claudio micheletto, md, f ccp r espiratory m edicine m ater s alutis hospital – legnago - vr e...
TRANSCRIPT

CLAUDIO MICHELETTO, MD, FCLAUDIO MICHELETTO, MD, FCCPCCPRRESPIRATORY ESPIRATORY MMEDICINEEDICINE
MMater ater SSalutis Hospitalalutis Hospital – Legnago - VR – Legnago - VR
EEARLY ARLY Diagnosis of COPD.Diagnosis of COPD.The COPD Alliance ModelThe COPD Alliance Model
ACCP Italian Delegate MeetingACCP Italian Delegate MeetingCOPD Early Diagnosis, Early TreatmentCOPD Early Diagnosis, Early Treatment
Using the Best FirstUsing the Best First

Conflict of interest disclosureConflict of interest disclosure
I have no, real or perceived, conflict of interest that relate to this presentation


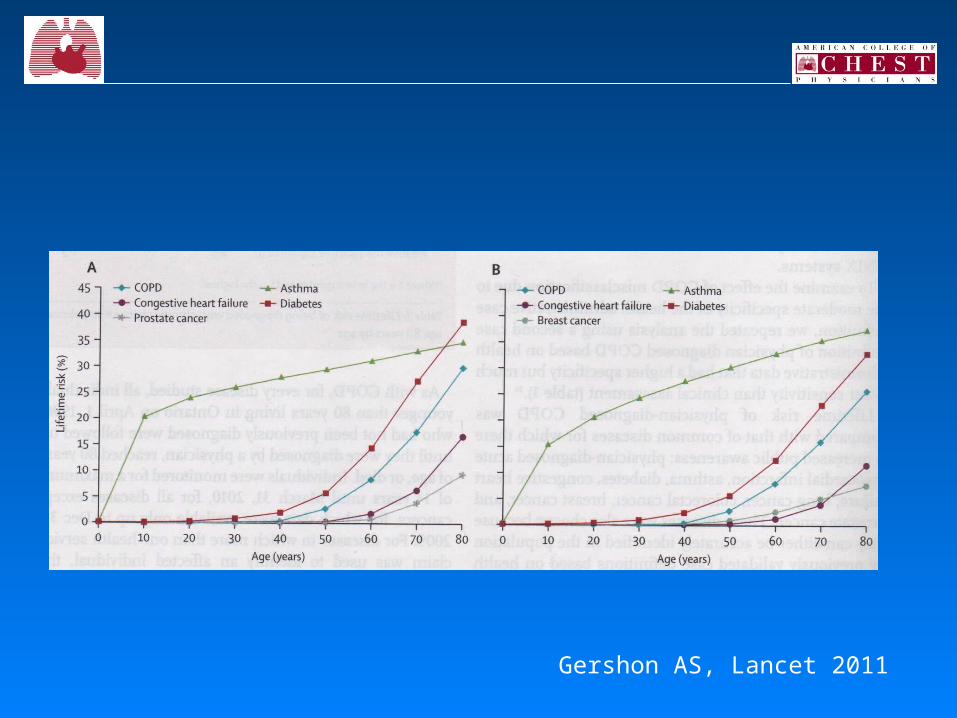
Lifetime risk of COPD with highly sensitiveand highly specific case definition
13 022 536 individuals lived in Ontario at the time of the studyLifetime risk of physicians-diagnosed COPD was
27.6 %27.6 %
Gershon AS, Lancet 2011
Gershon AS, Lancet 2011

Soriano JB, Zielinski J, Price D. Lancet 2009; 374: 721-32

Underdiagnosis of COPDUnderdiagnosis of COPD
Criteria of COPDCriteria of COPD Diagnosed (%)Diagnosed (%)
• NHANES III, USA BTS 37
• IBERPOC, Spain ERS 22
• DIMCA, Netherlands CNSLD 35
• OLIN, Sweden BTS 31
• An European
assumption clinical 25
Though being symptomatic, only a half of the subjects with severe COPDare properly labelled;
COPD is usually NOT DIAGNOSED until it is clinically apparent and already advanced.
Lindberg A, et al. Resp Med 2005; 100: 264-72

