg Hydroxide, Magnebind (with Calcium
Follow Mg++
Maximum level 3.5-3.8 : toxic
Diarrhea
Directly inhibits PTH
Is that good ?
Consider if Ca++ included
Binders: Sevelamer Sevelamer HCl; Carbonate; others
Weak , more expensive
Drug interaction: Thyroid, Vit D ,E & K, Calcitriol, Quinolones, Tetracyclines
Non Toxic : risk Obstruction
Lower Bad Cholesterol
May improve mortality vs. Ca binders
Binders : Lanthanum Carbonate Second only to Al+3 in power
Soon as powder (homemade also)
Non Toxic
Cost, tolerance
Drug Interactions : Thyroid , Vit D’s , Quinolones, Tetracyclines

Binders: Iron Velphoro = Sucroferric oxyhydroxide =
1 per meal
Higher MW
Auryxia =Ferric Citrate =
2-3 tabs 1 gram each per meal
Lower MW
So far no Al+3 toxicity x 1y exposure
Both GI problems; dark stools. Some iron absorption; may trigger false OBS?


1 84847
37
53

1
47
8
10
15
37
2428
34
43
84
84
84848484
84
84
84
8484
Capture AbDetector Ab or Detector Ab
First-generation IMA
Second-generation IMA
1
Diagram of the multiple species of PTH peptides in the circulation. The major forms are depicted with heavy lines. The grey areas depict the regions of the PTH sequence that are detected by various antibodies for first-generation and second-generation immunometric assays and indicate the PTH peptides that would be detected in each assay. The symbol ( ) depicts a PTH 1-84 peptide that is likely post-translationally modified in a region which interferes with its detection by first-generation immunometric assays.
Circulating PTH Peptides
Normal Uremia
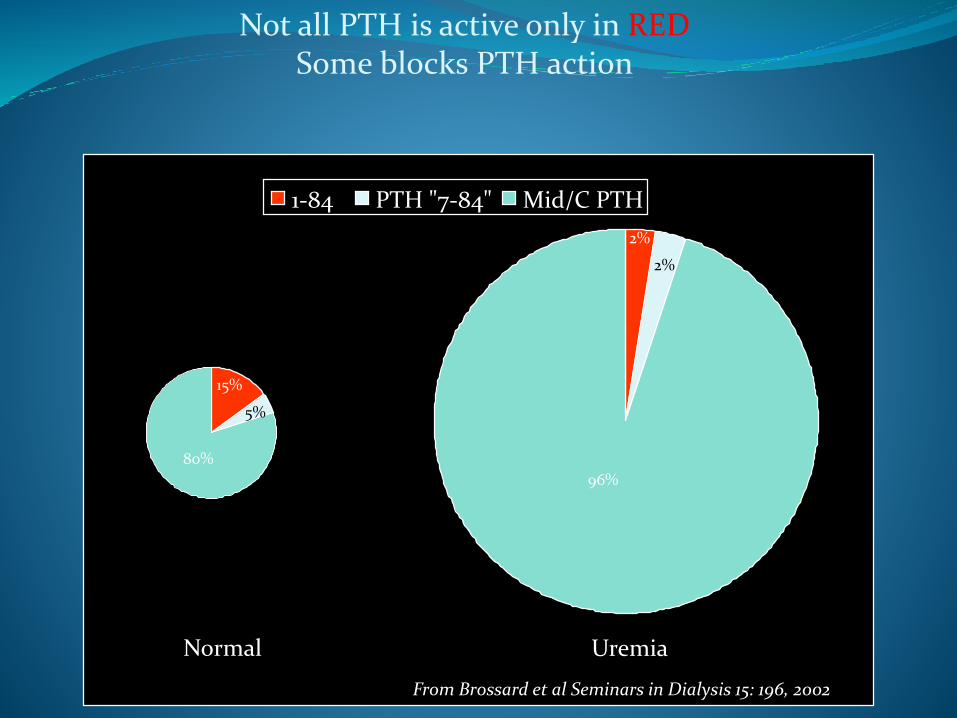
Not all PTH is active only in REDSome blocks PTH action
1-84 PTH "7-84" Mid/C PTH
From Brossard et al Seminars in Dialysis 15: 196, 2002
80%
15%
5%
2%
2%
96%
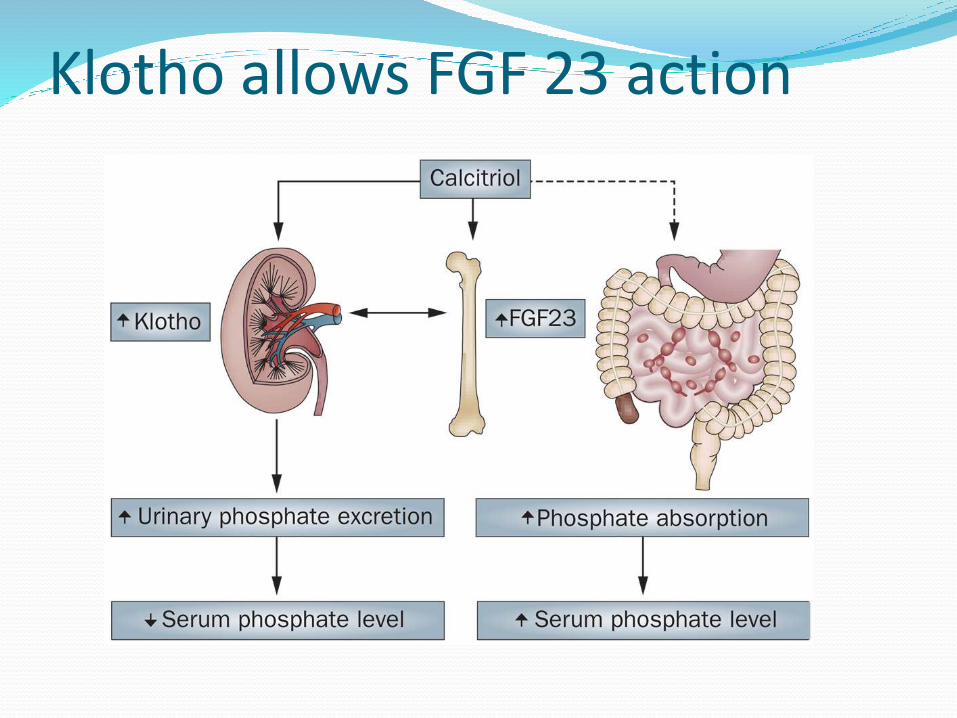
Klotho allows FGF 23 action


