clozapine service standards - nhs greater glasgow and...
TRANSCRIPT

NHS Greater Glasgow & Clyde Mental Health Services
Clozapine Service Standards
Policy Number: MHP – SUM Oct 2013
Implementation Date: Nov 2013
First Review Date: Nov 2015
Review Frequency: Bi-Annual
The MHS Clozapine Review Group is responsible for monitoring the policy
1

NHS Greater Glasgow & Clyde Mental Health Services
Clozapine Service Standards
Contents Background Registration Prescribing Dispensing Monitoring Communication Information Governance Appendices
In patient Clozapine initiation flowchart Standard titration regimes Prescribing Clozapine in special circumstances Protocol for the management of Clozapine patients who stop smoking Clozapine Out patient prescription Community pharmacy consent form Clozapine plasma monitoring Options for initiation of Clozapine
Developed by MHS Clozapine Review Group Date approved: 9/10/13 Date of first review:
2

NHS Greater Glasgow & Clyde Mental Health Services
Clozapine Service Standards
Background The second generation antipsychotic, clozapine, is the gold standard drug of choice for treatment resistant schizophrenia. Due to its serious side effect profile and licensing restrictions there are systems and criteria that must be met to ensure its safe use. This document details the standards mental health services in NHS Greater Glasgow & Clyde are expected to meet when using Clozapine regardless of the care setting. The standards consist of the following sections 1. Registration 2. Prescribing 3. Dispensing 4. Monitoring 5. Communication 6. Information Governance 7. Appendices 1. Registration 1.1 All patients, prescribers and pharmacy departments must be registered with the monitoring service associated with the contracted clozapine supplier for NHS Scotland. The registration process is summarised in appendix 1. 1.2 Clozapine may not be prescribed or dispensed until the registration process for a patient is complete. Forms for registering patients, prescribers, pharmacies, pharmacy staff and proxies are available on the ZTAS website (www.ztas.co.uk). 1.3 The patient’s consultant psychiatrist is responsible for their registration. 1.4 Once a patient is registered for clozapine the patient should be given the "community pharmacy consent form" by their named nurse/CPN and asked to complete if they agree to their community pharmacist being informed that they are now receiving clozapine. Completed forms (appendix 6) should be returned to the address on the consent form. 2. Prescribing 2.1 All consultant psychiatrists prescribing clozapine will be registered with the current clozapine monitoring service. 2.2 Clozapine will be prescribed by or under the supervision of a consultant psychiatrist in accordance with the licensed indications for the drug. Any unlicensed prescribing of clozapine must be notified to and agreed with the clozapine monitoring service (e.g. re-challenge following a red result, concomitant treatment with chemotherapy). See appendix 3. 2.3 For in patients the approved standard titration regimes, including a blank format for bespoke regimes (available via the following link and in appendix 2a & b) will be used to initiate clozapine therapy. http://www.staffnet.ggc.scot.nhs.uk/Partnerships/MHP/Care%20Governance/Prescribing%20Management/Pages/Rx_Guidelines.aspx For out patients the titration regime indicated in the Options for Initiation of Clozapine document will used. When a patient is discharged from hospital a Clozapine out-patient prescription (appendix 5) must be sent to pharmacy along with the discharge prescription. All changes to clozapine prescriptions must be communicated to pharmacy immediately.
3

NHS Greater Glasgow & Clyde Mental Health Services
3. Dispensing 3.1 All pharmacy departments dispensing clozapine will be registered with the current clozapine monitoring service. Each registered clozapine pharmacy will have a registered clozapine pharmacist who is responsible in conjunction the Mental Health Sector Chief Technician for ensuring clozapine dispensing standards are met. 3.2 Clozapine will be dispensed in accordance with the systems and rules dictated by the marketing authorisation (license) and the clozapine monitoring service. 3.3 Each dispensary will have standard operating procedures describing the dispensing process. These will cover • The roles and responsibilities of staff • Staff training • Dispensing procedures • Use of the ZTAS system • Quarantine processes • Delivery schedules • Communication If there is no valid blood result clozapine prescriptions will not be released from quarantine. 4. Monitoring 4.1 All patients prescribed clozapine will be monitored to the level described in the marketing authorisation and the clozapine monitoring service manual. Monitoring will be undertaken at ward level for in patients and in clozapine clinics or their equivalent for out patients. 4.2 Staff working in clozapine clinics and wards will receive training on the relevant clozapine systems e.g. ZTAS and the clinical use of the drug. A training package is available from pharmacy on request and a Learnpro unit is in development. All staff within clozapine clinics will have proxy access to the monitoring services web site. 4.3 Each clozapine clinic will have written Standard Operating Procedures describing all aspects of their function e.g. • The scope of the service. Clozapine services will have a geographic rather than specialty
remit i.e. they serve all clozapine patients within a defined catchment area. • Locations & timings • Staff & grades involved • Did not attend procedures • Amber result protocols • Red result protocols • Prescription collection procedures • Use of the monitoring system web site 4.4 Full blood counts Patients on clozapine will have full blood count measurements taken to the following schedule Baseline for registration Weekly For a minimum of 18 weeks from start Fortnightly From the end of weekly monitoring up to a minimum of 52
weeks Every 4 weeks For as long as treatment continues post 52 weeks
4

NHS Greater Glasgow & Clyde Mental Health Services
Twice weekly If an amber result is obtained. Continue until green Daily If a red result is obtained. Continue until two successive
green results Note: Patients may only progress from weekly to fortnightly or fortnightly to 4 weekly full blood counts if authorised by the clozapine monitoring service. Clozapine clinics and wards must have reliable processes for ensuring clozapine full blood counts are taken as scheduled. Full blood counts are normally sent to the clozapine monitoring service’s laboratory for analysis. If samples are analysed locally it is the responsibility of the ward or clozapine clinic to transmit the result to the clozapine monitoring service. Clozapine discontinuation full blood count monitoring will be undertaken as described in the ZTAS manual. 4.5 Physical Health Monitoring All patients on clozapine, regardless of setting, will be offered monitoring for physical health problems to the standards described in the table on the following page. Clear communication and joint working between mental health services and primary care will be required to ensure any physical health issues identified are appropriately managed. The standards below are those produced national by SGHD in 2013. http://www.sehd.scot.nhs.uk/cmo/CMO(2013)12.pdf
5

