clinical characteristics and outcome of hyperglycaemic emergencies in johannesburg africans
TRANSCRIPT
INTERNATIONAL SCENE
Clinical Characteristics and Outcome ofHyperglycaemic Emergencies inJohannesburg AfricansM. Zouvanis, A.C. Pieterse, H.C. Seftel, B.I. Joffe
Carbohydrate and Lipid Metabolism Research Group, Department ofMedicine, University of the Witwatersrand, Johannesburg 2193,South Africa
In this prospective analysis we investigated the clinical characteristics of black SouthAfrican diabetic patients admitted to hospital with hyperglycaemic emergencies. The studycases were selected from the medical admissions to an urbanized, Johannesburg academichospital over a period of 12 months. Only patients with severe diabetic ketoacidosis(DKA) or hyperosmolar non-ketotic hyperglycaemia (HNKH) as defined in the text wereincluded. Over the study period, we identified 58 patients with severe DKA (M: 32, F:26) and 24 with HNKH (M: 14, F:10). Thirty-two of the patients with DKA (55.2 %) wereclassified as having non-insulin dependent (Type 2) diabetes mellitus (NIDDM). Comparedto the 26 subjects with insulin-dependent (Type 1) diabetes mellitus (IDDM), the NIDDMpatients were older (51.7 vs 27.7 years) and had a significantly higher body mass index(BMI) (29.4 vs 23.5 kg m−2, p = 0.002), and glucose levels 47.5 vs 34 mmol l−1 p = 0.004).Mortality from DKA was 6.8 % and from HNKH 16.6 %. Infection was the leadingprecipitating factor for both DKA and HNKH, followed by first presentation and non-compliance. We conclude that the majority of urban African patients admitted to hospitalwith DKA have NIDDM. Mortality from DKA among the black Africans in Johannesburgis low and comparable to the mortality in western Europe. 1997 by John Wiley & Sons, Ltd.
Diabet. Med. 14: 603–606
No of Figures: 2. No of Tables: 2. No of Refs: 15
KEY WORDS Diabetic ketoacidosis African diabetes Hyperosmolar non-ketotichyperglycaemia
Received 21 October 1996; revised 7 March 1997; accepted 9 March 1997
Both diabetes and diabetic emergencies are commonIntroductionin Johannesburg Africans, but there is surprisingly littleinformation on the clinical characteristics and outcomesHyperglycaemic emergencies, both diabetic ketoacidosis
(DKA) and hyperosmolar non-ketotic hyperglycaemia of such emergencies admitted to academic hospitals.This prompted the present study.(HNKH), remain an important clinical problem among
the black inhabitants of Africa (hereafter designatedAfricans).1,2 Moreover, it has been suggested that the Patients and Methodsmortality is particularly high mainly due to the lack ofappropriate medical facilities and shortage of insulin.3 The study was undertaken at Hillbrow Hospital, which
is an academic institution of about 1000 beds, linked toThese latter observations have been largely based onstudies from Tanzania and Ghana.4,5 In an earlier study the University of the Witwatersrand. It is located in the
centre of Johannesburg and serves a predominantlyfrom Ethiopia, mortality was substantially less.6
In South Africa the situation is likely to be different. African community of approximately 200 000 people.7
Referrals from peripheral hospitals are also common. AllThe majority of the 35 million Africans, who comprisethree-quarters of the total population, are urbanized, and medical admissions were prospectively screened by
the investigators, during the period October 1994 toin Johannesburg which is the commercial centre of SouthAfrica, the majority of Africans are semi-westernized or September 1995. All diabetic emergencies were identified
and followed up in the ward until discharge. Specialwesternized and hence have access to better health careincluding a number of academic hospitals. note was taken of precipitating factors and whether the
