clinical evidence of onyx for the treatment of€¦ · onyx in peripheral avm •22 pats., 25...
TRANSCRIPT
Clinical evidence of Onyx for the treatment of
endoleakages and AVM‘s
LINC 2019
Leipzig, Germany, 24. January 2019
Walter A. Wohlgemuth
University Clinic and Policlinic of Radiology
Martin-Luther University Halle-Wittenberg, Germany

Conflicts of interest
Scientific grants:Siemens, Phillips, ab medica, ev3/covidien/medtronic, itm Flowmedical, Toshiba, Cook, W. L. Gore
Lectures: ev3/covidien/medtronic, Biotronic, St Jude Medical, Abbott, Siemens, ab medica, Boston Scientific, itm Flowmedical, Terumo, W. L. Gore
Consulting:1st WITiG, itm Flowmedical, Siemens, ev3/covidien/medtronic, ab medica
Proctoring:W. L. Gore, ev3/covidien/medtronic, ab medica
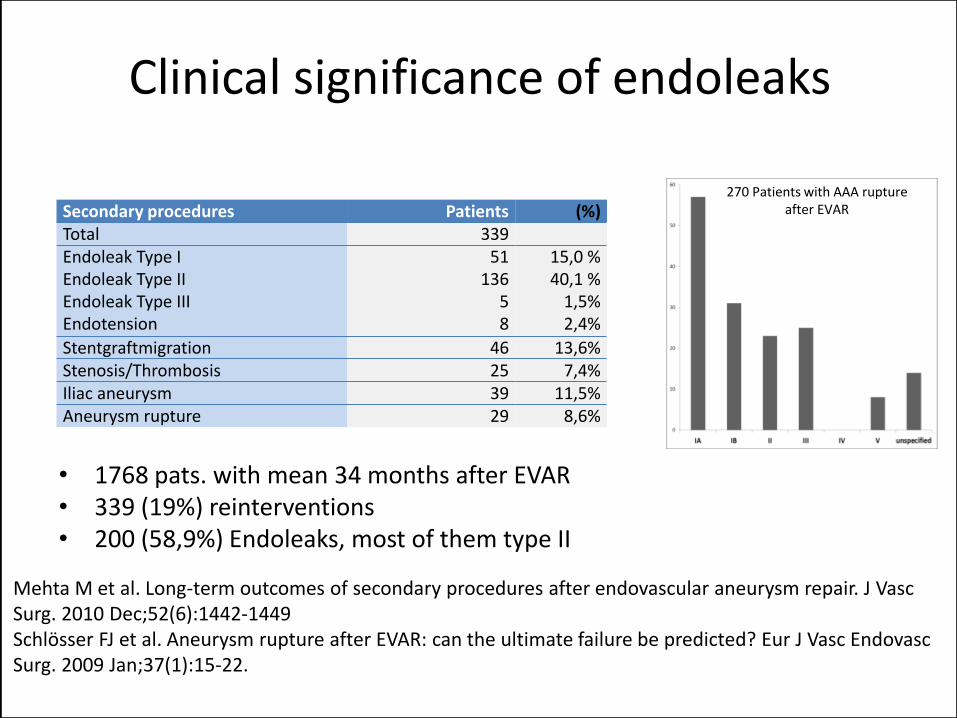
Clinical significance of endoleaks
Secondary procedures Patients (%)Total 339Endoleak Type IEndoleak Type IIEndoleak Type IIIEndotension
51136
58
15,0 %40,1 %
1,5%2,4%
Stentgraftmigration 46 13,6%Stenosis/Thrombosis 25 7,4%Iliac aneurysm 39 11,5%Aneurysm rupture 29 8,6%
Mehta M et al. Long-term outcomes of secondary procedures after endovascular aneurysm repair. J VascSurg. 2010 Dec;52(6):1442-1449Schlösser FJ et al. Aneurysm rupture after EVAR: can the ultimate failure be predicted? Eur J Vasc EndovascSurg. 2009 Jan;37(1):15-22.
• 1768 pats. with mean 34 months after EVAR • 339 (19%) reinterventions• 200 (58,9%) Endoleaks, most of them type II
270 Patients with AAA ruptureafter EVAR
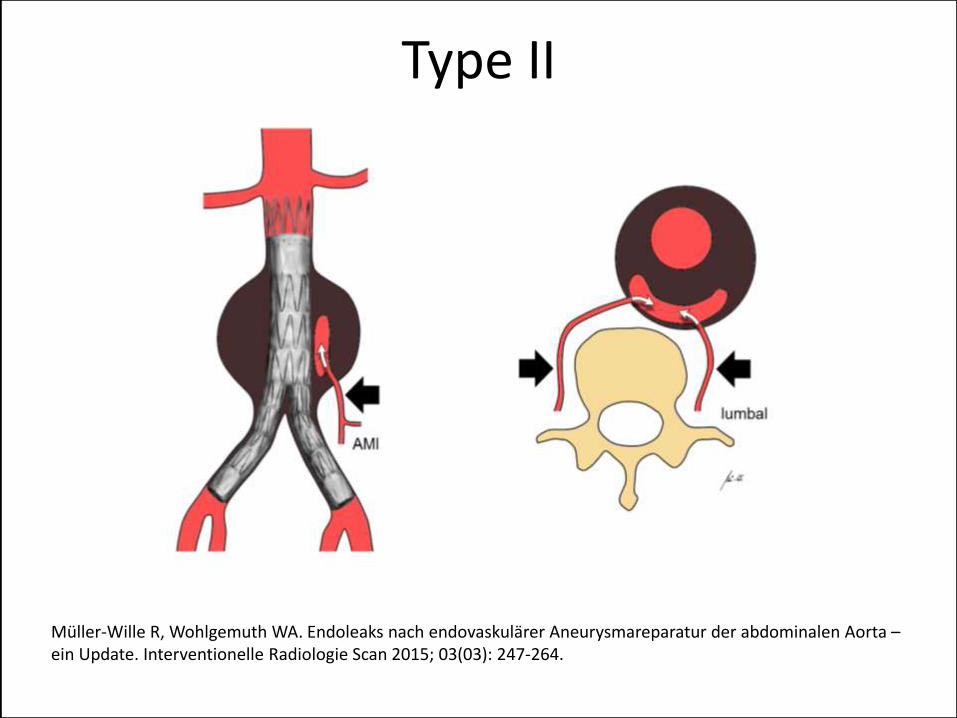
Type II
Müller-Wille R, Wohlgemuth WA. Endoleaks nach endovaskulärer Aneurysmareparatur der abdominalen Aorta –ein Update. Interventionelle Radiologie Scan 2015; 03(03): 247-264.
