cms and doh enforcement activities and proactive strategies · cms and doh enforcement activities...
TRANSCRIPT
CMS and DOH Enforcement Activities and Proactive
Strategies
PACAH 2017 Spring Conference
April 27, 2017
Paula G. Sanders, Esquire
CMS Requirements of Participation (RoPs)
• Published October 4, 2016 (81 Fed. Reg. 68688)
available at https://www.federalregister.gov/documents/2016/10/04
• First comprehensive update since 1991
• CMS’ estimated cost per SNF Year 1: ~ $62,900
Subsequent years: ~$55,000
(81 Fed. Reg. 68844)
2
Survey Implementation
• Phase 1: effective November 28, 2016 Same survey process
New RoPs merged into existing F-tags, SOM, Appendix PP, Eff. March 10, 2017, available at: https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/Downloads/Survey-and-Cert-Letter-17-19.pdf
• Phase 2: effective November 28, 2017 New SOM Appendix PP with all new F-tags
New survey process combines “traditional” and “Quality Indicator Survey” (QIS)
3
Department of Justice (DOJ) Initiatives
• Deputy Attorney General Yates issues memo, ”Individual Accountability for Wrongdoing,” on corporation cooperation with identification of culpable individuals, Sept. 9, 2015 (“Yates Memo)
• Assistant Attorney General Caldwell outlines how criminal division compliance counsel will identify effective compliance programs, Nov. 2, 2015
• DOJ hires new “Compliance Counsel” for Fraud Division, Hui Chen , as of Nov. 3, 2015
Changing Enforcement Environment
• DOJ launches 10 Elder Justice Task Forces including Eastern District of PA, March 30, 2016
Pursue nursing homes that provide grossly substandard care
• Centers for Medicare and Medicaid Services (CMS) releases new Civil Money Penalty (CMP) Analytic Tool
5

DOH CP “Guideline”
6
Mandatory Referrals
• CMS refers all civil money penalties (CMPs) to DOJ pursuant to a Memorandum of Understanding
• DOH is statutorily required to report immediately to the PA Attorney General (AG) or local law enforcement whenever it has “reasonable cause to believe” that a care dependent adult has suffered bodily injury or been unlawfully restrained” See, Act
28 of 1995, Neglect of Care-Dependent Person, 18 Pa.C.S. § 2713
Referrals to state licensing boards
7

Increased Enforcement a Reality
• Marked increase in citations and sanctions
• Marked increase in CMS & DOH civil money penalties
8
Federal Civil Penalties Inflation Adjustment Act Improvements Act
of 2015
• Intended to improve “effectiveness” of CMPs and maintain “deterrent effect” of CMPs
• Requires annual “adjustment” of CMPs using October Consumer Price Index for all Urban Consumers (CPI-U)
• First increase was in 2016; most recent increase effective February 3, 2017 (82 Fed. Reg. 9174, 2/3/2017)
Federal Civil Penalties Inflation Adjustment Act Improvements Act
of 2015
• Secretary of covered agency may provide lesser CMP by less than the new formula through a rulemaking only if:
Secretary finds that increasing penalty by required amount will have a negative economic impact or that the social costs outweigh the benefits and
Director of the Office of Management and Budget (OMB) concurs with this analysis
10

