clinical management of polycystic kidney disease
TRANSCRIPT
Clinical Medicine Vol 3 No 6 NovemberDecember 2003 509
CME Renal Medicine
Autosomal dominant polycystic kidneydisease (ADPKD) is a systemic diseasewith renal and various extrarenal mani-festations It is one of the most commonhereditary disorders affecting approxi-mately one in 1000 individuals and currently accounts for 65 of end-stagerenal disease (ESRD) in England andWales
Genetics
ADPKD is caused by mutations in twogenes12
PKD1 on chromosome 16p133 and
PKD2 on chromosome 4q21-23
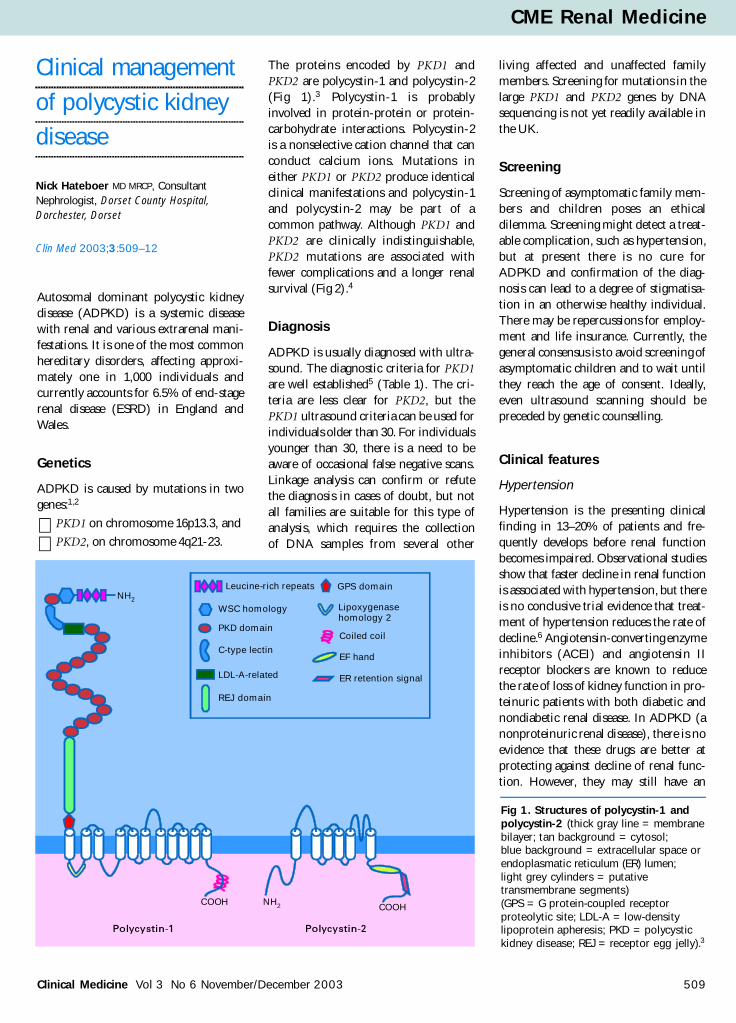
The proteins encoded by PKD1 andPKD2 are polycystin-1 and polycystin-2(Fig 1)3 Polycystin-1 is probablyinvolved in protein-protein or protein-carbohydrate interactions Polycystin-2is a nonselective cation channel that canconduct calcium ions Mutations ineither PKD1 or PKD2 produce identicalclinical manifestations and polycystin-1and polycystin-2 may be part of acommon pathway Although PKD1 andPKD2 are clinically indistinguishablePKD2 mutations are associated withfewer complications and a longer renalsurvival (Fig 2)4
Diagnosis
ADPKD is usually diagnosed with ultra-sound The diagnostic criteria for PKD1are well established5 (Table 1) The cri-teria are less clear for PKD2 but thePKD1 ultrasound criteria can be used forindividuals older than 30 For individualsyounger than 30 there is a need to beaware of occasional false negative scansLinkage analysis can confirm or refutethe diagnosis in cases of doubt but notall families are suitable for this type ofanalysis which requires the collection of DNA samples from several other
living affected and unaffected familymembers Screening for mutations in thelarge PKD1 and PKD2 genes by DNAsequencing is not yet readily available inthe UK
Screening
Screening of asymptomatic family mem-bers and children poses an ethicaldilemma Screening might detect a treat-able complication such as hypertensionbut at present there is no cure forADPKD and confirmation of the diag-nosis can lead to a degree of stigmatisa-tion in an otherwise healthy individualThere may be repercussions for employ-ment and life insurance Currently thegeneral consensus is to avoid screening ofasymptomatic children and to wait untilthey reach the age of consent Ideallyeven ultrasound scanning should bepreceded by genetic counselling
Clinical features
Hypertension
Hypertension is the presenting clinicalfinding in 13ndash20 of patients and fre-quently develops before renal functionbecomes impaired Observational studiesshow that faster decline in renal functionis associated with hypertension but thereis no conclusive trial evidence that treat-ment of hypertension reduces the rate ofdecline6 Angiotensin-converting enzymeinhibitors (ACEI) and angiotensin IIreceptor blockers are known to reducethe rate of loss of kidney function in pro-teinuric patients with both diabetic andnondiabetic renal disease In ADPKD (anonproteinuric renal disease) there is noevidence that these drugs are better atprotecting against decline of renal func-tion However they may still have an
Nick Hateboer MD MRCP ConsultantNephrologist Dorset County HospitalDorchester Dorset
Clin Med 20033509ndash12
Clinical management
of polycystic kidney
disease
Fig 1 Structures of polycystin-1 andpolycystin-2 (thick gray line = membranebilayer tan background = cytosol blue background = extracellular space orendoplasmatic reticulum (ER) lumen light grey cylinders = putativetransmembrane segments) (GPS = G protein-coupled receptorproteolytic site LDL-A = low-densitylipoprotein apheresis PKD = polycystickidney disease REJ = receptor egg jelly)3
NH2
Leucine-rich repeats
WSC homology
COOHCOOH
Polycystin-1 Polycystin-2
NH2
PKD domain
C-type lectin
LDL-A-related
REJ domain
GPS domain
Coiled coil
EF hand
ER retention signal
Lipoxygenasehomology 2
advantage over some other antihyperten-sive classes in reducing the developmentof left ventricular hypertrophy (LVH)
Left ventricular hypertrophy
The leading cause of death in ADPKD iscardiovascular disease7 LVH is well estab-lished as a risk factor for cardiovascularmorbidity and mortality its incidence isincreased in ADPKD most probably aresult of early untreated hypertension In a large seven-year prospective ran-domised study8 comparing the impact ofrigorous (lt12080 mmHg) versus stan-dard (135ndash14085ndash90 mmHg) bloodpressure control on LVH and renal func-tion the former was more effective indecreasing LVH However as in theModification of Diet in Renal Diseasestudy6 there was no difference in renalfunction decline
Haematuria
Frank haematuria is common inADPKD It often occurs spontaneouslybut is occasionally associated with uri-nary tract infection strenuous activityand rarely with kidney stones The inci-dence is related to kidney size the pres-
ence of hypertension and the degree ofrenal impairment Gross haematuriausually ceases within several days andrarely requires specific medical or sur-gical intervention Clinicians shouldremain wary of missing alternativecauses particularly bladder cancer
Pain
Flank or abdominal pain is experiencedby at least 50ndash60 of patients withADPKD at some time during theirlife Chronic pain is most probablyrelated to cyst distension whereas acutepain is more suggestive of intracystichaemorrhage infection or urinarytract obstruction Most patients withchronic pain are helped by simple anal-gesics but sometimes surgical decom-pression or percutaneous intracysticinjection of a sclerosing agent may beconsidered