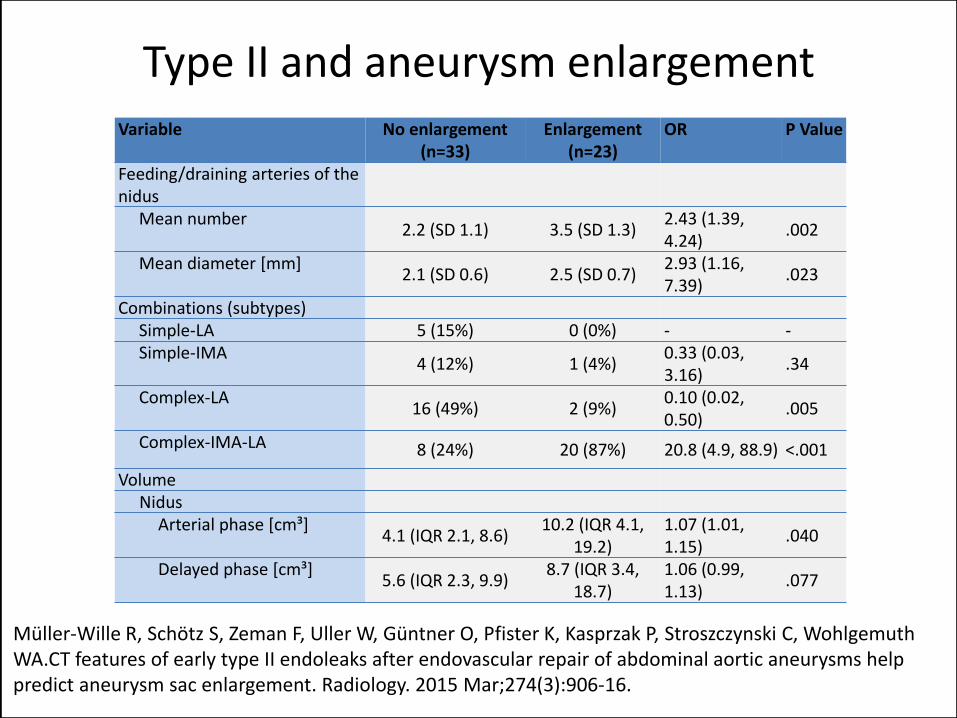
Variable No enlargement (n=33)
Enlargement (n=23)
OR P Value
Feeding/draining arteries of the nidus
Mean number2.2 (SD 1.1) 3.5 (SD 1.3)
2.43 (1.39, 4.24)
.002
Mean diameter [mm]2.1 (SD 0.6) 2.5 (SD 0.7)
2.93 (1.16, 7.39)
.023
Combinations (subtypes)Simple-LA 5 (15%) 0 (0%) - -Simple-IMA
4 (12%) 1 (4%)0.33 (0.03, 3.16)
.34
Complex-LA16 (49%) 2 (9%)
0.10 (0.02, 0.50)
.005
Complex-IMA-LA 8 (24%) 20 (87%) 20.8 (4.9, 88.9) <.001
Volume Nidus
Arterial phase [cm³]4.1 (IQR 2.1, 8.6)
10.2 (IQR 4.1, 19.2)
1.07 (1.01, 1.15)
.040
Delayed phase [cm³]5.6 (IQR 2.3, 9.9)
8.7 (IQR 3.4, 18.7)
1.06 (0.99, 1.13)
.077
Müller-Wille R, Schötz S, Zeman F, Uller W, Güntner O, Pfister K, Kasprzak P, Stroszczynski C, Wohlgemuth WA.CT features of early type II endoleaks after endovascular repair of abdominal aortic aneurysms helppredict aneurysm sac enlargement. Radiology. 2015 Mar;274(3):906-16.
Type II and aneurysm enlargement
0,57 mm
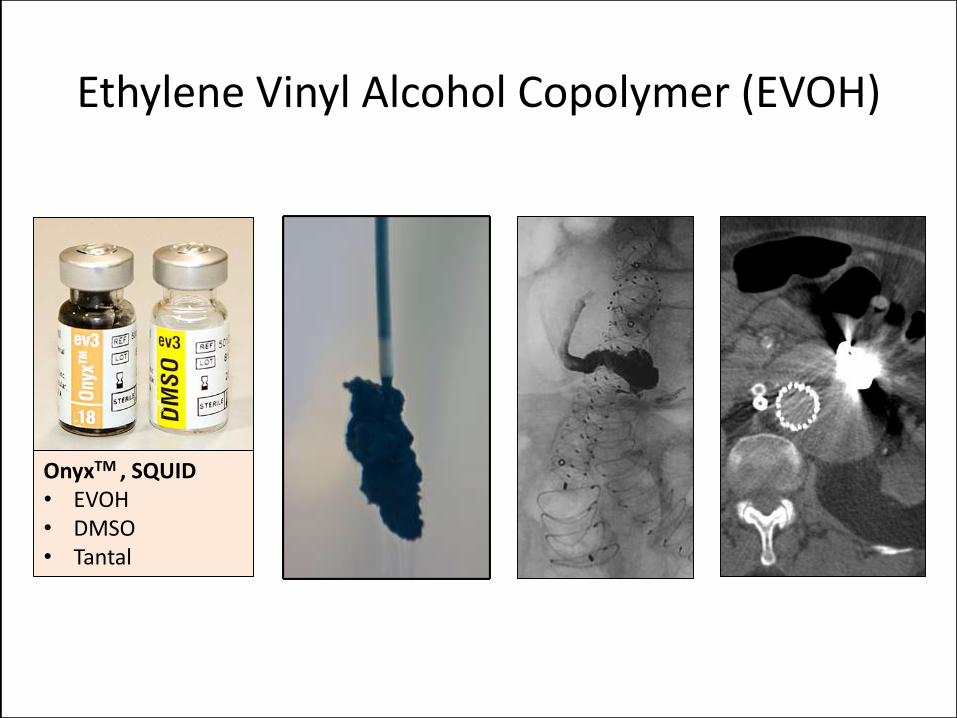
Ethylene Vinyl Alcohol Copolymer (EVOH)
OnyxTM , SQUID• EVOH• DMSO• Tantal
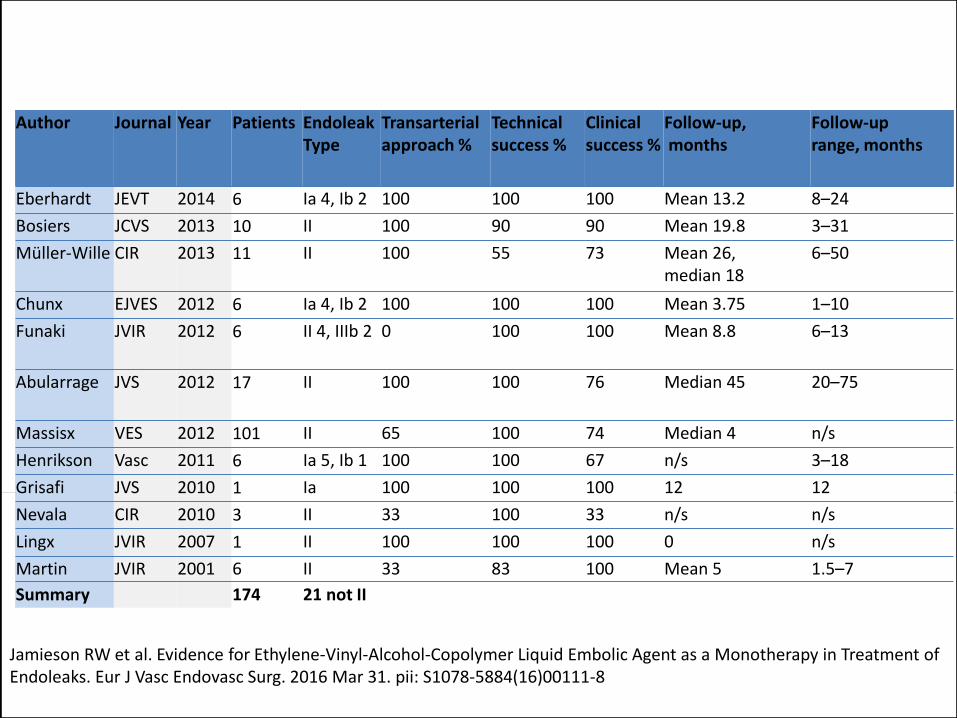
Jamieson RW et al. Evidence for Ethylene-Vinyl-Alcohol-Copolymer Liquid Embolic Agent as a Monotherapy in Treatment of Endoleaks. Eur J Vasc Endovasc Surg. 2016 Mar 31. pii: S1078-5884(16)00111-8
Author Journal Year Patients Endoleak Type
Transarterialapproach %
Technical success %
Clinical success %
Follow-up, months
Follow-uprange, months
Eberhardt JEVT 2014 6 Ia 4, Ib 2 100 100 100 Mean 13.2 8–24
