cohen_oct202011
DESCRIPTION
http://cddep.org/sites/cddep.org/files/cohen_oct202011.pdfTRANSCRIPT

Influencing Behavior of Providers and Pa4ents: The Micro-‐Financial
Environment
Jessica L. Cohen Harvard School of Public Health & Brookings Ins4tu4on
October 20, 2011

The Pa4ent: Incen4ves to Use RDTs
Ø An RDT is a “consump4on good”: consume informa4on about true cause of illness
Ø “Value of informa4on” = willingness to pay for info, prior to decision
Ø Value = Benefit – Cost
Ø Direct and indirect costs of purchasing informa4on.
Ø No direct benefits to RDTs per se—benefit is the aversion of costs – One benefit is poten4ally avoiding cost of unnecessary an4malarial. – Another is avoiding an illness that progresses in severity
Ø Pa4ents who want informa4on on true cause of illness have op/ons, of which RDTs are only one, each with an associated cost and benefit – Presump4ve treatment of malaria is one way of purchasing info – “Wait and see” is a form of informa4on acquisi4on too

Condi4ons for Pa4ents to Want RDTs I. There is Some Value to the Informa4on
Ø RDTs only valuable in condi4ons of uncertainty
Ø Value of informa4on is low when: 1) People are sure they know when symptoms equal malaria or symptoms do not equal malaria. 2) People don’t believe test is accurate. Or at least more accurate than subjec4ve assessment of probe(malaria|symptoms).
Ø The RDT most valuable (i.e. WTP highest) when least certain in own assessment and most certain about accuracy of test.

Cost:
Ø Price of the RDT Ø Opportunity cost of 4me Ø Non-‐economic (e.g. psychological, sociological)—fear, reluctance to try new
technology, etc.
Benefit:
Benefit is in aversion of costs incurred if don’t take RDT. Directly linked to what alterna/ves people have.
E.g., if relevant alterna4ve is presump4ve treatment, poten4al benefits are:
Ø Avoiding the cost of the an4malarial Ø Avoiding mis-‐diagnosis (poten4ally lead to worse illness) Ø Non-‐economic (e.g. psychological)—uncertainty avoidance
Condi4ons for Pa4ents to Want RDTs II. Benefit of the Informa4on Exceeds its Cost

Costs are lowered when:
Ø RDTs subsidized and/or measures taken to reduce mark-‐ups
Ø RDTs are easily accessible & available (OTC, provided by CHWs, etc.)
Ø They become familiar, there is learning-‐by-‐doing or learning from peers
Benefits are increased when:
Ø An4malarials are expensive (or have side effects)
Ø Public facili4es are far, inconvenient, not well-‐stocked, etc. Ø Probability it is not malaria is high & consequences of delay in trea4ng
not-‐malarial illness is high (e.g. for pneumonia in children)
Ø Alterna4ve types of learning unreliable—e.g. microscopy high error rate
Condi4ons for Pa4ents to Want RDTs II. Benefit of the Informa4on Exceeds its Cost

Op4on 1: Do Nothing/Wait Costs: Zero today. Possibly high future costs if illness gets worse.
Benefits: Avoid the cost of medicine and opportunity cost of seeking care.
Op4on 2: Treat Presump4vely with OTC An4-‐malarial Costs: Direct cost of meds. Possibly high future costs if not malaria & gets worse. Benefits: Avoid the cost of seeking care at facility & possibility of missed malaria.
Op4on 3: Buy an RDT at Drug Shop Costs: Direct cost of RDT & of meds if test posi4ve. Possibly high future cost if RDT is
nega4ve and true illness gets worse. Benefits: Avoid the cost of seeking care at facility & possibility of missed malaria.
Op4on 4: Go to Health Facility Costs: Direct costs of health facility visit (depends on context; usually an4malarials
free). Direct & indirect costs of travel & wai4ng, stockouts. Benefits: Possibly most accurate diagnosis (including assessment & treatment of
alterna4ve illness)—avoid missed illness. Avoid costs of an4malarial.
Condi4ons for Pa4ents to Want RDTs III. Net Benefit of RDTs Higher than Alterna4ves

Cohen, Dupas & Schaner (2011); Western Kenya
• Pre-‐AMFm, gave households cards allowing purchase of subsidized ACTs & RDTs in local drug shops
• Random varia4on in price of ACTs & RDTs; RDTs varied from $0 -‐ $0.20 • Measured WTP & impact on treatment seeking
Some basic results:
Ø Doubled rate at which illnesses diagnosed (from 22% to 44%) Ø Did not crowd out diagnosis (microscopy) at health center Ø Good distribu4onal effects : illiterate: 14%-‐> 31%; literate: 27% -‐> 52% Ø RDT seeking increasing with “predicted posi4vity” (Figure )
Ø 80% of the 4me, when people bought ACTs, bought RDT also. Willing to pay (at these low prices).
Ø People no more likely to use RDT when ACT price was higher. Ø 99% of RDT-‐posi4ve bought ACT; 60% of RDT-‐nega4ve bought ACT
Pa4ents: Evidence

