cognitive dysfunction underlying auditory …
TRANSCRIPT

COGNITIVE DYSFUNCTION UNDERLYING
AUDITORY HALLUCINATIONS IN SCHIZOPHRENIA: A COMBINED-DEFICITS MODEL.
Flavie Waters BSc (Hons), MSc
This thesis is presented for the degree of Doctor of Philosophy and as
a partial requirement for the degree of Master of Psychology (Clinical Neuropsychology) of the University of Western Australia
School of Psychiatry and Clinical Neurosciences and School of Psychology University of Western Australia
2004

iii
ABSTRACT
Auditory hallucinations are some of the most distressing and disabling symptoms of
schizophrenia. However very little is known about the exact processes responsible for
auditory hallucinations. The aim of this thesis is to provide a new perspective on the nature
of the cognitive deficits underlying auditory hallucinations in schizophrenia.
As a preliminary study to the investigation of auditory hallucinations in
schizophrenia, a factor analysis of a measure of hallucinatory predisposition, the Launay-
Slade Hallucination Scale-Revised (Bentall & Slade, 1985), was carried out on data from a
large sample of undergraduate students (N = 562). An overlap in characteristics between
hallucinatory-like experiences in normal individuals and auditory hallucinations in
schizophrenia should draw attention to factors that are important to the hallucinatory
experience in general. One of the findings from this study was that intrusiveness is a
commonly reported characteristic of hallucinatory-like experiences in normal individuals.
Intrusiveness is also one of the defining features of auditory hallucinations in
schizophrenia. Since the process of inhibition is essential for suppressing unwanted
thoughts, the first set of two studies using patients with schizophrenia (N = 43) investigated
the presence of an (intentional) inhibition failure in auditory hallucinations using the
Hayling Sentence Completion Test (HSCT; Burgess & Shallice, 1996) and the Inhibition of
Currently Irrelevant Memories Task (ICIM; Schnider & Ptak, 1999). It was found that
auditory hallucinations were linked to a deficit in intentional inhibition as measured by
these tasks. The process of inhibition was further investigated using the Affective Shifting
task, but auditory hallucinations were not associated with a deficit on this task. Possible
differences in the inhibitory demands of the HSCT, ICIM and Affective Shifting tasks are
discussed.
In addition to the notion of intrusiveness, healthy individuals vulnerable to
hallucinations identified experiences that are referred to an external agency. Similarly,
schizophrenia patients with auditory hallucinations fail to recognize mental events as being
self-generated. A recent theory suggests that the patients’ failure to identify the origins of
auditory hallucinations results from a fundamental deficit in context memory (Nayani &
David, 1996). The second set of studies in patients with schizophrenia (N = 43)
investigated the proposal that auditory hallucinations are linked to an impairment in context
memory. A task that assessed memory for events, the source of these events (self/other)

iv
and their location in time (session 1/2) was utilized. The results showed that significantly
more patients with auditory hallucinations had a deficit in some form of memory for
context compared to patients without auditory hallucinations, although this deficit was not
found to be specific to those with auditory hallucinations.
A new model of auditory hallucinations was then developed. It was suggested that at
least two cognitive deficits, in intentional inhibition and context memory, must be present
to explain auditory hallucinations. As a result of these combined deficits, mental events are
experienced as involuntary and intrusive and are not recognized because the contextual
cues that would allow them to be identified correctly are missing or incomplete. In support
of this proposal, nearly all patients currently experiencing auditory hallucinations showed
the combination of deficits. However, critical consideration of the findings suggests that
additional cognitive processes may be necessary for auditory hallucinations to occur.
Finally, one prediction of the model is that nonhallucinating individuals (with or
without schizophrenia) may show a deficit on either, but not both, intentional inhibition or
context memory processes. As a formal test of the model, the last study tested this
prediction on a group of patients with Obsessive Compulsive Disorder (OCD; N = 14).
OCD patients also report intrusive and unwanted thoughts, although they do not mistake
the origins of these thoughts. The results showed that only one of the 14 OCD patients
showed the combination of deficits, providing strong support for our model of auditory
hallucinations. The OCD patient who showed the combined deficits was found to
experience frequent hypnopompic hallucinations, perhaps suggesting similar cognitive
processes between hallucination-like experiences in non-psychotic states and auditory
hallucinations in schizophrenia.
Together, the studies suggest that a combination of deficits in intentional inhibition
and contextual memory is necessary for auditory hallucinations to occur in schizophrenia.
However, a critical analysis of the results indicated that additional cognitive processes are
likely to be important for the expression of this symptom. The power in our model comes
from its ability to explain a broad range of phenomena that previous models cannot account
for.
v
References Bentall, R. P., & Slade, P. D. (1985). Reliability of a scale measuring disposition towards
hallucination: a brief report. Personality and Individual Differences, 6(4), 527-529.
Burgess, P., & Shallice, T. (1996). Response suppression, initiation and strategy use
following frontal lobe lesions. Neuropsychologia, 34(4), 263-273.
Nayani, T., & David, A. (1996). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & B. T. R. E (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 : John Wiley & Sons
Ltd.
Schnider, A., & Ptak, R. (1999). Spontaneous confabulators fail to suppress currently
irrelevant memory traces. Nature Neuroscience, 2(7), 677-681.

vii
TABLE OF CONTENTS Abstract…………………………………………………………………………. iii Manuscripts and publications generated from this thesis…………………… xiii Acknowledgments……………………………..……………………………….. xv Preamble……………………………..…………………………………………. xvii INTRODUCTION………………………………………………………………. 1 Chapter 1. An overview of schizophrenia, auditory hallucinations, inhibition and context memory………………………………………………..
3
Abstract……………………………..…………………………………………… 3 Schizophrenia……………………………………………………………………. 4
Cognitive Neuropsychiatry……………………………………………… 6 Auditory hallucinations………………………………………………………….. 7
Definition………………………………………………………………… 7 Auditory hallucinations in individuals other than with schizophrenia….. 8 Main descriptive features of auditory hallucinations……….…………… 8
Theories of auditory hallucinations……………………………………… 11 Inner speech..….………………………………………………… 11 Mental imagery….…..….……………………………………….. 13 Context memory deficit...……………………………………….. 14 Social-psychological theories….………………………………… 16 Neuropathology of auditory hallucinations……………………………… 17
Key cognitive processes under investigations…………………………………… 20 Inhibition………………………………………………………………… 20 Context memory……………………………………………………….… 23 Aims and organization of the thesis……………………………………………… 25 References……..…………………………………..…………………………….. 28 PREDISPOSITION TO HALLUCINATIONS IN THE NORMAL POPULATION………………………………………………………………….
45
Foreword to Chapter 2…………………………………………………………… 47 Chapter 2. Revision of the factor structure of the Launay-Slade Hallucination Scale (LSHS-R) …………………………………………………
49
Abstract……………………………..…………………………………………… 49 Introduction……..…………………………………..…………………………… 50 Method……..…………………………………..………………………………… 51 Results……..…………………………………..………………………………… 51 Discussion……..…………………………………..…………………………….. 55 References……..…………………………………..…………………………….. 57

viii
INTENTIONAL INHIBITION AND AUDITORY HALLUCINATIONS… 59 Foreword to Chapter 3, 4 and 5…………………………………………………. 61 Chapter 3. Inhibition in schizophrenia: association with auditory hallucinations……………………………………………………………………
63
Abstract……………………………..…………………………………………… 63 Introduction……………………………..……………………………………….. 64 Method……………………………..……………………………………………. 65 Participants..…………………………………………………………….. 65 Clinical ratings..………………………….……………………………... 65 Tasks and questionnaires……………………………..…………………. 66 Results……………………………..…………………………………………….. 67 Comparisons of patients and controls……………………………..…….. 67 Correlations with hallucinations severity..………………………………. 68 Association of variables with severity of other symptom groups.………. 69 Effects of antipsychotic medication……..………………………………. 70 Discussion……………………………..………………………………………… 70 Acknowledgements……………………………………………………………… 71 References……………………………..………………………………………… 72 Chapter 4. Auditory hallucinations: failure to inhibit irrelevant memories 75 Abstract……………………………..…………………………………………… 75 Introduction……………………………..……………………………………….. 76 Method……………………………..……………………………………………. 77 Participants.……………………………..………………………………. 77 Clinical ratings………………………..………………………………… 77 Cognitive assessment.……………………………..…………………….. 78 Results……………………………..…………………………………………….. 79 Analysis of target hits.……………………………..……………………. 79 Analysis of false alarms.……………………………..………………….. 80 Discussion……………………………..………………………………………… 81 Acknowledgements……………………………………………………………… 84 References……………………………..………………………………………… 85 Chapter 5. Inhibitory and affective processes in schizophrenia and auditory hallucinations……………………………………………………………………
87
Abstract……………………………..…………………………………………… 87 Introduction……………………………..………………………………………. 88 Inhibitory processes……………………………..………………………. 88

ix
Inhibition in schizophrenia………………………………………... 88 Inhibition in auditory hallucinations..…………………………….. 90 Affective Processes.……………………………..………………………. 90 Affective processes in schizophrenia……..………………………. 90 Affective processes in auditory hallucinations……..…………….. 92 Summary of goals.……………………………..………………………... 93 Method……………………………..……………………………………………. 94 Participants.……………………………..………………………………. 94 Clinical ratings………………………………….……………………….. 94 Tasks and questionnaires………………………………….…………….. 95 Results…………………………..……………………………………………….. 99 Affective Shifting task…………………………..………………………. 99 Patients versus controls comparisons………………..…….……… 99 Analyses of patients with and without hallucinations……..……... 100 Questionnaire Results…………………………..……………………….. 101 BDI-II and BAI……………………………..…………………….. 101 Performance on Affective Shifting task and depression/anxiety… 102 Negative voice content: Auditory Hallucinations Questionnaire…. 104 BAVQ-R……………………………..……………………………. 104 Relationship between BDI-II, negative content and BAVQ-R…… 106 Performance on Affective Shifting task - negative voice content 106 Discussion…………………………..…………………………………………… 106 Inhibitory processes……………………………..………………………. 107 Inhibition in schizophrenia………………………………………... 107 Inhibition in auditory hallucinations..…………………………….. 108 Affective Processes.……………………………..………………………. 110 Affective processes in schizophrenia……..………………………. 110 Affective processes in auditory hallucinations……..…………….. 112 Theoretical developments……..………………………………………… 114 References……..…………………………………..……………………………. 117 CONTEXT MEMORY AND AUDITORY HALLUCINATIONS…………. 125 Foreword to Chapters 6 and 7……………………………………………………. 127 Chapter 6. Context memory and binding in schizophrenia…………………. 129 Abstract……………………………..…………………………………………… 129 Introduction……..…………………………………..…………………………… 130 Method……..…………………………………..………………………………… 131 Participants……………………………..……………………………….. 131 Memory for Context task……..…………………………………………. 132

x
Data analysis……..…………………………………..………………….. 132 Results……..…………………………………..……………………………….. 133 Intact versus rearranged object pair recognition.……………………….. 133 Source and temporal judgements……..………………………………… 135 Low-functioning controls……..………………………………………… 136 Binding of source and temporal information……..…………………….. 137 Demographic and clinical factors……..………………………………… 138 Discussion……..…………………………………..……………………………. 138 Acknowledgements……………………………………………………………… 140 References……..…………………………………..……………………………. 141 Chapter 7. Context memory and auditory hallucinations………………….. 145 Abstract……………………………..…………………………………………… 145 Introduction……..…………………………………..…………………………… 146 Method……..…………………………………..………………………………… 147 Participants……………………………..……………………………….. 147 Tasks……..……………………………………………………………… 147 Results……..…………………………………..………………………………… 148 Intact versus rearranged object pair recognition………………………… 150 Source and temporal judgements……..…………………………………. 150 Binding of source and temporal information……..……………………... 151 Specificity of deficits in auditory hallucinations..…………………….…. 154 Discussion……..…………………………………..……………………………. 155 References……..…………………………………..……………………………. 161 AUDITORY HALLUCINATIONS: A COMBINATION OF DEFICITS IN INTENTIONAL INHIBITION AND CONTEXT MEMORY………………
165
Foreword to Chapter 8…………………………………………………………… 167 Chapter 8. Auditory hallucinations in schizophrenia: intrusive thoughts and forgotten memories…………………………………………………….…
169
Abstract……………………………..…………………………………………… 169 Introduction……..…………………………………..…………………………… 170 A deficit in intentional inhibition……..…………………………………………. 171 Inhibition: definition and taxonomy……..……………………………….. 171 Inhibition deficits in auditory hallucinations of schizophrenia…………… 172 New empirical support for a failure in intentional inhibition……..………. 173 A deficit in memory for context……..………………………………………….. 177 Context memory: definition……..………………………………………... 178 Context memory deficits in auditory hallucinations of schizophrenia…… 179

xi
New empirical support for a context memory failure…………………….. 180 A combined deficit in intentional inhibition and context memory……..……….. 182 Assessment of the model……..………………………………………………….. 183 Potential empirical and theoretical developments………………………………. 186 Acknowledgements……………………………………………………………… 188 References……..…………………………………..……………………………. 189 INHIBITION AND CONTEXT MEMORY IN OBSESSIVE-COMPULSIVE DISORDER (OCD)………………………………………….
201
Foreword to Chapters 9 and 10………………………………………………….. 203 Chapter 9. OCD: similarities with auditory hallucinations in schizophrenia. A literature review……………………………………………………………..
205
Abstract……………………………..…………………………………………… 205 Introduction……..…………………………………..…………………………… 206 Epidemiological and clinical features of OCD. ………………………………… 206 Neuropathology of OCD……..………………………………………………….. 208 Neuropsychological findings……..……………………………………………… 208 Maintenance theories of OCD……..……………………………………………. 211 Conclusion and direction……..………………………………………………….. 212 References……..…………………………………..……………………………. 213 Chapter 10. OCD: Intentional inhibition and context memory processes…. 221 Abstract……………………………..………………………………………….. 221 Introduction……..…………………………………..…………………………… 222 Method……..…………………………………..……………………………….. 224 Participants……..…………………………………..…………………… 224 Clinical ratings……..……………………………………………………. 224 Tasks and questionnaires……..…………………………………………. 225 Results……..…………………………………..………………………………… 227 Intentional inhibition..…………………………………………………… 227 Context memory……..………………………………………………….. 230 Combined deficits in inhibition and context memory…………………... 232 Discussion……..…………………………………..…………………………….. 233 Intentional inhibition processes……..………………………………….. 233 Context memory processes……..………………………………………. 236 A combination of deficits in inhibition and context memory…………… 237 References……..…………………………………..……………………………. 240

xii
GENERAL DISCUSSION…………………………………………………….. 245 Chapter 11. General Discussion………………………………………………. 247 Hallucinatory predisposition in healthy individuals..……………………………. 247 Summary of results of Chapter 2……..…………………………………… 247 Intentional inhibition and auditory hallucinations..……………………………… 248 Summary of results of Chapter 3……..…………………………………… 248 Summary of results of Chapter 4……..…………………………………… 249 Summary of results of Chapter 5……..…………………………………… 249 Summary of results of Chapter 8……..…………………………………… 250 General comments regarding the role of intentional inhibition processes... 251 Context memory and auditory hallucinations..…………………………………... 252 Summary of results of Chapter 6……..…………………………………… 252 Summary of results of Chapter 7……..…………………………………… 253 General comments regarding the role of context memory processes.……. 255 Issues of affect..…………………………….. ..…………………………………. 257 Summary of results of Chapter 5……..…………………………………… 257 General comments regarding issues of affect and auditory hallucinations.. 259 A combination of deficits in intentional inhibition and context memory……….. 260 Intentional inhibition and context memory in OCD..……………………………. 262 Summary of results and comments regarding inhibition and OCD.……… 263 Summary of results and comments regarding context memory and OCD.. 264 Summary of results and comments regarding combined deficits in inhibition and context memory and OCD...……………………………….
265
Final comments..…………………………….. ..……………………………….. 270 References……..…………………………………..……………………………. 273 APPENDIX Appendix A: An analysis of the main clinical features of auditory hallucinations in schizophrenia…………...……………………………………...
277
Appendix B: Words used in the Affective Shifting task………………………... 285

xiii
MANUSCRIPTS AND PUBLICATIONS GENERATED FROM THIS THESIS
Waters, F.A.V., Badcock, J.C., & Maybery, M.T. (2003) Revision of the factor structure of
the Launay-Slade Hallucination Scale (LSHS-R). Personality and Individual
Differences, 35, 1351-1357 (Chapter 2).
Waters, F.A.V., Badcock, J.C., Maybery, M.T., & Michie, P.T. (2003) Inhibition in
schizophrenia: Association with auditory hallucinations. Schizophrenia Research. 62,
275-280. (Chapter 3).
Badcock, J.C., Waters, F.A.V., & Maybery, M.T. (in press) Auditory hallucinations: failure
to inhibit irrelevant memories. Cognitive Neuropsychiatry (Chapter 4).
Waters, F.A.V., Badcock, J.C., Maybery, M.T., & Michie, P.T. (2004) Inhibitory and
affective processes in schizophrenia and auditory hallucinations. Unpublished
manuscript, University of Western Australia. (Chapter 5).
Waters, F.A.V., Maybery, M.T., Badcock, J.C., & Michie, P.T. (2004) Context memory
and binding in schizophrenia. Schizophrenia Research, 68(2-3), 119-125 (Chapter 6).
Waters, F.A.V., Badcock, J.C., Maybery, M.T., & Michie, P.T. (2004) Context memory
and auditory hallucinations. Unpublished manuscript, University of Western
Australia. (Chapter 7).
Waters, F.A.V., Badcock, J.C., Michie, P.T. & Maybery, M.T. (2004) Auditory
hallucinations in schizophrenia: intrusive thoughts and forgotten memories.
Manuscript submitted for publication (Chapter 8).
Waters, F.A.V., Badcock, J.C., Maybery, M.T., & Michie, P.T. (2004) OCD: Intentional
inhibition and memory for context. Unpublished manuscript, University of Western
Australia. (Chapter 10).
Waters, F.A.V., Badcock, J.C. & Maybery, M.T. (2004). An analysis of the main clinical
features of auditory hallucinations in schizophrenia. Unpublished manuscript,
University of Western Australia. (Appendix A).
Contribution of the Candidate to Publications
Please note: In regard to Regulation 31 (points 2 and 3) from the Regulations Governing
Research Higher Degrees, all study design, task development, participant recruitment and
testing, data entry, analysis, interpretation, preparation of manuscripts and revisions were

xiv
conducted by the candidate. One exception concerns the manuscript presented in Chapter
4. This chapter entails a reanalysis of one of the tasks presented in Chapter 3 (Waters,
Badcock, Maybery & Michie, 2003). The manuscript was prepared by one of the
candidate’s supervisors, Dr Johanna Badcock, however the candidate contributed to the
form and design of the analysis and made corrections to the text prior to publication.

xv
ACKNOWLEDGMENTS
I have been very fortunate to have two great supervisors. Johanna Badcock has
been a remarkable mentor and guide throughout my candidature. Her focus and passion for
neuropsychiatric research have greatly stimulated my career aspiration to remain in this
field of research. I have also come to know her as a friend and I could not have done
without her support of the important decisions I have made during my PhD. I am also
greatly indebted to Murray Maybery. His opinions, advice and patience have been
invaluable. I am also very grateful for his guidance and knowledge, and I could not have
reached this point without his help. The contribution of Patricia Michie must also be
acknowledged. Together with Jo Badcock, Pat contributed to the original proposal that
gave rise to this PhD. Although she now works at another university, I have really valued
the time I spent in her company and she has inspired me more than she will ever know.
I could not have carried out this research without the assistance of Danny Rock and
Sarah Howell who helped me with the recruitment of patients. Many thanks also to David
Castle and Helen Stain for many hours of psychiatric interviewing training. Much
appreciation to Matt Huitson who developed some of the tasks used in this thesis, and to
Andrew Heathcote for his helpful statistical advice in one of the manuscripts. Professor
Aaron Beck also provided valued assistance and thoughtful comments in the early stages of
this thesis.
My best appreciation also to the patients and other participants who gave their time
and effort so generously to this project. This research was genuinely carried out in the hope
that it will lead to a better understanding of auditory hallucinations. Any step forward,
however small, is a step closer towards some relief for affected patients.
Thanks also to Kate Frencham, Keira Thomson and Dana Wong for the memorable
Thursday evening sessions.
Finally, but most importantly, many important life events have happened during this
PhD. My Father, Jean-Francois Aubert, passed away suddenly. He was a very unique,
vibrant and loving person whom I continue to miss every day. I also miss dearly my
grandparents who passed away shortly before my Father. My son Luke was born during
this difficult time and is my little happy ray of sunshine. Everlasting thanks to Mike, my
life companion, who has been a pillar of strength during all these events. I have found
great comfort in his advice that a PhD is all about surviving whatever life throws at you.

xvii
PREAMBLE
Schizophrenia is a severe psychiatric disorder where sufferers commonly have
widespread neuropsychological impairment, very low levels of occupational and social
functioning, a poor quality of life and reduced life expectancy (Elvevag & Goldberg, 2000;
Lehman, 1996). Individuals with schizophrenia are often tormented by “voices” and other
nonverbal sounds over which they have little control. These auditory hallucinations are
experienced by most patients with schizophrenia and are one of the most pervasive,
disabling and distressing of all symptoms. Research into this symptom is motivated by the
belief that understanding the factors that are responsible for auditory hallucinations will
lead to better treatment and services, and ultimately outcome, for sufferers. Auditory
hallucinations are also reported in other clinical groups and in the “normal” population.
However, it cannot be assumed that the mechanisms responsible for auditory hallucinations
are the same for all conditions. Consequently, this thesis focuses primarily on the cognitive
processes underlying auditory hallucinations in schizophrenia.
A number of influential theories, essentially single-deficit accounts, have been
developed in the search for cognitive abnormalities associated with auditory hallucinations
(e.g. Aleman & de Haan, 2000; Frith, 1996). Although significant progress has been made,
still very little is known about the exact cognitive processes underlying auditory
hallucinations. There is a growing concern that a single deficit is unlikely to result in such
a complex event (Nayani & David, 1996). Furthermore, the diverse phenomenology of
auditory hallucinations suggests that a combination of deficits might be needed to explain
this mental phenomenon.
The essence of this thesis is that a specific combination of cognitive deficits in
intentional inhibition and context memory is essential for auditory hallucinations to occur.
Chapters 1 to 10 report a series of studies that describe the steps that have led to this
proposal. As a preliminary study, Chapter 2 examines the characteristics of factors
underlying predisposition to hallucinations in healthy individuals, with the aim of
identifying some experiences that are common in both hallucinatory-like experiences in
normal individuals and auditory hallucinations in schizophrenia. Chapters 3-8 investigate
the proposal that the processes of intentional inhibition and context memory are impaired in
schizophrenia patients with auditory hallucinations, and particularly that a specific

xviii
combination of deficits in both cognitive domains is necessary for auditory hallucinations
to occur. As a test of the specificity of this particular combination of deficits to patients
with auditory hallucinations, Chapter 10 investigates the performance of a group of
individuals with obsessive-compulsive disorder (OCD) on tasks of intentional inhibition
and context memory.
Chapters 1 and 9 provide overviews of research findings pertinent to the current
investigations. In particular, Chapter 1 presents a review of the literature in the areas of
schizophrenia, auditory hallucinations and the cognitive processes of inhibition and context
memory. Chapter 9 reviews literature in the area of OCD.
This thesis is presented as a collection of papers in a format suitable for publication.
At the time of submission, Chapters 2, 3 and 6 have been published, Chapter 4 is in press
and Chapter 8 has been submitted for publication. Because of restrictions on the length of
the manuscripts imposed by some journals, a detailed overview of pertinent previous
research is not presented in the empirical chapters, but a literature review of issues covered
in Chapters 2-8 is presented in Chapter 1. For the same reason, some manuscripts were
necessarily restricted to specific issues, consequently, where appropriate, different analyses
of the same task are presented in separate chapters, as is the case with Chapters 3 and 4 and
with Chapters 6 and 7.
Although 42 patients with schizophrenia participated in the study presented in
Chapter 3, another patient was recruited following the write-up of this study as a
manuscript for publication. Consequently, all studies subsequent to Chapter 3 report the
results of analyses comprising 43 patients with schizophrenia. The addition of this
participant did not result in any difference in statistical outcomes.
Finally, there is a common approach throughout this thesis regarding the group
assignment of patients with auditory hallucinations. Schizophrenia patients currently
experiencing hallucinations were selected on the basis of having experienced auditory
hallucinations on at least half of the days during the preceding four weeks, as assessed by
self-reports and case note reviews. Other schizophrenia patients who did not fit this
criterion, or who did not report experiencing auditory hallucinations, were assigned to the
"non-hallucinating group". This criterion was especially chosen so that patients with very
infrequent hallucinations were not categorized as having auditory hallucinations present.
One exception to this approach is in the manuscript presented in Chapter 4. This chapter

xix
was specifically oriented to answer a precise question regarding whether patients who have
had no auditory hallucinations in the past four weeks also showed the specified cognitive
deficit; consequently, an even more conservative approach to group selection (i.e. absence
vs. presence) was adopted.
References
Aleman, A., & de Haan, E. (2000). Nonlanguage cognitive deficits and hallucinations in
schizophrenia. American Journal of Psychiatry, 157(3), 487.
Elvevag, B., & Goldberg, T. E. (2000). Cognitive impairment in schizophrenia is the core
of the disorder. Critical Reviews in Neurobiology, 14(1), 1-21.
Frith, C. (1996). The role of the prefrontal cortex in self-consciousness: the case of auditory
hallucinations. Philosophical Transactions of the Royal Society of London: B, 351,
1505-1512.
Lehman, A. F. (1996). Quality of life issues and assessment among persons with
schizophrenia. In M. Moscarelli, A. Rupp, & N. Sartorius (Eds.), Handbook of Mental
Health Economics and Health Policy (Vol. 1. Schizophrenia). New York: John Wiley
& Sons Ltd.
Nayani, T., & David, A. (1996). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & T. R. E. Barnes (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 . New York: John Wiley
& Sons Ltd.

- 1 -
INTRODUCTION
- 3 -
Chapter 1
An overview of schizophrenia, auditory hallucinations, inhibition and context memory
Abstract
The aim of this chapter is to provide the theoretical background underpinning our
investigations of auditory hallucinations in schizophrenia. In the first section, the main
epidemiological, cognitive and clinical features of schizophrenia are briefly reviewed.
The second section provides a review of the current literature on auditory
hallucinations. Besides providing a general introduction to hallucinations in
schizophrenia, and in other clinical and normal populations, this section summarizes 1)
the primary features of auditory hallucinations, as delineated in published
phenomenological surveys and data from our own group, 2) current theories about the
nature of the cognitive and socio-psychological processes that result in the hallucinatory
experience, and 3) brain systems thought to be involved in the pathogenesis of auditory
hallucinations in schizophrenia. Since the cognitive domains of inhibition and context
memory are key mechanisms investigated in this thesis, the third section provides an
overview of the main theories about those processes in the normal population. The
fourth and final section presents an outline, and the aims, of the next chapters.

Chapter 1
- 4 -
Schizophrenia
Schizophrenia is a common psychiatric illness, being present in all populations
and cultures with a prevalence between 1.4 and 4.6 per 1000, and incidence rate in the
range of 0.16 and 0.42 per 1000 population (Jablensky, 2000). There is a strong genetic
influence in the aetiology of schizophrenia, although environmental factors remain very
important (Andreasen, 2000; Jablensky, 2000). Typically, individuals develop the
disorder in their early to mid-20s, although an early or late onset is possible. Some
studies have shown that males and females are affected in roughly equal numbers, with
little evidence of significant sex differences in symptom profile (Jablensky, 2000). The
course of the illness may be variable, with some patients remaining chronically ill while
others display exacerbations and remissions. Antipsychotic medications have been
successful in managing the symptoms but unpleasant side effects frequently occur,
especially with typical antipsychotic medications (see reviews by Schultz & Andreasen,
1999; Wong & Van Tol, 2003). In conjunction with medications, psychosocial
rehabilitation (targeting the importance of psychological support, family interventions,
vocational rehabilitation and community support) has been very useful in reducing
acute-care needs, shortening recovery after an acute episode and managing some of the
prominent psychotic symptoms, although ongoing intervention is required to maintain
treatment gains (Penn & Mueser, 1996; Rector & Beck, 2001; Schultz & Andreasen,
1999).
The health care costs, treatment issues and other economic costs attributable to
schizophrenia are very substantial (Schultz & Andreasen, 1999; Wong & Van Tol,
2003). The personal cost to the individual is also high, with a significant percentage of
patients having a poor quality of life, significant economic burden and a loss of
supportive social network (Lehman, 1996). Cognitive, affective, social and
occupational functioning is usually severely disrupted following the onset of the
disorder. In particular, schizophrenia is associated with widespread neuropsychological
impairment, specifically in attention, memory and executive functioning (e.g. Aleman,
Hijman, de Haan & Kahn, 1999; Crider, 1997; Elliott & Sahakian, 1995; Elvevag &
Goldberg, 2000; Gur, Moelter & Ragland, 2000; Heinrichs & Zakzanis, 1998;
Nathaniel-James, Brown & Ron, 1996; Tollefson, 1996). A recent review of the
evidence, based on 204 studies, concluded that schizophrenia is characterized by a
broad range of cognitive deficits with varying degrees of impairment in many domains
(Heinrichs & Zakzanis, 1998). Tollefson (1996) also observed that cognitive deficits

Chapter 1
- 5 -
are not limited to a small subset of patients, but are a frequent feature of the disorder
and are independent of the patient’s clinical state or of the subtype of the illness. Based
on this type of evidence, it is now commonly believed that cognitive deficits are a
central feature of schizophrenia and are at the very core of the dysfunction of this
disease (e.g. Elvevag & Goldberg, 2000). Other supporting evidence for the suggestion
of cognitive deficits as a primary characteristic of the disorder is the finding that such
impairments appear before a first episode and reflect a drop-off from an individual’s
previous level of functioning (Tollefson, 1996).
Widespread structural and functional brain abnormalities have also been
consistently demonstrated in individuals with schizophrenia. Most notable are an
enlargement of the ventricular system, prominent sulci, reduced cerebral size, decreased
temporal, hippocampal and frontal lobe size and disruptions in the prefrontal cortex and
distributed functional circuits (e.g. Andreasen, Paradiso & O’Leary, 1998; Arnold,
1997; Fletcher, McKenna, Friston, Frith & Dolan, 1999; Lewis & Anderson, 1995;
McCarley, Shenton, O’Donnell & Nester, 1993; Nelson, Saykin, Flashman & Riordan,
1998; Pantelis et al, 1997; Schultz & Andreasen, 1999; Weinberger, Aloia, Goldberg &
Berman, 1994).
Schizophrenia has come to be understood as having multiple symptom dimensions
(e.g. Bentall, 1997; Haier, 1980; Klimidis, Stuart, Minas, Copolov & Singh, 1993;
Lenzenweger, 1999; Liddle et al, 1992, Seaton, Goldstein & Allen, 2001). In terms of
the commonly accepted description of the disorder as expressed in the Diagnostic
Statistical Manual of Mental Disorders-4th Edition (DSM-IV, 1995), there are two main
groups of symptoms: positive symptoms, which can be described as normal functions
that are distorted or exaggerated, such as abnormalities in perception (hallucinations), in
inferential thinking (delusions), in language (disorganized speech) and in behavioural
monitoring / control (disorganized behaviour); and negative symptoms, where there is a
diminution or absence of mental functions that are normally present, such as in the case
of alogia (decrease in fluency of ideas and language), affective blunting (diminution in
the ability to express emotion), avolition (decrease in the ability to initiate and pursue
goal-directed activity), anhedonia (decrease in the ability to seek out and experience
pleasure), and attentional impairment (decrease in the ability to focus attention). The
DSM-IV diagnostic criteria for schizophrenia include at least one month of active phase
symptoms (i.e. two or more of the following; delusions, hallucinations, disorganized
speech, grossly disorganized or catatonic behaviour, negative symptoms) with some
signs of the disorder persisting for at least 6 months, and a substantial decline in

Chapter 1
- 6 -
functioning in one or more major areas of functioning. The clinical diversity of
schizophrenia has led to many attempts to identify syndromes of the illness. Briefly,
one formulation proposes a distinction between positive and negative symptomatology
(e.g. Crowe, 1980), but more recent evidence suggests that three distinguishable
syndromes, reality distortion (delusions and hallucinations), disorganisation (disorders
of the form of thought and inappropriate affect) and psychomotor poverty (including
poverty of speech, flatness of affect and decreased spontaneous movement symptoms)
may better describe the illness (e.g. Harris, Gordon, Bahramali & Slewa-Younan, 1999;
Liddle, 1987; Liddle et al, 1992).
The value of the concept of schizophrenia as a unitary disease, however, is
increasingly being questioned. For example, concerns regarding the heterogeneity of
symptom presentation, course, prognosis and cognitive profile have led researchers to
question the validity of schizophrenia as representing a homogeneous entity (e.g.
Bentall, 1997; Elliott & Sahakian, 1995; McGlashan, 1998; Mojtabai, 1999; Seaton,
Golstein & Allen, 2001). In addition, although some symptoms have been given greater
weight in current classification systems, a poor correlation has been found between
presentation of any particular symptom and diagnosis, or outcome (Bentall, 1997). This
has raised doubts with regard to the scientific validity of the current diagnostic system,
and many researchers now support the view that schizophrenia may best be explored by
examining patients who share the same symptoms (e.g. Baxter & Liddle, 1998; Bentall,
1997, Bentall, Baker & Havers, 1991).
Cognitive Neuropsychiatry
Since diagnosis is based upon the presence of symptoms, it has been proposed that
a better approach to understanding the mechanisms of this disorder is to investigate
individual symptoms, an approach which has recently been referred to as “Cognitive
Neuropsychiatry” (David & Halligan, 2000). This approach begins with the assumption
that psychiatric disorders are predominantly brain disorders. It then applies methods
from Cognitive Neuropsychology in an attempt to understand how disruptions to
specific brain regions or networks give rise to symptoms that characterise and define
these disorders (Pantelis & Maruff, 2002). In particular, Cognitive Neuropsychiatry
aims to offer a cognitive explanation for a disorder by investigating patterns of impaired
and intact cognitive performance. Functional models of individual symptoms can then
be developed, with the secondary gain of being able to contribute to current
understanding of models of normal cognitive functioning (David & Halligan, 2000).

Chapter 1
- 7 -
Advantages to this approach include the ability to scrutinize individual symptoms in
isolation from other confounding factors, and avoiding potential misclassification
problems associated with diagnostic disorders. The Cognitive Neuropsychiatry
approach has led to an increasing understanding that different symptoms, such as
auditory hallucinations and delusions, have a distinct neuropsychological and
neuropathological profile (e.g. Baxter & Liddle, 1998; Blackwood, Howard, Bentall &
Murray, 2001; Davies, Coltheart, Langdon & Breen, 2001; Frith & Done, 1988;
Kurachi, 2003; Langdon & Coltheart, 2000; Liddle et al, 1992). As a consequence, it is
hoped that one day it will be possible to identify factors that may predispose an
individual to show these symptoms.
Given the appeal of the Cognitive Neuropsychiatry approach, the current thesis
takes this symptom-oriented focus. In particular, given the importance of auditory
hallucinations in the diagnosis of schizophrenia, the aim of this thesis is to identify
some of the cognitive processes that are responsible for the hallucinatory experience, in
order to develop a model that will lead to a better understanding of auditory
hallucinations in schizophrenia.
Auditory Hallucinations
Description
David (2004) has recently proposed the following definition of hallucinations: ‘A
sensory experience which occurs in the absence of corresponding external stimulation
of the relevant sense organ, has sufficient sense of reality to resemble a veridical
perception, over which the subject does not feel s/he has direct and voluntary control,
and which occurs in the awake state’ (p. 110).
Auditory hallucinations occur in approximately 74% of individuals with
schizophrenia (Mueser, Bellack & Brady, 1989; Sartorius, Shapiro & Jablensky, 1974).
These hallucinations, referred to as voices by patients themselves, usually consist of
spoken speech, but can also include nonverbal sounds. Auditory hallucinations are
experienced as being highly distressing. In extreme cases, they can result in suicide and
other dangerous behaviours (Falloon & Talbot, 1981, Walsh et al, 1999). In about 25%
of cases, voices respond only partially or not at all to currently available drug therapy
(Shergill, Murray & McGuire, 1998).

Chapter 1
- 8 -
Auditory hallucinations in individuals other than with schizophrenia
While auditory hallucinations are of singular importance in schizophrenia, they
are not restricted to this disorder. They have been found to occur in organic states such
as focal brain lesions of the temporal lobes, fever, delirium, Wernicke's encephalopathy
and dementia (Alpert & Silvers, 1970; Asaad & Shapiro, 1986; Slade & Bentall, 1988)
and they have also been reported in patients with severe affective disorders (Bentall,
1990, Bliss, Larson & Nakashima, 1983; Honig et al, 1998; Lowe, 1973; Mueser et al,
1990). The characteristics of auditory hallucinations in those groups have been found to
be similar to that of auditory hallucinations in schizophrenia (Junginger & Frame,
1985), although differences in the frequency, emotional quality and perceived level of
control have been noted (Alpert & Silvers, 1970; Bentall, 2000; Davies, Griffin & Vice,
2001; Honig et al, 1998, Johns, Hemsley & Kuipers, 2002; Lowe, 1973). Some
experiences akin to auditory hallucinations also occur in the realm of “normal”
experiences, and a number of studies have shown that between 10 to 38% of the normal,
healthy, population report some type of hallucinatory experience (Bentall & Slade,
1985a; Davies, Griffin & Vice, 2001; Ohayon, 2000; Young, Bentall, Slade & Dewey,
1987). The experience has been described as being qualitatively different from auditory
hallucinations in schizophrenia – with higher perceived control and predominantly
positive (rather than negative) content (Honig et al, 1998). Another commonly reported
auditory hallucination-like experience in healthy people occurs when falling asleep
(hypnagogic) and on waking (hypnopompic). Finally, hallucinations are also
experienced under the influence of drugs such as LSD (Aggernaes, 1972, Asaad &
Shapiro, 1986) although, again, the characteristics of these experiences are different
from the hallucinatory experience in schizophrenia.
The main focus of this thesis is concerned with understanding the cognitive
processes that underlie the experience of auditory hallucinations in schizophrenia. The
reasons are twofold. Firstly, it cannot be assumed that the mechanisms responsible for
auditory hallucinations are the same in different populations (Frith & Dolan, 1997) and,
secondly, focussing exclusively on auditory hallucinations in schizophrenia eliminates
possible confounding factors associated with other pathologies and is therefore more
likely to lead to an explanation of this symptom.
Main descriptive features of auditory hallucinations in schizophrenia
Auditory hallucinations are complex mental events often described as comprising
a mixture of different phenomenological features, which combine to produce a highly
Chapter 1
- 9 -
individualized experience. One of the most comprehensive published phenomenological
surveys of auditory hallucinations was carried out by Nayani and David (1996b) on 100
psychotic patients. Although only 61% of their patients had a diagnosis of
schizophrenia, this study provides an interesting insight into the complexity and multi-
facetedness of auditory hallucinations. However, given the singular importance of
auditory hallucinations in the diagnosis of schizophrenia, there are surprisingly few
detailed surveys of the main phenomenological features of auditory hallucinations in
this patient group alone. We conducted our own investigation of the clinical features of
auditory hallucinations, using 35 patients with a DSM-IV diagnosis of schizophrenia
(Waters, Badcock & Maybery, 2004, see Appendix A). These patients completed a
questionnaire comprising selected items from the Psychotic Symptom Rating Scales
(PSYRAT; Haddock, McCarron, Tarrier & Faragher, 1999) and the Mental Health
Research Institute Unusual Perceptions Schedule (MUPS; Carter, Mackinnon, Howard,
Zeegers & Copolov, 1995).
The phenomenology of auditory hallucinations, as delineated in published surveys
and data from our own group, can be categorized using a number of characteristics.
Although there is still debate whether these parameters are valuable diagnostically (e.g.
Honig et al, 1998; Junginger & Frame, 1985) they provide a useful preliminary
framework for research purposes and are relevant to the investigation of auditory
hallucinations in schizophrenia.
Frequency
The frequency of auditory hallucinations may vary from once or twice weekly to
continuously (Nayani & David, 1996b). Intriguingly, a small group of patients with
schizophrenia never experience auditory hallucinations during the course of their
illness.
Content
In schizophrenia, auditory hallucinations are usually experienced as voices
although they can also take the form of other, nonverbal sounds (e.g. bangs, animal
sounds). Although the majority of research on auditory hallucinations focuses on the
experience of verbal hallucinations, approximately 60% of patients admit to hearing
sounds in addition to voices (Nayani & David, 1996b; Waters, Badcock & Maybery,
2004). Nayani and David also reported that the most frequently reported types of
hallucinated voices are commands, personal insults and abuse, although the content of
voices are sometimes reported to be positive or neutral. The message carried by the
hallucinated voices is often interpreted as being very personal, with patients reporting

Chapter 1
- 10 -
that the voices have access to highly private details (Birchwood & Chadwick, 1997).
This knowledge of personal information, together with commentaries on the patient’s
actions or thoughts, may contribute to the feeling that the voice is omnipotent and
powerful (Birchwood & Chadwick, 1997).
Form
Form refers to the characteristic, often perceptual, features by which the content is
carried. For example, Nayani and David's (1996b) survey showed that male voices are
most likely to be heard and hallucinated voices often speak with accents different to the
region or social class of the patient. The tone of voices is predominantly perceived as
being negative and critical, although pleasant voices are also common. In our sample,
the voices were predominantly experienced as being of the same loudness as the
patient’s own voice or quieter, confirming the results obtained by Nayani and David.
In verbal hallucinations, different types of grammatical speech have been identified.
Second or third person hallucinations (e.g. 'you are going to die' and 'he's going to bed'
respectively) and purely descriptive non-personal sentences ('the grass is green') are the
most common. The results from our own investigations confirmed that verbal
hallucinations are not restricted to any one type of grammatical speech but rather
include a mixture of grammatical types. Auditory hallucinations are traditionally
reported as being distinct from one's own thoughts, and may be perceived to originate
from inside or outside the head, or both (Copolov, Trauer & MacKinnon, in press;
Hunter, 2004; Waters, Badcock & Maybery, 2004).
External attribution
A distinguishing feature of schizophrenic hallucinations is that the experience is
perceived to originate from an external agent. Nayani and David (1996b) and David
(2004) observed that the person experiencing auditory hallucinations usually assigns an
identity to the hallucinated voices, the most commonly reported being persons known to
the patients in real life, and a minority being assigned a delusional interpretation (e.g.
Satan). Our investigations showed that close to half of all patients believed that their
voices were familiar and similar to voices of people who had spoken to them in the past.
Perceived Intrusiveness
Verbal, and nonverbal, hallucinations are reported to be intrusive because they are
unintended, persistent, beyond the control of the voice-hearer and because the patients
are often unable to escape from the experience (Oulis, Mavreas, Mamounas & Stefanis,
1995; Slade & Bentall, 1988). The feeling of lack of control has been perceived as

Chapter 1
- 11 -
being a crucial factor in the development of distress and other affective responses linked
to auditory hallucinations (e.g. Close & Garety, 1998).
Affect
There is often considerable distress associated with auditory hallucinations. Our
survey showed that most patients (82.9%) admitted that at least some of their voices
were distressing. This percentage is higher than that reported by Nayani and David
(1996b) but is consistent with Honig et al’s (1998) findings. Half of our patient sample
reported that their hallucinated voices caused them moderate to severe disruption in
everyday life. Consistent with these findings, auditory hallucinations have often been
found to co-occur with depression, anger, fear, anxiousness and low self-esteem (Alpert
& Silvers, 1970; Carter, Mackinnon & Copolov, 1996; Close & Garety, 1998;
Delespaul, deVries, van Os, 2002; Hustig & Hafner, 1990; Johns, Hemsley & Kuipers,
2002).
This brief review of the main phenomenological features of auditory
hallucinations reveals the striking complexity of the hallucinatory experience and
indicates the broad range of features that potentially contribute to a highly
individualized experience. The results of our survey were similar to the findings of
Nayani and David, with the exception of a higher rate of distress, confirming that the
results of their survey of psychotic patients provides an accurate indication of the main
features of auditory hallucinations in schizophrenia specifically. Importantly, it also
suggests that our sample of hallucinating patients was not unusual and therefore that the
empirical findings presented in the next few chapters are not limited to an atypical
sample of patients.
Theories of auditory hallucinations in schizophrenia
Both cognitive and socio-psychological theories have been put forward to explain
auditory hallucinations in schizophrenia. With regard to cognitive theories of auditory
hallucinations, there are three contemporary influential classes of theories which are
essentially single-deficit accounts: Inner Speech theories, Mental Imagery theories and a
Context Memory deficit account. These will be addressed in turn.
Inner speech accounts
The first group of cognitive theories is characterised by the proposal that auditory
hallucinations consist of inner speech that is misattributed to an external source due to
defective reality- or self-monitoring (e.g. Bentall, Kaney & Dewey, 1991; Frith, 1996).
One version (e.g. Frith, 1996; Frith & Dolan, 1997) suggests that this is due to

Chapter 1
- 12 -
difficulties in distinguishing sensations caused by one’s own actions from those that
arise from external influences because of a deficit in forward modelling or 'corollary
discharge', a failure of prior knowledge about motor intentions. In support, there is a
large body of evidence indicating that patients with auditory hallucinations have
difficulties recognizing their own actions or thoughts (e.g. Blakemore, Smith, Steel,
Johnstone & Frith, 2000; Brébion, Smith, Amador, Malaspina & Gorman, 1998; Cahill
& Frith, 1994) and are more likely than those without hallucinations to misattribute self-
generated items to an external source (e.g. Baker & Morrison, 1998; Johns & McGuire,
1999). Findings from functional brain imaging techniques have also been presented as
evidence that inner speech is involved in auditory hallucinations. For example,
McGuire, Shah and Murray (1993) observed greater activity in Broca’s area when
patients were hallucinating, a region shown to be active during internal speech. In
addition, imaging studies have presented some evidence for defective self-monitoring,
showing attenuation of activation in regions concerned with the monitoring of inner
speech (McGuire et al, 1995).
This class of theories has been very influential in the search for cognitive
abnormalities associated with auditory hallucinations. One criticism, however, has been
that the relationship between monitoring and auditory hallucinations may be more
complex than it has been proposed. Goldberg, Gold, Coppola and Weinberger (1997),
for instance, tested the forward modelling proposal in a sample of patients with
schizophrenia with a delayed auditory feedback task and failed to find a link between
corollary discharge and monitoring failures. Recently, Allen et al (2004) also
demonstrated that a self-monitoring deficit alone cannot account for the presence of
hallucinations. A group of hallucinating and nonhallucinating patients and a healthy
control group made recordings of their own voice and were subsequently asked to make
self/nonself judgements about the source of the pre-recorded speech. Patients with
hallucinations tended to misidentify their own recorded material. Since the task did not
require self-monitoring, the authors concluded that hallucinations were not solely a
function of defective self-monitoring. Further criticism of the claim of monitoring as a
central cognitive deficit in auditory hallucinations arises from evidence that this deficit
lacks specificity. A range of studies have shown a deficit in source monitoring in
delusional and thought disordered patients independent of the presence of auditory
hallucinations (e.g. Brébion, Smith, Gorman & Amador, 1997), in schizophrenia
patients regardless of symptomatology (e.g. Aleman et al, 2003; Keefe, Arnold, Bayen
& Harvey, 1999) and in non-schizophrenic confabulators (Nathaniel-James & Frith,

Chapter 1
- 13 -
1996), suggesting that the monitoring impairment, on its own, has little predictive value
for auditory hallucinations.
A variant on the proposal of auditory hallucinations as inner speech proposes that
hallucinations reflect a disruption in the brain’s language processing circuitry (Hoffman,
1986; Hoffman & McGlashan, 1997, 1998). In an earlier model, these authors proposed
disruptions in language planning processes whereby there is a breakdown of
anticipatory pre-representations of motor plans, contributing to unintended verbal
speech. In a more recent version, Hoffman and McGlashan (1997, 1998; Hoffman,
Rapaport, Mazure & Quinlan, 1999) moved on from this position and proposed a model
of exaggerated linguistic expectation resulting from a faulty verbal working memory
system. However, from an empirical point of view, there is little evidence that working
memory is especially impaired in individuals with hallucinations (Bagner, Melinder &
Barch, 2003; David & Lucas, 1993; Haddock, Slade, Prasaad & Bentall, 1996).
Although the proposal of auditory hallucinations as consisting of inner speech is a
compelling one, it does not encompass, in its current form, some of the more prominent
characteristic features of auditory hallucinations. It cannot explain, for example, why
patients experience nonverbal auditory hallucinations. An explanation for the voices'
social identity and why the voices are often recognised as belonging to people that the
patients know is also lacking. In addition, it is difficult to reconcile the proposal of
inner speech with some of the more perceptual characteristics of auditory hallucinations,
such as variations in loudness or voices with an accent or gender different from that of
the patient. Furthermore, while inner speech is mainly experienced in the first person,
auditory hallucinations often consist of descriptive comments or occur in the second or
third person. Finally, it is not clear how inner speech may be experienced as coming
from outside the head. In sum, although the idea that auditory hallucinations involve
the misattribution of inner speech has been very productive in terms of understanding
possible mechanisms underlying auditory hallucinations, it cannot, on its own, account
for many of the distinctive features of auditory hallucinations. This is not to deny the
importance of its contribution; rather, our view is that this account is not sufficient, as it
is currently conceptualised, to explain auditory hallucinations.
Mental imagery account
The second prominent theory of auditory hallucinations proposes an abnormality
of mental imagery (Aleman & de Haan, 2000, Aleman, Böcker, Hijman, Kahn & De
Haan, 2002; Mintz & Alpert, 1972). Proponents of this view suggest that individuals
who experience hallucinations have very vivid mental imagery which would result in

Chapter 1
- 14 -
confusion as to whether the hallucinated voices were imagined or heard. In a recent
development of this theory, Aleman, Böcker, Hijman, de Haan and Kahn (2003)
propose that, in individuals susceptible to auditory hallucinations, top-down factors are
given higher priority than bottom-up processes resulting in an imbalance between
sensory and mental elements and an increasing influence of imagery on perception.
Evidence for this group of theories primarily rests on the basis of studies that have
shown particularly vivid imagery in patients with auditory hallucinations (e.g. Mintz &
Alpert, 1972; Young, Bentall, Slade & Dewey, 1987) and in healthy individuals who
score high on scales designed to measure predisposition to hallucinations (Aleman,
Böcker & de Haan, 1999; Barrett & Etheridge, 1992). However, this view has not
always consistently been supported by empirical evidence (see Bentall, 1997). For
example, some studies have failed to find particularly vivid imagery in those with
auditory hallucinations, in fact suggesting a decrease in the vividness of auditory images
in these individuals (e.g. Starker & Jolin, 1982). Others have failed to find differences
in either auditory or visual imagery between hallucinating and nonhallucinating groups
of patients (Aleman et al, 2003; Böcker, Hijman, Kahn & de Haan, 2000; Evans,
McGuire & David, 2000). Furthermore, the theoretical basis of this class of theories has
been criticized on the grounds that there is no evidence that vividness of an imagined
event is enough to believe that it is real and that healthy individuals who report vivid
mental events do not necessarily interpret them as being real (Bentall, 1997). Finally,
there are also fundamental problems in making direct comparisons between results of
studies on imagery tasks and the experience of auditory hallucinations, since imagery
involves volitational behaviour whereas auditory hallucinations are, by definition,
unintended. The strength of this theory however relies on its ability to account for the
perceptual features of hallucinations since imagery is thought to share important
characteristics with perception (Aleman et al, 2003). In addition it is able to provide an
explanation for nonverbal hallucinations and a range of social identities for verbal
hallucinations. However, the uncontrollable nature of auditory hallucinations, the
characteristic feelings of intrusiveness that many patients experience and the complex
role of affect in hallucinations still remain to be explicitly outlined, indicating that this
group of theories still has some way to go before being able to explain all of the
phenomenological features of auditory hallucinations.
Context memory deficit account
The third, and recently emerging, cognitive theory concerns context memory and
auditory hallucinations. It is now a consistent view that schizophrenia is linked to a

Chapter 1
- 15 -
deficit in integrating contextual information in memory, and several authors have
proposed that many of the cognitive deficits observed in schizophrenia result from an
impairment in the ability to process contextual information (e.g. Bazin, Perruchet,
Hardy-Bayle, & Feline, 2000; Cohen & Servan-Schreiber, 1992; Rizzo, Danion, Van
der Linden, & Grange, 1996; Servan-Schreiber, Cohen, & Steingard, 1996).
There are also increasing suggestions that a deficit in context memory may be
linked to positive symptoms, and in particular to auditory hallucinations (Brébion et al,
1999; Brébion, Gorman, Amador, Malaspina & Sharif, 2002; Guillem et al, 2003;
Servan-Schreiber, Cohen, & Steingard, 1996). A context memory theory of auditory
hallucinations has been proposed by Nayani and David (1996a), who suggested that
auditory hallucinations result from a disturbance of the processes that serve to bind the
contextual components of memories together. In particular, they suggested that
auditory hallucinations consist of memories of speech fragments which are not
recognized because of a deficit in context memory, resulting in an incomplete
representation of memories and consequently a failure to identify their origins.
Support for the proposal of a context memory deficit in auditory hallucinations
comes primarily from studies that have shown a failure to identify the source of actions
and thoughts among schizophrenia patients currently experiencing auditory
hallucinations, as described in the previous section on Inner Speech (e.g. Baker &
Morrison, 1998; Bentall, Baker & Havers, 1991; Brébion, Smith, Gorman, Amador,
1996; Brébion et al, 2000, 2002; Franck et al, 2000; John & McGuire, 1999). Brébion
et al (2000), for instance, showed that patients with hallucinations made false
recognition of non-produced items in a memory task and misattributed self-produced
items. A number of other studies have replicated the finding that patients with
hallucinations have difficulties discriminating between self-generated and other-
generated actions and distinguishing between internal and external events (e.g. Baker &
Morrison, 1998; Brébion, Smith, Gorman & Amador, 1996; Brébion, Gorman, Amador,
Malaspina & Sharif, 2002; Franck et al, 2000). A deficit in identifying the origins of
mental events has also been demonstrated in normal individuals who score high on a
predisposition to hallucinations scale (Rankin & O’Carroll, 1995). Interestingly, a
number of studies have also shown that patients with hallucinations are more likely to
make errors when words are derogatory, rather than when words are neutral or
complimentary (e.g. John & McGuire, 1999; Morrison & Haddock, 1997). The only
study that considered a loss of context information other than source in patients with
auditory hallucinations is Brébion et al (2002). In this study, patients with

Chapter 1
- 16 -
schizophrenia attempted a task of free recall in which four lists of words were
presented. The authors noted that auditory hallucinations severity was correlated with
the erroneous recall of words presented in different lists, and interpreted this deficit as
an impairment in the ability to remember temporal context during production of the
words.
The appeal of Nayani and David's theory is that it can address some of the
criticisms directed to Inner Speech theories regarding the characteristic features of
hallucinations. The proposal of auditory hallucinations as memories can account for the
broad variations in form and content of auditory hallucinations. It can also explain why
patients experience nonverbal auditory hallucinations and why the voices’ social
identity can be different from that of the patients, although it is not clear how it explains
the characteristic feature of intrusiveness.
However, there is still insufficient evidence to fully support Nayani and David's
theory. The only empirical evidence supporting their theory is the finding of a deficit in
source monitoring in auditory hallucinations and there is indict evidence of a deficit in
retaining the temporal context of memories, suggesting that the exact nature of the
contextual memory deficit in auditory hallucinations has not yet been clearly
established. One of the aims of the current thesis is to test Nayani and David’s proposal
of an association between auditory hallucinations and a context memory deficit, with a
new task that directly assesses memory for the content of events in conjunction with
memory for the source and the temporal context of these events.
Another important criticism of this theory as a single-deficit explanation of
hallucinations is that its only directly supporting evidence, a deficit in source memory,
occurs in schizophrenia patients independently of the presence of auditory
hallucinations, as reviewed earlier (e.g. Brébion, Smith, Gorman et al, 1997; Keefe,
Arnold, Bayen & Harvey, 1999). Consequently, a context memory deficit, on its own,
does not directly predict the presence of auditory hallucinations. The only way this
deficit may be convincingly incorporated into a model of auditory hallucinations is if it
is only one of at least two deficits that are essential for hallucinations. In this thesis, we
will propose a new theory of auditory hallucinations which suggests that a deficit in
context memory is critically relevant to the aetiology of auditory hallucinations when
combined with another cognitive deficit.
Socio-psychological theories
Although this thesis has mostly a cognitive focus, it is important to be aware that
some explanations of hallucinatory experiences have been developed independently of

Chapter 1
- 17 -
cognitive theories. Proponents of these accounts have emphasized the “reflexive”
relationship between the person and the person’s experience of voices (e.g. Davies,
Thomas & Leudar, 1999; Leudar, Thomas, McNally & Glinski, 1997; Thomas, Bracken
& Leudar, 2004). In particular, it has been suggested that the idiosyncratic ways in
which individuals respond to an abnormal perceptual experience affect their perception
of the experience, which influences their coping strategies and emotional response
(Baker & Morrison, 1998; Birchwood & Chadwick, 1997; Chadwick & Birchwood,
1994; Close & Garety, 1998; Morrison, Haddock & Tarrier, 1995). Chadwick and
Birchwood (1994), for instance, proposed that a person's belief about his or her voices is
a mediating factor between hallucinations and the distress that is experienced, and that
these beliefs may develop as a result of an attempt to explain unusual experiences.
Birchwood and Chadwick (1997) identified two different constructs relevant to these
issues: (a) the belief about the voices' intent to do harm or good and (b) the beliefs about
the voices' omnipotence, and the reaction to these beliefs in terms of engagement or
resistance. Morrison and colleagues (Morrison, Haddock & Tarrier, 1995; Baker &
Morrison, 1998; Morrison, 2001) have emphasized the role of exaggerated significance
about the meaning of auditory hallucinations and metacognitive beliefs, or cognitive
biases, in the development of hallucinations. Metacognitive beliefs are thought to occur
when an individual experiences something that is incompatible with the beliefs about
his/her thinking; hallucinations are therefore experienced when intrusive thoughts are
attributed to an external source in order to reduce cognitive dissonance (e.g. the
interpretation that auditory hallucinations threaten the integrity of the individual).
Langdon and Coltheart (2000) have also recently explained how individual differences
in cognitive bias, and in particular in the various motives that patients ascribe to their
voices, result in different types of hallucinatory experiences. These socio-psychological
theories are important because they incorporate the role of the relationship between the
patient and his/her hallucinations as a crucial component to understanding
hallucinations. However, although these theories are useful models of the maintenance
of auditory hallucinations, they do not explain so well the onset of hallucinations.
Neuropathology of auditory hallucinations
It is important to have a clear understanding of the neuropathological processes
involved in this symptom as they set the boundaries in which models of cognitive
processes must occur. One approach to understanding auditory hallucinations has been
to investigate neurochemical mechanisms, on the basis that neurotransmitters are

Chapter 1
- 18 -
responsible for information transmission in the central nervous system (see David,
1999; David & Busatto, 1998 for reviews). Dopamine D2 receptors have been linked to
auditory hallucinations based on findings that drugs that increase dopamine activity
produce psychotic-like symptoms (which include auditory hallucinations) in normal
individuals. GABA receptors have also been implicated because of their interaction
with dopamine receptors (see David, 1999; David & Busatto, 1998; Gray, 1998 for
recent reviews).
Another approach has been to examine the anatomical and functional brain
mechanisms associated with auditory hallucinations, mostly with the help of brain
imaging tools. A few brain regions appear to have been consistently associated with
auditory hallucinations. Given the auditory nature of the experience, it is not surprising
that the left temporal and parietal auditory-language association areas have often been
implicated in auditory hallucinations. For example, post-mortem and structural
neuroimaging studies have found that the auditory cortex bilaterally and the left superior
temporal gyrus (STG) are reduced in volume bilaterally in hallucinating patients
compared to psychiatric control groups (e.g. Weiss & Heckers, 1999). In a review of
the literature, Stephane, Barton and Boutros (2001) identified that 5 out of 10 studies
found some association between size of the STG and auditory hallucinations. Imaging
studies have also found activation of the left superior temporal regions during auditory
hallucinations (e.g. Ait Bentaleb, Beauregard, Liddle & Stip, 2002; Cleghorn et al,
1992; Copolov et al, 2003; David et al, 1996; Lennox, Bert, Park, Jones & Morris,
1999; Levitan & Ward, 1999; Stephane et al, 2001; Woodruff et al, 1997). Finally,
Hoffman et al (2003) have found that repetitive transcranial magnetic stimulation
(rTMS) in the left superior region of the temporal cortex produced a reduction in
frequency of auditory hallucinations, indicating that this region may participate in the
hallucinatory experience. Others have found activation of the right, but not the left,
temporal cortex (Lennox et al, 1999; McGuire et al, 1996). Involvement of the right
temporal regions is not unusual since they, too, are activated during normal auditory
speech perception (Silbersweig & Stern, 1996). Temporal cortical areas are usually
activated during auditory-verbal perception and during auditory-verbal imagery
(McGuire et al, 1995, 1996; McGuire, Silbersweig & Frith, 1996) and such findings
have been used to support the suggestion that auditory hallucinations occur as a result of
a disturbance in unintended inner speech and imagery.
Functional Magnetic Resonance Imaging (fMRI) and positron emission
tomography (PET) studies of patients with auditory hallucinations have supported the

Chapter 1
- 19 -
involvement of areas usually associated with the production of language, such as
activation of Broca's area (Cleghorn et al, 1992; McGuire et al, 1993, 1995). This
evidence has led to the suggestion that speech generation pathology is a fundamental
mechanism for auditory hallucinations, and has been cited as support for the hypothesis
that auditory hallucinations arise from misidentified internal speech. However, Broca's
area has not been implicated in all fMRI and PET studies of patients' auditory
hallucinations (Ait Bentaleb et al, 2002; Copolov et al, 2003; McGuire et al, 1995;
Woodruff et al, 1997), raising doubts about the proposal of misidentified inner speech in
auditory hallucinations. Furthermore, Silbersweig et al (1996) also explain that Broca’s
area may be activated during cognitive tasks that do not entail inner speech, so the
activation of this region does not necessarily mean that inner speech is involved.
Other regions of the frontal cortex which have been found to be activated in
auditory hallucinations include the left orbitofrontal cortex (OFC; Silbersweig et al,
1995) and the anterior (Lennox et al, 1999; McGuire et al, 1993; Silbersweig et al,
1995) and posterior (Copolov et al, 2003) cingulate gyrus. Other cerebral regions
implicated include the hippocampus, parahippocampal gyrus, bilateral thalamus and
ventral striatum (Copolov et al, 2003; Silbersweig et al, 1995; Takebayashi, Takei &
Mori, 2002; Woodruff & Murray, 1994). Activation of the hippocampus in particular
suggests that memories may play a role in the hallucinatory experience.
There are also suggestions that abnormal interconnections between the prefrontal
cortex and the temporal lobes could be responsible for auditory hallucinations (e.g.
Frith, 1995). In normal individuals, the left superior temporal regions are inhibited
during speech (McGuire, Silbersweig & Frith, 1996). However, such inhibition has not
been found in patients with schizophrenia (e.g. Fletcher et al, 1999) and it has been
suggested that this inhibitory system is impaired as a result of reduced frontal-temporal
connections (Fletcher, 1998; Ford et al, 2002; Friston, 1999; Frith, 1995, 1996).
Abnormal interactions between these two centres have been thought to be responsible
for auditory hallucinations (Frith, 1995, 1996) and recent electrophysiological and
imaging evidence has been found to support this suggestion (Ford et al, 2002; Lawrie et
al, 2002; Shergill, Brammer, Williams, Murray & McGuire, 2000).
In sum, numerous brain regions have been found to be associated with auditory
hallucinations. Although the finding that so many different neural regions are involved
in the experience of auditory hallucinations has not been integrated into a cohesive
explanation of hallucinatory phenomenon, it is consistent with the heterogenous and
complex nature of this mental phenomenon.

Chapter 1
- 20 -
Key cognitive processes under investigation
Inhibition
One of the cognitive domains discussed in this thesis in relation to auditory
hallucinations is inhibition. Inhibition is a basic cognitive mechanism which has been
defined as a collection of processes which allows the suppression of previously
activated cognitive contents, the clearing of irrelevant actions or attention from
consciousness, the control of overt behaviour and motor movements and the resistance
to interference from potentially attention-capturing stimuli (Harnishfeger, 1995).
Failure to maintain control through inhibitory efficiency is thought to result in less than
optimal processing of task-relevant stimuli to the detriment of task performance. There
is general agreement that inhibition is not a unitary construct, but that it is better
described as a family of processes, each with its own distinct operating characteristics.
Support for this suggestion includes (a) a number of studies that have shown that
correlations between different measures of inhibitory functions are generally low (e.g.
Friedman & Miyake, 2004; Kramer, Humphreys, Larish, Logan & Stager, 1994;
Spinella, 2002, Stuss et al, 1999), (b) divergent findings in the same population sample
when inhibition is measured by different tasks (e.g. Kramer et al, 1994, Stuss et al,
1999), and (c) evidence of different operating characteristics between tasks of inhibition
(namely different levels of working memory involvement) (e.g. Kramer, 1994). As a
result, there have been various attempts at producing a workable taxonomy of the main
types of inhibition (eg. Clark, 1996; Dempster, 1993; Kok, 1999; Nigg, 2000;
Harnishfeger, 1995; Wilson & Kipp, 1998).
A number of theories have been proposed, based on research about the different
developmental rates of various forms of inhibition (Dempster & Corkill, 1999;
Harnishfeger, 1995; Nigg, 2000). Different models use different terminology but
generally agree on the major conceptual distinctions of inhibitory processes. One
influential classification has been suggested by Harnishfeger and colleagues
(Harnishfeger, 1995; Wilson & Kipp, 1998). Their model is one that will be referred to
in this thesis because it incorporates recent empirical findings, and also because the
distinction it proposes concurs relatively well with the dissociation in performance
between tasks discussed in this thesis.
Harnishfeger and colleagues make a distinction between inhibitory processes that
are automatic (or unintentional) and those that are intentional. Automatic inhibition
occurs when an individual automatically suppresses an item and is unaware that the

Chapter 1
- 21 -
suppression is taking place. By contrast, intentional inhibition occurs when an
individual deliberately suppresses the activation of an item after deciding it is irrelevant.
Whereas automatic inhibition is unconscious, intentional inhibition is effortful,
available to conscious reflection and available for strategic interventions (Nigg, 2000).
Experimental paradigms used to assess automatic inhibition include the inhibition of
return task and Negative Priming (NP), because the inhibitory processes take place
below awareness. Tasks used to assess intentional inhibition include directed forgetting
tasks and antisaccade tasks because the stimulus is consciously and deliberately
inhibited.
In support for the distinction between automatic and intentional processes, Nigg et
al (2002), for instance, showed that participants with Attention Deficit Disorder,
compared to controls, showed an impairment on an antisaccade task but not on a NP
task. This selective impairment suggests that these two processes are supported by
different operating mechanisms. In addition, Amieva, Phillips, Della Sala and Henry
(2004) recently reviewed studies assessing inhibitory functioning in Alzheimer’s
disease, and found that patients with Alzheimer’s disease were particularly affected on
tasks requiring controlled and effortful inhibition processes but that performance on
tasks requiring more automatic inhibition was relatively preserved.
In addition, Harnishfeger (1995) proposed that inhibitory processes should be
categorized according to whether they involve (a) behavioural inhibition, involving the
control of overt behaviour or (b) cognitive inhibition, concerning the control of mental
contents. Tasks of behavioural inhibition tend to involve intentional inhibition
processes, but cognitive tasks of inhibition can be either automatic or intentional.
Friedman and Miyake (2004) have recently provided evidence that behavioural and
cognitive inhibition load on different factors, as assessed by latent-variable analysis.
Finally, any discussion about inhibitory processes is not complete without
mention of the process of interference control. Although the terms are often used
interchangeably in the literature, there is general agreement that interference control
should be separated from other domains of inhibition (e.g. Dempster, 1991, 1993,
1995). Interference control refers primarily to the ability to maintain performance in the
presence of competing and distracting stimuli. One paradigm used to assess
interference control is the Stroop colour-word interference test. The relationship
between interference control and other inhibition constructs is complex because,
although the mechanisms underlying these processes are thought to be different (Stuss
et al, 1999), interference control uses processes of inhibition for resisting interference

Chapter 1
- 22 -
(Dempster, 1995; Joormann, 2004). In addition, Wilson and Kipp (1998) stated that
inhibition and interference control may be controlled by similar neurological substrates.
This thesis comprises investigations of the association between auditory
hallucinations and inhibition. In order to examine whether brain regions commonly
associated with auditory hallucinations are also activated during the process of
inhibition, a short review of the neural processes involved in inhibitory control is now
presented. The neuropsychological literature proposes that inhibitory processes require
some degree of executive control, which is purported to involve the frontal cortices and
their connections (e.g. Bjorklund & Harnishfeger, 1995; Conway & Fthenaki, 2003;
Diaz, Robins & Roberts, 1997; Fuster, 1999; Goldman-Rakic, 1987; Metzler & Parkin,
2000; Rogers, Andres, Grasby, Brooks, Robbins, 2000; Stuss et al, 1999; West, 1996).
Evidence comes from studies that show that damage to brain circuits involving the
prefrontal cortex results in different kinds of inhibition failures in action, cognition,
emotion and personality, such as distractibility, neglect, preservative behaviour,
impulsivity and disinhibition (Dempster, 1993; Fuster, 1999; Goldman Rakic, 1987;
Starkstein & Robinson, 1997). Regions of the prefrontal lobes are thought to provide
inhibitory control for the different domains of inhibition and interference control (Aron,
Robbins & Poldrack, 2004; Konishi et al, 1999; Metzler & Parkin, 2000; West, 1996;
Wyland, Kelley, Macreae, Gordon & Heatherton, 2003). One view suggests that there
are highly localized areas of the frontal lobes, particularly the inferior frontal cortex
alone (which includes the OFC, triangular and opercular regions), which modulate all
types of inhibitory processes (Aron, Robbins & Poldrack, 2004). Another view posits
the involvement of specific frontal regions in different domains of inhibition. Friedman
and Miyake (2004) and West (1996), for instance, have proposed that the OFC region of
the prefrontal cortex may be involved in cognitive inhibition whereas the dorsolateral
prefrontal cortex may be involved in more behavioural inhibitory processes. The
cingulate gyrus has also been associated with a number of “conflict monitoring”
functions on tasks involving response competition, interference control and control of
behaviours (Carter et al, 1998; Dolan, Fletcher, McKenna, Friston & Frith, 1999;
Dreher & Berman, 2002; Wyland et al, 2003). Inhibitory processes have also been
associated with more posterior brain structures (Stuss et al, 1999). For example, the
basal ganglia and its connections with the frontal lobes have been implicated on tasks
requiring set shifting and on motor inhibition tasks (e.g. Nigg, Butler, Huang-Pollock,
Henderson, 2002).

