clinical anatomy and embryology of thyroid gland dr. a. podcheko 2015
TRANSCRIPT

Clinical Anatomy and Embryology of Thyroid Gland
Dr. A. Podcheko2015

Intended Learning Outcomes1. Describe the anatomical locations of the thyroid gland of
adult human2. Describe cells responsible for the hormone secretions of
the thyroid gland and functional outcomes of the endocrine hormones from the thyroid gland
3. Describe the blood supply and innervation to the thyroid gland
4. Describe the lymphatic drainage of the thyroid gland5. Understand the embryological derivatives of the thyroid
gland 6. Medical imaging of thyroid 7. Clinical correlations

Why should I KNOW ?
• More than 12 percent of the population in US have diseases of thyroid
• Thyroid cancer is the most common endocrine cancer
• Most thyroid cancers respond to treatment, although a small percentage can be very aggressive
• Clinically important aspects of thyroid anatomy are commonly tested on USMLE step 1 and 2CK

Viscera of the Neck
Three layers of the cervical viscera1. Endocrine layer: the thyroid and parathyroid glands2. Respiratory layer: the larynx and trachea3. Alimentary layer: the pharynx and esophagus

Thyroid gland as part of endocrine system
• The endocrine system consists of the endocrine glands that release their secretions (hormones) into the bloodstream to reach and act on target cells of specific organs.
• The thyroid gland (largest endocrine gland) produces:
a. thyroid hormones (T3 - triiodothyronine (20%, highly active) and T4 - thyroxine(80%, low activity), control the rate of metabolism in almost all types of human cells
b. Calcitonin, decreases calcium level in the blood by direct inhibition of mediated bone resorption and by enhancing calcium excretion by the kidney

• Increase basal metabolic rate• Normalize insulin levels• Improve insulin resistance• Increase glucose use for ATP production• Increase breakdown of fat into energy• Increase oxygen consumption and use of ATP
by cells• Many others
Thyroid Hormones Actions

Mechanism of Thyroid Hormone Action
Both T3 and T4:1. Facilitate
normal growth3. Facilitate
normal mental development (Brain development!!!)
4. Increase the local effects of catecholamines
Any somatic cells (e.g. epithelium)

Histology of Thyroid Gland
• Follicular cells produce
thyroid hormones and their cell surfaces possess thyroid-stimulating hormone (TSH) receptors
• Thyroglobulin (aka Colloid) is an inactive storage for the T4 and T3 hormones
•Thyroid follicles = follicular cells and large pools of colloid
•Parafollicular cells (C cells) along the periphery of the thyroid follicles secrete calcitonin

Thyroid Gland Location•The thyroid gland lies deep to the sternothyroid and sternohyoid muscles, located anteriorly in the neck at the level of the C5 - T1 vertebrae
•Consists of right and left lobes, anterolateral to the larynx and trachea
•A relatively thin isthmus unites the lobes over the trachea, usually anterior to the second and third tracheal rings, the isthmus may be incomplete

Thyroid Gland Location•The thyroid gland lies deep to the sternothyroid and sternohyoid muscles, located anteriorly in the neck at the level of the C5 - T1 vertebrae
•Consists of right and left lobes, anterolateral to the larynx and trachea
•A relatively thin isthmus unites the lobes over the trachea, usually anterior to the second and third tracheal rings, the isthmus may be incomplete
C5
C6
C7
T1
Sternohyoid m.Sternothyroid m.

Thyroid Gland Location•The thyroid gland lies deep to the sternothyroid and sternohyoid muscles, located anteriorly in the neck at the level of the C5 - T1 vertebrae
•Consists of right and left lobes, anterolateral to the larynx and trachea
•A relatively thin isthmus unites the lobes over the trachea, usually anterior to the second and third tracheal rings, the isthmus may be incomplete

•~50% of thyroid glands have a pyramidal lobe•Pyramidal lobe extends superiorly from the isthmus of the thyroid gland•The fibrous tissue connecting pyramidal lobe with hyoid bone may contain levator glandulae thyroidae muscle (elevatior of thyroid gland) •A band of connective tissue, often containing accessory thyroid tissue, may continue from the apex of the pyramidal lobe to the hyoid
Pyramidal Lobe of the Thyroid Gland

Thyroid Imaging: Thyroid Scintigraphy
• Procedure producing one or more
planar images of the thyroid obtained within
15–30 min after intravenous injection of
Tc-99m pertechnetate or 3–24 hr
after the oral ingestion of radioactive
iodine (I-131)
• Common Indications:A. To relate the structure of the thyroid
gland to its functionB. To locate ectopic thyroid tissue C. To evaluate a neck or substernal
mass
Gamma-camera or scanner

