clozapine: does it work? analysis of a 15 year experience · clozapine: does it work? analysis of a...
TRANSCRIPT

Article ID: WMC002228 ISSN 2046-1690
Clozapine: Does it work? Analysis of a 15 yearexperienceCorresponding Author:Dr. Ennio Piantato,Division Chief / Dept of Mental Health, Azienda Ospedaliera Nazionale , Alessandria, 15121 - Italy
Submitting Author:Dr. Ennio Piantato,Division Chief / Dept of Mental Health, Azienda Ospedaliera Nazionale , Alessandria, 15121 - Italy
Article ID: WMC002228
Article Type: Case Report
Submitted on:24-Sep-2011, 12:17:58 PM GMT
Article URL: http://www.webmedcentral.com/article_view/2228
Subject Categories:PSYCHIATRY
Keywords:Clozapine, Schizophrenia, Results
Source(s) of Funding:
No funding required
Competing Interests:
None
WebmedCentral > Case Report Page 1 of 21
WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Clozapine: Does it work? Analysis of a 15 yearexperienceAuthor(s): Piantato E , Sartore F
Abstract
Clozapine: does it work?
Analysis of a 15 year experience.
Ennio PIANTATO and Francesca SARTORE
ABSTRACT
This is an overview of results after a 15 year follow-up of psychotic
patients treated mainly with Clozapine. We have found out that their
quality of life has improved, they are good compliant in taking their
medications and the number of hospitalizations is greatly reduced
after beginning treatment with Clozapine.
INTRODUCTION
This report contains data about use of Clozapine in our Psychiatric
Unit during the period June 1995-June 2009.
Clozapine is an anti-psychotic drug created at the end of 60’s, with a
particular receptor profile.
Due to some cases of granulocytopenia noted in Finland the drug was
withdrawn in 1975. It was reintroduced in the 90’s with indication for
“resistant schizophrenia” and a recommendation to monitor blood cell
counts. Since 1995 Clozapine has been officially used in Italy for
“resistant schizophrenia”.
In 1995 we started using Clozapine after two of us attended a course
at the Psychiatric Clinic of the Bern University, Switzerland.
Our Psychiatric Unit is part of a Department of Mental Health and
situated in the Alessandria general hospital, in the region of Piedmont
in NW Italy, serving a population of 180.000 inhabitants. The unit has
15 beds plus 1 bed for Day Hospital service.
Initially Clozapine was used with so-called treatment-resistant
schizophrenic patients, showing resistance to traditional and at least
two atypical antipsychotic treatments as reported in international
guidelines. [1]
Afterwards the treatment with Clozapine was extended to patients
affected by non-schizophrenic disturbances such as bipolar disorder.
MATERIAL AND METHODS
Our report includes the group of patients currently taking Clozapine
and attending our centre for blood test control. Almost all of them
started Clozapine while hospitalized in our Psychiatric Unit.
At the moment the group is made up of 54 patients: 41 males (76%)
and 13 females (24%).
Originally the use of Clozapine began with 6 patients (4 males and 2
females) who are still under the care of our centre.
Average age of patients is 43±9.9 for the total group: for the male
group average age is 40, for the female group it is 46.
Age range is from 26 to 69 years.
All patients live at home with 8 exceptions: 6 of them live in sheltered
apartments and 1 is in a nursing home.
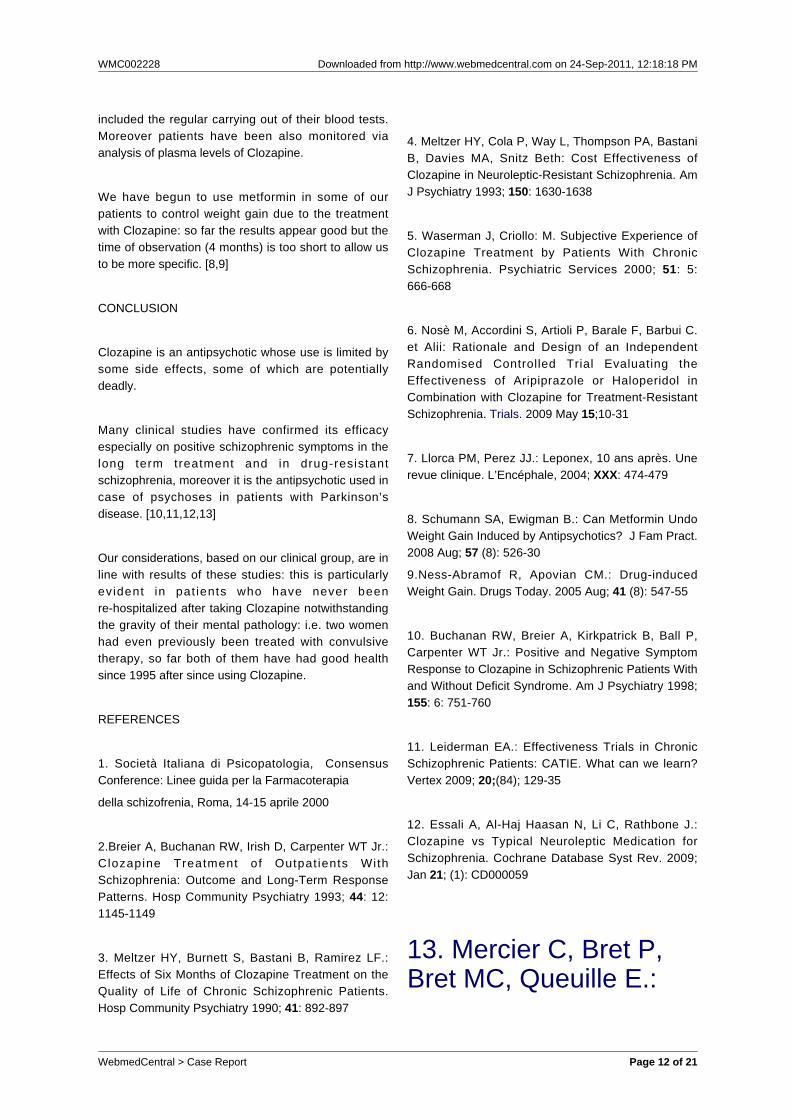
Regarding the diagnoses, 48 patients (88.9%) are affected by
schizophrenia, 4 (7.4%) by a schizoaffective disorder and 2 (3.7%) by
bipolar disorder with psychotic behaviour. (Tab 1).
