cleveland clinic retiree health plan total care
TRANSCRIPT
Cleveland Clinic
Cleveland ClinicRetiree Health PlanTotal CareSummary Plan Description

Your Guide toQuality Healthcare Services
and Healthier LivingWelcome to Cleveland Clinic Retiree Health Plan (RHP) Total Care. As a ClevelandClinic or Regional hospital employee, you have access to some of the very besthealthcare services in the world. To help you understand the healthcare servicesand benefits available to you under this health plan, EHP Total Care developedthis Summary Plan Description (SPD), which is updated as necessary. QuarterlyHealthWise Bulletins are also sent to members informing them of any health planupdates throughout the year.
The Cleveland Clinic Retiree Health Plan Total Care SPD is the health plan document.There are no other documents to reference when determining health plan coverage.We encourage you to take the time to read it carefully and to file for future reference.Summary Plan Description information is also available on the Cleveland Clinicwebsite at www.clevelandclinic.org/healthplan.
Begin with Section One: “Getting Started,” and then review the rest of the SPD tofind helpful information about:
• Medical and behavioral health benefits;
• Prescription drug benefits;
• Network providers;
• Medical and behavioral health case coordination;
• Pharmacy Coordination programs;
• The Third-Party Administrator and coordination of benefits;
• The Medicare prescription drug benefit and eligibility;
• Administrative and enrollment procedures; and
• Customer service.
Refer to the back of this booklet for detailed definitions of the terms used throughoutthe SPD. If you have any questions, refer to the RHP Total Care Quick ReferenceGuide on page 9 in Section One: “Getting Started” for appropriate phone numbersand addresses.
This is your guide to quality healthcare services and healthier living. Qualityhealthcare is everybody’s responsibility. We encourage you to pursue a lifestyle ofhealthy living. Cleveland Clinic Employee Health Plan Total Care looks forward toassisting you with your healthcare needs.
iii

Table of ContentsSection One GETTING STARTEDCleveland Clinic Retiree Health Plan Total Care Mission . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Coordination of Benefits (COB) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
COB Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1COB Form Sample . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Two-Tiered Provider Network . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2RHP Total Care Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Medical and Behavioral Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Prescription Drug Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
RHP Total Care Benefits Summary Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Non-Medicare Eligible RHP Total Care Prescription Drug Benefit Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Medicare Eligible RHP Total Care Prescription Drug Benefit Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Accurate Registration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Claims Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Communication and Service . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Customer Service Unit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Medical Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Life Event Changes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8RHP Total Care Quick Reference Guide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Section Two TIERED NETWORK OF PROVIDERSTwo-Tier Network . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Tier 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Tier 1 Hospitals in the Cleveland Clinic RHP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Other Cleveland Clinic Ambulatory Facilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Tier 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Section Three HEALTH PLAN COVERAGECleveland Clinic Retiree Health Plan Total Care Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14EHP Total Care Medical Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Utilization Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Prior Authorization and Concurrent Review for Clinical Appropriateness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Prior Authorization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Member Responsibility for Prior Authorization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Concurrent Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Member Responsibility for Concurrent Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Medical and Behavioral Health Services That Require Prior Authorization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Inpatient Services (both Medical and Behavioral Health) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Outpatient Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Special Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Pharmaceuticals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Care Outside of Tier 1 Cleveland Clinic RHP Total Care Network of Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Benefits Coverage Clarification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Services That Must Be Provided by RHP Total Care Tier 1 Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Coverage Clarification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Behavioral Health Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
ADHD Summer Treatment Program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Autism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Full Spectrum Light Boxes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Intensive Home-Based Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Pain Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Psychological and Neuro-psychological Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Psychological Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Neuro-psychological Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
v
Section Three HEALTH PLAN COVERAGE (continued)Behavioral Health Services (continued)
Residential Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Medical Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Bariatric Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Botox for Migraine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Breast Reconstruction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Cataract Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Chiropractic Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Contact Lenses and Lens Fittings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Cosmetic Surgery Combined with Clinically Appropriate Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Dental . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25DXA Scans (Bone Density) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Durable Medical Equipment (DME) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Emergency Care/Transfers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Transfers from Within a 50-Mile Radius of the Cleveland Clinic Main Campus . . . . . . . . . . . . . . . . . . . . . . . . . . 26Transfers from Outside a 50-Mile Radius of the Cleveland Clinic Main Campus . . . . . . . . . . . . . . . . . . . . . . . . . 26
Enteral Feedings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Genetic Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Hair Loss . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Hearing Aids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Hospice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Immunizations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Infertility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Infusion for Migraine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27IUD and Depo-Provera Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Maternity Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Orthotics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Pain Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28PAP/HPV Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Personal Grooming . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28RAST (Allergy Blood) Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Routine (Annual) Vision Examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Spider Veins and Varicose Veins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Temporomandibular Joint Syndrome (TMJ) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Occupational . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Physical . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Speech . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Vestibular Testing Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Case Coordination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Coordinated Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Chronic Disease Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Asthma (for adults and children) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Chronic Kidney Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Depression (for adults and children) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Diabetes (for adults and children) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Heart Failure (CHF) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Hyperlipidemia (High Cholesterol) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Hypertension (High Blood Pressure) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Migraine (for adults and children) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Health Promotion Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Pre-Diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Prenatal Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Rare Disease Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Prescription Drug Coverage Under Medicare . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
vi

Section Three HEALTH PLAN COVERAGE (continued)Prescription Drug Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Cleveland Clinic Retiree Health Plan Total Care Coverage Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
General Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Medical Coverage Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Behavioral Health Coverage Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Prescription Drug Benefit Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Section Four THIRD-PARTY ADMINISTRATOR — MUTUAL HEALTH SERVICESCleveland Clinic Retiree Health Plan Total CareThird-Party Administrator (TPA) Mutual Health Services (MHS) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Coordination of Benefits (COB) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Medicare Coordination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Process for Determining Which Health Plan Is Primary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39How the TPA Pays as Primary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39How the TPA Pays as Secondary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Enforcement of Coordination of Benefits (COB) Provision . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Facility of Payment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Right of Recovery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Coordination Disputes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
Claims Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Explanation of Benefits (EOB) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
The Coded Explanations for EOB Sample . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Section Five ADMINISTRATIVE INFORMATIONThe Registration Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Eligibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Coverage Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Dependents Eligible for Coverage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Eligibility Verification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
New Enrollees . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Domestic Partners . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Health Benefit Enrollment Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Retiree Contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Plan Identification Card . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Life Event Changes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Continuation of Coverage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Consolidated Omnibus Budget Reconciliation Act (COBRA) Coverage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Qualifying Events: Who, When, and for How Long . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45When Continued Coverage Ends . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46How to Obtain Coverage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
Termination of Coverage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
Section Six RHP MEMBERS’ RIGHTS AND RESPONSIBILITIESBenefit Determination for Claims . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Urgent Care Claims . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Concurrent Care Claims . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Pre-Service Claims . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48Post-Service Claims . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48Benefit Determination Notices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
Filing a Complaint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49Appeals Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Expedited Review Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49Filing an Appeal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
vii

viii
Section Six RHP MEMBERS’ RIGHTS AND RESPONSIBILITIES (continued)Appeals Process (continued)
First Level Mandatory Appeal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50Urgent Care Appeal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51Pre-Service Claim Appeal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51Post-Service Claim Appeal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Appeal Denial Notices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51Second Level of Appeal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51Time Periods for Making Decision on Appeals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
External Review Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53External Review for Non-Urgent Care Claims Appeals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53Expedited External Review for Urgent Care Claim Appeals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Reimbursement and Subrogation Rights of the Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54The Health Insurance Portability and Accountability Act of 1996 (HIPAA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56Employee Retirement Income Security Act of 1974 (ERISA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
About the Cleveland Clinic Retiree Health Plan (RHP) Total Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56Future of Cleveland Clinic Retiree Health Plan (RHP) Total Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
A Statement of Your Rights Under ERISA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57Receive Information About Your Plan and Benefits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57Continue Group Health Plan Coverage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57Reduction or Elimination of Exclusionary Periods of Coverage for Pre-existing ConditionsUnder Your Group Health Plan if You Have Creditable Coverage from Another Plan . . . . . . . . . . . . . . . . . . . . . . . . . 57Prudent Actions by Plan Fiduciaries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58Enforce Your Rights . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58Assistance With Your Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
Section Seven TERMS AND DEFINITIONSDefinition of Terms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Prior Authorization/Formulary Exception Form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
viii

1
Cleveland Clinic Retiree Health Plan Total Care Mission To manage the retiree health plan benefits in a manner that is consistently customer-focused, quality-oriented,and fiscally responsible.
This section of the Summary Plan Description (SPD) helps ensure that you get the healthcare coverage you’reentitled to when you need it. It summarizes your responsibilities to Cleveland Clinic Retiree Health Plan(RHP) Total Care, as well as your covered health benefits and access to network providers. RHP Total Careneeds accurate information from you to pay for the benefits you receive. Our healthcare providers needaccurate information from you to provide you and your covered dependents with quality care.
Review this overview section of the SPD to familiarize yourself with the:
• Coordination of Benefits Process
• Two-Tiered Network of Providers
• Medical and Behavioral Health Coverage Summary
• Prescription Drug Benefit Summaries
This section also addresses the importance of accurate registration, updating life event changes, claimsprocessing information, and customer service. A Quick Reference Guide is on page 9.
Coordination of Benefits (COB)Coordination of Benefits (COB) is the process used to pay healthcare expenses when you or an eligibledependent is covered by more than one healthcare insurance policy, including Medicare. EHP Total Careis partnered with Mutual Health Services, our Third-Party Administrator (TPA), to administer your healthplan benefits and provide claims processing for healthcare services.
Each year, you are responsible for providing Cleveland Clinic Employee Health Plan (EHP) Total Care withinformation pertaining to additional medical benefits that you or any of your participating dependents areeligible to receive. This is done through Mutual Health Services by following the COB process described below.
COB ProcessAll members are required to complete the COB process upon enrollment and in January of each year thereafter.If you do not complete the COB process, healthcare claims will not be paid for your dependent(s).
The following three options are available for submitting your COB information to the TPA:
1. Complete the online COB form via the Mutual Health Services website. You can access the website viathe Cleveland Clinic HRConnect Portal or log in as follows:https://chn.mutualhealthservices.com/ReceptionArea/Welcome.aspx
2. Complete the form where applicable, sign the bottom of the form, and return to the TPA at the addressincluded on the form.
3. Call the TPA Customer Service at 1-800-451-7929 to update your COB information.
Note: This option is only available if you have no other insurance in the plan year being updated or theprior plan year.
Section OneGETTING STARTED
2
If the COB process is not completed, the TPA will send the form again when the first claim for a dependentis submitted. The form will be sent for each dependent’s initial claim until the COB process is complete. Ifno response is received within 45 days, the TPA will send an Explanation of Benefits (EOB) form notifyingthe member that all claims will deny for the retiree’s dependents until the form is completed. Membershave one year to complete the COB process. After one year, claim payment will become the responsibilityof the member. For more information about Mutual Health Services and Coordination of Benefits, seeSection Four of the Summary Plan Description (SPD): “Third-Party Administrator (TPA) — Mutual HealthServices” on page 37.
COB Form
Cleveland Clinic EHP Total Care Employee Signature Date / /Ohio Revised Code Section 3999.21 — Insurance Fraud Warning “Any person who, with intent to defraud or knowing that he is facilitating a fraud against an insurer,submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud.”
ID CardEHP No.:
SSN: Date of Birth: / /
MEDICARE INFORMATION Please enclose a copy of your Medicare card.Medicare ID No.
Medicare Recipient Name
Effective Date: Part A / / Part B / /
Medicare Coverage is the result of:
� Age (65 years)
� Disability
� End-Stage Renal DiseaseIf yes, please check one of the following:
� Transplant
� Dialysis
Please check one: � Home Dialysis � Facility Dialysis
Is there legal documentation stating who is responsible for carrying the healthcare coverage for you or your dependents?� YES � NO If yes, legal documents must accompany the form stating who is responsible for carrying healthcare coverage.
Name of Custodial Parent
OTHER INSURANCE INFORMATION (NON MEDICARE) Please enclose a copy of the other insurance ID cards.
Policyholder’s Name
Policyholder’s Date of Birth / / ID No. Group No.
Original Effective Date / / Policy Term Date (if applicable*) / /*Please provide a copy of Creditable Coverage Letter(s).
Policy Obtained Through: � Group Employment � Individual Purchase � School � Medicaid � Other
Policy Status: � Active Benefits � Retiree Benefits � COBRA Policy Covers: � Medical � Pharmacy � Dental � Vision
Policy Type: � Employee Only � Employee + Child/Children � Employee + Spouse � Family � Other
Name of Customer ServiceOther Insurance Company Telephone No.
Name of Employer
Please complete columns below for those covered under the other insurance policy listed above. Use additional COB forms if necessary. Last Name First Name Date of Birth Relationship Effective Date Term Date
/ / / / / /
/ / / / / /
/ / / / / /
/ / / / / /
/ / / / / /
/ / / / / /
Date Approved for Medicare Benefits
Relationship toCleveland Clinic Employee
Rev. 11/11
PLAN YEAR 2012Cleveland Clinic EHP Total Care Employee (Print)
Do (did) you or your participating dependents have other Medical, Pharmacy, Dental, Vision, Medicare or Medicaid coverage in 2011 and/or 2012?
� YES � NOPlease complete the form and refer to the letter for submission instructions.
Date of Transplant
Date of First Dialysis
/ /
/ /
/ /
Medicare ID No.
Medicare Recipient Name
Effective Date: Part A / / Part B / /
Medicare Coverage is the result of:
� Age (65 years)
� Disability
� End-Stage Renal DiseaseIf yes, please check one of the following:
� Transplant
� Dialysis
Please check one: � Home Dialysis � Facility Dialysis
Date Approved for Medicare Benefits
Date of Transplant
Date of First Dialysis
/ /
/ /
/ /
SAMPLE
Two-Tiered Provider NetworkCleveland Clinic and Regional hospitals, including participating physicians, comprise the RHP Total CareTier 1 provider network. The Tier 2 provider network consists of three different networks: Cleveland HealthNetwork (CHN), Medical Mutual Traditional Network (MMO), and USA Managed Care Organization (USAMCO).Your RHP Total Care Identification (ID) card reflects these relationships by displaying the CHN logo on the

3
front of the card with the written words “Cleveland Clinic Retiree Health Plan Total Care.” The Mutual HealthServices (TPA) logo is on the back of your ID card. See page 43 in Section Five: “Administrative Information”for ID card details.
As an RHP Total Care member, you can use either provider tier at anytime throughout the benefit year.However, to receive maximum coverage, you must use Tier 1 providers. See page 10 in Section Two: “TieredNetwork of Providers” for explanations of both tiers and the benefits of each.
RHP Total Care BenefitsCleveland Clinic RHP Total Care includes medical, behavioral, and prescription drug benefits. Thiscomprehensive healthcare coverage is summarized in the charts on the following pages.
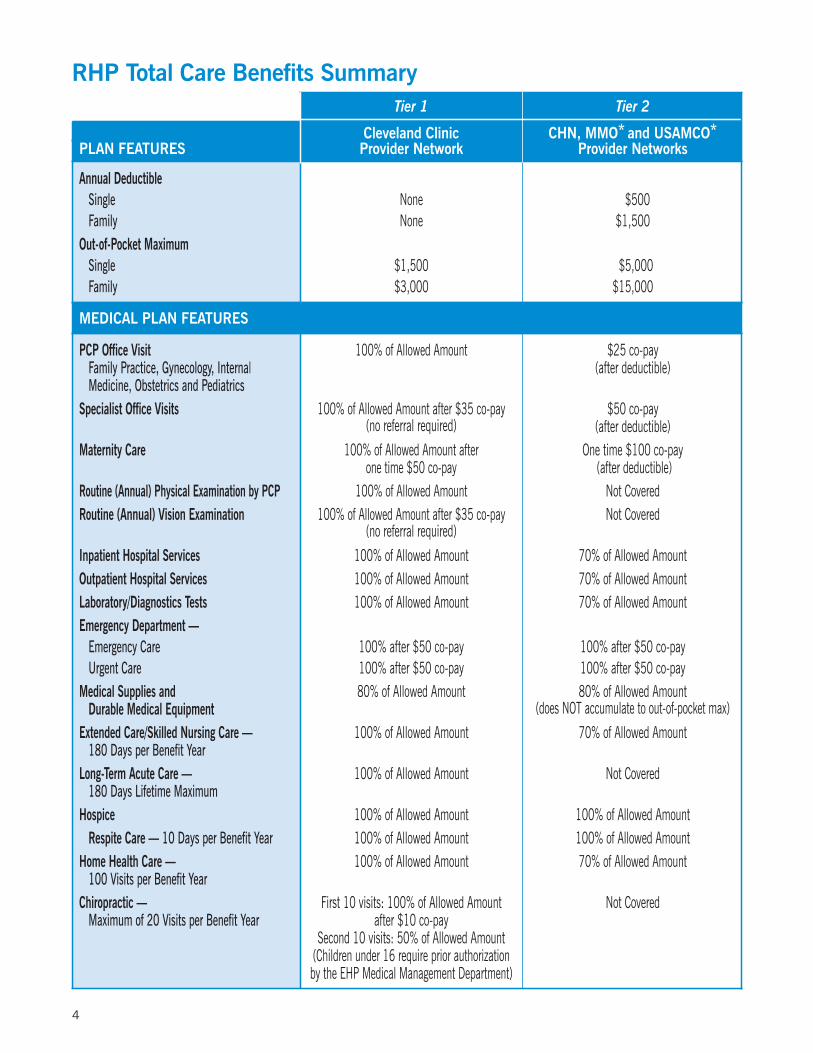
Medical and Behavioral PlanThe RHP Total Care Benefits summary chart on pages 4 and 5 summarizes Tier 1 and Tier 2 provider coveragefor medical and behavioral health services, as well as deductible and out-of-pocket maximum information.Medical Plan features include physician office visits, hospital services, diagnostic services and emergencycare, to name a few. Behavioral Health features include all services for mental health and substance abuse.
Prescription Drug PlanThe RHP Total Care Prescription Drug Benefit summary charts on pages 6 and 7 outline drug categories, listsprescription drug delivery options, including Cleveland Clinic Pharmacies, and lists annual deductibles andco-insurance amounts for both groups of retirees (non-Medicare eligible and Medicare eligible).
The RHP Total Care Prescription Drug Benefit provides coverage for FDA-approved prescription drugs thatare included in the Cleveland Clinic RHP Total Care Prescription Drug Benefit and Formulary* Handbook (hereafterreferred to as Handbook in this SPD). As a Total Care member, you will receive a printed copy of the Handbook.The online version of the Handbook is updated twice a year and can be accessed at www.clevelandclinic.org/healthplan. Medications are listed in the Handbook by both their brand and generic names.
Note: *Medicare eligible SilverScript members have a separate Formulary which is provided by SilverScript.It is also available on our website at www.clevelandclinic.org/healthplan. Click on the “Retiree”tab. Updates to the formulary will be sent to members by SilverScript.
Prescription drugs in both the Handbook and SilverScript’s Formulary are categorized in four tiers:
Generic Medications (Tier 1) — EHP Total Care supports and encourages the use of FDA-approved genericequivalents that are as effective and safe as brand name products. Using generic medications delivers thesame quality treatment as brand name medications and is cost effective.
Preferred Brands (Tier 2) — FDA-approved brand name medications of proven therapeutic effectiveness andsafety considered essential for patient care and approved for inclusion in the Handbook.
Non-Preferred Brands (Tier 3) — These are FDA-approved brand name medications that are considered non-formulary and are therefore not included in the Handbook. Higher co-payments are charged for Non-PreferredBrands.
Specialty Drugs (Tier 4) — These medications are only available through a Cleveland Clinic Pharmacy or theCVS Caremark’s Specialty Drug Program. Please note: The member may have higher out-of-pocket expensesif he/she chooses to obtain their specialty medications from CVS Caremark.
In addition to reviewing the RHP Total Care Benefits and Prescription Drug Benefit summary charts, readSection Three: “Health Plan Coverage” (see page 14) in its entirety so that you have a thorough understandingof your medical, behavioral health, and prescription drug benefits. EHP Total Care services, coordinatedcare programs, prior authorization guidelines, options for filling your prescription medications, and TotalCare pharmacy programs are addressed in detail.
4
RHP Total Care Benefits SummaryTier 1 Tier 2
Cleveland Clinic CHN, MMO* and USAMCO*PLAN FEATURES Provider Network Provider Networks
Annual DeductibleSingle None 1,$500Family None $1,500
Out-of-Pocket MaximumSingle $1,500 1$5,000Family $3,000 $15,000
MEDICAL PLAN FEATURES
PCP Office Visit 100% of Allowed Amount $25 co-payFamily Practice, Gynecology, Internal (after deductible)Medicine, Obstetrics and Pediatrics
Specialist Office Visits 100% of Allowed Amount after $35 co-pay $50 co-pay(no referral required) (after deductible)
Maternity Care 100% of Allowed Amount after One time $100 co-payone time $50 co-pay (after deductible)
Routine (Annual) Physical Examination by PCP 100% of Allowed Amount Not CoveredRoutine (Annual) Vision Examination 100% of Allowed Amount after $35 co-pay Not Covered
(no referral required)Inpatient Hospital Services 100% of Allowed Amount 70% of Allowed AmountOutpatient Hospital Services 100% of Allowed Amount 70% of Allowed AmountLaboratory/Diagnostics Tests 100% of Allowed Amount 70% of Allowed AmountEmergency Department —
Emergency Care 100% after $50 co-pay 100% after $50 co-payUrgent Care 100% after $50 co-pay 100% after $50 co-pay
Medical Supplies and 80% of Allowed Amount 80% of Allowed AmountDurable Medical Equipment (does NOT accumulate to out-of-pocket max)
Extended Care/Skilled Nursing Care — 100% of Allowed Amount 70% of Allowed Amount180 Days per Benefit Year
Long-Term Acute Care — 100% of Allowed Amount Not Covered180 Days Lifetime Maximum
Hospice 100% of Allowed Amount 100% of Allowed AmountRespite Care — 10 Days per Benefit Year 100% of Allowed Amount 100% of Allowed Amount
Home Health Care — 100% of Allowed Amount 70% of Allowed Amount100 Visits per Benefit Year
Chiropractic — First 10 visits: 100% of Allowed Amount Not CoveredMaximum of 20 Visits per Benefit Year after $10 co-pay
Second 10 visits: 50% of Allowed Amount(Children under 16 require prior authorizationby the EHP Medical Management Department)

