claims reports: overview - health insurance texas · claims reports: overview ... cmc coordination...
TRANSCRIPT

Page E — 1 Rev. 06/25/07
Claims Reports: Overview
Introduction
BCBSTX provides explanations of claims handling to you and the patient. There are
two reports that may be sent to your office, and they are each described in this
section.
In this
Section
This section describes the following claims reports:
Report Title Page
Provider Claim Summary for CMS 1500 (08/05) Claims E — 2
Provider Claim Summary for UB-04 Claims E — 7
Explanation of Benefits (EOB) E — 11

Rev.06/25/07 Page E — 2
Sample of Provider Claim Summary
Page E — 3 Rev. 06/25/07
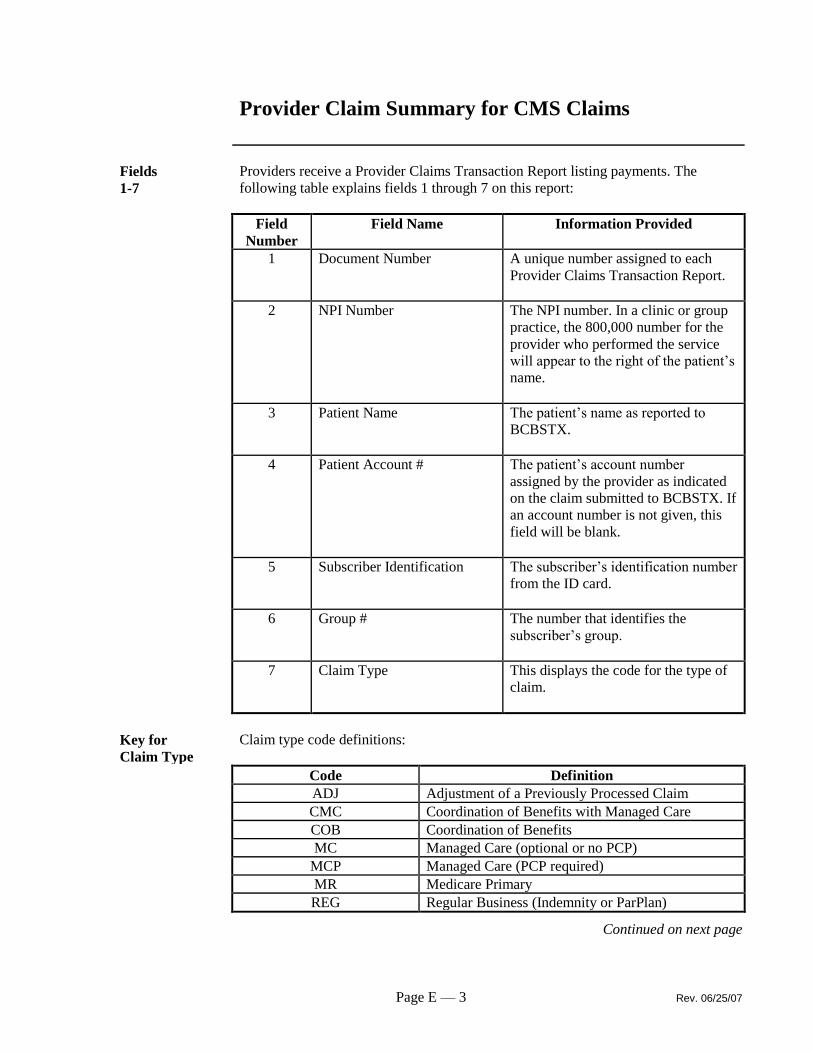
Provider Claim Summary for CMS Claims
Fields
1-7
Providers receive a Provider Claims Transaction Report listing payments. The
following table explains fields 1 through 7 on this report:
Field
Number
Field Name Information Provided
1 Document Number A unique number assigned to each
Provider Claims Transaction Report.
2 NPI Number The NPI number. In a clinic or group
practice, the 800,000 number for the
provider who performed the service
will appear to the right of the patient’s
name.
3 Patient Name The patient’s name as reported to
BCBSTX.
4 Patient Account # The patient’s account number
assigned by the provider as indicated
on the claim submitted to BCBSTX. If
an account number is not given, this
field will be blank.
5 Subscriber Identification The subscriber’s identification number
from the ID card.
