clinical trials for quality of life endpoints in oncology oncology education session rochester,...
TRANSCRIPT

Clinical Trials Clinical Trials for Quality of Life Endpointsfor Quality of Life Endpoints
in Oncology in Oncology
Clinical Trials Clinical Trials for Quality of Life Endpointsfor Quality of Life Endpoints
in Oncology in Oncology
Oncology Education Session Oncology Education Session
Rochester, November 1, 2005Rochester, November 1, 2005
Oncology Education Session Oncology Education Session
Rochester, November 1, 2005Rochester, November 1, 2005
Jeff A. Sloan, Ph.D.Jeff A. Sloan, Ph.D.Mayo Clinic, Rochester, MN, USA

QOL challengesQOL challengesQOL challengesQOL challenges
• Reliability: if I were to use this tool under the Reliability: if I were to use this tool under the same conditions would I get the same results?same conditions would I get the same results?
• Validity: am I measuring what I want to measure?Validity: am I measuring what I want to measure?
• Missing data: imputation, design considerationsMissing data: imputation, design considerations
• Response shift: hospice patients at 75%Response shift: hospice patients at 75%
• Reliability: if I were to use this tool under the Reliability: if I were to use this tool under the same conditions would I get the same results?same conditions would I get the same results?
• Validity: am I measuring what I want to measure?Validity: am I measuring what I want to measure?
• Missing data: imputation, design considerationsMissing data: imputation, design considerations
• Response shift: hospice patients at 75%Response shift: hospice patients at 75%

Take home message:Take home message:there is good newsthere is good news
Take home message:Take home message:there is good newsthere is good news
• There are problems with using QOL There are problems with using QOL assessments as indicators of efficacy in assessments as indicators of efficacy in clinical trials.clinical trials.
• There are scientifically sound solutions to There are scientifically sound solutions to these problems. The problems have been these problems. The problems have been disseminated widely and consistently. The disseminated widely and consistently. The solutions have not.solutions have not.
• There are problems with using QOL There are problems with using QOL assessments as indicators of efficacy in assessments as indicators of efficacy in clinical trials.clinical trials.
• There are scientifically sound solutions to There are scientifically sound solutions to these problems. The problems have been these problems. The problems have been disseminated widely and consistently. The disseminated widely and consistently. The solutions have not.solutions have not.

Checklist for designing, conducting and reporting HRQL - Checklist for designing, conducting and reporting HRQL - PRO in clinical trialsPRO in clinical trials
Patient Reported Outcomes (PRO) and Regulatory Issues : A European Guidance Document for the improved integration Patient Reported Outcomes (PRO) and Regulatory Issues : A European Guidance Document for the improved integration of health-related quality of life assessment in the drug regulatory process. of health-related quality of life assessment in the drug regulatory process. Chassany O et Chassany O et ERIQAERIQA Working Group. Drug Working Group. Drug
Information Journal 2002.Information Journal 2002.
Checklist for designing, conducting and reporting HRQL - Checklist for designing, conducting and reporting HRQL - PRO in clinical trialsPRO in clinical trials
Patient Reported Outcomes (PRO) and Regulatory Issues : A European Guidance Document for the improved integration Patient Reported Outcomes (PRO) and Regulatory Issues : A European Guidance Document for the improved integration of health-related quality of life assessment in the drug regulatory process. of health-related quality of life assessment in the drug regulatory process. Chassany O et Chassany O et ERIQAERIQA Working Group. Drug Working Group. Drug
Information Journal 2002.Information Journal 2002.
HRQL / PRO objectives• Added value of HRQL / PRO• Choice of the questionnaires• Hypotheses of HRQL / PRO changes
Study design• Basic principles of RCT fulfilled ?• Timing and frequency of assessment• Mode and site of administration...
HRQL / PRO measure• Description of the measure (items, domains…)• Evidence of validity• Evidence of cultural adaptation
Statistical analysis plan• Primary or secondary endpoint • Superiority or equivalence trial• Sample size• ITT, type I error, missing data
Reporting of results• Participation rate, data completeness• Distribution of HRQL / PRO scores
Interpreting the results• Effect size, • Minimal Clinically Important Difference• Comparison with other criteria / scores• Number needed to treat…

EMEA RECOMMENDATIONS EMEA RECOMMENDATIONS Points to consider (Points to consider (CPMP/EWP/562/98CPMP/EWP/562/98) on clinical investigation of medicinal products in the chronic ) on clinical investigation of medicinal products in the chronic
treatment of patients with treatment of patients with COPDCOPD, 1999, 1999
EMEA RECOMMENDATIONS EMEA RECOMMENDATIONS Points to consider (Points to consider (CPMP/EWP/562/98CPMP/EWP/562/98) on clinical investigation of medicinal products in the chronic ) on clinical investigation of medicinal products in the chronic
treatment of patients with treatment of patients with COPDCOPD, 1999, 1999
• In the major efficacy studies of symptomatic benefit the primary endpoint In the major efficacy studies of symptomatic benefit the primary endpoint should reflect the clinical benefit the applicant wishes to claim in the should reflect the clinical benefit the applicant wishes to claim in the future SPC (Summary of Product Characteristics) future SPC (Summary of Product Characteristics)
• It should include the It should include the FEV1FEV1 as a measure of lung function and include a as a measure of lung function and include a measure of measure of symptomatic benefitsymptomatic benefit
• A significant benefit for A significant benefit for both endpointsboth endpoints, should be demonstrated so that , should be demonstrated so that no multiplicity adjustment to significance levels is indicatedno multiplicity adjustment to significance levels is indicated
• The primary symptomatic benefit endpointThe primary symptomatic benefit endpoint should be justified by referencing should be justified by referencing published data which supports its validity; one example is the published data which supports its validity; one example is the St George’s St George’s Respiratory QuestionnaireRespiratory Questionnaire
• There are number of There are number of secondary endpointssecondary endpoints which may provide useful which may provide useful information. information. … … e.g. symptom scales, … and e.g. symptom scales, … and quality of life assessmentquality of life assessment
• In the major efficacy studies of symptomatic benefit the primary endpoint In the major efficacy studies of symptomatic benefit the primary endpoint should reflect the clinical benefit the applicant wishes to claim in the should reflect the clinical benefit the applicant wishes to claim in the future SPC (Summary of Product Characteristics) future SPC (Summary of Product Characteristics)
• It should include the It should include the FEV1FEV1 as a measure of lung function and include a as a measure of lung function and include a measure of measure of symptomatic benefitsymptomatic benefit
• A significant benefit for A significant benefit for both endpointsboth endpoints, should be demonstrated so that , should be demonstrated so that no multiplicity adjustment to significance levels is indicatedno multiplicity adjustment to significance levels is indicated
• The primary symptomatic benefit endpointThe primary symptomatic benefit endpoint should be justified by referencing should be justified by referencing published data which supports its validity; one example is the published data which supports its validity; one example is the St George’s St George’s Respiratory QuestionnaireRespiratory Questionnaire
• There are number of There are number of secondary endpointssecondary endpoints which may provide useful which may provide useful information. information. … … e.g. symptom scales, … and e.g. symptom scales, … and quality of life assessmentquality of life assessment

NHRQOL
Health Status(HS)
Activities ofDaily Living
(ADL)
Symptoms/Toxicity
SocialSpiritualPhysical
EmotionalIntellectual
QOL is not Survival or Treatment Response
HRQOL
Q O L
QOL: The big pictureQOL: The big picture