Tab 1: Diagnosis (total group)
Diagnosis TOTAL MEN WOMEN
Schizophrenia 48 37 11
Schizoaffective disorder 4 3 1
Bipolar disorder 2 1 1
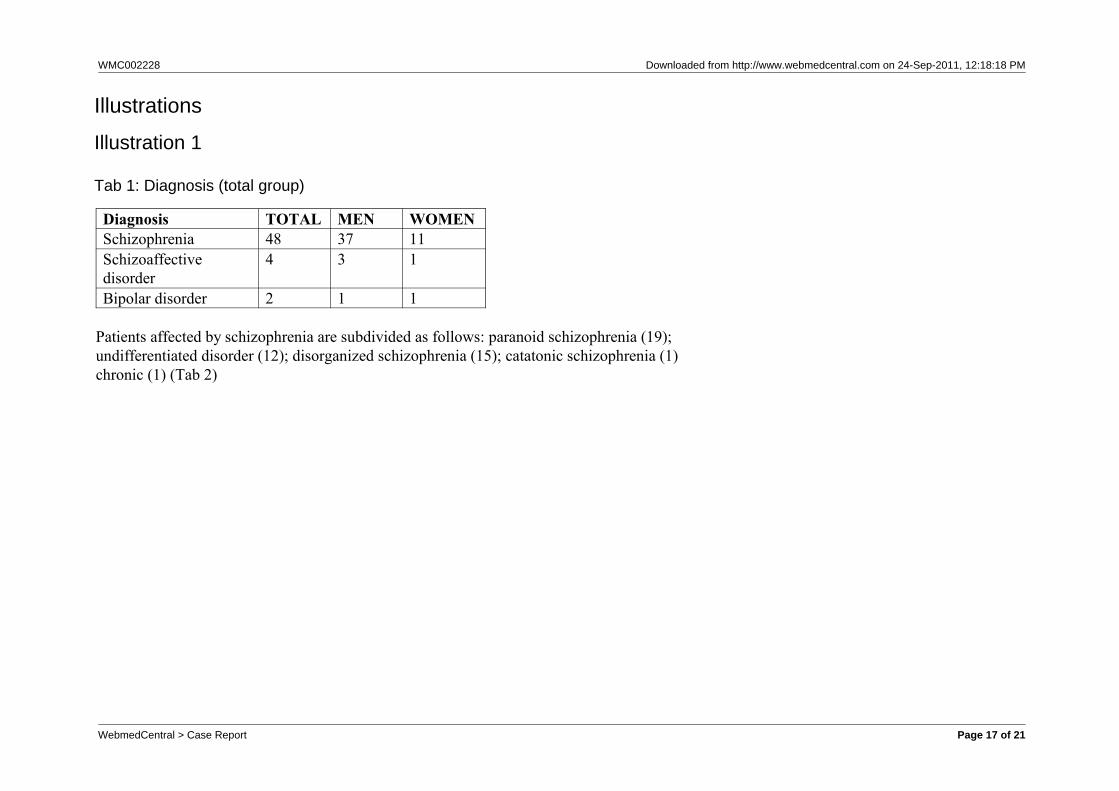
Patients affected by schizophrenia are subdivided as follows: paranoid
schizophrenia (19); undifferentiated disorder (12); disorganized
schizophrenia (15); catatonic schizophrenia (1) chronic (1) (Tab 2)
Tab 2 : Schizophrenia sub-types
Sub-type TOTAL MEN WOMEN
Catatonic 1 1 -
Disorganized 15 11 4
Undifferentiated 12 9 3
Paranoid 19 15 4
Chronic 1 1 -
Our doses of Clozapine vary from 100 to 900 mg per day: doses are
higher – usually - on discharge from hospital (150 to 900 mg per day)
WebmedCentral > Case Report Page 2 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
then they tend to diminish to a medium 75 to 600 mg per day.
Clozapine is used as monotherapy in 19 patients (35.1%) . It’s also
used in association with other psychotropic drugs (sometimes more
than one per category) in remaining cases: more precisely in
association with mood-stabilizers in 19 patients, antisialorroic drugs
in 4 patients, anticholinergic medications in 19 patients, other
antipsychotic drugs in 20 patients, benzodiazepines in 10 patients and
antidepressants in 3 patients.
We have observed that the side effects of treatment with Clozapine
are most frequently:-
sialorrea (excessive salivation); constipation; low blood pressure;
psychomotor slowing; weight increase; in one case an epileptic fit
was controlled by adding an anti-epileptic drug so the global
treatment could be continued without having any other problem; two
patients are affected by epilepsy in co-morbidity and take
anti-epileptic drugs.
In this group we have not had any granulocytopenia.
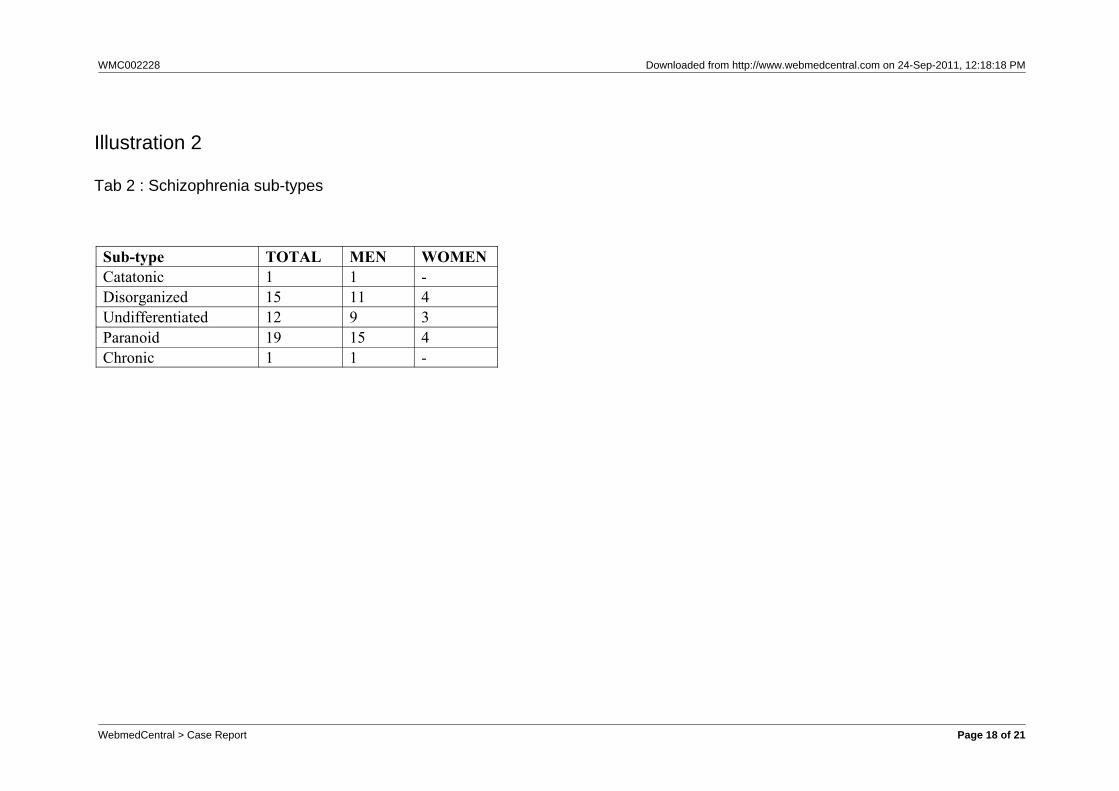
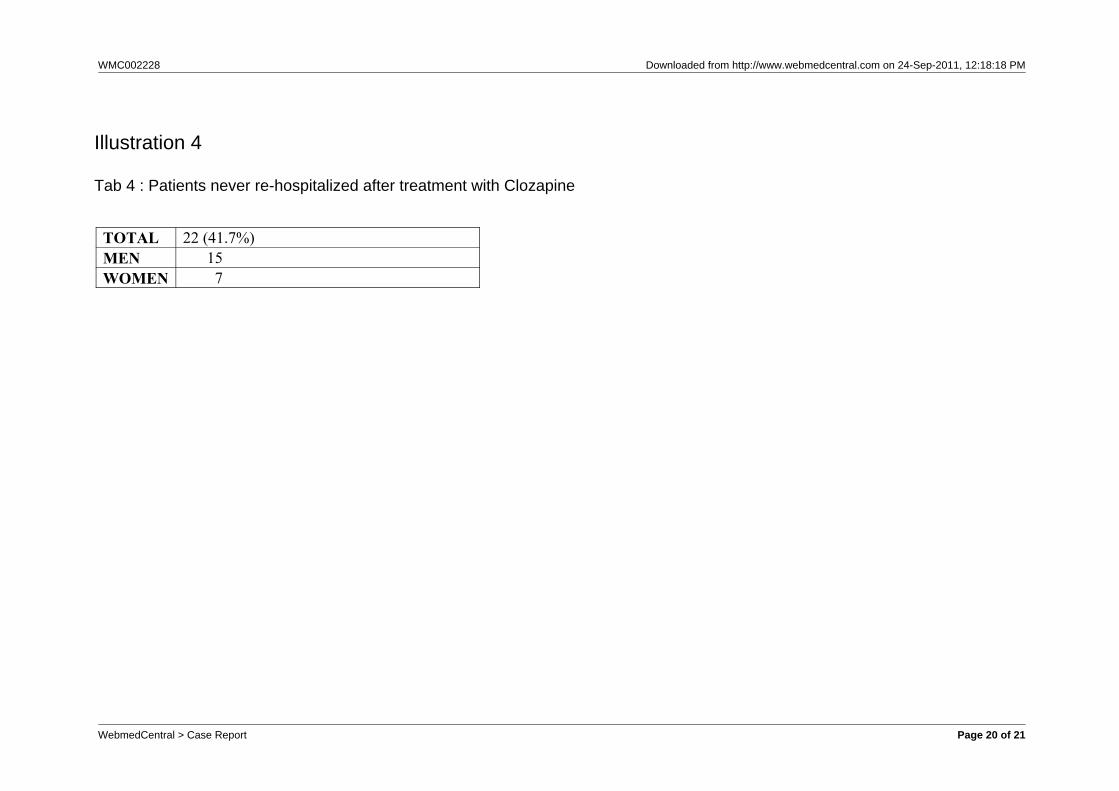
We have observed a reduction in hospital admissions after beginning
treatment with Clozapine, above all in the male group. In 22 patients
(40.7% of the group) we haven’t had further hospital admissions.
(Tab 3 and 4).
Tab 3 : Hospitalizations
TOTAL MEN WOMEN
Total number of hospitalizations 522 447 75
Before treatment with clozapine 413 354 59
After treatment with clozapine 109 93 16
Tab 4 : Patients never re-hospitalized after treatment with Clozapine
TOTAL 22 (41.7%)
MEN 15
WOMEN 7
DISCUSSION
Results
The reduction of hospitalizations is reported [2,3] and explained as
“effect of objective improvement of some clinical parameters and
better social and job adaptability” [4] this is consistent with the self
evaluated subjective improvement registered by our patients and by
authors. [5]
Clozapine alone isn’t always enough. In our group Clozapine is often
associated with other psychotropic drugs and it is used as the only
antipsychotic drug in 19 patients; among most frequently used drugs
in association there are other first and second generation
antipsychotics.
Regarding the association between Clozapine and other antipsychotics
we found that two patients of the group have been included in the
CHAT study (experimental cohort with Clozapine enhanced
associating another antipsychotic drug, aripiprazole or haloperidol).
[6]
