coimbatore medical college, coimbatore april...
TRANSCRIPT
A Dissertation on
HAEMATOLOGICAL MANIFESTATIONS IN
CHRONIC OBSTRUCTIVE LUNG DISEASE
IN RELATION TO FEV1
COIMBATORE MEDICAL COLLEGE HOSPITAL
Dissertation Submitted to
THE TAMILNADU Dr.M.G.R. MEDICAL UNIVERSITY
CHENNAI - 600 032
With partial fulfillment of the regulations
for the award of the degree of
M.D. GENERAL MEDICINE
BRANCH-I
COIMBATORE MEDICAL COLLEGE,
COIMBATORE
APRIL 2015
CERTIFICATE
Certified that this is the bonafide dissertation in “HAEMATOLOGICAL
MANIFESTATIONS IN CHRONIC OBSTRUCTIVE LUNG
DISEASE IN RELATION TO FEV1” done by Dr. GOWRI SANKAR.
M and submitted in partial fulfillment of the requirements for the Degree
of M.D., General Medicine, Branch I of The Tamilnadu Dr. M.G.R.
Medical University, Chennai.
Date: Guide, Professor & Chief
Medical Unit III
Date: Professor & Head
Department of Medicine
Date: Dean
Coimbatore Medical College
Coimbatore
DECLARATION
I solemnly declare that the dissertation titled “HAEMATOLOGICAL
MANIFESTATIONS IN CHRONIC OBSTRUCTIVE
LUNG DISEASE IN RELATION TO FEV1” was done by me
from AUGUST 2013 to JULY 2014 under the guidance and supervision of
Professor Dr. S.USHA .M.D. This dissertation is submitted to
The Tamilnadu Dr.M.G.R. Medical University towards the partial
fulfillment of the requirement for the award of MD Degree in General
Medicine (Branch I).
Place: Coimbatore Dr. GOWRI SANKAR.M
Date:
ACKNOWLEDGEMENT
I wish to express my sincere thanks to our respected
Dean Prof. Dr.S.REVWATHY, M.D.DGO.DNB., for having allowed
me to conduct this study in our hospital.
I express my heartfelt thanks and deep gratitude to the Head of the
Department of Medicine Prof. Dr. KUMAR NATARAJAN, M.D. for his
generous help and guidance in the course of the study.
I am extremely grateful to Prof. Dr. S. USHA, M.D., Professor of
medicine for her continuous motivation,timely advice and valuable
criticism which enabled me to complete the dissertation.
I would also like to thank wholeheartedly the professor of the
Department of Pulmonology Prof. Dr. S. KEERTHIVASAN, MD., for
his encouragement and guidance during the study.
I’m privileged to extend my gratitude and respect to
Dr. R. VANI. MBBS., DTCD, and Dr. K. ANBANANTHAN, MD., the
assistant professor of Department of Pulmonology. I’m thankful to them
for their valuable thoughts, inspiring comments and guidance.
I sincerely thank all Professors and Asst. Professors
Dr. T.GEETHA M.D., Dr. P.S.RANI M.D., Dr. SIVAKUMAR. M.D.,
I would like to thank them for their Valuable suggestions. I’m indebted to
them for being a constant source of inspiration.
My sincere thanks to all my friends and post-graduate colleagues for
their whole hearted support and companionship during my studies.
I thank all my PATIENTS, who formed the backbone of this study,
without whom this study would not have been possible.
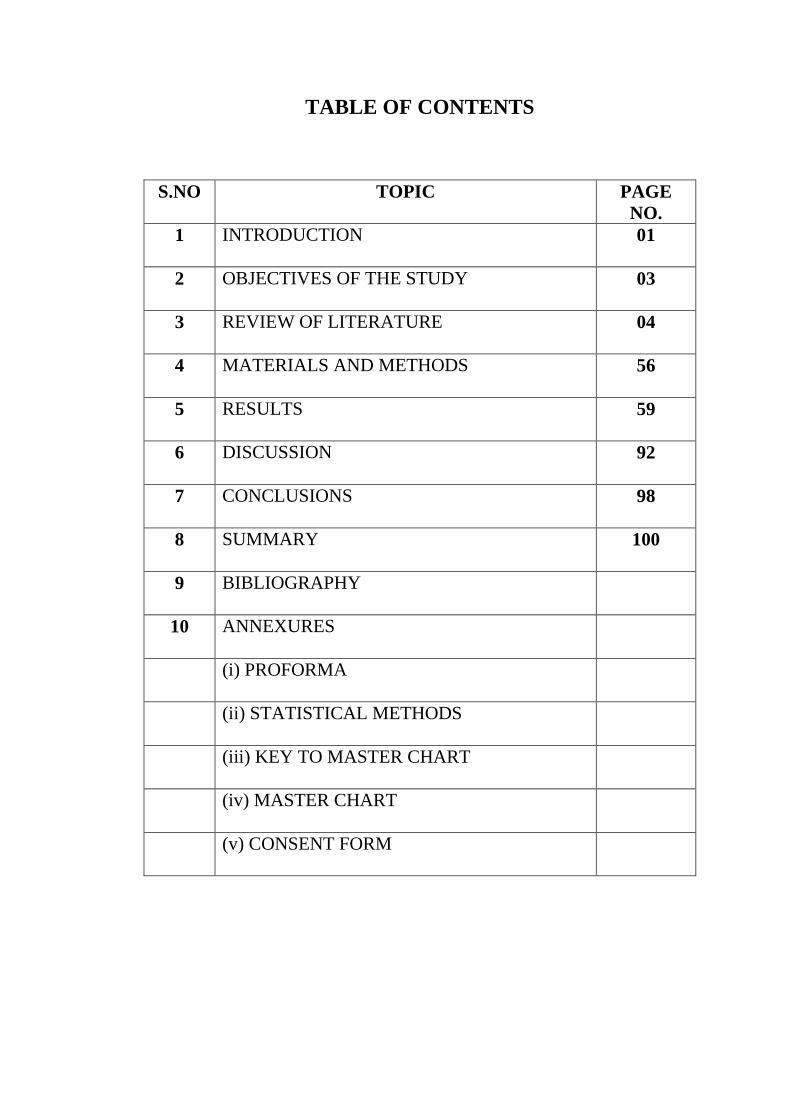
TABLE OF CONTENTS
S.NO TOPIC PAGE
NO.
