co-contraction and stretch reflexes in spasticity during
TRANSCRIPT

Journal ofNeurology, Neurosurgery, and Psychiatry, 1977, 40, 30-38
Co-contraction and stretch reflexes in spasticityduring treatment with baclofenD. L. McLELLAN'
From the Department ofNeurology, Section ofNeurological Sciences, The London Hospital, London
SUMMARY Surface electromyograms were recorded from the quadriceps and hamstring muscles of11 spastic patients during cyclical flexion and extension movements of the knee. A potentiometerstrapped to the knee recorded the angle of the joint, the output signal being displayed on an oscillo-scope. The patient used this signal to track a sine wave target for 20 cycles. The observer then movedthe patient's limb through a further 20 cycles tracking the same target. Recordings were repeated atintervals for four hours after an oral dose of baclofen. Analysis of the recordings showed that theresponse of a spastic muscle to lengthening is not the same during passive movement as duringvoluntary movement. In mild spasticity stretch reflexes appear to be suppressed by voluntary effortwhereas in severe spasticity they are enhanced. Baclofen suppressed the response to passive stretchby over 30% at plasma concentrations of over 250 ng/ml and by 5000 at concentrations of over400 ng/ml, but this effect was largely extinguished during voluntary movement.
In clinical practice, spasticity denotes a characteristicsyndrome of increased stretch reflexes and abnormalpatterns of muscular contraction leading to impairedvoluntary movement. Stretch reflexes are usuallytested by gauging the strength of reflex muscularcontraction during passive movement of the limb.It is often assumed that similar contraction (co-contraction) occurs during voluntary movement andthus opposes it. There are two obvious objections tothis assumption. Firstly, some spastic patients haverelatively flaccid limbs but nevertheless showtypically 'spastic' patterns of movement. Secondly,drugs that reduce stretch reflex activity to theclinician's satisfaction are often discarded as in-effective by the patient. The present investigationwas designed to assess the amount of co-contractionin a spastic muscle as it lengthens during the course ofa voluntary movement, and to compare this with thecontractions induced by passive movement at thesame rate. Baclofen, an anti-spastic drug thatsuppresses spinal reflexes, was administered to thepatients during the recordings in order to see whetherits effects upon muscle tone were accompanied bysuppression of co-contraction.
I Address for correspondence: Department of Neurologic Surgery,St. Barnabas Hospital, 4422 Third Avenue, Bronx, New York 10457,USA.Accepted 13 September 1976
Methods
SUBJECTS STUDIEDThe patients were selected on the basis of surfaceelectromyograms from the quadriceps and ham-string muscles during voluntary flexion and extensionmovements of the knee. They sat with both legshanging over the edge of a couch for this screeningprocedure. Surprisingly, most patients with moderatespasticity-that is, with brisk tendon reflexes,increased muscle tone, and extensor plantar res-ponses, but with moderate to strong voluntary powerand only mild impairment of gait-showed little, ifany, co-contraction under these conditions. Mostpatients were unable voluntarily to flex and extendthe knee faster than once a second. This is slower thannormal subjects (3-4 Hz) and it was also slower, inmost cases, than the threshold rate at which passivemovement provoked a stretch response. Thusslowing of voluntary movement could rarely beascribed to co-contraction alone. Out of 32 subjectsscreened in this way, 14 were finally selected who hadboth co-contraction during voluntary movement anda stretch response to passive movement at the samerate. Satisfactory recordings were obtained from11 of the patients whose clinical details are shown inthe Table.
