clinical dilemma: which adjuvant chemotherapy is just right? dr. maureen trudeau head, division of...
TRANSCRIPT
Clinical Dilemma:Which Adjuvant
Chemotherapy is Just Right?Dr. Maureen Trudeau
Head, Division of Medical Oncology/HematologyToronto Sunnybrook Regional Cancer Centre
Associate Professor, University of Toronto
June 15, 2007
Systemic Therapy - Chemotherapy
• Overall survival improvement in clinical trials both for standard and newer treatments
• Choice – for patients, for physicians (anthracycline +/- taxanes)
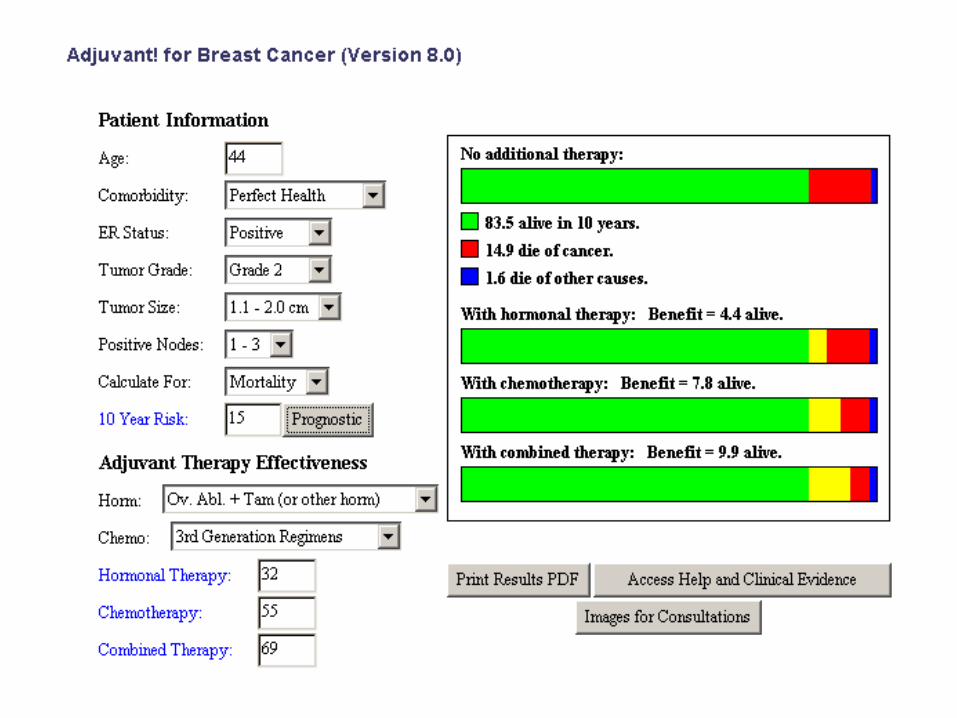
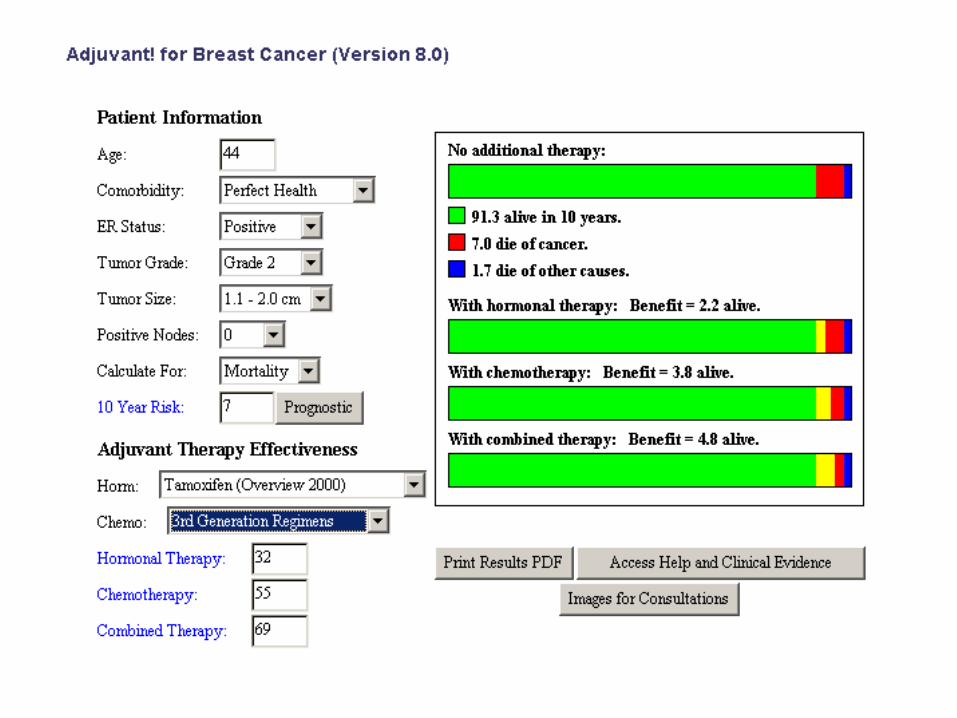
• Better decision making aids– www.adjuvantonline.com
• Molecular profiles – Oncotype Dx, MammoPrint• Improved supportive care
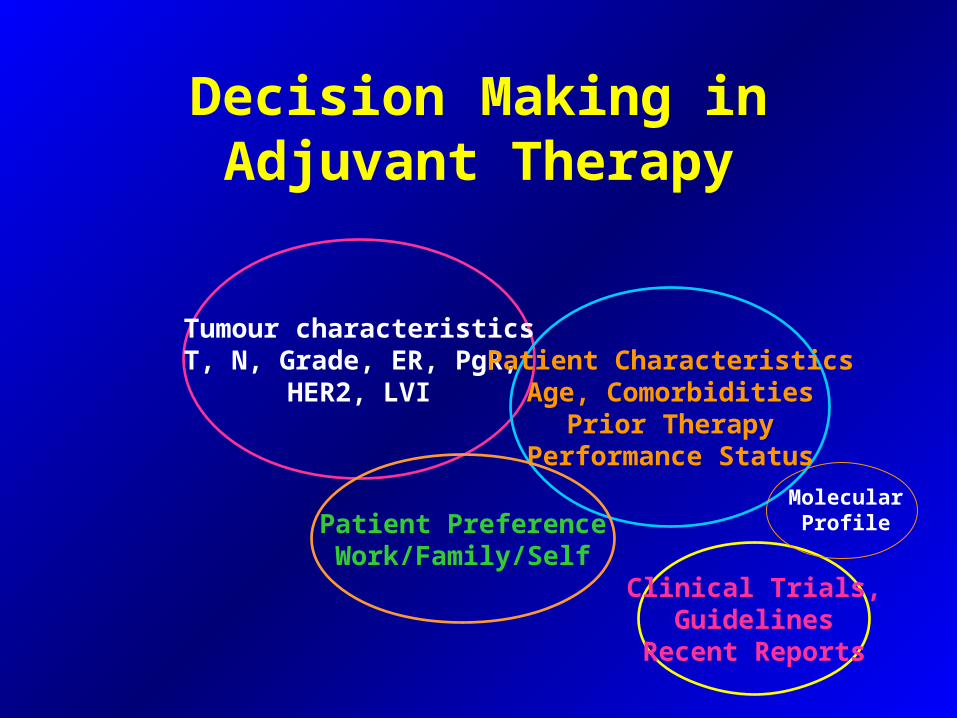
Decision Making in Adjuvant Therapy
Tumour characteristicsT, N, Grade, ER, PgR,
HER2, LVIPatient Characteristics
Age, ComorbiditiesPrior Therapy
Performance Status
Patient PreferenceWork/Family/Self
Clinical Trials,Guidelines
