cme auricular reconstruction for microtia: part ii ...lipteh.com/study-notes/articles/cme from...
TRANSCRIPT

CME
Auricular Reconstruction for Microtia: Part II.Surgical TechniquesRobert L. Walton, M.D., and Elisabeth K. Beahm, M.D.Chicago, Ill., and Houston, Texas
Learning Objectives: After studying this article, the participant should be able to: 1. Describe the Brent and Nagatatechniques for auricular reconstruction and discuss the advantages, disadvantages, and complications of each technique.2. Describe the general approach for one-stage microtia repair. 3. Discuss the common problems encountered in microtiareconstruction and how these are currently addressed. 4. Be familiar with current research endeavors in tissue engineeringas this technology applies to auricular reconstruction.
Reconstruction of the microtic ear represents one ofthe most demanding challenges in reconstructive surgery.In this review the two most commonly used techniques forear reconstruction, the Brent and Nagata techniques, areaddressed in detail. Unique to this endeavor, the origi-nator of each technique has been allowed to submit rep-resentative case material and to address the pros and consof the other’s technique. What follows is a detailed, in-sightful overview of microtia reconstruction, as a state ofthe art. The review then details commonly encounteredproblems in ear reconstruction and pertinent technicalpoints. Finally, a glimpse into the future is offered withan accounting of the advances made in tissue engineer-ing as this technology applies to auricular recon-struction. (Plast. Reconstr. Surg. 110: 234, 2002.)
OPERATIVE PROTOCOLS FOR AURICULAR
RECONSTRUCTION
A variety of surgical strategies have been de-vised for the reconstruction of the external ear,with each composed of several stages. Thestages depend largely on the severity of thepatient’s deformity; the size, position, andquality of the microtic elements; and the sur-geon’s preference.
Tanzer advocated a four-stage reconstruc-tion.1 In the first stage, the lobular remnantwas transposed transversely to its correct ana-tomic position. In the second stage, costal car-tilage, harvested sub-perichondrially from thesixth, seventh, and eighth contralateral ribs,was implanted beneath the mastoid skin, usinga V-shaped postlobule incision. The sixth and
seventh costal cartilages were used for the baseand antihelix, and the eighth costal cartilagebecame the helical rim. The carved cartilageelements were coapted with fine-gauge wire. Inthe third stage, the construct was elevated fromthe head by advancement of postauricular skinand placement of a retroauricular, full-thicknessskin graft. The concha and tragus were subse-quently created with composite contralateral earand skin/cartilage grafts. Tanzer later modifiedthis sequence by combining the lobular transpo-sition and placement of the cartilage frameworkinto one stage, prefacing this modification withthe admonition that if extensive mobilization orsurgical manipulation of the lobule is necessary,it is best to use four separate stages to avoidvascular compromise of the lobular element.2
Numerous modifications of Tanzer’s tech-nique have been championed over the past 20years, but two particular techniques for totalear reconstruction have enjoyed considerableacceptance by the plastic surgery communityfor both their quality and reproducibility.3–14 Assuch, these techniques by Brent and Nagatawill be examined in detail.
BRENT TECHNIQUE
Brent uses a three-stage or four-stage tech-nique, similar to that of Tanzer, although witha slightly varied sequence:
From The University of Chicago, Section of Plastic Surgery, and M. D. Anderson Cancer Center. Received for publication August 13, 2001;revised November 16, 2002.
234

First Stage
In the first stage, a pattern for the constructis made by placing a piece of x-ray film againstthe normal ear and tracing its anatomic land-marks (Fig. 1). The template is then reversedand made several millimeters smaller through-out to accommodate for the thickness of theskin cover. The lobular component is altereddepending on the quality and amount of resid-ual lobular tissue. In patients with a very lowhairline, Brent suggests creating slightlysmaller ears to minimize problems with hirsutehelices. This approach is less problematic withbilateral microtia, but it may require resectionof a scapha crescent of the contralateral ear in
unilateral cases to create symmetry betweenthe normal and reconstructed ears. Once con-figured, the template is aligned symmetricallywith the contralateral ear using the ear’s rela-tionship to the nose, lateral canthus, and posi-tion of the lobule. In patients with hemifacialmicrosomia, this may be somewhat problem-atic because facial asymmetry always requires acompromise of the position of the recon-structed ear. In these situations, Brent recom-mends positioning the ear relative to the supe-rior pole of the contralateral ear, because thelateral canthus is a less dependable landmarkfor positioning the auricle.8 Brent also cautionsthat the lobular remnant may be positioned
FIG. 1. Brent technique, first stage. Ear framework fabrication with sculpted rib cartilage. (Above, left) The chest incision ismade contralateral to the ear being constructed. (Above, left center) Film pattern. Note that the proposed framework is smallerthan the reversed ear tracing, which allows for added thickness of covering skin; the framework tip is made substantially smallerto accommodate the lobule when it is transposed. (Above, right center) The rib cartilage specimens. The tapered, “floating” cartilageserves as a helix. (Above, right) The thinned helix, attached at its crus. (Below, left) The helix is affixed to the main block; outlineof the inferior crus-posterior conchal wall contour line. (Below, left center) Carving in progress; auricular details are outlined withink. (Below, right center) Sculpting details with chisel. (Below, right) The completed framework. To best demonstrate the fabricationprocess, several frameworks are used for this figure. (Courtesy Dr. Burt Brent.)
Vol. 110, No. 1 / AURICULAR RECONSTRUCTION FOR MICROTIA 235
too close to the eye, and a compromise be-tween the measured distance and the lobulemay be the most appropriate solution for posi-tioning in these cases.
The contralateral sixth, seventh, and eighthcostal cartilages are usually harvested. The con-struct base is formed by the synchondrosis of thesixth and seventh cartilages, whereas the “float-ing” eighth rib is used to fabricate the helicalelement, which is then attached to the base.Brent carves the cartilage base with “exaggerateddetails” to compensate for the dampening thatthe overlying thickened skin produces on thefinal three-dimensional relief. Fixation of the car-tilage pieces is achieved with clear nylon suture.The construct is placed into a subcutaneouspocket through an incision located at the poste-rior inferior border of the vestige. Dissection ofthe auricular pocket preserves the subdermalplexus, and the field of dissection is wide enough
to afford adequate drape of the skin flaps overthe framework without undue tension. The lob-ule is not repositioned in the first stage. By plac-ing the framework in the first stage under a virginskin envelope and using a high-profile construct,this technique will maximize definition of thereconstruction while minimizing the risk of vas-cular compromise of the skin flap. It is this ad-vantage that sets Brent’s technique apart fromTanzer’s, which transposes the lobule in the firststage.
Suction drains beneath and adjacent to theframework are used to occlude the overlying skinflap to the construct and thus achieve the defin-ing relief of the ear form. Brent finds that thistechnique minimizes the number of complica-tions related to pressure and bolster dressings,which in his first 15 cases resulted in a 33 percentrate of skin loss and infection.8 Since using suc-tion drains, these complications have been re-
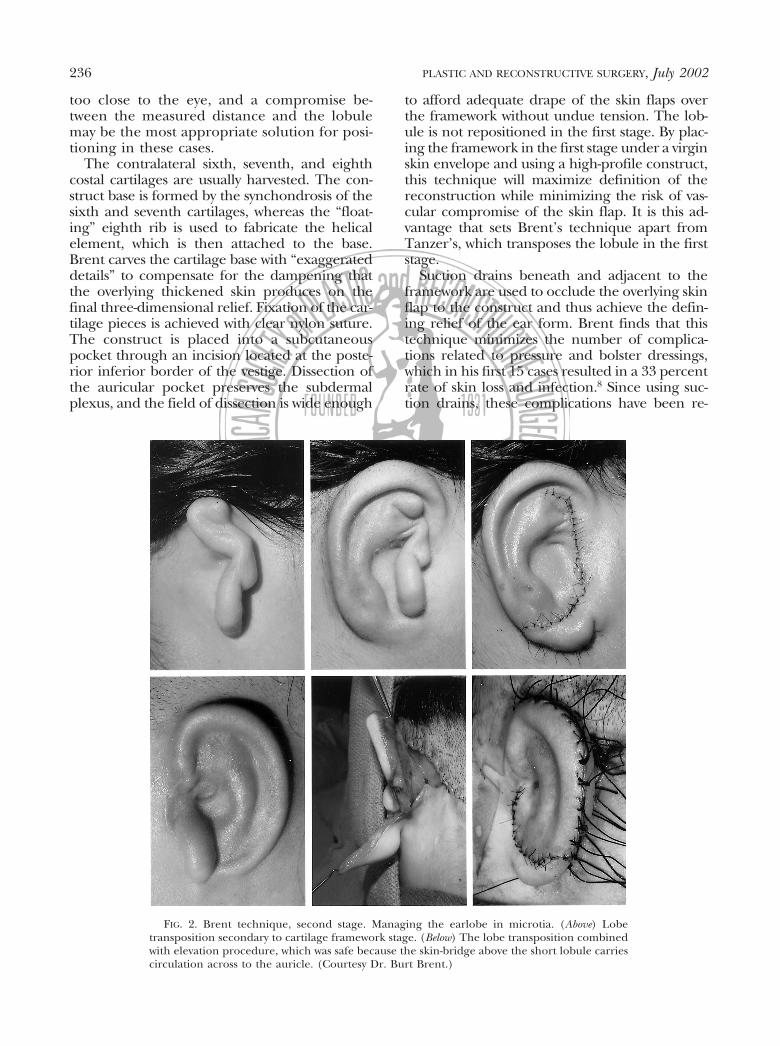
FIG. 2. Brent technique, second stage. Managing the earlobe in microtia. (Above) Lobetransposition secondary to cartilage framework stage. (Below) The lobe transposition combinedwith elevation procedure, which was safe because the skin-bridge above the short lobule carriescirculation across to the auricle. (Courtesy Dr. Burt Brent.)
236 PLASTIC AND RECONSTRUCTIVE SURGERY, July 2002

