classification of brain tumors neoplastic - cuhk surgery clinical... · • classification –...
TRANSCRIPT

Clinical Aspects of Brain Clinical Aspects of Brain TumoursTumours
Master of Science in Neurological SciencesDanny TM ChanNeurosurgeryOct 29 2012
Brain Tumors
• Classification– Histological / Pathological
– Clinical / Anatomical
Classification of Brain TumorsClassification of Brain Tumors
• Primary – Benign : Meningioma 20%– Malignant : Glioma 30%
• Secondary (30%)– Commonest tumors in the brain– Lung /Breast /Skin– Colorectal /Kidney /Prostate /Gonadal– Unknown Primary (15% of all brain 2’)
NeoplasticNeoplastic
• Primary– Glioma
– Meningioma
– Neuroma
– Others
• Secondary– Metastasis
NeoplasticNeoplastic
• Primary– Glioma
– Meningioma
– Neuroma
– Others
• Secondary– Metastasis
Primary Brain Tumors
• Neuroectodermal– Glial cells– Astrocytoma– Oligodendroglioma– Ependymoma– Medulloblastoma
• Mesenchymal– Meningioma– Haemangioblastoma– Sarcoma
• Lymphoid– Lymphoma
• Nerve Sheath– Acoustic neuroma– Trigeminal neuroma
• Germ Cell Tumor– Germinoma– NG‐GCT
Classification of Brain Tumors
• Supratentorial– Metastasis, glioma, meningioma
• Infratentorial– Metastasis, glioma(ependymoma, medulloblastoma), meningioma, haemangioblastoma
• Specific locations– Pituitary / Sellar– Pineal– Cerebellar‐pontine angle
Symptoms & SignsSymptoms & Signs
• Raised intracranial pressure (ICP)– Headache / Nausea / Vomiting– Papilloedema– Coma
• Local (focal) brain dysfunction– Compression – Hemiparesis/hemianopia– Infiltration– Seizure– CN palsy

Pressure Effects
Seizures
Focal Effects Acute
Events
Systemic / hormonal Effects
Elevated ICPElevated ICP
• Mass (SOL)
• Edema
• Hydrocephalus
ICP
Volume
Kelly Monro Doctrine
Brain tissue
CSF
Blood
Tumor

Pressure Effects
Seizures
Focal Effects Acute
Events
Systemic / hormonal Effects
Function of BrainFunction of Brain
Vision
Motor & Sensation
Memory & Emotion
Language
Distribution of Control in BrainDistribution of Control in Brain Left brain‐Right sideRight brain‐Left side

Kernohan’s sign
Ipsilateral limb
False localising sign
Contralaterallimb weakness
False localizing sign
Weakness Weakness
Right RightLeft Left
Right
Kernohan’snotch
Left
Pressure Effects
Seizures
Focal Effects Acute
Events
Systemic / hormonal Effects
SeizureSeizure
• Focal– Jacksonian
• Generalized
2012/10/29 21
Indications for operationIndications for operation• To confirm the diagnosis
• Evidence of significant mass effect
• Relief of hydrocephalus
• Cytoreduction
2012/10/29 22
Preoperative InvestigationsPreoperative Investigations• CT scan
• Magnetic Resonance Imaging (MRI) or angiography (MRA)
• Digital subtraction angiography (DSA)
• Work‐up for primary disease
2012/10/29 23
General PreGeneral Pre‐‐Op TreatmentOp Treatment
• Observation• Dexamethasone• Anticonvulsant• Osmotherapy if acute deterioration
2012/10/29 24
Urgency of treatmentUrgency of treatment
• Depends on the mass effect of the tumour• The rate of growth • Associated hydrocephalus• Preserving function e.g. vision