Trends in Age-Standardized Death Rates for the 6 Leading Causes of Death in the United States, 1970-2002 Rates are age-adjusted to the 2000 US standard population.
Jemal, A. et al. JAMA 2005;294:1255-1259

Prevalence and underdiagnosis of chronic obstructive Prevalence and underdiagnosis of chronic obstructive pulmonary disease among patients at risk in primary carepulmonary disease among patients at risk in primary care
We suoght to measure the prevalence of spirometrically confirmed COPD in an at-risk population of adults aged 40 years or more with a smoking history of at least 20 pack-years who visited a primary care practioner for any reason and to describe their characteristics.
Hill K, Goldstein RS, Guyatt GH et al. Can Med Ass J 2010; 182 (7), 673-678
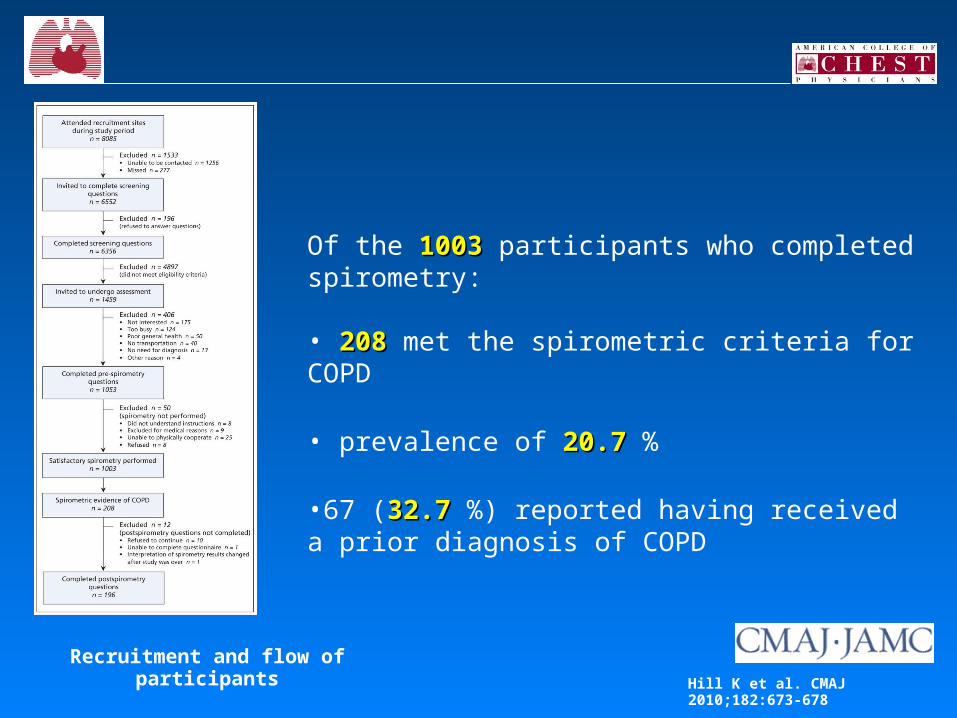
Recruitment and flow of participantsHill K et al. CMAJ 2010;182:673-678
Of the 10031003 participants who completed spirometry:
• 208208 met the spirometric criteria for COPD
• prevalence of 20.720.7 %
•67 (32.7 32.7 %) reported having received a prior diagnosis of COPD