duced to less than 1 percent. The risk of injury tothe construct from pressure dressings has ledBrent to suggest that parents should be pre-vented from changing any of the ear dressings.
Second Stage
Lobule transposition is the second stage inBrent’s technique (Fig. 2). He believes it is saferand easier to position the lobular remnantaround an established construct. This stage isperformed several months after the initial carti-lage grafting. The lobule is rotated and oftenfilleted to receive the end of the framework.
Third Stage
The construct is elevated in the third stage toachieve projection of the helical rim (Fig. 2).An incision is made several millimeters from themargin of the rim, and dissection is carried overthe capsule of the posterior surface of the con-struct until the correct amount of projection isachieved. The ear position is stabilized by placinga piece of banked costal cartilage posteriorly be-neath the framework in a fascial pocket. Theretroauricular scalp is then advanced to mini-mize visible scarring. The remaining postauricu-
FIG. 3. Brent technique. Tragal reconstruction, concha excavation, and canal mimicry in theunilateral microtia patient. (Above, left) Chondrocutaneous graft harvested from the contralateralear. To avoid setting this particular ear too close to the head by the usual direct closure of thedefect, the concha is repaired with a small skin graft harvested just anterior to the hairline. (Above,center and below, left) A composite conchal cartilage/skin graft from the opposite ear is appliedbeneath the “tragal flap,” developed by a J-shaped incision placed at the proposed location ofthe tragal margin and intertragic notch. (Above, right) Excision of excess soft tissues accentuatesthe conchal depth. (Below, center) A composite graft is pulled under the tragal flap with a bolstersuture; the conchal floor is resurfaced with a full-thickness skin graft harvested from the posteriorcontralateral ear lobule. (Below, right) Result 2 years postoperatively. The shadow cast beneaththe constructed tragus mimics the external auditory meatus. (Courtesy of Dr. Burt Brent.)
Vol. 110, No. 1 / AURICULAR RECONSTRUCTION FOR MICROTIA 237

lar defect is closed with a “medium-thick” split-thickness skin graft from the hip.
Fourth StageTragus construction, conchal excavation, and
symmetry adjustment are performed in thefourth stage (Fig. 3). By reconstructing the traguslast, the final healing of the elevation has oc-curred, allowing precise adjustment of the oppo-site ear to ensure symmetry on the frontal view.The tragus is formed using a composite skin/cartilage graft from the contralateral conchalvault through an anterior approach. A J-shapedincision is fashioned along the posterior tragalmargin, and the composite graft is inserted andpositioned so that it produces both projection ofthe neotragus and cavitation of the retrotragalhollow. The subcutaneous tissues are then exca-vated to deepen the conchal bowl. In patients
with bilateral microtia, Brent recommends theuse of an anteriorly based conchal flap, similar tothe technique described by Kirkham, but adds acartilage strut for support.8,15 Recently, Brent de-vised a new method for tragus reconstruction asan alternative to this technique (Fig. 4).16
The most recent modifications of Brent’stechnique include incorporating a small carti-lage addition to the framework, as notedabove, to create a tragus, and laser hair re-moval of the scalp flaps before commencementof the ear reconstruction. Brent has experi-ence with over 1200 cases of ear reconstructionspanning a 25-year period. Long-term fol-low-up to 18 years attests to the safety anddurability of this method over time (Fig. 5).3
A major criticism of Brent’s technique is thenumber of stages required to achieve the final
FIG. 4. Brent technique. Ear framework fabrication with integral tragal strut.(Above) Construction of the frame. The floating cartilage creates the helix, andsecond strut is arched around to form the antitragus, intertragic notch, andtragus. This arch is completed when the tip of the strut is affixed to the crus helixof the main frame with a horizontal mattress suture of clear nylon. (Below) Actualframework fabrication with patient’s rib cartilage. (Courtesy Dr. Burt Brent.)
238 PLASTIC AND RECONSTRUCTIVE SURGERY, July 2002