Renal calculi
The estimated prevalence of renal calculiin ADPKD is 11ndash34 but they are oftenasymptomatic Uric acid can be found in57 of stones and calcium oxalate in47 Options for treatment and prophy-
laxis are in general the same as those fornon-ADPKD stone-formers
Infection
ADPKD is associated with an increasedincidence of upper and lower urinarytract infections It is often difficult to dis-tinguish between pyelonephritis andrenal cyst infection but in cyst infectionthe urine culture is often negative andthere is a poor clinical response tolipophobic antibiotics (eg aminoglyco-sides beta-lactams) Lipophilic anti-biotics (eg ciprofloxacin trimethoprim)have better cyst penetration Prolongedantibiotic therapy may be necessary andoccasionally cyst drainage or evennephrectomy may be required to controlinfection
Renal failure
Kidney failure is one of the most seriouscomplications of ADPKD The medianage for reaching ESRD is around 54 yearsin PKD1 and 74 years in PKD24 Onceglomerular filtration rate falls below50 mlmin it will decline further atapproximately 5 mlmin per year Someindividuals never develop ESRD butconversely ESRD is occasionally seen invery young children The treatment ofESRD is no different from that in thenon-ADPKD population with the pos-sible exception of the occasional trans-plant recipient who will require apre-emptive nephrectomy for anatomicalreasons
510 Clinical Medicine Vol 3 No 6 NovemberDecember 2003
CME Renal Medicine
100
80
60
40
20
0100806040200
Age
Controls
Median age
PKD1 530 (512 plusmn 548)PKD2 691 (669 plusmn 713)Controls 780 (738 plusmn 822)
PKD2
PKD1
Fig 2 Survival curves to end-stage renal disease ordeath for PKD1 PKD2 and unaffected controls(median ages and 95 confidence intervals)4
Age (years) Criteria
lt30 at least 2 renal cysts (unilateral or bilateral)
30ndash59 at least 2 cysts in each kidney
sup360 at least 4 cysts in each kidney
Table 1 Ultrasound criteria
Clinical Medicine Vol 3 No 6 NovemberDecember 2003 511
CME Renal Medicine
Extrarenal manifestations
Cysts
Cysts can also be identified in the liverspleen pancreas and brain (arachnoidcysts) and occasionally in the oeso-phagus ovaries uterus and seminalvesicles Liver cysts are common with ahigher prevalence in women Pregnancyis a risk factor for massive hepatic cysticinvolvement (Fig 3) thought to berelated to oestrogens Some authors havetherefore suggested that hormonereplacement therapy should be avoided
in women with liver cysts Liver cysts areusually asymptomatic but occasionallygive rise to abdominal pain symptomsdue to compression of the gastro-intestinal tract obstructive jaundiceportal hypertension or compression ofthe intrahepatic vena cava
Intracranial aneurysms
The association between ADPKD andintracranial aneurysms (ICAs) is wellestablished The prevalence of asympto-matic ICA in the ADPKD population is
about 8 4ndash5 times higher than in thegeneral population10 it may be as high as25 among those with a family history ofICA Rupture of ICA accounts forapproximately 6 of all deaths inADPKD7 and also occurs at a younger agethan in the general population Screeningfor ICAs with magnetic resonanceangiography (MRA) might be beneficialfor certain categories of patients but itremains unclear precisely who should bescreened with MRA However there isconsensus that those with a family historyof brain haemorrhage should be offeredscreening (Fig 4)
Cardiac valvularcardiovascularpathology
ADPKD is associated with various car-diac valve abnormalities including mitralincompetence mitral valve prolapse tri-cuspid incompetence tricuspid valveprolapse and aortic incompetence Otherreported cardiovascular abnormalities in ADPKD include coronary arteryaneurysms atrial-septal aneurysms dias-tolic dysfunction dissection of the verte-bral artery aortic dissection and LVHThe prevalence of abdominal aorticaneurysms is probably not increased inADPKD
Hernia and other connective tissueproblems
Inguinal and umbilical hernias are com-monly found in ADPKD Taken togetherwith the valvular and cardiovascular com-plications it is clear that ADPKD shouldbe considered a connective tissue disorderwith similarities to conditions like Marfanand Ehlers-Danlos syndromes
Diverticular disease
There have been numerous case reportsof complications of diverticular diseasein patients with ADPKD and it has beensuggested that the incidence is increasedin ADPKD However there was a similarprevalence of diverticular disease in thepatients and the healthy controls in theonly controlled study in which 55patients with ADPKD underwent abarium enema11
Fig 3 Massive cystic hepatomegaly in a patient requiring combined kidney and livertransplantation (from Ref 9 with permission)
Fig 4 Algorithmfor screening forintracranialaneurysm (CT = computedtomography ICA = intracranialaneurysm MR = magneticresonance) (fromYves Pirson withpermission)
Age 18ndash55 years and family history
of ICA
Brain MR angiographyor spiral CT scan
ICA
Conventional angiography
Discuss managementwith neurosurgeon
Repeat every5 years
Noscreening
No
No
Yes
Yes
Renal cell carcinoma
The prevalence of renal cell carcinoma(RCC) is not increased in ADPKD12