NHS Greater Glasgow & Clyde Mental Health Services
Parameter/test Frequency Action if outside reference range
Full Blood Count Follow manufacturer’ s mandatory protocol
BMI Baseline, weight during initiation, 3 monthly for 1 year, then annually.
Offer lifestyle advice.
Plasma glucose (fasting) Baseline, at 1 month, then from 3 months, 3 monthly up to 1 year, then 6 monthly
Offer lifestyle advice. Obtain HbA1c. Consult with GP and/or specialist as appropriate.
Blood lipids Baseline, 3 monthly for 1 year, then 6 monhtly.
Offer lifestyle advice and consult with GP and/or specialist for consideration of treatment e.g. statin therapy as appropriate.
Blood pressure Baseline and as per initiation protocol, 3 monthly for 1 year, then annually. Also following dose changes.
If hypotensive:.Consider slower titration or dose reduction If Hypertensive: Offer lifestyle advice and consult with GP and/or specialist for consideration of treatment.
Pulse Baseline and as per initiation protocol, at 3 months, then annually
Consider slower titration or dose reduction. If tachycardia persistent, observe for other indicators of myocarditis or cardiomyopathy.
ECG Baseline, at 3 months and then annually. Act on abnormality according to significance, clinical indication. Refer to cardiologist if in doubt.
Urea & electrolytes Baseline then as clinically indicated. Investigate as clinically appropriate.
Liver function tests Baseline then annually or more frequently if clinically indicated.
Investigate as clinically appropriate.
Side-effects “ GASS for Clozapine” ocognised side-effect questionnaire for antipsychotic medication during initiation and regularly thereafter, with general side-effect enquiry at least at any point of blood sampling, with specific reference to constipation
As clinically appropriate.
Smoking status On initiation and at regular intervals thereafter, at least annually. Warn patient regarding effect of changes in smoking status.
Check Clozapine level and GASS for Clozapine if change of status.
Women of reproductive age Pregnancy/contraceptive status on initiation and at regular intervals thereafter, at least annually
In all cases: Pre-pregnancy discussion of pregnancy intentions. Offer advice/signposting on contraception. Early discussion of options if unplanned pregnancy.
4.6 Side effect monitoring Clozapine clinics and wards will perform additional side-effect monitoring relevant to clozapine as a matter of routine. This will include • Blood pressure • Pulse • Constipation • Hypersalivation
6

NHS Greater Glasgow & Clyde Mental Health Services
• Sedation • Incontinence • Signs of neutropenia – sore throat, temperature & flu like symptoms • Fits, faints & funny turns Clinical observation and the Glasgow Antipsychotic Side-effect Scale – clozapine variant should be used for this. GASS should be undertaken every 6 months and one month after a dose change. Side-effect assessments will be recorded formally and reported systematically to the multi-disciplinary team. 4.7 Clozapine plasma level monitoring Clozapine clinics and wards will perform clozapine plasma level monitoring in line with MHS guidance at the request of a consultant psychiatrist. The main indications for clozapine plasma level monitoring are • To monitor compliance • In poor responders after an adequate trial especially prior to consideration of augmentation
strategies • If dose reduction is being contemplated • To support the diagnosis of dose-related side effects* • If a drug interaction is suspected • Non-urgent investigation of suspected overdose • If the patient’s smoking status changes • Measuring baseline levels during successful treatment to use as a reference point. *Side effects that are thought to be dose-related include; sedation, dizziness, hypersalivation, tachycardia, postural hypotension, constipation and seizures. Often these can be avoided/minimised by careful and slow dose escalation or alleviated by reducing the dose. The table in appendix 7 gives some advice on how to manage high clozapine plasma levels. 5. Communication 5.1 To ensure safe and effective use of clozapine there must be effective communication between the elements of the clozapine service. This includes the patient, their consultant psychiatrist, the pharmacy, clozapine clinics, wards and the clozapine monitoring service. Each clozapine patient’s care plan will contain the relevant communication pathway with regards to their clozapine service and should include contact details for • Consultant psychiatrist • Clozapine pharmacy • Clozapine clinic • GP practice • Community pharmacy GPs should be informed when Clozapine is prescribed or treatment is stopped and encouraged to add Clozapine to their prescribing records using the process developed by the prescribing support team. 5.2 The clozapine monitoring service (ZTAS) send alert faxes to the clozapine pharmacist and consultant psychiatrists. The table below lists these alerts and indicates the actions and responsibilities associated with them.
7

NHS Greater Glasgow & Clyde Mental Health Services
Alert fax Actions & Responsibilities Eligibility reminders Pharmacy contact consultant & CMHT, ward to advise of move to
fortnightly or monthly bloods & supplies. Late reminders Consultant, ward or CMHT to organise urgent local FBC Discontinuation notification
Pharmacy to cancel prescription Consultant, ward or CMHT to organise discontinuation bloods
Non-Rechallengeable Consultant to place in case record – indicates genuine red result therefore any future clozapine treatment unlicensed and must be approved by ZTAS
Amber warning Consultant, ward or CMHT to organise twice weekly FBC until green Red Alert Clozapine treatment stopped.
Pharmacy to contact consultant, ward or CMHT to confirm red alert. Consultant, ward or CMHT to organise urgent local FBC on a daily basis until two consecutive greens. Implement appropriate care as per ZTAS manual
Downward trend/single drop
Consultant, ward or CMHT review recent blood history and physical status and if appropriate undertake additional blood tests
Out of range warning – high eosinophils or low platelets
Review patient urgently. FBC twice a week. High eosinophils – stop clozapine until eosinophils less than 1. Monitor cardiac function including ECG. Low platelets – stop clozapine until levels greater than 50.
6. Information governance 6.1 The clozapine monitoring service and their website (ZTAS) are essential to the safe use of clozapine. ZTAS must be notified immediately and then the clozapine pharmacy informed in the following circumstances to ensure the data they hold is up to date and accurate. Data item Responsible person(s) for notifying ZTAS &/or
clozapine pharmacy New registration or re-titration Medical staff Apply & maintain clozapine PIMS alert CMHT staff - system still in development Change of consultant Medical staff Change of blood sampling location Clozapine clinic or ward staff Treatment break Medical staff or Clozapine clinic or ward staff Treatment discontinuation Medical staff Off label treatment e.g. red re-challenge, concomitant chemotherapy
Medical staff
Local blood sample Clozapine clinic or ward staff Forms for communicating with ZTAS are available on their website.
8