Impact of Inflation Adjustment Act
• CMS CMPs for surveys have increased astronomically
Pre-August2016
August 1, 2016
February 3, 2017
Cat.2 Per Day $50 -$3,000 $103 -$6,188
$105 –$6,289
Cat. 2 Per Instance
$1,000 -$10,000
$2,063 –$20,628
$2,097 -$20,965
Cat. 3 Per Day $3,050 -$10,000
$6,291 -$20,628
$6,394 -$20,955
Cat. 3 Per Instance
$1,000 -$10,000
$2,063 –$20,628
$2,097 -$20,965
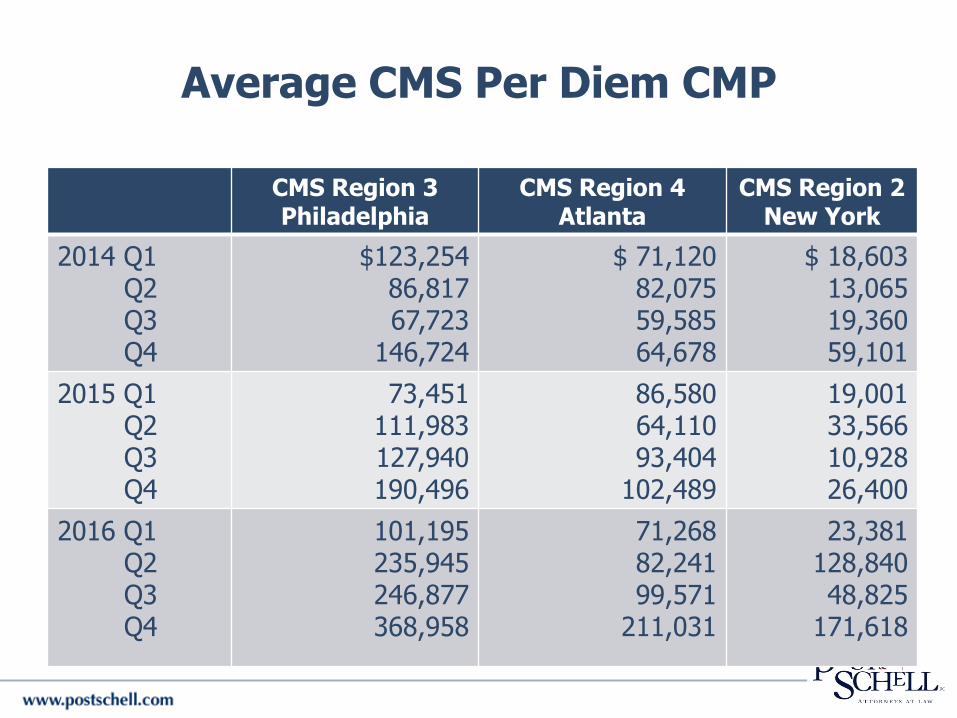
Average CMS Per Diem CMP
CMS Region 3Philadelphia
CMS Region 4Atlanta
CMS Region 2New York
2014 Q1Q2Q3Q4
$123,25486,81767,723
146,724
$ 71,12082,07559,58564,678
$ 18,60313,06519,36059,101
2015 Q1Q2Q3Q4
73,451111,983127,940190,496
86,58064,11093,404
102,489
19,00133,56610,92826,400
2016 Q1Q2Q3Q4
101,195235,945246,877368,958
71,26882,24199,571
211,031
23,381128,84048,825
171,618

Pennsylvania Nursing Care Facility Sanctions
P1 & CP P2 & CP P1 Only P2 Only P3 Only P4 Only BAN CP Only
Amount Imposed
2014 1 2 4 2 8 $62,000.00
2015 6 2 7 2 1 1 1 24 $176,170.00
2016 4 31 4 51 $401,600.00
Jan.-March 2017
1 3 1 2 63 $570,250.00