Chapter 1
- 23 -
In sum, the involvement of these brain regions in such a wide range of tasks
reflects an overlap of the functional activations associated with these different measures
of inhibition, making it difficult to identify specific networks associated with domains
of inhibition. In any case, the findings of abnormal activations of the prefrontal cortex,
cingulate gyrus and basal ganglia in auditory hallucinations support the proposal that
inhibition may be impaired in those who suffer from this symptom.
Context memory
The second cognitive domain under investigation in this thesis in relation to
auditory hallucinations is context memory. In episodic memory research, a distinction
is made between content and context information. Content information refers to the
event itself, whereas contextual information refers to details which are encoded with the
event, but which are not part of the event itself. Context refers to information such as
the source (“who”), temporal (“when”) or spatial (“where”) characteristics of the
memory event (Chalfonte & Johnson, 1996). The context of memories are cues that
allow the differentiation of one memory from other memories. Evidence of a distinction
between content and context memory is supported by neuropsychological (Glisky,
Polster & Routhieaux, 1995; Spencer & Raz, 1995; Troyer, Winocur, Craik,
Moscovitch, 1999) and neuropathological evidence (Burgess, Maguire, Spiers &
O’Keefe, 2000; Mayes et al, 2001; Sullivan, Shear, Zipursky, Sagar & Pfefferbaum,
1997). Johnson and colleagues have also proposed that memories require not only the
retention of particular features, but also the cognitive processes for binding the features
together (Chalfonte & Johnson, 1996; Johnson, Hashtroudi & Lindsay, 1993). Binding
processes combine different elements into a complete memory representation and
provide the knowledge that certain features belong together (Chalfonte & Johnson,
1996). Contextual memory and binding processes are intrinsically linked as contextual
memory depends on the binding of each contextual cue to the content of the event and
thus impaired binding ability would result in impaired contextual memory.
Some early theories suggested that contextual information was “tagged” to the
memory event, so that every memory carried labels identifying its origins (where, when,
who etc) (see Johnson, Foley & Leach, 1988, for a review). This view proposed that a
failure to identify the context of memories may occur because tags somehow get lost.
However, Johnson, Foley and Leach (1988) have provided evidence against this
proposal when they showed that when sensory characteristics are held constant in a
memory task, there is confusion about the origins of memory. The authors suggested

Chapter 1
- 24 -
that this argues against the ‘tagging’ theory because tagging would produce equal
discrimination of origin, independently of the qualitative characteristics of the original
encoding. Johnson and colleagues subsequently proposed the most influential theory of
how contextual memory is recalled, with their Source-Monitoring Framework (Johnson,
Hashtroudi & Lindsay, 1993; Johnson, Kounios & Reeder, 1994). Their central claim is
that memory records are evaluated through a decision process performed during
remembering. During this process, the origins of memories are inferred on the basis of
available cues (perceptual details, contextual information, affect, semantic content and
cognitive operations). Retrieval success depends on the quality of information that was
encoded and on the quality of the decision process. Disruption may occur because the
cues are missing, incomplete or ambiguous and/or because the judgment process
responsible for attributing the context to the memory event is incorrect. Johnson,
Hashtroudi and Linsay (1993) have proposed that a loss of qualitative information, such
as contextual details, would make it difficult to identify correctly the origins of mental
events and would result in confusion with other stimuli. This proposal is relevant for
our purpose, because, in this thesis, we will investigate the proposal that patients with
auditory hallucinations have a deficit in context memory that results in difficulties
forming an intact representation of mental events leading to confusion about their
origins (Nayani and David, 1996).
A review of the neural systems involved in context memory also supports the
involvement of context memory processes in auditory hallucinations. Brain regions
involved in content memory have now been fairly well mapped (see reviews by
Fletcher, Frith & Rugg, 1997; Tulving, 2002). The medial temporal lobes,
hippocampus and prefrontal cortex, play a crucial role in memory formation and
retrieval (e.g. Aggleton & Brown; Fletcher, Shallice & Dolan, 1998; Otten & Rugg,
2002). Less information is known about the exact systems implicated in the retrieval of
context. There is evidence that the frontal lobes are associated with source and
temporal context memory. Studies have found that a large amount of variance in source
memory performance can be explained by neuropsychological tests of frontal lobe
function (e.g. Glisky, Polster & Routhieaux, 1995). Difficulties in recalling the source
or temporal order of events is also a prominent feature of patients with frontal lobe
damage (Glisky, Polster & Routhieaux, 1995; Glisky, Rubin & Davidson, 2001;
Sullivan et al, 1997; Stuss, Eskes & Foster, 1994) and of frontal cortex atrophy in
patients with semantic dementia (Simons et al, 2002). Finally, fMRI (Henson, Shallice
& Dolan, 1999; Rugg, Fletcher, Chua & Dolan, 1999), PET (Cabeza et al, 1997) and

Chapter 1
- 25 -
ERP measures (e.g. Johnson, Kounios & Nolde, 1996) have also supported the
involvement of the prefrontal cortex regions in both source and temporal memory. The
temporal lobes have also been associated with source memory (Spencer & Raz, 1995;
Thaiss & Petrides, 2003) and the medial temporal lobes with temporal memory (Mayes
et al, 2001). Although it is still unclear whether there are brain regions specialized for
source and temporal memory, there is increasing evidence that there are distinct and
functionally domain-specific brain systems in memory (e.g. Halbig, Mecklinger,
Schriefers & Friederici, 1998; Spencer & Raz, 1995; Troyer et al, 1999). With regard to
binding of context memory events, it has been proposed that the frontal lobes may be
involved in the integration of multiple independent features of an experience into a
composite memory trace, and that reduced frontal lobe functions result in impoverished
memory traces that lack rich contextual detail (Fuster, 1999; Stuss & Benson, 1989).
Other studies have linked binding to the frontal lobes and to its connections with the
hippocampus and medial temporal system (Chalfonte & Johnson, 1996; Mitchell,
Johnson, Raye & D’Esposito, 2000). In sum, the frontal and temporal lobes have been
implicated in context memory. These regions have also been thought to be important in
auditory hallucinations of schizophrenia, supporting the proposal that context memory
may be compromised in patients with hallucinations.
Aims and organization of this thesis
Predisposition to hallucinations in the normal population
Hallucinatory experiences are thought to occur on a continuum from normal
mental states to those reported by patients with schizophrenia. As a preliminary study,
Chapter 2 presents an investigation into the defining characteristics of factors
underlying predisposition to hallucinations in normal individuals, as measured by the
Launay-Slade Hallucination Scale-Revised (Bentall & Slade, 1985). An overlap in
characteristics between hallucinatory-like experiences in normal individuals and
auditory hallucinations in schizophrenia should highlight factors that are important to
hallucinatory experiences in general.
Intentional inhibition and auditory hallucinations
The results from Chapter 2 show that the experience of intrusive mental events is
a commonly reported characteristic in healthy individuals with a predisposition to
hallucinations. Interestingly, patients with schizophrenia often describe their auditory
hallucinations as intrusive (Nayani & David, 1996a, b). Chapters 3-5 investigate the
Chapter 1
- 26 -
mechanisms that give rise to this previously ignored feature of auditory hallucinations in
schizophrenia.
A failure of inhibition is thought to result in intrusive thoughts, so Chapter 3
investigates whether auditory hallucination severity in schizophrenia is linked to a
deficit in inhibition, and in particular in intentional inhibition. In order to investigate
whether this deficit is specifically associated with the presence of auditory
hallucinations, Chapter 4 compares the performance of patients with and without
auditory hallucinations on a task of intentional inhibition. Chapter 5 uses performance
on the Affective Shifting task (Murphy et al, 1999) to further investigate inhibition
processes and to examine the role of emotional dysfunction in schizophrenia and
auditory hallucinations.
Context memory and auditory hallucinations
The results of Chapter 2 also show that individuals vulnerable to hallucinations
identify experiences that are referred to an external agency. One critical feature of
auditory hallucinations in schizophrenia is that the experience is perceived to originate
from another agency. In order to explain why patients with schizophrenia fail to
identify correctly the origins of this self-generated material, Nayani and David (1996a)
have proposed that patients with auditory hallucinations suffer from disturbance of the
processes that serve to bind the contextual components of memories together. Chapter
6 investigates whether a context memory deficit is present in patients with
schizophrenia using a novel task, the Memory for Context task, in which memory for
events and memory for the source and temporal information about these events could be
tested. Chapter 7 tests Nayani and David’s (1996a) proposal by comparing the
performance of patients with and without auditory hallucinations on the Memory for
Context task.
Auditory hallucinations: a combination of deficits in intentional inhibition and
context memory
Chapter 8 is a theoretical paper which outlines a new cognitive model of auditory
hallucinations in schizophrenia, building upon the results of the previous chapters. This
chapter proposes that a combination of deficits in at least intentional inhibition and
contextual memory is critical to the experience of auditory hallucinations. The failure
in intentional inhibition produces unwanted and uncontrollable mental events which are
not recognized because they have lost the contextual cues that would facilitate
recognition. Evidence is provided to support this proposal.

Chapter 1
- 27 -
Inhibition and context memory in OCD
A critical prediction of the model of auditory hallucinations is that only those with
auditory hallucinations will show the proposed combination of deficits. Chapter 10
tests this hypothesis by investigating whether another clinical group, namely patients
with OCD, also show the combined deficits. OCD patients also experience intrusive
and uncontrollable mental thoughts but, unlike patients with hallucinations, they do not
report a loss of personal agency. Chapter 10 is preceded by Chapter 9, which presents a
review of the pertinent current literature on OCD.
General discussion
Finally, Chapter 11 presents a summary and discussion of the findings reported in
the thesis.
In sum, this thesis aims to provide a new perspective on the nature of the
cognitive deficits underlying auditory hallucinations. The ideas and empirical work
presented provide a departure from the work that had been carried out in recent years.
The main hypothesis that is being investigated is that a combination of deficits
comprising impairments in both intentional inhibition and context memory is essential
for auditory hallucinations to occur.

Chapter 1
- 28 -
References
Aggernaes, A. (1972). The experienced reality of hallucinations and other psychological
phenomena: an empirical analysis.
Aggleton, J. P., & Brown, M. W. (1999). Episodic memory, amnesia, and the
hippocampal-anterior thalamic axis. Behavioral and brain sciences, 22, 425-489.
Ait Bentaleb, L., Beauregard, M., Liddle, P., & Stip, E. (2002). Cerebral activity
associated with auditory verbal hallucinations: a functional magnetic resonance
imaging case study. Journal of Psychiatry and Neuroscience, 27(2), 110-115.
Aleman, A., Böcker, K.B.E., & deHaan, E.H.F. (1999). Disposition towards
hallucination and subjective versus objective vividness of imagery in normal
subjects. Personality and Individual Differences, 27, 707-714.
Aleman, A., Böcker, K. B. E., Hijman, R., de Haan, E. H. F., & Kahn, R. S. (2003).
Cognitive basis of hallucinations in schizophrenia: role of top-down information
processing. Schizophrenia Research, 1926, 1-11.
Aleman, A., Böcker, K. B. E., Hijman, R., Kahn, R. S., & de Haan, E. H. F. (2002).
Hallucinations in schizophrenia: imbalance between imagery and perception?
Schizophrenia Research, 57(2-3), 315-316.
Aleman, A., & de Haan, E. (2000). Nonlanguage cognitive deficits and hallucinations in
schizophrenia. American Journal of Psychiatry, 157(3), 487.
Aleman, A., Hijman, R., de Hann, E. H. F., & Kahn, R. S. (1999). Memory impairment
in schizophrenia: A meta-analysis. The American Journal of Psychiatry, 156(9),
1358-1366.
Allen, P. P., Johns, L. C., Fu, C. H. Y., Broome, M. R., Vythelingum, G. N., &
McGuire, P. K. (2004). Misattribution of external speech in patients with
hallucinations and delusions. Schizophrenia Research,69(2-3), 277-287.
Alpert, M., & Silvers, K. N. (1970). Perceptual characteristics distinguishing auditory
hallucinations in schizophrenia and acute alcoholic psychoses. American Journal
of Psychiatry, 127(3), 298-393.
Amieva, H., Phillips, L. H., Della Sala, S., & Henry, J. D. (2004). Inhibitory functioning
in Alzheimer's disease. Brain, 127, 949-964.
Andreasen, N. C. (2000). Schizophrenia: the fundamental questions. Brain Research
Reviews, 31, 106-112.

Chapter 1
- 29 -
Andreasen, N. C., Paradiso, S., & O'Leary, D. S. (1998). "Cognitive Dysmetria" as an
integrative theory of schizophrenia: a dysfunction in cortical-subcortical-
cerebellar circuitry? Schizophrenia Bulletin, 24(2), 203-218.
Arnold, S. E. (1997). The medial temporal lobe in schizophrenia. The Journal of
Neuropsychiatry and Clinical Neurosciences, 9, 460-470.
Aron, A. R., Robbins, R. W., & Poldrack, R. A. (2004). Inhibition and the right inferior
frontal cortex. Trends in Cognitive Sciences, 8(4), 170-177.
Asaad, G., & Shapiro, B. (1986). Hallucinations: theoretical and clinical overview.
American Journal of Psychiatry, 143(9), 1088-1097.
Bagner, D. M., Melinder, M., & Barch, D. M. (2003). Language comprehension and
working memory language comprehension and working memory deficits in
patients with schizophrenia. Schizophrenia Research, 60(2-3), 299-309.
Baker, C. A., & Morrison, A. P. (1998). Cognitive processes in auditory hallucinations:
attributional biases and metacognition. Psychological Medicine, 28, 1199-1208.
Barrett, T., & Etheridge, J. (1992). Verbal hallucinations in normals, I: People who hear
'voices'. Applied Cognitive Psychology, 6(5), 379-387.
Baxter, R., & Liddle, P. (1998). Neuropsychological deficits associated with
schizophrenic syndromes. Schizophrenia Research, 30(3), 239-249.
Bazin, N., Perruchet, P., Hardy-Bayle, M., & Feline, A. (2000). Context-dependent
information processing in patients with schizophrenia. Schizophrenia Research,
45(1-2), 93-101.
Bentall, R. P. (1990). The illusion of reality: A review and integration of psychological
research on hallucinations. Psychological Bulletin, 107(1), 82-95.
Bentall, R.P. (1997). The syndromes and symptoms of psychosis. Or why you can't play
'twenty questions' with the concept of schizophrenia and hope to win. In R.
Bentall (Ed.), Reconstructing schizophrenia (pp. 23-59). London: Routledge.
Bentall, R. P. (2000). Hallucinatory Experiences. In E. Cadena, S. Lynn, & S. Krippner
(Eds.), Varieties of Anomalous Experience (pp. 85-120). Washington: APA.
Bentall, R. P., Baker, G. A., & Havers, S. (1991). Reality monitoring and psychotic
hallucinations. British Journal of Clinical Psychology, 30, 213-222.
Bentall, R. P., Kaney, S., & Dewey, M. E. (1991). Paranoia and social reasoning: an
attribution theory analysis. British Journal of Clinical Psychology, 30, 13-23.
Bentall, R. P., & Slade, P. D. (1985a). Reliability of a scale measuring disposition
towards hallucination: a brief report. Personality and Individual Differences, 6(4),
527-529.

Chapter 1
- 30 -
Bentall, R. P., & Slade, P. D. (1985b). Reality testing and auditory hallucinations: A
signal detection analysis. British Journal of Clinical Psychology, 24, 159-169.
Birchwood, M., & Chadwick, P. (1997). The omnipotence of voices: testing the validity
of a cognitive model. Psychological Medicine, 27, 1345-1353.
Bjorklund, D., & Harnishfeger, K. (1995). The evolution of inhibition mechanisms and
their role in human cognition. In F. Dempster & C. Brainerd (Eds.), Interference
and Inhibition in Cognition (pp. 141-173). San Diego, London: Academic Press,
Inc.
Blackwood, N. J., Howard, R. J., Bentall, R. P., & Murray, R. M. (2001). Cognitive
neuropsychiatric models of persecutory delusions. American Journal of
Psychiatry, 158(4), 527-539.
Blakemore, S., Smith, J., Steel, R., Johnstone, E., & Frith, C. (2000). The perception of
self-produced sensory stimuli in patients with auditory hallucinations and
passivity experiences: evidence for a breakdown in self-monitoring. Psychological
Medicine, 30, 1131-1139.
Bliss, E., Larson, E., & Nakashima, S. (1983). Auditory hallucinations and
schizophrenia. The Journal of Nervous and Mental Disease, 171(1), 30-33.
Böcker, K. B. E., Hijman, R., Kahn, R. S., & De Haan, E. H. F. (2000). Perception,
mental imagery and reality discrimination in hallucinating and nonhallucinating
schizophrenic patients. British Journal of Clinical Psychology, 39, 397-406.
Brébion, G., Amador, X., David, A., Malaspina, D., Sharif, Z., & Gorman, J. M. (2000).
Positive symptomatology and source-monitoring failure in schizophrenia - an
analysis of symptom specific effects. Psychiatry Research, 95, 119-131.
Brébion, G., Amador, X., Smith, M., Malaspina, D., Sharif, Z., & Gorman, J. (1999).
Opposite links of positive and negative symptomatology with memory errors in
schizophrenia. Psychiatry Research, 88, 15-24.
Brébion, G., Gorman, J. M., Amador, X., Malaspina, D., & Sharif, Z. (2002). Source
monitoring impairments in schizophrenia: characterization and association with
positive and negative symptomatology. Psychiatry Research, 112, 27-39.
Brébion, G., Smith, M., Amador, X., Malaspina, D., & Gorman, J. (1998). Word
recognition, discrimination accuracy and decision bias in schizophrenia:
association with positive symptomatology and depressive symptomatology. The
Journal of Nervous and Mental Disease, 186(10), 604-609.

Chapter 1
- 31 -
Brébion, G., Smith, M., Gorman, J., & Amador, X. (1996). Reality monitoring failure in
schizophrenia: The role of selective attention. Schizophrenia Research, 22, 173-
180.
Brébion, G., Smith, M., Gorman, J., & Amador, X. (1997). Discrimination accuracy and
decision biases in different types of reality monitoring in schizophrenia. The
Journal of Nervous and Mental Disease, 185(4), 247-253.
Burgess, N., Maguire, E., Spiers, H., & O'Keefe, J. (2000). A temporoparietal and
prefrontal network for retrieving the spatial context of lifelike events.
NeuroImage, 14(2), 439-453.
Burglen, F., Marczewski, P., Mitchell, K. J., van der Linden, M., Johnson, M. K.,
Danion, J.-M., & Salame, P. (2004). Impaired performance in a working memory
binding task in patients with schizophrenia. Psychiatry Research, 125, 247-255.
Cabeza, R., Mangels, J., Nyberg, L., Habib, R., Houle, S., McIntosh, A. R., & Tulving,
E. (1997). Brain regions differentially involved in remembering what and when: A
PET study. Neuron, 19, 863-870.
Cahill, C., & Frith, C. (1994). False perceptions or false beliefs? Hallucinations and
delusions in schizophrenia. In A. David & V. Cutting (Eds.), Neuropsychology of
Schizophrenia (Vol. 13, pp. 267-291). Cambridge: Hove, Sussex.
Carter, C. S., Perlsteim, W., Ganguli, R., Brar, J., Mintun, M., & cohen, J. (1998).
Functional hypofrontality and working memory dysfunction in schizophrenia. The
American Journal of Psychiatry, 155(9), 1285-1287.
Carter, D. M., Mackinnon, A., & Copolov, D. L. (1996). Patients' strategies for coping
with auditory hallucinations. The Journal of Nervous and Mental Disease, 184(3),
161-166.
Carter, D. M., Mackinnon, A., Howard, S., Zeegers, T., & Copolov, D. L. (1995). The
development and reliability of the Mental Health Research Institute Unusual
Perceptions Schedule (MUPS): an instrument to record auditory hallucinatory
experience. Schizophrenia Research, 16, 157-165.
Chadwick, P., & Birchwood, M. (1994). The omnipotence of voices - the cognitive
approach to auditory hallucinations. British Journal of Psychiatry, 164, 190-201.
Chalfonte, B. L., & Johnson, M. K. (1996). Feature memory and binding in young and
older adults. Memory and Cognition, 24(4), 403-416.
Clark, J. (1996). Contributions of inhibitory mechanisms to unified theory in
neuroscience and psychology. Brain and Cognition, 30, 127-152.

Chapter 1
- 32 -
Cleghorn, J. M., Franco, S., Szechtman, B., Kaplan, R., Szechtman, H., Brown, G. M.,
Nahmias, C., & Garnett, E. S. (1992). Toward a brain map of auditory
hallucinations. American Journal of Psychiatry, 149(8), 1062-1069.
Close, H., & Garety, P. (1998). Cognitive assessment of voices: further developments in
understanding the emotional impact of voices. British Journal of Clinical
Psychology, 37, 173-188.
Cohen, J. D., & Servan-Schreiber, D. (1992). A neural network model of disturbances in
the processing of context in schizophrenia. Psychiatric Annals, 22(3), 131-136.
Conway, M. A., & Fthenaki, A. (2003). Disruption of inhibitory control of memory
following lesions to the frontal and temporal lobes. Cortex, 39(4-5), 667-686.
Copolov, D. L., Seal, M. L., Maruff, P., Ulusoy, R., Wong, M. T. H., Tochon-Danguy,
H. J., & Egan, G. F. (2003). Cortical activation associated with the experience of
auditory hallucinations and perception of human speech in schizophrenia: a PET
correlation study. Psychiatry Research: Neuroimaging, 122, 139-152.
Copolov, D. L., Trauer, T., & MacKinnon, A. (in press). On the non-significance of
internal versus external auditory hallucinations. Schizophrenia Research.
Crider, A. (1997). Perseveration in schizophrenia. Schizophrenia Bulletin, 23(1), 63-74.
Crow, T. J. (1980). Positive and negative schizophrenic symptoms and the role of
dopamine. British Journal of Psychiatry, 137, 383-386.
David, A. S. (1999). Auditory hallucinations: Phenomenology, neuropsychology and
neuroimaging update. Acta Psychiatr Scand., 99(Suppl 395), 95-104.
David, A. S. (2004). The cognitive neuropsychiatry of auditory verbal hallucinations: an
overview. Cognitive Neuropsychiatry, 9(1/2), 107-123.
David, A. S., & Busatto, G. (1998). The hallucination: a disorder of brain and mind. In
M. A. Ron & A. S. David (Eds.), Disorders of Brain and Mind (pp. 336-362).
Cambridge: Cambridge University Press.
David, A. S., & Halligan, P. W. (2000). Cognitive neuropsychiatry: potential for
progress. The Journal of Neuropsychiatry and Clinical Neurosciences, 12(4), 506-
511.
David, A. S., & Lucas, P. A. (1993). Auditory-verbal hallucinations and the
phonological loop: A cognitive neuropsychological study. British Journal of
Clinical Psychology, 32, 431-441.
David, A. S., Woodruff, P. W. R., Howard, R., Mellers, J. D. C., Brammer, M.,
Bullmore, E., Wright, I., Andrew, C., & Williams, S. (1996). Auditory

Chapter 1
- 33 -
hallucinations inhibit exogenous activation of auditory association cortex.
NeuroReport, 7, 932-936.
Davies, M., Coltheart, M., Langdon, R., & Breen, N. (2001). Monothematic delusions:
Towards a two-factor account. In C. Hoerl (Ed.), On understanding and explaining
schizophrenia: Philosophy, Psychiatry and Psychology .
Davies, M. F., Griffin, M., & Vice, S. (2001). Affective reactions to auditory
hallucinations in psychotic, evangelical and control groups. British Journal of
Clinical Psychology, 40(4), 361-370.
Davies, P., Thomas, P., & Leudar, I. (1999). Dialogical engagement with voices: a
single case study. British Journal of Medical Psychology, 72, 179-187.
Dempster, F. N. (1991). Inhibitory processes: a neglected dimension of intelligence.
Intelligence, 15, 157-173.
Dempster, F. N (1993). Resistance to interference: Developmental changes in a basic
processing mechanism. In M. Howe & R. Pasnak (Eds.), Emerging themes in
cognitive development (Vol. I: Foundations, pp. 3-27). New-York: Springer-
Verlag.
Dempster, F. N. (1995). Interference and inhibition in cognition. In F. Dempster & C.
Brainerd (Eds.), Interference and inhibition in cognition (pp. 4-26). San Diego,
London: Academic Press.
Dempster, F. N & Corkill, A. (1999). Individual differences in susceptibility to
interference and general cognitive ability. Acta Psychologica, 101, 395-416.
Delespaul, P., deVries, M., & van Os, J. (2002). Determinants of occurrence and
recovery from hallucinations in daily life. Society of Psychiatry and Psychiatric
Epidemiology, 37, 97-104.
Dias, R., Robins, A. C., & Roberts, A. C. (1997). Dissociable forms of inhibitory
control within prefrontal cortex with an analog of the Wisconsin Card Sort Test:
Restriction to novel situation and independence from "on line" processing. Journal
of Neuroscience, 17(23).
Dolan, R. J., Fletcher, P. C., McKenna, P., Friston, K. J., & Frith, C. D. (1999).
Abnormal neural intergration related to cognition in schizophrenia. Acta
Psychiatrica Scandinavica, 99(Suppl. 395), 58-67.
Dreher, J.-C., & Berman, K. F. (2002). Fractionating the neural substrate of cognitive
control processes. Proceedings of the National Academy of Sciences of the USA,
99(22), 14595-14600.

Chapter 1
- 34 -
Elliott, R., & Sahakian, B. (1995). The neuropsychology of schizophrenia: Relations
with clinical and neurobiological dimensions. Psychological Medicine, 25, 581-
594.
Elvevag, B., & Goldberg, T. E. (2000). Cognitive impairment in schizophrenia is the
core of the disorder. Critical Reviews in Neurobiology, 14(1), 1-21.
Evans, C. L., McGuire, P. K., & David, A. S. (2000). Is auditory imagery defective in
patients with auditory hallucinations? Psychological Medicine, 30, 137-148.
Falloon, I. R. H., & Talbot, R. E. (1981). Persistent auditory hallucinations: coping
mechanisms and implication for management. Psychological Medicine, 11, 329-
339.
Fletcher, P. C. (1998). The missing link: a failure of fronto-hippocampal integration in
schizophrenia. Nature Neuroscience, 1(4), 266-267.
Fletcher, P. C., Frith, C. D., & Rugg, M. D. (1997). The functional neuroanatomy of
episodic memory. Trends in Neuroscience, 20(5), 217-218.
Fletcher, P.C., McKenna, P. J., Friston, K. J., Frith, C. D., & Dolan, R. J. (1999).
Abnormal cingulate modulation of fronto-temporal connectivity in schizophrenia.
NeuroImage, 9, 337-342.
Fletcher, P.C., Shallice, T., & Dolan, R. (1998). The functional roles of prefrontal
cortex in episodic memory. I. Encoding. Brain, 121, 1239-1248.
Ford, J. M., Mathalon, D. H., Whitfiled, S., Faustman, W. O., & Roth, W. T. (2002).
Reduced communication between frontal and temporal lobes during talking in
schizophrenia. Biological Psychiatry, 51, 485-492.
Franck, N., Rouby, P., Daprati, E., Dalery, J., Mari-Cardine, M., & Georgieff, N.
(2000). Confusion between silent and overt reading in schizophrenia.
Schizophrenia Research, 41, 357-364.
Friedman, N. P., & Miyake, A. (2004). The relations among inhibition and interference
control functions: a latent-variable analysis. Journal of Experimental Psychology:
General, 133(1), 101-135.
Friston, K. J. (1999). Schizophrenia and the disconnection hypothesis. Acta Psychiatrica
Scandinavica, 99(Suppl. 395), 68-79.
Frith, C. (1995). Functional imaging and cognitive abnormalities. The Lancet,
346(8975), 615-620.
Frith, C. (1996). The role of the prefrontal cortex in self-consciousness: the case of
auditory hallucinations. Philosophical Transactions of the Royal Society of
London: B, 351, 1505-1512.

Chapter 1
- 35 -
Frith, C., & Dolan, R. J. (1997). Brain mechanisms associated with top-down processes
in perception. Philosophical Transactions of the Royal Society of London, B, 352,
1221-1230.
Frith, C., & Done, D. (1988). Towards a neuropsychology of schizophrenia. British
Journal of Psychiatry, 153, 437-443.
Fuster, J. M. (1999). Synopsis of function and dysfunction of the frontal lobe. Acta
Psychiatrica Scandinavica, 99 (Suppl. 395), 51-57.
Glisky, E. L., Polster, M. R., & Routhieaux, B. C. (1995). Double dissociation between
item and source memory. Neuropsychology, 9(2), 229-235.
Glisky, R. L., Rubin, S. R., & Davidson, P. S. R. (2001). Source memory in older
adults: an encoding or retrieval problem? Journal of Experimental Psychology:
Learning, Memory and Cognition, 27(5), 1131-1146.
Goldberg, T., Gold, J. M., Coppola, R., & Weinberger, D. R. (1997). Unnatural
practices, unspeakable actions: a study of delayed auditory feedback in
schizophrenia. American Journal of Psychiatry, 154(6), 858-860.
Goldman-Rakic, P. S. (1987). Circuitry of primate prefrontal cortex and regulation of
behavior by representational memory. In A. P. Society. (Ed.), In Plum F (Ed)
Handbook of Physiology: The Nervous System .
Guillem, F., Bicu, M., Pampoulova, T., Hooper, R., Bloom , D., & Wolf, M.-A. e. a.
(2003). The cognitive and anatomico-functional basis of reality distortion in
schizophrenia: a view from memory event-related potentials. Psychiatry Research,
117, 137-158.
Gray, J. A. (1998). Integrating Schizophrenia. Schizophrenia Bulletin, 24(2), 249-266.
Gur, R. C., Moelter, S. T., & Ragland, J. D. (2000). Learning and memory in
schizophrenia. In T. Sharma & P. Harvey (Eds.), Cognition in Schizophrenia:
Impairments, importance and treatment strategies (pp. 73-92). Oxford: Oxford
University Press.
Haddock, G., McCarron, J., Tarrier, N., & Faragher, E. B. (1999). Scales to measure
dimensions of hallucinations and delusions: the psychotic symptom rating scales
(PSYRATS). Psychological Medicine, 29, 879-889.
Haddock, G., Slade, P. D., Prasaad, R., & Bentall, R. P. (1996). Functioning of the
phonological loop in auditory hallucinations. Personality and Individual
Differences, 20(6), 753-760.
Haier, R. J. (1980). The diagnosis of schizophrenia: a review of recent developments.
Schizophrenia Bulletin, 6(3), 417-428.

Chapter 1
- 36 -
Halbig, T. D., Mecklinger, A., Schriefers, H., & Friederici, A. D. (1998). Double
dissociation of processing temporal and spatial information in working memory.
Neuropsychologia, 36(4), 305-311.
Harnishfeger, K. K. (1995). The development of cognitive inhibition: theories,
definitions and research evidence. In F. N. Dempster & C. J. Brainerd (Eds.),
Interference and inhibition in cognition. Chap 6 (pp. 175-205). San Diego:
Academic Press.
Harris, A. W. F., Gordon, L. W., Bahramali, H., & Slewa-Younan, S. (1999). Different
psychopathological models and quantified EEG in schizophrenia. Psychological
Medicine, 29, 1175-1181.
Heinrichs, R. W., & Zakzanis, K. K. (1998). Neurocognitive deficit in schizophrenia: a
quantitative review of the evidence. Neuropsychology, 12(3), 426-445.
Henson, R. N. A., Shallice, T., & Dolan, R. J. (1999). Right prefrontal cortex and
episodic memory retrieval: a functional MRI test of the monitoring hypothesis.
Brain, 122, 1367-1381.
Hoffman, R. E. (1986). Verbal hallucinations and language production processes in
schizophrenia. The Behavioral and Brain Sciences, 9, 503-548.
Hoffman, R. E., Hawkins, K., Gueorguieva, R., Boutros, N., Rachid, F., Carroll, K., &
Krystal, J. (2003). Transcranial magnetic stimulation of left temporparietal cortex
and medication-resistant auditory hallucinations. Archives of General Psychiatry,
60, 49-56.
Hoffman, R. E., & McGlashan, T. H. (1997). Synaptic elimination, neurodevelopment
and the mechanism of hallucinated 'voices' in schizophrenia. American Journal of
Psychiatry, 154, 1683-1689.
Hoffman, R. E., & McGlashan, T. H. (1998). Reduced corticocortical connectivity can
induce speech perception pathology and hallucinated 'voices'. Schizophrenia
Research, 30, 137-141.
Hoffman, R. E., Rapaport, J., Mazure, C., & Quinlan, D. (1999). Selective speech
perception alternations in schizophrenic patients reporting hallucinated voices.
The American Journal of Psychiatry, 156(3), 393-399.
Honig, A., Romme, M. A. J., Ensink, B. J., Escher, S. D., Pennings, M. H. A., &
Devries, M. W. (1998). Auditory Hallucinations: A comparison between patients
and nonpatients. The Journal of Nervous and Mental Disease, 186(10), 646-651.
Hunter, M. D. (2004). Locating voices in space: a perceptual model for auditory
hallucinations. Cognitive Neuropsychiatry, 9(1/2), 93-105.

Chapter 1
- 37 -
Hustig, H. H., & Hafner, R. J. (1990). Persistent auditory hallucinations and their
relationship to delusions and mood. The Journal of Nervous and Mental Disease,
178(4), 264-267.
Jablensky, A. (2000). Epidemiology of schizophrenia: the global burden of disease and
disability. European Archives of Psychiatry and Clinical Neurosciences, 250, 274-
285.
Johns, L. C., Hemsley, D., & Kuipers, E. (2002). A comparison of auditory
hallucinations in a psychiatric and nonpsychiatric group. British Journal of
Clinical Psychology, 41(1), 81-86.
Johns, L. C., & McGuire, P. K. (1999). Verbal self-monitoring and auditory
hallucinations in schizophrenia. The Lancet, 353(9151), 469-470.
Johnson, M., Foley, M.-A., & Leach, K. (1988). The consequences for memory of
imagining in another person's voice. Memory & Cognition, 16(4), 337-342.
Johnson, M., Kounios, J., & Nolde, S. (1996). Electrophysiological brain activity and
memory source monitoring. NeuroReport, 7, 2929-2932.
Johnson, M., Kounios, J., & Reeder, J. A. (1994). Time-course studies of reality
monitoring and recognition. Journal of Experimental Psychology: Learning,
Memory and Cognition, 20(6), 1409-1419.
Johnson, M., Hashtroudi, S., & Lindsay, D. S. (1993). Source Monitoring.
Psychological Bulletin, 114(1), 3-28.
Joormann, J. (2004). Attentional bias in dysphoria: the role of inhibitory processes.
Cognition and Emotion, 18(1), 125-147.
Junginger, J., & Frame, C. L. (1985). Self-report of the frequency and phenomenology
of verbal hallucinations. The Journal of Nervous and Mental Disease, 173(3), 149-
155.
Keefe, R. S. E., Arnold, M. C., Bayen, U. J., & Harvey, P. D. (1999). Source monitoring
deficits in patients with schizophrenia: a multinomial modelling analysis.
Psychological Medicine, 29, 903-914.
Klimidis, S., Stuart, G. W., Minas, H. I., Copolov, D. L., & Singh, B. S. (1993). Positive
and negative symptoms in the psychoses. Reanalysis of published SAPS and
SANS global ratings. Schizophrenia Research, 9, 11-18.
Kok, A. (1999). Varieties of inhibition: manifestations in cognition, event related
potentials and aging. Acta Psychologica, 101, 129-159.

Chapter 1
- 38 -
Konishi, S., Nakajima, K., Uchida, I., Kikyo, H., Kameyama, M., & Miyashita, Y.
(1999). Common inhibitory mechanism in human inferior prefrontal cortex
revealed by event-related functional MRI. Brain, 122(5), 981-991.
Kramer, A., Humphrey, D., Larish, J., Logan, G., & Strager, D. (1994). Aging and
inhibition: Beyond a unitary view of inhibitory processing in attention.
Psychology and Aging, 9(4), 491-512.
Kurachi, M. (2003). Pathogenesis of schizophrenia: Part I. Symptomatology, cognitive
characteristics and brain morphology. Psychiatry and Clinical Neurosciences, 57,
3-8.
Langdon, R., & Coltheart, M. (2000). The cognitive neuropsychology of delusions.
Mind & Language, 15(1), 184-218.
Lawrie, S. M., Buechel, C., Whalley, H. C., Frith, C. D., Friston, K. J., & Johnstone, E.
C. (2002). Reduced frontotemporal functional connectivity in schizophrenia
associated with auditory hallucinations. Biological Psychiatry, 51(12), 1008-1011.
Lehman, A. F. (1996). Quality of life issues and assessment among persons with
schizophrenia. In M. Moscarelli, A. Rupp, & N. Sartorius (Eds.), Handbook of
Mental Health Economics and Health Policy (Vol. 1. Schizophrenia, ). New York:
John Wiley & Sons Ltd.
Lennox, B. R., Bert, S., Park, G., Jones, P. B., & Morris, P. G. (1999). Spatial and
Temporal mapping of neural activity associated with auditory hallucinations. The
Lancet, 353(9153), 644.
Lenzenweger, M. F. (1999). Schizophrenia: refining the phenotype, resolving
endophenotypes. Behaviour Research and Therapy, 37, 281-295.
Leudar, I., Thomas, P., McNally, D., & Glinski, A. (1997). What voices can do with
words: pragmatics of verbal hallucinations. Psychological Medicine, 27, 885-898.
Levitan, C., Ward, P. B., & V, C. S. (1999). Superior temporal gyral volumes and
laterality correlates of auditory hallucinations in schizophrenia. Biological
Psychiatry, 46, 955-962.
Lewis, D., & Anderson, S. (1995). The functional architecture of the prefrontal cortex
and schizophrenia. Psychological Medicine, 25, 887-894.
Liddle, P. F. (1987). Schizophrenic syndromes, cognitive performance and neurological
dysfunction. Psychological Medicine, 17, 49-57.
Liddle, P. F., Friston, K. J., Frith, C. D., Hirsch, S. R., Jones, T., & Frackowiak, R. S.
(1992). Patterns of Cerebral Blood Flow in Schizophrenia. British Journal of
Psychiatry, 160, 179-186.

Chapter 1
- 39 -
Lowe, G. R. (1973). The phenomenology of hallucinations as an aid to differential
diagnosis. British Journal of Psychiatry, 123, 621-633.
Mayes, A., Isaac, C., Holdstock, J., Hunkin, N., Montaldi, D., Downes, J., MacDonald,
C., Cezayirli, E., & Roberts, J. (2001). Memory for single items, word pairs and
temporal order of different kinds in a patient with selective hippocampal lesion.
Cognitive Neuropsychology, 18(2), 97-123.
McCarley, R. W., Shenton, M. E., O'Donnell, B. F., & Nester, P. G. (1993). Uniting
Kraepelin and Bleuler: the psychology of schizophrenia and the biology of
temporal lobe abnormalities. Harvard Review of Psychiatry, 1, 35-56.
McGlashan, T. H. (1998). The profiles of clinical deterioration in schizophrenia. Journal
of Psychiatric Research, 32, 133-141.
McGuire, P., Shah, G., & Murray, R. M. (1993). Increased blood flow in Broca's area
during auditory hallucinations in schizophrenia. The Lancet, 342, 703-706.
McGuire, P. K., Silbersweig, D. A., & Frith, C. D. (1996). Functional neuroanatomy of
verbal self-monitoring. Brain, 119, 907-917.
McGuire, P. K., Silbersweig, D. A., Murray, R. M., David, A. S., Frackowiak, R. S. J.,
& Frith, C. D. (1996). Functional anatomy of inner speech and auditory verbal
imagery. Psychological Medicine, 26, 29-38.
McGuire, P. K., Silbersweig, D. A., Wright, I., Murray, R. M., David, A. S.,
Frackowiak, R. S. J., & Frith, C. D. (1995). Abnormal monitoring of inner speech:
a physiological basis for auditory hallucinations. The Lancet, 346(8975), 596-600.
Metzler, C., & Parkin, A. (2000). Reversed negative priming following frontal lobe
lesions. Neuropsychologia, 38, 363-379.
Mintz, S., & Alpert, M. (1972). Imagery vividness, reality testing and schizophrenic
hallucinations. Journal of Abnormal Psychology, 79(3), 310-316.
Mitchell, K., Johnson, M., Raye, C., & D'Esposito, M. (2000). fMRI evidence of age-
related hippocampal dysfunction in feature binding in working memory.
Cognitive Brain Research, 10, 197-206.
Mojtabai, R. (1999). Duration of illness and structure of symptoms in schizophrenia.
Psychological Medicine, 29, 915-924.
Morrison, A. P. (2001). The interpretation of intrusions in psychosis: an integrative
cognitive approach to hallucinations and delusions. Behavioral and Cognitive
Psychotherapy, 29, 257-276.
Morrison, A. P., & Haddock, G. (1997). Cognitive factors in source monitoring and
auditory hallucinations. Psychological Medicine, 27, 669-679.

Chapter 1
- 40 -
Morrison, A. P., Haddock, G., & Tarrier, N. (1995). Intrusive thoughts and auditory
hallucinations: a cognitive approach. Behavioral and Cognitive Psychotherapy,
23, 265-280.
Mueser, K. T., Bellack, A. A., & Brady, E. U. (1989). Hallucinations in schizophrenia.
Acta Psychiatrica Scandinavica, 82, 26-29.
Murphy, F. C., Sahakian, B. J., Rubinsztein, J. S., Michael, A., Rogers, R. D., Robins,
T. W., & Paykel, E. S. (1999). Emotional bias and inhibitory control processes in
mania and depression. Psychological Medicine, 29, 1307-1321.
Nathaniel-James, D., & Frith, C. (1996). Confabulation in schizophrenia: evidence of a
new form? Psychological Medicine, 26, 391-199.
Nathaniel-James, D. A., Brown, R., & Ron, M. (1996). Memory impairment in
schizophrenia: its relationship to executive function. Schizophrenia Research, 21,
85-96.
Nayani, T., & David, A. (1996a). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & T. R. E. Barnes (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 . New York: John
Wiley & Sons Ltd.
Nayani, T. H., & David, A. S. (1996b). The auditory hallucination: a phenomenological
survey. Psychological Medicine, 26, 177-189.
Nelson, M. D., Saykin, A. J., Flashman, L. A., & Riordan, H. J. (1998). Hippocampal
volume reduction in schizophrenia as assessed by magnetic resonance imaging: a
meta-analytic study. Archives of General Psychiatry, 55(5), 433-440.
Nigg, J. T. (2000). On inhibition/disinhibition in developmental psychopathology:
Views from cognitive and personality psychology and a working inhibition
taxonomy. Psychological Bulletin, 126(2), 220-246.
Nigg, J. T., Butler, K. M., Huang-Pollock, C. L., & Henderson, J. M. (2002). Inhibitory
processes in adults with persistent childhood onset ADHD. Journal of Consulting
and Clinical Psychology, 70(1), 153-157.
Ohayon, M. M. (2000). Prevalence of hallucinations and their pathological associations
in the general population. Psychiatry Research, 97, 153-164.
Otten, L. J., & Rugg, M. D. (2002). The birth of a memory. Trends in Neurosciences,
25(6).
Oulis, P. G., Mavreas, V. G., Mamounas, J. M., & Stefanis, C. N. (1995). Clinical
characteristics of auditory hallucinations. Acta Psychiatrica Scandinavica, 92, 97-
102.
Chapter 1
- 41 -
Pantelis, C., Barnes, T. R. E., Nelson, H. E., Tanner, S., Weatherley, L., Owen, A. M.,
& Robbins, T. W. (1997). Frontal-striatal cognitive deficits in patients with
chronic schizophrenia. Brain, 120, 1823-1843.
Pantelis, C., & Maruff, P. (2002). The cognitive neuropsychiatric approach to
investigating the neurobiology of schizophrenia and other disorders. Journal of
Psychosomatic Research, 53, 655-664.
Penn, D. L., & Mueser, K. T. (1996). Research update on the psychosocial treatment of
schizophrenia. American Journal of Psychiatry, 153, 607-617.
Rankin, P. M., & O'Carroll, P. J. (1995). Reality discrimination, reality monitoring and
disposition towards hallucination. British Journal of Clinical Psychology, 34, 517-
528.
Rector, N. A., & Beck, A. T. (2001). Cognitive Behavioral Therapy for schizophrenia:
An empirical review. The Journal of Nervous and Mental Disease, 189(5), 278-
287.
Rizzo, L., Danion, J.-M., Van der Linden, M., & Grange, D. (1996). Patients with
schizophrenia remember that an event has occured, but not when. British Journal
of Psychiatry, 168, 427-431.
Rogers, R. D., Andrews, T. C., Grasby, P. M., Brooks, D. J., & Robbins, T. W. (2000).
Contrasting cortical and subcortical activations produced by attentional-set
shifting and reversal learning in humans. Journal of Cognitive Neuroscience, 12,
142-162.
Rugg, M., Fletcher, P., Chua, P., & Dolan, R. J. (1999). The role of the prefrontal cortex
in recognition memory and memory for source: an fMRI study. NeuroImage, 10,
520-529.
Sartorius, N., Shapiro, R., & Jablensky, A. (1974). The international pilot study of
schizophrenia. Schizophrenia Bulletin, 11, 21-34.
Schultz, S. K., & Andreasen, N. C. (1999). Schizophrenia. The Lancet, 353(9162),
1425-1430.
Seaton, B. E., Goldstein, G., & Allen, D. N. (2001). Sources of heterogeneity in
schizophrenia: the role of neuropsychological functioning. Neuropsychology
Review, 11(1), 45-73.
Servan-Schreiber, D., Cohen, J., & Steingard, S. (1996). Schizophrenic Deficits in the
processing of context: A test of a theoretical model. Archives of General
Psychiatry, 53(12), 1105-1112.

Chapter 1
- 42 -
Shergill, S., Brammer, M., Williams, S., Murray, R., & McGuire, P. (2000). Mapping
auditory hallucinations in schizophrenia using functional magnetic resonance
imaging. Archives of General Psychiatry, 57(11), 1033-1038.
Shergill, S., Murray, R. M., & McGuire, P. K. (1998). Auditory hallucinations: a review
of psychological treatments. Schizophrenia Research, 32, 137-150.
Silbersweig, D., & Stern, E. (1996). Functional neuroimaging of hallucinations in
schizophrenia: toward an integration of bottom-up and top-down approaches.
Molecular Psychiatry, 1, 367-375.
Silbersweig, D., Stern, E., C, F., et al (1995). A functional neuroanatomy of
hallucinations in schizophrenia. Nature, 378, 176-179.
Simons, J. S., Verfaellie, M., Galton, C. J., Miller, B. L., Hodges, J. R., & Graham, K.
S. (2002). Recollection-based memory in frontotemporal dementia: implications
for theories of long-term memory. Brain, 125(11), 2523-2536.
Slade, P. D., & Bentall, R. P. (1988). Sensory deception: A scientific analysis of
hallucinations. London: Croom Helm.
Spencer, W., & Raz, N. (1995). Differential effects of aging on memory for content and
context: A meta-analysis. Psychology and Aging, 10(4), 527-539.
Spinella, M. (2002). Correlations among behavioral measures of orbitofrontal function.
International Journal of Neuroscience, 112(11), 1359-1369.
Starker, S., & Jolin, A. (1982). Imagery and hallucination in schizophrenic patients. The
Journal of Nervous and Mental Disease, 170(8), 448-451.
Starkstein, S., & Robinson, R. (1997). Mechanism of disinhibition after brain lesions.
The Journal of Nervous and Mental Disease, 185(2), 108-114.
Stephane, M., Barton, S., & Boutros, N. N. (2001). Auditory verbal hallucinations and
dysfunction of the neural substrates of speech. Schizophrenia Research, 50, 61-78.
Stuss, D. T., & Benson, D. F. (1989) The Frontal Lobes.
Stuss, D. T., Eskes, G. A., & Foster, J. K. (1994). Experimental neuropsychological
studies of frontal lobe functions. In F. G. Boller, J (Eds) (Ed.), Handbook of
Neuropsychology (vol 9) .
Stuss, D., Toth, J., Franchi, D., Alexander, M., Tipper, s., & Craig, F. (1999).
Dissociation of attentional processes in patients with focal frontal and posterior
lesions. Neuropsychologia, 37, 1005-1027.
Sullivan, E. V., Shear, P. K., Zipursky, R. B., Sagar, H. J., & Pfefferbaum, A. (1997).
Patterns of content, contextual and working memory impairments in
schizophrenia and nonamnesic alcoholism. Neuropsychology, 11(2), 195-206.

Chapter 1
- 43 -
Takebayashi, H., Takei, N., & Mori, N. (2002). Unilateral auditory hallucinations in
schizophrenia after damage to the right hippocampus. Schizophrenia Research.
Thaiss, L., & Petrides, M. (2003). Source and content memory in patients with a
unilateral frontal cortex or a temporal lobe excision. Brain, 126(5), 1112-1126.
Thomas, P., Bracken, P., & Leudar, I. (2004). Hearing voices: a phenomenological-
hermeneutic approach. Cognitive Neuropsychiatry, 9(1/2), 13-23.
Tollefson, G. D. (1996). Cognitive Function in schizophrenic patients. Journal of
Clinical Psychiatry, 57(suppl 11), 31-39.
Troyer, A., Winocur, G., Craik, F., & Moscovitch, M. (1999). Source memory and
divided attention: reciprocal costs to primary and secondary tasks.
Neuropsychology, 13(4), 467-474.
Tulving, E. (2002). Episodic Memory: from mind to brain. Annual Review of
Psychology, 53, 1-25.
Walsh, E., Harvey, K., White, I., Manley, C., Fraser, J., Stanbridge, S., & Murray, R.
M. (1999). Prevalence and predictors of parasuicide in chronic psychosis. Acta
Psychiatrica Scandinavica, 100(5), 375-382.
Waters, FAV, Badcock, JC & Maybery, MT (2004). An analysis of the main clinical
features of auditory hallucinations in schizophrenia. Unpublished manuscript,
University of Western Australia.
Weinberger, D. R., Aloia, M. S., Goldberg, T. E., & Berman, K. F. (1994). The frontal
lobes and schizophrenia. The Journal of Neuropsychiatry and Clinical
Neurosciences, 6, 419-427.
Weiss, A., & Heckers, S. (1999). Neuroimaging of hallucinations: a review of the
literature. Psychiatry Research: Neuroimaging Section, 92, 61-74.
West, R. L. (1996). An application of Prefrontal Cortex Function theory to cognitive
ageing. Psychological Bulletin, 120(2), 272-292.
Wilson, S. P., & Kipp, K. (1998). The development of efficient inhibition: Evidence
from directed-forgetting tasks. Developmental Review, 18, 86-123.
Wong, A. H. C., & Van Tol, H. H. M. (2003). Schizophrenia: from phenomenology to
neurobiology. Neuroscience and Biobehavioural Reviews, 27, 269-306.
Woodruff, P. W. R., & Murray, R. M. (1994). The aetiology of brain abnormalities in
schizophrenia. In R. Ancill (Ed.), Schizophrenia: Exploring the Spectrum of
Psychosis . New York: John Wiley & Sons Ltd.
Woodruff, P. W. R., Wright, I., Bullmore, E., Brammer, M., Howard, R. J., Williams,
S., Shapleske, J., Rossell, S., David, A. S., McGuire, P. K., & Murray, R. (1997).

Chapter 1
- 44 -
Auditory hallucinations and the temporal cortical response to speech in
schizophrenia: A functional magnetic resonance imaging study. American Journal
of Psychiatry.
Wyland, C. L., Kelley, W. M., Macrae, C. N., Gordon, H. L., & Heatherton, T. F.
(2003). Neural correlates of thought suppression. Neuropsychologia, 41, 1863-
1867.
Young, H. F., Bentall, R. P., Slade, P. D., & Dewey, M. E. (1987). The role of brief
instructions and suggestibility in the elicitation of auditory and visual
hallucinations in normal and psychiatric subjects. The Journal of Nervous and
Mental Disease, 175(1), 41-47.

- 45 -
PREDISPOSITION TO HALLUCINATIONS IN THE NORMAL POPULATION

- 47 -
Foreword to Chapter 2
Experiences akin to auditory hallucinations occur spontaneously, and frequently, in
the normal population. In support, between 10-45% of normal, healthy people experience
some type of auditory hallucination (e.g. Barrett & Etheridge, 1992; Posey & Losch, 1983;
Young et al, 1986). In addition, it is commonly believed that auditory hallucinations in
schizophrenia exist on a continuum with normal mental events (e.g. Bentall & Slade,
1985b; Chapman , Chapman & Raulin, 1976; Chapman, Edell & Chapman, 1980). The
investigation of hallucinatory experiences in nonpsychiatric individuals is a useful research
strategy as it allows the examination of hallucinations without the possible confound
associated with psychopathology.
As a preliminary study of our investigations of auditory hallucinations in
schizophrenia, the defining characteristics of factors underlying predisposition to
hallucinations in normal individuals are investigated in Chapter 2. In particular, the aim
of this study is to examine the factor structure of the Launay-Slade Hallucination Scale
(Launay & Slade, 1981, modified by Bentall & Slade, 1985). Given that processes are
thought to occur on a continuum, an overlap in characteristics between hallucinatory-like
experiences in normal individuals and auditory hallucinations in schizophrenia should draw
attention to factors that are important to the hallucinatory experience in general. It should
be made clear at this point that this chapter is the only study addressing hallucinatory
experiences in healthy individuals.

- 48 -
References
Barrett, T., & Etheridge, J. (1992). Verbal hallucinations in normals, I: People who hear
'voices'. Applied Cognitive Psychology, 6(5), 379-387.
Bentall, R. P., & Slade, P. D. (1985). Reliability of a scale measuring disposition towards
hallucination: a brief report. Personality and Individual Differences, 6(4), 527-529.
Chapman, L. J., Edell, W., & Chapman, J. P. (1980). Physical anhedonia, perceptional
aberration and psychosis proneness. Schizophrenia Bulletin, 6(4), 639-653.
Chapman, L. L., Chapman, J. P., & Raulin, M. L. (1976). Scales for physical and social
anhedonia. Journal of Abnormal Psychology, 85(4), 374-382.
Launay, G., & Slade, P. (1981). The measurement of hallucinatory predisposition in male
and female prisoners. Personality and Individual Differences, 2, 221-234.
Posey, T., & Losch, M. (1983). Auditory hallucinations of hearing voices in 375 normal
subjects. Imagination, Cognition and Personality, 3(2), 99-113.
Young, H. F., Bentall, R. P., Slade, P. D., & Dewey, M. E. (1986). Disposition towards
hallucination, gender and EPQ scores: a brief report. Personality and Individual
Differences, 7(2), 247-249

- 49 -
Chapter 2
Revision of the factor structure of the Launay-Slade Hallucination Scale (LSHS-R) Abstract
The Launay-Slade Hallucination Scale (LSHS-R) (Launay & Slade, 1981, modified
by Bentall & Slade, 1985a) is a frequently used measure of predisposition to hallucinations
in normal individuals. The current study administered the LSHS-R to a large sample of
English-speaking undergraduate students (N = 562). Principal Component Analyses
identified three factors characterised as (1) vivid/intrusive mental events, (2) hallucinations
with a religious theme, and (3) auditory and visual hallucinatory experiences. The first
factor refers to mental events where the experience is recognised as one’s own whereas the
other two factors have in common that the experience is attributed to another source. The
current factor structure is similar to the factors obtained by Levitan, Ward, Catts and
Hemsley (1996) for participants with a psychiatric disorder and a history of auditory
hallucinations, supporting the view that hallucinations exist on a continuum with normal
experiences.
Flavie A.V. Waters, Johanna C. Badcock, Murray T. Maybery (2003). Revision of the
factor structure of the Launay-Slade Hallucination Scale (LSHS-R). Personality and
Individual Differences, 35, 1351-1357.

Chapter 2
- 50 -
The Launay-Slade Hallucination Scale (LSHS-R) (Launay & Slade, 1981, modified
by Bentall & Slade, 1985a) is a scale designed to measure predisposition to hallucinations
in healthy individuals. It was developed on the basis that hallucinatory experiences occur
on a continuum with normal mental states (Launay & Slade, 1981). In support, a
surprisingly large number of individuals in the normal population report a history of
hallucinatory experience. For example, Bentall and Slade (1985a) found that 17.7% of
male undergraduate participants reported that they often heard a voice speaking their
thoughts aloud and 15.4% said that they have had the experience of hearing a person's
voice when no one was present, supporting the idea that hallucinations may occur
spontaneously in the normal population. Although the scale has frequently been utilised in
research as a method for measuring predisposition to auditory hallucinations in healthy
individuals (e.g. Bentall & Slade, 1985b; Feelgood & Rantzen, 1994; Jakes & Hemsley,
1986; Rankin & O'Carroll, 1995), its factor structure has not been well established.
When Launay and Slade (1981) developed the 12-item scale, which required
participants to respond either true or false to each item, a Principal Component Analysis
(PCA) on the scores of 296 participants (200 prisoners, 54 controls and 42 psychiatric
patients with auditory hallucinations) revealed a two-factor solution. The first factor,
characterised as tendency to hallucinatory experience, accounted for 83.1% of the variance
(items 1, 2, 3, 4, 5, 6, 7, 8, 10 and 12 – see Table 1) and the second factor, negative
response set, accounted for 16.9% of the total variance (items 9 and 11).
In 1985, Bentall and Slade modified the questionnaire by changing the two negative
response items (items 9 and 11) to positive ones and replacing the true/false response
format with a 5-point Likert scale. The factor structure of this revised scale, the LSHS-R,
has been studied in a mixed psychiatric population by Levitan, Ward, Catts and Hemsley
(1996). PCA with varimax rotation on the scores of 169 psychiatric patients with a history
of auditory hallucinations yielded four factors accounting for 65.3% of the variance. The
factors were characterised as vivid dreams (items 2, 3, 5, 6 and 9), clinical auditory
hallucinations (items 7, 9, 10, 11 and 12), intrusive or vivid thoughts (items 1, 3, 4 and 12)
and subclinical auditory hallucinations (items 8 and 9).
To date, the structure of the LSHS-R has been investigated only once in the normal
population. Aleman, Nieuwenstein, Böcker and de Haan (2001) administered a Dutch
translation of the scale to 243 undergraduate participants. The PCA analysis yielded a

Chapter 2
- 51 -
three-factor solution characterised by general hallucinatory tendency (items 1, 2, 7, 8, 10
and 12), subjective externality of thought (items 3, 4 and 11) and vividness of daydreams
(items 5, 6 and 12). Item 9 loaded on the first factor according to the PCA with oblique
rotation on the raw data, or on the third factor after the data were transformed.
The aim of the present study was to administer the LSHS-R to a larger sample of
English speaking healthy participants in order to test the stability of its factor structure.
Method
Five hundred and sixty two first-year undergraduate psychology students (176 males
and 386 females) took part in this study. The mean age of participants was 18.79 years (SD
= 4.03).
The participants completed the 12-item LSHS-R version as described by Bentall and
Slade (1985a). Each item was scored "certainly applies to me" (4), "possibly applies to me"
(3), "unsure" (2), "possibly does not apply to me" (1), "certain does not apply to me" (0).
Total scores can range from 0 to 48.
Results
Examination of the histograms, skewness and kurtosis for participants' responses on
each item indicated positively skewed distributions for items 10, 11 and 12, which
replicates the findings by Aleman et al. (2001). A number of outliers were also identified
for these items (defined as scores more than 3 SD above the mean). These were trimmed to
the score 3 SD above the mean (n = 21 for item 10, n = 8 for item 11 and n = 24 for item
12). The trimmed scores were used in all subsequent analyses.
Total scores ranged from 0 to 43 and the mean total score was 17.72 (SD = 7.49)
(with untrimmed scores), or 17.62 (SD = 7.41) (with trimmed scores). Those means are
comparable to the untrimmed means obtained for similar samples of undergraduates by
Bentall and Slade (1985a) (N = 136, M = 19.35, SD = 7.27), Young, Bentall, Slade and
Dewey (1986) (N = 204, M = 17.60, SD = 8.62), and Feelgood and Rantzen (1994) (N =
136, M = 21.9, SD = 8). Aleman et al. (2001) report a somewhat lower mean of 13.9 (SD =
6.7) in their administration of the Dutch translation to 243 students.

Chapter 2
- 52 -
Table 1
Mean scores, standard deviations, and percentages of students endorsing the positive responses for the Launay-Slade
Hallucination Scale (LSHS-R) items (N = 562)
M SD Possibly applies Certainly applies
1. No matter how hard I try to concentrate, unrelated thoughts always creep 2.56 1.14 295 (52.49 %) 96 (17.08 %)
into my mind
2. In my daydreams I can hear the sound of a tune almost as clearly as if 2.54 1.17 221 (39.39 %) 122 (21.74 %)
I were actually listening to it
3. Sometimes my thoughts seem as real as actual events in my life 2.46 1.13 249 (44.38 %) 89 (15.86 %)
4. Sometimes a passing thought will seem so real that it frightens me 1.97 1.25 184 (32.91 %) 54 (9.66 %)
5. The sounds I hear in my daydreams are generally clear and distinct 2.09 1.13 188 (33.51 %) 49 (8.73 %)
6. The people in my daydreams seem so true to life that sometimes I think 1.71 1.23 135 (24.15 %) 41 (7.33 %)
they are
7. I often hear a voice speaking my thoughts aloud 1.51 1.34 116 (20.75 %) 49 (8.76 %)
8. In the past, I have had the experience of hearing a person's voice and then 1.31 1.37 119 (21.25 %) 41 (7.32 %)
found that no-one was there
9. On occasions, I have seen a person's face in front of me when no-one was .71 1.05 48 (8.60 %) 10 (1.79 %)
in fact there
10. I have heard the voice of the Devil .10 .37 9 (1.60 %) 5 (0.88 %)
11. In the past, I have heard the voice of God speaking to me .37 .84 27 (4.82 %) 8 (1.42 %)
12. I have been troubled by hearing voices in my head .26 .66 17 (3.02 %) 7 (1.24 %)

Chapter 2
- 53 -
There was no gender difference in comparing the means for the total scores [t (560) =
.17, p = .85]. Table 1 presents the mean score and the percentage of students endorsing the
positive response sets for each item on the scale.
Scores on all items correlated significantly with total test score (range of Pearson r
values = .26 to .69, p < .001). The factor structure of the 12 variables was initially
examined by PCA. PCA with an oblique rotation (Oblimin with Kaiser normalization) was
carried out as reported in Aleman et al. (2001). A Keiser-Meyer-Olkin statistic of .79
indicated factorability of items. All factors with eigenvalues greater than one were retained
and compared with Cattel's scree plot to determine the number of factors to retain. On this
basis, three factors accounting for 56.2% of the variance were retained. The rotated factor
loadings above .30 for the three-factor solution are shown in Table 2. The first factor,
which accounted for 32.4% of the variance (items 1, 2, 3, 4, 5 and 6) contained items that
refer to vivid/intrusive mental events where the experience is recognised as one's own (‘my
daydreams’, ‘my thoughts’). The second and third factors accounted for 13.9% and 9.8%
of the variance respectively and refer to hallucinations with a religious theme (items 10, 11
and 12) and auditory and visual hallucinatory experiences (items 7, 8, 9 and 12). In
contrast to the first factor, these two latter factors have in common that the experience is
directly attributed to another source (God, the Devil) or attribution of the experience to
another source is implied. The same factor structure was obtained when the outliers were
not trimmed.
Of note, item 12 loaded on both Factor II and Factor III and item 7 loaded on Factor I
and Factor III. All the correlations between factors were significant (p < .001), with r = .10
for Factors I and II, r = -.32 for Factors I and III, and r = -.19 for Factors II and III.
Principal factor analysis was subsequently carried out in order to check the fit of the
PCA. It revealed exactly the same factor loadings as the PCA with the only difference
being that item 1 was no longer identified as carrying any loading on any of the three
factors. In addition, in case the use of the oblique rotation on the PCA was not appropriate
because the factors were in fact independent, PCA with Varimax rotation was carried out.
This analysis identified similar factors as those obtained with PCA with oblique rotation
with the only difference being that Factor III now accounted for more of the variance
(13.8%) than Factor II (9.8%). These analyses suggest that the factors identified with the
PCA were fairly robust and that three separate factors may be identified.