Prevalence and underdiagnosis of chronic obstructive Prevalence and underdiagnosis of chronic obstructive pulmonary disease among patients at risk in primary carepulmonary disease among patients at risk in primary care
Among adult patients visiting a primary care practitioner, as many as one in five with known risk factors met spirometric criteria for COPD.
Although more than three-quarters of the patients with COPD reported at least one respiratory symptom, two-thirds were unaware of their diagnosis.
These findings suggest that adults who attend a primary care practice with known risk factors for COPD are important targets for screening and early intervention.
Hill K, Goldstein RS, Guyatt GH et al. Can Med Ass J 2010; 182 (7), 673-678

• 60%60% of patients usually visited their of patients usually visited their GPGP for COPD for COPD (an average of (an average of 3 visits/patient3 visits/patient) in the last 12 months;) in the last 12 months;
• > 40%> 40% of patients were under the care of a of patients were under the care of a specialistspecialist (an average of 1.2 visits/patient) in the same period;(an average of 1.2 visits/patient) in the same period; • 19%19% of total of total visitsvisits were were unscheduledunscheduled;;
• 11%11% of patients were of patients were hospitalizedhospitalized during the last 12 months during the last 12 months (n=130 hospitalizations, such as (n=130 hospitalizations, such as 3 episodes/patient); 3 episodes/patient);
• 6%6% visited the visited the ERER;;
Dal Negro R. et al. Resp Med 2003; 97 :S43-50
Confronting COPD. Italian dataConfronting COPD. Italian data
Diagnosis of COPD or chronic bronchitisDiagnosis of COPD or chronic bronchitis

• 35%35% of patients were of patients were currentlycurrently receiving prescription receiving prescription medicationsmedications, namely ICS; theophylline, short-acting , namely ICS; theophylline, short-acting beta-2 agonists;beta-2 agonists;
• 50% 50% of patients received of patients received antibioticsantibiotics (up to 20 (up to 20 courses) in the last 12 months;courses) in the last 12 months;
• mostmost of treatments were of treatments were unrespectiveunrespective of int. guidelines of int. guidelines
Dal Negro R, et al. Resp Med 2003; 97 :S43-50

Dal Negro R, et al. Respir Med 2003

COPD management in primary care, what are the challenges ?
• Prevention
• Earlier and more accurate diagnosis
• More accurate assessment and phenotyping
• Appropriate therapeutic intervention
• Early improved pathways of care

Screening Case-Screening Case-FindingFinding
A “man on the street” Patient being seen by a physician
May not have symptoms Has respiratory symptoms
May be a cigarette smoker Has COPD risk factors
No cost and no reimbursement Medicare will pay $ 20 fo the test
Enright P, Kaminsky D. Resp Care 2003; 48 (12): 1194-1201

Criteria for early detection of diseaseCriteria for early detection of disease
1. The disease would progress and cause substantial morbidity or mortality
2. Treatment is available and is more effective when used at the early stage
3. There is a feasible, affordable, safe, and relatively simple testing method that is accurate enough to avoid producing large number of false-positive or false-negative results
4. There is an action plan that minimizes adverse effects
Marshall KG. CMAJ 1996; 154 (10): 1493-1499

Criteria for early detection of diseaseCriteria for early detection of disease
1. The disease would progress and cause substantial morbidity or mortality
2. Treatment is available and is more effective when used at the early stage
3.3. There is a feasible, affordable, safe, and relatively There is a feasible, affordable, safe, and relatively simple testing method that is accurate enough to simple testing method that is accurate enough to avoid producing large number of false-positive or avoid producing large number of false-positive or false-negative resultsfalse-negative results
4. There is an action plan that minimizes adverse effects
Marshall KG. CMAJ 1996; 154 (10): 1493-1499

spirometry is a:
• reliablereliable
• simplesimple
• non-invasivenon-invasive
• safesafe
• non-expensive procedurenon-expensive procedure
for detection of airflow obstruction

