clinical study of ziabetus shakari (diabetes mellitus type ... · wadood, dr. ghulamuddin sofi, dr....
TRANSCRIPT

I
Clinical Study of Ziabetus Shakari (Diabetes Mellitus Type II)
and Evaluation of Efficacy of a Unani Formulation in its
Management
by
QUTUBUDDIN
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillment
of the requirements for the degree of
MAHIRE TIB
(MD Unani)
in
MOALAJAT
(Medicine)
Under the guidance of
Dr. Mohd Anwar
Department of Moalajat
National Institute of Unani Medicine
Bangalore
2012

II
Rajiv Gandhi University of Health Sciences, Karnataka
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “Clinical Study of Ziabetus Shakari
(Diabetes Mellitus Type II) and Evaluation of Efficacy of a Unani Formulation in
its Management” is a bonafide and genuine research work carried out by me under
the guidance of Dr. Mohd Anwar, Reader, Department of Moalajat, National
Institute of Unani Medicine, Bangalore.
Date:
Place: Bangalore Qutubuddin
III
National Institute of Unani Medicine (Dept. of AYUSH, Ministry of Health & Family Welfare, Govt. of India)
Kottigepalya, Magadi Main Road, Bangalore-91 Telephone: 080-23584260, Ext: 262, Telefax: 080-23580725
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “Clinical Study of Ziabetus
Shakari (Diabetes Mellitus Type II) and Evaluation of Efficacy of a Unani
Formulation in its Management” is a bonafide research work done by Qutubuddin
in partial fulfillment of the requirement for the degree of Mahire Tib (MD Unani) in
Moalajat (Medicine) under my supervision and guidance.
Dr. Mohd Anwar
Reader
Department of Moalajat
Date: National Institute of Unani Medicine
Place: Bangalore Bangalore
IV
National Institute of Unani Medicine (Dept. of AYUSH, Ministry of Health & Family Welfare, Govt. of India)
Kottigepalya, Magadi Main Road, Bangalore-91 Telephone: 080-23584260, Ext: 262, Telefax: 080-23580725
ENDORSEMENT BY THE HOD AND HEAD OF THE INSTITUTION
This is to certify that the dissertation entitled “Clinical Study of Ziabetus Shakari
(Diabetes Mellitus Type II) and Evaluation of Efficacy of a Unani Formulation in its
Management” is a bonafide research work done by Qutubuddin under the guidance
of Dr. Mohd Anwar, Reader, Department of Moalajat, National Institute of
Unani Medicine, Bangalore.
Prof. Mansoor Ahmad Siddiqui Prof. M. A. Jafri
Head Director
Dept. of Moalajat National Institute of Unani Medicine
National Institute of Unani Medicine Bangalore
Bangalore
Date: Date:
Place: Bangalore Place: Bangalore
V
COPYRIGHT
Declaration by the Candidate
I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka shall
have the right to preserve, use and disseminate this dissertation / thesis in print or
electronic format for academic / research purpose.
Date:
Place: Bangalore Qutubuddin
©Rajiv Gandhi University of Health Sciences, Karnataka

Acknowledgement
VI
ACKNOWLEDGEMENT
All praises be to “Almighty Allah” the lord of the world, the most beneficent and merciful
and peace be upon his Prophet Mohammed (SAWS). Through the grace of Almighty Allah, the
uphill task on my shoulder has been accomplished.
The completion of this dissertation is not only fulfilment of my dreams but also of my
parents who have sacrificed a lot for me in completion of this course. The writing of a dissertation
is obviously not possible without the support and company of numerous people. It is a pleasant
aspect that I have now the opportunity to express my gratitude for all of them.
It gives me immense pleasure to express my deep sense of gratitude and sincere respect to
my teacher and guide, Dr. Mohd Anwar, Reader, Department of Moalajat, National Institute of
Unani Medicine, Bangalore, for his sustained sincerity, precious guidance, vigorous suggestion,
constructive criticism, extra efforts and immense help without which I could not be able to
complete this dissertation. I acknowledge his intelligent, diligent and serious help in transforming
these would be fantastic ideas into comprehensive and logical statements which are in front of you
as a dissertation.
I express my sincere thanks to Prof. M A Siddiqui, HOD Department of Moalajat, NIUM
Bangalore, for providing necessary facilities to carry out the work smoothly. I extend my profound
respect and regards for his guidance, suggestions, moral and material support.
I take this opportunity to express my deep sense of gratitude and obligation to Director
NIUM, Prof. M. A. Jafri for kindly permitting me to do this study and providing the best possible
facilities that led to successful completion of my project.
I am very thankful to all my teachers, Dr. Tanzeel Ahmad, Dr. Aleemuddin Quamri, and
Dr. Abdul Nasir Ansari Reader, Lecturers, Department of Moalajat for their kind support,
guidance and valuable suggestions.
I wish to acknowledge my deep sense of gratitude to my esteemed teachers Dr. Abdul
Wadood, Dr. Ghulamuddin Sofi, Dr. Nasreen Jahan, Dr. Najeeb Jahan, Dr. Arish Sherwani, Dr.

Acknowledgement
VII
Abdul Haseeb Ansari, and from different Department of NIUM, and Clinical Registrars Dr.
Shakeel Ansari and Dr. Mohd Azam, for his help during compilation of the dissertation work.
I am also highly obliged to my colleagues who gave me moral and friendly support
whenever I felt exhausted. Dr. Mohammad Ali, Dr. Md Razaur Rasheed. Dr Abdur Rasheed, Dr.
Mushta Ali, Dr. Nadim Ahmad, Dr. A H A Fazeena, Dr. Firoz Khan, Dr. Farhan Hussain, Dr.
Mateen Ahmad, Dr. Mujassam, Dr. Azeez, Dr. Zahid, Dr. Athar and Dr. Raudas deserve all of
my praises.
I also express my thanks to all my seniors especially Dr. Mohd Nayab, Dr. Abdul Azeez
Faris, Dr. Shamim Akhtar, Dr. Rafiuddin, Dr. Shamim Rather, Dr. Nusrath Fatima, Dr. Akhtar
Hussain Jamali as well as juniors Dr. Asim Khan, Dr. Mohd Yasir, Dr. Aslam, Dr. Sheeraz, Dr.
Imtiyaz, Dr. Nasimul Hasan, Dr. Sarfaraz, Dr. Humaira Tabassum, Dr. Arshid, Dr. Kamal, Dr.
Sadique and Dr. Shamim who helped me in every step to complete this dissertation.
I would fail in my duty if I do not express my heartfelt and sincere thanks to to Dr.
Renuka BN, Pathologist Hospital Laboratory for her kind support, advice and showing practical
interest in my laboratory work. I owe my sincere thanks to hospital laboratory staff, Biochemist,
Mrs. Sanjeeda Tabassum, Mr. Haneef, and Mr. Zaki and for helping me in my laboratory work. I
would like to thank pharmacy staff Dr. Nafees Khan, Chief Pharmasist, Mr. Fazil, and Mr.
Kashif for providing best quality drugs.
I express my intense sense of thanks to library staff Mr. Ehtisham and Mr. Mudassir for
their co-operation during literature survey, keeping the required books handy and out of the way
support at the hour of desperate need.
To Ahmadi Begam and Sharfuddin Khan my beloved parents, my role models: First, I’d
like to thank you for bringing me into this world, instilling good values and beliefs in me,
providing me with all the necessities of life, and with an education. Thank you for your never-
ending support, wisdom, prayers, and encouragement, for being a listening ear, for giving me
advice- be it warranted or not, for being an outlet for my emotions, for making me laugh, and for
Acknowledgement
VIII
wiping my tears. Thank you for ingraining the faith of almighty Allah in my heart. For without
him, all of this would be null and void. Thank you for making me the person I am, because
without you I wouldn’t be where I am today. My hope is that one day I become even half as good
a parent as each of you has been to me. May Allah bless you with the best of this life and the
hereafter- Aameen.
I owe a debt of gratitude to my sisters Mohsina Khatoon, Nasira Khatoon, Rabiya
Khatoon and my younger brothers Naseer, Raees and Zubair for their indispensable aid, moral
support, encouragement, unfailing courtesy and everlasting love that served a source of my
inspiration, strength, determination and enthusiasm at each and every front of my life to transfer
my dreams into reality.
My acknowledgment would remain incomplete without making a special mention for the
sustained encouragement and sympathy that I received from my dearest friends, Dr. Abu Bakar,
Dr. Shaikh Haneef, Dr. Waris Ali, Dr. Mohd Asif, Dr. Noor Muzammil, Paigam, Shuaib,
Mahmood, Shamsheer, without which this dissertation would never have seen the light of the day.
Last but not the least; I convey my heartfelt gratitude to all the patients, without whose
co-operation, this study would not be possible.
It is not possible to acknowledge individually all of my friends and colleagues who helped
me in various ways and in different aspect of the study, nevertheless, I am grateful to all of them
and at the same time I express my apology for all those whom I could not mention by their names.
Lastly, I pray to Almighty Allah to show me the right path, the path of those whom He
has favoured and not the path of those who earn His anger or those who go astray-Aameen.
Date: 5-03-2011
Place: Bangalore Qutubuddin
IX
List of Abbreviations and Symbols Used
A. D. Anno Domini (after the
birth of Christ)
ADA American diabetes
association
ALT Alanine amino transferase
AST Aspartate amino
transferase
AT After treatment
B.C Before Christ
BT Before treatment
CRF Case Report Form
cu mm cubic millimeter
dl Deciliter
DLC Differential Leucocytes
Count
Dr Doctor
ECG Electro cardiogram
ed Edition
IRS Insuline receptor
substrates
IU/L International Unit per
Liter
e.g. Exempli grati (for
example)
et al. Et alii or et alia (and
others)
etc. et cetera
FBS Fasting Blood Sugar
F Female
GHI Glucagon-like peptide
Hb Haemoglobin
HDL Hight Density
Lipoprotien
HTN Hypertension
ICMR Indian council of medical
research
IDDM Insulin Dependent
Diabetes mellitus
IDF International Diabetes
Federation
i.e. idest (that is)
IFG Impaired Fasting Glucose
IHD Ischemic Heart Disease
Kg kilogram
KFT Kidney Function Test
LFT Liver Function Test
LDL Low Density Lipoprotein
M Male
MODY Maturity onset diabetes of
young
mg/dl milligram per deciliter
mg milligram
n Total Number
NIDDM Non Insulin Dependent
Diabetes mellitus
ns Not Significant
OGTT Oral glucose tolerance
test
OPD Out Patient Department
p Probability of error
PNM Print Not Mention
PPBS Post Prandial Blood
Sugar
S Significant
SES Socioeconomic Status
SEM Standard Error of Mean
S. No. Serial Number
Tab. Tablet
TLC Total Leucocyte Count
TNF Tumour necrosis factor
Vol. Volume
YNM Year Not Mentioned
X
List of Contents
S. No. Topic
Page No.
1
Introduction
1-5
2 Aims & Objectives
6
3 Review of Literature
7-59
4 Materials and Methods
60-66
5 Observations and Results
67-90
6 Discussion
91-101
7 Conclusion
102-103
8 Summary
104-108
9 Bibliography
109-122
10 Annexure
123-140

XI
List of Tables
S. No. Titles Page No.
1 Distribution of Patients According to Age 67
2 Distribution of Patients According to Sex 68
3 Distribution of Patients According to Religion 69
4 Distribution of Patients According to Marital Status 70
5 Distribution of Patients According to Family History 71
6 Distribution of Patients According to Socio Economic Status 72
7 Distribution of Patients According to Diet 73
8 Distribution of Patients According to Mizaj 74
9 Distribution of Patients According to Duration of Illness 75
10 Distribution of Patients According to Treatment History 76
11 Effect on Polyuria 77
12 Effect on Polydipsia 78
13 Effect on Polyphagia 79
14 Effect on Tiredness 80
15 Effect on Progressive weakness 81
16 Effect on Dizziness 82
17 Effect on Unexplained Weight Loss 83
18 Effect on Pruritus 84
19 Effect on FBS 85
20 Effect on PPBS 86
21 Effect on Urine Sugar 87
XII
S. No.
Titles
Page No.
22 Effect on HbA1c 88
23 Effect of Test drug on safety parameters 89
24 Effect of Control drug on safety parameters 90
List of Figures
S. No. Titles Page No.
1 Distribution of patients according to Age 67
2 Distribution of patients according to Gender 68
3 Distribution of patients according to Religion 69
4 Distribution of patients according to Marital Status 70
5 Distribution of Patients According to Family History 71
6 Distribution of patients according to Socio Economic Status 72
7 Distribution of Patients According to Diet 73
8 Distribution of patients according to Mizaj 74
9 Distribution of Patients According to Duration of Illness 75
10 Distribution of Patients According to Treatment History 76
11 Effect on Polyuria 77
12 Effect on Polydipsia 78
13 Effect on Polyphagia 79
14 Effect on Tiredness 80
15 Effect on Progressive weakness 81

XIII
S. No. Titles Page No.
16 Effect on Dizziness 82
17 Effect on Unexplained Weight Loss 83
18 Effect on Pruritus 84
19 Effect on FBS 85
20 Effect on PPBS 86
21 Effect on Urine Sugar 87
22 Effect on HbA1c 88

Introduction
1
Introduction
Ziabetus Shakari (Diabetes mellitus) commonly known as diabetes, is one of the
world’s oldest known diseases. The prevalence of diabetes is rapidly rising all over
the globe at an alarming rate.1
It is estimated that 20% of global burden of DM resides
in South East Asia Region (SEAR), is likely to triple by 2025 increasing from present
estimates of about 30 million to 80 million.2
The International Diabetes Federation
(IDF) estimates the total number of diabetic subjects to be around 40.9 million in
India and this is further set to rise to 69.9 million by the year 2025.3
Ziabetus Shakari (Diabetes mellitus) is a state of chronic hyperglycemia, classically
associated with excessive thirst, increased urine volume, and weight-loss. It is a
complex and a multifarious group of disorders that disturbs the metabolism of
carbohydrates, fats and proteins. It results from shortage or lack of insulin secretion or
reduced sensitivity of the tissue to insulin.
The term Ziabetus is a Greek word which means “to run through” or “Siphon”, is
characterized by hyperglycaemia, glycosuria, increased appetite, excessive thirst and
gradual loss of body weight.
The concept of Ziabetus also exists in ancient world; it is proved by the discovery of
Eberes papyrus, written about 1550 BC. Eberes papyrus contains descriptions of
various diseases including a polyuric state resembling Ziabetus Shakari. Aretaeus was
the first to use the term “Ziabetus” in connection with this ailment, which means “to
run through” or “Siphon” and provided the accurate description of the symptoms of
Ziabetus for the first time. After Arsyatoos, Jalinoos described Ziabetus as a rare
disease, and referred to the ailment as “Diarrhoea Urinosa (Diarrhoea of Urine)”,
and “Dipsakos (the thirsty disease)”. After that, during the Arabic era Ibne Sina
Introduction
2
described accurately the clinical features of the disease and mentioned two specific
complications of the disease, namely gangrene and the collapse of sexual function.
In present era due to resemblance in clinical features of the disease, Ziabetus Shakari
has been correlated with diabetes mellitus. Diabetes Mellitus is a clinical syndrome
characterized by hyperglycaemia due to absolute or relative deficiency of insulin.
Lack of insulin whether absolute or relative, affects the metabolism of carbohydrate,
protein, fat, water and electrolytes. Chronic hyperglycaemia leads to complications of
Diabetes and affects most characteristically the eye, the kidney, the nervous system,
the cardiovascular system. It also causes recurrent infections and Diabetic foot.
There are various types of diabetes mellitus; among them Type 1 or insulin dependent
diabetes mellitus (IDDM) and Type 2 Non-insulin dependent diabetes mellitus
(NIDDM) are two major types.
Type 1 Diabetes Mellitus: It is characterized by β cell destruction, which usually leads
to an absolute deficiency of insulin. Most cases of Type 1 Diabetes are immune-
mediated characterized by autoimmune destruction of the β cells in the Islets of
Langerhans of the pancreas, destroying them or damaging them sufficiently to reduce
insulin production. However, some forms of Type 1 Diabetes are characterized by
loss of the β cells without evidence of autoimmunity.
Type 2 Diabetes Mellitus: It is characterized by insulin resistance and usually has
relative (rather than absolute) insulin deficiency.
The specific etiology of this form of Diabetes is not known, but many factors like
hereditary, age, obesity, diet, sex, sedentary life style, socio-economic status,
hypertension and various types of stresses are supposed to be involved in the etiology
of Diabetes Mellitus. Most patients of Type 2 Diabetes Mellitus are obese, and
obesity itself causes some degree of insulin resistance. It occurs more frequently in
Introduction
3
women with the history of GDM (Gestational Diabetes Mellitus) and in individuals
with hypertension or dyslipidemia and its frequency varies in different racial/ethnic
subgroups.
Classically, the age of onset of Type 2 Diabetes is above 40 years. However, in
Indians it has been found to be a decade earlier than in the west. Occasional patients
might develop Type 2 Diabetes in the second decade of life. Obesity is not a common
feature in Type 2 Diabetes in India. Only about 50% of cases have a BMI > 25 kg / m2
while, 15-20 % of the patients are underweight.
Diabetes mellitus is now one of the most common non-communicable diseases. It is a
silent killer that kills one person every 10 seconds, and kills about 3.2 million every
year worldwide. At least one in ten deaths among adults between 35-64 years old is
attributable to Diabetes. Further, it is the fourth or fifth leading cause of death in most
developed countries and there is substantial evidence that it is epidemic in many
developing and newly industrialized nations.
Diabetes Mellitus leads to complications like blindness, renal failure, coronary artery
disease, gangrene and coma. Due to these dreadful complications, Diabetes has
become a global problem despite tremendous advances in modern sciences.
Owing to dreadful complications of Diabetes Mellitus and lack of relatively safe and
effective drug for its management, search for better and safe therapeutic agent
becomes a thrust area for research, in every field of medical science. As far as the
Unani system of medicine is concerned, Diabetes Mellitus is being treated since
Greco-Arab period. Unani physicians described many safe and effective drugs as
mentioned in standard Qarabadeen, but most of the agents have not been evaluated on
scientific parameters.

Introduction
4
However, lifestyle management measures may be insufficient or patient compliance
difficult, rendering conventional drug therapies necessary in many patients. As an
alternative approach, Unani drugs with antihyperglycemic activities are increasingly
sought by diabetic patient and physicians. These drugs should have a similar degree of
efficacy without the troublesome side effects associated with these treatments. Hence,
Alternative treatments for diabetes have become increasingly popular for the last
several years.
Presently, there is growing interest in herbal remedies due to the side effects
associated with the oral hypoglycemic agents for the treatment of diabetes mellitus.
So the traditional herbal medicines especially Unani medicines are used which are
obtained mainly from plants, play important role in the management of diabetes
mellitus.
Several drugs such as biguanides and sulfonylureas are being prescribed to reduce
hyperglycemia in diabetes mellitus. But these drugs develop some serious side effects
and quite expensive therefore, long term use of these drugs could not be possible.
Management of diabetes without any side effect is still a challenge to medical
fraternity. Thus search of new antidiabetic drugs are quite necessary to overcome this
problem.
In Unani literature specially in Al Qanoon fil Tib, Zakhira Khwarzam Shahi, Sharahe
Asbab wal Alamat, Jamiul Hikmat, Bayaze Kabeer there are enough evidence
regarding the effective use of various herbal drugs for diabetes mellitus since long, yet
these drugs need clinical evaluation in the light of modern parameters. Therefore, it is
one of the areas which have to be given priority in scientific researches in Unani
Medicine. In recent years extensive researches has been carried out to explore the
efficacy of Unani drugs and many studies revealed that some of the drugs possess
Introduction
5
potent hypoglycemic properties. From the long list of such drugs, the formulation
consisting of Satte Gilo (Tinospora cardifolia) Tabasheer (Bambusa bambos) and
Maghze Kanwal Gatta (Nelumbo nucifera) has been selected for the study.4 Hence, a
Randomized single blind with standard controlled study was envisaged. The patients
were randomly allocated in test and control group. The test group was treated with the
Unani formulation (3 gram) whereas control group was given Diabecon 2 tablet twice
a day for the period 45 days. All the patients were advised strict dietary control and
45 minutes brisk walk daily. Every fortnightly assessment was recorded on CRF,
specially designed for the study. The efficacy of test formulation was evaluated on the
basis of standard parameters based on subjective parameters such as polyuria,
polydipsia, polyphagia, tiredness, progressive weakness, dizziness, unexplained
weight loss and pruritus and objective parameters such as fasting blood sugar, post
prandial blood sugar, urine sugar and HbA1c.
Apart from efficacy parameters, safety parameters such as haemogram, AST, ALT,
blood urea, serum creatinine, and ECG were also carried out before and after
treatment, in order to assess the toxicity of the test formulation, if any. At the end of
study the data were analyzed statistically. The efficacy of the test drug was compared
with the standard drug Diabecon.

Objective
6
OBJECTIVE OF THE STUDY
To evaluate the clinical efficacy of a Unani formulation in the management of
Ziabetus Shakari (Diabetes Mellitus Type II)
Disease Review
7
Historical Background
Ancient Period
Clinical features similar to diabetes mellitus were described 3000 years ago by the
ancient Egyptians. They were the first to write documents about diseases proved by
discovery of Eberes papyrus in graves of Thabes in 1862 by Georg Eberes which was
written in near about 1550 BC. It contained descriptions of a polyuric state resembling
diabetes mellitus.5,6,7,8
Buqrat known as Hippocrates (460 BC) mentioned a disease with excessive urinary
flow and wasting of body.9
The first known clinical description of diabetes appears to have been made by Aulus
Cornelius Celsus (30 BC-50 AD); but it was Aretaeus of Cappadocia (2nd century
AD) who provided a detailed and accurate account and introduced the name
"diabetes" from the Greek word for "siphon". Aretaeus comments that life does not
last very long, for great masses of flesh are liquefied into urine.8,10
Jalinoos (131-201) defined diabetes as “Diarrhoea Urinosa” (diarrhoea of urine) and
“dipsakos” (thirsty disease). He described it as a disease specific to kidneys because
of weakness in their retentive ability and secondly had seen only two cases therefore
termed it a rare disease. He believed that diabetics’ urine was unchanged drink which
may have accounted for a different aroma.7,9,11
Chinese (Chang Chung-Ching in 229 AD) and Japanese (Li Hsuan) literature
explained a disease with sweet urine which attracted dogs and insects. Such patients
were more prone to develop boils and tuberculosis.7,11
During 5th and 6th century, sweet taste of urine in polyuric patients was also
described in Sanskrit (Indian) literature by Susruta, Charaka and Vaghbata and

Disease Review
8
disease was named “Madhumeha”. They described that urine of these patients tasted
like honey (madhu), sticky to touch and ants are strongly attracted to it.
Ibne Sina (980-1037), who termed the disease “aldulab” (water wheel) and “zalqul
Kulliya” (diarrhea of the kidneys), terms that Jalinoos and others had used, added to
the complications of the disease those of mental troubles, impotence, gangrene, and
furunculosis. Ibne Sina was first who wrote differentiating feature of Diabetes
associated with emaciation form other causes of polyuria.7,9,12
The term "diabetes" was first coined by Araetus of Cappodocia (81-133AD). Later,
the word mellitus (honey sweet) was added by Thomas Willis (Britain) in 1675 after
rediscovering the sweetness of urine and blood of patients.5,8,12,13,14
Diagnostic period:
In 1674, Dr. Thomas Willis, personal physician to the late English King Charles II,
described the sweet taste of urine from diabetics "as if imbued with honey and sugar"
hence, the name "mellitus" is Latin for honey. In 1766 Mathew Dobson proved that
the sweet taste of diabetic urine was due to sugar. He made the crucial observation of
the excess of sugar in blood.5,15
It was only in 1776 that Dobson (Britain) firstly confirmed the presence of excess
sugar in urine and blood as a cause of their sweetness. In modern time, the history of
diabetes coincided with the emergence of experimental medicine.
An important milestone in the history of diabetes is the establishment of the role of
the liver in glycogenesis, and Claude Bernard (France) in 1857 pointed out that
diabetes is basically caused by excess glucose production.7
Diabetes: A Disease of the Pancreas
Cawley was the first to suggest a relationship between the pancreas and diabetes, an
association subsequently confirmed in various other diseases of the pancreas. These
Disease Review
9
initial clinical observations were confirmed in 1889, when Oscar Minkowski (1858-
1931) and Joseph Mering (1849-1908) showed that pancreatectomized dogs
developed diabetes, which could be reversed by the subcutaneous implantation of
pancreatic fragments.12
The specific role of the pancreas was further refined after Paul Langerhans (1849-
1888) described in 1869 the unique morphologic features of the pancreatic islands that
were subsequently named after him.
In 1909, Eugene L. Opie (1873-1971) reported hyaline degeneration of the islands in
diabetic patients, a finding subsequently confirmed in a series of experimental studies
that led Edward Sharpey-Schafer to suggest in 1916 that the islands of Langerhans
produced a glucoseregulating hormone that he termed insulin.
The race for isolating the hypothesized hormone was now on. Frederick Banting
(1891-1941) and Charles Best (1892-1978) finally did so in 1922. They called it
insulin.
The endocrine nature of diabetes was now clearly established. The stage of diabetes as
a disease of the kidneys was over.12
Insulin Era
The reversal of metabolic changes of diabetes by injection of a potent extract of
pancreatic islands was demonstrated. In December 1921, Banting and Macleod got
success in isolation of insulin; a milestone event. They got Noble prize for that in
1923. On 11th Jan 1922, 14 year old diabetic boy named Leonard Thombson was
treated with insulin first time. In 1923, Eli Lilly begins commercial production of
insulin (Isletin Insulin). In 1925, Home testing for sugar in urine through Benedict’s
solution was introduced. In 1926, John Jacob Abel purified insulin, isolated its
crystalline structure and hence chemically identified. In 1927, an oral medication

Disease Review
10
“horment” or “glukohorment” was developed as a replacement for insulin, but
dropped out due to its side effects. In 1928, Wintersteiner and his colleagues
described insulin as a protein composed of amino acids. In 1930s, Insulin was further
refined to Protamine zinc insulin, a long-acting insulin. Insulin therapy soon became
backbone of management that enabled individuals affected by this disease to live an
almost-normal life. It soon became apparent that insulin did not cure diabetes. As
people began to live longer, they experienced complications that had not previously
been seen. In 1936 Himsworth proposed two types of diabetes as insulin sensitive and
insulin insensitive, former being due to insulin deficiency. This observation laid the
foundation for the concept of impaired insulin action, which is now known to be a
crucial factor in pathogenesis of type 2 diabetes. In 1923, Collip found that onion has
a hypoglycemic effect in fasting and depancreatized animals. The first oral
hypoglycemic agent sulfonylurea was discovered in 1942 by M.J. Janbon. Franke and
Fuchs in Berlin applied it clinically. In 1979, Type 1 or Insulin Dependent Diabetes
Mellitus (IDDM) and type 2 or Non Insulin Dependent Diabetes Mellitus (NIDDM)
diabetes were formally recognized by American Diabetes Association (ADA).
National Diabetes Data Group and World Health Organization (WHO) developed
diagnostic criteria for diagnosis of diabetes using an oral glucose tolerance test which
were updated in 1997 by ADA, and then revised in 2003. Latest developments Today
Researchers are working on an insulin patch. A sensor-computer-pump system
(implantable pump) that mimics insulin response of normal pancreas is being
developed to function as an “artificial pancreas”. Genetic engineering is being used to
manipulate cells so they secrete more insulin e.g. insulin sensitizers. Pancreatic or
islet cell transplantation is also underway. Oral-Lyn is an oral spray formulation of
human insulin. Its clinical use has been started in Ecuador in 2005. Inhaled insulin
Disease Review
11
(Exubera) is one of the greatest breakthroughs in 2006 for people who must take
short-acting insulin. Taiwan scientists Sung et al. reported the success in early tests of
an oral insulin solution in diabetic rats. The use of Rituximab in turning off the
immune attack on beta cells is under research. Another under way study is testing
whether Mycophenolate Mofetil (MMF) or MMF plus Daclizumab (DZB) can slow
or arrest the autoimmunity of type 1 diabetes.7