5
Tier 1 Tier 2
MEDICAL Cleveland Clinic CHN, MMO* and USAMCO*PLAN FEATURES continued Provider Network Provider Networks
Therapy ServicesOccupational/Speech/Physical — 100% of Allowed Amount after 100% of Allowed Amount after26 Visits per Therapy, then $10 co-pay per visit $10 co-pay per visit and after deductibleprior authorization required (does NOT accumulate to out-of-pocket max)
Dental — Surgical extractions for soft/bony 100% of Allowed Amount Not Coveredimpactions, or Dental implants for certainmedical conditions or recent accidents/injuries
Family Planning 100% of Allowed Amount Not CoveredInfertility — Diagnostic Only 100% of Allowed Amount Not CoveredHearing Aids 50% of Charge up to $3,500/Ear — Not Covered
Limited to one aid per Ear every 3 yearsOrgan Transplant 100% of Allowed Amount 70% of Allowed Amount
Transplant Lifetime Maximum Unlimited UnlimitedOut-of-Pocket Maximum See Previous Page (Out-of-Pocket Maximum) Unlimited
BEHAVIORAL HEALTH PLAN FEATURES
Outpatient Coverage1
35 Outpatient (OP) Visits, then 100% of Allowed Amount $50 co-pay (after deductible)prior authorization required after $35 co-pay with 100% of Allowed AmountPsychological and Neuro-Psychological Testing2 100% of Allowed Amount Not Covered
after $35 co-payInpatient Coverage2 100% of Allowed Amount 70% of Allowed AmountIntensive Outpatient (IOP)2 100% of Allowed Amount 70% of Allowed AmountPartial Hospitalization Programs (PHP)2 100% of Allowed Amount 70% of Allowed Amount
For Tier 1, all co-insurance listed on this chart accumulate to your out-of-pocket maximum.For Tier 2 ancillaries (services such as dialysis, ambulance transportation, home health, skilled nursing facilities and hospice), co-payments DO NOT accrue tothe out-of-pocket maximum.*MMO Traditional for the state of Ohio and USAMCO outside the state of Ohio.1 Prior authorization and clinical appropriateness required after 35 visits — the 35 visit Outpatient Coverage for Behavioral Health includes any outpatient servicesprovided by a behavioral health practitioner for chronic pain management, sleep disorder, aftercare groups for substance abuse, and/or pre and post gastric surgeryvisits. There is no coverage for telephone counseling services or school meetings by outpatient behavioral health practitioners.
2 Prior authorization required.Note: Prior authorization, precertification, predetermination and prior approval are often used interchangeably.
Any unauthorized programs, services, or visits will not be covered by RHPTotal Care under any circumstances and the subsequent charges will be thefinancial responsibility of the member. This applies to any unauthorized out-of-network and out-of-area providers and facilities, with the only exceptionbeing for emergency care.
RHP Total Care Benefits Summary continued
6
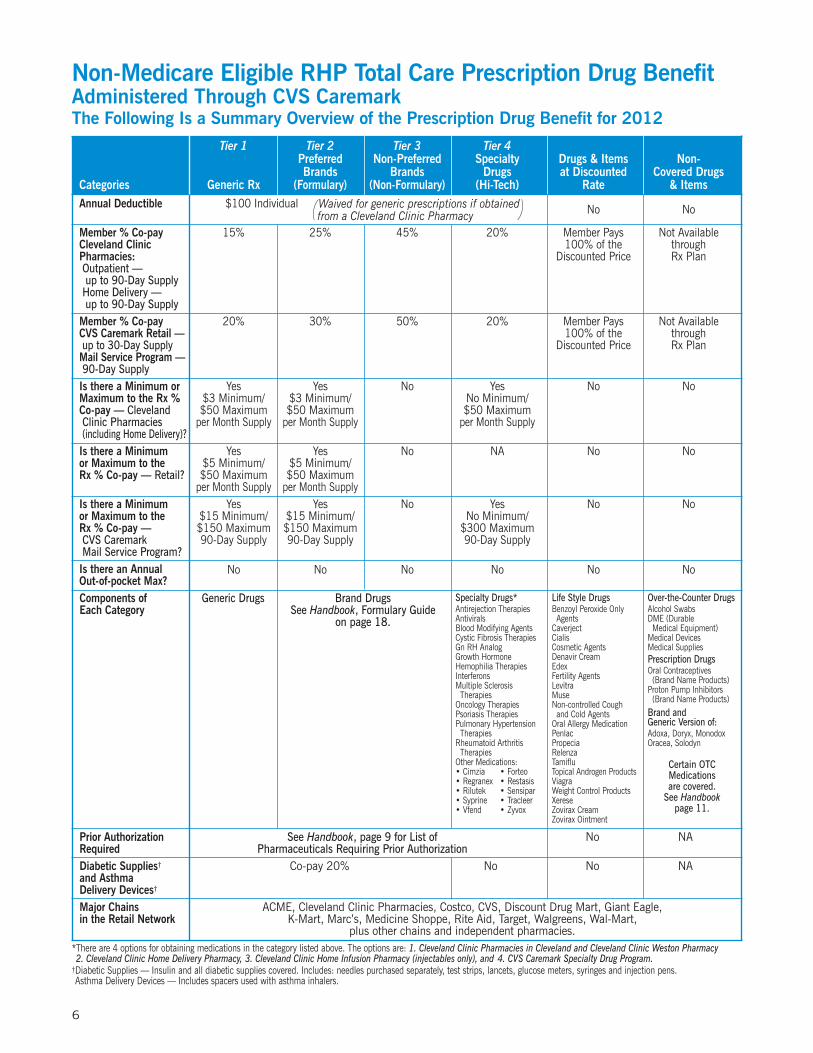
Non-Medicare Eligible RHP Total Care Prescription Drug BenefitAdministered Through CVS CaremarkThe Following Is a Summary Overview of the Prescription Drug Benefit for 2012
Tier 1 Tier 2 Tier 3 Tier 4Preferred Non-Preferred Specialty Drugs & Items Non-Brands Brands Drugs at Discounted Covered Drugs
Categories Generic Rx (Formulary) (Non-Formulary) (Hi-Tech) Rate & ItemsAnnual Deductible $100 Individual No No
Member % Co-pay 15% 25% 45% 20% Member Pays Not AvailableCleveland Clinic 100% of the throughPharmacies : Discounted Price Rx PlanOutpatient —up to 90-Day SupplyHome Delivery —up to 90-Day Supply
Member % Co-pay 20% 30% 50% 20% Member Pays Not AvailableCVS Caremark Retail — 100% of the throughup to 30-Day Supply Discounted Price Rx PlanMail Service Program —90-Day SupplyIs there a Minimum or Yes Yes No Yes No NoMaximum to the Rx % $3 Minimum/ $3 Minimum/ No Minimum/Co-pay — Cleveland $50 Maximum $50 Maximum $50 MaximumClinic Pharmacies per Month Supply per Month Supply per Month Supply(including Home Delivery)?Is there a Minimum Yes Yes No NA No Noor Maximum to the $5 Minimum/ $5 Minimum/Rx % Co-pay — Retail? $50 Maximum $50 Maximum
per Month Supply per Month SupplyIs there a Minimum Yes Yes No Yes No No or Maximum to the $15 Minimum/ $15 Minimum/ No Minimum/Rx % Co-pay — $150 Maximum $150 Maximum $300 MaximumCVS Caremark 90-Day Supply 90-Day Supply 90-Day SupplyMail Service Program?Is there an Annual No No No No No NoOut-of-pocket Max?Components of Generic Drugs Brand DrugsEach Category See Handbook, Formulary Guide
on page 18.
Prior Authorization See Handbook, page 9 for List of No NARequired Pharmaceuticals Requiring Prior AuthorizationDiabetic Supplies† Co-pay 20% No No NAand AsthmaDelivery Devices†
Major Chains ACME, Cleveland Clinic Pharmacies, Costco, CVS, Discount Drug Mart, Giant Eagle,in the Retail Network K-Mart, Marc’s, Medicine Shoppe, Rite Aid, Target, Walgreens, Wal-Mart,
plus other chains and independent pharmacies.*There are 4 options for obtaining medications in the category listed above. The options are: 1. Cleveland Clinic Pharmacies in Cleveland and Cleveland Clinic Weston Pharmacy2. Cleveland Clinic Home Delivery Pharmacy, 3. Cleveland Clinic Home Infusion Pharmacy (injectables only), and 4. CVS Caremark Specialty Drug Program.
†Diabetic Supplies — Insulin and all diabetic supplies covered. Includes: needles purchased separately, test strips, lancets, glucose meters, syringes and injection pens.Asthma Delivery Devices — Includes spacers used with asthma inhalers.
Specialty Drugs*Antirejection TherapiesAntiviralsBlood Modifying AgentsCystic Fibrosis TherapiesGn RH AnalogGrowth HormoneHemophilia TherapiesInterferonsMultiple SclerosisTherapies
Oncology TherapiesPsoriasis TherapiesPulmonary HypertensionTherapies
Rheumatoid ArthritisTherapies
Other Medications:• Cimzia • Forteo• Regranex • Restasis• Rilutek • Sensipar• Syprine • Tracleer• Vfend • Zyvox
Life Style DrugsBenzoyl Peroxide OnlyAgents
CaverjectCialisCosmetic AgentsDenavir CreamEdexFertility AgentsLevitraMuseNon-controlled Coughand Cold Agents
Oral Allergy MedicationPenlacPropeciaRelenzaTamifluTopical Androgen ProductsViagraWeight Control ProductsXereseZovirax CreamZovirax Ointment
Over-the-Counter DrugsAlcohol SwabsDME (DurableMedical Equipment)
Medical DevicesMedical SuppliesPrescription DrugsOral Contraceptives(Brand Name Products)
Proton Pump Inhibitors(Brand Name Products)
Brand andGeneric Version of:Adoxa, Doryx, MonodoxOracea, Solodyn
Certain OTCMedicationsare covered.
See Handbookpage 11.
Waived for generic prescriptions if obtained)(from a Cleveland Clinic Pharmacy

7
Medicare Eligible RHP Total Care Prescription Drug BenefitAdministered Through SilverScript®
The Following Is a Summary Overview of the Prescription Drug Benefit for 2012
Tier 1 Tier 2 Tier 3 Tier 4Preferred Non-Preferred SpecialtyBrands Brands Drugs
Categories Generic Rx (Formulary) (Non-Formulary) (Hi-Tech)
Annual Deductible $100 Individual (Waived for generic prescriptions if obtained from a Cleveland Clinic Pharmacy)Member % Co-insurance 15% 25% 45% 20%Cleveland Clinic Pharmacies :Outpatient — up to 90-Day Supply
Home Delivery —up to 90-Day Supply
Member % Co-insurance 20% 30% 50% 20%CVS Caremark Retail —up to 90-Day Supply
Mail Service Program —up to 90-Day Supply
Is there a Minimum or Yes Yes No YesMaximum to the Rx % Co-ins. — $3 Minimum/ $3 Minimum/ No Minimum/Cleveland Clinic Pharmacies $50 Maximum $50 Maximum $50 Maximum(including Home Delivery) per 30-Day Supply per 30-Day Supply per 30-Day Supply
Is there a Minimum or Yes Yes No N/AMaximum to the Rx % Co-ins. — $5 Minimum/ $5 Minimum/CVS Caremark Retail — $75 Maximum $75 Maximumup to 90-Day Supply per 30-Day Supply per 30-Day Supply
Is there a Minimum or Yes Yes No YesMaximum to the Rx % Co-ins. — $15 Minimum/ $15 Minimum/ No Minimum/CVS Caremark $225 Maximum $225 Maximum $300 MaximumMail Service Program? 90-Day Supply 90-Day Supply 90-Day Supply
Components of Each Category Generic Drugs Brand Drugs Specialty Drugs
Major Chains ACME, Cleveland Clinic Pharmacies, Costco, CVS, Discount Drug Mart,in the Retail Network Giant Eagle, K-Mart, Marc’s, Medicine Shoppe, Rite Aid, Target, Walgreens, Wal-Mart,
plus other chains and independent pharmacies.SilverScript is a registered trademark of SilverScript Insurance Company.
You will be sent a copy of the SilverScript’s Preferred Drug List.You may also contact SilverScript to request a copy of the Preferred Drug List
by calling the toll-free number on your SilverScript card.
8
Accurate RegistrationAccurate registration ensures timely claim reimbursement. Make sure that registration information iscorrect for each family member every time you or any of your dependents receive healthcare services.Make sure the correct ID card is being used, the address information is up-to-date, and the date of birthinformation is accurate (see page 41 in Section Five: “Administrative Information”).
Claims InformationRHP Total Care allows you, in most instances, to receive care without sending any claims or paperwork tothe Third-Party Administrator (TPA). After you receive care, you will receive an Explanation of Benefits (EOB)from the TPA. See page 37 in Section Four: “Third-Party Administrator —Mutual Health Services” for details.Additional information about claim types and benefit determination for claims can be found in SectionSix: “RHP Members’ Rights and Responsibilities” on page 47.
Communication and ServiceCleveland Clinic Employee Health Plan (EHP) Total Care continually updates members about new initiativesor changes regarding their health plan coverage. It is our goal to do this through the HealthWise Bulletin,through the local hospital newsletter, and through the centralized Cleveland Clinic Employee Health Plan(EHP) Total Care Customer Service Unit available during business hours. See the Quick Reference Guideon page 9 for appropriate contact information.
Customer Service UnitThe EHP Total Care Customer Service Unit is open Monday through Friday from 7:30 a.m. to 3:30 p.m. Atrained representative is available to answer health plan benefit questions. The Customer Service Unit willbe able to assist you with medical, behavioral health/substance abuse, and prescription drug questions andissues. If you have questions regarding any other benefit coverage you must contact the Benefits Department.
The Cleveland Clinic Employee Health Plan Total Care Customer Service Unit is responsible for providingkey information regarding RHP Total Care benefits. You can contact us by:
Phone: 216-448-0800 or toll-free at 1-866-811-4352
Fax: 216-448-9053
E-mail: [email protected] address:
Cleveland Clinic Employee Health Plan Total CareCustomer Service Unit / SCC1329050 Aurora RoadSolon, OH 44139
Medical ManagementFind out about Cleveland Clinic programs designed to assist members with complex medical and behavioralhealth needs; self-management care needs for those with chronic illnesses; health promotion programs; andrare disease management for uncommon conditions. See page 15 in Section Three: “Health Plan Coverage.”
Life Event ChangesCertain changes that affect you and/or your dependents — such as a marriage, birth, divorce, or qualifying forMedicare — and may result in the need to make changes to your BeneFlex elections (see page 44 in SectionFive: “Administrative Information”).
9
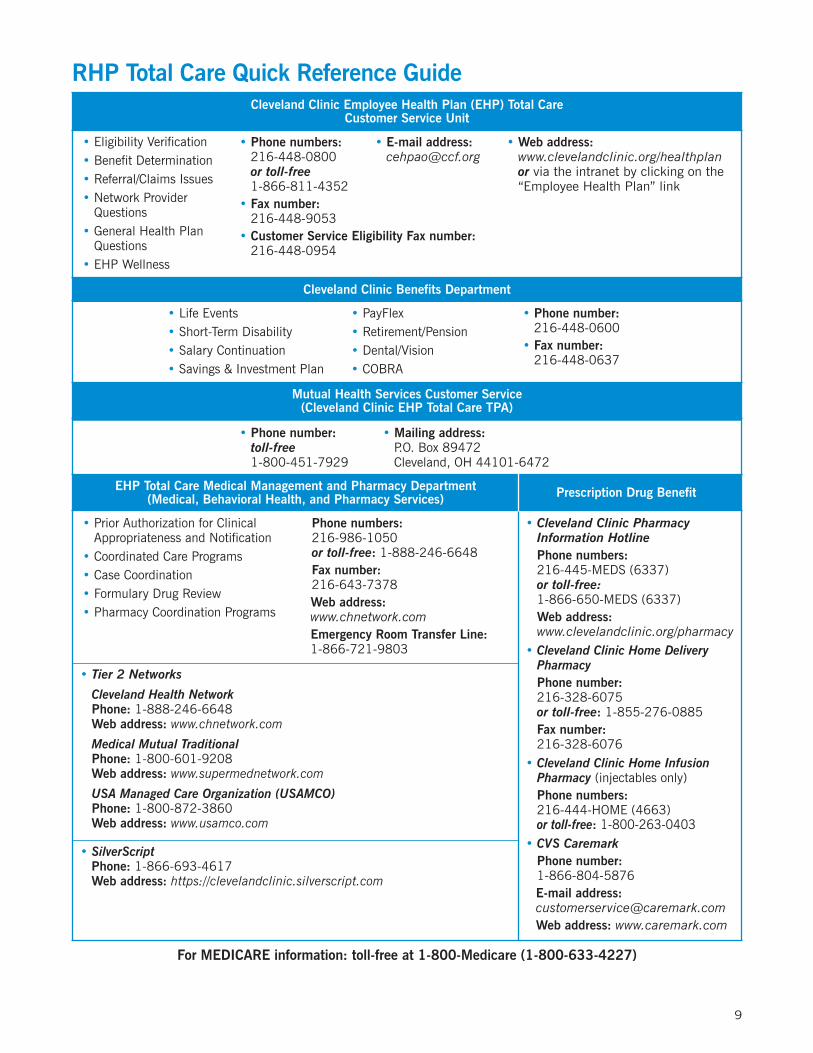
Cleveland Clinic Quick Reference GuideCleveland Clinic Employee Health Plan (EHP) Total Care
Customer Service Unit
• Eligibility Verification• Benefit Determination• Referral/Claims Issues• Network Provider
Questions• General Health Plan
Questions• EHP Wellness
Cleveland Clinic Benefits Department
• Life Events • PayFlex• Short-Term Disability • Retirement/Pension• Salary Continuation • Dental/Vision• Savings & Investment Plan • COBRA
Mutual Health Services Customer Service(Cleveland Clinic EHP Total Care TPA)
• Phone number:toll-free-
EHP Total Care Medical Management and Pharmacy Department Prescription Drug Benefit(Medical, Behavioral Health, and Pharmacy Services)
• Prior Authorization for ClinicalAppropriateness and Notification
• Coordinated Care Programs• Case Coordination• Formulary Drug Review• Pharmacy Coordination Programs
For MEDICARE information: toll-free at 1-800-Medicare (1-800-633-4227)
• SilverScriptPhone: 1-866-693-4617Web address: https://clevelandclinic.silverscript.com– Family Dependent Care Specialist — Toll-free phone: 1-800-445-1641– Legal Assist Specialist — Toll-free phone: 1-866-707-5385
• Tier 2 Networks
• Cleveland Health Network• Phone: 1-888-246-6648
Web address: www.chnetwork.com
• Medical Mutual Traditional• Phone: 1-800-601-9208
Web address: www.supermednetwork.com
• USA Managed Care Organization (USAMCO)• Phone: 1-800-872-3860
Web address: www.usamco.com
• Cleveland Clinic PharmacyInformation Hotline
• Phone numbers:216-445-MEDS (6337)or toll-free:1-866-650-MEDS (6337)
• Web address:www.clevelandclinic.org/pharmacy
• Cleveland Clinic Home DeliveryPharmacy
• Phone number:216-328-6075or toll-free: 1-855-276-0885
• Fax number:216-328-6076
• Cleveland Clinic Home InfusionPharmacy (injectables only)
• Phone numbers:216-444-HOME (4663)or toll-free: 1-800-263-0403
• CVS Caremark• Phone number:
1-866-804-5876E-mail address:[email protected] address: www.caremark.com
• Phone numbers:216-448-0800or toll-free1-866-811-4352
• Fax number:216-448-9053
• Customer Service Eligibility Fax number:216-448-0954
• E-mail address:[email protected]
• Web address:www.clevelandclinic.org/healthplanor via the intranet by clicking on the“Employee Health Plan” link
• Phone number:toll-free1-800-451-7929
• Mailing address:P.O. Box 89472Cleveland, OH 44101-6472
RHP Total Care Quick Reference Guide
• Phone number:216-448-0600
• Fax number:216-448-0637
• Phone numbers:216-986-1050or toll-free: 1-888-246-6648
• Fax number:216-643-7378
• Web address:www.chnetwork.com
• Emergency Room Transfer Line:1-866-721-9803

Two-Tier NetworkCleveland Clinic Retiree Health Plan (EHP) Total Care offers a two-tier Network of Providers. As an RHPTotal Care member, you can use either tier at anytime throughout the benefit year and may receive care fromproviders in both tiers if you choose. The tier you select, however, determines the amount of coverage youwill receive. To receive maximum coverage, you must use Tier 1 providers.
Tier 1Tier 1 providers consist of Cleveland Clinic and Regional hospitals, including participating physicianscredentialed by the Cleveland Clinic Community Physician Partnership (CPP). These providers are, for themost part, located in Cuyahoga County. The Tier 1 Network of Providers includes Primary Care Providers(PCP), Specialist Providers (SP), Behavioral Health Providers, and Ancillary Services Providers. Ancillaryservices are services such as dialysis, ambulance, transportation, durable medical equipment (DME), homehealth, skilled nursing facilities, hospice and others.
If you seek services from a Tier 1 PCP, you are covered at 100%. Physician practices considered primary careinclude Family Practice, Internal Medicine, Gynecology, Obstetrics, and Pediatrics. All other physicianspecialists are reimbursed at 100% after a $35 co-payment per visit. You do not require a referral to seea specialist.
Note: Some PCP’s are classified as “Specialists” because they specialize ina specific area and, for the most part, only see patients with medicalconditions in their area. For example, an Oncology Gynecologist mayonly see cancer patients. In these instances, a co-payment of $35is applied.
In addition to Specialty Care, co-payments are also required for other services such as annual visionexaminations, therapy services (Occupational (OT)/Physical (PT)/Speech (ST)), chiropractic services, maternityservices, custom orthotics, sclerotherapy for symptomatic varicose veins, and emergency/urgent care.Durable medical equipment (DME) and medical supplies are reimbursed at 80%.
Note: RHP Total Care members who have Medicare Part B as their primaryhealth plan (age 65 and older) are not subject to the co-payment whenRHP Total Care pays as secondary. However, for services not covered byMedicare, such as eye exams and the service is a covered benefit by RHPTotal Care, RHP Total Care then pays as primary. In this instance, youcould be responsible for the applicable co-payment.
You have a maximum out-of-pocket (OOP) expense per year. For those who elect Single coverage, the maximumis $1,500 per year; Family coverage is $3,000 per year. In Tier 1, all co-payments accrue to your annual OOPmaximum. See Prescription Drug Benefit charts on pages 6 and 7.
10
Section Two
TIERED NETWORK OF PROVIDERS