NHS Greater Glasgow & Clyde Mental Health Services
Appendix 1 In patient clozapine initiation flowchart
Full blood count (FBC) with differential (valid for
10 days) ECG, baseline lipids, glucose, weight, LFTs &
U&Es
Registration form completed and signed by consultant.
Forms are available on the log in page of the ZTAS website www.ztas.co.uk
Faxed to ZTAS on 02073655843.
Once confirmation of the registration is received from ZTAS, pharmacy will make an initial supply the amount of which will depend on the validity of the initial FBC.
If registration FBC is no longer valid pharmacy will contact ward for an urgent local FBC.
Day 1 of the titration should ideally be a Monday and clozapine should not be initiated over a weekend.
Monitor the patient as described in the titration regime.
This blood test is essential to allow weekly dispensing of clozapine.
Pharmacy will dispense the remainder on the titration regime to the appropriate schedule.
This blood test is essential to allow on-going weekly dispensing of clozapine.
The post titration regular dose should be prescribed on the in patient prescription sheet and this should be sent to pharmacy for a weeks supply of the post titration dose.
Every time the dose is changed the altered in patient prescription sheet must be sent to pharmacy.
*(http://www.staffnet.ggc.scot.nhs.uk/Partnerships/MHP/Care%20Governance/Prescribing%20Management/Pages/Rx_Guidelines.aspx) Note: When a local blood sample is taken it is the responsibility of the ward to communicate the result of this sample to ZTAS and pharmacy. Do not commence a clozapine titration out of hours.
Perform all pre-treatment tests required for clozapine
Register patient with ZTAS
Send titration regime & in patient prescription sheet to pharmacy (available
on MH Staffnet pages)*
Commence patient on clozapine as described in the protocol
Day 2 take first ‘on treatment FBC’ and send to ZTAS or local labs for
analysis
Initiate weekly FBC for the patient preferably on a Monday or Tuesday
to facilitate on going weekly dispensing each Friday
9

NHS Greater Glasgow & Clyde Mental Health Services
Appendix 2a Clozapine Titration Regime
Name: Ward: CHI Number: Consultant:
Day Date 8am Administered by 10pm Administered
by
1 12.5mg - -
2 12.5mg 12.5mg 3 12.5mg 25mg 4 25mg 25mg 5 25mg 50mg 6 25mg 75mg 7 25mg 75mg 8 50mg 75mg 9 50mg 100mg 10 50mg 100mg 11 50mg 125mg 12 75mg 125mg 13 100mg 125mg 14 100mg 150mg
15 100mg 175mg
Date Titration Commenced: Prescribing Doctor’s signature:
10

NHS Greater Glasgow & Clyde Mental Health Services
Important Information for Nursing Staff
• This titration regime must also be prescribed by medical staff on the mental health prescription sheet as:- “ As per Clozapine titration regime”
• Nursing staff must monitor for effect and side effects during titration [monitor blood pressure, pulse,
respiration and temperature] – and liaise with medical staff accordingly. * Should it be deemed necessary that a slower titration is required, this regime must be discontinued on the prescription sheet. Clozapine should then be prescribed as all other medications are prescribed and prescription dosages altered when required on the prescription sheet. Alternatively the blank titration regime may be used. • After initial 15-day titration is complete, Clozapine can then be prescribed routinely on the prescription
sheet.
Prescribe as suggested by ZTAS recommendations: 8am 10pm Days 16 – 20 100mg 200mg Days 21 – 24 100mg 250mg Days 25 – 29 100mg 300mg Or as per. Consultant’s prescription [Maintenance, reductions and increases thereafter as per. Consultants instructions]
• This regime is to be stapled to the reverse side of the current prescription kardex whilst in use then filed in case notes when complete.
All nursing staff must be aware of side effects of Clozapine & to be alert for signs and symptoms of infections, refer to ZTAS guidance at all times.
11

NHS Greater Glasgow & Clyde Mental Health Services
Appendix 2b Clozapine Titration Regime
Name: Ward: CHI Number: Consultant:
Day Date 8am Administered by 10pm Administered
by
1 -
2 3 4 5 6 7 8 9 10 11 12 13 14
15
Date Titration Commenced: Prescribing Doctor’s signature:
12

NHS Greater Glasgow & Clyde Mental Health Services
Important Information for Nursing Staff
• This titration regime must also be prescribed by medical staff on the mental health prescription sheet
as:- “ As per Clozapine titration regime” • Nursing staff must monitor for effect and side effects during titration [monitor blood pressure, pulse,
respiration and temperature) as per options for initiation document (appendix 8) and liaise with medical staff accordingly.
* Should it be deemed necessary that a slower titration is required, this regime must be discontinued on the prescription sheet. Clozapine should then be prescribed as all other medications are prescribed and prescription dosages altered when required on the prescription sheet. Alternatively the blank titration regime may be used. • After initial 15-day titration is complete, Clozapine can then be prescribed routinely on the prescription
sheet.
The dose should be increased at a rate determined by the patient’s response and their susceptibility to side effects.
• This regime is to be stapled to the reverse side of the current prescription kardex whilst in use then filed in case notes when complete.
All nursing staff must be aware of side effects of Clozapine & to be alert for signs and symptoms of infections, refer to ZTAS guidance at all times.
13