Disease Review
12
Diabetes Mellitus
Every cell in the human body needs energy in order to function. The body’s primary
energy source is glucose, a simple sugar resulting from the digestion of foods
containing carbohydrates. Glucose from the digested food circulates in the blood as a
ready energy source for any cell that needs it.
Diabetes mellitus is a condition in which the pancreas no longer produces enough
insulin or when cells stop responding to the insulin that is produced, so that glucose in
the blood cannot be absorbed into the cells of the body.16
Diabetes mellitus is a metabolic disorder characterized by hyperglycemia, glycosuria
and negative nitrogen balance and it is mainly due to lack of insulin secretion in beta
cells of pancreas and desensitization of insulin receptors for insulin. Lack of insulin
affects the metabolism of carbohydrate, protein and fat, and can cause a significant
disturbance of water and electrolyte homeostasis.17
It is not a single disease entity but rather a group of metabolic disorders sharing the
common underlying feature of hyperglycemia. Hyperglycemia in diabetes results
from defects in insulin secretion, insulin action, or, most commonly, both. The
chronic hyperglycemia and attendant metabolic dysregulation of diabetes mellitus
may be associated with secondary damage in multiple organ systems, especially the
kidneys, eyes, nerves, and blood vessels.18
It is characterized by increased fasting and
postprandial concentrations of glucose. It is the commonest metabolic disorder.19,20,21
Diabetes mellitus is a complex disorder of carbohydrates, proteins, and fats that leads
to premature death, usually due to heart attack and stroke. Many experts think that
although diabetes is commonly considered a disease of sugar, it is more accurately a
vascular disease that severely affects blood vessels throughout the body.22
Disease Review
13
Concepts of Ziabetus
The word Diabetes is derived from Greek word “Diabanmo” Which means “passing
through” or “to run through” or Siphon” is characterized by excessive thirst, excessive
urination, presence of sugar in urine, increased appetite, gradual loss of body weight
etc.23,24,25
Ziabetus is mentioned in most of the Unani literature like Al Qaanon, Al Hawi,
Kamilul Sana’ah etc. Unani Atibba considered that Ziabetus is a disease of kidneys.
Arab Atibba had described Ziabetus by some other terms also like Moattasha, Atsha,
Intesae Anmas, Zalaqul kulliya, Dolab, Dawwarah, Barkar, Barkarya, Qaramees
etc.23,26,27,28,29
According to Unani medicine, Ziabetus Shakari is a disease in which the consumed
water is passed out through the kidney immediately after intake by the patient. It is
like to Zalqul Meda wal Ama, in which the food passes rapidly through the stomach
and intestine without proper digestion.24
In this disease patient has excessive thirst
and takes plenty of water and passes all the water he consumed without any metabolic
change.30
In this disease Mizaj of kidneys become Haar so they absorb water from blood and
send to the urinary bladder immediately due to weakness in Quwate Masika (retentive
power). It also been described that the kidneys attract the watery substance of blood,
but the urinary bladder does not attract any thing. So kidneys attract the water from
the circulation, liver, stomach and intestines because of which patient has the
immoderate thirst (polydipsia).26,27,30
Disease Review
14
Prevalence
The prevalence of diabetes is rapidly rising all over the globe at an alarming rate.1
It is
estimated that 20% of global burden of DM resides in South East Asia Region
(SEAR) area, is likely to triple by 2025 increasing from present estimates of about 30
million to 80 million.2
The International Diabetes Federation (IDF) estimates the total
number of diabetic subjects to be around 40.9 million in India and this is further set to
rise to 69.9 million by the year 2025.3
It is a global problem and number of those affected is increasing day by day. If the
prevalence of diabetes mellitus type 2 (DMT2) continues to increase at the current
rate, the global burden of this disease will swell between 2000 to 2030 from 171
million to 366 million patients.31
This global pandemic principally involves type 2
diabetes, to which several factors contribute, including greater longevity, obesity,
unsatisfactory diet, sedentary lifestyle and increasing urbanisation. Many cases of
type 2 diabetes remain undetected. However, the prevalence of both types of diabetes
varies considerably around the world, and is related to differences in genetic and
environmental factors. The prevalence of known diabetes in Britain is around 2-3%,
but is higher in the Middle and Far East (e.g. 12% in the Indian subcontinent). A
pronounced rise in the prevalence of type 2 diabetes occurs in migrant populations to
industrialised countries, as in Asian and Afro-Caribbean immigrants to the UK. Type
2 diabetes is now being observed in children and adolescents, particularly in some
ethnic groups, such as Hispanic and Afro-Americans.32
Survey of large number of people from rural as well as urban population of India,
reported that prevalence of diabetes and impaired fasting glucose (IFG) is lower in
rural population compared to the urban population. The prevalence rate of diabetes
mellitus for persons above the age of 25 years was 3.77%. The prevalence in males
Disease Review
15
was 4.58% and in females it was 2.66%. Impaired fasting glucose was 2.82% in male
and 2.78 % in female. The maximum prevalence was observed in the age group of 56
to 65 in both males and females.33
The highest rate of growth is expected to occur in developing countries. Of people
with diabetes, 9 out of 10 have type 2 diabetes. The five countries with the largest
numbers of people with diabetes are India, China, the United States, Russia, and
Germany. Worldwide 3.8 million deaths are directly attributable to diabetes. The
disease also is contributing factor in many deaths due to cardiovascular disease.16
Type 1 diabetes is more common in Caucasian populations, and in Northern Europe
its prevalence in children has doubled in the last 20 years, with a particular increase in
children under 5 years of age. In Europe and North America the ratio of type 2 to type
1 is approximately 7:3.17
Disease Review
16
Classification of Ziabetus
1. According to the presence or absence of sugar in the urine, Ziabetus is divided
into two types:34
A) Ziabetus Sada (Diabetes insipidus), which is also called Ziabetus gair shakari.
It is characterized by excessive thirst and excessive urination but there is no
sugar in the urine.
B) Ziabetus Shakari (Diabetes mellitus), which is characterized by excessive
thirst and urination and presence of sugar in the urine.
2. According to the khiffat and shiddat (intensity) of the sign and symptom it is also
divided into two types:34,35
A) Ziabetus Haar: Acute symptoms of the Ziabetus with abrupt onset occur like
excessive thirst (polydipsia) and increase urination (polyuria) with the
symptom and sign of other sue mizaj haar like heat in flanks and dryness or
the body, due to sue mizaj haar sada of kidneys.
B) Ziabetus Barid: In which the thirst and frequency of urine is comparatively
less.
In the light of present science, the vast majority of cases of diabetes fall into one of
two broad classes:
Type 1 diabetes is characterized by an absolute deficiency of insulin caused by
pancreatic Β cells destruction. It accounts for approximately 10% of all cases. This
type of diabetes formerly called juvenile diabetes.21
Type 2 diabetes is caused by a combination of peripheral resistance to insulin action
and an inadequate secretary response by the pancreatic β cells. Approximately 80% to
90% of patients have type 2 diabetes.18,19,21,36,37
Disease Review
17
The American Diabetes Association classification scheme for diabetes mellitus is
summarized and clinical diabetes is divided into four general subclasses: type 1,
primarily caused by autoimmune pancreatic β cells destruction and characterized by
absolute insulin deficiency; type 2, characterized by insulin resistance and relative
insulin deficiency; other specific types of diabetes (associated with identifiable
clinical conditions or syndromes); and gestational diabetes mellitus.38
In addition to these clinical categories, two forms of pre-diabetes impaired glucose
tolerance and impaired fasting glucose have been defined to describe intermediate
metabolic states between normal glucose homeostasis and overt diabetes. Both
impaired glucose tolerance and impaired fasting glucose significantly increase the
future risk for development of diabetes mellitus and in many cases is part of the
disease's natural history. Patients with any form of diabetes may require insulin
therapy; for this reason, the previously used terms insulin dependent diabetes (for type
1) and non insulin dependent diabetes (for type 2) have been eliminated.38
Etiologic Classification of Diabetes Mellitus18,19,30,40
1. Type 1 Diabetes
β cells destruction, leads to absolute insulin deficiency
2. Type 2 Diabetes
Insulin resistance with relative insulin deficiency
3. Genetic Defects of β Cell Function
Maturity onset diabetes of young (MODY), caused by mutations in:
Hepatocyte nuclear factor [HNF]-4α (MODY1)
Glucokinase (MODY2)
Hepatocyte nuclear factor [HNF]-1α (MODY3)
Insulin promoter factor [IPF-1] (MODY4)
Disease Review
18
Hepatocyte nuclear factor [HNF]-1β (MODY5)
Neurogenic differentiation factor [Neuro D1] (MODY6)
Mitochondrial DNA mutations
4. Genetic Defects in Insulin Processing or Insulin Action
Defects in proinsulin conversion
Insulin gene mutations
Insulin receptor mutations
5. Exocrine Pancreatic Defects
Chronic pancreatitis
Pancreatectomy
Neoplasia
Cystic fibrosis
Hemochromatosis
Fibrocalculous pancreatopathy
6. Endocrinopathies
Growth hormone excess (acromegaly)
Cushing syndrome
Hyperthyroidism
Pheochromocytoma
Glucagonoma
7. Infections
Cytomegalovirus
Coxsackievirus B
8. Drugs
Glucocorticoids
Disease Review
19
Thyroid hormone
β adrenergic agonists
9. Genetic Syndromes Associated with Diabetes
Down syndrome
Kleinfelter syndrome
Turner syndrome
10. Gestational Diabetes Mellitus
The term gestational diabetes mellitus describes women with abnormal glucose
tolerance that appears or is first detected during pregnancy. Women with known
diabetes before conception are not classified as having gestational diabetes.
Gestational diabetes mellitus usually appears in the second or third trimester, when
pregnancy-associated insulin antagonistic factors reach their peak. After delivery,
glucose tolerance reverts to normal. However, within 10 years, type 2 diabetes
develops in most women with prior gestational diabetes; on occasion, pregnancy can
precipitate type 1 diabetes as well.39
Although patients with gestational diabetes
generally present with mild, asymptomatic hyperglycemia, rigorous treatment is
indicated to protect against hyperglycemia-associated fetal morbidity. Insulin is often
required.36,38
Disease Review
20
Physiology
Unani Concepts
The concept of Quwa is unique one in Tibb. The Quwa is a property of the body with
which phenomenon of the life is manifested. The Quwa provide the basis for the
different bodily functions. Each and every organ furnished with a power, Quwat
(power) through which specific physiological functions are performed by that
particular organ. These Quwa are specific for a particular tissue or organ on which the
specific functions of that organ depend. The organ is the seat of Quwa (faculties) and
Quwa give rise to functions.41,42
There are three major division of the Quwa (faculties) of the body.
1. Al Quwa at Tabi’yah (Natural faculties).
2. Al Quwa an Nafsaniyah (Psychic or mental faculties).
3. Al Quwa al Haywaniyah (Vital faculties).
Al Quwa at Tabi’yah are those which are responsible for ingestion, digestion,
absorption transformation (metabolism) and assimilation of ghiza (food) and
excretion of waste products and preservation of the race also. According to the
function Quwa at Tabi’yah have been divided by Ali Ibne Abbas into three faculties:
Quwate Ghaziyah (nutritive faculty), Quwate Murabbiyah (growth faculty) and
Quwate Muwallida (reproductive faculty).
Quwate ghaziyah (nutritive faculty) is that which is responsible for ingestion,
digestion, absorption transformation (metabolism) and assimilation of ghiza (food)
and excretion of waste products. According to the function this faculty divided into
four Quwa; Quwate Jazibah, Quwate masika, Quwate hazimah or Quwate
Disease Review
21
mughayirah (power of digestion and transformation) and Quwate dafi’ah (power of
propulsion and excretion).
1) Quwate Jaziba
This is the power which absorbs the Akhlat and runs into the cells with help of
various enzymes, hormones or simply through natural forces.
2) Quwate Masika
This is the power which retains the Akhlat inside the cells for their Istahalah
(metabolism).
3) Quwate Mughayirah
This is the power which transforms the materials such as phosphorylation of
glucose after entering the cells.
4) Quwate Dafi’ah
The power which helps the cells and tissues to expel out the waste products
produce in the course of istahalah (metabolism).
Each and every organ furnished with a Quwat (power) as previously discussed
through which specific physiological functions are performed. The organs of Quwate
Hazima (A’zae Hazm) include Banqaras (pancreas) along with oral cavity, salivary
glands, esophagus, stomach, intestines, liver and spleen. Liver is considered the main
centre of Quwate Tabi’yah.
According to the Abu Sahl Masihi each of the above four Quwa are in two folds, one
is found in the gastrointestinal tract and liver, other in all the cells of the body. So the
Quwa of all the cells of body absorb the food materials and Ruh and metabolize and
transform them into various compounds and replace the wear and tear by producing
the Quwat (energy) for the proper functioning of the body.41,42,43,44

Disease Review
22
Above description of Quwa and its function described in Umoore Tabi’yah specially
in the context of digestion and absorption of food materials from the GIT and
transportation of it toward the tissues, absorption and retention of materials by the
help of different Quwa into the cells can clearly understood. Attibbae Qadeem
(Ancient physicians) had not described the exact physiology due to lack of
advancement in the sciences, like today physicians can. Today phathophysiology of
diabetes almost stabilized, role of pancreas and insulin and its peripheral resistance
are revealed in the context of development of disease along with other causes in lesser
extent.
According to the modern Medicine Physiology are described below:
Normal insulin physiology
Normal glucose homeostasis is tightly regulated by three interrelated processes,
glucose production in the liver, glucose uptake and utilization by peripheral tissues,
chiefly skeletal muscle and actions of insulin and counter-regulatory hormones,
including glucagon on glucose.45
Insulin and glucagon have opposing regulatory
effects on glucose homeostasis. During fasting states, low insulin and high glucagon
levels facilitate hepatic gluconeogenesis and glycogenolysis while decreasing
glycogen synthesis, thereby preventing hypoglycemia. Thus, fasting plasma glucose
levels are determined primarily by hepatic glucose output. Following a meal, insulin
levels rise and glucagon levels fall in response to the large glucose load. Insulin
promotes glucose uptake and utilization in tissues. The skeletal muscle is the major
insulinresponsive site for postprandial glucose utilization, and is critical for
preventing hyperglycemia and maintaining glucose homeostasis.18,21,45
Disease Review
23
Insulin Biosynthesis, Secretion and Action
Biosynthesis: Insulin is produced in the beta cells of the pancreatic islets. It is
initially synthesized as a single-chain 86-amino-acid precursor polypeptide,
preproinsulin. The mature insulin molecule and C peptide are stored together and co-
secreted from secretory granules in the beta cells is a useful marker of insulin
secretion and allows discrimination of endogenous and exogenous sources of insulin
in the evaluation of hypoglycemia.18,19
Secretion: Glucose is the key regulator of insulin secretion by the pancreatic beta
cell, although amino acids, ketones, various nutrients, gastrointestinal peptides, and
neurotransmitters also influence insulin secretion. Glucose levels 70 mg/dL stimulate
insulin synthesis, primarily by enhancing protein translation and processing. Glucose
stimulation of insulin secretion begins with its transport into the beta cell by a
facilitative glucose transporter. Glucose phosphorylation by glucokinase is the rate-
limiting step that controls glucose-regulated insulin secretion. Insulin secretory
profiles reveal a pulsatile pattern of hormone release, with small secretory bursts
occurring about every 10 min, superimposed upon greater amplitude oscillations of
about 80-150 min. Incretins are released from neuroendocrine cells of the
gastrointestinal tract following food ingestion and amplify glucose-stimulated insulin
secretion and suppress glucagon secretion. The Glucagon-like peptide 1 (GLP-1),
most potent incretin, are released from L cells in the small intestine and stimulates
insulin secretion only when the blood glucose is above the fasting level.
Action: Once insulin is secreted into the portal venous system, 50% is removed and
degraded by the liver. Unextracted insulin enters the systemic circulation where it
binds to receptors in target sites. Insulin binding to its receptor stimulates intrinsic
tyrosine kinase activity, leading to receptor autophosphorylation and the recruitment

Disease Review
24
of intracellular signaling molecules, such as insulin receptor substrates (IRS). IRS and
other adaptor proteins initiate a complex cascade of phosphorylation and
dephosphorylation reactions, resulting in the widespread metabolic and mitogenic
effects of insulin. As an example, activation of the phosphatidylinositol-3′-kinase (PI-
3-kinase) pathway stimulates translocation of a facilitative glucose transporter to the
cell surface, an event that is crucial for glucose uptake by skeletal muscle and fat.
Activation of other insulin receptor signaling pathways induces glycogen synthesis,
protein synthesis, lipogenesis, and regulation of various genes in insulin-responsive
cells.18,19,21
Disease Review
25
Aetiology and Pathogenesis
Unani physicians Majoosi, Ibne Sina and Samarqandi described some underline
etiopathogenesis in detail. It was supposed that the disease is related to kidney. The
important etiological factors mentioned in Unani are following:
Zofe Gurda (Weakness of Kidney)
Water cannot be retained properly due to weakness in kidney and its Quwate masika
(retentive faculty) and kidney are unable to metabolize the water which is coming
from liver.23,26,27,46
Ittesae Gurda wa Majrae Bole (Dilatation of Kidney and Tubule)
Water cannot be retained for long/required time due to dilatation of Gurda wa Majrae
Baul (Dilatation of Kidney and Tubule) so it passed out rapidly (polyuria).24,27,46
Baroodate Badan, Jigar wa Gurda
Sometime Ziabetus develops due to excessive exposure of cold of whole body or liver
or kidney, which leads to sue mizaj barid (cold derangement in temperament).24,27,35,47
Sue Mizaj Haar Gurda (Hot derangement in temperament of Kidney)
Kidneys absorb water in very excess amount from circulation due to excessive
hotness or derangement in temperament so they cannot retain much amount of fluid
and pass in the form of urine frequently (polyuria) and patient drinks water frequently
(polydipsia) to overcome his thirst.26,45,46
Sue Mizaj Barid Gurda (Cold Derangement in Temperament of Kidney)
Sometime Ziabetus develops due to excessive exposure of cold to kidneys which may
leads to sue mizaj barid (cold derangement in temperament).23,27

Disease Review
26
According to the modern Medicine etiology and pathogenesis are described below:
I. predisposing factors
Susceptibility of diabetes increase in following population, specially type 2 diabetes
mellitus:18,36,38,49,50,53,57,58
Peoples who are 45 years or over
Peoples who are overweight
Peoples who have IGT (impaired glucose tolerance)
Peoples who have a family history of diabetes
Peoples who are physically inactive habitually
Peoples who had gestational diabetes
Peoples who are hypertensive
Peoples who are dyslipidemic
II. Pathogenesis
A) Type1 diabetes mellitus
This form of diabetes results from a severe lack of insulin caused by an
immunologically mediated destruction of β cells. Type 1 diabetes is an autoimmune
disease in which islet destruction is caused primarily by T lymphocytes reacting
against as yet poorly defined β cell antigens. As in all autoimmune diseases, genetic
susceptibility and environmental factors play important roles in the
pathogenesis.18,19,21,49,
i) Mechanisms of β Cells Destruction
Although the clinical onset of type 1 diabetes is abrupt, this disease in fact results
from a chronic autoimmune attack on β cells that usually starts many years before the
disease becomes evident. The classic manifestations of the disease (hyperglycemia
Disease Review
27
and ketosis) occur late in its course, after more than 90% of the β cells have been
destroyed.
Following mechanisms contribute to β cells destruction:
■ T lymphocytes react against β cell antigens and cause cell damage. These T cells
include (1) CD4+ T cells of the TH 1 subset, which cause tissue injury by activating
macrophages, and (2) CDR+ cytotoxic T lymphocytes, which directly kill β cells and
also secrete cytokines that activate macrophages.
■ Locally produced cytokines damage β cells. Among the cytokines implicated in the
cell injury are IFN-y, produced by T cells, and TNF and IL-1, produced by
macrophages that are activated during the immune reaction.
■ Autoantibodies against islet cells and insulin are also detected in the blood of 70%
to 80% of patients. The autoantibodies are reactive with a variety of β cell antigens,
including GAD.
ii) Genetic Susceptibility
Type 1 diabetes has a complex pattern of genetic associations, and putative
susceptibility genes have been mapped to at least 20 loci. Many of these associations
are with chromosomal regions, and the particular genes involved are not known yet.
Of the multiple loci that are associated with the disease, by far the most important is
the class II MHC (HLA) locus; according to some estimates, the MHC contributes
about half the genetic susceptibility, and all the other genes combined make up the
other half.18,19,21,49
iii) Environmental Factors
There is evidence that environmental factors, especially infections, are involved in
triggering autoimmunity in type 1 diabetes and other autoimmune diseases.
Epidemiologic studies suggest a role of viruses." Seasonal trends that often
Disease Review
28
correspond to the prevalence of common viral infections have long been noted in the
diagnosis of new cases, as has the association between coxsackieviruses of group B
and pancreatic diseases, including diabetes. Other implicated viral infections include
mumps, measles, cytomegalovirus, rubella, and infectious mononucleosis.18,19,21
B) Type 2 diabetes mellitus
The pathogenesis of type 2 diabetes remains enigmatic. Environmental factors, such
as a sedentary life style and dietary habits, clearly play a role, as will become evident
when obesity is considered. Nevertheless, genetic factors are even more important
than in type 1 diabetes.
i) Insulin resistance: A decreased ability of peripheral tissues to respond to insulin.
ii) β cell dysfunction that is manifested as inadequate insulin secretion in the face of
insulin resistance and hyperglycemia. In most cases, insulin resistance is the primary
event, and is followed by increasing degrees of β cell dysfunction
i) Insulin Resistance
One of the main conditions exhibited in type II diabetes is insulin resistance.
Although the causes may diverse due to the genetics aspects, it is commonly exhibited
throughout diverse ethnic backgrounds. It is also affected by the environment in the
form of diet and exercise; hence it plays a key role in type II diabetes.
Insulin resistance is defined as resistance to the effects of insulin on glucose uptake,
metabolism, or storage. Insulin resistance is a characteristic feature of most patients
with type 2 diabetes and is an almost universal finding in diabetic individuals who are
obese. The role of insulin resistance in the pathogenesis of type 2 diabetes can be
gauged from the findings that (1) insulin resistance is often detected 10 to 20 years
before the onset of diabetes in predisposed individuals (e.g. offspring of type 2
diabetics) and (2) in prospective studies, insulin resistance is the best predictor for
Disease Review
29
subsequent progression to diabetes. Insulin resistance leads to decreased uptake of
glucose in muscle and adipose tissues and an inability of the hormone to suppress
hepatic gluconeogenesis. It is recognized that insulin resistance is a complex
phenomenon.18,19,21,49,50,61
ii) Obesity and Insulin Resistance
The association of obesity with type 2 diabetes has been recognized for decades,
visceral obesity being a common phenomenon in the majority of type 2 diabetics. The
link between obesity and diabetes is mediated via effects on insulin resistance. Insulin
resistance is present even in simple obesity unaccompanied by hyperglycemia,
indicating a fundamental abnormality of insulin signaling in states of fatty excess. The
risk for diabetes increases as the body mass index (a measure of body fat content)
increases. Central obesity (abdominal fat) is more likely to be linked with insulin
resistance than are peripheral (gluteal/subcutaneous) fat depots.18,19,21,49,50

Disease Review
30
Clinical Features
In Unani literature some clinical features of Ziabetus are commonly
described:24,27,30,35,47
Increased frequency of micturition
Excessive thirst (which cannot be easily quenched by drinking water)
Dryness of mouth and whole body
Ants and flies are attracted to the urine
The onset of type 1 diabetes is usually quite dramatic with weight loss, polyuria, and
polydipsia. Often, it is precipitated by an infection or other severe physical stress
because patients lack the reserve of endogenous insulin secretion to overcome the
effects of counter-regulatory hormones on glucose metabolism. Severe dehydration
and ketoacidosis may be present. Type 2 usually has an insidious onset. The body will
attempt to dilute the high level of glucose in the blood, a condition called
hyperglycemia, by drawing water out of the cells and into the blood stream in an
effort to dilute the sugar and excrete it in the urine. It is not unusual for people with
undiagnosed diabetes to be constantly thirsty, drink large quantities of water, and
urinate frequently as their bodies try to get rid of the extra glucose. This creates high
levels of glucose in the urine.
Patients may complain of blurring of vision, myopia, episodes of recurrent skin
infections, or monilial vaginitis (females) or balanitis (males).
Occasionally, patients may present with evidence of chronic diabetic complications
(neuropathy, nephropathy, or retinopathy) but without symptoms related to glucose
intolerance. Symptoms such as polyuria, polydipsia, and polyphagia may only
develop in situations of increased insulin resistance such as pregnancy, infection, or
steroid use.51,52,53,54,56,57,57,58,61
Disease Review
31
Complications
Complication of Ziabetus is specially enumerated by Ismail Jurjani, that is the
Zooban (Emaciation of the body), develops due to excessive dehydration of the body
which cannot overcome by intake of water.27
Further, Ibne Sina elucidated other
specific complication of diabetes, such as collapse of the sexual functions and diabetic
gangrene.7,23
Both complication are develops as a sequel of neuropathy.58
In the light of present etiepathology, complications of diabetes can be divided into
two types:58,59,63,64
Acute complications
Chronic complications
I. Acute Complications
Diabetic ketoacidosis
Nonketotic hyperosmolar coma
Hypoglycaemia
Diabetic Ketoacidosis and Nonketotic Hyperosmolar Coma
Diabetic ketoacidosis and nonketotic hyperosmolar coma are potentially fatal
complications of diabetes. The distinction between ketoacidosis and nonketotic
diabetic coma is not absolute; mild ketonemia may be present in patients with a
hyperosmolar state. Diabetic ketoacidosis is more common in type 1 diabetes and
occurs in up to 5% of type 1 diabetes patients per year.
II. Chronic Complications 58,59,63,64
Macrovascular complications
Microvascular complications
Disease Review
32
A. Macrovascular Disease
i) Coronary Artery Disease and Stroke
Myocardial infarction and stroke occur more frequently, at an earlier age, and with
greater severity in diabetic men and women than in nondiabetic persons. Even
patients with impaired glucose tolerance are at a greater risk for the development of
atherosclerosis. Coronary artery disease is the leading cause of mortality in people
with diabetes. Because of autonomic neuropathy, myocardial ischemia or frank
infarction in diabetes may be asymptomatic; it may present as diabetic ketoacidosis or
be diagnosed incidentally by a routine electrocardiogram.18,19,20,58,59
ii) Peripheral Vascular Disease
Involvement of large or medium-sized blood vessels in the lower limbs is a common
complication of diabetes. A diagnosis of arterial insufficiency is suggested by a
history of claudication. Physical examination reveals absent or weak peripheral
pulses. Patients with peripheral vascular disease often cannot supply the increased
blood flow needed to heal foot infections, such as cellulitis and ulcerations. The
inability to heal these infections leads to osteomyelitis, gangrene, and
amputations.18,19,20,58,59
B. Microvascular Disease
i) Diabetic Retinopathy
Diabetic retinopathy is a leading cause of blindness. However, with yearly
ophthalmologic examinations and preventive eye care, significant vision loss is
prevented in all but a small fraction of patients. Diabetic retinopathy has two stages:
Background retinopathy and Proliferative retinopathy. Background retinopathy may
progress to the proliferative stage and cause vitreous hemorrhage, retinal detachment,
Disease Review
33
and vision loss. In addition to retinopathy, cataracts and glaucoma are more prevalent
in the diabetic population.18,19,20,58,59
ii) Diabetic Nephropathy
Diabetic nephropathy is often present along with retinopathy, and occurs in
approximately one third of patients. The specific lesion of diabetic nephropathy is
nodular sclerosis (Kimmelstiel-Wilson lesion), visible on light microscopy as a
rounded hyaline mass at the center of the glomerular lobules. More common, but less
specific, is diffuse glomerulosclerosis with thickening of the glomerular basement
membrane and an increased mesangial matrix. Microalbuminuria (20 to 300 mg per
24 hours) is signs of future development of gross proteinuria. Progressive
nephropathy results in heavy proteinuria and the development of nephrotic syndrome,
which typically progresses to renal failure and the need for hemodialysis within 5
years.
iii) Diabetic Neuropathy
Diabetic neuropathy affects both the peripheral and the autonomic nervous systems.
a) Peripheral Neuropathy
Distal, symmetric polyneuropathy is the most common form of diabetic peripheral
neuropathy. It usually occurs in a stocking-glove distribution with numbness, tingling,
burning, and/or pain in the feet and lower legs. Tendon reflexes and response to
sensory stimuli, particularly vibration, are decreased. Patients with peripheral
neuropathy are at risk for long-term complications of infection and amputation,
especially if peripheral vascular disease coexists.
Focal peripheral neuropathies include mononeuropathies and entrapment syndromes.
Examples of focal neuropathies are femoral and cranial nerve palsies, especially the
Disease Review
34
third nerve. Carpal tunnel syndrome is an example of an entrapment syndrome and is
more common in diabetic patients.18,19,20,58,59
b) Autonomic Neuropathies
Autonomic neuropathies can affect nearly all organs, more notably the skin, the
cardiovascular, gastrointestinal, and genitourinary systems. Diminished sweating of
the feet can result in drying, cracking, and ulcer formation. Diabetic patients with
autonomic neuropathy may present with postural hypotension (without compensatory
tachycardia). Gastroparesis presents as early satiety, vomiting after meals, and
increasing frequency of hypoglycemic episodes. Patients may also experience
alternating bouts of diarrhea and constipation (enteropathy). Bacterial overgrowth
secondary to stasis may contribute to diarrhea. Impotence, with preserved libido, is a
common manifestation of diabetic autonomic neuropathy and affects 75% of diabetic
men 60 to 65 years old. Neurogenic bladder may also occur.18,19,20,58,59
Disease Review
35
Diagnostic Criteria
The diagnosis of diabetes is established by noting elevation of blood glucose by any
one of three criteria:
1. A random glucose >200 mg/dl, with classical signs and symptoms
2. A fasting glucose >126 mg/dl on more than one occasion
3. HbA1c >6.5 %
An abnormal oral glucose tolerance test (OGTT), in which the glucose is > 200 mg/dl
2 hours after a standard carbohydrate load.
Individuals with fasting glucoses greater than 110 mg/dl but less than 126 mg/dl, or
OGTT values greater than 140 mg/dl but less than 200 mg/dl are considered to have
impaired glucose tolerance (IGT).16,36,37,38,39,60

Disease Review
36
Management
Physical Activity
Physical activity is an essential component of a healthy life-style and important to
achieve a better self-management of diabetes mellitus.16,19,20,38,50
Nutritional Therapy for Diabetes:
Emphasis should be placed on maintenance of desired weight and glucose, lipid and
blood pressure goals. Loss of 10% of current weight was shown to improve diabetes
control. Strategies may be aimed at improving food selection (e.g., reducing dietary
fats and saturated fats), spreading meals throughout the day, and incorporating regular
exercise habits. If dietary and behavioural intervention is not successful, an
antidiabetic agent may be needed.58,62
Diet:
A well-balanced, nutritious diet remains a fundamental element of therapy. The
American Diabetes Association (ADA) recommends about 45–65% of total daily
calories in the form of carbohydrates; 25–35% in the form of fat of which < 7% are
from saturated fat, and 10–35% in the form of protein. In patients with type 2
diabetes, limiting the carbohydrate intake and substituting some of the calories with
monounsaturated fats, such as olive oil, rapeseed (canola) oil, or the oils in nuts and
avocados, can lower triglycerides and increase HDL cholesterol. In obese individuals
with diabetes, an additional goal is weight reduction by caloric restriction.58,62
The current recommendations for both types of diabetes continue to limit cholesterol
to 300 mg daily, and individuals with LDL cholesterol more than 100 mg/dl should
limit dietary cholesterol to 200 mg daily.
Disease Review
37
High protein intake may cause progression of kidney disease in patients with diabetic
nephropathy; for these individuals, a reduction in protein intake to 0.8 kg/day or about
10% of total calories daily is recommended.
Dietary fiber:
Plant components such as cellulose, gum, and pectin are indigestible by humans and
are termed dietary "fiber." Insoluble fibers such as cellulose or hemicellulose, as
found in bran, tend to increase intestinal transit and may have beneficial effects on
colonic function. In contrast, soluble fibers such as gums and pectins, as found in
beans, oatmeal, or apple skin, tend to retard nutrient absorption rates so that glucose
absorption is slower and hyperglycemia may be slightly diminished. Although its
recommendations do not include insoluble fiber supplements such as added bran, the
ADA recommends food such as oatmeal, cereals, and beans with relatively high
soluble fiber content as staple components of the diet in diabetics. High soluble fiber
content in the diet may also have a favorable effect on blood cholesterol levels. 58,62
Artificial and other sweeteners:
Aspartame (NutraSweet) consists of two major amino acids, aspartic acid and
phenylalanine, which combine to produce a sweetener 180 times as sweet as sucrose.
A major limitation is that it is not heat stable, so it cannot be used in cooking.
Saccharin (Sweet 'N Low), Sucralose (Splenda), Acesulfame potassium (Sweet One),
and rebiana (Truvia) are other "artificial" sweeteners that can be used in cooking and
baking.
Fructose represents a "natural" sugar substance that is a highly effective sweetener,
induces only slight increases in plasma glucose levels, and does not require insulin for
its metabolism. However, because of potential adverse effects of large amounts of
fructose on raising serum cholesterol, triglycerides, and LDL cholesterol, it does not

Disease Review
38
have any advantage as a sweetening agent in the diabetic diet. This does not prevent,
however, ingestion of fructose-containing fruits and vegetables or fructose-sweetened
foods in moderation. 58,62
Micronutrients:
Two minerals commonly mentioned in relation to diabetes are chromium and
magnesium. Chromium deficiency has been related, hypothetically, to development of
diabetes in humans for many years, but persuasive studies in Western people are not
available for recommendation of chromium supplementation for diabetic individuals.
The chromium replacement has beneficial effect on glycemic control is for people
who are chromium deficient as a result of long-term chromium-deficient parenteral
nutrition. However, it appears that most people with diabetes are not chromium
deficient, and thus chromium supplementation cannot be routinely recommended.
Similarly, although magnesium deficiency may play a role in insulin resistance,
carbohydrate intolerance, and hypertension, the available data suggest routine
evaluation of serum magnesium levels only in patients at high risk for magnesium
deficiency. Magnesium should be repleted only if hypomagnesemia is demonstrated.
The magnesium question is controversial, and the ADA held a consensus conference
in 1992 and recommended measuring serum magnesium in persons at risk for
magnesium deficiency. Potassium loss may be sufficient to warrant dietary
supplementation in patients taking diuretics.
Nutritional recommendations for adults with diabetes
Fat:
20–35% of total caloric intake
Saturated fat < 7% of total calories
<200 mg/day of dietary cholesterol
Disease Review
39
Minimal trans fat consumption
Carbohydrate:
45–65% of total caloric intake (low-carbohydrate diets are not recommended)
Protein:
10–35% of total caloric intake (high-protein diets are not recommended)
Other components:
Fiber-containing foods may reduce postprandial glucose excursions
nonnutrient sweeteners
Treatment in Unani medicine
Tadabeer:
Ziabetus Haar: Hammame Garm, Fasde Basalique35
Ziabetus Barid: Tabreed wa Tarteeb, Stay in cold and wet air, Cold Aabzan23,27,46,35
Mufradat:
Aabe Kaddu Biriyan, Aabe Khayar with Isapghol, Aabe Anaar Tursh, Aabe Toot,
Aabe Aalubukhara, Rubbe Anaar, Arqe Gulab, Arade Jaw etc.
Murakkabat:
Qurse Gulnar, Qurse Tabasheer, Qurse Kafoor, Qurse Ziabetus etc.23,27,35
Drug review
40
Gilo
Introduction:
Gilo is a well known drug in Unani medicine. The plant is a climbing shrub growing
in deciduous and dry forest. Gilo was included in the Bengal pharmacopoeia of 1844
and the Indian pharmacopoeia of 1868.65
The Satte Gilo (starch) is obtained from the
roots and stems of the plant are similar to Arrow-root in appearance and effect. It is
used in the treatment of various diseases, particularly common fever, malarial fever,
Diabetes, cuts and wounds.
Botanical Name: Tinospora cordifolia66,67,68,69,70,71,72,73
Family: Menispemaceae66,67,68,69,70,71,72,73
Distribution:
Found throughout tropical India,74
Maynmar, Andman and Ceylon. Ascending to the
altitude of 900 meter.74,75
Vernacular Names:65,66,67,71,76,77
Assamese: Siddhilate, Amarlata
Bengali: Gulancha, Giloe, Gurach, Gadancha, Guluncha, Ningilo,
Golancha
Bombay: Ambravel, Gharol, Giroli, Guloe, Gulwel
Burmese: Singomoni
Ceylon : Chintil
China: K`uan chu Hsing
English: Gulancha Tinospora
French : Culancha
Gujarati: Galac, Garo, Gado, Galo, Gulo, Gulwel
Hindi: Ambarvel, Giloe, Gurcha, Gurach, Gulancha, Gubel,
Drug review
41
Gurudvel, Gulvel
Kannada: Amrutoballi, Amrulballi, Madhuparne, Uganiballi
Kashmiri: Amrita, Gilo, Bark
Kumaon: Gulancha, Guracha
Malayalam: Amrytu, Peyamarytam, Sittamrytu
Marathi: Ambarvel, Gharol, Giroli, Gulvel, Guloe
Nepali: Gurjo
Persian: Gulbel
Punjabi: Batindu, Gilo, Garham, Garum, Gilo-Gularish
Sanskrit : Amrita, Amritalata, Chakrangi, Dhira, Guluchi, Kundalli
Sikkim : Gurjo
Sindhi: Sutgilo
Tamil: Amridavalli, Kaipruchindil, Chindal, Seendal, Sindil
Silam, Kodi, Amudam, Asasi, Kunali, Sadi,
Telegu: Thippateega, Guduchi, Madhuka, Manpala, Somida
Urdu: Gilo
Uriya: Guluchi, Gulochi
Mahiyat (Morphology):
Botanical Description: Gilo is succulent glabrous deciduous climbing shrub pealing
of ash coloured bark. The flowers are small and yellow or greenish-yellow in colour.
The fruits are small and red in colour.
Stem: The stem is succulent, croky and grooved with long pendulous fleshy roots
from the branches.78
Leaves: The leaves are simple, alternate, extipulate, membranous and 7-8 nerved.65,78
Drug review
42
Flowers: The flowers are small and yellow or greenish-yellow in colour. There are
axillary and terminal racemes or racemose panicles. Flowering in April. 65,78
Fruit: The fruits are drupe, ovoid, glossy, succulent, pea-sized and red coloured on
maturity.65,78
Macroscopic Studies
Macroscopically the stems are succulent, soft, possessing long, filiform, aerial root
arising from branches. Bark warty, creamish white or grey brown; wood soft,
perforated. Dried sample consists of 5 to 10cm long conical pieces, light in weight;
bark light and papery, brittle, dark brown; wood with longitudinal surface ridges, and
radially divided into wedge shaped pieces in cross-sections. Pieces difficult to fracture
when fully dried and can be torn only by twisting; odourless; taste bitter.79
Microscopic Studies
Transverse section shows cork, cortex and vasculature. The cork tissue is broken at
some places due to tenticele cortex is wide. The outer zone of cortex consists of 3 to 5
rows of irregularly arranged tangentially elongated chlorenchymatous cell. Several
secretory cells found scattered in the cortex. Vascular zone is composed of discrete
vascular strands, with 10 to 12 or more wedge shaped strip of phloem, alternating
with wide medullary rays.80
Seeds: The seeds are curved.65,78
Part Used: Leaf, stem, stem bark and root.66,74,77,81,82
Mizaj: Har1 Yabis
1
23,27,27,47
Har1 Ratab
1 23,47
Murakkabul Quwa47
Af’al (Actions):
1. Dafae Bukhar (Antipyretic)23,30,27,47,65,67,69,73,77,86