Soriano JB, Zielinski J, Price D. Lancet 2009; 374: 721-32

Diagnose COPD: assessment of severity
• Assess severity of airflow obstruction using reduction in FEV1
NICE clinical
guideline 12 (2004)
ATS/ERS 2004
GOLD 2008 NICE clinical guideline 101
(2010)
Post-bronchodilator
FEV1/FVC
FEV1 % predicted
Post-bronchodilator
Post-bronchodilator
Post-bronchodilator
< 0.7 80% Mild Stage 1 (mild) Stage 1 (mild)*
< 0.7 50–79% Mild Moderate Stage 2 (moderate)
Stage 2 (moderate)
< 0.7 30–49% Moderate Severe Stage 3 (severe)
Stage 3 (severe)
< 0.7 < 30% Severe Very severe Stage 4 (very severe)**
Stage 4 (very severe)**
* Symptoms should be present to diagnose COPD in people with mild airflow obstruction** Or FEV1 < 50% with respiratory failure
[new 2010]
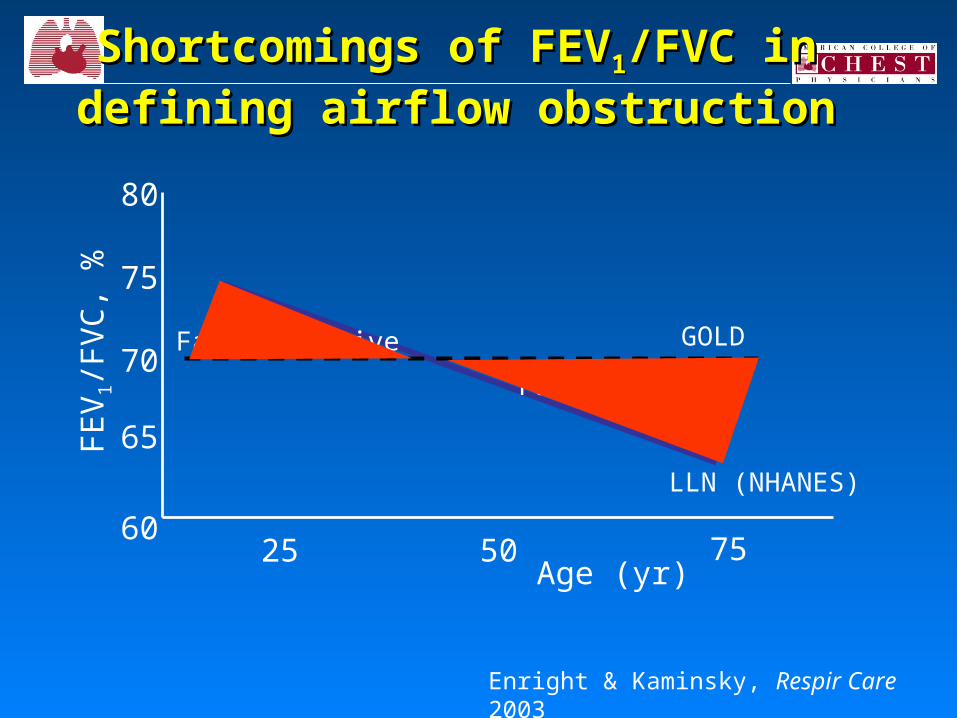
Shortcomings of FEVShortcomings of FEV11/FVC in /FVC in
defining airflow obstructiondefining airflow obstruction
Enright & Kaminsky, Respir Care 2003
25 50 75Age (yr)
FE
V1/F
VC
, %
GOLD
LLN (NHANES)
False positive
False negative
60
65
70
75
80

Lamprecht B, et al. Pulm Med 2011; 1, 1-6
24.224.2 %%
15.3 %15.3 %

Lamprecht B, et al. Pulm Med 2011; 1, 1-6

Distribution of overdiagnosed and severity levels of COPDDistribution of overdiagnosed and severity levels of COPD according to sex and age group.according to sex and age group.
García-Rio F et al. Chest 2011;139:1072-1080
The overdiagnosis of COPDaffected 4.64.6 % % of subjects aged40 to 80 years