11
It is important to understand that not all physicians on the Cleveland Clinic and Regional hospital medicalstaff are in the Cleveland Clinic CPP. It is the member’s responsibility to verify and obtain the most currentTier participation each time services are obtained. The most current Tier 1 provider information can be foundon the Internet at the CHN website: www.chnetwork.com and clicking on “EHP.” Information about specialarrangements with additional Tier 1 providers for employees who work at Cleveland Clinic locations outsideof Cuyahoga and Lorain Counties can be obtained by visiting the Cleveland Clinic Employee Health PlanTotal Care website at www.clevelandclinic.org/healthplan.
RHP Total Care does not print a hardcopy Provider Directory. If you do not have access to a website you caneither call Mutual Health Services toll-free at 1-800-451-7929 or the EHP Total Care Customer Service Unit at216-448-0800 or toll-free at 1-866-811-4352 to request a listing of doctors in your geographic area by physicianspecialty. The EHP Total Care Customer Service Unit can assist with problem resolution related to claimsfor healthcare services when services have been obtained from a Tier 1 provider.
Tier 1 Hospitals in the Cleveland Clinic RHPCleveland Clinic9500 Euclid AvenueCleveland, OH 44195 . . . . . . . . . . . . . . . . . . 216-444-2200 . . . . . . . www.ccf.org
Ashtabula County Medical Center2420 Lake AvenueAshtabula, OH 44004 . . . . . . . . . . . . . . . . . . . 440-997-2262 . . . . . . . . www.acmchealth.org
Cleveland Clinic Children’s Hospital for Rehabilitation2801 Martin Luther King, Jr. DriveCleveland, OH 44104 . . . . . . . . . . . . . . . . . . 216-448-6400 . . . . . . . www.clevelandclinic.org/childrensrehab
Euclid Hospital18901 Lakeshore Boulevard Euclid, OH 44119 . . . . . . . . . . . . . . . . . . . . . . 216-531-9000 . . . . . . . . www.euclidhospital.org
Fairview Hospital18101 Lorain AvenueCleveland, OH 44111 . . . . . . . . . . . . . . . . . . . 216-476-7000 . . . . . . . . www.fairviewhospital.org
Hillcrest Hospital6780 Mayfield RoadMayfield Heights, OH 44124 . . . . . . . . . . . . 440-312-4500 . . . . . . . . www.hillcresthospital.org
Lakewood Hospital14519 Detroit AvenueLakewood, OH 44107 . . . . . . . . . . . . . . . . . . . 216-521-4200 . . . . . . . . www.lakewoodhospital.org
Lutheran Hospital1730 W. 25th StreetCleveland, OH 44113 . . . . . . . . . . . . . . . . . . . 216-696-4300 . . . . . . . . www.lutheranhospital.org
Marymount Hospital12300 McCracken RoadGarfield Heights, OH 44125 . . . . . . . . . . . . . 216-581-0500 . . . . . . . . www.marymount.org
Medina Hospital1000 East Washington Street (Route 18)Medina, OH 44256 . . . . . . . . . . . . . . . . . . . . . 330-725-1000 . . . . . . . . www.medinahospital.org
South Pointe Hospital20000 Harvard RoadWarrensville Heights, OH 44122 . . . . . . . . 216-491-6000 . . . . . . . . www.southpointehospital.org
Tier 1 Hospitals in the Cleveland Clinic RHP (continued)Cleveland Clinic Florida*3100 Weston RoadWeston, FL 33331 . . . . . . . . . . . . . . . . . . . . . . 954-689-5000 . . . . . . . . www.ccf.org/florida
Cleveland Clinic Nevada888 West Bonneville AvenueLas Vegas, NV 89106 . . . . . . . . . . . . . . . . . . . . 702-483-6000
*If you choose to see a physician at Cleveland Clinic Florida, you must see a physician who is employed by the hospital.
Other Cleveland Clinic Ambulatory FacilitiesCleveland Clinic Beachwood Ambulatory Surgery Center
Cleveland Clinic Lorain Ambulatory Surgery Center
Cleveland Clinic Outpatient Surgery Center
Cleveland Clinic Richard E. Jacobs Health Center
Cleveland Clinic Stephanie Tubbs Jones Health Center
Cleveland Clinic Strongsville Ambulatory Surgery Center
Fairview Surgery Center
Marymount Ambulatory Surgery Center
Twinsburg Family Health Center
Wooster Clinic
Wooster Clinic Specialty Center (Endoscopy)
Tier 2The following three provider networks comprise the Tier 2 network:
• Cleveland Health Network (CHN) — a regional network of hospitals, physicians, and other healthcareproviders in northern Ohio and western Pennsylvania — website: www.chnetwork.com.
• Medical Mutual Traditional Network — a network of providers within the state of Ohio.website: www.supermednetwork.com and click on “Traditional.”
• USA Managed Care Organization (USAMCO) — a network of providers outside the state of Ohio.website: www.usamco.com.
The providers in the Cleveland Health Network are credentialed by the Cleveland Clinic Physician Partnership(CPP). CHN also services EHP Total Care with managing data analysis, case coordination, and networkcontracting. Providers in the MMO and USAMCO networks are credentialed by their respective companies.
Tier 2 benefits include treatment for non-routine services such as treatment and/or follow-up for sprains,diabetes, hypertension, or any chronic condition, rehab therapies, colds, wounds, follow-up treatment foremergent/urgent care services (usually used for students outside of the Tier 1 network or if a member is onvacation and requires care). Certain medical services including but not limited to routine health examinations,routine screening tests, and immunizations are not covered in Tier 2. See Benefits Coverage Clarificationsection on page 20.
Tier 2 benefits have an annual deductible. For those who elect Single coverage, the annual deductible is $500;for all other contract types the annual deductible is $1,500. After your deductible is met, Primary Care Provider(PCP) and Specialist office visits will reimburse at 100% after an applicable $25 or $50 co-payment is made.Inpatient hospital services, outpatient hospital services, and laboratory/diagnostic services will reimburseat 70% after the deductible is met.
12

13
Tier 2 has a maximum OOP expense per year. For those who elect Single coverage, the maximum is $5,000per year; for Family coverage, the maximum is $15,000 per year.
Note: Emergent/urgent care is covered at 100% after the applicable co-payment. Other specifics regardingTier 2 coverage can be found in the RHP Total Care Benefit Summary chart on pages 4 and 5.
If you would like to choose a provider from one of the Tier 2 networks, you can obtain provider informationon their websites listed above. You can also contact Mutual Health Services Customer Service toll-free at1-800-451-7929.
The Cleveland Clinic Employee Health Plan Total Care Customer Service Unit has limited ability to assistwith non-Tier 1 provider problem resolution.
Note: RHP Total Care has contracts with each of the Tier 2 networks listed on page 12. There are no individualcontracts with the providers in these networks. Because the network holds the individual providercontracts, members must contact the network that provided services directly to resolve discrepancieswith claim payment issues. RHP Total Care cannot resolve Tier 2 claim payment issues or quote the dollaramount of your financial obligation.
There are services that are covered benefits ONLY when provided within theTier 1 Network of Providers and all RHP Total Care guidelines have been met.Note that there is no Tier 2 coverage for these services. (See Benefits CoverageClarification on page 20.)

Cleveland Clinic Retiree Health Plan Total Care BenefitsCleveland Clinic Employee Health Plan (EHP) Total Care is committed to providing comprehensivehealthcare coverage for all members of RHP Total Care. This is accomplished by ensuring that quality-oriented, culturally sensitive healthcare services are provided at the appropriate level in the proper setting,in a timely manner. Reimbursement for all medical, behavioral health, and pharmacy services is based onclinical appropriateness.
The EHP Total Care Medical Management and Pharmacy Departments utilize evidence-based informationto authorize covered services for the employee population accessing services. The Medical Management andPharmacy Departments (Medical, Behavioral Health, and Pharmacy Services) oversee:
• Prior Authorization for Clinical Appropriateness and Notification
• Coordinated Care Programs
• Case Coordination
• Formulary Drug Review
• Pharmacy Coordination Program
Although you may choose to use a provider from either the Tier 1 or Tier 2 provider networks (as explainedin Section Two), we encourage you to develop a relationship with a Primary Care Provider (PCP). Physicianpractices considered primary care include most Family Practice, Internal Medicine, Gynecology, Obstetrics,and Pediatrics. This will provide you with the advantage of having a physician knowledgeable about yourhealthcare and can provide:
1. Preventive healthcare
2. Care if you become ill
3. Advice regarding the need to see a specialist
Because a single physician coordinates your care, you can feel assured that you are receiving the best possiblehealthcare available within the RHP Total Care Network of Providers.
See Section One: “Getting Started” for an overview of your medical, behavioral health, and pharmacy coverage.The RHP Total Care Benefits Summary chart on pages 4 and 5 summarizes Tier 1 and Tier 2 provider coveragefor medical and behavioral health services, as well as deductible and out-of-pocket maximum information.Medical Plan features include physician office visits, hospital services, diagnostic services and emergencycare, to name a few. Behavioral Health includes all services for mental health and substance abuse.
The RHP Total Care Prescription Drug Benefit summary charts on pages 6 and 7 outline drug categories, suchas generic and formulary. The Prescription Drug Benefit and Formulary Handbook provides detailed informationon prescription drug delivery options which include Cleveland Clinic Pharmacies, CVS Caremark Retail,and home delivery programs. These delivery options apply to both SilverScript and CVS Caremark members.
Read this section of the Summary Plan Description (SPD) in its entirety so that you have a thorough under-standing of your medical, behavioral health, and prescription drug benefits. RHP Total Care services,managed care programs, prior authorization/clinical appropriateness guidelines, and options for fillingyour prescription medications are explained in detail.
14
Section Three
HEALTH PLAN COVERAGE

15
This section of the SPD addresses:Page
EHP Total Care Medical Management . . . . . . . . . . . . . . . . . . . . . . . . 15Utilization Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Prior Authorization and Concurrent Review . . . . . . . . . . . . . . . . . 16Benefits Coverage Clarification . . . . . . . . . . . . . . . . . . . . . . . . . . 20Behavioral Health Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Medical Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Case Coordination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Coordinated Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Prescription Drug Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Health Plan Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Note that all covered services must be clinically appropriate and are subject to coverage exclusions. ClevelandClinic Retiree Health Plan Total Care has the right to review all claim reimbursements retrospectivelyand adjust payment according to RHP Total Care guidelines. This means the member may be financiallyaccountable for services after they have been rendered. If you want the maximum benefit reimbursement,you should contact the EHP Medical Management and/or Pharmacy Departments prior to obtaining medical,behavioral health, and pharmacy services.
EHP Total Care Medical ManagementThe following pages detail your health benefits coverage. Mutual Health Services is the Third-Party Administrator(TPA) that will reimburse medical and behavioral health claims (See Section Four: “Third-Party Administrator— Mutual Health Services” on page 41). If you are not certain that a claim paid/reimbursed correctly, youshould contact Mutual Health Services for review. If you still disagree, contact the Cleveland Clinic EmployeeHealth Plan Total Care Customer Service Unit at 216-448-0800 or toll-free at 1-866-811-4352.
EHP Total Care Medical Management includes five elements:
1. Utilization Management to establish prior authorization and determine clinical appropriateness ofrequested services.
2. Case Coordination for assistance with complex medical and behavioral health needs.
3. Coordinated Care addresses self-management care needs of members with chronic illnesses.
4. Health Promotion includes short telephonic programs to preserve healthy status.
5. Rare Disease Management provides assistance with uncommon conditions and is administered byAccordant, a CVS Company.
Utilization ManagementRHP Total Care is designed to provide coverage for members that is clinically appropriate. In order toensure that provided services are clinically appropriate, the EHP Medical Management and PharmacyDepartments have rules and processes for members to follow so that clinically appropriate care is reimbursedcorrectly and efficiently. These rules and processes are addressed below and in the “Prior Authorization andConcurrent Review for Clinical Appropriateness” section that follows on page 16.
A service is NOT considered clinically appropriate if it is:
1. Not ordered by a licensed or accredited physician, hospital, or healthcare provider or other healthcarefacility.
2. Not recognized throughout the Medical profession as safe and effective, is not required for the diagnosisand treatment of a particular illness (physical or behavioral) or injury, and is not employed appropriatelyin a manner consistent with generally accepted United States medical standards.
3. Provided for vocational training.
4. An Educational Service, including those listed below, are not considered clinically appropriate unlessrequired BECAUSE OF a new medical or behavioral condition or a change from baseline in a previouscondition. Educational services that can be received within a school system are NOT considered clinicallyappropriate. Examples of services that are not covered unless they are deemed clinically appropriateinclude:
• Training in the activities of daily living; and
• Instruction in scholastic skills such as reading and writing; and
• Preparation for an occupation, or treatment of learning disabilities for academic underachievement.
5. Experimental or Investigational — Generally, experimental or investigational refers to the medical use of aservice or supply still under study and the service or supply is not yet recognized throughout the Physician’sprofession in the United States as safe or effective for diagnosis and treatment of the illness or injury.This includes, but is not limited to: clinical trials, all treatment protocols based upon or similar to thoseused in clinical trials, and drugs approved by the Federal Food and Drug Administration that are beingused for unrecognized indications. Experimental or investigational procedures are usually identified bythose procedures that have no CPT code and are therefore coded into a “NOC — not otherwise classified”category. These will require prior authorization for clinical appropriateness.
Cleveland Clinic Employee Health Plan Total Care reserves the right for final determination of clinicalappropriateness.
Prior Authorization and Concurrent Review for Clinical AppropriatenessThe EHP Medical Management and Pharmacy Departments have prior authorization and clinical reviewprocesses to help ensure quality and cost-effective medical care for RHP Total Care members.
Prior AuthorizationClinical appropriateness approval is required before certain procedures will be covered. Prior authorization,precertification, predetermination and prior approval are often used interchangeably. This Summary PlanDescription (SPD) uses prior authorization. Many of our RHP Total Care network providers have detailedinformation about the process to ensure clinical appropriateness and will coordinate with the EHP MedicalManagement and/or Pharmacy Department to ensure that required prior authorization guidelines are met.Also, a complete list of medications that require prior authorization can be found in the Cleveland ClinicRHP Total Care Prescription Drug Benefit and Formulary Handbook.
Member Responsibility for Prior AuthorizationAs soon as a member learns from a physician that the services listed below are beingrecommended, he or she MUST call the EHP Medical Management and/or PharmacyDepartment:• Bariatric Surgery — see details on page 23.• Infusion for Migraine — see details on page 27.
It is to the member’s benefit to remind their physician/provider that this is a requirementso that claims payment issues can be avoided. The member is required to participatein the prior authorization/clinical appropriateness process for these services to ensurehis or her understanding of potential treatment options, to ensure the member hasparticipated in maintenance therapy before advancing to a more aggressive therapy,and to ensure the correct treatment in the correct setting. If the member does notparticipate in the prior authorization process before obtaining the service there willbe NO REIMBURSEMENT for the service.
16

17
Concurrent ReviewThis is a clinical appropriateness review for continued use of services that occurs either during a member’shospital stay or during the course of a prescribed treatment (e.g., inpatient stays, home care or skillednursing facility care).
Member Responsibility for Concurrent Review In the process of a concurrent review, a determination may be made that the hospitalstay or service is no longer clinically appropriate. In that case, the provider andmember will be notified via a letter that further services are being denied. The appealprocess will be outlined, but the member should be aware that he or she may beheld liable for all charges for continued services if the denial is upheld. It is up tothe member to discuss options for discontinuation of treatment and/or other optionsfor care with his or her physician or provider.
Prior authorization for clinical appropriateness and concurrent reviews are performed on either a prospectiveor concurrent timeline to assure appropriateness of admissions; continued length-of-stay and levels-of-carewithin inpatient facilities; and episode of treatment in the outpatient setting. The reviews are conducted as amechanism for assuring consistent procedures and treatment across the network and for the identificationof quality-of-care issues. The reviews are also done to identify discharge planning issues and to initiatedischarge planning in a timely fashion.
Any unauthorized programs, services, or visits will not be covered by RHP Total Care under any circumstancesand the subsequent charges will be the financial responsibility of the member. This applies to any unauthorizedout-of-network and out-of-area providers and facilities, with the only exception being for emergency care.
Business hours for the EHP Medical Management and Pharmacy Departments are from 8 a.m. until 4:30 p.m.Monday through Friday. If an urgent or emergency situation occurs, a Case Coordinator is on call afterbusiness hours and can be reached by calling the phone numbers below. These phone numbers are alsoon the back of your RHP ID card.
Cleveland Clinic EHP Medical Management and Pharmacy Departments6000 West Creek Road, Suite 20 • Independence, OH 44131
Phone: 216-986-1050 • Toll-Free: 1-888-246-6648 • Fax: 216-901-2050
Medical and Behavioral Health Services That Require Prior AuthorizationObtaining prior authorization for clinical appropriateness is the responsibility of the RHP Total Care networkprovider and, in some cases, the member (see Member Responsibility for Prior Authorization on page 16).
The following list includes those medical, behavioral health, and special services that must receive priorauthorization for clinical appropriateness, from the EHP Medical Management and/or Pharmacy Departments,prior to being rendered except for emergency/urgent situations:
Inpatient Services (both Medical and Behavioral Health)• Acute Rehabilitation Admission
• Elective Hospital Admission*
• All Inpatient Behavioral Health
• Out-of-Network and Out-of-Area Care (All) — See Emergency Care/Transfers on page 26
• Skilled Nursing Facility (SNF)/Transitional Care Unit (TCU)/Sub-Acute Admission
*May be subject to concurrent review

Outpatient Services• Behavioral Health
– Full spectrum light boxes– Intensive Home-Based Treatment– Intensive Outpatient (IOP)– Partial Hospitalization Programs (PHP)– Residential Treatment– Summer Treatment Program
• Medical– Breast Reduction– Botox– Capsule Endoscopies– Head, Cervical, Thoracic, Lumbar, and Lower Extremity MRI– Home Care– Home Use of Tocolytic Agents/Home Use of Uterine Monitoring– Infusion for Migraine– Neurofeedback and Biofeedback– Peripheral Nerve Stimulation– Potentially Cosmetic Procedures– Tilt Table Testing– Wound Vac– Vestibular Testing Battery– Durable Medical Equipment (DME)*:– ˚ Cochlear implants– ˚ Continuous glucose monitor and supplies– ˚ Continuous passive motion machines– ˚ Crutch substitute, lower leg platform, with or without wheels– ˚ Electric wheelchairs– ˚ Extension/Flexion (dynamic and bi-directional) devices– ˚ Fully automatic beds– ˚ High-end (hinged) braces– ˚ High-end prosthetics– ˚ High frequency chest wall oscillation system – ˚ Home oxygen therapy– ˚ Home CPAP or BiPap– ˚ Insulin Pumps and supplies– ˚ Low air loss beds– ˚ Non-standard size wheelchairs — lightweight/heavyweight– ˚ Osteogenesis stimulators – ˚ Pneumatic compression devices– ˚ Scooters– ˚ Speech assistance devices
*Reimbursement for DME will only be made at the established contracted rate for standard equipment. Anyrate differential for “deluxe” equipment will be the member’s responsibility.
18

19
Special ServicesThese services require prior authorization whether inpatient or outpatient:
• Autism specific services require prior authorization through the Autism School (prior authorization isthrough RHP).– Autism School– Outreach– Summer Treatment Program
• Bariatric restrictive procedures or malabsorptive procedures for weight reduction
• Experimental or Investigational treatments or procedures
• Hospice
• Human Organ or Bone Marrow Transplant
PharmaceuticalsSee the Prescription Drug Benefit and Formulary Handbook for a list of medications that require priorauthorization.
Care Outside of Tier 1 Cleveland Clinic RHP Total Care Network of ProvidersIn some cases, your Cleveland Clinic physician may wish to refer you for care outside of the Cleveland ClinicTier 1 network. This is appropriate for coverage under RHP Total Care only when medical or behavioralhealthcare cannot be provided within the Tier 1 network of providers. These services will be covered asa Tier 1 benefit if:
• The Cleveland Clinic EHP Chief Medical Officer authorizes the service before it is received.
• The service is determined to be clinically appropriate.
• The service is not available within the Cleveland Clinic Tier 1 network.
You and/or your physician should contact the EHP Medical Management Department prior to the servicebeing scheduled for further information.