Bosiers JCVS 2013 10 II 100 90 90 Mean 19.8 3–31
Müller-Wille CIR 2013 11 II 100 55 73 Mean 26, median 18
6–50
Chunx EJVES 2012 6 Ia 4, Ib 2 100 100 100 Mean 3.75 1–10
Funaki JVIR 2012 6 II 4, IIIb 2 0 100 100 Mean 8.8 6–13
Abularrage JVS 2012 17 II 100 100 76 Median 45 20–75
Massisx VES 2012 101 II 65 100 74 Median 4 n/s
Henrikson Vasc 2011 6 Ia 5, Ib 1 100 100 67 n/s 3–18
Grisafi JVS 2010 1 Ia 100 100 100 12 12
Nevala CIR 2010 3 II 33 100 33 n/s n/s
Lingx JVIR 2007 1 II 100 100 100 0 n/s
Martin JVIR 2001 6 II 33 83 100 Mean 5 1.5–7
Summary 174 21 not II
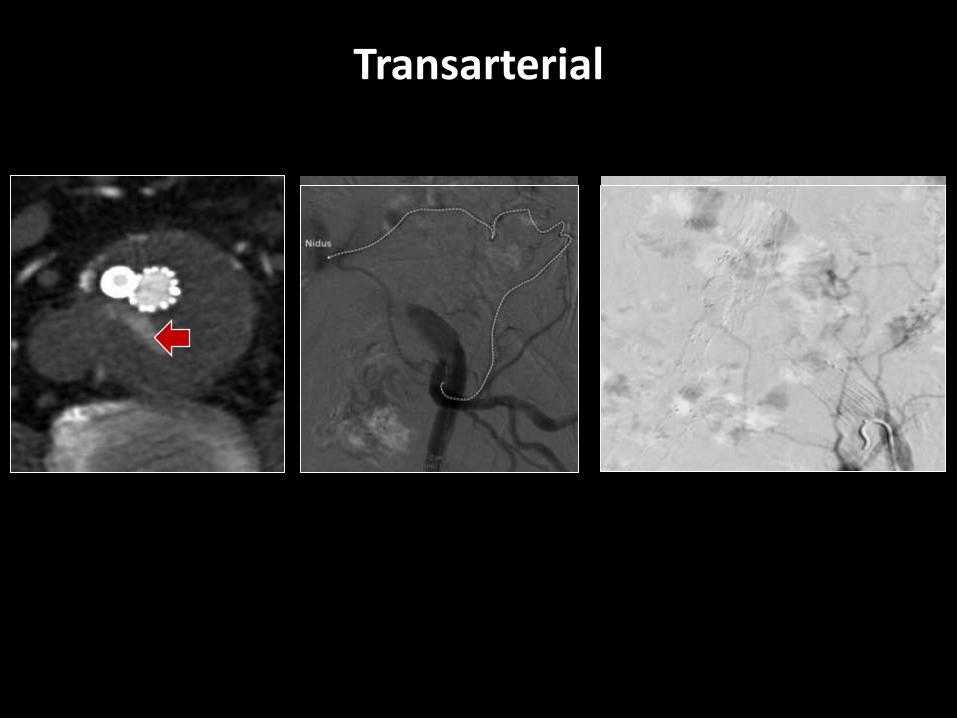
Transarterial
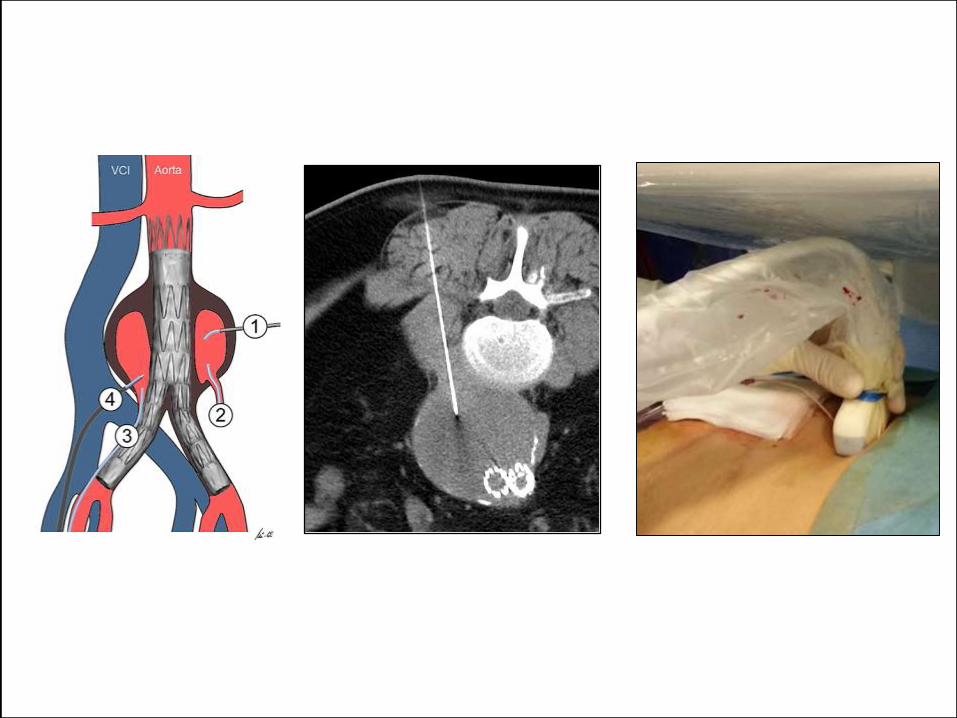
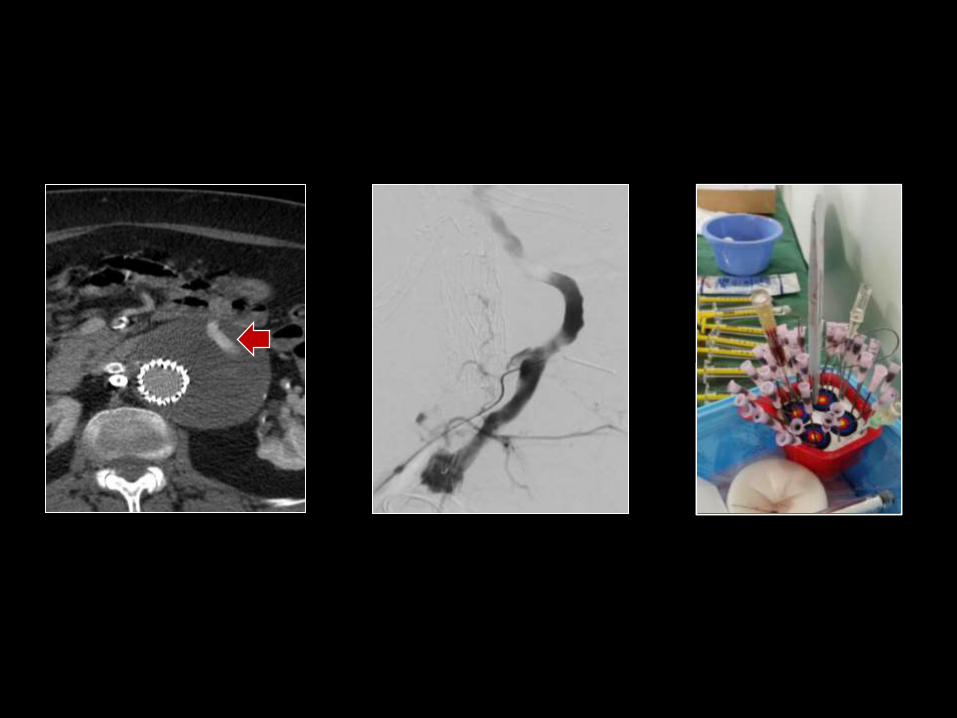
Direct puncture of endoleak
• 30 type II endoleak pats., retrospective
• Cyanoacrylate glue only (45.5%), glue/coils (36.4%), and Onyx with or without glue/coils (18.1%)
• Technical success 29/30 pats.
• Freedom of aneurysm growth in 85.2%
• Complication rate 9.1% (3/33) – 1 case of nontarget embolization with transient
neuropraxia and 2 self-limiting rectus sheath hematomas
Zener R, Oreopoulos G, Beecroft R, Rajan DK, Jaskolka J, Tan KT. Transabdominal Direct Sac PunctureEmbolization of Type II Endoleaks after Endovascular Abdominal Aortic Aneurysm Repair. J Vasc Interv Radiol. 2018 Aug;29(8):1167-1173
Onyx in type IA endoleaks
• 4 pats. with previous cuff, 1 pat. directly
• 4 x transfemoral, 1 case transfemoral failed direct puncture– Onyx, glue, coils in 3 pats.
– Onyx + glue 1 pat.