• Common Indications:A. Evaluation of the
presence, size, and location of the thyroid gland
B. Evaluation of the thyroid gland for suspicious nodules
C. Evaluation of the location and characteristics of palpable neck masses, including an enlarged thyroid
Thyroid Imaging: Thyroid Ultrasonography
• Should be performed with the neck in hyperextension.
• Thyroid gland should be imaged in the longitudinal and transverse planes

•Dense connective tissue attaches the capsule to the cricoid cartilage and superior tracheal rings•External to the capsule is a loose sheath formed by the visceral portion of the pretracheal layer of deep cervical fascia
Thyroid Gland Capsule•The thyroid gland is surrounded by a thin fibrous capsule, which sends septa deeply into the gland

•Dense connective tissue attaches the capsule to the cricoid cartilage and superior tracheal rings•External to the capsule is a loose sheath formed by the visceral portion of the pretracheal layer of deep cervical fascia
Thyroid Gland Capsule•The thyroid gland is surrounded by a thin fibrous capsule, which sends septa deeply into the gland
Platisma

Enlarging Thyroid is tend to grow downwards
and not upwards •Upper pole of thyroid gland can not expand above point of attachment of sternothyroid muscle•The srernothyroid muscles are attached onto the oblique lines of the thyroid cartilage•No limitation to the downward expansion of the thyroid gland•Pathologically enlarged thyroid gland (goitre) extended behind the sternum is termed retrosternal goitre
Sternothyroid M.
Oblique line of thyroid cartilage

Retrosternal Goitre
Midsaggital CT section
Female 44y.o. Graves Disease
Saggital CT section

Arteries of the Thyroid Gland•Thyroid gland is highly vascular•Supplied by the superior and inferior thyroid arteries•Vessels lie between the fibrous capsule and the loose fascial sheath•The first branch of the external carotid artery, the superior thyroid artery (STA), descend to the superior poles of the gland, pierce the pretracheal layer of deep cervical fascia, and divide into anterior and posterior branches supplying mainly the anterosuperior aspect of the gland
External carotid artery

Anatomical Relationships between Superior Thyroid Artery and External Branch of Superior Laryngeal Nerve
cricothyroid muscle

Summary:• Superior thyroid artery is
closely related to external laryngeal nerve at its origin
• Nerve moves away from the artery as artery approaches the upper pole of the gland.
• In order to avoid injury of external laryngeal nerve the superior thyroid artery need to be ligated during surgery just near the superior pole of thyroid gland
• A superior laryngeal nerve injury will lead to changes in the pitch of the voice and causes an inability to make explosive sounds due to paralysis of the cricothyroid muscle.
• A bilateral injury presents as a tiring and hoarse voice.
Superior Thyroid Artery and Vein
External BranchSuperior Laryngeal Nerve
Thyroid gland
- Do not ligate here
- Do ligate here

•Inferior thyroid arteries (ITA) are branches of the thyrocervical trunks arising from the subclavian arteries, run superomedially posterior to the carotid sheaths to reach the posterior aspect of the gland •Supply the postero-inferior aspect, including the inferior poles of the gland•The right and left superior and inferior thyroid arteries form anastamoses within the gland
Arteries of the Thyroid Gland
ITA
STA
Left Subclavian arteryThyrocervical trunk

Anatomical Relationships Between Recurrent Laryngeal Nerve and Inferior Thyroid Artery

The terminal branches of inferior thyroid artery are tightly related to recurrent laryngeal nerve
Inferior Thyroid Artery
Superior Thyroid Artery
Recurrrent Laryngeal Nerve
•Normally recurrent laryngeal nerve passes behind the ITA•In some cases it passes between branches of ITA or in front of terminal portion of inferior thyroid artery•It is easy to damage this nerve during ligation of inferior thyroid artery•Always perform ligation of inferior thyroid artery as far away as possible from thyroid gland!!!