Immediate Jeopardy Citations
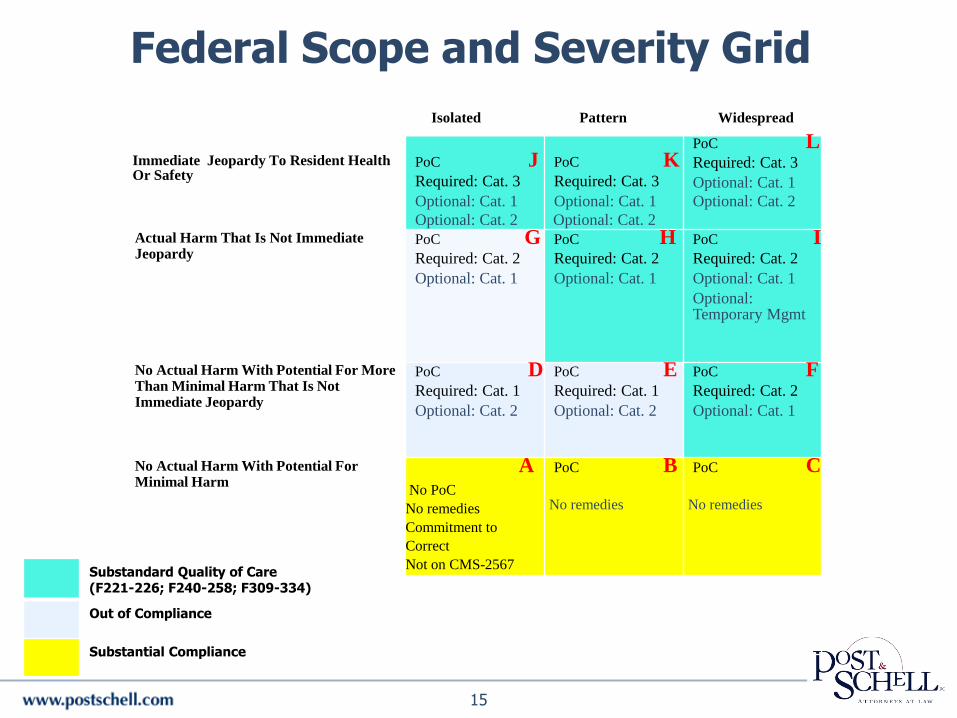
I
Immediate Jeopardy To Resident Health Or Safety
PoC JRequired: Cat. 3
Optional: Cat. 1
Optional: Cat. 2
PoC KRequired: Cat. 3
Optional: Cat. 1
Optional: Cat. 2
PoC LRequired: Cat. 3
Optional: Cat. 1
Optional: Cat. 2
Actual Harm That Is Not Immediate Jeopardy
PoC GRequired: Cat. 2
Optional: Cat. 1
PoC HRequired: Cat. 2
Optional: Cat. 1
PoC IRequired: Cat. 2
Optional: Cat. 1
Optional: Temporary Mgmt
No Actual Harm With Potential For More Than Minimal Harm That Is Not Immediate Jeopardy
PoC DRequired: Cat. 1
Optional: Cat. 2
PoC ERequired: Cat. 1
Optional: Cat. 2
PoC FRequired: Cat. 2
Optional: Cat. 1
No Actual Harm With Potential For Minimal Harm
ANo PoC
No remedies
Commitment to
Correct
Not on CMS-2567
PoC B
No remedies
PoC C
No remedies
Substandard Quality of Care (F221-226; F240-258; F309-334)
Out of Compliance
Substantial Compliance
15
Isolated Pattern Widespread
Federal Scope and Severity Grid

Federal Remedies Categories
Category 1 (Cat.1) Category 2 (Cat.2) Category 3 (Cat.3)
Directed Plan of Correction;State Monitor; and/or Directed In-Service Training
Note: If CMP >$10,4830 or SQC, automatic loss of Nurse Aide Training Competency Evaluation Program (NATCEP)
Denial of Payment for New Admissions;Denial of Payment for All Individuals imposed by CMS; Termination; Temp. Mgmt and/or Civil Money Penalties: Old: $50 - $3,000/day $1,000 - $10,000/ instanceNew: * $105 - $6,289/day$2,097 - $20,628/ instance
Temp. Mgmt.; Termination; Civil money penalties Old: 3,050-$10,000/day $1,000 - $10,000/ instanceNew:*$6,394 - $20,965/day$2,097 - $20,965/ instance
16
* Updated effective Feb. 3, 2017

Mandatory Immediate Imposition of Federal Remedies
• Immediate Jeopardy (IJ) on the current survey
• SQC deficiencies on current surrey
• G level at 42 CFR 483.13 (Resident Behavior and Facility Practices); 42 CFR 483.15 (Quality of Life); or 42 CFR 483.25 (Quality of Care)
• CMS S&C 16-31-NH: Mandatory Immediate Jeopardy of Federal Remedies and Assessment Factors Used to Determine the Seriousness of Deficiencies for Nursing Homes, (July 2016)
17

