clinical project reduction of primary post-partum haemorrhage filepost-partum haemorrhage (pph) is...
TRANSCRIPT

Clinical Project Reduction of Primary Post-Partum Haemorrhage

Clinical Services - Best Project Award 2017 2
Content
Main Information --------------------------------------------------------------------------------------- 3
The first criteria: Study and define project objectives ------------------------------------------- 4
The second criteria: Project Team ----------------------------------------------------------------- 18
The third criteria: Resource Management and Control --------------------------------------- 21
The fourth criteria: Risk Management and Project sustainability --------------------------- 24
The fifth criteria: Project execution --------------------------------------------------------------- 27
The sixth criteria: Results --------------------------------------------------------------------------- 33

Clinical Services - Best Project Award 2017 3
A summary of the project and its reasons Post-partum haemorrhage (PPH) is one of the leading causes of maternal death globally. Corniche Hospital runs a high risk obstetric service as the tertiary provider in Abu Dhabi. In 2016 the rate of PPH, greater than 1500 mls, was persistently above the agreed SEHA benchmark of 1% of all deliveries. Following literature review and service line agreement the benchmark was altered to 1.5% of deliveries above 2000 mls. However our focused mission at Corniche was to ensure that there were no avoidable PPH cases and any PPH was minimised to avoid morbidity. The objectives of the project are:
Reduce the rate of massive PPH ≥ 1500 mls to below 1.5% (as a stretch goal)
Analyse and redesign processes and procedures to facilitate clinical management of PPH
Update policies and procedures to reflect best practice Ensure sustainability of achieved results by maintaining a standardised approach to management and reporting of PPH Department: Labour and Delivery Suite
Project Manager: Jill Henry (LDS Unit Manager)
Main members of the project team
Name Role Mobile Email
Jill Henry LDS Unit Manager 4805062230 [email protected]
Provvidenza Stefanoni
Charge Midwife 0501390791 [email protected]
Anu Ravi Staff Midwife 0505629244 [email protected]
Sumitha Zachariah Staff Midwife 0505806752 [email protected]
Maria Thomas Staff Midwife 0569538429 [email protected]
Eman Mashal Staff Midwife 0543330525 [email protected]
Jane Kelly Director of Quality 0506121951 [email protected]
Rita Arslanian Performance Management Officer
0562125764 [email protected]
Dr. Saleema Wani Chair of Obstetrics 0506227139 [email protected]
Dr. Margaret Blott Chair of Academic Affairs 0506129184 [email protected]
Dr. Tarek Ansari Chief of Anesthesia 0561173994 [email protected]
Dr. Soha Said Consultant Obstetrician 0553528876 [email protected]
Dr. Priya Sequeira Specialist Physician 0501586885 [email protected]
01 / 04 / 2017 Project Starting Date
The person who can be contacted in with any issues related to the project submission :
Name Telephone Mobile Email
Jill Henry + 971 (2) 696 5578 + 971 (50) 622 3048 [email protected]

Clinical Services - Best Project Award 2017 4
The First Criteria: Study and Define Project Objective
Introduction
1. Identify and set goals and project document
Post-partum haemorrhage (PPH) is one of the leading causes of maternal death globally. Corniche Hospital runs a high risk obstetric service as the tertiary provider in Abu Dhabi. Our focused mission at Corniche was to ensure that there were no avoidable PPH cases and any PPH was minimised to avoid morbidity. Problem statement In 2016 the rate of PPH greater than 1500 mls was persistently above the agreed
SEHA benchmark of 1% of all deliveries. Following literature review and service line
agreement the benchmark was altered to 1.5% of deliveries above 2000 mls.
Project Objectives Reduce the rate of massive PPH ≥ 1500 mls to below 1.5%
Review of policies and procedures to reflect best practice
Analyse and redesign processes and procedures to facilitate clinical management of PPH
Ensure sustainability of achieved results by maintaining a standardised approach to
management and reporting of PPH
Project Document During the initiating phase all the documents needed to define the quality improvement project were
created including:
Quality Improvement Project Charter was submitted to the Quality Department for
registration. The Quality Department has a robust system to register all QIPs in order to
ensure commitment to all 5 phases of project management, as well as:
o Ensure alignment with the hospitals and Abu Dhabi Health Services Company SEHA’s
strategic priorities, this project was aligned with the strategic priority to ensure
quality outcomes meet or exceed benchmark performance.
o Registration and tracking of all QIPs
o Evaluate the progress of the QIP and hold the members accountable in their annual
performance evaluation (I-perform)
o Allow the Quality Department to have oversight of the project and to follow-up the
achievement and sustainability of planned objectives.
Data collection and analysis tools for all patients who had a blood loss