6 Group # The number that identifies the
subscriber’s group.
7 Claim Type This displays the code for the type of
claim.
Key for
Claim Type
Claim type code definitions:
Code Definition
ADJ Adjustment of a Previously Processed Claim
CMC Coordination of Benefits with Managed Care
COB Coordination of Benefits
MC Managed Care (optional or no PCP)
MCP Managed Care (PCP required)
MR Medicare Primary
REG Regular Business (Indemnity or ParPlan)
Continued on next page
Rev.06/25/07 Page E — 4
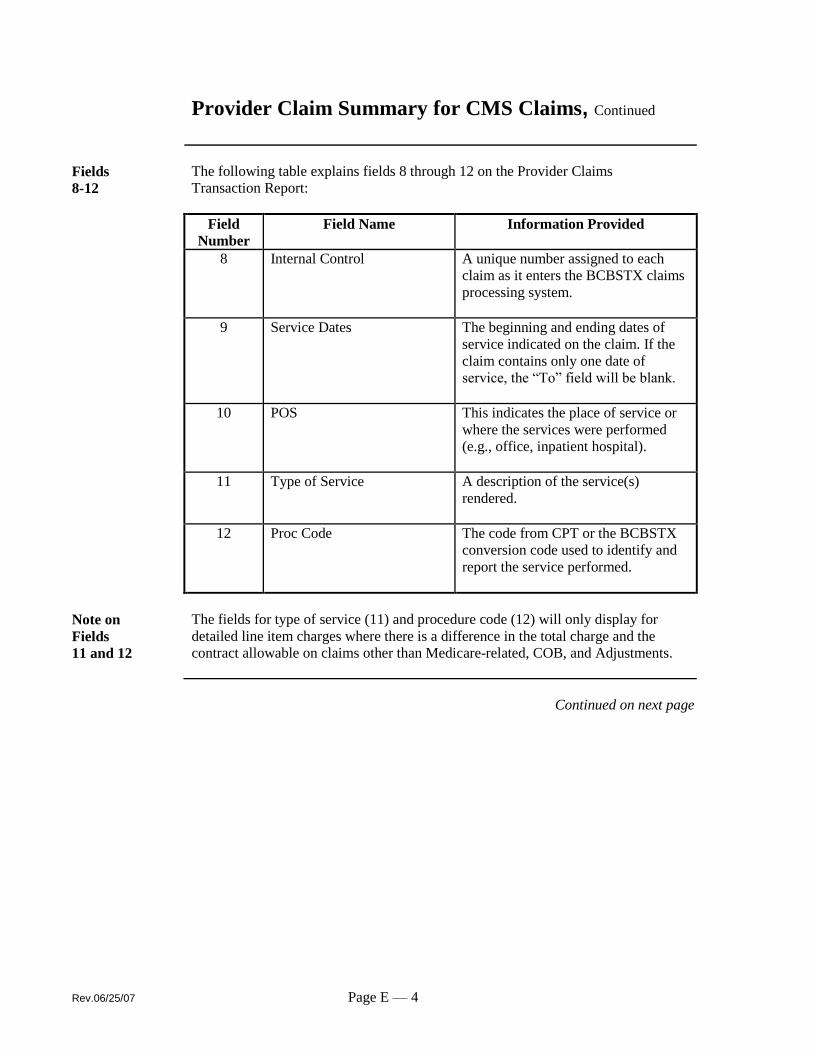
Provider Claim Summary for CMS Claims, Continued
Fields
8-12
The following table explains fields 8 through 12 on the Provider Claims
Transaction Report:
Field
Number
Field Name Information Provided
8 Internal Control
A unique number assigned to each
claim as it enters the BCBSTX claims
processing system.
9 Service Dates
The beginning and ending dates of
service indicated on the claim. If the
claim contains only one date of
service, the “To” field will be blank.
10 POS
This indicates the place of service or
where the services were performed
(e.g., office, inpatient hospital).
11 Type of Service A description of the service(s)
rendered.
12 Proc Code
The code from CPT or the BCBSTX
conversion code used to identify and
report the service performed.
Note on
Fields
11 and 12
The fields for type of service (11) and procedure code (12) will only display for
detailed line item charges where there is a difference in the total charge and the
contract allowable on claims other than Medicare-related, COB, and Adjustments.
