clinical evaluation of an ultrasound based imaging system for guiding cardiac ablation patrick d....
TRANSCRIPT

CLINICAL EVALUATION OF AN ULTRASOUND BASED IMAGING SYSTEM FOR GUIDING CARDIAC ABLATION
Patrick D. Wolf, Stephanie A. Eyerly, Douglas M. Dumont, Gregg E. Trahey, and Tristram D. Bahnson
Duke UniversityDepartment of Biomedical Engineering
Duke University Medical Center

IntroductionNormal Sinus Rhythm (NSR)
Atrial Fibrillation (AF)
Thousands of cardiac ablation procedures performed daily to treat tachy-arrhythmias
Increase in the number of procedures that are anatomically guided rather than electrically guided
Atrial Fibrillation 3 M now 7 M by 2050

Introduction
Single lesions directly ablate arrhythmogenic tissue AVNRT, WPW, MAT
Lines of lesion isolate regions (pulmonary veins) - AF
Treating Arrhythmias: Transcatheter Cardiac Ablation (TCA)
http://www.heart.org/HEARTORG/Conditions/Arrhythmia/PreventionandTreatmentofArrhythmia/Ablation_UCM_301991_Article.jsp

Introduction
Radiofrequency Ablation (RFA) in TCA procedures Lines of RFA lesions must be transmural and continuous to block conduction Electrical reconnection occurs at unablated gaps Blood flow around catheter tip and tip-tissue contact affect lesion formation
Lesion size not predictable from delivery parameters Real-time image based evaluation would confirm transmurality and line
contiguity
Non-transmural lesionTransmural
lesion
Unablated Gap
RFA Catheter
Transmural lesion
Endocardium
Epicardium
Blood flow

Introduction Radiofrequency Ablation (RFA)
Young’s Modulus of RFA treated tissue
Pernot et al. Mapping Myocardial Elasticity Changes After RF-Ablation Using Supersonic Shear Imaging. Computers in Cardiology. 2009; 36:793-796
In vitro
In vitro In vivo diastole
Un-treated ~ 27 kPa ~ 10 kPa
RF-treated ~ 54 kPa ~ 20-30 kPa
• RF current heats the tissuecreating a discrete and stiff lesion volume

