coding and staging for leukemia and other...
TRANSCRIPT

Slide 1
LeukemiaHematopoietic
ReticuloendothelialImmunoproliferativeMyeloproliferative
DiseasesRefractory Anemia
Others in 9731-9989 range
Coding and Staging for Leukemia and Other Hematopoietic Diseases
Part 2
In this presentation, we will discuss the rules for abstracting leukemia and other hematopoietic diseases. You should follow along in your ICD-O-3 and CS manuals. Again, this presentation will review certain points from the Hematopoietic Coding manual and discuss the rules for assigning the CS data items. You should follow along in your ICD-O-3, Hematopoietic Coding Rules and CS manuals. Sources: Hematopoietic and Lymphoid Neoplasm Case Reportability and Coding Manual ICD-O-3 Collaborative Stage Manual American Cancer Society Website

Slide 2
22
Review of Certain points
USE THE HEMATOPOIETIC CODING MANUAL
to determinePrimary Site and Histology!!
This presentation contains a review of some of the points from the Hematopoietic Coding Rules manual. It cannot be emphasized enough that the points in this presentation are not meant to stand alone. You MUST use the Hematopoietic Coding Manual. The manual will tell you exactly which code to assign. This is only a review to show you how this information is listed in the ICD-O-3 manual to help you become more familiar with the contents of the ICD-O-3.

Slide 3
3
3
Histologies
Plasma & Mast Cell Tumors (9731-9742)Histiocytic neoplasms (9750-9758)Immunoproliferative disorders (9760-9769)Leukemias (9800-9948)Myeloproliferative disorders (9950-9975)Myelodysplastic syndromes (9980-9992)
NEW CODES EFFECTIVE 1/1/2010!
Listed on the slide are the code ranges that are included in this presentation. It is important to note that new codes went into effect for cases diagnosed on or after 1/1/2010. These new codes are NOT in the ICD-O-3 manual. The first few pages of the Hematopoietic CS schema, which lists all the applicable histology codes for this schema, has been updated to include all the newly reportable codes that are staged under the Hematopoietic schema. These new codes are also included in the 2010 Hematopoietic and Lymphoid neoplasm rules (Table D1a: New Histology Terms and Codes – Alphabetic List, and Table F: Master Code Lists). The diseases with these new codes will follow the same staging rules discussed in this presentation.

Slide 4
Leukemia Groups
The type of white blood cell that is affected
LymphoidMyeloid
How quickly the disease develops and gets worse
Chronic – more slowlylook mature but are not completely normal
Acute – more quicklynot able to mature properly
CLL
CML
ALL
AML
Leukemia can be grouped 2 different ways. There are 2 by the type of white blood cell that is affected – lymphoid and myeloid. There are 2 by how quickly the disease develops and gets worse – chronic and acute. As a result, there are 4 groups: CLL, CML, ALL, AML