Thyroid Ima Artery•~10% of people have small unpaired thyroid ima artery (branch of brachiocephalic trunk)•Other possible sources of Ima artery: arch of the aorta, right common carotid, subclavian, or internal thoracic arteries
•Ascends on the anterior surface of the trachea and continues to the thyroid isthmus
•The presence of this artery must be considered before tracheotomy (as a potential source of bleeding!)
Right common carotid artery

Veins of the Thyroid Gland•Three pairs of thyroid veins (superior, middle, inferior) form thyroid plexus of veins on the anterior surface of the thyroid gland and anterior to the trachea
•Superior thyroid veins accompany the superior thyroid arteries
Middle thyroid veins do not accompany but run essentially parallel courses with the inferior thyroid arteries
Inferior thyroid veins accompany the thyroid ima artery (if artery is present)

•Superior and middle thyroid veins drain into the internal jugular veins•Inferior thyroid veins drain into the brachio-cephalic veins posterior to the manubrium of sternum
Thyroid Veins
Internal jugular veins
Brachio-cephalic veins
Superior VenaCava
SuperiorMiddleInferiorThyroid veins
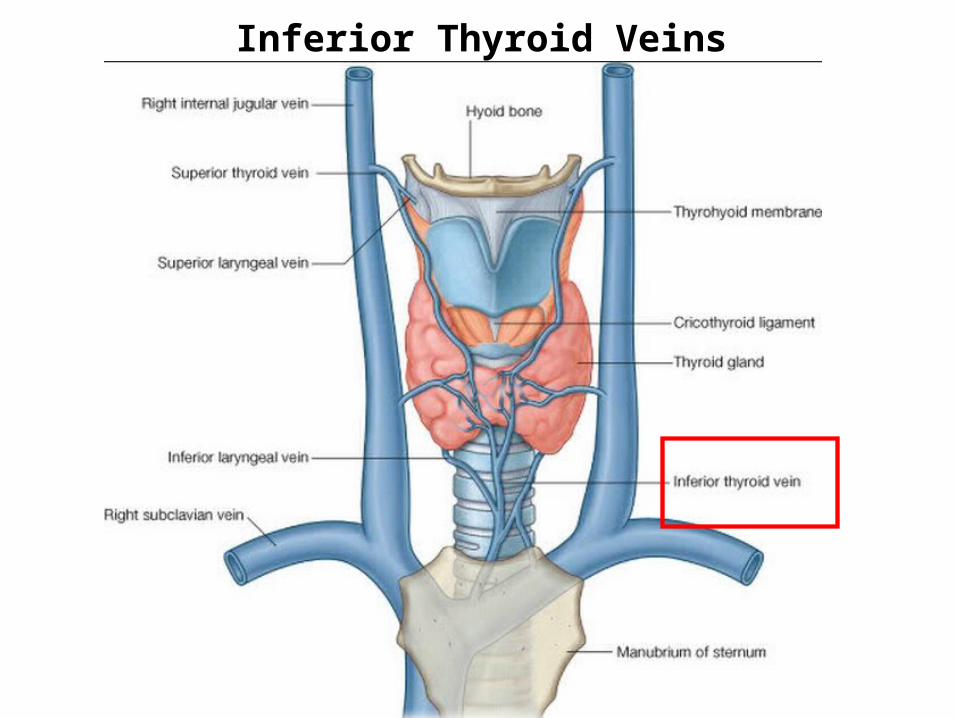
Inferior Thyroid Veins

Lymphatic Drainage of the Thyroid Gland
•Thyroid lymphatic vessels communicates with1st level: Prelaryngeal, Pretracheal, and Paratracheal lymph nodes2nd level: Superior deep cervical nodes (from the prelaryngeal nodes) and Inferior deep cervical nodes (from the pretracheal and paratracheal nodes). •Some lymphatic vessels may drain into the brachiocephalic lymphatic nodes or the thoracic duct
•Presence of metastases in lymphatic nodes of neck can be first sign of thyroid carcinoma!!!

Lymphatics of the Mediastinum 1, superior internal thoracic group; 2, superior phrenic or preaortic chain; 3, superior vagal or carotid subclavian preaortic chain; 4, left brachiocephalic chain; 5, aortic arch chain.6, inferior phrenic or prepericardial chain;
Brachiocephalic lymphatic nodes and thoracic duct collect lymph form Thyroid
•Left Jugular V.•Left Subclavian V.•Left Brachio-cephalic V.

Innervation of Thyroid Gland
•Nerves reach the thyroid through:
• Cardiac periarterial plexus•Superior and inferior thyroid plexus
•Only vasomotor fibers causing constriction of blood vessels
•Derived from the superior, middle, and inferior cervical sympathetic ganglia
•Endocrine secretion from the thyroid gland is hormonally regulated by the pituitary gland through TSH!