Continued on next page

Page E — 5 Rev. 06/25/07
Provider Claim Summary for CMS Claims, Continued
Fields
13 -16
The following table explains fields 13 through 16 on the Provider Claims
Transaction Report:
Field
Number
Field Name Information Provided
13 Total Charges The total charges filed on the claim.
14 Contract Allowable The benefits allowed by the
subscriber’s coverage.
15 MSG Code The message code for the explanation
of the difference between the billed
charges and the contract allowable for
that procedure. Multiple message
codes may indicate that the claim was
processed with more than one type of
coverage or policy. Please see
Message Code Explanation (18).
16 Patient’s Share Listing of any copayment, deductible,
cost share (coinsurance), and charges
for medically necessary, limited, or
noncovered services.
Patient’s Share
The subscriber is responsible for no other charges submitted on the claim except for
the following:
Patient’s Share Which Includes
Copay/Deductible
The amount of copayment and/or deductible taken
from the gross allowable charges.
Coinsurance
The amount taken from the gross allowable charges
and the patient’s portion when contract benefit
percentages were applied. This includes the patient’s
benefit contract.
Other Medically necessary items not covered or limited by
the patient’s benefit contract.
Continued on next page
Rev.06/25/07 Page E — 6
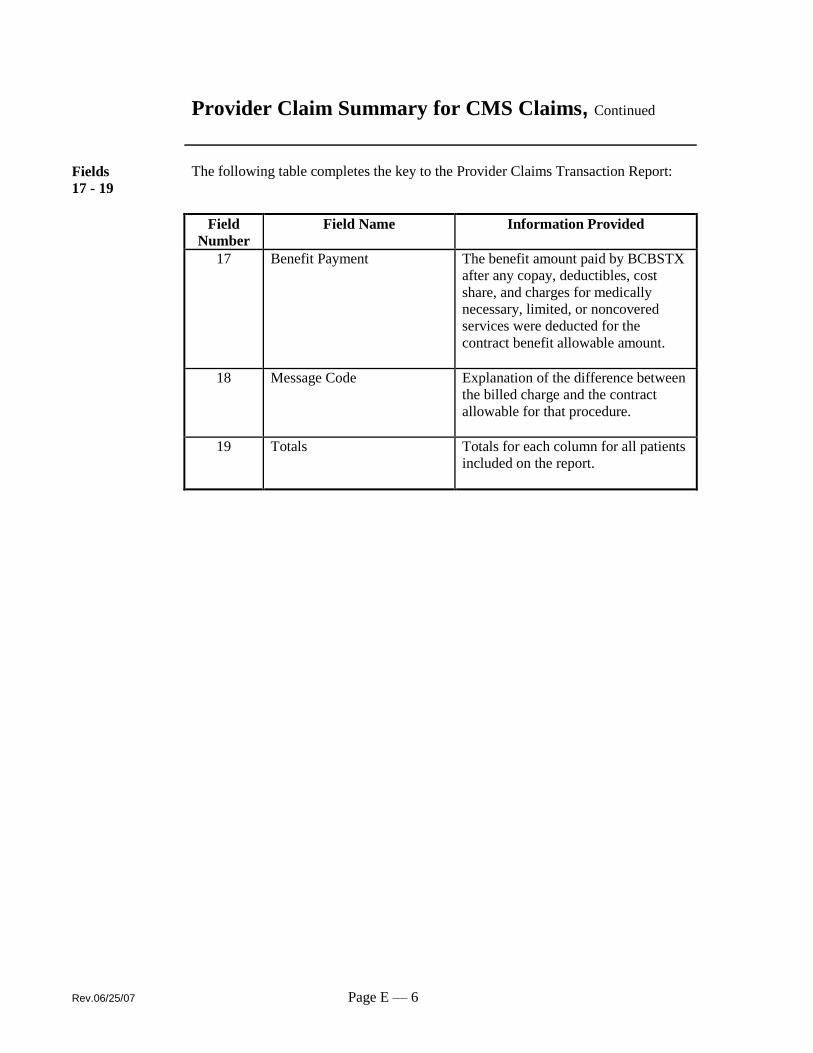
Provider Claim Summary for CMS Claims, Continued
Fields
17 - 19
The following table completes the key to the Provider Claims Transaction Report:
Field
Number
Field Name Information Provided
17 Benefit Payment The benefit amount paid by BCBSTX
after any copay, deductibles, cost
share, and charges for medically
necessary, limited, or noncovered
services were deducted for the
contract benefit allowable amount.