No patient of ours has tried or succeeded in committing suicide so far
and this is consistent with other reports [7].
Clozapine has also produced good results with patients whose
behaviour had been violent specially in a etero-directed way.
Scientific evidence shows that continuous use of anti-psychotic drugs
in schizophrenics prevents relapses.
Compliance with treatment is important in all chronic pathologies and
in our group especially an interruption of treatment provokes various
consequences, first of all the risk of a relapse with hospitalization (up
to “revolving-door” conditions) plus blockage of the personal
therapeutic and rehabilitation project. The reduction in hospitalization
observed in our group is the verification of good compliance with
treatment included the regular carrying out of their blood tests.
Moreover patients have been also monitored via analysis of plasma
levels of Clozapine.
We have begun to use metformin in some of our patients to control
weight gain due to the treatment with Clozapine: so far the results
appear good but the time of observation (4 months) is too short to
allow us to be more specific. [8,9]
CONCLUSION
Clozapine is an antipsychotic whose use is limited by some side
effects, some of which are potentially deadly.
Many clinical studies have confirmed its efficacy especially on
positive schizophrenic symptoms in the long term treatment and in
drug-resistant schizophrenia, moreover it is the antipsychotic used in
case of psychoses in patients with Parkinson’s disease. [10,11,12,13]
Our considerations, based on our clinical group, are in line with
results of these studies: this is particularly evident in patients who
have never been re-hospitalized after taking Clozapine
notwithstanding the gravity of their mental pathology: i.e. two women
had even previously been treated with convulsive therapy, so far both
of them have had good health since 1995 after since using Clozapine.
REFERENCES
1. Società Italiana di Psicopatologia, Consensus Conference: Linee
guida per la Farmacoterapia
della schizofrenia, Roma, 14-15 aprile 2000
WebmedCentral > Case Report Page 3 of 21
WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
2.Breier A, Buchanan RW, Irish D, Carpenter WT Jr.: Clozapine
Treatment of Outpatients With Schizophrenia: Outcome and
Long-Term Response Patterns. Hosp Community Psychiatry 1993; 44:
12: 1145-1149
3. Meltzer HY, Burnett S, Bastani B, Ramirez LF.: Effects of Six
Months of Clozapine Treatment on the Quality of Life of Chronic
Schizophrenic Patients. Hosp Community Psychiatry 1990; 41:
892-897
4. Meltzer HY, Cola P, Way L, Thompson PA, Bastani B, Davies MA,
Snitz Beth: Cost Effectiveness of Clozapine in Neuroleptic-Resistant
Schizophrenia. Am J Psychiatry 1993; 150: 1630-1638
5. Waserman J, Criollo: M. Subjective Experience of Clozapine
Treatment by Patients With Chronic Schizophrenia. Psychiatric
Services 2000; 51: 5: 666-668
6. Nosè M, Accordini S, Artioli P, Barale F, Barbui C. et Alii:
Rationale and Design of an Independent Randomised Controlled Trial
Evaluating the Effectiveness of Aripiprazole or Haloperidol in
Combination with Clozapine for Treatment-Resistant Schizophrenia.