Introduction Acoustic Radiation Force
Impulse (ARFI) Imaging An ultrasound pulse applies radiation
force F [kg/cm2·s2] over a small region at the focus[1]
absorbed power = Wabsorbed, [W/cm3]absorption coefficient = α ~ 0.00072 [Np/cm][2]
speed of sound = c ~ 1540 or 1615±15 [m/s][3]
Temporal average intensity = I [W/cm2]
Radiation force creates μm scale tissue displacements mechanical properties
Ultrasound scan lines spatially and temporally monitor tissue response
RF Lines
Dis
plac
emen
t [μ
m]
t4
TimeARFI! t0 t1 t2 t3
Axial Response
Time (t)[1] Trahey, G.E., et al., Acoustic radiation force impulse imaging of the mechanical properties of arteries: in vivo and ex vivo results. Ultrasound in Medicine & Biology, 2004.
[2] Sagar, K.B., et al., Quantitative ultrasonic assessment of normal and ischaemic myocardium with an acoustic microscope: relationship to integrated backscatter. Cardiovascular research, 1990.
[3] Masugata, H., et al., Relationship between myocardial tissue density measured by microgravimetry and sound speed measured by acoustic microscopy. Ultrasound in Medicine and Biology, 1999.
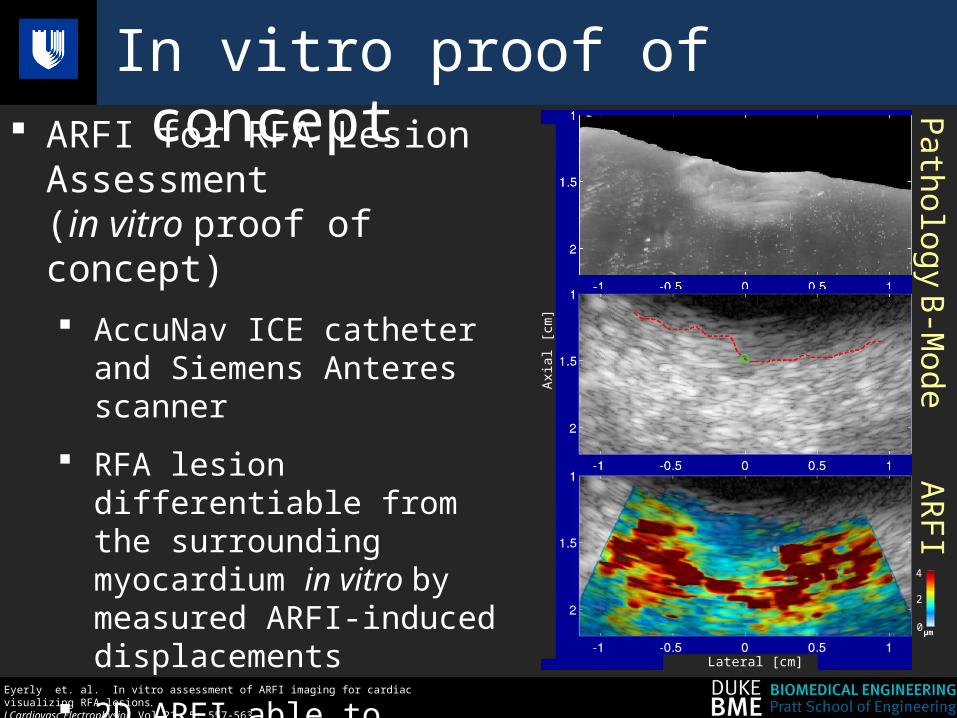
In vitro proof of concept ARFI for RFA Lesion Assessment
(in vitro proof of concept) AccuNav ICE catheter and
Siemens Anteres scanner
RFA lesion differentiable from the surrounding myocardium in vitro by measured ARFI-induced displacements
2D ARFI able to provide lesion assessment
Lateral [cm]
PathologyB-M
odeARFI
4
2
0 μm
Axi
al [c
m]
Eyerly et. al. In vitro assessment of ARFI imaging for cardiac visualizing RFA lesions . J Cardiovasc Electrophysiol. Vol 21, 5: 557-563.