Benefits Coverage Clarification
Services That Must Be Provided byRHP Total Care Tier 1 Providers
The following services are covered benefits ONLY when provided within the Tier 1 Networkof Providers AND Benefit Guidelines are met. There is NO coverage outside of the Tier 1Network of Providers.11. Autism/Outreach Program.12. Bariatric surgery.13. Botox for migraine.14. Breast reconstruction in connection with a mastectomy due to cancer.15. Chiropractic services.16. Cleveland Clinic Summer Treatment Program.17. Contact lens fitting (covered only when ophthalmologic condition cannot be corrected
by glasses).18. Custom-made orthotics.19. Dental implants for accidents or certain medical conditions.10. Family planning services.11. Genetic testing.12. Infusion for migraine.13. Left Ventricular Assist Device (LVAD).14. Neurofeedback and Biofeedback.15. Nutritional counseling.16. Outpatient cardiac rehabilitation programs.17. Protein Sparing Modified Fast (PSMF) diet.18. Psychological and Neuro-psychological testing.19. RAST (allergy blood) testing.20. Routine health maintenance tests, routine screening tests, and standard immunizations.21. Sclerotherapy or vein stripping for varicose veins.22. Services for long-term acute care.23. Services for routine eye and hearing examinations.24. Services for treatment of sleep apnea.25. Services provided for autism by the Cleveland Clinic Center for Autism.26. Services provided for the evaluation and conformity of hearing aids.27. Surgical extractions for soft/bony dental impactions.28. Temporomandibular Joint Syndrome (TMJ).29. Treatment for reduction mammoplasty.30. Vestibular testing battery.
20

21
Coverage Clarification The following pages (21 through 29) provide detailed benefit coverage clarification information about RHPTotal Care behavioral health and medical services. This information complements and further explains theBenefits Summary charts on pages 4, 5, 6 and 7 in Section One: “Getting Started.” Behavioral health, whichis listed first, includes all services for mental health and substance abuse. Medical services (pages 23 to 29),from bariatric surgery to vestibular testing, are defined and include additional information about coveragecriteria and co-payments.
Behavioral Health ServicesADHD Summer Treatment ProgramFull benefit coverage applies only if the child and parent each complete their designated portions of theprogram. Prior authorization and a clinical appropriateness review are required. RHP Total Care coveragefor the Summer Treatment Program is $2,000. The member is responsible for the difference between whatthe RHP Total Care covers and the billed charges for the program. An additional $500 will be covered ONLYif the parents participate in the parent education portion of the program. All outpatient social skills trainingfor children and adolescents with ADHD is covered as group therapy under the behavioral health outpatientbenefit.
AutismRHP Total Care will cover school, outreach program services, and the summer camp portion of Social SPIESfor Autism when provided by the Cleveland Clinic Center for Autism. A Financial Needs Assessment mustbe completed prior to determining RHP coverage. Members are required to notify RHP Total Care of anyoutside funding obtained for their child. If the child is enrolled in the Autism School Program and alsoreceives Outreach Autism Program services at the same time, the outside funding will be applied to theschool tuition costs and the parents will be responsible for covering the costs associated with the OutreachProgram services.
Benefit coverage is as follows and requires prior authorization through the EHP Medical ManagementDepartment.
• Autism School ProgramBenefit coverage for a school year is determined by the student’s age at the beginning of the school year(or at the start of services if other than September):< 4 years – 100%4 through 5 years – 50%> 6 years – 25 %
Although the benefit year is from January to December, RHP Total Care will reimburse the Autism Schoolfrom the dates of September through August and benefit coverage is determined by the student’s age as ofSeptember (or at the start of services if other than September). For example, a student starting the programin September at age three receives 100% coverage for the entire school year — the benefit coverage is notreduced for that school year when the student turns four.
Should outside funding such as state grants or scholarships be secured by the child’s parents, these fundsare applied to the total tuition cost, with the remaining tuition balance paid according to the benefitcoverage in effect at the time of enrollment.
Example: The total tuition cost for 2009-2010 school year was $67,020. If a $20,000 grant was secured,and the benefit coverage was 50%, the parent and RHP Total Care would both be responsiblefor $23,510 [$67,020 – $20,000 = $47,020 x 50% = $23,510].
• Outreach Autism ProgramBenefit coverage is determined by the student’s age at the beginning of the month the services are provided.
< 4 years – 100% > 4 years – 75 %
A student who turns four after the first day of any month receives 100% benefit coverage for that month.For example, a student turning four on March 5 receives 100% benefit coverage through March. Servicesprovided after March 31 are covered at 75%.
Call the EHP Total Care Customer Service Unit at 216-448-0800 or toll-free at 1-866-811-4352 for details.
• Center for Autism Social SPIES ProgramFull benefit coverage applies only if the child and parent each complete their designated portions of theprogram. Prior authorization for outpatient therapy and parent education is covered under the behavioralhealth outpatient benefit and count against the 35 outpatient visit maximum. RHP Total Care covers $2,000of the cost of the summer camp portion of the program. The member is responsible for the differencebetween what the RHP Total Care covers and the billed charges for the summer camp portion of theprogram. The Social SPIES program can be contacted for details.
Full Spectrum Light BoxesFor Seasonal Affective Disorder. Prior authorization and a clinical appropriateness review are required.Coverage is 80%. The member is responsible for all shipping and handling charges. Call the EHP MedicalManagement Department regarding supplier information. RHP Total Care does not provide coverage forfull spectrum light boxes for the purpose of treating a primary sleep disorder.
Intensive Home-Based TreatmentApproval for Intensive Home-Based Treatment (IHBT) is given on a case by case basis following a reviewwith the Chief Medical Officer. IHBT services are made available to individuals and their family and areprovided in the home by a specially trained behavioral health professional. Services are usually providedtwo to five times per week up to an average of four to 10 hours over several weeks. Prior authorization isrequired. Members are required to participate in Case Coordination to obtain this benefit.
Pain ManagementMembers in pain management programs that have a psychiatric component should contact the EHP MedicalManagement Department for prior authorization if the program is in Tier 2.
Psychological and Neuro-psychological TestingPsychological TestingUp to six hours of testing are automatically reimbursed without prior authorization. Testing is covered inTier 1 only.
Note: If more hours/visits than the Allowed Amounts listed above are utilized, the hours/visits will not be coveredby RHP Total Care under any circumstances and the subsequent charges will be the financial responsibilityof the member.
Neuro-psychological TestingUp to eight hours of testing are automatically reimbursed without prior authorization. Testing is coveredin Tier 1 only.
Note: If more hours/visits than the Allowed Amounts listed above are utilized, the hours/visits will not be coveredby RHP Total Care under any circumstances and the subsequent charges will be the financial responsibilityof the member.
22

23
Residential TreatmentResidential Treatment (RT): Room and board services are provided on a 24 hour per day basis in conjunctionwith a highly structured mental health and/or substance abuse treatment program. Residential Treatmentprograms are generally in non-hospital settings. The patient is able to participate in individual, group and/orfamily psychotherapy, as well as other activities and/or therapies that address the patient’s psychosocialneeds within a controlled environment. The focus of the treatment should be to resolve any problems withthe patient’s support system, as well as the development and maintenance of skills and behavioral changesthat will allow the patient to successfully reintegrate into the community. Halfway houses are not consideredto be Residential Treatment programs by RHP Total Care.
Approval for Residential Treatment will be determined by the Chief Medical Officer on an individual casebasis, following a review for clinical appropriateness. This level of care is only available to those memberswho have been referred to the EHP Medical Management Department. If approved there is a 30-day limit.Tier 1 reimbursement is 80/20% and Tier 2 is 70/30% after deductible.
Medical ServicesBariatric SurgeryTo be eligible for this benefit, a member must be a participant in RHP Total Care for a minimum of twoconsecutive years (see page 16). Second surgeries will not be covered (whether covered under RHP TotalCare or any other plan).
• Prior authorization is required through the EHP Medical Management Department. The member mustcall the EHP Medical Management Department when the workup begins to initiate the prior authorizationprocess.
• To be eligible for surgery, the member must meet the RHP Total Care’s established clinical criteria. Amember may qualify for surgery through the Bariatric Center, BUT NOT meet RHP Total Care clinicalcriteria. In this instance the surgery will not be authorized for reimbursement.
• Member must have a BMI greater than 40 for at least the preceding full year.
• Members with a BMI of 35 to 40 will be reviewed by the EHP Medical Management Department andapproval will require significant co-morbid(s) such as hypertension, diabetes, hyperlipidemia, or sleepapnea which are not amenable to maximum conservative treatment. Members must be enrolled inappropriate EHP Coordinated Care Programs and must be in both for six months prior to surgery.
• If a member with a BMI of 35 to 40 does not meet the above criteria and gains weight to reach a BMI of40, he or she will not be considered for surgery for one year.
• If approved, service is covered only when provided by Cleveland Clinic.
• If approved, all pre-workup physician visits require a $35 co-payment. Workup visits include diagnosticand laboratory tests, assessments by endocrinology, psychiatry/psychology, nutrition, general surgery,and possibly other specialists such as cardiology. It is estimated the total co-payment cost for physicianworkup visits will be $300 to $400.
• An upfront $2,750 co-payment is required for the surgical procedure.
• Repeat or revision bariatric surgeries are not covered.
Botox for MigraineBotox for chronic migraine requires prior authorization and will be approved when at least three preventivemedications have been tried (member must be compliant) and failed over a period of at least 90 days. Themember must be seen within six months of the request by a neurologist or headache clinic within Tier 1.
Breast ReconstructionBreast reconstruction is covered at 100% for a member who elects a breast reconstruction in connectionwith a mastectomy due to cancer or as prophylaxis. Services include the initial reconstruction of the removedbreast or breasts, and surgical revisions as needed on the reconstructed breast or breasts. If the breast isintact and “unaffected,” coverage is limited to one surgery if needed to produce a symmetrical appearance.Services must be provided in the Tier 1 network. Coverage includes treatment for postoperative complicationsof mastectomy and reconstruction surgeries.
Cataract SurgeryCataract surgery is a covered benefit under RHP Total Care for standard intraocular lenses. If the memberchooses to receive the Crystalens or ReSTOR lenses, RHP Total Care will only pay up to the contracted ratefor standard intraocular lenses. Crystalens and ReSTOR lenses are not considered standard and the memberwill be required to pay the difference from the standard lenses.
Chiropractic ServicesA maximum of 20 visits are covered per calendar year within the Tier 1 Network of Providers only. There is a$10 co-payment attached to the first 10 visits. The second 10 visits are reimbursed at 50% of the Allowed Amount.The member is financially responsible for 50%. X-rays done at the chiropractor’s office are a non-coveredbenefit. Patients under age 16 require prior authorization through the EHP Medical Management Department.Chiropractors are licensed to perform physical therapy. If the Chiropractor performs physical therapy, thevisit is counted as a Chiropractic visit. When there are both a chiropractic and physical therapy service, aco-payment will apply for each service. MRIs, regardless of the member’s age, ordered by a Chiropractorrequire prior authorization by the EHP Medical Management Department. If prior authorization is notobtained, the member may be responsible for payment.
Contact Lenses and Lens FittingsContact lenses and lens fittings will be covered only when an ophthalmologic condition that CANNOT becorrected by glasses, such as keratoconus, is present. Services must be provided by a Tier 1 Provider. Themember is responsible for submitting a letter from the servicing physician to the EHP Medical ManagementDepartment in order for the claim to be adjudicated appropriately.
Cosmetic Surgery Combined with Clinically Appropriate SurgeryIf a member chooses to have cosmetic surgery at the same time they are having surgery that is clinicallyappropriate, the coverage will be as follows:
• The professional fee for the cosmetic surgery will NOT be covered.
• The patient/member is responsible for 50% of the Allowed Amount for all technical/facility fees AND theanesthesia professional fee.
If the combined surgeries result in a hospital admission, the coverage will be as follows:
• If the usual course of the clinically appropriate procedure requires hospitalization, hospital days will becovered at 100%.
• If the usual course of the clinically appropriate procedure does not require hospitalization, the entirehospital charge is the patient/member’s responsibility.
Cosmetic surgery is always an excluded benefit. The treatment of complications resulting from cosmeticsurgery is also excluded. Life threatening complications that require inpatient care MAY be covered butmust be reviewed by the EHP Medical Management Department.
In addition, the EHP Medical Management Department reserves the right to retrospectively review these claimsand adjust them according to these guidelines. This means the member may be financially accountable forservices after they have been rendered.
24

25
DentalThis section pertains to dental benefits covered by RHP Total Care, NOT the Dental Plan. Questions aboutDental Plan coverage should be directed to the Benefits Department.
1. Dental Implants: Dental implants are covered under RHP Total Care when ALL of the following conditionsare met:• Implants are determined to be clinically appropriate and the medical need is primarily caused by a
specific medical condition or a recent (within one year) accident or injury. If clinical appropriatenessis determined due to an accident or injury within one year, the patient MUST have been an RHP TotalCare member at the time of the accident or injury to be eligible for coverage. Congenitally missing teethare covered for dental implant replacement.
• Prior authorization is required through the EHP Medical Management Department.• Services are performed within the Tier 1 Network of Providers.
If these conditions are met, the surgery (implant) and the prosthodontic (crown, bridge, etc.) will becovered under RHP Total Care. The implant will be covered at 100%. The coverage for the prosthodonticwill be 50%, up to a maximum of $1,250 annually. The prosthodontic coverage under RHP Total Careis the identical level of coverage as offered under the Cleveland Clinic Traditional Dental Plan.
2. Surgical Extraction for Soft or Bony Dental Impactions: • Surgical extraction for impacted teeth surgically removed is covered at 100% as long as services are
provided within the Tier 1 Network of Providers.• Treatment for non-impactions, which entails pulling of the teeth, is covered by the member’s Dental
Plan. For example, if all four of an employee’s wisdom teeth need removed, and only two are impacted,RHP Total Care covers the two teeth that are surgically removed. The other two are covered under theDental Plan. We recommend that you consult with your dentist and/or doctor before receiving treatment.
• Emergent surgical extractions follow Emergency/Urgent Care guidelines.
3. Anesthesia for dental procedures is NOT a covered benefit under RHP Total Care unless the dental procedureis one of the two procedures listed above. The only exceptions are cases where anesthesia is necessary todo dental work that is required because of an Underlying Medical Condition. These cases will be subjectto prior authorization through the EHP Medical Management Department. If approved, the anesthesiawill be reimbursed under the health plan but the dental work will not. Anesthesia for pediatric caseswhere extensive restoration is required will be covered for children under age seven and will requireprior authorization to meet medical necessity criteria. Anesthesia is also covered for members with certainunderlying medical conditions and also requires prior authorization.
4. Dental procedures such as root canals, crowns, caps, re-implantation, etc. are NOT covered underRHP Total Care even if they are recommended because of a minor accident or injury. The EHP MedicalManagement Department will review cases of severe trauma, in which major reconstruction is required,prior to services being rendered.
DXA Scans (Bone Density)One screening is covered every two years for women over 65 and men over age 70.
Screening for members under these ages or in need of more frequent scans are covered only if clinicallyappropriate.
Durable Medical Equipment (DME)Reimbursement for DME will only be made at the established contracted rate for standard equipment.Any rate differential for “deluxe” equipment will be the member’s responsibility. Over-the-counter DMEproducts are not a covered benefit (e.g., breast pumps).
• If the contracted rate is less than the amount of the co-payment, the member is still responsible for thecorresponding co-payment/co-insurance.
Emergency Care/TransfersEmergency and Urgent Care are covered at 100% regardless of the provider as long as the visit meets Emergencyor Urgent Care criteria as defined in Section Seven: “Terms and Definitions” on pages 61 and 63 respectfully.A co-payment is required for any emergency department visit that does not result in an admission.Observation stays in the hospital are not considered admissions.
Emergency transport to an emergency room, even if it is a non-Cleveland Clinic facility, is always covered.
Ambulance transport to home from any healthcare facility or to/from physician or outpatient care visits arenot covered.
The following information addresses transfers to a Cleveland Clinic facility:
Transfers from Within a 50-Mile Radius of the Cleveland Clinic Main Campus RHP Total Care will cover the transfer of our members from out-of-network facilities within a 50-mile radiusof the Cleveland Clinic main campus. Total Care requires members, family members or the admittinghospital/emergency room staff to contact the Cleveland Clinic transfer center at 1-866-721-9803 if the memberrequires admission to a non-Cleveland Clinic facility. This number is on the back of your medical ID card.
If a member is mentally incapacitated, and in the absence of family members who can make the contact,hospital staff can make the contact as soon as possible. In the event that a member is admitted to a non-Cleveland Clinic facility, the EHP Medical Management Department will make a determination if a transferwill be required.
Failure to contact the transfer center, if it was feasible, prior to admission, or refusal to accept the transferto a Cleveland Clinic facility when indicated by the transfer center or Medical Management, may result inTier 2 coverage or no coverage for the admission.
Transfers from Outside a 50-Mile Radius of the Cleveland Clinic Main CampusRHP Total Care may transfer members from a non-network facility outside of a 50-mile radius of the ClevelandClinic main campus to a Cleveland Clinic facility. All cases will be reviewed by the EHP Medical Director forappropriateness of transfer. If the member or family member would like to request a transfer, they shouldcontact the Cleveland Clinic transfer center at 1-866-721-9803 or Case Coordination at 1-888-246-6648 torequest a transfer.
Enteral FeedingsEnteral feedings, food supplements, lactose-free foods, specialized formulas, vitamins and/or mineralsthat do not require a prescription are not covered, even if they are required to maintain weight or strengthand regardless of whether these are prescribed by a physician.
Genetic TestingIf clinical appropriateness is determined, genetic testing is a covered benefit for a member or a member’scovered dependent. It is not covered when the service does not benefit the insured or the insured’s covereddependent.
Hair LossReimbursement will be made up to a $250 lifetime maximum for a cranial protheses (wig) and only as a resultof hair loss due to chemotherapy or radiation treatments and/or alopecia areata. The wig can be purchased fromthe provider of choice. Receipts must be submitted to RHP.
Hearing AidsHearing aids are covered at 50% of billed amount up to $3,500 per ear; one aid per ear every three yearswithin the Tier 1 Network of Providers. Evaluation, consulting, and dispensing fees are covered at 100%within the Tier 1 Network of Providers. Repair of hearing aids ARE NOT covered. There is NO coverage ofthe hearing aids, evaluation, consultation, or dispensing fees OUTSIDE of the Tier 1 Network of Providers.
26

27
HospiceTo be eligible to receive the hospice benefit, patients must have a life expectancy that is less than six months andhave a caregiver(s) in the home 24 hours a day, 7 days a week. The four levels of service that are included inthe benefit are: routine home care, continuous home care, inpatient respite care, and general inpatient care.Inpatient respite care provides rest and relief for the patient’s primary caregivers. General inpatient care providespain and symptom management not possible in the home setting. Services that are NOT covered under thehospice benefit include: custodial and/or experimental therapies. Notification to the EHP Medical ManagementDepartment is required for coordination of care. Hospice Respite Care is limited to 10 days per calendar year.
ImmunizationsStandard immunizations are covered only when given within the Tier 1 Network of Providers. Tetanus toxoid,Rabies vaccine, and Meningococcal polysaccharide vaccines will be covered outside of Cleveland Cliniconly if they are given as part of Emergency/Urgent Care Services. Hepatitis A is covered for children 12 to23 months. Outside this age group, Hepatitis A requires prior authorization for a medical condition. It isNOT covered for travel or when required for school.
Gardasil and Cervarix are vaccines for HPV and are covered for males and females age 9 to 26. Zostavax iscovered for adults over age 50.
Immunizations are covered under your medical benefit, not the Prescription Drug Benefit. If a physician asksyou to fill a prescription for an immunization, it will not be covered. Please call the EHP Medical Managementand/or Pharmacy Department at 1-888-246-6648 for assistance.
InfertilityCoverage for infertility is limited to diagnostic services only.
Infusion for MigraineInfusion for migraine requires prior authorization and will be approved only when maximum conservativeabortive therapy has been tried and failed over a period of four days. Members requesting more than twoinfusion therapy visits in a six month period must be compliant with preventive medications. Clinicalinformation will be required from the physician ordering the treatment. The member is responsible forobtaining prior authorization before obtaining services for maximum reimbursement (see page 16).
IUD and Depo-Provera GuidelinesIUD insertions are a form of birth control; and in most cases, Depo-Provera is used as a birth control method.
IUD insertions are a form of birth control and therefore will have a $50 co-payment charge at the provider’soffice.
If Depo-Provera is used as a birth control method, the member will be charged the Prescription Drug Benefitco-payment of $15 per injection when supplied by a doctor’s office. Standard co-payment rates are chargedif Depo-Provera is purchased at a pharmacy.
Maternity CareA one-time $50 co-payment for each pregnancy is required for maternity services. However, if you changeobstetricians during a pregnancy, an additional $50 co-payment will be required. The co-payment coversroutine physician visits throughout the pregnancy, as well as the six week follow-up visits. Routine is definedas 12 physician visits and approximately two ultrasounds for a normal pregnancy. More than the definednumber of visits or visits to a specialist will require additional co-payments.
RHP Total Care does not restrict benefits for any hospital length of stay in connection with childbirth formother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours followinga cesarean delivery. However, RHP Total Care will not prohibit the mother’s or newborn’s attending provider,after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours or 96 hours,as applicable. In any case, RHP Total Care will NOT require that a provider obtain authorization from theEHP Medical Management Department or the Third-Party Administrator for prescribing a length of stay notin excess of 48 or 96 hours. Doula services are NOT considered clinically appropriate and therefore are NOTa covered benefit. If you would like coverage for your newborn, you have 31 days from birth to add the babyto Cleveland Clinic Employee Health Plan Total Care. Contact the Benefits Department at 216-448-0600.
Orthotics• Custom-made: covered at 80% of Allowed Amount after $50 co-payment in the Tier 1 Network of
Providers only.
• General: not a covered benefit.
• If the contracted rate is less than the amount of the co-payment, the member is still responsible for thecorresponding co-payment/co-insurance.
Orthopedic shoes and diabetic shoes are not considered orthotics.
Pain ManagementTreatments, such as injections, are covered up to three injections per specific anatomical site per benefityear. More than three injections per specific site require prior authorization through the EHP MedicalManagement Department. Members in programs that have a psychiatric component should contact the EHPMedical Management Department for prior authorization of that component of their pain managementprogram if the program is in Tier 2. Tier 2 Behavioral Health counseling sessions require prior authorizationthrough the EHP Medical Management Department.
PAP/HPV Testing• Screening Pap/HPV tests are covered once every three years over age 30. A pelvic exam is still recommended
as part of the yearly physical; however, a Pap smear is not necessary.
• Diagnostic Pap smears are covered as needed for previous abnormal Pap or previous positive high riskHPV subtype.
• Women under 30 who are sexually active should have an annual Pap smear with their examination. AnHPV test is needed only if there is an abnormal Pap smear.
• Women of any age whose cervix has been removed during a hysterectomy have no coverage for Pap/HPV.
Members will be held financially responsible if they receive the tests more frequently without a medicalcondition.
Screening Pap smears will be covered once every three years and diagnostic Pap smears will be covered asneeded. Members will be held financially responsible if they receive the tests more frequently without amedical condition.
Personal GroomingReimbursement will be made up to a $250 lifetime maximum for a cranial protheses (wig) and only as a resultof hair loss due to chemotherapy or radiation treatments and/or alopecia areata. The wig can be purchased fromthe provider of choice. Receipts must be submitted to RHP.
RAST (Allergy Blood) TestingRAST testing (allergen specific IgE blood testing) will be covered if obtained by a Tier 1 network provider only.
Routine (Annual) Vision ExaminationOne routine (annual) vision examination is covered in a 12-month period in the Tier 1 network. Examinationsare not covered under the Cleveland Clinic Vision Plan. The Vision Plan covers hardware only. Services forcontact lenses and lens fittings are not a covered benefit unless the contact lenses are required because ofan ophthalmologic condition that cannot be corrected by glasses.
Spider Veins and Varicose Veins• Spider veins — Sclerotherapy is NOT a covered benefit.
• Varicose veins:– Sclerotherapy for symptomatic varicose veins is covered at 100% after a $50 co-payment per session; and– Vein stripping for symptomatic varicose veins is a covered benefit in the Tier 1 Network of Providers only.
28