However RCC is more often concur-rently bilateral multicentric and sarco-matoid in type than in the generalpopulation13 In addition the diagnosisis often difficult and delayed A recentlarge international study confirmed thatthere was no undue excess risk of kidneycancer in patients with ESRD due toADPKD11
Treatment
Many dietary and pharmacological inter-vention strategies have been studied inhumans and animals with PKD in aneffort to slow the rate of renal progres-sion To date no strategy has shown aconsistent benefit in preserving renalfunction in humans with PKD14 Moreencouraging are data from a recent epi-demiological study which compared sur-vival to ESRD in patient cohorts from1985ndash1992 and from 1992ndash2001 Thelatter cohort had lower blood pressuresincreased use of ACEIs and slowerprogression of renal decline15
Future prospects
New insights into the molecular geneticsof ADPKD and improved understandingof the pathophysiological processes nec-essary for cyst development may help inthe development of novel pharmacolog-ical and other interventions An excitingdiscovery has been that both polycystins1 and 2 are expressed in renal cilia16
Cilia are long thin tubular structures onthe surface of renal tubular cells Theirfunction in human kidneys is unknownbut they may have a chemosensory ormechanosensory function This dis-covery has opened another avenue forresearch When the function of these ciliabecomes clearer they may providefurther therapeutic opportunities
References
1 The polycystic kidney disease 1 geneencodes a 14 kb transcript and lies within aduplicated region on chromosome 16 TheEuropean Polycystic Kidney DiseaseConsortium Cell 199477881ndash94
2 Mochizuki T Wu G Hayashi TXenophontos SL et al PKD2 a gene forpolycystic kidney disease that encodes anintegral membrane protein Science 19962721339ndash42
3 Igarashi P Somlo S Genetics and pathogen-esis of polycystic kidney disease ReviewJ Am Soc Nephrol 2002132384ndash98
4 Hateboer N van Dijk M Bogdanova NCoto E et al Comparison of phenotypes ofpolycystic kidney disease types 1 and 2European PKD1-PKD2 Study GroupLancet 1999353103ndash7
5 Ravine D Gibson RN Walker RG SheffieldLJ et al Evaluation of ultrasonographicdiagnostic criteria for autosomal dominant
polycystic kidney disease 1 Lancet 1994343824ndash7
6 Klahr S Breyer JA Beck GJ Dennis VWet al Dietary protein restriction blood pres-sure control and the progression of poly-cystic kidney disease Modification of Dietin Renal Disease Study Group J Am SocNephrol 199552037ndash47
7 Fick GM Johnson AM Hammond WSGabow PA Causes of death in autosomaldominant polycystic kidney disease ReviewJ Am Soc Nephrol 199552048ndash56
8 Schrier R McFann K Johnson A ChapmanA et al Cardiac and renal effects of standardversus rigorous blood pressure control inautosomal-dominant polycystic kidney dis-ease results of a seven-year prospective ran-domized study J Am Soc Nephrol 2002131733ndash9
9 Taylor JE Calne RY Stewart WK Massivecystic hepatomegaly in a female patient withpolycystic disease treated by combinedhepatic and renal transplantation QJM199180771ndash5
10 Pirson Y Chauveau D Torres V Manage-ment of cerebral aneurysms in autosomaldominant polycystic kidney disease ReviewJ Am Soc Nephrol 200213269ndash76
11 Sharp CK Zeligman BE Johnson AMDuley I Gabow PA Evaluation of colonicdiverticular disease in autosomal dominantpolycystic kidney disease without end-stagerenal disease Am J Kidney Dis 199934863ndash8
12 Stewart JH Buccianti G Agodoa L GellertR et al Cancers of the kidney and urinarytract in patients on dialysis for end-stagerenal disease analysis of data from theUnited States Europe and Australia andNew Zealand J Am Soc Nephrol 200314197ndash207
13 Keith DS Torres VE King BF Zincki HFarrow GM Renal cell carcinoma in auto-somal dominant polycystic kidney diseaseReview J Am Soc Nephrol 199441661ndash9
14 Davis ID MacRae Dell K Sweeney WEAvner ED Can progression of autosomaldominant or autosomal recessive polycystickidney disease be prevented Review SeminNephrol 200121430ndash40
15 Schrier RW McFann KK Johnson AMEpidemiological study of kidney survival inautosomal dominant polycystic kidneydisease Kidney Int 200363678ndash85
16 Yoder BK Hou X Guay-Woodford LM Thepolycystic kidney disease proteins poly-cystin-1 polycystin-2 polaris and cystinare co-localized in renal cilia J Am SocNephrol 2002132508ndash16
512 Clinical Medicine Vol 3 No 6 NovemberDecember 2003
CME Renal Medicine
Autosomal dominant polycystic kidneydisease (ADPKD) is a systemicdisease with various extrarenalmanifestations
Subarachnoid haemorrhage fromintracranial aneurysms is the mostserious extrarenal complicationscreening with magnetic resonanceangiography should be offered toADPKD patients with a familyhistory of brain haemorrhage
Mutations in two different genesPKD1 on chromosome 16 andPKD2 on chromosome 4 causeADPKD Clinically the twoconditions are indistinguishablebut overall PKD1 is more severe
The diagnosis of ADPKD still relies onultrasound with clearly definedcriteria according to the number ofrenal cysts False negative scansoccasionally occur under the age of30
Hypertension and left ventricularhypertrophy are common earlycomplications cardiovasculardisease is the leading cause ofdeath in ADPKD
Kidney failure generally occurs aroundage 55 There is no specifictreatment which is known to slowdown the decline in renal function
In contrast to other renal conditionsangiotensin-converting enzymeinhibitors are not superior to otherdrugs in slowing progression torenal failure in ADPKD