NHS Greater Glasgow & Clyde Mental Health Services
Appendix 3 Prescribing clozapine in special circumstances
Clozapine is an effective therapy for treatment resistant schizophrenia. Unfortunately it can cause neutropenia and agranulocytosis and consequently there are mandatory registration and monitoring parameters in place to support the safe use of this drug. As a general rule, clozapine should not be prescribed in combination with other drugs known to suppress white blood cell production e.g. carbamazepine, chloramphenicol, co-trimoxazole, penicillamine, cytotoxic agents and depot antipsychotics. However, it is acknowledged that occasionally some patients who are treated with clozapine may need to receive short term or episodic treatment with otherwise contra-indicated agents e.g. chemotherapy or interferon. In such cases if there would be significant detriment to the patient’s health from discontinuing clozapine then, subject to approval from the clozapine monitoring service, a special treatment plan may be agreed to allow concomitant treatment. Essentially, this plan recognises that the suppression in white blood cells is due to the special treatment and not the clozapine and adjusts the monitoring requirements accordingly. The following describes the steps to be followed should such circumstances arise 1. As soon as a consultant psychiatrist becomes aware that their patient may be about to start
a course of treatment with chemotherapy, interferon treatment or similar drugs they should contact their local clozapine dispensary and ZTAS (clozapine monitoring service) to make them aware of this.
2. In conjunction with the doctor responsible for the relevant treatment (oncologist,
haematologist, gastro-enterologist etc) an agreed written treatment plan should be developed containing the following details (please see note 1 from the ZTAS SOPs below)
• The indication for the required treatment • The drug being used • The likely treatment course with a provisional end date • The likely impact of this treatment on clozapine haematological factors (white cells,
neutrophils and platelets) • The haematological factors threshold below which it would not be appropriate to
continue clozapine treatment (in the absence of any other treatment clozapine is stopped if the total white cell count falls below 3 and the neutrophils below 1.5).
• An indication of any other additional monitoring required 3. Once the treatment plan has been agreed locally it should be sent to ZTAS who will review it
and then give their consent to a variation to the monitoring requirements for the patient. A copy of the treatment plan should also be sent to the local clozapine dispensary.
4. If any changes are made to the treatment plan they should be communicated to ZTAS and
pharmacy as soon as possible. 5. ZTAS and pharmacy should be informed as soon as the treatment course ends, as the
patient will then revert to standard clozapine monitoring. Andrew Walker Lead Clinical Pharmacist. May 2011
14

NHS Greater Glasgow & Clyde Mental Health Services
Note 1 The following is additional advice from ZTAS. The ZTAS SOPs state that any re-challenge or decision to keep a patient from going to non-re-challengeable during concomitant treatment MUST be approved by a Consultant Haematologist. In this situation the treatment is not considered “off-label”. If a Consultant Haematologist does not provide/counter-sign the patient’s treatment plan, the clozapine treatment will be considered “off-label” and a statement to the effect of the following must be signed by the Consultant Psychiatrist and the additional treating physician: The consultant should explicitly mention that he/she is willing to take full responsibility of the patient’s medical situation for off-label treatment and that he/she absolves Leyden Delta from any liability should the patient’s condition deteriorate during Zaponex treatment. Should the off-label treatment occur as a temporary situation, e.g. use of concomitant medication that also effects blood results, ZTAS should be informed of the duration of the concomitant treatment. It is, of course, still possible for the treating team to complete a “ZTAS Haematologist Consultation Form” to be considered by our ZTAS Haematologist and Medical Advisor on a case-by-case basis.
Appendix 4 Protocol for the management of clozapine patients who stop smoking
Background
15

NHS Greater Glasgow & Clyde Mental Health Services
Tobacco smoke contains polycyclic aromatic hydrocarbons that increase the activity of certain hepatic enzymes especially CYP1A2. For patients who smoke this means that some drugs including clozapine undergo increased metabolism and consequently reduced plasma levels. This means a higher dose may be necessary to achieve a therapeutic effect. The effect of smoking is dose related i.e. the more cigarettes smoked the greater the enzyme induction. This also means that any reduction in the number of cigarettes smoked per day may result in increased clozapine plasma levels. This is worth bearing in mind should a patient begin to reduce their smoking in preparation for a quit attempt. When a patient stops smoking the increased enzyme activity reduces over a week or so. Once the enzyme activity returns to normal the dose of clozapine the patient is taking may be too high resulting in unwanted dose related side effects e.g. sedation, dizziness, hypersalivation, tachycardia, postural hypotension, constipation and seizures. The Maudsley Guidelines suggest the mean increase in plasma levels is 50% but as this is an average figure the actual increase could be lower or higher than this. For patients on clozapine who smoke and are also prescribed valproate, if they stop smoking the increase in clozapine plasma levels seen may be greater than that seen in patients not taking valproate. With the introduction of a smoke free environment in mental health patients will be compelled to stop smoking and therefore those on clozapine need to be carefully managed. This protocol describes the steps to be taken when a patient on clozapine stops smoking. 1. Take a clozapine plasma level before the patient stops smoking. Note this must be a trough
level (take in the morning before the next clozapine dose) and the results of clozapine plasma assays take about a week to come back from Magna Labs.
2. One week after stopping repeat the clozapine plasma level. During that initial week observe
the patient for dose related side effects. If any emerge, consider reducing the clozapine dose gradually to around 75% of the pre-quit dose. If the dose is reduced take the post-quit plasma level one week after the dose is stable.
3. Depending on the result of the post-quit plasma level consider further dose reductions on a
weekly basis. Subsequent plasma levels should be taken one week after any dose change. 4. Seek advice from pharmacy over interpretation of clozapine plasma assay results. It should be remembered that this ban on smoking is only enforceable whilst the patient remains in hospital. On discharge they may resume smoking. It is good practice to regularly ask patients about their smoking status and to review their clozapine dose accordingly. References: Maudsley Prescribing Guidelines in Psychiatry 11th Edition
16