Trials. 2009 May 15;10-31
7. Llorca PM, Perez JJ.: Leponex, 10 ans après. Une revue clinique.
L’Encéphale, 2004; XXX: 474-479
8. Schumann SA, Ewigman B.: Can Metformin Undo Weight Gain
Induced by Antipsychotics? J Fam Pract. 2008 Aug; 57 (8): 526-30
9.Ness-Abramof R, Apovian CM.: Drug-induced Weight Gain. Drugs
Today. 2005 Aug; 41 (8): 547-55
10. Buchanan RW, Breier A, Kirkpatrick B, Ball P, Carpenter WT Jr.:
Positive and Negative Symptom Response to Clozapine in
Schizophrenic Patients With and Without Deficit Syndrome. Am J
Psychiatry 1998; 155: 6: 751-760
11. Leiderman EA.: Effectiveness Trials in Chronic Schizophrenic
Patients: CATIE. What can we learn? Vertex 2009; 20;(84); 129-35
12. Essali A, Al-Haj Haasan N, Li C, Rathbone J.: Clozapine vs
Typical Neuroleptic Medication for Schizophrenia. Cochrane
Database Syst Rev. 2009; Jan 21; (1): CD000059
13. Mercier C, Bret P, BretMC, Queuille E.: Enquêteobservationelle de
prescription de laclozapine au centrehospitalier Charles-Perrensà Bordeaux, plus de 15 ansaprès l’AMM en France.L’Encéphale. 2009;XXXV (4): 321-9
Ennio Piantato MD,
Servizio Psichiatrico
Azienda OspedalieraNazionale SS Antonio eBiagio,
via Venezia 16
15121 Alessandria
Italy
Tel +39.01.31.20.64.10
Fax +39.01.31.20.66.16
WebmedCentral > Case Report Page 4 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Email: [email protected]
Francesca Sartore MD
Servizio Psichiatrico
Azienda OspedalieraNazionale SS Antonio eBiagio
Via Venezia 16
15121 Alessandria
Italy
Tel+39.01.31.20.66.12
Fax +39.01.31.20.66.16
>Email: [email protected]
Both Authors equallycontributed to this article.
Clozapine: does it work?
Analysis of a 15 year experience.
Ennio PIANTATO and Francesca SARTORE
ABSTRACT
This is an overview of results after a 15 year follow-upof psychotic patients treated mainly with Clozapine.We have found out that their quality of life hasimproved, they are good compliant in taking theirmedications and the number of hospitalizations isgreatly reduced after beginning treatment withClozapine.
INTRODUCTION
This report contains data about use of Clozapine inour Psychiatric Unit during the period June 1995-June2009.
WebmedCentral > Case Report Page 5 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Clozapine is an anti-psychotic drug created at the endof 60’s, with a particular receptor profile.
Due to some cases of granulocytopenia noted inFinland the drug was withdrawn in 1975. It wasreintroduced in the 90’s with indication for “resistantschizophrenia” and a recommendation to monitorblood cell counts. Since 1995 Clozapine has beenofficially used in Italy for “resistant schizophrenia”.
In 1995 we started using Clozapine after two of usattended a course at the Psychiatric Clinic of the BernUniversity, Switzerland.
Our Psychiatric Unit is part of a Department of MentalHealth and situated in the Alessandria general hospital,in the region of Piedmont in NW Italy, serving apopulation of 180.000 inhabitants. The unit has 15beds plus 1 bed for Day Hospital service.
Init ially Clozapine was used with so-calledtreatment-resistant schizophrenic patients, showingresistance to traditional and at least two atypicalantipsychotic treatments as reported in internationalguidelines. [1]
Afterwards the treatment with Clozapine was extendedto patients affected by non-schizophrenic disturbancessuch as bipolar disorder.
MATERIAL AND METHODS
Our report includes the group of patients currentlytaking Clozapine and attending our centre for bloodtest control. Almost all of them started Clozapine whilehospitalized in our Psychiatric Unit.
At the moment the group is made up of 54 patients: 41males (76%) and 13 females (24%).
Originally the use of Clozapine began with 6 patients(4 males and 2 females) who are still under the care ofour centre.
Average age of patients is 43±9.9 for the total group:for the male group average age is 40, for the femalegroup it is 46.
Age range is from 26 to 69 years.
All patients live at home with 8 exceptions: 6 of themlive in sheltered apartments and 1 is in a nursing home.
Regarding the diagnoses, 48 patients (88.9%) areaffected by schizophrenia, 4 (7.4%) by aschizoaffective disorder and 2 (3.7%) by bipolardisorder with psychotic behaviour. (Tab 1).
Tab 1: Diagnosis (total group)
Diagnosis TOTAL MEN WOMEN
Schizophrenia 48 37 11
Schizoaffective disorder 4 3 1
Bipolar disorder 2 1 1
Patients affected by schizophrenia are subdivided asfollows: paranoid schizophrenia (19); undifferentiateddisorder (12); disorganized schizophrenia (15);catatonic schizophrenia (1) chronic (1) (Tab 2)
Tab 2 : Schizophrenia sub-types
Sub-type TOTAL MEN WOMEN
Catatonic 1 1 -
Disorganized 15 11 4
Undifferentiated 12 9 3
Paranoid 19 15 4
Chronic 1 1 -
Our doses of Clozapine vary from 100 to 900 mg perday: doses are higher – usually - on discharge fromhospital (150 to 900 mg per day) then they tend todiminish to a medium 75 to 600 mg per day.
Clozapine is used as monotherapy in 19 patients(35.1%) . It’s also used in association with otherpsychotropic drugs (sometimes more than one percategory) in remaining cases: more precisely inassociation with mood-stabilizers in 19 patients,antisialorroic drugs in 4 patients, anticholinergicmedications in 19 patients, other antipsychotic drugsin 20 patients, benzodiazepines in 10 patients andantidepressants in 3 patients.
We have observed that the side effects of treatmentwith Clozapine are most frequently:-
sialorrea (excessive salivation); constipation; lowblood pressure; psychomotor slowing; weight increase;
WebmedCentral > Case Report Page 6 of 21
WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
in one case an epileptic fit was controlled by adding ananti-epileptic drug so the global treatment could becontinued without having any other problem; twopatients are affected by epilepsy in co-morbidity andtake anti-epileptic drugs.
In this group we have not had any granulocytopenia.
We have observed a reduction in hospital admissionsafter beginning treatment with Clozapine, above all inthe male group. In 22 patients (40.7% of the group) wehaven’t had further hospital admissions. (Tab 3 and 4).