29
Temporomandibular Joint Syndrome (TMJ) The treatment of TMJ is limited to $10,000 lifetime and is covered at 100%. Services must be received withinthe Tier 1 Network of Providers.
TherapyOccupational*26 visits per calendar year are covered after a $10 co-payment per visit. There is no prior authorizationrequirement.
Physical*26 visits per calendar year are covered after a $10 co-payment per visit. There is no prior authorizationrequirement.
Speech*26 visits per calendar year are covered after a $10 co-payment per visit. There is no prior authorizationrequirement.
Note: Additional visits require prior authorization and a $10 co-payment per visit is still applicable.
*Services are not a covered benefit when they are for non-medical conditions. Non-medical conditions include, butare not limited to, impulse control disorders and conduct disorders. Refer to Prior Authorization and ConcurrentReview for Clinical Appropriateness rules on page 16 for more information.
Vestibular Testing BatteryVestibular testing battery, used by some physicians to determine the causes of dizziness and vertigo, requiresprior authorization. The provider will be responsible for forwarding the following clinical information:
• Prior consultation by ENT or neurology.
• History of persistent (at least one month) and severe repeat episodes of vertigo for which diagnosis is notbenign positional vertigo.
Case CoordinationCleveland Clinic Retiree Health Plan (RHP) Total Care is committed to helping you and your family stayhealthy. However, if faced with medical illness, we are also committed to helping you with important decisionsto ensure that you get the healthcare you need.
The EHP Medical Management Department offers Case Coordination Programs that provides members withtelephone access to a Case Coordinator (Registered Nurse or Licensed Social Worker/Counselor) for assistancewith complex medical care needs, complex behavioral health needs, network access issues, and referralsto community services. Members can self-refer or be referred by their physician or family for evaluation.
Case Coordination Programs for medical conditions include End-Stage Renal Disease, high-risk maternity,complex care needs, palliative care needs, and transplant coordination, among others. Behavioral HealthCase Coordination Programs include anxiety disorders, childhood disorders, dual diagnoses, eating disorders,mood disorders, psychotic disorders, and substance abuse. Members requesting more than 35 outpatientvisits in a calendar year for behavioral health or substance abuse must agree to participate in EHP CoordinatedCare (see pages 30 to 32).
Case Coordinators also make courtesy calls to members who have repeat emergency room visits, repeatinpatient stays within 90 days or have an inpatient stay with a length-of-stay of five or more days to assessfor any post discharge care needs.
If you have a medical or behavioral health question related to a Case Coordination Program, the EHP MedicalManagement Department can be reached at 216-986-1050 or toll-free at 1-888-246-6648 during regularbusiness hours of 8 a.m. to 4:30 p.m. Monday through Friday, excluding holidays. A confidential voicemailbox is available to accept non-urgent messages after hours.
Coordinated CareEHP Medical Management offers Chronic Disease Management, Health Promotion, and Rare DiseaseManagement programs that address the self-management needs of members with chronic illnesses.Conversations with a Registered Nurse Care Coordinator will assist you in learning ways to stay feelingyour best and will work closely with you and your doctors to provide you with valuable information aboutyour condition, including ways to monitor progress and prevent complications. EHP Coordinated CarePrograms focus on education and self-management strategies, with a goal of improving overall healthand promoting the best quality of life. These programs are designed to compliment your doctor’s care,reinforcing recommendations so you stay healthier between office visits. The programs are offered atno extra cost to you and participation is completely voluntary.
If you have a condition addressed by one of the Coordinated Care programs and would like to join a program,please call the EHP Medical Management Department at 216-986-1050 or toll-free at 1-888-246-6648 duringregular business hours of 8 a.m. to 4:30 p.m. Monday through Friday. A referral from your physician is notnecessary.
Chronic Disease ManagementFeatures of the programs are based on individual specific health issues and may include:
• Monthly phone assessment interviews from a Registered Nurse Care Coordinator
• Educational mailings
• Referral to community resources
• Referral to informative websites
Continued program compliance can earn you prescription co-insurance reimbursement for some or all ofyour medications. Chronic Disease Management programs are outlined below. Contact the EHP MedicalManagement Department for more details.
Asthma (for adults and children)Learn how to identify and avoid personal asthma triggers and how to self-manage your condition using anasthma action plan.
Chronic Kidney DiseaseThis program is designed to help members learn what can be done to postpone or even prevent the needfor dialysis treatments.
Depression (for adults and children)Learn how working with an appropriate therapist, along with the right medications, can help you balancea more effective response to depressed mood stressors and triggers.
Diabetes (for adults and children)Learn how to control this condition through nutrition, diet, medication and regular monitoring throughperiodic physician visits and blood tests for hemoglobin A1c, cholesterol and kidney function.
Heart Failure (CHF)Learn how to improve and maintain your activity level by tracking your weight, watching your sodium intakeand recognizing symptoms early enough to prevent congestion in your lungs.
Hyperlipidemia (High Cholesterol)Learn what to do to bring your elevated LDL (bad) cholesterol level under control. Receive educationalmaterials on what your lipid panel numbers mean and become aware of how simple changes in your diet,activity level and medication routines can improve your heart health.
30
31
Hypertension (High Blood Pressure)Learn the importance of routine home blood pressure monitoring in combination with medication, dietand exercise compliance to prevent long-term health complications.
Migraine (for adults and children)Learn how to keep a headache diary to help identify and avoid your specific triggers and recognizing earlysigns of a migraine. Learn the difference between prophylactic and abortive medications and which kindsyou should talk to your doctor about.
The EHP Medical Management Department can be reached at 216-986-1050 or 1-888-246-6648 duringregular business hours of 8 a.m. to 4:30 p.m. Monday through Friday, excluding holidays. A confidentialvoicemail box is available to accept non-urgent messages after hours.
Health Promotion ProgramsPre-DiabetesLearn the important yet simple lifestyle changes you can start to prevent or postpone the onset of diabetes.
Prenatal CareLearn about timely topics during each trimester of your pregnancy, stay on time with your prenatal doctorvisits and earn your delivery co-payment back when you share your birth details with us.
Rare Disease ManagementAll medical conditions present challenges. But some diseases, often classified as “rare,” can be especiallydevastating physically and emotionally — and not just for the members who are diagnosed, but also fortheir families.
Cleveland Clinic RHP Total Care is partnered with Accordant Care, a CVS Caremark Company, to providemembers with a Rare Disease Management Program that specializes in 17 uncommon conditions. Thisprogram is voluntary and is provided at no additional cost to members. Incentives are also available forthese programs. Details are available through the Case Coordinator.
Members who enroll in the program will receive the latest information about their conditions, help inmanaging co-morbidities and services provided by RN case managers who will communicate and coordinatewith pharmacy staff, PCPs and specialists to help members maintain continuity, consistency and qualitycare. Rare Disease Management Program staff will work with the EHP Medical Management Departmentto ensure our members receive seamless, quality care within our network.
The complex, rare conditions covered under this program are:
• Amyotrophic lateral sclerosis (ALS)
• Chronic inflammatory demyelinatingpolyradiculoneuropathy (CIDP)
• Crohn’s disease
• Cystic Fibrosis
• Dermatomyositis
• Gaucher disease
• Hemophilia
• Lupus
• Multiple Sclerosis
• Myasthenia Gravis
• Parkinson’s disease
• Polymyositis
• Rheumatoid Arthritis
• Scleroderma
• Seizure disorders
• Sickle Cell Anemia
• Ulcerative Colitis
Accordant Care can be reached at 1-866-637-6340 during regular business hours of 8 a.m. to 4:30 p.m. Mondaythrough Friday, excluding holidays. A confidential voicemail box is available to accept non-urgent messagesafter hours.

32
Prescription Drug Coverage Under MedicareThe Medicare Prescription Drug Improvement and Modernization Act of 2003 (MMA) includes a prescriptiondrug program to Medicare Part D for individuals who are enrolled in Medicare.
Typically, individuals become “entitled to” Medicare Part A when they reach age 65 and receive Social Securitybenefits. An individual is eligible for Medicare Part D Prescription Drug Benefits if covered by MedicarePart A and/or enrolled in Medicare Part B. Individuals under age 65 may also become entitled to Medicarebenefits if they receive at least 24 months of Social Security benefits based on disability.
Cleveland Clinic Retiree Health Plan Total Care members potentially eligible for Medicare Part D include:
• Active working employees who become Medicare eligible;
• Dependents (such as spouses) of active working employees who are Medicare eligible;
• Disabled dependents (e.g., children) eligible for Medicare; and
• Long-Term Disability (LTD) recipients who become Medicare eligible.
All Medicare prescription drug plans provide a standard level of coverage established by Medicare. Someplans, however, offer additional coverage for a higher premium.
Cleveland Clinic Retiree Health Plan Total Care determined that your existing coverage with RHP TotalCare is as good as standard Medicare coverage. In many cases, coverage under RHP Total Care actuallyexceeds the standard Medicare coverage.
If you should become Medicare eligible, it is important that you evaluate both the RHP Total Care’s SliverScriptPrescription Drug Benefit and the Medicare Prescription Drug Benefit to determine which plan best meetsyour specific needs. Compare your current coverage, including which drugs are covered, with the drug coverageand cost of plans offering Medicare Prescription Drug Benefits before making a decision to enroll with aMedicare program.
It is important to note that if you enroll in a Medicare Part D plan other than through the RHP SilverScript,you may no longer participate in RHP Total Care. You will lose both your Cleveland Clinic medical andpharmacy benefits and will not be eligible to return to RHP Total Care in the future.
Detailed information about the Medicare prescription drug plans that offer prescription drug coverageis available on Medicare’s website at www.medicare.gov or by calling Medicare at 1-800-MEDICARE(1-800-633-4227). TTY users should call 1-877-486-2048.
Contact Cleveland Clinic Employee Health Plan Total Care Customer Service Unit with further questionsabout SliverScript at 216-448-0800 or toll-free at 1-866-811-4352.
33
Prescription Drug BenefitThe RHP Prescription Drug Benefit is administered through CVS Caremark under the guidance of the EHPPharmacy Coordination Department and is divided into two groups: Non-Medicare eligible and Medicareeligible.
The non-Medicare eligible retirees are insured under CVS Caremark. The Medicare eligible retirees areinsured under SilverScript Insurance Company. SilverScript is an affiliate of CVS Caremark and is anapproved Medicare Part D Prescription Drug Plan provider.
Both CVS Caremark and SilverScript have dedicated toll-free Customer Service phone numbers e-mail orwebsite addresses available 24 hours a day, seven days a week:
CVS Caremark SilverScript1-866-804-5876 1-866-693-4617
E-mail: [email protected] Website: https://clevelandclinic.silverscript.com
Both websites provide information for your applicable plan such as:• Prescription Refills for CVS Caremark Mail Service • Frequently Asked Questions• Order Status • 13 Month Drug History• Pharmacy Locations • Additional Health Information• Benefit Coverage • Drug Formulary (List of covered drugs)• Request Forms
When you call CVS Caremark or SilverScript, or visit their website, please have the following informationavailable:• Member’s ID Number• Member’s Date of Birth• Payment Method
The Prescription Drug Benefit and Formulary Handbook provides detailed information on prescription drugdelivery options which include Cleveland Clinic Pharmacies, CVS Caremark Retail, and home delivery programsfor both SilverScript members and CVS Caremark members.

34
ExclusionsCleveland ClinicRetiree Health Plan Total Care Coverage ExclusionsCoverage Is Not Provided for the Following Services and Supplies:
General Exclusions11. Treatment that is not a covered service, even if authorized or deemed clinically appropriate by your
physician.
12. Care which is not clinically appropriate and/or has not received prior authorization. If prior authorizationis required and NOT obtained, RHP Total Care is not obligated to reimburse for services even if it is acovered benefit.
13. Any treatment not recommended or approved by a physician or medical provider.
14. Medical services that do not benefit the insured (e.g., organ donation or genetic testing).
15. Services ordered or provided by a member of your immediate family.
16. Services that are not reasonable or necessary for the diagnosis or treatment of sickness or injury, includinga non-clinically appropriate circumcision for a non-newborn or non-newly adopted child (up to one yearafter adoption), or any services associated with the use of general anesthesia when local anesthesiawould be acceptable.
17. Expenses payable in your behalf under Medicare, whether you are enrolled or not.
18. Expenses paid by another Healthcare Plan.
19. Services received under the following circumstances:• Physical examinations or services required by an insurance company to obtain insurance;• Physical examinations or services required by a governmental agency such as the Federal Aviation
Administration, Department of Transportation, and Immigration and Naturalization Services;• Physical examinations or services required by an employer in order to begin or continue working,
unless clinically appropriate;• Premarital examinations and associated required testing; or• Physical examinations or screening test for professional school or private school.
10. Services provided at no charge or that normally would not generate a charge in the absence of this oranother insurance plan.
11. Services provided by a hospital or institution maintained by the U.S. government.
12. Treatment for any sickness or injury caused by war, acts of war or similar events — whether the war isdeclared or undeclared.
13. Treatment for sickness or injury contracted while in any branch of the armed forces.
14. Treatment for sickness or injury incurred while committing a felony, or other criminal activity.
15. Expenses reimbursed for which you are entitled to reimbursement through any public program.
16. Services or expenses that are prohibited by laws in the area in which you live.
17. Charges in connection with an occupational injury covered by workers’ compensation.
18. Services for educational, vocational, or training purposes unless for an underlying medical condition.
19. Services of any kind for developmental, diversional, or recreational purposes.
20. Charges associated with telephone consultations, missed appointments, completion of claim forms,or copies of medical records.
21. Expenses associated with custodial, domicillary, convalescent or intermediate care.
22. Hospitalization for “rest cures” or convalescence in a nursing home.