1 INTRODUCTION 01
2 OBJECTIVES OF THE STUDY 03
3 REVIEW OF LITERATURE 04
4 MATERIALS AND METHODS 56
5 RESULTS 59
6 DISCUSSION 92
7 CONCLUSIONS 98
8 SUMMARY 100
9 BIBLIOGRAPHY
10 ANNEXURES
(i) PROFORMA
(ii) STATISTICAL METHODS
(iii) KEY TO MASTER CHART
(iv) MASTER CHART
(v) CONSENT FORM

LIST OF ABBREVIATIONS USED
1. COPD - Chronic Obstructive Pulmonary Disease
2. HB – Haemoglobin
3. MCV - Mean Corpuscular Volume
4. MCH - Mean Corpuscular Haemoglobin
5. MCHC - Mean Corpuscular Haemoglobin Concentration
6. SABA - Short-Acting Beta-Agonist
7. SAMA - Short Acting Antimuscarninic Agent
8. LAMA - Long-Acting Antimuscarninic Agent
9. LABA - Long-Acting Beta-Agonist
10.ICA - Inhaled Corticosteroids
11. FEV1 - Forced Expiratory Volume in One Second
12. FVC - Forced Vital Capacity
13. WHO – World Health Organisation
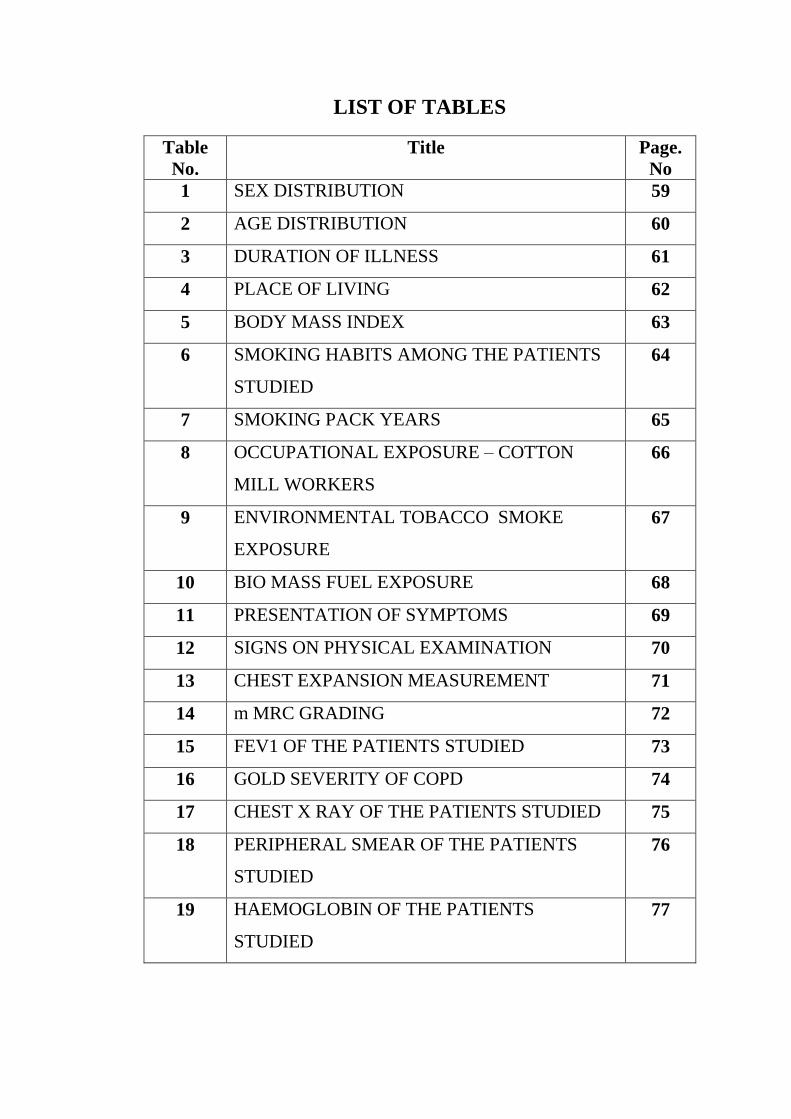
LIST OF TABLES
Table
No.
Title Page.
No
1 SEX DISTRIBUTION 59
2 AGE DISTRIBUTION 60
3 DURATION OF ILLNESS 61
4 PLACE OF LIVING 62
5 BODY MASS INDEX 63
6 SMOKING HABITS AMONG THE PATIENTS
STUDIED
64
7 SMOKING PACK YEARS 65
8 OCCUPATIONAL EXPOSURE – COTTON
MILL WORKERS
66
9 ENVIRONMENTAL TOBACCO SMOKE
EXPOSURE
67
10 BIO MASS FUEL EXPOSURE 68
11 PRESENTATION OF SYMPTOMS 69
12 SIGNS ON PHYSICAL EXAMINATION 70
13 CHEST EXPANSION MEASUREMENT 71
14 m MRC GRADING 72
15 FEV1 OF THE PATIENTS STUDIED 73
16 GOLD SEVERITY OF COPD 74
17 CHEST X RAY OF THE PATIENTS STUDIED 75
18 PERIPHERAL SMEAR OF THE PATIENTS
STUDIED
76
19 HAEMOGLOBIN OF THE PATIENTS
STUDIED
77

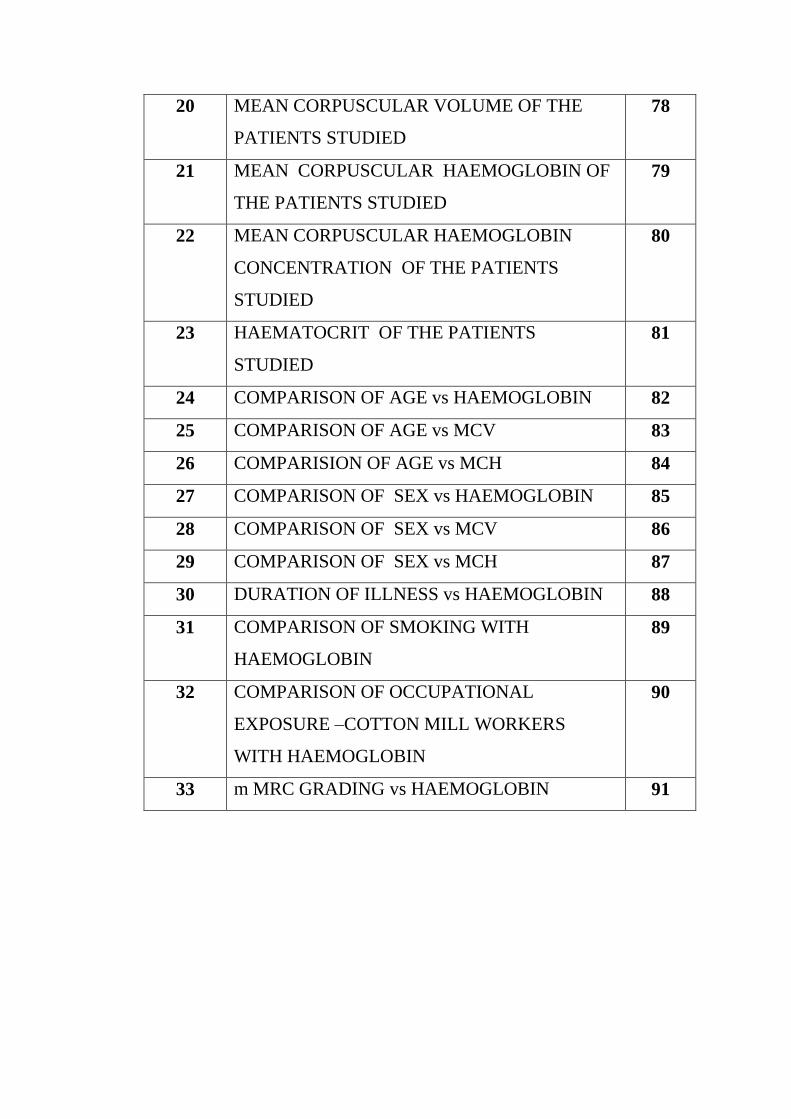
20 MEAN CORPUSCULAR VOLUME OF THE
PATIENTS STUDIED
78
21 MEAN CORPUSCULAR HAEMOGLOBIN OF
THE PATIENTS STUDIED
79
22 MEAN CORPUSCULAR HAEMOGLOBIN
CONCENTRATION OF THE PATIENTS
STUDIED
80
23 HAEMATOCRIT OF THE PATIENTS
STUDIED
81
24 COMPARISON OF AGE vs HAEMOGLOBIN 82
25 COMPARISON OF AGE vs MCV 83
26 COMPARISION OF AGE vs MCH 84
27 COMPARISON OF SEX vs HAEMOGLOBIN 85
28 COMPARISON OF SEX vs MCV 86
29 COMPARISON OF SEX vs MCH 87
30 DURATION OF ILLNESS vs HAEMOGLOBIN 88
31 COMPARISON OF SMOKING WITH
HAEMOGLOBIN
89
32 COMPARISON OF OCCUPATIONAL
EXPOSURE –COTTON MILL WORKERS
WITH HAEMOGLOBIN
90
33 m MRC GRADING vs HAEMOGLOBIN 91
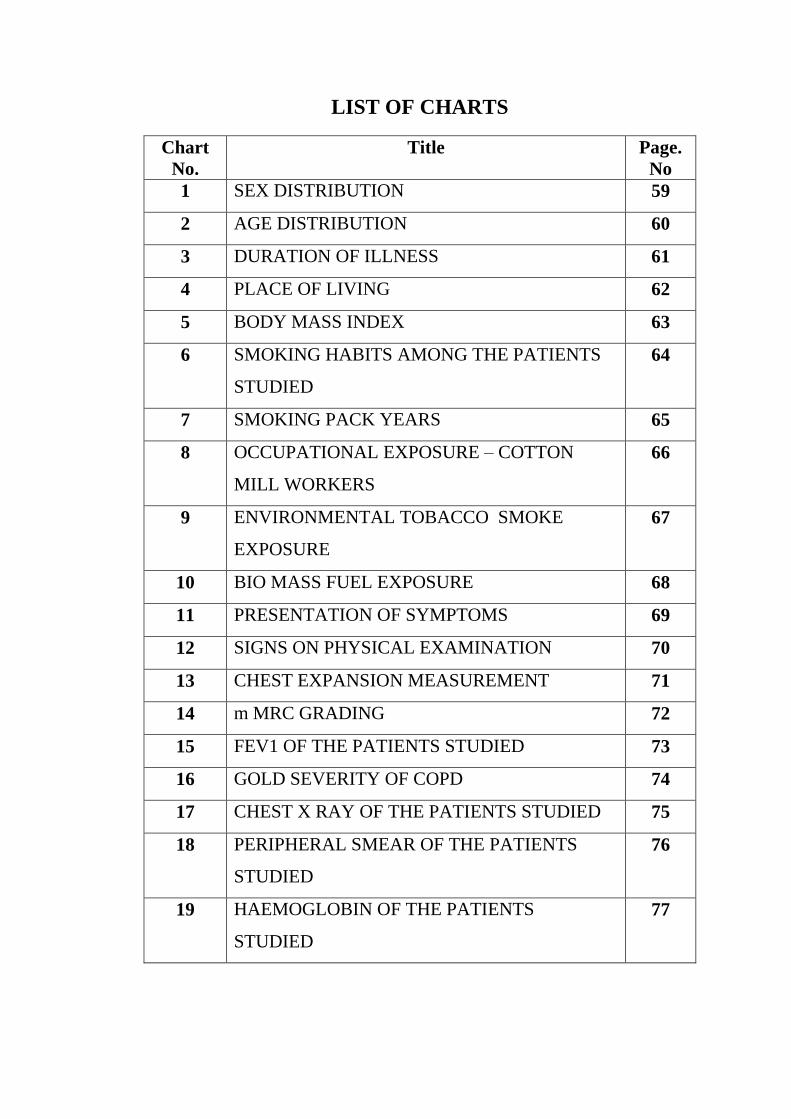
LIST OF CHARTS
Chart
No.