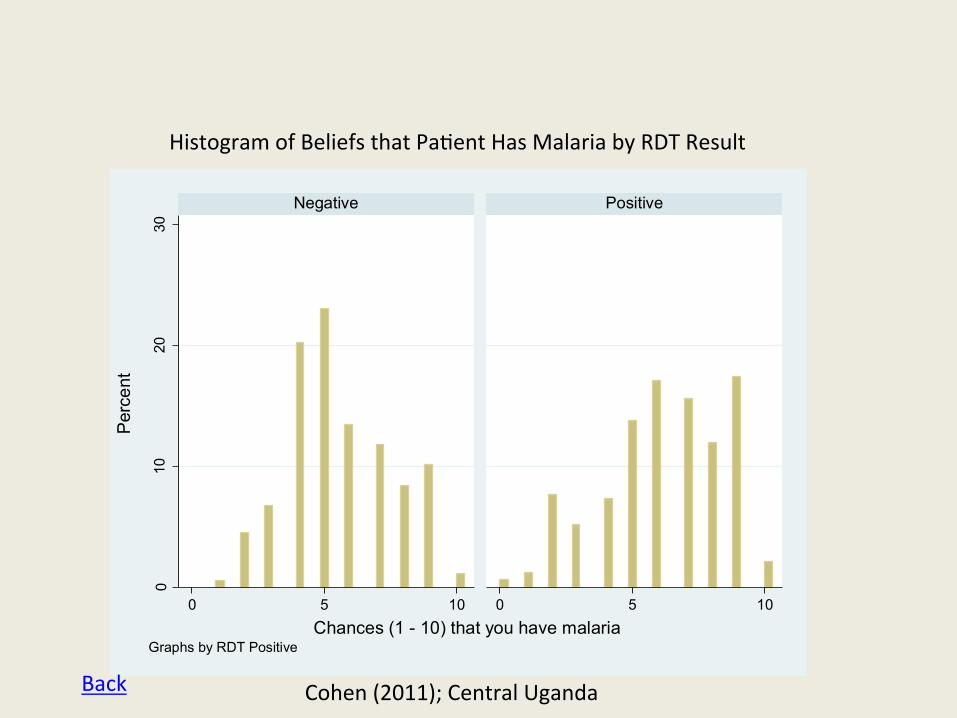
Cohen (2011); Central Uganda
• Pre-‐AMFm. Subsidized ACTs offered for sale with varying packaging/ messaging to encourage adherence
• RDTs randomly offered to some pa4ents when arrived at shops to buy ACT • Measuring impact of packaging and RDT on adherence to ACTs • Measure beliefs about whether the illness was malaria prior to doing RDT
Some basic results: Ø There is significant uncertainty about the likelihood of malaria (Fig1) Ø People are decent guessers (but not perfect) about chances (Fig2) Ø Over-‐treatment much more likely for adults (Fig 3) Ø RDT-‐posi4ve 25% more likely to adhere, but not necessarily the effect of RDTs
Pa4ents: Evidence
Cohen, Dupas, Schaner (on-‐going); Western Kenya • Ask about chances the illness is malaria before and ater RDT. Ø People revise upward when test posi4ve (but not to 1), revise downward when test nega4ve (but not to 0); suggests some belief in test but not perfect

Ø Commonly heard that shops wouldn’t want to sell RDTs. Why? – Well-‐known that people “over-‐treat” malaria – Shops could lose money on these unnecessary an4malarial purchases
Ø True, but they can make addi4onal profits from: – Selling the test – Selling alterna4ve treatment when test is nega4ve – Selling the an4malarial at a higher price (WTP could increase w/ certainty)
Ø As profits from these products increase, drug shops become more willing to sell RDTs
Ø Profit will depend on what they can charge, which in turn depends on the things highlighted on the part of consumers – E.g. price of RDT can be higher as belief in test increases
Ø Will depend on market condi4ons (compe44on) as well as things like value of reputa4on (avrac4ng repeat customers).
Providers: Incen4ves to Sell RDTs; Components of RDT Prices