Slide 5
Four main types of Leukemia
Acute lymphocytic leukemia (ALL)
Affects children and adultsMore common among childrenSlightly more than half of all
childhood leukemias
Acute myelogenous leukemia (AML)
Affects children and adultsJust under half of all childhood
leukemias
Chronic lymphocytic leukemia (CLL)
Affects adultsAlmost twice as common as CLL
Chronic myelogenous leukemia (CML)
Affects mostly adultsVery rare in children
Here are some common characteristics of the four main types of leukemia. While both children and adults can develop leukemia, certain types are more common in one age group than in another. ALL is more common in children. On the other end of the spectrum, CML is more common in adults.
Slide 6
Diagnostic Workup
Often found during workup for an unrelated health problem
General symptoms:Weight loss, bruising, bleeding, anemia, fatigue, bone pain
Lab work:Blood cell counts and blood tests
Lymphocytosis – too many white cellsBone marrow aspirations and biopsiesLumbar puncture
Because of the way leukemia is diagnosed and treated – usually in the doctor’s office – you have to be really careful that you are not missing cases. Most of the time you are going to pick them up if they come in for treatment. But, you should make sure you are not missing cases through other types of visits. IE: if the lab work is done in your facility. You can’t always count on having a pathology report. Because leukemia does not usually form tumors, imaging test are not always helpful and are usually only done to look for infections and other problems.
Slide 7
Staging
There is a complete list of histologies that are included in the hematopoietic staging scheme on the first few pages of the hematopoietic staging schema in the CS Manual. This list includes the new histology codes that became effective on January 1, 2010. Review this list carefully to ensure you are using the correct staging schema.
Slide 8
Reading Assignments
As each data item is being discussed, you should stop and read the information in CSv2 Part II and CSv2 Part I, Section 2 for that data item including the associated notes, codes and definitions.
8