Clinical Services - Best Project Award 2017 5
≥ 1500 mls within 24 hours of delivery.
The team in Labour and Delivery Suite (LDS) designed a survey to determine if any delay in
medication administration was contributing to an increase in blood loss. The survey called
“Snapshot Review of Third Stage Medications” was conducted before the implementation of
the changes, and repeated throughout the study.
A variety of communication tools were designed and used including the minutes of meeting
of the project team; “Risk Assessment for PPH” to standardize the interpretation of risk for all
clinicians in labour ward; regular presentations of the survey findings to the project team and
LDS team; update references material and policy to reflect the actual consumables used to
quantify blood loss.
Team assessment surveys.
2. Project Plan and Execution Stages of Implementation
Initiation Phase The scope of service of the project is to decrease post-partum hemorrhage in
all modes of delivery.
The preliminary idea of the project started in 2016, it was managed by the LDS
Buddy Group, but the approach was not structured and it failed to meet the
objectives. In 2017 to ensure a structured approach and the success of the
project, the LDS Unit Manager identified a new Buddy Group lead to drive the
project, key stakeholders and involved the Quality Department.
Stakeholders were identified; managing stakeholders is a key component of
successful project management and should never be ignored. Proper
stakeholder management can be used to gain support for a project and
anticipate resistance, conflict, or competing objectives.
Planning Phase Brainstorming sessions by the Taskforce clearly indicated the need for
individualised assessment of massive PPHs and an accurate data collection tool.
In addition to this there was a need to perform a Risk Assessment for PPH on
every admission to the unit. It was key to involve all clinicians responsible for
delivering babies on LDS, this included midwives and obstetricians. The PPH
taskforce group put together during the initiation phase communicated the
objectives to these clinicians and laid out clear guidelines of how the project

Clinical Services - Best Project Award 2017 6
Stakeholder Management
Effectively managing stakeholders is a key component of successful project management and should
never be ignored. Proper stakeholder management can be used to gain support for a project and
anticipate resistance, conflict, or competing objectives among the project’s stakeholders. It also gives
the project team a clear understanding of what the stakeholder’s needs and expectations are. This is
done at the initiation stage to allow the team to consider those expectations while planning the
project’s objectives and deliverables.
As part of the requirements to submit the QIP Proposals, project managers were required to do
stakeholder identification and have them included in their communication plan.
Identify Stakeholders The Quality Department led a brainstorming session with the LDS Buddy Group and unit manager
where stakeholders were identified as:
was to proceed. Regular reassessment of findings and updates were essential
and to be ongoing. Audits on administration of uterotonics were to be carried
out to identify any gaps in the process.
Implementation
Phase
A risk assessment tool for PPH and data collection sheets for cases of PPH was
drafted and education of clinicians given. The multidisciplinary daily shift
handover sessions were key to ensuring education and compliance of the
changes was being adhered to. Observational audits on compliance for
administering uterotonics with delivery of the anterior shoulder were also
carried out.
Monitoring and
Controlling Phase
Regular taskforce meetings were held to review cases of PPH and audit findings,
identifying any gaps in management. From this analysis the taskforce were able
to identify areas of improvement in the process which would be incorporated
into updating policy.
Closing Phase A third audit of uterotonic administration is to be completed by the end of
November. A change of uterotonic medication to carbetocin is underway. The
taskforce aims to continue its work on this issue into 2018.

Clinical Services - Best Project Award 2017 7
Different categories of stakeholders were identified:
Patient was identified as the key stakeholder since they are directly affected by the success of the
failure of the project. Any positive or negative outcomes from the project will have a direct impact
upon them.
All clinicians providing care on LDS and OT are key stakeholders because they are planning, providing,
and managing the care. Having their buy-in and commitment guarantees the success of the project.
The clinicians are comprised of two groups:
The midwives who were updated and educated about the objectives of the project
and progress. To ensure their full engagement the PPH rate became a departmental
performance objective in their annual
I-perform.
The physicians and anesthetists were a major stakeholder therefore having their full
commitment was very critical to the project’s success. By having the chairs and chiefs
as part of the project team from conception they were fully engaged with the project.
Operating Theatre/ HDU: For continuity of care, patients with uncontrolled massive bleeding are
usually transferred to these units for continued management. Maintaining an open communication
between these units and LDS is essential for management of information related to the project.
Clinics: Clear communication of the “Plan of Care” of a certain category of patients who require a
specific third stage management might prevent massive blood loss.
Pharmacy: to redefine the management process of third stage medication administration, and
properly manage stock levels.
Post natal units: Primary PPH is defined as massive bleeding within 24 hours of delivery which is why
post natal units are key in documenting and reporting further blood loss.

Clinical Services - Best Project Award 2017 8
Quality Department: was facilitating the project as a part of the team, but as stakeholders the main
role is to provide LDS with timely data, update policies as required, and assign incident reports for
review.
Administration: approve the project and provide high level support if needed.
Key Stakeholders
They key stakeholders who have the most influence over the project are the physicians and the
midwives in LDS and OT. To avoid any resistance to change their buy-in and commitment was
essential. The project team provided regular updates and open communication to manage them
closely throughout the project’s lifecycle.
Stakeholder Analysis
Here, the Stakeholder Management Strategy describes how the project team analysed its list of
identified stakeholders. This discussion included how stakeholders will be categorised or grouped as
well as the level of impact they may have based on their power, influence, and involvement in the
project. There are several tools and techniques that can be used to help quantify stakeholders. A
description of these tools and techniques should also be included in this section.
Department Position Interest (1 – 5)
Power (1 – 5)
Prioritization
A Obstetrics Chair of Obstetrics 5 5 25
B Anaesthesia Chief of Anaesthesia 4 5 20
C Academic Affairs Chief of Academic Affairs 4 5 20
D Obstetric Obstetric Lead for LDS 5 4 20
E Operating Theatre Charge Nurse 2 2 4
F Labour and Delivery Suite
All midwives 3 5 15
G Quality Department Director of Quality 4 3 12
H Pharmacy Senior Clinical Pharmacist 1 3 3
I HDU Unit Manager 1 1 1
J Clinics Unit Manager 1 3 3
K Post natal Units Unit Manager 1 3 3
L Administration Chief Nursing Officer Assistant Director of Nursing
1 5 5