PROCEDUREInformed consent was given by each patient, and all
30
Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from

Co-contraction and stretch reflexes in spasticity during treatment with baclofen
Table Clinical details of 11 spastic subjects
Patient No. Sex Age (yr) Diagnosis Troublesome Troublesome Effect ofbaclofenclonus spasms
Co-contrac tion Patients optingforsuppressed long-term treatment
I M 46 Idiopathic spastic paresis -+ + - *2 M 36 Multiple sclerosis + + +3 M 56 Idiopathic spastic paresis -- + ++4 M 52 Idiopathic spastic paresis - +5 M 52 Idiopathic spastic paresis + + ++ *6 M 37 Idiopathic spastic paresis + +7 M 26 Spinal cord injury + + +8 M 20 Spinal tuberculosis + +9 F 36 Multiple sclerosis - - -10 M 45 Multiple sclerosis - +11 M 14 Idiopathic spastic paresis - + - *
medication was stopped 48 hours before testing.Each patient was studied during the afternoon, had alight lunch of cold meat salad, dessert, with water todrink, and was then asked to empty bowel and bladderif possible. For the recordings, patients sat on a foamrubber block 6 cm thick with the back and shoulderssupported and both legs hanging over the edge of acouch (Fig. 1). A linear potentiometer was strappedto the knee to record flexion and extension move-ments of the joint. Surface recording electrodes wereapplied by adhesive rings with an inside diameter of5 mm to the skin overlying the quadriceps and ham-string muscles. The electrodes were placed 3 cmapart in the long axis of the muscle over the centre ofthe muscle belly. Patients were earthed via a strip ofVelcro tape containing a lead core and soaked inphysiological saline wrapped round the lower end ofthe thigh. The recording electrodes were fed througha standard DISA 14C 11 electromyograph, and theoutputs from the two EMG channels and thepotentiometer were recorded on tape for further
analysis, using a 4-channel Fenlow TR4 tape recorder.Practice established the fastest rate at which the
subject was able to continue to flex and extend theknee for 45 seconds through an arc of approxi-mately 1080O from full extension. The output fromthe goniometer was displayed on a storage oscillo-scope in front of the patient. A sine-wave target wasthen tailored for the patient's fastest sustainable rateof accurate movement using a variable functiongenerator (Wavetek 114), and the time base of theoscilloscope sweep was adjusted to allow approxi-mately 10 cycles to be displayed during the course of asingle sweep, using the storage mode.
This display of a series of 10 cycles was used as atarget that subjects then tracked with the gonio-meter output, by flexing and extending the knee.They were instructed to superimpose their signal uponthe target as the dot moved slowly across the screen.Thus the target was not only predictable, but waspresented as a stationary display upon which thesubject's signal was superimposed. After several trial
Fig. 1 Position ofsubject duringrecording. The oscilloscope showsa sine wave target. The subjecttracks the target using the outputsignalfrom the goniometerstrapped to his knee.
C
31
Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from

D. L. McLellan
sessions in which a target that was too difficultcould be expanded, in effect made slower, thepatient's attempt to follow the target for 20 cycles wasrecorded. Two further control readings were ob-tained at five minute intervals. A clinical assessmentof 'muscle tone' was made by the observer on eachoccasion by passive movements of the knee. In sixsubjects, passive movements were performed manu-
ally by the observer, one hand being placed just abovethe knee to steady the thigh while the other graspedthe ankle and performed the movement. The observerused the same system of tracking as the subjecthad done to follow the same target, ensuring thatboth voluntary and passive movements followedthe same pattern. The observer did not touch thesubject's limb during the periods of voluntarymovement.
After the series of control readings, an oral dose of20 mg baclofen was given (time 0) and furtherrecordings made at 0.5, 1.0, 1.5, 2.0, 3 and 4 hoursafter ingestion.Four patients attended twice. On one of these
occasions each was given two matching placebotablets instead of baclofen. The nature of the tabletswas known to the observer but not to the subject.Before tablets were given and again after each phaseof the recording, 20 ml of venous blood were with-drawn into a heparinised container for estimation ofthe plasma baclofen concentration. The plasma was
separated at once by centrifugation and the samplesstored at -200C until analysed, except for thesamples obtained during placebo runs which were
discarded.Recordings were also obtained from four normal
subjects aged 26-44 years who were not takingchemotherapy; the targets were set up as above andthe amount of co-contraction was recorded duringthree sessions, each consisting of 20 cycles ofvoluntary movement.