Tab 3 : Hospitalizations
TOTAL MEN WOMEN
Total number of hospitalizations 522 447 75
Before treatment with clozapine 413 354 59
After treatment with clozapine 109 93 16
Tab 4 : Patients never re-hospitalized after treatmentwith Clozapine
TOTAL 22 (41.7%)
MEN 15
WOMEN 7
DISCUSSION
Results
The reduction of hospitalizations is reported [2,3] andexplained as “effect of objective improvement of someclinical parameters and better social and jobadaptability” [4] this is consistent with the selfevaluated subjective improvement registered by ourpatients and by authors. [5]
Clozapine alone isn’t always enough. In our groupClozapine is often associated with other psychotropicdrugs and it is used as the only antipsychotic drug in19 patients; among most frequently used drugs inassociation there are other first and second generationantipsychotics.
Regarding the association between Clozapine andother antipsychotics we found that two patients of thegroup have been included in the CHAT study(experimental cohort with Clozapine enhancedassociating another antipsychotic drug, aripiprazole orhaloperidol). [6]
No patient of ours has tried or succeeded incommitting suicide so far and this is consistent withother reports [7].
Clozapine has also produced good results withpatients whose behaviour had been violent specially ina etero-directed way.
Scientific evidence shows that continuous use ofanti-psychotic drugs in schizophrenics preventsrelapses.
Compliance with treatment is important in all chronicpathologies and in our group especially an interruptionof treatment provokes various consequences, first ofall the risk of a relapse with hospitalization (up to“revolving-door” conditions) plus blockage of thepersonal therapeutic and rehabilitation project. Thereduction in hospitalization observed in our group isthe verification of good compliance with treatmentincluded the regular carrying out of their blood tests.Moreover patients have been also monitored viaanalysis of plasma levels of Clozapine.
We have begun to use metformin in some of ourpatients to control weight gain due to the treatmentwith Clozapine: so far the results appear good but thetime of observation (4 months) is too short to allow usto be more specific. [8,9]
CONCLUSION
Clozapine is an antipsychotic whose use is limited bysome side effects, some of which are potentiallydeadly.
Many clinical studies have confirmed its efficacyespecially on positive schizophrenic symptoms in thelong term treatment and in drug-resistantschizophrenia, moreover it is the antipsychotic used incase of psychoses in patients with Parkinson’sdisease. [10,11,12,13]
Our considerations, based on our clinical group, are inline with results of these studies: this is particularlyevident in pat ients who have never beenre-hospitalized after taking Clozapine notwithstandingthe gravity of their mental pathology: i.e. two women
WebmedCentral > Case Report Page 7 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
had even previously been treated with convulsivetherapy, so far both of them have had good healthsince 1995 after since using Clozapine.
REFERENCES
1. Società Italiana di Psicopatologia, ConsensusConference: Linee guida per la Farmacoterapia
della schizofrenia, Roma, 14-15 aprile 2000
2.Breier A, Buchanan RW, Irish D, Carpenter WT Jr.:Clozapine Treatment of Outpat ients WithSchizophrenia: Outcome and Long-Term ResponsePatterns. Hosp Community Psychiatry 1993; 44: 12:1145-1149
3. Meltzer HY, Burnett S, Bastani B, Ramirez LF.:Effects of Six Months of Clozapine Treatment on theQuality of Life of Chronic Schizophrenic Patients.Hosp Community Psychiatry 1990; 41: 892-897
4. Meltzer HY, Cola P, Way L, Thompson PA, BastaniB, Davies MA, Snitz Beth: Cost Effectiveness ofClozapine in Neuroleptic-Resistant Schizophrenia. AmJ Psychiatry 1993; 150: 1630-1638
5. Waserman J, Criollo: M. Subjective Experience ofClozapine Treatment by Patients With ChronicSchizophrenia. Psychiatric Services 2000; 51: 5:666-668
6. Nosè M, Accordini S, Artioli P, Barale F, Barbui C.et Alii: Rationale and Design of an IndependentRandomised Controlled Trial Evaluating theEffectiveness of Aripiprazole or Haloperidol inCombination with Clozapine for Treatment-ResistantSchizophrenia. Trials. 2009 May 15;10-31
7. Llorca PM, Perez JJ.: Leponex, 10 ans après. Unerevue clinique. L’Encéphale, 2004; XXX: 474-479
8. Schumann SA, Ewigman B.: Can Metformin UndoWeight Gain Induced by Antipsychotics? J Fam Pract.2008 Aug; 57 (8): 526-30
9.Ness-Abramof R, Apovian CM.: Drug-inducedWeight Gain. Drugs Today. 2005 Aug; 41 (8): 547-55
10. Buchanan RW, Breier A, Kirkpatrick B, Ball P,Carpenter WT Jr.: Positive and Negative SymptomResponse to Clozapine in Schizophrenic Patients Withand Without Deficit Syndrome. Am J Psychiatry 1998;155: 6: 751-760
11. Leiderman EA.: Effectiveness Trials in ChronicSchizophrenic Patients: CATIE. What can we learn?Vertex 2009; 20;(84); 129-35
12. Essali A, Al-Haj Haasan N, Li C, Rathbone J.:Clozapine vs Typical Neuroleptic Medication forSchizophrenia. Cochrane Database Syst Rev. 2009;Jan 21; (1): CD000059
13. Mercier C, Bret P,Bret MC, Queuille E.:Enquête observationellede prescription de laclozapine au centrehospitalierCharles-Perrens àBordeaux, plus de 15ans après l’AMM enFrance. L’Encéphale.2009; XXXV (4): 321-9
Ennio Piantato MD,
Servizio Psichiatrico
WebmedCentral > Case Report Page 8 of 21
WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Azienda OspedalieraNazionale SS Antonio eBiagio,
via Venezia 16
15121 Alessandria
Italy
Tel +39.01.31.20.64.10
Fax +39.01.31.20.66.16
Email: [email protected]
Francesca Sartore MD
Servizio Psichiatrico
Azienda OspedalieraNazionale SS Antonio eBiagio
Via Venezia 16
15121 Alessandria
Italy
Tel+39.01.31.20.66.12
Fax +39.01.31.20.66.16
>Email: [email protected]
Both Authors equallycontributed to this article.
WebmedCentral > Case Report Page 9 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Clozapine: does it work?
Analysis of a 15 year experience.
Ennio PIANTATO and Francesca SARTORE
ABSTRACT
This is an overview of results after a 15 year follow-upof psychotic patients treated mainly with Clozapine.We have found out that their quality of life hasimproved, they are good compliant in taking theirmedications and the number of hospitalizations isgreatly reduced after beginning treatment withClozapine.
INTRODUCTION
This report contains data about use of Clozapine inour Psychiatric Unit during the period June 1995-June2009.
Clozapine is an anti-psychotic drug created at the endof 60’s, with a particular receptor profile.
Due to some cases of granulocytopenia noted inFinland the drug was withdrawn in 1975. It wasreintroduced in the 90’s with indication for “resistantschizophrenia” and a recommendation to monitorblood cell counts. Since 1995 Clozapine has beenofficially used in Italy for “resistant schizophrenia”.