result. This has particular relevance when oneconsiders the operative morbidity and costs.For most microtia reconstructions, four stagesare used; however, Brent will occasionally com-bine the earlobe transposition and elevationstages if the local vascular anatomy allows forthe safe manipulation of the tissues (Fig. 2).Proponents of the Nagata technique have em-phasized dissatisfaction with the appearance ofBrent’s tragal reconstructions.17 In less experi-enced hands, the composite skin/cartilagegrafts may contract, diminishing the retrotra-gal hollow and, sometimes, everting the tragusitself.
Brent’s technique has also been criticized forits lack of definition of the conchal bowl, theintertragic notch, and the contour of the anti-tragus. This criticism is underscored by theneed for an additional step for conchal exca-vation to achieve the desired definition of earanatomy. Without the construction of a com-plete crus helicis, the conchal cavity is not sep-arated into its major components, the cymbaand cavum conchae. In addition, skin graftsapplied to the conchal bowl, if not taken fromthe opposite ear or adjacent scalp, may hyper-pigment and thereby compromise the final ap-pearance. Effacement of the postauricular sul-cus is a common sequela following elevation ofthe construct that can result in decreased pro-jection of the reconstructed ear. This is largelydue to contraction of the skin grafts.16,17 Thisproblem may be minimized by the applicationof thicker skin grafts (preferably full-thickness)
or by advancing the postauricular skin to thedepth of the sulcus and grafting only the pos-terior ear.
NAGATA TECHNIQUE
Nagata’s technique involves two stages. It wasfirst introduced in 1993 and has undergone sev-eral possible technical refinements, dependingon the type of microtia present (i.e., lobular,small concha, conchal, anotia, low hairline).9–14
In addition to the helix, crura, antihelix, andconchal elements, this technique provides forthe incisura intertragica and the tragus as keyelements in the reconstruction.
First Stage
In the first stage, the rib cartilage framework,which incorporates a tragal component, isplaced in a subcutaneous pocket and the lob-ule is transposed. This first stage thus roughlycorresponds to the first three stages in Brent’ssequence. In contrast to the three contralateralcostal cartilage segments used in the Brenttechnique, Nagata harvests the ipsilateral costalcartilages of the sixth, seventh, eighth, andninth ribs. The total perichondrium is left insitu except for the junctional region of thesixth and seventh costal cartilages. Nagata con-structs the framework base into three “floors,”with each floor representing different eleva-tions: the cymba and cavum conchae form thebase; the crus helicis, the fossa triangularis, andthe scapha form the second level; and the he-lix, antihelix, tragus, and antitragus the top
FIG. 5. Brent technique. (Left) A 13-year-old male patient is shown preoperatively. (Right) The same patient 10 years afterreconstruction. (Courtesy Dr. Burt Brent.)
Vol. 110, No. 1 / AURICULAR RECONSTRUCTION FOR MICROTIA 239

level. The base frame is constructed from thesixth and seventh costal cartilages (Fig. 6). Thehelix and crus helicis are constructed from theeighth costal cartilage. The ninth costal carti-lage is used to construct the superior crus,inferior crus, and antihelix. The remaining
structures are carved from residual cartilagepieces. The cartilage construct is assembledusing fine-gauge wire sutures (Fig. 7).
Nagata uses the skin of the posterior lobuleand mastoid to cover the conchal aspect of theconstruct. By converting the V-shaped poste-rior lobule incision used by Tanzer into a “W,”he also increases the surface area of skin avail-able to cover the framework (Fig. 8). This alsopermits lobule transposition, obviating theneed for a conchal skin graft or a switchbackprocedure for lobular transposition as necessi-tated in Tanzer’s technique. The skin incisionseparates the lobule into three skin flaps: theposteroanterior lobular skin flaps and an ante-rior tragal skin flap. A 2-mm circular portion ofskin is removed from the inferior portion ofthe anterior lobule/tragal incision. A subcuta-neous pocket is dissected through the accessprovided by the posterior lobule incision. Ves-tigial cartilage remnants are removed carefullyso as to not damage the subdermal plexus ofthe flaps. In lobule-type microtia, the centralportion of the posterior skin flap remains at-tached by means of a subcutaneous pedicle toaugment its blood supply. After creation andplacement of the cartilage framework, the pos-terior flap is advanced and sutured to the tra-gal flap. The small circular skin defect that wascreated at the inferior point of this juncture issutured, forming a closure cone (inverted dog-
FIG. 6. Nagata technique. Harvesting of the costal cartilages. (Left) The sixth through ninthcostal cartilages are harvested from the same side as the reconstruction, leaving the majority (75percent) of the perichondrium intact. (Recently, Nagata started leaving all of the perichondriumintact.) The harvested cartilages are reversed to take advantage of their configurations. (Center)A three-dimensional frame unit is oriented to the harvested cartilages. (Right) Clinical example.(Reproduced with permission from Nagata, S. Microtia: Auricular reconstruction. In: VanderKolk, C. A. (Ed.), Plastic Surgery: Indications, Operations, and Outcomes, Vol. 2. St. Louis: Mosby, 2000.Pp. 1023–1056.)
FIG. 7. Nagata technique. Carved framework. The baseframe is constructed from the sixth and seventh costal car-tilages; the helix and crus helicis are constructed from theeighth costal cartilage; and the ninth costal cartilage is usedto construct the superior crus, inferior crus, and antihelix.The remaining structures are carved from residual cartilagepieces. The cartilage construct is assembled using fine-gaugewire sutures. (Courtesy Dr. S. Nagata.)
240 PLASTIC AND RECONSTRUCTIVE SURGERY, July 2002

ear), which represents the incisura inter-tragica. In small concha-type microtia, the an-terior incision is varied only slightly and thearea directly posterior to the indentation isexcised. The lobule is transposed by reassem-bling the flaps in the fashion of a Z-plasty (Fig.9). Bolsters affixed with mattress sutures areused to approximate the skin flaps to theframework. These are left in place for 2 weeks.
Second Stage
Six months after the first stage, the construct iselevated using a crescent-shaped piece of carti-lage harvested from the fifth rib through theprevious chest wall incision (Fig. 10). The skinaround the construct is incised 5 mm posterior tothe construct.14 The framework is elevated and
held in this position by wedging the carved, cres-cent-shaped cartilage graft into a position thatsubstitutes for a posterior conchal wall. A tem-poroparietal fascia flap is then elevated and tun-neled subcutaneously to cover the posterior sur-face of the cartilage graft and reconstructedauricle and the mastoid surface. The retroauricu-lar skin is advanced toward the ear to minimizevisible scarring, and the posterior aspect of theconstruct is closed with a skin graft, which issecured with a tie-over bolster in a manner simi-lar to that of Brent. Nagata prefers a split-thickness graft harvested freehand from the oc-cipital scalp for this purpose (ultra-delicate split-thickness skin graft).
Nagata emphasized the need for a deep,high-definition framework to create a good
FIG. 8. Nagata technique. Incision planning, creation of skin flaps, placement of frame-work. (Above, left) Incision line for the anterior surface of the auricle. Note that the terminusof the anterior incision is circular (arrow). (Above, center) Incision line for the posterior surfaceof the auricle; note the W-shaped flap. The shaded area (S) depicts the area of subcutaneoustissue that will be left intact so as to optimize blood supply to the flaps. (Above, right) The skinflaps are undermined, and the wings of the W-shaped flap have been approximated to formthe cup of the intertragic notch (C). (Below, left and center) Insertion and positioning offramework. (Below, right) Transposition of lobule and closure of incisions. Excessive skin shownat (D) is inverted to construct the pseudoacoustic meatus. The skin flaps are then approxi-mated to the underlying framework with cotton cylinder compresses secured by bolster sutures.(Courtesy Dr. S. Nagata.)
Vol. 110, No. 1 / AURICULAR RECONSTRUCTION FOR MICROTIA 241