Clinical Services - Best Project Award 2017 9
The stakeholder analysis matrix was used to capture stakeholder concerns, level of involvement, and
management strategy based on the stakeholder analysis and power/interest matrix above. The
stakeholder analysis matrix was reviewed throughout the project’s duration in order to capture any
new concerns or stakeholder management strategy efforts.
Strategy Quadrant Concern Stakeholder
Engaging them at the conception
of the project as team members
Manage Closely
Manage Closely
Manage Closely
Manage Closely
Obstetrics A
Anaesthesia B
Academic Affairs C
Obstetric D
Communicate the project updates
by circulating the minutes
Keep Informed Operating Theatre E
Communicate updates
Recognition through appraisal
system
Keep Satisfied Labour and Delivery
Suite
F
Director of Quality and
Performance Management Officer
as project team members
Keep Informed Quality Department G
Face to face meeting and email
communication when required
Keep Informed Pharmacy H
ga et w ga taae ec f ec eca
ne e a e cai
Monitor HDU I
Face to face meeting and email
communication when required
Keep Informed Clinics J
Post natal Units K
Administration L
3. Develop an organised and comprehensive plan for internal and external communication Meetings are held monthly at a minimum and all meeting minutes are kept as a soft copy and
circulated to the team members with the assigned tasks. Review of minutes with standing agenda
items and progress on assigned tasks are carried out at every meeting.
Situation, Background, Assessment, and Recommendation (SBAR) communication is the tool used at
multidisciplinary handover meetings every morning to communicate internally all PPHs within the
last 24 hours. The patient MRN is used to communicate this information and the meetings are held
in a private setting involving only the concerned clinical team to ensure patient confidentiality.

Clinical Services - Best Project Award 2017 10
The progress of the project is discussed as a Buddy Group feedback standing item at the LDS monthly
meetings.
All new changes to the process are communicated to the LDS team by developing tools and
communicating the changes verbally through buddy group education.
To avoid communication constraints and communication based conflicts the following meeting date
and time are decided at the end of each meeting with team consensus. All minutes are circulated to
the members; an email group was created including all the team members called “PPH Taskforce” so
that none of the team members are missed out from any communication. There were different
channels of communication throughout the project:
1. Communication related to assigned actions are reviewed at every meeting and circulated by
email to all team members.
2. Progress on individual tasks and action items is relayed back by email and discussion at the
next meeting.
Communication
Type
Objective of
Communication
Frequency Audience Owner Deliverable Medium/ Format
Kickoff Meeting Introduce the
project team
and the project.
Review project
objectives and
management
approach.
Once Project
Sponsor
Project Team
Stakeholders
Project
Manager
Agenda
Meeting
Minutes
Soft copy archived
on project
SharePoint site
and project web
site
Regular
meetings
Follow on the
tasks and
review results to
plan for future
actions
Minimum
monthly
Project Team Project
Manager
Agenda
Meeting
Minutes
Adhoc meetings Communicate
project
requirements
with the
stakeholders in
the “Keep
Informed” grid
Ad Hoc Other units Project
Manager
Email Email
communication

Clinical Services - Best Project Award 2017 11
4. Develop a quality assurance plan (Continuous Quality Improvement Plan
The main purpose of the Project Quality Management Plan for the QIPs is to document necessary
information required to effectively manage project quality from project planning to delivery. It
defines the projects quality policies, procedures, criteria and areas of application, roles, and
responsibilities.
In the first section the plan focuses on identifying and clearly describing the primary roles and
responsibilities of the project staff as it relates to the practice of Project Quality Management.
Indicates responsibilities for activities such as mentoring or coaching, auditing work products,
auditing processes and participating in project reviews.
Name Role Quality Responsibility
Jill Henry Project Manager Quality mentoring & coaching
Valentina Stefanoni Team Lead Quality audits; Data collection
Anu Ravi Team member Quality audits; Data collection
Eman Mashal Team member Quality audits; Data collection
Sumitha Zachariah Team member Quality audits; Data collection
Maria Thomas Team member Quality audits; Data collection
Rita Arslanian Project Coordinator Meeting minutes ; Compliance with project
charter
Dr. Saleema Wani Team member Subject matter expert; Ensure obstetric support
Dr. Margaret Blott Team member Subject matter expert
Survey Findings Communicate
survey findings
When data is
available - at
unit meeting
LDS Midwives Project
Manager
Power point
presentation
Soft copy archived
on project
SharePoint site
and project web
site
Quality Board
Project Status /
Progress
Communicate
project progress
and changes in
KPI scores
Monthly at
unit
meeting