ANALYSIS OF ELECTROMYOGRAMSThe surface electromyograms were displayed on an
oscilloscope and on a loudspeaker during analysis inorder to detect possible artefacts. The signal fromeach muscle was half-wave rectified and then inte-grated electronically in two ways. First, a summingintegrator was used to sum the area of the signalduring specified phases of the movement. The gonio-meter output was used to trigger the integrator so thatthe extremes of flexion and extension were ignored:only the signals generated while the knee movedthrough the middle 450 of its arc were summed. Thesignals from flexion and extension were analysedseparately for each muscle. Data of voluntary move-
ment were available for 11 patients and of corres-
ponding passive movement for six patients.
The second system of integration used a smoothingtime constant of 100 ms that gave a continuousindication of the amount or profile of electromyo-graphic activity during the course of each cycle.The goniometer output and the rectified smoothedEMG from quadriceps and hamstring muscles werefed into a Biomac 1000 computer operating in theaveraging mode. It was found that 250 data points perchannel were adequate to cover a sweep time of2.56 seconds or less, but if doubt remained about thetiming of the peak EMG activity, the tapes werereanalysed using 500 data points per channel. Thecomputer was triggered by the goniometer outputand the analysis time chosen to include slightlymore than one cycle of movement. Thus alternatecycles were accepted by the averager and a second runthrough the tape was necessary to include the othersuntil 16 cycles had been analysed. The system wassimilar in principle to that devised by Burke et al.(1971). The averaged goniometer and integratedEMG signals were written out on an X-Y plotter,allowing identification of the timing of the peakEMG and its relationship to muscle length and therate of change of length.
ESTIMATION OF PLASMA BACLOFEN CONCENTRATIONThe samples were stored at - 20°C as above andanalysed by the Department of PharmacologicalChemistry, Ciba-Geigy Ltd., Basle, using a gas-liquid chromatographic assay procedure (Degen andRiess, 1976).
Results
PLASMA BACLOFEN CONCENTRATIONSNo baclofen was detected in any of the controlsamples. By half an hour all except subject 8 haddetectable concentrations of baclofen in the plasma,and the concentration increased rapidly, reaching apeak between one and two hours after ingestion.The pooled data from the 11 subjects are shown inFig. 2.
VOLUNTARY MOVEMENT-INDEX OF CO-CONTRACTIONIn order to avoid the problems inherent in comparingEMG amplitudes in different subjects, and in thesame subjects at different times, EMG activitywas expressed as a ratio. The ratio was derived fromthe records of the same muscle undergoing similardisplacements under different conditions, withintervals of less than four minutes between recordings.The amount of co-contraction-that is, the amountof contraction of the antagonist during voluntarymovement-was expressed as the ratio:
32
Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from

Co-contractioni an,d stretch reflexes in spasticity during treatnient wvith baclofen3
r- 60-bO-
o 50-
040Cu-o 30-
Ouads_20Upper limits of normnal 10-
Hams -_0
E 500-
o'5 400-0 o300-D .za 200-
o 100-
0 0-
Quadricep
Hamstrings
EMG in lengthening muscleduring passive stretch % = lengthening
EMG in lengthening muscle indexduring voluntary movementAs the co-contraction index was usually constant,
o2 z 90-u - 901
' 70
0
x0
-v
r -I 1
0 2 3Time afl-cr baclofen (h)
70, 0
aQ-x, X.20
-603
250 -
.D(4
Fig. 2 Data from 1I spastie patients showing timecourse ofchanges in the mean index ofco-contractionin quadriceps and hamstring muscles, and in plasmabaclofen concentration, after an oral dose of20 mgbaclofen. Arrows indicate upper limit ofco-contractionrecordedfrom four normal subjects. ± I SD shown forbaclofen levels.