18 Message Code Explanation of the difference between
the billed charge and the contract
allowable for that procedure.
19 Totals Totals for each column for all patients
included on the report.

Page E — 7 Rev. 06/25/07
Provider Claim Summary for UB-04 Claims
PROVIDER CLAIM SUMMARY
DATE: 02/10/05 1
PROVIDER NUMBER: 0000HH1234 2
CHECK NUMBER: 12345678 3
TAX IDENTIFICATION NUMBER: 123156769 4
5 COUNTY MEDICAL CENTER
P. 0. BOX 123456
YOUR CITY, TX. 12345-1234
ANY MESSAGES WILL BEGIN ON PAGE 1
*********** INPATIENT
PATIENT: HORMAN DOE PATIENT NO: 123456789 ADMIT DATE FROM DATE END DATE
CLAIM NO: 0000123456789000X CLAIM TYPE: 01/30/05 01/30/05 01/31/05
GROUP-SUB NO: FEPTX-12345678 HPI: D DRG
DAYS DRG PROVIDER OTHER PAYABLE FACILITY ADJUSTED MANAGED CARE TOTAL AMOUNT
/TRT CODE CHARGE / WITHHOLD ALLOWABLE PROV. CHARGE DEDUCTION(S) PAID
001 294 $10,816.00 $8,022.01- $2,795.99 $2,795.99 $500.00 $2,195.99
MESSAGES/REASONS: OE , OH , DRG
*** DEDUCTIONS/OTHER INELIGIBLE ***
CONTRACT DEDUCTIBLE/COPAY: $100.00
MANAGED CARE DEDUCTION(S): $500.00
TOTAL DEDUCTIONS/OTHER INELIGIBLE: ___$600.00
PATIENT'S SHARE: ___$600.00
--------------------------------------------------------------------------------
PROVIDER CLAIMS AMOUNT SUMMARY
MUMBER OF CLAIMS: 1 | AMOUNT PAID: $2,195.99
PROVIDER CHARGES: $10,618.00 | RECOUPMENT AMOUNT: $0.00
ADJUSTED PROVIDER CHARGES: $2,795.99 | NET AMOUNT AMOUNT: $2,195.99
PATIENT'S SHARE: $600.00 |
---------------------------------------------------------------------------------
CLAIM TYPE
---------------------------------------------------------------------------------
MESSAGES/REASONS:
(OE ). A CONTRACT DEDUCT I BLE/COPAY HAS BEEN TAKEN.
(OH ). PROGRAM REQUIREMENTS AS IDENTIFIED BY THE MEMBER'S CONTRACT HAVE NOT
BEEN FULFILLED. THIS IS THE PATIENT'S LIABILITY.
(DRG). THE PAYMENT ON THIS CLAIM HAS BEEN PROCESSED ACCORDING TO THE OMNIBUS
BUDGET RECONCILIATION ACT OF 1990. THE PAYMENT PROVIDED IS THE SAME
AS THE PAYMENT YOU WOULD HAVE RECEIVED HAD THE PATIENT BEEN ENROLLED
IN MEDICARE PART A. THE PAYMENT IS BASED ON THE MEDICARE DRG PRICE.
THE SUBSCRIBER IS NOT RESPONSIBLE FOR THE DIFFERENCE.
1 OF 1

Rev.06/25/07 Page E — 8
Provider Claim Summary for UB-04 Claims, Continued
Fields
1-9
The Provider Claim Summary (PCS) is a notification statement sent to contracting
providers with Blue Cross and Blue Shield of Texas (BCBSTX) after a claim has
been processed. The following table explains fields 1 through 9 on this report:
Field
Number
Field Name Information Provided
1 Date Date the summary was finalized.
2 NPI Number NPI Number
3 Check Number Number assigned to the check for this
summary.
4 Tax Identification Number Number which identifies provider’s
taxable income.
5 Provider or Group Name &
Address
The provider/group address where the
services were rendered.
6 Patient Name of the individual who received
the service.
7 Claim Number The Blue Cross number assigned to
the claim.