Drug review
43
2. Musakkine Alam (Analgesic)73,69,86
3. Muqawie Bah (Aphrodisiac)65,69,71,81,83,84,86,88,89
4. Qabiz (Astringent)65,69,76,90
5. Mudirre Baol (Diuretic)65,66,67,68,76,85
6. Dafae Suaale (Antitussive)83,89
7. Kasire Riyah (Carminative)84
8. Dafe Atshak (Antisyphilitic) 66,6975,76,78,90
9. Dafae Sozak (Useful in gonorrhea)69,70,77,85,87,88,89,90
10. Ma’ane Naubat (Antiperiodic)65,66,69,79,83,84,85
11. Mussaffie Dam (Blood purifier)76,78,85,89,90
12. Qatile Kirmeshikam (Antihelminthic)76,77,85,90
13. Mukhrije Balgham84
14. Muqawwie Meda76,85,90
15. Mushtahi (Appetizer)84,88
16. Muhallile Awram (Anti-inflammatory)69,73,76,77,89
17. Mowallide Mani (Spermatogouge)84,88
18. Mudire Haiz (Amenogouge)85
Istemaal (Uses):
1. Tape Damwi 83,84
2. Tape Safrawi 83,84,88
3. Alam69,77,83,89
4. Zo’fe Bah81,84,88
5. Aatshak66,69,75,77,78
6. Sozaak69,70,71,85,87,88
7. Bawaaseer65,67,69,77,84
8. Yarqaan65,69,70,77,84,88,89
9. Kirme Shikam81,85,65,76
10. Is’hale Muzmin65,69,71,76,77,84,87,90
11. Qillate Mani84,88
12. Hararate Jigar88
13. Ghashi84,88
14. Hirqatul Baol85
Drug review
44
15. Shozishe Dil wa Jigar83
16. Niqris66,68,69,77,86
17. Zo’fe Ishteha84,88
Ethnobotanical Actions:
1. Hypoglyceamic65,67,68,69,77,82,86
2. Hypocholesterolimic68
3. Immunostimulant 68,69,77
4. Tonic65,67,68,69,70,75,78,83,89,91
5. Antiinflammatory73,86,91
6. Antacid83,86
7. Antioxidant68,69
8. Deobstruent69
9. Antibacterial 69,77
10. Antiallergic68
11. Alterative69,91
12. Antispasmodic69,91
13. Antiviral69
14. Antiulcer68
15. Stimulant91
16. Bronchodialator68
17. Lipolytic69
18. Nutritious83
19. Hepatoprotective69
Ethnobotanical Uses:
1. Fever65, 66,67,76,77,82,87,91
2. Intermittent fever66,75
3. Diabetes65,67,68,69,77,82,91
4. Debility65,66,75,77,78
5. Dyspepsia65,66,77,79
6. Anemia67,69,77
7. Diarrhea83,84
8. Cough66,67,68,77,83,84,88
9. Dysentery65,69,71,76,77,87
10. Dysuria69,77
11. Erysipelas65,68,69,77
12. Escherichia68,69,77
13. Fracture68,77
14. Giddiness77
15. Inflammation73,76,86,91
16. Nausea68,69,77,78
17. Vomiting67,77
18. Rheumatism65,68,69,70,75,79,87
19. Leucorrhoea68,82,91
20. Stress68,77
21. Hypertension65
22. Snake bite67,69,75,77
Drug review
45
23. Tuberculosis69,77,84
24. Spermatorrhoea69,82
25. Filaria77
Miqdare khuraq (Dose): Up to 2 Masha of Satte Gilo
83
Muzir Asrat (Adverse effects):
Various Unani physicians stated that Gilo has almost no side effect84
except Muqi.85
Musleh (Correctives): Tabasheer and Dana Heel.83,84,85
Taste: Bitter83
Badal (Substitute): Gilo83,84
Murakkabat:
Safoofe Satte Gilo81
Arqe Badawar Shikai81
Arqe Gilo81,95
Lauq Sapistan93,94
Lauq Motadil93
Safoofe Ziabetus94
Fawakehe Satte Gilo94
Keemiyai ajza (Chemical constituents):
A variety of constituents have been isolated from Tinospora cordifolia plant and their
structures were elucidated. They belong to different classes such as alkaloids,
diterpenoid lactones, glycosides, steroids, sesquiterpenoid, phenolics, aliphatic
compounds and polysaccharides.66,71,77,78
The stem contains alkaloidal constituents, including berperine; bitter principles,
including berbrin, columbin, chasmenthin, palmerin, tinosporin, tinosporol,
tinosporid, tinosporon, tinosporic acid, tinosporidine, columbin, chasmanthin, giloin,
giloin1,2-substituted pyrrolidine, norclerodanediterpene-O-glocoside,cordifolide,
unosporin cordifol, cordifolone, magnoflorine, tembitarine, cordifoliosides A and
tinosporol.66,71,77,78
Drug review
46
Scientific Reports
Hypoglycemic activity:
The methanol extract of Tinospora cordifolia stem was found to exhibit a signifying
hypoglycemic and antioxidant activity in alloxan induced diabetic rats.96
Oral administration of the water extract of Tinospora cordifolia root caused a
significant reduction in blood glucose, brain lipid level, hepatic glucose-6-
phosphatase, serum acid phosphatase, alkaline and lactate dehydrogenase and increase
in body weight, total haemoglobin and hepatic hexokinase in alloxanized diabetic rats.
97
Tinospora cordifolia shows hypoglycemic activity possibly by stimulating
endogenous insulin secretion by altering the cell membrane permeability. 98
The petroleum ether extract of Tinospora cartdifolia stem administered to rats
significantly decreased the glucose, triglycerides and body weight, and increased the
HDL-cholesterol levels. 99
Compound tinosporaside isolated from the n-butanol fraction of the stem of T.
cordifolia exhibited significant antihyperglycemic activity in streptozotocin-model
which is comparable to metformin.100
Various studies demonstrate amelioration of experimental diabetic neuropathy and
gastropathy in rats, reduction of blood sugar in alloxan-induced hyperglycemic rats
and rabbits, significant reduction in blood glucose and brain lipids, increase in
glucose tolerance in rodents, increase in glucose metabolism,
inhibitory effect on
adrenaline-induced hyperglycemia by pyrrolidine derivative, and significant
hypoglycemic effect in normal and alloxan diabetic rabbits following administration
of T. cordifolia.101,102,103,104
Drug review
47
Anti Allergic Activity
In a clinical study, 100% relief was reported from sneezing in 83% of the patients on
treatment with T. cordifolia,. Thus T. cordifolia significantly decreased all symptoms
of allergic rhinitis and was well tolerated.105
Cardioprotective Activity
A dose-dependent reduction in infarct size and in serum and heart lipid peroxide
levels were observed with prior treatment with T. cordifolia in ischemia-reperfusion-
induced myocardial infarction in rats.106
The stem extract has been normalize alterations in the lipid metabolism caused by
diabetes mellitus in streptozotocin-induced diabetic rats indirectly benefiting the
heart.107
Hepatoprotective
The hepatoprotective action of T. cordifolia was reported in one of the experiment in
which goats treated with T. cordifolia have shown significant clinical and hemato-
biochemical improvement in CCl4 induced hepatopathy. Extract of T. cordifolia has
also exhibited in vitro inactivating property against Hepatitis B and E surface antigen
in 48-72 Hours.108
Anti-stress and tonic property
The anti-stress and tonic property of the plant was clinically tested and it was found
that it brought about good response in children with moderate degree of behaviour
disorders and mental deficit. It has also significantly improved the I.Q. levels. 109
Antispasmodic
The aqueous extract of the stem antagonizes the effect of agonists such as 5
hydroxytryptamine, histamine, bradykinin and prostaglandins E1 and E2 on the rabbit
Drug review
48
smooth muscle, relaxes the intestinal, uterine smooth muscle and inhibits the
constrictor response of histamine and acetylcholine on smooth muscle. 109
Anti-inflammatory
The alcoholic extract of T. cordifolia has been found to exert anti-inflammatory
actions in models of acute and subacute inflammation. 110
Antineoplastic Activity
Intraperitoneal injection of the alcoholic extract of T. cordifolia has been shown to
Dalton's lymphoma (DL) bearing mice stimulated macrophage functions like
phagocytosis, antigen-presenting ability and secretion of Interleukin-1 (IL-1), tumour
necrosis factor (TNF) and Reference Nutrient Intake (RNI) as well as slowed tumor
growth and increased lifespan of the tumor-bearing host. 111
Osteoprotective Activity
Rats treated with T. cordifolia showed an osteoprotective effect, as the bone loss in
tibiae was slower than that in controls. Serum osteocalcin and cross-laps levels were
significantly reduced. This study demonstrates that extract of T. cordifolia has the
potential for being used as antiosteoporotic agent.112
Antifertility Activity
Oral administration of 70% methanolic extract of T. cordifolia stem to male rats at a
dose level of 100 mg/d for 60 days did not cause body weight loss but decreased the
weight of testes, epididymis, seminal vesicle and ventral prostate in a significant
manner.113
Anti Ulcer Activity
Treatment with a formulation containing T. cordifolia has been shown to reduce ulcer
index total acidity,with an increase in the pH of gastric fluid in pylorus-ligated rats
and in the ethanol-induced gastric mucosal injury in rats.114

Drug review
49
Anti Leprotic Activity
T. cordifolia is used for its kushtahara (anti-leprotic) properties, along with wide use
in kandu and visarpa (types of skin disorders) and has been shown to exert anti-
leprotic activity in a combination formulation.115
Diuretic Activity
In a scientific study on rats and human volunteers, T. cordifolia was found to have
diuretic effects.116
It was also found effective in modulation of morphology and some
gluconeogenic enzymes activity in diabetic rat kidney. 117
Drug review
50
Tabasheer
Introduction:
Tabasheer is a well known drug in Unani medicine. It is obtained from the stem’s
internodes of Bambusa bambos, a genus of large erect some-times climbing plants,
known as bamboos, found in tropical, sub tropical and moist part of Asia, Africa and
America. Approximately 33 species occurs in India. Bambusa bambos syn. B.
arundinacea is a graceful, spinous bamboo, distributed throughout the moist part of
India, upto an altitude of 1250 meter, particularly near river banks and on the hills of
Andhra Pradesh, Tamil Nadu and Karnataka. It possesses property like Mufarreh
Qalb, Mubarrid, Muqawwie qalb wa jigar and Muqawwie meda and mainly used in
the treatment of various diseases, particularly in palpitation, fever and dyspepsia.
Botanical Name: Bambusa bambos68,69,71,73,76
Family: Gramineae68,69,71,73,76
Vernacular Names:76,77,78,91
Arabi: Tabasghir, Qasab
Assami: Kotoha, Bnah, Kata, Koto, Kotoha
Bengali: Bans, Behurbans, Ketua, Kutuasi, Bansha
English: Spiny Bamboo, Thorny Bamboo, Bamboo
Gujrati: Toncor, Wans, Gemeiner Bambos, Bans
Hindi: Bans, Kanta Bans, Kattang, Magarbans, Malbans
Kanada: Biduri
Malyalam: Illi, Kampu, Kaniyaram, Karmmaram, Mula, Mulmulam, Pattil,
Tejanam, Trinadhavajan, Valiyamula, Venu Mungil, Moongil
Marathi: Dougi, Kalak, Mangda, Padhai, Conogui, Kanaki, Vellu, Bans,
Bambu
Drug review
51
Punjabi: Magar
Tamil: Onteveduru, Ambal, Ambu, Aril, Iraivarai, Kalai, Kambul,
Mulai, Bongu, Kuluaimungil, Masukkaram, Miruttusam, Nettil,
Tattai, Panai, Valai, Vanu, Viyal, Vindil, Mungil, Mangal,
Moongilanisi, Moongiluppu
Telgu: Bongu, Bonguveduru, Kichaakmu, Amskaramu,
Mudusuveduru, Petiveduru, Trinadhvajamu, Veduru, Bonga,
Vedurubeeam, Vederuppu
Botanical description:
Leaves: Linear or linearlanceolate, 7-18 cm in length and 2-20 mm in width.66,67,68
Rhizomes: Short stout, knotty; culms dense, reaching 24-30 m in height and 15-17
cm in diameter, green hollow, purplish green when young, turning golden yellow,
with prominent nodesand long internodes, lower once rooting.67,68,77,78
Flowers: It flowers gregariously once in 30-45 years, occurs in large penicles,
sometimes occupying the whole stem. Flowering in the summer season and fruits later
on.68,78
Distribution: A common bamboo found throughout India, up to an altitude of 1250
meter particularly near the river banks, in Central and South India on the Nilgiri66
Also cultivated in many places in North West India and Bengal. It is also found in Sri
Lanka, Malasia, Peru and Myanmar.67,71
Cultivation: It is cultivated only in the lower Himalayas and in the valleys of Ganges
and Indus.77,78
Part Used: Leaf, roof, shoot, seed and tabasheer.77,78

Drug review
52
Tabasheer
The bamboo manna or tabasheer is the siliceous secretion found in the internodes of
the stems.68,118
It is a white camphor like crystalline in appearance, slightly sticky to
the tongue and sweet in the taste. 77,118,119
It is consist of irregularly shaped
fragments of an opaque white or bluish opalescent colour, the larger pieces are about
an inch in diameter, concavo-convex, and have evidently drived their form from the
joint of the bamboo in which the deposit has collected.70
Chemical constituent
Tabasheer- Silica 90.56%, Potash 1.10%, peroxide of Iron 0.90%, Almina 0.40%
Moiture 4.87%.66,77
Taste: Sweet
Mizaj: Sard3 Khushk
3 83
Sard2 Khushk
3 23,120
Musleh: Mastagi, Honey and Unnab. 23,120
Badal: Tukhme Khurfa biriyan, Simaq, Gile Makhtoom and Sandal
safed.23,83,84,85,88
Murakkabat:
Habbe Jadwar93,121
Khameera Marwareed93,123
Jawarish Anarain93,95,123
Jawarish Ood Tursh93,95,121
Jawarish Tamrhindi95,121
Safoofe Kushta Qalai,93,123
Qurse Sartaan Kafoori93
Jawarish Tabasheer95,121,122,123
Habbe Paan94
Habbe Amber Momiyai95
Habbe Ghafis94
Dawaul Misk Sada94,123
Dawaul Misk Motadil94,123
Dawaul Misk Jawaharwali94,123
Safoofe Teen94,95

Drug review
53
Doses: 3.5-7 Masha, 1-3 gm67,78
Af’al:
1. Qabiz (Astringent)23,83,92,124
2. Mufarreh Qalb83,84,88
3. Mubarrid (Cooling effect)23,90
4. Muqqawwie Qalb wa Jigar (Tonic for heart and liver)23,66,84,85,88,90,120,124,125
5. Muqqawwie Meda23,83,85,124
6. Mussakkine Astash23,83,84,88,90,120,125
Ethanobotanical Actions:
1. Hypoglycaemic118
2. Emmenagogue66,68,71,91,126
3. Anthelmintic66,68,91
4. Blood purifier68
5. Febrifuge66,68
6. Analgesic77
7. Antiinflammatory77
8. Ulcer healing77
9. Antinfertility77
10. Stimulant66,91
11. Antispasmodic66
12. Sedative66
Actions of Tabasheer:
1. Tonic67,70,71
2. Cooling67,70
3. Aphrodisiac67,71,77
4. Astringent66,68,70,90
5. Expectorant67
6. Carminative67
7. Antipyretic71,77
Ethnobotnical Uses:
1. Haematemesis66,70,71,126
2. Haemoptysis66
3. Cold and cough66,67,70,71,126
4. Ulcer77,78
5. Gonorrhea66,68,91
6. Palpitation66
7. Vomiting66
8. Thread worms66

Drug review
54
9. Leukoderma78
10. Ring worm78
Uses of Tabasheer:
1. Fever66,68,71,77
2. Cough67,71
3. Asthma66,67,77
4. Leprosy66,77,78,91
5. Anaemia77
6. Burning sensation77
7. Snake and Scorpion bite66,77
8. Thirst66,70
9. Urinary infection67
10. Debilitating diseases66,67
11. Aphthous70
12. Bilious dyspepsia70
13. Bronchitis68
14. Tuberculosis70
Drug review
55
Kanwal Gatta
Introduction:
The Kanwal Gatta (Nelumbo nucifera) is a fresh-water plant that grows in
semitropical climates. It originated in India and used as food and a medicinal herb for
over 1,500 years. It is cultivated extensively in Southeast Asia, primarily for food and
rarely for the medicinal purpose. All parts of the plant are utilized, but the primary
reason for its current widespread cultivation is to collect the rhizomes and seeds. It
possess properties like astringent, cardiotonic, febrifuge, hypotensive, tonic and
vasodilating activities and mainly used for the treatment of Hiddate Dam, Zarbatus
Shamsh and Amraze Safravi.
Vernacular Names:65,66,71,76,86,119,127
Arabic : Nilufer, Ussulneelufir
Assamese: Podum
Bengali: Padma, Kamal, Pankaj, Kombol, Swet Padma
Burmese: Pa-dung-ma
Deccan: Kungwelka-gudda
English: Sacred lotus, Egyptran, or phythogoreen been, Indian lotus
Chinese Waterlily, Egyptian lotus
French : Nelumbo
German: Pactige nelumbo
Gujarati: Suriyakamal
Hindi: Kamala, Kanwal
Kannad: Kamala, Tavaregadde, Tavaribija, Taveri
Kashmiri: Pamposh
Khasi: Soh-lapudong

Drug review
56
Malyalam: Thamara, Santhamra, Arvindam
Marathi: Kamal
Mundari: Salukid ba, U palba, Kombol Ba
Oriya: Pudamj
Panjabi: Kanwal, Pamposh, Kanwalkakri, Bhe or phe (Root)
Persian : Nilufer, Nilufu, Bey Khaeelufir
Sanskrit: Ambuja, Padma, Pankaja, Kamla, Kamlam, Swet Kamla
Shatapatra
Sinbalese: Nelum
Sindhi: Pabbon (plant), Beh (root) Paduro (Seeds), Nilofir (drug)
Tamil: Ambal, Thamarai, Shivapputamaraver
Telgu: kalung, Cerra-tameara
Botanical Name: Nelumbo nucifera66,67,68,72,73,89
Family: Nymphaeceae66,67,68,72,73,89
Distribution:
An aquatic herb found throughout the India, and Pakistan also found in Persia, Sri
Lanka, China, Cochin China, Japan, Malay Islands, Philippines, and throughout
Nepal, tropical Australia upto an altitude of 1800 meter.72
Description: It is large aquatic herb with stout creeping yellowish white or whitish
brown coloured rhizome sending out roots at the nodes. The leaves are two types arial
and floating both of which are orbiculare, large peltate, entire, glaucous and leathery.
On drying they become membranous. The diameter is 0.3 to 0.6 meter or more.67,77
Flowers: Flower is white or red, fragrant having diameter 10-25 cm; peduncles
coming from the nodes of the stem. Sepals, petals and stamens numerous and spirally
arranged.
Drug review
57
Fruits: An aggregate of indehiscent nut-lets, which remain loosely embedded in the
cavity of the enlarge spongy torous seeds having three cotyledons, green large top
shaped, 5-10 cm. in diameter and spongy.65,66,67
Ajzae Musta’mala (Parts used):
Flowers, filaments, anthers, stalks, seeds, leaves and roots i.e. entire plants66
.
Maghz.92
Mizaj (Temperament):
Sard Tar (Maghe Kham)83,88,90
Sard Khushk (Maghe Pukhta)83
Af’al (Actions):
1. Musakkine Atash67,83,84,85,88,90
2. Musakkine Safra67,84,85,88,90,92
3. Qate Safra83
4. Musaffie Dam83
5. Qabiz83,88,90
6. Nafe Juzam83
7. Dafe Qai (Anti emetic) 67,72,83
8. Mudirre Baul (Diuretic)72,83,85
9. Nafae Ishal
(Antidiarrhoeal)72,84
10. Mughallize Mani92
11. Dafe Bukhar66,67,84
12. Habisud Dam84
13. Muqawwie Bah84
Istemaal (Uses):
1. Qai67,83,91
2. Zarbatus Shams83
3. Ishal72,83,85,88
4. Jiryan83,85,92
5. Sailan85
6. Bukhar66,67,83
7. Zo’fe Bah83
8. Amraze Chashm66,67,120
9. Amraze Jild66,67,72,120
10. Sual120
11. Shaqeeqa (Migraine) 120
12. Fasade Dam83
13. Atsh83,84,85,88,90
14. Juzam83

Drug review
58
15. Bawaseer Damvi84
Ethnobotanical Actions:
Seeds;
1. Demulcent66
2. Nutritive66
Filament and flower;
1. Cooling66,67,72,128
2. Sedative66
3. Astringent66,128
4. Expectorant66
5. Tonic66
6. Antidote to Snake66
Ethnobotanical Uses:
1. Insomnia119
2. Haemorrhage119
3. Haematemesis119
4. Haematuria119
5. Bloody stools119
6. Uterine haemorrhage119
7. Dysentery66,72,119
8. Fever67
9. Piles67,72
10. Menorrhagia66
11. Leprosy66,67
External Uses:
1. Burning Skin66
2. Cephalgia66
Miqdare Khuraq (Dose): 3-5 Masha92
Muzir Asrat (Adverse effects): Der Hazm84
Musleh (Correctives): Shahad,84,88
Nabat Safed83
Badal (Substitute): Tukhme Amla, Sharbate Aalubukhara84
Keemiyai ajza (Chemical constituents):
The leaves contain following alkaloids:
1. Nuciferine76,127,128
2. Roemerine72,127
3. Non nuciferine and the
flavanoid quercetin72,76,127
Drug review
59
4. Isoquercetin72
5. Nelumbin72
6. Leukoanthocyanidin72
The flower contains:
1. Quercetin66,72,76
2. Luteolin and their glycosides72,76
3. Kaempferol glycosides72
4. Robinine76
Scientific Reports:
The antidiabetic activity of methanolic extract of Nelumbo nucifera was carried out
which showed that it decreased the blood sugar levels significantly.129
The antioxidant activity of crude polysaccharides was carried which showed that
crude polysaccharides have distinct antioxidant capacity when compared with
vitamin C as the positive control.131
It was found that natural products from Nelumbo nucifera rhizomes were have
potencies to counter oxidation, inhibit key HIV-1 enzymes and affect immune
regulation. Most chemically synthetic HIV-1 inhibitors could not deal with the mutant
virus. Natural products with multiple anti- HIV-1 effects may circumvent this
disadvantage. Therefore, the present investigation may be importance to anti HIV-1
drug development and application of natural products in HIV-1 therapy.129,130
It was found that both white and pink Nelumbo nucifera flower extracts showed
effective antiplatelet activity in a dose-dependent manner with maximum activity at
500μg/ml concentration. Furthermore, the antiplatelet activity of white flowers was
relatively high compared to the pink flowers.132
Methodology
60
Methodology
The present study entitled as “Clinical Study of Ziabetus Shakari (Diabetes
Mellitus Type II) and Evaluation of Efficacy of a Unani Formulation in its
Management” has been carried out at the department of Moalajat in National
Institute of Unani Medicine (NIUM), Bangalore. Before starting study, the protocol
was submitted for ethical clearance. Accordingly Institutional Ethical Committee had
approved the protocol. Subjects were selected from OPD of NIUM Hospital, after
clinical examination with detail history of the disease and necessary haematological,
biochemical investigations. Clinical symptoms, history and investigations were
recorded on the prescribed Case Report Form (CRF) designed for the study with
specific inclusion criterion. The clinical study was started by enrolling eligible
patients into Test and Control groups by random allocation. This study stretched from
September 2010 to February 2012. A total of 50 patients were screened for the study.
During screening, 10 patients did not fulfil inclusion criteria so not included in the
study, remaining 40 patients were randomly allocated into Test (Group A) and
Control (Group B) groups respectively by lottery method. But 4 patients from Test
group and 5 patients from Control group were lost the follow-up, leaving behind
dropouts 16 patients in Test and 15 patients in Control group who completed the
course of treatment. Statistical analysis was done on 31 patients who completed the
course of treatment. All the patients were kept under strict observation.
1. Criteria for Selection of Subjects
a) Inclusion criteria: Diagnosed cases of Ziabetus Shakari (Diabetes Mellitus Type
II) with blood sugar level:
Fasting blood sugar (FBS) > 126mg/dl
Post Prandial blood sugar (PPBS) > 200mg/dl
Methodology
61
HbA1c >7%
Patients between 35-65years of age of either sex.
Patients ready to participate in the study and ready to follow the instructions.
Patients having ALT, AST, Serum creatinine and Blood urea within normal
limit.
b) Exclusion Criteria:
Patients below 35 and above 65 years of age.
Patients of Insulin dependent diabetes mellitus (Type I).
Patients of Gestational Diabetes.
Patients of Malnutrition related diabetes mellitus.
Complicated cases of Diabetes Mellitus (Diabetic ketoacidosis, retinopathy,
neuropathy, nephropathy, coronary artery disease, peripheral vascular disease,
cerebrovascular disease, liver disease)
Pregnancy and lactation.
Advanced liver, kidney, cardiac, pulmonary diseases.
Patients who fail to follow up.
Patients who fail to give written consent.
2. Selection of subjects:
After the screening, during the selection of the patients, complete history including
general physical and systemic examination was carried out and recorded on a
prescribed case report form which was designed according to the objectives of the
study. A detailed history was recorded regarding their chief complaints with duration,
age, sex, religion, marital status, occupation, address, socioeconomic status on the
basis Kuppaswamy’s socioeconomic scale. Personal history, treatment history, past
history of any disease and family history were also recorded in a predesigned
Methodology
62
proforma. After history taking, general physical examination was done with special
emphasis on height (in cm), weight (in kg), pulse rate/minute, blood pressure in mm
of Hg, peripheral pulses, presence of carotid, subclavian or vertebral bruit. Any other
positive finding during general physical examination was recorded in CRF. Likewise,
a careful systemic examination of cardiovascular system, respiratory system, renal
system, gastrointestinal system was also done to look for any findings of other serious
illness. After that detailed examination specific to the diabetes mellitus was carried
out in all the patients. During examination, common and uncommon manifestations of
diabetes were also assessed like, dehydration, sweet smells of ketones in breath in
diabetic ketoacidosis, skin infections with boil and abscesses, acanthosis nigricans in
the axillae and groins, necrobiosis lipoidica on the shin and eruptive xanthomata.56
Physical Examination
1. Pinprick sensation, sensation to light touch, and pain sensation.
2. Vibration sense.
3. Motor disturbances (decreased deep tendon reflex, weakness and atrophy of
interossei muscles); the patient has trouble picking up all small objects, dressing, and
turning pages in a book.
5. Diplopia, abnormalities of visual fields.
6. Evidence of dehydration (tachycardia, hypotension, dry mucous membranes,
sunken eyeballs, poor skin turgor).
7. Clouding of mental status.
8. Tachypnea with air hunger (Kussmaul’s respiration).
9. Fruity breath odour (caused by acetone).

Methodology
63
3. Assessment of Mizaj
Determination of Mizaj was done on the basis of assessment of different parameters
mentioned in classical Unani literature. These parameters have been shown in the
table attached with the case record form in the annexure.
4. Informed consent
Patients coming under the inclusion criteria mentioned above were given the
information sheet having details regarding the nature of the study, the drug to be used,
method of treatment etc and explained verbally also about study. Patients were given
enough time to go through the contents of informed consent sheet. They were given
the opportunity to ask any question and if they agreed to participate in the study, they
were asked to sign the informed consent form.
5. Investigations
Certain investigations were carried out with the aim to exclude the patients with
pathological conditions mentioned under exclusion criteria and to assess the efficacy
of treatment group and to establish the safety of the test drug.
Following investigations were done in each and every case before and after the
treatment to evaluate the safety of the Unani formulation.
Hb%, TLC, DLC,
Urine routine and microscopy
AST ALT
Blood Urea, Serum Creatinine, Serum Uric Acid
ECG
Following investigation were done on each and every follow up as: 0 day, 15th
day,
30th
day and 45th
day for the diagnosis and evaluation of the efficacy of the drugs.
FBS

Methodology
64
PPBS
Urine sugar
HbA1c (done on 0 day and 45th
day of follow up)
6. Method of Collection of Data
Through clinical study of patients visiting Moalajat OPD, NIUM, Bangalore.
a) Subjective parameters:
Polyuria
Polydipsia
Polyphagia
Tiredness
Progressive weakness
Dizziness
Unexplained weight loss
Pruritus
b) Objective parameters:
Fasting blood sugar
Post prandial blood sugar
Urine sugar
HbA1c
7. Study design
The study was designed as a randomized single blind with standard controlled clinical
trial.
8. Sample size
The sample size was fixed as 40 patients.
Methodology
65
9. Allocation of subjects into groups
Forty patients were randomly allocated by using simple randomization method into
two groups comprising 20 patients in each of Test (Group A) and Control (Group B)
group respectively.
10. Duration of protocol
The treatment period in both Test and Control groups was determined as 45 days.
11. Follow up during treatment:
Patients were kept under strict observation and advised to come forth weekly in OPD
for the assessment of disease till the completion of study. 45 days study was divided
into three visits of follow up, which were made at an interval of 15 days. At every
visit, patients were asked about the progression or regression in their symptoms, and
subjected to assess the clinical findings; and were investigated for FBS, PPBS and
urine for sugar.
12. Test drug:
The ingredients of test formulation are given below.
1. Satte Gilo (Tinospora cardifolia)
2. Tabasheer (Bambusa bambos)
3. Magaze Kanwal Gatta (Nelumbo nucifera)
13. Control drug:
Diabecon
14. Method of preparation, dosage and mode of administration of test drug
The ingredients were provided by pharmacy of National Institute of Unani Medicine.
Proper identification of the ingredients was done by chief pharmacist, National
Institute of Unani Medicine, to make certain their originality and authenticity. The
drugs were cleaned by weeding out superfluous material and impurities. All the
ingrediants were taken in equal quantity and pulverised to make a fine powder, after
Methodology
66
that tablet were prepared by automated tablet making machine. The tablets were
prepared for exact quantification of drug dose and for patient convience to use. Each
patient in Test group was given test drug in the dose of 3 gm twice a day in the form
of tablet (4 tablets twice a day each tablet weighing 750 mg of test drug).
15. Administration of standard control drug
The control drug Diabecon was purchased from the market and 2 tablets were advised
orally twice a day in Group B.
16. Withdrawal criteria
a) Failure to follow the protocol
b) Any adverse reaction or adverse event
c) Drug defaulters
17. Adverse drug documentation
No adverse event or reaction was noted during the test or control drug administration.
18. Methods
The GCP (Good Clinical Practice) was adopted and regular monitoring was done as
per prescribed proforma.
19. Documentation
The case record form and consent forms were submitted to the Dept. of Moalajat after
completion of the study.
20. Statistical analysis:
The results were analyzed statistically by Friedman test, Kruskal-Wallis with Dunn’s
multiple comparisons test, Wilcoxon matched pairs test, Repeated measures ANOVA
with post test, Paired and unpaired ‘t’ tests and data was analyzed by using instat
graph pad and difference in the treatment groups were considered significant at
p<0.05.
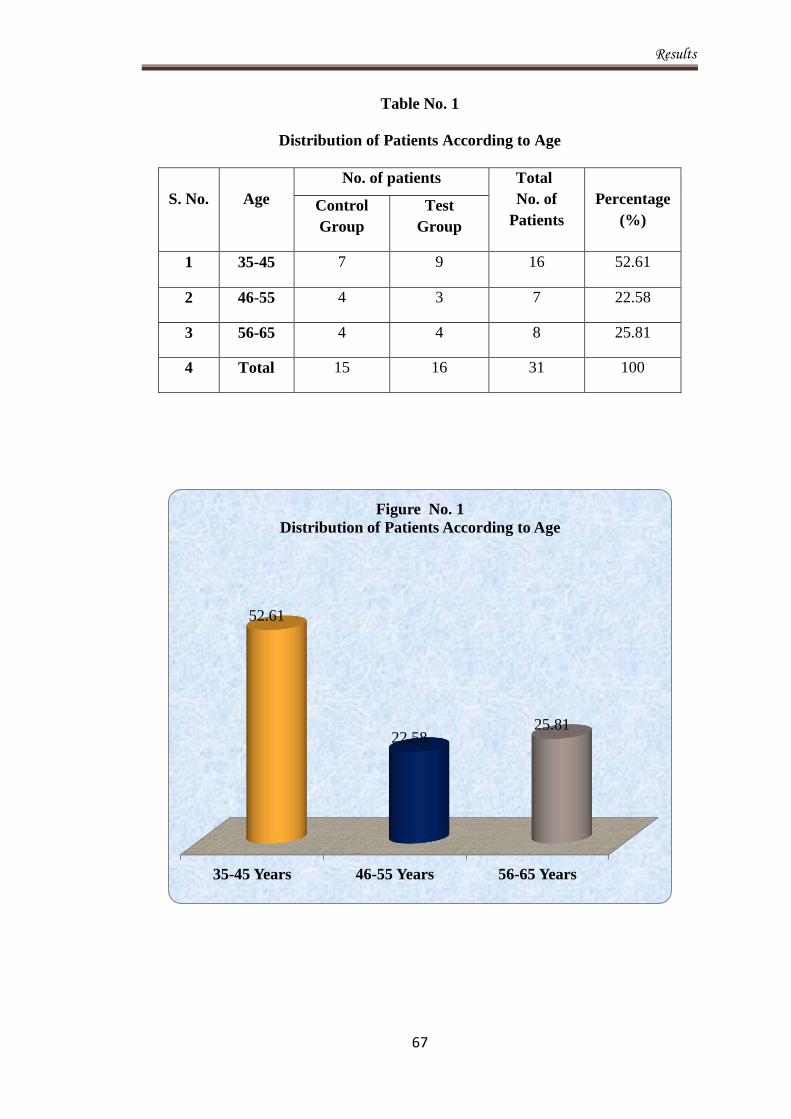
Results
67
Table No. 1
Distribution of Patients According to Age
S. No.
Age
No. of patients Total
No. of
Patients
Percentage
(%) Control
Group
Test
Group
1 35-45 7 9 16 52.61
2 46-55 4 3 7 22.58
3 56-65 4 4 8 25.81
4 Total 15 16 31 100
35-45 Years 46-55 Years 56-65 Years
52.61
22.58 25.81
Figure No. 1
Distribution of Patients According to Age
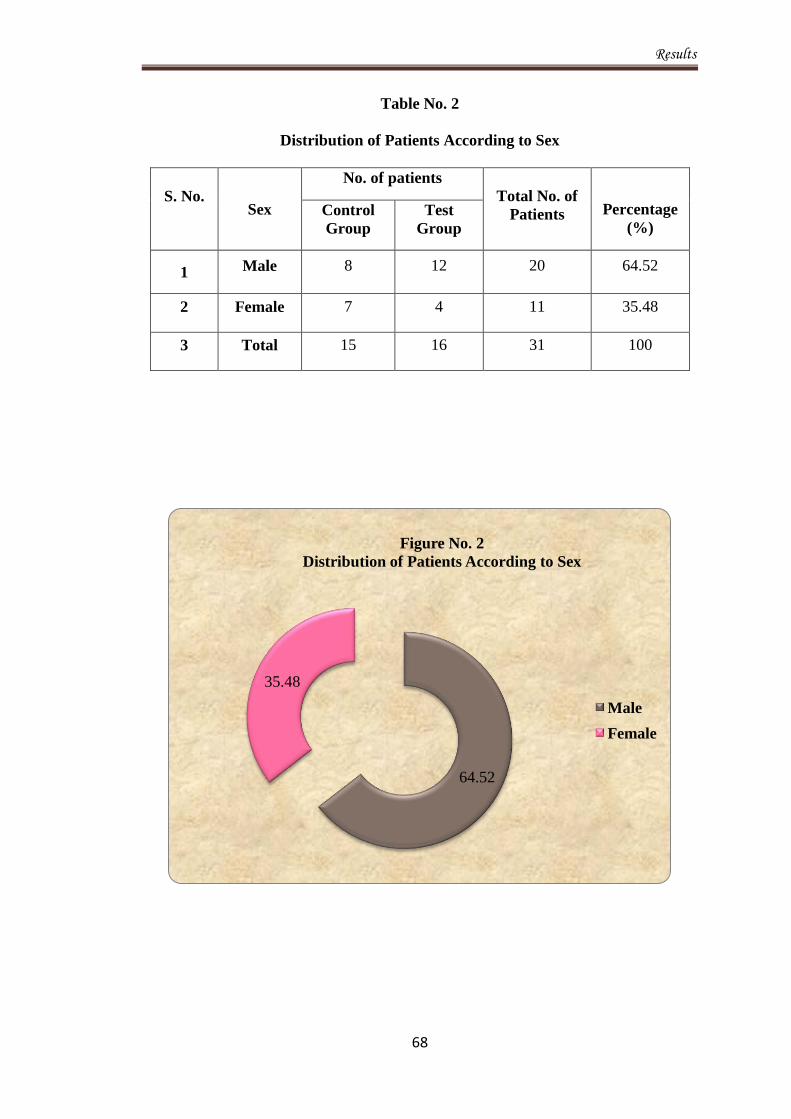
Results
68
Table No. 2
Distribution of Patients According to Sex
S. No.
Sex
No. of patients
Total No. of
Patients
Percentage
(%) Control
Group
Test
Group
1 Male 8 12 20 64.52
2 Female 7 4 11 35.48
3 Total 15 16 31 100
64.52
35.48
Figure No. 2
Distribution of Patients According to Sex
Male
Female