– Onyx + coil 1 pat
• Technical success 5/5
• No non-target embolization
• 4 pats. Stable, 1 decrease of aneurysm size
Ierardi AM, Franchin M, Fontana F, Piffaretti G, Crippa M, Angileri SA, Magenta Biasina A, Piacentino F, Tozzi M, Pinto A, Carrafiello G. The role of ethylene-vinyl alcohol copolymer in association with other embolic agents forthe percutaneous and endovascular treatment of type Ia endoleak. Radiol Med. 2018 Aug;123(8):638-642
Onyx in type IA endoleaks after chimney
• 9 pats. with chimney EVAR
• Onyx only, transarterial
• Technical success 9/9, no complications
• Follow-up 16 months
• Primary clinical efficacy 8/9 patients (89%)
• Primary technical efficacy for 6/9 patients (67%)
Marcelin C, Le Bras Y, Petitpierre F, Midy D, Grenier N, Ducasse E, Cornélis F. Embolization for persistent type IA endoleaks after chimney endovascular aneurysm repair with Onyx®. Diagn Interv Imaging. 2017 Dec;98(12):849-855
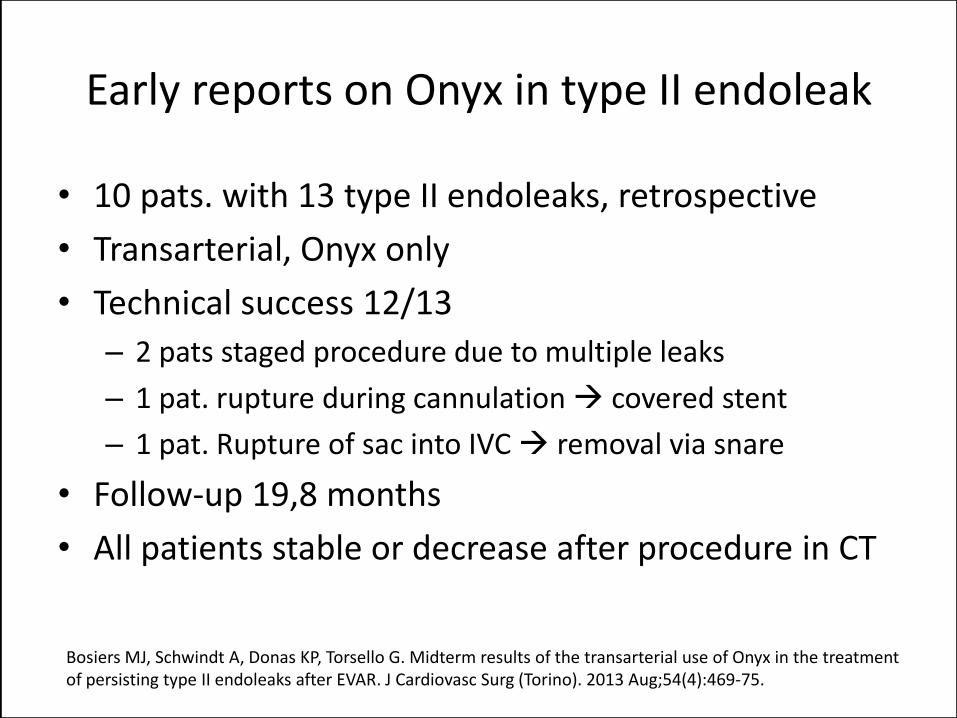
Early reports on Onyx in type II endoleak
• 10 pats. with 13 type II endoleaks, retrospective
• Transarterial, Onyx only
• Technical success 12/13
– 2 pats staged procedure due to multiple leaks
– 1 pat. rupture during cannulation covered stent
– 1 pat. Rupture of sac into IVC removal via snare
• Follow-up 19,8 months
• All patients stable or decrease after procedure in CT
Bosiers MJ, Schwindt A, Donas KP, Torsello G. Midterm results of the transarterial use of Onyx in the treatmentof persisting type II endoleaks after EVAR. J Cardiovasc Surg (Torino). 2013 Aug;54(4):469-75.