Title Page.
No
1 SEX DISTRIBUTION 59
2 AGE DISTRIBUTION 60
3 DURATION OF ILLNESS 61
4 PLACE OF LIVING 62
5 BODY MASS INDEX 63
6 SMOKING HABITS AMONG THE PATIENTS
STUDIED
64
7 SMOKING PACK YEARS 65
8 OCCUPATIONAL EXPOSURE – COTTON
MILL WORKERS
66
9 ENVIRONMENTAL TOBACCO SMOKE
EXPOSURE
67
10 BIO MASS FUEL EXPOSURE 68
11 PRESENTATION OF SYMPTOMS 69
12 SIGNS ON PHYSICAL EXAMINATION 70
13 CHEST EXPANSION MEASUREMENT 71
14 m MRC GRADING 72
15 FEV1 OF THE PATIENTS STUDIED 73
16 GOLD SEVERITY OF COPD 74
17 CHEST X RAY OF THE PATIENTS STUDIED 75
18 PERIPHERAL SMEAR OF THE PATIENTS
STUDIED
76
19 HAEMOGLOBIN OF THE PATIENTS
STUDIED
77
20 MEAN CORPUSCULAR VOLUME OF THE
PATIENTS STUDIED
78
21 MEAN CORPUSCULAR HAEMOGLOBIN OF
THE PATIENTS STUDIED
79
22 MEAN CORPUSCULAR HAEMOGLOBIN
CONCENTRATION OF THE PATIENTS
STUDIED
80
23 HAEMATOCRIT OF THE PATIENTS
STUDIED
81
24 COMPARISON OF AGE vs HAEMOGLOBIN 82
25 COMPARISON OF AGE vs MCV 83
26 COMPARISION OF AGE vs MCH 84
27 COMPARISON OF SEX vs HAEMOGLOBIN 85
28 COMPARISON OF SEX vs MCV 86
29 COMPARISON OF SEX vs MCH 87
30 DURATION OF ILLNESS vs HAEMOGLOBIN 88
31 COMPARISON OF SMOKING WITH
HAEMOGLOBIN
89
32 COMPARISON OF OCCUPATIONAL
EXPOSURE –COTTON MILL WORKERS
WITH HAEMOGLOBIN
90
33 m MRC GRADING vs HAEMOGLOBIN 91

LIST OF FIGURES
Figure
No.
Figure Title Page No.
1 TEOFILO BONET 04
2 GIAMBATISA MORGAGNI 04
3 JOSEF LEOPOLD AUENBRUGGER 05
4 TREATISE OF DISEASES OF THE CHEST 05
5 SHADOW IMAGE OF JOHN HUTCHINSON
AND HIS SPIROMETRY
05
6 DEVELOPMENT OF THE RESPIRATORY
SYSTEM
08
7 MAJOR PHASES OF RESPIRATORY
DEVELOPMENT
09
8 BRONCHI AND THEIR DIVISIONS 12
9 BRONCHOPULMONARY SEGMENTS 13
10 STRUCTURES OF THE LUNGS /
GENERATIONS
14
11 PULMONARY CIRCULATION 16
12 LUNG VOLUMES AND CAPACITIES 18
13 RISK FACTORS OF COPD 24
14a. THE OVERLAP OF COPD AND ASTHMA 29
14b. THE OVERLAP OF COPD AND ASTHMA 29
15 MECHANISMS OF AIRWAY
OBSTRUCTION IN COPD
30
16 SYSTEMIC MANIFESTATIONS OF COPD 32
17 PATHOGENESIS OF COPD 32
18 CAUSES OF EXACERBATION OF COPD 34
19 SPIROMETRY 39
20 CLASSIFICATION OF SEVERITY OF COPD 40
21 DYNAMIC FLOW –VOLUME LOOPS 41
22 BODE INDEX FOR STAGING COPD 42
23 CHEST X-RAY OF COPD 43
24 NICOTINE PATCH 47
25 NICOTINE INHALER 47
26 ROLE OF PHYSICAL REHABILITATION 48
27 GOLD THERAPY AT EACH STAGE OF
COPD
50
28 PHARMACOLOGIC TREATMENT OPTIONS
IN COPD
51
29 COPD INHALED PHARMACOTHERAPY 51
30 WORLD COPD DAY-2014 LOGO 55
ABSTRACT
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a complex disease characterized
by airflow limitation resulting from airway inflammation, parenchymal destruction
and the development of emphysema. COPD results from inflammatory
mechanisms, the “SPILL-OVER” of inflammatory mediators like IL6, IL-8,
TNF-∝ leads to systemic inflammation and also initiates or worsens comorbid
diseases. About 15-30% of COPD patients have anemia and this is noticed
especially in patients with severe disease, and the occurrence of polycythaemia is
only 6%. Anemia is related to depressed functional capacity and for low quality
and standard of life.
METHODOLOGY
This clinical observational study was undertaken to investigate the pattern and
magnitude of Hematological parameters in the relationship with the severity of the
disease by Forced Expiratory Volume1 (FEV1). 60 Patients were included in this
study.
All the Patients were subjected to detailed History and Physical examination. Lung
function parameters were assessed with the help of spirometer. All patients
underwent Haematological parameters with particular reference to HB%, MCV,
MCH, MCHC, HAEMATOCRIT, and PERIPHERAL SMEAR along with routine
tests.
RESULTS AND DISCUSSION
In our study, 56% of patients had anemia, among them 70% had Normocytic
Normochromic Anemia and 30% had Microcytic Hypochromic Anemia. Patients
with duration of illness 6-10 yrs had 57% risk for anemia and > 10 yrs had 87%
risk for anemia. Patients with history of exposure to Cotton mill dust had 71% risk
for anemia.
CONCLUSION
Patients with decreased FEV1, having prolonged duration of illness and increasing
grades of dyspnea had high risk for anemia. Patients with exposure to Cotton Mill
dust and with the history of smoking had increased risk for anemia, but its
association was not statistically significant.