It is important that you follow along and make notes in your manual. In addition to reading the slides and the instructor’s notes, it is important that you stop and read the related sections in your manual as not every point will be discussed in detail.
Slide 9
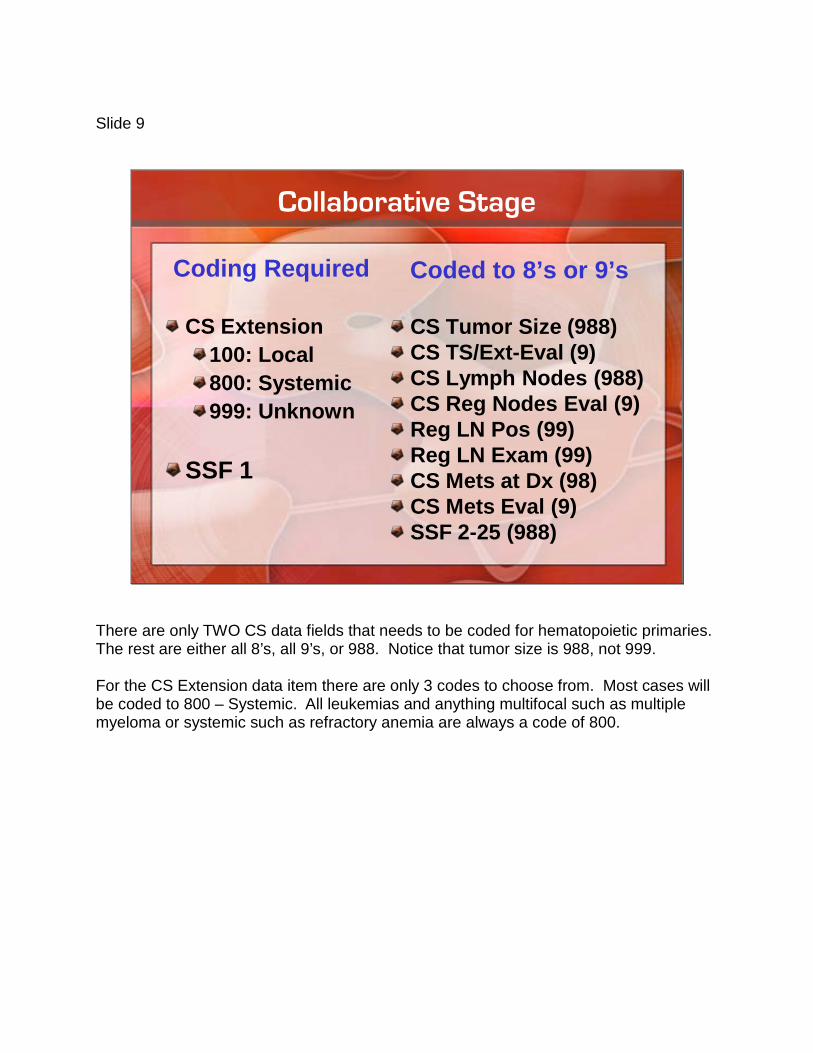
Collaborative Stage
Coding Required
CS Extension100: Local800: Systemic999: Unknown
SSF 1
Coded to 8’s or 9’s
CS Tumor Size (988)CS TS/Ext-Eval (9)CS Lymph Nodes (988)CS Reg Nodes Eval (9)Reg LN Pos (99)Reg LN Exam (99)CS Mets at Dx (98)CS Mets Eval (9)SSF 2-25 (988)
There are only TWO CS data fields that needs to be coded for hematopoietic primaries. The rest are either all 8’s, all 9’s, or 988. Notice that tumor size is 988, not 999. For the CS Extension data item there are only 3 codes to choose from. Most cases will be coded to 800 – Systemic. All leukemias and anything multifocal such as multiple myeloma or systemic such as refractory anemia are always a code of 800.
Slide 10
10
10
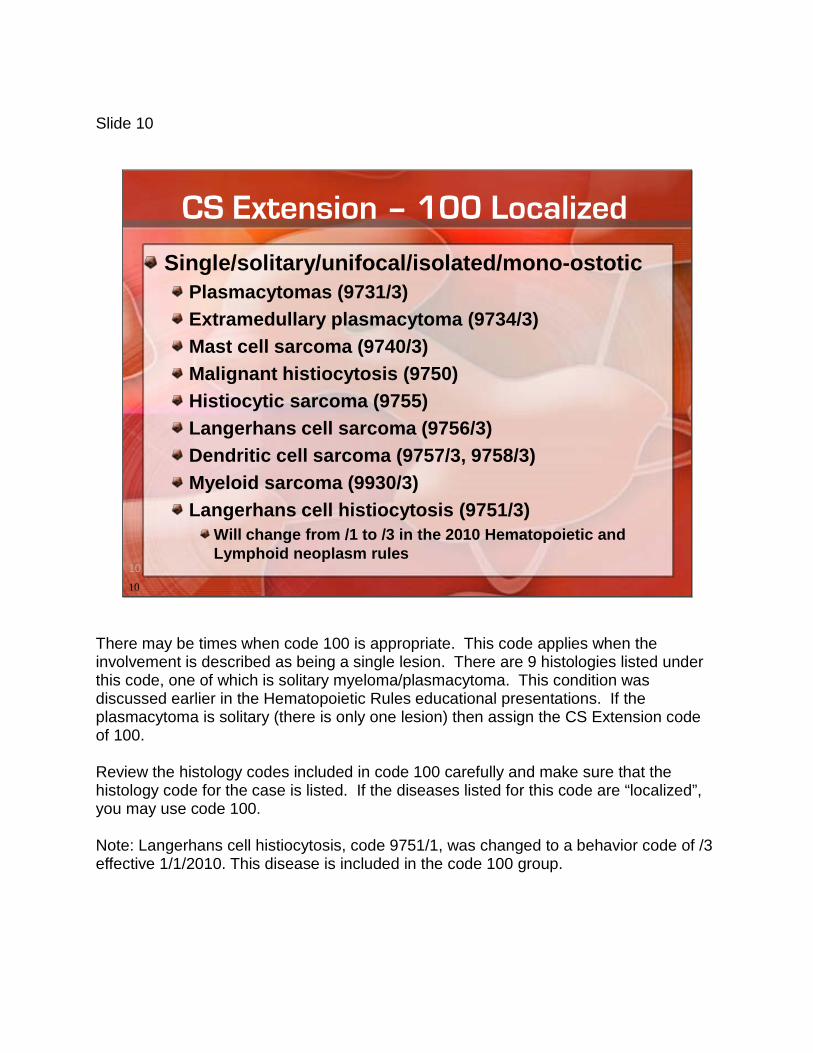
CS Extension – 100 Localized
Single/solitary/unifocal/isolated/mono-ostoticPlasmacytomas (9731/3)Extramedullary plasmacytoma (9734/3)Mast cell sarcoma (9740/3)Malignant histiocytosis (9750)Histiocytic sarcoma (9755)Langerhans cell sarcoma (9756/3)Dendritic cell sarcoma (9757/3, 9758/3)Myeloid sarcoma (9930/3)Langerhans cell histiocytosis (9751/3)
Will change from /1 to /3 in the 2010 Hematopoietic and Lymphoid neoplasm rules
There may be times when code 100 is appropriate. This code applies when the involvement is described as being a single lesion. There are 9 histologies listed under this code, one of which is solitary myeloma/plasmacytoma. This condition was discussed earlier in the Hematopoietic Rules educational presentations. If the plasmacytoma is solitary (there is only one lesion) then assign the CS Extension code of 100. Review the histology codes included in code 100 carefully and make sure that the histology code for the case is listed. If the diseases listed for this code are “localized”, you may use code 100. Note: Langerhans cell histiocytosis, code 9751/1, was changed to a behavior code of /3 effective 1/1/2010. This disease is included in the code 100 group.