Recent Reports
Molecular Profile
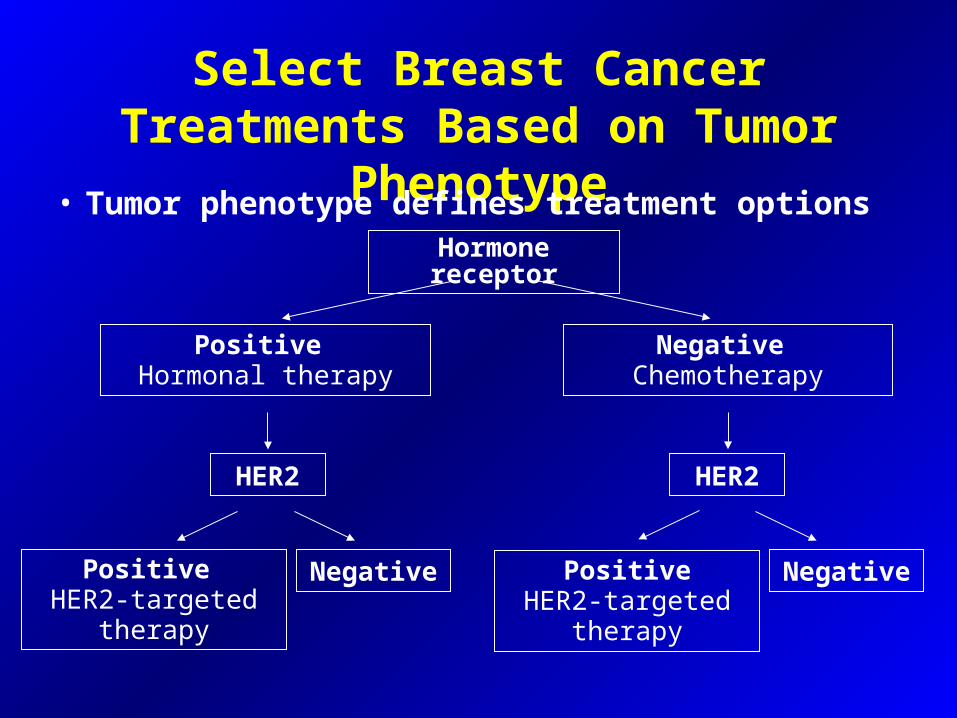
Select Breast Cancer Treatments Based on Tumor Phenotype
• Tumor phenotype defines treatment options
Hormone receptor
Positive Hormonal therapy
Negative Chemotherapy
Positive HER2-targeted
therapy
HER2 HER2
Negative PositiveHER2-targeted
therapy
Negative
BIGBIG--TRANSBIG TRANSBIG SecretariatSecretariat–– Used with permissionUsed with permissionMarch 2005 March 2005 -- ConfidentialConfidential
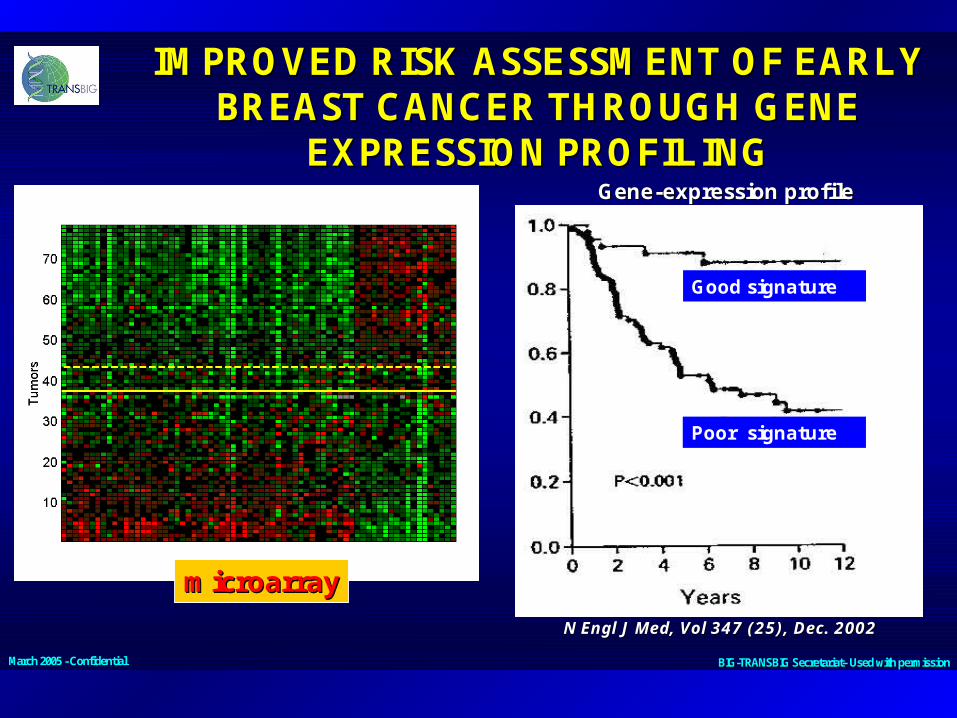
IMPROVED RISK ASSESSMENT OF EARLY IMPROVED RISK ASSESSMENT OF EARLY BREAST CANCER THROUGH GENE BREAST CANCER THROUGH GENE
EXPRESSION PROFILINGEXPRESSION PROFILING
microarraymicroarray
GeneGene--expression profileexpression profile
Good signature
Poor signature
N Engl J Med, Vol 347 (25), Dec. 2002N Engl J Med, Vol 347 (25), Dec. 2002
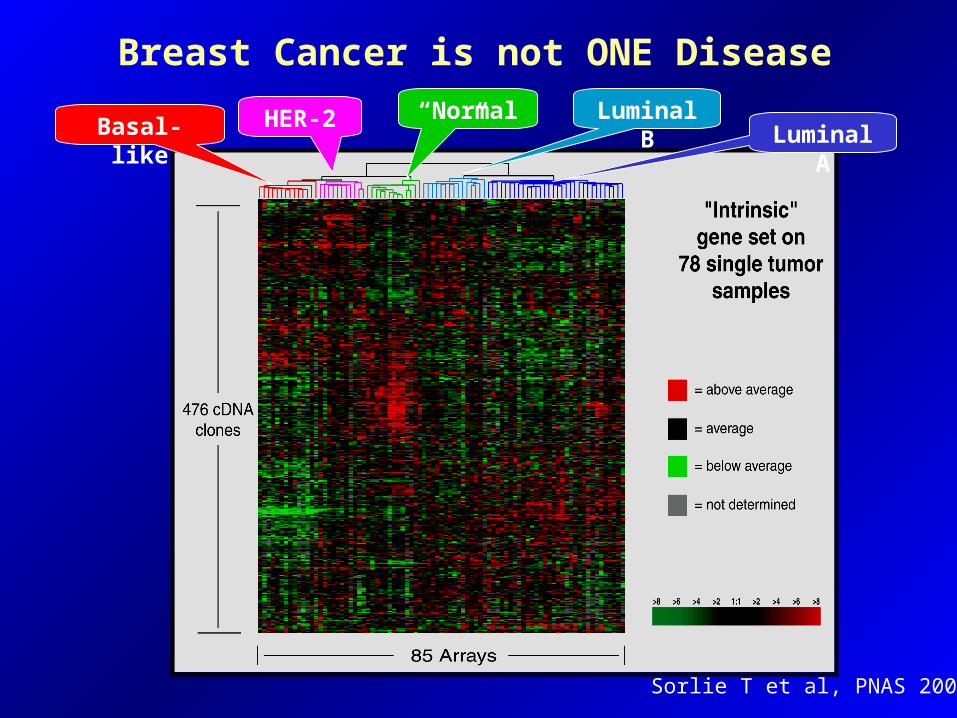
Breast Cancer is not ONE Disease
HER-2Basal-like Luminal ALuminal B“Normal”
Sorlie T et al, PNAS 2001