KEY WORDS
COPD
ANEMIA
FEV1

INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a complex
disease characterized by airflow limitation resulting from airway
inflammation, parenchymal destruction and the development of
emphysema. COPD results from inflammatory mechanisms, the “SPILL-
OVER” of inflammatory mediators like IL6, IL-8, and TNF-∝ leads to
systemic inflammation and also initiates or worsens comorbid diseases. So
the comorbities complicate the management of COPD and need to be
evaluated carefully1. Diseases with higher morbidity in COPD are
associated with an increased risk of hospital admissions,mortality and
healthcare costs2-3. According to World Health Organisation, in 2020
COPD will become the 3 rd leading cause of death. Meta-analysis study in
India suggests that the prevalence of COPD above 30 yrs in males is 5%
and in females is 2.7%.
According to a study, about 15-30% of COPD patients have
anemia and this is noticed especially in patients with severe disease, and
the occurrence of polycythaemia is only 6% 4-6 . Anaemia is related to
depressed exercise capacity along with functional dyspnea.This is a
significant reason for depressed functional capacity and for low quality and
standard of life.7-9

Forced Expiratory Volume in one second (FEV1) is an objective
measurement,viewed as the most accurate predictor of severity of airway
obstruction. The advantage of FEV1 is that it requires lesser effort to
measure and can be carried out in all stages of COPD patients .COPD
progression can be assessed by serial measurements of FEV1. In this
dissertation an effort is made to assess the hematological manifestations in
COPD Patients and the relationship to FEV1.

OBJECTIVES OF THE STUDY
To study the Haematological manifestations in relation to FEV1 in 60
cases of Chronic Obstructive Pulmonary Disease.
REVIEW OF LITERATURE
HISTORY OF COPD
Empysema goes for description with hierarchial reference as follows:
“Voluminous lungs” was widely explained by Bonet in 1679;
Morgagni’s (1769) showed the lungs were “turgid”, particularly from
air.
FIG 1: TEOFILO BONET FIG 2: GIAMBATISA MORGAGNI
(1620 -1689) (1682-1771)
Baille's descriptions about the emphysematous lung, was exactly similar
to Samuel Johnson’s one.
The emergence of our clinical apprehension of the chronic bronchitis rose
from Badham (1814), who attributed chronic cough and mucus
hypersecretion jointly to the word "catarrh".10
Percussion probably got developed as a way of ascertaining how much
fluid remained in barrels of wine by Austrian physician Josef Leopold
Auenbrugger who applied percussion of chest, having learned this method
in his father’s wine cellar.11

FIG 3: Josef Leopold Auenbrugger (1722-1809)
Laennec, the inventor of Stethescope ,in 1821, explained exhaustively
about Emphysema in his “Treatise of Diseases of the Chest”
FIG 4: “Treatise of Diseases of the Chest”.
In 1846, John Hutchinson (1811-1861) invented spirometer and he
described the values of vital capacity in measurement.
FIG 5 : SHADOW IMAGE OF JOHN HUTCHINSON AND
HIS SPIROMETRY

Tiffeneau ten decades later, mentioned Timed Vital Capacity as a
parameter in Spirometry.
Gaensler introduced the concept of Forced Vital Capacity ,which
forms the foundation for FEV1 and FEV1/FVC.10
In 1916, Osler’s Principles and Practices of Medicine describes
“EMPHYSEMA”
In 1956, Barach and Bickerman presented the first comprehensive
text book on “Pulmonary Emphysema”.
DEVELOPMENT OF THE RESPIRATORY SYSTEM12-17
The human developmental phases between fertilization and birth are
generally divided into
Embryonic Period Fetal period
The embryonic period occurs during the first 8 weeks and is
traditionally organized into 23 stages. During the embryonic period, all
major organs begin their development.
The fetal period occurs during the remaining32 weeks of gestation.
During this period, the organs continue to develop and refine their structure
and function.
There are three embryologically germinal tissue layers that eventually
forms all tissues and organ.
ENDODERM
MESODERM
ECTODERM
During the development, lung bud forms the trachea and two lateral
out pocketings, the bronchial buds. At the beginning of the fifth week, each
of these buds enlarges to form right and left main bronchi. The right then
forms three secondary bronchi, and the left forms two secondary bronchi.
The mesoderm, which covers the outside of the lungs, develops into
the visceral pleura. The somatic mesoderm layer, covering the body wall
from the inside, becomes the parietal pleura. The space between the parietal
and visceral pleura is pleural cavity.
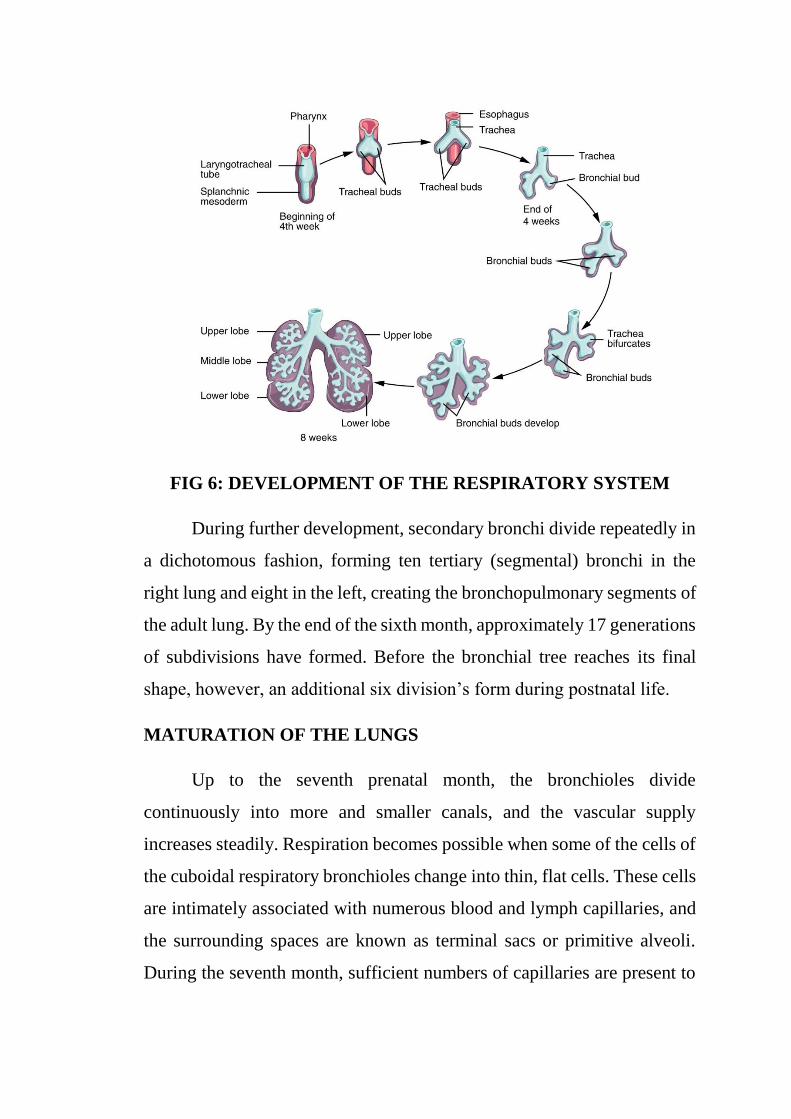
FIG 6: DEVELOPMENT OF THE RESPIRATORY SYSTEM
During further development, secondary bronchi divide repeatedly in
a dichotomous fashion, forming ten tertiary (segmental) bronchi in the
right lung and eight in the left, creating the bronchopulmonary segments of
the adult lung. By the end of the sixth month, approximately 17 generations
of subdivisions have formed. Before the bronchial tree reaches its final
shape, however, an additional six division’s form during postnatal life.
MATURATION OF THE LUNGS
Up to the seventh prenatal month, the bronchioles divide
continuously into more and smaller canals, and the vascular supply
increases steadily. Respiration becomes possible when some of the cells of
the cuboidal respiratory bronchioles change into thin, flat cells. These cells
are intimately associated with numerous blood and lymph capillaries, and
the surrounding spaces are known as terminal sacs or primitive alveoli.
During the seventh month, sufficient numbers of capillaries are present to
guarantee adequate gas exchange, and the premature infant is able to
survive.