Sum ofEMG duringlengthening of muscle % = index ofSum ofEMG during co-contractionshortening of muscle
In normal subjects under the particular conditionsof these recordings, the greatest index of co-con-traction recorded from the quadriceps was 17% andthe greatest index recorded from the hamstrings was50%. The patients were able to perform the move-ments at less than half the speed of normal subjects.The pooled data from the spastic patients show
little change in the indices of co-contraction for eithermuscle during the course of the afternoon's recording(Fig. 2), there being no significant difference betweenthe effects of baclofen and the effects of placebo(Fig. 3). Analysis of individual data did, however,show that patients differed in their response tobaclofen (Fig. 4). The patients showing a definiteeffect tended to suffer from spontaneous clonus andobvious spasms during voluntary movement, pro-nounced suppression of co-contraction being foundin patients 2, 3, and 5 (see Table). Patients whoresponded in this way had similar baclofen con-centrations to those who did not.
PASSIVE MOVEMENT-LENGTHENING INDEX
Passive movement was analysed in six of the patients.It did not produce contraction in normal subjects,nor in the majority of mildly spastic patients initiallyconsidered for study. For the reasons given above,the amount of EMG in the passively stretchedmuscle was given as the ratio:
O 400-uo o 300-.0 Z
200-
a U 100-u
0 2 3 4Time after tablets (h)
Fig. 3 Mean data from six spastic patients showing timecourse of changes in quadriceps co-contraction (x),quadriceps response to passive stretch (-), andplasmabaclofen concentration after an oral dose ofbaclofen( ) andplacebo (-----, four patients only). Theappearance ofbaclofen in plasma is accompanied by areduction in response to passive stretch, but co-contractionduring voluntary movement is unchanged. ± 1 SD shownfor lengthening index and baclofen levels.
o 901
a- 80-
c_ 00 30
o~ 20C-_
ou m 400u o 3C0-0)5
10
D oj
E U 400-3001
2ll200-I
aE0 ui IIC)XC
0 0
Patient SI \\
-v------a
4---
// Patient 7Patient 7
/--II, Patient 7
0 2 3 4Time after baclofen (h)
Fig. 4 Data from two spastic patients, showing timecourse ofchanges in the amount ofco-contraction ofquadriceps muscles and in plasma baclofen concentrations.Plasma levels ofbaclofen were similar in both subjects.Patient 7 suffered spontaneous clonus and spasms whichwere suppressed by baclofen, but co-contraction was notsuppressed in patient 5.
33
Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from

D. L. McLellan
this lengthening index principally reflected theamount of activity induced by passive stretch. Ifco-contraction were to be suppressed, the lengtheningindex would tend to underestimate the amount bywhich the response to passive stretch had declined.
Responses to passive stretch of the quadricepsmuscle were reduced by baclofen in all six subjectsbut placebo tablets had no effect (Fig. 3). Thelengthening index at one and 1 J hours after baclofenwas significantly different from the control values(p< 0.02 using the paired t test), and was significantlydifferent also from the values obtained in the samesubjects at one and 1 j hours after placebo (p < 0.05).Placebo tablets caused no significant change in thelengthening index of the quadriceps. The response tostretch declined by more than 30% once the plasmabaclofen concentration reached 250 ng/ml, beingalmost halved at concentrations of over 400 ng/ml(Fig. 4). That this change was due to baclofen isfurther indicated by the delay in suppression occur-ring in patient 8, the only subject in whom baclofenwas still undetected in the plasma half an hour afteringestion (Fig. 5). Despite a pronounced effect uponpassive stretch, co-contraction was virtually un-changed (Figs. 3 and 5).
.2 130-
_ 01IIo- 80 00~~~~~~~~~~~U,z6 I00- 7 0
70 C-00-~~ ~ ~~~~~~3
C E Q0 7
o 4001
o 200-
0Io
'-c2
Time after baclofen (h)3 4
Fig. 5 Effect ofbaclofen in patient 8. Suppression ofresponse to passive stretch, andpossibly ofco-contraction,is delayed untilplasma baclofen concentration belatedlystarts to rise.