Scientific basis for using VDRA’ s to Rx hyperpara CKDV
“Current vitamin D therapy in ESRD appears largely based on the dramatic responses we described in the 1970s. These responses were seen in an highly selected group of patients with very severe disease. We did not study asymptomatic patients or patients with mild/moderate PTH elevations, patients who make up the bulk of those now treated with calcitriol and its descendants.> So, whether we are harming or benefitting such patients with our current approaches is quite unclear to me. I suspect in these patients, the complications of treatment may well outweigh the benefits”Don Sherrard NEPHROLCochran Collaboration 2009 Issue 4 = no data to support any VDRA more
Many Studies Show a Clinical Advantage for VDRA Therapy
Decrease in mortality: Teng et al., J Am Soc Nephrol. 2005;16:1115-1125 Kalantar-Zadeh et al., Kidney Int. July 2006 Tentori et al, Kidney Int. Oct 2006 Lee et al, J Renal Nutr. 2007 Melamed et al, Kidney Int. March 2006 Young EW et al, ASN Proceedings 2005 TH-PO735 (DOPPS study) Wolf et al., ASN Proceedings 2006 TH-FC 093 Spiegel DM, et al. ASN Proceedings 2006 F-FC080 Schumock et al., ASN Proceedings 2006 SA-PO340 Naves et al., ASN Proceedings 2006 TH-PO977 and TH-PO976 (CORES study) Japanese Society for Dialysis Therapy Ann. Report 1999
Decrease in hospitalizations: Go et al., NEJM 2004; 351: 1296-1305 Dobrez DG et al, Neph Dial. Trans. 2004; 19(5): 1174- 1181 Tentori et al., ASN Proceedings 2006 SA-PO577 Melnick et al, 25th Ann Dialysis Conf. 2005 Proceedings, 9 (1):90-90
What is ahead in pipeline
“Son of Cinacalcet” =R568 2-Chloro-N-[(1R)-1-(3-methoxyphenyl)ethyl]-benzenepropanamine HCl
“Son of Sevelamer” Japan 13 Pt’sChitosan chewing Gum PO4 absorption blockers
Alcohol injection Parathyroids??
More Indirect Studies Few Survival Studies:
IMPACT-SHPT “Paricalcitol or Cinacalcet centered ..markers CKD-MBD” Neph Dial Transp 2014: Feb 4 (Epub)iPTH 300-800 PO4 < 6.5 = Paricalcitol won
What do I do ?Keep reading criticallyNew Binders , PO4 blockersSupplement nutritional VitDAvoid Proton PoisoningCKD Follow PO4 + TRPLimit added inorganic PO4 Binders : Ca/Non CaPTH Rx only if Alk PhosNothing beats steel for PTH ??
Our Job in CKD-MBD