Results
69
Table No. 3
Distribution of Patients According to Religion
S. No.
Religion
No. of patients
Total
No. of
Patients
Percentage
(%) Control
Group
Test
Group
1 Muslim 13 9 22 71
2 Hindu 2 7 9 29
4 Total 15 16 31 100
Hindu Muslim
29
71
Figure No. 3
Distribution of Patients According to Religion

Results
70
Table No. 4
Distribution of Patients According to Marital Status
S. No.
Marital Status
No. of patients
Total
No. of
Patients
Percentage
(%) Control
Group
Test
Group
1 Married 15 16 31 100
2 Unmarried 0 0 0 0
3 Total 15 16 31 100
100
0 0
20
40
60
80
100
120
Married Unmarried
Figure No. 4
Distribution of Patients According to Marital Status
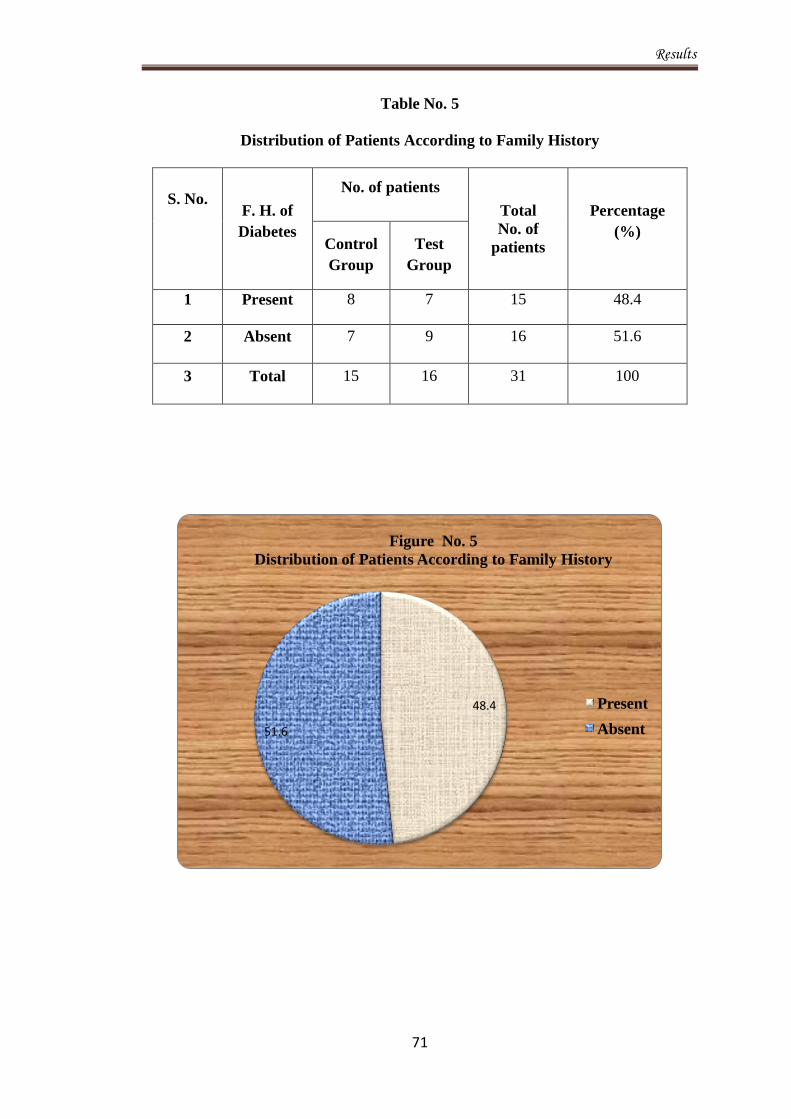
Results
71
Table No. 5
Distribution of Patients According to Family History
S. No. F. H. of
Diabetes
No. of patients
Total
No. of
patients
Percentage
(%) Control
Group
Test
Group
1 Present 8 7 15 48.4
2 Absent 7 9 16 51.6
3 Total 15 16 31 100
48.4
51.6
Figure No. 5
Distribution of Patients According to Family History
Present
Absent

Results
72
Table No. 6
Distribution of Patients According to Socio-economic Status
S.
No.
Socioeconomic
Status
No. of patients
Total
No. of
Patients
Percentage
(%)
Control
Group
Test
Group
1 Upper (I) 0 0 0 0
2 Upper Middle (II) 3 3 6 19.36
3 Lower Middle (III) 4 7 11 35.49
4 Upper Lower (IV) 6 6 12 38.72
5 Lower (V) 2 0 2 6.45
6 Total 15 16 31 100
Upper(I)
Upper
Middle(II)
Lower
Middle(III)
Upper Lower
(IV)
Lower(V)
0
19.36
35.49
38.72
6.45
Figure No. 6
Distribution of Patients According to SES
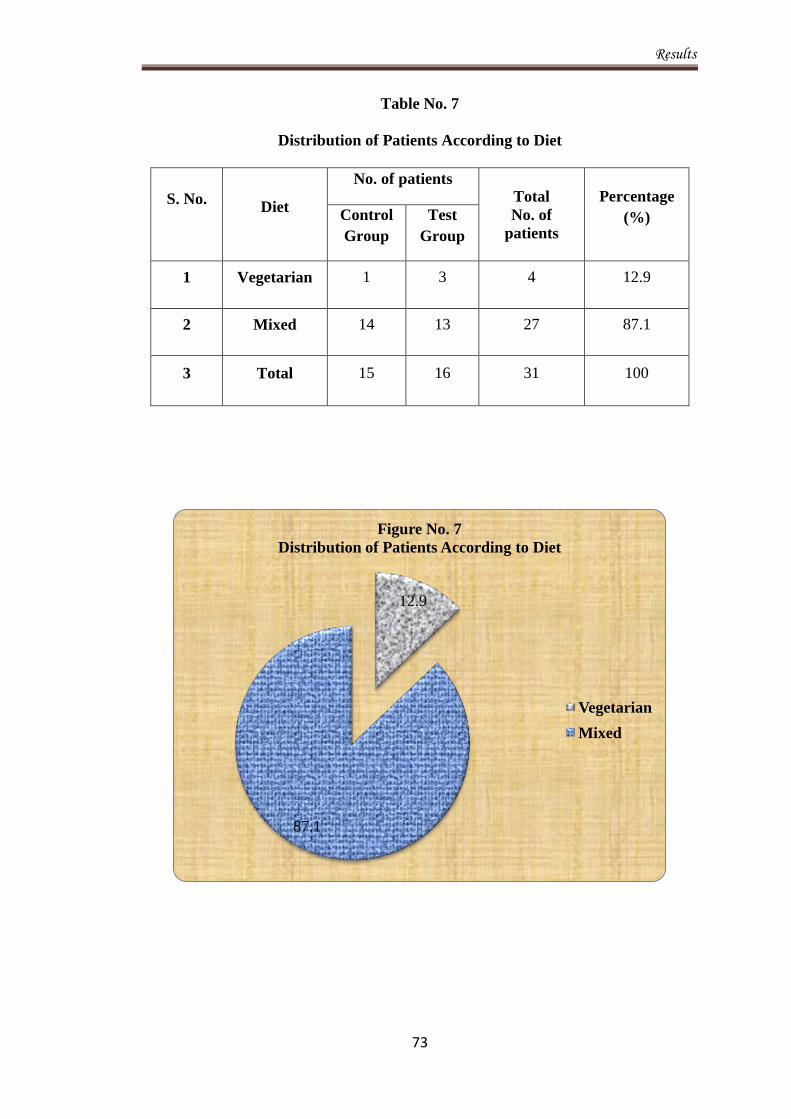
Results
73
Table No. 7
Distribution of Patients According to Diet
S. No. Diet
No. of patients Total
No. of
patients
Percentage
(%) Control
Group
Test
Group
1 Vegetarian 1 3 4 12.9
2 Mixed 14 13 27 87.1
3 Total 15 16 31 100
12.9
87.1
Figure No. 7
Distribution of Patients According to Diet
Vegetarian
Mixed
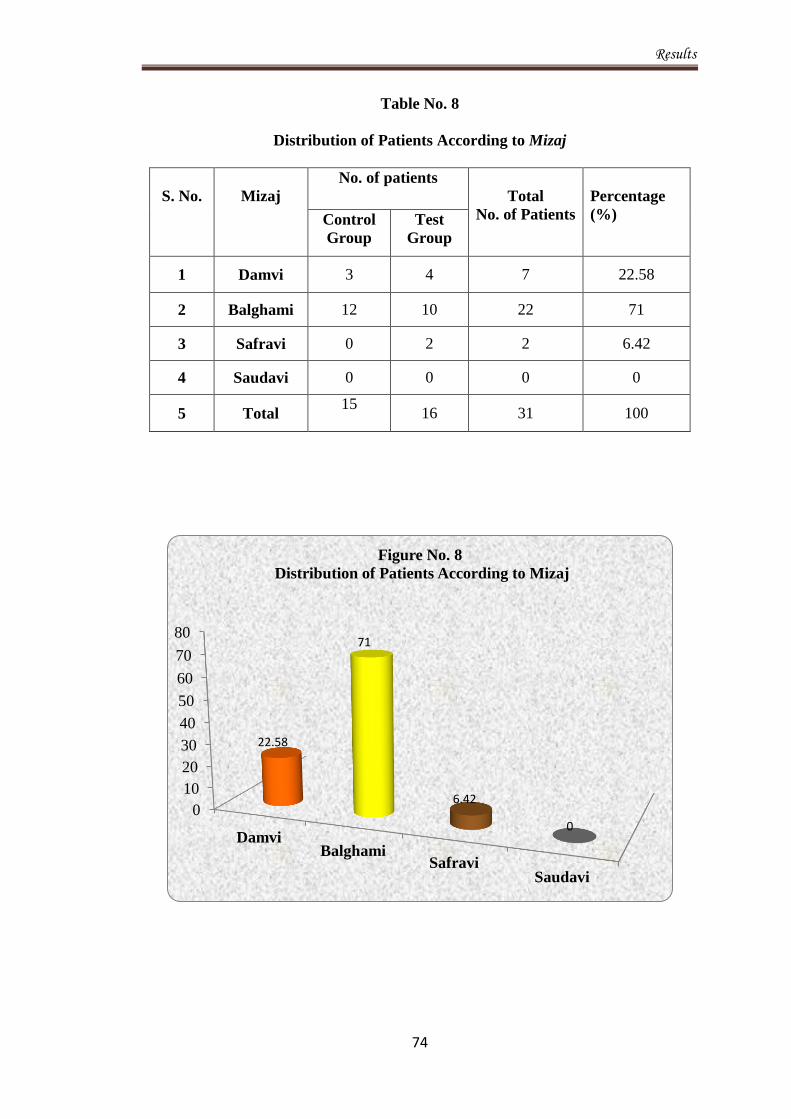
Results
74
Table No. 8
Distribution of Patients According to Mizaj
S. No.
Mizaj
No. of patients
Total
No. of Patients
Percentage
(%) Control
Group
Test
Group
1 Damvi 3 4 7 22.58
2 Balghami 12 10 22 71
3 Safravi 0 2 2 6.42
4 Saudavi 0 0 0 0
5 Total 15
16 31 100
0
10
20
30
40
50
60
70
80
Damvi Balghami
Safravi Saudavi
22.58
71
6.42
0
Figure No. 8
Distribution of Patients According to Mizaj
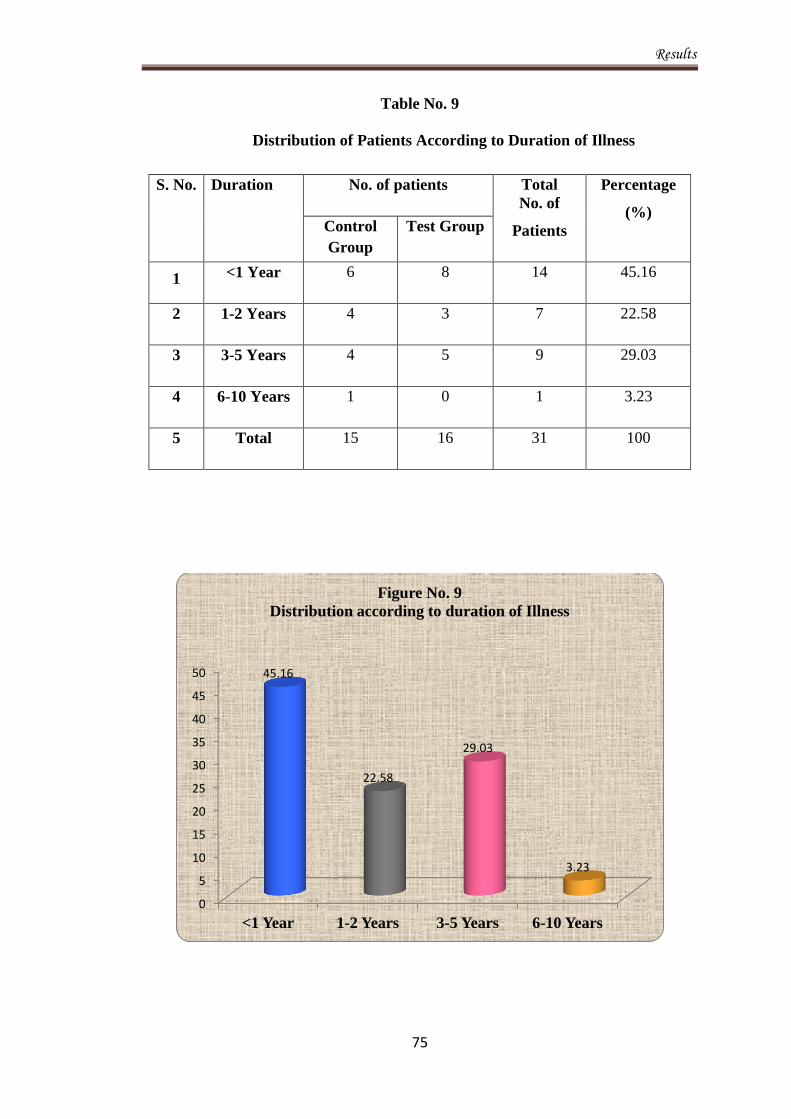
Results
75
Table No. 9
Distribution of Patients According to Duration of Illness
0
5
10
15
20
25
30
35
40
45
50
<1 Year 1-2 Years 3-5 Years 6-10 Years
45.16
22.58
29.03
3.23
Figure No. 9
Distribution according to duration of Illness
S. No. Duration No. of patients Total
No. of
Patients
Percentage
(%) Control
Group
Test Group
1 <1 Year 6 8 14 45.16
2 1-2 Years 4 3 7 22.58
3 3-5 Years 4 5 9 29.03
4 6-10 Years 1 0 1 3.23
5 Total 15 16 31 100
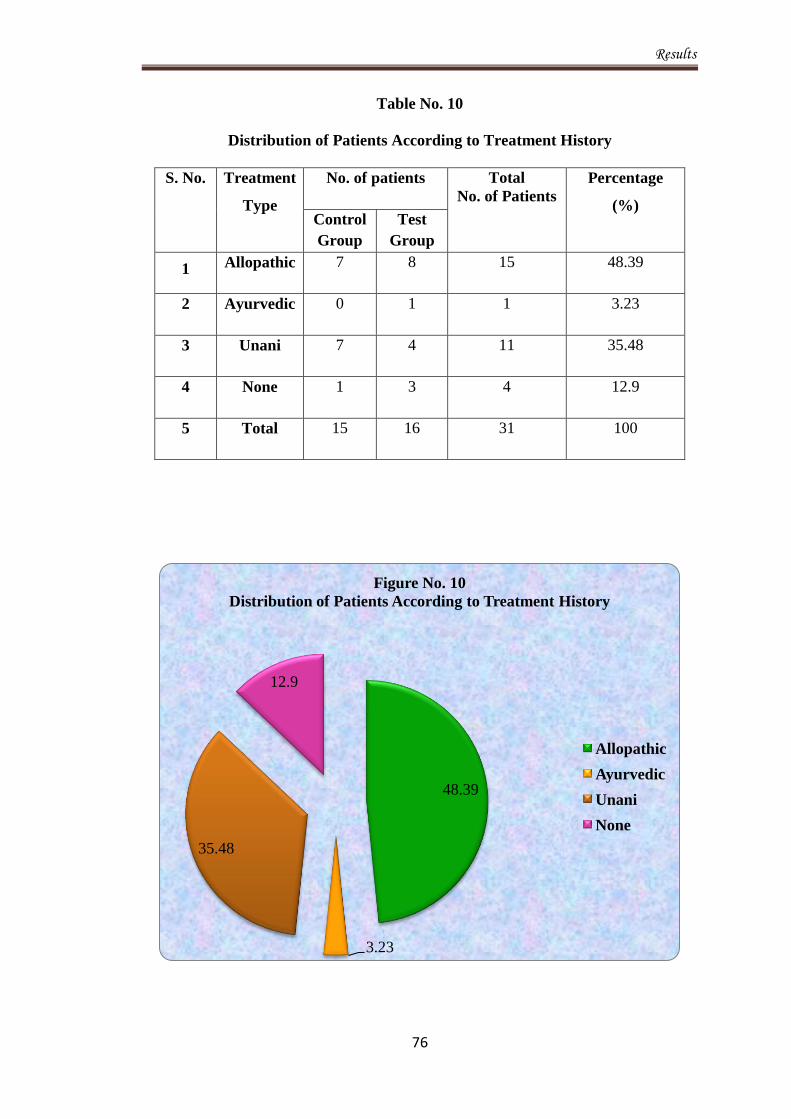
Results
76
Table No. 10
Distribution of Patients According to Treatment History
S. No. Treatment
Type
No. of patients Total
No. of Patients
Percentage
(%) Control
Group
Test
Group
1 Allopathic 7 8 15 48.39
2 Ayurvedic 0 1 1 3.23
3 Unani 7 4 11 35.48
4 None 1 3 4 12.9
5 Total 15 16 31 100
48.39
3.23
35.48
12.9
Figure No. 10
Distribution of Patients According to Treatment History
Allopathic
Ayurvedic
Unani
None
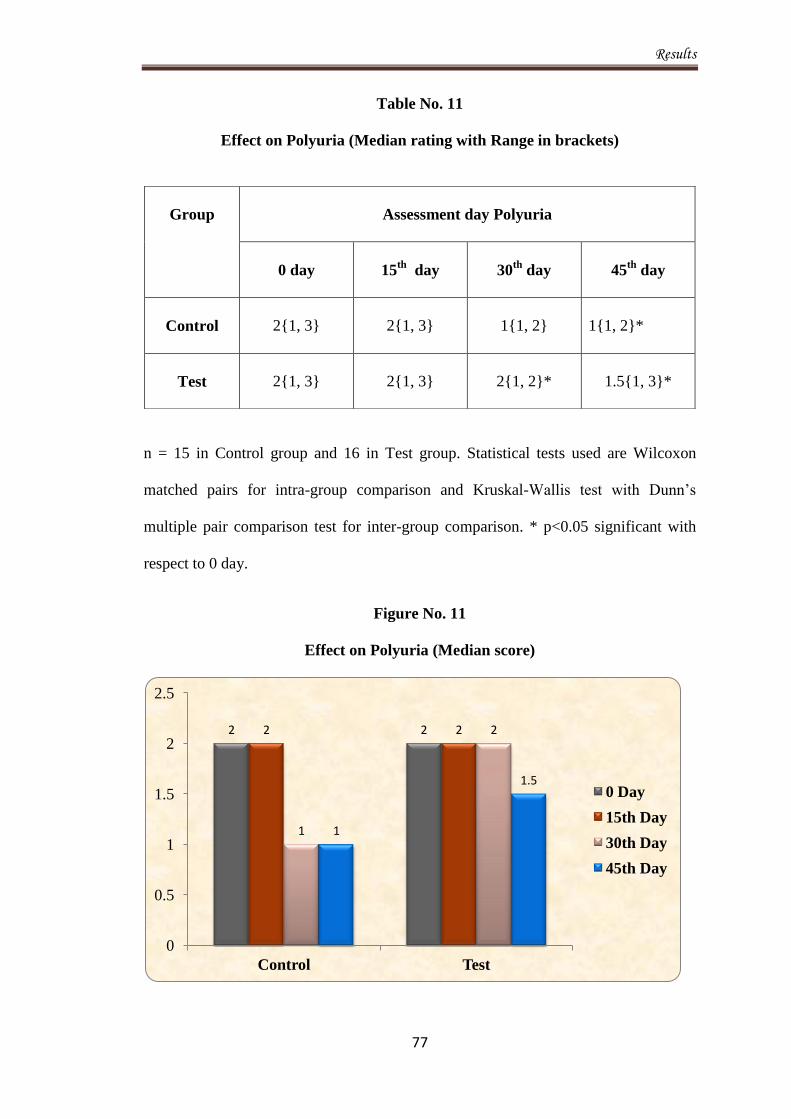
Results
77
Table No. 11
Effect on Polyuria (Median rating with Range in brackets)
n = 15 in Control group and 16 in Test group. Statistical tests used are Wilcoxon
matched pairs for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison. * p<0.05 significant with
respect to 0 day.
Figure No. 11
Effect on Polyuria (Median score)
2 2 2 2
1
2
1
1.5
0
0.5
1
1.5
2
2.5
Control Test
0 Day
15th Day
30th Day
45th Day
Group
Assessment day Polyuria
0 day
15th
day 30th
day 45th
day
Control
2{1, 3}
2{1, 3}
1{1, 2}
1{1, 2}*
Test
2{1, 3}
2{1, 3}
2{1, 2}*
1.5{1, 3}*

Results
78
Table No. 12
Effect on Polydipsia (Median rating with Range in brackets)
Group
Assessment day Polydipsia
0 day
15th
day 30th
day 45th
day
Control
2{1, 3}
2{1, 3}
1{1, 2}*
1{1, 2}*
Test
2{1, 3}
1{1, 2}
1{1, 3}*
1{1, 3}**
n = 15 in Control group and 16 in Test group. Statistical tests used are Friedman test
with post test for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison. * p<0.05 significant with
respect to 0 day. ** p<0.001 extremely significant with respect to 0 day.
Figure No. 12
Effect on Polydipsia (Median score)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
Control Test
2 2 2
1 1 1 1 1
0 Day
15th Day
30th Day
45th Day
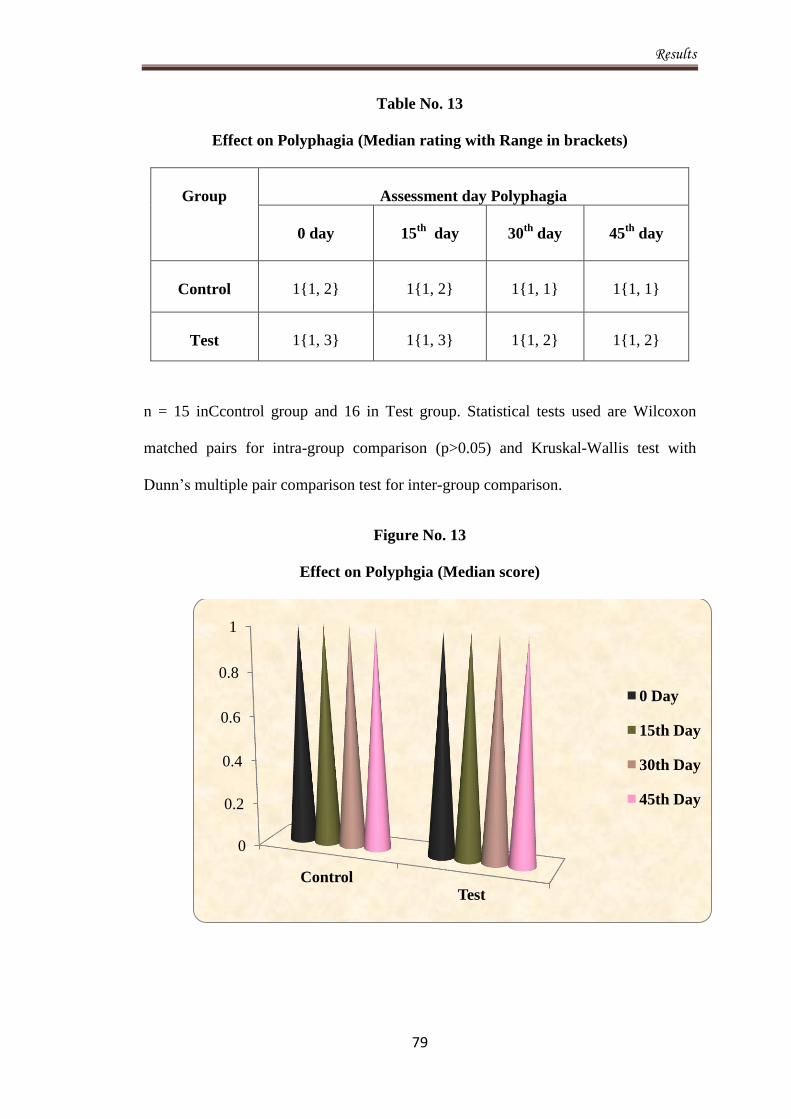
Results
79
Table No. 13
Effect on Polyphagia (Median rating with Range in brackets)
Group
Assessment day Polyphagia
0 day
15th
day 30th
day 45th
day
Control
1{1, 2}
1{1, 2}
1{1, 1}
1{1, 1}
Test
1{1, 3}
1{1, 3}
1{1, 2}
1{1, 2}
n = 15 inCcontrol group and 16 in Test group. Statistical tests used are Wilcoxon
matched pairs for intra-group comparison (p>0.05) and Kruskal-Wallis test with
Dunn’s multiple pair comparison test for inter-group comparison.
Figure No. 13
Effect on Polyphgia (Median score)
0
0.2
0.4
0.6
0.8
1
Control Test
0 Day
15th Day
30th Day
45th Day