Chapter 2
- 54 -
Table 2
Three-factor Oblimin solution showing item loadings above .30 on the LSHS-R Items Factor I Factor II Factor III
5. The sounds I hear in my daydreams are generally clear and distinct .81
2. In my daydreams I can hear the sound of a tune almost as clearly as if .76
I were actually listening to it
3. Sometimes my thoughts seem as real as actual events in my life .74
6. The people in my daydreams seem so true to life that sometimes I think .65
that they are
4. Sometimes a passing thought will seem so real that it frightens me .63
1. No matter how hard I try to concentrate, unrelated thoughts always creep .32
into my mind
10. I have heard the voice of the Devil .84
11. In the past, I have heard the voice of God speaking to me .79
12. I have been troubled by hearing voices in my head .49 -.48
9. On occasions, I have seen a person's face in front of me when no-one was -.82
in fact there
8. In the past, I have had the experience of hearing a person's voice and then -.81
found that no one was there
7. I often hear a voice speaking my thoughts aloud .36 -.46
Chapter 2
- 55 -
Discussion
The current study aimed to extend our knowledge about the factors underpinning the
LSHS-R in a large sample of English speaking students. A factor analysis identified three
factors accounting for 56.2% of the variance. The first factor was characterised by
intrusive or vivid mental events where the self is nominated as the agent and the experience
is still recognised as one’s own (‘my daydreams'). The second and third factors referred to
hallucinations with a religious theme and to the experience of visual and auditory
hallucinations respectively, where in both cases, the experience is described as being
separate and distinct from the self (‘a voice’, ‘voice of God’). The attribution of the
experience separates Factor I from Factors II and III and suggests that this may reflect
different facets of the hallucinatory experience. All the items represented in each of the
three factors appear to be appropriately characterised by the factor labels. An important
argument for the validity of this solution is that repeated factor analyses with different
rotations yielded practically identical solutions.
The contents of the present three-factor solution have little in common with the three
factors previously obtained by Aleman et al. (2001). The reasons for this discrepancy are
not clear although, of particular note, their total mean score was lower than that reported in
previous studies suggesting that their Dutch translation of the scale may be somewhat
different from the original English version. The current results are actually closer to
Levitan et al.'s (1996) factor structure for psychiatric participants with a history of auditory
hallucinations: Factors II and III in the current analysis contain the same items as in Factors
II (clinical auditory hallucinations) and IV (sub-clinical hallucinations) of Levitan et al's
(1996) analysis, suggesting that both analyses may be tapping into similar hallucinatory
processes in different populations. The similarity between Levitan's and the current study
firmly supports the view that hallucinations exist on a continuum with normal experiences.
However, only a small percentage of normal participants in the present study endorsed
items with a religious theme. Yet, misattribution of the hallucinatory experiences to
supernatural forces is a common phenomenon in psychiatric patients with a history of
hallucinations (Nayani & David, 1996). This suggests that a delusional interpretation of the
hallucinatory phenomenon may differentiate the experience of healthy participants from
that of psychiatric patients. In order to identify whether this factor is critical in
differentiating psychiatric patients and healthy participants, future research should obtain

Chapter 2
- 56 -
detailed item endorsement frequencies in a psychiatric sample for comparison with the
current ratings on healthy participants.
What is the relationship between predisposition to hallucinations and schizotypy?
Like schizophrenia, schizotypy is a multi-dimensional construct, of which hallucinatory-
like experiences form a dimension (Venables & Rector, 2000). Falling within the positive
cluster (Bentall, Claridge & Slade, 1989), predisposition to hallucinations does not imply
predisposition to schizotypy in general. Given increasing evidence that hallucinations have
a distinctive cognitive basis in schizophrenia (e.g. Waters, Badcock, Maybery & Michie,
2003) predisposition to hallucinatory experience in schizotypy and in healthy individuals
may share a unique aetiology.
Finally, the experience of auditory hallucinations in schizophrenia is frequently
described as intrusive and vivid - the mechanisms underlying the intrusiveness have been
linked to deficits in inhibition (Waters et al, 2003). The first factor in the current analysis
of the LSHS-R suggests that vivid and perhaps intrusive mental events may also be part of
the predisposition to hallucinations in healthy individuals. In addition, the current results
also draw attention to an important distinction between intrusive experiences which are
recognised as belonging to the self and other intrusive experiences which are misattributed.
The attribution of internal mental events to another source is a characteristic feature of
auditory hallucinations in psychopathology, and in particular schizophrenia. The current
results are particularly interesting in view of evidence that show that participants scoring
high on the LSHS-R misattribute internal events to an external source (Bentall & Slade,
1985b, Jakes & Hemsley, 1986, Rankin & O'Carroll, 1995), a deficit commonly attributed
to hallucinating patients with schizophrenia. Our results suggest that a cognitive deficit in
source attribution may be present only in those individuals scoring high on items 7-12 of
the LSHS-R. Further research is needed to investigate this prediction and to attempt to
replicate the current factor structure of the LSHS-R.

Chapter 2
- 57 -
References
Aleman, A., Nieuwenstein, M. R., Böcker, K. B. E., & De Haan, E. H. F. (2001). Multi-
dimensionality of hallucinatory predisposition: factor structure of the Launay-Slade
Hallucination Scale in a normal sample. Personality and Individual Differences, 30,
287-292.
Bentall, R. P., Claridge, G. S., & Slade, P. D. (1989). The multidimensional nature of
schizotypal traits: a factor analytic study with normal subjects. British Journal of
Clinical Psychology, 28, 363-375.
Bentall, R. P., & Slade, P. D. (1985a). Reality testing and auditory hallucinations: A signal
detection analysis. British Journal of Clinical Psychology, 24, 159-169.
Bentall, R. P., & Slade, P. D. (1985b). Reliability of a scale measuring disposition towards
hallucination: a brief report. Personality and Individual Differences, 6(4), 527-529.
Feelgood, S. R., & Rantzen, A. J. (1994). Auditory and visual hallucinations in university
students. Personality and Individual Differences, 17(2), 293-296.
Jakes, S., & Hemsley, D. R. (1986). Individual differences in reaction to brief exposure to
unpatterned visual stimulation. Personality and Individual Differences, 7(1), 121-123.
Launay, G., & Slade, P. (1981). The measurement of hallucinatory predisposition in male
and female prisoners. Personality and Individual Differences, 2, 221-234.
Levitan, C., Ward, P. B., Catts, S. V., & Hemsley, D. R. (1996). Predisposition toward
auditory hallucinations: the utility of the Launay-Slade Hallucination Scale in
psychiatric patients. Personality and Individual Differences, 21(2), 287-289.
Nayani, T. H., & David, A. S. (1996). The auditory hallucination: a phenomenological
survey. Psychological Medicine, 26, 177-189.
Rankin, P. M., & O'Carroll, P. J. (1995). Reality discrimination, reality monitoring and
disposition towards hallucination. British Journal of Clinical Psychology, 34, 517-
528.
Venables, P. H., & Rector, N. A. (2000). The content and structure of schizotypy: A study
using confirmatory factor analysis. Schizophrenia Bulletin, 26(3), 587-602.
Waters, F. A. V., Badcock, J. C., Maybery, M. T., & Michie, P. T. (2003). Inhibition in
schizophrenia: association with auditory hallucinations. Schizophrenia Research, 62,
275-280.

Chapter 2
- 58 -
Young, H. F., Bentall, R. P., Slade, P. D., & Dewey, M. E. (1986). Disposition towards
hallucination, gender and EPQ scores: a brief report. Personality and Individual
Differences, 7(2), 247-249.

- 59 -
INTENTIONAL INHIBITION AND
AUDITORY HALLUCINATIONS

- 61 -
Foreword to Chapters 3, 4 and 5
The previous chapter has revealed that one of the factors underpinning predisposition
to hallucinations in the normal population is characterised as the experience of intrusive
mental events. Interestingly, intrusiveness is one of the defining features of auditory
hallucinations in schizophrenia. This characteristic is so common in patients with
schizophrenia that modern definitions include the observation that auditory hallucinations
are not amenable to voluntary control (e.g. David, 2004). However, this characteristic has
mostly been ignored in current cognitive theories of auditory hallucinations and little is
known about the mechanisms that give rise to this particular feature of the hallucinatory
experience in schizophrenia.
The process of inhibition is essential for suppressing unwanted and irrelevant
thoughts. Consequently, the following three chapters investigate the proposal that auditory
hallucinations in schizophrenia are associated with a failure in cognitive inhibition, and in
particular a deficit in intentional inhibition.
Chapter 3 investigates whether the severity of auditory hallucinations is associated
with increasingly impaired control of intentional inhibition as measured on the Hayling
Sentence Completion Test (Burgess & Shallice, 1996) and the Inhibition of Currently
Irrelevant Memories Task (ICIM) (Schnider & Ptak, 1999).
Chapter 4 extends these findings by presenting group comparisons between patients
with and without hallucinations on the ICIM task. For the purpose of this paper only, the
presence of auditory hallucinations is determined using a strict PANSS criterion (a score of
1 means that auditory hallucinations have been totally absent in the past four weeks and
scores 2-7 mean that auditory hallucinations have been present during this time), in order to
answer a specific question regarding the nature of the cognitive deficits in patients with a
total absence of auditory hallucinations in the past four weeks.
Chapter 5 presents an analysis of performance on the Affective Shifting Task
(Murphy et al, 1999) in patients with schizophrenia (with and without auditory
hallucinations) to further investigate inhibition processes and to examine the role of
emotional dysfunction in schizophrenia and auditory hallucinations. In this, and all
subsequent chapters, the presence of auditory hallucinations is categorized according to
whether patients have had auditory hallucinations on more than half of the days during the

- 62 -
past 4 weeks. As explained earlier, this criterion was chosen so that patients with very
infrequent hallucinations were not classified as having auditory hallucinations present.
References
Burgess, P., & Shallice, T. (1996). Response suppression, initiation and strategy use
following frontal lobe lesions. Neuropsychologia, 34(4), 263-273.
David, A. S. (2004). The cognitive neuropsychiatry of auditory verbal hallucinations: an
overview. Cognitive Neuropsychiatry, 9(1/2), 107-123.
Murphy, F. C., Sahakian, B. J., Rubinsztein, J. S., Michael, A., Rogers, R. D., Robins, T.
W., & Paykel, E. S. (1999). Emotional bias and inhibitory control processes in mania
and depression. Psychological Medicine, 29, 1307-1321.
Schnider, A., & Ptak, R. (1999). Spontaneous confabulators fail to suppress currently
irrelevant memory traces. Nature Neuroscience, 2(7), 677-681.

- 63 -
Chapter 3
Inhibition in schizophrenia: association with auditory hallucinations
Abstract
The study investigates whether auditory hallucinations (AH) in schizophrenia are
linked to a deficit in inhibition. Two tasks assessing the intentional suppression of
cognitive events - the Hayling Sentence Completion Test (HSCT) (Burgess & Shallice,
1996) and the Inhibition of Currently Irrelevant Memories Task (ICIM) (Schnider & Ptak,
1999) - were administered to 42 patients with schizophrenia and 24 normal controls.
Presence and severity of symptoms in the patient group were examined using the Positive
and Negative Syndrome Scale (PANSS). Patients performed significantly worse on the
measures of inhibition compared to controls. More importantly, among patients, significant
positive correlations were obtained between an index of AH severity (defined as an
increase in frequency of AH on PANSS) and the number of type A errors on the HSCT and
errors in the last three runs of the ICIM. An increase in AH severity was, therefore,
associated with increasingly impaired control of intentional inhibition. Furthermore, no
significant correlations were found between these indices of inhibition and either negative,
general or positive symptoms (excluding AH scores).
Waters, F.A.V., Badcock, J.C., Maybery, M.T. & Michie, P.T. (2003). Inhibition in
schizophrenia: Association with auditory hallucinations. Schizophrenia Research. 62, 275-
280.
Chapter 3
- 64 -
Similarities between auditory hallucinations (AH) and unwanted intrusive thoughts
have increasingly been noted and several theories implicate the involvement of intrusive
cognition in AH (e.g. Nayani & David, 1996a; Morrison, 2001). Intrusive thoughts have
been linked to a deficit in inhibition in disorders such as Obsessive-Compulsive Disorder
(e.g. Enright & Beech, 1993) and Post-Traumatic Stress Disorder (e.g. Vasterling et al,
1998). There is considerable experimental evidence that schizophrenia is linked to a deficit
in inhibition (e.g. Beech et al, 1989; Brebion et al, 1996) and Frith (1979) also suggested an
association between AH and inhibition. However, the few studies that have investigated
the role of inhibitory processes in AH have failed to demonstrate any such role using
negative priming (Peters et al, 2000) and interference (Brebion et al, 1998) tasks. One of
the reasons why these studies may have failed to find a deficit in inhibition in AH may be
because of the type of inhibitory processes measured by those tasks. Recently, a conceptual
distinction has been made between automatic and intentional forms of inhibition (Kipp
Harnishfeger, 1995). Automatic inhibition occurs below awareness whereas with
intentional inhibition the individual consciously suppresses the activation of an item.
Negative priming and interference control are not categorized as intentional forms of
inhibition so the failure of previous studies to establish a relationship between AH and
inhibition may be because it is a deficit in intentional inhibition that is critical to AH. Since
AH are consciously experienced mental events, it is reasonable to argue that they may
reflect an impairment in intentional inhibition processes.
Given the uncertainly surrounding the role of inhibitory processes in AH, we
examined the link between AH and task performance on relatively new tests thought to
reflect intentional inhibition processes. The Hayling Sentence Completion Test (HSCT)
(Burgess & Shallice, 1996) is a task that requires the ability to voluntarily suppress
currently active mental representations. Patients with schizophrenia have been found to
make more errors than controls on this task (Nathaniel-James & Frith, 1996) however the
study failed to address the relationship between HSCT performance and individual
symptoms. The Inhibition of Currently Irrelevant Memories task (ICIM) (Schnider & Ptak,
1999) measures the ability to suppress memory traces that are not relevant to ongoing
reality. Some theories have suggested that AH may in fact be memories that are not
recognized (e.g. Nayani & David, 1996a), consequently this task was chosen as an index of
whether AH are also linked to a problem in regulating memories. Both tasks assess the

Chapter 3
- 65 -
intentional suppression of conscious cognitive events and the performance of each has been
found to be mediated by the frontal lobes (Nathaniel-James et al, 1997; Schnider et al,
2000). However, they also differ in that the HSCT measures the ability to inhibit currently
active mental events while the ICIM measures the ability to suppress irrelevant memories.
Morrison and Baker (2000) also implicated the role of negative mood in the
maintenance process of AH and predicted that an increase in negative mood should
correlate with an increase in frequency of AH. Therefore, the BDI-II (Beck, 1996) and BAI
(Beck, 1990) were included as measures of depression and anxiety levels respectively.
Method
Participants
Forty-two patients with a DSM-IV diagnosis of schizophrenia were selected from a
psychiatric hospital in Perth, Western Australia. Information concerning the patients’
demographic and clinical data is presented in Table 1. All patients were receiving typical,
atypical or a combination of neuroleptics. A control group comprised 24 individuals
recruited from the community. Exclusionary criteria for all participants included a history
of head injury and neurological illness. Controls who reported a personal or first-degree
family history of psychiatric illness were also excluded. The patients and controls did not
differ in premorbid IQ as measured with the National Adult Reading Test (NART, Nelson,
1982), handedness, gender or educational level (see Table 1). The study was approved by
UWA and Graylands Hospital Ethics Committees and signed informed consent was
obtained from all participants.
Clinical ratings
Patients were interviewed using the Positive And Negative Syndrome Scale (PANSS)
(Kay, Opler & Fiszbein, 1987). The PANSS measures both the presence and severity of
Positive (which include AH together with delusions, etc.), Negative (e.g. blunted affect)
and General symptoms (e.g. somatic concerns) on a 7-point scale. AH severity was rated
from the PANSS with higher ratings signalling an increase in AH frequency. The symptom
composition of the patient group is described in Table 1.

Chapter 3
- 66 -
Table 1
Demographic and clinical data for patients with schizophrenia and healthy control
participants (means and standard deviations)
Controls (n = 24) Patients (n = 42) Group
Comparisons p
Age 34.67 (8.81) 36.73 (8.41) t = .95 .34
Gender 20 M, 4 F 35 M, 7 F X2 =.00 .63
Handedness 19 R, 4 L 35 R, 6 L X2 = .25 .88
Years Education 11.75 (1.89) 10.97 (1.97) t = 1.55 .12
NART 103.62 (4.75) 100.21 (9.32) t = 1.66 .10
Age of first hospitalisation - 23.09 (5.80)
Number of admissions - 9.35 (7.79)
Duration of illness (years) - 13.64 (8.14)
Level of positive symptoms1 - 19.19 (5.12)
Level of negative symptoms1 - 12.33 (3.22)
Level of general symptoms1 - 28.85 (5.47)
AH severity1 - 2.95 (2.05)
Chlorpromazine equivalent - 942.78 (445.35) 1 on PANSS
Tasks and questionnaires
Digits Forward (Digit Span subtest, WAIS-III, Wechsler, 1997)
This simple measure of memory span (maximum score of 14) was used as a general
measure of cognitive function.
The Beck Depression Inventory (BDI-II) and Beck Anxiety Inventory (BAI) (Beck, 1996,
1990, respectively)
These tests both have a maximum score of 21.
Hayling Sentence Completion Test (HSCT) (Burgess & Shallice, 1996)
In this test the participant is required to provide single-word completions to
sentences. In the critical inhibition condition, each completion should be unrelated to the
preceding sentence. Two errors types were recorded: A category A error was where the

Chapter 3
- 67 -
supplied word completed the sentence in a plausible fashion (e.g. 'most cats see very well
at...night'), and a category B error was where the response was semantically connected to
the sentence, but was not the most plausible completion (e.g. 'the dough was put in the
hot…kitchen').
Inhibition of Currently Irrelevant Memories (ICIM) (adapted from Schnider & Ptak, 1999)
This task involves the presentation of a series of animal pictures (selected from the
Berkeley Digital Library Project collection) for repeated identification. Four runs were
shown of the same basic set of 52 pictures. Four pictures were repeated 8 times within each
run as described by Schnider and Ptak. These target items were different for the 4 runs.
The pictures were presented for 2000 ms each with an inter-stimulus interval of 1000 ms.
Immediately after the 1st run, the 2nd run was presented. A 3rd run was made 5 minutes after
the 2nd run, and the 4th run was made after a 30-minute delay. For the first run, participants
were told that pictures of animals would be presented and that some would be shown more
than once. The task was to identify which pictures were repeated. For each subsequent run,
participants were instructed to forget that they had already seen the pictures and to indicate
picture reoccurrences only within that run. Performance on the first run depended on new
learning, whereas subsequent runs required active inhibition of memory of pictures seen in
the previous runs (Schnider et al, 2000). Consequently the number of false alarms (FA) in
the last three runs, but not the first, was used to index inability to inhibit irrelevant
memories.
Results
Comparisons of patients and controls
Table 2 shows mean scores and standard deviations on all measures. Parametric and
non-parametric tests revealed no differences in outcomes, so parametric tests are reported
in Table 2. Compared to controls, the patient group had significantly lower spans as
measured by the Digits Forward subtest, and had higher levels of depression and anxiety.
On the HSCT, one-way ANOVAs showed that the patient group made more type A and
type B errors compared to controls. For the ICIM task, one-way ANOVAs showed that
patients did not differ from controls in the number of FA on the first run but made more FA
than controls on the three subsequent runs combined. There were no sex differences for
any experimental measures (p > .25).

Chapter 3
- 68 -
Table 2
Means and standard deviations on Digits Forward, BDI-II, BAI, HSCT (number of Type A
and B errors) and ICIM (number of FA for run 1 and 2-4 combined) for controls and
patients
Controls Patients Group
M SD M SD Comparisons p
Forward Span 8.79 1.61 6.90 1.67 t = 4.30 <.001
BDI-II 2.04 1.98 12.95 12.90 F = 16.79 <.001
BAI 1.54 1.79 9.63 9.33 F = 17.53 <.001
HSCT Type A Errors .12 .44 1.30 2.20 F = 6.73 .01
HSCT Type B Errors 2.75 3.22 6.19 3.12 F = 18.10 <.001
ICIM FA (1) .50 .72 2.04 4.10 F = 3.56 .06
ICIM FA (2-4) 3.66 5.28 12.35 16.45 F = 6.28 .01
Correlations with AH severity in the patient group
Digits Forward, BDI-II and BAI scores were not found to be significantly correlated
with AH severity (p > .09). Table 3 reports the correlation coefficients between AH
severity and experimental measures. Spearman Rho correlation coefficients were used
when the distributional assumptions of Pearson correlation coefficients were not met.
On the HSCT, analyses revealed a significant correlation between the number of type
A errors and AH severity suggesting that an increase in frequency of hallucinations was
associated with an increase in failure to inhibit salient and active mental representations.
Type B errors were not found to be correlated with AH severity, demonstrating that an
increase in frequency of AH was selectively associated with an increasing failure to inhibit
the most salient and prepotent responses as measured by type A errors.

Chapter 3
- 69 -
Table 3
Correlations of HSCT (Type A and B errors) and ICIM (FA on run 1 and runs 2-4
combined) with AH severity, Negative, General, Positive and Positive without AH symptom
groups
HSCT HSCT ICIM ICIM
Errors A Errors B FA 1 FA 2-4
AH severity .41** -.04 .02 .42**
Negative Symptoms -.09 .26 -.11 .09
General Symptoms -.19 .08 .01 .09
Positive Symptoms .35* .02 -.11 .35*
Positive Symptoms .26 .06 -.15 .28
without AH
** Significant at the .01 level, * Significant at the .05 level
On the ICIM task, correlations of AH severity with the number of FA responses
revealed no significant relationship for the first run but a significant correlation for the three
subsequent runs combined. The first run consists in identifying picture reoccurrence within
that run, whereas in each of the three subsequent runs, participants need to inhibit the
memory of pictures that had been seen in the previous runs. Therefore FA in the last three
runs, and not the first, represents a failure to inhibit past memory traces. The correlation
between type A errors (HSCT) and FA on runs 2-4 (ICIM) was not significant (rho = .21, p
= .44).
Association of cognitive variables with severity of other symptom groups
In order to test the specificity of the link between inhibitory failure and AH severity,
the correlations above were recomputed utilizing the positive, negative and general
symptom groups scores from the PANSS (see Table 3). No significant correlations were
obtained between any of the inhibition measures and either negative or general symptoms.
Severity of positive symptoms correlated with Type A errors (HSCT), and FA on runs 2-4
(ICIM). However when AH ratings were subtracted from the broader set of positive
symptom ratings, these correlations were no longer significant. This suggests that an
increase in inhibitory failure on these tasks was specifically related to an increase in the
symptoms severity of AH in schizophrenia.

Chapter 3
- 70 -
Effects of antipsychotic medication
The only significant correlation with chlorpromazine dosage equivalents was with
type B errors (HSCT), rho = .36, p = .02. The correlation between AH severity and type B
errors was repeated using chlorpromazine dosage as a covariate and the correlation
remained non significant, r = -.27, p = .10.
Discussion
The current study aimed to clarify the role of inhibition in the experience of AH in
schizophrenia with two new measures targeted at intentional inhibition. Firstly, the results
show that patients with schizophrenia exhibited deficits on all measures of inhibition. This
is consistent with previous findings indicating that schizophrenia is linked to a deficit in
inhibiting irrelevant and distracting stimuli (e.g. Nathaniel-James & Frith, 1996).
Secondly, AH severity was linked to a failure in intentional inhibition. An increase in AH
was associated with an increasing inability to inhibit both currently active mental
associations and memory traces that were no longer relevant - these processes were not
significantly correlated with each other suggesting that they measure different aspects of
inhibition. Furthermore, AH severity was not found to be associated with a decrease in
general cognitive functioning or an initial ability to discriminate targets from distractors
(number of FA in the first run of the ICIM), suggesting that AH frequency was not related
to a widespread cognitive impairment.
Furthermore, impaired intentional inhibition was significantly correlated with AH
severity but was not associated with other positive, general or negative symptoms,
highlighting the utility of a symptoms-based approach in the investigation of cognitive
deficits in schizophrenia. There was also no evidence to support the view that an increase
in negative mood is correlated with an increase in frequency of AH suggesting that,
contrary to Morrison and Baker's (2000) proposal, negative mood may not be directly
implicated in the maintenance of AH.
Altogether, the results clearly implicate the role of an inhibitory impairment in AH.
As both the HSCT and ICIM tasks assess the effortful and conscious suppression of
cognitive contents, the current study was able to identify a deficit in intentional inhibition
associated with AH of schizophrenia. The results further demonstrated that an increase in
AH severity was associated with an increasing difficulty in controlling the contents of

Chapter 3
- 71 -
active mental events and past memory traces. To our knowledge, this is the first
unequivocal demonstration of an association between a failure of inhibition and AH. The
process of inhibition is essential for suppressing irrelevant thoughts and a failure of
inhibition results in information that intrudes into ongoing thinking. This notion of
intrusion is particularly relevant to AH in schizophrenia as patients describe their
hallucinations as disturbing, unbidden and uncontrollable (Nayani & David, 1996b). We
believe that the failure to inhibit current associations and representations in memories is, at
least in part, the cause of the intrusive nature of the hallucinatory experience.
Acknowledgements The authors wish to thank A. T. Beck for his support, David Castle for his helpful
advice, Danny Rock for his invaluable help in recruiting patients and Berkeley Digital
Library Project for permission to use their pictures.

Chapter 3
- 72 -
References
Beck, A. (1990). BAI: The Psychological Corporation.
Beck, A. (1996). BDI-II. San Antonio: The Psychological Corporation.
Beech, A., Powell, T., McWilliam, J., & Claridge, G. (1989). Evidence of reduced
'cognitive inhibition' in schizophrenia. British Journal of Clinical Psychology, 28,
109-116.
Brebion, G., Smith, M., Gorman, J., & Amador, X. (1996). Reality monitoring failure in
schizophrenia: The role of selective attention. Schizophrenia Research, 22, 173-180.
Brebion, G., Smith, M., Gorman, J., Malaspina, D., & Amador, X. (1998). Resistance to
interference and positive symptomatology in schizophrenia. Cognitive
Neuropsychiatry, 3, 179-190.
Burgess, P., & Shallice, T. (1996). Response suppression, initiation and strategy use
following frontal lobe lesions. Neuropsychologia, 34(4), 263-273.
Enright, S. J., & Beech, A. R. (1993). Reduced cognitive inhibition in obsessive-
compulsive disorder. British Jouranl of Clinical Psychology, 32, 67-74.
Frith, C. D. (1979). Consciousness, information processing and schizophrenia. British
Journal of Psychiatry, 134, 225-235.
Kay, S. R., Fiszbein, A., & Opler, L. A. (1987). The Positive and Negative Syndrome Scale
(PANSS) for Schizophrenia. Schizophrenia Bulletin, 13, 261-276.
Kipp Harnishfeger, K. (1995). The development of cognitive inhibition: theories,
definitions and research evidence. In F. N. Dempster & C. J. Brainerd (Eds.),
Interference and inhibition in cognition. Chap 6 (pp. 175-205). San Diego: Academic
Press.
Kramer, A., Humphrey, D., Larish, J., Logan, G., & Strager, D. (1994). Aging and
inhibition: Beyond a unitary view of inhibitory processing in attention. Psychology
and Aging, 9(4), 491-512.
Morrison, A. (2001). The interpretation of intrusions in psychosis: an integrative cognitive
approach to hallucinations and delusions. Behavioural and Cognitive Psychotherapy,
29, 257-276.
Morrison, A. P., & Baker, C. A. (2000). Intrusive thoughts and auditory hallucinations: a
comparative study of intrusions in psychosis. Behaviour Research and Therapy, 38,
1097-1106.

Chapter 3
- 73 -
Nathaniel-James, D., & Frith, C. (1996). Confabulation in schizophrenia: evidence of a new
form? Psychological Medicine, 26, 391-199.
Nathaniel-James, D. A., Fletcher, P., & Frith, C. (1997). The functional anatomy of verbal
initiation and suppression using the Hayling Test. Neuropsychologia, 35(4), 559-566.
Nayani, T., & David, A. (1996a). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & B. T. R. E (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 : John Wiley & Sons
Ltd.
Nayani, T. H., & David, A. S. (1996b). The auditory hallucination: a phenomenological
survey. Psychological Medicine, 26, 177-189.
Nelson, H. E. (1982). The National Adult Reading Test (NART): Test Manual. Windsor,
Berks: NFER-Nelson.
Peters, E. R., Pickering, A., Kent, A., Glasper, A., Irani, M., David, A., Day, S., &
Hemsley, D. (2000). The relationship between cognitive inhibition and psychotic
symptoms. Journal of Abnormal Psychology, 109(3), 386-395.
Schnider, A., & Ptak, R. (1999). Spontaneous confabulators fail to suppress currently
irrelevant memory traces. Nature Neuroscience, 2(7), 677-681.
Schnider, A., Treyer, V., & Buck, A. (2000). Selection of currently relevant memories by
the human posterior medial orbital cortex. The Journal of Neuroscience, 20(15),
5880-5884.
Vasterling, J., Brailey, K., Constans, J., & Sutker, P. (1998). Attention and memory
dysfunction in post-traumatic stress disorder. Neuropsychology, 1998(12), 1, 125-
133.
Wechsler, D. (1997). Wechsler Adult Intelligence Scale-III (WAIS-III) . New York: The
Psychological Corporation.

- 75 –
Chapter 4
Auditory hallucinations: failure to inhibit irrelevant memories Abstract
Auditory hallucinations are the most common symptom of schizophrenia. The
frequency of auditory hallucinations is significantly associated with the failure to inhibit
memory traces that are no longer relevant (Waters, Badcock, Maybery & Michie, 2003).
We extend these findings by comparing the performance on a repeated continuous
recognition task1 of two subgroups of schizophrenia patients: (1) patients with auditory
hallucinations present and (2) patients with auditory hallucinations absent (including a
small sample with no history of auditory hallucinations). The results show that patients
with current auditory hallucinations make significantly more inappropriate responses
(false alarms) to distracters seen on previous runs of the task than non-hallucinating
patients. Consistent with our predictions, the presence of auditory hallucinations
involves a failure to suppress memories that are not relevant to ongoing reality. The
results could not simply be explained as being due to impaired encoding in memory
since hallucinators and non-hallucinators did not differ significantly in the number of
correctly identified targets (hits) across repeated runs. An alternative to the “inner
speech” model is proposed which suggests that auditory hallucinations arise from a
combination of deficits in inhibition and (episodic) memory.
Badcock, JC, Waters, FAV, Maybery, MT. (in press) Auditory Hallucinations: failure to
inhibit irrelevant memories, Cognitive Neuropsychiatry.
1refered to as the ICIM task (Inhibition of Currently Irrelevant Memories Task, Schnider &
Ptak, 1999) in previous and subsequent chapters.

Chapter 4
- 76 –
Current cognitive theories propose that auditory hallucinations (AH) are based on
inner speech that is misattributed to an external source (Frith & Done, 1989; Frith,
1992; David, 1994; Evans, McGuire & David, 2000). Recent neural imaging of verbal
hallucinations points to activations in inferior frontal cortex, anterior cingulate,
temporal cortex and hippocampal/parahippocampal cortex, regions involved in the
processing of inner speech but also prominently involved in inhibition and memory,
consistent with disturbed connectivity in fronto-temporal cortical circuits (Shergill et
al., 2000).
We have previously employed a repeated continuous recognition task to examine
the cognitive processes underlying AH (Waters, Badcock, Maybery & Michie, 2003).
This task, adapted from Schnider and Ptak (1999), involves the presentation of a
sequence of meaningful pictures, one at a time, from which the participant must detect
those pictures that are repeated (targets) within a single run. Targets from one run
become distracters on subsequent runs. The number of false positive responses to these
distracters (false alarms) reflects the ability to suppress memories that are no longer
relevant. Furthermore, the increase in false-alarms is assumed to depend on the interval
between runs (which determines the level of activation of memory traces). A marked
increase in false alarms on this task has been shown to be closely associated with
lesions in orbitofrontal cortex (Schnider & Ptak, 1999; Schnider et al., 2000a,b).
Our research with this task in AH demonstrated that the number of false alarms,
reflecting impaired intentional suppression, was positively associated with the
frequency of AH but not with other positive symptoms (Waters et al., 2003). These
findings suggest that AH are related to a failure to inhibit memory traces that are no
longer relevant to ongoing reality. In other words, it seems that AH arise as a result of
the intrusion of strongly activated representations previously acquired in memory. Since
Waters et al. (2003) adopted a correlational approach it might still be argued that this
impairment in inhibitory control is a general feature of schizophrenia rather than
specifically associated with the presence of AH (Beck & Rector, 2003). A stronger test
of the contribution of the suppression of irrelevant memories to the experience of
hallucinations would be provided by comparing the performance of schizophrenia
patients both with and without AH. Therefore, the aim of this report is to extend these
findings using the repeated continuous recognition task by contrasting the performance
of schizophrenia patients who are (a) currently hallucinating (AH present within the last
4 weeks) and (b) not currently hallucinating (AH absent over the last 4 weeks), and (c)
healthy controls. We predict that patients with no current evidence of AH will not

Chapter 4
- 77 –
display an increase in the number of false alarms across repeated runs of the task
compared with healthy controls, whilst patients with current AH will do so.
Furthermore we examine the ability to correctly identify targets in repeated runs in
order to determine whether the results can be explained in terms of impaired encoding
in memory.
Method
The study protocol was approved by the human research ethics committee of the
University of Western Australia and the institutional ethics committee at Graylands
Hospital. All participants provided signed informed consent prior to their participation
in the study.
Participants
Twenty three patients with a DSM-IV diagnosis of schizophrenia who were
currently experiencing auditory hallucinations (Current AH) together with 20 patients
who had not experienced auditory hallucinations within the last four weeks (Non AH)
were selected from a large psychiatric hospital in Perth, Western Australia. The latter
group included four patients whose clinical interview and case histories, indicated that
they had never experienced auditory hallucinations (Never AH). Information concerning
patient demographic and clinical characteristics is presented in Table 1. All patients
were receiving typical, atypical or a combination of antipsychotic medications. The
control group comprised 24 healthy individuals recruited from the community.
Exclusionary criteria for all participants included a history of head injury and
neurological illness. Healthy controls who reported a personal or first-degree family
history of major psychiatric illness were also excluded.
Clinical ratings
Patients were interviewed using the Positive and Negative Syndrome Scale
(PANSS) (Kay, Opler & Fiszbein, 1987). The PANSS measures both the presence and
severity of Positive (which include AH together with delusions, etc.), Negative (e.g.
blunted affect) and General (e.g. somatic concerns) symptoms on a 7-point scale. AH
severity was rated from the PANSS, with higher ratings signalling an increase in AH
frequency. All patients in the Non-AH subgroup had a rating of 1 on AH severity,
indicating that the symptom was absent (see Table 1). In addition, current level of
depression was assessed using the Beck Depression Inventory (BDI-II; Beck, 1996).

Chapter 4
- 78 –
Table 1
Demographic and clinical characteristics (means and S.D.) of controls and patients
with (Current AH) and without (Non AH) current auditory hallucinations
Controls
(n = 24)
Current AH
(n = 23)
Non AH
(n = 20)
Age
(range)
34.7 (8.7)
20-54
34.1 (8.9)
19-54
39.15 (7.3)
24-50
Education 11.75 (1.89) 10.82 (2.06) 11.25 (1.88)
NART 103.6 (4.75) 96.26 (8.40) 105.4 (8.19)
AH severity (PANSS)
(range)
-- 4.56 (1.38)
2-6
1 (0)
--
No. of Admissions -- 10.35 (9.85) 7.8 (4.29)
Duration of illness -- 11.30 (7.38) 15.7 (8.79)
Cognitive assessment
Inhibition of Currently Irrelevant Memories (ICIM)
An adapted version of the continuous recognition task previously described by
Schnider and Ptak (1999) was used. This task consisted of four runs of a continuous
recognition task for meaningful stimuli (animal pictures selected from the Berkeley
Digital Library Project collection with their permission); some of which were repeated.
In each run, 80 pictures were presented, drawn from the same basic set of 52 pictures.
Four pictures recurred throughout each run (7 times following the initial presentation)
yielding 28 targets. The remaining pictures were not repeated (52 distracters). Target
pictures were different for the 4 runs. The pictures were presented using PowerPoint for
approximately 2000 ms each with an inter-stimulus interval of 1000 ms. Immediately
after the 1st run, the 2nd run was presented. A 3rd run was presented 5 minutes after the
2nd run, and the 4th run after a 30-minute delay. For the first run, participants were told
that pictures of animals would be presented and that some of these pictures would be
shown more than once. The participants’ task was to identify which pictures were
repeated. For each subsequent run, participants were instructed to forget that they had
already seen the pictures and to indicate picture re-occurrences only within that run.
Performance on the first run, therefore, depends on new learning, whereas in the

Chapter 4
- 79 –
subsequent runs participants were required to actively inhibit the memory of pictures
that had been seen in the previous runs (Schnider et al, 1996). Both the number of hits
(correct detection of recurring pictures) and the number of false alarms (FA: incorrectly
selecting a distracter) were examined. False alarms for the last three runs were of
particular interest since they would reflect any failure to inhibit memories of target
pictures from previous runs, however, false alarms were also examined for the first run,
since they reflected influences on recognition judgments other than the failure to inhibit
memories of target pictures.
Assessment of general intelligence
Premorbid intelligence was estimated using the National Adult Reading Test-
revised (Nelson & Willison, 1991).
Results
Preliminary analyses of the distributions of the continuous recognition data
indicated that the assumptions of multivariate analyses were not met, hence non-
parametric analyses were performed. One way analysis of variance indicated that the
three participant groups did not differ significantly in age, F(2,66) = 2.27, p = 0.11, or
education, F (2,66) = 1.32, p = 0.27, but did differ in estimated premorbid intelligence,
F (2,66) = 9.96, p < 0.001. The Current AH patients had significantly lower NART
scores than both the Non AH patients (Bonferroni adjusted probability, p < 0.001) and
the healthy controls (Bonferroni adjusted probability, p = 0.003). Comparisons between
the two patient subgroups showed that they did not differ significantly in terms of the
duration of illness, F (1, 41) = 3.17, p = 0.08, number of admissions, F (1,41) = 1.14, p
= 0.29, or level of depression, Mann-Whitney U = 214.5, p = 0.91. Whilst the Current
AH patients, by definition, exhibited more positive symptoms (hallucinations) than the
Non AH patients (see Table 1), analysis of the remaining PANSS scores showed that
the two patient groups did not differ in the average score for Negative symptoms, Mann
Whitney U = 183.5, p = 0.25, or General symptoms, Mann Whitney U = 219.0, p =
0.78.
Analysis of target hits
The ability to correctly detect targets on the ICIM task was assessed by analysing
the number of hits for repeated targets across the four runs of the task. There was a
significant difference in the average number of hits made by the current AH (M = 26.8,
SEM = 0.21), Non AH (M = 26.74, SEM = 0.33) and healthy control (M = 27.54, SEM =

Chapter 4
- 80 –
0.13) groups, Kruskal-Wallis chi-square = 6.99, df = 2, p = 0.03. Follow-up
comparisons showed that healthy controls produced significantly more hits than the
current AH group, Mann-Whitney U = 158.0, p = 0.01, and also the Non AH group,
Mann-Whitney U = 161.5, p = 0.05. However, the two patient subgroups did not differ
in the average number of hits made, Mann-Whitney U = 216.00, p = 0.73. Spearman
correlation coefficients were calculated in order to examine the relationship between
NART scores and hit rates. No correlation approached significance with alpha set at
0.05.
Analysis of false alarms
The number of false alarms made on the first run of the ICIM task reflects new
learning, rather than suppression. The number of false alarms on run 1 did not differ
significantly between the three groups, Kruskal-Wallis chi-square = 2.37, df = 2, p =
0.30. In contrast the number of false alarms made on subsequent runs (i.e. runs 2-4)
differed significantly between the groups, Kruskal-Wallis chi-square = 13.25, df = 2, p =
0.001. Follow-up comparison between group pairs showed that the current AH patients
made significantly more false alarms than healthy controls, Mann-Whitney U = 111.5, p
< 0.001. The Non AH patients made significantly fewer false alarms than the current
AH group, Mann-Whitney U = 139.5, p = 0.02, and were not significantly different
from healthy controls, Mann-Whitney U = 180.00, p = 0.15. This pattern of results is
shown in Figure 1. In order to check whether the results for the Non AH patients were
unusual due to the inclusion of the 4 patients (Never AH) with no history of AH, the
entire analysis was repeated with these patients excluded. The average performance of
this subgroup alone is shown in Figure 1. The overall pattern of results was unchanged
in this analysis (data not shown). Spearman correlations were used to examine the
relationship between NART scores and false alarms (FA 2-4) within each group. All
correlations were low and non-significant (Current AH rs = 0.09, p = 0.66; Non AH rs =
-0.30, p = 0.18; Healthy controls rs = -0.32, p = 0.12).
Since the increase in FA scores is assumed to depend on the interval between
runs, the number of false alarms was compared between the 3rd and 4th run within the
Current AH subgroup in order to examine whether performance changed following the
30 minute delay (during which the activation level of memory traces is assumed to
decrease). Results from a paired sample t-test showed that the number of FA was
significantly lower following this delay, t(22) = 2.53, p = 0.01.

Chapter 4
- 81 –
Figure 1
Mean number of false alarms (+/- 1 SEM) on each run of the ICIM task in the Current
AH ( solid lines), Non AH ( dotted lines), Never AH (▲dashed lines) schizophrenia
patients and Healthy Controls ( solid lines). (Note: the Never AH subgroup are shown
separately for references purposes only. Analyses were based on comparisons with the
larger Non AH group which includes these cases)
Finally, a critical additional analysis was also conducted on the number of false
alarms to distracters that had been targets in previous runs. These specific false alarms
were significantly greater in Current AH, but not Non AH, patients compared to healthy
controls, Mann Whitney U = 92, p = 0.01.
Discussion
The results of this investigation confirm that patients with auditory hallucinations
fail to suppress recently activated memory traces (Waters et al., 2003). In contrast, when
auditory hallucinations are absent the ability to inhibit such memory traces is not
0
1
2
3
4
5
6
7
8
1 2 3 4Run
Mea
n nu
mbe
r of f
alse
ala
rms

Chapter 4
- 82 –
significantly different from that of healthy controls. This inhibitory impairment is not,
therefore, a general feature of schizophrenia (Beck & Rector, 2003). These findings
indicate a subtle interplay between inhibition and (episodic) memory in the genesis of
auditory hallucinations. Thus, in patients currently experiencing hallucinations failure to
inhibit memories of prior events allows old memories to intrude into current events (the
“now”) and become confused with ongoing reality.
Several alternative explanations of why hallucinators fail to suppress responses to
irrelevant memory associations may be ruled out by the current data. First it may be
argued that patients who are actively hallucinating are generally more unwell than
patients who are not currently experiencing hallucinations. However, comparison of a
range of clinical indicators including duration of illness, number of admissions, negative
and general (somatic) symptoms and current level of depression revealed no significant
differences between the two patient subgroups, arguing against a significant role of
these variables. Similarly, prior research suggests that older adults show increased
impairment on a range of measures of inhibition (Persad et al., 2002), however, the
Current AH patients were not significantly older than the Non AH group.
The number of hits made on the continuous recognition task was lower in all
schizophrenia patients than in healthy controls. However, this difference in the ability to
encode new targets cannot account for the tendency of patients with hallucinations to
respond to distracters since the number of hits was not significantly different between
patients with and without hallucinations. Similarly the results do not seem to be due to
an overall bias to respond ‘yes’ in the Current AH group since there was no significant
difference between the three participant groups in the number of false alarms on the first
run. Rather the failure to suppress irrelevant memory traces was evident only as
distracters became more familiar (more strongly activated) with repeated presentation.
Failure to suppress currently irrelevant memories has previously been described in
patients with spontaneous confabulations with lesions consistently involving the
orbitofrontal cortex (Schnider et al, 1996; Ptak & Schnider, 1999; Schnider & Ptak,
1999; Schnider et al, 2000a), pointing to a possible role of this region in the occurrence
of auditory hallucinations. However, detailed comparisons of the data also suggest some
significant differences, suggesting that the underlying mechanisms are not identical.
Most notably, the overall rate of false alarm errors made by confabulators increased
markedly from run to run, even though runs were separated by delays of up to 1 hour. In
contrast, the current findings are suggestive of more transitory effects, in this version of
the task, in patients with auditory hallucinations. This is because suppression ability was

Chapter 4
- 83 –
significantly better following the 30-minute delay, during which time the level of
activation of memory representations is assumed to decrease.
The current findings may also indicate that the capacity to suppress irrelevant
memories varies over time in conjunction with the presence or absence of auditory
hallucinations; a finding that has also been observed to parallel the course of
spontaneous confabulations (Schnider et al, 2000b). A limitation of the current study
lies in the between groups nature of the design, which precludes a direct test of this
interpretation. A possible exception to this proposal may exist in patients who never
experience auditory hallucinations. The capacity of this group to suppress irrelevant
memories appears to be all but indistinguishable from that of healthy controls (see
Figure 1). Again, however, the small sample size available in this study is a limitation
of the current research.
Auditory hallucinations are commonly defined as false perceptions in the absence
of external stimulation and with a compelling sense of reality (Gelder et al 1993). The
intersection between perception and memory, however, is well documented (Jacoby,
1983; Roediger 1996; Goldinger et al 1999) including the similarity of underlying
neural networks (Damasio; 1989; Fuster, 1995; Singer, 1998). Based on the current
findings, therefore, auditory hallucinations might best be viewed as another example of
the ‘sins’ of memory (Schacter, 1999). Whilst the strength of activation of memory
traces in this research is experimentally manipulated by means of repeated presentation
of stimuli, the mechanism which induces activation of memory episodes in
schizophrenia is still unknown.
At least two important implications arise from this research. First, electro-
physiological evidence reveals that suppression of memories that are not currently
relevant is distinct from, and occurs much earlier than, processes engaged in monitoring
the source or veridicality of memories (Schnider et al, 2002). This may explain the
compelling sense of reality, and omnipotence, of hallucinatory experiences (Chadwick
& Birchwood, 1995), since they comprise the intrusion of highly familiar information
(from memory) for which specific contextual details have not been recollected.
Second, the presence of auditory hallucinations involves the failure to suppress
memories of previously encountered events. This mechanism may, therefore, also
explain at least two features of auditory hallucination in schizophrenia that are not
accommodated well (if at all) by current cognitive models based on “inner speech”: (1)
the richness of voice features which are reported, including varieties of grammatical
form, tone, dialect etc., and (2) the less frequent, but persistent report of auditory

Chapter 4
- 84 –
hallucinations involving environmental noises rather than voices (Nayani and David,
1996). Recent research, for example, suggests that episodic memory retains traces of
both voice characteristics and words (Goldinger, 1996), which might account for the
complex qualitative features of auditory hallucinations. In sum, we propose that an
alternative model of auditory hallucinations, which involves a combination of deficits in
inhibition and episodic memory, more accurately describes the nature of the cognitive
deficits underpinning this symptom.
Acknowledgements
The research reported in this article was conducted as part of the doctoral studies of one
of the authors (F.A.V. Waters) at the University of Western Australia.

Chapter 4
- 85 –
References
Beck, A.T. and Rector, N.A. 2003. A cognitive model of hallucinations. Cognit. Ther.
Res. 27, 19-52.
Beck, A.T., Steer, R.A., Ball, R. and Ranieri, W.F., 1996. Comparison of Beck
Depression Inventories-IA and -II in psychiatric outpatients. J. Pers. Assess.
67(3), 588-597.
Chadwick, P. and Birchwood, M., 1997. The omnipotence of voices II: The beliefs
about voices questionnaire (BAVQ). Br. J. Psychiatry. 166, 773-776.
David, A.S., 1994. The Neuropsychological Origin of Auditory Hallucinations. In:
Code, C and Müller, D. (Series Eds.), Brain Damage, Behaviour and Cognition:
A.S. David and J.C. Cutting (Eds), The Neuropsychology of Schizophrenia.
Lawrence Erlbaum Associates, Hove (UK), pp. 269-313.
Damasio, A. R., 1989. Time-locked multiregional retroactivation: a systems-level
proposal for the neural substrates of recall and recognition. Cognition. 33, 25-62.
Evans, C.L., McGuire, P.K. and David, A.S., 2000. Is auditory imagery defective in
patients with auditory hallucinations? Psychol. Med. 30, 137-148.
Frith, C.D., 1992. The Cognitive Neuropsychology of Schizophrenia. Lawrence
Erlbaum Associates, Hove (UK).
Frith, C.D. and Done, J.D., 1989. Experiences of alien control in schizophrenia reflect a
disorder in the central monitoring of action. Psychol. Med. Vol 19(2), 359-363.
Fuster, J.M., 1995. Memory in the Cerebral Cortex. MIT Press, Cambridge, MA.
Gelder, M., Gath, D. and Mayou, R.1993. Oxford textbook of psychiatry (2nd
edition). Oxford University Press, Oxford.
Jacoby, L.L., 1983. Perceptual enhancement: persistent effects of an experience. J. Exp.
Psychol.: Learn. Mem. Cogn. 9, 21-38.
Kay, S.R., Fiszbein, A. and Opler L.A., 1987. The positive and negative syndrome scale
(PANSS) for schizophrenia Schizophr. Bull. 13(2):261-76.
Goldinger, S.D., 1996. Words and voices: episodic traces in spoken word identification
and recognition memory. J. Exp. Psychol.: Learn. Mem. Cogn. 22(5):1166-83.
Goldinger, S.D., Kleider, H.M., Shelley, E., 1999. The marriage of perception and
memory: creating two-way illusions with words and voices. Mem.Cognit.
27(2):328-38.
Nelson, H. and Willison, J. 1991. National Adult Reading Test – Revised: Test Manual.
NFER-Nelson, Windsor.

Chapter 4
- 86 –
Nayani, T.H. and David, A.S., 1996. The auditory hallucination: a phenomenological
survey. Psychol. Med. 26(1):177-89.
Persad, C.C., Abeles, N., Zachs, R. and Denburg, N.L. 2002. Inhibitory changes after
age 60 and their relationship to measures of attention and memory. J. Gerontol. B.
Psychol. Sci. Soc. Sci., 57, 223-232.
Roediger, H.L., III, 1996. Memory illusions. J. Memory Lang. 35, 76-100.
Schnider, A., Treyer, V. and Buck, A., 2000. Selection of currently relevant memories
by the human posterior medial orbitofrontal cortex. J. Neurosci. 20(15):5880-4.
Schnider, A. and Ptak, R., 1999. Spontaneous confabulators fail to suppress currently
irrelevant memory traces. Nat. Neurosci. 2(7), 677-81.
Schnider, A., Valenza, N., Morand, S. and Michel, C.M., 2002. Early cortical
distinction between memories that pertain to ongoing reality and memories that
don't. Cereb. Cortex. 12(1), 54-61.
Schnider, A., von Daniken, C. and Gutbrod, K., 1996. The mechanisms of spontaneous
and provoked confabulations. Brain. 119, 1365-75.
Schnider, A., Treyer, V. and Buck, A. 2000a. Selection of currently relevant memories
by the human posterior medial orbitofrontal cortex. J. Neurosci. 20, 5880-5884.
Schnider, A., Ptak, R., von Däniken, C. and Remonda, L., 2000b. Recovery from
spontaneous confabulations parallels recovery of temporal confusion in memory.
Neurol. 55, 74-83.
Schacter, D.L. 1999. The seven sins of memory. Insights from psychology and
cognitive neuroscience. Am. Psychol. 54(3), 182-203.
Shergill, S.S., Brammer, M.J., Williams, S.C., Murray, R.M. and McGuire, P.K., 2000.
Mapping auditory hallucinations in schizophrenia using functional magnetic
resonance imaging. Arch. Gen. Psychiatry. 57(11), 1033-8.
Singer, W. 1998. Consciousness and the structure of neuronal representations. Philos.
Trans. R. Soc. Lond., B, Biol. Sci. 353, 1829-1840.
Waters, F.A.V., Badcock, J.C., Maybery, M.T. and Michie, P.T., 2003. Inhibition in
schizophrenia: association with auditory hallucinations. Schizophr. Res., 62, 275-
280.
- 87 -
Chapter 5
Inhibitory and affective processes in schizophrenia and auditory hallucinations
Abstract
The current study examines, firstly, intentional inhibition performance on a measure
of task shifting in patients with schizophrenia (with and without auditory hallucinations).
In contrast to our predictions, the results show that (a) patients with schizophrenia do not
show a task-shifting deficit compared to healthy controls and (b) a subgroup of patients
with hallucinations do not show an impairment on task shifting abilities compared to
patients without hallucinations. However, the results do show that the severity of auditory
hallucinations is associated with an increase in overall false alarms, confirming prior
findings of a failure to suppress previously relevant but currently inappropriate stimuli (e.g.
Badcock et al, in press; Waters et al, 2003). Secondly, the study investigates the role of
emotional dysfunction in patients with schizophrenia and those with auditory hallucinations
specifically. The results confirm that depression and anxiety are associated with
schizophrenia, but also that emotional dysfunction is not a necessary feature of the illness.
An attentional inhibitory bias for negative information is found in depressed patients with
schizophrenia, but not in patients who showed no sign of depression. Similarly, the results
show that (a) approximately one third of patients with auditory hallucinations have high
levels of depression and anxiety, thus, negative affect is not specifically associated with
auditory hallucinations; (b) depression in patients with auditory hallucinations is associated
with an attentional bias for negative material; finally it was also found that affective voice
content and beliefs about voices are linked to levels of depression but negative voice
content and beliefs about malevolence and/or omnipotence are not always associated with
negative affect.

Chapter 5
- 88 -
Inhibitory processes
The first aim of this study is to investigate inhibitory processes in patients with
schizophrenia and, in particular, in a subgroup of patients with auditory hallucinations.
Inhibition in schizophrenia
There is considerable experimental evidence across a range of paradigms that shows
that schizophrenia is associated with poor inhibitory functioning in the form of: (a)
intentional inhibition, as shown by deficits on the Hayling Sentence Completion Test
(HSCT, Nathaniel-James, Brown & Ron, 1996; Nathaniel-James & Frith, 1996; Waters,
Badcock, Maybery & Michie, 2003), on antisaccade tasks (Maruff, Danckert, Pantellis &
Currie, 1998; Ross et al, 1998; Schwartz & Evans, 1999) and on motor tasks (Badcock,
Michie, Johnson & Combrinck, 2002; Kopp & Rist, 1994); (b) automatic inhibition as
demonstrated by reduced or reversed negative priming effects (Beech, Powell, McWilliam
& Claridge, 1989; Laplante, Everett & Thomas, 1992), and (c) interference control as
evidenced by increased interference on studies involving the Stroop color/word interference
task (Boucart, Mobarek, Cuervo & Danion, 1999; Brebion, Smith, Gorman & Amador,
1996).
The current study investigates task-shifting abilities in patients with schizophrenia.
Task-shifting involves “moving flexibly from one behavior to another in response to
changing environmental contingencies” (Manoach et al, 2002, p. 816). Task-shifting is
usually thought to require inhibition of attention or responding from a previously reinforced
target and resolving this inhibition in order to reengage in a newly reinforced stimulus
(Arbuthnott & Frank, 2000; Dreher & Berman, 2002). Task-shifting can be argued to
involve primarily intentional inhibition processes on the basis that it is deliberately
invoked, goal-directed, effortful and available to conscious reflection and strategic
interventions (Nigg, 2000; Wilson & Kipp, 1998).
Whereas some studies have found that schizophrenia patients have impaired task-
shifting abilities, mostly on the Wisconsin Card Sorting Test (WCST) (see Crider, 1997, for
a review; Elliott, McKenna, Robbins & Sahakian, 1995), others have failed to find such a
deficit, often using the same task (e.g. Manoach et al, 2002). The reason for this
discrepancy is not clear although methodological differences have been put forward as an
explanation for differences in findings (Manoach et al, 2002). Based on our own findings
which link deficits in intentional inhibition to auditory hallucinations, variation in the

Chapter 5
- 89 -
symptom profile of patients may also have contributed to the differences in outcome of
previous studies. It is important to assess task-shifting abilities in patients with
schizophrenia because preserved task-shifting abilities appear to be inconsistent with
reports of impaired performance on other tasks of intentional inhibition (e.g. Nathaniel-
James & Frith, 1996; Ross et al, 1998; Waters et al, 2003). If task shifting involves
intentional inhibition processes then it is expected that patients with schizophrenia should
be impaired on this measure of inhibition. Consequently, the current study aims to
reexamine the task-shifting abilities of patients with schizophrenia using a novel Affective
Shifting Task originally developed by Murphy et al (1999) to assess inhibitory control in
mania and depression.
In the Affective Shifting Task, participants are asked to respond to target positive or
negative words as quickly as possible while inhibiting responses to words of the opposite
affective category. Words are presented one by one in test blocks, and every two blocks the
target valence is changed (see Table 1). On the ‘shift blocks’, participants are required to
ignore previously relevant targets, shift attention and respond to stimuli that were
distractors in the previous block. On the ‘non-shift blocks’, for the second block in a pair,
participants need to continue responding to targets and ignore distractors.
Table 1
Target description of the 10 blocks of words in the Affective Shifting Task Positive (NS1) P3
Positive (NS) P
Negative (S2) T14
Negative (NS) T2
Positive (S) T3
Positive (NS) T4
Negative (S) T5
Negative (NS) T6
Positive (S) T7
Positive (NS) T8
OR Negative (NS) P
Negative (NS) P
Positive (S) T1
Positive (NS) T2
Negative (S) T3
Negative (NS) T4
Positive (S) T5
Positive (NS) T6
Negative (S) T7
Negative (NS) T8
1 Non-shift blocks; 2 Shift blocks, 3 Practice trials, 4 Test trials
This task assesses different types of inhibitory processes which can be measured
independently: (a) selective attention and maintenance of responding in the presence of
distracting stimuli (interference control) can be assessed by examining overall performance,
(b) reversal/shifting of association (task-shifting) is examined by comparing performance
on ‘shift blocks’ and ‘non-shift blocks’, and (c) a measure of inhibitory control over

Chapter 5
- 90 -
emotional stimuli of a particular valence is obtained by contrasting performance between
negative and positive target stimuli. One of the aims of this study is, therefore, to examine
performance on the measures of interference control, task-shifting and valence-dependent
inhibitory control, to assess whether participants with schizophrenia show an impairment in
these domains.
Inhibition in patients with and without auditory hallucinations
The Affective Shifting Task is also particularly relevant to the study of auditory
hallucinations in schizophrenia because of the inhibitory constructs it examines. Task-
shifting abilities have not previously been investigated in patients with auditory
hallucinations, although auditory hallucinations have been found to be associated with a
deficit in intentional inhibition, as measured by the HSCT and Inhibition of Currently
Irrelevant Memories task (ICIM task, Schnider & Ptak, 1999) (Badcock, Waters &
Maybery, in press; Waters et al, 2003). If auditory hallucinations are associated with a
deficit in intentional inhibition, then patients with this symptom should show impaired
performance on the task-shifting component of the Affective Shifting Task. In addition,
previous research has shown that auditory hallucinations are not associated with a deficit in
interference control, as measured with a latency index on the Stroop Color-Word Test
(Brebion, Smith, Gorman, Malaspina & Amador, 1998). Therefore, it is anticipated that
patients with auditory hallucinations should not show significantly longer latencies overall
on the Affective Shifting Task compared to patients without hallucinations.
Affective processes
The second aim of this study is to examine the role of affective processes in patients
with schizophrenia and in a subgroup of patients with auditory hallucinations.
Affective processes in schizophrenia
Emotional dysfunction is a frequent feature of schizophrenia (Bentall, 1997,
Birchwood, 2003; McGhie & Chapman, 1961). Estimates of the frequency of depression in
patients with schizophrenia range from 13 to 70% (Baynes et al, 2000; Birchwood, Iqbal,
Chadwick & Trower, 2000; Lancon, Auquier, Reine, Bernard & Addington, 2001; Siris et
al, 2001). Some studies have suggested that depression may be associated with a greater
risk of suicide in schizophrenia (e.g. Heila et al, 1997) and may increase the probability of
relapse (Birchwood, 2003).

Chapter 5
- 91 -
There is also some evidence that individuals with schizophrenia process emotional
information differently to healthy people (e.g. Calev & Edelist, 1993; Gooding & Tallent,
2002; Suslow, Roestel, Droste & Arolt, 2003). For instance, patients with schizophrenia
have consistently been found to be less accurate than healthy controls in recognizing facial
expressions of most emotions (e.g. Gooding & Tallent, 2002). However, the cognitive
processes involved in the development and maintenance of negative emotions in
schizophrenia are not yet known.
The current study aims to investigate the possible presence of an attentional bias for
negative material in patients with schizophrenia. Cognitive models of depression and
anxiety (e.g. Beck, 1976; see MacLeod & Rutherford, 1998, and Mineka & Nugent, 1995,
for reviews) have emphasised the role of biases in attention, memory, perception and
reasoning. In support, it is now well recognized that depressed and anxious patients show a
range of cognitive biases to emotionally negative or threatening features in the environment
(Hertel, 2002; MacLeod & Rutherford, 1998; Mineka & Nugent, 1995, for reviews). For
example, depressed patients attend to and remember more negative information than
nondepressed patients (e.g. Murray, Whitehouse & Alloy, 1999). Recent studies have also
shown that depression is associated with faulty inhibitory mechanisms of selective attention
for negative information (e.g. Joormann, 2004; Murphy et al, 1999). Murphy et al (1999),
for example, demonstrated an attentional inhibition deficit for negative words on the
Affective Shifting Task in depressed patients. On this task, the performance of depressed
and manic patients was compared with that of healthy controls. Both clinical groups
exhibited biases for emotional stimuli congruent with their current mood and were found to
show a specific pattern of impairment on the measures of inhibitory control. Depressed
patients showed an attentional bias for negative material, as demonstrated by faster
latencies when negative words were the targets. They also showed a specific impairment in
their ability to shift responding from one affective category to the next. By contrast, manic
patients had a bias for processing happy stimuli, as shown by faster latencies on positive
targets, and were impaired on the interference control component of the task.
The question of attentional bias for negative material in individuals with
schizophrenia has received little attention, although Rossell, Shapleske and David (1998)
showed that patients with delusions had theme-specific deficits. Since negative affect is
such a frequent feature in schizophrenia, it is possible that both clinical depression and

Chapter 5
- 92 -
schizophrenia have similar causal mechanisms in terms of an attentional bias towards
negative stimuli. The current study examines whether patients with schizophrenia show an
attentional bias towards negative material using Murphy et al’s Affective Shifting Task.
Affective processes in auditory hallucinations
Auditory hallucinations have also often been found to co-occur with depression,
anger, fear, anxiousness and low self-esteem (Alpert & Silvers, 1970; Carter, Mackinnon &
Copolov, 1996; Close & Garety, 1998; Delespaul, deVries & van Os, 2002; Hustig &
Hafner, 1990; Johns, Hemsley & Kuipers, 2002) and with an increased risk of suicide
(Falloon & Talbot, 1981; Walsh et al, 1999). In addition, abnormal activations in the
ventral striatum and limbic circuit have been reported in auditory hallucinations (e.g.
Copolov et al, 2003; Silbersweig et al, 1995; Takebayashi, Takei & Mori, 2002; Woodruff,
2004), regions that have been implicated in the identification of stimuli of emotional
significance and the production of affective states (Phillips, Drevets, Rauch & Lane, 2003).
However, the exact role of affect in auditory hallucinations is not well understood. The
current study aims to further advance our understanding of the role of affect in auditory
hallucinations by addressing a number of specific issues.
Firstly, it is not clear whether negative mood is implicated in the presence of auditory
hallucinations. In Waters et al (2003), we showed that depression and anxiety were not
associated with the severity of auditory hallucinations. However, some authors (e.g. Johns
et al, 2002) have proposed that negative affective response is a direct consequence of the
hallucinations themselves. The current study therefore aims to examine whether depression
and anxiety scores, on the BDI-II and BAI respectively, are associated with the presence of
auditory hallucinations, regardless of their degree of severity.
Secondly, negative affective voice content is a prominent feature of auditory
hallucinations in schizophrenia. A relationship between derogatory voice content and
depression has been reported (e.g. Hustig & Hafner, 1990; Soppitt & Birchwood, 1997),
but many questions remain regarding the maintenance process of negative auditory
hallucinations, and the association between negative affective voice content and emotional
dysfunction. It is unclear, for example, whether a depressed/anxious mood is always
associated with negative voice content. Conversely, do patients who experience positive,
or neutral, voice content also report negative mood? The present investigation aims to

Chapter 5
- 93 -
explore the relationship between affective voice content of auditory hallucinations and
anxiety and depression.
Thirdly, an influential psychological explanation of the maintenance process of
auditory hallucinations proposes that a person's belief about his or her voices is a mediating
factor between auditory hallucinations and the distress that is experienced (Chadwick &
Birchwood, 1994). Birchwood and Chadwick (1997) further suggested that it is the belief
about voices, and not the voice activity itself, that contributes to the ensuing affect and
coping behaviour. They identified two different constructs relevant to these issues: (a) the
belief about the voices' intent to do harm or good (malevolence vs benevolence) and the
belief about the voices' omnipotence, and (b) the reaction to these beliefs in terms of
engagement or resistance. In support for their model, they found associations between
belief in malevolence, negative affective response and resistance, and also an association
between belief in benevolence and engagement (Birchwood & Chadwick, 1997; Chadwick
& Birchwood, 1994, 1995; Chadwick, Lees & Birchwood, 2000; Soppitt & Birchwood,
1997). The current study uses Chadwick, Lees and Birchwood’s (2000) Belief About
Voices Questionnaire-Revised (BAVQ-R) to examine whether Birchwood and Chadwick’s
findings on the role of beliefs (malevolence, benevolence and omnipotence) and coping
strategies (resistance and engagement) is replicated in the current sample. The study also
investigates the relationship between beliefs, depression/anxiety and negative affective
voice content.
Lastly, the final aim of this study is to investigate the role of attentional inhibitory
biases for negative material in auditory hallucinations. Since auditory hallucinations have
been linked to depression, the examination of patients’ performance on the measure of the
Affective Shifting Task assessing attentional inhibitory control over emotional stimuli is
particularly relevant. If depression is an common component of auditory hallucinations,
patients should demonstrate a bias for negative targets. In addition, because a bias towards
negative material might partly explain the predominance of negative material in auditory
hallucinations, the association between the index of inhibitory control over negative
emotional stimuli and voice content will also be examined.
Summary of goals
The first goal of the study is to investigate inhibitory processes in patients with
schizophrenia, compared to healthy controls, on the Affective Shifting Task, in order to

Chapter 5
- 94 -
determine whether patients show an impairment on task shifting. The pattern of
performance of patients with and without auditory hallucinations on the task shifting index
of the Affective Shifting Task will also be examined. The second and third goals of this
study are to explore the role of affective processes in schizophrenia and auditory
hallucinations respectively. With regard to patients with auditory hallucinations, the
relationships between the presence and severity of hallucinations and affective voice
content, beliefs about voices, depression, anxiety and attentional inhibitory bias for
affective material are examined.
Method
Participants
The patient group consisted of 43 patients with a DSM-IV diagnosis of schizophrenia
selected from a psychiatric hospital in Perth, Western Australia. Patients currently
experiencing hallucinations were selected on the basis of having experienced auditory
hallucinations on at least half of the days during the preceding four weeks, as assessed by
self-reports and case note reviews (“Current AH”, N = 19). Other schizophrenia patients
who did not fit this criterion were assigned to the non-hallucinating group (“Non AH”, N =
24). The control group comprised 24 healthy individuals recruited from the community
through a blood donor agency. Exclusionary criteria for all participants included a history
of head injury and neurological illness. Controls who reported a personal or first-degree
family history of psychiatric illness were also excluded. Information concerning the
patients’ and controls’ demographic and clinical data is presented in Table 2. The study
was approved by the University of Western Australia and Graylands Hospital Ethics
Committees and signed informed consent was obtained from all participants.
Clinical ratings
Patients were interviewed using the Positive And Negative Syndrome Scale (PANSS)
(Kay, Opler & Fiszbein, 1987). The PANSS measures both the presence and severity of
Positive (which include AH together with delusions, etc.), Negative (e.g. blunted affect)
and General symptoms (e.g. somatic concerns) on a 7-point scale. AH severity was rated
from the PANSS with higher ratings signaling an increase in AH frequency. The symptom
composition of the patient group is described in Table 2.

Chapter 5
- 95 -
Tasks and questionnaires
Assessment of general intelligence
Premorbid intelligence was estimated using the National Adult Reading Test-revised
(NART) (Nelson, 1982).
Affective Shifting Task (Murphy et al, 1999)
In this task, individual words were rapidly presented on the computer screen of a PC
running Windows 95. The task was programmed in MetaCard. Participants were required
to respond (press the space bar) to target words of either positive or negative valence, while
inhibiting responses to words of the competing affective category. There were 180 stimuli
used in the task, made up of 45 positive and 45 negative words, each used twice. Words
were presented individually in the centre of the screen for 300ms each with an inter-
stimulus interval of 900ms.
There were 2 practice blocks and 8 test blocks. Each block consisted of 18 words (9
positive and 9 negative words). The words were randomly allocated to, and within, each
block, and freshly randomized for each subject. For each block, positive (P) or negative
(N) words were specified as targets in set sequences (see Table 1). Every 2 blocks,
participants were required to shift response set from one affective category to the other (on
'shift blocks') and to inhibit responding to stimuli that were targets in the previous two
blocks and start responding to words that had been distractors. For the other four test
blocks ('non-shift blocks'), participants had to continue responding to targets of the same
valence category and inhibiting responding to distractors of the alternate category. The two
target category presentation orders (see Table 1) were alternated between participants. An
interval of 15s separated blocks of trials. There was a 500ms/450Hz tone that sounded for
false alarms (but not for omissions).
For the pilot testing of the words, a list of 60 positive and 60 negative adjectives was
given to 25 university students (age range 18-33 years) who rated each adjective on a scale
from 1 to 6 according to how positive or negative it was in connotation. The adjectives
were ranked with respect to mean ratings and the 45 positive and 45 negative words which
attracted the highest and lowest ratings were selected (see Appendix B). Positive and
negative words did not differ in word length, t(88) = 1.83, p > .05, or word frequency, t(88)
= 1.84, p > .05 (Kucera & Francis, 1967).