Key Points
KEY WORDS autosound dominantpolycystic kidney

advantage over some other antihyperten-sive classes in reducing the developmentof left ventricular hypertrophy (LVH)
Left ventricular hypertrophy
The leading cause of death in ADPKD iscardiovascular disease7 LVH is well estab-lished as a risk factor for cardiovascularmorbidity and mortality its incidence isincreased in ADPKD most probably aresult of early untreated hypertension In a large seven-year prospective ran-domised study8 comparing the impact ofrigorous (lt12080 mmHg) versus stan-dard (135ndash14085ndash90 mmHg) bloodpressure control on LVH and renal func-tion the former was more effective indecreasing LVH However as in theModification of Diet in Renal Diseasestudy6 there was no difference in renalfunction decline
Haematuria
Frank haematuria is common inADPKD It often occurs spontaneouslybut is occasionally associated with uri-nary tract infection strenuous activityand rarely with kidney stones The inci-dence is related to kidney size the pres-
ence of hypertension and the degree ofrenal impairment Gross haematuriausually ceases within several days andrarely requires specific medical or sur-gical intervention Clinicians shouldremain wary of missing alternativecauses particularly bladder cancer
Pain
Flank or abdominal pain is experiencedby at least 50ndash60 of patients withADPKD at some time during theirlife Chronic pain is most probablyrelated to cyst distension whereas acutepain is more suggestive of intracystichaemorrhage infection or urinarytract obstruction Most patients withchronic pain are helped by simple anal-gesics but sometimes surgical decom-pression or percutaneous intracysticinjection of a sclerosing agent may beconsidered
Renal calculi
The estimated prevalence of renal calculiin ADPKD is 11ndash34 but they are oftenasymptomatic Uric acid can be found in57 of stones and calcium oxalate in47 Options for treatment and prophy-
laxis are in general the same as those fornon-ADPKD stone-formers
Infection
ADPKD is associated with an increasedincidence of upper and lower urinarytract infections It is often difficult to dis-tinguish between pyelonephritis andrenal cyst infection but in cyst infectionthe urine culture is often negative andthere is a poor clinical response tolipophobic antibiotics (eg aminoglyco-sides beta-lactams) Lipophilic anti-biotics (eg ciprofloxacin trimethoprim)have better cyst penetration Prolongedantibiotic therapy may be necessary andoccasionally cyst drainage or evennephrectomy may be required to controlinfection
Renal failure
Kidney failure is one of the most seriouscomplications of ADPKD The medianage for reaching ESRD is around 54 yearsin PKD1 and 74 years in PKD24 Onceglomerular filtration rate falls below50 mlmin it will decline further atapproximately 5 mlmin per year Someindividuals never develop ESRD butconversely ESRD is occasionally seen invery young children The treatment ofESRD is no different from that in thenon-ADPKD population with the pos-sible exception of the occasional trans-plant recipient who will require apre-emptive nephrectomy for anatomicalreasons
510 Clinical Medicine Vol 3 No 6 NovemberDecember 2003
CME Renal Medicine
100
80
60
40
20
0100806040200
Age
Controls
Median age
PKD1 530 (512 plusmn 548)PKD2 691 (669 plusmn 713)Controls 780 (738 plusmn 822)
PKD2
PKD1
Fig 2 Survival curves to end-stage renal disease ordeath for PKD1 PKD2 and unaffected controls(median ages and 95 confidence intervals)4
Age (years) Criteria
lt30 at least 2 renal cysts (unilateral or bilateral)
30ndash59 at least 2 cysts in each kidney
sup360 at least 4 cysts in each kidney
Table 1 Ultrasound criteria
Clinical Medicine Vol 3 No 6 NovemberDecember 2003 511
CME Renal Medicine
Extrarenal manifestations
Cysts
Cysts can also be identified in the liverspleen pancreas and brain (arachnoidcysts) and occasionally in the oeso-phagus ovaries uterus and seminalvesicles Liver cysts are common with ahigher prevalence in women Pregnancyis a risk factor for massive hepatic cysticinvolvement (Fig 3) thought to berelated to oestrogens Some authors havetherefore suggested that hormonereplacement therapy should be avoided
in women with liver cysts Liver cysts areusually asymptomatic but occasionallygive rise to abdominal pain symptomsdue to compression of the gastro-intestinal tract obstructive jaundiceportal hypertension or compression ofthe intrahepatic vena cava
Intracranial aneurysms
The association between ADPKD andintracranial aneurysms (ICAs) is wellestablished The prevalence of asympto-matic ICA in the ADPKD population is
about 8 4ndash5 times higher than in thegeneral population10 it may be as high as25 among those with a family history ofICA Rupture of ICA accounts forapproximately 6 of all deaths inADPKD7 and also occurs at a younger agethan in the general population Screeningfor ICAs with magnetic resonanceangiography (MRA) might be beneficialfor certain categories of patients but itremains unclear precisely who should bescreened with MRA However there isconsensus that those with a family historyof brain haemorrhage should be offeredscreening (Fig 4)
Cardiac valvularcardiovascularpathology
ADPKD is associated with various car-diac valve abnormalities including mitralincompetence mitral valve prolapse tri-cuspid incompetence tricuspid valveprolapse and aortic incompetence Otherreported cardiovascular abnormalities in ADPKD include coronary arteryaneurysms atrial-septal aneurysms dias-tolic dysfunction dissection of the verte-bral artery aortic dissection and LVHThe prevalence of abdominal aorticaneurysms is probably not increased inADPKD