Gene Expression Patterns of Breast Carcinomas
Basal-likeSubgroup
= E
HER2Subgroup
= D
Normalbreast
like
LuminalSubtype
C
LuminalSubtype
B
LuminalSubtype
A
ERGene
expression
ERGene
expression
E
DCB
A
O.S.
months
Adapted from PNAS, 2001, vol 98 no. 19

All Breast Cancer
ER+65-75%
HER2+15-20%
Basaloid15%

Molecular Classifications of Breast Tumors
Luminal A ER +
high
Prolif
-
P53 mutations
16%
Luminal B ER +
low
+ 71%
Basal -like ER - + 75%, also
BRCA1
ERBB2 + ER-/+ -/+ 86%
Normal-like ER - -
Sorlie 2007
The “Triple Negative” Breast Cancer
Estrogen Receptor (ER) negativeProgesterone receptor (PR) negative
Her2neu (HER2) negative
Up to 90% of Triple Negative Breast Cancers are Basal-Like Breast Cancers
ER/PR/HER2 -

Basal like Breast Cancers (BLC)
• BLCs comprise 15% of all invasive cancers
• More common in:– Younger pts– African Americans (40% premenopausal women)– BRCA1 mutation carriers
• BLC are associated with:– high grade– p53 mutations– Increased expression of EGFR– CK5/6 (recent studies in 2006…Vimentin, cKIT, SRC)
Sample
• From the HBBC database, 1601 (80%) of patients had details on hormone receptors/HER2 and were eligible for the study
• 180 (12%) of the 1601 patients were defined as basal-like breast cancers
• Mean follow up was 8.1 years
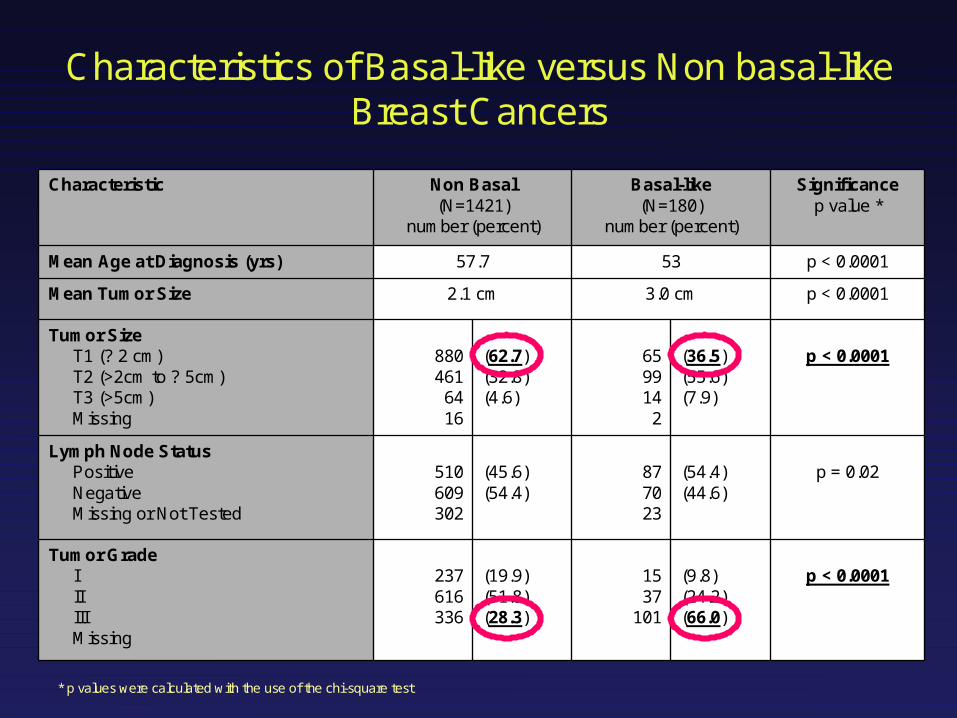
p = 0.02(54.4)(44.6)
877023
(45.6)(54.4)
510609302
Lymph Node StatusPositiveNegativeMissing or Not Tested
p < 0.0001(9.8)(24.2)(66.0)
1537
101
(19.9)(51.8)(28.3)
237616336
Tumor GradeIIIIIIMissing
p < 0.0001(36.5)(55.6)(7.9)
659914
2
(62.7)(32.8)(4.6)
880461
6416
Tumor SizeT1 (? 2 cm)T2 (>2cm to ? 5cm)T3 (>5cm)Missing
p < 0.00013.0 cm2.1 cmMean Tumor Size
p < 0.00015357.7Mean Age at Diagnosis (yrs)
Significancep value *
Basal-like(N=180)
number (percent)
Non Basal(N=1421)
number (percent)
Characteristic
Characteristics of Basal-like versus Non basal-like Breast Cancers
* p values were calculated with the use of the chi-square test

Hazard Rate of Distant Recurrence
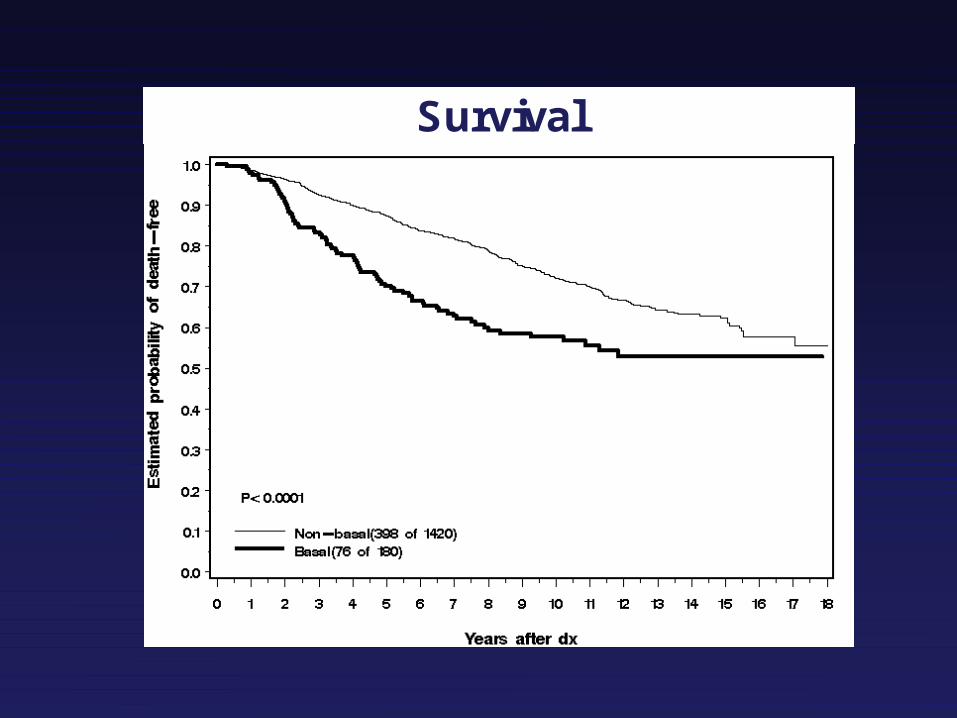
Survival

Novel Therapies for TN
• BRCA1 involved in repair of double stranded DNA breaks– Mutations implicated in breast/ovarian susceptibility
• BRCA1 cancers appear to closely resemble sporadic triple negative breast cancers on molecular level
• in vitro chemo-sensitivity studies have found that basal-like breast cancers may be particularly sensitive to cisplatin and to other drugs that cause double-strand breaks in DNA
• Agents such as cisplatin and carboplatin may be more effective treatment than other types of chemotherapy for the basal like group
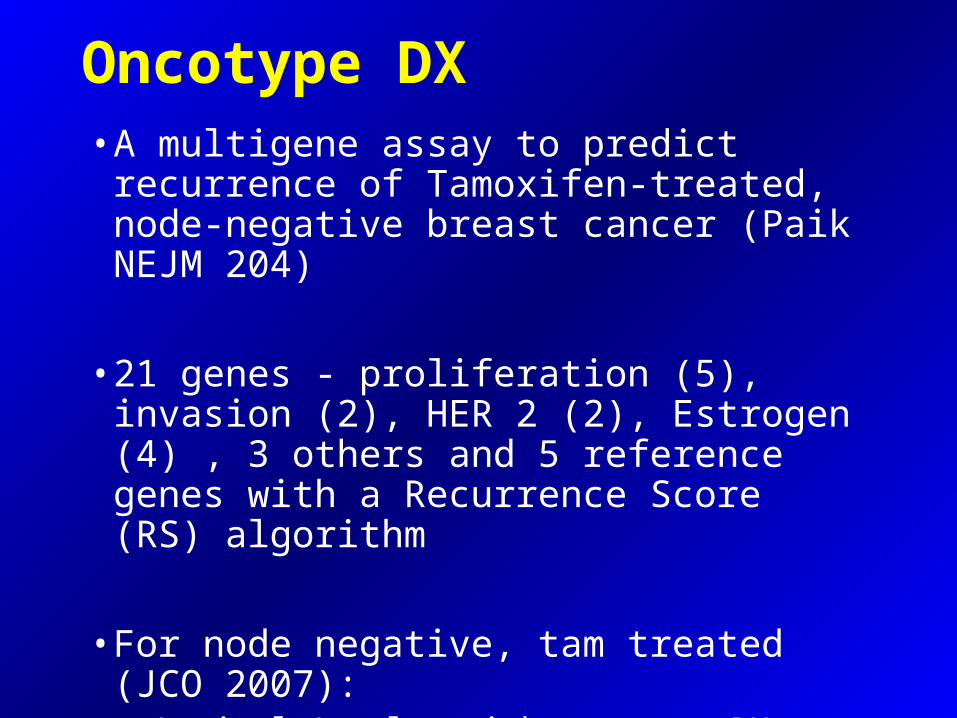
Oncotype DX• A multigene assay to predict recurrence of
Tamoxifen-treated, node-negative breast cancer (Paik NEJM 204)
• 21 genes - proliferation (5), invasion (2), HER 2 (2), Estrogen (4) , 3 others and 5 reference genes with a Recurrence Score (RS) algorithm
• For node negative, tam treated (JCO 2007): –Luminal A = low risk oncotype DX–Luminal B = mod/high risk

Program for the Assessment of Clinical Program for the Assessment of Clinical Cancer Tests (PACCTCancer Tests (PACCT--1):1):
TTrial AAssigning IIndividuaLLized OOptions for TRReatment (TAILORxTAILORx)
Participating Groups:Participating Groups:ECOG, North American Breast Cancer Intergroup ECOG, North American Breast Cancer Intergroup
(CALBG, SWOG, NCCTG, NCIC, & ACOSOG) (CALBG, SWOG, NCCTG, NCIC, & ACOSOG)
& NSABP& NSABP

Background:Background:Management of ER-Positive, Lymph-
Node Negative Breast Cancer
• ~ 137,000 diagnosed annually in North America• ~ 80-85% are adequately treated with
• surgery +/- irradiation• hormonal therapy
• Adding chemotherapy recurrence by ~ 25%• absolute benefit is small (~3-5% or less)
• Current practice guidelines • chemotherapy recommended for most