Chapter 5
- 96 -
Fourteen first-year psychology students (age range 18-33 years) participated in the
piloting of the task to ensure the task yielded similar results to the control participants in
Murphy et al’s (1999) study. Our pilot testing showed comparable results (within one
standard deviation) to those reported by Murphy et al for each condition of the task and
each variable, apart from the number of omissions per block of trials. Whereas Murphy et
al (1999) found that participants made an average of .26 omissions (S.E. = .06), the pilot
participants from our study made an average of .92 omissions (S.E. = .22). Although the
reasons for this difference are not clear, variations in demographics may have contributed
to differences in performance. Whereas the pilot subjects from this study were young
university students, Murphy et al’s control sample comprised individuals drawn from the
wider community with a mean age of 36.1 years and selected to match the demographic
characteristics of manic patient.
The Beck Depression Inventory (BDI-II) and Beck Anxiety Inventory (BAI) (Beck, 1996,
1990, respectively)
These tests both have a maximum score of 21.
Auditory Hallucinations Questionnaire (based on PSYRAT and MUPS; Haddock,
McCarron, Tarrier & Faragher, 1999; Carter, Mackinnon, Howard, Zeegers & Copolov,
1995; Appendix A)
Only one item regarding negative voice content was used for this study: “Do your
voices say unpleasant things or negative things?” Scores range from 1 (never) – 5 (always).
Beliefs about Voices Questionnaire-Revised (BAVQ-R) (Chadwick, Lees & Birchwood,
2000)
This questionnaire has 35 items, rated on a 4-point scale: disagree (0), unsure (1),
agree slightly (2) and agree strongly (3). It has three subscales related to beliefs:
Malevolence, Benevolence and Omnipotence (each with 6 items and a range of scores = 1-
18); and two subscales measuring emotional and behavioural response to auditory
hallucinations: Resistance (9 items, range of scores = 0-27) and Engagement (8 items,
range of scores = 0-24). Individuals hearing more than one voice are required to complete
the questionnaire for their dominant voice.

Chapter 5
- 97 -
Table 2
Demographic and clinical characteristics (mean, SD) of healthy controls and patients with schizophrenia, and subgroups of patients with
(Current AH) and without (Non AH) auditory hallucinations
Controls (n = 24)
Patients (n = 43)
Current AH (n = 19)
Non AH (n = 24)
Controls-Patients comparisons
Current–Non AH comparisons
Age (years) 34.67 (8.81) 36.73 (8.41) 34.10 (9.65) 38.29 (7.22) t = .95, p = .34 t =1.62, p = .11
Education (years) 11.75 (1.89) 10.97 (1.97) 10.78 (2.12) 11.20 (1.86) t =1.55, p = .12 t = .68, p = .49
Sex (M/F) 20 M, 4 F 35 M, 7 F 16 / 3 19 / 5
NART 103.62 (4.75) 100.21 (9.32) 95.89 (7.77) 104.16 (9.11) t =1.66, p = .10 t = 3.15, p < .05
BDI-II 2.04 (1.98) 12.80 (12.78) 13.84 (15.62) 11.95 (10.16) t =4.08, p < .001 t =.47, p = .64
BAI 1.54 (1.79) 9.52 (9.25) 9.15 (9.01) 9.82 (9.63) t =5.41, p < .001 t =.23, p = .81
Length of illness* (yrs) - 13.64 (8.14) 10.89 (7.11) 15.41 (8.55) - t = 1.85, p = .07
Number of admissions - 9.35 (7.79) 9.52 (10.02) 8.87 (5.68) - t = .26, p = .78
Level of positive symptoms (PANSS) - 19.06 (5.12) 23.63 (3.60) 15.45 (2.63) - t = 8.58, p < .001
Level of negative symptoms (PANSS) - 12.25 (3.22) 13.00 (2.80) 11.66 (3.45) - t = 1.36, p = .18
Level of general symptoms (PANSS) - 28.72 (5.47) 29.78 (4.79) 27.87 (5.92) - t = 1.14, p = .26
Chlorpromazine equivalent - 942.78 (445.3) 1075.52
(496.08) 814.04
(3.78.33) - t = 1.96, p = .06
* calculated as time since first admission

Chapter 5
- 98 -
Table 3
Means (and standard deviations) for latencies (RT), false alarms (FA) and omissions per block of trials as a function of shift and
valence conditions of healthy controls and patients with schizophrenia, and subgroups of patients with (Current AH) and without
(Non AH) auditory hallucinations.
Controls All Patients Current AH Non AH (n = 24) (n = 43) (n = 19) (n = 24)
RT Shift 516.77 (69.39) 594.98 (88.79) 573.41 (87.13) 612.06 (88.13)
Non-shift 514.47 (60.01) 595.21 (88.15) 577.74 (85.87) 609.04 (89.26)
Positive 512.17 (67.69) 598.28 (86.25) 578.36 (84.75) 614.05 (85.89)
Negative 519.10 (61.38) 591.68 (86.92) 572.28 (81.35) 607.05 (89.77)
FA Shift .96 (1.09) 1.66 (1.15) 2.02 (1.15) 1.38 (1.10)
Non-shift .71 (.90) 1.52 (1.28) 1.80 (1.46) 1.31 (1.11)
Positive .50 (.59) 1.65 (1.12) 1.85 (1.12) 1.48 (1.12)
Negative .35 (.41) 1.54 (1.45) 1.97 (1.62) 1.20 (1.23)
Omissions Shift .47 (.87) 1.30 (1.48) 1.71 (1.86) .97 (1.02)
Non-shift .38 (.72) 1.01 (1.29) 1.18 (1.47) .87 (1.15)
Positive .25 (.47) 1.22 (1.38) 1.56 (1.69) .94 (1.05)
Negative .18 (.31) 1.09 (1.35) 1.32 (1.54) .90 (1.17)

Chapter 5
- 99 -
Results
Preliminary analyses showed that the patients and controls did not differ in premorbid
IQ as measured with the NART, age or educational level (see Table 2). Comparisons
between the patient subgroups showed that Current AH and Non AH patients did not differ
in age, educational level, length of illness, number of admissions, and Negative and
General symptoms scores on the PANSS (Kay, Fiszbein & Opler, 1987). However,
Current AH patients had significantly higher Positive symptoms ratings, as measured by the
PANSS, compared to Non AH patients. Current AH patients also had lower premorbid IQ
scores, as measured by the NART, compared to Non AH patients and tended to have higher
chlorpromazine dosages although the difference did not reach the conventional level of
significance (Table 2). The results of the Affective Shifting Task are presented first,
followed by an analysis of the questionnaires.
Affective Shifting Task
For all conditions on the Affective Shifting Task, latencies (RT), false alarms (FA)
and omissions were computed for all participants. Anticipatory responses (with a RT less
than 100ms) were excluded from the analysis (Murphy et al, 1999). Table 3 presents
means and standard deviations for these variables as a function of the different shift and
valence conditions. The controls’ performance was within one standard deviation of the
performance of the control group of Murphy et al’s study. The data set contained a number
of outliers but the text presents results of parametric tests since results of nonparametric
tests showed no differences in outcome.
Comparisons between groups were carried out with two ANOVAs. For RT, an
ANOVA was performed with group as the between subjects factor and target valence
(positive/negative) and shift condition (shift/nonshift block) as within subject factors. For
the analysis of errors, an ANOVA was performed with group as the between subjects factor
and error type (FA, omissions), target valence and shift condition as within subjects factors.
Schizophrenia patients versus controls comparisons
Analyses showed that, overall, schizophrenia patients were significantly slower to
respond, F(1, 65) = 16.14, p < .001. Patients also made significantly more errors than
controls, F (1, 65) = 9.84, p < .01. A main effect of error type revealed that participants, on
average, made significantly more FA than omissions, F (1, 65) = 6.47, p < .01. Overall,
Chapter 5
- 100 -
more errors were made on negative than positive words, and on shift blocks than nonshift
blocks, F (1,65) = 4.56, p < .05, and F (1, 65) = 8.22, p < .01, respectively. The interaction
between subject group and shift condition was not significant for RT or errors, F (1, 65) =
.05, p =.81, and F (1, 65) = .10, p = .75, respectively. Similarly, the interaction between
subject group and target valence did not approach significance for RT or errors, F (1, 65) =
2.34, p = .13, and F (1, 65) = .39, p = .53, respectively. No other interactions were
significant (all p > .09). The results suggest that task shifting was not impaired in
schizophrenia and that patients did not show a bias towards negative words.
Analyses of patients with and without hallucinations
Despite the absence of a shifting deficit in the group of schizophrenia patients, it was
important to test whether such a deficit exists in relation to the symptom of auditory
hallucination. Group comparisons between the Current AH and Non AH patients showed
that there were no significant differences for RT, F (1, 41) = 1.89, p = .17, or errors, F (1,
41) = 3.34, p = .07. Overall, significantly more errors were made on shift compared to
nonshift blocks, F (1,41) = 7.19, p < .01. However, there were no significant effects
between subject group and (a) shift condition, (b) target valence or (c) error type, or their
interaction, for RT or errors (all p > .10).
Investigations were also carried out to examine whether the severity of auditory
hallucinations was associated with impaired task shifting performance or overall
performance, or with a bias towards negative material: (a) task shifting was examined by
computing the cost of shifting. The cost of shifting reflects the additional time, or errors,
incurred as a result of the task-shifting process and is a convenient measure to use in
correlations. It is calculated as the difference in RT/FA/omissions between shift and non-
shift blocks. Severity of auditory hallucinations was not found to be correlated with RT,
FA or omissions shifting costs (all p > .12); (b) In order to assess general accuracy of
performance, overall RT, FA and omission rates were correlated with auditory
hallucinations severity. Analyses revealed a significant correlation between overall FA
rates and auditory hallucinations severity, r = .31, p < .05, suggesting that an increase in the
severity of hallucinations was associated with an overall increase in FA on the Affective
Shifting Task. However, overall RT and omission rates were not found to be correlated
with auditory hallucinations severity, r = -.20, p = .18, and r = .14, p = .35, respectively.
Finally, (c) a bias for negative material was examined by computing a “valence cost”,

Chapter 5
- 101 -
calculated as the difference in RT/FA/omissions between negative and positive words.
There were no significant correlations between severity of auditory hallucinations and
valence cost for RT, FA or omissions (all p > .13). Overall, the results suggest that
auditory hallucinations were not associated with an impairment in task shifting or a bias
towards negative material. However, the severity of hallucinations was found to be
associated with an increase in overall FA, but not with an increase in response latency.
Questionnaire results
The following analyses report the results of nonparametric tests when the
assumptions of parametric tests were not met.
BDI-II and BAI
Healthy controls reported only minimal levels of depression and anxiety. One patient
with schizophrenia did not want to complete the BDI-II and BAI so the results include the
scores of 42 patients. Compared to controls, schizophrenia patients had significantly higher
levels of depression and anxiety (Table 2). Thirty-three percent of patients had mild,
moderate or severe levels of depression and 43% had mild, moderate or severe levels of
anxiety. Analyses were carried out to examine whether there was a specific demographic
or clinical profile associated with depression or anxiety in the schizophrenia patient group.
BDI-II and BAI scores were not found to be significantly correlated with age, years of
education, intellectual functioning, number of periods of hospitalization, length of illness,
chlorpromazine equivalents or positive, negative or general symptom scores on the PANSS
(all p> .08).
Thirty-two percent of the Current AH patients and 34% of the Non AH patients had
mild, moderate or severe levels of depression. Forty-two percent of the Current AH
patients and 43% of the Non AH patients had mild, moderate or severe levels of anxiety.
Current AH and Non AH patients did not differ significantly in levels of depression or
anxiety (Table 2).
In summary, these results show that patients with schizophrenia had significantly
higher levels of depression and anxiety compared to healthy controls, although not all
patients were rated as depressed or anxious. There were no significant differences in
depression and anxiety levels between patients with and without current hallucinations.

Chapter 5
- 102 -
Performance on the Affective Shifting Task and depression/anxiety
In order to investigate whether the depression status of schizophrenia patients was
critical to Affective Shifting Task performance, the schizophrenia patient group was
divided into those who reported low levels of depression (minimal or mild scores on the
BDI-II, between 0 and 19; n = 35) and those who reported high levels of depression
(moderate or severe scores on the BDI-II, 20 and above, n = 7). The division of the patient
group into high and low depressed groups was necessary to run similar analyses to those
reported by Murphy et al (1999).
An analysis of RT showed no significant group difference between low-depressed or
high-depressed patients, F(1, 40) = .18, p = .66. However, there was a near-significant
interaction between participant group and target valence, F (1, 40) = 3.51, p = .06. Figure 1
shows mean RT as a function of target valence for low-depressed and high-depressed
patients. A paired-samples t-test revealed that high-depressed schizophrenia patients were
slower to respond to positive targets compared to negative targets, t(6) = 2.86, p < .05,
paralleling results with patients suffering major depression (Murphy et al, 1999). For low-
depressed patients, there was no significant difference in RT between positive and negative
targets, t(34) = .10, p = .92. Analyses of errors revealed that, overall, participants made
more errors on shift than nonshift trials, F (1, 40) = 5.98, p < .01, but no other effects were
significant (all p < .08). No significant associations were found between anxiety levels as
measured by the BAI and performance on the Affective Shifting Task.
Investigations were also carried out to examine whether depression severity in the
patient group was associated with task shifting performance, overall performance and a bias
towards negative material. The valence cost for FA was found to be significantly
correlated with BDI-II scores, rho = .30, p < .05, suggesting that the number of FA on
negative words when positive words were the target increased with higher depression
scores. RT and omissions valence costs were not found to be significantly correlated with
BDI-II scores (both p > .27). Task shifting was examined using shifting costs. BDI-II
scores were not found to be significantly correlated with RT, FA or omission shifting costs
(all p > .40). Finally, overall RT, FA and omission rates were correlated with BDI-II scores
to examine general performance. None of the correlations were found to be significant (all
p > .22). Again, there were no significant correlations between BAI scores and
performance on the Affective Shifting Task (all p > .12).

Chapter 5
- 103 -
570
580
590
600
610
620
630
640
650
Low-depressed High-depressed
Patients with schizophrenia
Mea
n R
T
Positive valence Negative valence
Figure 1
Mean RT(and SD) as a function of target valence for low-depressed and high-depressed
patients with schizophrenia
In summary, patients with schizophrenia, compared to healthy controls, did not
demonstrate a bias towards negative material. However, highly depressed schizophrenia
patients showed an attentional bias for negative words, compared to low depressed patients,
as demonstrated by faster latencies when negative words were the target. In addition,
higher depression scores in the patient group were found to be associated with an increasing
number of false alarms involving negative words when positive words were the target.
The same group comparison analyses could not be carried out in the subgroup of
patients with auditory hallucinations since the number of high-depressed patients (n = 4)
was too low for meaningful analyses. However, correlations between BDI-II scores and
performance on the Affective Shifting Task were carried out in the subgroup of patients
with auditory hallucinations. The depression-related effects observed in patients with
schizophrenia were also found in hallucinating patients. BDI-II scores were found to be
positively and significantly correlated with FA valence costs, rho = .47, p < .05, suggesting
that the number of FA on negative words when positive words were the target increased

Chapter 5
- 104 -
with higher depression scores. Correlations between BDI-II scores and RT/omission
valence costs were not found to be significant, rho = -.06, p = .80, and rho = -.01, p = .97,
respectively. Correlations between BDI-II scores and RT/FA/omission shifting costs and
overall RT/FA/omissions rates were not significant either (all p > .09). There were no
significant correlations between BAI scores and measures of task-shifting, overall
performance and bias towards negative material on the Affective Shifting Task in the group
of patients with auditory hallucinations (all p > .37).
Negative voice content: Auditory Hallucinations Questionnaire
All 19 patients with current hallucinations responded to the questionnaire. The mean
score for the Negative Content item was 3.00 (SD = 1.33). Most patients (14/19, 89.4%)
responded that their voices were negative at least some of the time (score = 2-5). Three of
those reported that their voices were always negative (15.7%). Only 2 patients (10.5%)
said that their voices were never negative.
BAVQ-R
Eighteen patients agreed to fill-in the questionnaire. Subscale means on the BAVQ-R
were as follows: malevolence 5.55 (SD = 5.43), benevolence 8.94 (SD = 6.09),
omnipotence 7.66 (SD = 4.64), engagement 9.33 (SD = 7.79) and resistance 14.22 (SD =
7.64). These scores are similar to those reported by Chadwick et al (2000). Also replicated
(see Table 4), were the positive relationships between belief in malevolence and resistance
activity, and between belief in benevolence and engagement. Contrary to Chadwick et al’s
findings, no significant correlations were found between omnipotence and malevolence and
between omnipotence and resistance activity.
A cut-off point for malevolence, benevolence and omnipotence was derived to carry
out investigations on patients who believed their voices to be malevolent, omnipotent and
benevolent (as described in Chadwick & Birchwood, 1994). Since the distributions were
normally distributed, a cut-off point based on mean scores was computed. Accordingly, the
chosen cut off point for malevolence was a score of 5 or more, benevolence 9 or more and
omnipotence 6 or more. According to this criterion, it was found that 8 patients (44.4 %)
believed their voices to be malevolent, 10 (55.5 %) benevolent, and 11 (61.1 %)
omnipotent.

Chapter 5
- 105-
Table 4
Correlations between variables assessing belief about malevolence, benevolence, omnipotence and engagement and resistance behaviours
on the BAVQ, depression on the BDI-II, anxiety on the BAI and negative voice content in the Current AH group (n = 18)
BAVQ-R subscales Affect
Malevolence Benevolence Omnipotence Engagement Resistance BDI-II BAI
Negative
Content item
Malevolence - -.35 .41 -.48* .62** .56** .24 .38
Benevolence - - .03 .82*** -.40 -.43 -.18 -.70**
Omnipotence - - - .27 .50* .59** .03 .29
Engagement - - - - -.23 -.20 -.08 -.54**
Resistance - - - - - .70*** .38 .42
BDI-II - - - - - - .60*** .54*
BAI - - - - - - - .36
* p < .05, ** p < .01, *** p < .001

Chapter 5
- 106-
Relationship between BDI-II, BAI, Negative Content and BAVQ-R
Table 4 shows that Negative Content scores were significantly correlated with BDI-II
scores, suggesting that higher negative voice content was associated with increasing levels
of depression. The two patients who did not report any negative voice content (score = 1)
rated only minimal levels of depression. Thirty-five percent of patients (6/17) who reported
some negative voice content at least some of the time (score = 2-5) had mild, moderate or
severe levels of depression, while the remainder (64%) reported only minimal levels of
depression. The 3 patients who reported hearing exclusively negative voice content
showed mild, moderate and severe levels of depression. Negative Content scores were not
significantly correlated with BAI scores.
Consistent with Chadwick et al (2000), beliefs in malevolence and omnipotence were
significantly associated with increasing depression scores (see Table 4). However, 60%
(9/15) of patients with beliefs in malevolence and/or omnipotence still scored in the
minimal range of the BDI-II, suggesting that negative beliefs are not always linked with
depression. Contrary to Chadwick et al’s finding, no significant relationship was found
between any of the BAVQ-R items and BAI scores.
Belief about benevolence was significantly and negatively correlated with Negative
Content scores. As Negative Content scores increased, levels of engagement were also
found to decrease. However, there was no significant relationship between beliefs about
malevolence and omnipotence and Negative Content scores.
Performance on the Affective Shifting Task and negative voice content
Correlations were carried out between Affective-Shifting Task performance and
negative voice content scores, but no significant correlations emerged between Negative
Voice Content and (a) RT, FA or omission shifting costs (all p > .09), (b) overall RT, FA
and omission rates (all p > .09) and (c) RT, FA or omission valence costs (all p > .09).
DISCUSSION
The results of the analyses of inhibitory processes are discussed initially and are
followed by a discussion of affective processes in patients with schizophrenia and in
relation to the experience of auditory hallucinations.

Chapter 5
- 107-
Inhibitory processes
Inhibition in schizophrenia
The first goal of the study was to investigate whether patients with schizophrenia
show an impairment in task-shifting compared to healthy controls on the Affective Shifting
Task. Firstly, analyses show that significantly more errors were made on shift compared to
nonshift trials in both the control and patient groups, suggesting that task shifting effects
were replicated in the current task (Murphy et al, 1999). Secondly, the results reveal that
patients with schizophrenia were not impaired in shifting attention and responding, as the
difference in performance in both response accuracy and latency between shift and non-
shift blocks was not significantly more pronounced relative to controls. The finding of
intact task shifting abilities in patients with schizophrenia contrasts with findings of
impaired performance on other tasks of intentional inhibition, such as the HSCT and ICIM
task (Nathaniel-James et al, 1996; Waters et al, 2004). We may speculate on the reason for
this discrepancy in findings. Similarly to the HSCT and ICIM task, task shifting on the
Affective Shifting Task is deliberately invoked, goal-directed, effortful and available to
conscious reflection and strategic interventions, thereby matching the definition of
intentional inhibition processes (Nigg, 2000; Wilson & Kipp, 1998). In addition, the
current or relevant goal is explicit for all of these tasks. What is different, however, is that,
on the Affective Shifting task, the response options are clearly defined and limited (since
only instances of negative and positive response options are presented to the participant).
In contrast, in tasks such as the HSCT and ICIM task, the response options are either open-
ended (HSCT) or unknown (ICIM task). Consequently, it may be speculated that the
Affective Shifting Task is an easier measure of intentional inhibition and may require less
inhibitory demands than tasks such as the HSCT and ICIM task, on which patients have
been found to be impaired. In support, Amieva, Phillips, Della Sala and Henri (2004) have
recently proposed that there are different degrees of inhibitory demand within tasks of
intentional inhibition and that the extent of controlled suppression is likely to vary
depending on various factors including different task requirements. It is possible, therefore,
that the material to be suppressed in the Affective Shifting task imposed weaker inhibitory
demands than other paradigms assessing intentional inhibition processes, such as the HSCT
or ICIM task.

Chapter 5
- 108-
This explanation may also accommodate the conflicting results on other task-shifting
paradigms, such as on the WCST, saccadic tasks (Manoach et al, 2002), a Rule Shift Cards
test and Discrimination Shift Learning paradigms (Cools, Brouwer, de Jong & Slooff,
2000; Crider, 1997; Elliott et al, 1995). In those paradigms where the response options
were limited or clearly defined, patients may have found it easier to inhibit the currently
irrelevant stimuli or category, compared to other paradigms where response alternatives
were open-ended or unspecified. Even within the same family of tasks, such as on the
WCST, different experimental designs varying in, for instance, the number of sorting
categories could have resulted in mixed findings. In order to test the proposal that patients
with schizophrenia have intact task shifting abilities when the response options are defined
or limited, it would be useful to carry out studies in the same sample of patients, in which
the difficulty of the same task-switching paradigm is manipulated by increasing the number
of possible options available to participants. An alternative explanation for the discrepancy
in findings in the literature has been provided by Manoach et al (2002). These authors
speculated that findings of impaired performance in some studies might have been due to
high working memory demands on the shifting component of the task used in these studies.
Healthy controls could predict and prepare for switch trials, but schizophrenia patients, as a
consequence of poor working memory, may have been at a disadvantage in the task-shifting
conditions leading to poor response accuracy on switch trials. In support, separate neural
processes have been identified in task-shifting performance according to the recency of
previously reinforced trials (Dreher & Berman, 2002). Further studies should aim to test
and contrast these two alternative explanations.
The results of this investigation also suggested that the patients responded more
slowly and made more FA and omissions relative to controls, suggesting difficulties
focusing attention and inhibiting inappropriate responding to interfering stimuli.
Difficulties in maintaining overall performance suggests impaired interference control in
patients with schizophrenia, confirming previous findings of interference control failure in
schizophrenia, as demonstrated by longer response latencies and greater number of errors
on a Stroop paradigm (Boucart et al, 1999; Brebion et al, 1996).
Inhibition in patients with and without auditory hallucinations
The second goal of this study was to examine the performance of patients with
auditory hallucinations, relative to those without, on the task-shifting and interference

Chapter 5
- 109-
control measures of the Affective Shifting Task. Firstly, the results show that auditory
hallucinations were not associated with impaired task-shifting abilities as measured by the
Affective Shifting Task. The finding of intact task-shifting abilities in patients with
auditory hallucinations contrasts with findings of impaired performance on other tasks of
intentional inhibition, such as the HSCT and ICIM task (Badcock et al, in press; Waters et
al, 2004). It may be speculated that, as discussed above, the demands of the task shifting
component of the Affective Shifting Task may have been easier than those required in these
other tasks because of a lower number of response options. This raises the possibility that,
in some situations, patients with auditory hallucinations are able to inhibit intrusive
cognitions. This finding may, at least partly, explain why hallucinations do not occur
continuously.
Secondly, analyses were carried out between the severity of hallucinations and
overall performance on the Affective Shifting Task. No significant correlations were found
between hallucination severity and overall RT. The finding that auditory hallucinations are
not associated with significantly longer response latencies replicates findings from Brebion
et al (1998) on the Stroop Color-Word Test and suggests that this aspect of interference
control is not particularly impaired in auditory hallucinations. Furthermore, the finding of
intact performance on a measure of overall performance argues against any explanation
based on impaired motivation, or general cognitive impairment, of patients with auditory
hallucinations.
Interestingly, the current results did show that the severity of hallucinations was
associated with an overall increase in false alarms. False alarms represent a failure to
inhibit inappropriate responding to previously relevant but currently inappropriate stimuli.
We previously identified similar difficulties in suppressing recently activated memory
representations in patients with auditory hallucinations, as measured by the ICIM task
(Badcock et al, in press; Waters et al, 2003). In particular, we showed that patients with
auditory hallucinations fail to suppress memories of prior events that are not relevant to
current goals. The present finding of an association between false alarms on the Affective
Shifting Task and auditory hallucinations provides further support for the proposal that the
severity of auditory hallucinations is associated with increasingly impaired control of
unwanted and irrelevant cognition.

Chapter 5
- 110-
In summary, the results of this study indicate that patients with schizophrenia did not
show task-shifting difficulties. Similarly, auditory hallucinations were not found to be
associated with a task-shifting impairment. Methodological differences, leading to
variation in the degree of intentional demand, between studies might have accounted for the
discrepancies with previous findings. This type of problem highlights the complexity of
unravelling a complex set of processes such as inhibitory control and the need of a clear
taxonomy of tasks of inhibition. Further studies should (a) aim to identify common
mechanisms that can help towards a systematic mapping of tasks assessing inhibitory
processes by undertaking a large study using a range of tasks on a variety of clinical and
healthy population groups and (b) develop better tasks where the inhibitory demands are
manipulated more systematically. The results also show that auditory hallucinations were
not associated with longer response latencies overall, suggesting that some aspect of
interference control was intact. However, it was found that severity of hallucinations was
associated with an increase in overall false alarms, indicating a failure to suppress currently
irrelevant stimuli and replicating previous results (e.g. Badcock et al, in press; Waters et al,
2003).
Affective processes
Affective processes in schizophrenia
The results reveal that patients with schizophrenia reported significantly higher
depression levels compared to controls. It was also found that a third of patients with
schizophrenia showed mild, moderate or severe levels of depression, replicating findings by
Siris et al (2001) in an international survey of depression in schizophrenia. The results also
show that 43% of patients report mild, moderate or severe levels of anxiety. These results
indicate that although negative mood is significantly associated with schizophrenia, it is not
a necessary feature of the illness.
Scores on the BDI-II and BAI were not found to be significantly correlated with
positive, negative or general symptoms severity as measured by the PANSS. This suggests
that although emotional disturbances were identified in the patient group, they are not
directly related to the severity of major symptom groups. Although some correlational
studies have found that depression is associated with positive symptoms (e.g. Zisook et al,
1999), other studies have found depression to be independent of the symptoms of
schizophrenia (Marengo, Harrow, Herbener & Sands, 2000). Lancon et al (2001) provided

Chapter 5
- 111-
an explanation for the discrepancy in findings, suggesting that the relationship between
depression and symptoms of schizophrenia depends largely on factors such as whether the
patients are in an acute or stable period. Depression and anxiety scores were not
significantly associated with any specific demographic or clinical characteristics either, a
finding which replicates previous studies (Baynes et al, 2000; Zisook et al, 1999)
The presence of attentional bias for negative material in patients with schizophrenia
was also investigated in this study. It was found that the patients, as a group, did not show
an attentional bias for negative material when compared to healthy controls. However, the
results did indicate an association between depression and a bias towards negative targets in
patients with schizophrenia. The subgroup of patients who scored high levels of depression
demonstrated faster latencies when negative words were the targets, and higher depression
scores in the patient group were found to be associated with an increasing number of false
alarms on negative words when positive words were the targets. The demonstration of
faster RTs for negative words, compared to positive words, in depressed schizophrenia
patients resembles the results reported for depressed individuals in Murphy et al’s (1999)
study. The finding of the same bias on negative words in the two patient groups, who are
both depressed, indicates an overlap in affective cognitive mechanisms. Beck’s (1976)
model of depression suggests that depression is characterized by distortions in information
processing, or negative schemas, and is subject to biases that overvalue negative or
threatening features in the environment (Hertel, 2002). The current results suggest that an
attentional bias for negative information may also be part of the development and
maintenance process of depression in schizophrenia patients and merit further investigation.
Overall, the results of this investigation reveal that about one third of patients with
schizophrenia were depressed and approximately one half showed elevated anxiety scores.
This suggests that emotional dysfunction is often present in schizophrenia although it is not
a core component of the disorder. Clinical and demographic factors were not found to
contribute to BDI-II and BAI scores. Consequently, what contributes to depression and
anxiety in patients with schizophrenia? Auditory hallucinations have often been linked to
emotional dysfunction. The following discussion examines the role of depression and
anxiety in patients with auditory hallucinations.

Chapter 5
- 112-
Affective processes in auditory hallucinations
Approximately one third of patients with auditory hallucinations had elevated
depression and anxiety scores, although the results also show that depression and anxiety
were not specifically related to the presence, or severity, of auditory hallucinations. This
indicates that negative affect is associated with auditory hallucinations, but not specifically
so. These findings do not support the proposal that negative affect is a direct consequence
of the hallucinations themselves (Johns et al, 2002) or that an increase in negative mood
should correlate with an increase in frequency of auditory hallucinations (Morrison &
Baker, 2000).
The results also show that only 10% of patients reported that their voices were never
negative, suggesting that negative affective hallucinations are very common in patients with
schizophrenia. The relationship between affective voice content and negative mood was
also examined. There were three significant findings: (a) those patients with no negative
voice content reported only minimal levels of depression; (b) depression levels were
significantly correlated with the amount of negative voice content; but (c) most patients
with negative voice contents still rated themselves as being minimally depressed.
Altogether, the results indicate that depression is linked to, but is not a necessary outcome
or a precondition of negative voice content of auditory hallucinations.
Exploratory analyses of the BAVQ-R reveal that, consistent with Chadwick and
Birchwood’s (1994, 1995) findings, beliefs in malevolence and omnipotence were
associated with increasing depression and resistance activity, supporting their proposal that
beliefs about voices contribute to ensuing affect. However, it was also found that beliefs in
malevolence and/or omnipotence did not necessarily result in elevated depression scores.
This supports findings by Close and Garety (1998) that show that the patients’ affective
response is not always dependent on beliefs about voices. The results also show that belief
in malevolence or omnipotence was not related to negative voice content, although belief in
benevolence was found to decrease with increasing reports of negative voice content. In
sum, the results of this investigation suggest that beliefs about voices are important
components to understanding affect and content of auditory hallucinations, although they
are not always effective predictors of negative affective states or negative voice content.
The role of attentional bias for negative material in patients with auditory
hallucinations was also investigated in this study. The results reveal that the presence of

Chapter 5
- 113-
auditory hallucinations was not associated with an attentional bias for negative material.
Similar findings have recently been reported in healthy individuals identified as being
disposed to developing hallucinations using an affective priming task (van ‘t Wout,
Aleman, Kessels, Laroi and Kahn, 2004).
However, the depression-related effect on the Affective Shifting task observed in the
schizophrenia sample group was also found to apply to patients with auditory
hallucinations who are also depressed. Although the results are preliminary given the size
of the sample group, depression in patients with auditory hallucinations was associated with
a bias towards negative material. In particular, higher depression scores were found to be
associated with an increasing number of false alarms on negative words when positive
words were the targets. This suggests that, when present, depression in patients with
hallucinations is linked to the intrusion of unwanted negative material from memory. It
may be speculated that depression, therefore, may be linked to the occurrence of negative
voice contents frequently reported by hallucinating patients. Difficulties with this proposal
include (a) as discussed above, negative voice contents still occur in patients who rate
themselves as being minimally depressed and (b) negative voice content was not found to
be associated with a bias for negative targets on the Affective Shifting Task. These
findings perhaps suggest that a more socio-psychological explanation should be put
forward to explain the frequent negative voice content reported by patients. In support,
some argue against a purely cognitive explanation for auditory hallucinations. Proponents
of this approach propose that “cognitivism” is insufficient to explain the uniqueness of
human experience, and that a better approach is to try to understand the “reflexive”
relationship between the person and the person’s experience of voices (e.g. Davies, Thomas
& Leudar, 1999; Leudar, Thomas, McNally & Glinski, 1997; Thomas, Bracken & Leudar,
2004). They suggest that voice contents can only be explained in the context of each
individual’s social, cultural, history and political framework (Thomas, Bracken & Leudar,
2004), and that only investigations at this level can explain the voices’ content. Further
research is needed to investigate this proposal.
In summary, the results show that negative mood is commonly found in patients with
auditory hallucinations although it is not necessarily linked to the presence or severity of
auditory hallucinations. In patients with auditory hallucinations, depression was found to
be related to negative voice content and beliefs in malevolence and omnipotence.
Chapter 5
- 114-
However, negative voice content and negative beliefs could not fully explain the emotional
state of hallucinating patients, since their presence did not always predict whether patients
were depressed or not. Anxiety levels were not found to be associated with any of the
current factors examined in relation to auditory hallucinations. Overall, the results suggest
that voice contents and beliefs about voices are not significant determinants of, and do not
directly result from, elevated depression/anxiety reported by hallucinating patients with
schizophrenia. Finally, an attentional bias for negative material was found to be associated
with depression in hallucinating patients, although a critical analysis of the results
suggested that this bias for negative material could not fully account for negative voice
content.
Theoretical developments
A particularly interesting new development is raised by the finding of a relationship
between belief in malevolence and omnipotence and resistance activity. Resistance activity
on the BAVQ-R is measured by the following statements: “When I hear my voice, usually:
I tell it to leave me alone, I try and take my mind off it, I try and stop it, and I do things to
prevent it talking”. The same attempts at thought control have been implicated as an
etiological and maintaining factor in Obsessive Compulsive Disorder (OCD). OCD is
characterised by recurring and persistent unwanted thoughts that are actively resisted
(Purdon & Clark, 2001; Salkovskis, Richard & Forrester, 1995). It is believed that thought
control and deliberate thought suppression efforts lead to the paradoxical effect of
persistent recurrence of those unwanted thoughts. It has been found that participants
instructed to suppress thoughts about ‘white bears’ report increasing occurrence of thoughts
about white bears in a thought suppression session compared to participants who expressed
white bear thoughts prior to suppressing them (Purdon, 1999). These findings have been
incorporated into models of OCD that suggest that efforts to control intrusive obsessional
thoughts backfire by making those thoughts more accessible and by priming negative
appraisal of the thoughts (Purdon & Clark, 2001; Salkovskis, 1985, 1989).
It may be speculated that these findings are relevant to the current investigations,
since hallucinating patients claim to resist voices that are believed to be malevolent and
omnipotent. It is possible that, in this way, the actual occurrence of these beliefs comes to
play a key role in the maintenance process of auditory hallucinations. Attempts at
suppressing negative and other unwanted mental events, which may originally occur as a

Chapter 5
- 115-
result of the deficit in inhibition (see Waters et al, 2003), produce a recurrence of these
events. As a result, the motivation to suppress increases and serves as a further cue for the
intrusion, and so on. Therefore, the notion of thought suppression might lead to a clearer
understanding of the maintenance process of negative affective auditory hallucinations.
One challenge to this proposal, however, is how to explain the maintenance process of
positive/neutral hallucinations. One possibility is that positive voice contents occur
randomly as a result of the inhibitory deficit outlined in Waters et al and are not actively
suppressed, so do not tend to reoccur. Alternatively, or perhaps additionally, the
engagement activities associated with belief in benevolence, at least in some cases,
promotes the reoccurrence of future hallucinatory episodes containing positively valenced
material.
This proposal has implications for the treatment of patients with auditory
hallucinations. The finding that depression and anxiety, at least as measured by the BDI-II
and BAI respectively, were not directly associated with auditory hallucinations suggests
that treatment directed at negative affect may not always contribute towards remission of
auditory hallucinations. However, if beliefs in malevolence and omnipotence are central to
resistance activities then effective treatments should target these beliefs. This is an
approach which has had some success in the past (e.g. Chadwick & Birchwood, 1994;
Chadwick, Sambrooke, Rasch & Davies, 2000). Those authors have developed a cognitive
behaviour therapy treatment that targets the beliefs held by patients about their voices.
They propose that a weakening or loss of these beliefs reduces negative mood states and
facilitates more adaptive coping strategies. The above proposal, however, suggests that this
therapeutic approach is beneficial because a weakening of these beliefs results in
decreasing resistance activity. These suggestions, however, are purely speculative, but they
may be worthy of further investigation in future studies.
Finally, the current study showed that less than half of the schizophrenia patients had
signs of affective disorder and no single factor investigated was found to accurately predict
whether a patient would show signs of depression or anxiety. So what determines negative
affect in patients with schizophrenia with/without auditory hallucinations? One suggestion
is that the scales used in this study were not accurate or sensitive enough to capture
emotional dysfunction in these patients. In support, the use of the BDI-II to assess
depression in schizophrenia has been questioned on the grounds that it was developed to

Chapter 5
- 116-
assess depressed mood in clinical depression, and that the symptom complaints may be
different in both disorders (Lancon et al, 2001). Instead, specific scales have been
developed to evaluate symptoms of depression independently of other negative or extra-
pyramidal symptoms of schizophrenia (Addington et al, 1993). Another possibility is that
depression and anxiety are not key affective components in schizophrenia. Other negative
moods such as fear, distress or low self-esteem, may be better contributors to negative
affect in schizophrenia. Another suggestion was raised by Marengo et al (2000). In order to
explain why only some patients develop schizophrenia, Marengo and colleagues have
simply proposed various levels of vulnerability to depression, with some patients showing
low levels of vulnerability and others showing high vulnerability to depression. In support,
they showed that some patients experience recurring depressive symptoms during the
course of their illness but a subgroup of patients are resistant to depression. The data
shown in the current study could fit a vulnerability view of depression. Only further
research in the domain of negative affect and schizophrenia can shed some light into this
complex problem.

Chapter 5
- 117-
References
Addington, D., Addington, J., Maticka-Tyndale, E. (1993). Rating depression in
schizophrenia. A comparison of a self report and an observer report scale. Journal of
Nervous and Mental Disease. 181(9): 561-565.
Alpert, M., & Silvers, K. N. (1970). Perceptual characteristics distinguishing auditory
hallucinations in schizophrenia and acute alcoholic psychoses. American Journal of
Psychiatry, 127(3), 298-393.
Amieva, H., Phillips, L. H., Della Sala, S., & Henry, J. D. (2004). Inhibitory functioning in
Alzheimer's disease. Brain, 127, 949-964.
Arbuthnott, K., & Frank, J. (2000). Executive control in set-switching: residual switch cost
and task-set inhibition. Canadian Journal of Experimental Psychology, 54(1), 33-41.
Badcock, J. C., Waters, F. A. V. & Maybery, M. T (in press). Auditory hallucinations:
failure to inhibit irrelevant memories. Cognitive Neuropsychiatry.
Badcock, J. C., Michie, P. T., Johnson, L., & Combrinck, J. (2002). Acts of control in
schizophrenia: dissociating the components of inhibition. Psychological Medicine, 32,
287-297.
Baynes, D., Mulholland, C., Cooper, S. J., Montgomery, R. C., MacFlynn, G., Lynch, G.,
Kelly, C., & King, D. J. (2000). Depressive symptoms in stable chronic
schizophrenia: prevalence and relationship to psychopathology and treatment.
Schizophrenia Research, 45, 47-56.
Beck, A. (1976). Cognitive therapy and the emotional disorders. Penguin Psychology.
Beck, A. (1990). BAI . San Antonio: The Psychological Corporation.
Beck, A. (1996). BDI-II . San Antonio: The Psychological Corporation.
Beech, A., Powell, T., McWilliam, J., & Claridge, G. (1989). Evidence of reduced
'cognitive inhibition' in schizophrenia. British Journal of Clinical Psychology, 28,
109-116.
Bentall, R. (1997). The syndromes and symptoms of psychosis. Or why you can't play
'twenty questions' with the concept of schizophrenia and hope to win. In R. Bentall
(Ed.), Reconstructing schizophrenia (pp. 23-59). London: Routledge.
Birchwood, M. (2003). Pathways to emotional dysfunction in first-episode psychosis. The
British Journal of Psychiatry, 182, 373-375.

Chapter 5
- 118-
Birchwood, M., & Chadwick, P. (1997). The omnipotence of voices: testing the validity of
a cognitive model. Psychological Medicine, 27, 1345-1353.
Birchwood, M., Iqbal, Z., Chadwick, P., & Trower, P. (2000). Cognitive approach to
depression and suicidal thinking in psychosis. The British Journal of Psychiatry, 177,
516-528.
Boucart, M., Mobarek, N., Cuervo, C., & Danion, J.-M. (1999). What is the nature of
increased Stroop interference in schizophrenia. Acta Psychologica, 101, 3-25.
Brebion, G., Smith, M., Gorman, J., & Amador, X. (1996). Reality monitoring failure in
schizophrenia: The role of selective attention. Schizophrenia Research, 22, 173-180.
Brebion, G., Smith, M., Gorman, J., Malaspina, D., & Amador, X. (1998). Resistance to
interference and positive symptomatology in schizophrenia. Cognitive
Neuropsychiatry, 3, 179-190.
Calev, A., & Edelist, S. (1993). Affect and memory in schizophrenia: Negative emotion
words are forgotten less rapidly than other words by long-hospitalised schizophrenics.
Psychopathology, 26, 229-235.
Carter, D. M., Mackinnon, A., & Copolov, D. L. (1996). Patients' strategies for coping with
auditory hallucinations. The Journal of Nervous and Mental Disease, 184(3), 161-166.
Carter, D. M., Mackinnon, A., Howard, S., Zeegers, T., & Copolov, D. L. (1995). The
development and reliability of the Mental Health Research Institute Unusual
Perceptions Schedule (MUPS): an instrument to record auditory hallucinatory
experience. Schizophrenia Research, 16, 157-165.
Chadwick, P., & Birchwood, M. (1994). The omnipotence of voices - the cognitive
approach to auditory hallucinations. British Journal of Psychiatry, 164, 190-201.
Chadwick, P., & Birchwood, M. (1995). The Omnipotence of Voices II: The Beliefs About
Voices Questionnaire (BAVQ). British Journal of Psychiatry, 166, 773-776.
Chadwick, P., Lees, S., & Birchwood, M. (2000). The revised Beliefs About Voices
Questionnaire. British Journal of Psychiatry, Sept, 229-232.
Chadwick, P., Sambrooke, S., Rasch, S., & Davies, E. (2000). Challenging the
omnipotence of voices: group cognitive behaviour therapy for voices. Behaviour
Research and Therapy, 38, 993-1003.

Chapter 5
- 119-
Close, H., & Garety, P. (1998). Cognitive assessment of voices: further develoments in
understanding the emotional impact of voices. British Journal of Clinical Psychology,
37, 173-188.
Cools, R., Brouwer, W. H., de Jong, R., & Slooff, C. (2000). Flexibility, inhibition and
planning: frontal dysfunctioning in schizophrenia. Brain and Cognition, 43, 108-112.
Copolov, D. L., Seal, M. L., Maruff, P., Ulusoy, R., Wong, M. T. H., Tochon-Danguy, H.
J., & Egan, G. F. (2003). Cortical activation associated with the experience of
auditory hallucinations and perception of human speech in schizophrenia: a PET
correlation study. Psychiatry Research: Neuroimaging, 122, 139-152.
Crider, A. (1997). Perseveration in schizophrenia. Schizophrenia Bulletin, 23(1), 63-74.
Davies, P., Thomas, P., & Leudar, I. (1999). Dialogical engagement with voices: a single
case study. British Journal of Medical Psychology, 72, 179-187.
Delespaul, P., deVries, M., & van Os, J. (2002). Determinants of occurrence and recovery
from hallucinations in daily life. Society of Psychiatry and Psychiatric Epidemiology,
37, 97-104.
Dreher, J.-C., & Berman, K. F. (2002). Fractionating the neural substrate of cognitive
control processes. Proceedings of the National Academy of Sciences of the USA,
99(22), 14595-14600.
Elliott, R., McKenna, P. J., Robbins, T. E., & Sahakian, B. J. (1995). Neuropsychological
evidence for frontostriatal dysfunction in schizophrenia. Psychological Medicine, 25,
619-630.
Falloon, I. R. H., & Talbot, R. E. (1981). Persistent auditory hallucinations: coping
mechanisms and implication for management. Psychological Medicine, 11, 329-339.
Friedman, N. P., & Miyake, A. (2004). The relations among inhibition and
interference control functions: a latent-variable analysis. Journal of Experimental
Psychology: General, 133(1), 101-135.
Gooding, D.C., & Tallent, K.A. (2002) Schizophrenia patients’ perceptual biases in
response to positively and negatively valenced emotion chimeras. Psychological Medicine,
32(6), 1101-1107.
Haddock, G., McCarron, J., Tarrier, N., & Faragher, E. B. (1999). Scales to measure
dimensions of hallucinations and delusions: the psychotic symptom rating scales
(PSYRATS). Psychological Medicine, 29, 879-889.

Chapter 5
- 120-
Haila, H., Isometsa, E.T., Henriksson, M.M., Heikkinen, M.E., Marttunen, M.J., &
Lonnqvist, J.K. (1997). Suicide and schizophrenia: a nationwide psychological
autopsy study on age- and sex-specific clinical characteristics of 92 suicide victims
with schizophrenia. American Journal of Psychiatry. 154, 1235-1242.
Hertel, P. T. (2002). Cognitive biases in anxiety and depression: introduction to the special
issue. Cognition and Emotion, 16(3), 321-330.
Hustig, H. H., & Hafner, R. J. (1990). Persistent auditory hallucinations and their
relationship to delusions and mood. The Journal of Nervous and Mental Disease,
178(4), 264-267.
Johns, L. C., Hemsley, D., & Kuipers, E. (2002). A comparison of auditory hallucinations
in a psychiatric and nonpsychiatric group. British Journal of Clinical Psychology,
41(1), 81-86.
Joormann, J. (2004). Attentional bias in dysphoria: the role of inhibitory processes.
Cognition and Emotion, 18(1), 125-147.
Kay, S. R., Fiszbein, A., & Opler, L. A. (1987). The Positive and Negative Syndrome Scale
(PANSS) for Schizophrenia. Schizophrenia Bulletin, 13, 261-276.
Kopp, B., & Rist, F. (1994). Error-correcting behaviour in schizophrenia patients.
Schizophrenia Research, 13, 11-22.
Lancon, C., Auquier, P., Reine, G., Bernard, D., & Addington, D. (2001). Relationships
between depression and psychotic symptoms of schizophrenia during an acute
episode and stable episode. Schizophrenia Research, 47, 135-140.
Laplante, L., Everett, J., & Thomas, J. (1992). Inhibition through negative priming with
Stroop stimuli in schizophrenia. British Journal of Clinical Psychology, 31, 307-327.
Leudar, I., Thomas, P., McNally, D., & Glinski, A. (1997). What voices can do with words:
pragmatics of verbal hallucinations. Psychological Medicine, 27, 885-898.
MacLeod, C., & Rutherford, E. (1998). Automatic and strategic cognitive biases in anxiety
and depression. In K. Kirsner & C. Speelman (Eds.), Implicit and explicit mental
processes (pp. 468pp). Mahwah, NJ< USA: Lawrence Erlbaum Associates, Inc.
Manoach, D. S., Lindgren, K. A., Cherkasova, M. V., Goff, D. C., Halpern, E. F.,
Intriligator, J., & Barton, J. J. (2002). Schizophrenic subjects show deficient
inhibition but intact task switching on saccadic tasks. Biological Psychiatry, 51, 816-
826.

Chapter 5
- 121-
Marengo, J., Harrow, M., Herbener, E. S., & Sands, J. (2000). A prospective longitudinal
10-year study of schizophrenia's three major factors and depression. Psychiatry
Research, 97(1).
Maruff, P., Danckert, J., Pantellis, C., & Currie, J. (1998). Saccadic and attentional
abnormalities in patients with schizophrenia. Psychological Medicine, 28, 1091-1100.
McGhie, A., & Chapman, J. (1961). Disorders of attention and perception in early
schizophrenia. British Journal of Medical Psychology, 34, 103-116.
Mineka, S., & Nugent, K. (1995). Mood-congruent memory biases in anxiety and
depression. In D. L. Schacter (Ed.), Memory distortion: How minds, brains and
societies reconstruct the past (pp. 173-193). London, England: Harvard University.
Morrison, A. P., & Baker, C. A. (2000). Intrusive thoughts and auditory hallucinations: a
comparative study of intrusions in psychosis. Behaviour Research and Therapy, 38,
1097-1106.
Murphy, F. C., Sahakian, B. J., Rubinsztein, J. S., Michael, A., Rogers, R. D., Robins, T.
W., & Paykel, E. S. (1999). Emotional bias and inhibitory control processes in mania
and depression. Psychological Medicine, 29, 1307-1321.
Murray, L. A., Whitehouse, W., & Alloy, L. (1999). Mood congruence and depressive
deficits in memory: a forced-recall analysis. Memory, 7(2), 175-196.
Nathaniel-James, D. A., Brown, R., & Ron, M. (1996). Memory impairment in
schizophrenia: its relationship to executive function. Schizophrenia Research, 21, 85-
96.
Nathaniel-James, D., & Frith, C. (1996). Confabulation in schizophrenia: evidence of a new
form? Psychological Medicine, 26, 391-199.
Nelson, H. E. (1982). The National Adult Reading Test (NART): Test Manual. Windsor,
Berks: NFER-Nelson.
Nigg, J. T. (2000). On inhibition/disinhibition in developmental psychopathology: Views
from cognitive and personality psychology and a working inhibition taxonomy.
Psychological Bulletin, 126(2), 220-246.
Phillips, M. L., Drevets, W. C., Rauch, S. L., & Lane, R. (2003). Neurobiology of emotion
perception I: the neural basis of normal emotion perception. Biological Psychiatry,
54, 504-514.

Chapter 5
- 122-
Purdon, C. (1999). Though suppression and psychopathology. Behaviour Research and
Therapy, 37, 1029-1054.
Purdon, C., & Clark, D. (2001). Suppression of obsession-like thoughts in nonclinical
individuals: impact on thought frequency, appraisal and mood state. Behaviour
Research and Therapy, 39, 1163-1181.
Ross, R., Harris, J., Olincy, A., Radant, A., Adler, L., & Freedman, R. (1998). Familial
transmission of two independent saccadic abnormalities in schizophrenia.
Schizophrenia Research, 30, 59-70.
Rossell, S. L., Shapleske, J., & David, A. S. (1998). Sentence verification and delusions: a
content-specific deficit. Psychological medicine, 28, 1189-1198.
Salkovskis, P. M. (1985). Obsessional-compulsive problems: a cognitive behavioural
analysis. Behaviour, Research & Therapy, 23(5), 571.
Salkovskis, P. M. (1989). Cognitive-behavioural factors and the persistence of intrusive
thoughts in obsessional problems. Behavioural Research and Therapy, 27(6), 677-
682.
Salkovskis, P. M., Richards, H. C., & Forrester, E. (1995). The relationship between
obsessional problems and intrusive thoughts. Behavioural and Cognitive Psychotherapy,
23, 281-299.
Schnider, A., & Ptak, R. (1999). Spontaneous confabulators fail to suppress currently
irrelevant memory traces. Nature Neuroscience, 2(7), 677-681.
Schwartz, B. D., & Evans, W. J. (1999). Neurophysiologic mechanisms of attention deficits
in schizophrenia. Neuropsychiatry, Neuropsychology & Behavioural Neurology.
Silbersweig, D. A., Stern, E., C, F., & al, e. (1995). A functional neuroanatomy of
hallucinations in schizophrenia. Nature, 378, 176-179.
Siris, S. G., Addington, D., Azorin, J.-M., Fallon, I. R., Gerlach, J., & Hirsch, S. R. (2001).
Depression in schizophrenia: recognition and management in the USA. Schizophrenia
Research, 47, 185-197.
Soppitt, C. W., & Birchwood, M. (1997). Depression, beliefs, voice content and
topography: a cross sectional study of schizophrenia patients with auditory verbal
hallucinations. Journal of Mental Health, 6(5), 525-532.
Suslow, T., Roestel, C., Droste, T. Arolt, V. (2003). Automatic processing of verbal
emotional stimuli in schizophrenia. Psychiatry Research, 120(2), 131-144.

Chapter 5
- 123-
Takebayashi, H., Takei, N., & Mori, N. (2002). Unilateral auditory hallucinations in
schizophrenia after damage to the right hippocampus. Schizophrenia Research.
Thomas, P., Bracken, P., & Leudar, I. (2004). Hearing voices: a phenomenological-
hermeneutic approach. Cognitive Neuropsychiatry, 9(1/2), 13-23.
van 't Woot, M., Aleman, A., Kessels, R., Laroi, F., & Kahn, R. S. (2004). Emotional
processing in a non-clinical psychosis-prone sample. Schizophrenia Research, 68,
271-281.
Walsh, E., Harvey, K., White, I., Manley, C., Fraser, J., Stanbridge, S., & Murray, R. M.
(1999). Prevalence and predictors of parasuicide in chronic psychosis. Acta
Psychiatrica Scandinavica, 100(5), 375-382.
Waters, F. A. V., Badcock, J. C., Maybery, M. T., & Michie, P. T. (2003). Inhibition in
schizophrenia: association with auditory hallucinations. Schizophrenia Research, 62,
275-280.
Wilson, S. P., & Kipp, K. (1998). The development of efficient inhibition: Evidence from
directed-forgetting tasks. Developmental Review, 18, 86-123.
Woodruff, P. W. R. (2004). Auditory hallucinations: insights and questions from
neuroimaging. Cognitive Neuropsychiatry, 9(1/2), 73-91.
Zisook, S., McAdams, L. A., Kuck, J., Harris, J., Bailey, A., Patterson, T. L., Judd, L. L., &
Jeste, D. V. (1999). Depressive symptoms in schizophrenia. American Journal of
Psychiatry, 156, 1736-1743.

- 125 -
CONTEXT MEMORY
AND
AUDITORY HALLUCINATIONS

- 127 -
Foreword to Chapter 6 and 7
The results presented in previous chapters suggest that an impairment in intentional
inhibition is associated with the presence and severity of auditory hallucinations. Since a
failure of inhibition results in mental events intruding into consciousness, the inhibitory
deficit might account for the commonly reported complaint that auditory hallucinations are
intrusive and uncontrollable. However this impairment is clearly not enough for auditory
hallucinations to occur since inhibitory deficits are also present in conditions who do not
commonly report auditory hallucinations (i.e. Post-Traumatic Stress Disorder, Vasterling,
Braily, Constans & Sutker, 1998). Another deficit must also be present, which, when
combined with the inhibitory deficit, would result in auditory hallucinations.
The preliminary study presented in Chapter 2 has shown that, in addition to the
notion of intrusiveness, individuals vulnerable to hallucinations identify experiences which
are referred to an external agency. Since schizophrenia patients with auditory
hallucinations also attribute mental events to an external agent, it is possible that the failure
to assign mental events to the self might be a generic feature of the hallucinatory
experience. The following two chapters aim to investigate the mechanisms that are
responsible for this particular feature of the hallucinatory experience in schizophrenia.
A recent cognitive model of auditory hallucinations has proposed that the patients’
failure to identify correctly the origins of auditory hallucinations results from a fundamental
deficit in context memory (Nayani & David, 1996). In support, Johnson, Hashtroudi and
Linsay (1993) have suggested that a loss of qualitative information in memory, such as
contextual details, would make it difficulty to identify correctly the origins of mental
events. The aim of Chapters 6 and 7 is to investigate the proposal that a context memory
deficit is associated with auditory hallucinations in patients with schizophrenia.
Chapter 6 starts by investigating whether a deficit in context memory is present in
patients with schizophrenia, compared to a group of healthy controls. A new task was
developed, in which memory for events is assessed in conjunction with memory for both
the source and temporal characteristics of those events.
Chapter 7 subsequently presents the results of subgroup analyses, comparing the
performance of patients with and without auditory hallucinations on the Context Memory
task.

- 128 -
References
Johnson, M. K., Hashtroudi, S., & Lindsay, D. S. (1993). Source Monitoring. Psychological
Bulletin, 114(1), 3-28.
Nayani, T., & David, A. (1996). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & T. R. E. Barnes (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 . New York: John Wiley
& Sons Ltd.
Vasterling, J., Brailey, K., Constans, J., & Sutker, P. (1998). Attention and memory
dysfunction in post-traumatic stress disorder. Neuropsychology, 1998(12), 1, 125-
133.

- 129 -
Chapter 6
Context Memory and Binding in Schizophrenia
Abstract
The current study aimed to provide evidence for the context-memory hypothesis
which proposes that schizophrenia is linked to a deficit in retrieving contextual information
and in binding the different components of a memory together. A new task was developed
in which memory for the content of events could be assessed in conjunction with memory
for both source and temporal information. Forty-three patients with schizophrenia and 24
normal controls took part in the study. Patients were found to be less accurate in
identifying the source and temporal context of events. Furthermore, whereas controls
tended to identify correctly both source and temporal context of events, patients tended to
have a more fractionated recollection of those events. The study provides support for the
context-memory hypothesis by demonstrating that patients with schizophrenia show a
fundamental deficit in binding contextual cues together to form a coherent representation of
an event in memory.
Waters, FAV, Maybery, MT, Badcock, JC, Michie, PT. (2004) Context Memory and
Binding in Schizophrenia, Schizophrenia Research, 68(2-3), 119-125.

Chapter 6
- 130 -
Schizophrenia has increasingly been linked to a deficit in integrating contextual
information in memory and several authors have proposed that many of the cognitive
deficits observed in schizophrenia result from an impairment in the ability to process
contextual information (e.g. Bazin, Perruchet, Hardy-Bayle, & Feline, 2000, Cohen &
Servan-Schreiber, 1992; Rizzo, Danion, Van der Linden, & Grange, 1996a; Servan-
Schreiber, Cohen, & Steingard, 1996). In the sphere of long-term memory research, a
context-memory hypothesis (e.g. Danion, Rizzo & Bruant, 1999; Rizzo et al, 1996a,b;
Schwartz et al, 1991) suggests that patients with schizophrenia have a deficit in binding
together different contextual information to form an intact memory representation.
In episodic memory research, a distinction between the 'content' and 'context' of
memory events is often made, the content referring to the event itself while information
about context usually refers to extrinsic features that are not part of the stimulus itself, such
as the source of an action or its temporal context. There is evidence that memory for the
content and context of an event may be functionally dissociable and may rely on different
anatomical regions of the brain (Cabeza et al, 1997; Nyberg et al, 1996). However,
memories require not only the retention of particular features but also the cognitive
processes for binding the features together. Binding processes combine different elements
into a complete memory representation and provide the knowledge that certain features
belong together (Chalfonte & Johnson, 1996).
Evidence supporting the context memory hypothesis in schizophrenia rests primarily
on findings of impairment in source recognition (Danion et al, 1999; Keefe, Arnold, Bayen,
& Harvey, 1999; Vinogradov et al, 1997), in judgements of temporal order as assessed by
recency discrimination tasks (Rizzo et al, 1996a; Schwartz et al, 1991) and in memory for
spatial location (Rizzo et al, 1996b). While this hypothesis is supported by demonstrations
that patients perform poorly on tasks assessing individual contextual cues, more convincing
evidence for a general binding impairment would lie in demonstrating that patients are not
able to reconstruct a complex memory occurrence based on a combination of contextual
cues.
The current study aimed to test directly the hypothesis that schizophrenia is linked to
a deficit in binding different elements in memory together. A new task was developed
where memory for events could be assessed in conjunction with memory for both source
and temporal information: each participant watched or performed pairings of common

Chapter 6
- 131 -
household objects in two different sessions. The task therefore tested recognition for
specific events, the source of these events, when the events occurred and the ability to bind
the two contextual features together.
Method
Participants
Forty-three patients with a DSM-IV diagnosis of schizophrenia were selected from a
psychiatric hospital in Perth, Western Australia. Their demographic and clinical data are
presented in Table 1. All patients were receiving typical, atypical or a combination of
neuroleptics. A control group comprised 24 individuals with no personal or first-degree
family history of psychiatric illness was then selected from the community. Exclusionary
criteria for all participants included a history of head injury and neurological illness.
Patients and controls did not differ in premorbid IQ as measured with the National Adult
Reading Test (Nelson, 1982), age or educational level. The study was approved by the
University of Western Australia and Graylands Hospital Ethics Committees and signed
informed consent was obtained from all participants.
Table 1
Demographic and clinical data for patients with schizophrenia and healthy control
participants (means and standard deviations)
Controls (n = 24) Patients (n = 43) Group
Comparisons p
Age 34.67 (8.81) 36.73 (8.41) t = .95 .34
Gender 20 M, 4 F 35 M, 7 F
Handedness 19 R, 4 L 35 R, 6 L
Years Education 11.75 (1.89) 10.97 (1.97) t = 1.55 .12
NART 103.62 (4.75) 100.21 (9.32) t = 1.66 .10
Age of first hospitalisation - 23.09 (5.80)
Number of admissions - 9.35 (7.79)
Duration of illness (years) - 13.64 (8.14)
Chlorpromazine equivalent - 942.78 (445.35)

Chapter 6
- 132 -
Memory for context task (adapted from Conway & Dewhurst, 1995; Danion et al, 1999;
Huppert & Piercy, 1978).
Participants watched or performed pairings of two sets of 24 household objects over
two sessions 30 minutes apart.
Materials: There were 48 common household objects. Half were allocated to the
'watch' action (participants watched the experimenter pair the objects) and half to the
'perform' action (participants performed the pairing themselves). A series of cards provided
instructions to position objects next to one another or to watch the experimenter perform
the action. In the recognition test, 24 pairs of objects were presented: 16 pairs were kept in
their original combination (“intact pairs”), and 8 pairs were objects that were re-paired in
new combinations (“rearranged pairs”). No new objects were added. Objects in new
combinations were kept within the same action sequence (watch/perform) and presentation
session (1 or 2).
Procedure: In the first session, participants were shown 24 common objects set out
randomly on a table. They were told that they would pair objects together or watch the
experimenter pair objects together in two different sessions and were instructed that they
should try to remember which objects went together, who paired them and in which
session, for a test later on. Thirty minutes after the first session the second session took
place. A different set of 24 objects was presented but the procedure remained the same.
Five minutes after the end of the second session, the recognition test was administered
verbally. Pairs of objects were read out individually. Participants indicated whether each
pair was an intact or rearranged combination, and for pairs judged as being intact they had
to specify who performed the pairing (self/experimenter), and when (session 1/2).
Data analysis
Multinomial modelling (Batchelder & Riefer, 1990) and signal-detection methods
(Hilford, Glanzer, Kim & DeCarlo, 2002) are alternative analytic techniques advocated for
source memory paradigms, with each providing estimates of sensitivity to item information,
sensitivity to source information and guessing biases. We adopted signal-detection
methods for two reasons. First, substantial reviews of evidence concerning both item
recognition (Kinchla, 1994) and source recognition (Hilford et al, 2002) favour the
predictions of signal detection models over the predictions of threshold models, of which

Chapter 6
- 133 -
multinomial models are instances. Second, multinomial modelling is not suited to our task
design. In contrast to traditional source monitoring designs, our rearranged test pairs were
not novel: each consisted of two objects that had been encountered previously in the same
study session and in relation to the same source. This meant that the rearranged pairs could
not be used in the way new items are used in traditional designs when estimating
parameters of multinomial models. Therefore we applied signal-detection analyses (with
corrections recommended by Snodgrass & Corwin, 1988) to the recognition of intact versus
rearranged pairs, to judgments of source, and to temporal judgments. These analyses
provided independent estimates of discrimination accuracy and bias for each type of
judgement.
Results
Analyses of memory for content are presented initially followed by analyses of
context judgements. We then report comparisons of the patient group to a low-scoring
subgroup of controls. In the last analysis, binding is investigated by examining whether
participants had intact memory for the conjunction of the contextual cues. Table 2 shows a
detailed breakdown of responses and Table 3 shows proportions correct data for object pair
recognition and for source and temporal judgments for correctly recognized intact pairs,
and results of binding investigations.
Intact versus rearranged object pair recognition
The proportions of object pairs correctly recognized as intact or rearranged were subjected
to an analysis of variance (ANOVA) with participant group as a between-subjects factor
and intact versus rearranged object pairs as a within-subjects factor. Recognition accuracy
was lower for the patient group compared to the control group, F(1, 65) = 17.82, p < .001.
Recognition accuracy did not differ significantly for intact versus rearranged stimuli, F(1,
65) = .49, p = .48, nor was the interaction significant, F(1, 65) = 2.37, p = .12.
Discrimination accuracy was higher for controls (M = 1.03, SD = .91) than for patients (M
= .37, SD = .55), t(65) = 3.66, p < .001, although both groups were significantly better than
chance, smaller t(42) = 4.28, p < .01. The group difference in response bias (controls: M =
1.05, SD = .76; patients: M = 1.24, SD = .58) was not significant, t(65) = 1.11, p = .26.

Chapter 6
- 134 -
Table 2
Number of responses (means and standard deviations) for source and temporal judgements
for controls and patients
Responses1
SOURCE JUDGEMENTS Intact-Performed Intact-Watch Rearranged
CONTROLS
Test stimuli:
Intact – Performed
Intact – Watched
Rearranged
5.45 (1.55)
.37 (.71)
1.33 (1.27)
1.0 (1.10)
5.33 (2.01)
1.54 (1.41)
1.54 (1.47)
2.29 (1.65)
5.12 (2.07)
PATIENTS
Test stimuli:
Intact – Performed
Intact – Watched
Rearranged
3.51 (2.24)
.51 (.79)
1.11 (1.05)
1.39 (1.17)
3.39 (2.00)
2.09 (1.68)
3.09 (2.05)
4.09 (2.00)
4.79 (2.23)
TEMPORAL JUDGEMENTS Intact-Session 1 Intact-Session 2 Rearranged
CONTROLS
Test stimuli:
Intact – Session 1
Intact – Session 2
Rearranged
5.00 (1.71)
1.29 (1.42)
1.45 (1.31)
.95 (.95)
4.91 (2.08)
1.41 (1.28)
2.04 (1.51)
1.79 (1.81)
5.12 (2.07)
PATIENTS
Test stimuli:
Intact – Session 1
Intact – Session 2
Rearranged
2.32 (1.82)
2.23 (2.12)
1.83 (1.67)
1.46 (1.36)
2.76 (2.07)
1.37 (1.30)
4.20 (2.05)
3.00 (2.01)
4.79 (2.23)
1 Out of a possible 8 per condition/row. The underlined scores represent the number of
correct responses per condition.