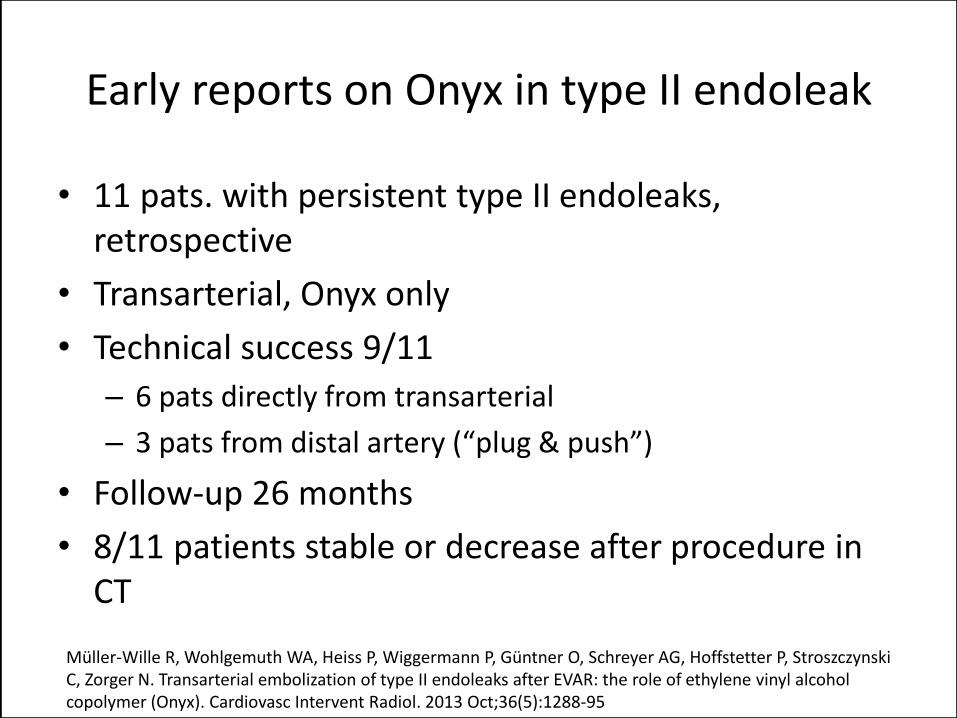
Early reports on Onyx in type II endoleak
• 11 pats. with persistent type II endoleaks, retrospective
• Transarterial, Onyx only
• Technical success 9/11
– 6 pats directly from transarterial
– 3 pats from distal artery (“plug & push”)
• Follow-up 26 months
• 8/11 patients stable or decrease after procedure in CT
Müller-Wille R, Wohlgemuth WA, Heiss P, Wiggermann P, Güntner O, Schreyer AG, Hoffstetter P, Stroszczynski C, Zorger N. Transarterial embolization of type II endoleaks after EVAR: the role of ethylene vinyl alcoholcopolymer (Onyx). Cardiovasc Intervent Radiol. 2013 Oct;36(5):1288-95
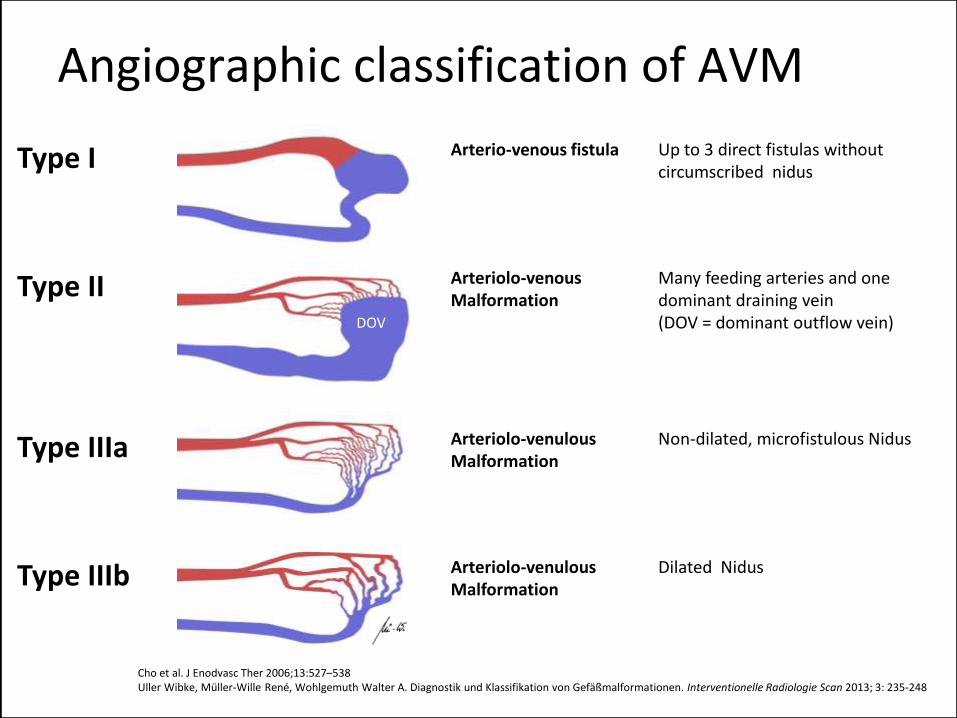
Angiographic classification of AVM
Type I Arterio-venous fistula Up to 3 direct fistulas withoutcircumscribed nidus
Type II Arteriolo-venousMalformation
Many feeding arteries and onedominant draining vein(DOV = dominant outflow vein)
Type IIIa Arteriolo-venulousMalformation
Non-dilated, microfistulous Nidus
Type IIIb Arteriolo-venulousMalformation
Dilated Nidus
DOV
Cho et al. J Enodvasc Ther 2006;13:527–538 Uller Wibke, Müller-Wille René, Wohlgemuth Walter A. Diagnostik und Klassifikation von Gefäßmalformationen. Interventionelle Radiologie Scan 2013; 3: 235-248
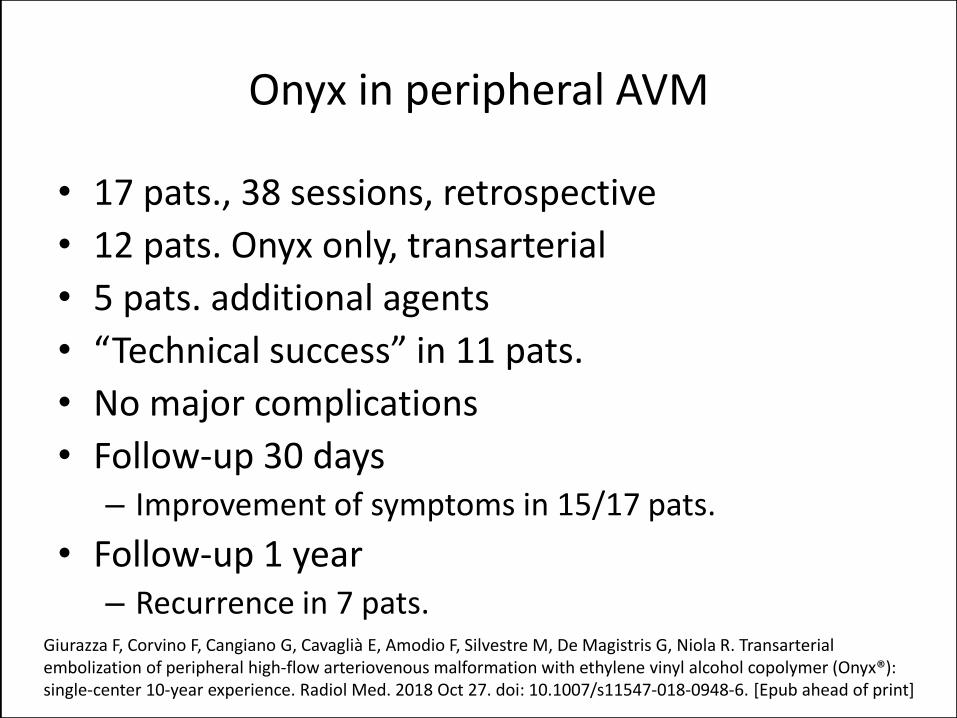
Onyx in peripheral AVM
• 17 pats., 38 sessions, retrospective
• 12 pats. Onyx only, transarterial
• 5 pats. additional agents
• “Technical success” in 11 pats.