Ways to reduce spurious prevalence of Ways to reduce spurious prevalence of COPD using GOLD criteriaCOPD using GOLD criteria
1.Only testing people with a high pre-test probability of COPD (clinical diagnosis, smoking history)
2.Confirming that airway obstruction persists after inhaling a bronchodilator (post-BD FEV1)
3.Requiring that the FEV1 be <80% of predicted (i.e., GOLD II or more)


Barriers to performing spirometry in a community setting:Barriers to performing spirometry in a community setting:
• Lack of access to calibrated spirometers
• Inadequate training in performing spirometry
• Lack of quality-control systems to ensure accurate results
• Inadequate interpretation skills among health professionals performing the test
Price D, et al. Prim Care Resp J 2009; 18 (3): 216-23
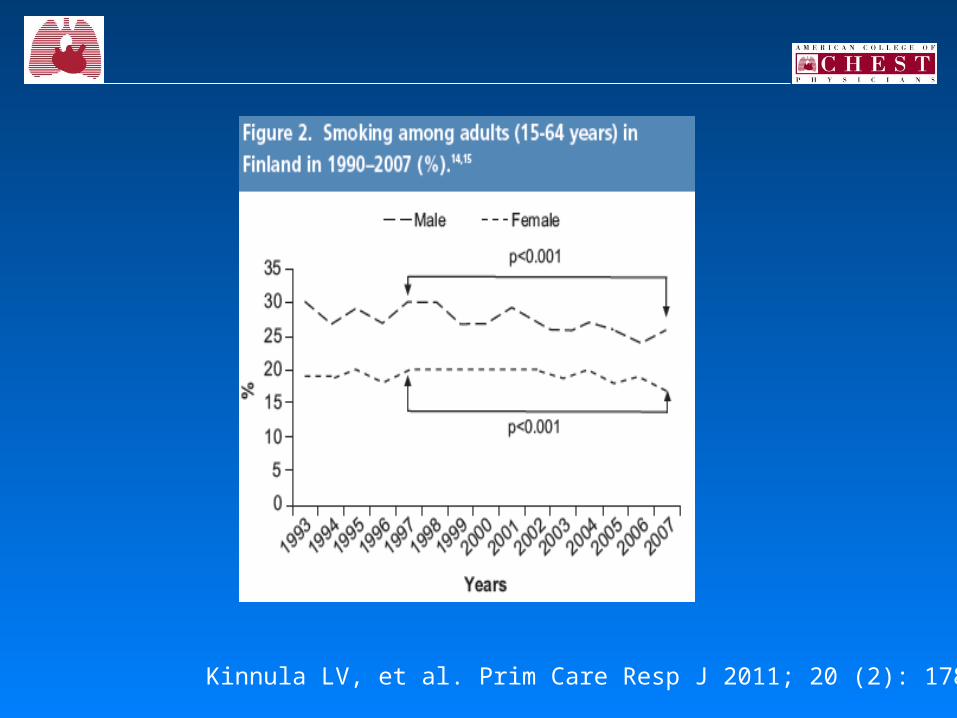
The 10-year COPD programme in Finland: effects on quality of
diagnosis, smoking prevalence, hospital admissions and mortality
Kinnula LV, et al. Prim Care Resp J 2011; 20 (2): 178-83
The major aims of this 10-year Programme in Finland, a country with a population of 5 million, included:
1. A reduction in COPD prevalence2. Improvement in COPD diagnosis, especially in primary care3. A reduction in the number of moderate to severe cases of
the disease4. Reduction in the number of COPD-related hospitalisations5. Reduction in treatment costs due to COPD

Kinnula LV, et al. Prim Care Resp J 2011; 20 (2): 178-83
Kinnula LV, et al. Prim Care Resp J 2011; 20 (2): 178-83