Chapter 6
- 135 -
Table 3
Means and standard deviations of (1) proportions correct for object pair recognition and
for source and temporal judgements for correctly recognized intact pairs, and (2)
proportions of correctly recognized intact pairs for which 'who & when' , 'who only', 'when
only' and 'neither' were recognised
Controls Low Controls Patients
M SD M SD M SD
1. Content and context memory judgements
Object pair recognition .69 .22 .63 .22 .57 .25
Source judgements .88 .12 .88 .13 .75 .17
Temporal judgements .81 .14 .81 .12 .57 .24
2. Binding of source and temporal information
Who & When 0.73 .19 0.70 .18 0.41 .23
Who only 0.15 .11 0.17 .12 0.31 .22
When only 0.08 .10 0.10 .14 0.14 .12
Neither 0.03 .05 0.01 .03 0.12 .17
Source and temporal judgments
Participants provided source and temporal judgments only for stimulus pairs they
judged to be intact so analyses of context recognition were restricted to correctly
recognized intact stimulus pairs. For these pairs, the proportions of source and temporal
judgements that were correct were calculated for each participant. These proportions were
then subjected to an ANOVA with participant group as a between-subjects factor and
context (source versus temporal) as a within-subjects factor. There was a significant main
effect of group, F(1, 64) = 23.84, p < .01, indicating that controls were more accurate in
recalling the source or temporal context of an event compared to patients. The effect of
context was also significant, F(1, 64) = 14.64, p < .01, with source being identified
correctly more often than temporal context. The interaction was not significant, F(1, 64) =
2.59, p = .11.

Chapter 6
- 136 -
Discrimination accuracy values calculated in separate signal detection analyses for
source and temporal information1 were subjected to ANOVA. Discrimination accuracy was
higher overall for controls (M = 1.86, SD = .87) than for patients (M = .82, SD = 1.03), F(1,
65) = 27.36, p < .001. The effect of context was also significant, F(1, 65) = 19.32, p < .001,
but the interaction was not, F(1, 65) = 2.18, p = .14.
An analysis of bias for source (i.e. the preference to identify stimuli as self-paired
rather than experimenter-paired) revealed a nonsignificant difference between controls (M
= 1.52, SD = .74) and patients (M = 1.32, SD = .67), t(65) = 1.10, p = .27. An analysis of
bias for temporal context (i.e. the preference to identify stimuli as having been presented in
session 1 rather than session 2) also showed a nonsignificant difference between controls
(M = 1.08, SD = .63) and patients (M = 1.24, SD = .69), t(65) = .90, p = .37.
Low-functioning controls
Direct comparisons of contextual memory between patients and controls are not
entirely satisfactory since overall patients recalled significantly fewer intact object pairs
than controls. Consequently, it is not clear whether the deficit in context memory is due to
a specific deficit in schizophrenia or is present in all individuals with poor memory. In
order to examine this possibility, controls with high levels of recognition accuracy for intact
object pairs were removed and ten participants remained with a mean level of recognition
accuracy on intact pairs (M = .58, SD = .08) that was similar to that of patients (M = .54, SD
= .22).
The proportions of object pairs correctly recognized as intact or rearranged were
subjected to ANOVA with participant group as a between-subjects factor. There were no
significant effects in this analysis (the main effect of group yielded F(1, 51) = 2.97, p =
.09). In addition, discrimination accuracy did not differ significantly for the low-
functioning controls (M = .78, SD = .88) and patients (M = .37, SD = .55), t(51) = 1.82, p =
.07, nor did bias (controls: M = 1.64, SD = .82; patients: M =1.24, SD = .58), t(51) = 1.83, p
= .07.
1 For the analysis of source judgments, correct source identification for self-paired stimuli constituted hits, and incorrect source identification of experimenter-paired stimuli constituted false alarms. For the analysis of temporal judgments, correct temporal judgments for session-1 stimuli constituted hits, and incorrect temporal judgments for session-2 stimuli constituted false alarms. Outcomes were unchanged when alternative analyses (i.e. in which correct identification of experimenter-paired stimuli constituted hits in the analysis of source, and correct identification of session-2 stimuli constituted hits in the analysis of temporal judgments) were conducted.

Chapter 6
- 137 -
Table 3 shows that the performance of the low-functioning controls in identifying
source and temporal context was almost identical to the broader control group; although
they recalled fewer than 60% of all intact pairs correctly, those object pairs were nearly
always accompanied by correct source and temporal recollection. An ANOVA conducted
on the accuracy of source and temporal context recognition yielded a significant main
effect of group, F(1, 50) = 12.02, p < .01, showing that the low-functioning controls were
more accurate in recalling the context of an event compared to patients. The effect of
context was significant, F (1, 50) = 6.12, p < .01, but the interaction was not, F (1, 50) =
1.16, p = .28.
Discrimination accuracy of context judgements was also subjected to ANOVA. The
analysis confirmed that discrimination accuracy for context judgments was higher for low-
functioning controls than for patients, F(1, 51) = 10.50, p < .01. Analyses of bias values
again failed to reveal any group differences for source or temporal judgements (all p > .37).
These results show that although the low functioning controls had intact object pair
recognition comparable to that of the patients they still recalled source and temporal
context significantly more often than patients.
Binding of source and temporal information
In this section, binding ability was examined by investigating whether patients had an
intact memory for all contextual cues. This was assessed by investigating how many
contextual features were recalled in conjunction with each correctly recognized intact
event. Four variables extracted were the proportions of object pairs: (1) where both source
and temporal information were correctly retrieved ('who & when'), (2) where source only
was correctly retrieved (‘who only’), (3) where temporal information only was correctly
retrieved (‘when only’), and (4) where neither source nor temporal information was
correctly retrieved (‘neither’). A 2 (patients vs. controls) x 3 (context: 'who only' vs. ‘when
only' vs. 'who & when') ANOVA was performed. Proportions for 'neither' were not
included to prevent collinearity problems arising from using all four proportions, which
would sum to one. There were significant main effects of context, F(1, 65) = 158.21, p <
.001, and group, F(1, 65) = 8.40, p < .01, and a significant interaction, F(1, 65) = 25.62, p
< .001. Table 3 shows that, in controls, correct item recognition was accompanied by
retrieval of both contextual cues approximately three quarters of the time. Patients, by
contrast, retrieved correctly both source and temporal features much less than half the time

Chapter 6
- 138 -
with the majority retrieving only one or the other contextual feature, or none at all. T-tests
confirmed that patients differed from controls for each of the four recognition variables,
smallest t(65) = 2.11, p < .05. These results support the hypothesis that patients have a
deficit in binding individual features together. Table 3 also shows that the performance on
source and temporal judgements of low-functioning controls was almost identical to the
control group before the high-scoring individuals were removed and thus that poor item
recognition is not necessarily linked to a decrease in binding efficiency.
Demographic and clinical factors
No significant correlations were found between object pairs, source or temporal
recognition conditions and age, NART scores, duration of illness, chlorpromazine dosage
equivalents or number of admissions.
Discussion
The current study investigated whether schizophrenia was associated with a deficit in
binding contextual cues together. Firstly, at the level of content and individual contextual
features, patients recognized significantly fewer object pairs than controls and were less
accurate in recalling the source and temporal context of events. These results are consistent
with some findings that episodic memory is impaired in schizophrenia (e.g. Gur, Moelter,
& Ragland, 2000) and that schizophrenia is also associated with source and temporal
context deficits (Danion et al, 1999; Keefe et al., 1999; Rizzo et al., 1996a; Vinogradov et
al., 1997). Furthermore, although discrimination accuracy was lower for patients than
controls, the results showed that this was not linked with an unusual bias in responding in
the patient group. Secondly, the results suggested that schizophrenia is associated with an
impairment in combining contextual cues together to form an integrated representation of
an event in memory. While controls tended to retrieve all the features of events, patients
tended to have a more fractionated recollection of these events, retrieving only individual
features in isolation or none at all. This points to an abnormality in the ability to bind
together all the original components of an experience. Furthermore the current findings
were strengthened by the comparison of the patients' performance with that of controls who
also performed poorly on content memory. Although the lower-functioning controls had
low recognition accuracy for intact object pairs, source and temporal context judgments and

Chapter 6
- 139 -
binding abilities were still intact, suggesting that the deficit in binding is specific to patients
with schizophrenia and is not a general feature of participants with poor content memory.
In summary, the study showed that patients had a disproportionately severe deficit in
combining contextual cues in memory. This is the first demonstration of such a deficit in
schizophrenia and provides direct evidence for theories of schizophrenia that posit a deficit
in context memory and relational binding (Rizzo et al., 1996a,b; Schwartz et al., 1991).
The results are also consistent with similar theories of schizophrenia that propose a deficit
in integrating contextual information, as defined by background information temporarily
held in mind to mediate an appropriate response (Bazin et al, 2000; Cohen & Servan-
Schreiber, 1992; Servan-Schreiber et al, 1996).
What underlies this poor performance in contextual memory and binding? Johnson
and colleagues' (1993, 1994) source-monitoring framework posits that memory records are
inferred on the basis of available cues and other decision processes and therefore that a lack
of qualitative information and poor decision-making processes would contribute to poor
judgements about the origins of memories. Similarly, binding ability depends on encoding
processes and the ability to 'reactivate' information based on inferences and other cognitive
processes (Chalfonte & Johnson, 1996). This view would be consistent with findings from
the current patient group since schizophrenia has often been linked to deficient encoding
(Gur et al., 2000) and some common symptoms have been linked to a lax criterion in
responding ( Baker & Morrison, 1998).
Although contextual memory and binding are discussed separately in this paper, they
are not separate constructs. Contextual memory depends on the binding of each contextual
cue to the content of the event and thus impaired binding ability would result in impaired
contextual memory (Chalfonte & Johnson, 1996). However, separation of these processes
in the current study was necessary to determine whether schizophrenia is linked to a
specific impairment in retrieving a particular type of context or in binding the different
contextual features together.
In conclusion, the current study showed that schizophrenia is linked to a deficit in
binding contextual cues together to form a whole representation of an episode in memory.
Complex event memories are central for a sense of who we are and our place in relation to
others. Such a deficit is consistent with the view that schizophrenia is linked to

Chapter 6
- 140 -
dysfunctional integration as proposed by the disconnection hypothesis of schizophrenia
(e.g. Friston, 1999).
Acknowledgements
The authors wish to thank particularly all the participants of this study, Andrew Heathcote
for his very helpful statistical advice, David Castle for his training on psychiatric scales and
Danny Rock for his invaluable help in recruiting patients.

Chapter 6
- 141 -
References
Baker, C. A., & Morrison, A. P. (1998). Cognitive processes in auditory hallucinations:
attributional biases and metacognition. Psychological Medicine, 28, 1199-1208.
Batchelder, W.H. & Riefer, R.M. (1990) Multinomial processing models of source
monitoring. Psychological Review, 97(4), 548-564.
Bazin, N., Perruchet, P., Hardy-Bayle, M., & Feline, A. (2000). Context-dependent
information processing in patients with schizophrenia. Schizophrenia Research, 45(1-
2), 93-101.
Cabeza, R., Mangels, J., Nyberg, L., Habib, R., Houle, S., McIntosh, A. R., & Tulving, E.
(1997). Brain regions differentially involved in remembering what and when: A PET
study. Neuron, 19, 863-870.
Chalfonte, B. L., & Johnson, M. K. (1996). Feature memory and binding in young and
older adults. Memory and Cognition, 24(4), 403-416.
Cohen, J. D., & Servan-Schreiber, D. (1992). A neural network model of disturbances in
the processing of context in schizophrenia. Psychiatric Annals, 22(3), 131-136.
Conway, M. A., & Dewhurst, S. A. (1995). Remembering, Familiarity, and Source
Monitoring. The Quarterly Journal of Experimental Psychology, 48A(1), 125-140.
Danion, J.M., Rizzo, L., & Bruant, A. (1999). Functional mechanisms underlying impaired
recognition memory and conscious awareness in patients with schizophrenia.
Archives of General Psychiatry, 56(7), 639-644.
Friston, K. J. (1999). Schizophrenia and the disconnection hypothesis. Acta Psychiatrica
Scandinavica, 99(Suppl. 395), 68-79.
Gur, R. C., Moelter, S. T., & Ragland, J. D. (2000). Learning and memory in
schizophrenia. In T. Sharma & P. Harvey (Eds.), Cognition in Schizophrenia:
Impairments, importance and treatment strategies (pp. 73-92). Oxford: Oxford
University Press.
Hilford, A., Glanzer, M., Kim, K., & DeCarlo, L.T. (2002). Regularities of source
recognition: ROC analysis. Journal of Experimental Psychology: General, 131(4),
494-510.
Huppert, F., & Piercy, M. (1978). The role of trace strength in recency and frequency
judgements by amnesic and control subjects. Quarterly Journal of Experimental
Psychology, 30, 347-354.

Chapter 6
- 142 -
Keefe, R. S. E., Arnold, M. C., Bayen, U. J., & Harvey, P. D. (1999). Source monitoring
deficits in patients with schizophrenia: a multinomial modeling analysis.
Psychological Medicine, 29, 903-914.
Kinchla, R.A. (1994). Comments on Batchelder and Riefer's multinomial model for source
monitoring. Psychological Review, 101, 166-171.
Johnson, M. K., Hashtroudi, S., & Lindsay, D. S. (1993). Source Monitoring. Psychological
Bulletin, 114(1), 3-28.
Johnson, M. K., Kounios, J., & Reeder, J. A. (1994). Time-course studies of reality
monitoring and recognition. Journal of Experimental Psychology: Learning, Memory
and Cognition, 20(6), 1409-1419.
Nelson, H. E. (1982). The National Adult Reading Test (NART): Test Manual. Windsor,
Berks: NFER-Nelson.
Nyberg, L., McIntosh, A. R., Cabeza, R., Habib, R., Houle, S., & Tulving, E. (1996).
General and specific brain regions involved in encoding and retrieval of events:
What, where and when. Proceedings of the National Academy of Science, 93, 11280-
11285.
Rizzo, L., Danion, J.-M., Van der Linden, M., & Grange, D. (1996a). Patients with
schizophrenia remember that an event has occured, but not when. British Journal of
Psychiatry, 168, 427-431.
Rizzo, L., Danion, J.-M., Van Der Linden, M., Grange, D., & Rohmer, J.-G. (1996b).
Impairment of memory for spatial context in schizophrenia. Neuropsychology, 10(3),
376-384.
Schwartz, B. L., Deutsch, L. H., Cohen, C., Warden, D., & Deutsch, S. I. (1991). Memory
for temporal order in schizophrenia. Biological Psychiatry, 29, 329-339.
Servan-Schreiber, D., Cohen, J., & Steingard, S. (1996). Schizophrenic Deficits in the
processing of context: A test of a theoretical model. Archives of General Psychiatry,
53(12), 1105-1112.
Snodgrass, J.G. & Corwin, J. (1988) Pragmatics of measuring recognition memory:
Applications to dementia and amnesia. Journal of Experimental Psychology:
General, 117(1), 34-50.

Chapter 6
- 143 -
Vinogradov, S., Willis-Shore, J., Poole, J. H., Marten, E., Ober, B. A., & Shenaut, G. K.
(1997). Clinical and Neurocognitive aspects of source monitoring errors in
schizophrenia. American Journal of Psychiatry, 154(11), 1530-1537.

- 145 -
Chapter 7
Context memory and auditory hallucinations
Abstract
Waters, Maybery, Badcock and Michie (2004) have shown that a deficit in context
memory and binding is present in schizophrenia. According to Johnson, Hashtroudi and
Linsay (1993), this loss of information would make it difficulty to identify correctly the
origins of mental events. Since patients with auditory hallucinations incorrectly attribute
hallucinated events to an external agent, the aim of the current study is to investigate
whether patients with auditory hallucinations have particularly impaired context memory
compared to patients without hallucinations. The performance of patients with and without
auditory hallucinations on the Context Memory task (Waters et al, 2004) was compared.
The results show that significantly more patients with auditory hallucinations have a deficit
in some form of memory for context (source and/or temporal context) compared to patients
without auditory hallucinations, although the deficit was not found to be specific to patients
with auditory hallucinations.

Chapter 7
- 146 -
Auditory hallucinations are often described as comprising a mixture of different
phenomenological features. One critical feature is that the experience is perceived to
originate from another agency. In individuals vulnerable to auditory hallucinations,
experiences are also referenced to an external agency (Waters, Badcock, Maybery &
Michie, 2003), suggesting that it may be a generic feature of the hallucinatory experience.
Why are auditory hallucinations attributed to an external agent? Nayani and David
(1996a) have proposed that auditory hallucinations are memories of speech fragments that
are not recognized because they have lost the contextual details that would allow them to be
correctly situated in time, in place and in person. In particular, they proposed that there is a
disorder of the relationship between “mental events, time and self” (p. 363), resulting in a
failure to identify the origins of memories. The contents of these memories would be
retained in the absence of identifying features, so that an individual may correctly report
that the voice of another is being heard, but often cannot identify its source nor situate it in
its correct timeframe.
There is empirical evidence to support the suggestion that source memory is impaired
in patients with auditory hallucinations compared to non hallucinating schizophrenia
patients (e.g. Baker & Morrison, 1998; Brebion, Smith, Gorman & Amador, 1996; Brebion,
Amador, David, Malaspina, Sharif & Gorman, 2000; Franck et al, 2000), and in normal
individuals who score high on a predisposition to hallucinations scale relative to low
scorers (Rankin & O’Carroll, 1995). Apart from investigations regarding the source of
memories, there has been no direct investigation of whether patients with hallucinations
also suffer from a deficit in other contextual details, such as temporal information.
However, Brebion, Gorman, Amador, Malaspina and Sharif (2002) provided indirect
evidence for this proposal by interpreting their finding of list intrusions in a free-recall
memory task as an impairment in the ability to remember the temporal context of the
production of words. No studies, to date, have examined processing of multiple contextual
information in patients with auditory hallucinations and the ability to bind this together
with an event in memory.
The current study entails a reanalysis of the results presented in Waters, Maybery,
Badcock and Michie (2004), in which we showed that patients with schizophrenia have a
fundamental deficit in binding contextual cues together to form a coherent representation of
an event in memory. In particular, the aims of the current study are to 1) examine whether

Chapter 7
- 147 -
patients with hallucinations would show a deficit in remembering individual contextual
cues, and particularly the source of events in memory and the temporal context of those
events, and 2) examine whether context binding generally, as defined by a deficit in source
and/or temporal context, is particularly impaired in patients with current auditory
hallucinations compared to those without.
Method
Participants
Forty-three patients with a DSM-IV diagnosis of schizophrenia were selected from a
psychiatric hospital in Perth, Western Australia. Patients currently experiencing
hallucinations were selected on the basis of having experienced auditory hallucinations on
at least half of the days during the preceding four weeks, as assessed by self-reports and
case note reviews (“Current AH”, N = 19). Other schizophrenia patients who did not fit
this criterion were assigned to the non-hallucinating group (“Non AH”, N = 24, including 4
individuals with no history of auditory hallucinations). Exclusionary criteria included a
history of head injury and neurological illness. See Table 1 for demographic and clinical
descriptions of these patient groups and statistical tests comparing the two. The study was
approved by the University of Western Australia and Graylands Hospital Ethics
Committees and signed informed consent was obtained from all participants.
Tasks
Memory for context task (adapted from Conway & Dewhurst, 1995; Danion et al, 1999;
Huppert & Piercy, 1978; as used by Waters et al, 2004).
Participants watched or performed pairings of two sets of 24 household objects over
two sessions 30 minutes apart.
Materials: There were 48 common household objects. Half were allocated to the
'watch' action (participants watched the experimenter pair the objects) and half to the
'perform' action (participants performed the pairing themselves). A series of cards provided
instructions to position objects next to one another or to watch the experimenter perform
the action. In the recognition test, 24 pairs of objects were presented: 16 pairs were kept in
their original combination (“intact pairs”), and 8 pairs were objects that were re-paired in
new combinations (“rearranged pairs”). No new objects were added. Objects in new

Chapter 7
- 148 -
combinations were kept within the same action sequence (watch/perform) and presentation
session (1 or 2).
Procedure: In the first session, participants were shown 24 common objects set out
randomly on a table. They were told that they would pair objects together or watch the
experimenter pair objects together in two different sessions and were instructed that they
should try to remember which objects went together, who paired them and in which
session, for a test later on. Thirty minutes after the first session the second session took
place. A different set of 24 objects was presented but the procedure remained the same.
Five minutes after the end of the second session, the recognition test was administered
verbally. Pairs of objects were read out individually. Participants indicated whether each
pair was an intact or rearranged combination, and for pairs judged as being intact they had
to specify who performed the pairing (self/experimenter), and when (session 1/2).
Assessment of General Intelligence
Premorbid intelligence was estimated using the National Adult Reading Test-revised
(Nelson, 1982).
Digits Forward (Digit Span subtest, WAIS-III, Wechsler, 1997)
This simple measure of memory span (maximum score of 14) was used as a general
measure of cognitive function.
The Beck Depression Inventory (BDI-II) and Beck Anxiety Inventory (BAI) (Beck, 1996,
1990, respectively)
These tests both have a maximum score of 21.
Results
Preliminary analyses showed that the Current AH and Non AH patients did not differ
in age, educational level, Digits Forward span scores, length of illness, number of
admissions, and Negative and General symptoms scores on the PANSS (see Table 1).
However, Current AH patients had significantly higher Positive symptoms ratings, as
measured by the PANSS, compared to Non AH patients. Current AH patients had lower
premorbid IQ scores, as measured by the NART, compared to Non AH patients and also
tended to have higher chlorpromazine dosages, although the difference did not reach the
conventional level of significance (Table 1).
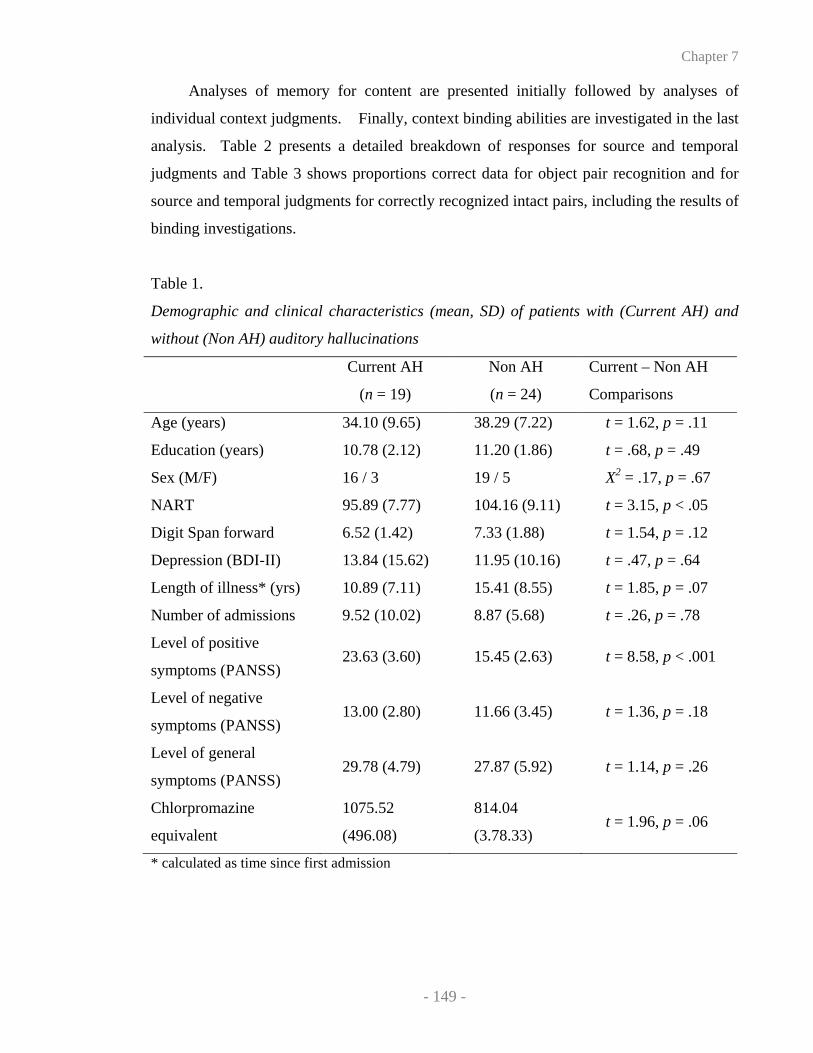
Chapter 7
- 149 -
Analyses of memory for content are presented initially followed by analyses of
individual context judgments. Finally, context binding abilities are investigated in the last
analysis. Table 2 presents a detailed breakdown of responses for source and temporal
judgments and Table 3 shows proportions correct data for object pair recognition and for
source and temporal judgments for correctly recognized intact pairs, including the results of
binding investigations.
Table 1.
Demographic and clinical characteristics (mean, SD) of patients with (Current AH) and
without (Non AH) auditory hallucinations
Current AH
(n = 19)
Non AH
(n = 24)
Current – Non AH
Comparisons
Age (years) 34.10 (9.65) 38.29 (7.22) t = 1.62, p = .11
Education (years) 10.78 (2.12) 11.20 (1.86) t = .68, p = .49
Sex (M/F) 16 / 3 19 / 5 X2 = .17, p = .67
NART 95.89 (7.77) 104.16 (9.11) t = 3.15, p < .05
Digit Span forward 6.52 (1.42) 7.33 (1.88) t = 1.54, p = .12
Depression (BDI-II) 13.84 (15.62) 11.95 (10.16) t = .47, p = .64
Length of illness* (yrs) 10.89 (7.11) 15.41 (8.55) t = 1.85, p = .07
Number of admissions 9.52 (10.02) 8.87 (5.68) t = .26, p = .78
Level of positive
symptoms (PANSS) 23.63 (3.60) 15.45 (2.63) t = 8.58, p < .001
Level of negative
symptoms (PANSS) 13.00 (2.80) 11.66 (3.45) t = 1.36, p = .18
Level of general
symptoms (PANSS) 29.78 (4.79) 27.87 (5.92) t = 1.14, p = .26
Chlorpromazine
equivalent
1075.52
(496.08)
814.04
(3.78.33) t = 1.96, p = .06
* calculated as time since first admission

Chapter 7
- 150 -
Intact versus rearranged object pair recognition
The proportions of object pairs correctly recognized as intact or rearranged were
subjected to a 2 (Current AH vs Non AH) x 2 (intact vs rearranged object pairs) ANOVA.
Overall recognition accuracy did not differ significantly for intact versus rearranged
stimuli, F(1, 41) = .84, p = .34, and the difference between groups was not significant, F (1,
41) = .20, p = .65. However, the interaction was found to be significant, F(1, 41) = 5.06, p
< .05. On proportions of object pairs correctly recognized as intact, the difference between
the groups was found to be significant, t(41) = 2.14, p < .05, with Non AH patients
recognizing significantly more intact object pairs than Current AH patients (see Table 3).
By contrast, Current AH patients tended to correctly recognize significantly more
rearranged object pairs compared to Non AH patients, t(41) = 2.01, p = .05. Signal
detection parameters (representing estimates of discrimination accuracy and bias) were
calculated but were not found to be significantly different between the two groups, t(41) =
.44, p = .66, and t(41) = .37, p = .70, respectively.
Source and temporal judgments
Participants provided source and temporal judgments only for stimulus pairs that they
judged to be intact so analyses of context recognition were restricted to correctly
recognized intact stimulus pairs. The proportions of correct source and temporal judgments
were subjected to a 2 (subgroup) x 2 (source vs temporal context) ANOVA. There was a
nonsignificant main effect of group, F (1, 40) = .21, p = .64, but there was a significant
main effect of context, with source being recalled correctly more often than temporal
context, F (1, 40) = 13.44, p < .001. The interaction was also significant, F (1, 40) = 5.75, p
< .05. Follow-up analyses showed that there was a significant difference between the
patient subgroups in source judgments, t (40) = 2.41, p < .05, with Current AH patients
making a significantly smaller number of correct source judgments compared to Non AH
patients (see Table 3). In contrast, the groups did not differ in temporal judgments, t (40) =
1.08, p = .28.
Discrimination accuracy values were calculated in separate signal-detection analyses
for source and temporal information. For source discrimination, there was a significant
difference between the two groups, t(40) = 2.36, p < .05, with Non AH patients having
significantly better discrimination accuracy than Current AH patients (see Table 3). For
temporal discrimination, there was no significant difference between Current AH and Non

Chapter 7
- 151 -
AH patients, t(40) = .68, p = .50. The analysis of bias for source (the preference to identify
stimuli as experimenter-paired rather than self-paired) showed a nonsignificant difference
between the patient subgroups, t(40) = .08, p = .93. Analysis of bias for temporal context
(the preference to identify stimuli as having been presented in session 1 rather than session
2) showed a nonsignificant difference between Current AH and Non AH patients, t(40) =
1.24, p = .21 (see Table 3).
We previously showed that schizophrenia is linked to a context memory deficit
compared to healthy controls (Waters et al, 2004). In order to examine the specificity of
this deficit to auditory hallucinations, the percentage of patients currently experiencing
hallucinations impaired on source and temporal context memory relative to healthy controls
(for details of selection procedures and demographics see Waters et al, 2004) was
calculated and then compared to the percentage of patients without hallucinations who also
exhibited the context memory failures. The percentage of patients impaired on source and
temporal memory was calculated with reference to whether scores were in excess of one
standard deviation from control group means. For comparison, the probability that an
individual would score more than one standard deviation from the mean on a normal
distribution is 15% (.158). Twelve of the 19 patients with Current AH patients (63%) were
found to have a deficit in source memory, compared to 8 of the 24 patients with Non AH
patients (33%), a difference which is significant, X2(1) = 3.79, p = .05. Eleven of the
Current AH patients (57%) and 13 of the Non AH patients (54%) had a deficit in temporal
memory, a difference which was not significant, X2(1) = .20, p = .65.
Binding of source and temporal information
Firstly, the proportions of contextual features recalled in conjunction with each
correctly recognized intact event was calculated. The measures were calculated for each
individual, including the proportions of object pairs (1) where both source and temporal
information were correctly retrieved ('who & when'), (2) where source only was correctly
retrieved (‘who only’), (3) where temporal information only was correctly retrieved (‘when
only’), and (4) where neither source nor temporal information was correctly retrieved
(‘neither’). A 2 (subgroup) x 3 (context: 'who only' vs. ‘when only' vs. 'who & when')
ANOVA was performed. Proportions for 'neither' were not included to prevent collinearity
problems arising from using all four proportions, which would sum to one.
Table 2

Chapter 7
- 152 -
Number of responses (means and standard deviations) for source and temporal judgments
for patients with (Current AH) and without (Non AH) auditory hallucinations.
Responses1
SOURCE JUDGMENTS Intact-Performed Intact-Watch Rearranged
Current AH
Test stimuli:
Intact – Performed
Intact – Watched
Rearranged
2.61 (2.09)
.50 (.70)
.83 (.70)
1.77 (1.06)
3.05 (1.69)
1.77 (1.59)
3.61 (1.94)
4.44 (1.75)
5.38 (1.85)
Non AH
Test stimuli:
Intact – Performed
Intact – Watched
Rearranged
4.33 (2.01)
.54 (.88)
1.37 (1.20)
1.16 (1.20)
3.79 (2.10)
2.41 (1.71)
2.50 (1.81)
3.66 (2.03)
4.20 (2.34)
TEMPORAL JUDGMENTS Intact-Session 1 Intact-Session 2 Rearranged
Current AH
Test stimuli:
Intact – Session 1
Intact – Session 2
Rearranged
2.33 (1.71)
1.88 (1.84)
1.50 (1.54)
1.27 (1.17)
2.44 (1.58)
1.11 (.96)
4.38 (1.91)
3.66 (1.71)
5.38 (1.85)
Non AH
Test stimuli:
Intact – Session 1
Intact – Session 2
Rearranged
2.41 (1.90)
2.58 (2.30)
2.16 (1.73)
1.66 (1.49)
3.12 (2.34)
1.62 (1.49)
3.91 (2.06)
2.29 (1.80)
4.20 (2.34)
1 Out of a possible 8 per condition/row. The underlined scores represent the number of
correct responses per condition.

Chapter 7
- 153 -
Table 3
Means and standard deviations of (1) proportions correct for intact and new object pair
recognition and for source and temporal judgments for correctly recognized intact pairs,
(2) discrimination accuracy and bias in response parameters for object pair recognition
and for source and temporal judgments and (3) proportions of correctly recognized intact
pairs for which 'who & when , 'who only', 'when only' and 'neither' were recognised.
Current AH Non AH
M SD M SD
1. Content and context memory judgments
Intact object pair recognition .46 .22 .61 .21
New object pair recognition .68 .23 .51 .30
Source judgments .68 .18 .81 .16
Temporal judgments .62 .21 .54 .26
2. Discrimination accuracy and bias for content and context memory judgments
Object discrimination accuracy .42 .56 .34 .56
Object response bias 1.27 .65 1.21 .53
Source discrimination accuracy .92 .83 1.58 .95
Bias for experimenter pairs 1.32 .50 1.34 .79
Temporal discrimination accuracy .51 1.03 .27 1.20
Bias for session 1 1.09 .54 1.36 .79
2. Binding of source and temporal information
Who & When .42 .20 .44 .27
Who only .25 .20 .36 .22
When only .20 .13 .10 .10
Neither .11 .09 .08 .11

Chapter 7
- 154 -
There was a significant main effect of context, F(1, 40) = 37.01, p < .001; both
contextual features were retrieved correctly more often than source judgments alone, which
were retrieved correctly more often than temporal judgments alone. However, there was a
nonsignificant main effect of group, F(1, 40) = .59, p = .44, and a nonsignificant
interaction, F(1, 40) = 1.87, p = .17. In addition, there was no significant group difference
for the proportions of ‘neither’ cases, t(40) = .74, p = .46.
Secondly, the proportions of patients impaired in source and/or temporal memory,
using the criterion of a score more extreme than one standard deviation from the mean of
Waters et al’s (2004) control group, was computed. As comparison, the probability that an
individual would score more than one standard deviation away from the means of controls
on one task or the other is 29% [Pr A or B = Pr A + Pr B – Pr (A*B) = .29]. It was found
that 17 out of the 19 patients (89.5%) with current hallucinations had a deficit in source
and/or temporal memory, compared to 15 out of 24 of patients without hallucinations
(62.5%), a difference which is significant, X2(1) = 4.05, p < .05, suggesting that
significantly more patients with auditory hallucinations had some form of memory for
context impairment compared to patients without hallucinations. Of the four patients with
no previous history of hallucinations, none showed a context memory deficit.
Specificity of deficits to auditory hallucinations and alternative explanations of
performance
Since source judgments and accuracy of intact object pair recognition were found to
be particularly impaired in patients with auditory hallucinations, the specificity of these
deficits to auditory hallucinations was tested. Correlations between accuracy of source
judgments and positive, negative and general symptom group scores from the PANSS
revealed that accuracy of source judgments was negatively correlated with severity of
positive symptoms scores, r = -.35, p < .02, but not with severity scores for any other
symptom group (all p > .33). The correlation with positive symptoms remained significant
even after hallucination ratings were subtracted from the broader set of positive symptom
ratings, r = -.35, p = .05. Accuracy of intact object pair recognition was not found to be
significantly correlated with severity scores for any of the symptom groups (p > .06). The
results also showed that proportions of correct intact pair recognition was significantly
correlated with correct source judgments, r = .40, p < .01.

Chapter 7
- 155 -
Since Seal, Crowe and Cheung (1997) argued that source memory impairments may
be due to poor verbal intelligence, correlations were carried out to examine the relationship
between NART scores and accuracy of source judgments. The correlation was not
significant, r = .13, p = .39. NART scores were not significantly correlated with
proportions of correct intact pair recognition either, r = .06, p = .66, suggesting that poor
verbal intelligence was not the direct cause of impaired content, and source, memory recall.
Given that Current AH patients tended to have higher chlorpromazine dosage than Non AH
patients, the relationship between chlorpromazine dosage and proportions of correct object
pair recognition and accuracy of source judgments was investigated. None of the
correlations were found to be significant (smallest p = .23).
Discussion
In Waters et al (2004), we showed that patients with schizophrenia have a deficit in
context memory and binding compared to healthy controls. The current study investigated
the specificity of this deficit to auditory hallucinations. In particular, the aim of this study
was to examine whether patients with hallucinations would show a deficit in remembering
individual contextual cues in memory, and particularly the source of events in memory and
the temporal context of those events, and whether they would be particularly impaired in
context binding generally, compared to patients without hallucinations.
Firstly, patients with current hallucinations were found to be particularly impaired in
recalling the source of memories, compared to patients without hallucinations. The finding
of an association between auditory hallucinations and a source memory deficit replicates
and extends previous findings that have shown that patients with hallucinations are less
able than nonhallucinating patients to identify the source of an action or a thought (e.g.
Blackmore, Smith, Steel, Johnstone & Frith, 2000). Such a deficit actually forms the basis
of reality- and self-monitoring theories of auditory hallucinations (e.g. Frith, 1995).
However, these theories also propose that this impairment is associated with poor decision-
making in identifying the origins of memories, and in particular with a bias towards the
erroneous attribution of internal events as being real (e.g. Bentall & Slade, 1985; Rankin &
O’Carroll, 1995), and with a bias towards misattributing self-produced material to another
source (e.g. Johns & McGuire, 1999). The results from the current Context Memory task
are not compatible with this proposal; subgroup membership was not found to be associated
Chapter 7
- 156 -
with a particular response bias in object and source recognition, showing that patients with
hallucinations did not show an unusual decision criterion in content or source recognition.
Secondly, the results revealed that patients with hallucinations, compared to patients
without, were not found to be disproportionally impaired in the recall of the temporal
context of memories, suggesting that impairments in temporal memory are not related to
the presence of auditory hallucinations specifically. The results, therefore, indicate that the
temporal context deficit is present in patients with schizophrenia, irrespective of their
hallucinating status. It is important to note, however, that this does not imply that an
impairment in temporal memory does not play an important role in auditory hallucinations,
since hallucinating patients still present with this deficit compared to healthy controls. The
current results are inconsistent with Brebion et al’s proposal (2002) that temporal memory
is especially impaired in hallucinating patients. In their study, Brebion et al used the
increase in list intrusions in a memory task as an indirect index of the ability to remember
the temporal context of the production of words. By contrast, the current Context Memory
task directly assessed temporal memory and failed to find that patients with hallucinations
were relatively more impaired on this condition compared to patients without
hallucinations.
Thirdly, at the level of content memory, the results revealed that patients with
auditory hallucinations correctly recognized fewer intact object pairs, but more rearranged
pairs, compared to patients without hallucinations. The finding of an event memory deficit
in patients with auditory hallucinations replicates the results of Brebion et al (2002), who
showed that the severity of hallucinations was associated with an increasing number of
errors in a verbal memory task. The content memory deficit may be the result of deficits in
contextual memory. According to Johnson, Hashtroudi and Lindsay (1993) and Johnson
and Chalfonte (1994), the processes involved in retrieving memories include a decision
process that is reached on the basis of the availability of memories details such as
contextual information. This proposal is consistent with the current finding that a decrease
in source recognition was associated with a reduced proportion of intact object pairs
correctly recognized. It is more difficult to explain the dissociation in performance
between intact and rearranged pairs in patients with auditory hallucinations, although the
Context Memory task is a forced-choice decision paradigm so a decrease in correct intact

Chapter 7
- 157 -
object pairs may be inversely related to an increase in correct rearranged object pair
recognition.
Fourthly, the current study aimed to evaluate the proposal that auditory hallucinations
are linked to a deficit in context binding in memory. The findings revealed that almost
90%, i.e. nearly all, patients with auditory hallucinations showed a deficit in identifying the
origins of memories, as shown by deficits in either source and/or temporal memory, and
that significantly more patients with hallucinations showed this deficit compared to patients
without. These results provide strong support for Nayani and David’s (1996a) proposal
that contextual memory is impaired in patients with auditory hallucinations. However, the
current findings also demonstrated that a deficit in both source and temporal context is not
necessary for hallucinations to occur, since there was no significant difference between
patients with and without hallucinations in the proportion of objects where both source and
temporal information were correctly retrieved. Rather, it appears that missing contextual
cues in some form of memory for context, such as source or/and temporal memory, are
associated with the hallucinatory experience; for instance, sometimes the temporal context
but not the source might be lost and other times the reverse might happen, or both forms of
context might be lost. This finding is consistent with the results of a phenomenological
survey that shows that a significant proportion of patients with auditory hallucinations are
very clear about the identity of some of their voices and that 46% of verbal hallucinatory
experiences are believed to belong to people familiar in real life (e.g. relative) (Nayani &
David, 1996b).
We may speculate on the processes that contribute towards making source judgments
in patients with auditory hallucinations. Recent findings suggest that episodic memory
retains traces of both voice characteristics and words (Goldinger, 1996). Furthermore, it
has been noted that the human voice carries important information such as the affect,
gender, age and other physical characteristics of a talker (Belin, Fecteau & Bedard, 2004;
Stevens, 2004). It may, therefore, be speculated that some of the auditory sensory features
of the remembered events are retained and that patients make attributions based on
information that is recalled. However, recognition may ultimately depend on the amount
and type of information available for making source judgments. The proposal of preserved
auditory sensory features in auditory hallucinations is consistent with findings from Hunter
and Woodruff (2004) who recently described three case studies of functional auditory

Chapter 7
- 158 -
hallucinations. In all three cases, these authors noted that the patients’ auditory
hallucinations retained certain acoustic features that were present in the original signal,
providing support for the current suggestion that some elements of memory may be
preserved during the hallucinatory experience. In sum, our results suggest that context
information, as assessed by the Context Memory task which is largely based on
visuo/motor context cues, may be impaired in patients with auditory hallucinations, while
other evidence indicates that auditory sensory features in memory may be retained. An
explanation for the dissociation between impaired visuo/motor information and intact
auditory sensory information is provided by the proposal of a distinction between intrinsic
and extrinsic context information, the former referring to cues which are part to the
stimulus itself (e.g. colour of an object, pitch/prosody of a voice) and the latter referring to
information which is not part of the stimulus itself but which needs to be encoded
separately (e.g. temporal context) (Troyer & Craik, 2000). Support for a dissociation
between intrinsic and extrinsic cues has been provided by Troyer and Craik (2000), who
have found that these processes are dissociable in a study using young adults. Accordingly,
we propose that patients with auditory hallucinations have a deficit in extrinsic context, but
intact intrinsic context information. Other factors may also be relevant and this proposal
requires further investigation. However it has previously been noted that the experience of
auditory hallucinations is highly personalized (Nayani & David, 1996b). The current
suggestion leaves open the possibility that variation in the details of events from memory
contributes to variability of the hallucinatory experience from person to person.
Overall, the results showed that significantly more patients with auditory
hallucinations have a deficit in some form of memory for context than patients without.
However, the results also demonstrated that (a) 62% of patients without hallucinations
showed context binding difficulties, (b) impaired source memory was associated with
positive symptoms in general and (c) temporal memory judgments did not differ
significantly between current- and non-hallucinators. These findings lead to the conclusion
that a context memory deficit is not specific to patients with auditory hallucinations.
However, if a context memory deficit is not specific to auditory hallucinations, why are
patients without hallucinations not reporting hearing voices? The only explanation is that a
deficit in context memory, on its own, is not sufficient for auditory hallucinations to occur.
Only when combined with (at least one) other deficits (i.e. the unbidden and uncontrollable

Chapter 7
- 159 -
retrieval of auditory representations) would the symptom of auditory hallucinations become
manifest (see Badcock, Waters & Maybery, in press; Waters, Badcock, Maybery & Michie,
2003). In support, there is growing awareness that a single cognitive deficit is unlikely to
result in such a complex event (Nayani & David, 1996a) and that a combination of deficits
might be needed to explain auditory hallucinations in schizophrenia (e.g. Aleman, Bocker,
Hijman, de Haan & Kahn, 2003; Beck & Rector, 2003). In Waters, Badcock, Michie and
Maybery (2004), we explore the proposal that a combination of deficits in context memory
and intentional inhibition is critical for hallucinations to occur.
The finding that a context memory deficit is not specific to patients with auditory
hallucinations does not necessarily imply that an impairment in context memory is not a
prerequisite to auditory hallucinations. In support for the role of context memory in the
aetiology of auditory hallucinations, most of the Non AH patients have had hallucinations
in the past and none of the four patients who have never hallucinated showed context
memory deficits. Although this latter group is too small for definitive conclusions, the
results appear to indicate that context memory difficulties may be a trait-dependent marker
for auditory hallucinations. Further studies should target individuals who have no history
of hallucinations to test this proposal. The role of context memory deficits in other positive
symptoms such as delusions also deserves investigating.
The current findings of impaired context memory are also consistent with the pattern
of activated neural systems in auditory hallucinations. The frontal lobes, medial temporal
lobes and the amygdala have been linked with source and temporal context memory, and
with context memory generally (e.g. Davachi, Mitchell & Wagner, 2002; Glisky, Rubin &
Davidson, 2001; Mayes et al, 2001; Sullivan, Shear, Zipursky, Sagar & Pfefferbaum,
1997). Neural imaging of auditory hallucinations also points to the activation of the frontal
cortex, temporal cortex and hippocampal/parahippocampal cortex (McGuire et al, 1995;
Woodruff et al, 1997), and to abnormal frontal-temporal connections (Shergill, Brammer,
Williams, Murray & McGuire, 2000), supporting the role of disturbed contextual memory
deficits in auditory hallucinations of schizophrenia.
Several alternative explanations of why patients experiencing auditory hallucinations
showed these deficits may be ruled out. Group comparisons (see Table 1) for a range of
demographic factors such as age and years of education, and clinical indicators including
duration of illness, depression and number of admissions, suggested that patients with

Chapter 7
- 160 -
current hallucinations were not generally more unwell. Patients with hallucinations showed
more positive symptoms than non-hallucinators, but there were no significant differences in
negative and general (somatic) symptoms. Compared to non-hallucinators, patients with
hallucinations tended to have higher chlorpromazine equivalents and lower verbal
intelligence, although these variables did not correlate with performance on source memory
performance. In addition, Digits Forward, commonly used as a general measure of
cognitive function, was not found to be disproportionally impaired in hallucinating patients,
suggesting that they were not more cognitively impaired than patients not currently
hallucinating.
In conclusion, the results from the present study are clearly preliminary and ought to
be replicated before any definite conclusions can be drawn. An interesting and revealing
study would investigate whether the context deficits lie at the encoding, storage or retrieval
phase. This is a relevant issue because Rizzo, Danion, Van der Linden and Grange (1996)
proposed that the context memory deficit in schizophrenia stems from difficulties in the
early stages of encoding that comprise the processes responsible for establishing
associations between different features in working memory. This hypothesis was recently
supported by Burglen et al (2004) who showed that schizophrenia patients exhibited
deficits in binding object and location features in a working memory task. Future studies
should examine feature binding in working memory in patients with auditory
hallucinations.

Chapter 7
- 161 -
References
Aleman, A., Bocker, K. B. E., Hijman, R., de Haan, E. H. F., & Kahn, R. S. (2003).
Cognitive basis of hallucinations in schizophrenia: role of top-down information
processing. Schizophrenia Research, 1926, 1-11.
Badcock, J. C., Waters, F. A. V. & Maybery, M. T (in press). Auditory hallucinations:
failure to inhibit irrelevant memories. Cognitive Neuropsychiatry.
Baker, C. A., & Morrison, A. P. (1998). Cognitive processes in auditory hallucinations:
attributional biases and metacognition. Psychological Medicine, 28, 1199-1208.
Beck, A. (1990). BAI . San Antonio: The Psychological Corporation.
Beck, A. (1996). BDI-II . San Antonio: The Psychological Corporation.
Beck, A. T., & Rector, N. A. (2003). A cognitive model of hallucinations. Cognitive
Therapy and Research, 27(1), 19-52.
Belin, P., Fecteau, S., & Bedard, C. (2004). Thinking the voice: neural correlates of voice
perception. Trends in Cognitive Sciences, 8(3), 129-1355.
Bentall, R. P., & Slade, P. D. (1985). Reality testing and auditory hallucinations: A signal
detection analysis. British Journal of Clinical Psychology, 24, 159-169.
Blakemore, S., Smith, J., Steel, R., Johnstone, E., & Frith, C. (2000). The perception of
self-produced sensory stimuli in patients with auditory hallucinations and passivity
experiences: evidence for a breakdown in self-monitoring. Psychological Medicine,
30, 1131-1139.
Brebion, G., Amador, X., David, A., Malaspina, D., Sharif, Z., & Gorman, J. M. (2000).
Positive symptomatology and source-monitoring failure in schizophrenia - an analysis
of symptom specific effects. Psychiatry Research, 95, 119-131.
Brebion, G., Gorman, J. M., Amador, X., Malaspina, D., & Sharif, Z. (2002). Source
monitoring impairments in schizophrenia: characterisation and association with
positive and negative symptomatology. Psychiatry Research, 112, 27-39.
Brebion, G., Smith, M., Gorman, J., & Amador, X. (1996). Reality monitoring failure in
schizophrenia: The role of selective attention. Schizophrenia Research, 22, 173-180.
Burglen, F., Marczewski, P., Mitchell, K. J., van der Linden, M., Johnson, M. K., Danion,
J.-M., & Salame, P. (2004). Impaired performance in a working memory binding task
in patients with schizophrenia. Psychiatry Research, 125, 247-255.

Chapter 7
- 162 -
Conway, M. A., & Dewhurst, S. A. (1995). Remembering, Familiarity, and Source
Monitoring. The Quarterly Journal of Experimental Psychology, 48A(1), 125-140.
Danion, J. M., Rizzo, L., & Bruant, A. (1999). Functional mechanisms underlying impaired
recognition memory and conscious awareness in patients with schizophrenia.
Archives of General Psychiatry, 56(7), 639-644.
Davachi, L., Mitchell, J. P., & Wagner, A. D. (2003). Multiple routes to memory: distinct
medial temporal lobe processes build item and source memories. Proceedings of the
National Academy of Sciences of the United States of America, 100(4), 2157-2162.
Franck, N., Rouby, P., Daprati, E., Dalery, J., Mari-Cardine, M., & Georgieff, N. (2000).
Confusion between silent and overt reading in schizophrenia. Schizophrenia
Research, 41, 357-364.
Frith, C. (1995). Functional imaging and cognitive abnormalities. The Lancet, 346(8975),
615-620.
Glisky, R. L., Rubin, S. R., & Davidson, P. S. R. (2001). Source memory in older adults: an
encoding or retrieval problem? Journal of Experimental Psychology: Learning,
Memory and Cognition, 27(5), 1131-1146.
Goldinger, S.D. (1996). Words and voices: episodic traces in spoken word identification
and recognition memory. Journal of Experimental Psychology: Learning, Memory
and Cognition. 22(5):1166-83.
Hunter, M. D., & Woodruff, W. R. (2004). Characteristics of functional auditory
hallucinations. The American Journal of Psychiatry, 161(5), 923.
Huppert, F., & Piercy, M. (1978). The role of trace strength in recency and frequency
judgments by amnesic and control subjects. Quarterly Journal of Experimental
Psychology, 30, 347-354.
Johns, L. C., & McGuire, P. K. (1999). Verbal self-monitoring and auditory hallucinations
in schizophrenia. The Lancet, 353(9151), 469-470.
Johnson, M. K., & Chalfonte, B. L. (1994). Binding Complex Memories: the role of
reactivation and the hippocampus. In D. L. Schacter & E. Tulving (Eds.), Memory
Systems (pp. 311-350). Cambridge, MA, US: The MIT Press.
Johnson, M. K., Hashtroudi, S., & Lindsay, D. S. (1993). Source Monitoring. Psychological
Bulletin, 114(1), 3-28.

Chapter 7
- 163 -
Mayes, A., Isaac, C., Holdstock, J., Hunkin, N., Montaldi, D., Downes, J., MacDonald, C.,
Cezayirli, E., & Roberts, J. (2001). Memory for single items, word pairs and temporal
order of different kinds in a patient with selective hippocampal lesion. Cognitive
Neuropsychology, 18(2), 97-123.
McGuire, P. K., Silbersweig, D. A., Wright, I., Murray, R. M., David, A. S., Frackowiak,
R. S. J., & Frith, C. D. (1995). Abnormal monitoring of inner speech: a physiological
basis for auditory hallucinations. The Lancet, 346(8975), 596-600.
Nayani, T.H., & David, A. (1996a). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & T. R. E. Barnes (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 . New York: John Wiley
& Sons Ltd.
Nayani, T. H., & David, A. S. (1996b). The auditory hallucination: a phenomenological
survey. Psychological Medicine, 26, 177-189.
Nelson, H. E. (1982). The National Adult Reading Test (NART): Test Manual. Windsor,
Berks: NFER-Nelson.
Rankin, P. M., & O'Carroll, P. J. (1995). Reality discrimination, reality monitoring and
disposition towards hallucination. British Journal of Clinical Psychology, 34, 517-
528.
Rizzo, L., Danion, J.-M., Van der Linden, M., & Grange, D. (1996). Patients with
schizophrenia remember that an event has occured, but not when. British Journal of
Psychiatry, 168, 427-431.
Seal, M. L., Crowe, S. F., & Cheung, P. (1997). Deficits in source monitoring in subjects
with auditory hallucinations may be due to differences in verbal intelligence and
verbal memory. Cognitive Neuropsychiatry, 2(4), 273-290.
Shergill, S., Brammer, M., Williams, S., Murray, R., & McGuire, P. (2000). Mapping
auditory hallucinations in schizophrenia using functional magnetic resonance
imaging. Archives of General Psychiatry, 57(11), 1033-1038.
Stevens, A. A. (2004). Dissociating the cortical basis of memory for voices, words and
tones. Cognitive Brain Research, 18, 162-171.
Sullivan, E. V., Shear, P. K., Zipursky, R. B., Sagar, H. J., & Pfefferbaum, A. (1997).
Patterns of content, contextual and working memory impairments in schizophrenia
and nonamnesic alcoholism. Neuropsychology, 11(2), 195-206.

Chapter 7
- 164 -
Troyer, A., & Craik, F. (2000). The effect of divided attention on memory for items and
their context. Canadian Journal of Experimental Psychology, 54(3), 161-170.
Waters, F.A.V., Badcock, J.C., Maybery, M.T (2003) Revision of the factor structure of the
Launay-Slade Hallucination Scale (LSHS-R). Personality and Individual Differences,
35, 1351-1357.
Waters, F. A. V., Badcock, J. C., Maybery, M. T., & Michie, P. T. (2003). Inhibition in
schizophrenia: association with auditory hallucinations. Schizophrenia Research, 62,
275-280.
Waters, F. A. V., Badcock, J. C., Michie, P. T. & Maybery, M. T. (2004). Auditory
hallucinations in schizophrenia: Intrusive thoughts and forgotten memories.
Submitted for publication.
Waters, F.A.V., Maybery, M.T., Badcock, J.C.& Michie, P.T. (2004) Context memory and
binding in schizophrenia. Schizophrenia Research, 68(2-3), 119-125.
Wechsler, D. (1997). Wechsler Adult Intelligence Scale-III (WAIS-III) . New York: The
Psychological Corporation.
Woodruff, P., Wright, I., Bullmore, E., Brammer, M., Howard, R. J., Williams, S.,
Shapleske, J., Rossell, S., David, A. S., McGuire, P. K., & Murray, R. (1997).
Auditory hallucinations and the temporal cortical response to speech in schizophrenia:
A functional magnetic resonance imaging study. American Journal of Psychiatry.

- 165 -
AUDITORY HALLUCINATIONS: A COMBINATION OF DEFICITS IN
INTENTIONAL INHIBITION AND CONTEXT MEMORY

- 167 -
Foreword to Chapter 8
So far, the results of our investigations have identified that intentional inhibition and
context memory processes are impaired in patients with auditory hallucinations. We
proposed that the inhibitory deficit might lead to mental events intruding into
consciousness in a manner that is beyond the control of the sufferer, and that the deficit in
context memory might contribute in the attribution of mental events to an external agent.
However, a single deficit in either intentional inhibition or context memory is not
sufficient for auditory hallucinations to occur, since inhibitory impairments are also present
in clinical conditions that do not report hallucinatory experiences (e.g. Post-Traumatic
Stress Disorder), and context memory deficits also occur in schizophrenia patients,
irrespective of their hallucinatory status. These findings reflect an increasing concern in
auditory hallucination research that a single deficit is unlikely to result in such a complex
event. By contrast, the complexity of this mental phenomenon points to the suggestion that
a combination of deficits might be needed to explain it. In support, dual-deficit models
have started to emerge as an explanation of other complex symptomatology such as
delusions (e.g. Langdon & Coltheart, 2000). There has been a recent trend in suggesting a
combination of deficits in auditory hallucinations (e.g. Aleman, Böcker, Hijman, de Haan
& Kahn, 2003; Beck & Rector, 2003) but no empirical evidence has yet been put forward.
In the next chapter (Chapter 8), a new model of auditory hallucinations is presented
which differs from contemporary single-deficit cognitive accounts of auditory
hallucinations by the proposal that auditory hallucinations arise as a result of a combination
of a minimum of two deficits. We propose that there must be a failure in, at least,
intentional inhibition and context memory for auditory hallucinations to occur. The failure
in intentional inhibition produces unwanted and uncontrollable mental events which are not
recognized because they have lost the contextual cues that would facilitate recognition.
This proposal allows for nonhallucinating individuals to show a deficit on either, but not
both, of these cognitive processes. Chapter 8 presents a novel reanalysis of the data
presented in preceding studies and a review of published behavioural and neuroanatomical
evidence to support this position.
- 168 -
References
Aleman, A., Böcker, K. B. E., Hijman, R., de Haan, E. H. F., & Kahn, R. S. (2003).
Cognitive basis of hallucinations in schizophrenia: role of top-down information
processing. Schizophrenia Research, 1926, 1-11.
Beck, A. T., & Rector, N. A. (2003). A cognitive model of hallucinations. Cognitive
Therapy and Research, 27(1), 19-52.
Langdon, R., & Coltheart, M. (2000). The cognitive neuropsychology of delusions. Mind &
Language, 15(1), 184-218.

- 169 -
Chapter 8 Auditory hallucinations in schizophrenia: intrusive thoughts and forgotten memories
Abstract
Introduction. This paper presents a new cognitive model of auditory hallucinations
in schizophrenia. We suggest that auditory hallucinations are auditory representations
derived from the unintentional activation of memories and other irrelevant current mental
associations. Our model proposes that a combination of deficits in intentional inhibition
and contextual memory is critical to the experience of auditory hallucinations. The failure
in intentional inhibition produces unwanted and uncontrollable mental events which are not
recognized because they have lost the contextual cues that would normally facilitate
recognition. Method. This article amalgamates recently published data and presents a re-
analysis of the findings on 43 patients with a diagnosis of schizophrenia using a case-by-
case approach (Badcock, Waters, Maybery, Michie, in press; Waters, Badcock, Maybery &
Michie, 2003, Waters, Maybery, Badcock and Michie, 2004). Results. Almost 90% of
patients currently experiencing auditory hallucinations showed the predicted combination
of deficits on both inhibition and context memory, compared to only a third of patients
without hallucinations. Conclusions. The results of our investigations strongly support the
role of intentional inhibition and context memory in auditory hallucinations. Critical
consideration of the findings also suggests that additional cognitive processes might be
important for the expression of this symptom.
Waters, F.A.V., Badcock, J.C., Michie, P.T. & Maybery, M.T. (2004). Auditory
hallucinations in schizophrenia: intrusive thoughts and forgotten memories. Submitted for
publication.

Chapter 8
- 170 -
It has been estimated that approximately 74% of those with a diagnosis of
schizophrenia will experience auditory hallucinations during the course of their illness
(Sartorius, Shapiro & Jablensky, 1974). Traditional definitions of auditory hallucinations
suggest that they are an auditory sensory experience in the absence of external stimuli and
with the compelling sense of reality of a true perception (Gelder, Gath & Mayou, 1993).
Auditory hallucinations are not restricted to schizophrenia (Assad & Shapiro, 1986; Honig
et al, 1998; Waters, Badcock & Maybery, 2003). However, our focus is on auditory
hallucinations in schizophrenia, primarily because the mechanisms responsible for them
may vary between different populations (Frith & Dolan, 1997).
The aim of the present paper is to identify some of the cognitive processes that are
responsible for auditory hallucinations in schizophrenia. We propose a novel approach that
differs from contemporary cognitive accounts of auditory hallucinations, which are
essentially single-deficit accounts. There is a growing concern that a single deficit is
unlikely to result in such a complex event (e.g. Nayani & David, 1996a). In contrast, the
diverse phenomenology of auditory hallucinations (Nayani & David, 1996b) suggests that a
combination of deficits might be needed to explain this mental phenomenon.
Our model proposes that auditory hallucinations consist of the activation of auditory
mental events that include memories and other currently active mental associations. We
also suggest that at least two cognitive deficits must be present to explain auditory
hallucinations: a) a fundamental deficit in intentional inhibition which leads to auditory
mental representations intruding into consciousness in a manner that is beyond the control
of the sufferer; and b) a deficit in binding contextual cues, resulting in an inability to form a
complete representation of the origins of mental events. Our model posits that, as a result
of these combined deficits, mental events are experienced as involuntary and intrusive and
are not recognized because the contextual cues that would allow them to be identified
correctly are missing or incomplete. We propose that this combination of deficits can
readily account for a broad range of phenomenological characteristics of auditory
hallucinations. Our model further posits that nonhallucinating individuals (with
schizophrenia or with another clinical condition) may show a deficit on either cognitive
process, but only schizophrenia patients with auditory hallucinations will show the
combination of deficits in intentional inhibition and context memory. In this paper, we
review evidence supporting our position and present a novel reanalysis of recently

Chapter 8
- 171 -
published empirical findings using a case-by-case approach. The deficits in inhibition and
context memory will be considered in turn.
A deficit in intentional inhibition
Patients often describe their hallucinations as disturbing, unwanted and
uncontrollable (Morrison, Haddock & Tarrier, 1995; Nayani & David, 1996a). Auditory
hallucinations are reported to be intrusive because they are unintended and because patients
are often unable to escape from the experience (Carter, Mackinnon & Copolov, 1996; Close
& Garety, 1998). Intrusiveness is such a common component of auditory hallucinations
that some authors have added to current definitions of auditory hallucinations that they are
not amenable to voluntary control (e.g. David, 2004; Seal, Aleman & McGuire, 2004).
Several researchers have noted the importance of the intrusiveness and unintendedness of
the experience (e.g. Morrison, 2001; Nayani & David, 1996a). For example, Morrison and
Baker (2000) showed that schizophrenia patients with auditory hallucinations had more
intrusive thoughts compared to non-hallucinating psychotic patients and a nonpatient
control group, and that the former group of patients described their intrusive thoughts as
more uncontrollable and unacceptable than the other groups. In order to explain the
unintended and intrusive characteristic of auditory hallucinations, our model proposes that
individuals with auditory hallucinations suffer from a failure in inhibition, and in particular
in intentional inhibition.
Inhibition: definition and taxonomy
Inhibition is a basic cognitive mechanism which has been defined as a collection of
processes which allow the suppression of previously activated cognitive contents, the
clearing of irrelevant actions or attention from consciousness and the control of overt
behavior and motor movements (Harnishfeger, 1995). The process of inhibition is essential
for suppressing irrelevant thoughts, and a failure to maintain control through inhibitory
efficiency is thought to result in information that intrudes into ongoing thinking. There is a
general agreement that inhibition is not a unitary construct, but that it is better described as
a family of processes, each with its own distinct operating characteristic (e.g. Kramer,
Humphrey, Larish, Logan & Strager, 1994; Spinella, 2002, Stuss et al, 1999). Harnishfeger
and colleagues (1995; Bjorklund & Harnishfeger, 1995; Wilson & Kipp, 1995) make a
distinction between inhibitory processes that are automatic (or unintentional) and those that

Chapter 8
- 172 -
are intentional. Automatic inhibition occurs when an individual automatically suppresses
an item and is unaware that the suppression is taking place (e.g. inhibition of return). By
contrast, intentional inhibition occurs when an individual deliberately suppresses the
activation of an item after deciding it is irrelevant (e.g. Directed Forgetting tasks).
Intentional inhibition is thought to be effortful, available to conscious reflection and
available for strategic interventions (Nigg, 2000). There is recent empirical support for the
distinction between automatic and intentional processes, with studies showing dissociations
in performance between clinical populations (e.g. Amieva, Phillips, Della Sala & Henry,
2004; Nigg, Butler, Huang-Pollock & Henderson, 2002).
Inhibition deficits in auditory hallucinations of schizophrenia
Theoretical support for the suggestion that an inhibitory failure is involved in
auditory hallucinations of schizophrenia arises from studies that have shown that a failure
in inhibition results in intrusive thoughts (e.g. Enright & Beech, 1993; Kramer et al, 1994;
Vasterling, Brailey, Constans & Sutker, 1998). There is also considerable experimental
evidence that schizophrenia is linked to a deficit in inhibition (e.g. Beech, Powell,
McWilliam & Claridge, 1989; Brebion, Smith, Gorman & Amador, 1996; Crider, 1997;
Nathaniel-James, Brown & Ron, 1996). An association between the positive symptoms of
schizophrenia and a failure in inhibition has also often been proposed (e.g. Bullen &
Hemsley, 1987; Cornblatt, Lenzenweger, Dworking & Erlenmeyer-Kimling, 1985; Frith,
1979; Gray, 1998; Peters et al, 2000; Williams, 1996). In addition, there is recent indirect
evidence that there may be a breakdown of inhibitory processes in those with auditory
hallucinations. For example, Hoffman, Rapaport, Mazure and Quinlan (1999), using a
speech tracking task, showed that patients with hallucinations had misheard portions of text
as verbalizations related to their voices and made more intrusive errors when shadowing
noise-contaminated speech compared to nonhallucinating patients. These intrusions in
performance were interpreted as a breakdown in the regulation of auditory mental events.
DiGirolamo and Posner (1996) also proposed that auditory hallucinations arise because of a
hyperactive executive attentional network, leading to poor regulatory control of internal
activations and competing ideas that are then interpreted as voices. However, it should be
noted at the outset that the few studies that have directly investigated the role of inhibitory
processes in auditory hallucinations using negative priming (Peters et al, 2000) and
interference tasks (Brebion, Smith, Amador, Malaspina & Gorman, 1998) have failed to

Chapter 8
- 173 -
demonstrate any such role. However, since auditory hallucinations are consciously
experienced mental events, it is possible that they may reflect impairments in intentional
inhibitory processes rather than other forms of inhibition. Neither negative priming nor
interference control are categorized as intentional forms of inhibition (Harnishfeger, 1995).
Therefore the failure of previous studies to establish a relationship between auditory
hallucinations and inhibition may be because of the form of inhibition investigated.
New empirical support for a failure in intentional inhibition in auditory hallucinations
Recent investigations have been carried out by our research group to test the
prediction that those schizophrenia patients with auditory hallucinations suffer from a
deficit in intentional inhibition (Badcock, Waters, Maybery, Michie, in press; Waters,
Badcock, Maybery & Michie, 2003). There were two tasks assessing the intentional
suppression of cognitive events – the Hayling Sentence Completion Test (HSCT; Burgess
& Shallice, 1996) and the Inhibition of Currently Irrelevant Memories task (ICIM; Schnider
& Ptak, 1999), which require the volitional inhibition of currently active mental
associations and irrelevant memories respectively. The patient group consisted of 43
patients with schizophrenia (19 with auditory hallucinations, and 24 without, 4 of whom
had never experienced auditory hallucinations in the past) (see Table 1 for a description of
the participants). It was found that auditory hallucinations severity (as measured by the
PANSS) was significantly correlated with performance on the inhibitory conditions of the
HSCT (type A errors) and ICIM (false alarms on the last three runs) tasks, and thus linked
to a deficit in intentional inhibition. In Badcock et al (in press), we further demonstrated
that those patients who were not current hallucinating and those who had never hallucinated
showed a pattern of performance on the ICIM task that was not significantly different from
that of healthy controls, suggesting that this impairment might not be a general feature of
schizophrenia but is specifically associated with the presence of hallucinations.

