clin nephro & hypertens
DESCRIPTION
CLIN NEPHRO & HYPERTENSTRANSCRIPT

GINJAL & HIPERTENSI
T. Realsyah

Holistic Approach in Medicine
Nephrology and Hypertension is a portion of Internal Medicine.
The need to apply systematic/methodology used in Internal Medicine in the clinical approach of patients with Renal and Hypertension problems

Anamnesis Physical examination Laboratory examination - basic/routine - advanced Imaging Biopsy/HistopathologyOthers
SYSTEMATICA

Anamnesis. Identity/particulars History/Anamnesis:
Symptoms that make the patient comes to see the doctor elaborate to details:how long,how big, how often etc
Complaints pertaining to disturbances of body organs: Heart& blood vessels, respiratory,
G-I tract, neurologic, urinary: polyuria, anuria, oliguria, dysuria etc Social status Previous illness Drug use

Physical Examination: Status Praesens: Consciousness, BP, pulse, resp. anemic, icteric etcHead: scalp, eyes, ears, mouth, teeth
Neck: thyroid, trachea, glands
Thorax : chest wall, heart, lungs
Abdomen: liver, GB, spleen, ballottement, ascites
Extremities : upper, lower
Laboratory:
Basic /routine: Hematology: Hb, WBC, thrombocyt diff.count, ESR Urinalysis: Chemistry: Protein, sugar, bilirubin, urobilinogen
Microscopy: rbc, wbc, casts: granular, erythrocyte leukocytes, crystals: phosphates, uric acids, struvites jenkolic acid.

Advanced Lab:
Renal function test, Liver function test etc
Electrolytes, acid-base status Lipid Profile
Immunologic: IgA, IgG, IgM etc

Imaging:
Radiologic: KUB, IVU,RPG, APG etc
Computed Tomography (CT-scan)
Magnetic Resonance Imaging (MRI)
Ultrasonography, Doppler USG

HISTOPATHOLOGY:
Biopsy: Kidneys: blind-percutaneous, open bones lymph glands tumours etc
Fine Needle Aspiration Biopsy (FNAB)
Microscopy: Light: staining: HE, PAS, Silver Impregnation Immunofluoroscence Electron
Renal Function: Excretory Regulatory Endoctine
Excretory Function: Metabolic Glomerular Glomerular Filtration Rate (GFR) Creatinin Clearance. UxV/P ml/min

GFR: inulin clearance EDTA isotop
99 Tc isotop Iohexal High Performance liquid chromatography
Clinical setting:
Cockroft-Gault Formula
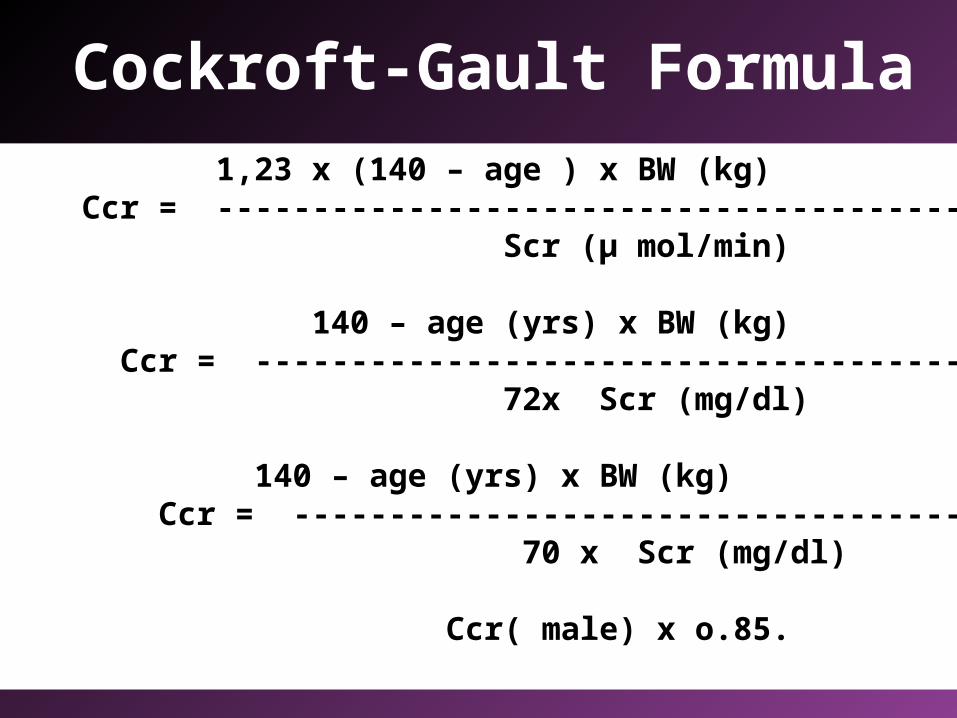
Cockroft-Gault Formula
Male: 1,23 x (140 – age ) x BW (kg) Ccr = ----------------------------------------- ml/min Scr (µ mol/min)
Or 140 – age (yrs) x BW (kg) Ccr = ----------------------------------------- ml/min 72x Scr (mg/dl)
Female: 140 – age (yrs) x BW (kg) Ccr = ----------------------------------------- ml/min 70 x Scr (mg/dl)
Or Ccr( male) x o.85.