Symptoms and QOL:Symptoms and QOL:Is there a difference?Is there a difference?Symptoms and QOL:Symptoms and QOL:Is there a difference?Is there a difference?
• If you count the number of emetic episodes, If you count the number of emetic episodes, you are assessing a symptomyou are assessing a symptom
• If you ask the patient how bad their nausea If you ask the patient how bad their nausea is, you are assessing QOLis, you are assessing QOL
• The measurement issues and analytical The measurement issues and analytical procedures are the sameprocedures are the same
• Literature is converging to the term patient-Literature is converging to the term patient-reported outcomes (PRO)reported outcomes (PRO)
• If you count the number of emetic episodes, If you count the number of emetic episodes, you are assessing a symptomyou are assessing a symptom
• If you ask the patient how bad their nausea If you ask the patient how bad their nausea is, you are assessing QOLis, you are assessing QOL
• The measurement issues and analytical The measurement issues and analytical procedures are the sameprocedures are the same
• Literature is converging to the term patient-Literature is converging to the term patient-reported outcomes (PRO)reported outcomes (PRO)

Developmental Timeline of Commonly Developmental Timeline of Commonly Used QOL Measurement ToolsUsed QOL Measurement Tools
Developmental Timeline of Commonly Developmental Timeline of Commonly Used QOL Measurement ToolsUsed QOL Measurement Tools
Uni-scale
SF-36
EORTCQLQ-C30
BPIPOMS
COOP/WONCA EQ5D BFI
'67 '78 '85 '86 '87 '88 '89 '91 '92 '94 '95 '98 '99 '00
SDS FLIC FACT&
CARES
ESAS SF-12 MDASI SF-8

What is an What is an Appropriate QOL Instrument?Appropriate QOL Instrument?
What is an What is an Appropriate QOL Instrument?Appropriate QOL Instrument?
• Research objective (HYPOTHESIS DRIVEN)Research objective (HYPOTHESIS DRIVEN)
• Specific rationale for the QOL part of the studySpecific rationale for the QOL part of the study
• Relevant domains of QOL (LIST & MATCH)Relevant domains of QOL (LIST & MATCH)
• Disease and patient population characteristicsDisease and patient population characteristics
• Psychometric characteristics (reliability & Psychometric characteristics (reliability & validity) of QOL instrumentvalidity) of QOL instrument
• Practical considerations (e.g. respondentPractical considerations (e.g. respondent burden, burden, language translations)language translations)
• Research objective (HYPOTHESIS DRIVEN)Research objective (HYPOTHESIS DRIVEN)
• Specific rationale for the QOL part of the studySpecific rationale for the QOL part of the study
• Relevant domains of QOL (LIST & MATCH)Relevant domains of QOL (LIST & MATCH)
• Disease and patient population characteristicsDisease and patient population characteristics
• Psychometric characteristics (reliability & Psychometric characteristics (reliability & validity) of QOL instrumentvalidity) of QOL instrument
• Practical considerations (e.g. respondentPractical considerations (e.g. respondent burden, burden, language translations)language translations)

Timing of QOL AssessmentTiming of QOL AssessmentTiming of QOL AssessmentTiming of QOL Assessment
• Study objectiveStudy objective
• Characteristics and natural course of Characteristics and natural course of disease disease
• Baseline and one follow-up QOL Baseline and one follow-up QOL assessment are necessaryassessment are necessary
• Treatment regimen Treatment regimen • Similar timing of QOL assessment Similar timing of QOL assessment
across treatment armsacross treatment arms
• Expected effects of the treatmentExpected effects of the treatment
• Study objectiveStudy objective
• Characteristics and natural course of Characteristics and natural course of disease disease
• Baseline and one follow-up QOL Baseline and one follow-up QOL assessment are necessaryassessment are necessary
• Treatment regimen Treatment regimen • Similar timing of QOL assessment Similar timing of QOL assessment
across treatment armsacross treatment arms
• Expected effects of the treatmentExpected effects of the treatment

QOL Research ThemesQOL Research ThemesQOL Research ThemesQOL Research Themes
1. Assess QOL within clinical trials 1. Assess QOL within clinical trials with efficiency, consistency, with efficiency, consistency, specificityspecificity
2. Improve QOL methodology2. Improve QOL methodology
3. Develop intervention studies 3. Develop intervention studies targeted at QOL endpointstargeted at QOL endpoints
1. Assess QOL within clinical trials 1. Assess QOL within clinical trials with efficiency, consistency, with efficiency, consistency, specificityspecificity
2. Improve QOL methodology2. Improve QOL methodology
3. Develop intervention studies 3. Develop intervention studies targeted at QOL endpointstargeted at QOL endpoints

QOL in NCCTG Clinical TrialsQOL in NCCTG Clinical TrialsQOL in NCCTG Clinical TrialsQOL in NCCTG Clinical Trials
• Since 1995, 84 trials with QOL componentSince 1995, 84 trials with QOL component
• >50 different QOL questionnaires used>50 different QOL questionnaires used
• >20 papers per year published with QOL>20 papers per year published with QOL
• Average baseline compliance rate: 94%Average baseline compliance rate: 94%
• Since 1995, 84 trials with QOL componentSince 1995, 84 trials with QOL component
• >50 different QOL questionnaires used>50 different QOL questionnaires used
• >20 papers per year published with QOL>20 papers per year published with QOL
• Average baseline compliance rate: 94%Average baseline compliance rate: 94%

What underlies these QOL metrics?What underlies these QOL metrics?What underlies these QOL metrics?What underlies these QOL metrics?
• ““NCCTG does not experience the problems NCCTG does not experience the problems that other groups report with respect to that other groups report with respect to QOL”.QOL”.
• ““Efforts to make the inclusion of QOL Efforts to make the inclusion of QOL components in treatment trials easy and components in treatment trials easy and efficient have been well received by efficient have been well received by investigators”. investigators”. (Integrating cancer control research into the CCOP (Integrating cancer control research into the CCOP network: a case study of the NCCTG, NCI, 2004)network: a case study of the NCCTG, NCI, 2004)
• ““NCCTG does not experience the problems NCCTG does not experience the problems that other groups report with respect to that other groups report with respect to QOL”.QOL”.
• ““Efforts to make the inclusion of QOL Efforts to make the inclusion of QOL components in treatment trials easy and components in treatment trials easy and efficient have been well received by efficient have been well received by investigators”. investigators”. (Integrating cancer control research into the CCOP (Integrating cancer control research into the CCOP network: a case study of the NCCTG, NCI, 2004)network: a case study of the NCCTG, NCI, 2004)

QOL Team ResourcesQOL Team ResourcesQOL Team ResourcesQOL Team Resources
• MD tumor group liaisonsMD tumor group liaisons
• Operations manualOperations manual
• Forms bankForms bank
• Literature bankLiterature bank
• Background templatesBackground templates
• Web-based utilitiesWeb-based utilities
• MD tumor group liaisonsMD tumor group liaisons
• Operations manualOperations manual
• Forms bankForms bank
• Literature bankLiterature bank
• Background templatesBackground templates
• Web-based utilitiesWeb-based utilities

Cancer Patient AssessmentCancer Patient AssessmentCancer Patient AssessmentCancer Patient Assessment
• Cancer patient assessment involves Cancer patient assessment involves tumor growth and survival data.tumor growth and survival data.
• We measure these scientifically and the We measure these scientifically and the effect of interventions on these effect of interventions on these endpoints.endpoints.
• Cancer also involves other things Cancer also involves other things besides tumors and reduced lifespan that besides tumors and reduced lifespan that can be measured…..can be measured…..
• Cancer patient assessment involves Cancer patient assessment involves tumor growth and survival data.tumor growth and survival data.
• We measure these scientifically and the We measure these scientifically and the effect of interventions on these effect of interventions on these endpoints.endpoints.
• Cancer also involves other things Cancer also involves other things besides tumors and reduced lifespan that besides tumors and reduced lifespan that can be measured…..can be measured…..