Malignant Malignant GliomaGlioma
Classification :Typing & GradingClassification :Typing & Grading
••WHO 1993 WHO 1993 •• KleihuesKleihues, Burger & , Burger & ScheithauerScheithauer
Grade I Grade I ‐‐ PilocyticPilocytic AstrocytomaAstrocytomaGrade II Grade II ‐‐ Low Grade Low Grade AstrocytomaAstrocytomaGrade III Grade III ‐‐ AnaplasticAnaplastic AstrocytomaAstrocytomaGrade IVGrade IV‐‐ GBM (GBM (GlioblastomaGlioblastoma Multiforme)Multiforme)
Prognosis & Median survivalPrognosis & Median survival
• Glioblastoma
• Anaplastic glioma
• Low grade glioma
• Pilocytic glioma
• 9 Months
• 2 Years
• Long
• Good
TreatmentTreatment
Surgery + RadiotherapySurgery + Radiotherapy+/+/‐‐ ChemotherapyChemotherapy

SurgerySurgery
• AIM :Maximal removal of tumor without production of new neurological deficit.
• Gross total• Subtotal (Debulking)• Biopsy : Open vs stereotactic
SurgerySurgery
• Histopathology• Immediate palliation• Oncological control (Cytoreduction)• Facilitate adjuvant therapies
SurgerySurgery
• Gross total resection
• Subtotal resection
Ammirati 1987
Median SurvivalMedian Survival• 90 weeks
• 43 weeks

SurgerySurgery
Benefit of radical surgery Benefit of radical surgery isis
Positive but modestPositive but modest
Minimal Invasive NeurosurgeryMinimal Invasive Neurosurgerywith Maximal Safetywith Maximal Safety
Awake CraniotomyAwake CraniotomyBrain MappingBrain Mapping
SubcorticalSubcortical
Cortical Cortical
Glioma
Infiltrative
Eloquent area
Tumor at eloquent area
• Maximal surgical removal
• Minimal neurological deficit

Contra‐indications
• Existing irreversible deficit– Hemiparesis– Dysphasia
• Children– Cooperation– Immature brain
Awake Patients ‐ Preparation
• Patient briefing & training– Psychological anticipation– Pain threshold– Intra‐operative sequence of events
fMRIfMRI –– RightRight handhand fMRIfMRI –– SpeechSpeech‐‐ReadingReading

fMRIfMRI –– SpeechSpeech‐‐NamingNaming
Images courtesy of Johann Wolfgang Goethe University Hospital, Frankfurt, Germany
MR Spectroscopy

Choice of TE
Cho Map
Cr Map
NAA Map
Formation of Metabolic Maps
CSI ‐ Example of CSI maps
Choline Map
NAA Map
Axial Survey
Normal Glioma
TE = 136 ms
TE = 272 ms
TE = 136 ms

(1) Image(1) Image‐‐NavigationNavigation

Motor mapping
• Usually no need for intra‐Op ECoG
• Localisation of central sulcus– Anatomy & Neuronavigation– Phase‐reversal SSEP
•Strip electrode
(2) (2) Phase Reversal SSEPPhase Reversal SSEP
11
22
33
44
(3) Direct Cortical Stimulation(3) Direct Cortical Stimulation Motor mappingMotor mapping
• Cortical stimulation– Ojemann Cortical Stimulator– Bipolar / biphasic stimulation– PW – 1ms– Frequency 60Hz– Current : 0.5mA to 15mA (Max. 20mA)– Stimulation probe parallel to gyrus– Stimulation of parafalcine cortex – Lower limb

Speech Mapping
• Intra-Op ECoG– GRASS EEG electrodes holder – “the Crown”– Maximal stimulation current– Seizure threshold – After-discharges (Ads)
• Counting• Naming
– Flash cards / Computer slides• Stimulation for 5 sec• Stimulations between every other sildes• Speech disturbance
– Speech arrest (Anomia)– Delay– Substitution with wrong name or mispronunciation
• Repeat for confirmation
這是
這是