• Approved diagnostic test by regulatory agencies in the United States (CLIA)
• No special processing required - may be performed on routinely collected and processed formalin-fixed, paraffin embedded tissue
• Extensive post-marketing experience and familiarity in U.S. oncology community
• Increasing precedent for third party reimbursement• Prior successful collaboration between NCI-
sponsored groups and industry partner
Background:Background:Practical Considerations Practical Considerations for Selectingfor Selecting
Oncotype DX AssayOncotype DX Assay
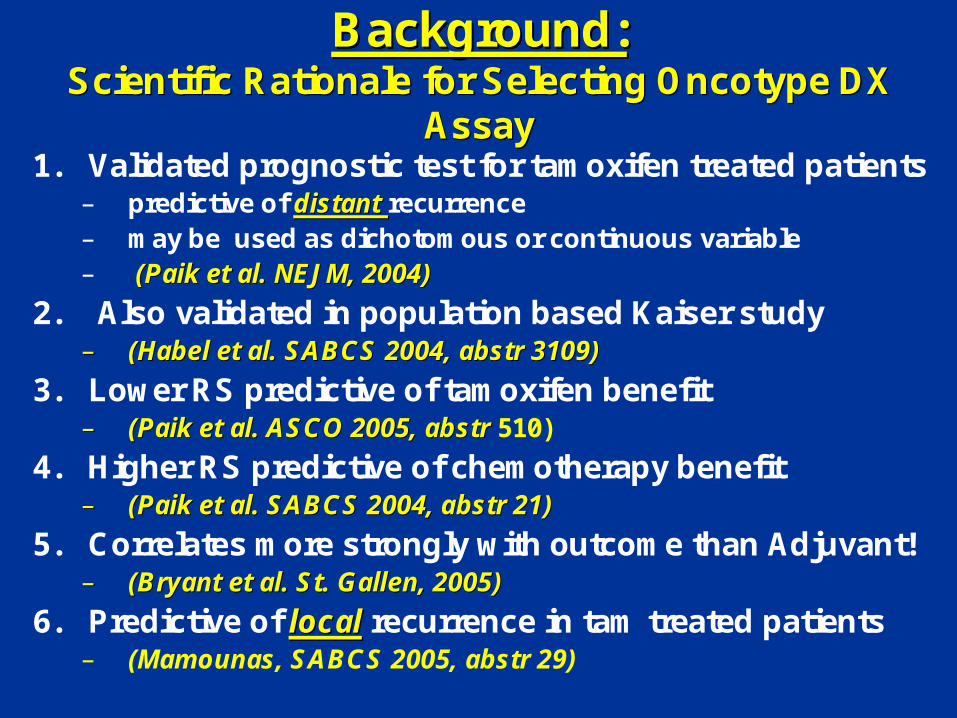
Background:Background:Scientific Rationale for Selecting Oncotype DX Scientific Rationale for Selecting Oncotype DX
AssayAssay1. Validated prognostic test for tamoxifen treated patients
– predictive of distant distant recurrence – may be used as dichotomous or continuous variable– (Paik et al. NEJM, 2004)(Paik et al. NEJM, 2004)
2. Also validated in population based Kaiser study –– (Habel et al. SABCS 2004, abstr 3109)(Habel et al. SABCS 2004, abstr 3109)
3. Lower RS predictive of tamoxifen benefit –– (Paik et al. ASCO 2005, abstr(Paik et al. ASCO 2005, abstr 510)
4. Higher RS predictive of chemotherapy benefit–– (Paik et al. SABCS 2004, abstr 21)(Paik et al. SABCS 2004, abstr 21)
5. Correlates more strongly with outcome than Adjuvant! –– (Bryant et al. St. Gallen, 2005)(Bryant et al. St. Gallen, 2005)
6. Predictive of locallocal recurrence in tam treated patients – (Mamounas, SABCS 2005, abstr 29)

T A I L O R xT A I L O R xS t u d y D e s i g nS t u d y D e s i g n
ARM AHormona l Therapy
A lone
Secondary S tudy Group 1RS < 11
~29% of P opulation
ARM BHormona l Therapy
A lone
ARM CChemotherapy P lusHormona l Therapy
RANDOMIZEStratification Factors :
Tumor S ize , Menopausal S tatus ,P lanned Chemo, P lanned Radiation
Primary S tudy GroupRS 11-25
~44% of P opulation
ARM DChemotherapy P lusHormona l Therapy
Secondary S tudy Group 2RS > 25
~27% of P opulation
REGISTERSpecimen Banking
ONCOTYPE DX ASSAY
Pre-REGISTER

Background:Background:Definition of Risk Groups for TAILORxDefinition of Risk Groups for TAILORx
•• Risk groups originally defined as (NEJM, 2004):Risk groups originally defined as (NEJM, 2004):– < 18 “Low Risk”– 18-30 “Intermediate Risk”– > 30 “High Risk”
•• Definitions modified for Definitions modified for TAILORxTAILORx::– 11-25 “Primary Study Group”– < 11 “Secondary Study Group 1”– > 25 “Secondary Study Group 2”
•• Rationale for selecting RS 11 as the lower bound for Primary StuRationale for selecting RS 11 as the lower bound for Primary Study Group:dy Group:– RS predicts distant and local recurrence– RS 11: ~ 10% local & distant recurrence rate at 10 years– 10% threshold is typically used for recommending adjuvant chemotherapy
•• Rationale for selecting 25 as upper bound for Primary Study GrouRationale for selecting 25 as upper bound for Primary Study Group:p:– RS 30 associated with 20% risk of distant recurrence– Lowering threshold to 25 reduces risk for undertreatment– When viewing chemotherapy and tamoxifen benefit as a continuous
variables, 95% Confidence Intervals overlap in the 11-25 RS range (shown in next slides)