tragus, which he believes is the weak link inmost contemporary ear reconstructions. Inaddition, he reasons that carving the crushelicis into the base frame ensures a morerealistic and smooth curve of the helix as itjoins the lobule. By eliminating the need forconchal excavation, his technique results in amore natural and deeper conchal bowl.9 –14
Despite the excellent appearance of Naga-ta’s ear reconstructions, a number of criticismshave arisen from others who have attempted toadopt his techniques. These stem from thevascular compromise of the peri-lobular flaps,most especially, the posterior flap. In his orig-inal description of 36 cases, Nagata describedno complications, but in the hands of others,flap necrosis has approached 14 percent.17 Thestresses inflicted on the skin envelope duringthe first stage of the Nagata technique wouldseem to be greater than with the Brent tech-nique, because of the relatively higher frame-work relief and the incisional compromise ofskin circulation attendant to the lobule trans-position. Nagata suggests preserving a subcuta-neous pedicle to the posterior skin flap to avertthis complication, but others doubt that thiseffectively increases the flap’s blood supply.17
Some think that the sacrifice of posterior earlobe skin to provide additional lining for thetragus reconstruction also compromises thenatural shape and contour of the lobule, therebydiminishing the natural appearance of the recon-
struction.16 Brent has argued that the refinementof Nagata’s tragal reconstruction is less than thatof a composite skin/cartilage graft, yet Brent hasrecently begun incorporating a tragal compo-nent into his framework for bilateral microtiacases.3,7
Although all techniques using autologouscostal cartilage produce a permanent anteriorchest wall deformity, the amount of costal car-tilage harvested by Nagata (the sixth throughninth costal cartilages) is considerable and mayresult in a significant chest wall deformity. Na-gata emphasizes that the degree of chest walldeformity can be minimized if the perichon-drium is left intact at the site of harvest to allowfor cartilage regeneration.18 This, however,would seem to have a greater likelihood ofsuccess in children than in adults.
Some have argued that the relatively greateramount of cartilage used by Nagata to achievethe high relief in his reconstructions producesunnaturally thick ears. Nagata believes that nat-ural-appearing reconstructed auricles are at-tained by carving the posterior margin of thebase frame of the fabricated framework, result-ing in the attainment of a thin and normalreconstructed auricle.19 Partial resorption ofthe piecemeal components of the frameworksmay also lead to the late development of con-tour irregularities, although the relatively shortfollow-up on patients in Nagata’s publishedseries is insufficient to derive any definitive
FIG. 9. Nagata technique, first stage. Clinical case. (Left) A 29-year-old woman with lobule type microtia. (Center) Immediateresult after placement of framework and skin closure. (Right) Six months after the first-stage operation. (Courtesy Dr. S. Nagata.)
242 PLASTIC AND RECONSTRUCTIVE SURGERY, July 2002

conclusions as to long-term stability.7 Neverthe-less, using his current two-stage method, whichnow exceeds 600 cases with a maximum fol-low-up of 14 years, Nagata reports no untowardproblems or complications with cartilage re-sorption or framework distortion.20
Nagata’s use of wire sutures to assemble hiscartilage framework has been criticized be-cause of the high (8 percent) extrusion rateobserved by others using this technique.17 Na-gata argues that this problem does not occur ifthe subcutaneous pedicle of the posterior flapis properly constructed and the loop portion ofthe wire suture is embedded into the substanceof the anterior surface of the framework, as hedescribes in his original article.14,21 Finally, the
use of a temporal fascial flap in every caseseems somewhat excessive, with its attendantrisks of scalp scarring, temporal hair thinning,and the sullying of a potential reconstructivelifeboat. Even though the temporoparietal fas-cia flap is used during the second-stage auric-ular reconstruction (auricular projection) inall cases, Nagata counters that the deep tem-poral fascia is preserved and remains a poten-tial source of vascularized soft tissue for use insalvage operations.22
Although Nagata’s two-stage techniqueholds a certain advantage over Brent’s three-stage or four-stage technique in the number ofoperations used, as in most abbreviated ap-proaches used in reconstructive surgery, some
FIG. 10. Nagata technique, second stage. Clinical case. (Above, left) The design for incision lines and harvesting of theultra-delicate split-thickness scalp graft and temporoparietal fascia. (Above, center) A crescent-shaped costal cartilage block isfabricated from the harvested fifth costal cartilage. (Above, right) The constructed cartilage is undermined and elevated. Thecartilage graft is wedged in the postauricular sulcus to create the posterior conchal wall. A temporal parietal fascial flap is thentransposed to provide soft-tissue coverage over the postauricular surface. The wound is closed with an ultra-delicate split-thicknessscalp skin graft. (Below, left) Lateral view shown 2 years after the second-stage operation. (Below, center) Frontal view shown 2 yearsafter the second-stage operation. (Below, right) Posterior view shown 2 years after the second-stage operation. (Courtesy Dr. S.Nagata.)
Vol. 110, No. 1 / AURICULAR RECONSTRUCTION FOR MICROTIA 243

vulnerability may exist in the ability to achieveprecise, consistent results by all users. Brentargues that Nagata has not specifically ad-dressed the issue of frontal symmetry in hisreconstructions, and were he to do so a thirdstage would likely be required.23 Nagata con-tends that favorable and desired results areconsistently attained using his two-stage tech-nique.14 He believes that failure to achieve thedesired endpoint is the result of compromiseof the surgical technique or the omission ofcertain procedures during the reconstruc-tion.24 In the case example, the ear projectionachieved by the Nagata technique on frontalinspection appears remarkably symmetrical tothe normal side (Fig. 10).
SINGLE-STAGE TOTAL EAR RECONSTRUCTION
Single-stage ear reconstructions have beenused primarily for the reconstruction of partialdefects such as the superior helix or lobule.25,26
Current techniques for single-stage total earreconstruction involve the fabrication of a car-tilage framework, followed by coverage using acombination of local skin flaps, fascial flaps,and skin grafts.27–29 External stents are com-monly used to maintain contour. Unfortu-nately, early results have fallen short in dupli-cating the precision and refinement achievedthrough the use of established, staged tech-niques. This is underscored by the experienceof Park, who modified his two-flap, single-stagereconstruction into an expanded, two-flap,three-stage reconstruction with significant im-provement in the results.30,31 The concept ofsingle-stage auricular reconstruction, neverthe-less, remains promising and will likely grow inapplicability as further experience is gained.
PROBLEMS ENCOUNTERED IN EAR RECONSTRUCTION
Hair
The low hairline in many microtic patientsnecessitates placement of a portion of the carti-lage framework beneath hair-bearing scalp. Thisresults in hair growth on the construct, whichsubstantially detracts from the final result. More-over, the hair-bearing scalp is thicker and con-tours less well to the underlying framework,thereby compromising the fine definitions thatmight otherwise have been achieved through theuse of a thinner flap. Use of the scalp in earreconstruction may also lead to inflammation/infection complications from ingrown hair, ker-atin accumulation, maceration, and difficulties
with hygiene. To address these problems, manysurgeons recommend manual depilation, al-though this technique has been shown to inducecirculatory problems in the flaps, leading to ne-crosis and increased scarring.32,33 Brent has rec-ommended electrolysis or resurfacing the areawith a skin graft.3,8 Recent attempts at preopera-tive laser depilation are promising but have notwithstood the rigors of critical, long-term analy-sis.3 Using the temporoparietal fascia, a three-dimensional framework, a cartilage block, and anultra-delicate split-thickness scalp graft to pre-cisely position the reconstructed ear and reposi-tion the hairline, Nagata believes that the prob-lems associated with low hairline have beensolved.14,34
Soft-Tissue Cover
An adequate skin envelope of good quality iscritical for a successful ear reconstruction. Theskin must be supple, thin, and well vascularizedto drape over the numerous convolutions ofthe framework to render an adequate defini-tion. Skin quality may be compromised by thepresence of hair, previous trauma, or at-tempted microtia repair. Certain patients maypresent with very taut, inelastic skin that resistsconformation. These patients constitute a spe-cial group that often defies the traditional ap-proaches to ear reconstruction.
First introduced by Fox and Edgerton in197633 and popularized by Tegtmeier in 1977,34
the temporoparietal fascial flap has become aworkhorse flap for external ear reconstruction.This flap is primarily used in secondary proce-dures or in ear salvage.6 It has also been used inprimary procedures to supplement inadequatesoft-tissue cover.35,36 Nagata advocates the useof the temporoparietal fascia flap in combina-tion with an ultra-delicate split-thickness scalpgraft for complicated auricular reconstructionsand for secondary reconstructions.14 Brent usesa Y-shaped scalp incision, although a curvilin-ear incision beginning in the preauricular re-gion is usually adequate for most operativeexposures.6,7 The temporoparietal fascia flap isbased on the superficial temporal artery andvein. The vessels are mapped out with a Dopp-ler and are carefully dissected in a plane justdeep to the hair follicles. It is a tedious dissec-tion; care must be taken to avoid injury to thehair follicles, axial vessels, and frontal branchof the facial nerve. The flap is elevated fromthe deep temporal fascia and then draped overthe framework as needed. Complications of
244 PLASTIC AND RECONSTRUCTIVE SURGERY, July 2002