這是
Intra‐Op Seizure
• Prevention– Adequate to high normal range of AED– Intra-Op ECoG for Ads
• Seizure abortion– Iced saline (4’C) applied to cortex– Methohexital– Midazolam
Video

Glioma SurgerySeeing the invisible
5‐ALA (5‐aminolevulinic acid)
• Elicits synthesis and accumulation of fluorescent porphyrins within malignant glioma tissue
• More complete resections of contrast‐enhancing tumour(OR 3.28 95% CI 1.99‐5.40, p<0.0001)
Walter Stummer et al. 2006
5-ALA
PpIX

Indication and contra‐I
Indication• Malignant glioma for gross / near‐gross total removal
• Expected minimum residual disease
Contra‐I• Porphyria/Pregnancy
• Debulking surgery• Pre‐existing fixed deficit
• Eloquent area (without mapping)
Usage
• 20mg/kg body weight• 3‐4 hours before surgery, orally• Active from 3rd ‐12th hr• Dark theatre : Ambient light : Neon tubes (red component)
• Photobleaching• Photosensitivity (24 hours)
Outcomes Assessment
• Primary outcomes– No. of patients without residual– 6‐month PFS
• Secondary outcomes– Post‐Op MRI residual volume– Overall survival– Neurological deficit– Toxic effects

Max. Rescetion vs Neurological deficit
• “It is the responsibility of the surgeon to decide how far he is prepared to remove fluorescing tissue”
• 5‐ALA fluorescence accumulation > contrast‐enhancement in MRI
Summary
5‐ALA is a surgical adjunct for maximum resection of malignant glioma.
However, it does not preserve function or avoid operative neurological deficit.
Instead it may increase the chance of neurological deficit in certain groups of patients without intra‐Op monitoring.

HK$2.5M
HK$25,000/1.5g HK~$561/g
Trained surgeon
Conclusion
• Maximal surgical removal of the maligantglioma provides modest benefit in survival and facilitates adjuvant therapies.
• Surgical risk should be balanced and neurological complications should be avoided as much as possible
• Awake craniotomy and cortical mapping is advised for tumor locating at or near eloquent cortex.
Intratumoral Chemotherapy
• Overcoming BBB• Increase local drug conc.• Minimizing systemic side effects• Sustain release drug for specific cell cycle phase
• Henry Brem 1995• Lancet• Prospective• Randomized• Placebo controlled• MS 31 vs 23 weeks

Local Chemotherapy ‐ Gliadel
• Biodegradable 1,3‐bis(2‐chloroethyl)‐1‐nitrosourea (BCNU) wafer
• Contains 3.85% BCNU to be release within 2‐3 weeks
• BCNU•Ability to cross blood‐brain barrier•Small fraction of dose at interested site with systemic
toxicity • Prospective multi-centre, double-blinded, placebo-controlled trial
• Dec 1997 - June 1999
• n = 240
2‐3 years follow‐up