patients had new or previously diagnosed diabetes. Serumosmolality was calculated according to the formula, using
* Correspondence to: Dr M. Zouvanis, Department of Medicine, millimolar concentrations, of (Na+K) × 2 + urea + glucose.University of the Witwatersrand Medical School, 7 York Road, Analysis was confined to severe DKA and HNKHParktown, Johannesburg 2193, South Africa
patients. Severe DKA was defined as pH , 7.25, bloodSponsors: South African Medical Research Council and University ofthe Witwatersrand Research Committee Grant. glucose . 16 mmol l−1 and marked ketonuria on urine
603CCC 0742–3071/97/070603–04$17.50 1997 by John Wiley & Sons, Ltd. DIABETIC MEDICINE, 1997; 14: 603–606
INTERNATIONAL SCENE
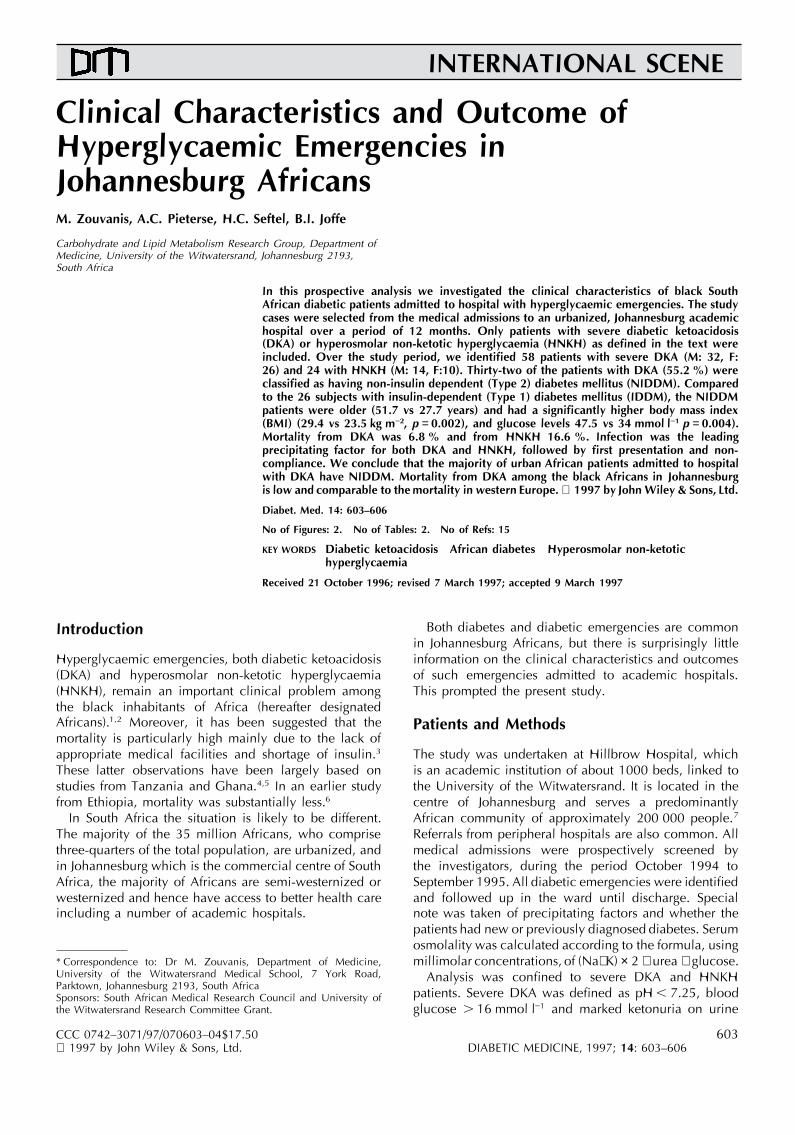
Figure 1. Flowsheet for the distribution of diabetes-related admissions to Hillbrow Hospital over a 1-year period
dipstix (Combur 9, Boehringer Mannheim). Severe HNKH 12 were known NIDDM, well controlled with oralhypoglycaemic agents (OHA) for a period of at least 1was defined as a serum osmolality . 330 mosm l−1, blood
glucose . 25 mmol l−1, absent or minimal ketonuria, and year. Four of these were known to be on sulphonylureasalone and two were receiving a combination of sulphonyl-decreased sensorium.
Statistical analysis was performed by means of Student’s ureas and metformin but the type of OHA used in theother six patients was not specified. Nine patients weret-test, or chi square test where applicable.treated for at least 1 year with OHA and now requiredinsulin, alone or in combination. The remaining 11Resultspatients were newly diagnosed. Nine of these patientswere older than 40 years of age and two who were inDuring the 1-year study period, we screened 7812
medical admissions to the Hillbrow Hospital. Of these the age group between 30 and 40 years had a BMI. 28 kg m−2 as previously mentioned.admissions, 614 were diabetes related (7.8 %) and of
those 58 had severe DKA and 24 severe HNKH (Figure 1). Twenty-six of the DKA patients were classified ashaving insulin-dependent (type 1) diabetes mellitusNone of the DKA patients had evidence of respiratory
acidosis, as the paCO2 values were low (below 3.8 kPa) (IDDM). Nineteen of these patients were known to haveIDDM, as they had presented previously with DKA inin all patients. Serum lactate was not measured in any
of the patients as this is not routinely available in our young age (, 30 years). Of the seven newly diagnosedpatients, four were under the age of 30 years or, if theyhospital. All patients showed evidence of elevated serum
urea and creatinine on presentation, which however was were in the age group 30–40 years, had a BMI, 23 kg m−2 (three patients).corrected after rehydration in all but two cases, both of
whom had evidence of chronic renal failure. As seen in Table 1, the NIDDM patients were olderand they had a significantly higher BMI. The mean pHOut of 58 DKA patients, 32 could be classified as
having non-insulin-dependent (Type 2) diabetes mellitus was similar in the two groups, but the glucose wassignificantly higher in the NIDDM group and this(NIDDM) (Table 1). All but two patients were over the
age of 40 years at onset. The two exceptions, both aged was largely responsible for their higher osmolality.Approximately two-thirds of the patients in each group33, had a body mass index (BMI) of 28 and 33.2 kg m−2,
respectively, on first presentation. Of these 32 patients, had a precipitating factor for the acute event. Morbidity
Table 1. Clinical and biochemical characteristics of patients admitted to Hillbrow Hospital with severe DKA
Type of Number Sex Age BMI pH Glucose Osmolality Hospital 1st pres. Precip. Deathsdiabetes M:F (yr) (kg m−2) (mmol l−1) (mosm l−1) days factor