Clinical Services - Best Project Award 2017 12
Dr. Tarek Ansari
Dr. Soha Said
Dr. Priya Sequeria
Dr. Reem Taha
In the second section the plan focuses on listing and defining the data requirements and the quality
tools that will be used to measure the quality of the project and conformance with the defined
indicators.
Tools Description
Literature review http://www.rcog.org.uk/womens-health/clinical-guidance/maternity-dashboard-clinical-
performance-and-governance-score-card
Intramuscular Oxytocics: A Comparison Study of Intramuscular Carbetocin, Syntocinon and Syntometrine for the Third Stage of Labour Following Vaginal Birth (IMOX) North Bristol NHS Trust Carbetocin for the Prevention of Postpartum Hemorrhage D. Cordovani, J. C. A. Carvalho, M.
Boucher and D. Farine
Paerto Diagram Survey was conducted regarding the time of administration of the Uterotonics and to identify
why they were not given with anterior shoulder. The reasons were clustered by categories and
action plans were implemented to address the main 2 categories.
Learn from experience of
other SEHA BEs
Other SEHA BE Labour & Delivery Units were approached to identify their third stage
medication management. A uterotonic Carbetocin was the medication of choice by the
majority. Unfortunately they could not provide the data surrounding the subsequent
implementation of the medication.
Lessons learned from previous projects
Brainstorming session with the team who tried to implement the project last year to identify
the pitfalls
Obstetric Drills Multidisciplinary unit based obstetric emergency drills incorporating management of PPH were
increased on LDS. Scores improved accordingly.
Education An audio visual teaching tool on the management of PPH was compiled by a group of LDS
midwives. This was presented at the multidisciplinary morning meeting and is available for staff
reference on the Intranet.

Clinical Services - Best Project Award 2017 13
This graph
demonstrates
the outstanding
improvement on
how clinical staff
performed
during unit based
Obstetric PPH
drills
The team conducted a brainstorming session and detailed analysis of the primary reasons leading
to high PPH, delay in administering a uterotonic was identified as a possible leading cause.
Therefore an audit was conducted as a Snapshot Review of Third Stage Medication for 70 vaginal
deliveries (22%) in April to confirm the assumption and to identify the reasons for the delay.
Observational assessment was done in April and it indicated that 63% of Uterotonics were given
appropriately, whereas 37% were not. A breakdown analysis of the 37% was done and indicated
that the primary reason not administering the uterotonics appropriately was PPID (47%) (Positive
Patient Identification) this is an automated medication dispensing system (Pyxis) and the process
time is longer than the timeframe for administering the medication. Staff being busy with other
tasks (30%) was the second most common reason (see the table below). The LDS management
raised awareness of the importance of prioritising tasks properly and simultaneously discussed with
pharmacy the feasibility of overriding the PPID for uterotonics and that they be classified as
emergency medication. To assess and refine, the survey was repeated after 4 months in August
observing 78 vaginal deliveries (23%), unfortunately the results showed a decrease in compliance
to 58% and PPID remained the main contributing factor but it decreased to 23%, and the second
contributing factor was still other tasks but it also decreased to 16%. To further assess and refine
ongoing education the audit will be repeated in November.

Clinical Services - Best Project Award 2017 14
A. Definition and measurement of Quality

Clinical Services - Best Project Award 2017 15
B. Continuous Improvement – RADAR
The EFQM RADAR logic is adopted by Corniche Hospital as the roadmap to continuous quality
improvement and to assessing the maturity of the approaches implemented and the excellence of
the results achieved.
C. Sustainability
Sustainability is a part of the Assess and Refine phase of the RADAR and it is conducted throughout
the life cycle of the project. Sustainability is also related to how well the project is closed and handed
over to the Operations, as soon as that occurs it is the responsibility of the Unit/ Department Manager
to continue monitoring and keeping track of the performance indicators. As a part of its oversight to
the projects the Quality Department will ask the Quality Ambassadors to discuss those KPIs in Quality
Ambassadors Meeting on a Quarterly Basis. The Quality Department might conduct random audits
and look for track of monitors for closed projects during the tracer activities.
• Stakeholder involvement
• Communication and education
• Assessment through survey
• Indidual case reviews
• Retrospective analysis of PPH cases
• Analysis of individual PPH cases in multudisciplinary teams
• Detailed assessment of the management of PPH
• Identification of the root causes
•
• In 2016, the rate of PPH ≥2000𝑚𝑙𝑠 𝑤𝑎𝑠 1.15%,𝑎𝑛𝑑 PPH ≥
1500𝑚𝑙𝑠 𝑤𝑎𝑠 2.55%,
•Reduce the rate of massive PPH ≥ 1,500 ml to below 1.5% (as a
stretch goal)
ResultsHow do you need to
Approach the problem to get the
results you need
DeployAssess
and Refine