In vivo obstacles Three (3) major obstacles to performing
this imaging in vivo:
1. Heart stiffens and softens during each beat
2. Small ARFI induced displacements must be measured in the presence of substantial gross motion
3. A blind search of the myocardium to find lesions is extremely difficult
Eyerly et. al. In vitro assessment of ARFI imaging for cardiac visualizing RFA lesions . J Cardiovasc Electrophysiol. Vol 21, 5: 557-563.
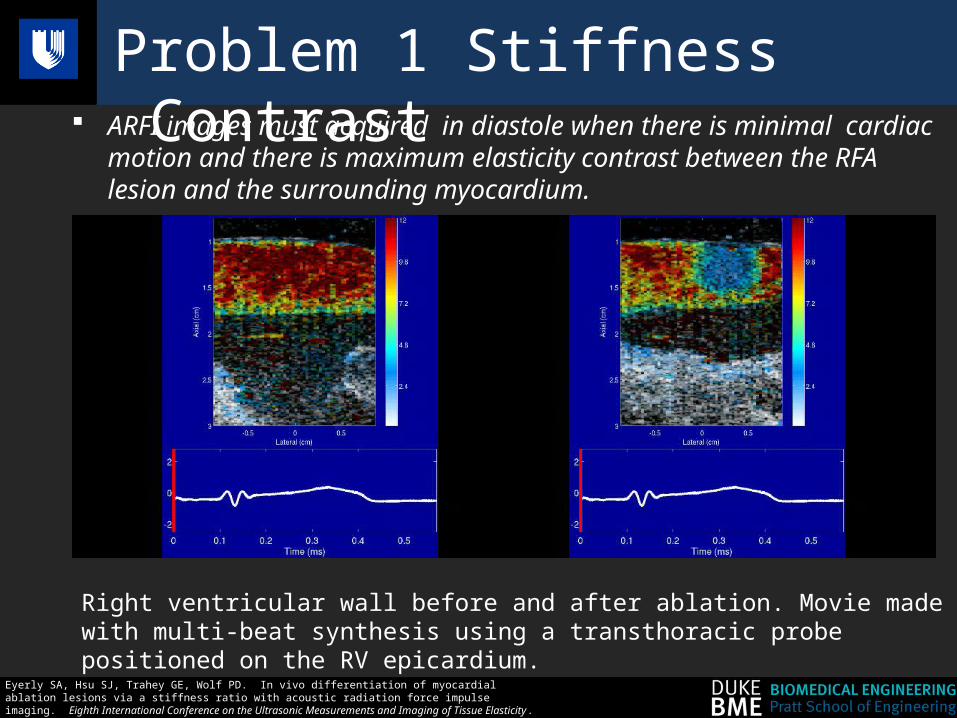
Problem 1 Stiffness Contrast ARFI images must acquired in diastole when there is minimal cardiac
motion and there is maximum elasticity contrast between the RFA lesion and the surrounding myocardium.
Eyerly SA, Hsu SJ, Trahey GE, Wolf PD. In vivo differentiation of myocardial ablation lesions via a stiffness ratio with acoustic radiation force impulse imaging. Eighth International Conference on the Ultrasonic Measurements and Imaging of Tissue Elasticity. Vlissingen, Netherlands: September 2009.
Right ventricular wall before and after ablation. Movie made with multi-beat synthesis using a transthoracic probe positioned on the RV epicardium.
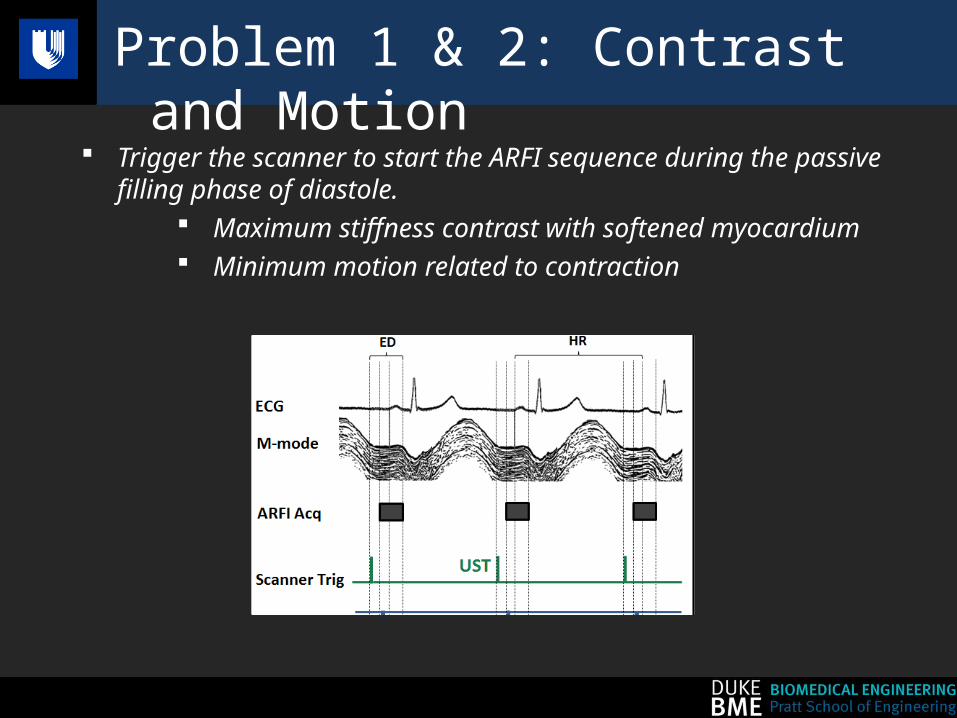
Problem 1 & 2: Contrast and Motion
Trigger the scanner to start the ARFI sequence during the passive filling phase of diastole.
Maximum stiffness contrast with softened myocardium Minimum motion related to contraction