… … by answering scientific questionsby answering scientific questions… … by answering scientific questionsby answering scientific questions
• What is the value added of loooooong QOL What is the value added of loooooong QOL assessments to treatment trials?assessments to treatment trials?
• What is the evidence for the use of single-item What is the evidence for the use of single-item QOL assessments?QOL assessments?
• How do you deal with multiple endpoints?How do you deal with multiple endpoints?
• How do you handle missing data? How do you handle missing data?
• What is the clinical significance of QOL What is the clinical significance of QOL assessments?assessments?
• What is the value added of loooooong QOL What is the value added of loooooong QOL assessments to treatment trials?assessments to treatment trials?
• What is the evidence for the use of single-item What is the evidence for the use of single-item QOL assessments?QOL assessments?
• How do you deal with multiple endpoints?How do you deal with multiple endpoints?
• How do you handle missing data? How do you handle missing data?
• What is the clinical significance of QOL What is the clinical significance of QOL assessments?assessments?

What is the value added What is the value added of additional questions?of additional questions?

Less is MoreLess is MoreLess is MoreLess is More
• Numerous studies indicate shorter assessments are “just Numerous studies indicate shorter assessments are “just as good” as longer assessmentsas good” as longer assessments
• Bernhard. single item quality of life indicators in cancer clinical Bernhard. single item quality of life indicators in cancer clinical trials. Brit J Cancer 84(9)1156-1165, 2002trials. Brit J Cancer 84(9)1156-1165, 2002
• Vickers. Contolled Clinical Trials, 24: 731 – 735, 2003 Vickers. Contolled Clinical Trials, 24: 731 – 735, 2003
• Abdel-Khalek. Measuring anxiety. Death Studies 22(8):763-772, Abdel-Khalek. Measuring anxiety. Death Studies 22(8):763-772, 1998 1998
• Gardner. Ed Psych Measurement 58(6):898-915, 1998 Gardner. Ed Psych Measurement 58(6):898-915, 1998
• Sloan. Overall QOL. JCO 16:3662-3673, 1998Sloan. Overall QOL. JCO 16:3662-3673, 1998
• Sloan. Clinical significance of single items relative to summated Sloan. Clinical significance of single items relative to summated scores. Mayo Clinic Proc 77: 479-487, 2002 scores. Mayo Clinic Proc 77: 479-487, 2002
• Numerous studies indicate shorter assessments are “just Numerous studies indicate shorter assessments are “just as good” as longer assessmentsas good” as longer assessments
• Bernhard. single item quality of life indicators in cancer clinical Bernhard. single item quality of life indicators in cancer clinical trials. Brit J Cancer 84(9)1156-1165, 2002trials. Brit J Cancer 84(9)1156-1165, 2002
• Vickers. Contolled Clinical Trials, 24: 731 – 735, 2003 Vickers. Contolled Clinical Trials, 24: 731 – 735, 2003
• Abdel-Khalek. Measuring anxiety. Death Studies 22(8):763-772, Abdel-Khalek. Measuring anxiety. Death Studies 22(8):763-772, 1998 1998
• Gardner. Ed Psych Measurement 58(6):898-915, 1998 Gardner. Ed Psych Measurement 58(6):898-915, 1998
• Sloan. Overall QOL. JCO 16:3662-3673, 1998Sloan. Overall QOL. JCO 16:3662-3673, 1998
• Sloan. Clinical significance of single items relative to summated Sloan. Clinical significance of single items relative to summated scores. Mayo Clinic Proc 77: 479-487, 2002 scores. Mayo Clinic Proc 77: 479-487, 2002

Sloan et al, Biopharm Stat 14(1): 73-96, 2004.

Situations where a single item maysuffice
Situations where a multi-item indexmay be needed
Phase II study attempting to assesswhether a treatment has any impact onQOL
A Phase III study where it is known thatQOL is impacted and more delineationof which QOL components are affectedis needed
A stratification factor for the presenceor absence of depressive issues
A screen to identify the presence orabsence of clinical depression
Need to assess fatigue/pain as acorrelate of toxicity (brief fatigue/paininventory)
Need to assess the impact offatigue/pain on the activities of dailyliving (ADL items for pain/fatigue)
Identifying patients who have need offurther QOL assessment (e.g., score of6 or less on a single item)
Detailing the QOL-related issues oncea cut off score on a single item hasbeen obtained
A clinical setting wherein a basic ideaof which domains of QOL (mental,physical, social) may be affected by aparticular treatment or situation
A clinical setting wherein preciseindications of the way in which thedifferent domains of QOL may beaffected by a particular treatment orsituation
Single-Item or Multiple-Item PRO?Single-Item or Multiple-Item PRO?
Sloan et al, Mayo Clinic Proc 77: 479-487, 2002.

A Comparison of Simple Single-Item Measures and the Common Toxicity Criteria in Detecting the Onset of Oxaliplatin-Induced
Peripheral Neuropathy in Patients with Colorectal Cancer
R. F. Morton, J. A. Sloan, A. Grothey, D. J. Sargent, H. McLeod, E. M. Green, C. Fuchs, R. K. Ramanathan,
S. K. Williamson, R. M. Goldberg
ASCO 2005

• Peripheral neuropathy (PN) is common during treatment Peripheral neuropathy (PN) is common during treatment with Oxaliplatinwith Oxaliplatin
• Assessment of PN is historically done via the Common Assessment of PN is historically done via the Common Toxicity Criteria (CTC)Toxicity Criteria (CTC)
• We developed a single-item numerical analogue scale We developed a single-item numerical analogue scale assessment to help measure PNassessment to help measure PN
• We compared the two measures to look at the sensitivity of We compared the two measures to look at the sensitivity of the CTC in detecting the onset of PNthe CTC in detecting the onset of PN
• Peripheral neuropathy (PN) is common during treatment Peripheral neuropathy (PN) is common during treatment with Oxaliplatinwith Oxaliplatin
• Assessment of PN is historically done via the Common Assessment of PN is historically done via the Common Toxicity Criteria (CTC)Toxicity Criteria (CTC)
• We developed a single-item numerical analogue scale We developed a single-item numerical analogue scale assessment to help measure PNassessment to help measure PN
• We compared the two measures to look at the sensitivity of We compared the two measures to look at the sensitivity of the CTC in detecting the onset of PNthe CTC in detecting the onset of PN
Background

• 696 patients randomized to FOLFOX4696 patients randomized to FOLFOX4
• PN assessed bi-weekly during treatmentPN assessed bi-weekly during treatment
• NAS filled out at baseline and every 12 weeks NAS filled out at baseline and every 12 weeks during treatmentduring treatment
• 696 patients randomized to FOLFOX4696 patients randomized to FOLFOX4
• PN assessed bi-weekly during treatmentPN assessed bi-weekly during treatment
• NAS filled out at baseline and every 12 weeks NAS filled out at baseline and every 12 weeks during treatmentduring treatment
Methods