During the last 2 months of prenatal life and for several years
thereafter, the number of terminal sacs increases steadily. Mature alveoli
are not present before birth. In addition to endothelial cells and flat alveolar
epithelial cells, another cell type develops at the end of the sixth month.
These cells, type II alveolar epithelial cells, produces surfactant, a
phospholipids-rich fluid capable of lowering surface tension at the air-
alveolar interface.
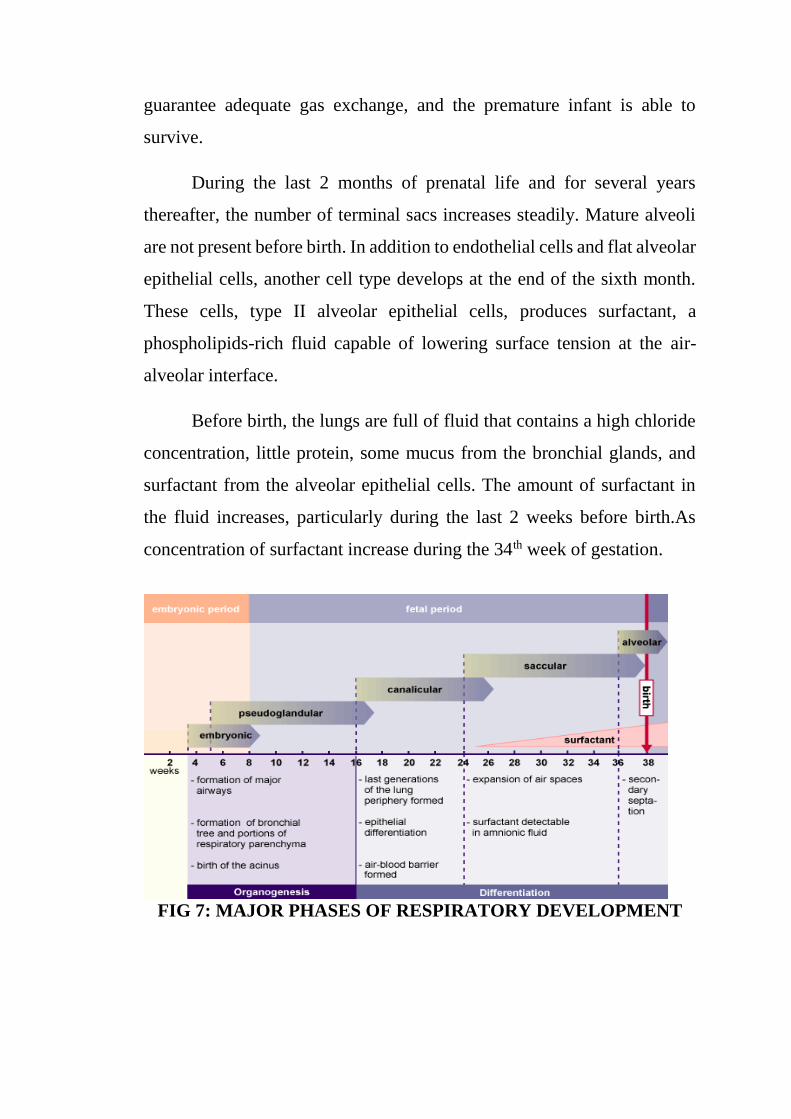
Before birth, the lungs are full of fluid that contains a high chloride
concentration, little protein, some mucus from the bronchial glands, and
surfactant from the alveolar epithelial cells. The amount of surfactant in
the fluid increases, particularly during the last 2 weeks before birth.As
concentration of surfactant increase during the 34th week of gestation.
FIG 7: MAJOR PHASES OF RESPIRATORY DEVELOPMENT
Throughout the developmental period, lung growth is similar in
male and female fetuses. A full-term newborn has about 50 million alveoli,
and the number continues to elevation for about 2 to 3 years after birth.
The developmental branching process of the airways and blood vessels of
the lung is highly regulated by the timely activation various genes in
different locations. Of the approximate 22,000 genes in the human genome,
about 40 are required for normal respiratory development.
ANATOMY18
UPPER RESPIRATORY TRACT
The Upper respiratory tract includes nose, pharynx, paranasal
sinuses and larynx. The nose is lined with ciliated epithelium helps in
clearance of particles and microorganisms.
Functions of the upper airway:
Passageway for gas flow
Filter
Heater
Humidification
Phonation
Protection of airways
Sense of smell and taste
LOWER RESPIRATORY TRACT
Trachea
It extends down from cricoid cartilage and bifurcates in the superior
mediastinum at the level of angle of Louis. The adult trachea is
approximately 12cm long and has inner diameter of 2cm. It is lined by
pseudo stratified ciliated columnar epithelium containing goblet cells. The
adult has 16 to 20 cartilaginous ring.The cartilaginous rings armor the
trachea so that it does not collapse during exhalation.
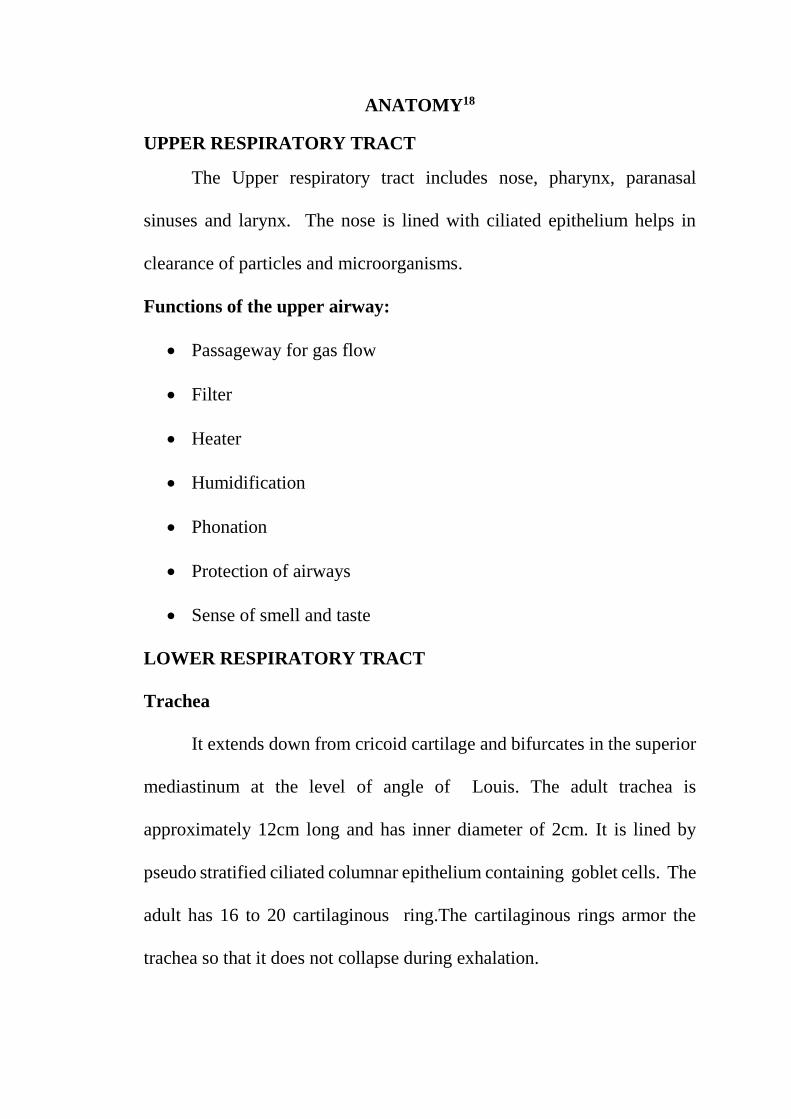
BRONCHI AND THEIR DIVISIONS
FIG 8: BRONCHI AND THEIR DIVISIONS
At the base of the trachea, Carina is a landmark where the trachea
bifurgates. The left bronchus branches with an angle of about 45 to 55
degrees and runs more horizontally and is about 5 cm long. The right main
bronchus branches with an angle of about 20 to 30 degrees and it is only
about 1 to 2.5 cm and is a more direct continuation of trachea.