Results
80
Table No. 14
Effect on Tiredness (Median rating with Range in brackets)
Group
Assessment day Tiredness
0 day
15th
day 30th
day 45th
day
Control
2{1, 3}
2{1, 3}
2{1, 3}*
1{1, 2}**
Test
2{2, 3}
2{2, 3}
2{1, 3}*
1{1, 3}***
n = 15 in Control group and 16 in Test group. Statistical tests used are Wilcoxon
matched pairs for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison. *p<0.05 with respect to day
0, **p<0.01 with respect to 0 day, ***p<0.001 with respect to 0 day.
Figure No. 14
Effect on Tiredness (Median score)
2 2 2 2 2 2
1 1
0
0.5
1
1.5
2
2.5
Control Test
0 Day
15th Day
30th Day
45th Day
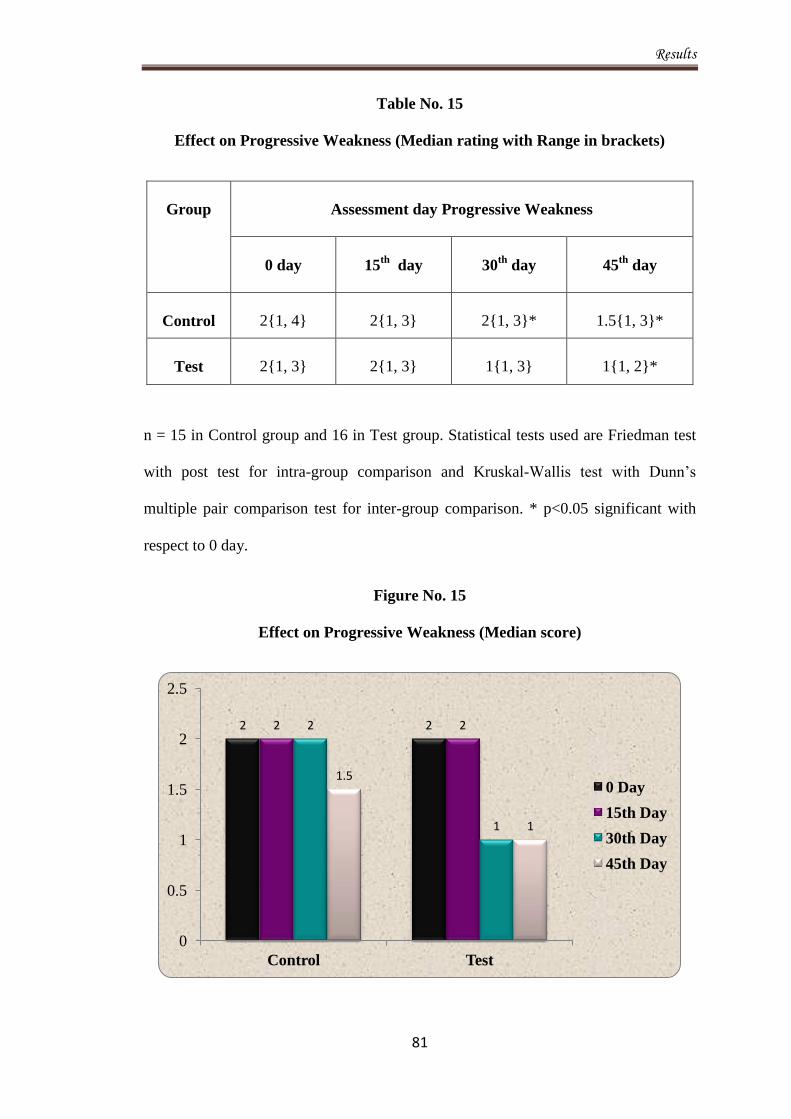
Results
81
Table No. 15
Effect on Progressive Weakness (Median rating with Range in brackets)
Group
Assessment day Progressive Weakness
0 day
15th
day 30th
day 45th
day
Control
2{1, 4}
2{1, 3}
2{1, 3}*
1.5{1, 3}*
Test
2{1, 3}
2{1, 3}
1{1, 3}
1{1, 2}*
n = 15 in Control group and 16 in Test group. Statistical tests used are Friedman test
with post test for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison. * p<0.05 significant with
respect to 0 day.
Figure No. 15
Effect on Progressive Weakness (Median score)
2 2 2 2 2
1
1.5
1
0
0.5
1
1.5
2
2.5
Control Test
0 Day
15th Day
30th Day
45th Day
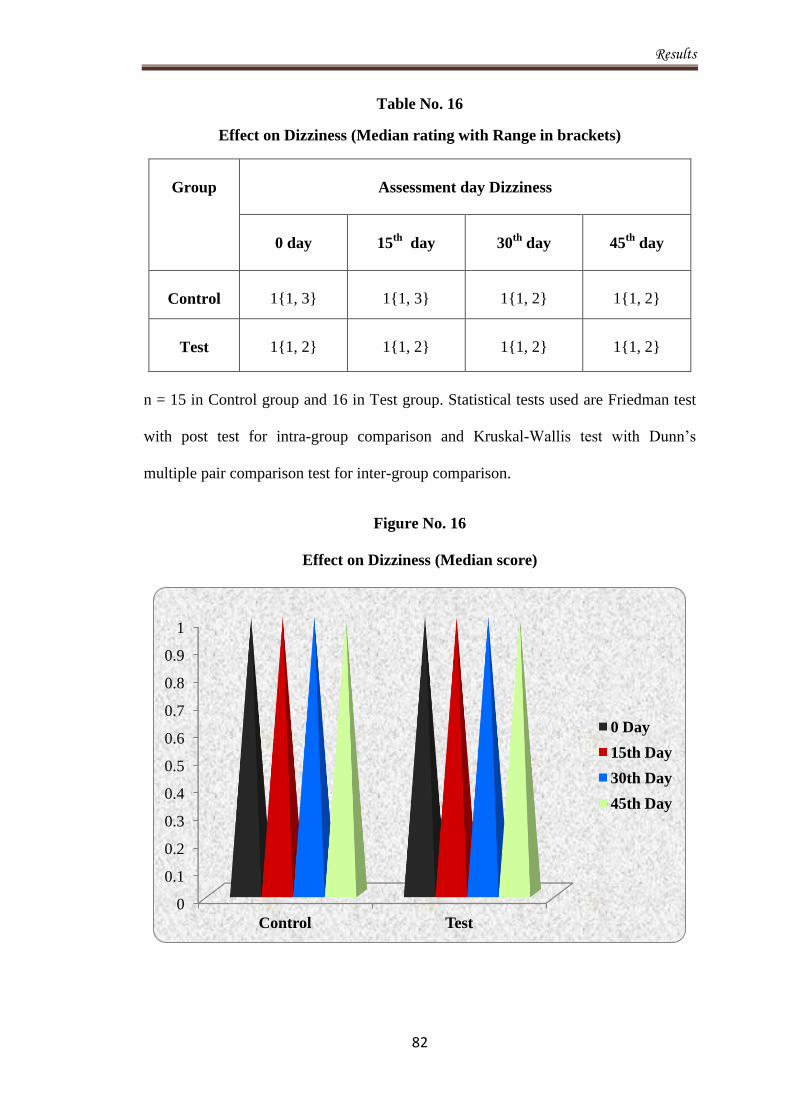
Results
82
Table No. 16
Effect on Dizziness (Median rating with Range in brackets)
n = 15 in Control group and 16 in Test group. Statistical tests used are Friedman test
with post test for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison.
Figure No. 16
Effect on Dizziness (Median score)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Control Test
0 Day
15th Day
30th Day
45th Day
Group
Assessment day Dizziness
0 day
15th
day 30th
day 45th
day
Control
1{1, 3}
1{1, 3}
1{1, 2}
1{1, 2}
Test
1{1, 2}
1{1, 2}
1{1, 2}
1{1, 2}
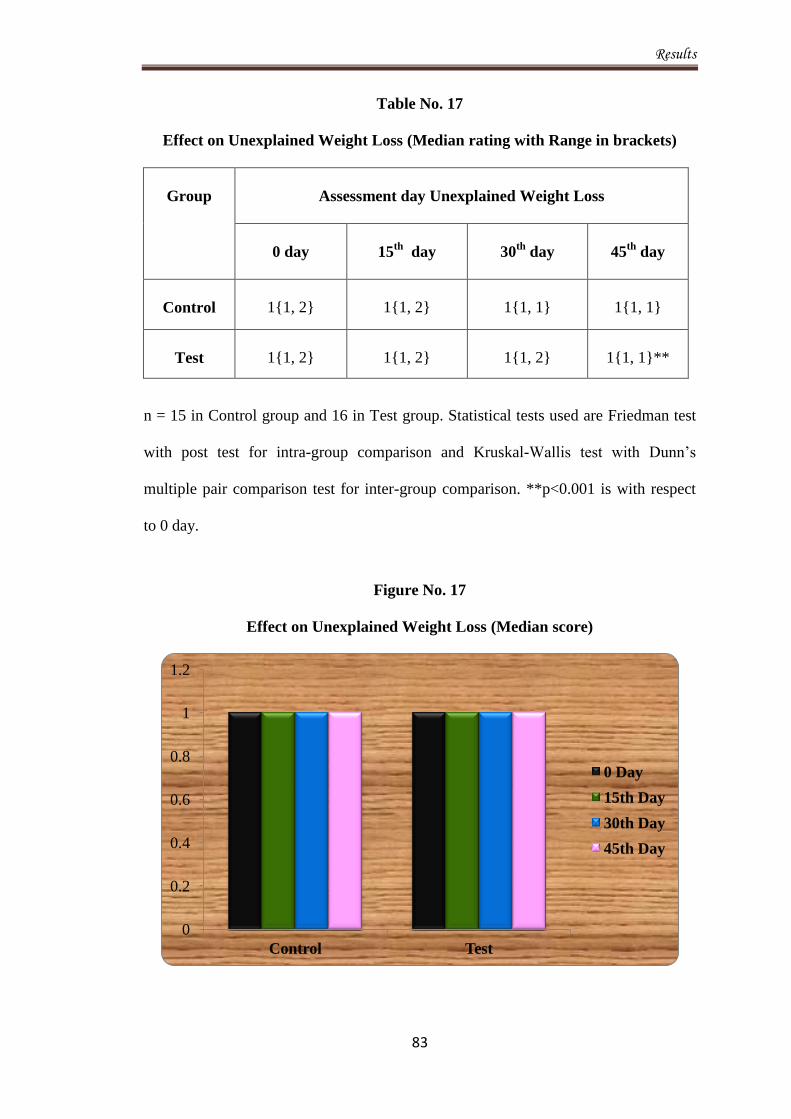
Results
83
Table No. 17
Effect on Unexplained Weight Loss (Median rating with Range in brackets)
Group
Assessment day Unexplained Weight Loss
0 day
15th
day 30th
day 45th
day
Control
1{1, 2}
1{1, 2}
1{1, 1}
1{1, 1}
Test
1{1, 2}
1{1, 2}
1{1, 2}
1{1, 1}**
n = 15 in Control group and 16 in Test group. Statistical tests used are Friedman test
with post test for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison. **p<0.001 is with respect
to 0 day.
Figure No. 17
Effect on Unexplained Weight Loss (Median score)
0
0.2
0.4
0.6
0.8
1
1.2
Control Test
0 Day
15th Day
30th Day
45th Day

Results
84
Table No. 18
Effect on Pruritus (Median rating with Range in brackets)
Group
Assessment day Pruritus
0 day
15th
day 30th
day 45th
day
Control
1{1, 2}
1{1, 2}
1{1, 1}
1{1, 1}
Test
1{1, 3}
1{1, 2}
1{1, 2}
1{1, 2}
n = 15 in Control group and 16 in Test group. Statistical tests used are Friedman test
with post test for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison.
Figure No. 18
Effect on Pruritus (Median score)
0
0.2
0.4
0.6
0.8
1
1.2
Control Test
0 Day
15th Day
30th Day
45th Day
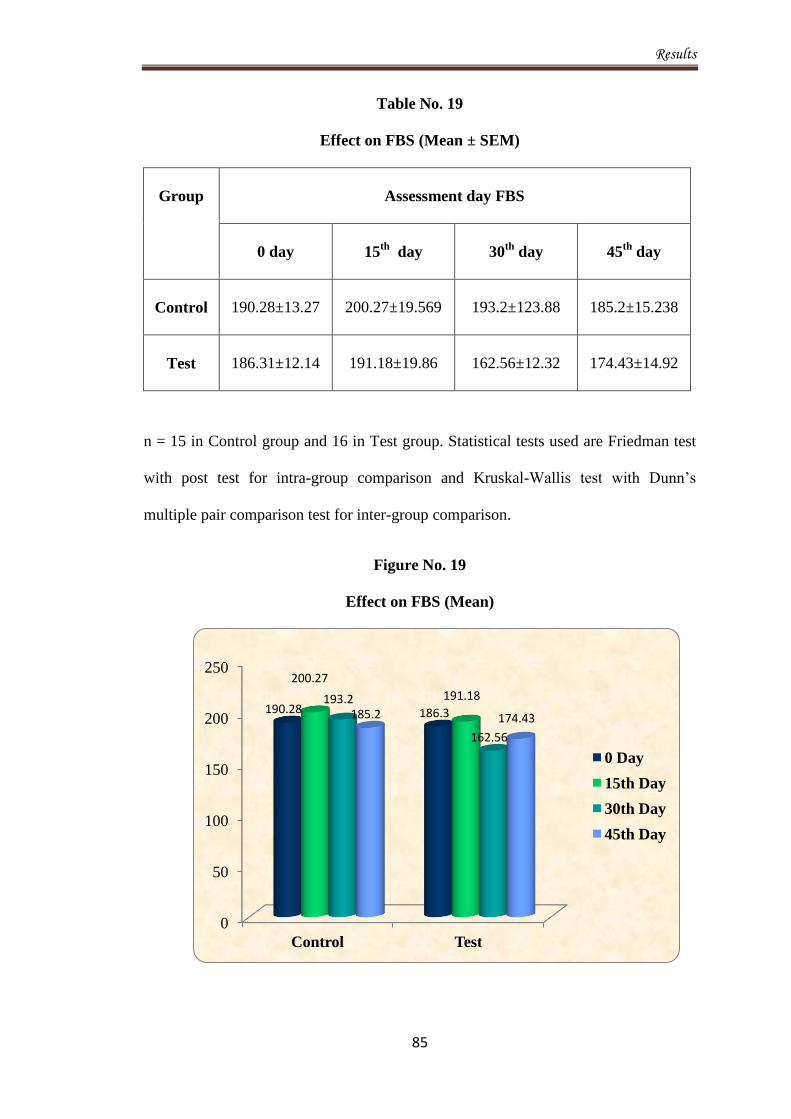
Results
85
Table No. 19
Effect on FBS (Mean ± SEM)
Group
Assessment day FBS
0 day
15th
day 30th
day 45th
day
Control
190.28±13.27
200.27±19.569
193.2±123.88
185.2±15.238
Test
186.31±12.14
191.18±19.86
162.56±12.32
174.43±14.92
n = 15 in Control group and 16 in Test group. Statistical tests used are Friedman test
with post test for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison.
Figure No. 19
Effect on FBS (Mean)
0
50
100
150
200
250
Control Test
190.28 186.3
200.27
191.18 193.2
162.56
185.2 174.43
0 Day
15th Day
30th Day
45th Day
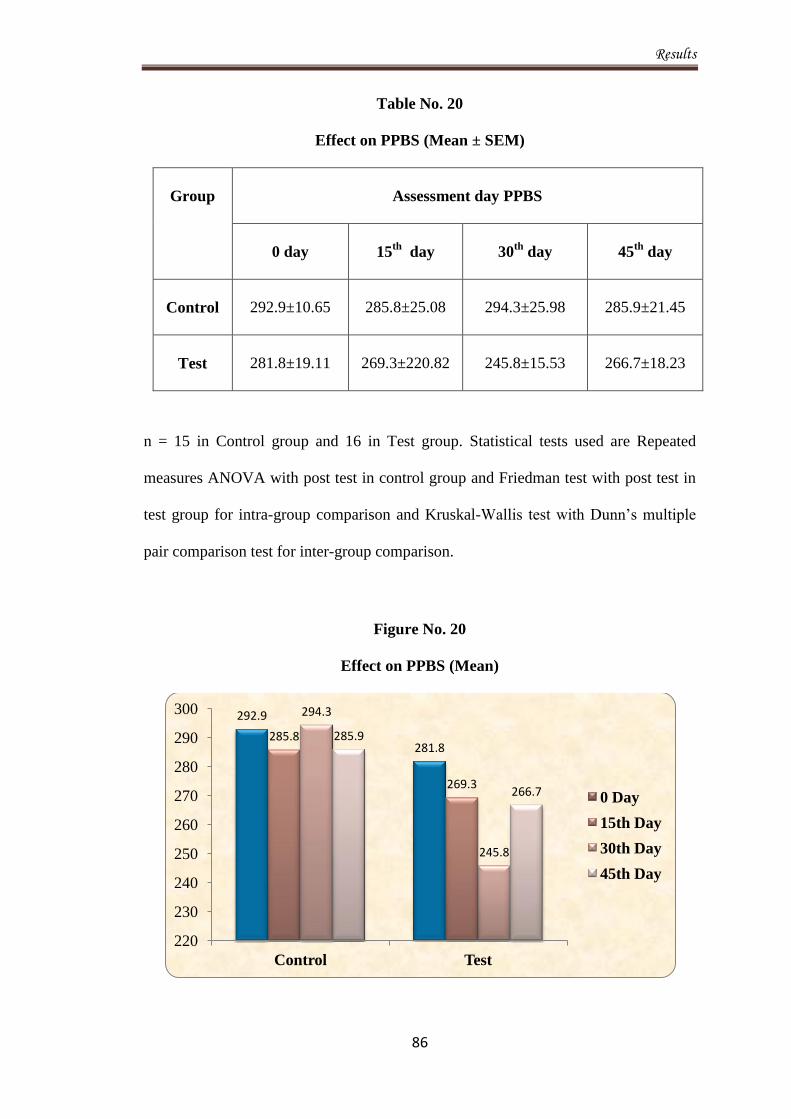
Results
86
Table No. 20
Effect on PPBS (Mean ± SEM)
Group
Assessment day PPBS
0 day
15th
day 30th
day 45th
day
Control
292.9±10.65
285.8±25.08
294.3±25.98
285.9±21.45
Test
281.8±19.11
269.3±220.82
245.8±15.53
266.7±18.23
n = 15 in Control group and 16 in Test group. Statistical tests used are Repeated
measures ANOVA with post test in control group and Friedman test with post test in
test group for intra-group comparison and Kruskal-Wallis test with Dunn’s multiple
pair comparison test for inter-group comparison.
Figure No. 20
Effect on PPBS (Mean)
292.9
281.8 285.8
269.3
294.3
245.8
285.9
266.7
220
230
240
250
260
270
280
290
300
Control Test
0 Day
15th Day
30th Day
45th Day

Results
87
Table No. 21
Effect on Urine Sugar (Mean ± SEM)
Group
Assessment day Urine Sugar
0 day
15th
day 30th
day 45th
day
Control
1.033±0.226
0.766±0.233
0.733±0.223
0.333±0.159*
Test
0.687±0.187
0.575±0.196
0.406±0.1894
0.218±0.101**
n = 15 in Control group and 16 in Test group. Statistical tests used are Wilcoxon
matched pair test for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple pair comparison test for inter-group comparison. * p<0.05 significant with
respect to 0 day. **p<0.001 highly significant with respect to 0 day.
Figure No. 21
Effect on Urine Sugar (Mean)
0
0.2
0.4
0.6
0.8
1
1.2
Control Test
1.033
0.687 0.766
0.575
0.733
0.406 0.333
0.218
0 Day
15th Day
30th Day
45th Day
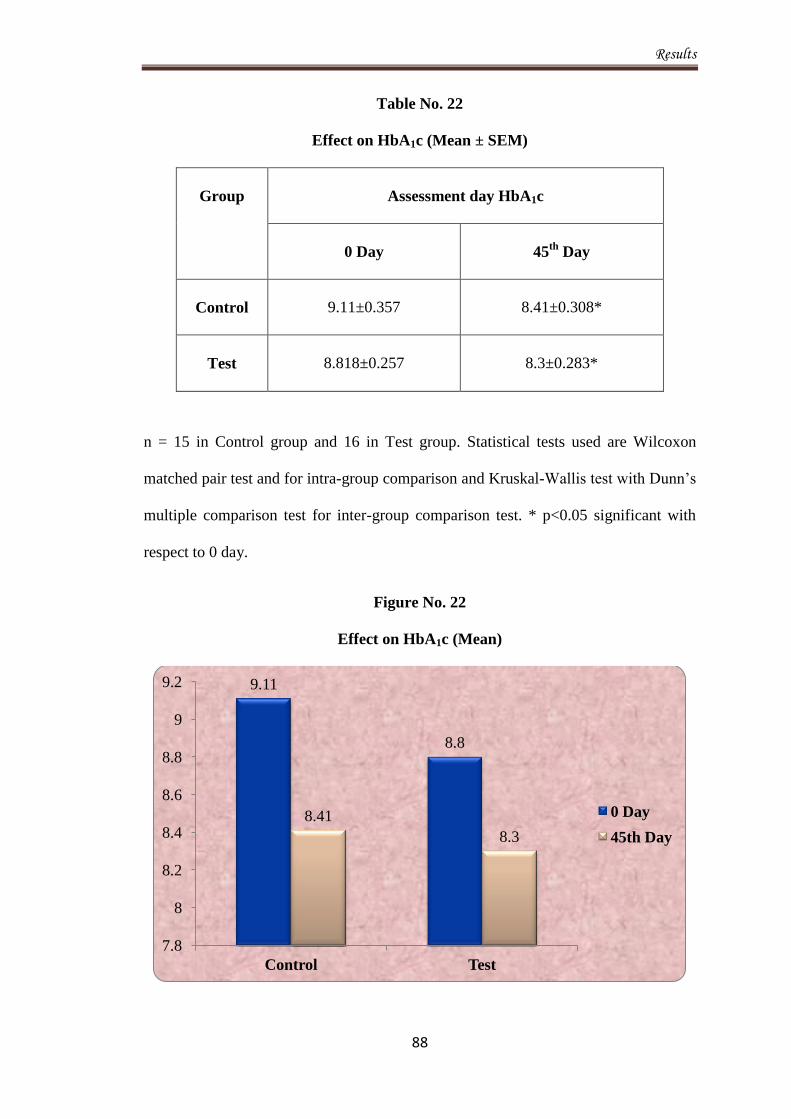
Results
88
Table No. 22
Effect on HbA1c (Mean ± SEM)
Group
Assessment day HbA1c
0 Day
45th
Day
Control
9.11±0.357
8.41±0.308*
Test
8.818±0.257
8.3±0.283*
n = 15 in Control group and 16 in Test group. Statistical tests used are Wilcoxon
matched pair test and for intra-group comparison and Kruskal-Wallis test with Dunn’s
multiple comparison test for inter-group comparison test. * p<0.05 significant with
respect to 0 day.
Figure No. 22
Effect on HbA1c (Mean)
9.11
8.8
8.41
8.3
7.8
8
8.2
8.4
8.6
8.8
9
9.2
Control Test
0 Day
45th Day
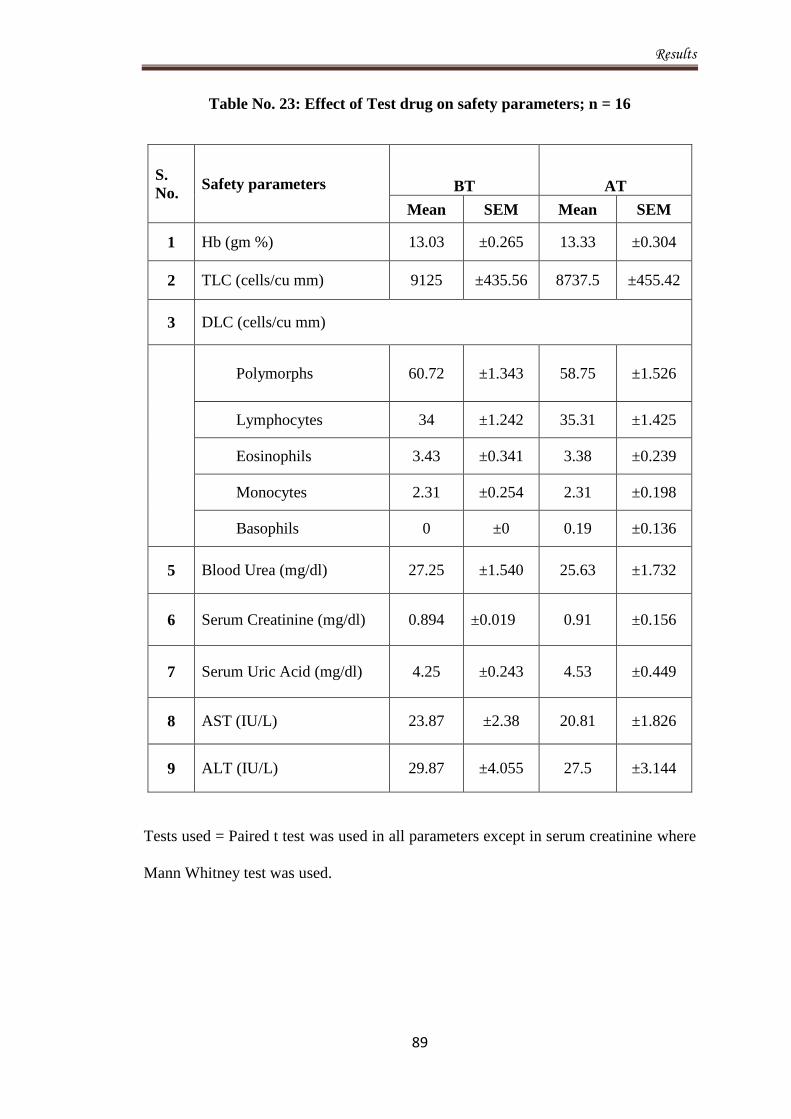
Results
89
Table No. 23: Effect of Test drug on safety parameters; n = 16
S.
No. Safety parameters BT AT
Mean SEM Mean SEM
1 Hb (gm %) 13.03 ±0.265 13.33 ±0.304
2 TLC (cells/cu mm) 9125 ±435.56 8737.5 ±455.42
3 DLC (cells/cu mm)
Polymorphs 60.72 ±1.343 58.75 ±1.526
Lymphocytes 34 ±1.242 35.31 ±1.425
Eosinophils 3.43 ±0.341 3.38 ±0.239
Monocytes 2.31 ±0.254 2.31 ±0.198
Basophils 0 ±0 0.19 ±0.136
5 Blood Urea (mg/dl) 27.25 ±1.540 25.63 ±1.732
6 Serum Creatinine (mg/dl) 0.894 ±0.019 0.91 ±0.156
7 Serum Uric Acid (mg/dl) 4.25 ±0.243 4.53 ±0.449
8 AST (IU/L) 23.87 ±2.38 20.81 ±1.826
9 ALT (IU/L) 29.87 ±4.055 27.5 ±3.144
Tests used = Paired t test was used in all parameters except in serum creatinine where
Mann Whitney test was used.
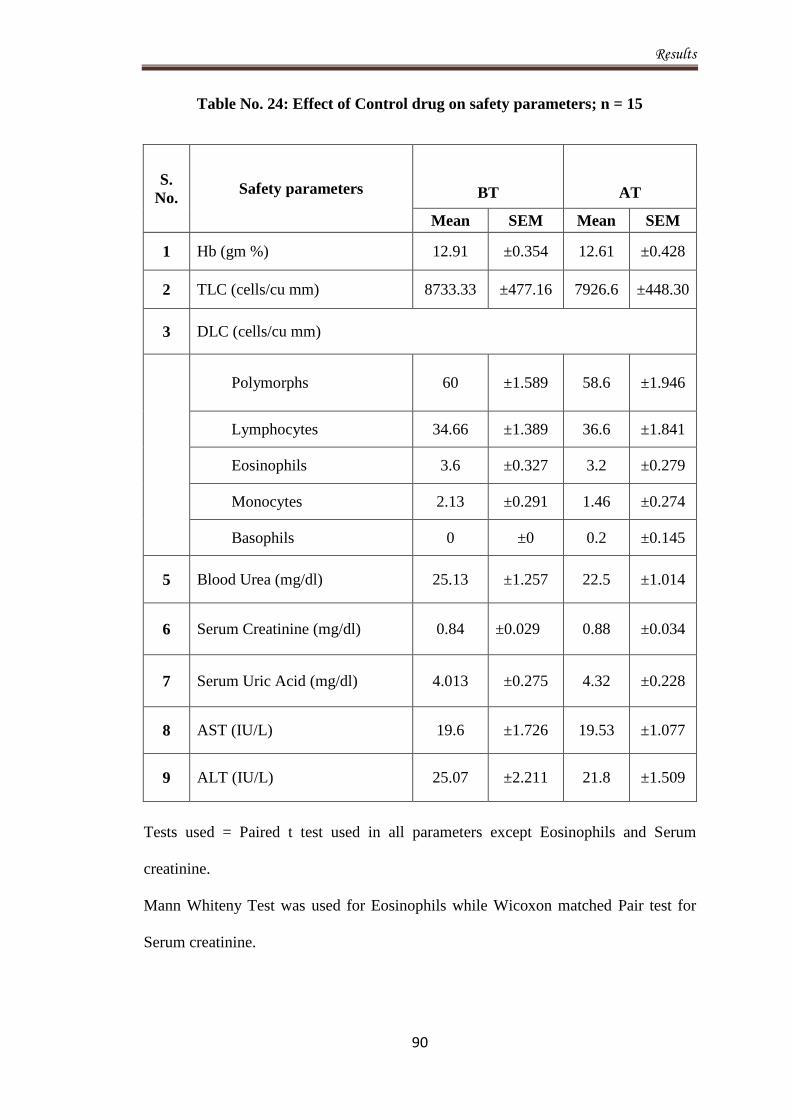
Results
90
Table No. 24: Effect of Control drug on safety parameters; n = 15
S.
No. Safety parameters BT AT
Mean SEM Mean SEM
1 Hb (gm %) 12.91 ±0.354 12.61 ±0.428
2 TLC (cells/cu mm) 8733.33 ±477.16 7926.6 ±448.30
3 DLC (cells/cu mm)
Polymorphs 60 ±1.589 58.6 ±1.946
Lymphocytes 34.66 ±1.389 36.6 ±1.841
Eosinophils 3.6 ±0.327 3.2 ±0.279
Monocytes 2.13 ±0.291 1.46 ±0.274
Basophils 0 ±0 0.2 ±0.145
5 Blood Urea (mg/dl) 25.13 ±1.257 22.5 ±1.014
6 Serum Creatinine (mg/dl) 0.84 ±0.029 0.88 ±0.034
7 Serum Uric Acid (mg/dl) 4.013 ±0.275 4.32 ±0.228
8 AST (IU/L) 19.6 ±1.726 19.53 ±1.077
9 ALT (IU/L) 25.07 ±2.211 21.8 ±1.509
Tests used = Paired t test used in all parameters except Eosinophils and Serum
creatinine.
Mann Whiteny Test was used for Eosinophils while Wicoxon matched Pair test for
Serum creatinine.
Discussion
91
Discussion
Ziabetus Shakari (Diabetes mellitus Type II) is a rising pandemic and has become
threat to the World population. It is one of the major causes of morbidity and
mortality. It has serious economical effects on society. In the United States, diabetes
is the leading cause of blindness among working age adults, nontraumatic loss of
limb, and it is also the fifth-leading cause of death. Once considered a disease of
wealthy nations, type II diabetes now constitutes a truly global affliction. The
International Diabetes Federation (IDF) anticipates that the worldwide incidence of
diabetes among those aged 20 to 79 years will increase by around 70% in the next 20
years. Billions of people are suffering from type II diabetes throughout the world.
Hence obviously it is a subject of interest to scientists and health care providers. Type
II diabetes is recognized as a failure in the regulation mechanism to maintain plasma
glucose in an appropriate concentration level in response to endogenous glucose
production or diet input. Type II diabetes patients typically exhibit symptoms of
insulin resistance and impaired insulin secretion. Initially the body is able to adapt to
maintain glucose concentration with high levels.
The present study was a randomized single blind standard controlled trial,
accomplished to evaluate the safety and efficacy of a Unani formulation in the
management of Ziabetus Shakari (Diabetes mellitus type 2) on scientific basis and
modern parameters. The study was conducted at National Institute of Unani Medicine
Hospital, Bangalore for a period of 18 months from September 2010 to February
2012. A total of 50 patients were registered for the study. A total 40 patients were
randomly assigned into Test (Group A) and Control (Group B) groups respectively,
but 4 patients from Test group and 5 patients from Control group were lost to follow-
up, leaving behind 16 patients in Test and 15 patients in Control group who finally
Discussion
92
completed the course of treatment. Statistical analysis was done only for those
patients who completed the course of treatment.
Patients of Group A were given an Unani formulation consisting of Satte Gilo
(Tinospora cardifolia) Tabasheer (Bambusa bambos) and Maghze Kanwal Gatta
(Nelumbo nucifera) for oral administration 2 tablet twice a day while patients of
Group B were treated with the standard drug, Diabecon 2 tablet twice a day for a
period of 45 days. The severity of 8 different signs and symptoms (polyuria,
polydipsia, polyphagia, tiredness, progressive weakness, dizziness, unexplained
weight loss, pruritus) was rated on a 4 point scale (1, absent; 2, mild; 3, moderate; 4,
severe). The scores were reckoned for each patient at each assessment point on 0, 15th
,
30th
and 45th
day. At every visit, patients were asked about the progression or
regression in their symptoms, and subjected to assess the clinical findings; and were
investigated for FBS, PPBS and urine for sugar.
The observations and results concerning demography and assessment parameters
obtained from the trial have been illustrated in tables and figures. They are discussed
in the following paragraphs consecutively to draw presumption and to turn up at a
conclusion.
According to the age maximum number of patients, 16 (52.63%) were observed in
age group of 35-45 years, while 7 (22.58%) patients in 46-55 years, and 8 (25.81%)
patients in 56-65 years of age group. This data suggested that the disease is more
prevalent in the age group of 35-45 (Table No. 1).
In this study, the highest incidence of 20 (64.5%) was observed in male patients while
11 (35.5%) in female patients (Table No. 2). This study suggested a male
preponderance among the patients of Ziabetus Shakari. This finding is in conformity
with the study showed prevalence of diabetes among men and women in China that
Discussion
93
prediabetes were 9.7% (10.6% among men and 8.8% among women) and 15.5%
(16.1% among men and 14.9% among women), respectively, accounting for 92.4
million adults with diabetes (50.2 million men and 42.2 million women) and 148.2
million adults with prediabetes (76.1 million men and 72.1 million women).133
Out of total patients, 22 (71%) patients were Muslim followed by 9 (29%) Hindu
patients (Table No. 3). No compelling data is available that demonstrates the
distribution of disease among different religious communities in the society. This
study however reflects a predominance of Muslims among the patients of Diabetes
mellitus. However the predominance of Muslim patients (71%) in present study may
be absolutely due to the fact that majority of patients attending NIUM hospital are
from Muslim community which is reflected in my study. There is no persuasive data
is available to demonstrate the existence of this disease among different religious
communities in the society or is likely reason may be that there is no any relation of
this existence.
As far as the Marital Status of diabetes mellitus patients is concerned, all 31 (100%)
patients were married (Table No. 4). As this disease usually occurs in the 4th
and 5th
decade, therefore all the patients were married.
Out of 40 patients, 14 (45.16%) were having the disease since <1 year, 7 (22.58%)
since 1-2 years, 9 (29.03%) since 3-4 years and 1(3.23%) since 6-10. (Table No. 10)
As far as the family history of diabetes is concerned, 48.4% patients had positive
family history (Table 5). This finding is in conformity with the finding described by
Jali MV, Kamber S.135
This study indicates that there is a strong association between
heredity and diabetes mellitus. Further stronger the family history greater is the
tendency of getting diabetes. Similarly, positive family history is use as a risk factor
and screening tool shown in study of Vadez R.136
Discussion
94
As it is evident from Table No. 6 that the highest incidence of 11 (35.48%) was in
lower middle and upper lower class each (III, IV), followed by 6(19.35%) in upper
middle class (II), 2 (6.45%) in lower class (V), and 0 (0%) in upper class (I)
respectively. The present study demonstrates that diabetes mellitus is more prevalent
among the middle socioeconomic class. This finding is not in accordance with the
findings suggested by Connolly V. et al134
who proved in their epidemiological study
by the finding, suggests that exposure to factors that are implicated in the causation of
diabetes is more common in deprived areas (high SES) in comparison to low SES.
This may be due to the small sample size of study and the subject only confined to the
patients attending our hospital those are mostly belonging to middle and lower class
socioeconomic status.
Out of the total of 31 patients, 3 (9.68%) patients were vegetarian while 28 (90.32%)
patients had mixed dietary habits (Table No. 7). The maximum numbers of patients
had mixed dietary habits. The present study demonstrates that diabetes mellitus is
more common in people consuming mixed diets. As the person consuming mixed diet
are prone to develop obesity and obesity is one of the important risk factor for
development of the diabetes.
The study demonstrated relation between Mizaj of the patients and the disease. It is
determined as per the proforma enclosed with the case record form especially
designed for the study in the light of parameters mentioned in classical Unani
literature. A maximum of 22 (71%) patients were found having Balghami mizaj
followed by 7 (22.58%) patients having Damvi, 2 (6.42%) patients having the Safravi
and 0 (0%) patients having the Saudavi mizaj (Table No. 8). It indicates that the
disease is more prevalent in Balghami mizaj patients.
Discussion
95
The median scores of polyuria in both groups were compared statistically using
Friedman test for intra group comparison and Kruskall Wallis test with post Dunn’s
Multiple comparison test for intergroup comparison, it was found that the difference
between the median scores of Test group at 15th
day and at baseline was not
significant (p>0.05) while significant (p<0.05) at 30th
day and 45th
day. While in the
case of Control group, the difference of median scores was not significant (p>0.05) at
15th
day and 30th
day while significant (p<0.05) on 45th
day when compared with
respect to baseline score. Results are summarised in table No 11.
The response of the test drug on polyuria may be due to the Qabiz (astringent)
property of Tabasheer23,83,92,124
and Satte Gilo65,69,76,90
with overall effect of anti-
diabetic effect of test drug which is discussed below.
The median score of the polydipsia in Test group was 2 (1, 3) on baseline, 1 (1, 3) on
15th
day, 1 (1, 3) on 30th
day and 1 (1, 3) on 45th
day; whereas in Control group, the
median score was 2 (1, 3) on 0 day , 2 (1, 3) on 15th
day, 1 (1, 2) on 30th
day and 1 (1,
2) on 45th
day. When the median scores of polydipsia in both groups, Test and
Control, were compared statistically by using Friedman test for intragroup
comparisons and Kruskal-Wallis test with post Dunn’s multiple comparisons test for
intergroup comparison. It was found that the difference between the median scores of
Test group and Control group at 30th
day and 45th
day compared with baseline was
significant (p<0.05). Results are summarised in table No 12.The effect may be due to
Musakkine Atash property of Tabasheer23,83,84,88,90,120,125
and Kanwal Gatta67,83,8485,88
described by Ibne Sina, Ibne Hubl, Najmul Ghani, Kabeeruddin and Kritikar Basu.
In the assesment of polyphagia, median score in group A (Test group) was 1(1, 3) on
0 day, 1(1, 3) on 15th
day, 1(1, 2) on 30th
day and 1 (1, 2) on 45th
day; whereas in
group B (Cotrol group) the median score was 1 (1, 2) on 0 day ,1 (1, 2) on 15th
day, 1
Discussion
96
(1, 1) on 30th
day and 1 (1, 1) on 45th
day. When the median scores of polyphagia in
both Groups, A and B were compared statistically by using Friedman test for
intragroup comparisons and Kruskal-Wallis test with post Dunn’s multiple
comparisons test for intergroup comparison. It was found that the difference between
the median scores of Test and Control group at any one of the assesment days
compared with baseline was not significant (p>0.05). Intergroup comparison was also
not significant at 45th
day (p>0.05) (Table No 13). Although the result was not
statistically significant in polyphagia due to very less patient have had the symptom,
even though who had it, were in mild degree; the test and control drug showed some
effect on polyphagia clinically which may be due to over all improvement.
The median score of tiredness in group A (Test group) was 2 (2, 3) on 0 day, 2 (2, 3)
on 15th
day, 2 (1, 3) on 30th
day and 2 (1, 3) on 45th
day; whereas in group B (Control
group) median was 2 (1, 3) on 0 day, 2 (1, 3) on 15th
day, 2 (1, 3) on 30th
day and 2 (1,
3) on 45th
day. When the median scores of tiredness in both Groups, A and B, were
compared statistically by using Friedman test for intragroup comparisons and
Kruskal-Wallis test with post Dunn’s multiple comparisons test for intergroup
comparison. The result was significant on 30th
day of assesment with comparision to
the base line in Control group and Test group, and at 45th
day result found very
significant (p<0.01) with comparision to base line in Control group and hightly
significant (p<0.001) in Test group. Results are summarised in table No 14. This effct
may be due to Muqawwi Aam (general tonic) property of Gilo65,67,68,69,70,75,78,83,89,90,91
and Kanwal Gatta,66
described by Kabiruddin, Nadkarni, James A. Duke, Kritikar and
Basu, Battacharjee SK.
The median score of progressive weakness was calculated on 0 day, 15th
day 30th
day
and 45th
day as 2 (1, 3) , 2 (1, 3), 2 (1, 3) and 1 (1, 2) in Test group respectively, while
Discussion
97
the same was observed as 2 (1, 4), 2 (1, 3) , 2 (1, 3) and 1.5 (1, 3) on 0 day, 15th
day,
30th
day and 45th
day respectively in Control group. When the two groups were
compared statistically by using Friedman test for intragroup comparisons and
Kruskal-Wallis test with post Dunn’s multiple comparisons tests for intergroup
comparison. It was found that the difference between the median scores of Control
group at 30th
day and 45th
day with baseline was significant (p<0.05), while in Test
group on 45th
day compared with baseline was significant (p<0.05). Intergroup
comparison was also not significant at 45th
day (p>0.05). Results are summarised in
table No 15. The results indicate that both the test and control drugs are effective in
reducing progressive weakness. The improvement in progressive weakness may be
due to the Muqawwi Aam (general tonic) property of Gilo65,67,68,69,70,75,78,83,89,90,91
and
Kanwal Gatta66
described by Kabiruddin, Nadkarni, James A. Duke, Kritikar and
Basu and Battacharjee SK.
The median score of Dizziness was calculated on 0 day, 15th
day 30th
day and 45th
day
as 1 (1, 2) , 1 (1, 2), 1 (1, 2) and 1 (1, 2) in Test group respectively, while the same
was observed as 1 (1, 3), 1 (1, 3) , 1 (1, 2) and 1 (1, 2) on 0 day, 15th
day, 30th
day
and 45th
day respectively in Control group. When the two groups were compared
statistically by using Friedman test for intragroup comparisons and Kruskal-Wallis
test with post Dunn’s multiple comparisons tests for intergroup comparison. It was
found that the difference between the median scores of Test group and Control group
at 45th
day compared with baseline was not significant (p>0.05). Intergroup
comparison was also not significant at 45th
day (p>0.05). Results are summarised in
table No 16. Although the result was not statistically significant in Dizziness due to
very less patient have had the symptom, even though who had it, were in mild degree;
the test and control drug showed some effect on Dizziness clinically which may be
Discussion
98
due to over all improvement in patients of diabetes.
In the assesment of unexplained weight loss, median score in group A (Test group)
was 1(1, 2) on 0 day, 1(1, 2) on 15th
day, 1(1, 2) on 30th
day and 1 (1, 1) on 45th
day;
whereas in group B (Cotrol group) the median score was 1 (1, 2) on 0 day ,1 (1, 2) on
15th
day, 1 (1, 1) on 30th
day and 1 (1, 1) on 45th
day. When the median in both group
were compared statistically by using Friedman test for intragroup comparisons and
Kruskal-Wallis test with post Dunn’s multiple comparisons test for intergroup
comparison. It was found that the difference between the median scores of Test and
Control group at 45th
day compared with baseline was not significant (p>0.05) in
Control group while in Test group was significant (p<0.01) at 45th
day. Intergroup
comparison was also not significant at 45th
day (p>0.05) (Table No 17).
The median score of pruritus was calculated on 0 day, 15th
day 30th
day and 45th
day
as 1 (1, 3), 1 (1,2), 1 (1, 2) and 1 (1, 2) in Test group respectively, while the same was
observed as 1 (1, 2), 1 (1, 2) , 1 (1, 1) and 1 (1, 1) on 0 day, 15th
day, 30th
day and 45th
day respectively in Control group. When the two groups were compared statistically
by using Friedman test for intragroup comparisons and Kruskal-Wallis test with post
Dunn’s multiple comparisons tests for intergroup comparison. It was found that the
difference between the median scores of priritus in Test group at 45th
day compared
with baseline was not significant (p>0.05). Intergroup comparison was also not
significant at 45th
day (p>0.05). Although the result was not statistically significant in
pruritus due to very less patient have had this symptom but clinicaly both groups (Test
and Control) are showed adequate improvement (Table No 18).
The Mean ± SEM score for FBS in Test group was on 0 day, 15th
day 30th
day and
45th
day as 186.31±12.14, 191.18±19.86, 162.56±12.32 and 174.43±14.92
respectively, while the same was observed as 190.28±13.27, 200.27±19.569,
Discussion
99
193.2±123.88 and 185.2±15.238 on 0 day, 15th
day, 30th
day and 45th
day respectively
in Control group. When Mean ± SEM score of FBS in both Groups, Test and Control,
were compared statistically by using Friedman test with post test for intra-group
comparison and Kruskal-Wallis test with Dunn’s multiple pair comparison test for
inter-group comparison it was found that the difference between the Mean ± SEM
score of Test and Control groups at 45th
day compared with baseline was not
significant (p>0.05). Although the result was not statistically significant in FBS, but
both the test drug and control drug managed the blood sugar level and reduced it upto
some extent and prevent further hyperglycemia, which can be perceived by the Mean
± SEM score of FBS on base line and 45th
day (Table No 19).
The Mean ± SEM score for PPBS in Test group was on 0 day, 15th
day 30th
day and
45th
day as 281.8±19.11, 269.3±220.82, 245.8±15.53 and 266.7±18.23 respectively,
while the same was observed as 292.9±10.65, 285.8±25.08, 294.3±25.98 and
285.9±21.45 on 0 day, 15th
day, 30th
day and 45th
day respectively in Control group.
When Mean ± SEM score of PPBS in both Groups, Test and Control, were compared
statistically by using Repeated measures ANOVA with post Test in Control group and
Friedman test with post test in Test group for intra-group comparison and Kruskal-
Wallis test with Dunn’s multiple pair comparison test for inter-group comparison, it
was found that the difference between the Mean ± SEM score of PPBS in Test group
and Control group both at 45th
day compared with baseline was not significant
(p>0.05). Although the result was not statistically significant in PPBS, but the test
drug and control drug both were manage the sugar level and reduce it upto some
extent and prevent further hyperglycemia, which can perceived by the Mean ± SEM
score of PPBS on base line and 45th
day summarised in table No 20.
Discussion
100
The Mean ± SEM score of urine sugar was calculated on 0 day, 15th
day 30th
day and
45th
day as 0.687±0.187, 0.575±0.196, 0.406±0.1894 and 0.218±0.101 in Test group
respectively, while the same was observed as 1.033±0.226, 0.766±0.233, 0.733±0.223
and 0.333±0.159 on 0 day, 15th
day, 30th
day and 45th
day respectively in Control
group. When the two groups were compared statistically by using Friedman test for
intragroup comparisons and Kruskal-Wallis test with post Dunn’s multiple
comparisons tests for intergroup comparison. It was found that the difference between
the median scores of Control group at 45th
day with baseline was significant
(p<0.05), while in Test group on 45th
day compared with baseline was very
significant (p<0.01). Intergroup comparison was also not significant at 45th
day
(p>0.05). The response of the test drug on urine sugar may be due to the qabiz
(astringent) property of the Tabasheer and Satte Gilo with overall effect of anti-
diabetic effect of test drug (Table No 21).
The Mean ± SEM score for HbA1c in Test group was 8.818±0.257 on baseline and
8.3±0.283 on 45th
day, whereas in Control group the Mean ± SEM score of HbA1c
was 9.11±0.357 on 0 day and 8.41±0.308 on 45th
day. When Mean ± SEM score of
HbA1c in both Groups, Test and Control, were compared statistically by using
Wilcoxon matched pair test for intra-group comparison and Kruskal-Wallis test with
Dunn’s multiple pair comparison test for inter-group comparison it was found that the
difference between the Mean ± SEM score of Test and Control groups at 45th
day
compared with baseline was significant (p<0.05) (Table No 22).
During the normal practice of diabetes, physician always observes that the patients of
well estabilish/developed diabetes, who are not taking any pharmacological treatment
and not following control diet and regulre exercise, always develope hyperglycemia
and its complication after few days or months. In this study we can see that the
Discussion
101
treatments which were given in Test group and Control group both managed the blood
sugar level and reduced it upto some extent and prevents further hyperglycemia. So
we conclude that the test drug have antidiabetic effect. It is supported by several
experimental studies, demonstrating the hypoglycemic activity of Gilo.96,97,98,99 Further
more Kanwal Gatta have antioxidative property studied by Wang L. et al. Diabetes
mellitus is characterized by oxidative stress, which in turn determines endothelial
dysfunction. It has been reported that anti-oxidative property of the drug potentially
protects the vasculature through improvements in plasma lipid levels and platelet
function.137
The management of Ziabetus depends upon the controlled diet and regular exercise
very much, along with pharmacological treatment. The response of the drug is also
dose dependent, while, in this study, fixed dose of the drug were given which was
chalked out earlier at the time of the protocol designing.
In the light of the above discussion it can be concluded that test drug is safe and
effective in relieving symptoms and controlling glycaemic index in the patient of
diabetes mellitus.
Safety and Tolerability:
The safety of both test drug and control drug was evaluated by some standard safety
parameter i.e. Haemogram, AST, ALT, Blood Urea, Serum Creatinine, and ECG
which done before and after the treatment and were analyzed statistically which
showed no significant difference in any of these parameters. No any obnoxious
adverse effect was observed during and after the study in either group. Both the test
formulation and standard drug are safe and fairly well accepted by the patients proved
by this study.
Conclusion
102
Conclusion
The present study was conducted at National Institute of Unani Medicine Hospital,
Bangalore for a period of 18 months from September 2010 to February 2012.
Diagnosed patients of Ziabetus Shakari, belonging to the age group of 35-65 years of
either sex were registered as per protocol and were randomly divided into Test and
Control groups by random allocation. Patients of Test Group were advised Unani
formulation, consisting of Gilo (Tinospora cardifolia), Tabasheer (Bambusa bambos)
and Maghze Kanwal Gatta (Nelumbo nucifera) orally twice a day while in Control
group, the standard drug Tab. Diabecon was administered twice a day. Duration of
treatment in both Test and Control groups was 45 days and follow up was done
fortnightly. All the patients were advised planed diet and regular brisk walk for 30-40
minutes. Patients were kept under strict observation and assessment of the efficacy of
treatment of test and control drug was carried out on the basis of subjective and
objective parameters.
As evident from observations and results, patients treated with Unani formulation and
Control drug both showed significant deference on some subjective parameters like
Polyuria, Polydipsia, Tiredness, Progressive weakness and Unexplained Weight loss;
while there was no effect on other subjective parameters such as Polyphagia,
Dizziness and Pruritus. The objective parameters were also assessed and analyzed in
both groups. There was no significant difference in both groups on parameters of FBS
PPBS but significant difference was observed on Urine Sugar in Test Group and
Control group, Test group showed slightly quicker results. There was also significant
difference on parameter HbA1c in both groups equally. The safety markers i.e.
Haemogram, AST, ALT, Blood Urea, Serum Creatinine and ECG remained within
normal limit during the study. On the basis of above results and observation it may be
Conclusion
103
concluded that the test drug is effective in reducing the symptoms of Ziabetus
Shakari, and control the Urine Sugar and reduce the HbA1c levels. Further, no
obnoxious side effect was observed in Test group during and after the study and
overall compliance to the treatment was good. On the basis of these results it can be
concluded that the Unani formulation is safe and can be used in the treatment of
Ziabetus Shakari. The management of Ziabetus is depends upon the controlled diet
and regular exercise very much, along with pharmacological treatment. The response
of the drug is also dose dependent, while in this study fixed dose of the drug were
given, which was chalked out earlier at the time of the protocol designing. However,
long term study with a bigger sample size is required to elucidate further
pharmacological actions of the test formulation.
Summary
104
Summary
Ziabetus Shakari (Diabetes mellitus) is a serious chronic metabolic disorder that has a
significant impact on the health, quality of life and life expectancy of patients, as well
as on the health care system. It is a multi-systemic illness associated with a variety of
short-term and long term complications. The short term complications include
hypoglycemia and hyperglycemia. The long-term complications of untreated or
ineffectively treated diabetes include retinopathy, nephropathy and peripheral
neuropathy. In addition, diabetic patients have an increased risk of cardiovascular
disease and stroke.
However, lifestyle management measures may be insufficient or patient compliance
difficult, rendering conventional drug therapies necessary in many patients. As an
alternative approach, Unani drugs with antihyperglycemic activities were increasingly
sought by diabetic patient and physicians. Unani drugs with antidiabetic activity have
been researched extensively in India. These drugs should have a similar degree of
efficacy without the troublesome side effects associated with these treatments.
Keeping all this in the mind, a protocol of single blind randomized controlled clinical
trial was conducted in the National Institute of Unani Medicine, Bangalore, to
evaluate the efficacy of a Unani formulation in the management of Ziabetus Shakari.
The formulation consisting of Satte Gilo (Tinospora cardifolia) Tabasheer (Bambusa
bambos) and Maghze Kanwal Gatta (Nelumbo nucifera) was selected. Before starting
the treatment, the protocol was put forth for the ethical clearance, which was
approved by the Institutional Ethical Committee. Cases were selected on the basis of
Laboratory diagnosis and as per inclusion and exclusion criteria in the research
protocol. The protocol therapy duration was 45 days. Total 40 patients were randomly
allocated into Test (Group A) and Control (Group B) groups respectively. But 4
Summary
105
patients from Test group and 5 patients from Control group were lost to follow-up,
leaving behind 16 patients in Test and 15 patients in Control group who completed the
course of treatment.
Summary of demographic data, effects of treatment on different subjective and
objective parameters are as follows:
Demographic data
Age: Out of total 31 patients, 16 (52.63%) patients were observed in age group of 35-
45 years, 7 (22.58%) patients in 46-55 years, and 8 (25.81%) patients in 56-65 years
of age group.
Sex: The incidence was observed as 20 (64.5%) in male patients while 11 (35.5%) in
female patients.
Marital status: All 31 (100%) patients were married.
Religion: The highest 22 (71%) patients were Muslim followed by 9 (29%) patients
were Hindu.
Dietary Habit: Out of total 31 patients, 3 (9.68%) patients were vegetarian while 28
(90.32%) patients recorded of having mixed diet.
Socio-Economic Status: The highest incidence of 22 (71%) was in lower middle and
upper lower class [11 (35.48%) in each class III and IV], followed by 6 (19.35%) in
upper middle class (II), 2 (6.45%) in lower class (V), and 0 (0%) in upper class (I)
respectively.
Family History of Diabetes Mellitus: Positive family history of diabetes mellitus
was in 48.4% patients and negative in 51.6% patients.
Mizaj: A maximum of 22 (71%) patients were found having Balghami mizaj followed
by 7 (22.58%) patients having Damvi, 2 (6.42%) patients having the Safravi and 0
(0%) patients having the Saudavi mizaj.