IFL:Irinotecan +
5-FU/LV
IFL:Irinotecan +
5-FU/LV
IROX: Irinotecan IROX: Irinotecan + Oxaliplatin+ Oxaliplatin
IROX: Irinotecan IROX: Irinotecan + Oxaliplatin+ Oxaliplatin
FOLFOX4: FOLFOX4: Oxaliplatin + Oxaliplatin +
5-FU/LV5-FU/LV
FOLFOX4: FOLFOX4: Oxaliplatin + Oxaliplatin +
5-FU/LV5-FU/LV
RRAANNDDOOMMIIZZAATTIIOONN
RRAANNDDOOMMIIZZAATTIIOONN
Goldberg et al, JCO 2004
NCCTG/Intergroup Trial N9741

NAS Tools

• According to CTC only 20% of patients According to CTC only 20% of patients experienced serious PNexperienced serious PN
• Clinical knowledge suggested the incidence Clinical knowledge suggested the incidence rate should be much higher (about 80%)rate should be much higher (about 80%)
• According to CTC only 20% of patients According to CTC only 20% of patients experienced serious PNexperienced serious PN
• Clinical knowledge suggested the incidence Clinical knowledge suggested the incidence rate should be much higher (about 80%)rate should be much higher (about 80%)
An Empirical Anomaly

2 Point Change in 2 Point Change in QOLQOL
NoNo
(N=420)(N=420)
YesYes
(N=276)(N=276)
% Agreement% Agreement Kappa Kappa StatisticStatistic
Grade 2+ Grade 2+ PNPN
No (N=440)No (N=440) 308308 132132 65%65% 0.250.25
YesYes
(N=256)(N=256)
112112 144144
Grade 3+ Grade 3+ PNPN
NoNo
(N=597)(N=597)
380380 217217 63%63% 0.130.13
YesYes
(N=99)(N=99)
4040 5959
The agreement of < 65% indicates CTC and NAS measure different aspects of PN.
Agreement

Dose to PN: CTC versus NASWhich Comes First?
Median dose to NAS CSD of 424 mg/m2 versus Median dose to NAS CSD of 424 mg/m2 versus 765 ( 961) mg/m2 765 ( 961) mg/m2 for CTC grade 2+ (3+) eventfor CTC grade 2+ (3+) event

Time to PN: CTC versus NASWhich Comes First?
Patients notice an increase in PN two or three months earlier via the NASPatients notice an increase in PN two or three months earlier via the NAS

• Grade 2+ PN is found to be a significant Grade 2+ PN is found to be a significant problem according to the NASproblem according to the NAS
• Using CTC, PN is under-reportedUsing CTC, PN is under-reported
• NAS may allow for earlier detectionNAS may allow for earlier detection
• NAS should be used in conjunction with NAS should be used in conjunction with CTCCTC
• Grade 2+ PN is found to be a significant Grade 2+ PN is found to be a significant problem according to the NASproblem according to the NAS
• Using CTC, PN is under-reportedUsing CTC, PN is under-reported
• NAS may allow for earlier detectionNAS may allow for earlier detection
• NAS should be used in conjunction with NAS should be used in conjunction with CTCCTC
Conclusions

Are the occurrence of adverse events Are the occurrence of adverse events and clinically significant changes in and clinically significant changes in
symptom specific and global quality of symptom specific and global quality of life measures predictable?life measures predictable?
Are the occurrence of adverse events Are the occurrence of adverse events and clinically significant changes in and clinically significant changes in
symptom specific and global quality of symptom specific and global quality of life measures predictable?life measures predictable?
Sumithra J. Mandrekar, Ph.D.Sumithra J. Mandrekar, Ph.D.
Mashele M. Huschka, B.S.Mashele M. Huschka, B.S.
James R. Jett, M.D.James R. Jett, M.D.
Jeff A. Sloan, Ph.D.Jeff A. Sloan, Ph.D.
Mayo ClinicMayo Clinic
Rochester, MNRochester, MN
Sumithra J. Mandrekar, Ph.D.Sumithra J. Mandrekar, Ph.D.
Mashele M. Huschka, B.S.Mashele M. Huschka, B.S.
James R. Jett, M.D.James R. Jett, M.D.
Jeff A. Sloan, Ph.D.Jeff A. Sloan, Ph.D.
Mayo ClinicMayo Clinic
Rochester, MNRochester, MN

NCCTG Lung Cancer Trials NCCTG Lung Cancer Trials NCCTG Lung Cancer Trials NCCTG Lung Cancer Trials
Study Number
Description Sample Size Assessments Assessment Schedule
95-20-53A Pilot Study of High-Dose Thoracic Radiation Therapy w/ Concomitant Cisplatin/Etoposide in Limited-Stage SCLC
76Uniscale
LCSS
Baseline, prior to irradiation, prior to last cycle and at 3 months, 1 year & 2 year follow-up visits
95-24-52A Phase II Trial of Edatrexate in Combo w/ Vinblastine, Adriamycin, Cisplatin & Filgrastim in Pts w/ Advanced NSCLC
34Uniscale
FACT-L v3
Baseline and prior to each treatment cycle
97-24-51Phase III Randomized, Double-Blind Study of CAI & Placebo w/ Advanced NSCLC
177Uniscale FACT-L v4
Baseline and monthly during course of treatment
98-24-52Randomized Phase II Study of Docetaxel & Gemcitabine for Stage IIIB/IV NSCLC
99Uniscale
LCCSBaseline and prior to each treatment cycle
N0021Phase II Study of Gemcitabine and Epirubicin for the Treatment of Mesothelioma
68Uniscale
SDSBaseline, at each evaluation and 3 months & 1 year follow-up visits
N0022
Oral Vinorelbine For the Treatment of Metastatic Non-Small Cell Lung Cancer in Patients >= 65 Years of Age: A Phase II Trial of Efficacy, Toxicity, and Patients' Perceived Preference for Oral Therapy
58Uniscale
LCSS
Baseline and immediately after completion of second cycle of chemotherapy

QOL AssessmentsQOL AssessmentsQOL AssessmentsQOL Assessments
• Spitzer’s UniscaleSpitzer’s Uniscale
• 1 question for the global assessment of QOL1 question for the global assessment of QOL
• Functional Assessment of Cancer Therapy Lung (FACT-L)Functional Assessment of Cancer Therapy Lung (FACT-L)
• 27 questions divided into 4 well-being constructs: physical, 27 questions divided into 4 well-being constructs: physical, social/family, emotional, and functional social/family, emotional, and functional
• 10 questions specific to lung cancer 10 questions specific to lung cancer
• Lung Cancer Symptom Scale (LCSS)Lung Cancer Symptom Scale (LCSS)
• 9 questions pertaining to lung cancer symptoms9 questions pertaining to lung cancer symptoms
• Symptom Distress Scale (SDS)Symptom Distress Scale (SDS)
• 12 questions related to symptoms commonly experienced by 12 questions related to symptoms commonly experienced by cancer patientscancer patients
• Spitzer’s UniscaleSpitzer’s Uniscale
• 1 question for the global assessment of QOL1 question for the global assessment of QOL
• Functional Assessment of Cancer Therapy Lung (FACT-L)Functional Assessment of Cancer Therapy Lung (FACT-L)
• 27 questions divided into 4 well-being constructs: physical, 27 questions divided into 4 well-being constructs: physical, social/family, emotional, and functional social/family, emotional, and functional
• 10 questions specific to lung cancer 10 questions specific to lung cancer
• Lung Cancer Symptom Scale (LCSS)Lung Cancer Symptom Scale (LCSS)
• 9 questions pertaining to lung cancer symptoms9 questions pertaining to lung cancer symptoms
• Symptom Distress Scale (SDS)Symptom Distress Scale (SDS)
• 12 questions related to symptoms commonly experienced by 12 questions related to symptoms commonly experienced by cancer patientscancer patients