Hernia and other connective tissueproblems
Inguinal and umbilical hernias are com-monly found in ADPKD Taken togetherwith the valvular and cardiovascular com-plications it is clear that ADPKD shouldbe considered a connective tissue disorderwith similarities to conditions like Marfanand Ehlers-Danlos syndromes
Diverticular disease
There have been numerous case reportsof complications of diverticular diseasein patients with ADPKD and it has beensuggested that the incidence is increasedin ADPKD However there was a similarprevalence of diverticular disease in thepatients and the healthy controls in theonly controlled study in which 55patients with ADPKD underwent abarium enema11
Fig 3 Massive cystic hepatomegaly in a patient requiring combined kidney and livertransplantation (from Ref 9 with permission)
Fig 4 Algorithmfor screening forintracranialaneurysm (CT = computedtomography ICA = intracranialaneurysm MR = magneticresonance) (fromYves Pirson withpermission)
Age 18ndash55 years and family history
of ICA
Brain MR angiographyor spiral CT scan
ICA
Conventional angiography
Discuss managementwith neurosurgeon
Repeat every5 years
Noscreening
No
No
Yes
Yes
Renal cell carcinoma
The prevalence of renal cell carcinoma(RCC) is not increased in ADPKD12
However RCC is more often concur-rently bilateral multicentric and sarco-matoid in type than in the generalpopulation13 In addition the diagnosisis often difficult and delayed A recentlarge international study confirmed thatthere was no undue excess risk of kidneycancer in patients with ESRD due toADPKD11
Treatment
Many dietary and pharmacological inter-vention strategies have been studied inhumans and animals with PKD in aneffort to slow the rate of renal progres-sion To date no strategy has shown aconsistent benefit in preserving renalfunction in humans with PKD14 Moreencouraging are data from a recent epi-demiological study which compared sur-vival to ESRD in patient cohorts from1985ndash1992 and from 1992ndash2001 Thelatter cohort had lower blood pressuresincreased use of ACEIs and slowerprogression of renal decline15
Future prospects
New insights into the molecular geneticsof ADPKD and improved understandingof the pathophysiological processes nec-essary for cyst development may help inthe development of novel pharmacolog-ical and other interventions An excitingdiscovery has been that both polycystins1 and 2 are expressed in renal cilia16
Cilia are long thin tubular structures onthe surface of renal tubular cells Theirfunction in human kidneys is unknownbut they may have a chemosensory ormechanosensory function This dis-covery has opened another avenue forresearch When the function of these ciliabecomes clearer they may providefurther therapeutic opportunities
References
1 The polycystic kidney disease 1 geneencodes a 14 kb transcript and lies within aduplicated region on chromosome 16 TheEuropean Polycystic Kidney DiseaseConsortium Cell 199477881ndash94
2 Mochizuki T Wu G Hayashi TXenophontos SL et al PKD2 a gene forpolycystic kidney disease that encodes anintegral membrane protein Science 19962721339ndash42
3 Igarashi P Somlo S Genetics and pathogen-esis of polycystic kidney disease ReviewJ Am Soc Nephrol 2002132384ndash98
4 Hateboer N van Dijk M Bogdanova NCoto E et al Comparison of phenotypes ofpolycystic kidney disease types 1 and 2European PKD1-PKD2 Study GroupLancet 1999353103ndash7
5 Ravine D Gibson RN Walker RG SheffieldLJ et al Evaluation of ultrasonographicdiagnostic criteria for autosomal dominant
polycystic kidney disease 1 Lancet 1994343824ndash7
6 Klahr S Breyer JA Beck GJ Dennis VWet al Dietary protein restriction blood pres-sure control and the progression of poly-cystic kidney disease Modification of Dietin Renal Disease Study Group J Am SocNephrol 199552037ndash47
7 Fick GM Johnson AM Hammond WSGabow PA Causes of death in autosomaldominant polycystic kidney disease ReviewJ Am Soc Nephrol 199552048ndash56
8 Schrier R McFann K Johnson A ChapmanA et al Cardiac and renal effects of standardversus rigorous blood pressure control inautosomal-dominant polycystic kidney dis-ease results of a seven-year prospective ran-domized study J Am Soc Nephrol 2002131733ndash9
9 Taylor JE Calne RY Stewart WK Massivecystic hepatomegaly in a female patient withpolycystic disease treated by combinedhepatic and renal transplantation QJM199180771ndash5
10 Pirson Y Chauveau D Torres V Manage-ment of cerebral aneurysms in autosomaldominant polycystic kidney disease ReviewJ Am Soc Nephrol 200213269ndash76
11 Sharp CK Zeligman BE Johnson AMDuley I Gabow PA Evaluation of colonicdiverticular disease in autosomal dominantpolycystic kidney disease without end-stagerenal disease Am J Kidney Dis 199934863ndash8
12 Stewart JH Buccianti G Agodoa L GellertR et al Cancers of the kidney and urinarytract in patients on dialysis for end-stagerenal disease analysis of data from theUnited States Europe and Australia andNew Zealand J Am Soc Nephrol 200314197ndash207
13 Keith DS Torres VE King BF Zincki HFarrow GM Renal cell carcinoma in auto-somal dominant polycystic kidney diseaseReview J Am Soc Nephrol 199441661ndash9