Slide 11
11
CS Extension – 800 Systemic
800 Systemic diseasePoly-ostoticAll histologies, including those in code 100 that are systemicAlways for ALL leukemia histologiesAlways for ALL myelodysplastic histologiesHematopoietic codes effective 1/1/2010
999 Unknown11
Code 800 includes diseases from code 100 that have become systemic (or there are multiple lesions). All leukemia and myelodysplastic histologies should ALWAYS be coded 800. These are by nature systemic diseases. For the hematopoietic diseases that became reportable with the 2010 Hematopoietic and Lymphoid neoplasms rules, code 800 is the appropriate code. Only use code 999 for those codes that are listed in code 100 where you don’t know whether they are localized or systemic (or single or multiple lesions).

Slide 12
12
12
New Data Items
Data Item Code Explanation
Grade Path Value Blank Not applicable
Grade Path System Blank Not applicable
Lymph vascular invasion 8 Not applicable
Mets at Dx-Bone 8 Not applicable
Mets at Dx-Lung 8 Not applicable
Mets at Dx-Brain 8 Not applicable
Mets at Dx-Liver 8 Not applicable
The data items listed on this slide are “not applicable” for Hematopoietic diseases. For the Grade Path Value/System, the only codes available are 2, 3, 4 and blank, which is why this field would be left blank instead of having a numerical code.

Slide 13
13
13
SSF1 JAK2
Can be used to help determine reportability
A MPN with a positive JAK2 is reportableOther tests needed to determine exact histology
If JAK2 is done, record results regardless of histology
JAK2 is a gene mutation that increases susceptibility to several Myeloproliferative neoplasms (MPN). Testing for the JAK2 mutation is done on whole blood. Nearly all people with polycythemia vera and about half of those with essential thrombocythemia and primary myelofibrosis have the mutation. The most common mutations used now are the V617F in exon 14 and exon 12. When JAK2 is positive the MPN is definitely reportable; however, JAK2 itself does not specify which MPN is present. Other diagnostic tests are required to determine the specific histology. Note: you should use the Hematopoietic rules to make a final decision as to reportability. Code the result of the JAK-2 test as documented in a laboratory test or elsewhere in the medical record. Code this field for any hematopoietic, reticuloendothelial, immunoproliferative, myeloproliferative, or myelodysplastic disease for which JAK-2 is tested. If you have a JAK 2 positive with no other information, use code 850. For those diseases where JAK 2 is not mentioned in the record, or it is a disease where it is normally not done (i.e. leukemia and multiple myeloma), code 999.

Slide 14
SSF1 JAK2
Sample Report
This is a sample report showing JAK2 results.
Slide 15
Additional Commentsrelated to the
Hematopoietic Rules

Slide 16
Primary Site
All leukemias, myeloproliferative and
lymphoproliferative disorders and myelodysplastic syndromes
(9800 – 9992)
Leukemia along with the other types of disorders and syndromes in the 9800-9992 range are a malignant disease of the bone marrow. Therefore the site code will almost ALWAYS be coded to C42.1. Refer to the Hematopoietic Coding Rules manual for specific instructions on coding the primary site as there may be situations where this differs. However, if you have a histology in the 9800-9992 range, and the site is NOT C42.1, consider it a flag to double check to make sure you have followed the rules correctly and have assigned the correct site code.