Thyroid Gland Development• Thyroid glands arises as an endodermal diverticulum from the floor of
the pharynxWeek 3: Thickening in the floor between the first and second pharyngeal
pouches Week 4: Endoderm evaginates ventrally into the mesoderm to form the thyroid
diverticulumWeek 5: a. Formation of thyroglossal duct b. Bifurcation on the tip of
Thyroglossal duct forms isthmus and the lateral lobes of the glandWeeks 5-6: Growth of duct down to the neck, migration f thyroid gland down to
the neckWeek 7: Gland reaches the final position in relation to the larynx and the
trachea

Thyroid gland development: some important facts • As the thyroid glandular tissue migrates inferiorly, the duct portion begins to involute • Site of connection thyroglossal duct with pharynx makes a foramen caecum• The distal part of the thyroglossal duct may develop pyramidal lobe of the thyroid
gland• The thyroid gland may develop in any part at the midline of the thyroglossal duct and
results in lingual,suprahyoid, retrohyoid, or infrahyoid positions• The thyroid gland is relatively large in newborn babies
By the seventh week gland reaches the final position

Thyroglossal Duct Cyst
• Thyroglossal duct normally disappears but remnants of epithelium may remain and form a thyroglossal duct cyst
• The cyst is usually near or within the body of the hyoid and forms a swelling in the anterior part of the neck always on the midline of the neck!!!!
• Size 1 to 4 cm in diameter• Lined by stratified squamous
epithelium, and cyst may harbor lymphoid aggregates or remnants of recognizable thyroid tissue –important diagnostic sign!

A 16-year-old girl has noted a lump on her neck for the past 3 years. On physical examination there is a firm, non-tender, 2 cm discrete mass on her anterior neck at the level of the hyoid bone. Which of the following is the most likely diagnosis?
A: Thyroglossal duct cyst

Ectopic Thyroid Gland
Variants:A. Lingual thyroid gland (90%)B. Sublingual (suprahyoid, infrahyoid)C. Others (trachea, submandibular,
lateral cervical regions, axilla, palatine tonsils, carotid bifurcation, iris of the eye, pituitary gland)
• Important to differentiate between an ectopic thyroid gland and a thyro-glossal duct cyst when excising a cyst!!! Failure to do so may result in total thyroidectomy!!!!
•Definition: presence of thyroid tissue in locations other than the normal anterior neck region between the second and fourth tracheal cartilages •Most frequent form of thyroid dysgenesis •Up to 10% of adults may harbor ectopic tissue

Accessory Thyroid Glandular Tissue
•Definition: additional thyroid tissue in locations other than the normal along with normally positioned thyroid gland•May appear anywhere along the embryonic course of the thyroglossal duct •MC location of accessory thyroid gland is on the thyrohyoid muscle•Caution: it is often of insufficient size to maintain normal function if the thyroid gland is removed

Enlargement of the Thyroid Gland
•Definition: A non-neoplastic and non-inflammatory enlargement of the thyroid gland•Most common causes of GOITRE: A. Endemic Iodine deficiency (N=150mcg/day), MC cause in the worldB. Graves Disease (autoimmune) + Autoimmune Thyroiditis MC causes in US•Goitres can be associated with increased or decreased production of thyroid hormones•May compress the trachea, esophagus, and recurrent laryngeal nerves

Goitre ClassificationA. Toxic goitre Non-toxic goitre -determined by levels of T3, T4, TSH and and clinical presentationB. Diffuse goitre; Nodular goitre; Multinodular goitre -determined by UltraSound examination and palpation of Thyroid
Multinodular goitre Diffuse goitre

THYROID CARCINOMAS• 1.5% of all cancers. • A female predominance has been noted among patients who
develop thyroid carcinoma in the early and middle adult years. In contrast, cases presenting in childhood and late adult life are distributed equally among males and females.
• Most thyroid carcinomas (except medullary carcinomas) are derived from the thyroid follicular epithelium
• There are 4 types of thyroid carcinomas:• Papillary carcinoma (>85% of cases) - Most Common • Follicular carcinoma (5% to 15% of cases) • • Anaplastic (undifferentiated) carcinoma (<5% of cases) • Medullary carcinoma (5% of cases)Major type of treatment for thyroid carcinomas is
thyroidectomy!

Thyroidectomy•Removal of the gland•If possible, posterior part of each lobe of the thyroid gland is usually preserved, a procedure called near-total thyroidectomy, to protect the recurrent and superior laryngeal nerves and to spare the parathyroid glands•Technique: Collar incision•Use of intraoperative RLN monitoring •Complications: •A. Postoperative hemo-rrhage after thyroid gland surgery may compress the trachea, making breathing difficult•B. Hypocalcemia–monitor Ca level and clinical signs and serum level of Ca2+!!!