Clinical Services - Best Project Award 2017 16
The Second Criteria: Project Team
Manage and Lead Project Team
The foundation of the team was the Midwifery Buddy group, which was selected specifically because
of the team’s high interest and self-motivation to move the project forward and guarantee its
success. The project objectives are linked to the mid-year and annual performance appraisal of the
midwives to hold them accountable and recognise their efforts simultaneously.
The physician leads were selected to be on the team because of their expert opinion and authority
to adapt, implement policy, and cascade information about the project to the physicians and
safeguard the sustainability of outcomes. As for the quality team, their involvement in the team was
crucial to coordinate the project and keep it on track.
To avoid conflict due to vagueness of roles which might result in delays of completion of tasks, all
roles and responsibilities were assigned clearly for all team members. At every meeting the tasks
were discussed and reviewed. The following responsibility assignment matrix RACI was used to shows
the relationship between project tasks and team members. Any proposed changes to project
responsibilities was reviewed and approved by the project manager and the Corniche Leadership
Team member owning the project.
Task List Jill Henry Valentina and Buddy
Group
Dr. Saleema Wani
Quality Department
(Rita Arslanian Jane Kelly)
Rest of the team
Risk Assessment Plan R R I A I
Quality Management Plan R R I A I
Data collection and analysis tool
AI R CI R CI
Developing forms to discuss and hand over all blood loss cases in a shift
AC R RC R CI
Develop survey tool, conduct and analyze the survey – Snapshot Review of Third Stage Medication
AC R I I I

Clinical Services - Best Project Award 2017 17
Key: R – Responsible for completing the work A – Accountable for ensuring task completion/sign off C – Consulted before any decisions are made I – Informed of when an action/decision has been made
The main challenge was engaging the team from theater and committing them to the project as team
members. Out of the 11 meeting there was only 2 meetings with OT nursing representation, after
the 8th meeting the Chair of Anesthesia joined the project team representing anesthesia and OT.
Since the roles and responsibilities were very clearly defined and tracked there was very little room
for conflict.
The efforts of the buddy group are directly linked to their annual appraisal, and the team receives
thank you cards in recognition of their commitment to the project.
Risk assessment reference tool
A R C I CI
Dry weight consumable reference tool
A R I I I
Create PPH taskforce mailing list and shared drive
CI CI CI RA CI
Overriding PPID for uterotonic medication administration
AR I I I I
2016 and 2017 data analysis I I RI AR I
Clarify definition of Post-Partum Hemorrhage and calculation criteria
I I RC ARI CI
Coordinate with all post-natal units and HDU to standardize quantitative blood loss measurement
AR I I I I
Coordinate with all post-natal units and HDU to report back blood losses in the units
AR I I I I
Literature review I R R I R

Clinical Services - Best Project Award 2017 18

Clinical Services - Best Project Award 2017 19
The Third Criteria: Resource Management and Control
1. Manage financial resources related to the project
The final recommendation was to change the uterotonic medication to a more expensive
alternative, Carbetocin 100mcg which is already on SEHA Formulary.
Clinical time, stationary and meeting room space were the only notable expenditures
2. Manage and direct knowledge resources and identify a systematic and comprehensive plan
Taskforce meetings were minuted and circulated to the PPH Taskforce group using the
collective contact group address which had been set up at the onset of the project. Minutes
detailed action responsibilities and timelines. All action points were reviewed at each meeting
and updates shared. The group contact address was used to share research articles and any
new developments. Laterally the shared drive was accessible for referencing each PPH case
dating back to January
3. Manage and direct suppliers
Name of group member and
designation
Reason chosen
Jill Henry - LDS Unit Manager LDS Unit Manager and the department’s performance directly impacts the PPH rate
Valentina and Buddy Group – LDS
Buddy Group
LDS Buddy Group and driver of change to improve the performance which directly impacts the PPH rate
Jane Kelly – Director of Quality Quality department measures the performance
Rita Arslanian – Performance
Management Officer
Coordinator for the project
Chairs and Chiefs of Departments
and Consultants
The physicians performance directly impacts the PPH rate and for expert
advice

Clinical Services - Best Project Award 2017 20
Suppliers of Carbetocin have been contacted by our pharmacy to confirm adequate ongoing
availability for our needs when we transfer to this uterotonic. Supplies are sufficient and a
review of stocks of current uterotonics have taken place to identify a timeframe for the
crossover
4. Assure optimum Resources use
Actual Benefits (Effectiveness) Actual Costs
1. Positive outcomes Reduction in PPH rates
Reduced resources utilization (cost, manpower, and physician
resources)
PPH rates with will aligned with international best practices as a center
of excellence for high risk obstetric care
2. Resources Expanded Cost of new medication Cost of stationary Cost of clinical time
3. Negative outcomes avoided Short/long term negative outcomes avoided Increase of patients’ complaints due to complex process in discharging
the patients.
4. Negative outcomes
Patient identification process
Project Dependent Project Independent Observed Impacts
X Increased awareness throughout the disciplines
X Increased staff engagement and interest to improve
reduce the rate of PPH
X Updated knowledge on the latest clinical trials
X Improved patient safety
Enabling Factors Hindering Factors
All stakeholders were highly engaged and involved. The project plan and implementation was well structured. Effective communication by regular updates, feedback, and meetings.
Difficulty getting information related to PPH medication and
management from other SEHA facilities.
Lengthy internal process to introduce a change in medication
Lengthy process to override PPID for third stage medication