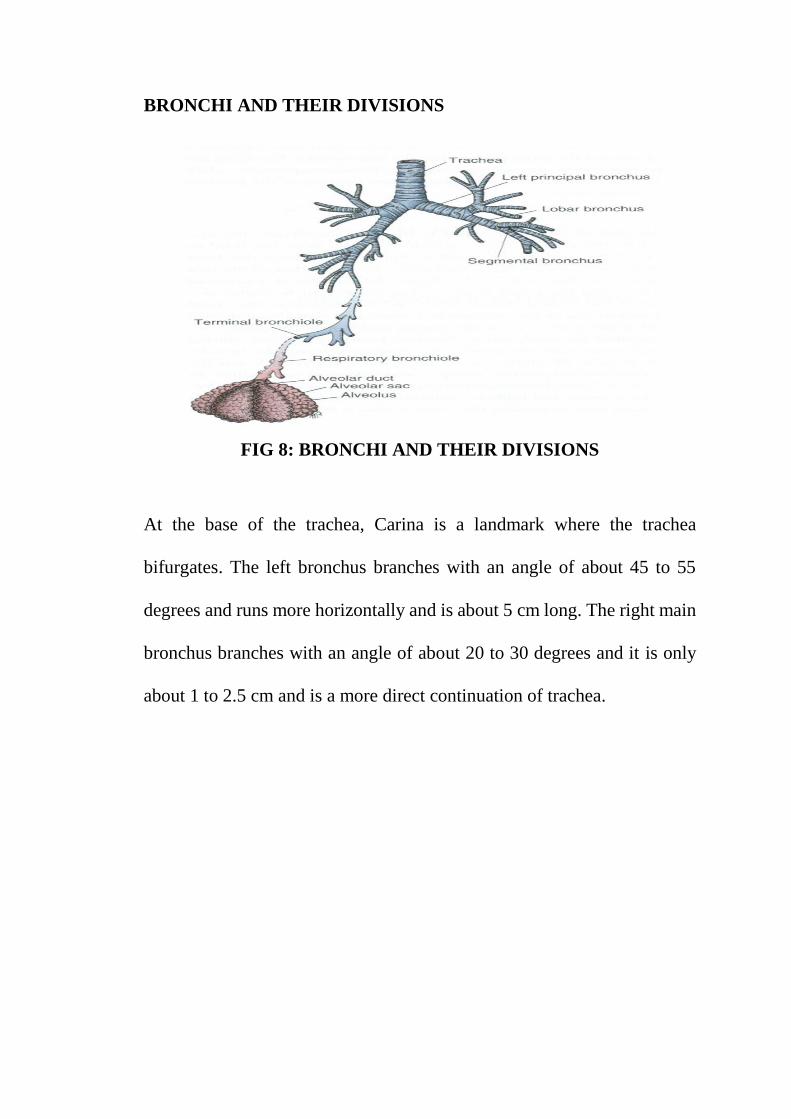
BRONCHOPULMONARY SEGMENTS
FIG 9: BRONCHOPULMONARY SEGMENTS
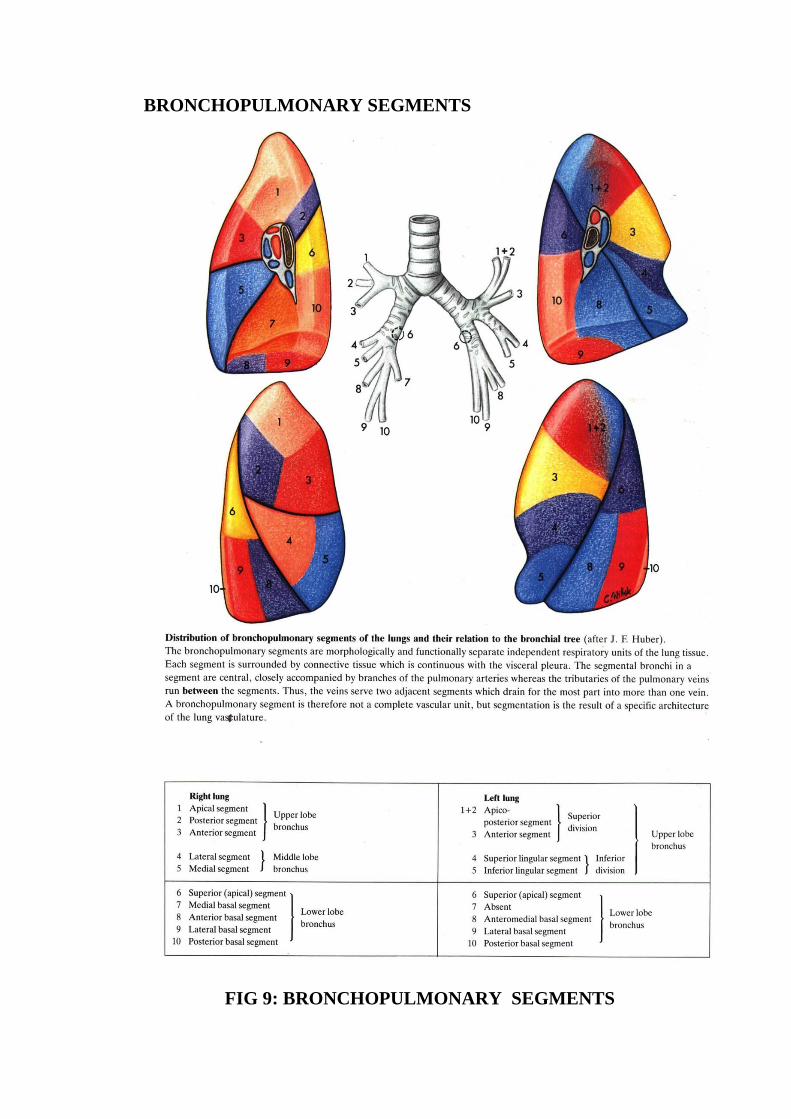
INTRA PULMONARY AIRWAYS are divided in to three major
groups
1) BRONCHI-has cartilage and serve as a airway
2) MEMBRANOUS BRONCHIOLES- non-cartilaginous airways
3) RESPIRATORY BRONCHIOLES-serve as a airways and for gas
exchange
There are about 28 generations of Tracheobronchial tree which serve as
a Conducting zone and Respiratory zone
FIG 10: STRUCTURES OF THE LUNGS
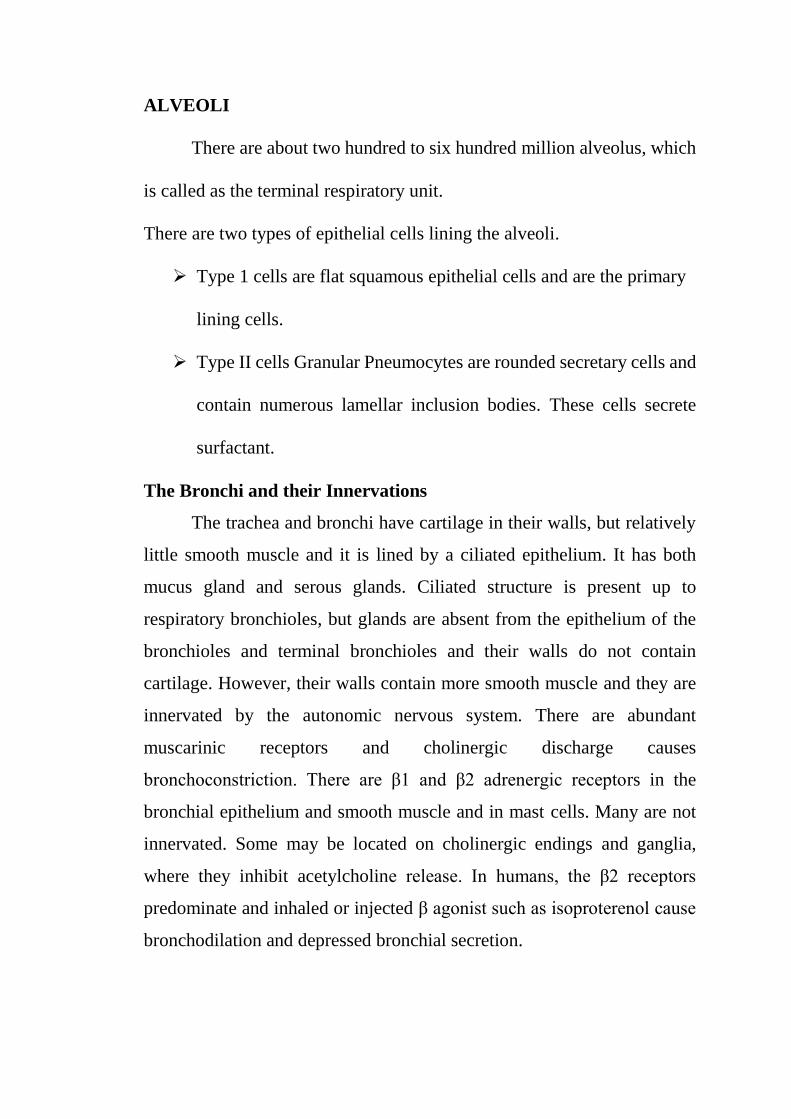
ALVEOLI
There are about two hundred to six hundred million alveolus, which
is called as the terminal respiratory unit.