Summary
106
Effect of Test and Standard Drugs on Subjective Parameters:
Effect on Polyuria: The median scores of polyuria in both Test and Control were
compared, the difference between the median scores of Test group at 15th
day and at
baseline was not significant (p>0.05) while significant (p<0.05) at 30th
day and 45th
day. In Control group, the difference of median scores was not significant (p>0.05) at
15th
day and 30th
day while significant (p<0.05) on 45th
day when compared with
respect to baseline score.
Effect on Polydipsia: When the median scores of polydipsia in both groups, Test and
Control, were compared statistically at 30th
day and 45th
day with baseline was
significant (p<0.05).
Effect on Polyphagia: when the median scores of polyphgia of Test and Control
group were compared statistically on 15th
day, 30th
day and 45th
day with baseline,
were not significant (p>0.05). Intergroup comparison was also not significant at 45th
day (p>0.05).
Effect on Tiredness: The median score of tiredness in both Groups, A and B, were
compared. The result show significant on 30th
day of assesment with comparision to
the base line in Control group and Test group, and at 45th
day result comes very
significant (p<0.01) with comparision to base line in Control group highly significant
(p<0.001) in Test group.
Effect on Progressive weakness: It was found that the difference between the
median scores of progressive weakness in Control group at 30th
day and 45th
day with
baseline was significant (p<0.05), while in Test group on 45th
day compared with
baseline was also significant (p<0.05). Intergroup comparison was also not
significant at 45th
day (p>0.05).
Effect on Dizziness: It was found that the difference between the median scores of
Summary
107
Dizziness in Test group and Control group at 45th
day compared with baseline was not
significant (p>0.05). Intergroup comparison was also not significant at 45th
day
(p>0.05).
Effect on Unexplained weight loss: It was found that the difference between the
median scores of unexplained weight loss in Test and Control group at 45th
day
compared with baseline was not significant (p>0.05) in Control group while in Test
group was significant (p<0.01) at 45th
day. Intergroup comparison was also not
significant at 45th
day (p>0.05).
Effect on Pruritus: It was found that the difference between the median scores of
pruritus in Test group at 45th
day compared with baseline was not significant
(p>0.05).
Objective Parameters:
Effect on FBS: The Mean ± SEM score for FBS in Test group was 186.31±12.145 on
baseline and 174.43± 14.919 on 45th
day, whereas in Control group the Mean ± SEM
score of FBS was 190.286± 13.27 on baseline and 185.2 ± 15.238 on 45th
day. The
baseline and 45th
day comparision of mean scores for FBS in Test and Control group
not found significant difference statistically.
Effect on PPBS: The Mean ± SEM score for PPBS in Test group was 281.8 ± 19.113
on baseline and 266.7 ± 18.226 on 45th
day, whereas in Control group the Mean ±
SEM score of PPBS was 292.9± 45.377 on 0 day and 285.9 ± 21.449 on 45th
day.
When Mean ± SEM score of PPBS in both Groups, Test and Control, were compared
statistically, it was found that the difference between the Mean ± SEM score of Test
group and Control group both at 45th
day compared with baseline was not significant
(p>0.05).
Summary
108
Effect on Urine sugar: The Mean ± SEM score of urine sugar was calculated on 0
day, 15th
day 30th
day and 45th
day as 0.687±0.187, 0.575±0.196, 0.406±0.1894 and
0.218±0.101 in Test group respectively, while the same was observed as 1.033±0.226,
0.766±0.233, 0.733±0.223 and 0.333±0.159 on 0 day, 15th
day, 30th
day and 45th
day
respectively in Control group. When the two groups were compared statistically found
that the difference between the median scores of Control group at 45th
day with
baseline was significant (p<0.05), while in Test group on 45th
day compared with
baseline was very significant (p<0.01). Intergroup comparison was not significant at
45th
day (p>0.05).
Effect on HbA1c: The Mean ± SEM score for HbA1c in Test group was 8.818±0.257
on baseline and 8.3±0.283 on 45th
day, whereas in Control group the Mean ± SEM
score of HbA1c was 9.11±0.357 on 0 day and 8.41±0.308 on 45th
day. When Mean ±
SEM scores of HbA1c in both Groups, Test and Control, were compared statistically,
it is found that the difference between the Mean ± SEM score of Test and Control
groups at 45th
day compared with baseline was significant (p<0.05).
Bibliography
109
Bibliography
1. Huizinga MM, Rothman RL. Addressing the diabetes pandemic: A
comprehensive approach. Indian J Med Res 2006; 124: 481-4.
2. Park K. Park’s Text Book of Preventive and Social Medicine. 20th
ed.
Jabalpur India: Banarasidas Bhanot; 2009: 341-345.
3. Sicree R, Shaw J, Zimmet P. Diabetes and impaired glucose tolerance.
International Diabetes Federation, 3rd
ed. Belgium: 2006; 15-103.
4. Firozuddin MS. Romoozul Atibba. Vol. II. New Delhi: Idara Kitabul Shifa;
2009: 262.
5. Jani DK, Nesari MT, Vijayakumar D, Loriaux, Lynn D. Diabetes and the
Ebers Papyrus: 1552 BC. The Endocrinologist 2006; 16(2): 55-6.
6. Barthold SW. Unsung heroes in the battle against diabetes. ILAR: 2004; 45;
227-30.
7. Singh M, Kumar N, Sood S, Makkar B, Arora V. Historical Milestones in
Diabetes. Australasian Medical Journal 2010; 3, 13, 860-864.
8. Savona-Ventura C. The History of Diabetes Mellitus, A Maltese perspective.
e-book. 2003: 1-7.
9. Sanders LJ. From Thebes to Toronto and the 21st century: An incredible
journey. Diabetes Spectrum 2002; 15: 56-60.
10. Gemmill CL. The Greek Concept of Diabetes. Bull. N. Y. Acad. Med
September 1972; 48, 8, 1033-1036.
11. Kirchhof M, Popat N, Malowany J. A historical perspective of the diagnosis
of diabetes. UWOMJ 2008; 78(1): 7-11.
Bibliography
110
12. Eknoyan G, Nagy J. A history of diabetes mellitus or how a disease of the
kidneys evolved into a kidney disease. Advances in Chronic Kidney Disease
April 2005; 12, 2, 223-229.
13. Henschen F. On the term diabetes in the works of Aretaeus and Galen. Med
Hist 1969; 13(2): 190-2.
14. Ahmed AM. History of diabetes mellitus. Saudi Medical Journal 2002; 23
(4): 373-8.
15. Rengachary SS, Xavier A, Manjila S, Smerdon U, Parker B, Hadwan S. et al.
The legendary contributions of Thomas Willis (1621–1675): the arterial
circle and beyond. J Neurosurg 2008; 109:765-75.
16. Longe JL. The Gale Encyclopedia of Alternative Medicine. Vol II, 2nd
ed.
Farmington Hills USA: Gale Group; 2005: 617-623.
17. Edwards CRW, Toft AD, Walker BR. Davidson’s Principles and Practice of
Medicine. 19th
ed. New York: Churchill Livingstone; 2004: 642-63.
18. Vinay K, Abbas A, Nelson F. Robbins and Cotran Pathologic Basis of
Disease. 7th
ed. Philadelphia: Elsevier Saunders; 2005: 1189-1205.
19. Fauci AS, Braunwald E, Kasper L. Dennis. Harrison’s Principal of Internal
Medicine. Vol. II, 17th
ed. New York: McGraw Hill’s; 2008: 2275-95.
20. David HH, Herbert L. Dupont. Kelley’s Textbook of Internal Medicine. 4th
ed. Vol. II. New York: Lippincott, Williams & Wilkins Publishers; 2000:
2642-45.
21. Becker KL, Ronald C. Principles and Practice of Endocrinology and
Metabolism. 3rd
ed. New York: Lippincott Williams & Wilkins Publishers;
2002: 1086-94, 1106-11.
22. Goodman HM. Basic Medical Endocrinology. 3rd ed. e-Book: 2002: 178-81.
Bibliography
111
23. Ibne Sina. Al Qanoon Fit Tib (Urdu translation by Kantoori GH). New Delhi:
Idara Kitabul Shifa; 2009: 1031-33, 353-54.
24. Ibne Sina. Al Qanoon Fit Tib (Arabi). 1st ed. Vol. III, Part 2. New Delhi:
Jamia Hamdard; 1408H: 263-64, 783-85.
25. Khan M Ajmal. Haziq. New Delhi: Jasem Book Depot; 1983: 387-90.
26. Majoosi A. Kamilus Sana (Urdu translation by Kantoori GH) Vol. I.
Lucknow: Munshi Nawal Kishore; 1889: 469-70.
27. Jurjani AHI. Zakhira Khawarzam Shahi (Urdu translation by khan HH) Vol.
II, Part 6. New Delhi: Idara Kitabul Shifa; 1996::540-41.
28. Ibne Zohar. Kitabut Taiseer (Urdu translation by CCRUM). New Delhi:
CCRUM; 1986: 160-63.
29. Ibne Hubal B. Kitabul Mukhtarat Fil Tib (Urdu translation by CCRUM).
Vol. III. New Delhi: CCRUM; 2005: 326-8.
30. Razi MZ. Kitabul Havi. (Urdu translation by CCRUM). Vol. 10. New Delhi:
CCRUM; 2002: 181-87.
31. Wild S, Rogli G, Green A, Sicree R, King H. Global prevalence of diabetes:
estimates for the year 2000 and projections for 2030. Diabetes Care 2004;
27:1047-1053.
32. Berrens M, Kahn R, Nolan J, Pramming S, Riazza RA. Definition, Diagnosis
and Classification of Diabetes Mellitus and its Complications, Report of a
WHO Consultation, Part 1. Geneva: World Health Organization, Department
of Noncommunicable Disease Surveillance; 1999: 2-10.
33. Sajeeth CI, Manna PK, Manavalan R, Jolly CI. Antidiabetic activity of a
polyherbal formulation esf/ay/500 in streptozotocin induced diabetic male
Bibliography
112
albino rats: a research. International Journal of Drug Formulation &
Research. Aug-Sep. 2010; Vol. 1(1) 2229-5054.
34. Qarshi MH, Jameul Hikmat. Vol. II. New Delhi: Idara Kitabul Shifa; 2011:
864-70.
35. Khan MA. Romooze Aazm (Farsi). Vol. I. New Delhi: CCRUM; 2006: 139-
41.
36. Hui D, Leung A, Padwal R. Approach to Internal Medicine. 3rd
ed. Houston
USA: Springer; 2001: 337-42.
37. Ghosh AK, Wittich CK, Rhodes DJ. Mayo Clinic Internal Medicine Review. 8th
ed. Canada: Mayo Foundation Scientific Press; 2008: 234-39.
38. Goldman L, Dennis A. Cecil Text book of Medicine. 23th
ed. Vol. II. USA:
Saunders Elsevier Publication; 2003: 1424-33
39. Foster C, Mistry NF, Peddi PF, Sharma S. The Washington Manual of
Medical Therapeutics. Philadelphia, USA: Lippincott Williams & Wilkins;
2010: 794-797.
40. Lloyed RV. Endocrine Pathology Differential Diagnosis and Molecular
Advances. 2nd
ed. New York: Springer Science Business Media; 2010: 367,
368, 372-75.
41. Kirmani NBA. Kulliyate Nafeesi (Urdu translation by Kabeeruddin) Vol. I.
New Delhi: Idara Kitabul Shifa; YNM: 103, 106-8, 114-18.
42. Ahmed SI. Introduction to Al Umur Attabiyah. 1st ed. New Delhi: Saini
Printers; 1980: 146, 162-72.
43. Azmi AA. Basic Concepts of Unani Medicine. 1st ed. New Delhi: Jamia
Hamdard; 1995: 131
Bibliography
113
44. Maseehi AS. Kitabul Miya (Fit Tib) (Urdu Translation by CCRUM). New
Delhi: CCRUM; 2008: 127-133.
45. Davies A, Blakeley AGH, Kidd C. Human Physiology. 1st ed. London: Harcout
Puplisher; 2001: 451-56.
46. Khan AM, Rzaq MA, Ahad MA. Mojizul Mahsha (Arabi). New Delhi:
Mujtabai; 1415: 387-78.
47. Samarqandi N. Sharah Asbab (Urdu translation by Ayyub M.). Vol. III. New
Delhi: Aijaz Pulishing House; YNM: 38-48.
48. Khan MA. Akseere Azam (Urdu translation by Kabeeruddin M.). Vol. II.
New Delhi: Idara Kitabul Shifa; 2011: 705-709.
49. Souhami RL, Moxham J. Textbook of Medicine. 4th
ed. London: Churchill
Livingstone, Medical division of Pearson limited; 2004: 979-80, 984-86,
994-95.
50. Wilson, Foster, Kronenberg HM, Larsen PR. Williams Textbook of
Endocrinology. 10th
ed. Philadelphia, USA: Saunders Company; 2003: 1427-
68.
51. Stephen J. McPhee, Maxine A. Papadakis, Tierney LM. Current Medical
Diagnosis and Treatment. San Francisco, USA: McGraw Hill’s; 2010: 97,
1104-9.
52. Shah Siddharth N. API Text Book of Medicine. Vol. II. 8th
ed. Mumbai: The
Association of Physicians of India; 2008: 1043-69
53. Dale DC, Federman DD. APC Medicine. Web MD; 2005: Chapter-6, 1780-
1815.
54. Walter Siegenthaler. Differential Diagnosis in Internal Medicine.19th
ed.
Germany: Georg Thieme Verlag Rüdigerstrasse Stuttgart; 2007: 38-40.