8 Group-Sub Number Number that identifies the employer
group and member.
9 Patient Number The patient’s account number
assigned by the provider.
Continued on next page

Page E — 9 Rev. 06/25/07
Provider Claim Summary for UB-04 Claims, Continued
Fields
10-19
The following table explains fields 10 through 19 on this report:
Field
Number
Field Name Information Provided
10 Claim Type Code for type of claim (benefit plan) –
see field 27.
11 HPI Indicator Blue Cross payment method for this
claim.
IND DESCRIPTION
D DRG
B Outpatient DRG Cap
W Withhold/Discount
R Case Rate
E % of charge w/cap
F Fee Schedule
P Per Diem
N Negotiated
C Inpatient Case Rate
12 Admit Date Date if admission.
13 From Date Beginning and ending dates of
services rendered.
14 End Date
15 Days/Treatment Number of days/treatment.
16 DRG Code DRG code for this type of service.
17 Provider Charge Total amount of billed charges.
18 Other Payable/Withhold Other payable amounts, such as
discounts or withholds, that affect the
adjusted provider charges.
19 Facility Allowable The provider’s allowed amount
according to negotiated contract.
Continued on next page
Rev.06/25/07 Page E — 10
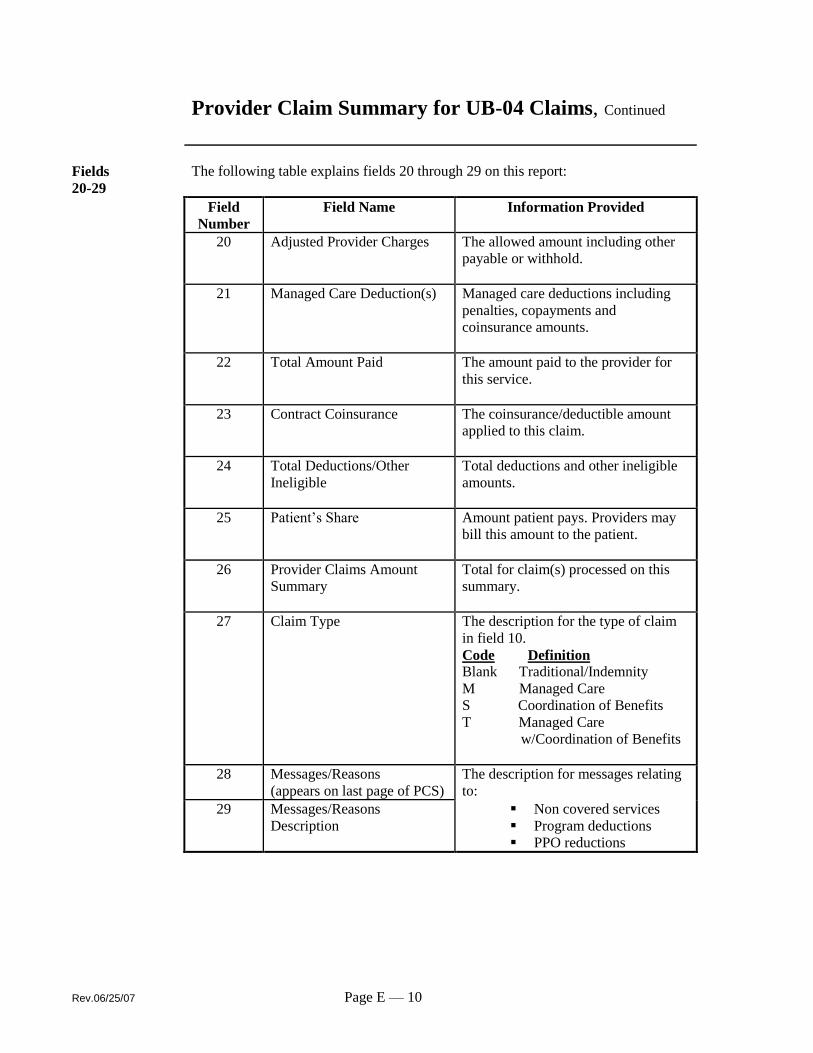
Provider Claim Summary for UB-04 Claims, Continued
Fields
20-29
The following table explains fields 20 through 29 on this report:
Field
Number
Field Name Information Provided
20 Adjusted Provider Charges The allowed amount including other
payable or withhold.