Clinical Services - Best Project Award 2017 21
The Fourth Criteria: Risk Management and Project Sustainability
Risk management is essential to effectively manage a project, and describes what is needed before
risk management can begin. Risk management should be done at the beginning of the project,
during the mid-project review, if there are any changes in scope, and once the project is closed
and handed over to operations.
Risk Identification
At the initiation phase of the project, the new Buddy Group responsible for the
implementation of the project had a structured risk assessment meeting with a
representative from the previous project group and subject matter expert.
The “Risk Assessment” meeting was minuted and a risk assessment tool was used to identify
the occurrence, severity, and detection of each risk. For every detected risk the team voted
for the type of strategy to address the risk (accept, mitigate or avoid it), and devised
strategy to address each risk.
The risks were divided into three main categories:
a. Historical review of similar
b. Risks which can delay or hinder the project
c. Risks which are an outcome of the project and can have a negative impact on the
operations

Clinical Services - Best Project Award 2017 22
Risk Qualification and Prioritization
Risk Identified Risk Type Occurrence Severity Detection Priority Strategy to address the risk
Less
on
s Le
arn
ed
fro
m p
revi
ou
s p
roje
ct
No robust planning Management related
1 4 1 4 Avoid
No ownership of the project, the project was led by a buddy group and then handed over to a lead who was not a part of the initial group
Management related
3 5 1 15 Avoid
No delegation Management related
3 5 1 15 Avoid
No clarity in roles and responsibilities
Management related
3 5 1 15 Avoid
Lack of clear communication
Management related
3 5 1 15 Avoid
No commitment from the subject matter experts
Physician related
4 5 3 60 Mitigate
Changes were not supported by the LDS education department ( Staff education)
Midwife related
2 5 1 10 Avoid
Lack of buy in of the key stakeholders
Physician related
3 5 1 15 Avoid
Was not linked to individual performance appraisal as a motivating factor
Midwife related
3 5 1 15 Avoid
Pro
ject
Co
mp
leti
on
Ris
ks
Poor attendance at the regular meetings which delay follow-up on completion of planned actions and hinders communication
Management related
4 5 1 20 Avoid
Response rate to the survey
Midwife related
3 5 2 30 Avoid
LDS staff compliance and commitment
Midwife related
3 5 1 15 Avoid
OR staff commitment and buy-in
Physician related
4 5 3 60 Avoid