NHS Greater Glasgow & Clyde Mental Health Services
Appendix 5 CLOZAPINE OUT PATIENT PRESCRIPTION REQUEST FORM
Patient’s Name: Consultant Clozapine Registration Number Collection address CHI number (10 digits)
Professional Check by;
Number:
START DATE*
DRUG FORM DOSE MORN ING
LUNCH TIME
TEA TIME
NIGHT STOP DATE*
DATE QUANTITY SUPPLIED
DISP BY
CHECK BY
A B C D E F
* To be used during dose escalation (see guidance notes) Compliance aid required Y / N
Date prescribed
Doctor’s signature
Date to commence
Doctors’ name (print)
17
NHS Greater Glasgow & Clyde Mental Health Services
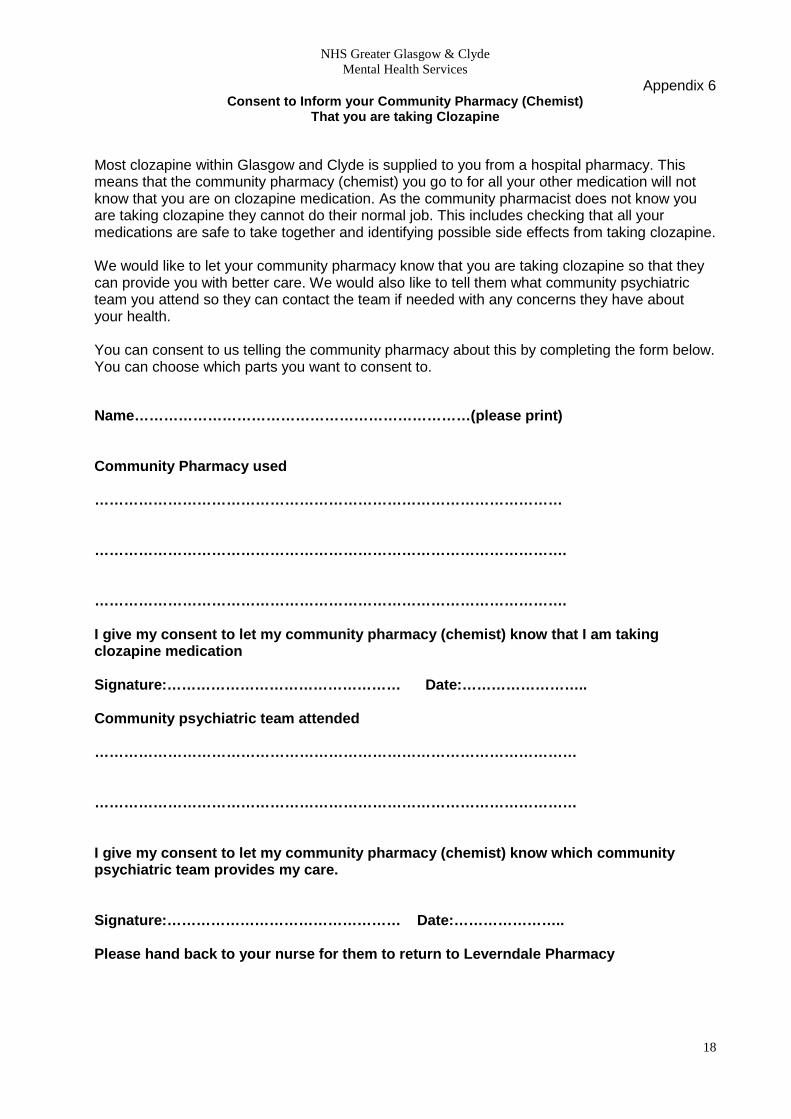
Appendix 6 Consent to Inform your Community Pharmacy (Chemist)
That you are taking Clozapine
Most clozapine within Glasgow and Clyde is supplied to you from a hospital pharmacy. This means that the community pharmacy (chemist) you go to for all your other medication will not know that you are on clozapine medication. As the community pharmacist does not know you are taking clozapine they cannot do their normal job. This includes checking that all your medications are safe to take together and identifying possible side effects from taking clozapine. We would like to let your community pharmacy know that you are taking clozapine so that they can provide you with better care. We would also like to tell them what community psychiatric team you attend so they can contact the team if needed with any concerns they have about your health. You can consent to us telling the community pharmacy about this by completing the form below. You can choose which parts you want to consent to. Name……………………………………………………………(please print) Community Pharmacy used …………………………………………………………………………………… ……………………………………………………………………………………. ……………………………………………………………………………………. I give my consent to let my community pharmacy (chemist) know that I am taking clozapine medication Signature:………………………………………… Date:…………………….. Community psychiatric team attended ……………………………………………………………………………………… ……………………………………………………………………………………… I give my consent to let my community pharmacy (chemist) know which community psychiatric team provides my care. Signature:………………………………………… Date:………………….. Please hand back to your nurse for them to return to Leverndale Pharmacy
18

NHS Greater Glasgow & Clyde Mental Health Services
When is it appropriate to measure clozapine plasma levels?
How do I interpret the result?
• To monitor compliance • In poor responders after an
adequate trial • If dose reduction is being
contemplated • To diagnose dose-related side
effects • If a drug interaction is
suspected • Non urgent investigation of
suspected overdose • If the patient’s smoking status
changes • Measuring baseline levels during
successful treatment to use as a reference point
Level = 0mg/L Review patient – if dose >50mg/day suggests no clozapine taken for up to a week before sampling
Level <0.35mg/L If response good maintain current dose.
If response poor review and address issue of compliance. If compliance OK, consider cautious dose increase and repeat assay after 1 week.
Level 0.35 – 0.6mg/L If response good maintain current dose. If side effects present and are serious or persistent consider cautious dose reduction. If response poor and there has been an adequate trial consider cautious dose increase or augmentation
Level 0.6 – 1.0mg/L If response good review current dose and consider cautious dose reduction if mental state allows. Consider sodium valproate as prophylaxis against seizures. If response poor cautiously reduce dose to bring level down below 0.6mg/L. Monitor mental state and repeat level at least 1 week after dose reduction.
Level 1.1 – 1.9mg/L If response good with no signs of toxicity review dose and consider cautious dose reduction to bring level below 1 and possibly below 0.6mg/L. Consider sodium valproate as prophylaxis against seizures. If response poor cautiously reduce dose to bring level down below 1 and possibly below 0.6mg/L. Monitor mental state and repeat level at least 1 week after dose reduction. Plasma clozapine may continue to rise in the short term even after dose reduction commenced.
Level 2mg/L & above If response good with no signs of toxicity URGENT REVIEW and consider cautious dose reduction if mental state allows. Consider sodium valproate as prophylaxis against seizures. If response poor URGENT REVIEW and dose reduction. If patient in the community consider admitting. Stop clozapine for 24 hours and re-start at 75% of last dose and reduce dose by 25mg per week to bring plasma clozapine below 1 and possibly below 0.6mg/L. Monitor mental state and repeat level at least 1 week after dose reduction. Plasma clozapine may continue to rise in the short term even after dose reduction commenced.
Note: Contact a clinical pharmacist for advice & help interpreting levels.
19