There are two types of epithelial cells lining the alveoli.
Type 1 cells are flat squamous epithelial cells and are the primary
lining cells.
Type II cells Granular Pneumocytes are rounded secretary cells and
contain numerous lamellar inclusion bodies. These cells secrete
surfactant.
The Bronchi and their Innervations
The trachea and bronchi have cartilage in their walls, but relatively
little smooth muscle and it is lined by a ciliated epithelium. It has both
mucus gland and serous glands. Ciliated structure is present up to
respiratory bronchioles, but glands are absent from the epithelium of the
bronchioles and terminal bronchioles and their walls do not contain
cartilage. However, their walls contain more smooth muscle and they are
innervated by the autonomic nervous system. There are abundant
muscarinic receptors and cholinergic discharge causes
bronchoconstriction. There are β1 and β2 adrenergic receptors in the
bronchial epithelium and smooth muscle and in mast cells. Many are not
innervated. Some may be located on cholinergic endings and ganglia,
where they inhibit acetylcholine release. In humans, the β2 receptors
predominate and inhaled or injected β agonist such as isoproterenol cause
bronchodilation and depressed bronchial secretion.
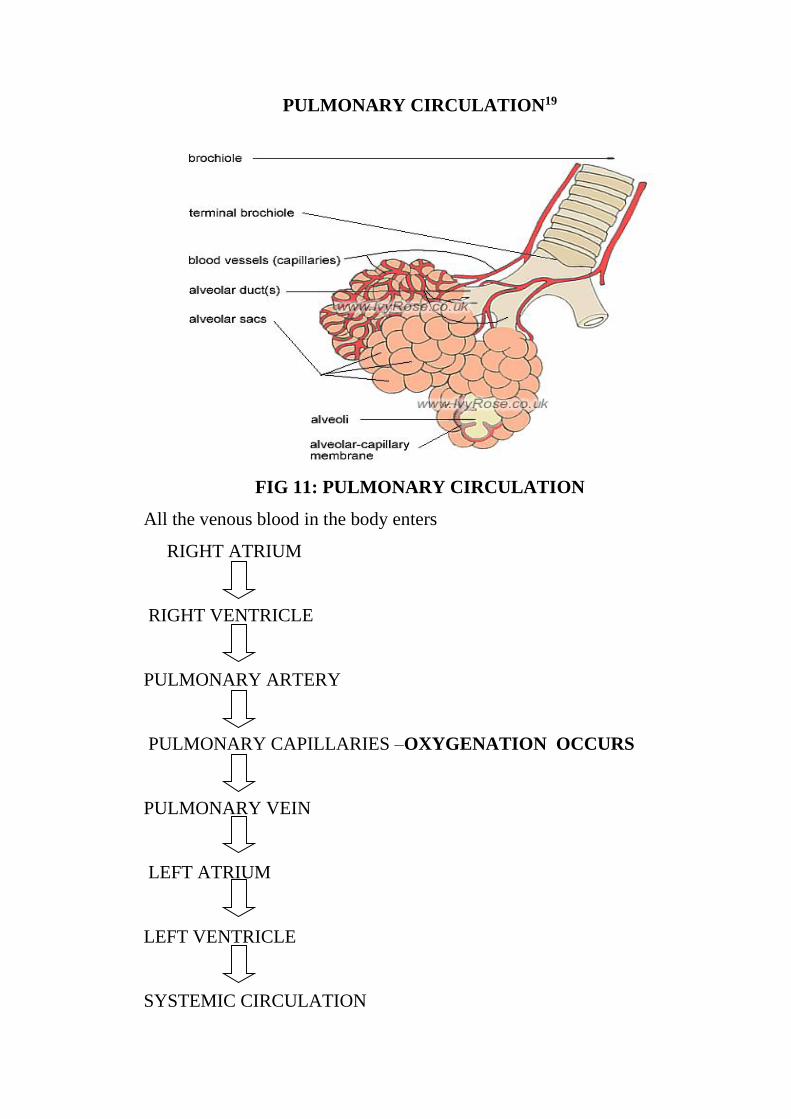
PULMONARY CIRCULATION19
FIG 11: PULMONARY CIRCULATION
All the venous blood in the body enters
RIGHT ATRIUM
RIGHT VENTRICLE
PULMONARY ARTERY
PULMONARY CAPILLARIES –OXYGENATION OCCURS
PULMONARY VEIN
LEFT ATRIUM
LEFT VENTRICLE
SYSTEMIC CIRCULATION
The separate and much smaller bronchial arteries come from
systemic arteries. They form capillaries, which drain into bronchial vein or
anastomose with pulmonary capillaries or veins. The bronchial veins drain
into the azygos vein. The bronchial circulation nourishes the bronchi and
pleura.
LYMPHATIC SYSTEM
Lymphatic channels are more abundant in the lungs than in any other
organ.
Lymphatics of the lung is divided in to two plexus
SUPERFICIAL PLEXUS DEEP PLEXUS
Superficial plexus is present in the visceral pleura
Deep plexus is located in peri broncho vascular connective
tissues
Alveolar wall devoid of lymphatics
Lymph is flow towards hilum from there it drains in to the
extrapulmonary lymph nodes.
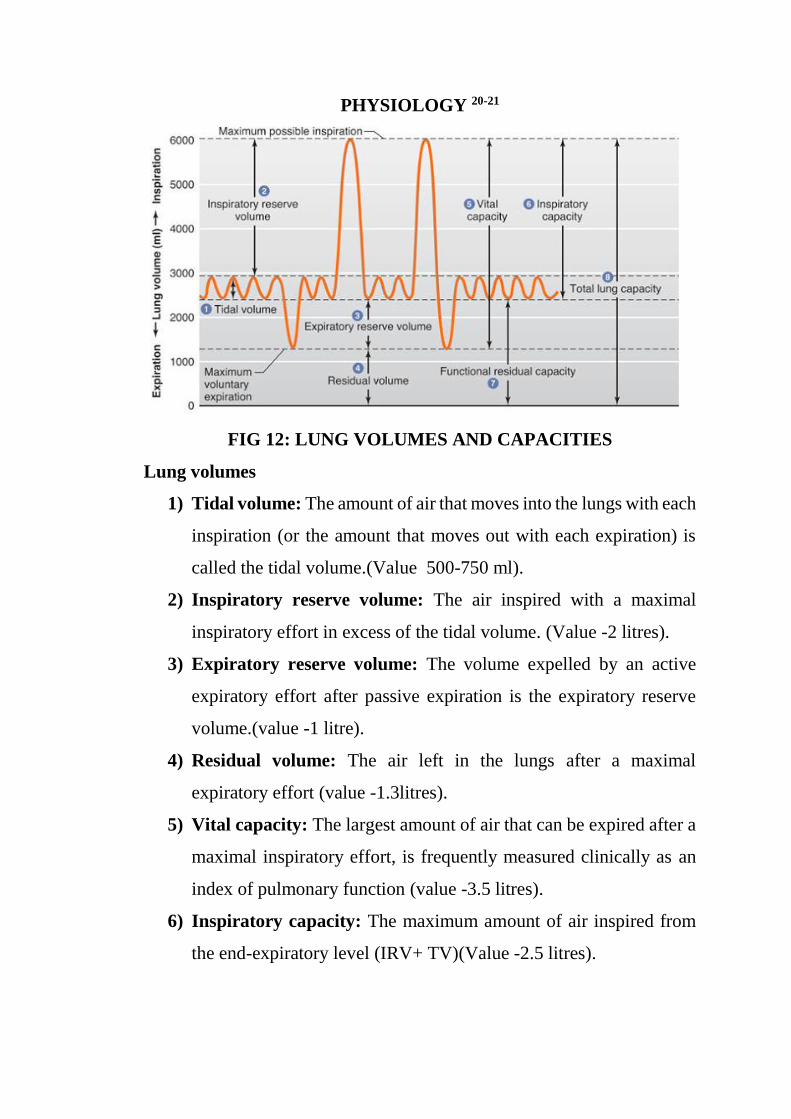
PHYSIOLOGY 20-21
FIG 12: LUNG VOLUMES AND CAPACITIES
Lung volumes
1) Tidal volume: The amount of air that moves into the lungs with each
inspiration (or the amount that moves out with each expiration) is
called the tidal volume.(Value 500-750 ml).