Determine the relationship of a single-item assessment with the multiple-item summated scales
Determine the relationship of a single-item assessment with the multiple-item summated scales
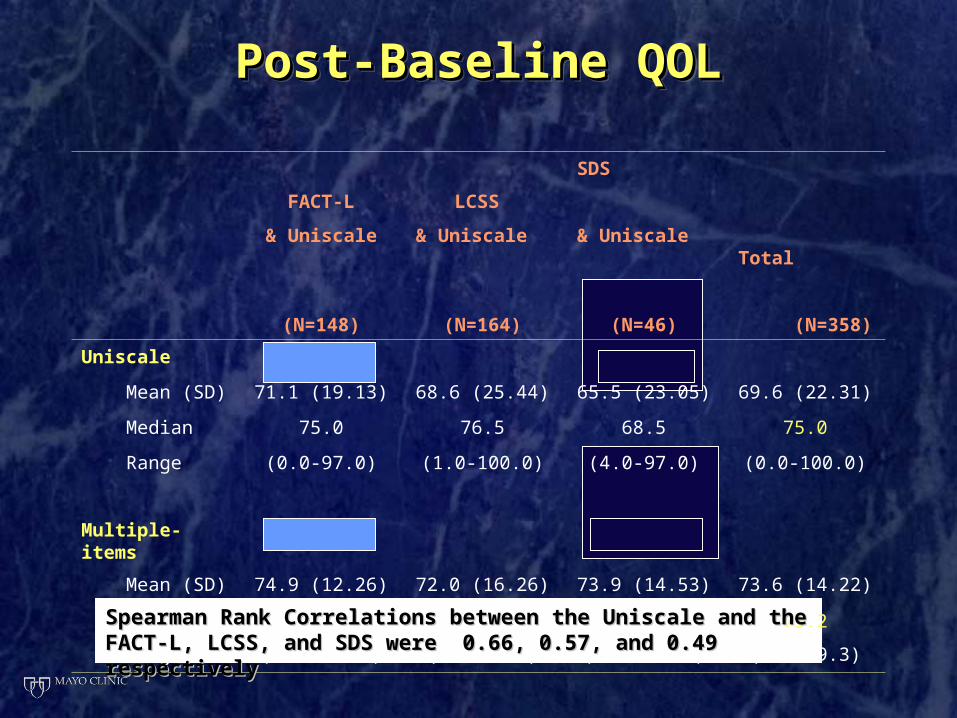
Post-Baseline QOLPost-Baseline QOLPost-Baseline QOLPost-Baseline QOL
FACT-L
& Uniscale
(N=148)
LCSS
& Uniscale
(N=164)
SDS & Uniscale
(N=46)
Total (N=358)
Uniscale
Mean (SD) 71.1 (19.13) 68.6 (25.44) 65.5 (23.05) 69.6 (22.31)
Median 75.0 76.5 68.5 75.0
Range (0.0-97.0) (1.0-100.0) (4.0-97.0) (0.0-100.0)
Multiple-items
Mean (SD) 74.9 (12.26) 72.0 (16.26) 73.9 (14.53) 73.6 (14.22)
Median 75.7 74.0 77.9 75.2
Range (30.7-99.3) (0.0-99.3) (38.5-96.2) (0.0-99.3)
Spearman Rank Correlations between the Uniscale and the FACT-L, Spearman Rank Correlations between the Uniscale and the FACT-L, LCSS, and SDS were 0.66, 0.57, and 0.49 respectivelyLCSS, and SDS were 0.66, 0.57, and 0.49 respectively

Correlation=0.43Correlation=0.43
When QOL is high: Uniscale > LCSSWhen QOL is high: Uniscale > LCSSWhen QOL is low: Uniscale < LCSSWhen QOL is low: Uniscale < LCSS Greater variability in Uniscale Scores Greater variability in Uniscale Scores

Determine if clinically significant declines are more readily detected by a single-item or multiple-item
assessment
Determine if clinically significant declines are more readily detected by a single-item or multiple-item
assessment

Individual Patient Data over time; Greater variability in Uniscale Scores Individual Patient Data over time; Greater variability in Uniscale Scores

Clinically Significant Decline (CSD) Clinically Significant Decline (CSD) [[10-point decline on a 0-100 scale]10-point decline on a 0-100 scale]
Clinically Significant Decline (CSD) Clinically Significant Decline (CSD) [[10-point decline on a 0-100 scale]10-point decline on a 0-100 scale]
FACT-L
& Uniscale
(N=120)*
LCSS
& Uniscale
(N=152)*
SDS & Uniscale
(N=45)*
Total (N=317)*
Uniscale
n (%) 73 (60.8%) 91 (59.9%) 20 (44.4%) 184 (58.0%)
Multiple-items
n (%) 46 (38.3%) 66 (43.4%) 13 (28.9%) 125 (39.4%)
Percent Agreement 56% 59% 71% 59%
*Represents the number of patients that completed the Uniscale at baseline and at least once post-baseline and completed a multiple-item assessment at baseline and at least once post-baseline
Uniscale more likely to detect a CSD in QOL than the multiple-item Uniscale more likely to detect a CSD in QOL than the multiple-item assessments (58% vs. 39%)assessments (58% vs. 39%)
The overall percent agreement in detecting a CSD in QOL between The overall percent agreement in detecting a CSD in QOL between Uniscale and multiple-item assessments was 59%Uniscale and multiple-item assessments was 59%

Determine how single-item Determine how single-item assessment and multiple-item assessment and multiple-item
summated scales relate to adverse summated scales relate to adverse events dataevents data
Determine how single-item Determine how single-item assessment and multiple-item assessment and multiple-item
summated scales relate to adverse summated scales relate to adverse events dataevents data

Adverse Events (AE)Adverse Events (AE)Adverse Events (AE)Adverse Events (AE)
• Severe adverse eventSevere adverse event is defined as a grade 3, 4, or 5, regardless of is defined as a grade 3, 4, or 5, regardless of attribution attribution
• 33% experienced a severe AE post baseline33% experienced a severe AE post baseline
• Nine AEsNine AEs experienced by at least 2% of the population that can experienced by at least 2% of the population that can also be collected via a QOL instrument also be collected via a QOL instrument
• Alopecia, Anorexia, Constipation, Diarrhea, Dyspnea, Fatigue, Alopecia, Anorexia, Constipation, Diarrhea, Dyspnea, Fatigue, Nausea, Neurosensory, VomitingNausea, Neurosensory, Vomiting
• 95% experienced at least one of the nine AEs95% experienced at least one of the nine AEs
• 20% had at least one of the nine graded as severe20% had at least one of the nine graded as severe
• CSD in AECSD in AE is defined as a baseline AE of grade 0, 1, or 2 that is defined as a baseline AE of grade 0, 1, or 2 that changes to a grade 3, 4, or 5 post baselinechanges to a grade 3, 4, or 5 post baseline
• Severe adverse eventSevere adverse event is defined as a grade 3, 4, or 5, regardless of is defined as a grade 3, 4, or 5, regardless of attribution attribution
• 33% experienced a severe AE post baseline33% experienced a severe AE post baseline
• Nine AEsNine AEs experienced by at least 2% of the population that can experienced by at least 2% of the population that can also be collected via a QOL instrument also be collected via a QOL instrument
• Alopecia, Anorexia, Constipation, Diarrhea, Dyspnea, Fatigue, Alopecia, Anorexia, Constipation, Diarrhea, Dyspnea, Fatigue, Nausea, Neurosensory, VomitingNausea, Neurosensory, Vomiting
• 95% experienced at least one of the nine AEs95% experienced at least one of the nine AEs
• 20% had at least one of the nine graded as severe20% had at least one of the nine graded as severe
• CSD in AECSD in AE is defined as a baseline AE of grade 0, 1, or 2 that is defined as a baseline AE of grade 0, 1, or 2 that changes to a grade 3, 4, or 5 post baselinechanges to a grade 3, 4, or 5 post baseline