14 Davis ID MacRae Dell K Sweeney WEAvner ED Can progression of autosomaldominant or autosomal recessive polycystickidney disease be prevented Review SeminNephrol 200121430ndash40
15 Schrier RW McFann KK Johnson AMEpidemiological study of kidney survival inautosomal dominant polycystic kidneydisease Kidney Int 200363678ndash85
16 Yoder BK Hou X Guay-Woodford LM Thepolycystic kidney disease proteins poly-cystin-1 polycystin-2 polaris and cystinare co-localized in renal cilia J Am SocNephrol 2002132508ndash16
512 Clinical Medicine Vol 3 No 6 NovemberDecember 2003
CME Renal Medicine
Autosomal dominant polycystic kidneydisease (ADPKD) is a systemicdisease with various extrarenalmanifestations
Subarachnoid haemorrhage fromintracranial aneurysms is the mostserious extrarenal complicationscreening with magnetic resonanceangiography should be offered toADPKD patients with a familyhistory of brain haemorrhage
Mutations in two different genesPKD1 on chromosome 16 andPKD2 on chromosome 4 causeADPKD Clinically the twoconditions are indistinguishablebut overall PKD1 is more severe
The diagnosis of ADPKD still relies onultrasound with clearly definedcriteria according to the number ofrenal cysts False negative scansoccasionally occur under the age of30
Hypertension and left ventricularhypertrophy are common earlycomplications cardiovasculardisease is the leading cause ofdeath in ADPKD
Kidney failure generally occurs aroundage 55 There is no specifictreatment which is known to slowdown the decline in renal function
In contrast to other renal conditionsangiotensin-converting enzymeinhibitors are not superior to otherdrugs in slowing progression torenal failure in ADPKD
Key Points
KEY WORDS autosound dominantpolycystic kidney

Clinical Medicine Vol 3 No 6 NovemberDecember 2003 511
CME Renal Medicine
Extrarenal manifestations
Cysts
Cysts can also be identified in the liverspleen pancreas and brain (arachnoidcysts) and occasionally in the oeso-phagus ovaries uterus and seminalvesicles Liver cysts are common with ahigher prevalence in women Pregnancyis a risk factor for massive hepatic cysticinvolvement (Fig 3) thought to berelated to oestrogens Some authors havetherefore suggested that hormonereplacement therapy should be avoided
in women with liver cysts Liver cysts areusually asymptomatic but occasionallygive rise to abdominal pain symptomsdue to compression of the gastro-intestinal tract obstructive jaundiceportal hypertension or compression ofthe intrahepatic vena cava
Intracranial aneurysms
The association between ADPKD andintracranial aneurysms (ICAs) is wellestablished The prevalence of asympto-matic ICA in the ADPKD population is
about 8 4ndash5 times higher than in thegeneral population10 it may be as high as25 among those with a family history ofICA Rupture of ICA accounts forapproximately 6 of all deaths inADPKD7 and also occurs at a younger agethan in the general population Screeningfor ICAs with magnetic resonanceangiography (MRA) might be beneficialfor certain categories of patients but itremains unclear precisely who should bescreened with MRA However there isconsensus that those with a family historyof brain haemorrhage should be offeredscreening (Fig 4)
Cardiac valvularcardiovascularpathology
ADPKD is associated with various car-diac valve abnormalities including mitralincompetence mitral valve prolapse tri-cuspid incompetence tricuspid valveprolapse and aortic incompetence Otherreported cardiovascular abnormalities in ADPKD include coronary arteryaneurysms atrial-septal aneurysms dias-tolic dysfunction dissection of the verte-bral artery aortic dissection and LVHThe prevalence of abdominal aorticaneurysms is probably not increased inADPKD
Hernia and other connective tissueproblems
Inguinal and umbilical hernias are com-monly found in ADPKD Taken togetherwith the valvular and cardiovascular com-plications it is clear that ADPKD shouldbe considered a connective tissue disorderwith similarities to conditions like Marfanand Ehlers-Danlos syndromes
Diverticular disease
There have been numerous case reportsof complications of diverticular diseasein patients with ADPKD and it has beensuggested that the incidence is increasedin ADPKD However there was a similarprevalence of diverticular disease in thepatients and the healthy controls in theonly controlled study in which 55patients with ADPKD underwent abarium enema11
Fig 3 Massive cystic hepatomegaly in a patient requiring combined kidney and livertransplantation (from Ref 9 with permission)
Fig 4 Algorithmfor screening forintracranialaneurysm (CT = computedtomography ICA = intracranialaneurysm MR = magneticresonance) (fromYves Pirson withpermission)
Age 18ndash55 years and family history
of ICA
Brain MR angiographyor spiral CT scan
ICA
Conventional angiography
Discuss managementwith neurosurgeon
Repeat every5 years
Noscreening
No
No
Yes
Yes
Renal cell carcinoma
The prevalence of renal cell carcinoma(RCC) is not increased in ADPKD12
However RCC is more often concur-rently bilateral multicentric and sarco-matoid in type than in the generalpopulation13 In addition the diagnosisis often difficult and delayed A recentlarge international study confirmed thatthere was no undue excess risk of kidneycancer in patients with ESRD due toADPKD11
Treatment