Adapted by Dr. Maureen E. Trudeau, MD
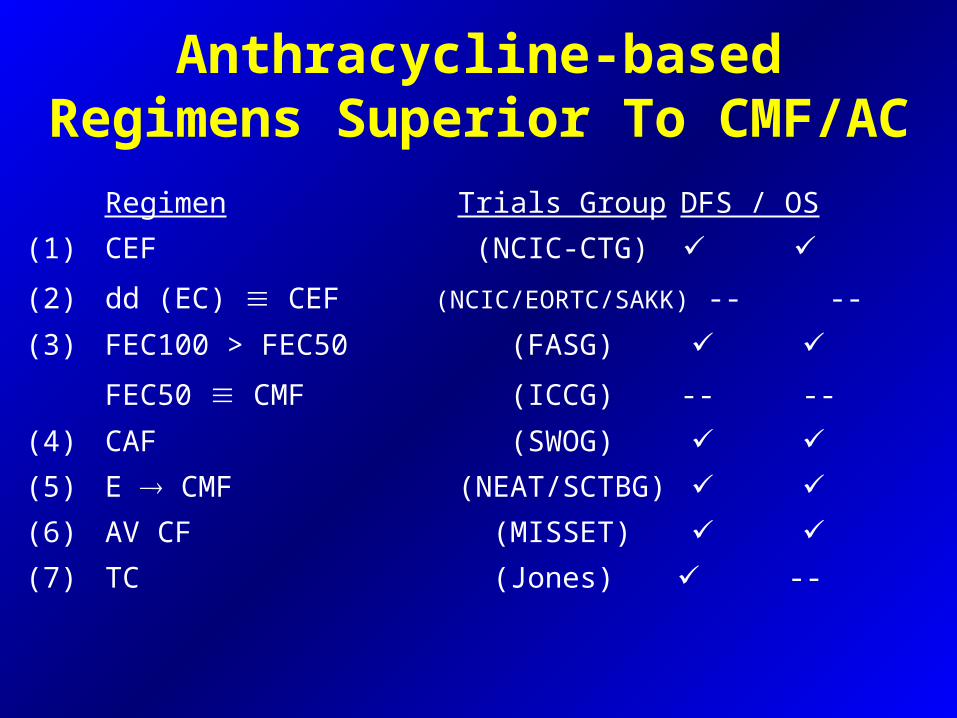
Anthracycline-based Regimens Superior To CMF/AC
Regimen Trials Group DFS / OS
(1) CEF (NCIC-CTG)
(2) dd (EC) CEF (NCIC/EORTC/SAKK) -- --
(3) FEC100 > FEC50 (FASG)
FEC50 CMF (ICCG) -- --
(4) CAF (SWOG)
(5) E CMF (NEAT/SCTBG)
(6) AV CF (MISSET)
(7) TC (Jones) --
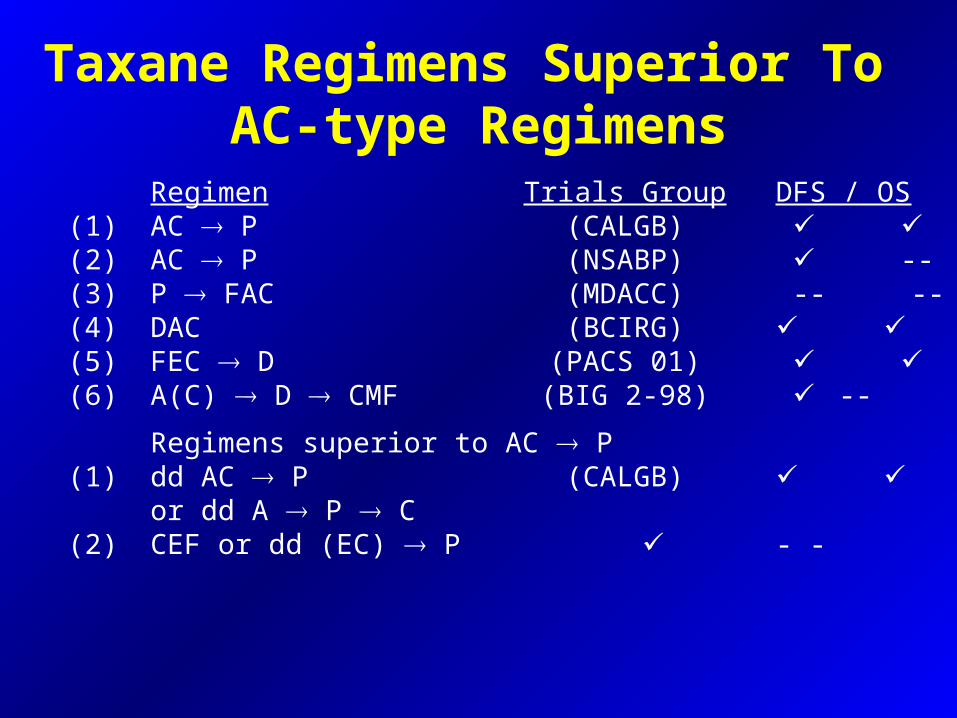
Taxane Regimens Superior To AC-type Regimens
Regimen Trials Group DFS / OS(1) AC P (CALGB) (2) AC P (NSABP) --(3) P FAC (MDACC) -- --(4) DAC (BCIRG) (5) FEC D (PACS 01) (6) A(C) D CMF (BIG 2-98) --
Regimens superior to AC P(1) dd AC P (CALGB)
or dd A P C(2) CEF or dd (EC) P - -
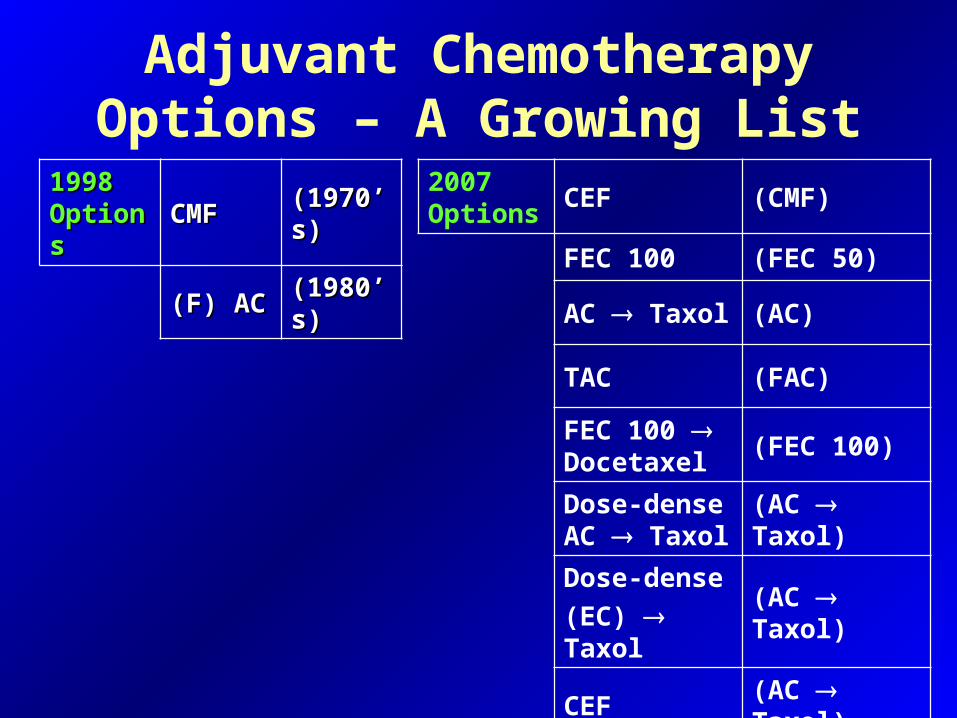
Adjuvant Chemotherapy Options – A Growing List
2007 Options
CEF (CMF)
FEC 100 (FEC 50)
AC Taxol (AC)
TAC (FAC)
FEC 100 Docetaxel
(FEC 100)
Dose-dense AC Taxol
(AC Taxol)
Dose-dense
(EC) Taxol(AC Taxol)
CEF (AC Taxol)
1998 1998 OptionsOptions CMFCMF (1970’s)(1970’s)
(F) AC(F) AC (1980’s)(1980’s)
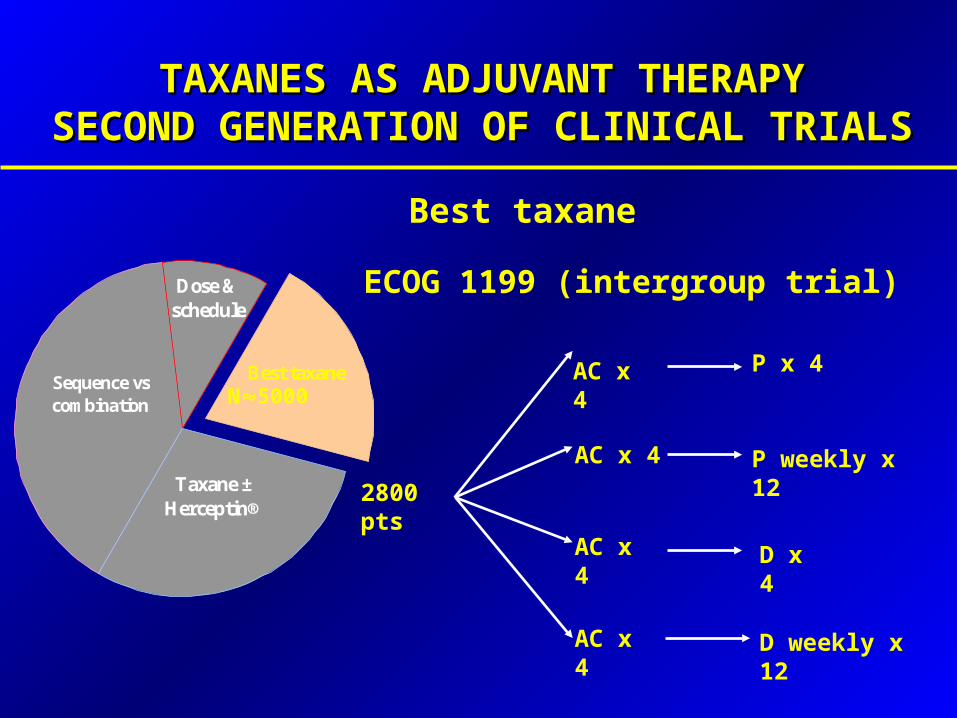
TAXANES AS ADJUVANT THERAPYTAXANES AS ADJUVANT THERAPYSECOND GENERATION OF CLINICAL TRIALSSECOND GENERATION OF CLINICAL TRIALS
Taxane ± Herceptin®
Best taxane
Dose & schedule
Sequence vs combination N5000
Best taxane
ECOG 1199 (intergroup trial)
AC x 4 P x 4
P weekly x 12
D x 4
D weekly x 12
2800 pts
AC x 4
AC x 4
AC x 4