- 52.9 %- 52.9 %

Recent trends in COPD prevalence in Spain: a repeated cross-sectional
survey 1997-2007
IBERPOC 1997
EPISCAN 2007
Underdiagnosis 78 % 73 % Same
Undertreatment 81 % 54 % BetterBetter
Undertreatment in severe COPD
50 % 10 % BetterBetter
Previous spirometry ? 17 % 59 % BetterBetter
Soriano JB, et al. Eur Resp J 2010; 36: 758-765

Recent trends in COPD prevalence in Spain: a repeated cross-sectional survey 1997-2007
• To further reduce underdiagnosis, the implementation and wider use of spirometry screening in all setting, including quality spirometry in primary care, pharmacies, and elsewhere, require further research and resources.
Soriano JB, et al. Eur Resp J 2010; 36: 758-765

Early detection of COPD in general practice
Ulrich SC, et al. Int J of COPD 2011

Feasibility and validation of telespirometry in general practice: the Italian Alliance study
• 70 %70 % of the test met the criteria for good or partial co-operation, allowing spirometric abnormalities to be detected in more than 40 % of the tracing
• The rate of telespirometries that could not be evaluated at all was reasonably low (9.29.2 %%)
Bonavia M, et al. Resp Med 2009

Office spirometry can improve the diagnosis of obstructive airway disease
in primary care setting
• 9312 subjects were recruited and 7262 (7878 %%) performed an acceptable telespirometric examination
• Among symptomatic subjects, 1433/3725 (3838 %%) had abnormal spirometries (682 with moderate to severe obstruction)
Averame G, et al. Respir Med 2009

MissionMission
• The COPD Alliance was formed to provide primary care clinicians with timely information, tools, and support to facilitate the recognition, diagnosis, and treatment of COPD.
• We are composed of multidisciplinary societies and corporations whose commitment is to help primary care clinicians improve their patients’ quality of life through early recognition and management of COPD.

Founding members
• Five health-care societies, representing over 300,000 primary care and specialty clinicians, have partnered together in the fight against COPD. The promise of the COPD Alliance to its clinicians, patients, and partners is to facilitate appropriate identification, diagnosis, and management of COPD. We are committed to making a difference today where it matters most—in the health of our patients

Founding members
• AANPAANP AMERICAN ACADEMY OF NURSE PRACTITIONERS WWW.AANP.ORG
• AAPAAAPA AMERICAN ACADEMY OF PHYSICIAN ASSISTANTS WWW.AAPA.ORG
• ACCP ACCP AMERICAN COLLEGE OF CHEST PHYSICIANS WWW.CHESTNET.ORG
• ACOFP ACOFP AMERICAN COLLEGE OF OSTEOPATHIC FAMILY PHYSICIANS WWW.ACOFP.ORG
• ACOI ACOI AMERICAN COLLEGE OF OSTEOPATHIC INTERNISTS WWW.ACOI.ORG

The COPD Alliance’s unified voice promotes early diagnosis ofCOPD through enhanced awareness and understanding of thispreventable and treatable disease utilizing the acronym STEP:
SS Screen patients at risk
TT Test and diagnose utilizing spirometry when indicated
EE Educate patients about COPD
PP Provide appropriate medical care and support
All Clinicians are encouraged to STEP forward in the fightagainst COPD—the fourth leading cause of deathin the United States.

Four Easy STEPs to become COPD Prepared
To support clinicians in the four-STEP process for the recognition, diagnosis, and treatment of COPD, the COPD Alliance offers a variety of free tools, resources, and education programs.