Many dietary and pharmacological inter-vention strategies have been studied inhumans and animals with PKD in aneffort to slow the rate of renal progres-sion To date no strategy has shown aconsistent benefit in preserving renalfunction in humans with PKD14 Moreencouraging are data from a recent epi-demiological study which compared sur-vival to ESRD in patient cohorts from1985ndash1992 and from 1992ndash2001 Thelatter cohort had lower blood pressuresincreased use of ACEIs and slowerprogression of renal decline15
Future prospects
New insights into the molecular geneticsof ADPKD and improved understandingof the pathophysiological processes nec-essary for cyst development may help inthe development of novel pharmacolog-ical and other interventions An excitingdiscovery has been that both polycystins1 and 2 are expressed in renal cilia16
Cilia are long thin tubular structures onthe surface of renal tubular cells Theirfunction in human kidneys is unknownbut they may have a chemosensory ormechanosensory function This dis-covery has opened another avenue forresearch When the function of these ciliabecomes clearer they may providefurther therapeutic opportunities
References
1 The polycystic kidney disease 1 geneencodes a 14 kb transcript and lies within aduplicated region on chromosome 16 TheEuropean Polycystic Kidney DiseaseConsortium Cell 199477881ndash94
2 Mochizuki T Wu G Hayashi TXenophontos SL et al PKD2 a gene forpolycystic kidney disease that encodes anintegral membrane protein Science 19962721339ndash42
3 Igarashi P Somlo S Genetics and pathogen-esis of polycystic kidney disease ReviewJ Am Soc Nephrol 2002132384ndash98
4 Hateboer N van Dijk M Bogdanova NCoto E et al Comparison of phenotypes ofpolycystic kidney disease types 1 and 2European PKD1-PKD2 Study GroupLancet 1999353103ndash7
5 Ravine D Gibson RN Walker RG SheffieldLJ et al Evaluation of ultrasonographicdiagnostic criteria for autosomal dominant
polycystic kidney disease 1 Lancet 1994343824ndash7
6 Klahr S Breyer JA Beck GJ Dennis VWet al Dietary protein restriction blood pres-sure control and the progression of poly-cystic kidney disease Modification of Dietin Renal Disease Study Group J Am SocNephrol 199552037ndash47
7 Fick GM Johnson AM Hammond WSGabow PA Causes of death in autosomaldominant polycystic kidney disease ReviewJ Am Soc Nephrol 199552048ndash56
8 Schrier R McFann K Johnson A ChapmanA et al Cardiac and renal effects of standardversus rigorous blood pressure control inautosomal-dominant polycystic kidney dis-ease results of a seven-year prospective ran-domized study J Am Soc Nephrol 2002131733ndash9
9 Taylor JE Calne RY Stewart WK Massivecystic hepatomegaly in a female patient withpolycystic disease treated by combinedhepatic and renal transplantation QJM199180771ndash5
10 Pirson Y Chauveau D Torres V Manage-ment of cerebral aneurysms in autosomaldominant polycystic kidney disease ReviewJ Am Soc Nephrol 200213269ndash76
11 Sharp CK Zeligman BE Johnson AMDuley I Gabow PA Evaluation of colonicdiverticular disease in autosomal dominantpolycystic kidney disease without end-stagerenal disease Am J Kidney Dis 199934863ndash8
12 Stewart JH Buccianti G Agodoa L GellertR et al Cancers of the kidney and urinarytract in patients on dialysis for end-stagerenal disease analysis of data from theUnited States Europe and Australia andNew Zealand J Am Soc Nephrol 200314197ndash207
13 Keith DS Torres VE King BF Zincki HFarrow GM Renal cell carcinoma in auto-somal dominant polycystic kidney diseaseReview J Am Soc Nephrol 199441661ndash9
14 Davis ID MacRae Dell K Sweeney WEAvner ED Can progression of autosomaldominant or autosomal recessive polycystickidney disease be prevented Review SeminNephrol 200121430ndash40
15 Schrier RW McFann KK Johnson AMEpidemiological study of kidney survival inautosomal dominant polycystic kidneydisease Kidney Int 200363678ndash85
16 Yoder BK Hou X Guay-Woodford LM Thepolycystic kidney disease proteins poly-cystin-1 polycystin-2 polaris and cystinare co-localized in renal cilia J Am SocNephrol 2002132508ndash16
512 Clinical Medicine Vol 3 No 6 NovemberDecember 2003
CME Renal Medicine
Autosomal dominant polycystic kidneydisease (ADPKD) is a systemicdisease with various extrarenalmanifestations
Subarachnoid haemorrhage fromintracranial aneurysms is the mostserious extrarenal complicationscreening with magnetic resonanceangiography should be offered toADPKD patients with a familyhistory of brain haemorrhage
Mutations in two different genesPKD1 on chromosome 16 andPKD2 on chromosome 4 causeADPKD Clinically the twoconditions are indistinguishablebut overall PKD1 is more severe
The diagnosis of ADPKD still relies onultrasound with clearly definedcriteria according to the number ofrenal cysts False negative scansoccasionally occur under the age of30
Hypertension and left ventricularhypertrophy are common earlycomplications cardiovasculardisease is the leading cause ofdeath in ADPKD
Kidney failure generally occurs aroundage 55 There is no specifictreatment which is known to slowdown the decline in renal function
In contrast to other renal conditionsangiotensin-converting enzymeinhibitors are not superior to otherdrugs in slowing progression torenal failure in ADPKD
Key Points
KEY WORDS autosound dominantpolycystic kidney

Renal cell carcinoma
The prevalence of renal cell carcinoma(RCC) is not increased in ADPKD12
However RCC is more often concur-rently bilateral multicentric and sarco-matoid in type than in the generalpopulation13 In addition the diagnosisis often difficult and delayed A recentlarge international study confirmed thatthere was no undue excess risk of kidneycancer in patients with ESRD due toADPKD11