the flap include alopecia (28.6 percent), scalpnumbness (17.4 percent), and objection to thevisible scar (25 percent in male patients).8 Theanatomy and course of the superficial temporalsystem vary considerably in microtic patientsand can complicate the surgical planning. Theuse of fascia combined with a skin graft mayalso result in less definition in the recon-structed ear compared with that using a suppleskin flap. To overcome this shortcoming, thecartilage construct can be carved to a higherrelief and the conchal vault expanded to ac-commodate for the additional thickness of thecomposite soft-tissue envelope and for the an-ticipated skin contraction. Having used the ul-tra-delicate split-thickness scalp graft with tem-poroparietal fascia in the majority of hismicrotia reconstructions, however, Nagata re-ports that the ears have excellent definitionand that steps to create frameworks with higherrelief and an expanded conchal vault areunnecessary.14,22,35
Tissue expansion could theoretically net ad-ditional soft tissue for coverage. The use of thistechnique in auricular reconstruction, how-ever, is quite controversial. Opponents arguethat the thick fibrous capsule formed adjacentto a previously implanted tissue expander pre-vents adequate skin draping over the cartilageframework, thereby obscuring its detail andnegatively affecting the quality of the recon-struction.37 Although current thinking doesnot favor the use of tissue expansion in auric-ular reconstruction, expanded skin and fasciahas been successfully used in over 146 microtiareconstructions by Park with excellent resultsand relatively few complications, thus givingnew cause for reconsideration of this tech-nique.31 Brent has advocated “intraoperative”tissue expansion, using a large Foley catheterto relieve “marginal” skin tension, but thistechnique has limited application.8
COMPLICATIONS
Regardless of the method used, complica-tions arising from surgical efforts to recon-struct the external ear may occur both at theear reconstructive site and at the donor sitesfor tissue harvest.
Chest Wall Donor-Site Complications
The complications associated with costal car-tilage harvest include the immediate problemsof the pneumothorax and atelectasis and thedelayed issues of chest wall deformity and scar-
ring.18,38 The precise frequency of the inci-dence of pneumothorax during rib harvest isunclear, because most authors suggest theplacement of a temporary catheter to evacuatethe air leak. Brent notes no need for pro-longed chest tube drainage in his initial expe-rience with over 600 costal cartilage graft har-vests.8 Anterior chest wall deformity occurs inmost patients, and it is considered by most tobe an inevitable consequence of the harvestthat is well justified by the improvement gainedin facial appearance resulting from the recon-struction. In evaluating a series of 32 donorsites used in 18 patients undergoing microtiareconstruction, Ohara et al. observed chestwall deformities in over 64 percent of childrenunder the age of 10 years compared with a 20percent rate in older children, leading them torecommend delaying costal cartilage harvest aslong as possible.38 Many surgeons have adoptedthis policy, which seems to be more accepted inEastern cultures than in the West. The psycho-logical stigmata of impaired socialization inunreconstructed patients, however, remain tobe addressed. The trend to leave the posteriorperichondrium intact when harvesting the cos-tal cartilage, as recommended by Nagata, issound and may help to stifle the deformity thatwould otherwise result from excision of all ofthe perichondrium.19
The age group that most commonly under-goes auricular reconstruction is also prone tothe development of hypertrophic scars thatmay prove to be rather unsightly. These scarsusually atrophy over time. Careful placementof the surgical incision in the medial infra-mammary fold, especially in female patients, isa useful adjunct that will be especially appreci-ated as the child grows into adolescence.
Costal cartilage harvest evokes considerablepain and discomfort and easily constitutes themost immediately problematic postoperativeevent. To minimize pain in the chest wall, it ishelpful to place a small-diameter infusion cath-eter in the wound bed at the time of graftharvest for use as a conduit for the administra-tion of bupivacaine or other local anestheticsduring the postoperative period.
Complications at the Ear Reconstruction Site
Exposure of the cartilage framework due tooverlying skin flap necrosis can be devastatingto the reconstruction and may necessitate thecomplete removal of the framework. In cases offlap compromise, early intervention is manda-
Vol. 110, No. 1 / AURICULAR RECONSTRUCTION FOR MICROTIA 245