The responses obtained from the hamstringsmuscle during passive stretch fluctuated widelyduring the course of the recording session, despitereasonably consistent levels of hamstring co-con-traction. The lengthening ratio sometimes variedfrom 20% to 500% from one half hour to the next.Thus the amount of contraction during passive
stretch was sometimes much less than the amount ofco-contraction of the hamstrings, and at other timesgreatly exceeded it. By contrast, the amount ofEMGduring passive stretch of the quadriceps was alwaysless than the EMG during co-contraction. This mayhave reflected partly a greater instability in hamstringstretch responses, and partly a restraining action ofthe quadriceps as it helped to track the target duringthe flexion phase, when gravity was assisting themovement. It was to minimise such artefacts that thepatient's fastest rate of movement was used in settingup the target. The hamstring response to passivestretch was too variable for useful quantitativeanalysis.
PROFILES OF CONTRACTION IN LENGTHENINGMUSCLE-PASSIVE MOVEMENTThe characteristic response of the quadriceps isshown in Fig. 6. If one complete cycle of the kneemovement is regarded as containing 3600, eachphase of movement-that is, flexion and extension-of the knee contains 1800. The quadriceps EMGactivity starts about 450 after extension of the kneeand the peak activity leads the most stretched point ofthe muscle by 900. This type of phase relationshipwas found in spastic quadriceps muscles by Burkeet al. (1971) and was considered to reflect an interplayof motor neurone facilitation by spindle primaryendings with inhibition by spindle secondary endings.Figure 6 shows progressive abolition and then re-covery of the stretch response in patient 11. As thestretch response declines, its starting point is delayedbut its peak does not shift phase.The hamstring responses are shown in Fig. 7. No
significant change is seen.
PROFILES OF CONTRACTION DURING VOLUNTARYMOVEMENTNormal subjects Figure 8 shows a typical profile ofEMG activity during voluntary movement by anormal subject. The activity in each muscle startsafter the limb has reached maximum velocity,deceleration resulting from declining contraction inthe agonist followed by increasing contraction of theantagonist.Spastic patients Figure 9 shows profiles of volun-tary movement, again from patient no. 11. Neithermuscle is silent at any stage. Quadriceps contractionstarts to build up much earlier than in a normalsubject, at about 450 rather than 1300 from fullextension of the knee. This is the point at whichcontraction is induced by passive stretch (Fig. 6).The peak of the passive stretch response coincidesprecisely with the peak of co-contraction (Fig. 10)Activation of the hamstrings is similarly advanced,occurring at about the same time as the passive
34
Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from

Co-contraction and stretch reflexes in spasticity during treatment with baclofen
cx t -_
C -.
70- _ _
105 -
min after baclofenFig. 6 Integrated EMG from quadriceps muscle ofpatient 11 during passive movement (16 cycles averaged).The target repeats every 2.44 second; sweep time shown is2.56 s. Top trace indicates position ofknee joint(10° 80° from full extension). The other traces show EMGactivity during the cycle before baclofen (C) and at varioustimes after baclofen. The stretch response is completelysuppressed at 70 min, reappearing at 105 min. The peakEMG leads the most stretched point by 90°. This phaselead does not alter as the amplitude ofresponsediminishes. (Note that the gain is increased in later tracesto allow satisfactory identification ofposition ofEMGpeak.)
stretch response (Fig. 7), well ahead of normalvoluntary contraction (Fig. 8). Moreover a secondburst of hamstring contraction is necessary to over-
come the abnormal quadriceps activity (Figs. 9and 11).
After baclofen, activation of the quadriceps isdelayed, though it does not become normal; thehamstrings are unaffected (Fig. 9).