Mandatory Immediate Imposition of Federal Remedies
• Actual harm or above on current survey and deficiencies of actual harm or above on the previous standard health or LSC survey OR deficiencies of actual harm or above on any type of survey between the current survey and the last standard survey surveys must be separated by a period of compliance (i.e., from different noncompliance cycles)
• Special Focus Facility (SFF) has a deficiency citation at level “F” or higher on its current survey
18
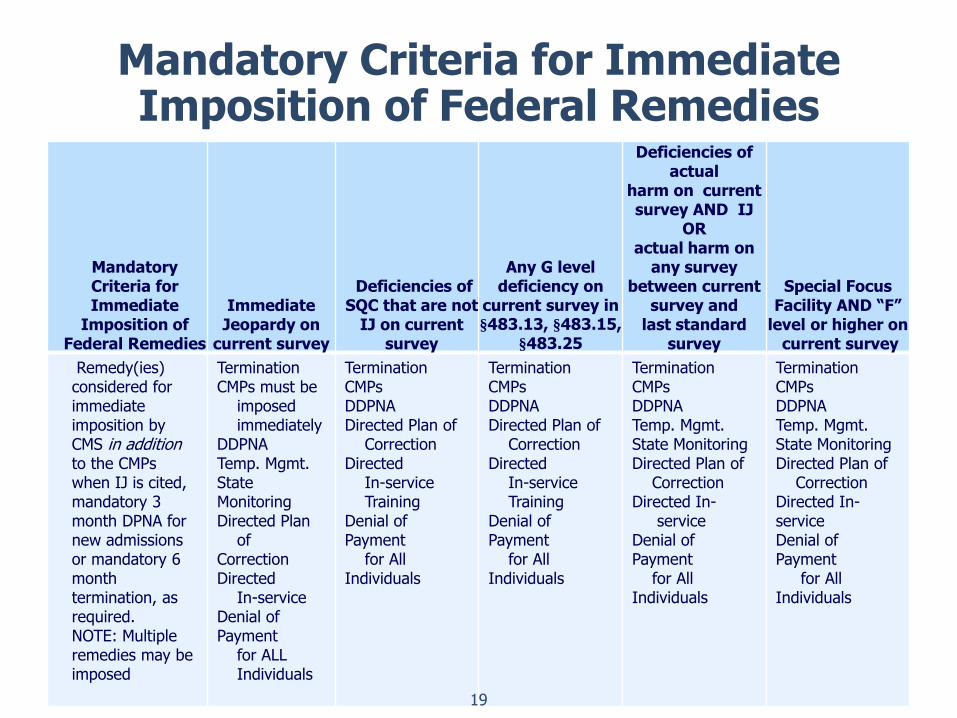
Mandatory Criteria for ImmediateImposition of Federal Remedies
Mandatory Criteria for Immediate
Imposition of Federal Remedies
ImmediateJeopardy on
current survey
Deficiencies of SQC that are not
IJ on current survey
Any G level deficiency on
current survey in§483.13, §483.15,
§483.25
Deficiencies of actual
harm on current survey AND IJ
OR actual harm on
any survey between current
survey and last standard
survey
Special Focus Facility AND “F”
level or higher oncurrent survey
Remedy(ies) considered for immediate imposition by CMS in addition to the CMPs when IJ is cited, mandatory 3month DPNA for new admissions or mandatory 6month termination, as required. NOTE: Multiple remedies may be imposed
TerminationCMPs must be
imposedimmediately
DDPNATemp. Mgmt.State MonitoringDirected Plan
of CorrectionDirected
In-serviceDenial of Payment
for ALL Individuals
TerminationCMPsDDPNADirected Plan of
CorrectionDirected
In-service Training
Denial of Payment
for All Individuals
TerminationCMPsDDPNADirected Plan of
CorrectionDirected
In-service Training
Denial of Payment
for All Individuals
TerminationCMPsDDPNATemp. Mgmt.State MonitoringDirected Plan of
CorrectionDirected In-
serviceDenial of Payment
for All Individuals
TerminationCMPsDDPNATemp. Mgmt.State MonitoringDirected Plan of
CorrectionDirected In-serviceDenial of Payment
for All Individuals
19