NHS Greater Glasgow & Clyde Mental Health Services
Options for the initiation of clozapine
Background A review of clozapine services in NHS Greater Glasgow & Clyde undertaken in 2011 recommended that out patient clozapine initiation be adopted as standard. However whilst seeing this as potentially desirable the Mental Health Services Governance group requested that an options paper be prepared describing a range of solutions for the initiation of clozapine treatment. This paper has been prepared by a subgroup of the MHS Clozapine Review Group and is endorsed by the overall group. The options described are those that services with appropriate resources, planning and co-ordination can implement. It should be noted these options relate to new patients starting clozapine not re-titration of existing patients after a treatment break. Standards The group believes that it is a fundamental standard that the minimum monitoring parameters must apply to all patients starting clozapine regardless of where that might be. The monitoring will be mandatory and that requirement has influenced the options described in this document. The monitoring standards are as follows 1. Mandatory full blood count monitoring as required by the clozapine marketing authorisation. 2. Cardiac parameters as describe in the following table Day Parameters Frequency 1 Temperature, pulse, blood pressure (standing &
lying) Immediately before dose then hourly for 6 hours
2 Temperature, pulse, blood pressure (standing & lying)
Immediately before dose then after 2 and 6 hours
3 - 15 Temperature, pulse, blood pressure (standing & lying)
Immediately before dose then after 6 hours
It is also recommended that patients be assessed daily for evidence of dizziness, drowsiness, hypersalivation, constipation and urinary problems. Any abnormal parameters or emerging side effects must be reported to medical staff immediately. For community based initiation, during days 1 & 2, it is advisable that the patient remain in the monitoring area, for the remainder of the titration they may leave and return after 6 hours for monitoring. If they leave they should be advised to contact the service immediately if they experience any unusual symptoms. Options The group believes there are three feasible options for the initiation of clozapine 1. Hospital admission. This is standard practice at present and will remain necessary for many patients. With the exception of ensuring in patient services observe the monitoring standards the group will not comment further on this option.
20
NHS Greater Glasgow & Clyde Mental Health Services
2. Shared Care This option represents a flexible solution that incorporates brief admission (of varying duration) and early transfer to a community based approach. Patient assessment, planning and properly resourced community services will be essential to the success of this option. The elements of this option are • Pre-assessment, patient selection and registration within Community Mental Health Teams • Short term admission to hospital. • Discharge to community support when clinically appropriate (minimum of three days after
commencing clozapine). 3. Community initiation Where patient assessment deems it appropriate clozapine treatment may be commenced in a community setting, this may be achieved either by attending a resource centre on a daily basis or in the patient’s home. It is the responsibility of the community mental health team to ensure they can safely deliver this option within the resources that they have available. With this option treatment must always commence on a Monday. The following issues are associated with this option • Patient assessment • Resources – staffing and infrastructure For options 2 & 3 where there is a community component to the titration there must be a named individual who is responsible for co-ordinating the process. Their role will include • Communication with RMO, Pharmacy, the ward as appropriate • Identifying who is seeing patient where and when • Ensuring the patient and their carers/relatives have all the relevant information including
information about the drug, services and how to get support routinely and in an emergency etc
There is an expectation that community services within the CHP including Crisis or similar services will provide support to deliver community based clozapine initiation. Patient assessment/selection To be eligible for option 2 or 3 patients must be assessed against the following criteria • Patients must meet the licensed indications for community clozapine initiation (see the
Summary of Product Characteristics) • Patients should be considered suitable for out patient care in view of their current symptoms
and safety risk. A thorough clinical assessment will be undertaken to determine suitability. • Prior to treatment patients should be counselled and given standard information on
clozapine treatment (ZTAS patient booklet & Choice and Medication literature) and then give consent (documented in care notes) to clozapine treatment and blood testing. Details of information provided should be recorded in the care notes. Patients must be aware of and agree to the requirement for attendance at a local mental health base in some circumstances, for daily home visits or that admission to local mental health hospital may be
21
NHS Greater Glasgow & Clyde Mental Health Services
required. It is the responsibility of the multi-disciplinary team to ensure that patients are appropriately informed of the relevant aspects of Clozapine treatment.
• An adequately resourced healthcare team must be in place. • Sites should consider their capacity to support community initiation. • It is advised that the patient is not left alone during the first week of treatment. Ideally
someone (family/social carer) should stay overnight with the patient during that period.
• Patients must be able to contact the clinical team and out of hours support at all times (for
option 2 from discharge onwards). If they can’t then admission is the only option. • Community initiation will not be appropriate for patients with a history of diabetes, cardiac
disease, seizures or neuroleptic malignant syndrome or where they continue to misuse alcohol or drugs.
• Mandatory pre-treatment screening will be undertaken by the community mental health team
and is primarily a medical responsibility and will include
Full medical history particularly: diabetes, cardiovascular, seizure, or haematological disorders. Smoking status, use of caffeine. Baseline measurement of mental state using a standardised tool e.g. CGI Full physical examination including: weight, pulse, temperature, and blood pressure (standing and lying), and recent electrocardiogram (ECG). Recent is defined as within the last 6 months assuming no change in cardiac status or risk factors. If anything has changed an ECG should be performed as part of the pre-assessment process. Baseline blood screening: full blood count including differential white cell count, liver function tests, random plasma glucose, lipids, blood pressure, pulse, weight, urea and electrolytes. Registration with the clozapine monitoring service currently ZTAS. Where any of the following circumstances apply titration in hospital is recommended - Patient has significant difficulties in tolerating regime - Patient continues to misuse alcohol/substances - Patient or carer requests Hospital admission due to deterioration in mental state - Titration cannot be fully undertaken due to service demands
Prescribing Standard clozapine titration regimes are used for in patient services. The group recommends that a standard prescription be adopted for options 2 & 3. Due to the constraints of community initiation that regime will differ from the in patient regime and will be as follows Day Dose 1 Monday 12.5mg in the morning 2 Tuesday 25mg in the morning 3 Wednesday 37.5mg in the morning
22