Problem 2: Motion Take multiple scan lines before and after the ARFI ‘push’
Track bulk motion Fit to a quadratic function and interpolate Subtract bulk motion Find ‘Peak Displacement’ Confirm motion filter with ‘zero push’ sequences
Hsu, S., Acoustic Radiation Force Impulse Imaging of Myocardial Performance , in Biomedical Engnieering2009, Duke University.
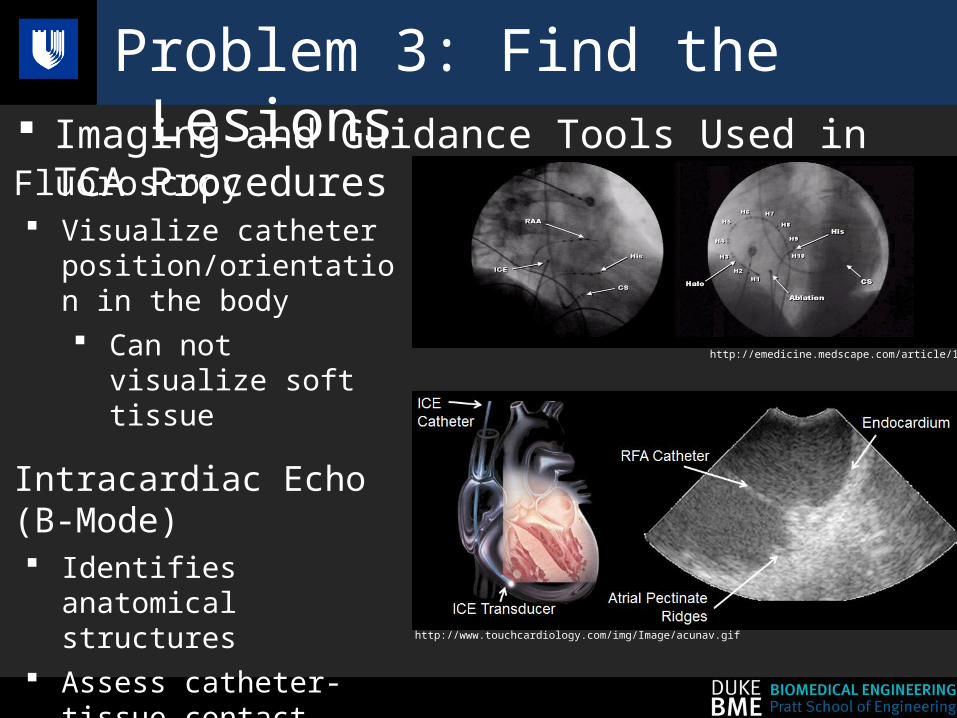
Problem 3: Find the Lesions Imaging and Guidance Tools Used in TCA Procedures
Fluoroscopy Visualize catheter
position/orientation in the body Can not visualize soft
tissue
Intracardiac Echo (B-Mode) Identifies anatomical
structures Assess catheter-tissue
contact Can not differentiate lesion
from normal tissue
http://emedicine.medscape.com/article/151907-overview
http://www.touchcardiology.com/img/Image/acunav.gif