Severe AE and CSD in QOLSevere AE and CSD in QOLSevere AE and CSD in QOLSevere AE and CSD in QOL
FACT-L
& Uniscale
LCSS
& UniscaleSDS & Uniscale Total
Uniscale
Number evaluable* 122122 155 46 323
Severe AE 26 (21.3%)26 (21.3%) 74 (47.7%) 17 (37.0%) 117 (36.2%)
CSD in QOL 74 (60.7%) 92 (59.3%) 20 (43.5%) 186 (57.6%)
Percent agreement 46% 51% 46% 48%
Multiple-items
Number evaluable* 140 156 45 341
Severe AE 30 (21.4%) 76 (48.7%) 17 (37.8%) 123 (36.1%)
CSD in QOL 52 (37.1%) 67 (43.0%) 13 (28.9%) 132 (38.7%)
Percent agreement 64% 53% 60% 59%
*Represents the number of patients that had an adverse event (any grade) and completed a QOL assessment at baseline and at least once post-baseline
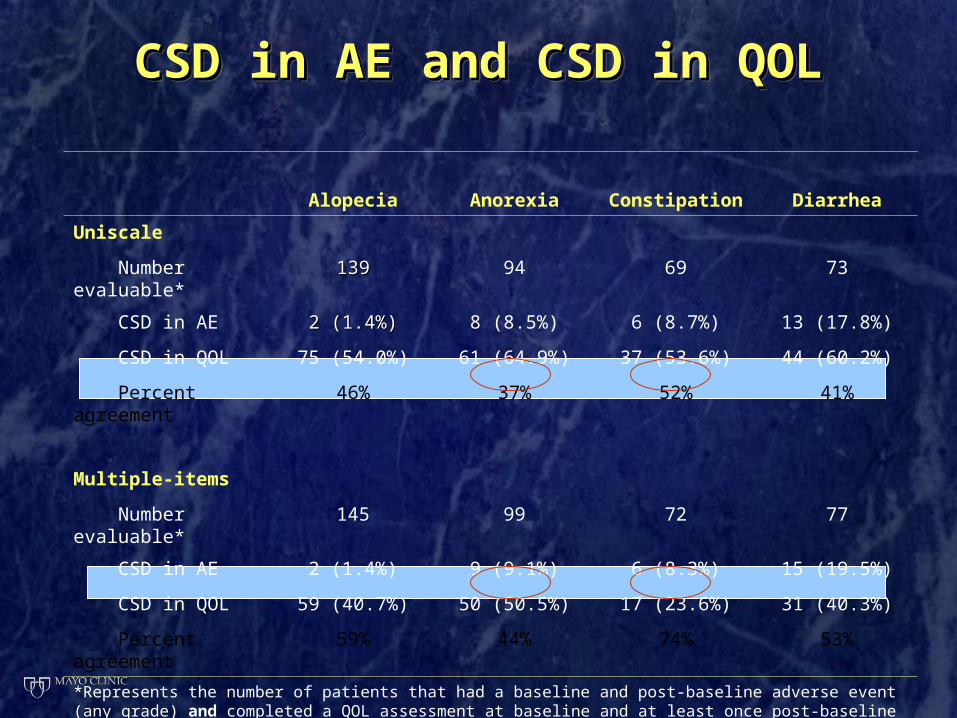
CSD in AE and CSD in QOLCSD in AE and CSD in QOLCSD in AE and CSD in QOLCSD in AE and CSD in QOL
Alopecia Anorexia Constipation Diarrhea
Uniscale
Number evaluable* 139139 94 69 73
CSD in AE 2 (1.4%)2 (1.4%) 8 (8.5%) 6 (8.7%) 13 (17.8%)
CSD in QOL 75 (54.0%) 61 (64.9%) 37 (53.6%) 44 (60.2%)
Percent agreement 46% 37% 52% 41%
Multiple-items
Number evaluable* 145 99 72 77
CSD in AE 2 (1.4%) 9 (9.1%) 6 (8.3%) 15 (19.5%)
CSD in QOL 59 (40.7%) 50 (50.5%) 17 (23.6%) 31 (40.3%)
Percent agreement 59% 44% 74% 53%
*Represents the number of patients that had a baseline and post-baseline adverse event (any grade) and completed a QOL assessment at baseline and at least once post-baseline

CSD in AE and CSD in QOLCSD in AE and CSD in QOLCSD in AE and CSD in QOLCSD in AE and CSD in QOL
Dyspnea Fatigue NauseaNeuro-sensory Vomiting
Uniscale
Number evaluable* 155155 226 208 189 142
CSD in AE 43 (27.7%)43 (27.7%) 42 (18.6%) 34 (16.4%) 9 (4.8%) 23 (16.2%)
CSD in QOL 90 (58.1%) 139 (61.5%) 118 (56.7%) 116 (61.4%) 72 (50.7%)
Percent agreement 46% 42% 42% 39% 50%
Multiple-items
Number evaluable* 159 236 216 202 150
CSD in AE 43 (27.0%) 45 (19.1%) 33 (15.3%) 11 (5.5%) 23 (15.3%)
CSD in QOL 67 (42.1%) 96 (40.1%) 84 (38.9%) 73 (36.1%) 60 (40.0%)
Percent agreement 57% 59% 58% 64% 63%
*Represents the number of patients that had a baseline and post-baseline adverse event (any grade) and completed a QOL assessment at baseline and at least once post-baseline

K-M Estimate of the Time to First Occurrence of Severe AE and CSD in QOL
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5
Time (years)
% E
ven
t-fr
ee
Severe AE Median: 304 days
Multiple-item Median: 142 days
Uniscale Median: 67 days

K-M Estimate of Time to First Occurrence of Severe Fatigue and CSD in LCSS Fatigue
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3Time (years)
% E
ven
t-fr
ee
AE
LCSS Median: 81 days
70%70%
12%12%

K-M Estimate of Time to First Occurrence of Severe Fatigue and CSD in SDS Fatigue
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12Time (months)
% E
ven
t-fr
ee
AE
SDS Median: 52 days
•6 events reported via CTC6 events reported via CTC•25 CSD reported via SDS25 CSD reported via SDS
83.7%83.7%
25.3%25.3%

SummarySummarySummarySummary
• Uniscale demonstrates greater variability than the multiple-item indices
• The Uniscale is better able to detect a CSD in QOL than the multiple item assessments, and captures a CSD earlier than the multiple item assessments
• Correlations and percent agreement between Uniscale and multiple-item assessments were modest
• Uniscale demonstrates greater variability than the multiple-item indices
• The Uniscale is better able to detect a CSD in QOL than the multiple item assessments, and captures a CSD earlier than the multiple item assessments
• Correlations and percent agreement between Uniscale and multiple-item assessments were modest

SummarySummarySummarySummary
• There is indication that a CSD in QOL occurs earlier than CTC AE reporting
• Consistent with a recent finding that single-item QOL assessments detect a patient-perceived problem in peripheral neuropathy more than six weeks earlier than CTC (Morton et al, ASCO 2005)
• The multiple-item assessments are in better agreement with occurrence or CSD in AE compared to the Uniscale
• There is indication that a CSD in QOL occurs earlier than CTC AE reporting
• Consistent with a recent finding that single-item QOL assessments detect a patient-perceived problem in peripheral neuropathy more than six weeks earlier than CTC (Morton et al, ASCO 2005)
• The multiple-item assessments are in better agreement with occurrence or CSD in AE compared to the Uniscale

What is the evidence for the use of What is the evidence for the use of simple (single-item) LASA’s?simple (single-item) LASA’s?