Are There Factors that May Predict Response or Suggest
which Therapy to Use?
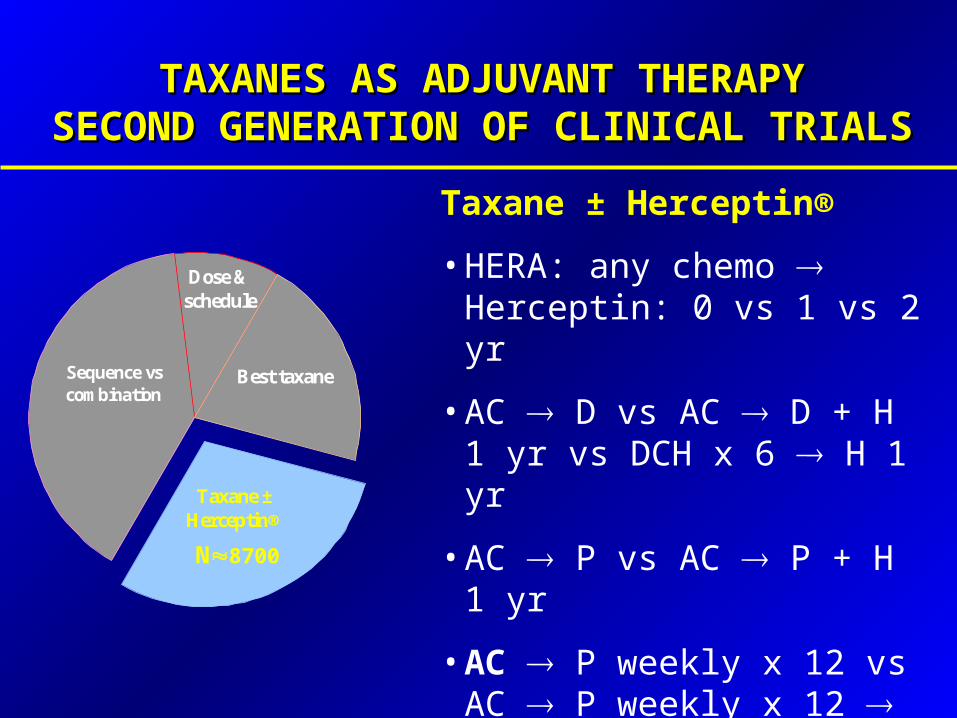
TAXANES AS ADJUVANT THERAPYTAXANES AS ADJUVANT THERAPYSECOND GENERATION OF CLINICAL TRIALSSECOND GENERATION OF CLINICAL TRIALS
Taxane ± Herceptin®
Best taxane
Dose & schedule
Sequence vs combination
N8700
Taxane ± Herceptin®
• HERA: any chemo Herceptin: 0 vs 1 vs 2 yr
• AC D vs AC D + H 1 yr vs DCH x 6 H 1 yr
• AC P vs AC P + H 1 yr
• AC P weekly x 12 vs AC P weekly x 12 H 1 yr vs AC P weekly x 12 + H 1 yr
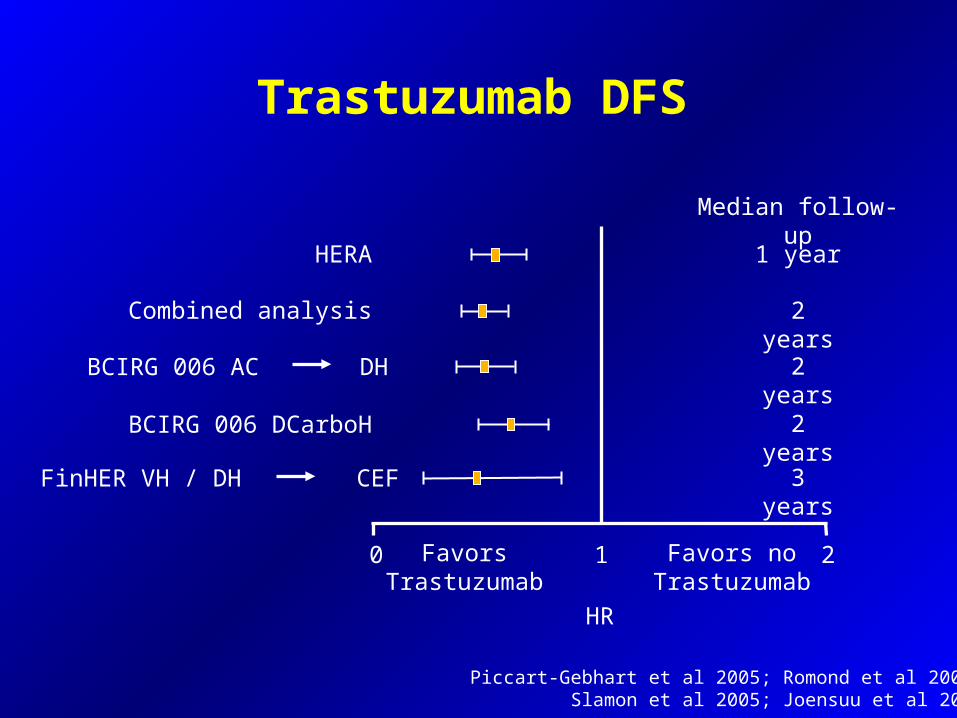
Trastuzumab DFS
Piccart-Gebhart et al 2005; Romond et al 2005;Slamon et al 2005; Joensuu et al 2005
0 1 2
HERA 1 year
Combined analysis 2 years
Median follow-up
FavorsTrastuzumab
Favors noTrastuzumab
HR
BCIRG 006 DCarboH 2 years
2 yearsBCIRG 006 AC DH
FinHER VH / DH CEF 3 years
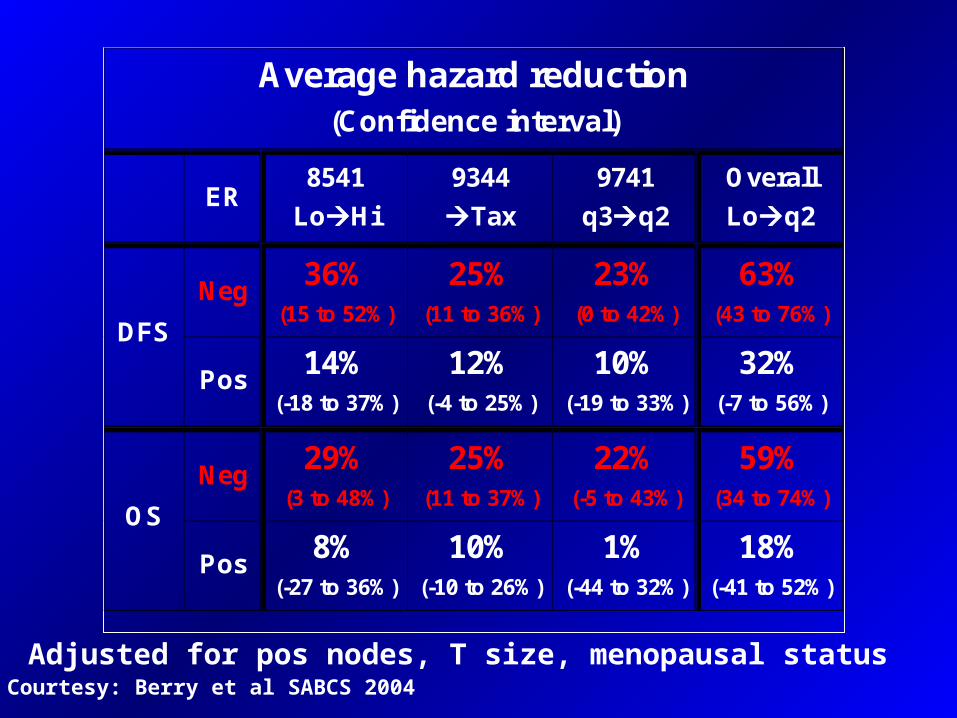
Adjusted for pos nodes, T size, menopausal status
Average hazard reduction (Confidence interval)
ER 8541
LoHi
9344
Tax
9741
q3q2
Overall
Loq2
Neg 36%
(15 to 52%)
25% (11 to 36%)
23% (0 to 42%)
63% (43 to 76%)
DFS
Pos 14%
(-18 to 37%)
12% (-4 to 25%)
10% (-19 to 33%)
32% (-7 to 56%)
Neg 29%
(3 to 48%)
25% (11 to 37%)
22% (-5 to 43%)
59% (34 to 74%)
OS
Pos 8%
(-27 to 36%)
10% (-10 to 26%)
1% (-44 to 32%)
18% (-41 to 52%)
Courtesy: Berry et al SABCS 2004

PACS 01DFS by Age, ITT
Kap
lan-
Mei
er E
stim
ate
Log-rank P-Value = 0.690HR (Cox model) = 0.98 [0.77-1.25]
0.00
0.25
0.50
0.75
1.00
Survival Time (years)
0 1 2 3 4 5 6 7 8
6FEC100
3FEC100-3D
Age < 50 yrs
Log-rank P-Value = 0.001HR (Cox model) = 0.67 [0.51-0.88]
Kap
lan-
Mei
er E
stim
ate
0.00
0.25
0.50
0.75
1.00
Survival Time (years)0 1 2 3 4 5 6 7 8
6FEC100
3FEC100-3D
Age 50 yrs
Multivariate Interaction Test HR: 0.66 [0.46-0.95] P-value = 0.026
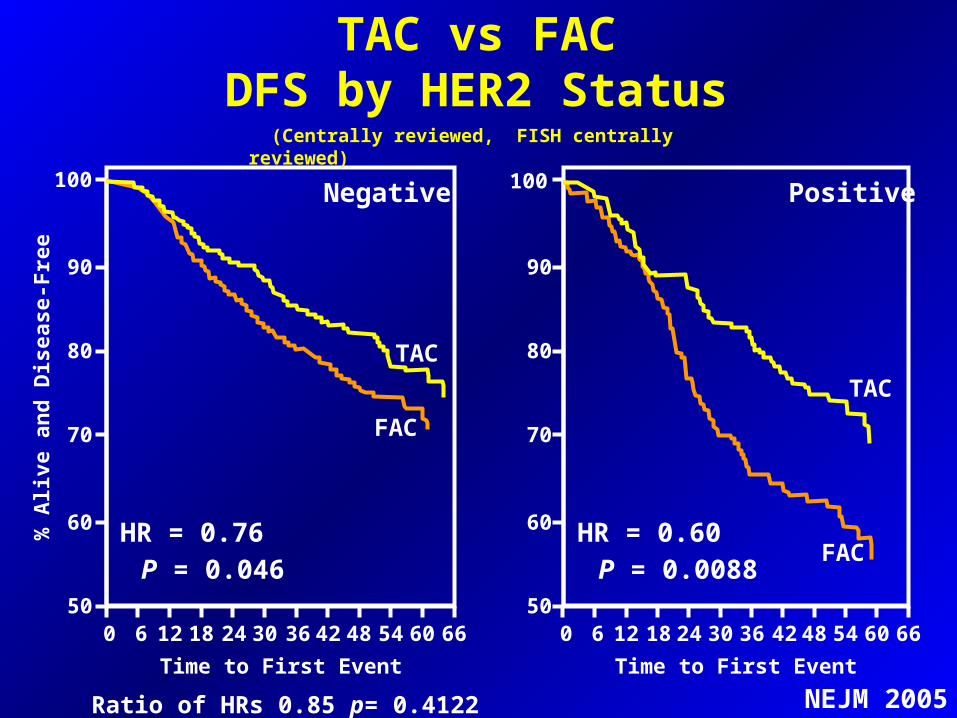
HR = 0.76 P = 0.046
0 6 12182430364248546066
100
90
80
70
60
50
FAC
TAC
Negative
0 6 12182430364248546066
90
80
70
60
50
FAC
TAC
HR = 0.60 P = 0.0088
Positive
Time to First Event
100
TAC vs FACDFS by HER2 Status
Time to First Event
% A
live a
nd
Dis
ease-F
ree
(Centrally reviewed, FISH centrally reviewed)
Ratio of HRs 0.85 p= 0.4122 NEJM 2005

Topoisomerase II
• Topoisomerase II is essential for DNA replication and recombination
• Anthracyclines target topoisomerase II• Increased sensitivity to HER2 due to co-
amplification of TOP2A?