Find the Lesions
Electroanatomical Mapping (EAM): CARTO (Biosense/Webster) Magnetic fields determine the 3D location of catheters
NaviStar™ mapping/ablation catheter: contains a location coil that measures magnetic field strength
All points plotted relative to a reference patch on the patient’s back
Real-time guidance for TCA procedures
http://www.ipej.org/0801/bhakta.htm http://www.pages.drexel.edu/~gn52/MEDICAL_ROBOTICS/Downloads_files/Carto%20XP%20EP%20Navigation%20System.pdf
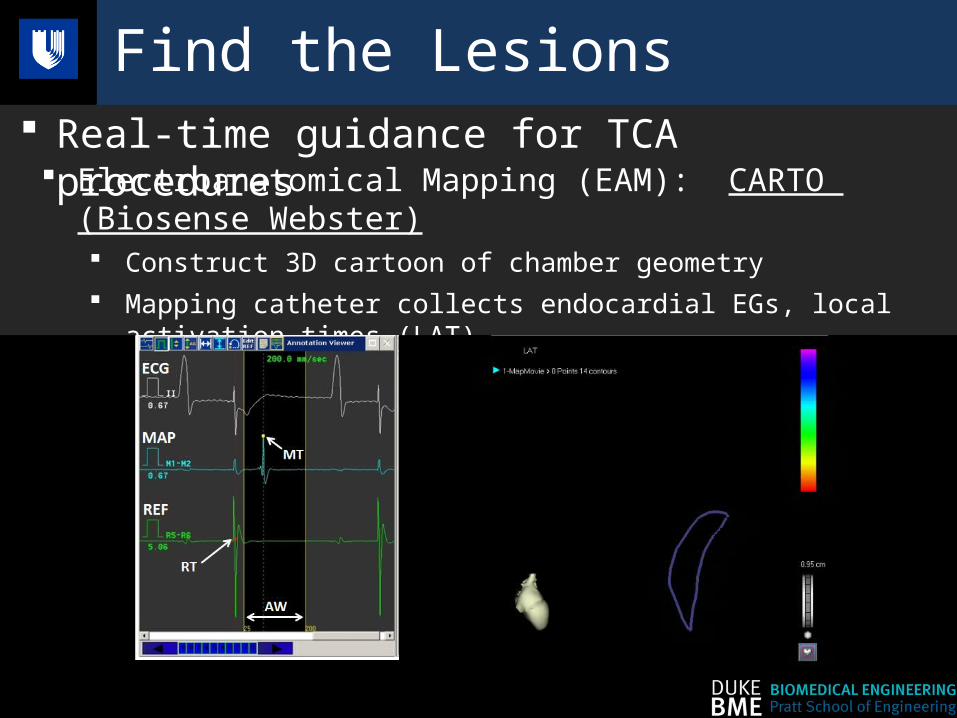
Find the Lesions
Electroanatomical Mapping (EAM): CARTO (Biosense Webster) Construct 3D cartoon of chamber geometry Mapping catheter collects endocardial EGs, local activation times (LAT) Visualization of electrical propagation, identifies arrhythmogenic regions
Real-time guidance for TCA procedures
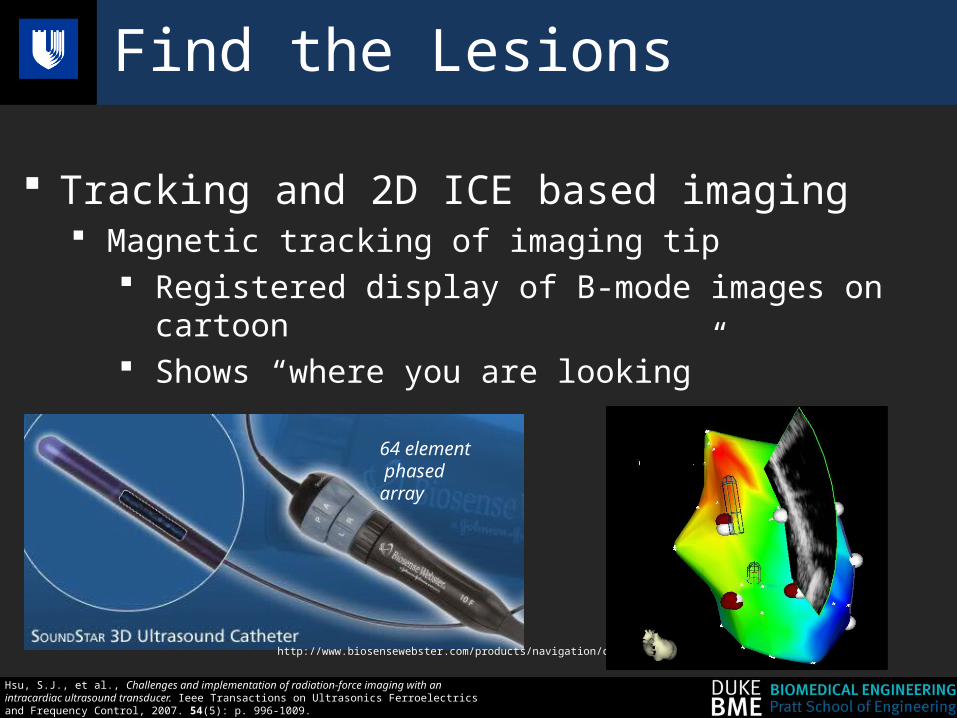
Find the Lesions
Tracking and 2D ICE based imaging Magnetic tracking of imaging tip
Registered display of B-mode images on cartoon Shows “where you are looking”
64 element phased array
http://www.biosensewebster.com/products/navigation/cartosound.aspx
Hsu, S.J., et al., Challenges and implementation of radiation-force imaging with an intracardiac ultrasound transducer. Ieee Transactions on Ultrasonics Ferroelectrics and Frequency Control, 2007. 54(5): p. 996-1009.