tory for salvage of the reconstruction. This isusually achieved with a combination of localskin and fascial flaps. A point to be emphasizedis the importance of placing the initial drainaccess sites remote to the superficial temporalsystem so as to avoid injury to a potential sal-vage resource, the temporal fascia. More com-monly, small areas of skin loss (�1 cm) may bedealt with conservatively with topical and sys-temic antimicrobial therapy, allowing the areato granulate and heal by secondary intent.Even a small area of skin loss or compromisemay have a negative affect on the resulting earreconstruction, and every effort must be madeto avoid this problem.
Careful intraoperative dissection with preser-vation of the subdermal plexus, and approxi-mation of the skin flaps to the underlying car-tilage framework, are imperative for anuncomplicated, successful outcome. Pressuredressings should be avoided.8 Infection is not acommon complication (0.5 percent), but itmay stem from either construct exposure orpathogens in the vestigial external ear canal. Assuch, careful assessment of any pathologic find-ings in the middle ear, such as otitis or cho-lesteatoma, and preoperative cleaning of thecanal are imperative. Similarly, although hema-toma is an infrequent complication (0.3 per-cent), its occurrence could have devastatingconsequences. Meticulous hemostasis is there-fore imperative.
Long-term complications in the recon-structed ear primarily relate to extrusion ofsuture material and resorption of the cartilageframework, which may alter the shape andform of the auricular components. Usually,these complications are minor in nature andcan be easily managed in the office setting.Significant resorption of the framework, how-ever, may require additional cartilage graftingto restore a satisfactory ear contour. The causeof cartilage resorption must be carefully deter-mined or the problem may repeat itself. Su-tures placed too tightly or placement of theframework in a scarred, ischemic bed may pre-dispose the cartilage to resorption. For thelatter, excision of the scarred bed and replace-ment with healthy, vascularized tissue (tem-poroparietal fascial flap) may be necessary toachieve stability in the reconstruction. Finally,resorption of the cartilage at the site of thesynchondrosis can sometimes lead to notchingof the framework, requiring reintervention.17
TECHNICAL POINTS
A successful reconstructive effort necessarilyfollows a thorough evaluation of the externalear with assessment of the associated patho-logic findings and establishment of the statusof the middle ear. Any need for otologic inter-vention must be carefully orchestrated with theexternal ear reconstruction. The appropriatesequence and timing of each operative stagemust be individualized. The minimum safenumber of operative stages needed to obtainthe highest quality reconstruction is the goalall surgeons must strive to achieve. A numberof different surgical techniques are available,and each surgeon must consider the most ap-propriate for his or her skills and experience.Autologous cartilage frameworks, despite theirpotential for donor-site complications, remainthe accepted standard for external ear recon-struction. All authors agree that maximum re-lief of the construct is essential for the highestquality of reconstruction. The use of fine-gauge stainless steel wire to coapt the cartilageelements of the framework has been associatedwith a higher incidence of construct notchingand wire extrusion, although this may relate tothe technical issues of wire placement and fix-ation.14 Suture fixation of the cartilaginousframework parts is an alternative that has beenshown to result in decreased extrusion/resorption rates, but it may not provide as rigida fixation of the various framework elements aswith wire.8
Minimizing the number of operative stagesand dissection over the framework will likelyoptimize its anatomic definition and enhancethe quality of the reconstruction. It must beremembered that the vascularity of the tissueadjacent the vestigial ear remnant is limited,and overly zealous dissection may result in di-saster. In certain cases, it may well be better touse an additional operative stage to avoid com-promise of the skin flaps than to risk completeloss of the reconstruction.
If middle ear reconstruction is included,the creation of the canal and performance ofthe middle ear surgery is usually done in oneor two stages through both conchal and post-auricular/mastoid approaches. Even in thebest of hands, this procedure carries a highcomplication rate, with frequent stenosis ofthe external auditory canal. To avoid thisproblem, Firmin et al. advocate lining thecanal with vascularized subgaleal fascia.39 In
246 PLASTIC AND RECONSTRUCTIVE SURGERY, July 2002

addition, it may be wise to perform the oto-logic portions of the reconstruction beforehelical elevation and then to stage the eleva-tion in two stages to avoid vascular compromiseof the construct.40,41
Dressings are a key adjunct to ear reconstruc-tion. Pressure dressings may compromise thevascularity of the already taut overlying skinenvelope, resulting in skin necrosis and expo-sure of the framework. Pressure and bolster-type dressings should be avoided during theframework placement stage and used only withextreme caution in secondary procedures.Some practitioners advocate the use of plica-tion sutures for securing the skin envelope tothe framework. In the hands of novices, how-ever, this technique may pose considerable riskfor producing skin necrosis and must be mon-itored closely. Nagata emphasizes that the useof bolsters is safe provided that the overlyingskin envelope is well vascularized and not tautfollowing placement of the framework. He se-cures the bolsters with sufficient tension suchthat they gently coapt the skin envelope to theframework without pressure or blanching. Inthis manner, he is able to avoid skin necrosiscomplications.12–14,24,35 Suction drains haveproved to be invaluable in achieving flap coap-tation to the framework, but they must be pre-cisely placed for optimal effect. Success of thesuction drain is improved by careful, airtightclosure of the surgical incisions. This may re-quire fine-layered closure and, occasionally,the use of an impervious elastic drape or asurgical adhesive applied over the suture line.The drains must be monitored closely for clot-ting of the drain system so as to stifle thedevelopment of hematoma or seroma forma-tion. Also, the vacutainer tubes must bechanged every 4 hours or less, which may im-pose some constraints on the available medicaland nursing staff.23
The highly complex nature of ear recon-struction places it in the higher echelons ofreconstructive surgical procedures. The multi-disciplinary issues surrounding congenital eardeformities, combined with the technical ex-pertise and experience necessary to satisfacto-rily conduct the surgery, suggest that thesetypes of reconstructions should not be per-formed by surgeons unfamiliar with the tech-nique. Optimal results can only be achievedthrough dedicated study and experience.
PROSTHETIC/OSSEO-INTEGRATED AURICULAR
RECONSTRUCTION
Recent advances in implantology and pros-thetic materials have lead to excellent resultsusing osseo-integrated anchoring devices andear prostheses. Prosthetic reconstruction maybe an excellent alternative in patients withpoor local tissues resulting from radiation, can-cer, or prior surgery (such as in previouslyunsuccessful autologous reconstructions), inelderly patients, or in those patients with highoperative risk factors. Provided that good bonestock is available, the surgical procedures forimplanting and exposing the osseo-integratedanchoring prostheses are relatively straightfor-ward, and the adverse effects of the percutane-ous connection are predominantly minor skinreactions. The weak link in this technology liesin the quality of the prosthesis itself, the lifelikeappearance of which is wholly dependent onthe artistry and skill of the anaplastologist. Pa-tients undergoing this approach have beengenerally quite satisfied with the prosthesesand wear them daily and for prolonged periodswithout difficulty.42–44 This represents a consid-erable improvement over the old style, “glue-on” type of prostheses.
FUTURE APPROACHES FOR AURICULAR
RECONSTRUCTION: TISSUE ENGINEERING
The majority of surgeons recognize the su-periority of autologous cartilage over the avail-able alternatives for constructing an ear frame-work. However, it would clearly be of greatbenefit if one could obviate the use of the chestwall donor site with its attendant risks andmorbidity. The potential to fabricate or engi-neer autologous parts has recently become ablooming field of scientific endeavor. The con-cept of engineering complex body parts is notnew. Proponents for creating complex partsinitially sought to render three-dimensionalform through the process of molding tissue.45,46
Unfortunately, the constructs did not maintaintheir engineered shape over time because ofthe lack of a stable substructure, or scaffolding.To address this problem, Walton et al. success-fully engineered a fibrovascular stroma with askin covering to various alloplast ear-shapedscaffolds.47,48 They demonstrated that three-dimensional facsimiles of ears could be fabri-cated by this technique and that these con-structs could be transferred microsurgically.The alloplastic materials used in these experi-
Vol. 110, No. 1 / AURICULAR RECONSTRUCTION FOR MICROTIA 247