21 Managed Care Deduction(s) Managed care deductions including
penalties, copayments and
coinsurance amounts.
22 Total Amount Paid The amount paid to the provider for
this service.
23 Contract Coinsurance The coinsurance/deductible amount
applied to this claim.
24 Total Deductions/Other
Ineligible
Total deductions and other ineligible
amounts.
25 Patient’s Share Amount patient pays. Providers may
bill this amount to the patient.
26 Provider Claims Amount
Summary
Total for claim(s) processed on this
summary.
27 Claim Type The description for the type of claim
in field 10.
Code Definition
Blank Traditional/Indemnity
M Managed Care
S Coordination of Benefits
T Managed Care
w/Coordination of Benefits
28 Messages/Reasons
(appears on last page of PCS)
The description for messages relating
to:
29 Messages/Reasons
Description
Non covered services
Program deductions
PPO reductions

Page E — 11 Rev. 06/25/07
Sample of Explanation of Benefits (EOB)
Rev.06/25/07 Page E — 12
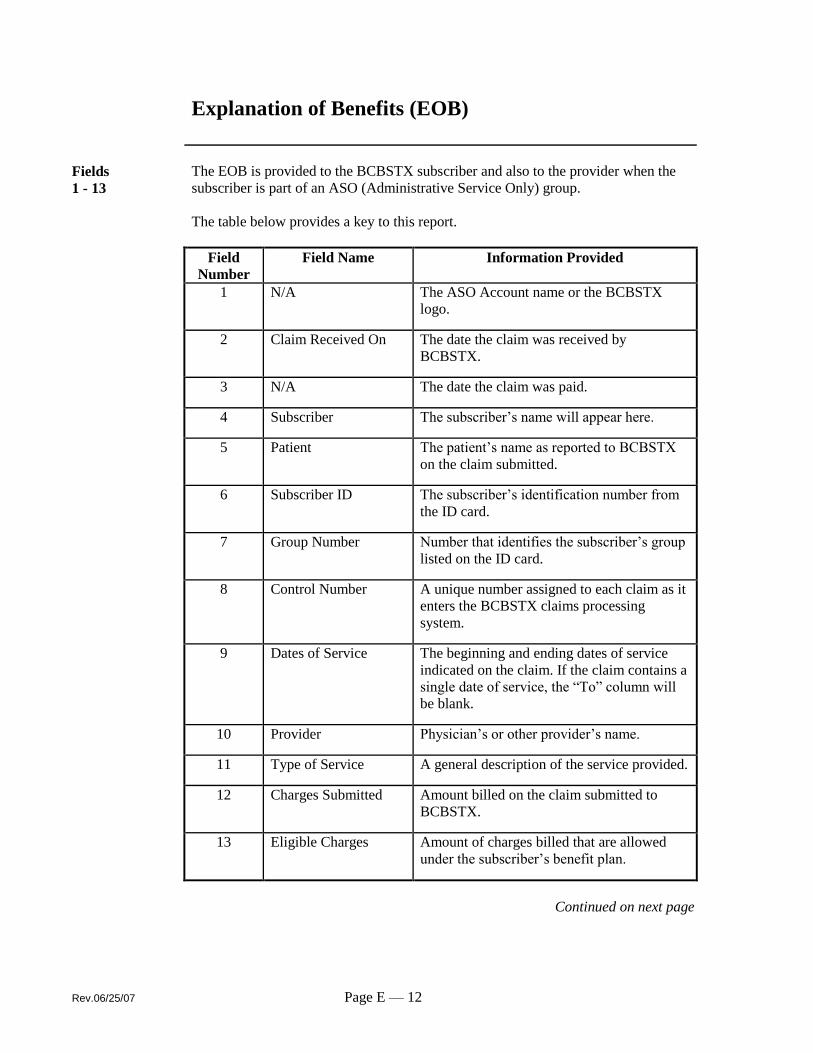
Explanation of Benefits (EOB)
Fields
1 - 13
The EOB is provided to the BCBSTX subscriber and also to the provider when the
subscriber is part of an ASO (Administrative Service Only) group.
The table below provides a key to this report.
Field
Number
Field Name Information Provided
1 N/A The ASO Account name or the BCBSTX
logo.