Clinical Services - Best Project Award 2017 23
Post- natal ward commitment and buy-in
Unit Managers 5 5 1 25 Avoid
Physician commitment and buy-in
Physician related
5 5 1 25 Avoid
Challenges in communication with medical team for issues related to the project (physicians)
Physician related
5 5 1 25 Mitigate
Pro
ject
Ou
tco
me
Ris
ks
Medication identification errors due to non- PPID of uterotonics
Midwife related
1 5 5 25 Avoid
Misinterpretation of “Risk Assessment for PPH Tool”
Midwife related Physician related
1 3 3 9 Avoid
Risk Monitoring
The “Risk Assessment” meeting was recoded and a risk assessment tool was used to identify
the occurrence, severity, and detection of each risk. For every detected risk the team voted
for the type of strategy to address the risk (accept, mitigate or avoid it), and devised strategy
to address them.
The risks with the highest scores to the project schedule were given high priority and
addressed at the planning phase of the project and all risks were monitored and reviewed at
the monthly meetings.
Clinical Services - Best Project Award 2017 24
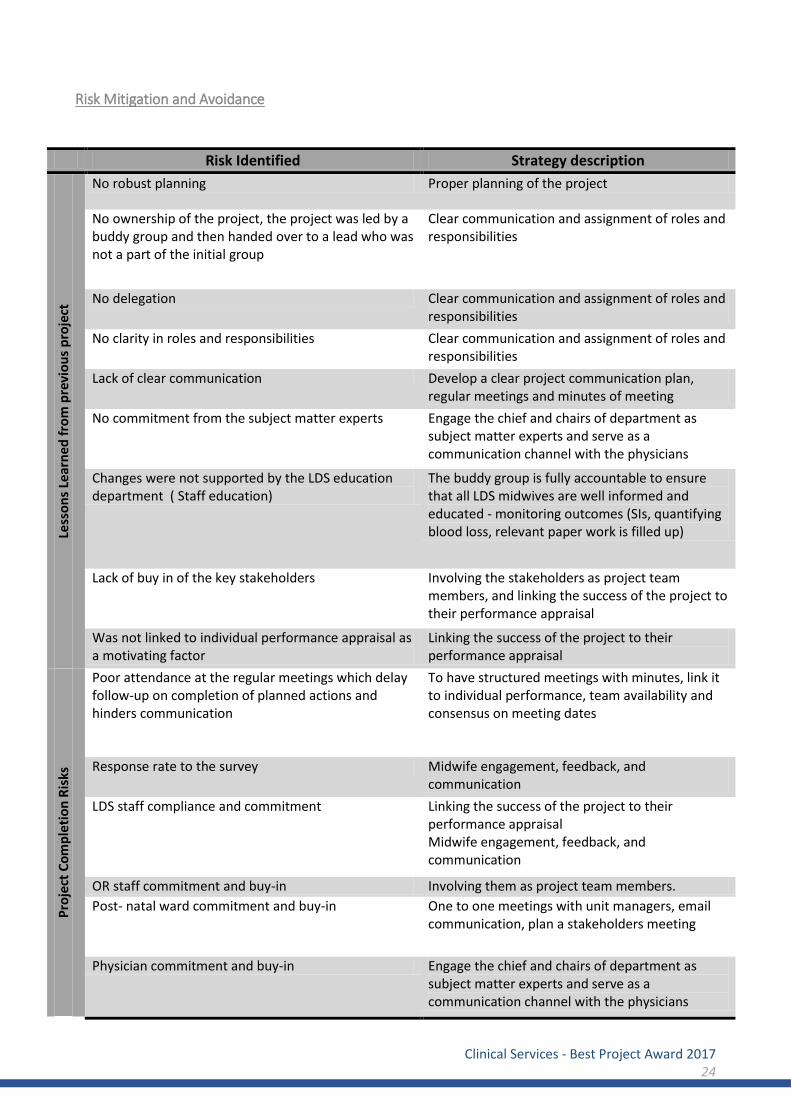
Risk Mitigation and Avoidance
Risk Identified Strategy description
Less
on
s Le
arn
ed
fro
m p
revi
ou
s p
roje
ct
No robust planning Proper planning of the project
No ownership of the project, the project was led by a buddy group and then handed over to a lead who was not a part of the initial group
Clear communication and assignment of roles and responsibilities
No delegation Clear communication and assignment of roles and responsibilities
No clarity in roles and responsibilities Clear communication and assignment of roles and responsibilities
Lack of clear communication Develop a clear project communication plan, regular meetings and minutes of meeting
No commitment from the subject matter experts Engage the chief and chairs of department as subject matter experts and serve as a communication channel with the physicians
Changes were not supported by the LDS education department ( Staff education)
The buddy group is fully accountable to ensure that all LDS midwives are well informed and educated - monitoring outcomes (SIs, quantifying blood loss, relevant paper work is filled up)
Lack of buy in of the key stakeholders Involving the stakeholders as project team members, and linking the success of the project to their performance appraisal
Was not linked to individual performance appraisal as a motivating factor
Linking the success of the project to their performance appraisal
Pro
ject
Co
mp
leti
on
Ris
ks
Poor attendance at the regular meetings which delay follow-up on completion of planned actions and hinders communication
To have structured meetings with minutes, link it to individual performance, team availability and consensus on meeting dates
Response rate to the survey Midwife engagement, feedback, and communication
LDS staff compliance and commitment Linking the success of the project to their performance appraisal Midwife engagement, feedback, and communication
OR staff commitment and buy-in Involving them as project team members.
Post- natal ward commitment and buy-in One to one meetings with unit managers, email communication, plan a stakeholders meeting
Physician commitment and buy-in Engage the chief and chairs of department as subject matter experts and serve as a communication channel with the physicians

Clinical Services - Best Project Award 2017 25
Challenges in communication with medical team for issues related to the project (physicians)
Communicate through Chiefs and chairs and hold the chiefs and chairs accountable
Pro
ject
Ou
tco
me
Ris
ks
Medication identification errors due to non- PPID of uterotonics
Reinforce medication and patient identification policy
Misinterpretation of “Risk Assessment for PPH Tool” Review of the tool and education

Clinical Services - Best Project Award 2017 26
The Fifth Criteria: Project Execution
Develop a system for Managing Records and project activities and assure document support and
operation execution, control, review, update and develop solutions and preventive and corrective
action
Individual PPH data collection sheet
This form was designed at the onset of the project in an attempt to capture individualised cases
of PPH >1500mls. The form was used for all modes of delivery in accordance with KPI criteria.
Education of the multidisciplinary team was provided, stakeholders included. This form became
a part of the LDS based multidisciplinary team handover. If forms had not been completed or
submitted then the primary caregiver was approached and requested to do so. This change took
time to achieve full compliance however it is now embedded in practice.