Externali4es from over-‐treatment
or Consumer probability belief > than shop owner’s
or Subsidies for an4malarials
Shop under-‐provides RDTs
No externali4es to over-‐treatment
& Shops & customers have accurate beliefs about malaria probability
Sell RDTs under all condi4ons we would want them to (max welfare)
Providers: Evidence I. Cohen & Dickens (2011): Economic Model of Shop Behavior
Mechanisms to increase RDT provision: 1. BCC targe4ng beliefs about malaria prevalence & accuracy of test 2. Increase compe44on between shops 3. Introduce RDT subsidy Op4mal RDT Subsidy = (Rate of overtreatment)*[(Subsidy for an4malarial) + (Social Cost of Over-‐treatment)]

Some results so far:
Ø RDTs are converging in price to around $1 (100% mark-‐up) Ø Rural shops more likely to sell/promote the RDTs than “urban” ones (stated
reason: proximity of urban shops to health centers) Ø RDTs more oten purchased for children than adults Ø Shops are crea4ve in promo4ng the RDTs (for example…) Ø RDTs maintaining quality (based on lot tes4ng ater 4me in field) Ø Shops easily trained for the most part & following protocol Ø Some crea4ve shops are offering a “bundle price” for the RDT and treatment
Providers: Evidence
Cohen, Fink, Dickens (Uganda; Ongoing)
• Sell subsidized RDTs ($0.50) through wholesaler to shops in 8 districts. • Implement BCC campaign (with Uganda Health Marke4ng Group) to test key messages on RDT use and adherence to test results

• Not really enough to know willingness to pay for RDTs. Why? Ø This is likely to change over 4me as people revise expecta4ons about the
prob(malaria|symptoms) and the belief in the test. Ø Very high rates of over-‐treatment & ignoring test results could be “short-‐
run” • What are the key behavioral messages to encourage diagnosis and
adherence to test results? This could speed up acceptance of RDTs. • Cri4cal need for bever evidence on how treatment seeking varies with
underlying endemicity – For example, oten assume RDTs more cost-‐effec4ve in low endemicity
se|ngs, but this is only if people are really bad at guessing. • How do RDTs affect adherence to ACTs?
– Important for cost-‐effec4veness calcula4ons which are majorly determined by probability of resistance
• What determines shops’ RDT pricing decisions? Are there any policy levers we can pull to influence them?
• Are there technological improvements in RDTs that bever fit consumer/provider beliefs/incen4ves ?
Summing Up: Some Key Missing Pieces

.4.6
.81
lpol
y sm
ooth
: J5:
wen
t to
chem
ist
0 .2 .4 .6 .8 1
No Subsidy ACT Subsidy
0.2
.4.6
Sha
re
0 .2 .4 .6 .8 1Predicted Positivity
A. All
0.2
.4.6
Sha
re
0 .2 .4 .6 .8 1Predicted Positivity
B. Illiterate Head
0.2
.4.6
Sha
re
0 .2 .4 .6 .8 1Predicted Positivity
C. Literate Head
Illness was treated with ACT
Back
Cohen, Dupas, Schaner 2011. (Kenya)

.2.4
.6.8
1
lpol
y sm
ooth
: J5:
wen
t to
chem
ist
0 .2 .4 .6 .8 1
ACT Subsidy Only ACT + RDT Subsidy
0.2
.4.6
Sha
re
0 .2 .4 .6 .8 1Predicted Positivity
A. All
0.2
.4.6
Sha
re
0 .2 .4 .6 .8 1Predicted Positivity
B. Illiterate Head
0.2
.4.6
Sha
re
0 .2 .4 .6 .8 1Predicted Positivity
C. Literate Head
Took Malaria Test
Back
Cohen, Dupas, Schaner 2011. (Kenya)

Cohen (2011); Central Uganda
05
1015
20P
erce
nt
0 2 4 6 8 10Chances (1 - 10) that you have malaria
Histogram of Beliefs About Likelihood Patient Has MalariaHistogram of Beliefs that Pa4ent Has Malaria
Back
010
2030
0 5 10 0 5 10
Negative Positive
Per
cent
Chances (1 - 10) that you have malariaGraphs by RDT Positive
Histogram of Beliefs that Pa4ent Has Malaria by RDT Result
Back Cohen (2011); Central Uganda

0.2
.4.6
.81
Sha
re M
alar
ia P
ositi
ve
0 20 40 60 80Age
kernel = epanechnikov, degree = 0, bandwidth = 4.08
Actual Posi4vity Among Subsidized ACT Buyers Local Linear Regressions of Posi4vity on Age
Cohen, Dupas and Schaner (2011); Western Kenya
Cohen (2011); Central Uganda
Back

Back

Back