• No major complications
• Follow-up 30 days– Improvement of symptoms in 15/17 pats.
• Follow-up 1 year– Recurrence in 7 pats.
Giurazza F, Corvino F, Cangiano G, Cavaglià E, Amodio F, Silvestre M, De Magistris G, Niola R. Transarterialembolization of peripheral high-flow arteriovenous malformation with ethylene vinyl alcohol copolymer (Onyx®): single-center 10-year experience. Radiol Med. 2018 Oct 27. doi: 10.1007/s11547-018-0948-6. [Epub ahead of print]
Onyx in peripheral AVM
• 19 pats., 28 sessions, retrospective• 13 pats. Onyx only, 12 transarterial, 1 direct• Complete devascularization in 12 pats.
– Surgical excision in 9 pats.
• Complications: 1 stroke, 1 microcatheter rupture, 1 pain + bradycardia (selflimiting)
• Follow-up 10 – 34 months– 2 patients with persisting symptoms– 1 pat. Lost to follow-up– Symptom free 16/19 pats.
Saeed Kilani M, Lepennec V, Petit P, Magalon G, Casanova D, Bartoli JM, Vidal V. Embolization of peripheralhigh-flow arteriovenous malformations with Onyx. Diagn Interv Imaging. 2017 Mar;98(3):217-226
Onyx in peripheral AVM
• 22 pats., 25 sessions, retrospective
• Onxy only or Onyx + other adjuncts (41%), transarterial
• Complete devascularization in 8 pats. (36%)
– Rest: “near-complete devascularization”
• Major complications in 2 pats.
• Symptom improvement in 18 pats. (82%)
• During follow-up recurrence in 7 pats.