35
23. Charges incurred for care in which the member left the medical facility against medical advice (AMA).
24. Bathroom convenience items including but not limited to tub rails, handrails and elevated toilet seats.
25. Charges for experimental or investigational procedures, drugs, devices, or medical treatments.
26. Marymount Hospital employees are subject to family planning exclusions, including all abortions,vasectomy, Norplant, Depo-Provera, IUD, tubal ligation, and oral contraceptives unless clinicallyappropriate.
27. Services related to gender reassignment.
28. Services that would normally be reimbursed by Corporate Health.
29. Personal clothing or comfort items such as orthopedic shoes, diabetic shoes, wigs, or hygiene items.
30. Non-covered services or services specifically excluded in the text of this Summary Plan Description.
31. Care that occurred prior to your effective date or after your coverage has been terminated.
Medical Coverage Exclusions32. Expenses solely for cosmetic procedures or complications from cosmetic procedures.
33. Expenses for the treatment of obesity, with the exception of registered dietician services, unless treatmenthas received prior authorization through the EHP Medical Management Department.
34. Services or expenses incurred for a second bariatric surgery.
35. Charges associated with teeth or periodontia unless specifically defined elsewhere in this SummaryPlan Description.
36. Reversal of voluntary infertility.
37. Services for couples in which either partner has undergone a sterilization procedure, with or withoutsurgical reversal, or in which the woman has had a hysterectomy, unless there are unique circumstancesas determined by the EHP Medical Management Department.
38. Costs associated with the acquisition of donor sperm or donor.
39. Costs associated with cryopreservation of sperm, eggs, or embryos for any reason.
40. Any new technology used in an experimental or investigational program.
41. Drugs related to the treatment of non-covered benefits or related to the treatment of infertility that arenot clinically appropriate based on current medical standards, including but not limited to IVIG.
42. Charges associated with a gestational carrier program (surrogate parenting) for the member or thegestational carrier unless the member has congenital absence of the uterus or a traumatic insult tothe uterus.
43. Coverage for infertility is limited to diagnostic services only.
44. Doula services.
45. Enteral feedings, food supplements, lactose-free foods, specialized formulas, vitamins and/or mineralsthat do not require a prescription are not covered, even if they are required to maintain weight or strengthand regardless of whether these are prescribed by a physician.
46. Services provided for fitting of contact lenses unless the contact lenses are required because of anophthalmologic condition that CANNOT be corrected by glasses.
47. Any surgical procedure for the correction of a visual refractive problem including, but not limited to,radial keratotomy and LASIK (laser in situ keratomileusis).
48. Hearing aid accessories.
49. Charges associated with the rental or purchase of durable medical equipment (DME) when rental expenseexceeds purchase price, or for replacement of equipment that can be repaired.
50. Sales tax on medical supplies/DME items.
51. Over-the-counter DME products, (i.e., breast pumps).
36
52. Rehabilitation (lift) chairs.
53. Home defibrillators.
54. Take home supplies.
55. Cardiac rehab stages 3 and 4.
56. General orthotics that can be purchased over-the-counter including devices such as splints, shoe inserts,arch supports, and braces.
57. Retrieval and implantation of non-human or artificial organs.
58. Harvesting of human organs or bone marrow when the recipient is not an RHP Total Care member.
59. Hypnosis.
60. Charges for acupuncture treatment.
61. Massage therapy even if provided by a physical therapist.
62. Alternative and homeopathic therapies.
63. Alternative Care Programs.
64. X-rays taken in a chiropractor’s office.
65. Treatment for paring of corns and calluses or trimming of toenails, unless the patient has complicationsassociated with circulation or diabetes.
66. Full body CT scans.
67. Quantitative Sensory Testing (QST).
68. Hepatitis A Immunization unless member has received prior authorization by the EHP MedicalManagement Department.
69. Nasal flu vaccine, FluMist for members greater than 18 years of age. (FluMist is covered for membersages 2 to 18.)
70. Travel Clinic and related services (e.g., immunizations, medications).
71. Sclerotherapy for spider veins.
72. Unattended electrical stimulation.
73. Cervical home traction units.
74. Services for treatment of infertility.
75. Ambulance transport to home from any healthcare facility or to/from physician or outpatient care visits.
Behavioral Health Coverage Exclusions76. Treatment, testing, or forensic evaluations that are Court ordered or recommended as a condition of
probation or parole or for any other reason including child custody. This applies to residential, inpatient,PHP, IOP, or outpatient levels of care. Approval may be considered for first time treatment episodes onlywith prior authorization from the EHP Medical Management Department. Repeat treatment episodesin this category are not covered.
77. Services for mental illnesses that cannot be treated; however, services to determine if the mental illnessis treatable are covered.
78. Services for mental deficiency or mental retardation, except for services rendered for necessity of evaluationof diagnosis of mental deficiency or retardation.
37
79. Athletic performance enhancement training, evaluation, or counseling.
80. Services required by an employer in order to begin or continue working, unless they are clinicallyappropriate and have received prior authorization from the EHP Medical Management Department.
81. Services for weight control or reduction that are not related to a primary Axis I disorder such asAnorexia or Bulimia.
82. Behavioral modification programs unless authorized through the EHP Medical Management Department.
83. Report writing and/or court testimony for any purpose.
84. School meetings for any purpose.
85. Time spent traveling or travel expenses incurred by a service provider.
86. Any travel expenses for a member other than for emergency transport by a private ambulance serviceor non-emergent transport that has received prior authorization from the EHP Medical ManagementDepartment.
87. Residential level of care solely for the purpose of treating nicotine and/or smoking addictions (excludingmarijuana).
88. Halfway houses.
89. There is no coverage for telephone counseling services or school meetings by outpatient behavioralhealth practitioners.
Prescription Drug Benefit Exclusions90. The replacement of lost or damaged prescriptions.* Stolen medications will be covered at the plan rate
when accompanied by a police report.
91. Drugs prescribed for the treatment of sexual dysfunction.
92. Drugs to enhance libido function.
93. Enteral feedings, food supplements, lactose-free foods, specialized formulas, vitamins and/or mineralsthat do not require a prescription are not covered, even if they are required to maintain weight or strengthand regardless of whether these are prescribed by a physician.
94. Drugs used for experimental or investigational purposes.
95. Drugs that can be purchased without a prescription.
96. Drugs used for cosmetic purposes.
97. Drugs used for the treatment of infertility.
98. Drugs not included in the Patient Protection and Affordable Care Act that can be purchased withouta prescription.
*Members may contact Pharmacy Coordination at 216-986-1050, option 4 or toll-free at 1-888-246-6648,option 4 between the hours of 8 a.m. and 4:30 p.m., Monday through Friday to request an override so thatthey are able to purchase a replacement supply at their expense. The member will be responsible for 100%of the discounted price.
Refer to the Prescription Drug Benefit charts on page 6 (for non-Medicare eligible) and page 7 (for Medicareeligible) to see the Drugs & Items at Discounted Rate and Non-covered Drugs & Items for additional exclusions.
38
Cleveland Clinic Retiree Health Plan Total CareThird-Party Administrator (TPA) Mutual Health Services (MHS)Cleveland Clinic Retiree Health Plan (RHP) Total Care is partnered with Mutual Health Services (MHS) toadminister your health plan benefits accurately and efficiently. Mutual Health Services provides claimsprocessing for all members who receive healthcare services and functions as the Third-Party Administrator(TPA) for Cleveland Clinic RHP Total Care. In this role, they are responsible for:
1. Member eligibility verification
2. Benefit coverage determinations
3. Processing claims and claims appeals
4. Issuing statements of Explanation of Benefits (EOB)
5. Coordinating benefits if a member is covered by more than one health plan
6. Subrogation processing
Information regarding contacting Mutual Health Services is available in the Quick Reference Guide on page 9.
Coordination of Benefits (COB)Coordination of Benefits (COB) is the process used to pay healthcare expenses when you or an eligibledependent is covered by more than one healthcare insurance policy, including Medicare. Annual healthcareexpenses for EHP Total Care exceeds $250 million per year. Coordination of Benefits helps achieve costsavings for members.
If you/your dependents are covered by more than one healthcare insurance policy, the TPA follows rulesestablished by Ohio law to decide which healthcare insurance policy pays first (primary plan) and theobligations of the other healthcare insurance policy (secondary plan). The combined payments of allhealthcare insurance policies will not exceed the actual amount of your bills. See Section One: “GettingStarted” for information about completing the COB form to ensure that your dependents’ healthcareclaims will be paid.
Medicare CoordinationWhen you or your covered dependent become Medicare eligible and retire, it is important for you to enrollin Medicare Part B. Cleveland Clinic Retiree Health Plan (RHP) Total Care becomes the secondary insuranceonce you become Medicare eligible. This means that if you do not enroll in Medicare Part B, you will beresponsible for 80% of your physicians’ bills (out of your pocket) because RHP Total Care pays only 20%(what Medicare does not pay) as the secondary insurance.
In order for this claims payment process to work correctly, it is EXTREMELY IMPORTANT that you bringboth your Medicare and RHP ID cards to all visits and inform the registrar that you are covered by two healthplans. If you have more than these two plans, bring ALL the health plan cards you have to the visit so thatcoordination of benefits can be done correctly.
Section Four
THIRD-PARTY ADMINISTRATOR —MUTUAL HEALTH SERVICES
39
Medical plan benefits provided are also subject to the following non-duplication provision:
• The combined payments of all healthcare plans will not exceed the actual amount of your bills. In other words, you cannot expect to receive benefits in excess of 100% of the cost you incur and receivereimbursement on claims through both RHP Total Care and any other company sponsored plan whereyou have coverage.
Process for Determining Which Health Plan Is PrimaryTo determine which health plan is primary, the TPA has to consider both the coordination of benefit provisionof the other health plan and which member of your family is involved in a claim. The primary health planwill be determined by the first of the following that applies:
1. Non-Coordinating Plan: If you have another group plan that does not coordinate benefits, it will alwaysbe primary.
2. Children:• Birthday Rule — When your children’s healthcare expenses are involved, the TPA follows the “birthday
rule.” The birthday rule states that the health plan of the parent with the first birthday in the calendaryear is always primary for the children. For example, if your birthday is in January and your spouse’sbirthday is in March, your health plan will be primary for all of your children.
• Gender Rule and other Health Plan Rules — Sometimes a spouse’s health plan has some other coordinationof benefits rule, such as a gender rule, which states that the father’s health plan is always primary. Incases of the gender rule or other specific health plan coordination of benefits rules for children, theTPA will follow the rules of that health plan.
3. Children (Parents Divorced or Separated):
• If the court decree makes one parent responsible for healthcare expenses, that parent’s plan is primary.
Note: Cleveland Clinic Retiree Health Plan Total Care reimburses claims according to its plan rules(i.e., network requirements must be adhered to even if a court decree dictates the Cleveland Clinicretiree’s health insurance is primary for children living outside of the Network of Providers).
• If the court decree gives joint custody and does not mention healthcare, the TPA follows the birthday rule.
• If neither of those rules applies, the order will be determined in accordance with the Ohio Departmentof Insurance rule on coordination of benefits.
4. Other Situations: For all other situations not described previously, the order of benefits will be determinedin accordance with the Ohio Department of Insurance rule on coordination of benefits.
How the TPA Pays as PrimaryAs primary, the TPA will pay the full benefit provided by your health plan as if you had no other coverage,provided it is a covered benefit under RHP Total Care and all Network Provider and EHP Medical ManagementDepartment rules have been followed.
40
How the TPA Pays as SecondaryBased on Coordination of Benefits (COB), if RHP Total Care is secondary, it will pay only if the services areprovided by an RHP Total Care network provider — Tier 1 or Tier 2. As secondary, the TPA’s payments will bebased on the balance left after the primary health plan has paid. A copy of the Explanation of Benefits (EOB)from the primary health plan must be submitted to the TPA. The TPA will pay no more than that balance.In no event will the TPA pay more than it would have paid had the TPA been primary. The TPA will pay nomore than the “allowable expense” for the healthcare involved. If the TPA’s allowable expense is lower thanthe primary plan’s, the TPA will use the primary health plan’s allowable expense. The primary health plan’sallowable expense may be less than the actual bill.
• The TPA will NOT pay any co-payments required by the primary health plan. The TPA will pay only forservices covered under your primary health plan only if you followed all of their procedural requirementsincluding prior authorization and network provider rules.
• If a member seeks services from a Tier 2 provider, before Cleveland Clinic Retiree Health Plan Total Carewill reimburse as secondary, the deductible must be met.
When the member becomes Medicare eligible at age 65, Cleveland Clinic Retiree Health Plan Total Carewill pay as secondary, as if the member has Medicare Part B, whether or not the member has enrolled inMedicare Part B. This means Cleveland Clinic Retiree Health Plan Total Care will only reimburse 20%of the Allowed Amount. This does not apply to actively working age 65 or older employees.
Enforcement of Coordination of Benefits (COB) ProvisionThe TPA will coordinate benefits provided that the TPA is informed by you, or some other person or organization,of your coverage under any other health plan.
In order to apply and enforce this provision or any provision of similar purpose of any other healthcare plan,it is agreed that:
• Any person claiming benefits described under this Plan will furnish the TPA with any information theTPA needs; and
• The TPA may, without the consent of or notice to any person, release or obtain from any source anynecessary information needed to complete the claims adjudication process.
Facility of PaymentIf payment is made under any other health plan that the TPA should have made under this provision, thenthe TPA has the right to pay whoever paid under the health plan; the TPA will determine the necessary amountunder this provision. Amounts so paid are benefits under this health plan and the TPA is discharged fromliability to the extent of such amounts paid for covered services.
Right of RecoveryIf the TPA pays more for covered services than this provision requires, the TPA has the right to recover theexcess from anyone to or for whom the payment was made. The member agrees to do whatever is necessaryto secure the TPA’s right to recover the excess payment.
Coordination DisputesIf you disagree with the way the TPA has paid a claim, your first attempt to resolve the problem should be bycontacting the TPA. You must follow the TPA appeal process (see page 49). If you are still not satisfied, youmay call the Ohio Department of Insurance for instructions on filing a consumer complaint at 614-644-2673or toll-free at 1-800-686-1526.
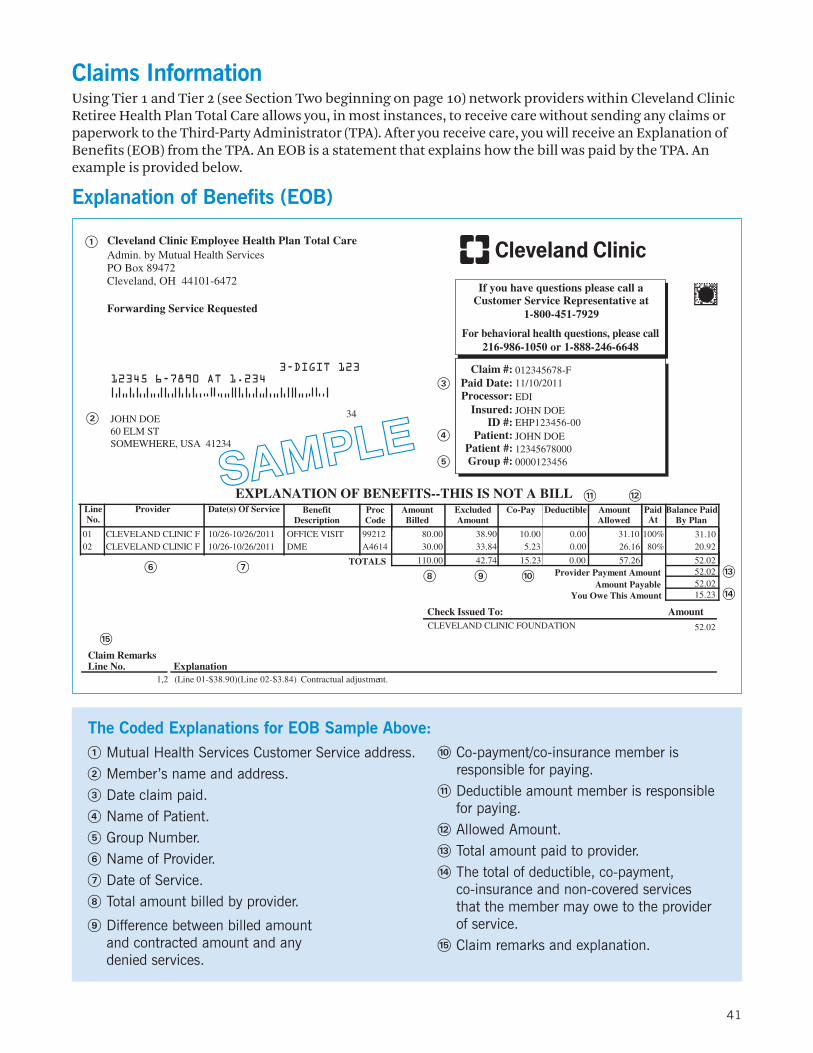
Claims InformationUsing Tier 1 and Tier 2 (see Section Two beginning on page 10) network providers within Cleveland ClinicRetiree Health Plan Total Care allows you, in most instances, to receive care without sending any claims orpaperwork to the Third-Party Administrator (TPA). After you receive care, you will receive an Explanation ofBenefits (EOB) from the TPA. An EOB is a statement that explains how the bill was paid by the TPA. Anexample is provided below.
Explanation of Benefits (EOB)
41
The Coded Explanations for EOB Sample Above:
! Mutual Health Services Customer Service address.
@ Member’s name and address.
# Date claim paid.
$ Name of Patient.
% Group Number.
^ Name of Provider.
& Date of Service.
* Total amount billed by provider.
( Difference between billed amountand contracted amount and anydenied services.
JOHN DOEEHP123456-00
11/10/2011012345678-F
12345678000
If you have questions please call aCustomer Service Representative at
Patient #:
Insured:ID #:
Paid Date:Claim #:
Patient:
EXPLANATION OF BENEFITS--THIS IS NOT A BILL
JOHN DOE
1-800-451-7929
Processor: EDI
Group #: 0000123456
Provider Co-PayDate(s) Of Service PaidAt
ProcCode
AmountAllowed
Balance PaidBy Plan
LineNo.
AmountBilled
ExcludedAmount
DeductibleBenefitDescription
LS
A IN 20.9226.165.23CLEVEL ND CL IC F 10/26-10/26/2011 30.00A461402 33.84 80%0.00DME A IN 31.1031.1010.00CLEVEL ND CL IC F 10/26-10/26/2011 80.009921201 38.90 100%0.00OFFICE VISIT
0.0042.74 52.02TOTA 110.00 15.23 57.2652.02Provider Payment Amount52.02Amount Payable15.23 You Owe This Amount
AmountCheck Issued To:CLEVELAND CLINIC FOUNDATION 52.02
Claim RemarksLine No. Explanation
(Line 01-$38.90)(Line 02-$3.84) Contractual adjustment.1,2
12345 6-7890 AT 1.234
34
3-DIGIT 123
PO Box 89472Cleveland, OH 44101-6472
Cleveland Clinic Employee Health Plan Total CareAdmin. by Mutual Health Services
Forwarding Service Requested
&^* ( )
1 2
5
!
JOHN DOE60 ELM STSOMEWHERE, USA 41234
@
4
3
#
$
%
For behavioral health questions, please call216-986-1050 or 1-888-246-6648
) Co-payment/co-insurance member isresponsible for paying.
1 Deductible amount member is responsiblefor paying.
2 Allowed Amount.
3 Total amount paid to provider.
4 The total of deductible, co-payment,co-insurance and non-covered servicesthat the member may owe to the providerof service.
5 Claim remarks and explanation.
SAMPLE
42
This section of the Summary Plan Description (SPD) includes all of the information you need about:• The Registration Process
• Eligibility
• Coverage Options
• The Enrollment Process
• Retiree Contributions
• Your Identification Card
• Life Event Changes
• Continuation of Coverage
• Prescription Drug Coverage Under Medicare
The Registration ProcessIt is important that your provider has your and your dependents’ correct address and telephone number, aswell as any information about your spouse’s employer and medical insurer. Correct registration informationhelps to ensure that your claim will be paid correctly and in a timely manner. Therefore, please bring allapplicable insurance cards with you when you receive medical services. The registrar will verify that thecorrect demographic and insurance information is accurate.
EligibilityYou are eligible to participate in Cleveland Clinic Retiree Health Plan (RHP) Total Care if, at the time ofretirement, you are at least age 55 with a minimum of 10 years of continuous service or age 65 with a minimumof five years of continuous service. In addition, you must be a current participant in one of the ClevelandClinic Employee Health Plan offerings immediately prior to retirement and begin your pension benefitimmediately. (Deferred vested participants of the Cleveland Clinic Retirement Plan are not eligible forRetiree Medical Benefits.)
Your eligible dependents will be covered under RHP Total Care only if you elect coverage for them and providedocumentation that they are eligible dependents.
Coverage Options1. Single: Only the retiree is covered under the Cleveland Clinic Retiree Health Plan.
2. Family: If coverage is elected, each family member will be covered under a single contract, and will havetheir own Identification Number and card.
Section Five
ADMINISTRATIVE INFORMATION
43
Dependents Eligible for CoverageDependents eligible for the Retiree Health Plan include:
1. Your lawful spouse (neither divorced nor legally separated).
2. Your children who are: your natural children, stepchildren, legally adopted children, or children underan officially court-appointed guardianship who are under age 26.
3. Your unmarried children age 26 or older who are disabled as determined by the Social SecurityAdministration. Proof of disability must be provided to Human Resources within 31 days after thedetermination of disability.
Ineligible members include the retiree’s parents, grandchildren, nieces, nephews, ex-spouses, common-lawmarriage partners (after the year 1991) and foster children who have not been legally adopted or who havenot been placed for adoption.
Eligibility VerificationNew EnrolleesRetirees enrolling a dependent for the first time are contacted by our consultant, Willis, to providesupporting documentation for verification of dependent eligibility. Acceptable documentation forverification is as follows:
Spouse• Copy of marriage license, or
• Copy of page one of your most recent tax return (you may cross out wage information)
Children under age 26Natural born children:
• Copy of birth certificate or one of the following:– Copy of page one of your most recent tax return (you may cross out wage information)– Copy of court-issued qualified medical child support order (QMCSO)– Copy of divorce decree
Stepchildren/Custodial:
• Copy of birth certificate and one of the following:– Marriage license– Copy of court-issued qualified medical child support order (QMCSO)– Copy of divorce decree – Custodial papers
Adopted Children:
• Adoption papers
Domestic Partners*
If you participate in the Retiree Health Plan Total Care, your same-gender domestic partner also is eligibleto participate in the plan(s) if all of these criteria are met:
1. You both are of the same gender.
2. You both are age 18 or older and mentally competent to enter into contracts.
3. You both reside in the same household.
4. You and your partner have been in a committed relationship with one another for at least six monthsand intend to remain in the relationship solely and indefinitely with one another.
5. You have joint responsibility for one another’s welfare and financial obligations.
6. You are not related by blood to a degree that would prohibit marriage under the law of the state in whichyou reside.

44
7. You are not currently married to any other person under either statutory or common law.
Note: Domestic Partner Benefits are not available to Marymount Hospital employees.
*Children of domestic partners also are eligible for coverage as long as they meet the eligibility requirementsfor dependents on page 42.
In order to enroll your domestic partner in RHP Total Care, you and your domestic partner must sign anAffidavit of Domestic Partnership. Under current Federal and State law, the amount you pay towards thecost of domestic partner coverage must be made on an after-tax basis. Additionally, the full cost of benefitscoverage for your domestic partner, less the amount of your after-tax contribution, is added to your incomeand subject to ordinary Federal, FICA, State, local and any other applicable payroll taxes. This amount ofadditional taxable income will be shown on your paychecks and reported on your W-2 at the end of the year.
Health Benefit Enrollment ProcessEligible employees have the opportunity to enroll in Cleveland Clinic Retiree Health Plan (RHP) Total Careat the same time they apply for their retirement benefits. If you do not enroll in Cleveland Clinic RHP TotalCare when you apply for retirement benefits, you will never be eligible to apply for the health plan again. Ifyou terminate coverage, you will not be able to re-enroll in Cleveland Clinic RHP Total Care.
Retiree ContributionsA retiree will pay a portion of the cost for coverage under RHP Total Care. The Cleveland Clinic pays theremainder of the cost for coverage. Information on retiree contributions is available through the BenefitsDepartment.
Plan Identification CardYour Cleveland Clinic Retiree Health Plan (RHP) Total Care Identification (ID) card(s) will be mailed to yourhome directly from the Third-Party Administrator (TPA). See Section Four for TPA information beginning onpage 37. Each RHP member will receive an ID card listing his/her name and personal identification numberfollowed by the two digit suffix 00.
For example:EHP123456–00
Your ID card(s) contains the following information:
1. Name of EHP Total Care Enrollee
2. Member ID Number (contract holder’s 9-character ID number + suffix)
3. Group Name
4. Group Number
5. Co-payment Requirements
6. Mutual Health Services Claim Submission Phone Number/Mailing Address
7. EHP Medical Management Department Phone Number, Prior Authorization for Clinical Appropriatenessfor Medical, Behavioral Health, and Case Coordination programs
8. Emergency Room Transfer Call Line
9. Information regarding Tier 2 Networks
It takes approximately 15 business days from the time you enroll to the time your benefit selection isprocessed with the TPA. Promptly submitting your selections reduces delays in receiving your ID cardsand helps avoid possible claims issues.
If your ID card(s) are lost or stolen, you may contact the Third-Party Administrator (TPA) for a replacement card.Please have the contract holder’s Social Security Number available for the Customer Service Representative.See the Quick Reference Guide on page 9 for appropriate phone numbers/contacts.

45
Life Event ChangesTo help Cleveland Clinic design a cost-effective healthcare plan each year, maintain costs, and to anticipatefuture needs, you are required to keep your selected BeneFlex elections unless you or your dependentsexperience a “Life Event Change.”
Under Internal Revenue Service guidelines, the following occurrences meet the definition of a qualifyinglife event and permit you to change certain elections:
1. Changes in legal marital status, including marriage, death of a spouse, divorce, legal separation orannulment.
2. Changes in the number of dependents for reasons that include birth, adoption, placement for adoption,the assumption of legal guardianship, or death.
3. Employment status changes, meaning an employee, spouse or dependent starts a new job or loses acurrent job.
4. A dependent satisfies — or no longer satisfies — the plan requirements for unmarried dependentsbecause of age, job status or other circumstances.
5. A qualified medical child support court order (QMCSO), or other similar order, that requires healthcoverage for an employee’s child.
6. The retiree, spouse or dependent qualifies for Medicare or Medicaid. (If this happens, health plan coveragemay be cancelled for that individual.)
If you experience a qualifying life event and wish to change your coverage, you must contact the BenefitsDepartment within 31 days of the event and provide the necessary supporting documentation. Any adjustmentto coverage must be consistent with the changes resulting from the qualifying life event.
Retirees/dependents covered under another health plan who lose that coverage as a result of one of the lifeevents listed above are eligible to participate in RHP Total Care.
Note: Life Event changes require the completion of a COB form at the time of the event.
Continuation of CoverageConsolidated Omnibus Budget Reconciliation Act (COBRA) CoverageThe Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) may require that you and/or yourdependents be provided with the opportunity to continue your group healthcare coverage on a contributorybasis under the following circumstances. The extension of coverage applies to almost all employee healthplans providing medical, dental, prescription drug, vision, or hearing benefits. You will be able to continuecoverage through COBRA by paying all of the costs of the health plan you choose, including any portionformerly paid for by the Cleveland Clinic facility that employed you.
Qualifying Events: Who, When, and for How LongIf your RHP Total Care coverage terminates, you and your covered dependents may continue medical carecoverage for up to 18 months:
1. If your employment terminates for any reason, including retirement, other than gross misconduct; or
2. If you lose your coverage due to a reduction in your hours of employment; or
3. If you or a dependent become disabled within the first 60 days of COBRA continuation, coverage may becontinued for an additional 11 months (29 months total).

46
Your covered dependents may continue such coverage under RHP Total Care for up to 36 months:
1. If you die while covered by the plan; or
2. If you and your spouse are divorced, your marriage is annulled or you are legally separated from yourspouse; or
3. If you become eligible for Medicare; or
4. If your dependent child is no longer eligible for coverage under RHP Total Care.
If you are entitled to Medicare benefits at the time coverage terminates due to your termination of employmentor reduction in hours, the continuation period for covered dependents will be the longer of:
1. 18 months from the date coverage terminates due to your termination of employment or reduction ofhours; or
2. 36 months from the date you became entitled to Medicare.
When Continued Coverage EndsThe continued coverage will end for any qualified person when:
1. The cost of continued coverage is not paid on or before the date it is due; or
2. That person becomes eligible for Medicare, if later than the date of the COBRA election; or
3. That person becomes covered under another group health plan unless that other plan contains anexclusion or limitation with respect to any pre-existing health condition; or
4. EHP Total Care terminates for all Employees; or
5. You or your dependent are no longer deemed disabled during the additional 11-month extendedperiod; or
6. The last day of the applicable 18, 29 or 36 month time limit.
How to Obtain CoverageWhen your coverage terminates, the Benefits Department will notify the COBRA Administrator (Ceridian).Ceridian then notifies you of your election rights. You will need to make your election within 60 days of theevent in order to be eligible for continuation of coverage. For questions regarding COBRA, Ceridian can bereached toll-free at 1-800-877-7994 or you can contact the Benefits Department. There is generally a 1-2week lag time between the time Ceridian processes the first paid premium and the time the Third-PartyAdministrator (TPA) is updated. You will be able to receive covered care during this lag time. However, beprepared to provide proof of insurance or be prepared to resubmit the claim if denied the first time.
If you elect to continue any benefits under COBRA, the first payment must be made within 45 days of yourelection to continue coverage. The first payment covers the period beginning with the date the qualifyingevent occurred through the date the continuation coverage was elected. Thereafter, monthly payments aredue on the first of the month and must be paid within the 31 day grace period following the due date.
COBRA regulations may change from time to time. The extension of coverage will be provided in accordancewith current law.
Because COBRA rules are complicated, if you have any questions about eligibility, contact the BenefitsDepartment.
Termination of CoverageCleveland Clinic will initiate Termination of Coverage if you stop premiumpayments for more than two months.