10 CLINCAL SYNDROMES OF RENAL DISEASES
BASED ON : CLINICAL PICTURES Laboratory results Imaging Histopathology etc

1.Acute Nephritic Syndrome Hematuria (gross or micro) + oliguria/anuria and/or increasing creatinin and/or hypertension and/or oedema.2. Nephrotic Syndrome Proteinuria > 3.5 gram/24 hrs with/without oedema hypoalbuminemia hyperlipidemia.
3. Asymptomatic urinary abnormalities : Hematuria and/or proteinuria and/or pyuria and/or cylindruria
Without the presence of other clinical syndromes of renal disease.

4. Acute Renal Failure (ARF)
Sudden loss of renal function (within days to a few weeks)
with/ without oliguria/anuria Oliguric = urine volume < 400ml/24 hrs Non-oliguric = Ccr < 5 ml/min
5. Chronic Kidney Disease (CKD).
Reduction of renal function, progressing slowly within years. Characrerized by the presence of signs of chronicity e.g. anemia, calcifications in soft tissues etc. 5 stages of progression.
6. Urinary Tract Infection (UTI) The presence of significant bacteriuria as shown By culture of - midstream urine ( bacterial count > 105 cfu) - supra pubic aspirate: any amount.
7. Obstrunctive Uropathy/Nephropathy Obstruction of urine flow in the urinary tract by any cause, as shown by imaging
8. Tubular abnormalities: Structural changes mainly in the medulla, manifested in disturbances of regulatory function of the kidney such as: electrolite, fluid and acid-base imbalance, Fanconi syndr, renal tubular acidosis (RTA)
9. Nephrolithiasis urinary stones located in the kidneys or urinary tract shown by surgical removal of stone(s) or by proper imaging.
Vesicolithiasis: belongs to urology.

10. Hypertension: Increase in blood pressure, as measured by a standardized procedure, exceeding: JNC VI criteria (1997) WHO/ISH criteria (1999).
JNC VII (2003) - WHO criteria (2004)
Robinson dan Bricker 1939: 120/80 mmHg Browne 1947: 130/70 -,,- Ayman 1934: 140/80 -,,- Perera 1948: 140/90 -,,- Thomas 1952: 150/90 -,,- Bechgard 1946: 160/100 -,,- Burgess 1948: 180/100 -,,- Evans 1956: 180/110 -,,-
Classification of Hypertension WHO 1962 SYSTOLIC DIASTOLIC (mmHg ) (mmHg)
NORMOTENSION: <140 <90BORDERLINE: 140-160 90-95HYPERTENSION : > 160 >90

JNC VI 1997 – WHO-ISH 1999

Blood Pressure Classification
BP Classification SBP mHg DBPmmHg
Normal <120 and <80
Prehypertension 120–139 or 80–89
Stage 1 Hypertension
140–159 or 90–99
Stage 2 Hypertension
>160 or >100
JNC VII 2003 WHO 2004

ESC/ESH 2003, WHO 2004 .