Bibliography
114
55. Warrell DA, Cox TM, Firth JD, Edward J, Benz MD. Oxford Textbook of
Medicine. 4th
ed. New York, USA: Oxford Press; 2003: 1305-42.
56. Douglas G, Nicol F, Robertson C. Macleods’s Clinical Examination. 12th
ed.
China: Elsevier; 2009: 94-95
57. Ferri FF. Practical Guide to the Care of the Medical Patients. USA: Mosby Ink;
5th ed. 2001: 212-32.
58. Godlee EF, Tivery D. BMJ Clinical Evidence. London: BMJ Publishing Group;
2004: 386-88.
59. Shils ME, Olson JA, Shike M, Ross AC. Modern Nutrition in Health and
Disease. 9th
ed. USA: Lippincott, Williams & Wilkins; 1999: 54-58.
60. Ledigham JGG, Warrel DA. Concise Oxford Textbook of Medicine. Landon:
Oxford University Press; 2000: 734-37.
61. Corwin EJ. Handbook of Pathophysiology. 3rd
ed. Columbus, Ohio:
Lippincott Williams & Wilkins; 2008: 558-567.
62. Essential of nutrition
63. Petit W, Adamec C. The Encyclopedia of Endocrine Diseases and Disorders.
New York: Facts on File, Inc; 2005: 60-67.
64. Torre DM, Lamb GC, Ruiswyk JJV, Schapira RM. Kochar's Clinical
Medicine for Students. 5th
ed. Milwaukee, Wisconsin: Lippincott Williams &
Wilkins; 2009: 379-90.
65. Raghunathan K, Mitra R. Pharmacognosy of Indigenous Drugs. Vol. II. New
Delhi: CCRAS; 806-12, 321-30.
66. Nadkarni KM. Indian Plants and Drugs. New Delhi: Srishti Book
Distributers; 2005: Vol. 1, 1220-21, 173-4, 844-45.
Bibliography
115
67. Kirtikar KR, Basu BD. Indian Medicinal Plants with Illustrations. Vol. I. 2nd
ed. Dehradun: Oriental Enterprises; 2003: 77-80, 116-20, 172-74
68. Anonymous. The Wealth of India. Vol. I A-F, II G-Ph, III Pi-Z. New Delhi:
Council of Scientific and Industrial Research; 2003: 207-8, 33-35, 215-16.
69. Duke JA, Godwin MJB. Handbook of Medicinal Herbs. 2nd
ed. London:
CRC Press 2002: 361.
70. William D. Pharmacographia Indica- A history of the principal drugs of
vegetable origin. Vol. I & III. New Delhi: Published by Srishti book
distributors; 2005: 54-56, 586-91.
71. Chopra RN, Nayar SL, Chopra IC. Glossary of Indian Medicinal Plants.
New Delhi: NISCAIR, CSIR; 2005: 244-45, 33, 244-45.
72. Khare CP. Indian Medicinal Plants. 1st ed. New Delhi: Springer Science;
2007, 80-81, 435-36.
73. Rastogi RP, Mehrotra BN. Compendium of Indian Medicinal Plants. Vol. I
& II. New Delhi: Central Drug Research Institute; 1999: 288-89, 679-80.
74. Squire Peter Wyatt. British Pharmacopoeia. Vol. 4. Delhi: Asiatic
Publishing House; 2009: 1216.
75. Bentley Robert. Medicinal Plants. Vol. I. Delhi: Asiatic Publishing House
Laxmi Nagar; 2002: 243-45.
76. Anonymous. The Unani Pharmacopeia of India. Vol. I Part-1& IV. New Delhi:
Ministry of Health and Family Welfare; 2007: 30-31, 66-67.
77. Sharma PC, Yelne MB, Dennis TJ. Database on Medicinal Plants Used in
Ayurveda. Vol. III. New Delhi: CCRAS: 2005: 256-60.
78. Behl PN. Srivastava G. Herbs Useful in Dermatological Therapy. 2nd
ed.
New Delhi: CBS Publisher and Distributor; 2002: 36-37, 136-37.
Bibliography
116
79. Nasreen S, Radha R, Jayashree N, Rajendran A. Assesment of Quality of
Tinospora cardifolia (Willd). (Menispermaceae): Pharmacognostical and
Phyto-Physicochemical profile. Internation Journal of Comprehensive
pharmacy 2010; 0976-8157.
80. Soni H, Nayak G, Patel SS, Mishra K, Singh RP & Singhai AK.
Pharmacognostic studies of the leaves of Tinospora cardifolia. IJPI’s
Journal of Pharmacognosy and Herbal Formulation 2011; 2229-6840.
81. Anonymous. Qarabadeen Sarkari. New Delhi: CCRUM; 2006: 99, 121-22.
82. Anonymous. Medicinal Plants in Folklores of Northern India. New Delhi:
CCRUM; 2001: 485.
83. Ghani N. Khazainul Advia. New Delhi: Idara Kitabul Shifa; YNM: 395-6,
1075, 789-90.
84. Hakeem HMA. Bustanul Mufradat. New Delhi: Idara Kitabul Shifa; 2002:
98, 459, 489-90, 210-11.
85. Rafeequddin M. Kanzul Adviyae Mufrada. Aligarh: University Publication
Unit, Sarfaraz House; 1985: 481-82, 594-95.
86. Kulkarni PH, Shahida Ansari. The Ayurvedic Plants. Delhi: Sri Satguru
Publications; 2004: 221, 313.
87. Handa SS, Rakesh DD. Compendium of Medicinal and Aromatic Plants
Asia. Vol. II. Trieste, Italy: ICS UNIDO; 2006: 126, 133.
88. Gulam Nabi M. Makhzane Mufradat wa Murakkabat. New Delhi: CCRUM;
2007: 191, 203.
89. Bhattacharjee SK. Handbook of Medicinal Plants. 4th
ed. Jaipur: Pointer
Publishers; 2004: 352, 235-36.
Bibliography
117
90. Kabeeruddin M. Makhzanul Mufradat. New Delhi: Idara Kitabul Shifa;
2007: 292, 336, 354-55.
91. Joy PP, Thomas J, Mathew S, Skaria BP. Medicinal Plants. Ernakulam,
Kerla: Agricultural University-Aromatic and Medicinal Plant Research
Station; 1998: 81, 187, 200.
92. Abdul Hakeem HM. Mufradate Azeezi. New Delhi: CCRUM; 2009: 33, 104,
101.
93. Khan S. Bayaze Khas Almaroof Ilajulamraz. New Delhi: Aijaz Pulishing
House; 2006: 252, 281, 282 302, 352, 362, 392, 485, 631, 776.
94. Kabeeruddin. Bayaze Kabir. Vol 2, Part 2. Hyderabad: Hikmat Book Depo;
1935: 27, 38, 55, 56, 57, 72, 74, 71, 78.
95. Hakeem M Said. Hamdard Pharmacopoeia of Eastern Medicine. 2nd
ed. New
Delhi: Indian Books Centre; 1997: 80, 81, 86, 92, 107, 125, 128, 130, 158,
202, 247.
96. Sivakumar V, Dhana Rajan MS. Hypoglycemic and antioxidant activity of
Tinospora cardifolia in experimental diabetes. International Journal of
Pharmacceutical Sciences and Research 2011; 2(3): 608-613.
97. Stanely P, Prince M and Menon VP: Hypoglycemic and other related actions
of Tinospora cordifolia roots in alloxan-induced diabetic rats. J
Ethnopharmacology 2000; 70 (1): 9 -15.
98. Stanely Mainzen Prince P, Menon VP, Gunasekaran G. Hypolipidaemic
action of Tinospora cordifolia roots in alloxan diabetic rats. J
Ethnopharmacology 1999; 64: 53–7.
Bibliography
118
99. Dinesh D, Vaneeta J, Sunil S, Kumar HR. Evaluation of antiobesity activity
of Tinospora cardifolia stems in rats. International Journal of Research in
Ayurveda and Pharmacy 2011; 2(1) 306-311
100. Maurya R, Wazir V, Tyagi A, Kapil RS. Clerodane diterpenoids from the
Tinospora cardifolia. Phytochemistry 1995; 38: 659.
101. Grover JK, Rathi SS, Vats V. Amelioration of experimental diabetic
neuropathy and gastropathy in rats following oral administration of plant
(Eugenia jambolana, Mucuna pruriens and Tinospora cordifolia)
extracts. Indian J Exp Biol 2002; 40: 273–6.
102. Raghunathan K, Sharma PV. The aqueous extract of T. cordifolia caused
reduction of blood sugar in alloxan induced hyperglycemic rats and rabbits. J
Res Ind Med. 1969; 3: 203-9.
103. Gupta SS, Verma SC, Garg VP, Rai M. Antidiabetic effect of Tinospora
cordifolia. I: Effect on fasting blood sugar level, glucose tolerence and
adrenaline induced hyperglycemia. Indian J Med Res.1967; 55: 733-45.
104. Wadood N, Wadood A, Shah SA. Effect of Tinospora cordifolia on blood
glucose and total lipid levels of normal and alloxan-diabetic rabbits. Planta
Med. 1992; 58: 131-6.
105. Badar VA, Thawani VR, Wakode PT, Shrivastava MP, Gharpure KJ,
Hingorani LL. et al. Efficacy of Tinospora cordifolia in allergic rhinitis. J
Ethnopharmacol. 2005; 96: 445-9.
106. Rao PR, Kumar VK, Viswanath RK, Subbaraju GV. Cardioprotective
activity of alcoholic extract of Tinospora cordifolia in ischemia-reperfusion
induced myocardial infarction in rats. Biol Pharm Bull. 2005; 28: 2319-22
Bibliography
119
107. Nagaraja PK, Kammar KF, Devi S. Efficacy of Tinospora cordifolia (Willd.)
extracts on blood lipid profile in streptozotocin diabetic rats: Is it beneficial
to the heart? Biomedical Research 2008; 19: 92-6.
108. Mehrotra R, Katiyar CK, Gupta AP. Hepatoprotective composition and
composition for treatment of conditions related to hepatitis Band E infection.
US Patent 2000; 749296
109. Singh SS, Pandey SC, Srivastava S, Gupta VS, Patro B, Ghosh AC.
Chemistry and medicinal properties of Tinospora cardifolia. Indian Journal
of Pharmacology 2003; 35: 83-91.
110. Wesley JJ, Christina AJ, Chidambaranathan N. Effect of alcoholic extract of
Tinospora Cordifolia on acute and subacute Inflammation.
Pharmacologyonline. 2008; 3: 683-7.
111. Singh N, Singh SM, Shrivastava P. Immunomodulatory and antitumor
actions of medicinal plant Tinospora cordifolia are mediated through
activation of tumor-associated macrophages. Immunopharmacol
Immunotoxicol. 2005; 26: 145-62.
112. Kapur P, Jarry H, Wuttke W, Pereira BM, Seidlova-Wuttke D. Evaluation of
the antiosteoporotic potential of Tinospora cordifolia in female
rats. Maturitas. 2008; 59: 329-38.
113. Gupta RS, Sharma A. Antifertility effect of Tinospora cordifolia (Willd.)
stem extract in male rats. Indian J Exp Biol. 2003; 41: 885-9.
114. Bafna PA, Balaraman R. Anti-ulcer and anti-oxidant activity of pepticare: A
herbomineral formulation. Phytomedicine. 2005; 12: 264-70.
Bibliography
120
115. Asthana JG, Jain S, Mishra A, Vijaykant MS. Evaluation of antileprotic
herbal drug combinations and their combination with Dapsone. Indian
Drugs. 2001; 38: 82-6.
116. Nayampalli SS, Ainapure SS, Samant BD, Kudtarkar RG, Desai NK, Gupta
KC. A comparative study of diuretic effects of Tinospora cordifolia and
hydrochloro-thiazide in rats and a preliminary phase I study in human
volunteers. J Postgrad Med. 1988; 34: 233-6.
117. Nagaraja PK, Kammar KF, Devi S. Modulation of morphology and some
gluconeogenic enzymes activity by Tinospora cordifolia (Willd.) in diabetic
rat kidney. Biomed Res. 2007; 18: 179-83.
118. Evans WC. Treas and Evans Pharmacognosy. 15th ed. London: Saunders
Publishers; 2004: 37-38.
119. Prajapati ND, Kumar U. Agro’s Dictionary of Medicinal Plants. Agrobios:
Jodhpur: 2005, 224.
120. Daood Antaki. Tazkete Ulul Albaab (Arabi). Vol. 1. New Delhi: CCRUM;
2008, 430-31.
121. Arzani MA. Qarabadeene Qadri. New Delhi: Aijaz Publishing House: 1998:
160, 197, 203, 205, 208, 437.
122. Anonymous. National formulary of Unani Medicine. Vol. 4. New Delhi:
CCRUM; 2007: 57.
123. Anonymous. Qarabadeen Majeedi. 9th
ed. New Delhi: Ajanta Offset &
Packaging Ltd; 2000: 43, 45, 54, 63, 119, 124, 125, 127, 128, 182, 325.
124. Ibraheem Almaghribi AS. Kitabul Fath Fil Tadawi (Urdu Translation). New
Delhi: NCPC Printers; 2007: 122-123.
Bibliography
121
125. Hubl Baghdadi. Al Mukhtarat Fit Tib. Vol. II. New Delhi: CCRUM; 2005:
162.
126. Anonymous. Medicinal Plants in Folklores of Southern India. New Delhi:
CCRUM; 2001: 52.
127. Prajapati ND, Purohit SS, Sharma AK. A Handbook of Medicinal Plants. 1st
ed. Jodhpur: Agrobios; 2009: 360.
128. Satyavati GV, Gupta AK. Medicinal Plants of India. Vol-2. New Delhi:
Indian Council of Medical Research; 1987: 325-28.
129. Rafiullah MRM, Ali M, Pillai KK, Singh S. Antidiabetic Activity of
Nelumbo nucifera extract in Normal and Streptozotocin Induced Diabetic
Rats. Hippocratice Journal of Unani Medicine June 2008; Vol. No. 2, 69-78.
130. Jiang Y, Bun Ng T, Liu Z, Wang C, Li N, Qiao W, Liu F. Imonoregulatory
and anti-HIV-1 Enjyme activities of antioxidants components from lotus
(Nelumbo nucifera Gaertn) rhizome. Bioscience Reports Immediate
Publication Nov 2010; 20100062.
131. Wang L, Yen JH, Liang HL, Wu MJ. Antioxidant Effect of Methanolic
Extracts from Lotus Plumle and Blossom (Nelumbo nucefera). Journal of
food and drug Analysis 2003; Vol. 11, 1: 60-66.
132. Durairaj B, Dorai A. Antiplatele activity of white and pink Nelumbo nucifera
Gaertn flowers. Razilian Journal of Pharmaceutical Sciences 2010; 46, 3.
133. Yang W, Lu J, Weng J, Jia W, Ji L, Xiao J, et al. Prevalence of Diabetes
among Men and Women in China. The New England Journal of Medicine
2010; 362: 12, 1090.
134. Connolly V, Unwin N, Sherriff P, Bilous R, Kelly W. Diabetes prevalence
and socioeconomic status: a population based study showing increased
Bibliography
122
prevalence of type 2 diabetes mellitus in deprived areas. J Epidemiol
Community Health 2000; 54: 173–177.
135. Jali MV, Kamber S. Prevalence of the family members of the known
diabetics. Int J Diab Dev Ctries October 2010; IP: 59.183.135
136. Valdez R. Detecting Undiagnosed Type 2 Diabetes: Family History as a Risk
Factor and Screening Tool. Journal of Diabetes Science and Technology July
2009; Volume 3, Issue 4,
137. Sena CM, Louro T, Matafome P, Nunes E, Monteiro P, Seiça R. Antioxidant
and Vascular Effects of Gliclazide in Type 2 Diabetic Rats Fed High-Fat
Diet: Physiol. Res. 2009: 58: 203-209.
Annexure
123
ANNEXURE I
PATIENT’S CONSENT FORM
I …………………………………………………....exercising my free power of
choice, hereby give my consent to be included as a subject in the clinical trial of
Clinical Study of Ziabetus Shakari (Diabetes Mellitus Type II) and Evaluation of
Efficacy of a Unani Formulation in its Management. I understand that I may be
treated with these drugs for the disease, I am suffering from. I have been informed to
my satisfaction, by attending physician the purpose of the clinical trial and the nature
of drug treatment and follow up including the laboratory investigation to monitor and
safeguard my body function.
I am also aware of my right to drop out of the trial at any time during the course of
the trial without having to give the reason for doing
Date: …………………….
Signature of Patient…………………
Signature of Doctor…………………
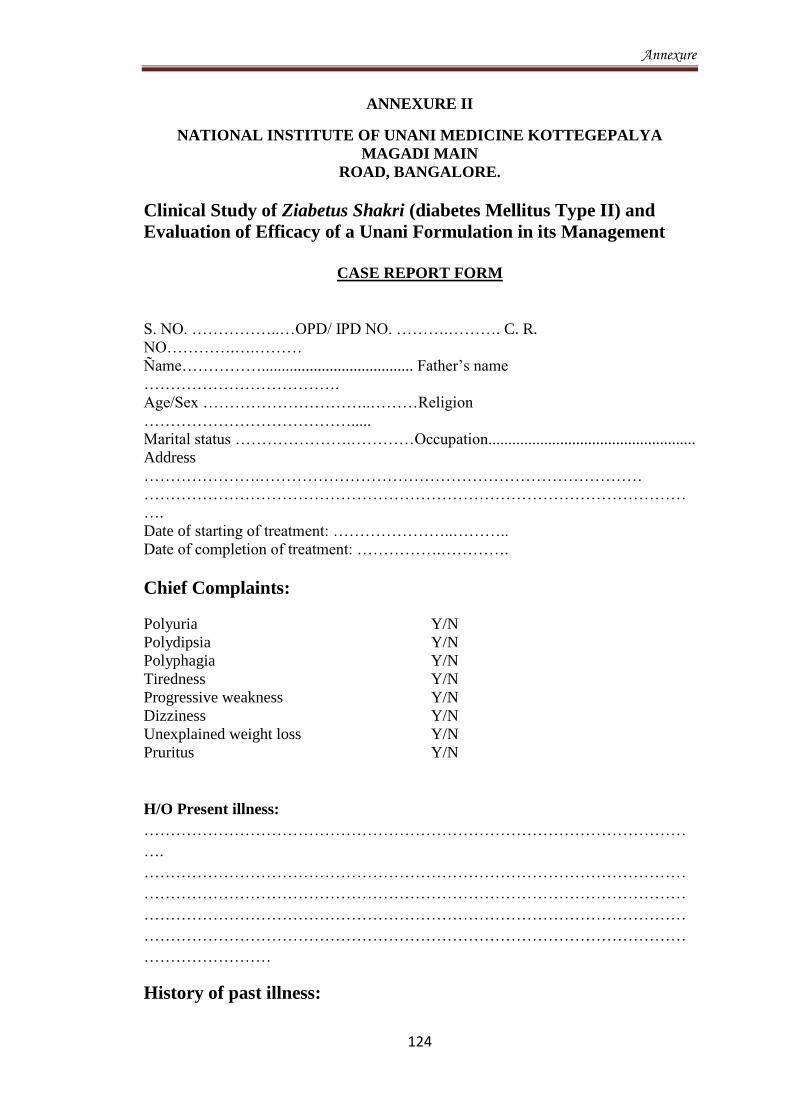
Annexure
124
ANNEXURE II
NATIONAL INSTITUTE OF UNANI MEDICINE KOTTEGEPALYA
MAGADI MAIN
ROAD, BANGALORE.
Clinical Study of Ziabetus Shakri (diabetes Mellitus Type II) and
Evaluation of Efficacy of a Unani Formulation in its Management
CASE REPORT FORM
S. NO. ……………..…OPD/ IPD NO. ……….………. C. R.
NO………….….………
Ñame……………...................................... Father’s name
……………………………….
Age/Sex …………………………..………Religion
………………………………….....
Marital status ………………….…………Occupation....................................................
Address
………………….………………………………………………………………
…………………………………………………………………………………………
….
Date of starting of treatment: …………………..………..
Date of completion of treatment: …………….………….
Chief Complaints:
Polyuria Y/N
Polydipsia Y/N
Polyphagia Y/N
Tiredness Y/N
Progressive weakness Y/N
Dizziness Y/N
Unexplained weight loss Y/N
Pruritus Y/N
H/O Present illness:
…………………………………………………………………………………………
….
…………………………………………………………………………………………
…………………………………………………………………………………………
…………………………………………………………………………………………
…………………………………………………………………………………………
……………………
History of past illness:

Annexure
125
1. DM…………………………………….
2 .HTN…………………………………...
3. Liver diseases ………………………...
4. Renal diseases……………………..…..
5. Cardiovascular Diseases………………
Family history:
Father.............................................. Mother……………………
Brother.................…………...…… Sister……………………...
Son…………….. ………………... Daughter………………….
Personal history:
1. Appetite: Good / Fair / Poor.
2. Diet: Veg. / Non Veg / Mixed.
3. Addiction: Smoking / Alcoholism / Pan Chewing / others...............................
4. Sleep: Good / fair / poor
5. Bowel habit: Day / Night…….………
6. Bladder habit: Day / Night……...........
7. Psychological status: …………………
8. Physical work: Sedentary /Mild/Moderate/Hard work
Social history: Upper class/Upper Middle class/Lower Middle Class/…………………………….
Upper Lower class/Lower class…………………………………………………….
Occupational history:
1. Name of work ……………………2. Nature of work …………………………
Treatment history: Allopathic/Unani/Ayurvedic/Homeopathic…………
Name of the medicine: ………………………….
H/O Allergy
……………………………………………………………………………..
Gynecological and Obstetrical History:
1. Age of menarche............. 2. Duration of cycle...............
3. Amount of flow............... 4. Duration of menses............
5. Dysmenorrhoea............... 6. Gravida..............................
7. Parity............................... 8. Abortion............................
9. Last delivery.................... 10. LMP................................
11. H/O Contraceptives...................
GENERAL PHYSICAL EXAMINATION
1. Built ……….. 2. Body weight………
3. Height............ 4. Pallor..........
5. Cyanosis …… 6. Clubbing of finger ………………
7. Icterus ……….. 8. Edema
9. Arcus Senilis...... 10. Xanthelasma………...…............
11. Lymphadenopathy ………………….....................
12. Cervical lymph node……………………….………
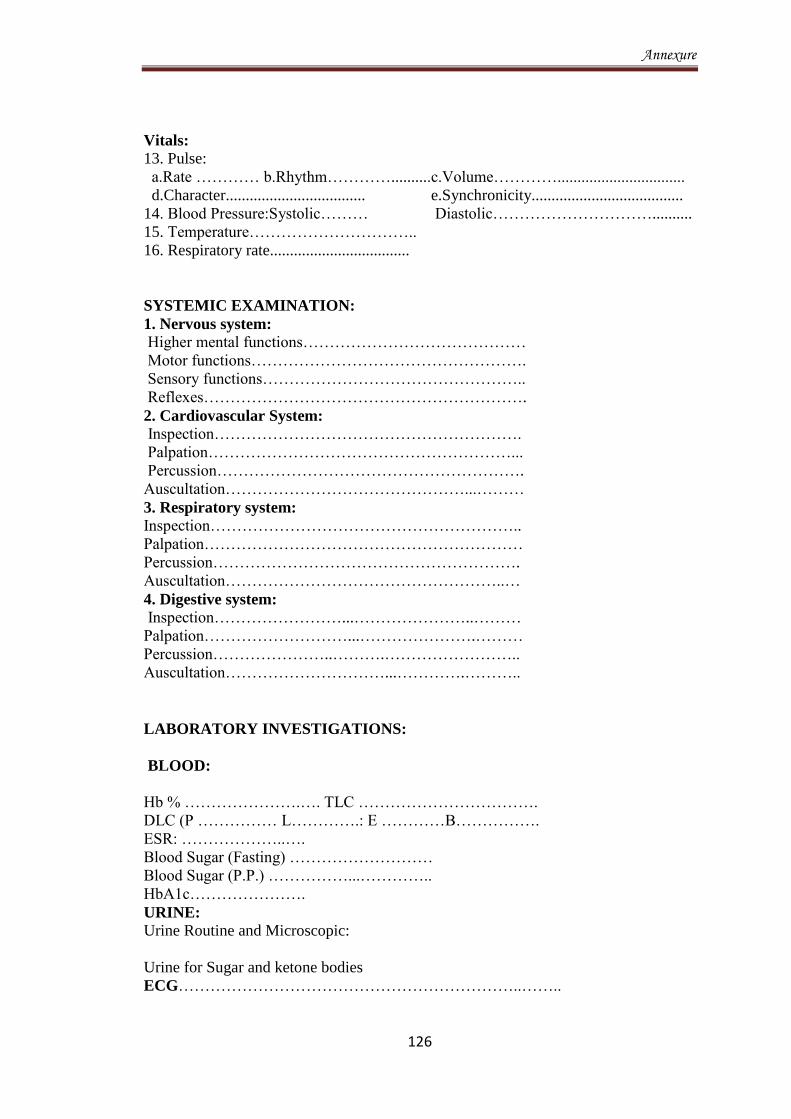
Annexure
126
Vitals:
13. Pulse:
a.Rate ………… b.Rhythm…………..........c.Volume…………................................
d.Character................................... e.Synchronicity......................................
14. Blood Pressure:Systolic……… Diastolic…………………………..........
15. Temperature…………………………..
16. Respiratory rate...................................
SYSTEMIC EXAMINATION:
1. Nervous system: Higher mental functions……………………………………
Motor functions…………………………………………….
Sensory functions…………………………………………..
Reflexes…………………………………………………….
2. Cardiovascular System:
Inspection………………………………………………….
Palpation…………………………………………………...
Percussion………………………………………………….
Auscultation………………………………………...………
3. Respiratory system:
Inspection…………………………………………………..
Palpation……………………………………………………
Percussion………………………………………………….
Auscultation……………………………………………..…
4. Digestive system:
Inspection……………………...…………………..………
Palpation………………………...………………….………
Percussion…………………..……….……………………..
Auscultation…………………………...………….………..
LABORATORY INVESTIGATIONS:
BLOOD:
Hb % ………………….…. TLC …………………………….
DLC (P …………… L………….: E …………B…………….
ESR: ………………..….
Blood Sugar (Fasting) ………………………
Blood Sugar (P.P.) ……………...…………..
HbA1c………………….
URINE:
Urine Routine and Microscopic:
Urine for Sugar and ketone bodies
ECG………………………………………………………..……..

Annexure
127
LFT………………………………………………………………..
KFT: ………………………………………………………………
Diagnosis…………………………………………………………..
Treatment………………………………………………………….
PARAMETER FOR ASSESMENT: Assessment of efficacy:
A. Clinical Parameter:
S.No. Sbjective
Parameter
0 day 15th
day 30th
day 45th
day
Grading
1.
Polyuria
2.
Polydipsia
3.
Polyphagia
4.
Tiredness
5.
Progressive
weakness
6.
Dizziness
7. Unexplained
weight loss
8. Pruritus
Nil: 0
Mild: +
Moderate: ++
Severe: +++
B. Laboratory Parameter:
S.No. Objective
Parameter
0 day 15th
day 30th
day 45th
day

Annexure
128
1.
Blood sugar (F)
2.
Blood Sugar
(P.P.)
3.
HbA1C
4.
Urine for sugar
Nil: 0
Mild: +
Moderate: ++
Severe: +++
Assessment of Safety Parameter:
S.No. Objective
Parameter
Before Treatment After Treatment
1.
Urine
Routine
Microscopic
Urine for
Ketone bodies
2.
Haemogram
Hb%
TLC
DLC
3.
KFT
Blood Urea
S. Creatinine
4.
LFT
AST
ALT
5.
ECG

Annexure
129
Date of starting treatment… ……
Follow up: 0…... 30…….60 days
Date of completion of treatment: …………….
Result... …………………….
Signature of PG scholar …………………….
Signature of supervisor …………………….