2 Claim Received On The date the claim was received by
BCBSTX.
3 N/A The date the claim was paid.
4 Subscriber The subscriber’s name will appear here.
5 Patient The patient’s name as reported to BCBSTX
on the claim submitted.
6 Subscriber ID The subscriber’s identification number from
the ID card.
7 Group Number Number that identifies the subscriber’s group
listed on the ID card.
8 Control Number A unique number assigned to each claim as it
enters the BCBSTX claims processing
system.
9 Dates of Service The beginning and ending dates of service
indicated on the claim. If the claim contains a
single date of service, the “To” column will
be blank.
10 Provider Physician’s or other provider’s name.
11 Type of Service A general description of the service provided.
12 Charges Submitted Amount billed on the claim submitted to
BCBSTX.
13 Eligible Charges Amount of charges billed that are allowed
under the subscriber’s benefit plan.
Continued on next page
Page E — 13 Rev. 06/25/07
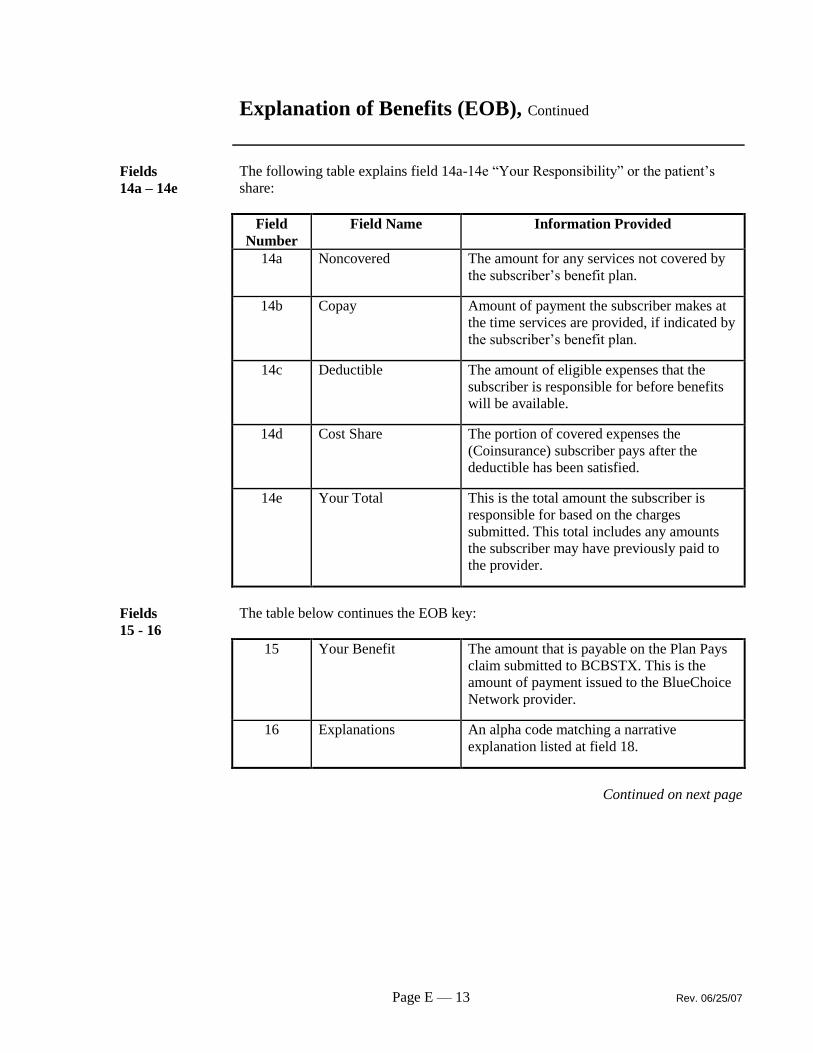
Explanation of Benefits (EOB), Continued
Fields
14a – 14e
The following table explains field 14a-14e “Your Responsibility” or the patient’s
share:
Field
Number
Field Name Information Provided
14a Noncovered The amount for any services not covered by
the subscriber’s benefit plan.
14b Copay Amount of payment the subscriber makes at
the time services are provided, if indicated by
the subscriber’s benefit plan.
14c Deductible The amount of eligible expenses that the
subscriber is responsible for before benefits
will be available.