Financial Hardship Requests
• Possible reduction of CMPs or 12 month repayment plan
• Analytic tool options: facility’s documentation proves that:
(1) “the facility lacks sufficient assets to pay the CMP without having to go out of business,” or
(2) “the facility does not lack sufficient assets to pay the CMP without having to go out of business.”
20

Financial Hardship Requests
• “[N]ot CMS's intent to impose CMPs that could, in and of themselves, put providers out of business.”
• Providers can file “compelling evidence of financial hardship,” which CMS “is willing, in the interest of the Medicare and Medicaid programs and their beneficiaries, to consider.”
• Must be filed within 15 days of CMS CMP letter
21
Areas of Potential Substandard Quality Of Care
• Major Expansion
• Resident Rights §483.10
Resident Rights
Exercise of Rights
Respect and Dignity
Self-Determination
Safe Environment
• F Tags
F221 – 226
F240 – 258
F309 - 334
22
New CMS CMP Analytic Tool
• New approach to federal per day (PD) Civil Money Penalties (CMPs)
• Begin CMP on 1st day noncompliance is documented, even if that date precedes the first day of the current survey
Unless facility can demonstrate that it corrected the noncompliance prior to the current survey (past noncompliance)
CMS Survey & Certification Memo, “Civil Money Penalty (CMP) Analytic Tool and Submission of CMP Tool Cases, S&C: 15-16-NH (Dec. 19, 2014)
23
Starting the PD CMP
• Calculate the start date for the proposed CMP with the “first supportable date of noncompliance, as determined by the evidence documented by surveyors in the statement of deficiencies (CMS form 2567)”
• Surveyors instructed to “determine the earliest date for which supportable evidence shows that the non-compliant practice began”
24

Ambiguity About Start of Deficient Practice
• CMS analysts will contact state agency if start date is ambiguous or not clearly identified and supportable, to see if start date can be determined
• CMS analysts required to document their discussions and conclusion with the state agency
25
If Start Date Not Determinable
• If start date cannot be determined, then PD CMP would start on 1st day during the survey on which the survey team identified the noncompliant practice
• If the team cannot document the first day of noncompliance, then the CMP should start on the day the noncompliance was observed and documented at the time of the current survey
26
CMS: Past Noncompliance
• Reduce a CMP by 50% if:
(i) self-reported noncompliance to CMS or
State before it was otherwise identified by or
reported to CMS or State; and
(ii) correction of the self-reported
noncompliance occurred within 15 days of the
incident. 42 C.F.R. § 488.438
27

Get Credit for Correcting Past Noncompliance
• Treat any incident that results in reporting to DOH as you would if it was on your 2567
• Develop corrective action and document monitoring and auditing for ongoing compliance
• Give evidence to surveyors at the time of the survey that a monitoring plan was implemented and maintained to assure continued compliance.