Treatment
Many dietary and pharmacological inter-vention strategies have been studied inhumans and animals with PKD in aneffort to slow the rate of renal progres-sion To date no strategy has shown aconsistent benefit in preserving renalfunction in humans with PKD14 Moreencouraging are data from a recent epi-demiological study which compared sur-vival to ESRD in patient cohorts from1985ndash1992 and from 1992ndash2001 Thelatter cohort had lower blood pressuresincreased use of ACEIs and slowerprogression of renal decline15
Future prospects
New insights into the molecular geneticsof ADPKD and improved understandingof the pathophysiological processes nec-essary for cyst development may help inthe development of novel pharmacolog-ical and other interventions An excitingdiscovery has been that both polycystins1 and 2 are expressed in renal cilia16
Cilia are long thin tubular structures onthe surface of renal tubular cells Theirfunction in human kidneys is unknownbut they may have a chemosensory ormechanosensory function This dis-covery has opened another avenue forresearch When the function of these ciliabecomes clearer they may providefurther therapeutic opportunities
References
1 The polycystic kidney disease 1 geneencodes a 14 kb transcript and lies within aduplicated region on chromosome 16 TheEuropean Polycystic Kidney DiseaseConsortium Cell 199477881ndash94
2 Mochizuki T Wu G Hayashi TXenophontos SL et al PKD2 a gene forpolycystic kidney disease that encodes anintegral membrane protein Science 19962721339ndash42
3 Igarashi P Somlo S Genetics and pathogen-esis of polycystic kidney disease ReviewJ Am Soc Nephrol 2002132384ndash98
4 Hateboer N van Dijk M Bogdanova NCoto E et al Comparison of phenotypes ofpolycystic kidney disease types 1 and 2European PKD1-PKD2 Study GroupLancet 1999353103ndash7
5 Ravine D Gibson RN Walker RG SheffieldLJ et al Evaluation of ultrasonographicdiagnostic criteria for autosomal dominant
polycystic kidney disease 1 Lancet 1994343824ndash7
6 Klahr S Breyer JA Beck GJ Dennis VWet al Dietary protein restriction blood pres-sure control and the progression of poly-cystic kidney disease Modification of Dietin Renal Disease Study Group J Am SocNephrol 199552037ndash47
7 Fick GM Johnson AM Hammond WSGabow PA Causes of death in autosomaldominant polycystic kidney disease ReviewJ Am Soc Nephrol 199552048ndash56
8 Schrier R McFann K Johnson A ChapmanA et al Cardiac and renal effects of standardversus rigorous blood pressure control inautosomal-dominant polycystic kidney dis-ease results of a seven-year prospective ran-domized study J Am Soc Nephrol 2002131733ndash9
9 Taylor JE Calne RY Stewart WK Massivecystic hepatomegaly in a female patient withpolycystic disease treated by combinedhepatic and renal transplantation QJM199180771ndash5
10 Pirson Y Chauveau D Torres V Manage-ment of cerebral aneurysms in autosomaldominant polycystic kidney disease ReviewJ Am Soc Nephrol 200213269ndash76
11 Sharp CK Zeligman BE Johnson AMDuley I Gabow PA Evaluation of colonicdiverticular disease in autosomal dominantpolycystic kidney disease without end-stagerenal disease Am J Kidney Dis 199934863ndash8
12 Stewart JH Buccianti G Agodoa L GellertR et al Cancers of the kidney and urinarytract in patients on dialysis for end-stagerenal disease analysis of data from theUnited States Europe and Australia andNew Zealand J Am Soc Nephrol 200314197ndash207
13 Keith DS Torres VE King BF Zincki HFarrow GM Renal cell carcinoma in auto-somal dominant polycystic kidney diseaseReview J Am Soc Nephrol 199441661ndash9
14 Davis ID MacRae Dell K Sweeney WEAvner ED Can progression of autosomaldominant or autosomal recessive polycystickidney disease be prevented Review SeminNephrol 200121430ndash40
15 Schrier RW McFann KK Johnson AMEpidemiological study of kidney survival inautosomal dominant polycystic kidneydisease Kidney Int 200363678ndash85
16 Yoder BK Hou X Guay-Woodford LM Thepolycystic kidney disease proteins poly-cystin-1 polycystin-2 polaris and cystinare co-localized in renal cilia J Am SocNephrol 2002132508ndash16
512 Clinical Medicine Vol 3 No 6 NovemberDecember 2003
CME Renal Medicine
Autosomal dominant polycystic kidneydisease (ADPKD) is a systemicdisease with various extrarenalmanifestations
Subarachnoid haemorrhage fromintracranial aneurysms is the mostserious extrarenal complicationscreening with magnetic resonanceangiography should be offered toADPKD patients with a familyhistory of brain haemorrhage
Mutations in two different genesPKD1 on chromosome 16 andPKD2 on chromosome 4 causeADPKD Clinically the twoconditions are indistinguishablebut overall PKD1 is more severe
The diagnosis of ADPKD still relies onultrasound with clearly definedcriteria according to the number ofrenal cysts False negative scansoccasionally occur under the age of30
Hypertension and left ventricularhypertrophy are common earlycomplications cardiovasculardisease is the leading cause ofdeath in ADPKD
Kidney failure generally occurs aroundage 55 There is no specifictreatment which is known to slowdown the decline in renal function
In contrast to other renal conditionsangiotensin-converting enzymeinhibitors are not superior to otherdrugs in slowing progression torenal failure in ADPKD
Key Points
KEY WORDS autosound dominantpolycystic kidney