47
This section of the Summary Plan Description (SPD) includes information about RHP Total Care members’rights and responsibilities. You will find information about:
• Benefit Determination for Claims
• Filing a Complaint
• Appeals Process
• Reimbursement and Subrogation Rights of the Plan
• The Health Insurance Portability and Accountability Act of 1996 (HIPAA)
• Employee Retirement Income Security Act of 1974 (ERISA)
• Statement of Your Rights Under ERISA
Benefit Determination for ClaimsUrgent Care ClaimsAn Urgent Care Claim is a claim for Medical Care or treatment where applying the timeframes fornon-urgent care could:1. seriously jeopardize the life or health of the claimant or the ability of the claimant to regain maximum
function; or
2. in the opinion of a Physician with knowledge of the claimant’s medical condition, would subject theclaimant to severe pain that cannot be adequately managed without the care or treatment that is thesubject of the claim.
Determination of urgent can be made by:1. an individual acting on behalf of the Plan and applying the judgment of a prudent lay person who
possesses an average knowledge of medicine; or
2. any physician with knowledge of the claimant’s medical condition can determine that a claim involvesurgent care.
If you file an Urgent Care Claim in accordance with the Plan’s claim procedures and all of the requiredinformation is received, the Plan will notify you of its benefit determination, whether adverse or not, assoon as possible but not later than 72 hours after the Plan’s receipt of the claim.
If you do not follow the Plan’s procedures or we do not receive all of the information necessary to make abenefit determination, the Plan will notify you within 24 hours of receipt of the Urgent Care Claim of thespecific deficiencies. You will have 48 hours to provide the requested information. Once the Plan receivesthe requested information, we will notify you of the benefit determination as soon as possible but not laterthan 48 hours after receipt of the information.
The Plan may notify you of its benefit determination decision orally and follow with written or electronicnotification not later than three days after the oral notification.
Concurrent Care ClaimsA Concurrent Care Claim is any claim for ongoing treatment, including the Plan’s approval for a numberof treatments. The decision is adverse if the Plan decided to reduce or terminate benefits for the ongoingtreatment (unless it’s due to a health plan amendment or health plan termination).
Section Six
RHP MEMBERS’ RIGHTS AND RESPONSIBILITIES
48
A request for an extension to an ongoing course of treatment must be filled in accordance with the Plan’sclaim procedures and must be made at least 24 hours prior to the expiration of the prescribed period of timeor number of treatments. The Plan will notify you of any benefit determination concerning the request toextend the course of treatment within 24 hours after its receipt of the claim.
If the Plan reduces or terminates a course of treatment before the end of the course previously approved,the reduction or termination is considered an adverse benefit determination. The Plan will notify you, inadvance, of the reduction of termination so that you may appeal and obtain an answer on the appeal beforethe benefit is reduced or terminated.
Pre-Service ClaimsA Pre-Service Claim is a claim for a benefit which requires some form of preapproval or precertificationby the Plan.
If you file a Pre-Service Claim in accordance with the Plan’s claim procedures and all the required informationis received, the Plan will notify you of its benefit determination within 15 days after receipt of the claim.The Plan may extend this time period for up to an additional 15 days if such an extension is necessary dueto circumstances beyond the control of the Plan. The Plan will notify you of such an extension and date bywhich it expects to render a decision.
If an extension is needed because you did not provide all the necessary information to process your claim,the Plan will notify you in writing, within the initial 15 day response period and will specifically describethe missing information. You will then have 45 days to provide the additional information. If you do notprovide the information, your claim may be denied.
Post-Service ClaimsA Post-Service Claim is any claim that is not a Pre-Service Claim.
If you file a Post-Service Claim in accordance with the Plan’s claim procedures and all of the requiredinformation is received, the Plan will notify you of its benefit determination within 30 days after receiptof the claim. The Plan may extend this time period for up to an additional 15 days if such an extension isnecessary due to circumstances beyond the control of the Plan. The Plan will notify you of such an extensionand date by which it expects to render a decision.
If an extension is needed because you did not provide all of the necessary information to process your claim,the Plan will notify you, in writing, within the initial 30 day response period and will specifically describethe missing information. You will then have 45 days to provide the additional information. If you do notprovide the information, your claim may be denied.
Benefit Determination NoticesYou will receive notice of a benefit determination, orally as allowed, or in writing. All notices of a denial ofa benefit will include the following:
• The specific reason for the denial;
• Sufficient information to identify the claim involved, including the date of services, the healthcareprovider, and the claim amount, if applicable;
• Reference to the specific Plan provision on which the denial is based;
• A description of any additional material or information necessary to process the claim and an explanationof why such information is necessary;
• A description of the Plan’s appeal procedures, applicable timeframes, including the expedited appealprocess, if applicable;
• Your right to bring a civil action under Federal law following the denial of a claim after review on appeal,if your group is subject to the Employee Retirement Income Security Act of 1974 (ERISA);
• If an internal rule, guideline, protocol or similar criteria was relied upon in making the benefit determination,then that information will be provided free of charge upon written request; and
49
• If the claim was denied based on Medical Necessity or Experimental treatment or a similar exclusion orlimit, then an explanation of the scientific or clinical judgment used for the determination applying theterms of the Plan to your circumstances will be provided free of charge upon request.
Filing a ComplaintIf you have a complaint, please call or write to Customer Service at the telephone number or address listedon your Explanation of Benefits (EOB) form and/or identification card. To expedite the processing of aninquiry, the member should have the following information available:• Name of patient
• Identification number
• Claim number(s) (if applicable)
• Date(s) of service
If your complaint is regarding a claim, a Mutual Health Services (MHS) Customer Service representativewill review the claim for correctness in processing. If the claim was processed according to terms of theGroup Contract, the Customer Service representative will telephone the member with the response. Ifattempts to telephone the member are unsuccessful, a letter will be sent explaining how the claim wasprocessed. If an adjustment to the claim is required, the member will receive a check, Explanation ofBenefits or letter explaining the revised decision.
If you are not satisfied with the results, you may continue to pursue the matter through the appeal process.
Appeals ProcessExpedited Review ProcessA request for an expedited review must be certified by your Provider that your condition could, withoutimmediate medical attention, result in any of the following:
1. Seriously jeopardize your life or health or your ability to regain maximum function; or
2. In the opinion of a physician with knowledge of your medical condition, would subject you to severepain that cannot be adequately managed without the care or treatment that is the subject of the claim.
The appeal does not need to be submitted in writing. You or your physician should call the EHP MedicalManagement telephone number on your identification card as soon as possible.
Expedited reviews will be resolved within 72 hours after you have submitted the request.
The expedited review process does not apply to prescheduled treatments, therapies, surgeries or otherprocedures that do not require immediate action.
When you request an internal review for an urgent care claim or for a concurrent care claim that is urgent,you may also file a request at the same time for an expedited external review.
Filing an AppealIf you are not satisfied with any of the following:• A benefit determination decision;
• A Medical Necessity determination decision;
• A determination of your eligibility to participate in the plan or health insurance coverage; or
• A decision to rescind your coverage (a rescission does not include a retroactive cancellation for failure totimely pay required premiums);
then you may file an appeal.
To submit an appeal, call the Customer Service telephone number on your identification card. You may alsowrite a letter with the following information: employee’s full name; patient’s full name; identification

50
number; claim number if a claim has been denied; the reason for the appeal; date of services; the provider/facility name; and any supporting information or medical records, dental X-rays or photographs you wouldlike considered in the appeal. Send the letter and records to:
Mutual Health Services Member Appeals Unit
P.O. Box 89472Cleveland, OH 44101-6472
Fax: 440-878-5451
The request for review must come directly from the patient unless he/she is a minor or has chosen anauthorized representative. You can choose another person to represent you during the appeal process, aslong as MHS has a signed and dated statement from you authorizing the person to act on your behalf.
You will receive continued coverage pending the outcome of the appeals process. This means that the Planmay not reduce or eliminate coverage of ongoing treatment until your appeal is exhausted.
First Level Mandatory AppealThe Plan offers all members a first level mandatory appeal. You must complete this first level of appeal beforeany additional action is taken.
First level mandatory appeals related to a claim decision must be filed within 180 days from your receiptof the notice of denial of benefits. All requests for appeal may be made by calling Customer Service or inwriting as described on page 49.
Under the appeal process, there will be a full and fair review of the claim in accordance with applicable lawfor this plan. The internal appeal process is a review of your appeal by an Appeals Coordinator, a physicianconsultant and/or other licensed healthcare professional. The review of an appeal will take into account allcomments, documents, medical records and other information submitted by you and the Provider relatingto the claim, without regard to whether such information was submitted or considered in the initial benefitdetermination. All determinations based on Medical Necessity and appropriateness, experimental treatment,or that are based in whole or in part on a medical judgment, are made by healthcare professionals whohave the appropriate training and experience in the field of medicine involved in the medical judgment.The healthcare professionals who review the appeal will not have made any prior decisions about your claimand will not be a subordinate of the professional who made the initial determination on your claim. Thesehealthcare professionals act independently and impartially. Decisions to hire, compensate, terminate,promote or retain these professionals are not based in any manner on the likelihood that these professionalswill support a denial of benefits.
You may submit written comments, documents, records, testimony and other information relating to theclaim that is the basis for the appeal. These documents should be submitted by you at the time you send inyour request for an appeal. Upon written request, you may have reasonable access to and copies of documents,records and other information used to make the decision on your claim for benefits that is the subject ofyour appeal.
If, during the appeal, the Plan considers, relies upon or generates any new or additional evidence, you willbe provided free of charge with copies of that evidence before a notice of denial is issued. You will have anopportunity to respond before our timeframe for issuing a notice of denial expires. Additionally, if the Plandecides to issue a final denial based on a new or additional rationale, you will be provided that rationalefree of charge before the final notice of denial is issued. You will have an opportunity to respond beforeour timeframe for issuing a notice of denial expires.
51
The appeal procedures are as follows:
Urgent Care Appeal• You, your authorized representative or your Provider may request an appeal for urgent care. Urgent care
claim appeals are typically those claims for Medical Care or treatment where withholding immediatetreatment could seriously jeopardize the life or health of a patient, or could affect the ability of the patient toregain maximum functions. The appeal must be decided within 72 hours of the request. When you requestan internal appeal for an urgent care claim, at the same time you may also file a request for an expeditedexternal appeal as described below.
Pre-Service Claim Appeal• You or your authorized representative may request a pre-service claim appeal. Pre-service claim appeals
are those requested in advance of obtaining Medical Care for approval of a benefit, as it relates to theterms of the plan. The pre-service claim appeal must be decided within 30 days of the request and mustbe requested within 180 days of the date you received notice of denial.
Post-Service Claim Appeal• You or your authorized representative may request a post-service claim appeal. Post-service claim appeals
are those requested for payment or reimbursement of the cost for Medical Care that has already beenprovided. As with pre-service claims, the post-service claim appeal must be decided within 30 days ofthe request and must be requested within 180 days of the date you received notice of the denial.
Appeal Denial NoticesAll notices of a denial of benefits relative to appeals will include the following:• The specific reasons for the denial;
• Sufficient information to identify the claim involved, including the date(s) of service, the healthcareprovider, and the claim amount, if applicable;
• Reference to the specific plan provisions on which the denial is based;
• Statement that you are entitled to receive, upon request and free of charge, reasonable access to andcopies of all documents, records, and other information relevant to your claim for benefits;
• If an internal rule, guideline, protocol or similar criteria was relied upon in making the determination,then that information will be provided free of charge upon written request;
• If the claim was denied based on a Medical Necessity, Experimental treatment or similar exclusion orlimit, an explanation of the scientific or clinical judgment used for the determination applying the termsof the plan to your circumstances will be disclosed, or you will be advised that this explanation will beprovided free of charge upon request; and
• A statement of your right to bring civil action under Federal law following the denial of a claim upon review,if your group is subject to the Employee Retirement Income Security Act of 1974 (ERISA).
Second Level of Appeal This is a voluntary appeal level and is filed with the Employee Health Plan to be reviewed by the HealthPlan Advisory Committee (HPAC). The member is not required to follow this internal procedure beforegoing to the External Review Process on page 53.
The HPAC members include EHP Total Care Chief Medical Officer, Senior Director, Legal Counsel, ClevelandClinic Medical Director, Director of Health and Welfare Benefits, Director of Retirement/Voluntary BenefitPlan, Director of EHP Medical Management, EHP Total Care Pharmacy Director, and Behavioral Healthrepresentatives.• Members who are not satisfied with the decision following the first appeal have the right to appeal the
denial a second time.
• Members or their Personal Representative must submit a written request for a second review within180 calendar days following the date they received the TPA’s decision regarding the first appeal. The RHPwill assume that the member received the determination letter regarding the first appeal five daysfollowing the date the TPA sends the determination letter.

52
• Members may submit written comments, documents, records and other pertinent information to explainwhy they believe the denial should be overturned. This information should be submitted at the sametime the written request for a second review is submitted.
• Members have the right to submit evidence that their claim is due to the existence of a physical or mentalmedical condition or domestic violence, under applicable federal nondiscrimination rules.
• The second review will take into account all comments, documents, records and other informationsubmitted that related to the claim that either were not submitted previously or were not consideredin the initial benefit decision. The review will be conducted by individuals who were not involved in theoriginal denial decision or the first appeal, and are not under the supervision of those individuals.
• If the benefit denial was based in whole or in part on a medical judgment, the RHP will consult witha healthcare professional with training and experience in the relevant medical field. This healthcareprofessional may not have been involved in the original denial decision or first appeal, nor be supervisedby the healthcare professional who was involved. If the RHP has obtained medical or vocational expertsin connection with the claim, they will be identified upon the member’s request, regardless of whetherthe RHP relies on their advice in making any benefit determinations.
• After the claim has been reviewed, the member will receive written notification letting them know if theclaim is being approved or denied. It will also notify them of their right to file suit under ERISA after theyhave completed all mandatory appeal levels described in this SPD.
Regarding voluntary appeal level on page 51, the RHP agrees that any statutory limitations that are applicableto pursuing the claim in court will be put on hold during the period of this voluntary appeal process. Thevoluntary appeal process is available only after the member has followed the mandatory appeal level arequired on page 50. The RHP also agrees that it will not charge the member a fee for going through thevoluntary appeal process, and it will not assert failure to exhaust administrative remedies if a member electsto pursue a claim in court before following this voluntary appeal process. A member’s decision aboutwhether to submit a benefit dispute through this voluntary appeal level will have no affect on their rightsto any other benefits under the RHP. For any questions regarding the voluntary level of appeal includingapplicable rules, a member’s right to representation (Personal Representative) or other details, pleasecontact the RHP. Refer to the ERISA Statement of Rights section on page 57 of this SPD for details on amember’s additional rights to challenge the benefit decision under section 502(a) of ERISA.Appeals should be sent within the prescribed time period as stated above.
Send Medical Appeals to:First Level Mandatory Appeals Second Level Voluntary AppealsMutual Health Services Cleveland ClinicMember Appeals Unit Employee Health Plan Total CareP.O. Box 89472 29050 Aurora Road / SCC-13Cleveland, OH 44101-6472 Solon, OH 44139Fax: 440-878-5451
Send Pharmacy Appeals to:Note: Pharmacy Appeals are not subject to the mandatory appeal level.
Cleveland Clinic Employee Health Plan Total CarePharmacy Appeals6000 Westcreek, Suite 10Independence, OH 44131Phone: 216-986-1050 (option 4)
or toll-free at 1-888-246-6648 (option 4)
53
Time Periods for Making Decision on AppealsAfter reviewing a claim that has been appealed, the TPA/RHP will notify the member of its decision withinthe following timeframes, although members may voluntarily extend these timelines. In addition, if anynew or additional evidence is relied upon or generated during the determination of the appeal, the Plan willprovide it to you free of charge and sufficiently in advance of the due date of the response to the AdverseBenefit Determination.
The timelines below only apply to the mandatory appeal level. The voluntary appeal level will not be subjectto specific timelines.• Pre-Service Claim: Within a reasonable period of time appropriate to the medical circumstances, but
not later than 30 calendar days after the Plan receives the request for review.
• Post-Service Claim: Within a reasonable period of time but not later than 30 calendar days after the Planreceives the request for review.
• Concurrent Care Claim: Before treatment ends or is reduced.
External Review Process In accordance with Federal law, RHP Total Care has also established an external review process to examinecoverage decisions under certain circumstances. The request for External Review must be made within 180 daysfrom your receipt of the notice of denial from the first-level mandatory internal appeal. You may be eligibleto have a decision reviewed through the external review process if you meet the following criteria:
1. For claims for which external review is initiated:
a. Before September 20, 2011, the adverse benefit determination does not relate to your failure to meetthe requirements of eligibility under the Plan;
b. On or after September 20, 2011, the adverse benefit determination involves medical judgment or arescission of coverage;
2. You have exhausted the mandatory internal appeal process unless under applicable law you are notrequired to exhaust the internal appeal process;
3. You are or were covered under the plan at the time the service was requested or, in the case of retrospectivereview, were covered under the Plan when the service was provided; and
4. You have provided all of the information and forms necessary to process the external review.
External Review will be conducted by Independent Review Organizations (IRO). You will not be required to payfor any part of the cost of the external review. All IROs act independently and impartially and are assignedto review your claim on a rotational basis or by another unbiased method of selection. The decision to usean IRO is not based in any manner on the likelihood that the IRO will support a denial of benefits.
The Plan is required by law to provide to the independent review organization conducting the review, a copyof the records that are relevant to your medical condition and the external review.
External Review for Non-Urgent Care Claims AppealsA request for an external review for a non-expedited or non-urgent claim must be in writing and should beaddressed to MHS’s Member Appeals Unit at the address listed on page 50.
If your request for external review is complete and you are eligible for external review, an IRO will conductthe review. The IRO will notify you and give you 10 business days to submit information for its consideration.The IRO will issue a written decision within 45 days after it receives the request for external review. Thiswritten decision will include the main reasons for the decision, including the rationale for the decision. Ifthe IRO reverses the adverse benefit determination, the Plan will provide coverage, subject to other terms,limitations and conditions of your plan.

54
Expedited External Review for Urgent Care Claim AppealsA request for an external review for Urgent or Expedited claims may be requested orally or in writing. Arequest for an expedited review should be made by contacting Mutual Health Services at the number onthe back of your identification card. You may also request an external review for Urgent or Expedited claimsat the same time you request an expedited internal review of your claim.
An expedited review may be requested if your condition, without immediate medical attention, could resultin any of the following:
1. Seriously jeopardize your life or health or your ability to regain maximum function; or
2. In the opinion of a physician with knowledge of your medical condition, would subject you to severepain that cannot be adequately managed without the care or treatment that is the subject of the claim.
If your request for external review is complete and you are eligible for external review, an IRO will conductthe review. The IRO will issue a decision within 72 hours after the IRO receives the request for external review.If the decision is not in writing, within 48 hours after providing that notice, the IRO will provide a writtenconfirmation. This decision will include the main reasons for the decision, including the rationale for thedecision. If the IRO reverses the adverse benefit determination, the Plan will provide coverage, subject toother terms, limitations and conditions of your Summary Plan Description.
Reimbursement and Subrogation Rights of the PlanThis Section of this Summary Plan Description addresses the Cleveland Clinic Retiree Health Plan TotalCare’s (referred to as the “Plan”) “subrogation” and “reimbursement” rights. The terms “Covered Person,”“ Third Party,” “Claim,” and “Claim Proceeds” are defined at the end of this section.
First, this Plan does not provide any benefits to a Covered Person to the extent that there is any othertype of non-healthcare insurance coverage that would provide reimbursement for a Covered Person’smedical expenses (including auto insurance that provides underinsured and non-insured motoristcoverage, and insurance maintained by Cleveland Clinic or its affiliates on employees and insurancemaintained by other employers).
Second, if a Covered Person has a Claim against a Third Party, this Plan will provide benefits to, or onbehalf of, a Covered Person only under the following terms and conditions:
1. To the extent that benefits are provided under this Plan, the Plan shall be subrogated to all of the CoveredPerson’s Claims against any Third Party. The Covered Person shall execute and deliver instruments andpapers and do whatever else is necessary to secure the subrogation rights of the Plan. The Covered Personshall do nothing to prejudice the subrogation rights of the Plan. By submitting a claim for benefits underthe Plan, the Covered Person hereby agrees to cooperate with the Plan and/or any representatives of thePlan in completing subrogation forms and in giving such information surrounding any accident or otherset of facts and circumstances as the Plan or its representatives deem necessary to fully investigate andenforce the Plan’s subrogation rights.
2. The Plan is also granted a right of reimbursement from any Claim Proceeds. This right of reimbursementis cumulative with, and not exclusive of, the subrogation right granted in paragraph 1, but only to theextent of the benefits provided under this Plan.
3. The Plan, by providing benefits hereunder, is hereby granted a lien on any Claim Proceeds intended for,payable to, or received by the Covered Person or his/her representatives, and the Covered Person herebyconsents to said lien and agrees to take whatever steps are necessary to help the company secure saidlien. The Covered Person agrees that said lien shall constitute a charge upon the Claim Proceeds andthe Plan shall be entitled to assert security interest thereon. By the acceptance of benefits under thePlan, the Covered Person and his/her representatives agree to hold the Claim Proceeds in trust for thebenefit of the Plan to the extent of 100% of all benefits paid by the Plan on behalf of the Covered Person.
4. By accepting benefits hereunder, the Covered Person hereby grants a lien and assigns to the Plan an amountequal to the benefits paid against any Claim Proceeds. This assignment is binding on any attorney whorepresents the Covered Person whether or not an agent of the participant and on any insurance companyor other financially responsible party against whom a Covered Person may have a claim.