CMS: Past Noncompliance Hypo
• Conflicting information about what staff/
departments were responsible for evaluating
residents’ transfer status
Under facility protocol, the nursing staff was
responsible
Interview with nurse indicated that rehabilitation
therapy department was responsible for
performing resident assessments for transfers
and/or use of lifts
29
Past Noncompliance Hypo (cont.)
During onsite survey, clear that staff did not have a consistent understanding of facility’s protocol for assessing appropriate transfer status
Facility failed to implement a mechanism(s) for ongoing monitoring to assure that residents were being transferred in accordance with their needs/assessment in order to ensure their safety
Facility failed to demonstrate that they implemented adequate corrective measures to address this event, after the incident occurred and before DOH’s survey
30
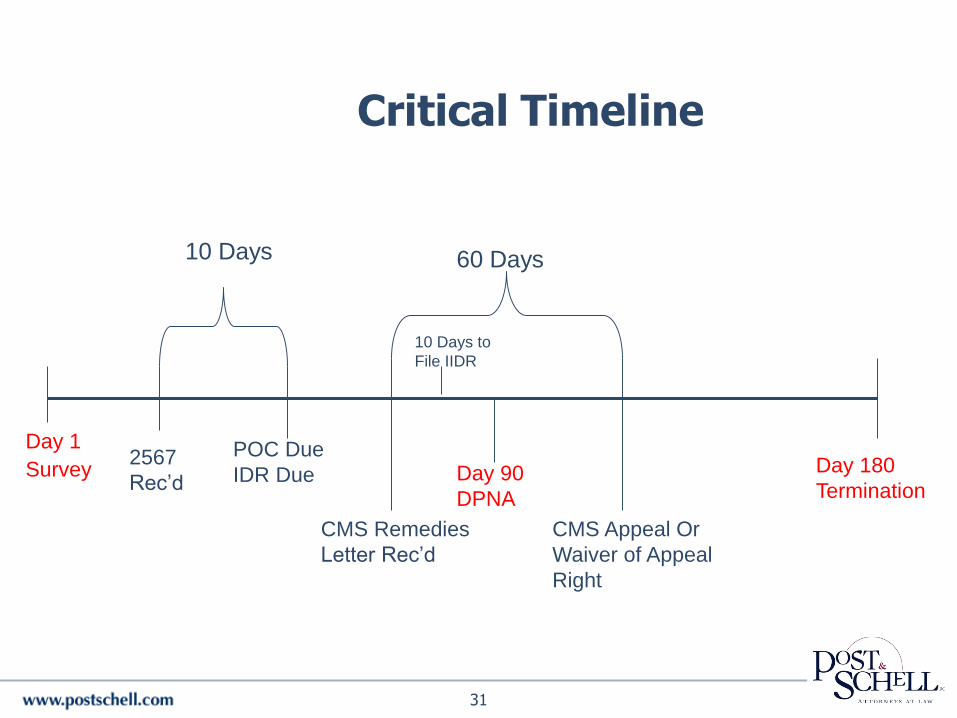
Critical Timeline
Day 1
Survey2567
Rec’d
10 Days
POC Due
IDR Due
CMS Remedies
Letter Rec’d
Day 90
DPNA
CMS Appeal Or
Waiver of Appeal
Right
60 Days
Day 180
Termination
31
10 Days to
File IIDR
How to Read the 2567
• What are the deficiencies?
• What are the regulatory violations?
Federal
State
• What is the best way to respond?
32

Know Your Regulators
Sanction Letters
• DOH imposes state sanctions against license and recommends federal sanctions to CMS
• CMS imposes sanctions against certification, often after time for state IDR has passed
CMS not required to follow DOH recommendation
• Challenges to federal CMP must include escrow of CMP
34
POC Disclaimer Language
• Preparation and submission of this POC is required by state and federal law. This POC does not constitute an admission for purposes of general liability, professional malpractice or any other court proceeding.
35

“Required” POC Elements
• What corrective action(s) will be accomplished for residents affected by the deficient practice?
• How will you identify other residents having the potential to be affected by the same deficient practice and corrective actions?
• What measures will be put in place or system changes will you make to ensure that the deficient practice does not recur?
36
“Required” POC Elements
• How will the corrective action be monitored to ensure the deficient practice will not recur, i.e., what quality assurance programs will be established?
• Dates when the corrective action will be completed.
37
Strategies for Preparing Effective POCs
• Less is more
• Read the F Tags and the state tags
• Don’t be afraid to have your POC rejected
• Be responsive and responsible
Don’t overpromise
Don’t admit liability
38
Strategies for Preparing Effective POCs
• Don’t go overboard with policies, procedures and plans of correction
• Keep your date of compliance as short as possible
Begin implementing corrective action during the survey and document corrections (e.g., inservicing of staff)
39
Post Survey Revisit
• Nature of deficiency dictates scope of revisit
• Required whenever S/S F-L level deficiencies exist
• 3rd Revisit subject to CMS Regional Office (RO) approval
• 4th Revisit subject to CMS Central Office (CO) approval
40