Discussion
Symptomatic treatment of spasticity at the presenttime is mainly in the hands of physiotherapists whoencourage the patient to develop more usefulpatterns of muscular activity. Little is known aboutthe mechanisms that allow this to be achieved. Inpatients with acquired spasticity, especially those
85
105
Fig. 7 IntegratedEMGfrom hamstrings muscle ofpatient 11 during passive movement. Format in this andsubsequent figures is similar to Fig. 6. The peak EMGresponse occurs as muscle reaches its most stretchedpoint, and its timing is unaffected by baclofen.
a x t-0.
flexIa/
Quads
Hams
Fig. 8 Integrated EMG from quadriceps and hamstringsmuscles during voluntary tracking ofa target by a normalsubject. The target repeats every 0.9 s.
with stroke, loss of sensation contributes consider-ably to their inability to move, so that in practice it isimpossible to improve movement without retrainingsensory function at the same time.The importance of stretch reflexes in spasticity
cxt_-.P.
flex -_x--
s ,
C
3 5
70 --
35
11-1 \.'
3 5
Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from
D. L. McLellancxt-...
flex -.
cx r_
- -
-Iflex-.l
CQ-'\
I/ v
70min
C~~~~~~
r V\>r r
I IV70 -_~~~~~~~ _ -
I. a-11-.-I~~
IH
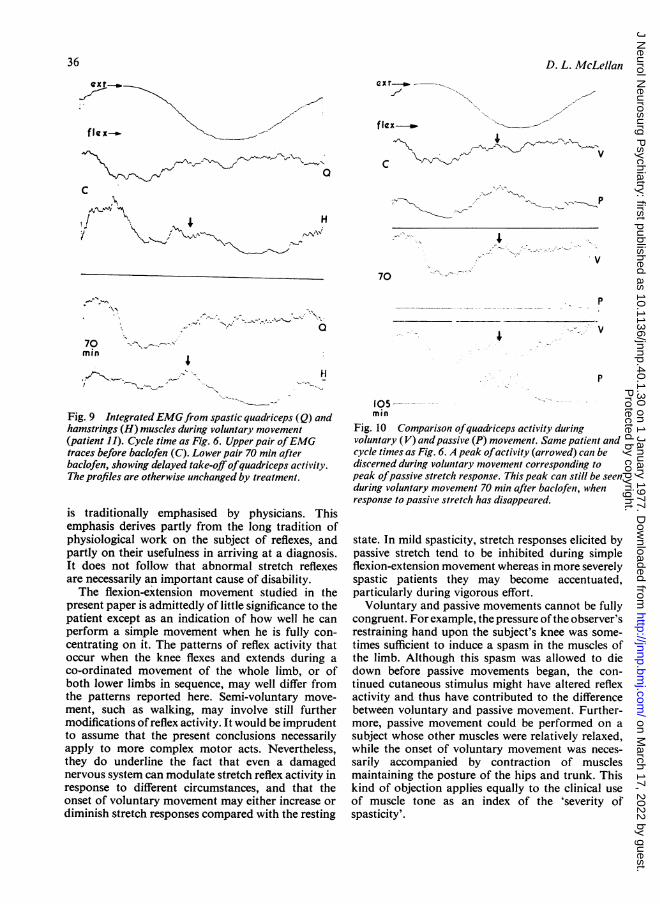
Fig. 9 IntegratedEMGfrom spastic quadriceps (Q) andhamstrings (H) muscles during voluntary movement(patient 11). Cycle time as Fig. 6. Upper pair ofEMGtraces before baclofen (C). Lower pair 70 min afterbaclofen, showing delayed take-offofquadriceps activity.The profiles are otherwise unchanged by treatment.