14d Cost Share The portion of covered expenses the
(Coinsurance) subscriber pays after the
deductible has been satisfied.
14e Your Total This is the total amount the subscriber is
responsible for based on the charges
submitted. This total includes any amounts
the subscriber may have previously paid to
the provider.
Fields
15 - 16
The table below continues the EOB key:
15 Your Benefit The amount that is payable on the Plan Pays
claim submitted to BCBSTX. This is the
amount of payment issued to the BlueChoice
Network provider.
16 Explanations An alpha code matching a narrative
explanation listed at field 18.
Continued on next page
Rev.06/25/07 Page E — 14
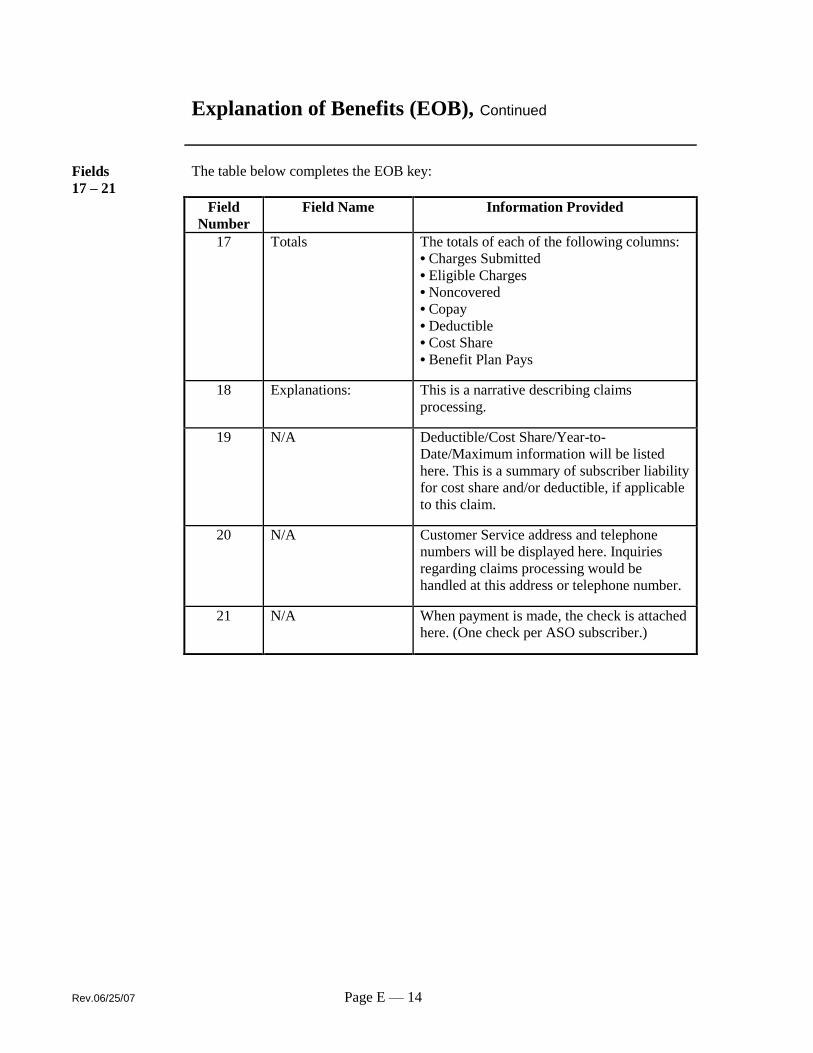
Explanation of Benefits (EOB), Continued
Fields
17 – 21
The table below completes the EOB key:
Field
Number
Field Name Information Provided
17 Totals The totals of each of the following columns:
• Charges Submitted
• Eligible Charges
• Noncovered
• Copay
• Deductible
• Cost Share
• Benefit Plan Pays
18 Explanations: This is a narrative describing claims
processing.
19 N/A Deductible/Cost Share/Year-to-
Date/Maximum information will be listed
here. This is a summary of subscriber liability
for cost share and/or deductible, if applicable
to this claim.
20 N/A Customer Service address and telephone
numbers will be displayed here. Inquiries
regarding claims processing would be
handled at this address or telephone number.
21 N/A When payment is made, the check is attached
here. (One check per ASO subscriber.)