In 1995 we started using Clozapine after two of usattended a course at the Psychiatric Clinic of the BernUniversity, Switzerland.
Our Psychiatric Unit is part of a Department of MentalHealth and situated in the Alessandria general hospital,in the region of Piedmont in NW Italy, serving apopulation of 180.000 inhabitants. The unit has 15beds plus 1 bed for Day Hospital service.
Init ially Clozapine was used with so-calledtreatment-resistant schizophrenic patients, showingresistance to traditional and at least two atypicalantipsychotic treatments as reported in internationalguidelines. [1]
Afterwards the treatment with Clozapine was extendedto patients affected by non-schizophrenic disturbancessuch as bipolar disorder.
MATERIAL AND METHODS
Our report includes the group of patients currentlytaking Clozapine and attending our centre for bloodtest control. Almost all of them started Clozapine whilehospitalized in our Psychiatric Unit.
At the moment the group is made up of 54 patients: 41males (76%) and 13 females (24%).
Originally the use of Clozapine began with 6 patients(4 males and 2 females) who are still under the care ofour centre.
Average age of patients is 43±9.9 for the total group:for the male group average age is 40, for the femalegroup it is 46.
Age range is from 26 to 69 years.
All patients live at home with 8 exceptions: 6 of themlive in sheltered apartments and 1 is in a nursing home.
Regarding the diagnoses, 48 patients (88.9%) areaffected by schizophrenia, 4 (7.4%) by aschizoaffective disorder and 2 (3.7%) by bipolardisorder with psychotic behaviour. (Tab 1).
Tab 1: Diagnosis (total group)
Diagnosis TOTAL MEN WOMEN
Schizophrenia 48 37 11
Schizoaffective disorder 4 3 1
Bipolar disorder 2 1 1
Patients affected by schizophrenia are subdivided asfollows: paranoid schizophrenia (19); undifferentiateddisorder (12); disorganized schizophrenia (15);catatonic schizophrenia (1) chronic (1) (Tab 2)
WebmedCentral > Case Report Page 10 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Tab 2 : Schizophrenia sub-types
Sub-type TOTAL MEN WOMEN
Catatonic 1 1 -
Disorganized 15 11 4
Undifferentiated 12 9 3
Paranoid 19 15 4
Chronic 1 1 -
Our doses of Clozapine vary from 100 to 900 mg perday: doses are higher – usually - on discharge fromhospital (150 to 900 mg per day) then they tend todiminish to a medium 75 to 600 mg per day.
Clozapine is used as monotherapy in 19 patients(35.1%) . It’s also used in association with otherpsychotropic drugs (sometimes more than one percategory) in remaining cases: more precisely inassociation with mood-stabilizers in 19 patients,antisialorroic drugs in 4 patients, anticholinergicmedications in 19 patients, other antipsychotic drugsin 20 patients, benzodiazepines in 10 patients andantidepressants in 3 patients.
We have observed that the side effects of treatmentwith Clozapine are most frequently:-
sialorrea (excessive salivation); constipation; lowblood pressure; psychomotor slowing; weight increase;in one case an epileptic fit was controlled by adding ananti-epileptic drug so the global treatment could becontinued without having any other problem; twopatients are affected by epilepsy in co-morbidity andtake anti-epileptic drugs.
In this group we have not had any granulocytopenia.
We have observed a reduction in hospital admissionsafter beginning treatment with Clozapine, above all inthe male group. In 22 patients (40.7% of the group) wehaven’t had further hospital admissions. (Tab 3 and 4).
Tab 3 : Hospitalizations
TOTAL MEN WOMEN
Total number of hospitalizations 522 447 75
Before treatment with clozapine 413 354 59
After treatment with clozapine 109 93 16
Tab 4 : Patients never re-hospitalized after treatmentwith Clozapine
TOTAL 22 (41.7%)
MEN 15
WOMEN 7
DISCUSSION
Results
The reduction of hospitalizations is reported [2,3] andexplained as “effect of objective improvement of someclinical parameters and better social and jobadaptability” [4] this is consistent with the selfevaluated subjective improvement registered by ourpatients and by authors. [5]
Clozapine alone isn’t always enough. In our groupClozapine is often associated with other psychotropicdrugs and it is used as the only antipsychotic drug in19 patients; among most frequently used drugs inassociation there are other first and second generationantipsychotics.
Regarding the association between Clozapine andother antipsychotics we found that two patients of thegroup have been included in the CHAT study(experimental cohort with Clozapine enhancedassociating another antipsychotic drug, aripiprazole orhaloperidol). [6]
No patient of ours has tried or succeeded incommitting suicide so far and this is consistent withother reports [7].
Clozapine has also produced good results withpatients whose behaviour had been violent specially ina etero-directed way.
Scientific evidence shows that continuous use ofanti-psychotic drugs in schizophrenics preventsrelapses.
Compliance with treatment is important in all chronicpathologies and in our group especially an interruptionof treatment provokes various consequences, first ofall the risk of a relapse with hospitalization (up to“revolving-door” conditions) plus blockage of thepersonal therapeutic and rehabilitation project. Thereduction in hospitalization observed in our group isthe verification of good compliance with treatment
WebmedCentral > Case Report Page 11 of 21
WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
included the regular carrying out of their blood tests.Moreover patients have been also monitored viaanalysis of plasma levels of Clozapine.
We have begun to use metformin in some of ourpatients to control weight gain due to the treatmentwith Clozapine: so far the results appear good but thetime of observation (4 months) is too short to allow usto be more specific. [8,9]
CONCLUSION
Clozapine is an antipsychotic whose use is limited bysome side effects, some of which are potentiallydeadly.
Many clinical studies have confirmed its efficacyespecially on positive schizophrenic symptoms in thelong term treatment and in drug-resistantschizophrenia, moreover it is the antipsychotic used incase of psychoses in patients with Parkinson’sdisease. [10,11,12,13]
Our considerations, based on our clinical group, are inline with results of these studies: this is particularlyevident in pat ients who have never beenre-hospitalized after taking Clozapine notwithstandingthe gravity of their mental pathology: i.e. two womenhad even previously been treated with convulsivetherapy, so far both of them have had good healthsince 1995 after since using Clozapine.