ments, however, eventually extruded, resultingin deformation and loss. The scaffolding,therefore, seems to be a critical component inthe engineering of a complex body part such asan ear. Biologic/autogenous materials for scaf-folding intuitively should work better, giventhe documented clinical experience with autol-ogous materials, for all types of reconstruc-tions, especially ear reconstructions. Vacantiand, later, Saadeh explored this concept in theexperimental setting.49,50 They demonstratedthat bovine chondrocytes transplanted intomice hosts onto synthetic, biodegradable scaf-folds, could, under special conditions, producede novo cartilage. When placed into specialmolds, others have shown that this de novoneocartilage could be rendered into complex,three-dimensional shapes and configura-tions.51–53 The chondrocytes in these experi-ments, however, were derived from nonhuman,fetal tissues, making the clinical applicability ofthis exercise somewhat suspect for both humanchildren and adults. Human chondrocytes havebeen extracted from a number of sources, in-cluding rib and ear. In younger age groups, atleast, these chondrocytes have been successfullyinduced to replicate their numbers and formimmature cartilage.54,55 Although the durabilityof this neocartilage as a scaffold for ear recon-struction remains to be demonstrated, the con-cept and the technology are promising.
Dr. Robert L. WaltonSection of Plastic SurgeryThe University of Chicago Hospitals5841 South Maryland Avenue, MC6035Chicago, Ill. [email protected]
ACKNOWLEDGMENT
The authors thank Drs. Burt Brent and Satoru Nagata fortheir invaluable advice and critique in the preparation of thisreview and for contributing the figures.
REFERENCES
1. Tanzer, R. C. Total reconstruction of the auricle: Theevolution of a plan of treatment. Plast. Reconstr. Surg.47: 523, 1971.
2. Tanzer, R. C. Microtia: A long-term follow-up of 44reconstructed auricles. Plast. Reconstr. Surg. 61: 161,1978.
3. Brent, B. Technical advances in ear reconstruction withautogenous rib cartilage grafts: Personal experiencewith 1200 cases. Plast. Reconstr. Surg. 104: 319, 1999.
4. Brent, B. The correction of microtia with autogenouscartilage grafts II: Atypical and complex deformities.Plast. Reconstr. Surg. 66: 13, 1980.
5. Brent, B. The correction of microtia with autogenous
cartilage grafts I: The classic deformity. Plast. Reconstr.Surg. 66: 1, 1980.
6. Brent, B., and Byrd, H. S. Secondary ear reconstructionwith cartilage grafts covered by axial, random, and freeflaps of temporoparietal fascia. Plast. Reconstr. Surg. 72:141, 1983.
7. Brent, B. Modification of the stages in total reconstruc-tion of the auricle: Parts I to IV (Discussion). Plast.Reconstr. Surg. 93: 267, 1994.
8. Brent, B. Auricular repair with autogenous rib cartilagegrafts: Two decades of experience with 600 cases. Plast.Reconstr. Surg. 90: 355, 1992.
9. Nagata, S. A new method of total reconstruction of theauricle for microtia. Plast. Reconstr. Surg. 92: 187, 1993.
10. Nagata, S. Modification of the stages in total recon-struction of the auricle: Part I. Grafting the three-dimensional costal cartilage framework for lobule-type microtia. Plast. Reconstr. Surg. 93: 221, 1994.
11. Nagata, S. Modification of the stages in total recon-struction of the auricle: Part II. Grafting the three-dimensional costal cartilage framework for concha-type microtia. Plast. Reconstr. Surg. 93: 231, 1994.
12. Nagata, S. Modification of the stages in total recon-struction of the auricle: Part III. Grafting the three-dimensional costal cartilage framework for small con-cha-type microtia. Plast. Reconstr. Surg. 93: 243, 1994.
13. Nagata, S. Modification of the stages in total recon-struction of the auricle: Part IV. Ear elevation. Plast.Reconstr. Surg. 93: 254, 1994.
14. Nagata, S. Microtia: Auricular reconstruction. In C. A.Vanderkolk (Ed.), Plastic Surgery: Indications, Opera-tions, and Outcomes. Vol 2. St. Louis: Mosby, 2000. Pp.1023–1056.
15. Kirkham, H. L. D. The use of preserved cartilage in earreconstruction. Ann. Surg. 111: 896, 1940.
16. Brent, B. Personal communication.17. Firmin, F. Ear reconstruction in cases of typical micro-
tia: Personal experience based on 352 microtic earcorrections. Scand. J. Plast. Reconstr. Surg. Hand Surg.32: 35, 1998.
18. Nagamizu, H., and Nagata, S. Minimization of postop-erative complications and problems at the donor siteafter costal cartilage resection. In K. Harii (Ed.), Plas-tic, Reconstructive, and Aesthetic Surgery. Amsterdam/New York: Kugler Publications, 1995. Pp. 423–424.
19. Nagata, S. Personal communication.20. Nagata, S. Personal communication.21. Nagata, S. Personal communication.22. Nagata, S. Personal communication.23. Brent, B. Personal communication.24. Nagata S. Personal communication.25. Yoshimura, K., Nakatsuka, T., Ichioka, S., Kaji, N., and
Harii, K. One-stage reconstruction of an upper partdefect of the auricle. Aesthetic Plast. Surg. 22: 352, 1998.
26. Park, C., and Chung, S. A single-stage two-flap methodfor reconstruction of partial auricular defect. Plast.Reconstr. Surg. 102: 1175, 1998.
27. Avelar, J. M., and Psillakis, J. M. Microtia: Total recon-struction of the auricle in one single operation. Br. J.Plast. Surg. 34: 224, 1981.
28. Song, Y., and Song, Y. An improved one-stage total earreconstruction procedure. Plast. Reconstr. Surg. 71:615, 1983.
29. Park, C., Lee, T. J., Shin, K. S., and Kim, Y. W. A single-stage two-flap method of total ear reconstruction.Plast. Reconstr. Surg. 88: 404, 1991.
248 PLASTIC AND RECONSTRUCTIVE SURGERY, July 2002