A pooled analysis on the interaction A pooled analysis on the interaction between HER-2 expression and between HER-2 expression and responsiveness of breast cancer responsiveness of breast cancer
to adjuvant chemotherapyto adjuvant chemotherapy
Alessandra Gennari, Maria Pia Sormani, Matteo Puntoni and Paolo Bruzzi
National Cancer Research Institute - Genoa
and University of Genoa - Italy
SABCS 2006

Characteristics of studies - ICharacteristics of studies - I
Study ComparisonHER2 status
determined (%)
NSABP B11 PF vs PAF 638/682 (94%)
NSABP B15 CMF vs AC 2.034/2.295 (89%)
GUN 3 CMF vs CMF/EV 123/220 (56%)
Brussels CMF vs HEC/EC 354/777 (46%)
Milan CMF vs CMF→ A 506/552 (92%)
DBCCG - 89 - D CMF vs FEC 805/980 (82%)
NCIC MA5 CMF vs CEF 628/710 (88%)
SABCS 2006
Total (available/randomised)Total (available/randomised) 5.088/6.216 (82%)5.088/6.216 (82%)
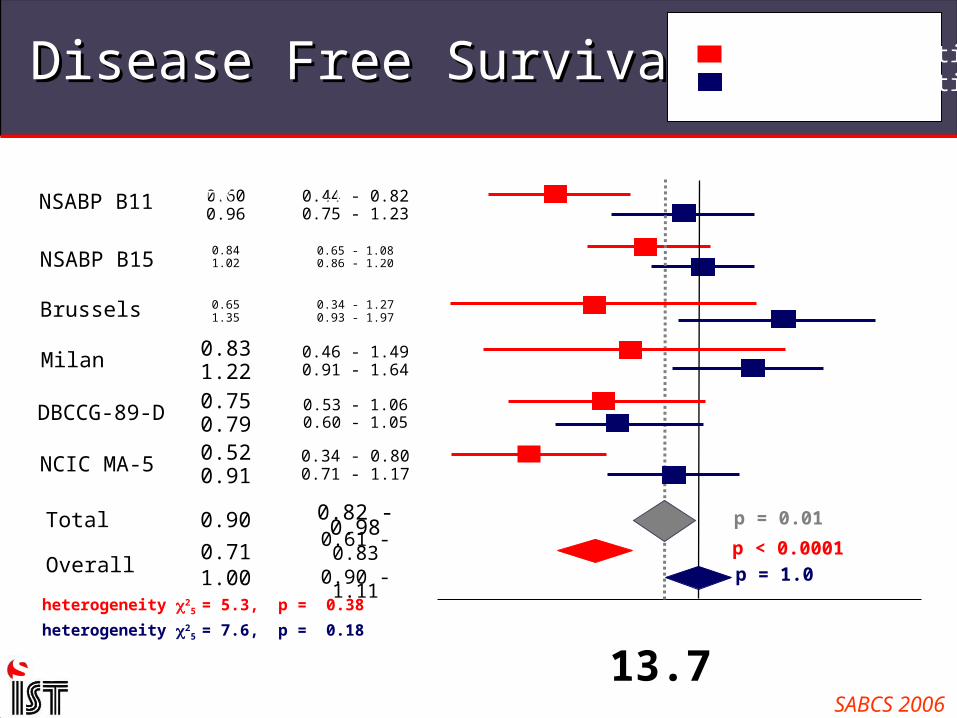
Disease Free SurvivalDisease Free Survival
Test for interaction 2 = 13.7 p < 0.001
non anthra better
0.34 - 0.800.71 - 1.17
0.520.91NCIC MA-5
0.61 - 0.830.90 - 1.11
0.53 - 1.06 0.60 - 1.05
0.46 - 1.490.91 - 1.64
0.65 - 1.080.86 - 1.20
0.44 - 0.820.75 - 1.23
0.711.00
Overall
0.750.79DBCCG-89-D
0.831.22Milan
0.34 - 1.270.93 - 1.97
0.651.35Brussels
NSABP B15
0.600.96
NSABP B11
0.841.02
heterogeneity 25 = 5.3, p = 0.38
heterogeneity 25 = 7.6, p = 0.18
Study HR 95% CI anthra better
0.6 1 2 50.4
p < 0.0001
p = 1.0
0.9
HER2 positive HER2 negative
SABCS 2006
0.82 - 0.980.90Total p = 0.01
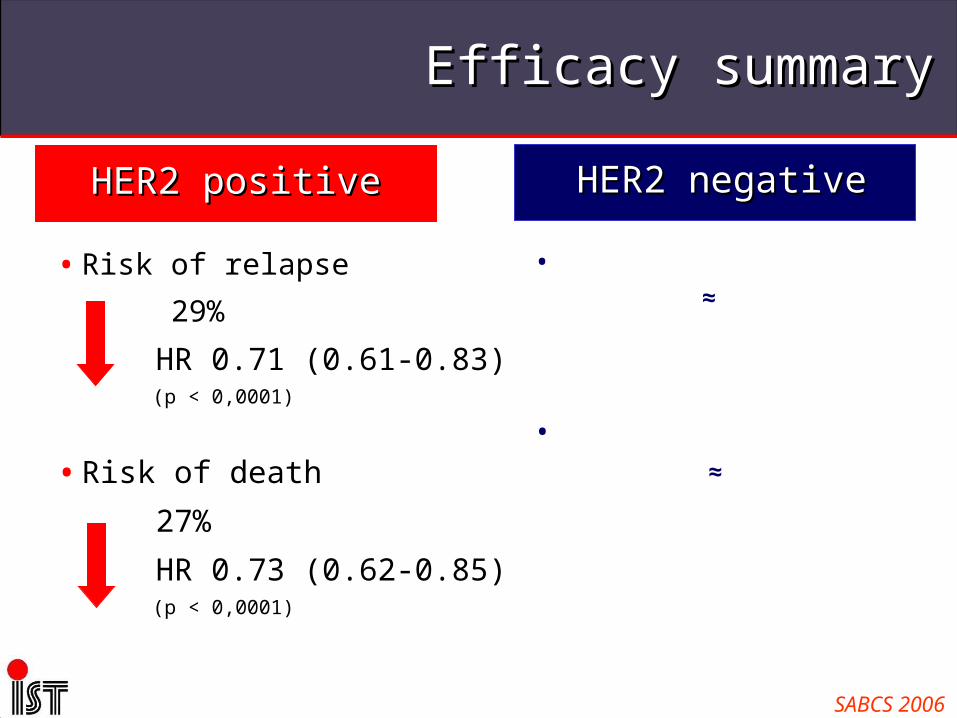
Efficacy summaryEfficacy summary
• Risk of relapse
29%
HR 0.71 (0.61-0.83) (p < 0,0001)
•Risk of death
27%
HR 0.73 (0.62-0.85) (p < 0,0001)
HER2 positiveHER2 positive
• Risk of relapse
anthra ≈ non anthra
HR 1.00 (0.90-1.11) (p = 1,0)
•Risk of death
anthra ≈ non anthra
HR 1.03 (0.92-1.16) (p < 0,86)
HER2 negativeHER2 negative
SABCS 2006

Hierarchy of Chemotherapy Regimens
Appropriate high Appropriate high riskrisk
populationpopulation
Older, no Older, no GCSFGCSF
Younger, Younger,
+ GCSF+ GCSF
Younger,Younger,
+/- GCSF+/- GCSF
Younger, Younger,
+ GCSF+ GCSF
Younger, Younger,
+ GCSF+ GCSF
# of cycles# of cycles 6 cycles6 cycles 10 cycles10 cycles6 cycles6 cycles
(12 visits)(12 visits)8 cycles8 cycles 6 cycles6 cycles
High riskHigh risk FECFECDD dd(EC)dd(EC)PP CEFCEF dd(AC)dd(AC)PP TACTAC
is better thanis better than
Moderate riskModerate risk FEC 100FEC 100CEFCEF
(MA 5)(MA 5)ACACPP
ACACPP
ACACDD
is better thanis better than
Low RiskLow Risk FEC 50FEC 50 CMFCMF ACAC DCDC ADAD
No TherapyNo TherapyP = paclitaxelP = paclitaxel
D = docetaxelD = docetaxel
CAF FAC