Survey Strategy
• Reevaluate how you approach survey
Surveyors may reject any documents not provided at time of survey
Where are your critical documents
What do your medical records look like
How up to date is your filing
• Review 2567 carefully and prepare IDRs for any factual inaccuracies
41
Prepare Now
• Review and implement new ROPs – focus on grievances, resident rights, policies and procedures
• Ongoing review of MDS accuracy
• Engage your medical director and attending physicians
• Reevaluate wound care protocol and scope of practice issues
42
Change Your Mock Survey Process
• Interview residents
• Interview families
• Interview staff
Prepare direct care staff for better surveyor interaction
What do you say when you are not sure of the answer?
43

QA and QAPI
• Make better use of your Quality Assurance (QA) and/or Quality Assurance & Process Improvement (QAPI) committee
• DOH expects to see evidence of investigations
Multiple issues should be documented separately
• Make certain electronic record reports (e.g., call bells) part of QAPI if they are used such purposes
44

Collateral Issues
• Potential repayment
Obligation to repay within 60 days of identification of known overpayment
• PA Preventable Serious Adverse Events (PSAE) Act
DOH has been filing reports with Department of Human Services (DHS, formerly Department of Public Welfare)
45
DOH Surveys: What Happened?
• Kaiser Family Foundation: about 40 percent of PA nursing homes have relatively low 5-star ratings, of 1 or 2-stars (May 2015)
See also: http://www.newsweek.com/you-dont-want-be-old-these-states-333052
• Community Legal Services of Philadelphia (CLS) report – “CARELESS: How the Pennsylvania Department of Health has Risked the Lives of Elderly and Disabled Nursing Home Residents” (June 2015)
46
CLS Recommendations to Gov. Wolf
• Conduct thorough investigation into why DOH has
failed to properly investigate nursing homes and
enforce regulations
• Implement system-wide changes within DOH to
ensure enforcement of regulations
• Require all DOH nursing home investigators be
retrained on an ongoing basis to ensure patient
safety
47
CLS Recommendations to Gov. Wolf
• Require DOH to provide better transparency to
public regarding investigations & characterization
of harm
• Provide better information to public about SNFs so
prospective SNF residents and families can make
informed decisions about care
48
DOH Surveys: What Happened?
• ProPublica reports PA cited fewest serious deficiencies of any state, tied with HI and DE (.02) “Inconsistent Penalties Across the States,” updated July 2015
• PA Attorney General staffing investigations
49
PA Attorney General (AG) Staffing Investigations
• 7 companies targeted in contingency fee contract between AG and private law firm (Cohen Milstein)
• April 2015: Declaratory judgment case to AG’s authority to:
Hire contingency fee counsel; and
Investigate staffing using Unfair Trade Practice and Consumer Protection laws
• Dec. 2016: SNFs’ declaratory judgment action ultimately dismissed
50
PA AG Staffing Investigations
• July 2015: AG files lawsuit against Golden Living
• Oct. 2016: Reliant settlement $2 million
• Nov. 2016: AG files suit against Grane Healthcare-
• Mar. 2017: Commonwealth Court dismisses AG lawsuit
• April 2017: AG appeals to PA Supreme Ct.51
DOH Response
• Accelerate efforts to evaluate regulatory process to determine what additional measures can be taken to ensure enhance quality
• Engage Auditor General to audit DOH policies and procedures to recommend ways to improve how DOH enforces its statutory enforcement authority
• Form task force charged with identifying ways DOH can advance quality improvement
52