30. Park, C. Modification of two-flap method and frame-work construction for reconstruction of atypical con-genital auricular deformities. Plast. Reconstr. Surg. 99:1846, 1997.
31. Park, C. Subfascial expansion and expanded two-flapmethod for microtia reconstruction. Plast. Reconstr.Surg. 106: 1473, 2000.
32. Fukuda, O., and Yamada, A. Reconstruction of the mi-crotic ear with autogenous cartilage. Clin. Plast. Surg.5: 351, 1978.
33. Fox, J. W., and Edgerton, M. T. The fan flap: An adjunctto ear reconstruction. Plast. Reconstr. Surg. 58: 663,1976.
34. Tegtmeier, R. E., and Gooding, R. A. The use of a fascialflap in ear reconstruction. Plast. Reconstr. Surg. 60: 406,1977.
35. Nagata, S. Recent advancements for surgical treatmentof complicated auricular reconstruction. Plast. Surg.Forum XIX: 252, 1996.
36. Nakai, H. Reconstruction of microtia with a contour-accentuated framework and supplemental coverage.Plast. Reconstr. Surg. 78: 604, 1986.
37. Oneal, R. M., Rohrich, R. J., and Izenberg, P. H. Skinexpansion as an adjunct to reconstruction of the ex-ternal ear. Br. J. Plast. Surg. 37: 517, 1984.
38. Ohara, K., Nakamura, K., and Ohta, E. Chest wall de-formities and thoracic scoliosis after cartilage graftharvesting. Plast. Reconstr. Surg. 99: 1030, 1997.
39. Firmin, F., Gratacap, B., and Manach, Y. Use of sub-galeal fascia to construct the auditory canal in microtiaassociated with aural atresia. Scand. J. Plast. Reconstr.Surg. Hand Surg. 32: 49, 1998.
40. Aguilar, E. A., III, and Jahrsdoerfer, R. A. The surgicalrepair of congenital microtia and atresia. Otolaryngol.Head Neck Surg. 98: 600, 1988.
41. Aguilar, E. F., III. Auricular reconstruction of congen-ital microtia (grade III). Laryngoscope 106(Suppl. 82):1, 1996.
42. Somers, T., De Cubber, J., Govaerts, P., et al. Totalauricular repair: Bone anchored prosthesis or plasticreconstruction? Acta Otorhinolaryngol. Belg. 52: 317,1998.
43. Wilkes, G. H., and Wolfaardt, J. F. Osseointegrated al-loplastic versus autogenous ear reconstruction: Crite-
ria for treatment selection. Plast. Reconstr. Surg. 93:967, 1994.
44. Tolman, D. E., Tjellstrom, A., and Woods, J. E. Recon-structing the human face by using the tissue-inte-grated prosthesis. Mayo Clin. Proc. 73: 1171, 1998.
45. Peer, L. A. Reconstruction of the auricle with dicedcartilage grafts in a vitallium ear mold. Plast. Reconstr.Surg. 3: 653, 1948.
46. Fisher, J., and Yang, W. Y. Experimental tissue moldingfor soft-tissue reconstruction: preliminary report.Plast. Reconstr. Surg. 82: 857, 1988.
47. Walton, R. L., Chick, L. R., and Brown, R. E. Creationof a vascularized alloplast. Plast. Surg. Forum IX: 160,1988.
48. Walton, R. L., and Brown, R. E. Tissue engineering ofbiomaterials for composite reconstruction: An exper-imental model. Ann. Plast. Surg. 30: 105, 1993.
49. Vacanti, C. A., and Vacanti, J. P. Bone and cartilagereconstruction with tissue engineering approaches.Otolaryngol. Clin. North Am. 27: 263, 1994.
50. Saadeh, P. B., Brent, B., Mehrara, B. J., et al. Humancartilage engineering: Chondrocyte extraction, pro-liferation, and characterization for construct develop-ment. Ann. Plast. Surg. 42: 509, 1999.
51. Kim, W. S., Vacanti, J. P., Cima, L., et al. Cartilageengineered in predetermined shapes employing celltransplantation on synthetic biodegradable polymers.Plast. Reconstr. Surg. 94: 233, 1994.
52. Paige, K. T., Cima, L. G., Yaremchuk, M. J., et al. Denovo cartilage generation using calcium alginate-chondrocyte constructs. Plast. Reconstr. Surg. 97: 168,1996.
53. Sims, C. D., Butler, P. E., Cao, Y. L., et al. Tissue engi-neered neocartilage using plasma derived polymersubstrates and chondrocytes. Plast. Reconstr. Surg. 101:1580, 1998.
54. Minas, T., and Nehrer, S. Current concepts in the treat-ment of articular cartilage defects. Orthopedics 20: 525,1997.
55. Rodriguez, A., Cao, Y. L., Ibarra, C., et al. Characteris-tics of cartilage engineered from human pediatricauricular cartilage. Plast. Reconstr. Surg. 103: 1111,1999.
Self-Assessment Examination follows onthe next page.
Vol. 110, No. 1 / AURICULAR RECONSTRUCTION FOR MICROTIA 249

Self-Assessment Examination
Auricular Reconstruction for Microtia: Part II. Surgical Techniquesby Robert L. Walton, M.D., and Elisabeth K. Beahm, M.D.
1. THE FIRST STAGE OF BRENT’S TECHNIQUE FOR MICROTIA RECONSTRUCTION INCLUDES WHICH ONEOF THE FOLLOWING SEQUENCES?A) Lobule transpositionB) Framework placement and lobule transpositionC) Framework placementD) Excision of remnant cartilages, laser hair removalE) Excision of remnant cartilages and lobule transposition
2. WHICH ONE OF THE FOLLOWING STATEMENTS ABOUT BRENT’S TECHNIQUE FOR AURICULARRECONSTRUCTION IS INCORRECT?A) Suction drains are used to secure the skin envelope to the cartilage framework.B) Wire sutures are used to fixate cartilage components of the framework.C) The tragus is constructed using a composite graft from the opposite ear.D) Lobule transposition is performed as the second stage.E) For most microtia reconstructions, four stages are involved.
3. WHICH OF THE FOLLOWING ASPECTS OF NAGATA’S METHOD FOR AURICULAR RECONSTRUCTIONDOES NOT DIFFER FROM THAT OF BRENT?A) Reconstruction of the incisura intertragicaB) Positioning of the frameworkC) Use of cotton bolsters to secure the skin envelope to the frameworkD) Use of wire sutures to secure elements of the frameworkE) None of the above
4. WHICH OF THE FOLLOWING IS A COMMON CRITICISM OF THE BRENT TECHNIQUE?A) Excessive number of reconstructive stages involvedB) Frontal symmetryC) Resorption of the cartilage frameworkD) ReproducibilityE) All of the above
5. WHICH OF THE FOLLOWING IS A COMMON CRITICISM OF THE NAGATA TECHNIQUE?A) Excessive harvest of costal cartilageB) Cartilage resorption and splitting of wire suturesC) Skin flap necrosisD) ReproducibilityE) All of the above
6. WHICH ONE OF THE FOLLOWING ASPECTS OF AURICULAR RECONSTRUCTION IS COMMON TO BOTHTHE BRENT AND THE NAGATA TECHNIQUES?A) Use of ipsilateral autologous costal cartilageB) Use of wire sutures to secure the cartilage frameworkC) Use of temporal-parietal fascia to cover the posterior frameworkD) Use of cotton bolstersE) Use of costal cartilage graft to elevate helix
7. WHICH OF THE FOLLOWING INTERVENTIONS HAS NOT BEEN USED FOR AURICULAR RECONSTRUCTIONIN LOW HAIRLINE PATIENTS?A) Temporoparietal fascial flapB) Laser ablationC) Manual depilationD) ElectrolysisE) Gene therapy
8. WHICH OF THE FOLLOWING STATEMENTS REGARDING THE TEMPOROPARIETAL FASCIAL FLAP IS NOTCORRECT?A) Temporal scalp alopecia occurs in over 25 percent of cases.B) Temporal artery course is inconsistent in microtia patients.C) Hyperpigmentation occurs in the overlying scalp.D) Use results in diminished definition of the reconstructed ear.E) All of the above
9. WHICH OF THE FOLLOWING COMPLICATIONS DOES NOT RESULT FROM ANTERIOR CHEST WALLHARVEST OF COSTAL CARTILAGE?A) Hypertrophic scarB) Diminished respiratory reserveC) Chest wall deformityD) PneumothoraxE) None of the above
To complete the examination for CME credit, turn to page 387 for instructions and the response form.