55
15. The subrogation and reimbursement rights and liens apply to any Claim Proceeds received or payableto the Covered Person, including but not limited to the following:
a. Payments made directly by a third party tortfeasor, or any insurance company on behalf of a thirdparty tortfeasor, or any other payments on behalf of a third party tortfeasor.
b. Any payments or settlements or judgment or arbitration awards paid by any insurance companyunder an uninsured or underinsured motorist coverage, whether on behalf of a Covered Personor other person.
c. Any other payments from any source designed or intended to compensate a Covered Person forinjuries sustained as the result of negligence or alleged negligence of a third party.
d. Any workers compensation award or settlement.
e. Any recovery made pursuant to no-fault insurance.
f. Any medical payments made as a result of such coverage in any automobile or homeowners insurancepolicy.
16. No adult Covered Person hereunder may assign any rights that such person may have to recover medicalexpenses from any Third Party to any minor child or children of said adult Covered Person withoutthe prior express written consent of the Plan. The Plan’s right to recover (whether by subrogation orreimbursement) shall apply to decedents’, minors’, and incompetent or disabled persons’ settlementsor recoveries.
17. No Covered Person shall make any settlement, which specifically reduces or excludes, or attempts toreduce or exclude the benefits provided by the Plan.
18. The Plan’s rights of subrogation and reimbursement shall be a prior lien against any Claim Proceeds,and shall not be defeated nor reduced by the application of any so-called “Make-Whole Doctrine,” “RimesDoctrine,” or any other such doctrine purporting to defeat the Plan’s recovery rights by allocating theproceeds exclusively to non-medical expense damages. Accordingly, the Plan’s rights of subrogationand reimbursement provide the Plan with the right to receive the first dollars of any Claim Proceeds,irrespective of whether the Covered Person has been fully compensated or partially compensated forall or any of injuries, damages or other claims of the Covered Person.
19. No Covered Person hereunder shall incur any expenses on behalf of the Plan in pursuit of the Plan’srights hereunder, specifically, no court costs or attorneys fees may be deducted from the Plan’s recoverywithout the prior express written consent of the Plan. This right shall not be defeated by any so-called“Fund Doctrine,” or “Common Fund Doctrine,” or “Attorney’s Fund Doctrine.”
10. The Plan shall recover the full amount of benefits provided hereunder without regard to any claim offault on the part of any Covered Person, whether under comparative negligence or otherwise.
11. The benefits under this Plan are secondary to any coverage under no-fault or similar insurance.
12. In the event that a Covered Person shall fail or refuse to honor its obligations hereunder, then the Planshall be entitled to recover any costs incurred in enforcing the terms hereof including but not limitedto attorney’s fees, litigation, court costs, and other expenses. The Plan shall also be entitled to offsetthe reimbursement obligation against any entitlement to future medical benefits hereunder until theCovered Person has fully complied with his reimbursement obligations hereunder, regardless of howthose future medical benefits are incurred.
13. Any reference to state law in any other provision of this Plan shall not be applicable to this provision ifthe Plan is governed by ERISA. By acceptance of benefits under the Plan, the Covered Person agrees thata breach hereof would cause irreparable and substantial harm and that no adequate remedy at lawwould exist. Further, the Plan shall be entitled to invoke such equitable remedies as may be necessaryto enforce the terms of the Plan, including, but not limited to, specific performance, restitution, theimposition of an equitable lien and/or constructive trust, as well as injunctive relief.
56
For purposes of this Section:
“Covered Person” includes, individually and collectively, a participant, beneficiary or any other covered personunder this Plan. A reference to a Covered Person includes the Covered Person’s estate and any representativeof the Covered Person.
“Third Party” refers to any person or entity who, with respect to a claim for benefits of a Covered Person, isnot the Covered Person (e.g., a third party tortfeasor). References to a Third Party include, without limitation,any auto or other insurer that provides coverage of any kind (including non-insured or underinsuredmotorists coverage) to the Covered Person or to any Third Party, including insurers that provide coverageto employees of the Cleveland Clinic or another employer. The term Third Party also may refer to anotherperson who is a Covered Person under this Plan.
“Claim” means any type of legal, equitable, insurance, or other claim that a Covered Person (or anyrepresentative of the Covered Person) has against a Third Party, if that claim could, or would, provide anyamount of money or other consideration to the Covered Person because of, or in any way attributable to,the Covered Person’s claim for benefits under this Plan, or because of any set of facts and circumstancesthat are in any way related to the Covered Person’s claim for benefits under the Plan. The reference to aCovered Person’s Claims includes, without limitation, claims of pain and suffering and loss of consortium,as well as claims for consequential, punitive, exemplary or other damages.
“Claim Proceeds” includes any money or other consideration recovered from, or payable by, any Third Partythat is attributable to a Claim of a Covered Person. Claim Proceeds includes, without limitation, amountsreceived by settlement, judgment or otherwise, and any insurance proceeds of any kind, or in satisfaction ofany judgment or settlement, insurance claim of any kind, or otherwise. Claim Proceeds includes, withoutlimitation, proceeds received by a Covered Person for claims of pain and suffering, loss of consortium,consequential, punitive, exemplary or other damages.
The Health Insurance Portability andAccountability Act of 1996 (HIPAA)HIPAA is Federal law that pertains to group health plans. HIPAA has the following three basic provisions:• It prohibits an employer health plan from imposing pre-existing condition exclusions on employees and
dependents, except in limited, specified circumstances and for limited periods of time.
• It prohibits an employer health plan from prohibiting enrollment or charging a higher employee contributionamount or premium because of “health status-related factors.”
• It requires an employer health plan to allow enrollment for employees and dependents who lose coverageunder other plans or insurance policies.
Any other questions or issues related to the HIPAA law should be directed to the Benefits Department.
Employee Retirement Income Security Act of 1974 (ERISA)About the Cleveland Clinic Retiree Health Plan (RHP) Total CareThe official name of this health plan is Cleveland Clinic Retiree Health Plan Total Care. It is part of theretiree benefit program of the Cleveland Clinic and Regional hospitals and provides medical benefits toretirees and their family members. Cleveland Clinic Retiree Health Plan Total Care is on file with the U.S.Department of Labor under employer identification number 34-0714585. Cleveland Clinic Retiree HealthPlan Total Care number is 510. Plan records are kept on a calendar year basis with the Plan year fromJanuary 1 through December 31.
Copies of the latest full annual report or other materials pertaining to the Plan are available at:
Cleveland Clinic Employee Health Plan Total CareCustomer Service Unit / SCC1329050 Aurora RoadSolon, OH 44139
57
A reasonable charge may be made to cover the cost of reproduction of these materials.
This booklet describes the Cleveland Clinic Retiree Health Plan Total Care as in effect January 1, 2012.
The Cleveland Clinic Retiree Health Plan Total Care’s agent for service of legal process is:
Cleveland Clinic Office of the Secretaryand General Counsel / AC3213050 Science Park DriveBeachwood, OH 44122
Future of Cleveland Clinic Retiree Health Plan (RHP) Total CareCleveland Clinic intends to continue the Cleveland Clinic Retiree Health Plan Total Care. However, ClevelandClinic reserves the right to modify, suspend, or terminate the Cleveland Clinic RHP Total Care, or any partof it, any time. The decision to change or end Cleveland Clinic RHP Total Care may be due to changes inFederal or State laws governing employee benefits, the requirement of the Internal Revenue Code or ERISA,or any other reason. A Health Plan change may provide for the transfer of Cleveland Clinic RHP Total Careassets and liabilities to another plan, split a plan into two or more parts, decrease benefits, or add/increasecontributions for coverage. If such steps are planned, you will be given notice. You will also be informedof the effect of any material change in Cleveland Clinic RHP Total Care or on your rights to benefits.
A Statement of Your Rights Under ERISAAs a participant in Cleveland Clinic Retiree Health Plan (RHP) Total Care, you are entitled to certain rightsand protections under the Employee Retirement Income Security Act of 1974 (“ERISA”), as amended. ERISAprovides that all Plan participants shall be entitled to:
Receive Information About Your Plan and Benefitsa. Examine, without charge, at the Plan Administrator’s office and at other specified locations, such as work
sites, all documents governing the Plan, including insurance contracts, and a copy of the latest annualreport (Form 5500 Series) filed by the Plan with the U.S. Department of Labor and available at the PublicDisclosure Room of the Pension and Welfare Benefits Administration.
b. Obtain, upon written request to the Plan Administrator, copies of documents governing the operation ofthe Plan, including insurance contracts, and copies of the latest annual report (Form 5500 Series) andupdated summary plan description. The Plan Administrator may make a reasonable charge for the copies.
c. Receive a summary of the Plan’s annual financial report. The Plan Administrator is required by law tofurnish each participant with a copy of this summary annual report.
Continue Group Health Plan CoverageYou, your spouse and your dependents may have the right to continue group health coverage if you losecoverage on account of a qualifying event. You or your spouse or dependents may have to pay for the coverage.Review this Summary Plan Description and the Plan documents regarding your COBRA continuationcoverage rights.
Reduction or Elimination of Exclusionary Periods of Coverage for Pre-existing ConditionsUnder Your Group Health Plan if You Have Creditable Coverage from Another PlanYou should be provided a certificate of creditable coverage, free of charge, from your group health plan orhealth insurance issuer when you lose coverage under the plan, when you become entitled to elect COBRAcontinuation coverage, or when your COBRA continuation coverage ceases, if you request it before losingcoverage or if you request it up to 24 months after losing coverage. Without evidence of creditable coverage,you may be subject to a pre-existing condition exclusion for 12 months (18 months for late enrollees) afteryour enrollment date in your coverage.

58
Prudent Actions by Plan FiduciariesIn addition to creating rights for Plan participants, ERISA imposes duties upon the people who are responsiblefor the operation of the employee benefit Plan. The people who operate your Plan, called “fiduciaries” of thePlan, have a duty to do so prudently and in the interest of you and other Plan participants and beneficiaries.No one, including your employer, or any other person, may fire you or otherwise discriminate against youin any way to prevent you from obtaining a benefit or exercising your rights under ERISA.
Enforce Your RightsIf your claim for a benefit is denied or ignored, in whole or in part, you have a right to know why this wasdone, to obtain copies of documents relating to the decision without charge, and to appeal any denial, allwithin certain time schedules.
Under ERISA, there are steps you can take to enforce the above rights. For instance, if you request a copy ofPlan documents or the latest annual report from the Plan and do not receive them within 30 days, you mayfile suit in a federal court. In such case, the court may require the Plan Administrator to provide the materialsand pay you up to $110 a day until you receive the materials, unless the materials were not sent becauseof reasons beyond the control of the Plan Administrator. If you have a claim for benefits that is denied orignored, in whole or in part, you may file suit in a state or federal court. In addition, if you disagree with thePlan’s decision or lack thereof concerning the qualified status of a domestic relations order or a medicalchild support order, you may file suit in federal court. If it should happen that Plan fiduciaries misuse thePlan’s money, or if you are discriminated against for asserting your rights, you may seek assistance fromthe U.S. Department of Labor, or you may file suit in a federal court. The court will decide who should paycourt costs and legal fees. If you are successful, the court may order the person you have sued to pay thesecosts and fees. If you lose, the court may order you to pay these costs and fees if, for example, it finds yourclaim was frivolous.
Assistance With Your QuestionsIf you have any questions about your Plan, you should contact the Plan Administrator. If you have any questionsabout this statement or about your rights under ERISA, you should contact the nearest office of the Pensionand Welfare Benefits Administration, U.S. Department of Labor, listed in your telephone directory or theDivision of Technical Assistance and Inquiries, Pension and Welfare Benefits Administration, U.S. Departmentof Labor, 200 Constitution Avenue N.W., Washington, D.C. 20210. You may also obtain certain publicationsabout your rights and responsibilities under ERISA by calling the publications hotline of the Pension andWelfare Benefits Administration.
59
Definition of TermsAccess to Care:• Immediate is defined as having access to emergency care immediately for a life-threatening emergency.
• Emergent is defined as having access to emergency care within six hours for a non-life-threatening emergency.
• Urgent is defined as having access to care within 48 hours.
• Routine is defined as having access to a routine office visit within 10 business days.
Activities of Daily Living — The skill and performance of physical, psychological, and emotional self care,work, and play/leisure activities to a level of independence appropriate to age, life-space, and disability.
Against Medical Advice (AMA) — The act of an individual leaving the care of a medical facility withoutproper discharge by a physician.
Allowed Charges — Negotiated charges for allowed healthcare services as described in this SPD.
Behavioral Health —Refers to and includes all services for mental health and substance abuse.
Behavioral Health Levels of Care
1. Outpatient Visits (OP): Ambulatory care, usually non-urgent, for problems or conditions that can betreated on a periodic basis.
2. Intensive Outpatient Program (IOP): Similar to Partial Hospitalization Program (PHP) in that they arestructured programs with a multi-disciplinary team approach and a variety of treatment modalities. Theprogram is usually less restrictive than a PHP. Patients are more stable, considered low risk for self harm,can function in the community and manage some daily activities, but require more comprehensiveservices than can be provided at an outpatient level of care. The patient participates in the program aminimum of nine hours per week.
3. Partial Hospitalization Program (PHP): Highly structured ambulatory, multi-disciplinary treatmentprogram with a high staff to patient ratio. A psychiatrist must be available for consultation as needed onan ongoing basis. A PHP includes treatment modalities found in a comprehensive inpatient program.The program may be appropriate whenever a patient does not require 24 hour acute care hospitalization,but does need more comprehensive services than can be provided at an outpatient level of care. Theprogram is open a minimum of 20 hours per week.
4. Inpatient (IP): A medical facility that is licensed to provide 24 hour, 7 days per week medical care and providesa high degree of safety. The facility employs a multi-disciplinary staff that must include psychiatrists andnurses. Services are comprehensive and usually include medication management, individual, groupand/or family psychotherapy, social services, milieu and activity therapy. Inpatient care is not the sameas residential care. See page 23 for information regarding Residential Treatment.
Benefits Period — The period of time specified in the Schedule of Benefits during which covered servicesare rendered and benefit maximums are accumulated; the first and last Benefit Periods may be less than12 months depending on the Effective Date and the date your coverage terminates.
Section Seven
TERMS AND DEFINITIONS

60
Cleveland Clinic and Regional hospitals — Fully integrated Healthcare Delivery System that covers allcomponents of healthcare services including Medical Professional, Ambulatory (outpatient/office), Hospital,and Ancillary Services.
Cleveland Clinic consists of the following group of hospitals:
Cleveland Clinic, Ashtabula County Medical Center, Cleveland Clinic Hospital for Children’s Rehabilitation,Euclid Hospital, Fairview Hospital, Hillcrest Hospital, Lakewood Hospital, Lutheran Hospital, MarymountHospital, Medina Hospital, South Pointe Hospital, Cleveland Clinic Florida Hospital in Weston, andCleveland Clinic Nevada.
Clinical Appropriateness — A service, supply, and/or prescription drug that is required to diagnose ortreat conditions which Cleveland Clinic Retiree Health Plan Total Care (administered through the TPA)determines is:• Appropriate with regard to the standards of good medical practice;
• Not primarily for your convenience or the convenience of a provider or another person; and
• The most appropriate supply or level of service that can be safely provided to you. When applied to the careof an Inpatient, this means that your medical symptoms or condition require that the services cannot besafely or adequately provided to you as an Outpatient. When applied to prescription drugs, this means theprescription drug is cost effective compared to alternative prescription drugs that produce comparableeffective clinical results. (See page 16 for complete information.)
Co-insurance — The payment the employee owes for services rendered when EHP Total Care coverage isless than 100%; co-insurance payments usually accrue toward an annual out-of-pocket maximum and/orannual deductible.
Concurrent Review — This review is conducted either during an EHP Total Care member’s hospital stay orduring the course of a prescribed treatment. The concurrent review may result in additional covered carethat exceeds the original authorized EHP Medical Management Department approval.
Contracted Rate — The hospital rate and physician fee schedule that is paid by the Third-Party Administrator(TPA) for the EHP Total Care contract.
Co-payment — A dollar amount that you are required to pay at the time covered services are rendered;generally, a co-payment does NOT accrue toward an annual out-of-pocket maximum and/or annualdeductible.
Covered Charges — Charges for medical services or procedures that are covered by Cleveland ClinicRetiree Health Plan Total Care.
Custodial Care — Care which does not require the constant supervision of skilled medical personnel toassist the patient in meeting their activities of daily living. Custodial Care is care which can be taught toand administered by a lay person and includes but is not limited to:• Administration of medication which can be self-administered or administered by a lay person; or
• Help in walking, bathing, dressing, feeding, or the preparation of special diets.
Deductible — An amount, usually stated in dollars, for which you are responsible each benefit period beforethe TPA will start to reimburse benefits.
Domicillary — A temporary residence, such as for disabled veterans.
Effective Date — Health benefit coverage is effective on the first day of your active employment at ClevelandClinic provided that you enrolled in Cleveland Clinic EHP Total Care.

61
Emergency — A medical condition manifesting itself by acute symptoms of sufficient severity (includingsevere pain) such that a prudent lay person, with an average knowledge of health and medicine, couldreasonably expect the absence of immediate medical attention to result in:• Serious jeopardy to the health of the individual, or, in the case of a pregnant woman, the health of the
woman or her unborn child; or
• Serious impairment to bodily functions; or
• Serious dysfunction of any bodily organ or part.
Examples of emergency medical conditions include, but are not limited to:• Chest pain
• Stroke/CVA
• Loss of consciousness
• Hemorrhage
• Multiple trauma
An emergency condition may or may not result in an inpatient hospital admission.
Experimental or Investigational — Drugs, Devices, Medical treatment, or Medical procedures that are notconsidered to be a standard of practice in this healthcare market for a particular diagnosis.
Explanation of Benefits (EOB) — A statement received by the patient from the TPA after services have beenrendered that explains how the bill was paid.
Fee schedule — The rate the physician is paid by the TPA for the Cleveland Clinic EHP Total Care contract.
Hospital — An institution which meets the specifications of Chapter 3727 of the Ohio Revised Code, exceptfor the requirement that such institution be operated within the State of Ohio.
Identification (ID) Card — Card provided to individuals having group health benefit coverage listing theindividual’s name, group number, and important contact phone numbers to call to verify coverage forhealth, prescription, and behavioral health/substance abuse benefits. This card should be carried withyou at all times.
Inpatient — A person who receives care as a registered bed patient in a hospital or other facility providerwhere a room and board charge is made.
Medical Care — Professional services received from a physician or another healthcare provider to treata condition.
Medical Management — A comprehensive Physician-directed program utilizing Registered Nurses to provideeducation and follow-up to employees to assure the delivery of clinically appropriate, high quality, andcost-effective healthcare in the most appropriate setting. The EHP Medical Management Departmentprovides Case Coordination and Coordinated Care Programs.
Medical Necessity — See Clinical Appropriateness.
Network Provider — A participating provider who has agreed to accept the Allowed Amount as payment infull for covered services rendered after applicable co-payment/co-insurance. The member is not liable forany amount charged over the Allowed Amount. • RHP Total Care offers a two-tier provider network. Tier 1 providers are contracted and credentialed
through the Cleveland Clinic Community Physician Partnership (CPP). Tier 2 providers are contractedand credentialed through their respective companies.
Non-Contracting — The status of a hospital or other facility provider which does not meet the definitionof a contracting Cleveland Clinic Retiree Health Plan Total Care Provider.
Non-Covered Charges — Billed charges for services and supplies which are not covered services underRHP Total Care.
62
Notification — Process required by RHP Total Care of informing the EHP Medical Management Departmentthat an emergency admission has occurred. Notification by the physician is required within two businessdays of the admission.
Out-of-Network — A provider that does not participate in the Tier 1 Network of Providers (Cleveland ClinicCPP Providers) or Tier 2 Network of Providers (CHN, MMO Traditional and USAMCO).
Out-of-Pocket Maximum — The accrued value of co-insurance payments that has to be satisfied before thereimbursement for covered services will be provided in full.
Outpatient — The status of a covered person who receives services or supplies through a hospital, otherfacility provider, physician, or other healthcare provider while not confined as an inpatient.
Participating — The status of a physician or other healthcare provider that has an agreement with ClevelandClinic Employee Health Plan Total Care to accept Allowed Amount as payment in full.
Physician — A person who is licensed and legally authorized to practice medicine.
Precertification — The process of verifying member eligibility and benefit coverage under RHP Total Care.Precertification also includes the process of determining whether or not a patient has met the clinicalappropriateness criteria outlined by EHP Total Care for medical, prescription drug, and behavioral health/substance abuse services. Approval for a service prior to the service being rendered. Precertification,predetermination, prior authorization and prior approval are often used interchangeably.
Predetermination — The process of verifying member eligibility and benefit coverage under RHP Total Care.Predetermination also includes the process of determining whether or not a patient has met the clinicalappropriateness criteria outlined by EHP Total Care for medical, prescription drug, and behavioral health/substance abuse services. Approval for a service prior to the service being rendered. Predetermination,precertification, prior authorization and prior approval are often used interchangeably.
Prescription Drug (Federal Legend Drug) — Any medication which by Federal or State law may not bedispensed without a prescription order.
Primary Care Providers (PCP) — Physician practices expert in providing diagnosis and treatment of illnessand provision of preventive care; they also serve as coordinators of the overall care of their patients.
Prior Approval — The process of verifying member eligibility and benefit coverage under RHP Total Care.Prior Approval also includes the process of determining whether or not a patient has met the clinicalappropriateness criteria outlined by EHP Total Care for medical, prescription drug, and behavioral health/substance abuse services. Approval for a service prior to the service being rendered. Prior approval,precertification, predetermination and prior authorization are often used interchangeably.
Prior Authorization — The process of verifying member eligibility and benefit coverage under RHP TotalCare. Prior Authorization also includes the process of determining whether or not a patient has met theclinical appropriateness criteria outlined by EHP Total Care for medical, prescription drug, and behavioralhealth/substance abuse services. Approval for a service prior to the service being rendered. Prior authorization,precertification, predetermination and prior approval are often used interchangeably.
Provider — A person or organization responsible for furnishing healthcare services.
Registration — Process of verifying patient information including name, current address, phone number,insurance plan, and group number. The registration process must be completed anytime you receive ahealthcare service.
Specialty Care Providers — Physician practices with expertise in a specific medical specialty or sub-specialty.
Student — Eligible/participating dependent attending a school, college, or university.
Surgery:• The performance of generally accepted operative and other invasive procedures;
• The treatment of fractures and dislocations;
• Usual and related preoperative and postoperative care; or
• Other procedures as reasonable and approved by EHP Total Care.

63
Urgent Care — Care received for medical conditions that are unforeseen and require attention within 24 hours.Examples of urgent care include, but are not limited to:
1. Minor cuts/lacerations
2. Minor burns
3. Minor trauma
4. Seemingly minor illnesses that include a high fever
5. Sprains
Usual and Customary Amount (U&C) — The maximum amount allowed for a covered service provided bya physician or other healthcare provider based on the following criteria:
1. The U&C Amount will never exceed the actual amount billed by the physician or other healthcare providerfor a given service and for some services may be the amount billed.
2. The U&C Amount may be limited to the customary charge based on the distribution of charges billed by allphysicians and other healthcare providers for a given service within a given specialty and geographic area.
3. The U&C Amount must also be reasonable as defined by the Cleveland Clinic Employee Health PlanTotal Care TPA with respect to customary charges or costs for services of comparable complexity anddifficulty.
64
NotesPlease use these pages to keep a record of
contact dates and names of correspondence for your personal records.
65
Notes

66
Notes

Cleveland Clinic
4/2012
Every life deserves world class care.
9500 Euclid Avenue, Cleveland, OH 44195
Cleveland Clinic is a top-ranked nonprofit academic medicalcenter founded in 1921. With more than 1,300 staffed beds,as well as research and education institutes, the organizationis dedicated to providing expert inpatient and hospital carethrough innovation, quality, teamwork and service.
© The Cleveland Clinic Foundation 2012