is traditionally emphasised by physicians. Thisemphasis derives partly from the long tradition ofphysiological work on the subject of reflexes, andpartly on their usefulness in arriving at a diagnosis.It does not follow that abnormal stretch reflexesare necessarily an important cause of disability.The flexion-extension movement studied in the
present paper is admittedly of little significance to thepatient except as an indication of how well he canperform a simple movement when he is fully con-centrating on it. The patterns of reflex activity thatoccur when the knee flexes and extends during aco-ordinated movement of the whole limb, or ofboth lower limbs in sequence, may well differ fromthe patterns reported here. Semi-voluntary move-ment, such as walking, may involve still furthermodifications ofreflex activity. It would be imprudentto assume that the present conclusions necessarilyapply to more complex motor acts. Nevertheless,they do underline the fact that even a damagednervous system can modulate stretch reflex activity inresponse to different circumstances, and that theonset of voluntary movement may either increase ordiminish stretch responses compared with the resting
P
4
P
105min
Fig. 10 Comparison ofquadriceps activity duringvoluntary (V) andpassive (P) movement. Same patienit andcycle times as Fig. 6. A peak ofactivity (arrowed) can bediscerned during volunitary movement corresponding topeak ofpassive stretch response. This peak can still be seenduring voluntary movement 70 min after baclofeni, whenresponse to passive stretch has disappeared.
state. In mild spasticity, stretch responses elicited bypassive stretch tend to be inhibited during simpleflexion-extension movement whereas in more severelyspastic patients they may become accentuated,particularly during vigorous effort.
Voluntary and passive movements cannot be fullycongruent. For example, thepressure ofthe observer'srestraining hand upon the subject's knee was some-times sufficient to induce a spasm in the muscles ofthe limb. Although this spasm was allowed to diedown before passive movements began, the con-tinued cutaneous stimulus might have altered reflexactivity and thus have contributed to the differencebetween voluntary and passive movement. Further-more, passive movement could be performed on asubject whose other muscles were relatively relaxed,while the onset of voluntary movement was neces-sarily accompanied by contraction of musclesmaintaining the posture of the hips and trunk. Thiskind of objection applies equally to the clinical useof muscle tone as an index of the 'severity ofspasticity'.
36
I
.., -..,I.,
I --\ - -'l- Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from

Co-contraction and stretch reflexes in spasticity during treatment with baclofen
ext-m-
C
70min
Fig. 11 Comnparison ofhamstrings activity durvoluntary (V) and passive (P) movement. Samecycle time as Fig. 6. Passive stretch ofhamstrin,a contraction slightly before the point at whichcontraction would be expected to occur (Fig. 8).movement in this spastic subject is characterisecadditional peak ofactivity during flexion ofkne,(arrowed). Presumably this is necessary to overcabnormalpeak ofquadriceps contraction arrowe
Fig. I0.
Under the conditions stated, co-contiquadriceps and hamstring muscle was r
consistent throughout an afternoon'ssession. The response of the quadricepspassive stretch was similarly stable but theresponse was variable.
This type of electromyographic techifirst used to measure the effect of backpassive stretch reflexes by Burke et al. (1lfound that baclofen increased the threshoat which muscle contraction was first indu(corresponds to the present findings c
initiation of the stretch response (Fig.baclofen, the rate of sinusoidal movemenhad chosen was insufficient to elicit a stretclso that the timing of the peak activity cocompared directly with the untreatedpresent findings show that, provided tlstretch remains constant, the peak actiN
quadriceps occurs at the same phase of the cycle,' after baclofen, even though the onset of contraction
is delayed. The effects of speeding up the stretchcycle were not recorded in the present study.
Baclofen reduces the amplitude of tendon jerks,H responses and slow passive stretch responses inspasticity (Birkmayer et al., 1967; Burke et al., 1971;
-'''"v McLellan, 1973). Patients whose stretch responsescan be diminished by cooling the limb respondbetter to baclofen than those in whom cooling has no
p effect (Knutson et al., 1973). Baclofen suppresses anumber of spinal cord functions but its net effect is to
-^.~ suppress the motor neurone facilitation that isgenerated by afferent input from the limb and fromthe muscle in particular (Pedersen et al., 1970;Knutson et al., 1973).