CKD V :Not all Poisons are equal :
High Ca > 10-11 : short term toxicLow Ca Harmless unless Tetany : no need to Rx !! Except hypoparathyroidism
PO4 : Slowly toxic : no level safe ? > 2-2.5 ??Low PO4 marker malnutrition
PTH : Wide range with few toxic effects
Low worse than High still weak poison
K : Acute high > 6 -6.5 ; slow can tolerate better : EKGLow (< 3.5-3.8) predialysis a risk if bath K low
Mg 3-3,5 OK over 4-6 respiratory depression
Al+3 : takes years to build up ; over 100 toxic
And the Emperor was Naked…
Calcitriol = 1,25 Circulating Hormone only made kidney1,25 level important Bone Heath
Aluminum binders not absorbedCorn, Beans are high in PhosphorusControl PTH by high bath Calcium (Ca =3.5)Ca binders good for you: Strong bones /lower PO4
If KT/V OK you are OK = Express Dialysis Vit D analogs will cure PTH; use plentyCinacalcet replaces parathyroidectomyParicalcitol safer than Hectorol or Calcitriol
Nothing beats steel for PTH

My Rx scheme 3/15Do as little harm as possible within ignorance
PTH Ca Binders VDRA's Cinacalcet
< 200 No No No
200-300 OK Yes No
> 300 OK Yes Yes
> 1000 OK Yes ?? Yes ??
tCa Ca Binders VDRA's Cinacalcet9.8-10 No ?? Yes< 9.8 Yes Yes if high PTH Alk>10 No No YesCaveats : Respect Max Ca dose (Antacids ) ; Ca x PO4 < 70; Parathyroidectomy ??Avoid Ca overload > HyperCaRx PTH = Not proven much help to Pt’s but need Chart buffed

STOP
Slide Show
Toxic Fosfatonins PTH no longer only one:
FGF-23
produced by osteocytes reduce the renal resorption of phosphate,
reduce 1,25 vitamin D levels
suppress PTH levels
“master regulator of the calcium-phosphate cross product,”
CV Toxic ??
Others under study
Trade off Hypothesis Normal SPO4 = 4 mg/dl filters 57600 mg in 24h
excretes 900 = reabsorbs 99%
CKDIV also SPO4 = 4 mg/dl filters 5760 mg in 24h but reabsorbs only 70% or less
Keep SPO4 fairly constant by cutting back reabsorption = trade off
Phosphatonins regulate (PTH, FGF23 ,others)
Management CKD-MBD II 2012
VDRA’s to control overactive/overgrown PTHsNot a simple problem of SS VDRA’s/Cinacalcet/Binders :Calci(fe)diol/Calcitriol/
Paricalcitol/DoxercalciferolCalcimimetics : Cinacalcet/ R568 iv Parathyroidectomy Subtotal/ Total + autograft
ETOH Injection (only Japan)Avoid Low Turnover/Adynamic Bone Dx !!
PTH < 2 x upper limit true hypocalcemia :
DC Calcimimetics, VDRA’s