A “local” oncologist
Is it worth doing?
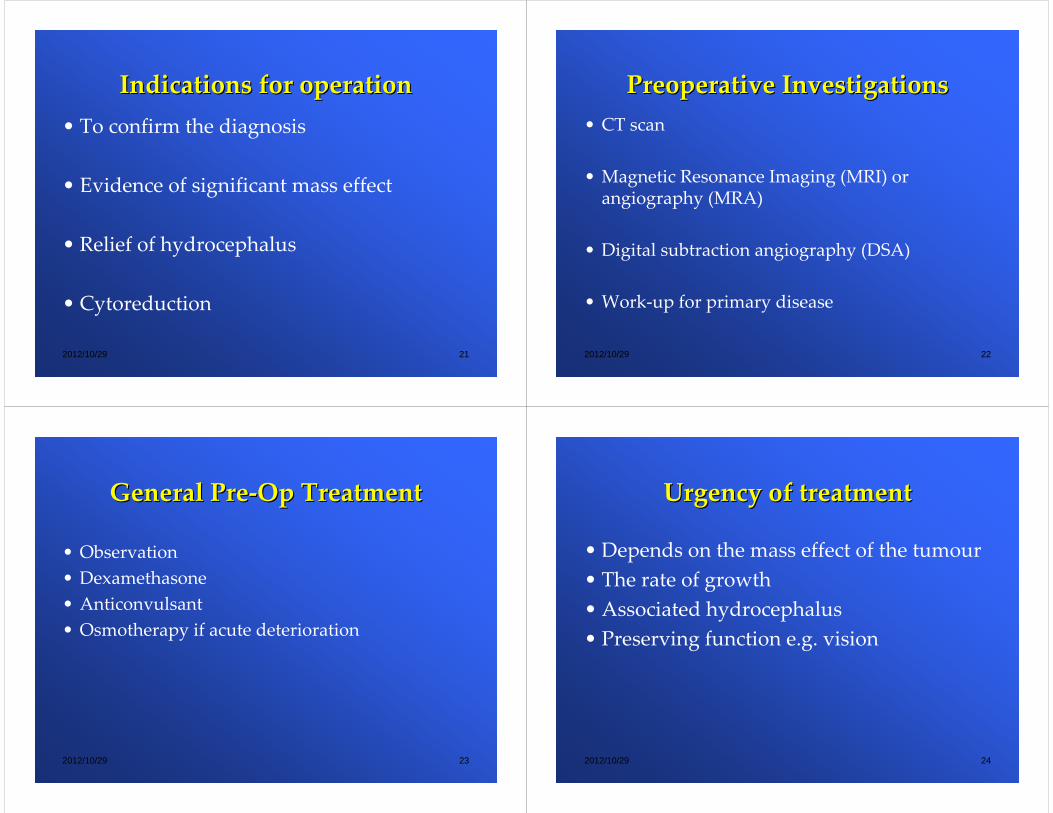
Brain Metastasis
BrainBrain
MetastasisMetastasis
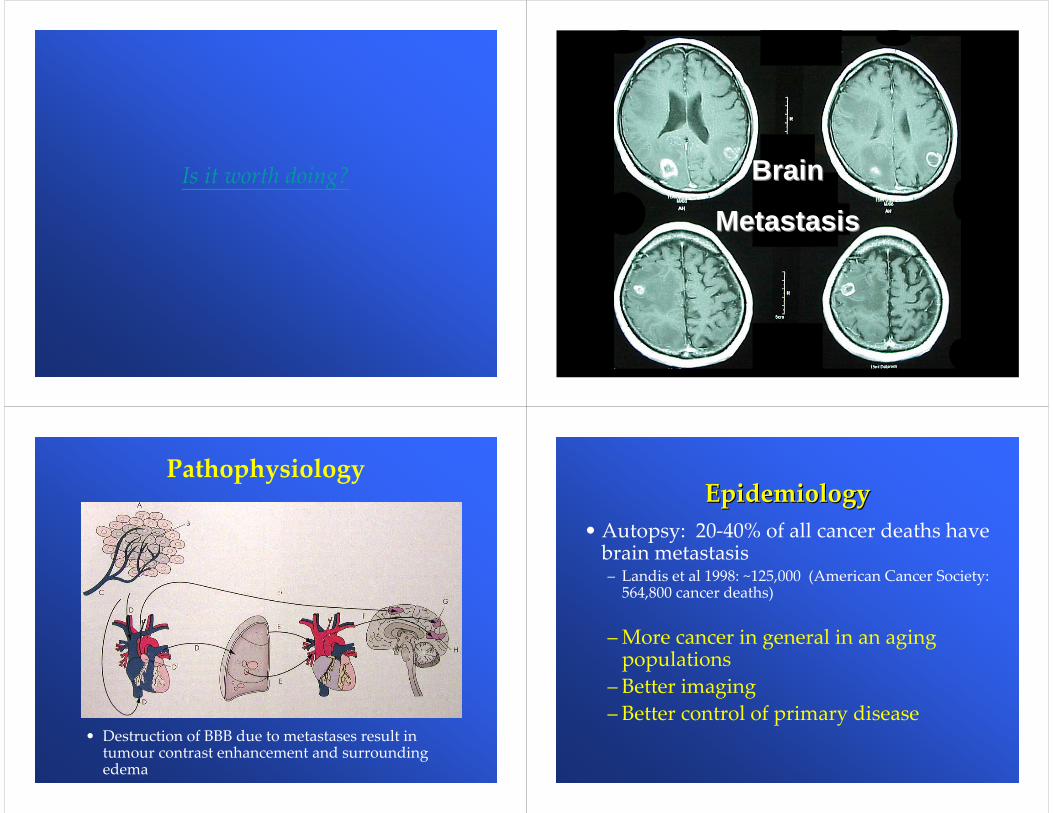
Pathophysiology
• Destruction of BBB due to metastases result in tumour contrast enhancement and surrounding edema
EpidemiologyEpidemiology• Autopsy: 20‐40% of all cancer deaths have brain metastasis– Landis et al 1998: ~125,000 (American Cancer Society: 564,800 cancer deaths)
– More cancer in general in an aging populations
– Better imaging– Better control of primary disease