Baclofen appeared in the blood within half an hourof ingestion in 10 of the 11 patients, reaching a peakbetween one and two hours. The response to passivestretch was reduced by 30% at plasma concentrationsof over 250 ng/ml and by 50% at concentrations ofover 400 ng/ml (Fig. 4). Co-contraction during
P voluntary movement, while the quadriceps was beingstretched by the same amount and at the same rate asduring passive movement, was unaltered by baclofen
ring in most patients even when the plasma concentrationpatient and exceeded 400 ng/ml.gs induces This marked difference between the effect of baclo-voluntary fen upon passive stretch responses and its effect onVoluntary co-contraction suggests that different physiological
i by an mechanisms are involved. Reciprocal innervation is a
,ome the basic mechanism that operates not only on a seg-odin mental level, but can be controlled from the brain. It
is not clear whether co-contraction occurs as a directresult of inappropriate supraspinal drive on anta-gonist motor neurones, or whether it reflects un-suppressed segmental stretch responses in the
raction in antagonist. The latter possibility is supported by thereasonably similarity in the EMG profile of co-contraction withrecording the EMG of the stretch iesponse (Fig. 10) but it ismuscle to probable that both mechanisms are involved. Ithamstring remains to be proved that the observed peak in the
co-contraction profile depends upon an input fromnique was the stretched muscle. It would be interesting toofen upon observe the effect of blocking the muscle afferent971). They nerve fibres.ld velocity Drugs that suppress passive stretch reflexes areced, which prescribed for spasticity on the assumption thatf delayed stretch reflexes impede voluntary movement. The6). After present study shows that co-contraction may be
t that they unaffected even in patients whose passive stretchh response, responses have been halved by treatment. As in thetuld not be studies of Hedley et al. (1975) and Duncan et al.state. The (1976), the patients who derived most benefit fromhe rate of baclofen were those whose voluntary movement wasvity in the impeded by spasms. Further work is needed to
37
I.1
I
Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from

D. L. McLellan
establish the physiological basis of co-contraction so
that it can be manipulated more effectively.
I wish to thank the subjects for their cooperation andCiba-Geigy Ltd for supplies of baclofen, estimation ofplasma baclofen concentrations and financialsupport. The work was supported also by TheLondon Hospital and The Multiple SclerosisSociety.
References
Birkmayer, W., Danielczyk, W., and Weiler, G. (1967).Zur Objektivierbarkeit des myotonolytischen Effekteseines Aminobuttersaurederivatives (CIBA 34647-Ba).Wien Medizinische Wochenschrift, 117, 7-9.
Burke, D., Andrews, C. J., and Gillies, J. D. (1971). Thereflex response to sinusoidal stretching in spastic man.Brain, 94, 455-470.
Degen, P. H., and Riess, W. (1976). The determination ofa-amino-,8 (p-chlorophenyl) butyric acid (Baclofen) in
biological material by gas-liquid chromatography.Journal of Chromatography, 117, 399405.
Duncan, G. W., Shahani, B. T., and Young, R. R. (1976).An evaluation of baclofen treatment for certain symp-toms in patients with spinal cord lesions. Neurology(Minneap.), 26, 441446.
Hedley, D. W., Maroun, J. A., and Espir, M. L. E. (1975).Evaluation of baclofen (Lioresal) for spasticity inmultiple sclerosis. Postgraduate Medical Journal, 51,615-618.
Knutsson, E., Lindblom, U., and Martensson, A. (1973).Differences in effects in gamma and alpha spasticityinduced by the GABA derivative baclofen (Lioresal).Brain 96, 29-46.
McLellan, D. L. (1973). Effect of baclofen upon mono-synaptic and tonic vibration reflexes in patients withspasticity. Journal of Neurology, Neurosurgery, andPsychiatry, 36, 555-560.
Pedersen, E., Arlien-S0borg, P., Grynderup, V., andHenriksen, 0. (1970). GABA derivative in spasticity.Acta Neurologica Scandinavica, 46, 257-266.
38
Protected by copyright.
on March 17, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.40.1.30 on 1 January 1977. Dow
nloaded from