De Beule T, Vranckx J, Verhamme P, Labarque V, Morren MA, Fourneau I, Maleux G. Transarterial embolizationof peripheral arteriovenous malformations with ethylenevinyl alcohol copolymer - feasibility, technicaloutcomes, and clinical outcomes. Vasa. 2016 Nov;45(6):497-504
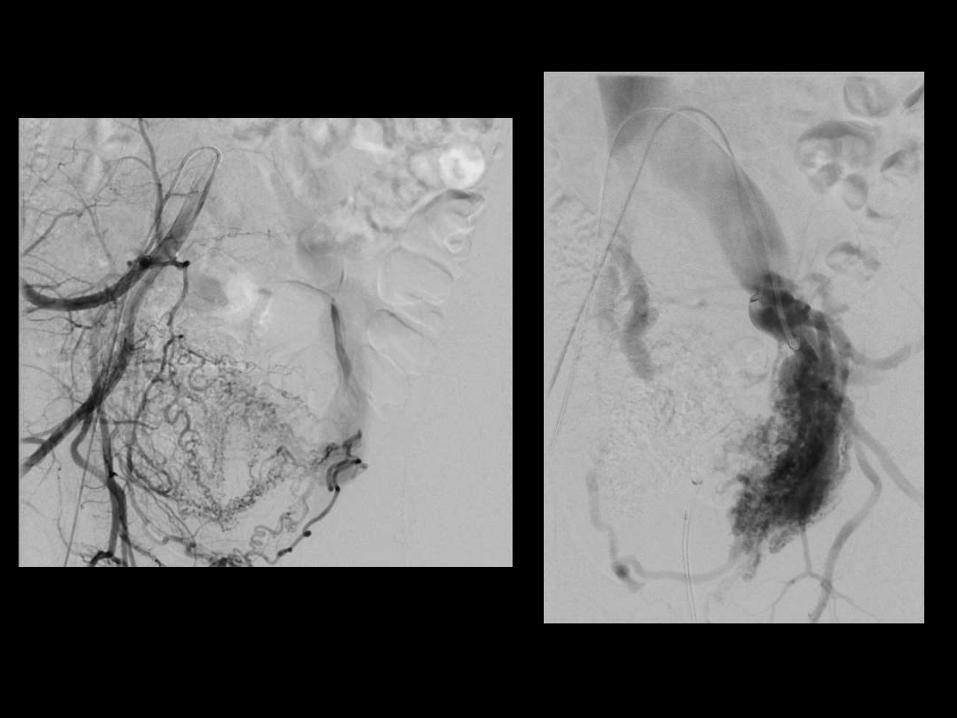
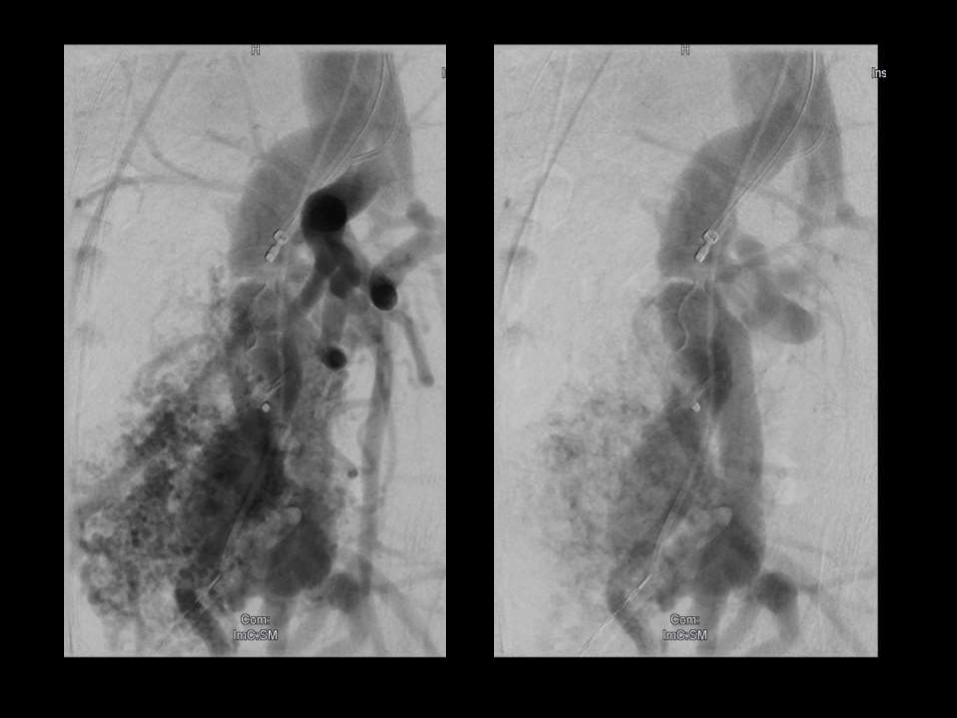
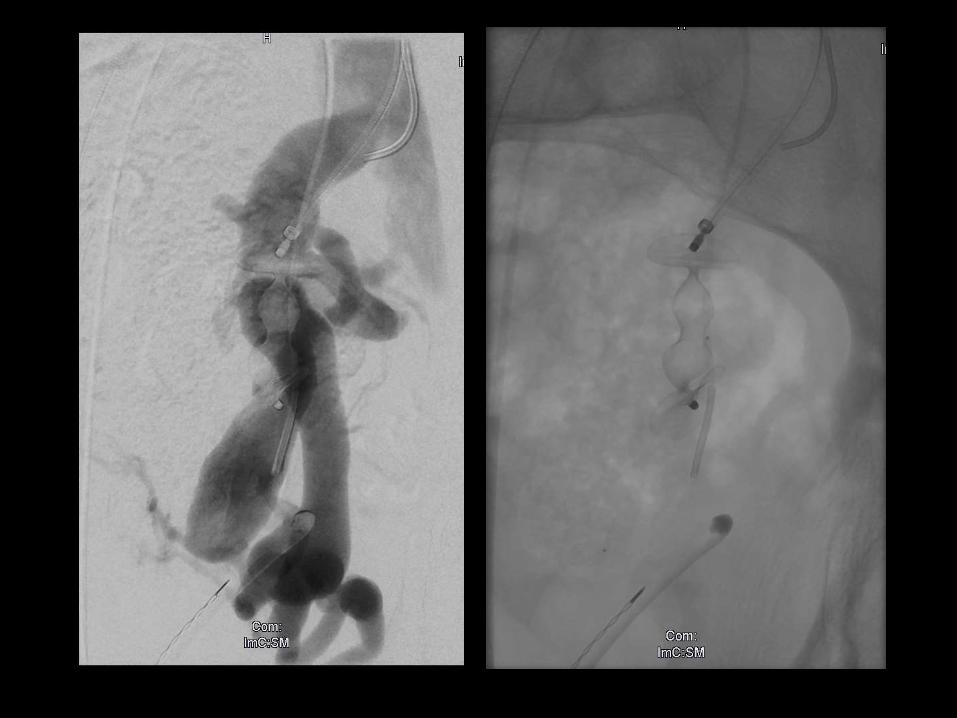
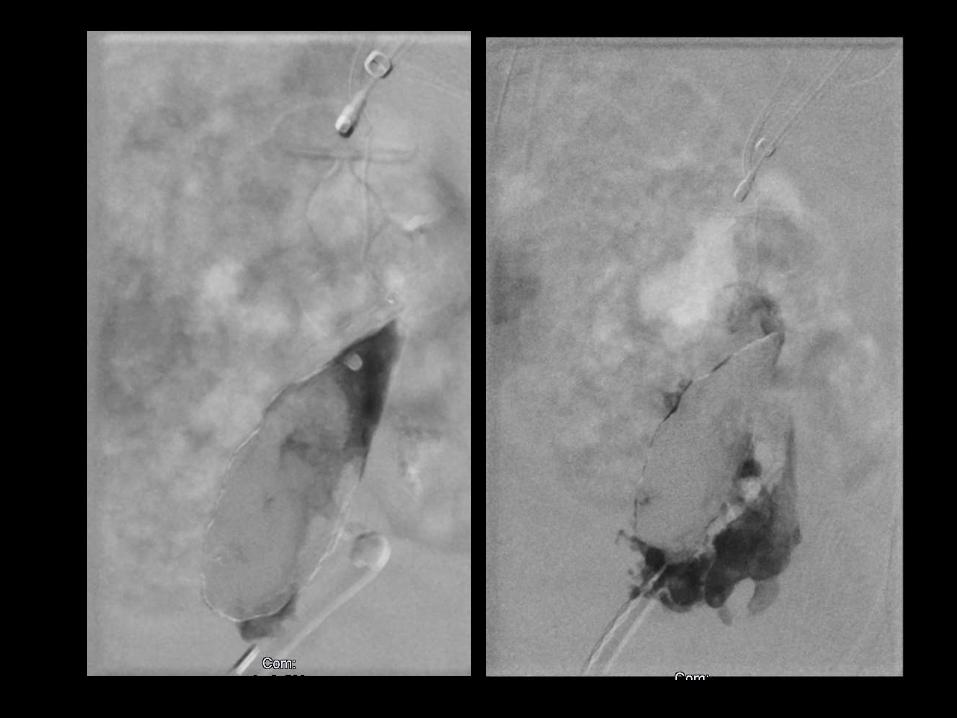
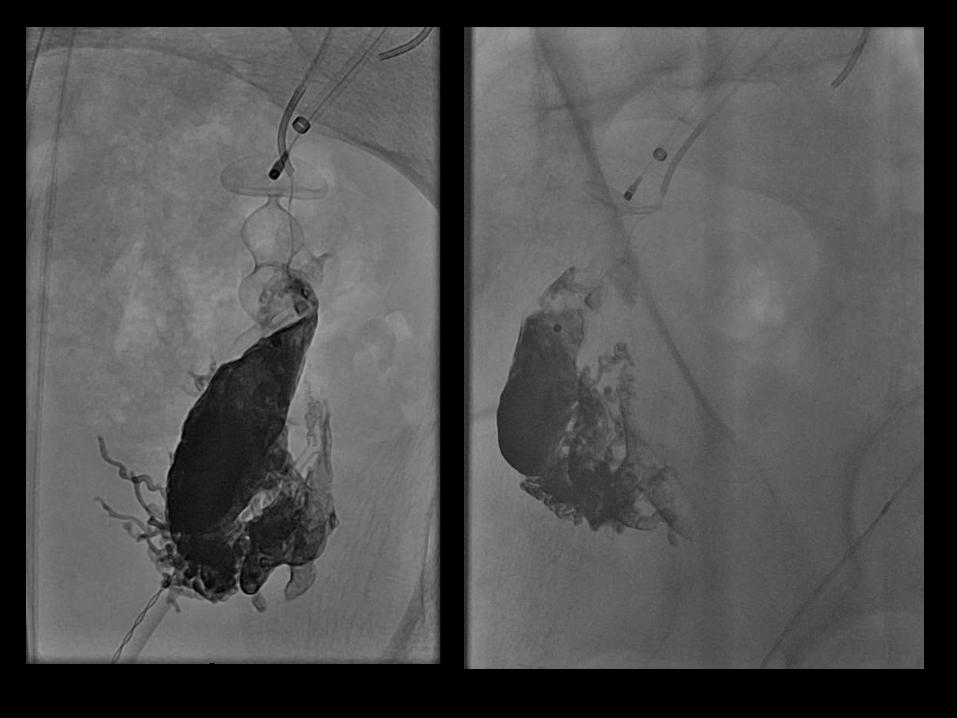
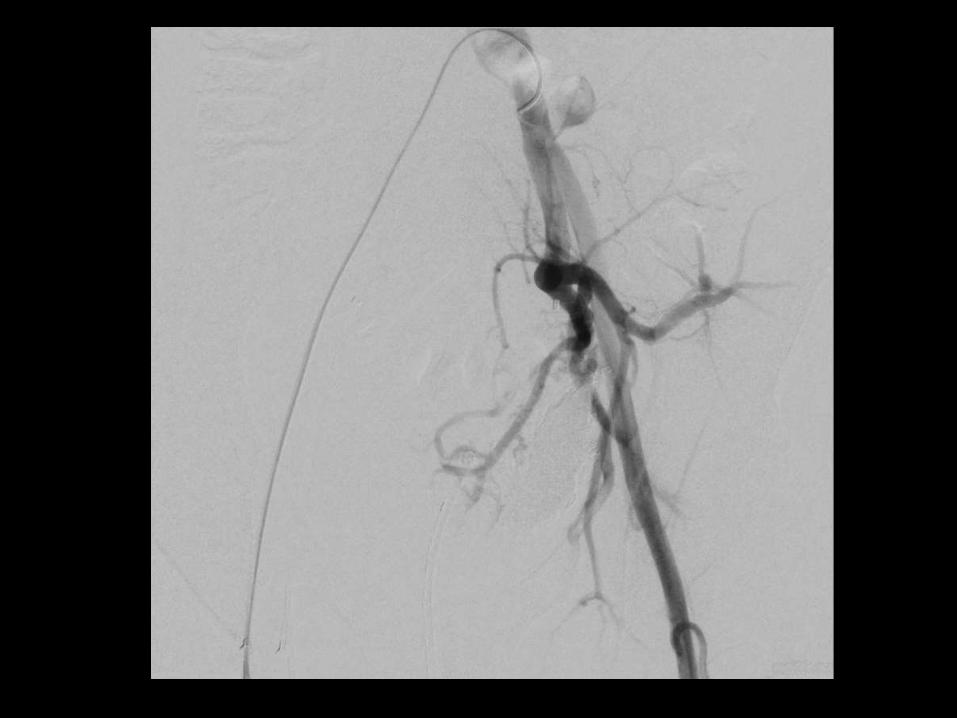
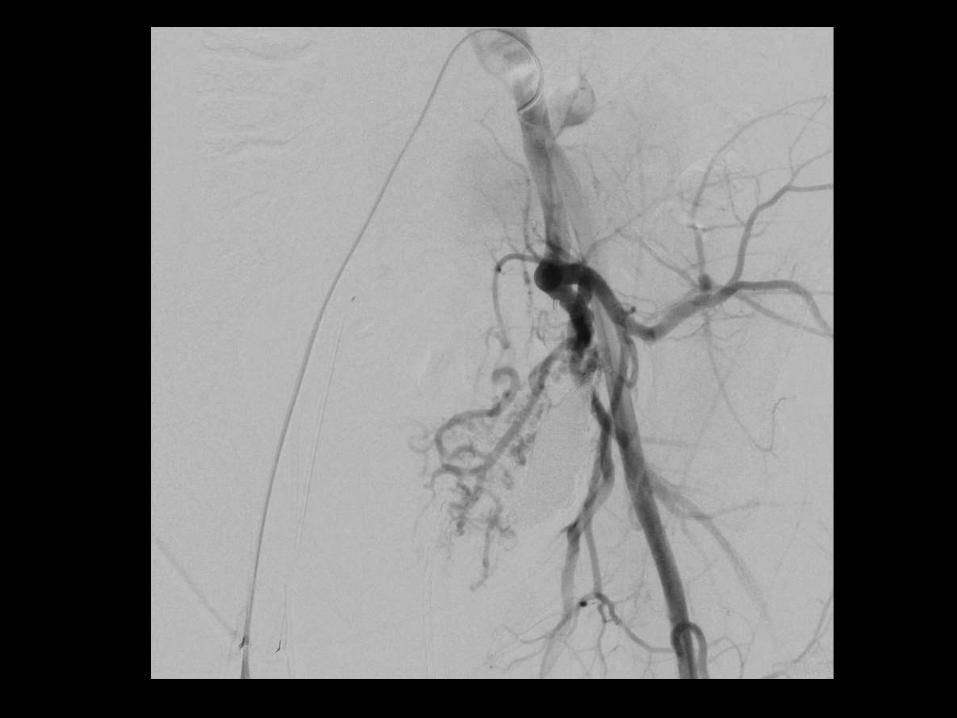
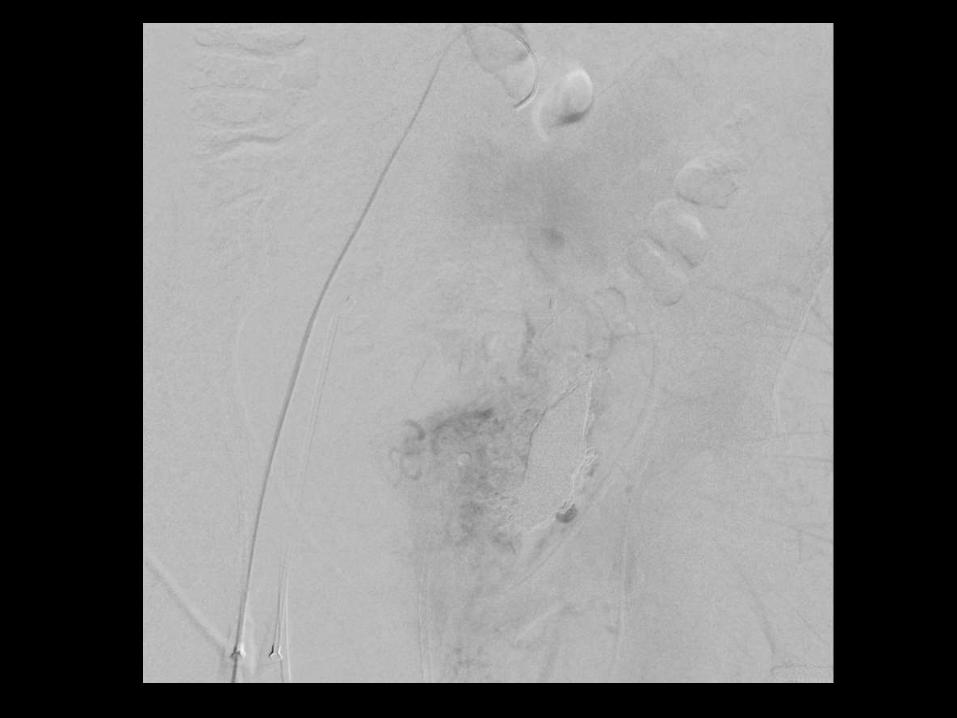
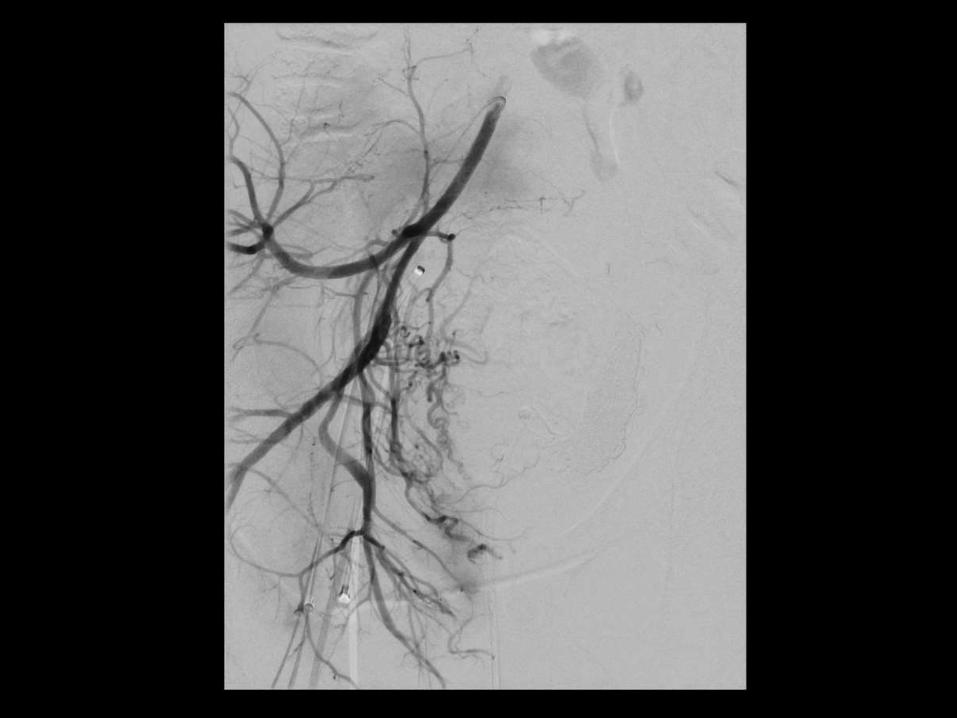
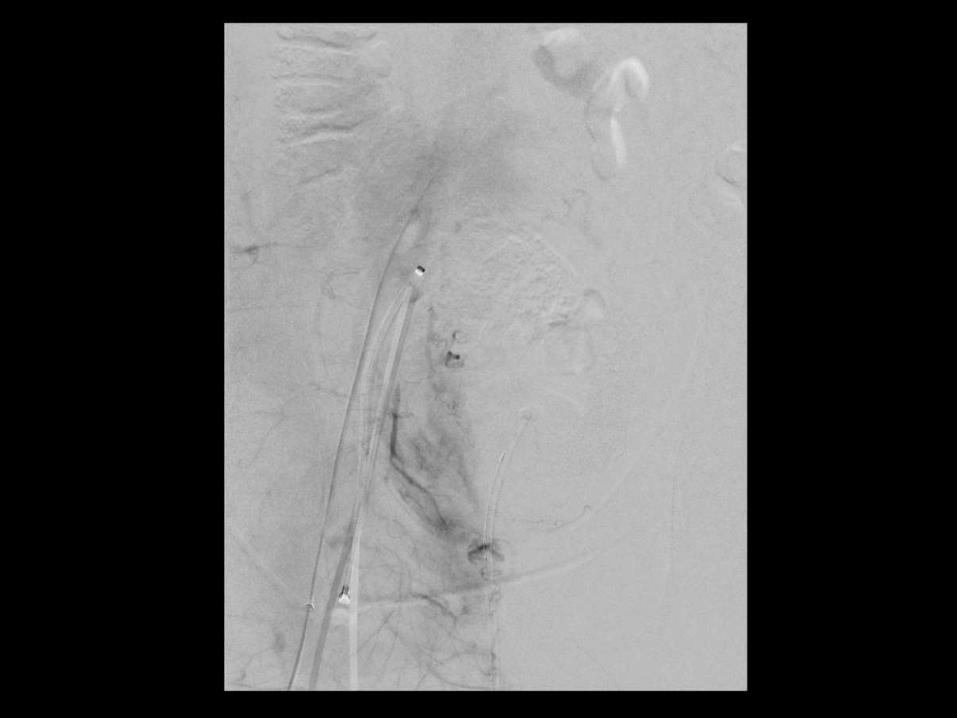
Onyx in peripheral AVM – transvenous retrograde
• 11 pats., 20 sessions, retrospective• Retrograde Onyx filling of Nidus via transvenous approach
– Type II AVM with dominant outflow vein– Preparation: transarterial flow-reduction in 73% and transvenous
Plugs in 27%
• Complete devascularization in 10 pats. (91%)• 95% devascularization in remaining patient
– Rest: “near-complete devascularization”
• 1 minor complication (pain + swelling)• No symptoms 8 pats. (73%)• Improved symptoms 3 pats. (27%• During follow-up 8 months 1 angiographic recurrence
(without symptoms)
Wohlgemuth WA, Müller-Wille R, Teusch VI, Dudeck O, Cahill AM, Alomari AI, Uller W. The retrograde transvenous push-through method: a novel treatment of peripheral arteriovenous malformations withdominant venous outflow. Cardiovasc Intervent Radiol. 2015 Jun;38(3):623-31

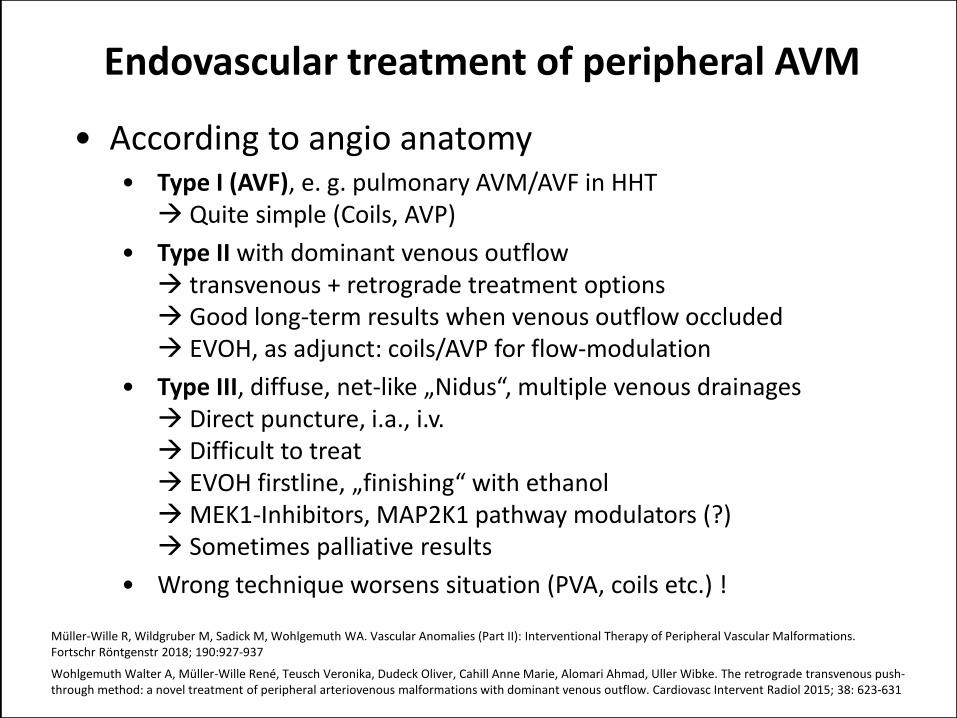
Endovascular treatment of peripheral AVM