Primary TumourPrimary Tumour
• Relative multiplicity of brain metastasis varies with primary tumour
• Overall 30‐40% are solitary
19Breast13Melanoma4Renal1Unknown primary
25Others100Total
38Lung
% of brain metastasisPrimary tumour
Localization of metastatic Localization of metastatic tumorstumors
•Tumor emboli :80% in cerebrum, 15% in posterior fossa, 5% in brainstem•“Soil & seed”
SymptomsSymptoms
~ 40%Hemiparesis14%Cognitive impairment
12%Seizure7%Ataxia
16%Others~7%No symptom
40 - 50%Headache% of patientsSymptoms
•Up to two-third of all metastases are symptomatic at some time in life, due to raise ICP or neuronal damage•15% of cancer firstly presented with brain metastasis
Radiation Therapy Oncology Radiation Therapy Oncology Group (RTOG)Group (RTOG)
• 1200 patients from 1979‐1993 (WBI)–– Recursive Prognostic Analysis (RPA)Recursive Prognostic Analysis (RPA)
• a statistical methodology which creates a regression tree according to prognostic significant
KPS <702.3 months3Not class 1 or 34.2 months2
KPS >= 70Controlled primary disease
Age < 65No systemic metastasis
7.1 months1
PatientsMedian SurvivalClass

Aggressive TreatmentsAggressive Treatments• Aggressive treatment with RS, MS, WBI
– Pollock BE J Neurooncol.2003– 52 patients from 1997‐2000
• Age: 58 y.o.; KPS: 90; Tumour no.: 3– Overall medium survival : 15.5 months– One year: 63% ; Two years: 27%– Class 1 : 19 months – Class 2 : 13 months – Class 3 : 8 months
SuggestionAggressive treatments to class 1 and 2 patientswith controlled primary and limited no. of brain
metastasis
Aggressive TreatmentsAggressive Treatments• Surgical resection + WBI
• Radiosurgery
• Until the 1990s, the role of surgical resection versus WBI for treatment of Single brain metastasis was an area of debate.
WBI or Surgery?WBI or Surgery?• Vecht CJ Ann Neurol 1993• Prospective randomized trial• 63 patients with single metastasis, stratified
9 months4 monthsFunctional independent survival
12 months7 monthsMedian survival
Surgery + WBI
WBI alone
Patient with progressive extracranial cancer carry poor survival (5 months) irrespective of treatment
Functional statusFunctional status improve rapid and longer than WBI