NHS Greater Glasgow & Clyde Mental Health Services
4 Thursday 50mg in the morning 5 Friday 75mg in the morning 6 Saturday 75mg in the morning 7 Sunday 75mg in the morning 8 Monday 100mg in the morning 9 Tuesday 100mg in the morning & 25mg in the evening 10 Wednesday 100mg in the morning & 50mg in the evening 11 Thursday 100mg in the morning & 50mg in the evening 12 Friday 100mg in the morning & 75mg in the evening 13 Saturday 100mg in the morning & 75mg in the evening 14 Sunday 100mg in the morning & 75mg in the evening 15 Monday 100mg in the morning & 100mg in the evening Please note that for option 3 treatment must commence on a Monday. Implications & issue for each option Option Implications & issues Comments Hospital Admission Only issue is in delayed access
to a bed for a planned admission to initiate clozapine.
Status quo option. Excessive delays could raise issues with meeting waiting times for treatment.
Community Team resources Environment Monitoring at weekends Systems development Support networks
Patient preference
Shared care As for community option plus Planning & co-ordination Communication Delayed access to a bed
Appendix 1
Pre clozapine physical and baseline blood screening
Date/sign
Results
Blood test; FBC
U&E’s LFT
Random Glucose Lipids
ECG History of ?Renal disease
23

NHS Greater Glasgow & Clyde Mental Health Services
?liver disease ?Cardiac disease ?Neutropenia ?Agranulocytosis ?Bone marrow disorder ?GI disease ? PTE or DVT Epilepsy Active alcoholism Glaucoma BP Pulse Temperature Baseline weight & measured height
Smoking status Pregnancy status List of medication/history of compliance
Sort paperwork and complete ZTAS registration
Diagnosis appropriate Confirm patients understanding , consent and commitment
Complete clozapine titration prescription
Fax first week’s prescription to Leverndale pharmacy
Suitable for community clozapine initiation; YES/NO Planned start date; Keyworker informed; Crisis team informed;
Appendix 2
CLOZAPINE CLINIC CONTACT INFORMATION
Treatment centre-
Patient Label with chi
24

NHS Greater Glasgow & Clyde Mental Health Services
Telephone- Monday to Friday – 9am to 5pm Out with these hours, in case of Emergency, Crisis Team- Out of Hours Service- Very common side effects are : • Drowsiness • Dizziness • Fast heartbeat • Constipation • Increased production of saliva. You Must ; Tell doctor/nurse immediately before taking the next clozapine tablet: • if you get signs of a cold, fever, flu-like symptoms, sore throat or any other infection. • if you feel unwell in any way • if you have constipation.
25

NHS Greater Glasgow & Clyde Mental Health Services
Appendix 3 Clozapine initiation in-patient observation record
Surname Forename Date of birth CHI number Consultant
Baseline Recordings Date
BP Pulse Weight Temp
DAY 1 Before
am dose
10 (1 hour post dose)
20 30 40 50 60 Before pm dose
Time
Temp
Pulse
BP (lying)
BP (stand)
DAY 2 Before am
dose 20 60 Before pm
dose
Time Temp Pulse BP (lying) BP (stand)
DAY 3 Before am dose
60 Before pm dose
DAY 4 Before am dose
60 Before pm dose
Time Time Temp Temp Pulse Pulse BP (lying)
BP (lying)
BP (stand)
BP (stand)
DAY 5 Before
am dose 60 Before
pm dose DAY 5 Before
am dose 60 Before
pm dose
Time Time Temp Temp Pulse Pulse BP (lying)
BP (lying)
BP (stand)
BP (stand)
26
NHS Greater Glasgow & Clyde Mental Health Services
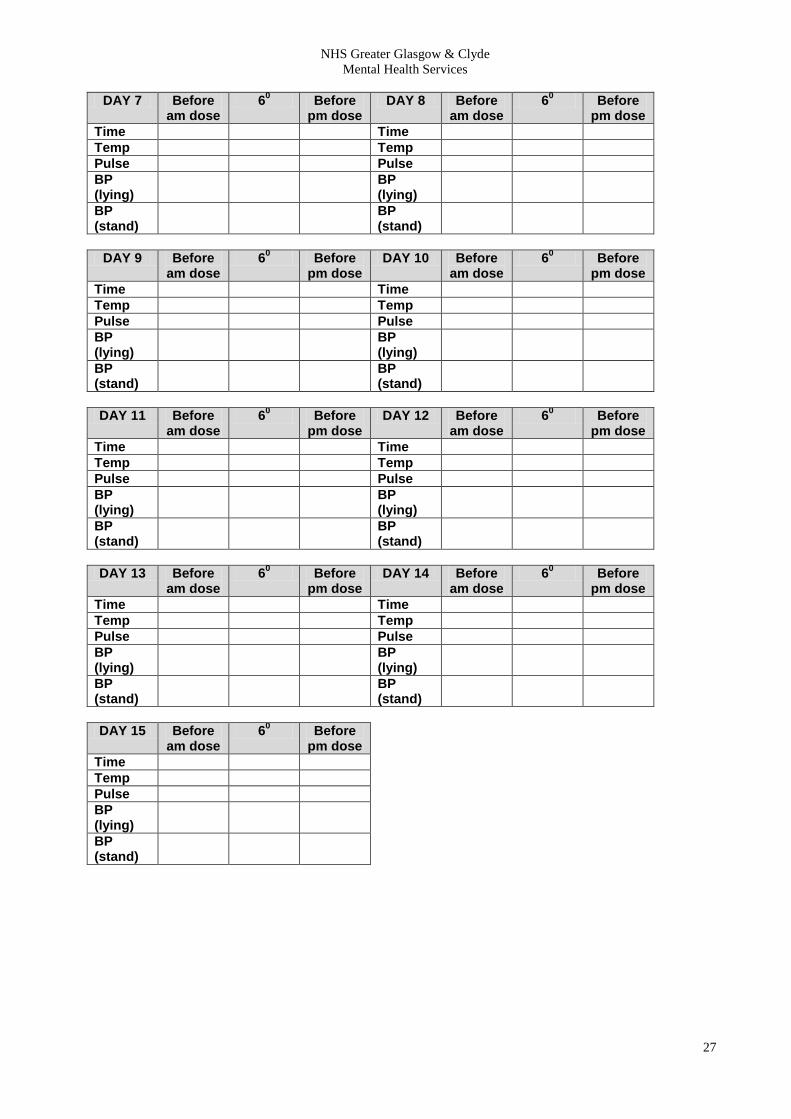
DAY 7 Before
am dose 60 Before
pm dose DAY 8 Before
am dose 60 Before
pm dose
Time Time Temp Temp Pulse Pulse BP (lying)
BP (lying)
BP (stand)
BP (stand)
DAY 9 Before
am dose 60 Before
pm dose DAY 10 Before
am dose 60 Before
pm dose
Time Time Temp Temp Pulse Pulse BP (lying)
BP (lying)
BP (stand)
BP (stand)
DAY 11 Before
am dose 60 Before
pm dose DAY 12 Before
am dose 60 Before
pm dose
Time Time Temp Temp Pulse Pulse BP (lying)
BP (lying)
BP (stand)
BP (stand)
DAY 13 Before
am dose 60 Before
pm dose DAY 14 Before
am dose 60 Before
pm dose
Time Time Temp Temp Pulse Pulse BP (lying)
BP (lying)
BP (stand)
BP (stand)
DAY 15 Before
am dose 60 Before
pm dose
Time Temp Pulse BP (lying)
BP (stand)
27