The literature for simple assessments is The literature for simple assessments is considerableconsiderable
The literature for simple assessments is The literature for simple assessments is considerableconsiderable
• Grunberg S.M. (1996). Grunberg S.M. (1996). Comparison of conditional quality of life terminology and Comparison of conditional quality of life terminology and visual analogue scale measurements. visual analogue scale measurements. Quality of Life ResearchQuality of Life Research; 5: 65-72.; 5: 65-72.
• Gudex C. (1996). Health state valuations from the general public using the Visual Gudex C. (1996). Health state valuations from the general public using the Visual Analogue Scale. Analogue Scale. Quality of Life ResearchQuality of Life Research, 5: 521-531., 5: 521-531.
• Hyland ME. Development of a new type of global quality of life scale and Hyland ME. Development of a new type of global quality of life scale and comparison and preference for 12 global scales. comparison and preference for 12 global scales. Quality of Life ResearchQuality of Life Research. 5(5): 469-. 5(5): 469-480. 1996.480. 1996.
• Sriwatanakul, K. (1983). Studies with different types of visual analog scales for Sriwatanakul, K. (1983). Studies with different types of visual analog scales for measurement of pain; measurement of pain; Clinical Pharmacology and Therapeutics;Clinical Pharmacology and Therapeutics; 34(2): 234-239. 34(2): 234-239.
• Wewers ME. (1990). A Critical Review of Visual Analogue Scales in the Wewers ME. (1990). A Critical Review of Visual Analogue Scales in the Measurement of Clinical Phenomena. Measurement of Clinical Phenomena. Research in Nursing & HealthResearch in Nursing & Health, 13: 227-236., 13: 227-236.
• Bretscher M. (1999). Quality of Life in Hospice Patients: A Pilot Study, Bretscher M. (1999). Quality of Life in Hospice Patients: A Pilot Study,
PsychosomaticsPsychosomatics, 40, 309-313., 40, 309-313.
• Grunberg S.M. (1996). Grunberg S.M. (1996). Comparison of conditional quality of life terminology and Comparison of conditional quality of life terminology and visual analogue scale measurements. visual analogue scale measurements. Quality of Life ResearchQuality of Life Research; 5: 65-72.; 5: 65-72.
• Gudex C. (1996). Health state valuations from the general public using the Visual Gudex C. (1996). Health state valuations from the general public using the Visual Analogue Scale. Analogue Scale. Quality of Life ResearchQuality of Life Research, 5: 521-531., 5: 521-531.
• Hyland ME. Development of a new type of global quality of life scale and Hyland ME. Development of a new type of global quality of life scale and comparison and preference for 12 global scales. comparison and preference for 12 global scales. Quality of Life ResearchQuality of Life Research. 5(5): 469-. 5(5): 469-480. 1996.480. 1996.
• Sriwatanakul, K. (1983). Studies with different types of visual analog scales for Sriwatanakul, K. (1983). Studies with different types of visual analog scales for measurement of pain; measurement of pain; Clinical Pharmacology and Therapeutics;Clinical Pharmacology and Therapeutics; 34(2): 234-239. 34(2): 234-239.
• Wewers ME. (1990). A Critical Review of Visual Analogue Scales in the Wewers ME. (1990). A Critical Review of Visual Analogue Scales in the Measurement of Clinical Phenomena. Measurement of Clinical Phenomena. Research in Nursing & HealthResearch in Nursing & Health, 13: 227-236., 13: 227-236.
• Bretscher M. (1999). Quality of Life in Hospice Patients: A Pilot Study, Bretscher M. (1999). Quality of Life in Hospice Patients: A Pilot Study,
PsychosomaticsPsychosomatics, 40, 309-313., 40, 309-313.

The Visual Analogue UniscaleThe Visual Analogue UniscaleThe Visual Analogue UniscaleThe Visual Analogue Uniscale
Please mark with an ‘X’ the appropriate place within the bar to Please mark with an ‘X’ the appropriate place within the bar to indicate your rating of this person’s quality of life during the indicate your rating of this person’s quality of life during the past week.past week.
Lowest quality applies to someone completely dependent Lowest quality applies to someone completely dependent physically on others, seriously impaired mentally, unaware physically on others, seriously impaired mentally, unaware of surroundings, and in a hopeless position.of surroundings, and in a hopeless position.
Highest quality applies to someone physically and mentally Highest quality applies to someone physically and mentally independent, communicating well with others, able to do independent, communicating well with others, able to do most of the things enjoyed, pulling own weight, with a most of the things enjoyed, pulling own weight, with a hopeful yet realistic attitude. hopeful yet realistic attitude.
Please mark with an ‘X’ the appropriate place within the bar to Please mark with an ‘X’ the appropriate place within the bar to indicate your rating of this person’s quality of life during the indicate your rating of this person’s quality of life during the past week.past week.
Lowest quality applies to someone completely dependent Lowest quality applies to someone completely dependent physically on others, seriously impaired mentally, unaware physically on others, seriously impaired mentally, unaware of surroundings, and in a hopeless position.of surroundings, and in a hopeless position.
Highest quality applies to someone physically and mentally Highest quality applies to someone physically and mentally independent, communicating well with others, able to do independent, communicating well with others, able to do most of the things enjoyed, pulling own weight, with a most of the things enjoyed, pulling own weight, with a hopeful yet realistic attitude. hopeful yet realistic attitude.
Lowest Quality
Highest Quality
(Please mark one ‘X’ within the bar)

Uniscale-NASUniscale-NAS(Numeric Analog Scale)(Numeric Analog Scale)
Uniscale-NASUniscale-NAS(Numeric Analog Scale)(Numeric Analog Scale)
Directions: Please circle the number (0-10) best reflecting your response to the followingthat describes your feelings during the past week, including today.
How would you describe:
1. your overall Quality of Life?
0 1 2 3 4 5 6 7 8 9 10As bad as As good asit can be it can be

Linear Analogue Self Assessment Linear Analogue Self Assessment (LASA)(LASA)
Linear Analogue Self Assessment Linear Analogue Self Assessment (LASA)(LASA)
• General measure of global QOL dimensional constructsGeneral measure of global QOL dimensional constructs
• Overall QOL Uniscale question plus domain specific questionsOverall QOL Uniscale question plus domain specific questions
• LASA 6 questionsLASA 6 questions• covering domains: QOL, Mental, Social, Spiritual, Emotional, covering domains: QOL, Mental, Social, Spiritual, Emotional,
Physical Physical e.g. How would you describe your overall physical well-being e.g. How would you describe your overall physical well-being during the past week, including today? during the past week, including today? (0: as bad as it can be; 10: as good as it can be)(0: as bad as it can be; 10: as good as it can be)
• LASA additional items (any understandable construct) LASA additional items (any understandable construct) e.g. How would you describe your anxiety during the past week, e.g. How would you describe your anxiety during the past week, including today? including today?
(0: anxiety as bad as it can be; 10: no anxiety)(0: anxiety as bad as it can be; 10: no anxiety)
• General measure of global QOL dimensional constructsGeneral measure of global QOL dimensional constructs
• Overall QOL Uniscale question plus domain specific questionsOverall QOL Uniscale question plus domain specific questions
• LASA 6 questionsLASA 6 questions• covering domains: QOL, Mental, Social, Spiritual, Emotional, covering domains: QOL, Mental, Social, Spiritual, Emotional,
Physical Physical e.g. How would you describe your overall physical well-being e.g. How would you describe your overall physical well-being during the past week, including today? during the past week, including today? (0: as bad as it can be; 10: as good as it can be)(0: as bad as it can be; 10: as good as it can be)
• LASA additional items (any understandable construct) LASA additional items (any understandable construct) e.g. How would you describe your anxiety during the past week, e.g. How would you describe your anxiety during the past week, including today? including today?
(0: anxiety as bad as it can be; 10: no anxiety)(0: anxiety as bad as it can be; 10: no anxiety)