Chapter 8
- 174 -
Table 1
Demographic and clinical characteristics (mean, SD) of patients with Schizophrenia
Current AH1
(n = 19)
Non AH2
(n = 24)
Never AH3
(n = 4)
Current vs. Non
AH comparisons
Age (years) 34.10 (9.65) 38.29 (7.22) 36.25 (10.84) t = 1.62, p = .11
Education (years) 10.78 (2.12) 11.20 (1.86) 12.50 (2.08) t = .68, p = .49
Sex (M/F) 16 / 3 19 / 5 2 / 2 X2 = .17, p = .67
Quick Test 93.68 (5.52) 95.54 (5.49) 98.00 (5.88) t = 1.09, p = .27
Digit Span forward 6.52 (1.42) 7.33 (1.88) 7.50 (2.08) t = 1.54, p = .12
Length of illness* 10.89 (7.11) 15.41 (8.55) 9.50 (4.20) t = 1.85, p = .07
Beck Depression
Inventory (BDI-II) 13.84 (15.62) 11.95 (10.16) 4.02 (5.30) t = .47, p = .64
Number of admissions 9.52 (10.02) 8.87 (5.68) 5.75 (4.27) t = .26, p = .78
Level of positive
symptoms (PANSS) 23.63 (3.60) 15.45 (2.63) 16.25 (3.30)
t = 8.58, p <
.001
Level of negative
symptoms (PANSS) 13.00 (2.80) 11.66 (3.45) 10.00 (2.70) t = 1.36, p = .18
Level of general
symptoms (PANSS) 29.78 (4.79) 27.87 (5.92) 27.75 (3.30) t = 1.14, p = .26
Chlorpromazine
equivalent
1075.52
(496.08)
814.04
(3.78.33)
740.50
(446.10) t = 1.96, p = .06
1 Current-AH = patients currently experiencing auditory hallucinations; 2 Non-AH = patients who have not had auditory hallucinations in the last four weeks or on less than half of the days in the last 4 weeks (includes 4 Never AH patients); 3 Never-AH = patients who have never experienced auditory hallucinations; * calculated as years since first admission.

Chapter 8
- 175 -
However, the most stringent test of whether a deficit is an essential component of
auditory hallucinations is to determine whether each and every individual currently
experiencing hallucinations exhibits the specified cognitive failure relative to other patients
with schizophrenia who do not report hallucinations. Consequently, the percentages of
patients impaired on the inhibitory tasks (HSCT type A errors or ICIM false alarms on the
last three runs, or both) were calculated with reference to whether scores were in excess of
one standard deviation from control group means. The probability that an individual would
score more than one standard deviation from the mean on a normal distribution is .158 so
the probability that an individual would score one standard deviation away from the mean
of controls on one inhibition task or another is .291 [where Pr A or B = Pr A + Pr B – (Pr A
* Pr B)]. Table 2 shows that all of the 19 patients with current auditory hallucinations
were found to have a deficit in inhibition, convincingly demonstrating the role of
intentional inhibition in the hallucinatory process. In comparison, less than half of patients
without hallucinations (45.8%) could be classified as impaired on intentional inhibition
using the above definition of impairment. This difference in frequency between the patient
groups was significant, X2(1) = 14.75, p < .001. Amongst the four patients who had never
hallucinated, only one showed such a deficit, a result that is not much different from
chance. When a more stringent criterion of two standard deviations from the mean of
controls was applied, the results showed that 84.2% of patients with hallucinations still
showed an inhibition deficit, compared to 37.5% of patients without hallucinations, a
difference that remained significant, X2(1) = 9.50, p < .01. Altogether these results
strikingly show that all patients with hallucinations showed a deficit in inhibition, with
varying degree of severity; this was not the case for the patients without auditory
hallucinations, the majority of whom did not exhibit a deficit. These observations support
the first part of our model - that a failure to inhibit current mental events and memory
representations is significantly associated with the hallucinatory experience.

Chapter 8
-176 -
Table 2
Percentage of patients impaired on the experimental tasks (as defined by scores more than
one standard deviation from that of the mean of controls)
Current AH1
(n = 19)
Non AH2
(n = 24)
Inhibition deficit
(on HSCT or ICIM or both)
100 % 45.8 %
Context memory deficit
(on source or temporal accuracy or both)
89.5 % 62.5 %
Inhibition and context deficit 89.5 % 33.3 %
1 Current-AH = patients currently experiencing auditory hallucinations; 2 Non-AH = patients who have not had auditory hallucinations in the last four weeks or on less than half of the days in the last 4 weeks (includes 4 Never AH patients).
In sum, these results demonstrate that those with auditory hallucinations showed
increasing intrusion of current mental events and other representations previously acquired
in memory, as measured by the HSCT and the ICIM respectively. We may speculate on the
involvement of the brain regions that have led to impairments on these tasks. Effective
performance on the HSCT has been linked with activation of prefrontal areas and the
anterior cingulate gyrus (Burgess & Shallice, 1996, Collette et al, 2001, Nathaniel-James,
Fletcher & Frith, 1997). The anatomical regions involved in the ICIM have been
investigated by Schnider, Treyer & Buck (2000). They found that performance on runs 2-4
provoked posterior orbitofrontal cortex (OFC) activation and other subcortical regions
contiguous with the left OFC structures: left caudate nucleus, left substantial nigra, ventral
tegmental area and right medial thalamus. In addition, the inhibitory mechanisms needed
to control distracting memories are thought to activate the prefrontal cortex and the anterior
cingulate gyrus (Levy & Anderson, 2002). Auditory hallucinations have also been linked
to abnormal activation of the prefrontal cortex including the OFC and anterior cingulate
(Lennox et al, 1999; McGuire, Shah & Murray, 1993; Silbersweig et al, 1995), and to
abnormalities in basal ganglia structures and the thalamus (Copolov et al, 2003;
Silbersweig et al, 1995; Takebayashi, Takei & Mori, 2002; Woodruff & Murray, 1994;

Chapter 8
-177 -
Woodruff, 2004), consistent with the role of disturbed intentional inhibition deficits in
auditory hallucinations of schizophrenia.
In addition to the role of inhibitory processes, the results obtained on the ICIM task
suggest that episodic memory also plays a role in the genesis of auditory hallucinations.
The relation between inhibition and memory has recently been explored in the normal
population (e.g. Anderson & Green, 2001; Conway, Harries, Noyes, Racsma’ny &
Frankish, 2000; Levy & Anderson, 2002). It is now believed that the ability to control
distracting memories is accomplished by inhibitory mechanisms, and consequently that a
failure in inhibition might help promote the formation of intrusive memories (Conway et al,
2000; Levy & Anderson, 2002). These findings suggest that more than one cognitive
process may be involved in the hallucinatory experience. Further consideration of the
current data supports this possibility since approximately 46% of those patients without
hallucinations still exhibited a deficit of intentional inhibition, indicating that such a deficit
is not sufficient for hallucinations to occur. Non-specificity of cognitive deficits is a
criticism often directed at contemporary theories of auditory hallucinations (e.g. Frith,
1996) as the proposed deficits are often found in nonhallucinating schizophrenia patients
(e.g. Keefe, Arnold, Bayen & Harvey, 1999). As a consequence, there has been an
increasing awareness that a combination of deficits might be needed to explain such a
complex event (e.g. Nayani & David, 1996a). Our model proposes that patients with
auditory hallucinations, in addition to the intentional inhibition deficit, also suffer from a
context deficit in memory.
A deficit in memory for context
Approximately 60% of all patients with auditory hallucinations report hearing sounds
other than voices, which include environmental noises (e.g. clicks, bangs, city traffic) and
animals sounds (Nayani & David, 1996b; Waters, Badcock & Maybery, 2004). This
finding alone is not easily explainable by exclusively language-based accounts of auditory
hallucinations (e.g. Frith & Dolan, 1997) but rather points to the role of auditory
representations in memory. Our own investigations (Waters, Badcock & Maybery, 2004)
also show that a majority of patients report knowing the identity of their voices and close to
half agree with the idea that the contents of their voices could be reproductions of speech
they had heard in the past. These results support the proposal that auditory hallucinations
are, at least partly, composed of memories of speech and sounds. Several authors have

Chapter 8
-178 -
also noted the importance of memory in auditory hallucinations (e.g. David & Lucas, 1993;
Nayani & David, 1996a). For instance, David and Lucas (1993) first proposed that
auditory hallucinations may be associated with a failure in regulating memories and other
unwanted mental events from being activated involuntarily. Also, Hemsley (1993),
Hoffman et al (1994), Nayani and David (1996a) and David (2004) have suggested that
hallucinations may be associated with the intrusion of material from long-term memory.
But why wouldn’t patients recognize these events as memories? Nayani and David
(1996a) observed that all memories carry contextual details that allow them to be correctly
situated in time, in place and in person. To explain why these memory activations are not
recognized by the patient, they proposed a disturbance of the processes that serve to bind
the contextual components of memories, resulting in an incomplete representation of
memories and consequently a failure to identify their origins. In particular, they proposed a
disorder of the relationship between “mental events, time and self” (p. 363), suggesting
confusion about the temporal locus and source of speech fragments in memory. We extend
this proposal by suggesting that the loss of contextual information is not always absolute
and that the amount of information being recalled varies between individuals and between
hallucinatory episodes. As such, some contextual elements of the original experience are
sometimes preserved, such as the familiar voice of a TV or radio personality, or that of a
person well known to the sufferer.
Context memory: definition
In episodic memory research, a distinction is made between content and context
information. Content information refers to the event itself, whereas contextual information
refers to details which are encoded with the event, but which are not part of the event itself.
Context refers to information such as the source (“who”) or temporal (“when”)
characteristics of the memory event (Chalfonte & Johnson, 1996). The context of
memories provides cues that allow us to differentiate one memory from other memories.
Johnson and colleagues have proposed the most influential theory of how contextual
memory is recalled, with their Source-Monitoring Framework (Johnson, Hashtroudi &
Lindsay, 1993; Johnson, Kounios & Reeder, 1994). Their central claim is that memory
records are evaluated through a decision process performed during remembering. During
this process, the origins of memories are inferred on the basis of available cues (perceptual
details, contextual information, affect, semantic content and cognitive operations during

Chapter 8
-179 -
encoding). Retrieval success depends partly on the quality of information that was encoded
and disruption may occur because cues are missing, incomplete or ambiguous.
Furthermore, Johnson, Hashtroudi and Linsay (1993) have proposed that a loss of
qualitative information such as contextual details would make it difficulty to identify
correctly the origins of mental events and results in confusion with other stimuli. We
suggest that schizophrenia patients with auditory hallucinations fail to access the contextual
cues that would allow them to form an intact representation of events in memories.
Context memory deficits in auditory hallucinations of schizophrenia
It is now a consistent view that schizophrenia is linked to a deficit in integrating
contextual information in memory, and several authors have proposed that many of the
cognitive deficits observed in schizophrenia result from an impairment in the ability to
process contextual information (e.g. Bazin, Perruchet, Hardy-Bayle, & Feline, 2000; Cohen
& Servan-Schreiber, 1992; Rizzo, Danion, Van der Linden, & Grange, 1996; Servan-
Schreiber, Cohen, & Steingard, 1996). There are also increasing suggestions that a deficit
in context memory may be linked to positive symptoms, and in particular to auditory
hallucinations (Brebion et al, 1999; Brebion, Gorman, Amador, Malaspina & Sharif, 2002;
Guillem et al, 2003; Servan-Schreiber, Cohen, & Steingard, 1996). Support for the
proposal of a context memory deficit in auditory hallucinations comes primarily from
studies that have shown a failure to identify the source of actions among schizophrenia
patients currently experiencing auditory hallucinations (Baker & Morrison, 1998; Bentall,
Baker & Havers, 1991; Brebion, Smith, Gorman, Amador, 1996; Brebion et al, 2000, 2002;
Franck et al, 2000; John & McGuire, 1999). A deficit in identifying the source of events
has also been demonstrated in normal individuals who score high on a measure of
predisposition to hallucinations (Rankin & O’Carroll, 1995). The only study that
considered a loss of context information other than source in patients with auditory
hallucinations is Brebion et al (2002). They gave patients with schizophrenia a task of free
recall in which four lists of words were presented. They found that auditory hallucinations
severity was correlated with the erroneous recall of words presented in different lists, and
interpreted this deficit as an impairment in the ability to remember temporal context during
production of the words. In sum, the only empirical evidence supporting Nayani and
David's theory is the finding of a deficit in source monitoring in auditory hallucinations
and, indirectly, a deficit in retaining the temporal context of memories, suggesting that the

Chapter 8
-180 -
exact nature of the contextual memory deficit in auditory hallucinations has not yet been
clearly established.
New empirical support for a failure in context memory in auditory hallucinations
We are now able to test the prediction that patients with auditory hallucinations suffer
from a deficit in context memory. In Waters, Maybery, Badcock and Michie (2004), the
contextual memory of patients with schizophrenia was tested with a new task in which
memory for events was assessed in conjunction with memory for both the source and the
temporal characteristics of those events. Each participant watched or performed pairings of
common household objects in two different sessions. Subsequently, the participant’s
memory for pairs of objects, for who paired the objects and for when the objects were
paired, was tested. Therefore, the task tested recognition for individual contextual cues
(source and temporal memory) as well as the ability to bind those contextual cues together.
The results showed that compared to healthy controls, patients with schizophrenia had an
impairment in combining contextual cues together to form an integrated representation of
an event in memory.
As explained earlier, the most stringent test of whether a deficit is an essential
component to auditory hallucinations is to examine individual cases and determine the
percentages of patients impaired in the particular cognitive domain. The percentage of
patients who had a context memory deficit (impaired on source memory or temporal
memory or both), as defined by scores one standard deviation away from the means of the
control group, was computed (see Table 2). The results showed that nearly all patients
with auditory hallucinations showed a context memory deficit (89.5%). These results
confirm the second part of our model that contextual memory is impaired in those with
auditory hallucinations. The finding that a few patients with hallucinations did not show a
deficit in contextual memory may reflect the insensitivity of the particular task we used and
suggests that future studies should consider different ways to measure context memory.
The results also showed that 62.5% of the schizophrenic patients without
hallucinations were impaired. The difference in frequencies for the two patient groups was
significant, X2 (1) = 4.05, p < .05, suggesting that significantly more patients with auditory
hallucinations showed a deficit in contextual memory compared to patients without
hallucinations.

Chapter 8
-181 -
The finding that a failure in context memory is also present in nonhallucinating
individuals is not a problem for our model, primarily because we are proposing that context
memory is only one of at least two cognitive processes which are thought to be impaired.
Thus any single deficit may be associated with many of the symptoms of schizophrenia;
only in combination with the inhibitory impairment would the symptom of auditory
hallucinations become manifest. Interestingly, of the four patients with no previous history
of hallucinations, none showed a context memory deficit. Using a more stringent two
standard deviations criterion, two thirds of all hallucinating patients (63.2%) and less than
half of nonhallucinating patients (41.7%) still showed a significant impairment. This
difference was however nonsignificant, X2(1) = 1.96, p = .16. Overall, these results
indicate that, in concordance with our model, patients currently hallucinating showed a
deficit in contextual memory with varying degrees of severity.
Further empirical evidence also supports the involvement of episodic and context
memory processes in auditory hallucinations in schizophrenia. There is ample evidence
that the prefrontal regions are associated with source and temporal context memory
retrieval (e.g. Cabeza et al, 1997; Glisky, Rubin & Davidson, 2001; Henson, Shallice &
Dolan, 1999; Johnson, Kounios & Nolde, 1996; Rugg, Fletcher, Chua & Dolan, 1999;
Simons et al, 2002; Sullivan, 1997; Stuss, Eskes & Foster, 1994). The frontal lobes may
also be involved in the integration of multiple independent features of an experience into a
composite memory trace, with reduced frontal lobe functions resulting in memory traces
that lack rich contextual detail (Fuster, 1999; Stuss & Benson, 1989). Other studies have
linked contextual binding to the frontal lobes and to its connections with the hippocampus
and medial temporal system (Chalfonte & Johnson, 1996; Mitchell et al, 2000). The
temporal lobes have also been associated with source and temporal memory (Mayes et al,
2001; Spencer & Raz, 1995; Thaiss & Petrides, 2003). The finding that schizophrenia
patients show activation of the hippocampus (e.g. Copolov et al, 2003; Silbersweig et al,
1995; Woodruff & Murray, 1994), temporal lobes (e.g. Silbersweig et al, 1995) and
prefrontal cortex (Bushara et al, 1999; Copolov et al, 2003) during auditory hallucinations
is consistent with the notion that selection/retrieval from memory, and context memory
deficits, are important in the hallucinatory process. Most recently, Stevens (2004)
investigated the neural systems associated with voice memory, independently of word
memory, with functional magnetic resonance imaging. Voice memory processes engaged a

Chapter 8
-182 -
network of left temporal, right frontal and right medial parietal areas. The involvement of
the frontal and temporal regions is certainly consistent with regions activated during
auditory hallucinations.
A combined deficit in inhibition and context memory
We have demonstrated that inhibition and context memory processes are commonly
impaired in individuals with auditory hallucinations. However, patients not experiencing
hallucinations also demonstrated such deficits, showing that these deficits, singly, are not
sufficient for hallucinations to occur. Our model proposes that the two deficits should co-
occur in those patients currently experiencing auditory hallucinations. To test this theory,
the percentage of patients impaired on tasks of both intentional inhibition and contextual
memory was computed. The probability that an individual would score one standard
deviation away from the mean of controls in both cognitive domains by chance is .085.
Table 2 shows that, using a one standard deviation criterion, nearly all patients
currently experiencing hallucinations (89.5%) exhibited the proposed combination of
deficits, compared to only 33.3% of patients without active hallucinations. The difference
was significant, X2(1) = 13.73, p < .001, confirming that significantly more patients with
hallucinations showed the predicted combination of deficits than patients without
hallucinations. Furthermore, when using the most stringent criterion of two standard
deviations, more than half of the hallucinating patients still showed the combination of
deficits (52.6%) compared to only 16.7% of nonhallucinating patients, the difference again
being significant, X2 = 6.24, p < .01. Of the patients who had never hallucinated, none
showed the combination of deficits.
A critical reflection on the pattern of data for current hallucinators indicates strong
support for the notion that the two deficits, in varying degrees of severity, are significantly
associated with the hallucinatory process. However, the results also revealed that some
past hallucinators also showed the combination of deficits, suggesting that two deficits
alone may not be sufficient to explain the presence of auditory hallucinations, but that an
additional cognitive process is important for the expression of this symptom. One proposal
is that the role of this third process may be to 'activate' the internal representations that
would lead to auditory hallucinations. Our model, and all other contemporary models of
hallucinations, still need to identify the processes responsible for the selection and
activation of the hallucinatory material.

Chapter 8
-183 -
Several alternative explanations of why the patients currently experiencing auditory
hallucinations showed these deficits may be ruled out. We investigated whether the
patients had a more severe illness or were more cognitively impaired on intellectual
measures than patients not currently experiencing hallucinations. The results of our studies
(Badcock et al, in press; Waters, Badcock, Maybery & Michie, 2003; Waters et al, 2004)
indicate that this was not likely to be the explanation for the pattern of results. Group
comparisons (see Table 1) for a range of demographic factors such as age and years of
education, and clinical indicators including duration of illness, depression and number of
admissions, suggested that patients with current hallucinations were not generally more
unwell. Patients with current hallucinations showed more positive symptoms than non
hallucinators, but there were no significant differences in negative and general (somatic)
symptoms. Compared to non hallucinators, patients with hallucinations tended to have
higher doses of chlorpromazine equivalents, although this variable did not correlate with
performance on inhibition and context memory tasks (Waters, Badcock, Maybery &
Michie, 2003; Waters et al, 2004). Finally, hallucinating patients were not found to be
significantly more impaired on other measures of current cognitive functioning such as
general intelligence quotient or short-term memory tasks, suggesting that the above deficits
were not associated with a widespread cognitive impairment.
Assessment of the model
The current investigations consolidated empirical evidence in support of the proposal
that deficits in both intentional inhibition and context memory are important components to
the hallucinatory experience in schizophrenia. However, can this proposal also explain the
clinical phenomenology of auditory hallucinations? One criterion for judging the adequacy
of a theory of auditory hallucinations is the extent to which it can explain the
phenomenology of the experience.
Our model proposes that auditory hallucinations consist of the activation of auditory
mental events that include memories and other currently active mental associations. The
proposal of auditory hallucinations as consisting of auditory reproductions from memories
is able to explain the different forms and contents of auditory hallucinations. For example,
it can explain why hallucinations can take the form of nonverbal sounds, in addition to
voices (e.g. bangs, animal sounds; Nayani & David, 1996b). The finding that patients
experience nonverbal auditory hallucinations has been a problem for language-based

Chapter 8
-184 -
theories of auditory hallucinations, such as Inner Speech theories (e.g. Bentall, Kaney &
Dewey, 1991; Frith, 1996; Frith & Dolan, 1997). Our explanation also accounts for why
voices are often recognized as belonging to people that the hearer knows, and why sufferers
report hearing different types of grammatical speech, such as second or third person
hallucinations. The proposal of auditory hallucinations as memories can also explain why
entire dialogues from a conversation may be recalled, and why voices often refer to the
patient’s personal details and are perceived to be intimate. This aspect may contribute to
the compelling sense of reality and omnipotence of auditory hallucinations (Chadwick &
Birchwood, 1995; Gelder et al, 1993) since they comprise the intrusion of highly familiar
information (i.e. memories).
Another distinguishing feature of schizophrenic hallucinations is that the experience
is perceived to originate from another agency, a finding that has traditionally been
explained with reference to difficulties in distinguishing sensations caused by one’s own
actions or a failure in self-monitoring (Frith & Dolan, 1997; McGuire et al, 1995). The
current suggestion of a disordered context memory system can also explain why the origins
of these mental events are often not recognized. The contextual features are missing or
incomplete, resulting in confusion about the origins of the experience. Misattribution can
therefore be understood as the transference of the origins of memories as a result of
impaired context memory abilities. It may also be speculated that the failure to identify the
origins of recalled memories would lead to misinterpretations about the message and the
intent of the experience, accounting for variations in beliefs about the voices and also for
negative affect such as distress and fear commonly experienced by patients with auditory
hallucinations (e.g. Close & Garety, 1998).
In addition, the proposal of hallucinations as memories provides, in our view, a
satisfactory explanation of why voices are perceived to have an external origin and believed
to be real. Recent findings suggest that episodic memory retains traces of both voice
characteristics and words (Goldinger, 1999). Furthermore, it has been noted that the human
voice carries important information such as the affect, gender, age and other physical
characteristics of a talker (Belin, Fecteau & Bedard, 2004; Stevens, 2004). The attributes
carried are such that voices have been described as an ‘auditory face’, carrying a
combination of individual features and emotional states (Belin et al, 2004), confirming the
patients’ firm assertions that that they are not just hearing words, but a real voice with,

Chapter 8
-185 -
sometimes, its own social and physical identity. The individual is therefore correct in
reporting that the voice of another is being heard. A similar line of argument regarding the
preserved perceptual aspects of memories of speech (Hunter and Woodruff, 2004) further
contribute to our understanding of the mechanisms of the location in space of hallucinated
speech. Auditory hallucinations are sometimes perceived to originate from inside the head,
and sometimes from outside (Copolov, Trauer & MacKinnon, in press; Hunter, 2004). In
our view, those sensory records, which includes the elements of the original perceptual
trace of an auditory event in external space, indicates that the experience originated from a
non-self source and from a location outside the head. In the case where the original
experience was actually generated by the patient’s own mental production, an absence of
these perceptual elements may lead to the correct conclusion that the voice originated from
inside the head.
As noted above, auditory hallucinations are often reported to be intrusive, unintended
and beyond the control of the voice-hearer (Slade & Bentall, 1988; Oulis, Mavreas,
Mamounas & Stephanis, 1995). This feature of the hallucinatory experience has often been
ignored in contemporary cognitive theories of auditory hallucinations (e.g. Aleman,
Böcker, Hijman, Kahn & de Haan 2002, Frith, 1996). Our model’s proposal of a failure in
the control of intentional inhibition explains that patients would find it difficult to suppress
irrelevant mental events, which would then be experienced as conscious events. It makes
intuitive sense that these unsolicited mental events would contribute to the perceived
intrusiveness of hallucinations.
It is important to note that our model should not be seen as an independent approach
to understanding auditory hallucinations. It is our view that the proposed deficits should be
seen as complementary to other explanations of hallucinations. For instance, the current
proposal of a context memory deficit in patients with auditory hallucinations is actually not
dissimilar to reality- and self-monitoring theories of auditory hallucinations (e.g. Frith,
1996). In support, Brebion et al (1996) suggested that difficulties in identifying the
contextual details of mental events would result in a failure to discriminate between real
and imaginary events, or between external events themselves, resulting in a failure in
reality monitoring. However, our proposal differs in the suggestion that the context
memory deficit is more extensive than simply a source-monitoring deficit. The lack of
specificity criticism often directed at these theories is not of primary importance to the

Chapter 8
-186 -
current theory as it allows for other conditions to show similar deficits, as long as they do
not show the exact same permutation of deficits.
In addition, it is unlikely that cognitive impairments are the sole factors responsible
for auditory hallucinations. It is now generally acknowledged that psychological factors
such as metacognitive biases, beliefs and attributions concerning the origins and intent of
voices have considerable explanatory power (e.g. Chadwick & Birchwood, 1995). This
level of explanation, for which the content of voices is so meaningful, may account for the
material comprising hallucinated speech and issues of affect, which our model cannot fully
account for. For instance, Thomas, Bracken and Leudar (2004) have argued that the voices
may only be explained in the context of each individual’s social, cultural, historical and
political framework, providing a useful approach to understanding the content of voices and
the special relationships that develop between patients and their voices. It is our view that,
although psychological explanations do not explain so well how hallucinations occur in the
first place, they are very convincing models of the maintenance process of auditory
hallucinations and their insight can be integrated with the current level of explanation to
understand the very personalized experience of sufferers.
Potential empirical and theoretical developments
We should elaborate on the specificity of the model to patients with auditory
hallucinations. It was explained earlier that nonhallucinating individuals may show a
deficit in either cognitive domain, but only hallucinating patients should show a deficit in
both. This explanation allows for the finding that these deficits, singly, may be present in
patients with schizophrenia, irrespective of their hallucinatory status, and in other disorders.
In particular, we may speculate that either of these deficits may be found in other psychotic
symptoms which frequently co-occur with auditory hallucinations, perhaps acting like a
predisposing factor for hallucinations. However, it is anticipated that only hallucinating
patients will show the combination of deficits.
The model described so far has focused largely on processes believed to be relevant
to the onset of hallucinations but further work is required to elaborate on the processes
responsible for the relapse and recovery phases. It may be speculated that fluctuations in
one of the cognitive mechanisms suggested above modulate the cognitive states the patients
pass through. In support, our studies have shown that the inhibitory deficit is present
particularly in periods in which hallucinations are actually experienced (e.g. Badcock et al,

Chapter 8
-187 -
in press). In addition, fluctuations in the level of control for auditory hallucinations have
been found in schizophrenia patients during different phases of their illness. Larkin (1979)
found that patients were able to stop auditory hallucinations during remission but not
during the acute phase of their illness. If the process of inhibition is instrumental in the
patient’s control over auditory hallucinations, then Larkin’s study also suggests that levels
of inhibitory control may vary according to the phase of the patient’s illness. A revealing
study would be to monitor the processes of inhibition and context memory longitudinally to
investigate how these vary according the state of the patient.
It is perhaps conceivable that fluctuations in these processes, and perhaps even the
onset of hallucinations, occur as a result of significant life changes associated with stress
and other emotive states. It has often been suggested that stress plays an important role in,
and often precedes, auditory hallucinations (Bentall, 1990, 1997; Hustig & Hafner, 1990;
Soppitt & Birchwood, 1997). Nayani and David (1996b) also found that some affective
states such as sadness, fear and anger sometimes trigger hallucinations. The mechanisms
by which these events trigger hallucinations can only be speculated but it is well recognized
that mood states such as arousal, depression or anxiety have been found to affect cognitive
performance such as inhibitory processes (Brewin et al, 1996; Reynolds & Brewin, 1998)
and encoding or retrieval of memories (Deffenbacher, 1994; Derix & Jolles, 1997) to a
significant degree. It may, therefore, be possible that, in a predisposed individual, an
intensely emotional event may activate auditory hallucinations by precipitating a change in
the balance of normal cognitive processes.
Our findings showed that a small number of patients who no longer experienced
auditory hallucinations showed the combination of deficits, suggesting that additional
cognitive process(es) may be necessary to explain auditory hallucinations in patients with
schizophrenia. We speculated that the role of this additional process may be to 'activate'
the representations that would lead to auditory hallucinations. Another process that may be
relevant to our investigations is mental imagery. One recently developed theory of auditory
hallucinations proposes that, in individuals susceptible to auditory hallucinations, top-down
processes are given higher priority than bottom-up processes resulting in an imbalance
between sensory and mental elements and an increasing influence of imagery on perception
(Aleman, Böcker, Hijman, de Haan & Kahn, 2003). The proposal of impaired imagery
may be of considerable value in identifying additional cognitive deficits in addition to the

Chapter 8
-188 -
ones already proposed. Although empirical evidence is still needed to convincingly support
the role of imagery in hallucinating schizophrenia patients, it is a factor that has been
consistently identified in research on normal people with a predisposition to hallucinations
(Aleman, Böcker & de Haan, 1999; Barrett & Etheridge, 1992).
Finally, the small sample size is a limitation of our research and replication is needed
using larger samples. Investigations should also particularly target individuals with
schizophrenia who have no history of auditory hallucinations to validate our model, as they
represent the strongest test of which combination of cognitive deficits is specific to auditory
hallucinations.
In conclusion, we propose a new model of auditory hallucinations in schizophrenia,
whereby a failure in both intentional inhibition and in contextual memory must be present
simultaneously for hallucinatory experiences to occur. Empirical evidence was assembled
to show that these deficits were significantly associated with this symptom. Given the
heterogeneous nature of schizophrenia, continued research using the research strategies
summarized here should further elucidate the relationship between psychotic symptoms and
cognitive impairment.
Acknowledgements
This research was supported by a University Postgraduate Award and a Departmental
Scholarship from the School of Psychology of the University of Western Australia to F.
Waters as well as research funds from the University of Western Australia Schools of
Psychology and of Psychiatry and Clinical Neurosciences. The authors wish to thank all of
the patients who took part in this study, Danny Rock whose help was invaluable in
recruiting the patients, and G. Haddock, D. Copolov and their colleagues for their
permission to use the PSYRAT and the MUPS respectively as part of our research.

Chapter 8
-189 -
References
Aleman, A., Böcker, K., & deHaan, E. (1999). Disposition towards hallucination and
subjective versus objective vividness of imagery in normal subjects. Personality and
Individidual Differences, 27, 707-714.
Aleman, A., Böcker, K. B. E., Hijman, R., Kahn, R. S., & de Haan, E. H. F. (2002).
Hallucinations in schizophrenia: imbalance between imagery and perception?
Schizophrenia Research, 57(2-3), 315-316.
Aleman, A., Böcker, K. B. E., Hijman, R., de Haan, E. H. F., & Kahn, R. S. (2003).
Cognitive basis of hallucinations in schizophrenia: role of top-down information
processing. Schizophrenia Research, 1926, 1-11.
Amieva, H., Phillips, L. H., Della Sala, S., & Henry, J. D. (2004). Inhibitory functioning in
Alzheimer's disease. Brain, 127, 949-964.
Anderson, M. C., & Green, C. (2001). Suppressing unwanted memories by executive
control. Nature, 410(6826), 366-369.
Asaad, G., & Shapiro, B. (1986). Hallucinations: theoretical and clinical overview.
American Journal of Psychiatry, 143(9), 1088-1097.
Badcock, J. C., Waters, F. A. V., Maybery, M. T., & Michie, P. T. (in press). Auditory
hallucinations: failure to inhibit irrelevant memories. Cognitive Neuropsychiatry.
Baker, C. A., & Morrison, A. P. (1998). Cognitive processes in auditory hallucinations:
attributional biases and metacognition. Psychological Medicine, 28, 1199-1208.
Barrett, T., & Etheridge, J. (1992). Verbal hallucinations in normals, I: People who hear
'voices'. Applied Cognitive Psychology, 6(5), 379-387.
Bazin, N., Perruchet, P., Hardy-Bayle, M., & Feline, A. (2000). Context-dependent
information processing in patients with schizophrenia. Schizophrenia Research, 45(1-
2), 93-101.
Beech, A., Powell, T., McWilliam, J., & Claridge, G. (1989). Evidence of reduced
'cognitive inhibition' in schizophrenia. British Journal of Clinical Psychology, 28,
109-116.
Belin, P., Fecteau, S., & Bedard, C. (2004). Thinking the voice: neural correlates of voice
perception. Trends in Cognitive Sciences, 8(3), 129-1355.
Bentall, R. P., Baker, G. A., & Havers, S. (1991). Reality monitoring and psychotic
hallucinations. British Journal of Clinical Psychology, 30, 213-222.

Chapter 8
-190 -
Bentall, R. P., Kaney, S., & Dewey, M. E. (1991). Paranoia and social reasoning: an
attribution theory analysis. British Journal of Clinical Psychology, 30, 13-23.
Bentall, R. P. (1990). The illusion of reality: A review and integration of psychological
research on hallucinations. Psychological Bulletin, 107(1), 82-95.
Bentall, R. (1997). The syndromes and symptoms of psychosis. Or why you can't play
'twenty questions' with the concept of schizophrenia and hope to win. In R. Bentall
(Ed.), Reconstructing schizophrenia (pp. 23-59). London: Routledge.
Bjorklund, D., & Harnishfeger, K. K. (1995). The evolution of inhibition mechanisms and
their role in human cognition. In F. Dempster & C. Brainerd (Eds.), Interference and
Inhibition in Cognition (pp. 141-173). San Diego, London: Academic Press, Inc.
Brebion, G., Smith, M., Gorman, J., & Amador, X. (1996). Reality monitoring failure in
schizophrenia: The role of selective attention. Schizophrenia Research, 22, 173-180.
Brebion, G., Smith, M., Amador, X., Malaspina, D., & Gorman, J. (1998). Word
recognition, discrimination accuracy and decision bias in schizophrenia: association
with positive symptomatology and depressive symptomatology. The Journal of
Nervous and Mental Disease, 186(10), 604-609.
Brebion, G., Amador, X., David, A., Malaspina, D., Sharif, Z., & Gorman, J. M. (2000).
Positive symptomatology and source-monitoring failure in schizophrenia - an
analysis of symptom specific effects. Psychiatry Research, 95, 119-131.
Brebion, G., Amador, X., Smith, M., Malaspina, D., Sharif, Z., & Gorman, J. (1999).
Opposite links of positive and negative symptomatology with memory errors in
schizophrenia. Psychiatry Research, 88, 15-24.
Brebion, G., Gorman, J. M., Amador, X., Malaspina, D., & Sharif, Z. (2002). Source
monitoring impairments in schizophrenia: characterisation and association with
positive and negative symptomatology. Psychiatry Research, 112, 27-39.
Brewin, C. R., Hunter, E., Carroll, F., & Tata, P. (1996). Intrusive memories in depression:
an index of schema. Psychological Medicine, 26(6), 1271-1276.
Bullen, J. G., & Hemsley, D. R. (1987). Schizophrenia: a failure to control the contents of
consciousness. British Journal of Clinical Psychology, 26, 25-33.
Burgess, P., & Shallice, T. (1996). Response suppression, initiation and strategy use
following frontal lobe lesions. Neuropsychologia, 34(4), 263-273.

Chapter 8
-191 -
Bushara, K. O., Weeks, R. A., Ishii, K., Catalan, M.-J., Tian, B., Rauschecker, J. P., &
Hallett, M. (1999). Modality-specific frontal and parietal areas for auditory and visual
spatial localization in humans. Nature Neuroscience, 2(8), 759-766.
Cabeza, R., Mangels, J., Nyberg, L., Habib, R., Houle, S., McIntosh, A. R., & Tulving, E.
(1997). Brain regions differentially involved in remembering what and when: A PET
study. Neuron, 19, 863-870.
Carter, D. M., Mackinnon, A., & Copolov, D. L. (1996). Patients' strategies for coping with
auditory hallucinations. The Journal of Nervous and Mental Disease, 184(3), 161-
166.
Chadwick, P., & Birchwood, M. (1995). The Omnipotence of Voices II: The Beliefs About
Voices Questionnaire (BAVQ). British Journal of Psychiatry, 166, 773-776.
Chalfonte, B. L., & Johnson, M. K. (1996). Feature memory and binding in young and
older adults. Memory and Cognition, 24(4), 403-416.
Close, H., & Garety, P. (1998). Cognitive assessment of voices: further develoments in
understanding the emotional impact of voices. British Journal of Clinical Psychology,
37, 173-188.
Cohen, J. D., & Servan-Schreiber, D. (1992). A neural network model of disturbances in
the processing of context in schizophrenia. Psychiatric Annals, 22(3), 131-136.
Collette, F., Van der Linden, M., Delfiore, G., Degueldre, C., Luxen, A., & Salmon, E.
(2001). The functional anatomy of inhibition processes investigated with the Hayling
Task. NeuroImage, 14, 258-267.
Conway, M., Harries, K., Noyes, J., Racsma'ny, M., & Frankish, C. (2000). The disruption
and dissolution of directed forgetting: inhibitory control of memory. Journal of
Memory and Language, 43, 409-430.
Copolov, D., Trauer, T., & MacKinnon, A. (in press). On the non-significance of internal
versus external auditory hallucinations. Schizophrenia Research.
Copolov, D. L., Seal, M. L., Maruff, P., Ulusoy, R., Wong, M. T. H., Tochon-Danguy, H.
J., & Egan, G. F. (2003). Cortical activation associated with the experience of
auditory hallucinations and perception of human speech in schizophrenia: a PET
correlation study. Psychiatry Research: Neuroimaging, 122, 139-152.

Chapter 8
-192 -
Cornblatt, B., Lenzenweger, M., Dworking, R., & Erlenmeyer-Kimling, L. (1985). Positive
and negative schizophrenia symptoms, attention and information processing.
Schizophrenic Bulletin, 11(3), 397-407.
Crider, A. (1997). Perseveration in schizophrenia. Schizophrenia Bulletin, 23(1), 63-74.
David, A. S. (2004). The cognitive neuropsychiatry of auditory verbal hallucinations: an
overview. Cognitive Neuropsychiatry, 9(1/2), 107-123.
David, A. S., & Lucas, P. A. (1993). Auditory-verbal hallucinations and the phonological
loop: A cognitive neuropsychological study. British Journal of Clinical Psychology,
32, 431-441.
David, A. S. (2004). The cognitive neuropsychiatry of auditory verbal hallucinations: an
overview. Cognitive Neuropsychiatry, 9(1/2), 107-123.
Deffenbacher, K. A. (1994). Effects of arousal on everyday memory. Human Performance,
7(2), 141-161.
Derix, M. M. A., & Jolles, J. (1997). Neuropsychological abnormalities in depression:
relation between brain and behavior. In A. Honig & H. M. van Praag (Eds.),
Depression: neurobiological, psychopathological and therapeutic advances (Vol. 3,
pp. 109-126). New York: John Wiley & Sons Ltd.
DiGirolamo, G. J., & Posner, M. I. (1996). Attention and schizophrenia: a view from
cognitive neuroscience. Cognitive Neuropsychiatry, 1(2), 95-102.
Enright, S. J., & Beech, A. R. (1993). Reduced cognitive inhibition in obsessive-
compulsive disorder. British Journal of Clinical Psychology, 32, 67-74.
Franck, N., Rouby, P., Daprati, E., Dalery, J., Mari-Cardine, M., & Georgieff, N. (2000).
Confusion between silent and overt reading in schizophrenia. Schizophrenia
Research, 41, 357-364.
Frith, C. D. (1979). Consciousness, information processing and schizophrenia. British
Journal of Psychiatry, 134, 225-235.
Frith, C. (1996). The role of the prefrontal cortex in self-consciousness: the case of auditory
hallucinations. Philosophical Transactions of the Royal Society of London: B, 351,
1505-1512.
Frith, C., & Dolan, R. J. (1997). Brain mechanisms associated with top-down processes in
perception. Philosophical Transactions of the Royal Society of London, B, 352, 1221-
1230.

Chapter 8
-193 -
Fuster, J. M. (1999). Synopsis of function and dysfunction of the frontal lobe. Acta
Psychiatrica Scandinavica, 99 (Suppl. 395), 51-57.
Gelder, M., Gath, D., & Mayou, R. (1993). Oxford textbook of psychiatry (2nd ed.).
Oxford: Oxford University Press.
Glisky, R. L., Rubin, S. R., & Davidson, P. S. R. (2001). Source memory in older adults: an
encoding or retrieval problem? Journal of Experimental Psychology: Learning,
Memory and Cognition, 27(5), 1131-1146.
Goldinger, S.D., Kleider, H.M., Shelley, E. (1999). The marriage of perception and
memory: creating two-way illusions with words and voices. Memory and Cognition,
27(2): 328-338.
Gray, J. A. (1998). Integrating Schizophrenia. Schizophrenia Bulletin, 24(2), 249-266.
Guillem, F., Bicu, M., Pampoulova, T., Hooper, R., Bloom , D., & Wolf, M.-A. e. a.
(2003). The cognitive and anatomo-functional basis of reality distortion in
schizophrenia: a view from memory event-related potentials. Psychiatry Research,
117, 137-158.
Harnishfeger, K. K. (1995). The development of cognitive inhibition: theories, definitions
and research evidence. In F. N. Dempster & C. J. Brainerd (Eds.), Interference and
inhibition in cognition. Chap 6 (pp. 175-205). San Diego: Academic Press.
Hemsley, D. R. (1993). A simple (or simplistic?) cognitive model for schizophrenia.
Behavior Research and Therapy, 31(7), 633-645.
Henson, R. N. A., Shallice, T., & Dolan, R. J. (1999). Right prefrontal cortex and episodic
memory retrieval: a functional MRI test of the monitoring hypothesis. Brain, 122,
1367-1381.
Hoffman, R. E., Oates, E., Hafner, J., Hustig, H. H., & McGlashan, T. H. (1994). Semantic
organization of hallucinated "voices" in schizophrenia. American Journal of
Psychiatry, 151, 1229-1230.
Hoffman, R. E., Rapaport, J., Mazure, C., & Quinlan, D. (1999). Selective speech
perception alternations in schizophrenic patients reporting hallucinated voices. The
American Journal of Psychiatry, 156(3), 393-399.
Honig, A., Romme, M. A. J., Ensink, B. J., Escher, S. D., Pennings, M. H. A., & Devries,
M. W. (1998). Auditory Hallucinations: A comparison between patients and
nonpatients. The Journal of Nervous and Mental Disease, 186(10), 646-651.

Chapter 8
-194 -
Hunter, M. D. (2004). Locating voices in space: a perceptual model for auditory
hallucinations. Cognitive Neuropsychiatry, 9(1/2), 93-105.
Hunter, M. D., & Woodruff, W. R. (2004). Characteristics of functional auditory
hallucinations. The American Journal of Psychiatry, 161(5), 923.
Hustig, H. H., & Hafner, R. J. (1990). Persistent auditory hallucinations and their
relationship to delusions and mood. The Journal of Nervous and Mental Disease,
178(4), 264-267.
Johns, L. C., & McGuire, P. K. (1999). Verbal self-monitoring and auditory hallucinations
in schizophrenia. The Lancet, 353(9151), 469-470.
Johnson, M., Kounios, J., & Nolde, S. (1996). Electrophysiological brain activity and
memory source monitoring. NeuroReport, 7, 2929-2932.
Johnson, M. K., Hashtroudi, S., & Lindsay, D. S. (1993). Source Monitoring. Psychological
Bulletin, 114(1), 3-28.
Johnson, M. K., Kounios, J., & Reeder, J. A. (1994). Time-course studies of reality
monitoring and recognition. Journal of Experimental Psychology: Learning, Memory
and Cognition, 20(6), 1409-1419.
Keefe, R. S. E., Arnold, M. C., Bayen, U. J., & Harvey, P. D. (1999). Source monitoring
deficits in patients with schizophrenia: a multinomial modelling analysis.
Psychological Medicine, 29, 903-914.
Kramer, A., Humphrey, D., Larish, J., Logan, G., & Strager, D. (1994). Aging and
inhibition: Beyond a unitary view of inhibitory processing in attention. Psychology
and Aging, 9(4), 491-512.
Larkin, A. R. (1979). The form and content of schizophrenic hallucinations. American
Journal of Psychiatry, 136(7), 940-943.
Lennox, B. R., Bert, S., Park, G., Jones, P. B., & Morris, P. G. (1999). Spatial and
Temporal mapping of neural activity associated with auditory hallucinations. The
Lancet, 353(9153), 644.
Levy, B. J., & Anderson, M. C. (2002). Inhibitory processes and the control of memory
retrieval. Trends in Cognitive Sciences, 6(7), 299-305.
Mayes, A., Isaac, C., Holdstock, J., Hunkin, N., Montaldi, D., Downes, J., MacDonald, C.,
Cezayirli, E., & Roberts, J. (2001). Memory for single items, word pairs and temporal

Chapter 8
-195 -
order of different kinds in a patient with selective hippocampal lesion. Cognitive
Neuropsychology, 18(2), 97-123.
McGuire, P., Shah, G., & Murray, R. M. (1993). Increased blood flow in Broca's area
during auditory hallucinations in schizophrenia. The Lancet, 342, 703-706.
McGuire, P. K., Silbersweig, D. A., Wright, I., Murray, R. M., David, A. S., Frackowiak,
R. S. J., & Frith, C. D. (1995). Abnormal monitoring of inner speech: a physiological
basis for auditory hallucinations. The Lancet, 346(8975), 596-600.
Mitchell, K., Johnson, M., Raye, C., & D'Esposito, M. (2000). fMRI evidence of age-
related hippocampal dysfunction in feature binding in working memory. Cognitive
Brain Research, 10, 197-206.
Morrison, A. P., Haddock, G., & Tarrier, N. (1995). Intrusive thoughts and auditory
hallucinations: a cognitive approach. Behavioral and Cognitive Psychotherapy, 23,
265-280.
Morrison, A. P., & Baker, C. A. (2000). Intrusive thoughts and auditory hallucinations: a
comparative study of intrusions in psychosis. Behaviour Research and Therapy, 38,
1097-1106.
Morrison, A. P. (2001). The interpretation of intrusions in psychosis: an integrative
cognitive approach to hallucinations and delusions. Behavioral and Cognitive
Psychotherapy, 29, 257-276.
Nathaniel-James, D. A., Brown, R., & Ron, M. (1996). Memory impairment in
schizophrenia: its relationship to executive function. Schizophrenia Research, 21, 85-
96.
Nathaniel-James, D. A., Fletcher, P., & Frith, C. (1997). The functional anatomy of verbal
initiation and suppression using the Hayling Test. Neuropsychologia, 35(4), 559-566.
Nayani, T. H., & David, A. S. (1996a). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & T. R. E. Barnes (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 . New York: John Wiley
& Sons Ltd.
Nayani, T. H., & David, A. S. (1996b). The auditory hallucination: a phenomenological
survey. Psychological Medicine, 26, 177-189.

Chapter 8
-196 -
Nigg, J. T. (2000). On inhibition/disinhibition in developmental psychopathology: Views
from cognitive and personality psychology and a working inhibition taxonomy.
Psychological Bulletin, 126(2), 220-246.
Nigg, J. T., Butler, K. M., Huang-Pollock, C. L., & Henderson, J. M. (2002). Inhibitory
processes in adults with persistent childhood onset ADHD. Journal of Consulting and
Clinical Psychology, 70(1), 153-157.
Oulis, P. G., Mavreas, V. G., Mamounas, J. M., & Stefanis, C. N. (1995). Clinical
characteristics of auditory hallucinations. Acta Psychiatrica Scandinavica, 92, 97-102.
Peters, E. R., Pickering, A., Kent, A., Glasper, A., Irani, M., David, A., Day, S., &
Hemsley, D. (2000). The relationship between cognitive inhibition and psychotic
symptoms. Journal of Abnormal Psychology, 109(3), 386-395.
Rankin, P. M., & O'Carroll, P. J. (1995). Reality discrimination, reality monitoring and
disposition towards hallucination. British Journal of Clinical Psychology, 34, 517-
528.
Reynolds, M., & Brewin, C. R. (1998). Intrusive cognition, coping strategies and emotional
responses in depression, post-traumatic stress disorder and a non-clinical population.
Behavior Research and Therapy, 36(2), 135-147.
Rizzo, L., Danion, J.-M., Van der Linden, M., & Grange, D. (1996). Patients with
schizophrenia remember that an event has occured, but not when. British Journal of
Psychiatry, 168, 427-431.
Rugg, M., Fletcher, P., Chua, P., & Dolan, R. J. (1999). The role of the prefrontal cortex in
reocgnition memory and memory for source: an fMRI study. NeuroImage, 10, 520-
529.
Sartorius, N., Shapiro, R., & Jablensky, A. (1974). The international pilot study of
schizophrenia. Schizophrenia Bulletin, 11, 21-34.
Schnider, A., & Ptak, R. (1999). Spontaneous confabulators fail to suppress currently
irrelevant memory traces. Nature Neuroscience, 2(7), 677-681.
Schnider, A., Treyer, V., & Buck, A. (2000). Selection of currently relevant memories by
the human posterior medial orbital cortex. The Journal of Neuroscience, 20(15),
5880-5884.

Chapter 8
-197 -
Seal, M. L., Aleman, A., & McGuire, P. K. (2004). Compelling imagery, unanticipated
speech and deceptive memory: neurocognitive models of auditory verbal
hallucinations in schizophrenia. Cognitive Neuropsychiatry, 9(1/2), 43-72.
Servan-Schreiber, D., Cohen, J., & Steingard, S. (1996). Schizophrenic Deficits in the
processing of context: A test of a theoretical model. Archives of General Psychiatry,
53(12), 1105-1112.
Silbersweig, D. A., Stern, E., Frith, C, Cahill, C, Holmes, A, Grootoonk, S, Seaward, J,
McKenna, P, Chua, S., Schnorr, L, Johnes, T, Frackowiak, R (1995). A functional
neuroanatomy of hallucinations in schizophrenia. Nature, 378, 176-179.
Simons, J. S., Verfaellie, M., Galton, C. J., Miller, B. L., Hodges, J. R., & Graham, K. S.
(2002). Recollection-based memory in frontotemporal dementia: implications for
theories of long-term memory. Brain, 125(11), 2523-2536.
Slade, P. D., & Bentall, R. P. (1988). Sensory deception: A scientific analysis of
hallucinations. London: Croom Helm.
Soppitt, C. W., & Birchwood, M. (1997). Depression, beliefs, voice content and
topography: a cross sectional study of schizophrenia patients with auditory verbal
hallucinations. Journal of Mental Health, 6(5), 525-532.
Spencer, W., & Raz, N. (1995). Differential effects of aging on memory for content and
context: A meta-analysis. Psychology and Aging, 10(4), 527-539.
Spinella, M. (2002). Correlations among behavioral measures of orbitofrontal function.
International Journal of Neuroscience, 112(11), 1359-1369.
Stevens, A. A. (2004). Dissociating the cortical basis of memory for voices, words and
tones. Cognitive Brain Research, 18, 162-171.
Stuss, D. T., & Benson, D. F. (1989). The Frontal Lobes.
Stuss, D. T., Eskes, G. A., & Foster, J. K. (1994). Experimental neuropsychological studies
of frontal lobe functions. In F. G. Boller, J (Eds) (Ed.), Handbook of
Neuropsychology (vol 9) .
Stuss, D., Toth, J., Franchi, D., Alexander, M., Tipper, s., & Craig, F. (1999). Dissociation
of attentional processes in patients with focal frontal and posterior lesions.
Neuropsychologia, 37, 1005-1027.

Chapter 8
-198 -
Sullivan, E. V., Shear, P. K., Zipursky, R. B., Sagar, H. J., & Pfefferbaum, A. (1997).
Patterns of content, contextual and working memory impairments in schizophrenia
and nonamnesic alcoholism. Neuropsychology, 11(2), 195-206.
Takebayashi, H., Takei, N., & Mori, N. (2002). Unilateral auditory hallucinations in
schizophrenia after damage to the right hippocampus. Schizophrenia Research.
Thaiss, L., & Petrides, M. (2003). Source and content memory in patients with a unilateral
frontal cortex or a temporal lobe excision. Brain, 126(5), 1112-1126.
Thomas, P., Bracken, P., & Leudar, I. (2004). Hearing voices: a phenomenological-
hermeneutic approach. Cognitive Neuropsychiatry, 9(1/2), 13-23.
Vasterling, J. V., Brailey, K., Constans, J. I., & Sutker, P. B. (1998). Attention and memory
dysfunction in Post-Traumatic Stress Disorder. Neuropsychology, 12(1), 125-133.
Waters, F. A. V., Badcock, J. C., & Maybery, M. T. (2003). Revision of the factor structure
of the Launay-Slade Hallucination Scale (LSHS-R). Personality and Individual
Differences, 35, 1351-1357.
Waters, F. A. V., Badcock, J. C., & Maybery, M. T. (2004). An analysis of the main
clinical features of auditory hallucinations. Unpublished manuscript.
Waters, F. A. V., Badcock, J. C., Maybery, M. T., & Michie, P. T. (2003). Inhibition in
schizophrenia: association with auditory hallucinations. Schizophrenia Research, 62,
275-280.
Waters, F. A. V., Maybery, M. T., Badcock, J. C., & Michie, P. T. (2004). Context memory
and binding in schizophrenia. Schizophrenia Research, 68 (2-3), 119-125.
Williams, L. M. (1996). Cognitive Inhibition and schizophrenic symptom subgroups.
Schizophrenia Bulletin, 22(1), 139-151.
Wilson, S. P., & Kipp, K. (1998). The development of efficient inhibition: Evidence from
directed-forgetting tasks. Developmental Review, 18, 86-123.
Wong, A. H. C., & Van Tol, H. H. M. (2003). Schizophrenia: from phenomenology
to neurobiology. Neuroscience and Biobehavioural Reviews, 27, 269-306.
Woodruff, P. W. R., & Murray, R. M. (1994). The aetiology of brain abnormalities in
schizophrenia. In R. Ancill (Ed.), Schizophrenia: Exploring the Spectrum of
Psychosis. New York: John Wiley & Sons Ltd.
Woodruff, P. W. R. (2004). Auditory hallucinations: insights and questions from
neuroimaging. Cognitive Neuropsychiatry, 9(1/2), 73-91.

Chapter 8
-199 -
Young, H. F., Bentall, R. P., Slade, P. D., & Dewey, M. E. (1987). The role of brief
instructions and suggestibility in the elicitation of auditory and visual hallucinations
in normal and psychiatric subjects. The Journal of Nervous and Mental Disease,
175(1), 41-47.

- 201 -
INTENTIONAL INHIBITION, CONTEXT MEMORY
AND OBSESSIVE-COMPULSIVE DISORDER

- 203 -
Foreword to Chapters 9 and 10
The results of our investigations of schizophrenia patients with auditory
hallucinations have suggested that a combination of deficits in both intentional inhibition
and context memory is critical, although not sufficient, for auditory hallucinations to occur.
We proposed that the deficit in inhibition leads to auditory mental representations intruding
into consciousness in a manner that is beyond the control of the sufferer, and that the deficit
in context memory results in an inability to form a complete representation of the origins of
mental events and therefore a failure to recognize these unintended mental representations.
Our model of auditory hallucinations anticipates that (a) non-hallucinating
individuals (with or without schizophrenia) may present with a deficit in either intentional
inhibition or context memory, but (b) none of these individuals should show a deficit in
both cognitive domains. The aim of this last investigation is to test this prediction by
investigating the proposed deficits in another clinical group, namely patients with
Obsessive-Compulsive Disorder (OCD). This patient group was selected because of the
similarities between OCD and auditory hallucinations. In particular, OCD patients
experience intrusive and unwanted thoughts but, unlike patients with auditory
hallucinations, they do not mistake the origins of these thoughts.
Chapter 8 presents a review of the phenomenological, clinical, cognitive and
neuropathological research findings concerning OCD, together with a critical analysis of
the similitudes between OCD and auditory hallucinations.
Chapter 9 investigates the prediction that none of the patients with OCD would
show deficits in both intentional inhibition functioning and memory for context.

- 205 -
Chapter 9 Obsessive-Compulsive Disorder: an overview
Abstract
Similarities between obsessive-compulsive disorder (OCD) and auditory
hallucinations have recently been the focus of much interest. The aim of this chapter is to
present a brief overview of the phenomenology of OCD, together with a summary of the
cognitive processes presumed to be important in OCD and pertinent neuropathological and
clinical research findings. A critical analysis of the similitudes at the symptom, cognitive
and neuropathological level between OCD and auditory hallucinations is also provided.
This review of the similarities between the two disorders suggests that there may be an
overlap of some cognitive mechanisms that have been the focus of this thesis.

Chapter 9
- 206 -
Obsessive-compulsive disorder (OCD) is a chronic and often disabling anxiety
disorder (Skoog & Skoog, 1999). Similarities between OCD and schizophrenia have been
the focus of much research (e.g. Enright, 1996; Hwang, Morgan & Losconzcy, 2000; Insel
& Akiskal, 1986; Lysaker et al, 2000; Tolin, Abramowitz, Przeworski & Foa, 2001).
Enright and Beech (1990) have even suggested that OCD may be a mild form of
schizophrenia. Recent research has shown that approximately 25-50% of individuals with
schizophrenia experience significant obsessive or compulsive symptomatology (Berman,
Kalinowski, Berman, Lengua & Green, 1995; Nechmad et al, 2003; Tibbo & Warneke,
1999) and that 15-26% meet the diagnostic criteria for OCD (Nechmad et al, 2003; Ohta,
Kokai & Morita, 2003). The similarities between obsessive-compulsive (OC) symptoms
and auditory hallucinations of schizophrenia have also been noted. For example, patients
with OCD have been found to have elevated scores on measures of schizotypy, especially
those related to positive symptomatology and predisposition to hallucinations (Enright &
Beech, 1990). The following is a review of the epidemiological, clinical, cognitive and
neuropathological features of OCD, together with a critical examination of the similarities
between OCD and auditory hallucinations.
Epidemiological and clinical features of OCD
Epidemiologic studies suggest that the lifetime prevalence of OCD is between 2%
and 3% in the general population (Andrews, Crino, Hurt, Lampe & Page, 2004), although
the true rates are difficult to estimate because of the secretive nature of the disorder and
because many do not seek treatment. The incidence of OCD is slightly higher in women
than men. Similar to schizophrenia, onset of OCD often occurs before 25 years of age,
there is poor prognosis and poor response to treatment (Enright, 1996).
Based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV, APA
1996), the diagnostic criterion for OCD is the presence of either obsessions or compulsions
that are time consuming, taking more than 1 hour each day and which significantly interfere
with the person’s normal functioning.
Obsessions are defined as ideas, thoughts and impulses that enter the subject's mind
repeatedly. They are recognized as the product of the sufferer's own mind, are recurrent
and persistent, and are perceived to be intrusive, inappropriate and senseless (Andrews et
al, 1994). Some of the more common obsessions include recurrent aggressive or horrific
images, pathologic doubt, fear of contamination and need for order or symmetry.

Chapter 9
- 207 -
Compulsions are repetitive or stereotyped behaviours that are performed in response to an
obsession, to prevent the occurrence of an unlikely event, or to prevent discomfort. The
most common compulsive behaviours include washing, checking, counting, ordering and
repeating words or actions (Andrews et al, 1994). Typically, patients experience both
obsessions and compulsions and only rarely are compulsions experienced without
obsessions. Although OCD is a unitary diagnosis, patients often experience multiple forms
of obsessions or compulsions and the phenomenology may change over time (Akhtar, Wig,
Varma, Pershad & Verma, 1975; Andrews et al, 1994; Calamari, Wiegartz & Janeck, 1999;
Lochner & Stein, 2003). Obsessive thoughts and compulsive behaviours are frequently, but
often unsuccessfully, resisted leading to distress and significant disruption in day-to-day
functioning.
The most striking similarity between OCD and auditory hallucinations is that they are
both characterised by persistent intrusive thoughts. Nayani and David (1996) noted that
"the perseverative and intrusive character of hallucinations bears a striking resemblance to
the phenomena of the obsessional patient” (p. 264). Chadwick and Birchwood (1994) also
reported that the contents of some patients' auditory hallucinations, which include being
told to kill or hit people, to steal and to commit suicide, are very similar to the contents of
obsessions, with the most typical themes involving aggression, sex and blasphemy. Aubrey
Lewis in 1935 (Insel & Akiskal, 1986) pointed out that: "it must be a very short step from
feeling that one must struggle against thoughts that are not one's own, to believing that they
are forced upon one by an external agency", highlighting the fact that although intrusive
thoughts in OCD are experienced as being unintended, they are not attributed to another
agency, as is the case with auditory hallucinations.
Other similarities between OCD and auditory hallucinations include the observation
that they are both highly distressing to the sufferer and that they both interfere significantly
with normal daily routine and occupational functioning (Clark, 1995; Morrison, 2001).
Patients are often impaired socially and suffer from lowered quality of life and significant
functional disability (Goodman, 1999). Both OCD and auditory hallucinations also often
co-occur with depression and with other anxiety disorders (Andrews et al, 1994; Rachman
& Hodgson, 1980).

Chapter 9
- 208 -
Neuropathology of OCD
There are a number of similarities in brain regions thought to be involved in both
OCD and auditory hallucinations. OCD has been associated with a deficit of the fronto-
striatal circuitry, involving the orbitofrontal cortex (OFC), cingulate gyrus and striatum
abnormalities (Breiter & Rauch, 1996; Kim, Park, Shin & Kwon, 2002; Mataix-Cols et al,
1999; Rauch, 1996; Rosenberg & Keshavan, 1998). Evidence arises partly from
neurosurgical data that shows that operations such as capsulotomy or cingulectomy are
often effective for patients with intractable symptoms (Dougherty et al, 2002). Structural
and functioning imaging studies have also identified abnormalities in the inferior prefrontal
cortex, the basal ganglia (especially the caudate nucleus), thalamus and the cingulate gyrus
(Breiter et al 1996; Hajcak & Simons, 2002; Kim et al, 2002; Pujol et al, 1999; Rauch et al,
1996; Saxena, Brody, Schwartz & Bazter, 1998; Szeszko et al, 1999). Abnormalities have
also been identified in the structures of the mesiotemporal lobes, the amygdala and the
hippocampus (Breiter et al, 1996; Szeszko et al, 1999).
The brain regions activated by the experience of auditory hallucinations are very
similar to the proposed neuroanatomical substrates of OCD. For instance, the inferior
prefrontal cortex (including the OFC), cingulate gyrus, basal ganglia, thalamus and
hippocampus have all been found to be activated in the hallucinatory experience (Copolov
et al, 2003; Silbersweig et al, 1995; Takebayashi, Takei & Mori, 2002; Woodruff &
Murray, 1994).
Neuropsychological findings
Patients with OCD and auditory hallucinations also share some similarities in
cognitive profile. The most consistent reports of cognitive impairment in OCD have been
on tests of executive functions (particularly inhibition) and memory functioning. The
following provides an overview of the cognitive findings in OCD, together with a review of
the similarities between deficits shown in OCD and auditory hallucinations.
The repetitive and uncontrollable thoughts in OCD suggest difficulties in cognitive
control and in inhibiting inappropriate response sets (Rachman & Hodgson, 1980). Such an
impairment forms the basis of some cognitive behavioural models, which suggest that
faulty inhibitory processes underlie the intrusive and repetitive clinical obsessions
(Rachman, 1998; Salkovskis, 1998; Tolin, Abramowitz et al, 2002; Tolin, Hamlin & Foa,

Chapter 9
- 209 -
2002). In support, OCD patients have consistently been found to show impaired inhibition
on various paradigms. There is some evidence of an impairment in intentional inhibition as
demonstrated by impairments on the task shifting conditions of the Wisconsin Card Sorting
Test (e.g. Okasha et al, 2000; Purcell, Maruff, Kyrios & Pantelis, 1998; Tallis, 1997), on
affective words in a Directed Forgetting procedure (Tolin, Hamlin & Foa, 2002; Wilhelm,
McNally, Baer & Florin, 1996), antisaccade tasks (Maruff, Purcell, Tyler, Pantelis &
Currie, 1999; Rosenberg, Averbach, O’Hearn, Seymour, Birmaher & Sweeny, 1997;
Rosenberg, Dick, O’Hearn & Sweeney, 1997), and on the Go/Nogo paradigm (Bannon et
al, 2002). Impaired automatic inhibition has also been identified on Negative Priming
tasks (Enright & Beech, 1990, 1993a, b), visuospatial priming tests (Hartston & Swerdlow,
1999) and a Lexical Decision paradigm (Tolin, Abramowitz et al, 2002). Finally, reduced
interference control has been demonstrated on the Stroop interference task (Bannon,
Gonsalvez, Croft & Boyce, 2002; Hartston & Swerdlow, 1999; Martinot et al, 19990;
Schmidtke, Schorb, Winkelmann & Hohagen, 1998) and other tests of selective attention
(Clayton, Richards & Edwards, 1999).
In sum, similarly to patients with auditory hallucinations, patients with OCD have
demonstrated impairments on tasks of intentional inhibition. However, OCD patients have
shown additional deficits on automatic forms of inhibition and in interference control, on
which patients with auditory hallucinations have not been found to be impaired.
Difficulties on other tasks of executive functions have also often been demonstrated
in OCD (e.g. Mataix-Cols et al, 1999; Okasha et al, 2000; Purcell et al, 1998; Tallis, 1997).
In particular, difficulties in abstract thinking (Tallis et al, 1997), mental control and
cognitive flexibility (Okasha et al, 2000) have been identified, although many studies have
failed to find impairments on executive tasks (e.g. Kim et al, 2002; Martinot et al, 1990;
Purcell et al, 1998; Schmidtke et al, 1998). Difficulties on tasks of executive functioning
have often been attributed to patients with schizophrenia (e.g. Elvevag & Goldberg, 2000),
although not specifically to auditory hallucinations.
Memory functioning has also been investigated in OCD. A number of studies have
identified compromised nonverbal memory abilities (Kim et al, 2002; Martinot et al, 1990;
Purcell, 1998; Tallis, Pratt & Jamani, 1999). There is also some evidence that OCD is
associated with a verbal memory deficit (Martinot et al 1990; Savage et al, 1999), although

Chapter 9
- 210 -
this has not been consistently supported (Rubenstein, Peynircioglu, Chambles & Pigott,
1993; Tallis, 1997).
Context memory abilities have also been examined in OCD. Similarly to the
proposal of a reality-monitoring deficit in auditory hallucinations, a poor memory for
actions has been identified in OCD, and particularly in OCD checkers (Rubenstein et al,
1993; Sher, Frost, Kushner, Crews & Alexander, 1989; Tolin, Abramowitz et al, 2002).
According to this proposal, OCD checkers have difficulties differentiating between
memories of performed acts and memories of imagined acts (Johnson, Hashtroudi &
Lindsay, 1993). Studies examining action memory have come up with mixed results. For
instance, Ruberstein et al (1993) and Ecker and Engelkamp (1995) found evidence to
support the proposal that individuals with OCD have difficulties remembering whether they
have performed or imagined certain actions. By contrast, other studies have shown no
difference from healthy controls in reality-monitoring skills (Constans, Foa, Franklin &
Mathews, 1995; McNally & Kohlbeck, 1993; Merckelback & Wesse, 2000; Tallis, 1997;
Tallis et al, 1999). An alternative proposal suggests that the deficit characterising OCD is
not one of memory per se but due to lack of confidence in memory, as doubts regarding a
memory may also result in repeated checking. In support, many studies have investigated
confidence judgements in OCD and have found impaired knowledge about one's memory
capabilities (Constans et al, 1995; Foa, Amir, Gershuny, Molnar & Kozak, 1997; Jurado,
Junque, Vallejo, Salgado & Grafman, 2002; MacDonald, Antony, Macleod & Richter,
1997; McNally & Kohlbeck, 1993; Merckelbach & Wessel, 2000; Rachman & Hodgson,
1980; Tolin, Abramowitz, Kozak & Foa, 2001; Tolin, Abramowitz, et al, 2002).
Temporal context memory was investigated by Jurado et al (2002). These authors
tested temporal ordering of a list of words in patients with OCD compared to healthy
controls. They found that OCD patients showed impairments in sequentially ordering
words despite normal recognition memory, and argued that the patients had a deficit in
temporal memory.
As a summary, executive functions, and particularly inhibitory processes, have been
found to be impaired in patients with OCD. OCD patients have also been shown to have
compromised memory functioning in nonverbal memory and, possibly, in context memory.
Although patients with auditory hallucinations also show deficits in intentional inhibition

Chapter 9
- 211 -
and context memory, it is unclear whether both disorders share the exact same deficits.
This is the subject of our next investigation.
Maintenance theories of OCD
Two main cognitive-behavioural formulations have been put forward to explain the
maintenance process of OC symptoms.
Central to Salkovskis’ (1985; 1989; 1998; Salkovskis, Richards & Forrester, 1995;
Salkovskis et al, 2000) theory is the notion of responsibility. He proposes that intrusive
thoughts escalate in frequency and intensity with the dysfunctional belief that one has
become or may become responsible for harm to oneself or others. This results in negative
appraisal of the thought and ultimately the conclusion that something must be done to put
matters right (neutralize, suppress, perform compulsive acts etc). A cycle is created
because this behaviour perpetuates the dysfunctional belief that one has the responsibility to
protect others or onself from harm. Thought suppression activities are also thought to be a
particularly important component of this theory, based on Wegner’s (1994) findings that
deliberate thought suppression is associated with an increase in frequency and persistent
recurrence of unwanted thoughts. Efforts to control obsessional thoughts are thought to
result in increasing accessibility of these thoughts and prime the negative appraisal of the
thoughts (Purdon & Clark, 2001; Salkovskis, 1985, 1989). Furthermore, this deliberate
effort at suppressing unwanted thoughts is thought to have a negative impact on mood by
prolonging the emotional intensity of the experience. (Purdon & Clark, 2001). Supporting
evidence for the role of responsibility and thought suppression in OCD comes from
findings that both these factors have been found to serve as mediators between intrusive
thoughts and OC symptoms in healthy people (Smari & Holmsteinsson, 2001).
In an alternative explanation of obsessions, Rachman (1993, 1997, 1998) proposes
that problems occur when there is exaggerated significance about the thoughts, for
example, that they reveal something meaningful about the individual (that one is bad, for
example), or that something negative is going to happen as a result. This catastrophic
misinterpretation of intrusive thoughts is thought to give rise to active resistance
(suppression) and avoidance. These behaviours provide short-term relief that serves to
preserve the misinterpretation. Rachman further proposes four vulnerability factors for
OCD: (a) elevated moral standards, (b) particular cognitive biases such as thought-action
fusion (such that unacceptable thoughts may actually influence the probability of the
Chapter 9
- 212 -
aversive event, or the belief that having a repugnant unacceptable thought is morally
equivalent to carrying out the relevant action), (c) depression and (d) anxiety.
These theories of OCD are not dissimilar to recent socio-psychological theories of
auditory hallucinations, as both propose that a key factor is the way in which the intrusive
thoughts are interpreted. The issue of belief, for example, is central to Birchwood and
Chadwick’s (1997) theory. They have proposed that beliefs about the voices’ intent to do
harm or good develops as a result of an attempt to explain unusual experiences and results
in distress and other negative affect. Morrison (2001) also proposes that the
misinterpretation of intrusive thoughts can result in psychotic symptoms such as auditory
hallucinations. For instance, he has proposed that hallucinating patients exaggerate the
significance of their hallucinations and misinterpret the voices content as being threatening
to their physical and psychological integrity. This produces an increase in negative mood
and physiological arousal, and leads to the development of metacognitive beliefs which, in
turn, contribute to the external attribution of voices and to the maintenance process of
hallucinations. In sum, the role of misinterpretation, dysfunctional beliefs and negative
affect is emphasised in maintenance theories of both OCD and auditory hallucinations.
Conclusions and direction
In sum, the current review highlighted the striking similarities in clinical features
between OCD and auditory hallucinations, particularly regarding the presence of intrusive
and uncontrollable thoughts in both disorders. A summary of the neuropathological and
cognitive processes associated with OCD also pointed out parallels with research findings
on auditory hallucinations. Finally, socio-psychological theories of OC symptomatology
and auditory hallucinations are converging in their proposal that interpretation of intrusive
thoughts is an important component to understanding the maintenance process of both
disorders.
On the basis of the similitudes between OCD and auditory hallucinations, it is
reasonable to investigate further the pattern of cognitive performance that underlies those
two disorders. The next chapter aims to examine the performance of patients with OCD on
tests which have been found to be particularly relevant to investigations of auditory
hallucinations, in particular the HSCT and ICIM test, assessing intentional inhibition
processes, and the Context Memory task, assessing context memory processes.