NIDDM 32 13/19 51.7 29.32 7.12 47.56 336.8 9.9 11/32 22/32 3(55.2 %) (10.1) (7.5) (0.09) (23.3) (42) (4.5) (34.3 %) (68.7 %)
IDDM 26 19/7 27.7 23.52 7.07 34.0 322.3 8.8 7/26 18/26 1(44.8 %) (6.9) (4.65) (0.11) (17.5) (27) (5.4) (26.9 %) (69.2 %)
Total 58 32/26 4(6.8 %)
p , 10−6 0.002 NS 0.009 NS NS NS NS NS
All values are means (SD).Student’s t-test (unpaired) or chi-square analysis.
604 M. ZOUVANIS ET AL.

INTERNATIONAL SCENETable 2. Clinical and biochemical characteristics of patients admitted to Hillbrow Hospital with severe HNKH; all patients NIDDM
Number Sex Glucose pH Age Osmolality 1st Precip. Hosp.M:F (mmol l−1) (yr) (mosm l−1) pres. factor days
Survivors 20 13/7 63.8 7.30 58.7 367.8 9/20 14/20 11.5(36.6) (0.07) (12.4) (36.4)
Non-survivors 4 1/3 46.3 7.30 60.5 371.2 1/4 4/4 2.5(16.6 %) (4.8) (0.09) (7.4) (26.1)
Total 24 14/10 60.87 7.30 59.04 368.3 10/24 18/24 9.8(33.7) (0.07) (11.5) (34.4)
p NS NS NS NS ND ND ND
All values are means (SD).ND, not done; NS, not significant.
as assessed by hospital stay was similar in the two hyperglycaemic emergenices presented in DKA, with agroups. There were four deaths (6.8 %), three in the preponderance of about 2:1 to the HNKH patients. TheNIDDM group and one in the IDDM group. All four next and most striking point, was that the majority ofdeaths had evidence of underlying infections and had a the DKA patients had NIDDM clinically (55.2 %). Therelow BMI (data not shown). No other clinical or biochemi- are a number of possible explanations for this finding.cal factor was related to mortality. Firstly, NIDDM, which is assuming epidemic proportions
All HNKH patients were classified as NIDDM. Their in black South Africans, comprises the bulk of diabeticdata are shown in Table 2. There were four deaths in patients, approximately 90 %.8 Secondly, there is athis group (16.6 %). No association was found between contribution from the previously reported findings ofmortality and any of the biochemical measurements, insulinopenia in black South African NIDDM patients.9however all four deaths had precipitating events, two Similar observations have been made in African Americanhad infection, one had a cerebrovascular accident and NIDDM patients in New York, the so-called ‘Flatbushone had both. The HNKH patients spent more days in Diabetes’ syndrome,10 and also in a previous study fromthe hospital than the DKA patients (11.5 vs 9.2), but this Ethiopia,6 where at least 9 out of 34 patients (26 %)was not significant. presenting with DKA were likely to have NIDDM. Finally,
Overall the most common precipitating factor was there is the frequent occurrence of severe infections ininfection, accounting for 39 % of all cases, followed by Africans with diabetes.1,4 The high levels of counterregu-first presentation in 23 % of the cases and non-compliance latory hormones that accompany infection, in conjuctionin 21 %. No precipitating factor was found in 7 % of with the insulinopenia, would be expected to precipitatecases and various other causes accounted for the DKA.11 Autoimmunity against b cell antigens leading torest (Figure 2). insulinopenia, is unlikely to be an important factor, since
this feature appears to be rare in African diabetics.12,13
Discussion The most common precipitating factor in this studywas infection, which is in contrast to recently published
The first point of interest in this study was that the data from the USA where infection accounted for onlymajority of the African patients coming to hospital with 14 % of cases.14 Surprisingly, cessation of insulin therapy
for whatever reason, was responsible for only 21 % ofthe total events in our patients, compared to 66 %reported in the African American study.