Slide 17
Cytogenetics
Looking at the cell’s chromosomesNormal human cells contain 46 chromosomes
In certain types of myeloid leukemia, chromosomes may change
Translocation: t(1;2)Inversion: inv(16)Deletion: del(7) or -7Additions: +8
If you look through the ICD-O-3 manual at the leukemia terms and codes, you may notice that some codes contain unusual terminology. The purpose of the next few slides is to describe the application of cytogenetics and FAB classification in the ICD-O-3 manual. The first topic we will discuss is cytogenetics. Because leukemia is a systemic disease that starts in the bone marrow, traditional staging is not useful. Instead, physicians look at the cellular level to identify not only the subtype, but also the prognosis, and the likely response to treatment. Clinicians use cytogenetic testing to identify certain types of myeloid leukemia. The results of the cytogenetic testing are written in shorthand form that describes which chromosome changes are present. For example, for translocation, this means that part of chromosome 1 is now located on chromosome 2 or vice versa. An inversion means that part of chromosome 16 is upside down and is now in reverse order.

Slide 18
Cytogenetics and the ICD-O-3
ICD-O-3, pages 102-103
Acute promyelocytic leukemia (9866/3)t(15;17)(q22;q11-12)
Part of chromosome 22 is now located on chromosome q11-12 and vice versa.
Part of chromosome 15 is now located on chromosome 17 and vice versa.
Look at pages 102-103 in your ICD-O. Notice beside selected myeloid leukemias, the histologic term is followed by a series of numbers written in parentheses. For example, under Acute Promyelocytic Leukemia (9866/3), the following shorthand is listed: t(15;17)(q22;q11-12). Based on this information, this means that part of chromosome 15 is now located on chromosome 17 and vice versa. And, part of chromosome q22 is now located on chromosome q11-12 and vice versa. While it is not vital that you know that it means that exactly, it is important that you understand, in general, what it is referring to so when you do see one, you can code it correctly. Under code 9866, notice that acute MYELOID leukemia is listed with the same shorthand. If the diagnosis doesn’t specify the shorthand or the FAB type, then code to Acute Myeloid Leukemia, NOS which is code 9861/3 – listed just above it.