Clinical Services - Best Project Award 2017 27
Monthly PPH data collection sheet.
From the individualised form the data was transferred to the monthly data collection sheet
above. This was managed by the Buddy Group and used for breakdown and comparison analysis
which was fed back to the Taskforce meetings. From October we have refined the process
further and now collect all information on an excel spreadsheet.
Project closure
The PPH Taskforce and Buddy Group have proved so successful with their focus on this topic
that the plan is to continue into 2018. Risk assessment has proved a valuable tool and prompted
the clinicians to review the patients’ risk of PPH on arrival to the unit. This is an ongoing
assessment during labour and risk factors may and can change dependent on situation. This
ultimately impacts management of the case in an individualised approach. We hope to develop
this tool as we collate further data.
Individual Data collection tool has proved invaluable and will continue. We are happy with the
layout and now have 100% compliance in completing the form from the primary clinicians.
An excel spreadsheet will help us review our data collection and with the help of our Quality
Department we hope to develop this further as the project matures.
The Taskforce feel that it is essential to continue with regular meetings, these will be held a
minimum of once per month.
The approval and introduction of Carbetocin 100mcg is imminent and will require a committed
analysis following implementation. The clinical and financial benefit will be scrutinized, which
will be carried out over a three month period to assess the clinical impact.
Policy changes have been drafted in line with the above mentioned changes and will be finalised
following the change over to carbetocin.

Clinical Services - Best Project Award 2017 28
Quantitative blood loss calculation is a robust process on both LDS and OT and shall continue.
The reporting system of PPH is robust and shall continue
Lessons Learned From Previous Projects
No robust planning
No ownership of the project, the project was led by a buddy group and then handed over to
a lead who was not a part of the initial group
No delegation
No clarity in roles and responsibilities
Lack of clear communication
No commitment from the subject matter experts
Changes were not supported by the LDS education department ( Staff education)
Lack of buy in of the key stakeholders
Was not linked to individual performance appraisal as a motivating factor
Lessons Learnt from the current Project
Process Improvement Recommendations:
Full Taskforce attendance at meetings
Action issues completed within timeframe
Audit compliance
Category Issue Problem/Success Impact Recommendation
Stakeholder Buy in Not all stakeholders fully committed to project
Failure to attend Taskforce meetings and provide valuable input
Moderate – loss of valuable knowledge
Ensure each area chooses a committed and motivated individual
Communication Failure to complete individualised data collection form
Initially when the PPH data collection tool was implemented not all cases were reported
High – cases not reported back to multidisciplinary team for review
Increased awareness through SBAR
Audit of third stage medication administration
Length of time to collect Although midwives were aware of the audit many did not complete the form
Moderate – caused a delay in analyzing contributing factors
As a new patient arrives in the department the form is automatically handed into the delivery room by the ward clerk
Research Review Too many members undertook to do this
Delay in feeding back research findings to Taskforce
High - Delay in planning and decision making
Nominate and delegate appropriately

Clinical Services - Best Project Award 2017 29
Post Project Review
Transition to Operations:
The taskforce and Buddy Group shall continue to develop the project into 2018. Both groups wish
to retain the same member group and as we have a variety of key people in the Taskforce
membership shall remain unchanged. The advantage of this will allow the transition into the coming
year to be unhindered with all members aware of ‘where we are at’ and the progress that has been
made.
Planned Deliverable Actual Deliverable Summary
Reduce the rate of massive PPH ≥ 1500 mls to below 1.5%
We have successfully categorised and
compared risk factors and causes. This vital
step has enabled us to analyse the way
forward to further reduce our PPH rates.
Our approach to PPH is standardised and
embedded. Awareness amongst clinicians
is extremely high.
We are reassured that by implementing changes in management through our project there has not been an increase in rates. The month to month results have not reduced as significantly as we had hoped however we appreciate that in this high risk tertiary setting we have unique challenges. Our mission as a Taskforce is to continue to combine our expertise in obstetrics and explore all avenues for continued improvement.
Analyse and redesign processes and procedures to facilitate clinical management of PPH
Increased education, obstetric drills scenarios and case reviews have allowed us ample scope to redesign and analyse our processes and procedures processes
We are satisfied with the clinical multidisciplinary approach to management of PPH. The teamwork is coordinated and follows policy
Update policies and procedures to reflect best practice
Policies updated to reflect current practice Policies and procedures will need further update following change of uterotonic. Research has also highlighted there may be a need to change the order of our PPH medications.

Clinical Services - Best Project Award 2017 30
The Sixth Criteria: Results
Project KPIs and results
Project Effect Indicators
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
% P
PH
% PPH ≥ 2,000 ml (2016 - 2017)
2016 2017

Clinical Services - Best Project Award 2017 31
This graph demonstrates a breakdown of Risk Assessment for all
women admitted to LDS that subsequently had a vaginal delivery
and PPH of ≥1500mls
This graph demonstrates a breakdown of causes in the above population of PPH.
This graph demonstrates a breakdown of the group identified in labour as low risk and their mode of vaginal delivery.
This graph demonstrates a breakdown of the group identified in labour as low risk and the cause of PPH (LSCS not included as this will always be due to atony).
This graph demonstrates a breakdown of the group
identified in labour as low risk that had a Cesarean
delivery.

Clinical Services - Best Project Award 2017 32
Project Team Indicators:
Project Team Evaluation; from the 13 evaluation forms we received 11 back
Strongly agree
Agree Neutral Disagree Strongly disagree
The project objectives were clear to all team members
11
The team had adequate skill mix and member resources to complete the tasks and achieve the objectives
11
The meetings were well attended by all the team members
4 3 3 1
The project manager was approachable
11
The meetings were run efficiently 8 3
Tasks were fairly divided among tam members
6 5
The team worked well together 9 2
.