The choice of chemotherapy
Depends on the following:
• Tumour characteristics and risk of relapse
• Patient comorbidities
• Patient age
• Social determinants
• Drug availability / costs
• Physician or patient preference

Cost of common regimens
Regimen N+ Study Total Treatment Costs USD
(drug acquisition + incidental + administration)
DAC BCIRG001 $8,226
AC ->P CALGB9344 $4,340
AC->P CALGB9741 $11,741
CE120F MA-5 $4,852
FE100C FASG-5 $3,557
FE100C->D PACS-01 ~ $6,200
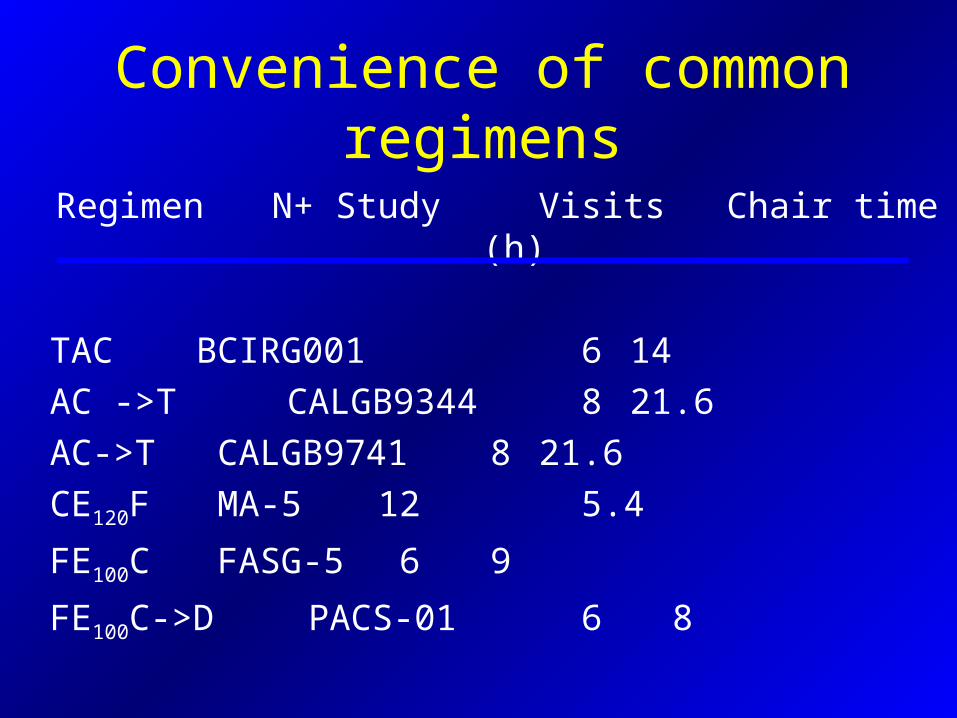
Convenience of common regimens
Regimen N+ Study Visits Chair time (h)
TAC BCIRG001 6 14
AC ->T CALGB9344 8 21.6
AC->T CALGB9741 8 21.6
CE120F MA-5 12 5.4
FE100C FASG-5 6 9
FE100C->D PACS-01 6 8

Adapted by Dr. Maureen E. Trudeau, MD
Where are we going?

Cases
A 68-year old woman presents with an infiltrating duct carcinoma
• 1.2 cm in size
• ER 80% PR 60%
• HER 2 -
• Sentinel node negative
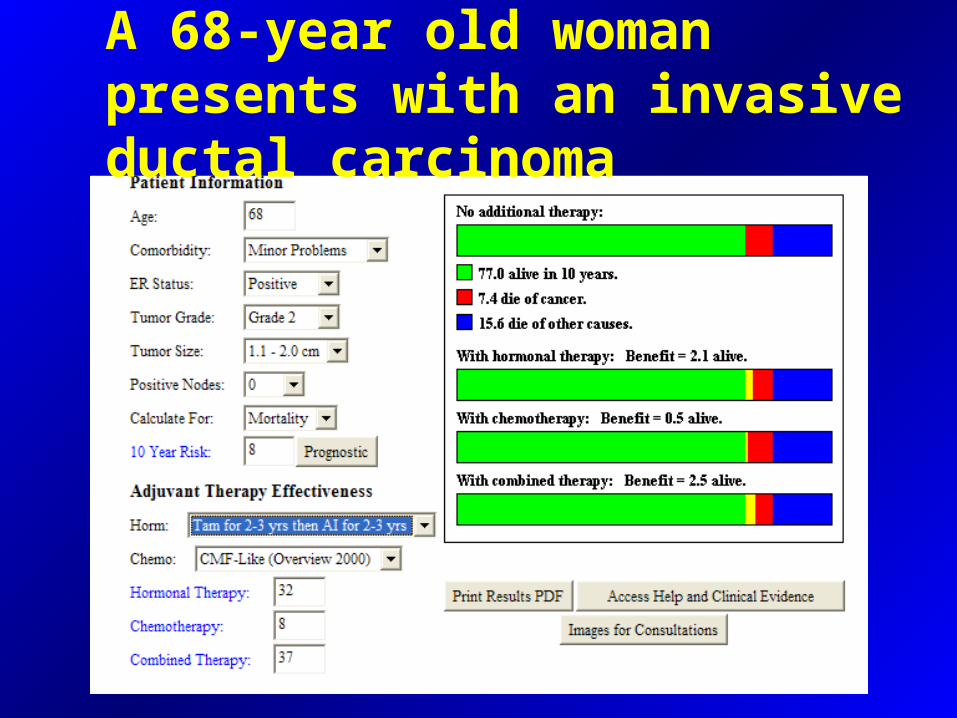
A 68-year old woman presents with an invasive ductal carcinoma

A 59-year old postmenopausal woman with invasive ductal carcinoma
• 1.9 cm in size
• ER 30% PR 0%
• HER 2+ (3+ by IHC)
• Grade 3
• Sentinel node negative

A 59-year old postmenopausal women with invasive ductal carcinoma

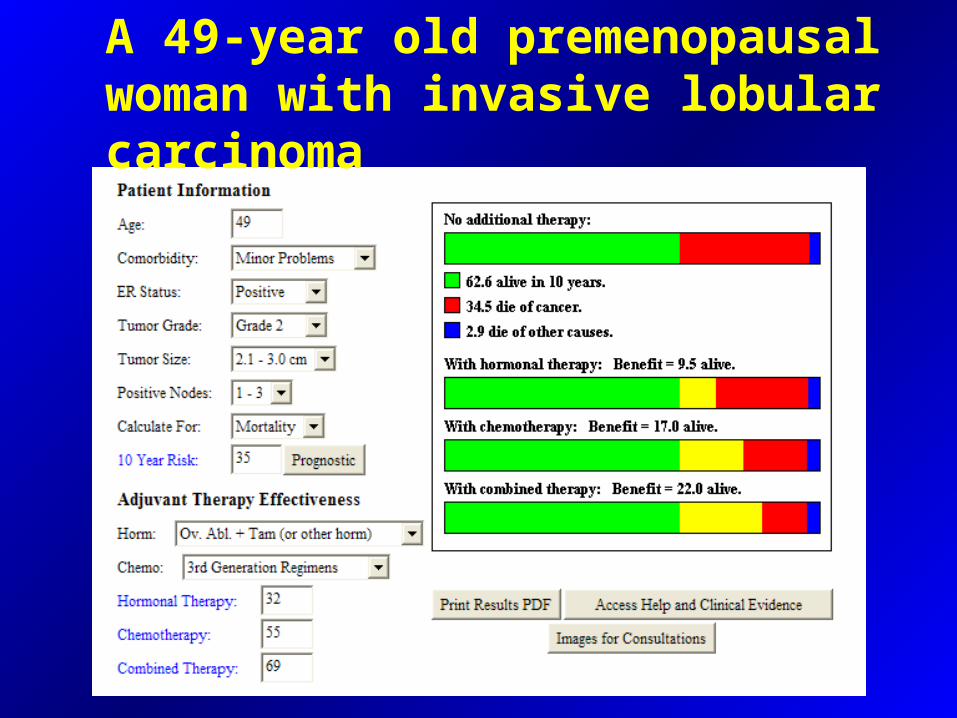
A 49-year old premenopausal woman with invasive lobular carcinoma
• 2.5 cm in size
• ER 70% PR 30%
• HER 2-
• Grade 2
• 2/10 positive lymph nodes
A 49-year old premenopausal woman with invasive lobular carcinoma

A 39-year old premenopausal woman with invasive ductal carcinoma
• 2.8 cm in size
• ER 0% PR 0%
• HER 2 -
• Grade 3
• 5 nodes positive

A 44-year old premenopausal woman with invasive ductal carcinoma
• 2.0 cm in size
• ER 100% PR 100%
• HER 2 -
• Grade 2
• 1/17 nodes positive
• 2 other smaller lesions, grade 1