NHS Greater Glasgow & Clyde Mental Health Services
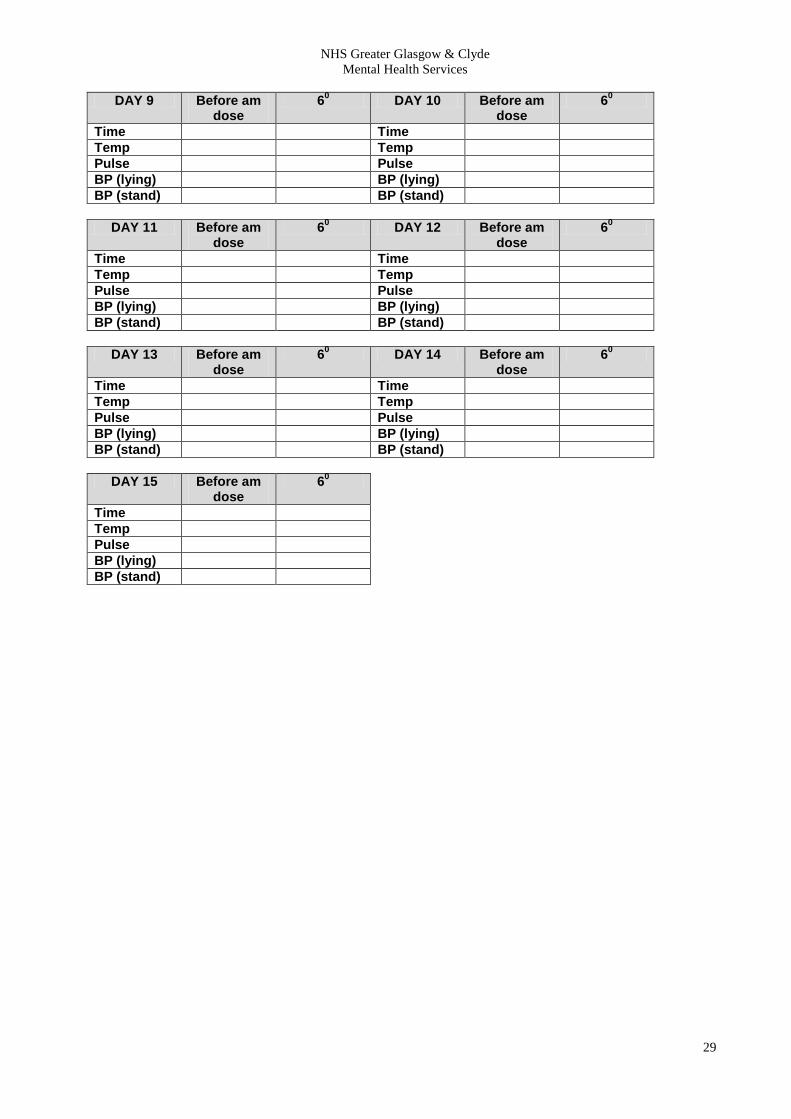
Appendix 4 Clozapine initiation community patient observation record
Surname Forename Date of birth CHI number Consultant
Baseline Recordings Date
BP Pulse Weight Temp
DAY 1 Before
am dose 10 (1 hour post dose)
20 30 40 50 60
Time Temp Pulse BP (lying)
BP (stand)
DAY 2 Before am
dose 20 60
Time Temp Pulse BP (lying) BP (stand)
DAY 3 Before am
dose 60 DAY 4 Before am
dose 60
Time Time Temp Temp Pulse Pulse BP (lying) BP (lying) BP (stand) BP (stand)
DAY 5 Before am
dose 60 DAY 6 Before am
dose 60
Time Time Temp Temp Pulse Pulse BP (lying) BP (lying) BP (stand) BP (stand)
DAY 7 Before am
dose 60 DAY 8 Before am
dose 60
Time Time Temp Temp Pulse Pulse BP (lying) BP (lying) BP (stand) BP (stand)
28
NHS Greater Glasgow & Clyde Mental Health Services
DAY 9 Before am
dose 60 DAY 10 Before am
dose 60
Time Time Temp Temp Pulse Pulse BP (lying) BP (lying) BP (stand) BP (stand)
DAY 11 Before am
dose 60 DAY 12 Before am
dose 60
Time Time Temp Temp Pulse Pulse BP (lying) BP (lying) BP (stand) BP (stand)
DAY 13 Before am
dose 60 DAY 14 Before am
dose 60
Time Time Temp Temp Pulse Pulse BP (lying) BP (lying) BP (stand) BP (stand)
DAY 15 Before am
dose 60
Time Temp Pulse BP (lying) BP (stand)
29