LASA Validity DataLASA Validity DataLASA Validity DataLASA Validity Data
• Median split adds 3 months to median survival in Median split adds 3 months to median survival in advanced cancer patients (Sloan, JCO, 1998)advanced cancer patients (Sloan, JCO, 1998)
• Qualitative study: score of 5 or less indicates need for Qualitative study: score of 5 or less indicates need for intervention (Frost, unpublished)intervention (Frost, unpublished)
• ““Stable” populations average roughly 7, with SD roughly 2 Stable” populations average roughly 7, with SD roughly 2 on 10-point scale (20 on 100 pointt scale) (Locke, in on 10-point scale (20 on 100 pointt scale) (Locke, in preparation)preparation)
• Median split adds 3 months to median survival in Median split adds 3 months to median survival in advanced cancer patients (Sloan, JCO, 1998)advanced cancer patients (Sloan, JCO, 1998)
• Qualitative study: score of 5 or less indicates need for Qualitative study: score of 5 or less indicates need for intervention (Frost, unpublished)intervention (Frost, unpublished)
• ““Stable” populations average roughly 7, with SD roughly 2 Stable” populations average roughly 7, with SD roughly 2 on 10-point scale (20 on 100 pointt scale) (Locke, in on 10-point scale (20 on 100 pointt scale) (Locke, in preparation)preparation)

LASA Norms (Various)LASA Norms (Various)LASA Norms (Various)LASA Norms (Various)
• Hospice patients 7.6Hospice patients 7.6
• Advanced cancer patients 7.2Advanced cancer patients 7.2
• Recovering surgical patients 6.6Recovering surgical patients 6.6
• Healthy volunteers 8.2Healthy volunteers 8.2
• Medical students 4.4Medical students 4.4
• Hospice patients 7.6Hospice patients 7.6
• Advanced cancer patients 7.2Advanced cancer patients 7.2
• Recovering surgical patients 6.6Recovering surgical patients 6.6
• Healthy volunteers 8.2Healthy volunteers 8.2
• Medical students 4.4Medical students 4.4

A Structured Multidisciplinary Psychosocial A Structured Multidisciplinary Psychosocial Intervention Intervention
Improves the Quality of Life Improves the Quality of Life of Patients with Advanced Stage Cancer
A Structured Multidisciplinary Psychosocial A Structured Multidisciplinary Psychosocial Intervention Intervention
Improves the Quality of Life Improves the Quality of Life of Patients with Advanced Stage Cancer
In press, JCOIn press, JCOIn press, JCOIn press, JCO
T Rummans, M Clark, J Sloan, M Frost, P Atherton, M Bostwick, G Gamble, M Johnson, J Richardson
Mayo Clinic, Rochester, MN

BackgroundBackgroundBackgroundBackground
• Some studies have suggested a psychosocial Some studies have suggested a psychosocial intervention has a positive effect on survival, intervention has a positive effect on survival, while others have not demonstrated such an while others have not demonstrated such an effect or suggested a negative effect on effect or suggested a negative effect on survival.survival. (Spiegel, 1990; Goodwin NEJM 2001; Spiegel, Cancer, 2002)(Spiegel, 1990; Goodwin NEJM 2001; Spiegel, Cancer, 2002)
• Most interventions are single - focus and have Most interventions are single - focus and have targeted mood targeted mood (Fawzy, AGP,1993; Jacobsen JCO 2002; Kolden, (Fawzy, AGP,1993; Jacobsen JCO 2002; Kolden, Psycho-Onc. 2002)Psycho-Onc. 2002)
• Some studies have suggested a psychosocial Some studies have suggested a psychosocial intervention has a positive effect on survival, intervention has a positive effect on survival, while others have not demonstrated such an while others have not demonstrated such an effect or suggested a negative effect on effect or suggested a negative effect on survival.survival. (Spiegel, 1990; Goodwin NEJM 2001; Spiegel, Cancer, 2002)(Spiegel, 1990; Goodwin NEJM 2001; Spiegel, Cancer, 2002)
• Most interventions are single - focus and have Most interventions are single - focus and have targeted mood targeted mood (Fawzy, AGP,1993; Jacobsen JCO 2002; Kolden, (Fawzy, AGP,1993; Jacobsen JCO 2002; Kolden, Psycho-Onc. 2002)Psycho-Onc. 2002)

Motivation for the present studyMotivation for the present studyMotivation for the present studyMotivation for the present study
• A multidisciplinary intervention had not been A multidisciplinary intervention had not been tried nor tested for feasibilitytried nor tested for feasibility
• Overall QOL is the composite, multidimensional Overall QOL is the composite, multidimensional psychosocial targetpsychosocial target
• A multidisciplinary intervention had not been A multidisciplinary intervention had not been tried nor tested for feasibilitytried nor tested for feasibility
• Overall QOL is the composite, multidimensional Overall QOL is the composite, multidimensional psychosocial targetpsychosocial target

Study Schema
Patients with Advanced Stage
Disease scheduled to
undergo radiation therapy
R
Arm A: Structured multi-disciplinary psychosocial intervention.
8 - 90 minute sessions over 4 weeks
Arm B: Standard Care
QOL assessed at baseline and week 4 (EOT)
Stratification: tumor type, ECOG PS, age

Linear Analogue Self Assessment (LASA) items
Profile of Mood States – Short Form (POMS)
Symptom Distress Scale (SDS)
FACIT – Spiritual Well-Being
Secondary endpoint assessment tools

Which is the “real” symptom endpoint?

At week 4, overall QOL was 10 points higher in the intervention arm than in the standard care arm (80 versus 70 on the 100-point scale respectively, p=0.047).
The treatment group improved 3.3 points from baseline, while the control group decreased 8.9 points on average, p=0.009.
More than three times as many patients in the treatment group reported a 10-point improvement in QOL from baseline compared to the control group (30% versus 9%, p=0.004).
Primary Result: Overall QOL at 4 weeks

MC997C: Mean LASA Scores at Week 4
Normal Transformed
Range 0-10, Best=10 Range 0-100, Best=100
Overall QOL 7.3 72.8
Mental Well-being 7.8 77.8
Physical Well-being 6.3 63.3
Emotional Well-being 7.6 75.9
Social Activity 6.2 62.4
Spiritual Well-being 8.4 83.9
MC997C: Mean POMS Scores at Week 4
Normal Transformed
SUBSCALE SCORES Range 0-20, Best=20 Range 0-100, Best=100
Tension-Anxiety Subscale 16.3 81.7
Depression-Dejection Subscale 17.7 88.5
Anger-Hostility Subscale 17.8 88.9
Vigor-Activity Subscale 7.2 36.0
Fatigue-Inertia Subscale 11.8 59.2
Confusion-Bewilderment Subscale
16.5 82.5
TOTAL SCORES Range 0-120, Best=120 Range 0-100, Best=100
POMS-SF Total Score 87.4 72.8

best
worst