REFERENCES
1. Società Italiana di Psicopatologia, ConsensusConference: Linee guida per la Farmacoterapia
della schizofrenia, Roma, 14-15 aprile 2000
2.Breier A, Buchanan RW, Irish D, Carpenter WT Jr.:Clozapine Treatment of Outpat ients WithSchizophrenia: Outcome and Long-Term ResponsePatterns. Hosp Community Psychiatry 1993; 44: 12:1145-1149
3. Meltzer HY, Burnett S, Bastani B, Ramirez LF.:Effects of Six Months of Clozapine Treatment on theQuality of Life of Chronic Schizophrenic Patients.Hosp Community Psychiatry 1990; 41: 892-897
4. Meltzer HY, Cola P, Way L, Thompson PA, BastaniB, Davies MA, Snitz Beth: Cost Effectiveness ofClozapine in Neuroleptic-Resistant Schizophrenia. AmJ Psychiatry 1993; 150: 1630-1638
5. Waserman J, Criollo: M. Subjective Experience ofClozapine Treatment by Patients With ChronicSchizophrenia. Psychiatric Services 2000; 51: 5:666-668
6. Nosè M, Accordini S, Artioli P, Barale F, Barbui C.et Alii: Rationale and Design of an IndependentRandomised Controlled Trial Evaluating theEffectiveness of Aripiprazole or Haloperidol inCombination with Clozapine for Treatment-ResistantSchizophrenia. Trials. 2009 May 15;10-31
7. Llorca PM, Perez JJ.: Leponex, 10 ans après. Unerevue clinique. L’Encéphale, 2004; XXX: 474-479
8. Schumann SA, Ewigman B.: Can Metformin UndoWeight Gain Induced by Antipsychotics? J Fam Pract.2008 Aug; 57 (8): 526-30
9.Ness-Abramof R, Apovian CM.: Drug-inducedWeight Gain. Drugs Today. 2005 Aug; 41 (8): 547-55
10. Buchanan RW, Breier A, Kirkpatrick B, Ball P,Carpenter WT Jr.: Positive and Negative SymptomResponse to Clozapine in Schizophrenic Patients Withand Without Deficit Syndrome. Am J Psychiatry 1998;155: 6: 751-760
11. Leiderman EA.: Effectiveness Trials in ChronicSchizophrenic Patients: CATIE. What can we learn?Vertex 2009; 20;(84); 129-35
12. Essali A, Al-Haj Haasan N, Li C, Rathbone J.:Clozapine vs Typical Neuroleptic Medication forSchizophrenia. Cochrane Database Syst Rev. 2009;Jan 21; (1): CD000059
13. Mercier C, Bret P,Bret MC, Queuille E.:
WebmedCentral > Case Report Page 12 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Enquête observationellede prescription de laclozapine au centrehospitalierCharles-Perrens àBordeaux, plus de 15ans après l’AMM enFrance. L’Encéphale.2009; XXXV (4): 321-9
Ennio Piantato MD,
Servizio Psichiatrico
Azienda OspedalieraNazionale SS Antonio eBiagio,
via Venezia 16
15121 Alessandria
Italy
Tel +39.01.31.20.64.10
Fax +39.01.31.20.66.16
Email: [email protected]
Francesca Sartore MD
Servizio Psichiatrico
Azienda OspedalieraNazionale SS Antonio eBiagio
Via Venezia 16
15121 Alessandria
Italy
Tel+39.01.31.20.66.12
Fax +39.01.31.20.66.16
WebmedCentral > Case Report Page 13 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
>Email: [email protected]
Both Authors equallycontributed to this article.
This is an overview of results after a 15 year follow-upof psychotic patients treated mainly with Clozapine.We have found out that their quality of life hasimproved, they are good compliant in taking theirmedications and the number of hospitalizations isgreatly reduced after beginning treatment withClozapine.
Introduction
This report contains data about use of Clozapine inour Psychiatric Unit during the period June 1995-June2009.Clozapine is an anti-psychotic drug created at the endof 60’s, with a particular receptor profile.Due to some cases of granulocytopenia noted inFinland the drug was withdrawn in 1975. It was
reintroduced in the 90’s with indication for “resistantschizophrenia” and a recommendation to monitorblood cell counts. Since 1995 Clozapine has beenofficially used in Italy for “resistant schizophrenia”.In 1995 we started using Clozapine after two of usattended a course at the Psychiatric Clinic of the BernUniversity, Switzerland.Our Psychiatric Unit is part of a Department of MentalHealth and situated in the Alessandria general hospital,in the region of Piedmont in NW Italy, serving apopulation of 180.000 inhabitants. The unit has 15beds plus 1 bed for Day Hospital service.Init ially Clozapine was used with so-calledtreatment-resistant schizophrenic patients, showingresistance to traditional and at least two atypicalantipsychotic treatments as reported in internationalguidelines. [1]Afterwards the treatment with Clozapine was extendedto patients affected by non-schizophrenic disturbancessuch as bipolar disorder.
Materials and Methods
Our report includes the group of patients currentlytaking Clozapine and attending our centre for bloodtest control. Almost all of them started Clozapine whilehospitalized in our Psychiatric Unit.
At the moment the group is made up of 54 patients: 41males (76%) and 13 females (24%).
Originally the use of Clozapine began with 6 patients(4 males and 2 females) who are still under the care ofour centre.
Average age of patients is 43±9.9 for the total group:for the male group average age is 40, for the femalegroup it is 46.
Age range is from 26 to 69 years.
All patients live at home with 8 exceptions: 6 of themlive in sheltered apartments and 1 is in a nursing home.
Regarding the diagnoses, 48 patients (88.9%) areaffected by schizophrenia, 4 (7.4%) by aschizoaffective disorder and 2 (3.7%) by bipolardisorder with psychotic behaviour. (Tab 1).
Our doses of Clozapine vary from 100 to 900 mg perday: doses are higher – usually - on discharge fromhospital (150 to 900 mg per day) then they tend todiminish to a medium 75 to 600 mg per day.
Clozapine is used as monotherapy in 19 patients(35.1%) . It’s also used in association with otherpsychotropic drugs (sometimes more than one percategory) in remaining cases: more precisely inassociation with mood-stabilizers in 19 patients,
WebmedCentral > Case Report Page 14 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
antisialorroic drugs in 4 patients, anticholinergicmedications in 19 patients, other antipsychotic drugsin 20 patients, benzodiazepines in 10 patients andantidepressants in 3 patients.
We have observed that the side effects of treatmentwith Clozapine are most frequently:-
sialorrea (excessive salivation); constipation; lowblood pressure; psychomotor slowing; weight increase;in one case an epileptic fit was controlled by adding ananti-epileptic drug so the global treatment could becontinued without having any other problem; twopatients are affected by epilepsy in co-morbidity andtake anti-epileptic drugs.
In this group we have not had any granulocytopenia.
We have observed a reduction in hospital admissionsafter beginning treatment with Clozapine, above all inthe male group. In 22 patients (40.7% of the group) wehaven’t had further hospital admissions. (Tab 3 and 4).
Discussion
Results
The reduction of hospitalizations is reported [2,3] andexplained as “effect of objective improvement of someclinical parameters and better social and jobadaptability” [4] this is consistent with the selfevaluated subjective improvement registered by ourpatients and by authors. [5]
Clozapine alone isn’t always enough. In our groupClozapine is often associated with other psychotropicdrugs and it is used as the only antipsychotic drug in19 patients; among most frequently used drugs inassociation there are other first and second generationantipsychotics.
Regarding the association between Clozapine andother antipsychotics we found that two patients of thegroup have been included in the CHAT study(experimental cohort with Clozapine enhancedassociating another antipsychotic drug, aripiprazole orhaloperidol). [6]
No patient of ours has tried or succeeded incommitting suicide so far and this is consistent withother reports [7].