Annexure
130
ANNEXURE III
Assessment of Mizaj (Temperament)
parameters DAMVI
(Sanguine)
BALGHAMI
(Phlegmatic)
SAFRAVI
(Bilious)
SAUDAVI
(Melancholic)
Complexion
Ruddy(Reddish
/brown)
1
Chalky
(Whitish)
.75
Pale
(Yellowish)
.5
Purple
(Black)
.25
Build
Muscular &
Broad
1
Fatty &
Broad
.75
Muscular &
Thin
.5
Skeletal
.25
Touch
Hot & Soft
1
Cold &
Soft
.75
Hot & Dry
.5
Cold & Dry
.25
Hair
Black & lusty,
thick, Rapid
Growth.
1
Black &
thin. Slow
Growth.
.75
Brown &
Thin. Rapid
Growth
.5
Brown &
Thin. Slow
Growth.
.25
Movement
Active
1
Dull
.75
Hyperactive
.5
Less Active
.25
Diet
(most liked)
Cold & Dry
1
Hot & Dry
.75
Cold & Moist
.5
Hot & Moist
.25
Weather
(most liked)
Spring
1
Summer
.75
Winter
.5
Autumn
.25
Sleep
Normal
(6-8 hrs.)
1
In excess
.75
Inadequate
.5
Insomnia
.25
Pulse
Normal
(70-80/min)
1
Slow
(60-70)
.75
Rapid
(80-100)
.5
Slow
(60-70)
.25
Emotions
Normal
1
Calm &
quiet
.75
Angry
.5
Nervous
.25
Total =
Range of temperament in numbers:
Sanguine: 7.5-10……………….. : Phlegmatic: 5.10-7.50…………… ;
Bilious: 2.51-5.00……………… : Melancholic: 0.00 – 2.50…………
Balghami Safravi Saudavi Damvi
ANNEXURE IV
Kuppuswamy’s Socioeconomic Status Scale (Modified for 2007)
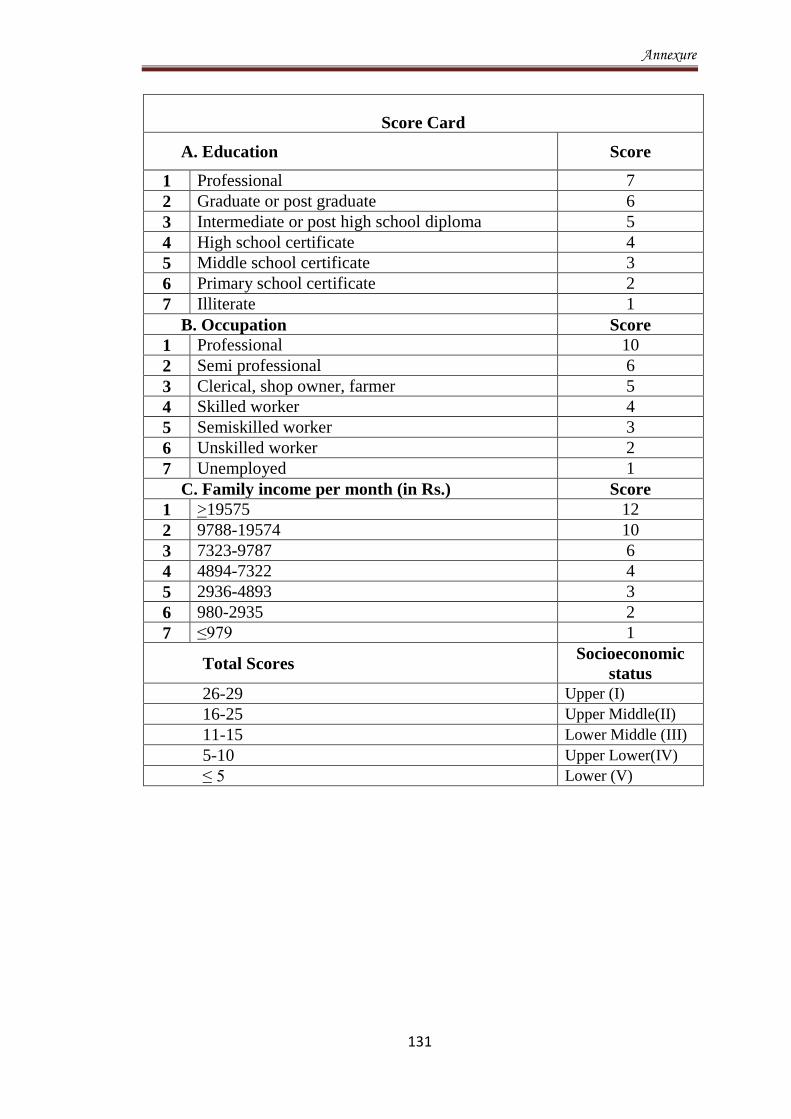
Annexure
131
Score Card
A. Education Score
1 Professional 7
2 Graduate or post graduate 6
3 Intermediate or post high school diploma 5
4 High school certificate 4
5 Middle school certificate 3
6 Primary school certificate 2
7 Illiterate 1
B. Occupation Score
1 Professional 10
2 Semi professional 6
3 Clerical, shop owner, farmer 5
4 Skilled worker 4
5 Semiskilled worker 3
6 Unskilled worker 2
7 Unemployed 1
C. Family income per month (in Rs.) Score
1 >19575 12
2 9788-19574 10
3 7323-9787 6
4 4894-7322 4
5 2936-4893 3
6 980-2935 2
7 ≤979 1
Total Scores Socioeconomic
status
26-29 Upper (I)
16-25 Upper Middle(II)
11-15 Lower Middle (III)
5-10 Upper Lower(IV)
≤ 5 Lower (V)
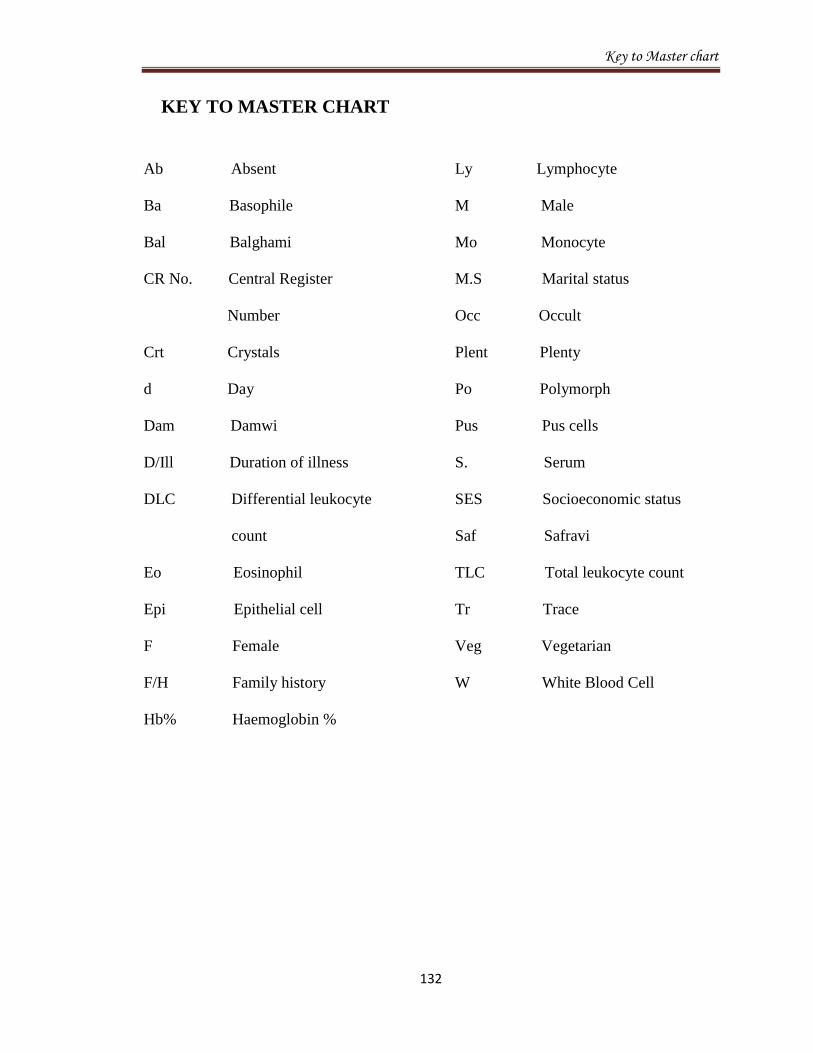
Key to Master chart
132
KEY TO MASTER CHART
Ab Absent
Ba Basophile
Bal Balghami
CR No. Central Register
Number
Crt Crystals
d Day
Dam Damwi
D/Ill Duration of illness
DLC Differential leukocyte
count
Eo Eosinophil
Epi Epithelial cell
F Female
F/H Family history
Hb% Haemoglobin %
Ly Lymphocyte
M Male
Mo Monocyte
M.S Marital status
Occ Occult
Plent Plenty
Po Polymorph
Pus Pus cells
S. Serum
SES Socioeconomic status
Saf Safravi
TLC Total leukocyte count
Tr Trace
Veg Vegetarian
W White Blood Cell
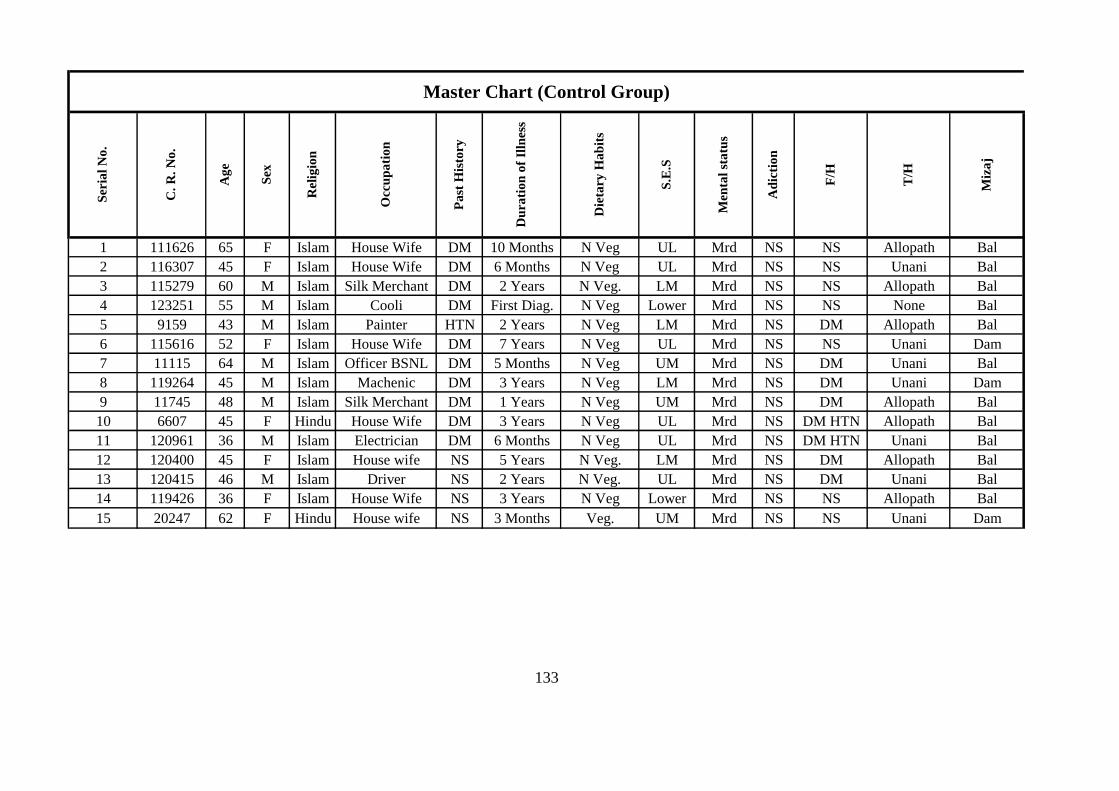
1 111626 65 F Islam House Wife DM 10 Months N Veg UL Mrd NS NS Allopath Bal
2 116307 45 F Islam House Wife DM 6 Months N Veg UL Mrd NS NS Unani Bal
3 115279 60 M Islam Silk Merchant DM 2 Years N Veg. LM Mrd NS NS Allopath Bal
4 123251 55 M Islam Cooli DM First Diag. N Veg Lower Mrd NS NS None Bal
5 9159 43 M Islam Painter HTN 2 Years N Veg LM Mrd NS DM Allopath Bal
6 115616 52 F Islam House Wife DM 7 Years N Veg UL Mrd NS NS Unani Dam
7 11115 64 M Islam Officer BSNL DM 5 Months N Veg UM Mrd NS DM Unani Bal
8 119264 45 M Islam Machenic DM 3 Years N Veg LM Mrd NS DM Unani Dam
9 11745 48 M Islam Silk Merchant DM 1 Years N Veg UM Mrd NS DM Allopath Bal
10 6607 45 F Hindu House Wife DM 3 Years N Veg UL Mrd NS DM HTN Allopath Bal
11 120961 36 M Islam Electrician DM 6 Months N Veg UL Mrd NS DM HTN Unani Bal
12 120400 45 F Islam House wife NS 5 Years N Veg. LM Mrd NS DM Allopath Bal
13 120415 46 M Islam Driver NS 2 Years N Veg. UL Mrd NS DM Unani Bal
14 119426 36 F Islam House Wife NS 3 Years N Veg Lower Mrd NS NS Allopath Bal
15 20247 62 F Hindu House wife NS 3 Months Veg. UM Mrd NS NS Unani Dam
Master Chart (Control Group)
S.E
.S
Men
tal
sta
tus
Ad
icti
on
Rel
igio
n
Occ
up
ati
on
Pa
st H
isto
ry
Du
rati
on
of
Illn
ess
Die
tary
Ha
bit
s
133
F/H
Miz
aj
T/H
Ser
ial
No
.
C.
R.
No
.
Ag
e
Sex
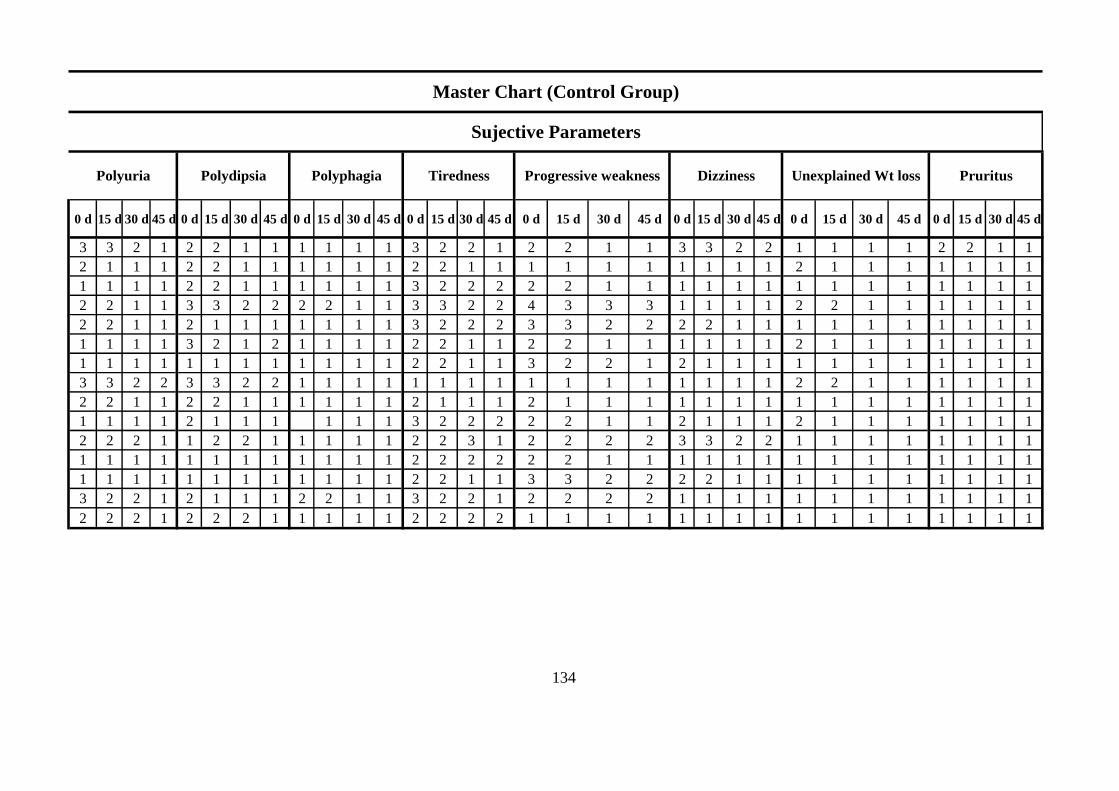
0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d
3 3 2 1 2 2 1 1 1 1 1 1 3 2 2 1 2 2 1 1 3 3 2 2 1 1 1 1 2 2 1 1
2 1 1 1 2 2 1 1 1 1 1 1 2 2 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1
1 1 1 1 2 2 1 1 1 1 1 1 3 2 2 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1
2 2 1 1 3 3 2 2 2 2 1 1 3 3 2 2 4 3 3 3 1 1 1 1 2 2 1 1 1 1 1 1
2 2 1 1 2 1 1 1 1 1 1 1 3 2 2 2 3 3 2 2 2 2 1 1 1 1 1 1 1 1 1 1
1 1 1 1 3 2 1 2 1 1 1 1 2 2 1 1 2 2 1 1 1 1 1 1 2 1 1 1 1 1 1 1
1 1 1 1 1 1 1 1 1 1 1 1 2 2 1 1 3 2 2 1 2 1 1 1 1 1 1 1 1 1 1 1
3 3 2 2 3 3 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2 1 1 1 1 1 1
2 2 1 1 2 2 1 1 1 1 1 1 2 1 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 1 1 1 2 1 1 1 1 1 1 3 2 2 2 2 2 1 1 2 1 1 1 2 1 1 1 1 1 1 1
2 2 2 1 1 2 2 1 1 1 1 1 2 2 3 1 2 2 2 2 3 3 2 2 1 1 1 1 1 1 1 1
1 1 1 1 1 1 1 1 1 1 1 1 2 2 2 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 1 1 1 1 1 1 1 1 1 1 1 2 2 1 1 3 3 2 2 2 2 1 1 1 1 1 1 1 1 1 1
3 2 2 1 2 1 1 1 2 2 1 1 3 2 2 1 2 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1
2 2 2 1 2 2 2 1 1 1 1 1 2 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Master Chart (Control Group)
Sujective Parameters
Polyuria Polydipsia Polyphagia Tiredness Progressive weakness Dizziness Unexplained Wt loss
134 135
Pruritus
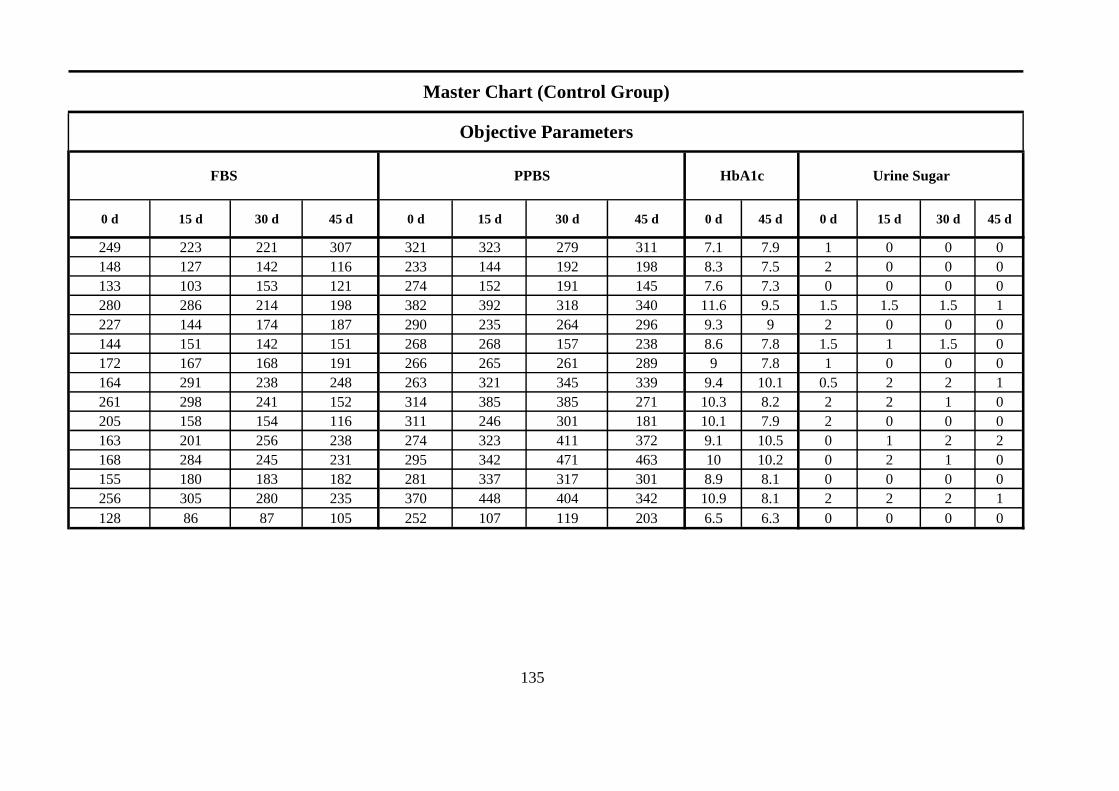
0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 45 d 0 d 15 d 30 d 45 d
249 223 221 307 321 323 279 311 7.1 7.9 1 0 0 0
148 127 142 116 233 144 192 198 8.3 7.5 2 0 0 0
133 103 153 121 274 152 191 145 7.6 7.3 0 0 0 0
280 286 214 198 382 392 318 340 11.6 9.5 1.5 1.5 1.5 1
227 144 174 187 290 235 264 296 9.3 9 2 0 0 0
144 151 142 151 268 268 157 238 8.6 7.8 1.5 1 1.5 0
172 167 168 191 266 265 261 289 9 7.8 1 0 0 0
164 291 238 248 263 321 345 339 9.4 10.1 0.5 2 2 1
261 298 241 152 314 385 385 271 10.3 8.2 2 2 1 0
205 158 154 116 311 246 301 181 10.1 7.9 2 0 0 0
163 201 256 238 274 323 411 372 9.1 10.5 0 1 2 2
168 284 245 231 295 342 471 463 10 10.2 0 2 1 0
155 180 183 182 281 337 317 301 8.9 8.1 0 0 0 0
256 305 280 235 370 448 404 342 10.9 8.1 2 2 2 1
128 86 87 105 252 107 119 203 6.5 6.3 0 0 0 0
Master Chart (Control Group)
Objective Parameters
135
PPBS HbA1c Urine SugarFBS
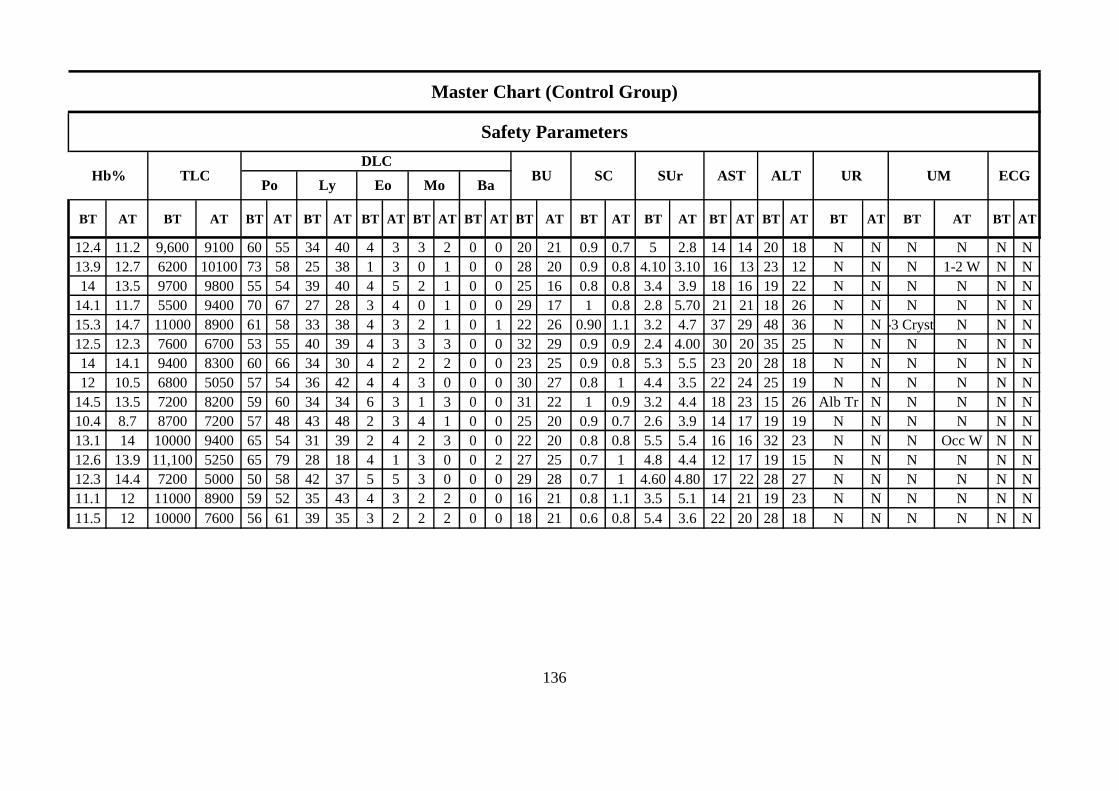
BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT
12.4 11.2 9,600 9100 60 55 34 40 4 3 3 2 0 0 20 21 0.9 0.7 5 2.8 14 14 20 18 N N N N N N
13.9 12.7 6200 10100 73 58 25 38 1 3 0 1 0 0 28 20 0.9 0.8 4.10 3.10 16 13 23 12 N N N 1-2 W N N
14 13.5 9700 9800 55 54 39 40 4 5 2 1 0 0 25 16 0.8 0.8 3.4 3.9 18 16 19 22 N N N N N N
14.1 11.7 5500 9400 70 67 27 28 3 4 0 1 0 0 29 17 1 0.8 2.8 5.70 21 21 18 26 N N N N N N
15.3 14.7 11000 8900 61 58 33 38 4 3 2 1 0 1 22 26 0.90 1.1 3.2 4.7 37 29 48 36 N N2-3 Crystal N N N
12.5 12.3 7600 6700 53 55 40 39 4 3 3 3 0 0 32 29 0.9 0.9 2.4 4.00 30 20 35 25 N N N N N N
14 14.1 9400 8300 60 66 34 30 4 2 2 2 0 0 23 25 0.9 0.8 5.3 5.5 23 20 28 18 N N N N N N
12 10.5 6800 5050 57 54 36 42 4 4 3 0 0 0 30 27 0.8 1 4.4 3.5 22 24 25 19 N N N N N N
14.5 13.5 7200 8200 59 60 34 34 6 3 1 3 0 0 31 22 1 0.9 3.2 4.4 18 23 15 26 Alb Tr N N N N N
10.4 8.7 8700 7200 57 48 43 48 2 3 4 1 0 0 25 20 0.9 0.7 2.6 3.9 14 17 19 19 N N N N N N
13.1 14 10000 9400 65 54 31 39 2 4 2 3 0 0 22 20 0.8 0.8 5.5 5.4 16 16 32 23 N N N Occ W N N
12.6 13.9 11,100 5250 65 79 28 18 4 1 3 0 0 2 27 25 0.7 1 4.8 4.4 12 17 19 15 N N N N N N
12.3 14.4 7200 5000 50 58 42 37 5 5 3 0 0 0 29 28 0.7 1 4.60 4.80 17 22 28 27 N N N N N N
11.1 12 11000 8900 59 52 35 43 4 3 2 2 0 0 16 21 0.8 1.1 3.5 5.1 14 21 19 23 N N N N N N
11.5 12 10000 7600 56 61 39 35 3 2 2 2 0 0 18 21 0.6 0.8 5.4 3.6 22 20 28 18 N N N N N N
Master Chart (Control Group)
AST ALT UR UM ECGHb% TLCDLC
BU SCPo Ly Ba
Safety Parameters
SUrEo Mo
136
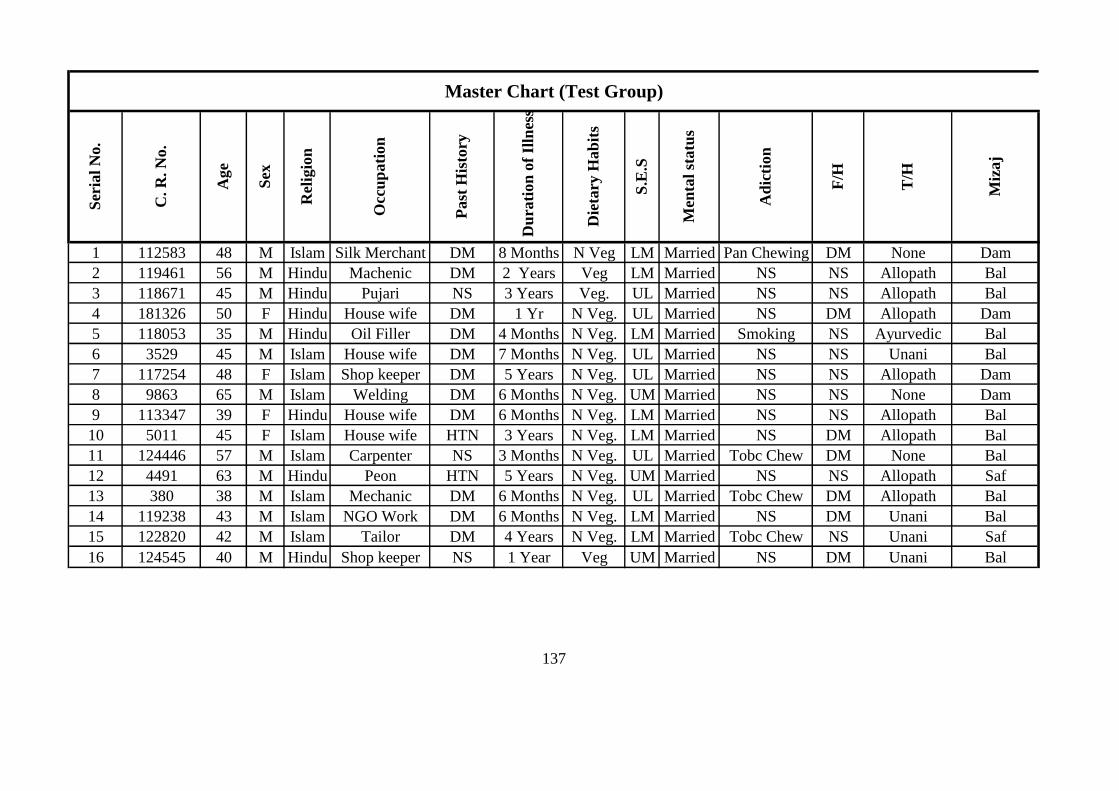
1 112583 48 M Islam Silk Merchant DM 8 Months N Veg LM Married Pan Chewing DM None Dam
2 119461 56 M Hindu Machenic DM 2 Years Veg LM Married NS NS Allopath Bal
3 118671 45 M Hindu Pujari NS 3 Years Veg. UL Married NS NS Allopath Bal
4 181326 50 F Hindu House wife DM 1 Yr N Veg. UL Married NS DM Allopath Dam
5 118053 35 M Hindu Oil Filler DM 4 Months N Veg. LM Married Smoking NS Ayurvedic Bal
6 3529 45 M Islam House wife DM 7 Months N Veg. UL Married NS NS Unani Bal
7 117254 48 F Islam Shop keeper DM 5 Years N Veg. UL Married NS NS Allopath Dam
8 9863 65 M Islam Welding DM 6 Months N Veg. UM Married NS NS None Dam
9 113347 39 F Hindu House wife DM 6 Months N Veg. LM Married NS NS Allopath Bal
10 5011 45 F Islam House wife HTN 3 Years N Veg. LM Married NS DM Allopath Bal
11 124446 57 M Islam Carpenter NS 3 Months N Veg. UL Married Tobc Chew DM None Bal
12 4491 63 M Hindu Peon HTN 5 Years N Veg. UM Married NS NS Allopath Saf
13 380 38 M Islam Mechanic DM 6 Months N Veg. UL Married Tobc Chew DM Allopath Bal
14 119238 43 M Islam NGO Work DM 6 Months N Veg. LM Married NS DM Unani Bal
15 122820 42 M Islam Tailor DM 4 Years N Veg. LM Married Tobc Chew NS Unani Saf
16 124545 40 M Hindu Shop keeper NS 1 Year Veg UM Married NS DM Unani Bal
137
Master Chart (Test Group)
Occ
up
ati
on
Past
His
tory
Die
tary
Hab
its
S.E
.S
Men
tal
statu
s
Ser
ial
No.
C. R
. N
o.
Age
Sex
Rel
igio
n
Miz
aj
Du
rati
on
of
Illn
ess
Ad
icti
on
F/H
T/H
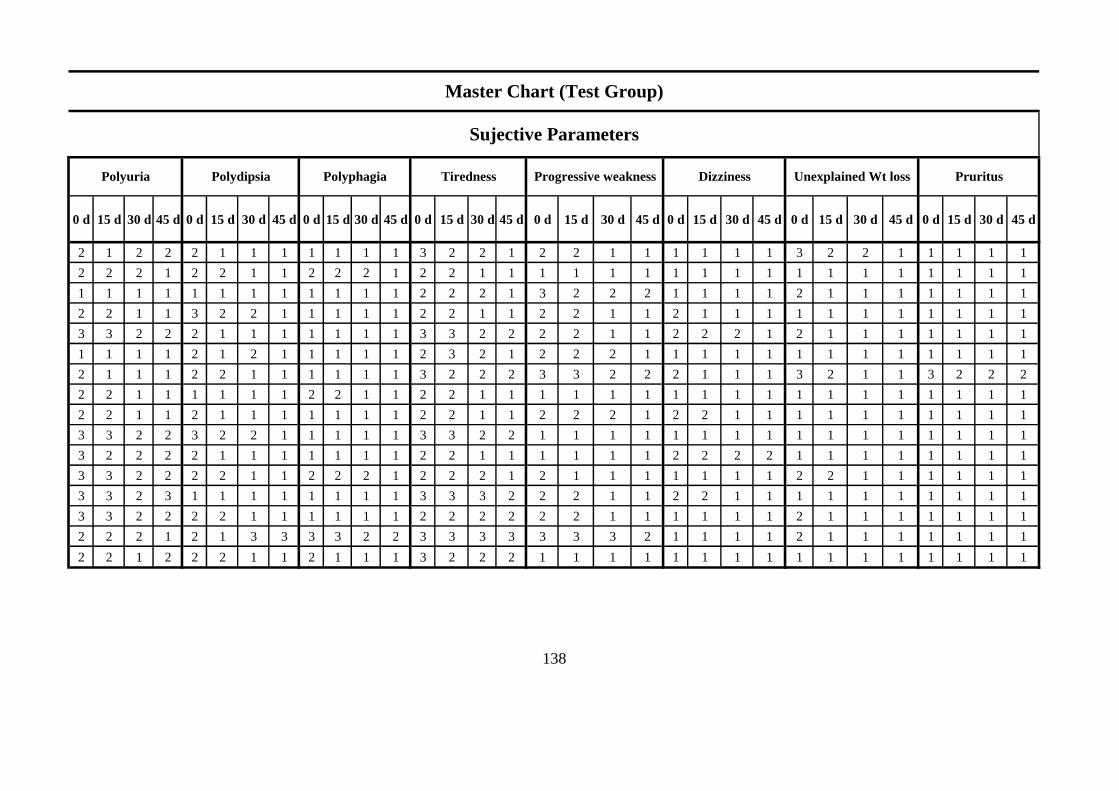
0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d
2 1 2 2 2 1 1 1 1 1 1 1 3 2 2 1 2 2 1 1 1 1 1 1 3 2 2 1 1 1 1 1
2 2 2 1 2 2 1 1 2 2 2 1 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 1 1 1 1 1 1 1 1 1 1 1 2 2 2 1 3 2 2 2 1 1 1 1 2 1 1 1 1 1 1 1
2 2 1 1 3 2 2 1 1 1 1 1 2 2 1 1 2 2 1 1 2 1 1 1 1 1 1 1 1 1 1 1
3 3 2 2 2 1 1 1 1 1 1 1 3 3 2 2 2 2 1 1 2 2 2 1 2 1 1 1 1 1 1 1
1 1 1 1 2 1 2 1 1 1 1 1 2 3 2 1 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1
2 1 1 1 2 2 1 1 1 1 1 1 3 2 2 2 3 3 2 2 2 1 1 1 3 2 1 1 3 2 2 2
2 2 1 1 1 1 1 1 2 2 1 1 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
2 2 1 1 2 1 1 1 1 1 1 1 2 2 1 1 2 2 2 1 2 2 1 1 1 1 1 1 1 1 1 1
3 3 2 2 3 2 2 1 1 1 1 1 3 3 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
3 2 2 2 2 1 1 1 1 1 1 1 2 2 1 1 1 1 1 1 2 2 2 2 1 1 1 1 1 1 1 1
3 3 2 2 2 2 1 1 2 2 2 1 2 2 2 1 2 1 1 1 1 1 1 1 2 2 1 1 1 1 1 1
3 3 2 3 1 1 1 1 1 1 1 1 3 3 3 2 2 2 1 1 2 2 1 1 1 1 1 1 1 1 1 1
3 3 2 2 2 2 1 1 1 1 1 1 2 2 2 2 2 2 1 1 1 1 1 1 2 1 1 1 1 1 1 1
2 2 2 1 2 1 3 3 3 3 2 2 3 3 3 3 3 3 3 2 1 1 1 1 2 1 1 1 1 1 1 1
2 2 1 2 2 2 1 1 2 1 1 1 3 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
138
Master Chart (Test Group)
Polyuria Polydipsia Polyphagia Tiredness Pruritus
Sujective Parameters
Progressive weakness Dizziness Unexplained Wt loss

0 d 15 d 30 d 45 d 0 d 15 d 30 d 45 d 0 d 45 d 0 d 15 d 30 d 45 d
228 180 179 136 283 261 238 197 10 7.3 2 1 2 1
191 141 117 140 283 195 168 243 9.3 8 0.5 0 0 0
187 370 157 198 389 442 305 394 9 9.3 0.5 2 0 0
191 160 147 179 263 202 193 277 8.3 8.5 1 0 0 0
191 149 192 180 288 186 210 253 7.1 6.5 1 0.5 1.5 0.5
172 183 175 180 347 265 247 296 10.2 9.1 0 0.5 0 0
183 284 169 166 311 396 259 265 8.8 8 1 2 0 0
209 175 164 187 290 245 253 296 8.1 9,2 0.5 0.2 0 0
176 128 145 133 200 226 180 242 8.3 7.8 0 0 0 0
141 122 130 125 229 199 243 204 9 8.6 0 0 0 0
127 113 114 113 242 205 212 153 7.2 6.7 0 0 0 0
153 151 163 224 232 263 242 315 9 9.9 0 0 0 0
173 199 158 205 237 305 281 301 10 9.4 0.5 0 0 0
151 136 148 150 245 220 220 210 8.3 7.9 0 0 0 0
342 360 326 360 490 430 437 430 10.6 10.1 2 2 2 1
166 208 117 115 180 269 246 192 7.9 6.7 2 1 1 1
139
Master Chart (Test Group)
HbA1c Urine SugarPPBSFBS
Objective Parameters
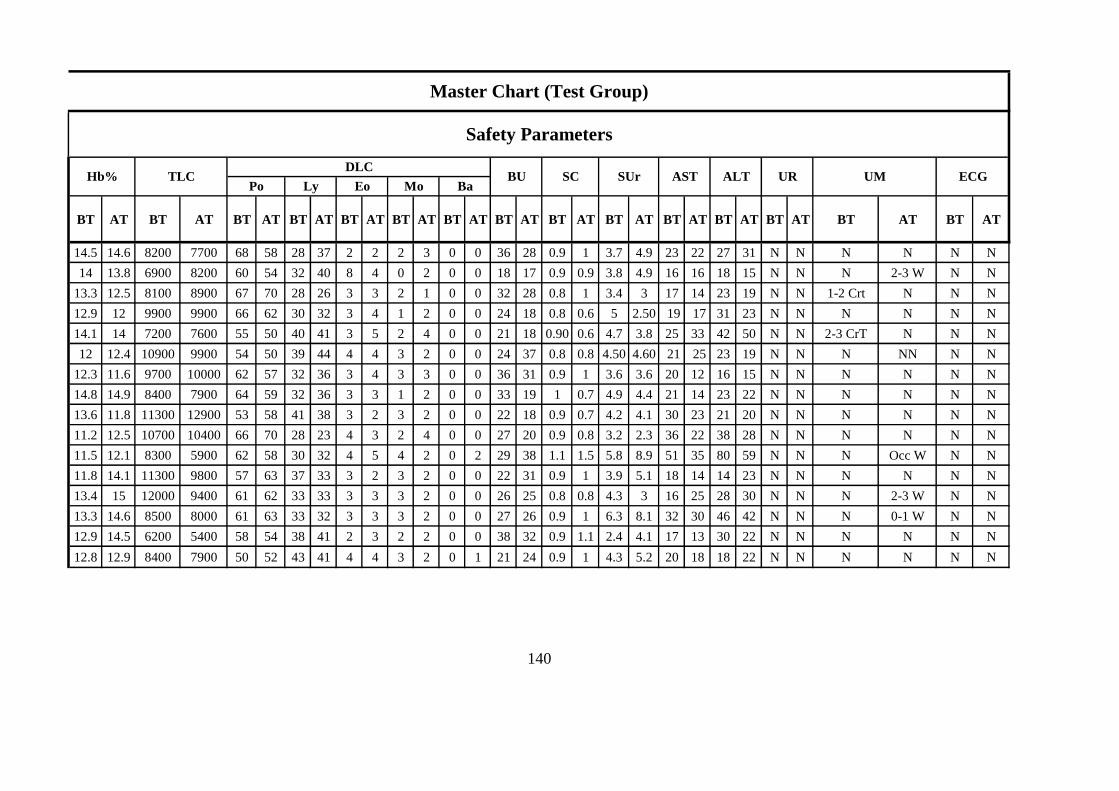
BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT
14.5 14.6 8200 7700 68 58 28 37 2 2 2 3 0 0 36 28 0.9 1 3.7 4.9 23 22 27 31 N N N N N N
14 13.8 6900 8200 60 54 32 40 8 4 0 2 0 0 18 17 0.9 0.9 3.8 4.9 16 16 18 15 N N N 2-3 W N N
13.3 12.5 8100 8900 67 70 28 26 3 3 2 1 0 0 32 28 0.8 1 3.4 3 17 14 23 19 N N 1-2 Crt N N N
12.9 12 9900 9900 66 62 30 32 3 4 1 2 0 0 24 18 0.8 0.6 5 2.50 19 17 31 23 N N N N N N
14.1 14 7200 7600 55 50 40 41 3 5 2 4 0 0 21 18 0.90 0.6 4.7 3.8 25 33 42 50 N N 2-3 CrT N N N
12 12.4 10900 9900 54 50 39 44 4 4 3 2 0 0 24 37 0.8 0.8 4.50 4.60 21 25 23 19 N N N NN N N
12.3 11.6 9700 10000 62 57 32 36 3 4 3 3 0 0 36 31 0.9 1 3.6 3.6 20 12 16 15 N N N N N N
14.8 14.9 8400 7900 64 59 32 36 3 3 1 2 0 0 33 19 1 0.7 4.9 4.4 21 14 23 22 N N N N N N
13.6 11.8 11300 12900 53 58 41 38 3 2 3 2 0 0 22 18 0.9 0.7 4.2 4.1 30 23 21 20 N N N N N N
11.2 12.5 10700 10400 66 70 28 23 4 3 2 4 0 0 27 20 0.9 0.8 3.2 2.3 36 22 38 28 N N N N N N
11.5 12.1 8300 5900 62 58 30 32 4 5 4 2 0 2 29 38 1.1 1.5 5.8 8.9 51 35 80 59 N N N Occ W N N
11.8 14.1 11300 9800 57 63 37 33 3 2 3 2 0 0 22 31 0.9 1 3.9 5.1 18 14 14 23 N N N N N N
13.4 15 12000 9400 61 62 33 33 3 3 3 2 0 0 26 25 0.8 0.8 4.3 3 16 25 28 30 N N N 2-3 W N N
13.3 14.6 8500 8000 61 63 33 32 3 3 3 2 0 0 27 26 0.9 1 6.3 8.1 32 30 46 42 N N N 0-1 W N N
12.9 14.5 6200 5400 58 54 38 41 2 3 2 2 0 0 38 32 0.9 1.1 2.4 4.1 17 13 30 22 N N N N N N
12.8 12.9 8400 7900 50 52 43 41 4 4 3 2 0 1 21 24 0.9 1 4.3 5.2 20 18 18 22 N N N N N N
140
Master Chart (Test Group)
ALT UR UM ECGPo Ly Eo Mo
Safety Parameters
Hb% SUr ASTTLC SCBa
DLCBU