Slide 19
Genetic Shorthand
p Short armq Long armt Translocationadd Addition of material of unknown
origin to a region or banddel Deletioninv Inversioni Iso-chromosome
This slide lists some of the commonly used genetic shorthand symbols.
Slide 20
FAB Classification
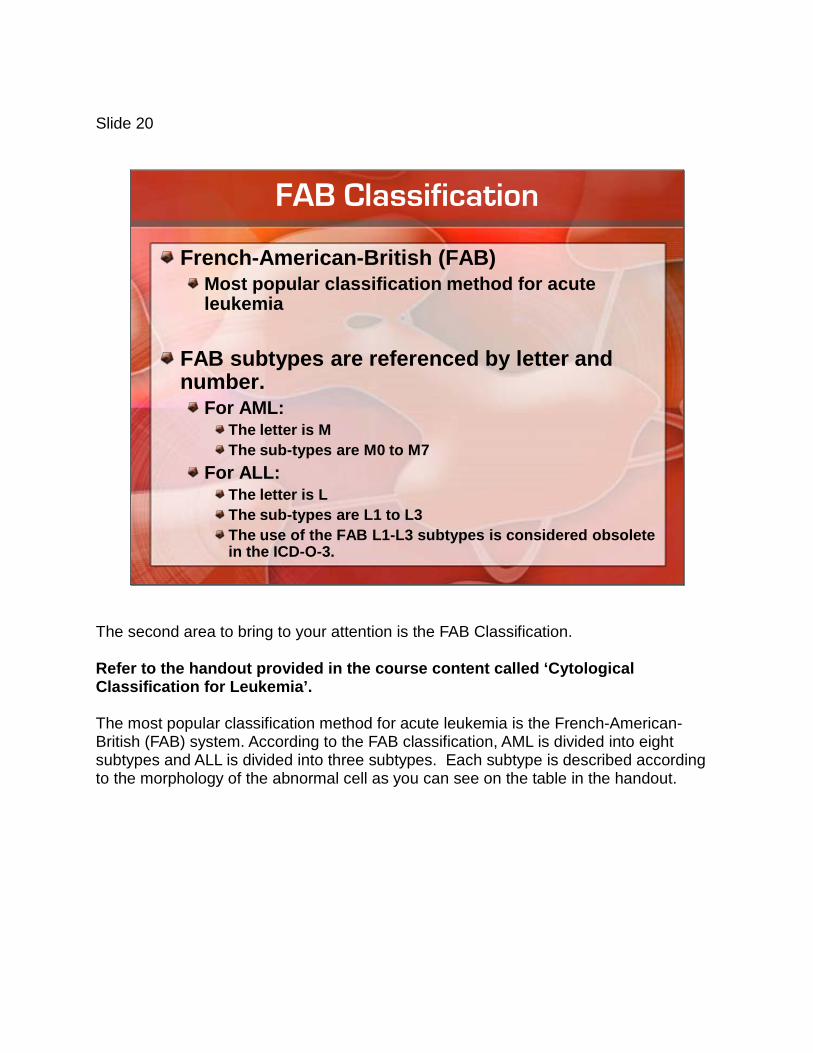
French-American-British (FAB)Most popular classification method for acute leukemia
FAB subtypes are referenced by letter and number.
For AML:The letter is MThe sub-types are M0 to M7
For ALL:The letter is LThe sub-types are L1 to L3The use of the FAB L1-L3 subtypes is considered obsolete in the ICD-O-3.
The second area to bring to your attention is the FAB Classification. Refer to the handout provided in the course content called ‘Cytological Classification for Leukemia’. The most popular classification method for acute leukemia is the French-American-British (FAB) system. According to the FAB classification, AML is divided into eight subtypes and ALL is divided into three subtypes. Each subtype is described according to the morphology of the abnormal cell as you can see on the table in the handout.

Slide 21
FAB and the ICD-O-3
ICD-O-3, pages 158-160FAB types listed on page 160FAB M1 = 9873 = Acute myeloid leukemia without maturation
M2 acute myelocytic leukemia
Remember, the FAB system was for acute leukemias. Find acute leukemia in the ICD-O alphabetic section (p158). Go down to the L’s for lymphoblastic (under acute). Do you see any of the FAB L1-3 types? There is one - L2. Now go on down to the M’s for myeloid (still under acute). Do you see any of the FAB M0-7 types? There is one - M6. Follow this down to where chronic leukemia ends and it starts with common, cortical, erythroid on pg 159. Turn the page, after “e” comes “f”, at the top of page 160 we have FAB and under it all the types are listed. The table on the handout cross-references the FAB subtype, the ICD-O-3 code and the terminology. For example, look at M1. On page 160, M1 is 9873. Go to 9873 in the numerical section – p 103. You can see the terminology that goes with that – Acute myeloid leukemia w/o maturation. This is what is on the table.

Go back to Acute myeloid in the alphabetic section – p158. Look for acute myeloid leukemia w/o maturation. M1 is not listed with it as a synonym. So what if the diagnosis is M2 acute myelocytic leukemia? Even though it doesn’t say “with maturation” in the diagnosis, because we have a FAB classification of M2, we should code to 9874/3. The M2 is telling us the “with maturation” part. If the FAB classification is not specified, you would have to use the NOS code of 9861/3. This is an excellent example of where looking something up in the alphabetic AND the numerical sections are an important concept. AND, knowing that the M0-7 subtypes are part of the FAB system and knowing that these are listed under “FAB” in the ICD-O is important in seeing that you assign the correct and most specific code. Again, knowing exactly what M1 or M2 means is not as important as knowing how to code them when the term is included in the final diagnosis.