The mortality in our trial was found to be low. It wascomparable to the findings of another prospective trialin DKA patients published from Baragwanath Hospitalin Soweto (an academic hospital on the outskirts ofJohannesburg), but the mortality from HNKH was substan-tially lower in our study.15 This low mortality from DKA,which is comparable to the figures from western Europeancountries, may however not be representative of thewhole of South Africa. Data from rural areas are lacking,thus making any reasonable comparisons impossible.
In conclusion, our study has shown that NIDDMFigure 2. Precipitating factors of hyperglycaemic emergencies patients form the majority of Africans presenting to(both diabetic ketoacidosis and hyperosmolar non-ketotic
hosptial in DKA. Hyperglycaemic emergencies requiringhyperglycaemia) admitted to Hillbrow Hospital; G/E, gastroent-eritis hospital admission in South Africa appear to be mainly
605HYPERGLYCAEMIC EMERGENCIES IN JOHANNESBURG AFRICANS

INTERNATIONAL SCENE7. Rasmussen K, Price M, Katz B, Wright A. Report ontriggered by infection. Lack of insulin, at least in urban
Hillbrow Hospital by University of the Witwatersrand,South Africa, does not appear to be a major problem.Faculty of Health Sciences task team. Johannesburg: Wits
The mortality from hyperglycaemic emergencies in University Press, December 1996.Johannesburg is low and comparable to the mortality 8. Levitt NS, Mollentzie WF. Diabetes mellitus and impaired
glucose tolerance. A review of South African studies. In:rates reported in most western societies.Fourie J, Steyn K, eds. Chronic Diseases of Lifestyle inSouth Africa. MRC Technical Report, Cape-Town: MRCPublications 1995; 99–126.
9. Joffe BI, Panz VR, Wing JR, Raal FJ, Seftel HC. PathogenesisAcknowledgementsof non-insulin-dependent diabetes mellitus in the blackpopulations of southern Africa. Lancet 1992; 340: 460–
This study was supported by the South African Medical 462.Research Council and the University of the Witwatersrand 10. Banerji MA, Chaiken RL, Huey H, Tuomi T, Norin AJ,
Mackay IR, et al. GAD antibody negative NIDDM inResearch Committee Grant. We thank J. Pieters for typingadult black subjects with diabetic ketoacidosis andthe manuscript.increased frequency of human leukocyte antigen DR3and DR4. Diabetes 1994; 43: 741–745.
11. Kinney JM, Felig P. The metabolic response to injury andinfection. In: De Groot LJ, Cahill GF, Odell WD, Martini
References L, Potts JT, Nelson DH, et al., eds. Endocrinology, vol.3. New York: Grune & Stratton, 1979: 1963–1985.
12. McLarty DG, Athaide I, Botazzo GF, Swai AMB, Alberti1. Buch E, Irwig LM, Huddle KR, Krige LP, Krut LH, KuylJM. Pointers to preventing hyperglycaemic emergencies KGMM. Islet cell antibodies are not specifically associated
with insulin-dependent diabetes in Tanzanian Africans.in Soweto. S Afr Med J 1983; 64: 705–709.2. Huddle KR, Gill GV. Reducing acute hyperglycaemic Diabet Res Clin Pract 1990; 9: 219–224.
13. Omar MAK, Botazzo GF, Asmal AC. Islet cell antibodiesmortality in African diabetic patients. Diabetic Med 1989;6: 64–66. and other autoantibodies in South African blacks and
Indians with insulin-dependent diabetes mellitus. Horm3. Alberti KGMM. Insulin dependent diabetes mellitus: alethal disease in the developing world. Br Med J 1994; Metab Res, 1986; 18: 126–128.
14. Musey VC, Jenny KL, Crawform R, Klatka MA, McAdams309: 754–755.4. McLarty DG, Kinabo L, Swai ABM. Diabetes in tropical D, Phillips LS. Diabetes in urban African Americans. I.
Cessation of insulin therapy is the major precipitatingAfrica: a prospective study, 1981–7. II Course andprognosis. Br Med J 1990; 300: 1107–1110. cause of diabetic ketoacidosis. Diabetes Care 1995; 18:
483–489.5. Adubofur KOM, Ofei F, Mensah-Adubofur J, Owusu SK.Diabetes in Ghana: a morbidity and mortality analysis. 15. Rolfe M, Ephraim GG, Lincoln DC, Huddle KRL. Hyperos-
molar non-ketotic diabetic coma as a cause of emergencyInt Diabetes Dig 1993; 4: 90–92.6. Lester FT. Ketoacidosis in Ethiopian diabetics. Diabetologia hyperglycaemic admission to Baragwanath Hospital. S
Afr Med J 1995; 85: 173–176.1980; 18: 375–377.
606 M. ZOUVANIS ET AL.