Clozapine has also produced good results withpatients whose behaviour had been violent specially ina etero-directed way.
Scientific evidence shows that continuous use ofanti-psychotic drugs in schizophrenics preventsrelapses.
Compliance with treatment is important in all chronic
pathologies and in our group especially an interruptionof treatment provokes various consequences, first ofall the risk of a relapse with hospitalization (up to“revolving-door” conditions) plus blockage of thepersonal therapeutic and rehabilitation project. Thereduction in hospitalization observed in our group isthe verification of good compliance with treatmentincluded the regular carrying out of their blood tests.Moreover patients have been also monitored viaanalysis of plasma levels of Clozapine.
We have begun to use metformin in some of ourpatients to control weight gain due to the treatmentwith Clozapine: so far the results appear good but thetime of observation (4 months) is too short to allow usto be more specific. [8,9]
Conclusion
Clozapine is an antipsychotic whose use is limited bysome side effects, some of which are potentiallydeadly.
Many clinical studies have confirmed its efficacyespecially on positive schizophrenic symptoms in thelong term treatment and in drug-resistantschizophrenia, moreover it is the antipsychotic used incase of psychoses in patients with Parkinson’sdisease. [10,11,12,13]
Our considerations, based on our clinical group, are inline with results of these studies: this is particularlyevident in pat ients who have never beenre-hospitalized after taking Clozapine notwithstandingthe gravity of their mental pathology: i.e. two womenhad even previously been treated with convulsivetherapy, so far both of them have had good healthsince 1995 after since using Clozapine.
References
1.Società Italiana di Psicopatologia, ConsensusConference: Linee guida per la Farmacoterapiadellaschizofrenia, Roma, 14-15 aprile 20002.Breier A,Buchanan RW, Irish D, Carpenter WT Jr.: ClozapineTreatment of Outpatients With Schizophrenia:Outcome and Long-Term Response Patterns. HospC o m m u n i t y P s y c h i a t r y 1 9 9 3 ; 4 4 : 1 2 :1145-11493.Meltzer HY, Burnett S, Bastani B,Ramirez LF.: Effects of Six Months of ClozapineTreatment on the Quality of Life of ChronicSchizophrenic Patients. Hosp Community Psychiatry1990; 41: 892-8974.Meltzer HY, Cola P, Way L,Thompson PA, Bastani B, Davies MA, Snitz Beth:
WebmedCentral > Case Report Page 15 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
C o s t E f f e c t i v e n e s s o f C l o z a p i n e i nNeuroleptic-Resistant Schizophrenia. Am J Psychiatry1993; 150: 1630-1638 5.Waserman J, Criollo: M.Subjective Experience of Clozapine Treatment byPatients With Chronic Schizophrenia. PsychiatricServices 2000; 51: 5: 666-6686.Nosè M, Accordini S,Artioli P, Barale F, Barbui C. et Alii: Rationale andDesign of an Independent Randomised ControlledTrial Evaluating the Effectiveness of Aripiprazole orHaloperidol in Combination with Clozapine forTreatment-Resistant Schizophrenia. Trials. 2009 May15;10-317.Llorca PM, Perez JJ.: Leponex, 10 ansaprès. Une revue clinique. L’Encéphale, 2004; XXX:474-4798.Schumann SA, Ewigman B.: Can MetforminUndo Weight Gain Induced by Antipsychotics? J FamPract. 2008 Aug; 57 (8): 526-30 9.Ness-Abramof R,Apovian CM.: Drug-induced Weight Gain. DrugsToday. 2005 Aug; 41 (8): 547-5510.Buchanan RW,Breier A, Kirkpatrick B, Ball P, Carpenter WT Jr.:Positive and Negative Symptom Response toClozapine in Schizophrenic Patients With and WithoutDeficit Syndrome. Am J Psychiatry 1998; 155: 6:751-76011.Leiderman EA.: Effectiveness Trials inChronic Schizophrenic Patients: CATIE. What can welearn? Vertex 2009; 20;(84); 129-3512.Essali A, Al-HajHaasan N, Li C, Rathbone J.: Clozapine vs TypicalNeuroleptic Medication for Schizophrenia. CochraneDatabase Sys t Rev . 2009; Jan 21 ; (1 ) :CD00005913.Mercier C, Bret P, Bret MC, Queuille E.:Enquête observationelle de prescription de laclozapine au centre hospitalier Charles-Perrens àBordeaux, plus de 15 ans après l’AMM en France.L’Encéphale. 2009; XXXV (4): 321-9
WebmedCentral > Case Report Page 16 of 21
WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Diagnosis TOTAL MEN WOMENSchizophrenia 48 37 11Schizoaffectivedisorder
4 3 1
Bipolar disorder 2 1 1
Patients affected by schizophrenia are subdivided as follows: paranoid schizophrenia (19);undifferentiated disorder (12); disorganized schizophrenia (15); catatonic schizophrenia (1)chronic (1) (Tab 2)
Illustrations
Illustration 1
Tab 1: Diagnosis (total group)
WebmedCentral > Case Report Page 17 of 21
WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
Sub-type TOTAL MEN WOMENCatatonic 1 1 -Disorganized 15 11 4Undifferentiated 12 9 3Paranoid 19 15 4Chronic 1 1 -
Illustration 2
Tab 2 : Schizophrenia sub-types
WebmedCentral > Case Report Page 18 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
TOTAL MEN WOMENTotal number ofhospitalizations
522 447 75
Before treatment withclozapine
413 354 59
After treatment withclozapine
109 93 16
Illustration 3
Tab 3 : Hospitalizations
WebmedCentral > Case Report Page 19 of 21
WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
TOTAL 22 (41.7%)MEN 15WOMEN 7
Illustration 4
Tab 4 : Patients never re-hospitalized after treatment with Clozapine
WebmedCentral > Case Report Page 20 of 21

WMC002228 Downloaded from http://www.webmedcentral.com on 24-Sep-2011, 12:18:18 PM
DisclaimerThis article has been downloaded from WebmedCentral. With our unique author driven post publication peerreview, contents posted on this web portal do not undergo any prepublication peer or editorial review. It iscompletely the responsibility of the authors to ensure not only scientific and ethical standards of the manuscriptbut also its grammatical accuracy. Authors must ensure that they obtain all the necessary permissions beforesubmitting any information that requires obtaining a consent or approval from a third party. Authors should alsoensure not to submit any information which they do not have the copyright of or of which they have transferredthe copyrights to a third party.
Contents on WebmedCentral are purely for biomedical researchers and scientists. They are not meant to cater tothe needs of an individual patient. The web portal or any content(s) therein is neither designed to support, norreplace, the relationship that exists between a patient/site visitor and his/her physician. Your use of theWebmedCentral site and its contents is entirely at your own risk. We do not take any responsibility for any harmthat you may suffer or inflict on a third person by following the contents of this website.
WebmedCentral > Case Report Page 21 of 21