Slide 22
Disease Progression versus Transformation
Disease transformation is an important part of the Hematopoietic rules.

Slide 23
Disease Progression
The worsening of a disease over timeMost often used for chronic or incurable diseasesSame:
Cell typeFunctiongenetics
Disease progression is defined as the worsening of a disease over time. It is most often used for chronic or incurable diseases. As you learned in the staging timing rules, “disease progression” after the diagnosis is established is not included in calculating the stage. Disease progression applies to solid tumors as well. Disease progression in solid tumors usually involves further tumor extension, LN metastasis, body cavity metastases, and/or blood-borne metastases. Hematopoietic disease can progress as well. Examples include: •Smoldering multiple myeloma to “full blown” multiple myeloma •Early stage/asymptomatic CLL to late stage/symptomatic CLL For both solid tumor and hematopoietic disease progression, the characteristics are the same. The cell type is the same, the “function” is the same, and the genetics are the same. There is also a change in the symptoms, treatment, and life expectancy.

Slide 24
Transformation
Change in nature, function or condition of diseaseExample: Polycythemia vera transforming to acute myeloid leukemiaDifferent
Cell typeFunctionGenetics
Transformation are a “new” primaryUse Hematopoietic Rules Manual
Transformation is a change in the nature, function, or condition of the disease. There is often a change in potential or cell type or the cell is undergoing genetic transformation. As with progression, there is also a change in the symptoms, treatment, and life expectancy. Example: Polycythemia vera (PCV) transforming to acute myeloid leukemia (AML). For each of these the characteristics are different: Cell Origin PV: Hematopoietic stem cells AML: Myeloid line of white blood cells Characteristics PV: Too many red blood cells causing blood to thicken AML: 20% or more blasts in blood or BM Treatment PV: Phlebotomy, aspirin, sometimes Anagrelide AML: Chemo, stem cell transplant

Survival PV: Treated properly, virtually normal AML: Develops quickly. Untreated, is fatal in a few months. Treated: 33% free of disease at 4 year interval (<65 Y/O) Conclusion Transformations are NOT the equivalent of disease progression. Transformations are considered to be a new primary as there is a different cell type, genetics, treatment, and survival. It is important to capture the incidence count for both chronic and acute. You should use the Hematopoietic Rules manual to make this determination of the number of primaries.

Slide 25
Sequence Number
Takes into consideration ALL cancer primaries during the lifetime of the patient
Only those neoplasms that were REPORTABLE AT THE TIME OF DIAGNOSISare to be taken into consideration
Changes in reporting rules:ICD-O-2 ICD-O-3 (01/01/2001)
Use the ICD-O-3 AppendicesHematopoietic DB (01/01/2010)
Use the Hematopoietic Rules manual
The year in which the hematopoietic primary was diagnosed depends on whether or not it is reportable and should be factored into the sequence number. Don’t forget about the changes when the ICD-O-3 came into effect in 2001 which added some hematopoietic primaries with a reportable behavior code of 3. And, the changes when the Hematopoietic DB came into effect in 2010 which added some new codes and some existing codes were changed from /1 to /3.
For example, refractory anemia was not reportable until the implementation of the ICD-
O-3 in 2001. These changes can be found in the appendices in the back of your ICD-O-3 manual. This may not be specified in the Hematopoietic DB as the DB does not address assigning the sequence code. Therefore, you may need to use the ICD-O-3 appendices to determine when a particular condition became reportable.

Slide 26
26
26
Concluding remarks
Remember which fields are not applicable (majority)
When coding, double check “code 100” to see if your histology is applicable for this code
Leukemias and MDS (9800-9989) are ALWAYS coded 800 in CS Extension
SSF for JAK2 has been added
Slide 27
This concludes Part 2.
Please return to the course content.