• According to angio anatomy• Type I (AVF), e. g. pulmonary AVM/AVF in HHT Quite simple (Coils, AVP)
• Type II with dominant venous outflow transvenous + retrograde treatment options Good long-term results when venous outflow occluded EVOH, as adjunct: coils/AVP for flow-modulation
• Type III, diffuse, net-like „Nidus“, multiple venous drainages Direct puncture, i.a., i.v. Difficult to treat EVOH firstline, „finishing“ with ethanolMEK1-Inhibitors, MAP2K1 pathway modulators (?) Sometimes palliative results
• Wrong technique worsens situation (PVA, coils etc.) !
Müller-Wille R, Wildgruber M, Sadick M, Wohlgemuth WA. Vascular Anomalies (Part II): Interventional Therapy of Peripheral Vascular Malformations.Fortschr Röntgenstr 2018; 190:927-937
Wohlgemuth Walter A, Müller-Wille René, Teusch Veronika, Dudeck Oliver, Cahill Anne Marie, Alomari Ahmad, Uller Wibke. The retrograde transvenous push-through method: a novel treatment of peripheral arteriovenous malformations with dominant venous outflow. Cardiovasc Intervent Radiol 2015; 38: 623-631
Univ.-Prof. Dr. Dr. Walter A. Wohlgemuth1) University Clinic and Policlinic of Radiology, Martin-Luther University Halle-Wittenberg, Germany
2) German Interdisciplinary Society of Vascular Anomalies
www.compgefa.de
Clinical evidence of Onyx for the treatment of
endoleakages and AVM‘s
LINC 2019
Leipzig, Germany, 24. January 2019
Walter A. Wohlgemuth
University Clinic and Policlinic of Radiology
Martin-Luther University Halle-Wittenberg, Germany