In vivo testing
Paced from coronary sinus catheter
Mapped electrical activation using CARTO ARFI imaged normal tissue
Created a lesion line with ≈1 cm gap ARFI imaged line and gap
Closed the gap ARFI imaged line Poster by Eyerly
Right atrium mapped using CARTO EAM system No
Lesion
Lesion with Gap
Gap Closed

Normal and Gap Images
RFA Lesion Gap
RFA Lesion
Gap

Linear RFA ARFI image lesion assessments correlate with electrical block in CARTO LAT maps
In vivo Results
CARTO LAT Maps
TA
81ms
24ms
TA
RFA LesionGap at TA
ContinuousRFA Lesion
RFA Lesion
86.44.8
1.63.2
0μm

Moving to the Clinic - ARFIi Clinical Tool
Research Tool
Acquire ECG synchronous ARFI data on S2000 scanner
Download data to laptop
Calculate and display ARFI displacements on laptop screen
Clinical Tool
Acquire ECG synchronous ARFI data on S2000 scanner
Process and display ARFI data on S2000 screen
Done by Duke in collaboration with Siemens Medical

Moving to the Clinic – FDA Considerations
Mechanical Index (MI)
FDA limit 1.9
Measured peak for our sequences <1.6
Face Heating
FDA limit < 6 °C in standing water
Siemens internal limit <2 °C
Measured change for our sequences <2 °C

Moving to the Clinic Clinically, we seek to understand
• The elasticity contrast for lesions in senescent and diseased hearts
• The ability to access all lesions in both the right and left atria with a limited field of view
• The effect of atrial fibrillation on ARFIi contrast
• The correlation of ARFIi evaluation with electrical outcome in atrial flutter and atrial fibrillation ablation procedures
Clinical Study Outline Patients undergoing AFl ablation or AF ablation
Following each round of ablation in the normal therapeutic procedure image normal and lesioned tissue with ARFI
blinded results to the physician
Characterize “normal” and ablated tissue
In sinus rhythm
In AF

ARFI imaging of ablation lesions can be implemented clinically with significant but minor modifications to existing equipment commonly used in the EP lab (CARTO, ICE).
Lesion boundary correlates with ARFI imaged stiffness boundary
Electrical block correlates with ARFIi determined contiguous and transmural lesions
The tools for clinical evaluation have been created
Summary
Thank you to Dr. Kapur et al for organizing workshop
NIH Grant: R21-EB-007741NIH Grant: R01-EB-012384
Biosense Webster and Siemens Medical Solutions USA, Inc. for their hardware and system support
Acknowledgements