Surgery +/Surgery +/‐‐WBIWBI• Patchell RA (JAMA 1998)• Randomized trial:
– 95 patients post-op. :
– However, there’s no survival benefit
17/39 (44%)6/43 (14%)Death due to CNS cause17(37%)7(14%)other site21(46%)5 (10%)original site
32 (70%)9 (18%)Intracranial recurrence
Observe (46)WBI (49)
Stereotactic RadiosurgeryStereotactic Radiosurgery
Stereotactic RadiosurgeryStereotactic Radiosurgery
1. Stereotactic co‐ordinate system • Rigid head‐mounted frame• MRI / CT / DSA
2. Deliver single high dose radiation accurately focusing at the target• Rapid radiation dose fall off at boundary
Radiosurgery-Lethal hit vs Radiotherapy-Diff. repair
Stereotactic Radiosurgery – SRSStereotactic Radiotherapy – SRTConventional Radiotherapy

Types of RadiosurgeryTypes of Radiosurgery
• Gamma knife – Cobalt 60
• Linear Accelerator (LINAC)
Current PracticeCurrent Practice• Treatment for resectable small (< 3cm) single brain
metastasis is still under debate• Awaiting prospective randomized trial
Risk of haemorrhage
Chemotherapy
Non-tolerateTolerate operationSystemic condition
AsymptomaticSymptomaticSymptomEloquentNon-eloquentLocation
<3cmLargeSize
RadiosurgerySurgery
Overall SurvivalOverall Survival
• Natural history: 1 month• With Steroid: 2 months• WBI: 3‐6 months• Surgery + WBI: 8‐12 months• Radiosurgery: 7‐12 months

Meningioma
• Commonest benign brain tumor• Arachnoid cap cell• Extra‐axial / shape margin / “dural tail”• Calcification / Hyperostosis• Locations
– Convexity / Parafalcine / Parasagittal– Olfactory groove / Sphenoidal ridge / Tentorial
Meningioma
Treatment for Meningioma
• Expectant policy
• Surgery
• Radiotherapy
Simpson Grade1. Total + Dura 9%2. Total + Coagulation 19%3. Total 29%4. Partial removal ~50%5. Biopsy >50%
Pituitary Tumor
• Anterior pituitary gland– TSH,ACTH,GH,FSH/LH,Prolactin
• Posterior pituitary gland– ADH, Oxytocin

Anatomy of pituitary gland
Optic chiasm
Carotid artery
CN
III
IV
V12
VI
Cavernous sinus
Sphenoid sinus
III ventricle
Anatomy of pituitary gland
Pituitary tumor
• Mass effect– Optic chiasm – Bitemporal hemianopsia– Third ventricle – hydrocephalus– Cranial nerves – III,IV,V,VI
• Hormonal disturbance– Functioning tumor– Non‐functioning tumor
Functioning tumor
• TSH• GH• ACTH• Prolactin• FSH/LH
• Hyperthyoridism• Acromegaly• Cushing disease• Galactorrhoea• rare

Acromegaly
DM / HT
Cardiomegaly
Carpal tunnel syndrome
Joints degeneration
Transphenoidal Surgery
2012/10/29 119
Transphenoidal approach for Pituitary tumour
2012/10/29 120
Acoustic Neuroma
• Benign tumour• arise from VIII nerve (Vestibular schwannoma)
• Difficult surgical assess
• Hearing loss

Acoustic Neuroma Acoustic Neuroma
• Hearing loss / Tinnitus / Dysequilibrium• Facial numbness / weakness• Abnormal corneal reflex / Nystagmus• Facial palsy (Rarely pre‐Op)
Treatment for Acoustic neuroma
• Expectant policy
• Radiation therapy
• Surgery
• Symptoms (Hearing)
• Size & Growth rate
• Patients
Neurofibromatosis type‐2 (NF2)
• Bilateral acoustic neuroma
• Chr. 22• Neurofibroma• Meningioma• Glioma• Schwannoma• Pheochromocytoma

The End