•The resources include a COPD patient screening tool, the Tobacco Dependence Treatment ToolKit, information regarding spirometry, and several patient education guides that clinicians can download and distribute to patients in their offices.
•We invite you to explore these valuable resources by clicking on any of the quadrants of the four stages of STEP below.
COPD ALLIANCECOPD ALLIANCE
Spirometry is an important tool in diagnosing COPD ?Spirometry is an important tool in diagnosing COPD ?
• Confirm a diagnosis of COPD
• Show the severity of your patient’s COPD
• Help you decide what medicines and health instructions are appropriate for your patient
• Show how well the prescribed treatment and disease management activities are working

How to screen for the risk of COPDHow to screen for the risk of COPD The COPD AllianceThe COPD Alliance11 recommends the utilization of a recommends the utilization of a
simple validatedsimple validated22 questionnaire questionnaire that can help that can help identify people age ≥35 identify people age ≥35 who are at risk for who are at risk for COPD COPD
A downloadable version entitled, A downloadable version entitled, COPD Population Screener COPD Population ScreenerTMTM can be found can be found on www.COPD.orgon www.COPD.org
Persons that are deemed to Persons that are deemed to be at risk should be asked to be at risk should be asked to complete the screener while in the complete the screener while in the waiting room waiting room1The COPD Alliance is composed of multidisciplinary societies, i.e., AANP, AAPA, ACCP, ACOFP, ACOI2 Martinez FJ et al. COPD.2008;5(2):85-95


EducateEducate
It is essential that you take the time to educate your patients about COPD, including symptoms, diagnosis, and how to live better with the disease.Use the following resources to help your patients learn more about COPD: A BREATH OF FRESH AIR: LIVING WITHCOPDPATIENTS GUIDES FOR COPDSPIROMETRY DEMONSTRATION VIDEO

Resources for the clinicians
The COPD Alliance provides access to the following COPD resources for clinicians and their patients, many of which are free and available for download:
COPD Population ScreenerTMThis validated COPD screening tool uses five questions to determine a patient’s risk
for COPD and the potential need for spirometry testing. The screener is available in English and Spanish.
Tobacco Dependence Treatment ToolKitHelp your patients stop smoking with the updated Tobacco Dependence Treatment
ToolKit from the American College of Chest Physicians. This user-friendly, interactive collection of tools will help you implement a proven approach to treating tobacco dependence. Online features include instruments for patient assessment, a video presentation on helping your patients, and multiple search options.
GOLD GuidelinesThe Gold Guidelines provide comprehensive, evidence-based guidelines for COPD
diagnosis, management, and prevention.Spirometry DemonstrationThis 5-minute instructional video shows patients and coaches how to perform a
spirometry test.
Copd.orgCopd.org
Resources for the clinicians
COPD: Importance of Early Diagnosis The following downloadable slides can be used by clinicians to highlight
the importance of early diagnosis for COPD, and how and when to screen patients for COPD.
Download slidesA Breath of Fresh Air: Living With COPDLiving With COPD is a "virtual flip chart" created by expert clinicians from
the American Academy of Nurse Practitioners. The flip chart includes content to support the counseling of patients diagnosed with COPD or at risk for the disease. Flip chart materials, including handouts, can be downloaded for use on a computer or tablet.
Download Flip chart »The Changing Face of COPDA public service announcement (PSA) illustrates how the face of COPD is
changing and how primary care clinicians can help uncover the disease by asking the right questions.
View Video »
Resources for the patients
• The COPD Alliance provides access to the following COPD resources for clinicians and their patients, many of which are free and available for download.
• COPD Population ScreenerTM• This validated COPD screening tool uses five questions to
determine a patient’s risk for COPD and the potential need for spirometry testing. The screener is available in English and Spanish.
• View Screener »• Patient Guides for COPD• These unbranded patient guides offer valuable and easy-to-
understand information about understanding the diagnosis of COPD, managing the disease through diet and exercise, smoking cessation, and more.
• View Guides »• © 2011 COPD Alliance

“ Primary care clinicians are the gatekeepers for our health. If they are unable to recognize the signs of COPD or high-risk individuals, the disease may
remain undiagnosed and, consequently, the patient
will not receive appropriate treatment.
By educating our primary care clinicians, we give them the tools
to identify high-risk patients, confirm a diagnosis of COPD,
and provide initial treatment”
Brian Carlin, MD, FCCP Chair, COPD Alliance
Thank you foryour attention