Chapter 9
- 213 -
References
Akhtar, S., Wig, N., Varma, V., Pershad, D., & Verma, S. (1975). A phenomenological
analysis of symptoms of obsessive-compulsive neurosis. British Journal of
Psychiatry, 127, 342-248.
Andrews, G., Crino, R., Hurt, C., Lampe, L., & Page, A. (1994). Obsessive-Compulsive
Disorder syndrome, The treatment of anxiety disorders. New York: Cambridge
University Press.
Bannon, S., Gonsalvez, C. J., Croft, R. J., & Boyce, P. M. (2002). Response inhibition
deficits in obsessive-compulsive disorder. Psychiatry Research, 110, 165-174.
Berman, I., Kalinowski, A., Berman, S. M., Lengua, J., & Green, A. (1995). Obsessive-
compulsive symptoms in chronic schizophrenia. Comprehensive Psychiatry, 36(1), 6-
10.
Birchwood, M., & Chadwick, P. (1997). The omnipotence of voices: testing the validity of
a cognitive model. Psychological Medicine, 27, 1345-1353.
Breiter, H. C., & Rauch, S. L. (1996). Functional MRI and the study of OCD: from
symptom provocation to cognitive-behavioural probes of cortico-striatal systems and
the amygdala. NeuroImage, 4, S127-S138.
Calamari, J. E., Wiegartz, P. S., & Janeck, A. S. (1999). Obsessive-compulsive disorder
subgroups: a symptom-based clustering approach. Behaviour Research and Therapy,
37, 113-125.
Chadwick, P., & Birchwood, M. (1994). The omnipotence of voices - the cognitive
approach to auditory hallucinations. British Journal of Psychiatry, 164, 190-201.
Clark, D. A. (1995). The assessment of unwanted intrusive thoughts: a review and critique
of the literature. Behaviour Research and Therapy, 33(8), 967-976.
Clayton, I. C., Richards, J. C., & Edwards, C. J. (1999). Selective attention in obsessive-
compulsive disorder. Journal of Abnormal Psychology, 108(1), 171-175.
Constans, J. I., Foa, E. B., Franklin, M. E., & Mathews, A. (1995). Memory for actual and
imagined events for OC checkers. Behaviour, Research and Therapy, 33(6), 665-671.
Copolov, D. L., Seal, M. L., Maruff, P., Ulusoy, R., Wong, M. T. H., Tochon-Danguy, H.
J., & Egan, G. F. (2003). Cortical activation associated with the experience of
auditory hallucinations and perception of human speech in schizophrenia: a PET
correlation study. Psychiatry Research: Neuroimaging, 122, 139-152.

Chapter 9
- 214 -
Dougherty, D.D.(2002). Surgery can aid patients with severe obsessive-compulsive
disorder. American Journal of Psychiatry, 159: 269-275.
Ecker, J. & Engelkamp, J. (1995). Memory for actions in obsessive-compulsive disorder.
Behaviour Cognitive Psychotherapy. 23: 349-371.
Elvevag, B., & Goldberg, T. E. (2000). Cognitive impairment in schizophrenia is the core
of the disorder. Critical Reviews in Neurobiology, 14(1), 1-21.
Enright, S., & Beech, A. (1990). Obsessional states: anxiety disorders or schizotypes? An
information processing and personality assessment. Psychological Medicine, 20, 621-
627.
Enright, S. J. (1996). Obsessive-compulsive disorder: Anxiety disorder or schizotype? In R.
M. Rapee (Ed.), Current controversies in the anxieties disorders (pp. 161-190). New-
York, London: Guilford Press.
Enright, S. J., & Beech, A. R. (1993a). Further evidence of reduced cognitive inhibition in
obsessive-compulsive disorder. Personality and Individual Differences., 14(3), 387-
395.
Enright, S. J., & Beech, A. R. (1993b). Reduced cognitive inhibition in obsessive-
compulsive disorder. British Journal of Clinical Psychology, 32, 67-74.
Foa, E. B., Amir, N., Gershuny, B., Molnar, C., & Kozak, M. J. (1997). Implicit and
Explicit Memory in Obsessive-Compulsive Disorder. Journal of Anxiety Disorders,
11(2), 119-129.
Frith, C. (1996). The role of the prefrontal cortex in self-consciousness: the case of auditory
hallucinations. Philosophical Transactions of the Royal Society of London: B, 351,
1505-1512.
Frith, C., & Dolan, R. J. (1997). Brain mechanisms associated with top-down processes in
perception. Philosophical Transactions of the Royal Society of London, B, 352, 1221-
1230.
Goodman, W. K. (1999). Obsessive-compulsive disorder: diagnosis and treatment. Journal
of Clinical Psychiatry, 60(18), 27-32.
Hajcak, G., & Simons, R. F. (2002). Error-related brain activity in obsessive-compulsive
disorder. Psychiatry Research, 110, 63-72.
Hartston, H. J., & Swerdlow, N. R. (1999). Visuospatial priming and Stroop performance in
patients with obsessive-compulsive disorder. Neuropsychology, 13(3), 447-457.

Chapter 9
- 215 -
Hwang, M., Morgan, J., & Losconzcy, M. (2000). Clinical and neuropsychological profiles
of obsessive-compulsive schizophrenia; A pilot study. The Journal of
Neuropsychiatry and Clinical Neurosciences, 12, 91-94.
Insel, T. R., & Akiskal, H. S. (1986). Obsessive-Compulsive Disorder with psychotic
features: A phenomenologic analysis. American Journal of Psychiatry, 143(12), 1527-
1533.
Johnson, M. K., Hashtroudi, S., & Lindsay, D. S. (1993). Source Monitoring. Psychological
Bulletin, 114(1), 3-28.
Jurado, M. A., Junque, C., Vallejo, J., Salgado, P., & Grafman, J. (2002). Obsessive-
Compulsive Disorder (OCD) patients are impaired in remembering temporal order
and in judging their own performance. Journal of Clinical and Experimental
Neuropsychology, 24(3), 261-269.
Kim, M.-S., Park, S.-J., Shin, M.-S., & Kwon, J. S. (2002). Neuropsychological profile in
patients with obsessive-compulsive disorder over a period of 4-month treatment.
Journal of Psychiatric Research, 36, 257-265.
Lochner, C., & Stein, D. J. (2003). Heterogeneity of obsessive-compulsive disorder: a
literature review. Harvard Review of Psychiatry, 11, 113-132.
Lysaker, P. H., Marks, K. A., Picone, J. B., Rollins, A. L., Fastenau, P. S., & Bond, G. R.
(2000). Obsessive-compulsive symptoms in schizophrenia. The Journal of Nervous
and Mental Disease, 188(2), 78-83.
Macdonald, P. A., Antony, M. A., Macleod, C. M., & Richter, M. A. (1997). Memory and
confidence in memory judgements among individuals with obsessive-compulsive
disorder and non-clinical controls. Behaviour, Research & Therapy, 35(6), 497-505.
Martinot, J. L., Allilare, J. F., Mazoyer, B. M., Hantouche, E., Huret, J. D., Legaut-Demare,
F., Deslauriers, A. H., Hardy, P., Pappata, S., Baron, J. C., & Syrota, A. (1990).
Obsessive-compulsive disorder: a clinical, neuropsychological and positron emission
tomography study. Acta Psychiatrica Scandinavica, 82, 233-242.
Maruff, P., Purcell, R., Tyler, P., Pantelis, C., & Currie, J. (1999). Abnormalities of
internally generated saccades in obsessive-compulsive disorder. Psychological
Medicine, 29, 1377-1385.

Chapter 9
- 216 -
Mataix-Cols, D., Junque, C., Sanchez-Turet, M., Vallejo, J., Verger, K., & Barrios, M.
(1999). Neuropsychological functioning in a subclinical obsessive-compulsive
sample. Biological Psychiatry, 45, 898-904.
McNally, R. J., & Kohlbeck, P. A. (1993). Reality monitoring in obsessive-compulsive
disorder. Behaviour Research and Therapy, 31(3), 249-253.
Merckelback, H., & Wessel, I. (2000). Memory for actions and dissociation in obsessive-
compulsive disorder. Journal of Nervous and Mental Disease, 188(12), 846-848.
Morrison, A. P. (2001). The interpretation of intrusions in psychosis: an integrative
cognitive approach to hallucinations and delusions. Behavioural and Cognitive
Psychotherapy, 29, 257-276.
Nayani, T., & David, A. (1996). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & T. R. E. Barnes (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 . New York: John Wiley
& Sons Ltd.
Nechmad, A., Ratzoni, G., Poyurovsky, M., Meged, S., Avidan, G., Fuchs, C., Bloch, Y., &
Weizman, R. (2003). Obsessive-compulsive disorder in adolescent schizophrenia
patients. American Journal of Psychiatry, 160, 1002-1004.
Ohta, M., Kokai, M., & Morita, Y. (2003). Features of obsessive-compulsive disorder in
patients primarily diagnosed with schizophrenia. Psychiatry and Clinical
Neurosciences, 57, 67-74.
Okasha, A., Rafaat, M., Mahallawy, N., El Nahas, G., Seif El Dawla, A., Sayed, M., & El
Kholi, S. (2000). Cognitive dysfunction in Obsessive-Compulsive Disorder. Acta
Psychiatrica Scandinavica, 101, 281-285.
Pujol, J., Torres, L., Deus, J., Cardoner, N., Pifarre, J., Capdevila, A., & Vallejo, J. (1999).
Functional magnetic resonance imaging study of frontal lobe activation during word
generation in obsessive-compulsive disorder. Biological Psychiatry, 45(7), 891-897.
Purcell, R., Maruff, P., Kyrios, M., & Pantelis, C. (1998). Neuropsychological Deficits in
Obsessive-Compulsive Disorder: A comparison with unipolar depression, panic
disorder, and normal controls. Archives of General Psychiatry, 55, 415-423.
Purdon, C., & Clark, D. (2001). Suppression of obsession-like thoughts in nonclinical
individuals: impact on thought frequency, appraisal and mood state. Behaviour
Research and Therapy, 39, 1163-1181.

Chapter 9
- 217 -
Rachman, S. (1993). Obsessions, responsibility and guilt. Behaviour Research and
Therapy, 31(2), 149-154.
Rachman, S. (1997). A cognitive theory of obsessions. Behaviour Research and Therapy,
35(9), 793-802.
Rachman, S. (1998). A cognitive theory of obsessions: elaborations. Behaviour Research
and Therapy, 36, 385-401.
Rachman, S. J., & Hodgson, R. J. (1980). Obsessions and Compulsions. New Jersey:
Prentice Hall Inc.
Rachman, S., & Hodgson, R. (1980). Obsessions and Compulsions.
Rauch, S. L. (1996). Neuroimaging in obsessive-compulsive disorder and related disorders.
In Jenike MA, chairperson. Recent developments in neurobiology of obsessive-
compulsive disorder. Journal of Clinical Psychiatry, 57(10), 492-495.
Rosenberg, D. R., & Keshavan, M. S. (1998). Toward a neurodevelopmental model of
obsessive-compulsive disorder. Biological Psychiatry, 43, 623-640.
Rosenberg, D. R., Averbach, D. H., O'Hearn, K. M., Seymour, A. B., Birmaher, B., &
Sweeney, J. A. (1997). Oculomotor response inhibition abnormalities in paediatric
obsessive-compulsive disorder. Arch Gen Psychiatry, 54, 831-838.
Rosenberg, D. R., Dick, E. L., O'Hearn, K. M., & Sweeney, J. A. (1997). Response-
inhibition deficits in obsessive-compulsive disorder: an indicator of dysfunction in
frontostriatal circuits. Journal of Psychiatry and Neuroscience, 22(1), 29-38.
Rubenstein, C. S., Peynircioglu, Z. F., Chambles, D. L., & Pigott, T. A. (1993). Memory in
sub-clinical obsessive-compulsive checkers. Behaviour, Research and Therapy, 31(8),
759-765.
Salkovskis, P. M. (1985). Obsessional-compulsive problems: a cognitive behavioural
analysis. Behaviour, Research & Therapy, 23(5), 571.
Salkovskis, P. M. (1989). Cognitive-behavioural factors and the persistence of intrusive
thoughts in obsessional problems. Behavioural Research and Therapy, 27(6), 677-
682.
Salkovskis, P. M. (1998). Psychological approaches to the understanding of obsessional
problems. In S. e. al (Ed.), OCD.
Chapter 9
- 218 -
Salkovskis, P. M., Richards, H. C., & Forrester, E. (1995). The relationship between
obsessional problems and intrusive thoughts. Behavioural and Cognitive
Psychotherapy, 23, 281-299.
Salkovskis, P. M., Wroe, A. L., Gledhill, A., Morrison, N., Forrester, E., Richards, C.,
Reynolds, M., & Thorpe, S. (2000). Responsibility attitudes and interpretations are
characteristic of obsessive compulsive disorder. Behaviour Research and Therapy, 38,
347-372.
Savage, C. R., Baer, L., Keuthen, N. J., Brown, H. D., Rauch, S. L., & Jenike, M. A.
(1999). Organizational strategies mediate nonverbal memory impairment in
obsessive-compulsive disorder. Biological Psychiatry, 45, 905-916.
Saxena, S., Brody, A. L., Schwartz, J. M., & Baxter, L. R. (1998). Neuroimaging and
frontal-subcortical circuitry in obsessive-compulsive disorder. British Journal of
Psychiatry, 173(Suppl. 35), 26-37.
Schmidtke, K., Schorb, A., Winkelmann, G., & Hohagen, F. (1998). Cognitive frontal lobe
dysfunction in obsessive-compulsive disorder. Biological Psychiatry, 43(9), 666-673.
Sher, K.J., Frost, R.O., Kushner, M., Crews, T.M. & Alexander, J.E. (1989). Memory
deficits in compulsive checkers: replication and extension in a nonclinical sample.
Behaviour Research and Therapy, 27, 65-69.
Silbersweig, D. A., Stern, E., C, F., & al, e. (1995). A functional neuroanatomy of
hallucinations in schizophrenia. Nature, 378, 176-179.
Skoog, G., & Skoog, I. (1999). A 40-year follow up of patients with obsessive-compulsive
disorder. Archives of General Psychiatry, 56, 121-127.
Smari, J., & Holmsteinsson, H. E. (2001). Intrusive thoughts, responsibility attitudes,
thought-action fusion, and chronic thought suppression in relation to obsessive-
compulsive symptoms. Behavioural and Cognitive Psychotherapy, 29, 13-20.
Szeszko, P., Robinson, D., Alvir, J., Bilder, R., Lencz, T., Ashtari, M., Wu, H., & Bogerts,
B. (1999). Orbital frontal and amygdala volume reductions in obsessive-compulsive
disorder. Archives of General Psychiatry, 56(10), 913-919.
Takebayashi, H., Takei, N., & Mori, N. (2002). Unilateral auditory hallucinations in
schizophrenia after damage to the right hippocampus. Schizophrenia Research.

Chapter 9
- 219 -
Tallis, F. (1997). The neuropsychology of obsessive-compulsive disorder: A review and
consideration of clinical implications. British Journal of Clinical Psychology, 36, 3-
20.
Tallis, F., Pratt, P., & Jamani, N. (1999). Obsessive-compulsive disorder, checking, and
non-verbal memory: a neuropsychological investigation. Behaviour Research and
Therapy, 37, 161-166.
Tibbo, P., & Warneke, L. (1999). Obsessive-compulsive disorder in schizophrenia:
epidemiologic and biologic overlap. Journal of Psychiatry & Neuroscience, 24(1), 15-
24.
Tolin, D. F., Abramowitz, J. S., Drigidi, B. D., Amir, N., Street, G. P., & Foa, E. B. (2001).
Memory and memory confidence in obsessive-compulsive disorder. Behaviour
Research and Therapy, 39, 913-927.
Tolin, D. F., Abramowitz, J. S., Kozak, M. J., & Foa, E. B. (2001). Fixity of belief,
perceptual aberration, and magical ideation in obsessive-compulsive disorder.
Anxiety Disorders, 15, 510-510.
Tolin, D. F., Abramowitz, J. S., Przeworski, A., & Foa, E. B. (2002). Thought suppression
in obsessive-compulsive disorder. Behaviour Research and Therapy, 40, 125501274.
Tolin, D. F., Hamlin, C., & Foa, E. B. (2002). Directed forgetting in obsessive-compulsive
disorder: replication and extension. Behaviour Research and Therapy, 40, 793-803.
Wilhelm, S., McNally, R., Baer, L., & Florin, I. (1996). Directed forgetting in obsessive-
compulsive disorder. Behaviour Research and Therapy, 34(8), 633-641.
Woodruff, P. W. R., & Murray, R. M. (1994). The aetiology of brain abnormalities in
schizophrenia. In R. Ancill (Ed.), Schizophrenia: Exploring the Spectrum of
Psychosis . New York: John Wiley & Sons Ltd.

- 221 -
Chapter 10
Obsessive-Compulsive Disorder: Intentional inhibition and context memory processes
Abstract
The model of auditory hallucinations in schizophrenia presented in Waters,
Badcock, Michie and Maybery (2004) suggests that a combination of deficits in both
intentional inhibition and context memory is necessary for auditory hallucinations to occur.
Consequently, patients who do not experience auditory hallucinations may show an
impairment in either intentional inhibition or context memory and none should present with
deficits in both. The current study tested this proposal in a group of patients with
Obsessive-Compulsive Disorder (OCD). Like patients with hallucinations, OCD patients
experience intrusive and unwanted thoughts but, unlike hallucinating patients, they do not
mistake the origins of these thoughts. Accordingly, the aims of this study were to assess
whether patients with OCD would show (a) poor inhibitory functioning but (b) intact
memory for context, and that, in a test of the model, (c) none of the patients with OCD
would present with deficits in both domains simultaneously. Fourteen participants with
OCD participated in the study and were tested on the Hayling Sentence Completion Test
(Burgess & Shallice, 1996) and the Inhibition of Currently Irrelevant Memories task
(Schnider & Ptak, 1999), assessing intentional inhibition processes, and a Context Memory
task. Consistent with the hypotheses, the results revealed that (a) patients with OCD
showed a deficit on tasks of intentional inhibition compared to healthy controls, (b) patients
were not significantly different from controls in any of the conditions of the Context
Memory task, and (c) only one of the 14 patients showed the specified combination of
deficits. The results provide strong support for our model of auditory hallucinations.
Results are discussed with reference to similar studies of schizophrenia patients with
auditory hallucinations.

Chapter 10
- 222 -
According to the model of auditory hallucinations in schizophrenia outlined in
Waters, Badcock, Michie and Maybery (2004), a combination of deficits in both intentional
inhibition and contextual memory is critical to the experience of auditory hallucinations. It
was proposed that the deficit in intentional inhibition leads to mental representations
intruding into consciousness in a manner that is beyond the control of the sufferer, and the
deficit in binding contextual cues results in an inability to form a complete representation of
the origins of mental events. Consequently, it was anticipated that patients (with or without
schizophrenia) who do not experience auditory hallucinations may demonstrate a deficit in
either intentional inhibition or context memory, but none should present with this particular
combination of deficits. As a test of this model, the current study examines the intentional
inhibition and context memory abilities of patients with Obsessive-Compulsive Disorder
(OCD).
Both auditory hallucinations and OCD are characterized by recurrent and persistent
thoughts which sufferers are not able to control. The co-expression of this characteristic
may reflect an overlap of cognitive deficits associated with OCD and auditory
hallucinations. Since a deficit in intentional inhibition has been linked to the intrusive and
unwanted character of hallucinations (see Badcock, Waters & Maybery, in press; Waters,
Badcock, Maybery & Michie, 2003), it is reasonable to suggest that OCD patients might
also show the same deficit. In Badcock et al (in press) and Waters et al (2003), we
demonstrated that auditory hallucinations were associated with deficits on the Hayling
Sentence Completion Test (HSCT, Burgess & Shallice, 1996) and/or the Inhibition of
Currently Irrelevant Memories task (ICIM, Schnider & Ptak, 1999), which require the
volitional inhibition of currently active mental associations and irrelevant memories
respectively. Accordingly, it was anticipated that patients with OCD would show a deficit
on these tasks.
One crucial difference between the two disorders, however, is that there is no loss of
personal agency in OCD, with sufferers claiming ownership of the intrusive thoughts. It
has been suggested that correctly identifying the origins of mental events is contingent on
intact context memory (Johnson, Hashtroudi & Lindsay, 1993). In episodic memory
research, a distinction between the 'content' and 'context' of memory events is often made,
content referring to the event itself while context usually refers to extrinsic features that are
not part of the stimulus itself, such as the source of an action or its temporal context. There

Chapter 10
- 223 -
is evidence that memory for the content and context of an event may be functionally
dissociable (Cabeza et al, 1997; Nyberg et al, 1996). In Waters, Badcock et al (2004), we
showed that significantly more patients with auditory hallucinations had a deficit in some
form of memory for context (source or temporal memory, or both) compared to patients
without hallucinations. We speculated that this deficit in context memory results in an
inability to form a complete representation of the origins of mental events, leading to a
failure to recognize hallucinated events as being self generated.
The ability of OCD patients to identify the origin of their thoughts suggests that
contextual memory should be intact in patients with OCD. However, this proposal
contrasts with studies that have shown poor memory for actions in OCD (e.g. Tolin,
Abramowitz, Przeworski & Foa, 2002). These studies show that OCD patients, and in
particular OCD checkers, have difficulties differentiating between memories of performed
acts and memories of imagined acts, which can be interpreted as a source memory deficit.
Jurado, Junque, Vallejo, Salgado and Grafman (2002) have also shown poor temporal order
judgment in patients with OCD, suggesting that temporal memory may be impaired in
OCD. In order to investigate whether context memory is impaired in OCD, the
performance of patients on the Context Memory task was examined. In this task (as used in
Waters, Maybery et al, 2004), memory for events is assessed in conjunction with memory
for both source and temporal information. The task therefore tests recognition for specific
events, the source of these events, when the events occurred and the ability to bind the two
contextual features together.
In sum, in view of the observations that patients with OCD experience intrusive
thoughts, but that they do not mistake the origins of these thoughts, the aims of the current
study were to identify whether patients with OCD would show 1) poor inhibitory
functioning on tasks of intentional inhibition, namely on the HSCT and ICIM task; but 2)
intact context memory abilities on the Context Memory task. In a crucial test of our
combined-deficit model of auditory hallucinations, the study will also test the proposal that
OCD patients may show a deficit in either intentional inhibition or context memory, but
none should show combined deficits in both cognitive domains.

Chapter 10
- 224 -
Method
Participants
Fourteen OCD outpatients were recruited via their treating psychiatrist or through
community advertising. The MINI (Mini International Neuropsychiatric Interview;
Sheehan et al, 1998) was administered to confirm the diagnosis of OCD and identify the
presence of other psychiatric disorders. Duration of illness ranged from 2 to 37 years. Ten
of the 14 patients were on antidepressant medication and one of these was also on a mood
stabilizer. The control group comprised 24 healthy individuals recruited from the
community through a blood donor organization. Exclusion criteria for all participants
included a history of head injury, neurological illness, substance abuse or dependence
within the last 6 months, English as a second language, a personal or family history of
psychosis or schizophrenia disorder and reports of any past or present auditory
hallucinations that were not as a result of a fever or drugs. The demographic and clinical
characteristics of participants are presented in Table 1. The study protocol was approved
by the human research ethics committee of the University of Western Australia and the
institutional ethics committee at Graylands Hospital. All participants provided signed
informed consent prior to their participation in the study.
Clinical ratings
The 10-item Yale-Brown Obsessive Compulsive Scale (Y-BOCS, Goodman et al,
1989a, b) is a self-report measure whereby patients are asked to answer 5 questions
regarding the severity of obsessions and 5 questions pertaining to the severity of
compulsions. The Y-BOCS has been reported to have good reliability and validity
(Goodman, 1999; Goodman et al, 1989a, b) and excellent internal consistency and test-
retest reliability (Steketee, Frost & Bogart, 1996). Total scores can range from 0 to 40.
The range of total scores in the present OCD sample was 9 – 31, confirming the presence of
significant symptomatology. The mean Y-BOCS subscale and total scores of the current
OCD sample (see Table 1) were within the range of previously reported data (e.g. Denys,
De Geux, Van Megen & Westenberg, 2000).

Chapter 10
- 225 -
Table 1.
Demographic data for controls and patients with OCD (means and SD) Controls OCD
(n = 24) (n = 14)
Age 34.67 (8.71) 36.00 (11.10)
Gender 20 M, 4 F 5 M, 9 F
Handedness 19 R, 4 L 13 R, 1 L
Years Education 11.75 (1.89) 14.79 (1.72)
NART 103.62 (4.75) 109.07 (6.26)
Y-BOCS total - 20.57 (6.19)
OBSESSION score1 - 10.21 (4.19)
COMPULSION score1 - 10.35 (2.64)
Duration of illness (yrs) - 13.28 (9.55)
Age onset - 22.71 (7.26)
BDI-II 2.04 (1.98) 18.71 (12.01)
BAI 1.54 (1.79) 14.36 (9.92) 1 On Y-BOCS
Tasks and questionnaires
Beck Depression Inventory (BDI-II) and Beck Anxiety Inventory (BAI) (Beck, 1996,
1990).
These tests both have a maximum score of 21.
Assessment of General Intelligence
Premorbid intelligence was estimated using the National Adult Reading Test-revised
(Nelson, 1982).
Hayling Sentence Completion Test (HSCT; Burgess & Shallice, 1996)
In this test the participant was required to provide single-word completions to
sentences. In the first condition (Response Initiation), subjects were required to finish the
sentence with a word that would complete it in a sensible fashion, and in the second
condition (Response Suppression) subjects were required to complete the sentence with a
word that was unrelated to the context of the sentence. Latencies for the two conditions

Chapter 10
- 226 -
were recorded. A Response Inhibition measure was obtained by calculating the difference
in latency for the Response Initiation and Response Suppression conditions. Consistent
with the test manual, two errors types were recorded in the Response Suppression
condition: A category A error was where the supplied word completed the sentence in a
plausible fashion (e.g. 'most cats see very well at...night'), and a category B error was where
the response was semantically connected to the sentence, but was not the most plausible
completion (e.g. 'the dough was put in the hot…kitchen'.
Inhibition of Currently Irrelevant Memories task (ICIM; adapted from Schnider & Ptak,
1999, as used in Waters et al, 2003)
This task involved the presentation of a series of animal pictures (selected from the
Berkeley Digital Library Project collection) for repeated identification. Four runs were
shown of the same basic set of 52 pictures. Four pictures were repeated 8 times within each
run as described by Schnider and Ptak. These target items were different for the 4 runs.
The pictures were presented for 2000 ms each with an inter-stimulus interval of 1000 ms.
Immediately after the 1st run, the 2nd run was presented. A 3rd run was made 5 minutes after
the 2nd run, and the 4th run was made after a 30-minute delay. For the first run, participants
were told that pictures of animals would be presented and that some would be shown more
than once. The task was to identify which pictures were repeated. For each subsequent run,
participants were instructed to forget that they had already seen the pictures and to indicate
picture reoccurrences only within that run. Performance on the first run depended on new
learning, whereas subsequent runs required active inhibition of memory of pictures seen in
the previous runs (Schnider, Treyer & Buck, 2000). Consequently the number of false
alarms (FA) in the last three runs, but not the first, was used to index inability to inhibit
irrelevant memories.
Context Memory task (adapted from Conway & Dewhurst, 1995; Danion, Rizzo & Bruant,
1999; Huppert & Piercy, 1978, as used in Waters, Maybery, Badcock & Michie, 2004)
Participants watched or performed pairings of two sets of 24 household objects over
two sessions 30 minutes apart.
Materials: There were 48 common household objects. Half were allocated to the
'watch' action (participants watched the experimenter pair the objects) and half to the
'perform' action (participants performed the pairing themselves). A series of cards provided
instructions to position objects next to one another or to watch the experimenter perform

Chapter 10
- 227 -
the action. In the recognition test, 24 pairs of objects were presented: 16 pairs were kept in
their original combination (‘intact pairs’), and 8 pairs were objects that were re-paired in
new combinations (‘rearranged pairs’). No new objects were added. Objects in new
combinations were kept within the same action sequence (watch/perform) and presentation
session (1 or 2).
Procedure: In the first session, participants were shown 24 common objects set out
randomly on a table. They were told that they would pair objects together or watch the
experimenter pair objects together in two different sessions and were instructed that they
should try to remember which objects went together, who paired them and in which
session, for a test later on. Thirty minutes after the first session the second session took
place. A different set of 24 objects was presented but the procedure remained the same.
Five minutes after the end of the second session, the recognition test was administered
verbally. Pairs of objects were read out individually. Participants indicated whether each
pair was an intact or rearranged combination, and for pairs judged as being intact they had
to specify who performed the pairing (self/experimenter), and when (session 1/2).
Results
Patients with OCD and healthy controls did not differ significantly in age, t(36) = .41,
p = .68. However, patients with OCD had significantly higher premorbid IQ as measured
by the NART, t(36) = 3.02, p < .005, and significantly more years of education compared to
controls, t(36) = 4.92, p < .001 (see Table 1). Patients with OCD also had greater levels of
depression and anxiety, as measured by the BDI-II and BAI respectively, t(36) = 6.70, p <
.001 and t(36) = 6.21, p < .001.
Intentional inhibition
HSCT
Table 2 shows mean scores and standard deviations on the HSCT for each group.
Distributions were approximately normal except for Type A errors which were positively
skewed. Consequently, parametric tests were carried out on all measures except for Type A
errors for which nonparametric tests were used. Patients with OCD were significantly
slower than controls in the Response Suppression condition and on the Response Inhibition
measure, t(36) = 2.59, p < .01, and t(36) = 2.54, p < .01, respectively. This is unlikely to
have been due to generally slower response speed since the two groups did not differ

Chapter 10
- 228 -
significantly on latencies from the Response Initiation condition, t(36) = 1.43, p = .16.
Patients with OCD also made significantly more type B errors than controls, t(36) = 2.22, p
< .05, but there was a nonsignificant difference between the groups on the number of type
A errors, Mann-Whitney U = 166.50, p = .92.
Table 2
Scores on the HSCT (means and SD) Response Initiation, Response Suppression and
Response Inhibition latencies (secs) and Category A and B errors for controls and patients
with OCD
Controls OCD
(n = 24) (n = 14)
Response Initiation 2.66 (1.73) 3.71 (2.78)
Response Suppression 29.33 (24.02) 53.14 (32.16)
Response Inhibition 26.66 (23.87) 49.42 (30.88)
Category A errors .12 (.44) .14 (.53)
Category B errors 2.75 (3.22) 5.42 (4.12)
ICIM task
On the ICIM task, the ability to correctly detect targets was assessed by analyzing the
number of hits for repeated targets across the four runs of the task. There was no
significant difference in total number of hits made by the OCD patients (M = 110.07, SD =
2.33) and healthy controls (M = 110.16, SD = 2.59), t(36) = .11, p = .91.
The number of false alarms made on the first run of the ICIM task reflects new
learning rather than suppression. This measure showed a nonsignificant difference between
patients with OCD and controls, t(36) = .27, p = .78. However, on subsequent runs (i.e.
runs 2-4), which required active inhibition, patients with OCD made significantly more
false alarms compared to controls, t(36) = 2.19, p < .05. This pattern of results is shown in
Figure 1. Finally, the proportion of false alarms to distracters that were targets in previous
runs was also computed. The difference between controls (M = .05, SD = .09) and patients
with OCD (M = .07, SD = .08) was not significant, Mann-Whitney U = 57.50, p = .12.

Chapter 10
- 229 -
0
1
2
3
4
5
6
1 2 3 4
Run
Mea
n nu
mbe
r of f
alse
ala
rms
Healthy controls OCD patients
Figure 1
Mean number of false alarms (with SE) on each run of the ICIM task in the OCD
patients and healthy controls
In summary, patients with OCD made significantly more type B errors compared to
controls on the Response Suppression condition of the HSCT and made significantly more
false alarms on the last three runs of the ICIM test (although not specifically to previous
targets). The percentage of patients with OCD impaired on either of these measures was
calculated with reference to whether scores were in excess of one standard deviation from
control group baseline means. By comparison, the probability that an individual would
score more than one standard deviation from the mean on a normal distribution is .158 so
the probability that an individual would score one standard deviation away from the mean
of controls on one task or another is .291 [using Pr A or B = Pr A + Pr B – (Pr A * Pr B)].
The analyses showed that 10/14 (71.4%) of patients had a deficit on either of these
measures. The patients who were impaired using this criterion were not necessarily those
who took medication, X2(1) = 1.26, p = .26. When a more stringent two standard deviations

Chapter 10
- 230 -
criterion was applied, the results showed that 6/14 (42.85%) of the OCD patients still had
the deficit. The same results were obtained when the calculations were repeated using the
Response Inhibition measure, since those OCD patients who made a high number of type B
errors were the same patients who had significantly longer response latencies compared to
controls on the HSCT.
Inhibitory performance on the HSCT and ICIM tasks was correlated with Y-BOCS
scores on the Obsession and Compulsions subscales, and with the total score, but there
were no significant associations (all p > .08) suggesting that these deficits were not
associated with symptom severity. We also examined whether the current findings could
be accounted for by differences in depression and anxiety, premorbid IQ and education.
BDI-II scores were found to be significantly correlated with latency of inhibition as shown
by the Response Inhibition measure of the HSCT, r = .62, p < .01, but no other correlations
were significant (all p > .08).
Context memory
Table 3 shows the proportions correct data for object pair recognition and for source
and temporal judgments for correctly recognized intact pairs, and the results of analyses
investigating binding. Analyses of memory for content are presented initially followed by
analyses of individual context judgments. Finally, context binding abilities are investigated
in the last analysis.
Intact versus rearranged object pair recognition
The proportions of object pairs correctly recognized as intact or rearranged were
subjected to a 2 (OCD vs. controls) x 2 (intact vs. rearranged object pairs) ANOVA.
Overall recognition accuracy did not differ significantly for intact versus rearranged
stimuli, F(1, 36) = 3.60, p = .07. More significantly, the difference between groups was not
significant, F(1, 36) = .25, p = .61, and there was no significant interaction, F(1, 36) = .25,
p = .61. Signal detection parameters (representing estimates of discrimination accuracy and
bias) were calculated but were not found to be significantly different between the two
groups, t(36) = .51, p = .61, and t(36) = .29, p = .77, respectively.
Source and temporal judgements
Participants provided source and temporal judgments only for stimulus pairs that they
judged to be intact so analyses of context recognition were restricted to correctly
recognized intact stimulus pairs. The proportions of correct source and temporal judgments

Chapter 10
- 231 -
were subjected to a 2 (group) x 2 (source vs temporal context) ANOVA. There was a
significant main effect of context, with source being recalled correctly more often than
temporal context, F(1, 36) = 12.24, p < .001. However, the main effect of group and the
interaction were not significant, F(1, 36) = 1.26, p = .26, and F(1, 36) = .50, p = .48,
respectively. Discrimination accuracy values drawn from separate signal detection
analyses for source and temporal information were subjected to a common 2 (group) x 2
(source vs. temporal context) ANOVA. There was a nonsignificant difference between
controls (M = 1.85, SD = .13) and patients (M = 1.68, SD = .17) in discrimination accuracy,
F(1, 36) = .71, p = .40. The effect of context was significant, F(1, 36) = 16.71, p < .001,
but the interaction was not, F(1, 36) = 1.16, p = .28.
Table 3
Means (and standard deviations) of (1) proportions correct for object pair recognition (for intact and new pairs) and for source and temporal judgements for correctly recognized intact pairs, and (2) proportions of correctly recognized intact pairs for which 'who & when' , 'who only', 'when only' and 'neither' were recognised for controls and OCD patients Controls OCD
(n = 24) (n = 14)
1. Content and context memory judgements
Intact object pairs .76 (.17) .75 (.16)
Rearranged object pairs .63 (.25) .68 (.22)
Source judgements .88 (.12) .86 (.13)
Temporal judgements .81 (.14) .75 (.09)
2. Binding of source and temporal information
Who & When .73 (.19) .64 (.14)
Who only .15 (.11) .22 (.11)
When only .08 (.10) .11 (.11)
Neither .03 (.05) .05 (.01)
An analysis of bias for source (i.e. the preference to identify stimuli as self-paired
rather than experimenter-paired) revealed a nonsignificant difference between controls (M
= .89, SD = .61) and patients (M = 1.19, SD = .51), t(36) = 1.53, p = .13. An analysis of
bias for temporal context (i.e. the preference to identify stimuli as being presented in

Chapter 10
- 232 -
session 1 rather than session 2) also showed a nonsignificant difference between controls
(M = 1.08, SD = .63) and patients (M = .90, SD = .33), t(36) = 1.02, p = .31.
Binding of source and temporal information to event memory
The proportions of contextual features recalled in conjunction with each correctly
recognized intact event were calculated. The measures were calculated for each individual
and included the proportions of object pairs (1) where both source and temporal
information were correctly retrieved (‘who & when‘), (2) where source only was correctly
retrieved (‘who only‘), (3) where temporal information only was correctly retrieved (‘when
only‘), and (4) where neither source nor temporal information was correctly retrieved
(‘neither‘). A 2 (subgroup) x 3 (context: ‘who only‘ vs. ‘when only‘ vs. ‘who & when‘)
ANOVA was performed. Proportions for ‘neither‘ were not included to prevent
collinearity problems arising from using all four proportions, which would sum to one.
There was a significant main effect of context, F(1, 36) = 170.23, p < .001, whereby both
contextual features were retrieved correctly more often than source judgments alone, which
were retrieved correctly more often than temporal judgments alone. However, there was a
nonsignificant main effect of group, F(1, 36) = 2.52, p = .12, and a nonsignificant
interaction, F(1, 36) = 1.75, p = .19. In addition, in a separate one-way ANOVA, there was
no significant group difference on the proportions of ‘neither‘, F(1, 36) = 3.19, p = .08.
In order to assess whether patients with OCD had a context binding deficit, the
proportion of patients showing an impairment in some form of memory for context was
calculated, as assessed by the percentage of patients with OCD who were impaired on
either source or temporal judgments or both. Using a one standard deviation criterion, the
results showed that only one of the 14 patients had a deficit on either of these variables
(.07%). Using the two standard deviations criterion, none of the patients with OCD had a
deficit.
In sum, patients with OCD did not show a context memory impairment, as their
performance on all aspects of the task showed no significant difference from the
performance of healthy controls.
Combined deficits in inhibition and context memory
The percentage of patients with OCD whose performance was impaired on both tasks
of intentional inhibition (as measured by deficits on the HSCT type B error variable or false
alarms on ICIM runs 2-4 or both) and contextual memory (as measured by deficits on

Chapter 10
- 233 -
source or temporal memory or both) was computed. The probability that an individual
would score one standard deviation away from the mean of controls in both cognitive
domains by chance alone is .085. With a one standard deviation criterion, the results
showed that only 1 patient (.07%) showed the combination of deficits. Using a two
standard deviation criterion, none of the patients showed a combined deficit in both
inhibition and context memory.
Discussion
Intentional inhibitory processes
The first goal of the study was to investigate whether OCD was associated with an
impairment in intentional inhibition, as measured by the HSCT and ICIM task. The results
showed that patients with OCD had a deficit on both tasks.
On the HSCT, the results revealed that patients with OCD showed an impairment in
both latency and accuracy compared to controls. Specifically, patients with OCD made
more type B errors and responded more slowly than controls on the Response Inhibition
measure of the HSCT. The increased latency was not related to a general decrease in
response speed since the patients did not show slower latency compared to controls in the
Response Initiation condition. The additional time was, therefore, due to “thinking time”
taken up to inhibit the dominant response and produce a novel word that was not a
straightforward sentence completion (Burgess & Shallice, 1996; Nathaniel-James, Fletcher
& Frith, 1997).
Patients with OCD also showed impaired performance on the inhibitory condition of
the ICIM task. Specifically, patients made significantly more false alarms in runs 2-4
compared to controls, indicating a deficit in suppressing activated memory traces that were
not immediately relevant. This performance cannot be attributed to learning and
recognition difficulties since patients showed normal performance in the first run of the
task. Difficulties with encoding can also be ruled out since the total number of hits across
the four runs was not significantly different between the two groups. In addition, the
results cannot be attributed to an overall bias to say ‘yes’ since there was no significant
difference between the two groups in the number of false alarms in the first run.
Poorer performance on the HSCT and ICIM task was not found to be associated with
a widespread cognitive impairment since patients with OCD did not differ from controls in

Chapter 10
- 234 -
terms of response speed on the Response Initiation condition of the HSCT and actually had
significantly more years of education than controls and higher intellectual functioning as
measured by the NART. BDI-II scores were found to be correlated with the Response
Inhibition measure of the HSCT, but depression scores were not significantly correlated
with any other inhibitory measures so cannot be the reason for poor inhibitory performance.
Performance on the HSCT or ICIM task was not associated either with symptom severity or
other clinical characteristics. An association between inhibitory impairment and symptom
severity is not a consistent finding in the literature. For example, Bannon, Gonsalvez, Croft
and Boyce (2002) showed that OCD severity scores on the Y-BOCS correlated with Stroop
reaction time but not with the number of commission errors on the Go/Nogo task.
In summary, it was found that patients with OCD showed a deficit in intentional
inhibition, as measured by the HSCT and ICIM task. The results support the proposal that
both OCD patients and schizophrenia patients with auditory hallucinations have a deficit in
intentional inhibition as assessed by these tasks. However, the nature of the deficits on the
two tasks was somewhat different for the two disorders, suggesting that the mechanisms of
intentional inhibition may be somewhat different in both patient groups. On the HSCT,
auditory hallucinations were associated with an increased number of type A, but not type B,
errors (Waters et al, 2003). Patients with OCD, by contrast, had a greater number of type B
errors and longer response latencies on the Response Inhibition condition. On the ICIM
task, patients with auditory hallucinations, compared to patients without hallucinations,
made significantly more false alarms on runs requiring active suppression (runs 2-4),
particularly on distracters that had been targets in previous runs (Badcock et al, in press).
By comparison, patients with OCD had a significantly greater number of false alarms on
runs 2-4 compared to healthy controls although the groups did not differ in the number of
errors on distracters that were previous targets. In addition, the pattern of performance of
hallucinating patients across the four runs of the ICIM task indicated that the overall rate of
false alarm errors increased up to the third run and decreased only on the fourth and final
run, after a 30 minute delay had occured. In contrast, the overall rate of false alarm errors
by OCD patients increased only up to the second run, which occurs immediately after the
first run.
The different performance profiles for the two patient groups is difficult to interpret
as there is no clear explanation of what the different errors on the HSCT and ICIM task

Chapter 10
- 235 -
represent. One possibility is that patients with auditory hallucinations are more prone to
making highly prepotent responses relative to OCD patients, as shown by deficits on Type
A errors on the HSCT and on distracters that were previous targets on the ICIM task. A
difficulty with this proposal, however, is that the patients with OCD have substantially
longer response latencies on the Response Suppression condition of the HSCT, which may
also indicate difficulties resisting prepotent responses. Similar problems with conceptual
coherence apply to other potential explanations we have been able to generate for the
different inhibitory profiles for the OCD and AH patient groups.
In sum, these explanations do not satisfactorily explain the difference in patterns of
performance on the HSCT and ICIM task in patients with OCD and patients with auditory
hallucinations, and no clearer picture has emerged as a result of our speculations. In the
future, studies should aim to explore further the processes underlying the different error
types on the HSCT and ICIM task.
In any case, the results support the proposal that both OCD and auditory
hallucinations are characterized by a deficit in intentional inhibition, as measured by the
HSCT and ICIM task. The number of OCD patients with a deficit in intentional inhibition
was calculated. It was found that 72% of all patients with OCD showed an intentional
inhibition deficit on either or both of the two tasks relative to healthy controls. Although
these results convincingly demonstrate the role of intentional inhibition in OCD, not all
patients exhibited the anticipated deficit. The current results perhaps suggest that the
HSCT and ICIM task were not sensitive enough to identify intentional inhibition processes
in OCD patients. Alternatively, levels of intrusive thoughts may vary between patients with
OCD, and a better experimental design would be to examine the association between a
measure of intrusive thoughts and intentional inhibition.
Context memory processes
The second goal of the current study was to examine the performance of patients with
OCD on the Context Memory task. It was found that patients with OCD were not
significantly different from healthy controls in any of the task conditions. Specifically,
OCD patients showed intact recognition accuracy for object pairs, intact source and
temporal context judgments and normal binding abilities, suggesting that contextual
memory was clearly not impaired in patients with OCD. Only one of the patients with

Chapter 10
- 236 -
OCD showed a deficit on either source or temporal context, a result that is not much
different from chance.
The finding of intact source memory contrasts with studies that have shown that OCD
patients have a poor memory for the origin of actions (e.g. Tolin et al, 2002). However,
studies have been inconsistent in outcomes, with many now proposing that the deficit is
primarily due to lack of confidence in memory (e.g. Constans, Foa, Franklin & Mathews,
1995). In support, many recent studies have found impaired knowledge about one's
memory capabilities in OCD patients (Constans, Foa, Franklin & Mathews, 1995; Foa,
Amir, Gershuny, Molnar & Kozak, 1997). The finding of intact temporal memory in the
Context Memory task, however, contrasts with Jurado et al’s (2002) findings. They
investigated temporal ordering of a list of words and found that, compared to a group of
healthy controls, patients with OCD showed normal recognition memory but compromised
ability to sequentially order words. The exact reason for this discrepancy is not clear,
although methodological differences may have accounted for the mixed results. The
processes for ordering a list of words in memory may differ quite substantially from
remembering which of two sessions an event had occurred in, and different levels of
working memory involvement and strategic encoding may have contributed to differences
in task performance.
In any case, the aim of the study was to test for the presence of a precise deficit in
patients with OCD, characterised by a deficit in contextual memory and defined by an
impairment in identifying the source and/or temporal features of events in memory. The
results supported our proposal that patients with OCD do not show compromised context
memory ability, as measured by the Context Memory task. As suggested by Johnson et al
(1993), this pattern of intact processes contributes to an efficient memory system, allowing
the patient to remember the origins of their intrusive thoughts and to distinguish between
different events in episodic memory.
A combination of deficits in inhibition and context memory
Finally, the main aim of this study was to examine whether any of the OCD patients
would show the combination of deficits in both intentional inhibition and context memory,
as presented by schizophrenia patients with auditory hallucinations. It was found that,
using the stringent criterion of scores two standard deviations away from the means of the
control group, none of the OCD patients showed the combination of deficits. When the

Chapter 10
- 237 -
more flexible criterion of one standard deviation away from the means of controls was
applied, only one patient out of 14 was found to have a combined impairment on tasks of
intentional inhibition and context memory. These results provide strong support for the
proposal that OCD is not associated with a combined deficit in intentional inhibition and
context memory.
However, the finding that one OCD patient showed the combination of deficits is
inconsistent with our model of auditory hallucinations, since it predicts that the
combination of deficits is associated with the experience of auditory hallucinations. A
close investigation of this patient’s details revealed that she was the only OCD patient who
reported hypnopompic hallucinations (auditory hallucination-like occurrences experienced
during the transition from sleep to wakefulness). These were reported as occurring
approximately every 6 weeks and consisted of the patient hearing faint voices and
conversations. Since hallucinations occurring as a result of falling asleep or waking up
were not a criterion for exclusion, this patient was included in the study.
These results would appear to imply that the processes underlying hallucination-like
experiences in the realm of non-psychotic states might also rely on similar cognitive
processes to those shown by schizophrenia patients with auditory hallucinations. In
support, similar deficits in reality monitoring (Bentall & Slade, 1985b; Rankin & O’Carroll,
1985) and metacognitive beliefs (e.g. Morrison et al, 2000; in press) have been identified in
patients with a predisposition to hallucinations and schizophrenia patients with auditory
hallucinations. This proposal is also consistent with David’s (2004) recent suggestion that
auditory hallucinations are still the result of a pathological process, even if they are
reported by the ‘normal’ population. Interestingly, some commonalities between processes
involved in hypnopompic and hypnagogic experiences (HHEs) and hallucinations in
psychotic individuals have recently been highlighted. For example, Cheyne, Rueffer and
Newby-Clark (1999) have pointed out that HHEs “begin with an affectively charged sense
of presence leading to interpretive efforts to corroborate that conviction” (p. 332). This
view is consistent with suggestions of biases and beliefs in patients with auditory
hallucinations (e.g. Chadwich & Birchwood, 1994; Morrison, Haddock & Tarrier, 1995).
In addition, HHEs have been linked to REM states, which have been found to involve
interactions between limbic structures such as the amygdala and the anterior cingulate.
Interestingly, the limbic system has also been linked to auditory hallucinations in

Chapter 10
- 238 -
schizophrenia (e.g. Copolov et al, 2003; Lennox, Bert, Park, Jones & Morris, 1999),
consistent with suggestions of commonalities between HHEs and auditory hallucinations of
schizophrenia.
Alternatively, this single OCD case presenting with the combination of deficits may
indicate vulnerability to schizophrenia (increased schizotypy). In support of this
possibility, there is evidence that HHEs are associated with a high rate of schizophrenia.
In addition, it is increasingly believed that OCD can be divided into clinical subtypes, and
in particular a subtype of OCD with schizotypal features has been identified (Harris &
Dinn, 2003; Hwang, Morgan & Losconzcy, 2000), explaining perhaps why the chance of
developing schizophrenia in OCD is significantly higher than in the general population
(Spitznagel & Suhr, 2002). Harris and Dinn (2003) have proposed that this OCD-
schizotypal subtype shows neuropsychological and neural characteristics of both OCD and
schizophrenia disorders. If a context memory deficit is common to patients with
schizophrenia in general (Waters, Maybery, Badcock & Michie, 2004), the combination of
the intentional inhibitory deficit found in OCD, together with the context memory
impairment in schizophrenia, may create the precise dual deficit combination necessary to
promote the emergence of hallucinations. In support, Hermesh et al (2004) have recently
reported that musical hallucinations are a particularly common experience among OCD
patients. However, they further identified that although OCD is a contributor to the
develoment of musical hallucinations, it is not enough on its own. An additional (i.e.
comorbid) mental disorder, such as schizophrenia, that interacts with OCD markedly
increases the likelihood of the occurrence of these hallucinations. This further supports our
proposal that only a combination of deficits may result in a hallucinatory experience.
Further research in other clinical samples is needed to support our proposal that the
combination of deficits in both intentional inhibition and context memory is specifically
associated with auditory hallucinations.
A shortcoming of this study is that the sample of OCD patients was not very large.
However, due to the reluctance of OCD patients to participate in research, it was not
possible to increase the sample size. One consequence of the small sample size is that it
was not possible to carry out analyses within subgroups. For example, differences in
patterns of performance on a Negative Priming task have been found in checkers and
noncheckers subgroups of the OCD population (e.g. Hoenig et al, 2002). Future research

Chapter 10
- 239 -
should assess cognitive inhibition efficiencies in those major groups to examine the range
of inhibitory deficit types present and their role in symptom presentation. Also, the current
OCD sample did not include nonmedicated patients so it was not possible to investigate the
roles of medications on cognitive performance. Although previous studies have not found
that common medications used for OCD have a significant effect on cognitive performance
(Bannon et al, 2002; Purcell et al, 1998), investigations of the effect of medication dosage
and type should be encouraged.
Finally, it should be made clear that the intention of this study was not to demonstrate
that OCD and auditory hallucinations of schizophrenia are one and the same disorder with
the exception of an intact context memory deficit. Although OCD and hallucinations may
share an intentional inhibition deficit, OCD is also associated with a range of other
cognitive deficits, in automatic forms of inhibition and in interference control, as well as
impairments in executive functions and visuospatial memory. This combination of deficits
results in the expression of a clinical disorder that is distinct from that of auditory
hallucinations. In support, OCD presents with very specific themes of obsessions, such as
fear of contamination or need for order or symmetry, and compulsions, confirming that the
two disorders are distinct disorders that merely share a common deficit in intentional
inhibition.

Chapter 10
- 240 -
References
Amieva, H., Phillips, L. H., Della Sala, S., & Henry, J. D. (2004). Inhibitory
functioning in Alzheimer's disease. Brain, 127, 949-964.
Badcock, J. C., Waters, F. A. V., Maybery, M. T., & Michie, P. T. (in press).
Auditory hallucinations: failure to inhibit irrelevant memories. Cognitive Neuropsychiatry.
Bannon, S., Gonsalvez, C. J., Croft, R. J., & Boyce, P. M. (2002). Response
inhibition deficits in obsessive-compulsive disorder. Psychiatry Research, 110, 165-174.
Beck, A. (1990). BAI . San Antonio: The Psychological Corporation.
Beck, A. (1996). BDI-II . San Antonio: The Psychological Corporation.
Breiter, H. C., & Rauch, S. L. (1996). Functional MRI and the study of OCD: from
symptom provocation to cognitive-behavioural probes of cortico-striatal systems and the
amygdala. Neuroimage, 4, S127-S138.
Burgess, P., & Shallice, T. (1996). Response suppression, initiation and strategy use
following frontal lobe lesions. Neuropsychologia, 34(4), 263-273.
Cabeza, R., Mangels, J., Nyberg, L., Habib, R., Houle, S., McIntosh, A. R., &
Tulving, E. (1997). Brain regions differentially involved in remembering what and when: A
PET study. Neuron, 19, 863-870.
Chadwick, P., & Birchwood, M. (1994). The omnipotence of voices - the cognitive
approach to auditory hallucinations. British Journal of Psychiatry, 164, 190-201.
Cheyne, J. A., Rueffer, S. D., & Newby-Clark, I. R. (1999). Hypnagogic and
hypnopompic hallucinations during sleep paralysis: neurological and cultural construction
of the night-mare. Consciousness and Cognition, 8, 319-337.
Cleghorn, J. M., Franco, S., Szechtman, B., Kaplan, R., Szechtman, H., Brown, G.
M., Nahmias, C., & Garnett, E. S. (1992). Toward a brain map of auditory hallucinations.
American Journal of Psychiatry, 149(8), 1062-1069.
Collette, F., Van der Linden, M., Delfiore, G., Degueldre, C., Luxen, A., & Salmon,
E. (2001). The functional anatomy of inhibition processes investigated with the Hayling
Task. NeuroImage, 14, 258-267.
Constans, J. I., Foa, E. B., Franklin, M. E., & Mathews, A. (1995). Memory for actual
and imagined events for OC checkers. Behaviour, Research and Therapy, 33(6), 665-671.
Conway, M. A., & Dewhurst, S. A. (1995). Remembering, Familiarity, and Source
Monitoring. The Quarterly Journal of Experimental Psychology, 48A(1), 125-140.

Chapter 10
- 241 -
Copolov, D. L., Seal, M. L., Maruff, P., Ulusoy, R., Wong, M. T. H., Tochon-
Danguy, H. J., & Egan, G. F. (2003). Cortical activation associated with the experience of
auditory hallucinations and perception of human speech in schizophrenia: a PET correlation
study. Psychiatry Research: Neuroimaging, 122, 139-152.
Danion, J. M., Rizzo, L., & Bruant, A. (1999). Functional mechanisms underlying
impaired recognition memory and conscious awareness in patients with schizophrenia.
Archives of General Psychiatry, 56(7), 639-644.
David, A. S. (2004). The cognitive neuropsychiatry of auditory verbal hallucinations:
an overview. Cognitive Neuropsychiatry, 9(1/2), 107-123.
Denys, D., De Geux, F., Van Megen, H. G. M., & Westenberg, H. G. M. (2000).
Clinical characteristics of obsessive-compulsive disorder: A sample of 300 OCD-
outpatients.
Enright, S., & Beech, A. (1990). Obessional states: anxiety disorders or schizotypes?
An information processing and personality assessment. Psychological Medicine, 20, 621-
627.
Foa, E. B., Amir, N., Gershuny, B., Molnar, C., & Kozak, M. J. (1997). Implict and
Explicit Memory in Obsessive-Compulsive Disorder. Journal of Anxiety Disorders, 11(2),
119-129.
Friedman, N. P., & Miyake, A. (2004). The relations among inhibition and
interference control functions: a latent-variable analysis. Journal of Experimental
Psychology: General, 133(1), 101-135.
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Delgado, P., Heninger,
G. R., & Charney, D. S. (1989a). The Yale-Brown Obsessive Compulsive Scale - Validity.
Archives of General Psychiatry, 46, 1012-1016.
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R. L.,
Hill, C. L., Heninger, G. R., & Charney, D. S. (1989b). The Yale-Brown Obsessive
Compulsive Scale: I. Development, use, and reliability. Archives of General Psychiatry,
46, 1006-1011.
Harnishfeger, K. K. (1995). The development of cognitive inhibition: theories,
definitions and research evidence. In F. N. Dempster & C. J. Brainerd (Eds.), Interference
and inhibition in cognition. Chap 6 (pp. 175-205). San Diego: Academic Press.
Chapter 10
- 242 -
Harris, C. L., & Dinn, W. M. (2003). Subtyping Obsessive-Compulsive Disorder:
Neuropsychological correlates. Behavioural Neurology, 14, 75-87.
Hermesh, H., Konas, S., Shiloh, R., Dar, R., Marom, S., Weizman, A., & Gross-
Isseroff, R. (2004). Musical hallucinations: prevalence in psychotic and nonpsychotic
outpatients. Journal of Clinical Psychiatry, 65, 191-197.
Hoenig, K., Hochrein, A., Muller, D. J., & Wagner, M. (2002). Different negative
priming impairments in schizophrenia and subgroups of obsessive-compulsive disorder.
Psychological Medicine, 32, 459-468.
Huppert, F., & Piercy, M. (1978). The role of trace strength in recency and frequency
judgments by amnesic and control subjects. Quarterly Journal of Experimental Psychology,
30, 347-354.
Hwang, M., Morgan, J., & Losconzcy, M. (2000). Clinical and neuropsychological
profiles of obsessive-compulsive schizophrenia; A pilot study. The Journal of
Neuropsychiatry and Clinical Neurosciences, 12, 91-94.
Johnson, M. K., Hashtroudi, S., & Lindsay, D. S. (1993). Source Monitoring.
Psychological Bulletin, 114(1), 3-28.
Jurado, M. A., Junque, C., Vallejo, J., Salgado, P., & Grafman, J. (2002). Obsessive-
Compulsive Disorder (OCD) patients are impaired in remembering temporal order and in
judging their own performance. Journal of Clinical and Experimental Neuropsychology,
24(3), 261-269.
Lennox, B. R., Bert, S., Park, G., Jones, P. B., & Morris, P. G. (1999). Spatial and
Temporal mapping of neural activity associated with auditory hallucinations. The Lancet,
353(9153), 644.
Maruff, P., Purcell, R., Tyler, P., Pantelis, C., & Currie, J. (1999). Abnormalities of
internally generated saccades in obsessive-compulsive disorder. Psychological Medicine,
29, 1377-1385.
Morrison, A. P., Haddock, G., & Tarrier, N. (1995). Intrusive thoughts and auditory
hallucinations: a cognitive approach. Behavioral and Cognitive Psychotherapy, 23, 265-
280.
Morrison, A.P., Wells, A., & Nothard, S. (2000). Cognitive factors in predisposition
to auditory and visual hallucinations. British Journal of Clinical Psychology, 39, 67-78.

Chapter 10
- 243 -
Morrison, A.P., Wells, A., & Nothard, S. (in press). Cognitive and emotional
predictors of predisposition to hallucinations in non-patients. British Journal of Clinical
Psychology.
Nathaniel-James, D. A., Fletcher, P., & Frith, C. (1997). The functional anatomy of
verbal initation and suppression using the Hayling Test. Neuropsychologia, 35(4), 559-566.
Nelson, H. E. (1982). The National Adult Reading Test (NART): Test Manual.
Windsor, Berks: NFER-Nelson.
Nigg, J. T. (2000). On inhibition/disinhibition in developmental psychopathology:
Views from cognitive and personality psychology and a working inhibition taxonomy.
Psychological Bulletin, 126(2), 220-246.
Nyberg, L., McIntosh, A. R., Cabeza, R., Habib, R., Houle, S., & Tulving, E. (1996).
General and specific brain regions involved in encoding and retrieval of events: What,
where and when. Proceedings of the National Academy of Science, 93, 11280-11285.
Okasha, A., Rafaat, M., Mahallawy, N., El Nahas, G., Seif El Dawla, A., Sayed, M.,
& El Kholi, S. (2000). Cognitive dysfunction in Obsessive-Compulsive Disorder. Acta
Psychiatrica Scandinavica, 101, 281-285.
Purcell, R., Maruff, P., Kyrios, M., & Pantelis, C. (1998). Cognitive deficits in
obsessive-compulsive disorder on tests of frontal-striatal function. Biological Psychiatry,
43, 348-357.
Schnider, A., & Ptak, R. (1999). Spontaneous confabulators fail to suppress currently
irrelevant memory traces. Nature Neuroscience, 2(7), 677-681.
Schnider, A., Treyer, V., & Buck, A. (2000). Selection of currently relevant
memories by the human posterior medial orbital cortex. The Journal of Neuroscience,
20(15), 5880-5884.
Sheehan, D. V., Lecrubier, Y., Harnett Sheehan, K., Janavs, J., Weiller, E., Keskiner,
A., Schinka, J., Knapp, E., Sheehan, M. F., & Dunbar, G. C. (1997). The validity of the
Mini International Neuropsychiatric Interview (MINI) according to the SCID-P and its
reliability. European Psychiatry, 12, 232-241.
Silbersweig, D. A., Stern, E., C, F., & et al (1995). A functional neuroanatomy of
hallucinations in schizophrenia. Nature, 378, 176-179.

Chapter 10
- 244 -
Spitznagel, M. B., & Suhr, J. A. (2002). Executive function deficits associated with
symptoms of schizotypy and obsessive-compulsive disorder. Psychiatry Research, 110,
151-163.
Steketee, G., Frost, R., & Bogart, K. (1996). The Yale-Brown Obsessive Compulsive
Scale: interview versus self report. Behaviour Research and Therapy, 34(8), 675-684.
Tolin, D. F., Abramowitz, J. S., Przeworski, A., & Foa, E. B. (2002). Thought
suppression in obsessive-compulsive disorder. Behaviour Research and Therapy, 40,
125501274.
Waters, F. A. V., Badcock, J. C., Maybery, M. T., & Michie, P. T. (2003). Inhibition
in schizophrenia: association with auditory hallucinations. Schizophrenia Research, 62,
275-280.
Waters, F. A. V., Badcock, J. C., Michie, P. T., & Maybery, M. T. (2004). Auditory
hallucinations in schizophrenia: intrusive thoughts and forgotten memories. Submitted for
publication.
Waters, F.A.V., Badcock, J.C., Maybery, M.T., & Michie, P.T. (2004) Context
Memory and auditory hallucinations. Unpublished manuscript, University of Western
Australia.
Waters, F. A. V., Maybery, M. T., Badcock, J. C., & Michie, P. T. (2004). Context
memory and binding in schizophrenia. Schizophrenia Research, 68(2-3), 119-125.