More Scrutiny of DOH
• PA Auditor General Performance Audit Report: Pennsylvania Department of Health, issued July 26, 2016
• Generated extensive media coverage
“Failing the Frail: Bad care leads to dozens of avoidable deaths in Pa. Nursing Homes.”*
• Senator Casey requests CMS investigation of PA DOH
* www.pennlive.com/news/page/failing_the_frail_part_1.html (Aug 2, 2016)
53
OPTIONS FOR REFUTINGNEGATIVE SURVEY FINDINGS
54
Informal Dispute Resolution
• Does not toll the federal appeals timetable or delay enforcement action
• Successful IDR expunges deficiency from CMS 2567 and provides for rescission of enforcement action predicated on withdrawn deficiency
• CMS’ findings of noncompliance can overrule state’s conclusions
55
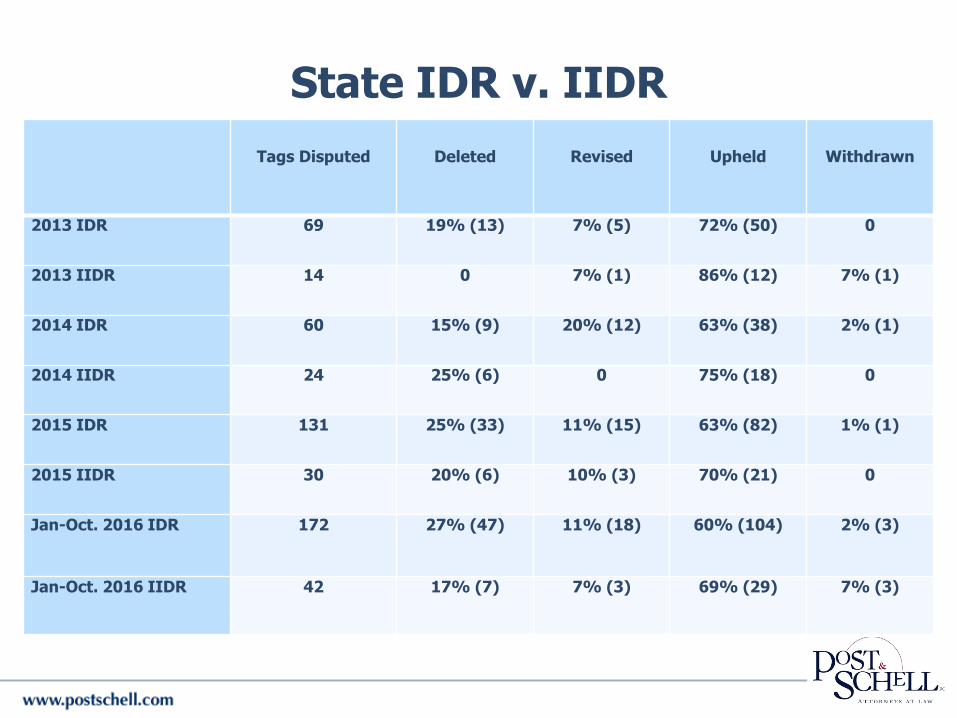
State IDR v. IIDR
Tags Disputed Deleted Revised Upheld Withdrawn
2013 IDR 69 19% (13) 7% (5) 72% (50) 0
2013 IIDR 14 0 7% (1) 86% (12) 7% (1)
2014 IDR 60 15% (9) 20% (12) 63% (38) 2% (1)
2014 IIDR 24 25% (6) 0 75% (18) 0
2015 IDR 131 25% (33) 11% (15) 63% (82) 1% (1)
2015 IIDR 30 20% (6) 10% (3) 70% (21) 0
Jan-Oct. 2016 IDR 172 27% (47) 11% (18) 60% (104) 2% (3)
Jan-Oct. 2016 IIDR 42 17% (7) 7% (3) 69% (29) 7% (3)
Sanction Letters
• Ability to file federal IIDR within 10 days of receipt of CMS CMP letter (often sent by certified or regular mail—keep envelope)
• Federal IIDR will often include contact of affected residents
• Waiver of appeal rights gets 35% reduction of CMP
File written notice within 60 days
57
Federal Appeals
• Departmental Appeals Board (DAB)
• U.S. District Court
• U.S. Court of Appeals
• Beyond?
58
State Appeals
• Administrative hearings
• Court appeals
59
Questions
Paula G. Sanders, EsquirePrincipal & Co-Chair, Health Care Practice Group
Post & Schell, [email protected]
717-612-6027
60