- 245 -
GENERAL DISCUSSION
- 247 -
Chapter 11 General discussion
The aim of this thesis was to provide a new perspective on the nature of the cognitive
deficits underlying auditory hallucinations. Firstly, we investigated the similitudes in
characteristics between hallucinatory-like experiences in healthy individuals and auditory
hallucinations in schizophrenia in order to identify factors that may be important to the
hallucinatory experience in general. Secondly, the processes of intentional inhibition and
context memory were examined individually in schizophrenia patients with auditory
hallucinations. Thirdly, the proposal that these two cognitive deficits, combined, must be
present for auditory hallucinations to occur was tested. Finally, the specificity of this
combination of deficits to patients with auditory hallucinations was investigated by
examining the integrity of these processes in another clinical group who also experiences
intrusive thoughts, namely patients with Obsessive-Compulsive Disorder (OCD). In this
chapter, the main findings relevant to auditory hallucinations are reviewed in turn, together
with a discussion of the implications of these results at the end of each section. Answering
one question often raises previously unconsidered questions, consequently some possible
directions for future research are also outlined in each section.
Hallucinatory predisposition in healthy individuals
Summary of results of Chapter 2
As a preliminary study to our investigations of auditory hallucinations in
schizophrenia, a factor analysis of a measure of hallucinatory predisposition, the Launay-
Slade Hallucination Scale-Revised (Bentall & Slade, 1985a), was carried out on a large
sample of undergraduate students (N = 562). One of the findings from this study was that
one of the factors underpinning predisposition to auditory hallucinations in the normal
population is characterised as the experience of intrusive mental events. In addition,
healthy individuals vulnerable to hallucinations identified experiences that are referred to
an external agency. These two characteristics are defining features of auditory
hallucinations in schizophrenia. Since mental processes are thought to occur on a

Chapter 11
- 248 -
continuum, an overlap in characteristics between hallucinatory-like experiences in normal
individuals and auditory hallucinations in schizophrenia suggests that these factors may be
important components to the hallucinatory experience in general.
Since little is known about the cognitive processes that give rise to these
characteristics in schizophrenic auditory hallucinations, the subsequent studies investigated
the mechanisms responsible for (a) the intrusiveness and (b) the attribution of mental events
to an external agent, in auditory hallucinations of schizophrenia.
Intentional inhibition and auditory hallucinations The cognitive process of inhibition is essential for suppressing irrelevant thoughts,
and a failure to maintain control through inhibitory efficiency is thought to result in
information that intrudes into ongoing thinking. In order to explain the intrusive and
unintended characteristic of auditory hallucinations in schizophrenia, we proposed that
individuals with auditory hallucinations suffer from a failure in inhibition, and in particular
in intentional inhibition (Harnishfeger, 1995) since auditory hallucinations are consciously
experienced mental events.
Summary of results of Chapter 3
The aim of Chapter 3 was to investigate the proposal that auditory hallucinations in
schizophrenia are linked to a deficit in intentional inhibition. Patients with schizophrenia
(N = 42) and healthy controls (N = 24) completed two tasks selected to assess the
intentional suppression of cognitive events, the Hayling Sentence Completion Test (HSCT)
(Burgess & Shallice, 1996) and the Inhibition of Currently Irrelevant Memories (ICIM)
task (Schnider & Ptak, 1999), which require the inhibition of currently active mental
associations and irrelevant memories respectively. Firstly, the patients performed
significantly worse on the measures of inhibition relative to controls. Secondly, it was
found that an increase in auditory hallucinations severity (as measured by the PANSS)
among the schizophrenia patients was associated with an increasing deficit on the two tasks
of inhibition, suggesting that difficulties suppressing unwanted mental associations and
irrelevant memory representations are associated with the experience of auditory
hallucination in schizophrenia.

Chapter 11
- 249 -
Summary of results of Chapter 4
In order to address the question of whether this deficit is a general feature of
schizophrenia or whether it is specifically associated with the presence of auditory
hallucinations, Chapter 4 contrasted the performance of patients who reported auditory
hallucinations in the last four weeks (N = 23) with patients who reported no auditory
hallucinations during the same period (N = 20) on the ICIM task. Whereas patients with
hallucinations showed a deficit inhibiting recently activated memory traces, the
performance of patients with no hallucinations was not significantly different from that of
healthy controls, indicating that the inhibitory impairment was specific to patients with
auditory hallucinations and not to all patients with schizophrenia.
Summary of results of Chapter 5
One of the aims of Chapter 5 was to revisit the integrity of intentional inhibition
processes in auditory hallucinations with a task-switching paradigm. The Affective
Shifting Task (Murphy et al, 1999) was specifically chosen because it assesses different
types of inhibitory processes, namely task-shifting abilities (assessing intentional inhibition
processes), interference control and valence-dependent inhibitory control. Patients
currently experiencing hallucinations were selected on the basis of having experienced
auditory hallucinations on at least half of the days during the preceding four weeks, as
assessed by self-reports and case note reviews (N = 19). Other schizophrenia patients who
did not fit this criterion were assigned to the non-hallucinating group (N = 24). Severity of
auditory hallucinations, measured with the PANSS, was also used to assess whether task
performance was associated with severity, rather than the presence, of auditory
hallucinations.
Firstly, the analyses revealed that neither the presence nor the severity of auditory
hallucinations was associated with an impairment in task-shifting on the Affective Shifting
Task. These results contrast with earlier findings of impaired performance on other tasks of
intentional inhibition such as the HSCT and ICIM task (see Chapters 3 and 4). We
speculated on the reason for this discrepancy in findings. On the Affective Shifting Task,
the response options are clearly defined and limited. In contrast, on the HSCT and ICIM
task, the response options are either open-ended (HSCT) or unknown (ICIM task).
Consequently, it is possible that the Affective Shifting Task is an easier task of intentional
inhibition and may require less inhibitory demands than tasks such as the HSCT and ICIM

Chapter 11
- 250 -
task. In support for this proposal, Amieva, Phillips, Della Sala and Henri (2004) have
recently proposed that tasks of intentional inhibition differ in terms of inhibitory demand,
depending on various factors such as different task requirements. In order to test the
suggestion that the Affective Shifting Task may have been easier than other tasks because
of a lower number of response options, an interesting study would manipulate the difficulty
of the same task-switching paradigm by increasing the number of possible options available
to participants. Future studies should develop better tasks where the inhibitory demands are
manipulated more systematically. In any case, the current suggestion leaves open the
possibility that, in some situations, patients with auditory hallucinations are able to exert
some control over mental events. This proposal may perhaps explain why patients do not
experience auditory hallucinations continuously.
Secondly, no significant association was found between severity of hallucinations and
overall latency on the Affective Shifting Task, suggesting that this aspect of interference
control is not particularly impaired in auditory hallucinations. This replicates previous
findings from Brebion, Smith, Gorman, Malaspina and Amador (1998) on the Stroop
Color-Word Test. However, the results showed that the severity of auditory hallucinations
was associated with an overall increase in false alarms. False alarms represent a failure to
inhibit inappropriate responding to previously relevant but currently inappropriate stimuli.
Similar difficulties in suppressing recently activated but irrelevant memory representations
were identified in Chapters 3 and 4. The present finding of an association between false
alarms on the Affective Shifting Task and severity of auditory hallucinations supports the
proposal that auditory hallucinations are associated with impaired control of unwanted and
irrelevant cognition, and is consistent with the suggestion that auditory hallucinations are
associated with a deficit in intentional inhibition.
Summary of results of Chapter 8
The analyses from Chapters 3 and 4 revealed that patients with auditory
hallucinations have an impairment in the intentional inhibition of active mental events and
irrelevant memory traces, as assessed using the HSCT and ICIM task. In order to
investigate whether this deficit is an essential component of auditory hallucinations, the
percentage of patients impaired on either, or both, of the two inhibitory tasks was calculated
with reference to whether scores were in excess of one standard deviation from control
group means. The results presented in Chapter 8 showed that all of the patients with

Chapter 11
- 251 -
auditory hallucinations (N = 19) were found to have a deficit in intentional inhibition,
supporting the role of intentional inhibition in the hallucinatory process. In comparison,
less than half of the patients without auditory hallucinations (N = 24) could be classified as
impaired. This latter group included 4 patients who had never experienced auditory
hallucinations in the past. Amongst those patients, only one showed such a deficit, a result
that is not much different from chance. These results strongly support the proposal that
auditory hallucinations are associated with a deficit in intentional inhibition.
General comments regarding the role of intentional inhibition processes in auditory
hallucinations
A number of studies have suggested that factors such as depression, poor processing
speed and low verbal intelligence (e.g. Brebion, Smith, Amador, Malaspina & Gorman,
1997; Brebion, Gorman, Malaspina, Sharif & Amador, 2001; Seal, Crowe & Cheung,
1997) may account for some cognitive deficits associated with auditory hallucinations.
Chapters 3, 4 and 8 investigated whether poor performance on tasks of inhibition may
actually reflect other types of deficits. It was found that auditory hallucinations were not
associated with widespread impairment in current intelligence quotient, speed of
responding, memory span or general discrimination ability. In addition, group comparisons
for a range of demographic factors such as age and years of education, and clinical
indicators including duration of illness, depression, anxiety and number of hospital
admissions, also suggested that patients with hallucinations were not generally more unwell
compared to patients without current hallucinations. Patients with hallucinations had more
positive symptoms than patients without, but there were no significant differences in
negative and general (somatic) symptoms. Patients with hallucinations also tended to have
higher chlorpromazine equivalents, although this variable did not correlate with
performance on the inhibition tasks. These findings argue against a significant role of these
variables in the inhibitory deficits associated with auditory hallucinations.
The issue of the specificity of the intentional inhibition deficit was also investigated.
Performance on the HSCT and ICIM task was not found to be associated with positive
(once hallucinations severity ratings were subtracted from the set of positive symptoms
ratings), general or negative symptoms as measured by the PANSS, confirming the finding
that the failure in intentional inhibition is associated with the presence of auditory
Chapter 11
- 252 -
hallucinations specifically and is not a general feature of patients with schizophrenia (see
Chapter 4).
As reviewed in Chapter 8, the proposal that auditory hallucinations are associated
with a deficit in intentional inhibition is consistent with imaging investigations of the brain
regions thought to be involved in intentional suppression, as measured by the HSCT and
ICIM task. In particular, the prefrontal areas, the anterior cingulate gyrus, the basal ganglia
structures and the thalamus, which have been found to be activated during HSCT and/or
ICIM task performance (Collette et al, 2001, Schnider, Treyer & Buck, 2000), are regions
which have also been found to be associated with the hallucinatory experience (Copolov et
al, 2003; Lennox, Bert, Park, Jones & Morris, 1999; McGuire, Shah & Murray, 1993;
McGuire et al, 1995; Silbersweig et al, 1995; Woodruff & Murray, 1994).
In summary, the current set of studies has identified the presence of an inhibitory
impairment in auditory hallucinations. In particular, the domain of intentional inhibition
was found to be particular affected. The results of our investigations also indicated that
performance on tasks of intentional inhibition may depend on the task requirement of
different paradigms and identified the need for a more systematic manipulation of task
difficulties in studies using tasks of inhibition.
Context memory and auditory hallucinations Another defining characteristic of auditory hallucinations is that the experience is
attributed to an external agent. In order to explain this feature of the hallucinatory
experience, Nayani and David (1996a) proposed that schizophrenia patients with auditory
hallucinations have a deficit in context memory. They suggested that the contextual
features of mental events are missing or incomplete, resulting in confusion about the origins
of these events. The aim of Chapters 6 and 7 was to investigate the proposal that a context
memory deficit is present in patients with schizophrenia, and those with auditory
hallucinations more specifically.
Summary of results of Chapter 6
Chapter 6 examined whether patients with schizophrenia, as a group, showed a
context memory deficit. The performance of a group of patients with schizophrenia (N =
43) was contrasted with the performance of a group of healthy controls (N = 24) on a
Memory for Context task, in which memory for events and memory for the source and
temporal information about those events was assessed. The results showed that patients

Chapter 11
- 253 -
with schizophrenia have a deficit in context memory, as shown by difficulties recalling both
the source and the temporal context of events in memory. Furthermore, while controls
tended to retrieve all the different contextual features of events (source and temporal
characteristics), patients tended to have a more fractionated recollection of the events,
retrieving only individual features in isolation or none at all, pointing to an inability to bind
together all the original components of an experience. The findings were strengthened by
the comparison of the patients' performance with that of a subgroup of controls who also
performed poorly on content memory. Although this group of controls had low recognition
accuracy for intact object pairs, source and temporal context judgments and binding
abilities were still intact, suggesting that the deficit in binding was specific to patients with
schizophrenia and did not extend to all participants with poor content memory.
Summary of results of Chapter 7
Chapter 7 investigated the specificity of context memory and binding deficits to
auditory hallucinations. The study involved a reanalysis of the results presented in Chapter
6. Patients were divided into those who reported auditory hallucinations on at least half of
the days during the preceding four weeks (N = 19) and those who did not (N = 23). The
aims of this study were to examine whether patients with hallucinations would show a
deficit in remembering individual contextual cues, and particularly the source of events in
memory and the temporal context of those events, and examine whether context binding
generally, as defined by a deficit in source and/or temporal context, is particularly impaired
in patients with current auditory hallucinations compared to patients without.
Firstly, patients with current hallucinations were found to be particularly impaired in
recalling the source of memories, compared to patients without hallucinations. However,
patients with auditory hallucinations were not found to be disproportionally impaired in the
recall of the temporal context of memories, suggesting that the deficit is present in
schizophrenia patients, irrespective of their hallucinating status. Secondly, the results
showed that nearly all patients with auditory hallucinations (89.5%) showed a deficit in
identifying the origins of memories, as shown by deficits in either source and/or temporal
memory relative to healthy controls, and that significantly more patients with hallucinations
showed this deficit compared to patients without. These results provide strong support for
Nayani and David’s (1996a) proposal that contextual memory is impaired in patients with
auditory hallucinations.

Chapter 11
- 254 -
The current findings also suggested that a deficit in both source and temporal context
is not necessary for hallucinations to occur. Rather, it appears that missing contextual cues
in source or/and temporal memory are associated with the hallucinatory experience; in
other words, sometimes the temporal context but not the source might be lost and other
times the reverse might happen, or both forms of context might be lost. Johnson,
Hashtroudi and Linsay (1993) have proposed that a loss of qualitative information in
memory would make it difficult to correctly identify mental events and may result in
confusion regarding the origins of these events. It is possible, therefore, that, in patients
with auditory hallucinations, this deficit accessing correctly any number of contextual cues
results in an incomplete representation of events in memories, leading to a failure to
recognize the hallucinated material.
The finding that auditory hallucinations are associated with correct context judgment
at least some of the time is consistent with Nayani and David’s (1996b) survey that showed
that a significant proportion of patients with auditory hallucinations are very clear about the
identity of some of their voices. In Chapter 7, we speculated about the processes that
contribute towards making source judgments in patients with auditory hallucinations.
Recent findings suggest that episodic memory retains traces of both voice characteristics
and words (Goldinger, 1996), and that the human voice carries important information such
as the affect, gender and other physical characteristics of a talker (e.g. Belin, Fecteau &
Bedard, 2004). Consequently, we argued that some of the auditory sensory features of the
remembered events may be retained, which are then used by the patients to make
attributions regarding the source of this remembered information, although recognition
depends on the amount and type of information available. The proposal of preserved
auditory sensory features in auditory hallucinations is consistent with the observation that
the acoustic qualities of an original event are retained in functional auditory hallucinations
(e.g. Hunter & Woodruff, 2004). In sum, our results indicate that context information, as
assessed by the Context Memory task which is largely based on visuo/motor context cues,
may be impaired in patients with auditory hallucinations, while other evidence suggests that
auditory sensory features in memory may be retained. An explanation for the dissociation
between impaired visuo/motor information and intact auditory sensory cues was provided
by the proposal of a distinction between intrinsic and extrinsic context information, which
has recently been found to be dissociable (Troyer & Craik, 2000). Accordingly, as

Chapter 11
- 255 -
suggested in Chapter 7, patients with auditory hallucinations may have a deficit in extrinsic
context, but intact intrinsic context information. This proposal requires further
investigation but the current suggestion proposes that variation in the details of events from
memory contributes to variability of the hallucinatory experience.
Overall, the results showed that significantly more patients with auditory
hallucinations have a deficit in some form of memory for context compared to patients
without hallucinations. However, it was also found that nearly two-thirds of patients
without current auditory hallucinations had context binding difficulties, suggesting that the
context memory impairment is not specific to patients with auditory hallucinations. Some
may argue that if a context memory deficit is not specific to patients with auditory
hallucinations, why are nonhallucinating patients not reporting auditory hallucinations? As
argued in Chapter 7, our proposal is that a deficit in context memory, singly, is essential,
but not sufficient, for auditory hallucinations to occur. Only when combined with (at least
one) other deficits would the symptom of auditory hallucinations become manifest. In sum,
it is our proposal that the finding of nonspecificity of the context memory impairment to
auditory hallucinations is not a setback in the search for cognitive deficits associated with
auditory hallucinations. There is a growing awareness that a single deficit is unlikely to
result in such a complex event and that a combination of deficits might be needed to
explain auditory hallucinations in schizophrenia (Nayani & David, 1996a). In a
forthcoming section, we explore the proposal that a combination of deficits in context
memory and intentional inhibition is critical for hallucinations to occur.
General comments regarding context memory processes in auditory hallucinations
The proposal that auditory hallucinations are associated with a deficit in context
memory is consistent with imaging investigations of the brain regions thought to be
involved in context memory. Retrieval of context memory and binding has been associated
with activation of the frontal lobes, medial temporal lobes and the amygdala (e.g. Davachi,
Mitchell & Wagner, 2003; Mayes et al, 2001), and neural imaging of auditory
hallucinations also points to the activation of the frontal cortex, temporal cortex and
hippocampal/parahippocampal cortex (e.g. McGuire et al, 1995; Woodruff et al, 1997).
The results from Chapter 7 revealed that patients with current auditory hallucinations
were particularly impaired in recalling the source of events in memory, compared to
patients without. This replicates and extends a commonly reported finding that patients

Chapter 11
- 256 -
with hallucinations have difficulties identifying the source of an action or a thought
compared to patients without hallucinations (e.g. Blackmore, Smith, Steel, Johnstone &
Frith, 2000). Such a deficit actually forms the basis of reality- and self-monitoring theories
of auditory hallucinations (e.g. Bentall & Slade, 1985b; Frith, 1996). However, our
proposal differs from these theories in three important ways. Firstly, they propose that this
impairment is also associated with poor decision-making in identifying the origins of
memories (e.g. Rankin & O’Carroll, 1995), or with a bias towards misattributing self-
produced material to another source (e.g. Johns & McGuire, 1999). The results from our
investigations are not compatible with this proposal, as patients with hallucinations did not
show an unusual decision criterion in event or source recognition. Secondly, our proposal
suggests that the extent of the deficit is more wide-ranging than simply a deficit in
identifying the source of mental events. Instead, we suggest that patients with auditory
hallucinations have a general deficit in identifying the context of mental events, involving
at least source memory, as well as other contextual cues such as temporal memory.
Finally, instead of suggesting a single-deficit account of auditory hallucinations, our model
proposes that context memory is only one of many (at least two) cognitive processes that
must be impaired in patients with auditory hallucinations, and therefore a context memory
deficit may not be necessarily specific to patients with auditory hallucinations. This
proposal allows for the finding that some nonhallucinating patients have been shown to
have this deficit without experiencing hallucinations.
The results from Chapter 7 also indicated that, although significantly more patients
with auditory hallucinations showed a deficit in some form of memory for context
compared to patients without, a context memory deficit was not specific to patients with
auditory hallucinations. This suggests that some of the current findings and analyses may
also be relevant to other (particularly positive) symptoms of schizophrenia. Context
binding difficulties, for instance, could provide a complimentary explanation of some
aspects of delusion formation. A failure to identify the origins of mental events may
contribute to some of the characteristic features of delusions, such as an inability to
generate and evaluate alternative explanations of a false conviction (Blackwood, Howard,
Bentall & Murray, 2001; Davies, Coltheart, Langdon & Breen, 2001; Langdon & Coltheart,
2000). In addition, the distinction between intrinsic and extrinsic cues in context memory
may be relevant to contemporary research on the sense of agency in symptoms such as

Chapter 11
- 257 -
delusions of control and thought insertion (i.e. Frith, 2004; Gallagher, 2004). In sum, the
role of context memory deficits in other positive symptoms deserves investigating.
Issues of affect
Summary of results of Chapter 5
Auditory hallucinations have often been found to co-occur with negative affect such
as depression. One of the aims of Chapter 5 was to examine further the role of affect in
auditory hallucinations. Forty-three patients with schizophrenia took part in this study, 19
of whom reported auditory hallucinations on at least half of the days during the preceding
four weeks and 23 who did not.
Firstly, the results revealed that approximately one third of patients with auditory
hallucinations had elevated depression and anxiety scores and that these were not
specifically related to the presence, or severity, of auditory hallucinations. This indicates
that negative affect is associated with auditory hallucinations, but not specifically so.
Secondly, the results showed that, consistent with previous findings (e.g. Hustig &
Hafner, 1990), negative voice content was commonly reported by hallucinating patients.
Depression levels (but not anxiety levels) were significantly correlated with the frequency
of negative voice content, although most patients who reported hearing negative voices still
rated themselves as being minimally depressed. These results were interpreted as
suggesting that depression is linked to, but is not a necessary outcome or a precondition of
negative voice content of auditory hallucinations.
Thirdly, exploratory investigations regarding beliefs about voices (i.e. malevolence,
benevolence and omnipotence) and reaction to these beliefs (i.e. resistance or engagement)
were carried out using Chadwick, Lees and Birchwood’s (2000) Belief About Voices
Questionnaire-Revised (BAVQ-R). The results were mostly consistent with Chadwick et
al’s findings. The results showed that (a) beliefs in malevolence and/or omnipotence were
associated with resistance activity and elevated levels of depression, but were not
necessarily linked to depression, and (b) belief in malevolence or omnipotence was not
related to negative voice content, although belief in benevolence was found to decrease
with increasing reports of negative voice content. The results therefore indicated that
beliefs about voices are important components to understanding affect and content of
auditory hallucinations, although they are not always effective predictors of negative
affective states or negative voice content

Chapter 11
- 258 -
Finally, the role of attentional bias for negative material in patients with auditory
hallucinations was investigated with the Affective Shifting Task. In addition to measures
of interference control and task-shifting ability (see Chapter 5), this task provides a
measure of valence-dependent inhibitory control. This allowed the investigation of the
presence of faulty inhibitory mechanisms of selective attention for negative information in
auditory hallucinations. Cognitive models of depression and anxiety have emphasized the
role of biases in attention for negative information in the environment (see MacLeod &
Rutherford, 1998, for a review). Auditory hallucinations have often been found to co-occur
with negative affect (e.g. Close & Garety, 1998) and negative affective voice content is a
prominent feature of auditory hallucinations in schizophrenia. Consequently, this measure
examined whether patients with auditory hallucinations, and those with negative voice
contents especially, showed a particular bias for negative targets. The results revealed that
an attentional bias for negative material was not associated with the presence of auditory
hallucinations, an outcome which is consistent with recent findings by van ‘t Wout,
Aleman, Kessels, Laroi and Kahn (2004) in individuals with a predisposition to
hallucinations. However, higher depression scores in patients with auditory hallucinations
were found to be associated with an increasing number of errors on negative words when
positive words were the targets, suggesting that depression in patients with auditory
hallucinations is associated with a bias towards negative material. Although these results
are preliminary, the results suggest that, when present, depression in patients with
hallucinations is linked to the intrusion of unwanted negative material from memory.
Could depression, therefore, be linked to negative voice contents in hallucinations? A
critical analysis of the data did not support this proposal, as negative voice contents were
still reported in patients who rate themselves as being minimally depressed and negative
voice content was not found to be associated with a bias for negative targets on the
Affective Shifting Task. As a result, we considered that a more psycho-psychological
explanation may be needed to explain negative voice content. For instance, Thomas,
Bracken and Leudar (2004) have proposed that, in order to explain the ephemeral properties
of the hallucinatory experience, the content of voices may only be explained in the context
of the individual’s social, historical and cultural background. These authors suggested that
researchers should attempt to understand the “reflexive” relationship between the person
and the person’s experience of voices, and that only investigations at this level can explain

Chapter 11
- 259 -
the voices’ content. Given the complexity of the multifactorial issues linking affect and
hallucinations, this proposal certain deserves further investigation.
In summary, it was found that a negative mood is commonly found in patients with
auditory hallucinations, although it is not directly related to the presence or severity of
auditory hallucinations. Depression was found to be related to voice content and beliefs in
malevolence and/or omnipotence. However, the results also showed that negative voice
contents and beliefs about voices were not direct determinants of, or did not directly result
from, elevated depression/anxiety reported by hallucinating patients. Finally, an attentional
bias for negative material was found to be associated with depression, although a critical
analysis of the results suggested that this bias for negative material could not fully account
for negative voice content.
General comments regarding issues of affect and auditory hallucinations
The current investigations were not able to fully determine the factors that contribute
significantly to negative affect in patients with auditory hallucinations. Marengo, Harrow,
Herbener and Sands (2000) proposed that patients with schizophrenia have different levels
of vulnerability to depression, explaining why only some patients are depressed. The data
shown in the current investigations could certainly fit a vulnerability view of depression. It
may be speculated that depression in those vulnerable individuals promotes the occurrence
of negative voice contents and beliefs in malevolence or omnipotence. One difficulty with
this proposal is how to explain the presence of positive voice contents in depressed
individuals. It appears more likely that, in the patients with a predisposition to depression,
the presence of negative hallucinatory content and/or beliefs in malevolence or
omnipotence may lead to the depressive symptoms. Further research is needed to
investigate this proposal.
An interesting development in this study was the finding of a strong association
between belief in malevolence and/or omnipotence and resistance activities, such as trying
to stop the voice or prevent it talking. As noted in Chapter 5, attempts at thought control
have been implicated as an etiological and maintaining factor in OCD. In support, BAVQ-
R statements assessing resistance activities (e.g. I try and take my mind off it; I try and stop
it) are activities commonly reported by patients with OCD to try to escape intrusive
thoughts. It is believed that deliberate thought control efforts lead to the contradictory
effect of making those thoughts more accessible and more persistent (e.g. Purdon & Clark,

Chapter 11
- 260 -
2001). We therefore speculated that resistance activities towards unwanted thoughts may
play a key role in the maintenance process of auditory hallucinations. In order to explain
the presence of positive/neutral voice contents, we further speculated that the content of the
hallucinatory material (negative, positive or neutral) is activated initially by random
generation of mental events occurring as a result of the deficit in inhibition described
earlier. Subsequently, negative voice hallucinations re-occur as a result of attempts at
thought control and positive voice contents do not re-occur because they are not actively
suppressed. Alternatively, or perhaps additionally, the engagement activities associated
with belief in benevolence, at least in some cases, promotes the reoccurrence of future
hallucinatory episodes containing positively valenced material. Clearly, these speculations
require further investigations, although the proposal of the role of resistance activities in the
maintenance process of auditory hallucinations is particularly intriguing.
A combination of deficits in intentional inhibition and context memory
A new cognitive model of auditory hallucinations was outlined in Chapter 8. To
begin with, our model proposes that auditory hallucinations consist of the activation of
auditory mental events that include memories and other currently active mental
associations. In addition, our model proposes that the following two cognitive deficits, at
least, must be present to explain auditory hallucinations: (a) a fundamental deficit in
intentional inhibition, which leads to auditory mental representations intruding into
consciousness in a manner that is beyond the control of the sufferer; and (b) a deficit in
binding contextual cues, resulting in an inability to form a complete representation of the
origins of mental events. As a result of these combined deficits, our model proposes that
mental events are experienced as involuntary and intrusive and are not recognized because
the contextual cues that would allow them to be identified correctly are missing or
incomplete.
In order to test this proposal, the percentage of patients impaired on tasks of both
intentional inhibition (HSCT and/or ICIM task) and context memory (source and/or
temporal memory), as defined by scores one standard deviation away from the means of the
control group, was computed. It was found that nearly 90% of patients currently
experiencing hallucinations (N = 19; auditory hallucinations on at least half of the days
during the preceding four weeks) showed the combination of deficits, compared to only a

Chapter 11
- 261 -
third of patients without hallucinations (N = 23; patients who did not fit the above
criterion). These results were interpreted as supporting our proposition that the two
deficits are significantly associated with the hallucinatory process.
It is our claim that this model is able to explain many of the clinical features of
auditory hallucinations. For instance, as noted by Nayani and David (1996a), the proposal
of auditory hallucinations as consisting of auditory reproductions from memories is able to
explain why patients report hearing speech as well as nonverbal sounds, why voices are
often recognized as belonging to people that the hearer knows and why sufferers report
hearing different types of grammatical speech, such as second or third person
hallucinations. The proposal of auditory hallucinations as memories can also explain why
voices often refer to the patient’s personal details. Auditory hallucinations as consisting of
current mental associations accounts for first person hallucinations and running
commentaries. The suggestion of a disordered context memory system can explain why the
origins of these mental events are often not recognized. It may also be speculated that the
failure to identify the origins of recalled memories may lead to misinterpretations about the
message and the intent of the experience, accounting for variations in beliefs about the
voices, negative affect and delusional personification of the experience. Finally, the
perceived intrusiveness so commonly reported by hallucinating patients can also be
explained by a failure in the control of intentional inhibition. Therefore, a range of
phenomenological features are now explained by our new model.
This model should not be taken as an independent approach to understanding auditory
hallucinations but should be seen as complementary to other explanations of hallucinations.
As discussed above, the current proposal of a context memory deficit in patients with
auditory hallucinations is actually not dissimilar to reality- and self-monitoring theories of
auditory hallucinations (e.g. Frith, 1996). In addition, it is unlikely that cognitive
impairments are the sole factors responsible for auditory hallucinations. Rather, socio-
psychological factors have been shown to have considerable explanatory power (e.g.
Chadwick & Birchwood, 1995; Morrison, 2001; Thomas et al, 2004) and may well
contribute to an explanation of issues of affect and of the material comprising hallucinated
speech, which are not fully explained by our model. We fully believe that insights from a
socio-psychological approach can be integrated with the current level of explanation to

Chapter 11
- 262 -
understand the very personalized experience of sufferers and to provide a more complete
understanding of the maintenance process of auditory hallucinations.
Although it was found that nearly all patients currently experiencing hallucinations
showed the combination of deficits, the results of our investigations also revealed that a
minority of past hallucinators showed the combination of deficits. This suggests that the
two deficits may not be sufficient to explain the presence of auditory hallucinations, and
that additional cognitive process(es) might be important for the expression of this symptom.
We can only speculate, at this stage, what these additional processes are. The role of a third
process, for instance, may be to 'activate' the representations that would lead to auditory
hallucinations.
Finally, it is now increasingly believed that the ability to control distracting memories
is accomplished by inhibitory mechanisms (Anderson & Green, 2001; Conway & Fthenaki,
2003; Levy & Anderson, 2002). According to Conway and Fthenaki (2003), the role of
inhibition is to promote forgetting of redundant information. Whereas a healthy inhibitory
system ‘shapes’ detailed memories by inhibiting redundant details which are not relevant
within the context of the situation, a deficient inhibitory system is not successful at sieving
out irrelevant material and makes too many items equally available for recall, hence
producing a flooding of irrelevant memories. Future studies should investigate the
relationship between inhibition and context memory processes in order to examine whether
the failure in inhibition is partly responsible for the formation of intrusive memories in
patients with auditory hallucinations.
Intentional inhibition and context memory in Obsessive-Compulsive Disorder (OCD)
According to this new model of auditory hallucinations in schizophrenia, a
combination of deficits in intentional inhibition and contextual memory is essential to the
experience of auditory hallucinations. Consequently, patients who do not experience
auditory hallucinations may demonstrate a deficit in either process but none should present
with this particular combination of deficits. As a test of this proposal, Chapter 10
examined the intentional inhibition and context memory abilities of patients with OCD.
Both auditory hallucinations and OCD are characterised by recurrent and persistent
thoughts which sufferers are not able to control, although, unlike patients with auditory
hallucinations, OCD patients do not mistake the origins of these thoughts. It was therefore

Chapter 11
- 263 -
hypothesized that patients with OCD would show poor inhibitory functioning on the HSCT
and ICIM task, but intact memory for context on the Context Memory task. In addition, it
was predicted that none of the patients with OCD would show deficits in both cognitive
domains simultaneously. Fourteen participants with OCD took part in this study, and their
performance was compared with that of a group of healthy controls (N = 24).
Summary of results and general comments regarding intentional inhibition processes in
OCD
Firstly, the results showed that OCD was associated with an impairment in intentional
inhibition, as measured by the HSCT and ICIM task. The results, therefore, supported the
proposal that both OCD patients and schizophrenia patients with auditory hallucinations
have a deficit in intentional inhibition. However, the nature of the deficit was slightly
different for the two disorders. On the HSCT, patients with hallucinations showed an
increased number of Type A errors whereas patients with OCD had a greater number of
Type B errors and longer response latencies. On the ICIM task, patients with auditory
hallucinations made significantly more false alarms on runs requiring active suppression
(runs 2-4), and particularly on distracters that had been targets in previous runs, compared
to patients without hallucinations. Patients with OCD also had a significantly greater
number of false alarms on runs 2-4 relative to healthy controls but the groups did not differ
in the number of errors on distracters that were previous targets.
The difference between the performance profiles of each patient group is difficult to
interpret as there is no clear explanation of what the different errors on the HSCT and ICIM
task represent. We can only conclude that it indicates that the mechanisms of intentional
inhibition are somewhat different in both patient groups. Future studies should aim to
explore further the processes underlying the different error types on the HSCT and ICIM
task.
In any case, impaired performance on these tasks indicates that patients with OCD
have a deficit in intentional inhibition processes. We may speculate on the commonalities
in functional anatomy in both disorders which has contributed to impaired performance in
intentional inhibition, as measured by the HSCT and ICIM task. Effective performance on
the HSCT has been linked with the activation of frontal areas and of the anterior cingulate
gyrus (Burgess & Shallice, 1996; Collette et al, 2001; Nathaniel-James, Fletcher & Frith,
1997), regions also associated with both OCD and auditory hallucinations (e.g. Breiter &

Chapter 11
- 264 -
Rauch, 1996; Cleghorn et al, 1992; Silbersweig et al, 1995). Performance on runs 2-4 of the
ICIM has been found to activate the posterior orbitofrontal cortex (OFC) and left caudate
nucleus, left substantial nigra, ventral tegmental area and right medial thalamus (Schnider,
Treyer & Buck, 2000). OCD and auditory hallucinations have also been linked to deficits
to the OFC, and abnormalities in basal ganglia structures and the thalamus (e.g. Breiter &
Rauch, 1996; Copolov et al, 2003; Silbersweig et al, 1995), supporting the finding that both
disorders show an overlap in intentional inhibition processes.
The study findings may be able to complement our understanding of the role of
intentional inhibitory processes generally. OCD has been associated with deficits in
inhibition across a range of inhibitory domains, although, until now, it has not been clear
which of these domains contribute to the intrusive and repetitive nature of OCD. The
finding of a commonality in intentional inhibition processes in patients with OCD and
auditory hallucinations, who both report intrusive and unwanted thoughts, suggests that
intentional inhibition may be responsible for the intrusive and persistent thoughts. One
difficulty with this proposal is that only approximately 70% of patients with OCD showed a
deficit on the HSCT and/or ICIM task. This suggests that an intentional inhibition deficit,
as measured by these tasks, is not essential for OCD to occur. However, levels of intrusive
thoughts may vary between patients with OCD and a better experimental design would be
to examine the association between a measure of intrusive thoughts and task performance.
Finally, the finding of impaired intentional inhibition in OCD also has implications
for our understanding of the processes underlying the inhibitory deficit generally. Patients
with OCD had significantly higher premorbid intelligence scores compared to both patients
with hallucinations and healthy controls, yet they still showed a deficit in inhibition. This
suggests that superior intelligence quotient does not necessarily result in better inhibitory
control (Krikorian, Zimmerman & Fleck, 2004) and, therefore, that it is not a protective
factor against an inhibitory impairment.
Summary of results and general comments regarding context memory and OCD
Secondly, the results showed that patients with OCD were not significantly different
from controls on any of the conditions of the Context Memory task, showing intact
recognition accuracy for object pairs, intact source and temporal context judgments and
normal binding abilities. This supports the proposal that contextual memory is not
impaired in patients with OCD.

Chapter 11
- 265 -
The combined results of the investigations of context memory in auditory
hallucinations and OCD confirm our understanding of the role of context memory
processes in everyday cognitive activities. Nayani and David (1996a) proposed that a
deficit in context memory would result in an incomplete representation of mental events
and consequently a failure to identify their origins. In support of this proposal, patients with
auditory hallucinations, who incorrectly attribute self-generated mental events to another
agent, showed a deficit in context memory, whereas OCD patients, who do not confuse the
origins of their intrusive thoughts, showed intact context memory abilities. These findings
are consistent with the proposal that intact qualitative information contributes to an efficient
memory system, allowing the patient to remember the origins of their intrusive thoughts
and to distinguish between different events in episodic memory (Johnson et al, 1993).
Summary of results and general comments regarding combined deficits in intentional
inhibition and context memory and OCD
If a combined impairment in intentional inhibition and context memory is crucial for
auditory hallucinations to occur, then it follows that nonhallucinating individuals should
not present with this particular combination of deficits. In support of this prediction, the
results of the study on OCD showed that only one patient out of 14 was found to have a
combined impairment on tasks of intentional inhibition and context memory, confirming
the proposal that OCD is not associated with a deficit in both cognitive domains.
However, the finding that one OCD patient showed the combination of deficits is
inconsistent with our model of auditory hallucinations which specifies that the combination
of deficits is associated with the experience of auditory hallucinations specifically. A close
investigation of this patient’s details revealed that she was the only OCD patient who
reported frequent hypnopompic hallucinations. This suggests that the processes underlying
hallucinations in the realm of “non-psychotic” experiences might be similar to those
underlying auditory hallucinations in schizophrenia, a proposal which is consistent with
findings by Bentall and Slade (1985b), Morrison et al (2000, in press) and Rankin and
O’Carroll, 1985). Future studies should examine the integrity of intentional inhibition and
context memory processes in individuals vulnerable to hallucinations.
Alternatively, this single OCD case presenting with this specific combination of
deficits may indicate vulnerability to schizophrenia. As noted in Chapter 10, a subtype of
OCD with schizotypal features has recently been identified which shows

Chapter 11
- 266 -
neuropsychological and neural characteristics of both OCD and schizophrenia (Harris &
Dinn, 2003; Hwang, Morgan & Losconzcy, 2000). We hypothesised that, since a context
memory deficit has been found to be common to patients with schizophrenia (Chapters 6 &
7), the added inhibitory deficit presented by OCD may create the precise dual deficit
combination necessary to promote the emergence of hallucinations. In support, we
reviewed that Hermesh et al (2004) recently identified that musical hallucinations are
particularly common in OCD. However, these authors also identified that an additional
comorbid mental disorder, such as schizophrenia, is necessary to increase the likelihood of
the occurrence of these hallucinations. The implication of this finding is that any individual
who presents with (a) a deficit in intentional inhibition similar to the one experienced in
hallucinations and (b) schizotypal features may be at risk of developing hallucinations,
since the combination of deficits in inhibition and context memory should, according to our
model, provide the right mixture of factors conducive to generating hallucinations.
Final comments The aim of this thesis was to contribute towards a better understanding of the
cognitive processes underlying auditory hallucinations of schizophrenia. Instead of the
conventional approach of examining a single deficit, the possibility that a combination of
deficits might be responsible for auditory hallucinations was investigated. The results of
our investigations showed that a combination of deficits in intentional inhibition and
context memory is critical, although perhaps not sufficient, for auditory hallucinations to
occur. The power in our model comes from its ability to explain a broad range of
phenomena that previous models could not account for. Our model accounts for the
perceived intrusiveness and unintendedness of the hallucinatory experience, it explains the
form and content of auditory hallucinations, it clarifies why the origins of the mental
contents are not recognized and it contributes to our understanding about external
attribution. Finally, it describes why voices are familiar with the patients’ intimate details
and it provides an explanation for the patients’ conviction about the veridicality of the
experience. However, a critical analysis of the results suggested that additional processes,
such as “activational” processes, might be necessary to fully account for auditory
hallucinations in schizophrenia. It would be very revealing for future research to
investigate the processes responsible for the selection and activation of the hallucinated
material. An additional strength of the research was the comparison of the pattern of

Chapter 11
- 267 -
performance of patients with auditory hallucinations with that of patients with OCD, who
also experience uncontrollable and intrusive thoughts. The results suggested that
impairments in both intentional inhibition and context memory are not found in any clinical
group who also experiences unwanted and intrusive thoughts.
In general, future studies should focus on extending the knowledge developed in this
thesis about the role of intentional inhibition and context memory processes in auditory
hallucinations. Currently, there is a paucity of studies that have examined the presence of
an inhibitory deficit in auditory hallucinations and the exact nature of the context memory
deficit is still unclear. Future studies should strive to test our proposal that only intentional
inhibitory processes are impaired in auditory hallucinations, and to examine whether the
context memory deficits extend to, for instance, binding in working memory.
The results of this thesis have practical implications beyond the immediate impact of
a theoretical account. Similarities in clinical features between auditory hallucinations and
OCD suggest that research into the treatment of OCD might become useful for
understanding the best approach to treating auditory hallucinations. For example, research
into OCD treatment has shown that strategies employing distraction techniques are often
the most effective way to reduce the frequency of unwanted thought activities.
Psychological therapy for hallucinating patients may therefore be most effective if it were
to employ techniques designed to encourage patients to participate in distracting activities,
rather than encourage attempts to exert some control over the experience, which may, in
fact, lead to an increase in the salience of the intrusion (Gibbs, 1996). It may be useful for
clinicians to provide specific distraction tasks for patients to implement when they find
themselves engaging in active thought suppression of hallucinations.
However, research into OCD has also informed us that distracting activities and other
coping strategies in general are much less effective in the presence of depressed mood
(Gibbs, 1996). We may, therefore, speculate that differences in levels of depressed mood
may be responsible for variations in the effectiveness of hallucinating patient’s coping
strategies and treatments (Shergill et al, 1998). Consequently, before recommending or
assigning distracting tasks to hallucinating patients, clinicians should assess for, and treat
first, the presence of a depressed mood. In addition, psychological theories of OCD (e.g.
Salkovskis, 1989) have informed us that a change in the meaning assigned to the intrusive
thought is required for a reduction in symptoms. When the thought no longer bears a

Chapter 11
- 268 -
special meaning, the individual does not feel compelled to engage in thought control
strategies. One specific application to hallucinations is that if resistance activity is the
product of belief about malevolence and omnipotence (Chadwick & Birchwood, 1995,
2000a) a useful strategy may consist in changing the idiosyncratic beliefs that the patient
has about their voices. This approach has been instigated with some success in patients
with auditory hallucinations (e.g. Birchwood & Chadwick, 1997; Chadwick & Birchwood,
1994, 2000b). There is also evidence that cognitive behavioural therapies targeting the
interpretations of hallucinations have become a useful treatment strategy (Dickerson, 2000;
Shergill et al, 1998; Rector & Beck, 2001).
Finally, theories of OCD have highlighted the role of factors that make it more likely
for individuals to develop OCD, such as misinterpretation of the intrusive thoughts,
dysfunctional beliefs and negative affect. There is an increasing interest in the role of such
factors in auditory hallucinations (i.e. Morrison, 2001; Morrison, Haddock & Tarrier,
1995). Cognitive and neuropathological similarities between OCD and auditory
hallucinations certainly suggest that such investigations should be actively pursued. Other
advances in theoretical understanding of OC symptomatology should also contribute to our
understanding of auditory hallucinations.
It was made explicit early in the thesis that the investigations would concentrate on
elucidating the processes responsible for auditory hallucinations in schizophrenia. To
determine the specificity of the findings to this group, future studies should explore the
integrity of inhibition and context memory mechanisms underlying visual, olfactory and
gustatory hallucinations, in patients with schizophrenia and in individuals in other clinical
groups.
Finally, there is an urgent need for prospective, longitudinal research into the
developmental process of auditory hallucinations. In addition to furthering our
understanding of the fluctuating processes responsible for auditory hallucinations, such
investigations may also provide information about protective factors which prevent
individuals from relapsing and promote well being.
In conclusion, auditory hallucinations of schizophrenia are one of the most difficult
symptoms to study in a manner acceptable to clinicians and researchers alike. However,
research into the causes and nature of hallucinations remain an exciting area of scientific
inquiry. Understanding the processes underlying auditory hallucinations remain an

Chapter 11
- 269 -
important priority, not only because of the health care and other economic costs attributable
to schizophrenia, but also because of the suffering of those affected with the illness and
their families.

Chapter 11
- 270 -
References Aleman, A., Bocker, K. B. E., Hijman, R., de Haan, E. H. F., & Kahn, R. S. (2003).
Cognitive basis of hallucinations in schizophrenia: role of top-down information
processing. Schizophrenia Research, 1926, 1-11.
Amieva, H., Phillips, L. H., Della Sala, S., & Henry, J. D. (2004). Inhibitory functioning in
Alzheimer's disease. Brain, 127, 949-964.
Anderson, M. C., & Green, C. (2001). Suppressing unwanted memories by executive
control. Nature, 410(6826), 366-369.
Birchwood, M., & Chadwick, P. (1997). The omnipotence of voices: testing the validity of
a cognitive model. Psychological Medicine, 27, 1345-1353.
Beck, A. T., & Rector, N. A. (2003). A cognitive model of hallucinations. Cognitive
Therapy and Research, 27(1), 19-52.
Belin, P., Fecteau, S., & Bedard, C. (2004). Thinking the voice: neural correlates of voice
perception. Trends in Cognitive Sciences, 8(3), 129-1355.
Bentall, R. P., & Slade, P. D. (1985a). Reliability of a scale measuring disposition towards
hallucination: a brief report. Personality and Individual Differences, 6(4), 527-529.
Bentall, R. P., & Slade, P. D. (1985b). Reality testing and auditory hallucinations: A signal
detection analysis. British Journal of Clinical Psychology, 24, 159-169.
Blakemore, S., Smith, J., Steel, R., Johnstone, E., & Frith, C. (2000). The perception of
self-produced sensory stimuli in patients with auditory hallucinations and passivity
experiences: evidence for a breakdown in self-monitoring. Psychological Medicine,
30, 1131-1139.
Blackwood, N. J., Howard, R. J., Bentall, R. P., & Murray, R. M. (2001). Cognitive
neuropsychiatric models of persecutory delusions. American Journal of Psychiatry,
158(4), 527-539.
Brebion, G., Gorman, J. M., Malaspina, D., Sharif, Z., & Amador, X. (2001). Clinical and
cognitive factors associated with verbal memory task performance in patients with
schizophrenia. American Journal of Psychiatry, 158, 758-764.
Brebion, G., Smith, M. J., Amador, X., Malaspina, D., & Gorman, J. M. (1997). Clinical
correlates of memory in schizophrenia: differential links between depression, positive
and negative symptoms and two types of memory impairment. American Journal of
Psychiatry, 154(11).

Chapter 11
- 271 -
Brebion, G., Smith, M., Gorman, J., Malaspina, D., & Amador, X. (1998). Resistance to
interference and positive symptomatology in schizophrenia. Cognitive
Neuropsychiatry, 3, 179-190.
Breiter, H. C., & Rauch, S. L. (1996). Functional MRI and the study of OCD: from
symptom provocation to cognitive-behavioural probes of cortico-striatal systems and
the amygdala. Neuroimage, 4, S127-S138.
Burgess, P., & Shallice, T. (1996). Response suppression, initiation and strategy use
following frontal lobe lesions. Neuropsychologia, 34(4), 263-273.
Chadwick, P., & Birchwood, M. (1994). The omnipotence of voices - the cognitive
approach to auditory hallucinations. British Journal of Psychiatry, 164, 190-201.
Chadwick, P., & Birchwood, M. (1995). The Omnipotence of Voices II: The Beliefs About
Voices Questionnaire (BAVQ). British Journal of Psychiatry, 166, 773-776.
Chadwick, P., Lees, S., & Birchwood, M. (2000a). The revised Beliefs About Voices
Questionnaire. British Journal of Psychiatry, Sept, 229-232.
Chadwick, P., Sambrooke, S., Rasch, S., & Davies, E. (2000b). Challenging the
omnipotence of voices: group cognitive behaviour therapy for voices. Behaviour
Research and Therapy, 38, 993-1003.
Cleghorn, J. M., Franco, S., Szechtman, B., Kaplan, R., Szechtman, H., Brown, G. M.,
Nahmias, C., & Garnett, E. S. (1992). Toward a brain map of auditory hallucinations.
American Journal of Psychiatry, 149(8), 1062-1069.
Close, H., & Garety, P. (1998). Cognitive assessment of voices: further develoments in
understanding the emotional impact of voices. British Journal of Clinical Psychology,
37, 173-188.
Collette, F., Van der Linden, M., Delfiore, G., Degueldre, C., Luxen, A., & Salmon, E.
(2001). The functional anatomy of inhibition processes investigated with the Hayling
Task. NeuroImage, 14, 258-267.
Conway, M. A., & Fthenaki, A. (2003). Disruption of inhibitory control of memory
following lesions to the frontal and temporal lobes. Cortex, 39(4-5), 667-686.
Copolov, D. L., Seal, M. L., Maruff, P., Ulusoy, R., Wong, M. T. H., Tochon-Danguy, H.
J., & Egan, G. F. (2003). Cortical activation associated with the experience of
auditory hallucinations and perception of human speech in schizophrenia: a PET
correlation study. Psychiatry Research: Neuroimaging, 122, 139-152.

Chapter 11
- 272 -
Davachi, L., Mitchell, J. P., & Wagner, A. D. (2003). Multiple routes to memory: distinct
medial temporal lobe processes build item and source memories. Proceedings of the
National Academy of Sciences of the United States of America, 100(4), 2157-2162.
Davies, M., Coltheart, M., Langdon, R., & Breen, N. (2001). Monothematic delusions:
Towards a two-factor account. In C. Hoerl (Ed.), On understanding and explaining
schizophrenia: Philosophy, Psychiatry and Psychology .
Dickerson, F. B. (2000). Cognitive behavioural psychotherapy for schizophrenia: a review
of recent empirical studies. Schizophrenia Research, 43, 71-90.
Frith, C. (1996). The role of the prefrontal cortex in self-consciousness: the case of auditory
hallucinations. Philosophical Transactions of the Royal Society of London: B, 351,
1505-1512.
Frith, C. (2004). Comments on Shaun Gallagher: "Neurocognitive models of schizophrenia:
a neurophenomenological critique". Psychopathology, 37, 20-22.
Gallagher, S. (2004). Neurocognitive models of schizophrenia: a neurophenomenological
critique. Psychopathology, 37, 8-19.
Gibbs, N. A. (1996). Non-clinical populations in research on obsessive-compulsive
disorders: a critical review. Clinical Psychology Review, 16, 729-773.
Goldinger, S.D., 1996. Words and voices: episodic traces in spoken word identification and
recognition memory. Journal of Experimental Psychology: Learning, Memory and
Cognition. 22(5):1166-83.
Harnishfeger, K. K. (1995). The development of cognitive inhibition: theories, definitions
and research evidence. In F. N. Dempster & C. J. Brainerd (Eds.), Interference and
inhibition in cognition. Chap 6 (pp. 175-205). San Diego: Academic Press.
Harris, C. L., & Dinn, W. M. (2003). Subtyping Obsessive-Compulsive Disorder:
Neuropsychological correlates. Behavioural Neurology, 14, 75-87.
Hermesh, H., Konas, S., Shiloh, R., Dar, R., Marom, S., Weizman, A., & Gross-Isseroff, R.
(2004). Musical hallucinations: prevalence in psychotic and nonpsychotic outpatients.
Journal of Clinical Psychiatry, 65, 191-197.
Hunter, M. D., & Woodruff, W. R. (2004). Characteristics of functional auditory
hallucinations. The American Journal of Psychiatry, 161(5), 923.

Chapter 11
- 273 -
Hustig, H. H., & Hafner, R. J. (1990). Persistent auditory hallucinations and their
relationship to delusions and mood. The Journal of Nervous and Mental Disease,
178(4), 264-267.
Hwang, M., Morgan, J., & Losconzcy, M. (2000). Clinical and neuropsychological profiles
of obsessive-compulsive schizophrenia; A pilot study. The Journal of
Neuropsychiatry and Clinical Neurosciences, 12, 91-94.
Johns, L. C., & McGuire, P. K. (1999). Verbal self-monitoring and auditory hallucinations
in schizophrenia. The Lancet, 353(9151), 469-470.
Johnson, M. K., Hashtroudi, S., & Lindsay, D. S. (1993). Source Monitoring. Psychological
Bulletin, 114(1), 3-28.
Krikorian, R., Zimmerman, M. E., & Fleck, D. E. (2004). Inhibitory control in Obsessive-
Compulsive Disorder. Brain and Cognition, 54, 257-259.
Langdon, R., & Coltheart, M. (2000). The cognitive neuropsychology of delusions. Mind &
Language, 15(1), 184-218.
Lennox, B. R., Bert, S., Park, G., Jones, P. B., & Morris, P. G. (1999). Spatial and
Temporal mapping of neural activity associated with auditory hallucinations. The
Lancet, 353(9153), 644.
Levy, B. J., & Anderson, M. C. (2002). Inhibitory processes and the control of memory
retrieval. Trends in Cognitive Sciences, 6(7), 299-305.
MacLeod, C., & Rutherford, E. (1998). Automatic and strategic cognitive biases in anxiety
and depression. In K. Kirsner & C. Speelman (Eds.), Implicit and explicit mental
processes (pp. 468pp). Mahwah, NJ, USA: Lawrence Erlbaum Associates, Inc.
Marengo, J., Harrow, M., Herbener, E. S., & Sands, J. (2000). A prospective longitudinal
10-year study of schizophrenia's three major factors and depression. Psychiatry
Research, 97(1).
Mayes, A., Isaac, C., Holdstock, J., Hunkin, N., Montaldi, D., Downes, J., MacDonald, C.,
Cezayirli, E., & Roberts, J. (2001). Memory for single items, word pairs and temporal
order of different kinds in a patient with selective hippocampal lesion. Cognitive
Neuropsychology, 18(2), 97-123.
McGuire, P. K., Silbersweig, D. A., Wright, I., Murray, R. M., David, A. S., Frackowiak,
R. S. J., & Frith, C. D. (1995). Abnormal monitoring of inner speech: a physiological
basis for auditory hallucinations. The Lancet, 346(8975), 596-600.

Chapter 11
- 274 -
McGuire, P., Shah, G., & Murray, R. M. (1993). Increased blood flow in Broca's area
during auditory hallucinations in schizophrenia. The Lancet, 342, 703-706.
Morrison, A. P., Haddock, G., & Tarrier, N. (1995). Intrusive thoughts and auditory
hallucinations: a cognitive approach. Behavioural and Cognitive Psychotherapy, 23,
265-280.
Morrison, A. P. (2001). The interpretation of intrusions in psychosis: an integrative
cognitive approach to hallucinations and delusions. Behavioural and Cognitive
Psychotherapy, 29, 257-276.
Morrison, A., Wells, A., & Nothard, S. (2000). Cognitive factors in predisposition to
auditory and visual hallucinations. British Journal of Clinical Psychology, 39, 67-78.
Morrison, A., Wells, A., & Nothard, S. (in press). Cognitive and emotional predictors of
predisposition to hallucinations in non-patients. British Journal of Clinical
Psychology.
Murphy, F. C., Sahakian, B. J., Rubinsztein, J. S., Michael, A., Rogers, R. D., Robins, T.
W., & Paykel, E. S. (1999). Emotional bias and inhibitory control processes in mania
and depression. Psychological Medicine, 29, 1307-1321.
Nathaniel-James, D. A., Fletcher, P., & Frith, C. (1997). The functional anatomy of verbal
initation and suppression using the Hayling Test. Neuropsychologia, 35(4), 559-566.
Nayani, T., & David, A. (1996a). The neuropsychology and neurophenomenology of
auditory hallucinations. In C. Pantelis, H. E. Nelson, & T. R. E. Barnes (Eds.),
Schizophrenia: A Neuropsychological Perspective. Chap. 17 . New York: John Wiley
& Sons Ltd.
Nayani, T. H., & David, A. S. (1996b). The auditory hallucination: a phenomenological
survey. Psychological Medicine, 26, 177-189.
Purdon, C., & Clark, D. (2001). Suppression of obsession-like thoughts in nonclinical
individuals: impact on thought frequency, appraisal and mood state. Behaviour
Research and Therapy, 39, 1163-1181.
Rankin, P. M., & O'Carroll, P. J. (1995). Reality discrimination, reality monitoring and
disposition towards hallucination. British Journal of Clinical Psychology, 34, 517-
528.
Rector, N. A., & Beck, A. T. (2001). Cognitive Behavioural Therapy for schizophrenia: An
empirical review. The Journal of Nervous and Mental Disease, 189(5), 278-287.
Chapter 11
- 275 -
Salkovskis, P. M. (1989). Cognitive-behavioural factors and the persistence of intrusive
thoughts in obsessional problems. Behavioural Research and Therapy, 27(6), 677-
682.
Schnider, A., & Ptak, R. (1999). Spontaneous confabulators fail to suppress currently
irrelevant memory traces. Nature Neuroscience, 2(7), 677-681.
Schnider, A., Treyer, V., & Buck, A. (2000). Selection of currently relevant memories by
the human posterior medial orbital cortex. The Journal of Neuroscience, 20(15),
5880-5884.
Seal, M. L., Crowe, S. F., & Cheung, P. (1997). Deficits in source monitoring in subjects
with auditory hallucinations may be due to differences in verbal intelligence and
verbal memory. Cognitive Neuropsychiatry, 2(4), 273-290.
Shergill, S. S., Murray, R. M., & McGuire, P. K. (1998). Auditory hallucinations: a review
of psychological treatments. Schizophrenia Research, 32, 137-150.
Silbersweig, D. A., Stern, E., C, F., & al, e. (1995). A functional neuroanatomy of
hallucinations in schizophrenia. Nature, 378, 176-179.
Stevens, A. A. (2004). Dissociating the cortical basis of memory for voices, words and
tones. Cognitive Brain Research, 18, 162-171.
Thomas, P., Bracken, P., & Leudar, I. (2004). Hearing voices: a phenomenological-
hermeneutic approach. Cognitive Neuropsychiatry, 9(1/2), 13-23.
Troyer, A., & Craik, F. (2000). The effect of divided attention on memory for items and
their context. Canadian Journal of Experimental Psychology, 54(3), 161-170.
van 't Woot, M., Aleman, A., Kessels, R., Laroi, F., & Kahn, R. S. (2004). Emotional
processing in a non-clinical psychosis-prone sample. Schizophrenia Research, 68,
271-281.
Woodruff, P. W. R., & Murray, R. M. (1994). The aetiology of brain abnormalities in
schizophrenia. In R. Ancill (Ed.), Schizophrenia: Exploring the Spectrum of
Psychosis . New York: John Wiley & Sons Ltd.
Woodruff, P., Wright, I., Bullmore, E., Brammer, M., Howard, R. J., Williams, S.,
Shapleske, J., Rossell, S., David, A. S., McGuire, P. K., & Murray, R. (1997).
Auditory hallucinations and t he temporal cortical response to speech in
schizophrenia: A functional magnetic resonance imaging study. American Journal of
Psychiatry.

Appendix A
- 277 -
Appendix A
An analysis of the main clinical features of auditory hallucinations in schizophrenia
Introduction It has been estimated that approximately 74% of those with a diagnosis of
schizophrenia will experience auditory hallucinations during the course of their illness
(Sartorius, Shapiro & Jablensky, 1974). Auditory hallucinations are complex mental
events often described as comprising a mixture of different phenomenological features,
which combine to produce a highly individualized experience. The phenomenological
features of auditory hallucinations have been comprehensively investigated by a number of
authors (e.g. Nayani & David, 1996; Oulis, Mavreas, Mamounas & Stephanis, 1995),
although these studies surveyed a range of psychotic patients, some of which did not have a
diagnosis of schizophrenia. Given the singular importance of auditory hallucinations in the
diagnosis of schizophrenia, there are surprisingly few detailed surveys of the main
phenomenological features of auditory hallucinations in this patient group alone. We
conducted a phenomenological investigation of auditory hallucinations selecting only
individuals with a primary diagnosis of schizophrenia.
Method Forty-three patients with a DSM-IV diagnosis of schizophrenia were recruited from a
psychiatric hospital. Four patients, on the basis of clinical interviews, questionnaire
responses and case histories, indicated that they had never experienced auditory
hallucinations and another four refused to fill in the questionnaire. Information concerning
the 35 remaining patients’ demographic and clinical data is presented in Table 1. All
patients were receiving typical, atypical or a combination of neuroleptics. Exclusionary
criteria included a history of head injury and neurological illness. Participants were asked
to complete a questionnaire comprising selected items from the Psychotic Symptom Rating
Scales (PSYRAT; Haddock, McCarron, Tarrier & Faragher, 1999) and the Mental Health

Appendix A
- 278 -
Research Institute Unusual Perceptions Schedule (MUPS; Carter, Mackinnon, Howard,
Zeegers & Copolov, 1995) addressing issues of interest.
Approval for this study was granted by the Human Research Ethics Committees of
the University of Western Australia and of Graylands Hospital, Perth, Australia, and signed
informed consent was obtained from all participants.
Table 1
Demographic and clinical characteristics (mean, SD) of patients with Schizophrenia
Questionnaire patients
(n = 35)
Age (years) 35.80 (8.28)
Education (years) 11.05 (1.89)
Sex (M/F) 29 / 6
Quick Test 94.60 (5.41)
Digit Span forward 7.00 (1.69)
Length of illness* (yrs) 13.14 (8.39)
Number of admissions 9.22 (8.29)
Level of positive symptoms (PANSS) 19.80 (5.32)
Level of negative symptoms (PANSS) 12.40 (3.27)
Level of general symptoms (PANSS) 28.82 (5.99)
Chlorpromazine equivalent 970.28 (457.95)
* calculated as time since first admission,
Results
The results of the 35 completed questionnaires on items addressing the characteristics
of auditory hallucinations are presented in Table 2.

Appendix A
- 279 -
Table 2
Frequencies of response on questionnaire items (n = 35)
Frequency %
Do you ever hear sounds other than voices that you suspect others can't hear? (hums, clicks, animal sounds, etc) No 42.9 % Yes 57.1 % In what 'person' does the main voice speak to you? 'I' only 0 % 'you' only 2.9 % 'he/she' only 5.7 % 'your name' only 0 % Other things only 11.4 % Mixture of above 77.1 % Not sure 2.9 % Do the voices say unpleasant things or negative things? Never unpleasant 14.3 % Occasionally unpleasant 37.1 % Minority unpleasant 11.4 % Majority unpleasant 17.1 % Always unpleasant 20.0 % Do you know the identity of the voices? No 37.1 % Yes 37.1 % Sometimes 25.7 % Are the voices similar to voices of people who have spoken to you in the past? No 37.1 % Yes 42.9 % Unsure 20.0 % Do you believe the voices could be replays of memories of previous conversations you have had or heard?
No 37.1 % Yes 45.7 % Unsure 17.1 % Are the memory replays identical or similar to conversations you have had or heard? Identical 5.7 % Similar 37.1 % Unsure 42.9 % Different 14.3 %

Appendix A
- 280 -
When you hear voices, how long do they last?
Few seconds 37.1 % Several minutes 28.6 % At least an hour 8.6 % Hours at a time 22.9 % Other 2.9 % How loud are they? Quieter than own 31.4 % Same as own 62.9 % Louder than own 5.7 % Extremely loud 0 % When you hear voices, where do they sound like they are coming from? Inside head 22.9 % Outside head 28.6 % Inside + outside 48.6 % Are your voices distressing? Not at all 17.1 % Occasionally 37.1 % Minority of voices distressing 11.4 % Majority of voices distressing 8.6 % Voices always distressing 22.9 % Not sure 2.9 % How distressing are the voices?
Not at all 17.1 % Slightly 31.4 % Moderate degree 17.1 % Very, but could be worse 17.1 % Extremely 11.4 % Not sure 5 % How much disruption do the voices cause you? Not at all 17.1 % Minimal 31.4 % Moderate 40.0 % Severe 11.4 % When you hear voices, is the mood of the voice like your mood at the time? No 42.9 % Yes 40.0 % Unsure 17.1 %

Appendix A
- 281 -
Do the voices tell you what to do?
Never 11.4 % Rarely 25.7 % Sometimes 48.6 % Often 14.3 % Are you able to resist doing what they tell you to?
Never 0 % Rarely 8.6 % Sometimes 20.0 % Often 62.9 %
Table 2 shows that nearly 60% of the sample admitted to hearing non-verbal
hallucinations, consistent with the findings from Nayani and David’s (1996) survey.
Verbal hallucinations were found not to be restricted to any one type of grammatical speech
but rather included a mixture of grammatical types. Similar to Linn’s (1977) finding that
voices are rarely expressed in the first person, none of the patients in the current sample
reported first person hallucinations. Most patients reported that their voices said negative
things and only a minority reported that their voices were never unpleasant.
Approximately 60% of patients reported knowing the identity of some of their voices, a
percentage similar to that obtained by Nayani and David. Close to half of all patients
believed that the voices that they experienced were familiar and similar to voices of people
who had spoken to them in the past. Forty-six percent thought it possible that the voices
could be memory reproductions of conversation they have had or heard in the past and, of
those, half felt that these memory reproductions were identical or at least similar to past
conversations.
With respect to the form of auditory hallucinations, the results suggested that the
majority of patients heard voices for up to several minutes at a time, although
approximately a third experienced auditory hallucinations for more than one hour at a time.
The voices were predominantly experienced as being of the same loudness as the patient’s
own voice or quieter, confirming the results obtained by Nayani and David. A quarter of
the sample perceived their voices to be coming from inside the head and another quarter
outside the head, the results being approximately similar to those found by Copolov et al
(in press).

Appendix A
- 282 -
Concerning the intrusive and affective nature of hallucinations, most patients (82.9%)
admitted that at least some of their voices were distressing. When asked to rate how
distressing their voices were, 48.5% stated them to be slightly to moderately distressing and
28.5% reported them to be very to extremely distressing. This percentage of patients
experiencing distress is higher than that reported by Nayani and David but is consistent
with Honig et al’s (1998) findings. Half of the patient sample reported that their
hallucinated voices caused them moderate to severe disruption. Forty percent of patients
explained that the mood of their hallucinated voices was similar to their own mood at the
time they were experiencing the hallucinations. A large majority of patients reported that
their voices had at one point or another told them what to do, although these patients stated
that they were generally able to resist following those commands.
Discussion
Overall, the results of this survey were similar to previous findings (e.g. Nayani &
David, 1996) confirming that the experiences of psychotic patients provides an accurate
indication of the main features of auditory hallucinations in schizophrenia specifically. The
results also indicate that our sample of patients is not atypical. This review of the main
phenomenological features of auditory hallucinations reveals the striking complexity of the
hallucinatory experience and indicates the broad range of features that potentially
contribute to a highly individualized experience.

Appendix A
- 283 -
References Carter, D. M., Mackinnon, A., Howard, S., Zeegers, T., & Copolov, D. L. (1995). The
development and reliability of the Mental Health Research Institute Unusual
Perceptions Schedule (MUPS): an instrument to record auditory hallucinatory
experience. Schizophrenia Research, 16, 157-165.
Copolov, D., Trauer, T., & MacKinnon, A. (in press). On the non-significance of internal
versus external auditory hallucinations. Schizophrenia Research.
Haddock, G., McCarron, J., Tarrier, N., & Faragher, E. B. (1999). Scales to measure
dimensions of hallucinations and delusions: the psychotic symptom rating scales
(PSYRATS). Psychological Medicine, 29, 879-889.
Honig, A., Romme, M. A. J., Ensink, B. J., Escher, S. D., Pennings, M. H. A., & Devries,
M. W. (1998). Auditory Hallucinations: A comparison between patients and
nonpatients. The Journal of Nervous and Mental Disease, 186(10), 646-651.
Nayani, T. H., & David, A. S. (1996). The auditory hallucination: a phenomenological
survey. Psychological Medicine, 26, 177-189.
Linn, E. L. (1977). Verbal auditory hallucinations: mind, self and society. The Journal of
Nervous and Mental Disease, 164(1), 8-17.
Oulis, P. G., Mavreas, V. G., Mamounas, J. M., & Stefanis, C. N. (1995). Clinical
characteristics of auditory hallucinations. Acta Psychiatrica Scandinavica, 92, 97-102.
Sartorius, N., Shapiro, R., & Jablensky, A. (1974). The international pilot study of
schizophrenia. Schizophrenia Bulletin, 11, 21-34.

Appendix B
- 285 -
Appendix B Words used in the Affective Shifting task
Negative words
Positive words
evil miserable fantastic witty
abusive ugly wonderful pleasant
revolting incapable brilliant handsome
cruel coward genuine confident
worthless inadequate joyful perceptive
deceitful depressed loyal truthful
cheat desperate honest tender
vulgar guilty wise competent
horrible crude generous thoughtful
vicious dull intelligent likable
useless powerless courageous beloved
imbecile weak admirable tolerant
selfish lonely warm respectable
shameful hurt friendly gentle
retard angry talented funny
pathetic unhappy perfect reliable
failure foolish clever humorous
idiot lazy cheerful earnest
greedy helpless charming smart
hopeless fearful blessed efficient
dishonest incompetent sincere considerate
stupid loser creative brave
offensive adorable