2) Inspiratory reserve volume: The air inspired with a maximal
inspiratory effort in excess of the tidal volume. (Value -2 litres).
3) Expiratory reserve volume: The volume expelled by an active
expiratory effort after passive expiration is the expiratory reserve
volume.(value -1 litre).
4) Residual volume: The air left in the lungs after a maximal
expiratory effort (value -1.3litres).
5) Vital capacity: The largest amount of air that can be expired after a
maximal inspiratory effort, is frequently measured clinically as an
index of pulmonary function (value -3.5 litres).
6) Inspiratory capacity: The maximum amount of air inspired from
the end-expiratory level (IRV+ TV)(Value -2.5 litres).
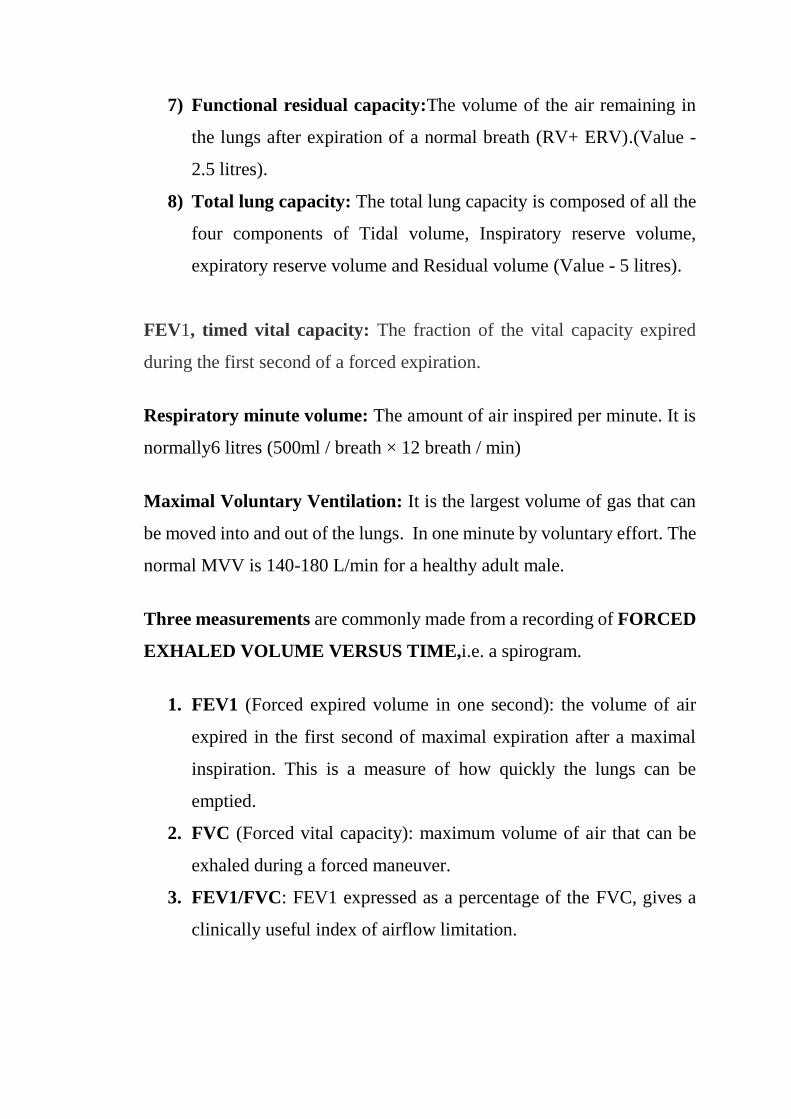
7) Functional residual capacity:The volume of the air remaining in
the lungs after expiration of a normal breath (RV+ ERV).(Value -
2.5 litres).
8) Total lung capacity: The total lung capacity is composed of all the
four components of Tidal volume, Inspiratory reserve volume,
expiratory reserve volume and Residual volume (Value - 5 litres).
FEV1, timed vital capacity: The fraction of the vital capacity expired
during the first second of a forced expiration.
Respiratory minute volume: The amount of air inspired per minute. It is
normally6 litres (500ml / breath × 12 breath / min)
Maximal Voluntary Ventilation: It is the largest volume of gas that can
be moved into and out of the lungs. In one minute by voluntary effort. The
normal MVV is 140-180 L/min for a healthy adult male.
Three measurements are commonly made from a recording of FORCED
EXHALED VOLUME VERSUS TIME,i.e. a spirogram.
1. FEV1 (Forced expired volume in one second): the volume of air
expired in the first second of maximal expiration after a maximal
inspiration. This is a measure of how quickly the lungs can be
emptied.
2. FVC (Forced vital capacity): maximum volume of air that can be
exhaled during a forced maneuver.
3. FEV1/FVC: FEV1 expressed as a percentage of the FVC, gives a
clinically useful index of airflow limitation.

CHRONIC OBSTRUCTIVE PULMONARY DISEASE
DEFINITION22
Chronic obstructive pulmonary disease (COPD) by definition goes
as abnormalities in expiratory flow tests that do not alter significantly over
several months of observation and this helps to distinguish COPD from
asthma.
Two disorders are mentioned in COPD:
EMPHYSEMA
CHRONIC BRONCHITIS
American Thoracic Society (ATS) defines COPD as23
“A disease state characterized by the presence of airflow limitation due
to chronic bronchitis are emphysema; the airflow obstruction is generally
progressive, may be accompanied by airway hyperreactivity that may be
partially reversible”.
The Global initiative for Chronic Obstruction Lung Disease
(GOLD) classified COPD as “A disease state characterized by airflow
limitation that is not fully reversible. The airflow limitation is usually both
progressive and associated with an abnormal inflammatory response of the
lungs to noxious particles or gases”.
The components of COPD are Chronic bronchitis and
Emphysema24.

Chronic bronchitis is defined as “the presence of a chronic productive
cough on most days for three months, in each of two consecutive years”.
Emphysemais defined as “abnormal, permanent enlargement of the distal
air spaces, distal to the terminal bronchioles, accompanied by destruction
of their walls and without obvious fibrosis”.
Cigarette smoking is the highest risk factor for COPD. The studies have
shown a strong relationship between smoking and COPD, in many a high
proportion of nonsmokers also develop COPD. There is an inverse
relationship between cigarette consumption and expiratory flow rate. The
cessation of smoking slows down the speed of pulmonary function
deteriorations to that of nonsmokers, but do not normalize the lungs
function.
The passive smoking, in other words, environmental tobacco smoke
(ETS), or second hand smoke, is associated with COPD. Indoor air
pollution due to domestic cooking and heating has been associated with
chronic respiratory symptoms as reported from many developed and
developing countries.
Occupational exposures to dusts alone or to dusts and in association
with fumes and vapors are the risk factors for COPD.
The most important factors were age, daily cigarette consumption,
possible alterations of smoking habits and the observed value of FEV1.
Smoking results in an over production of proteases (i.e. elastase).
Further, it inactivates the anti-elastases. Thus there is an imbalance
between the protease-antiprotease with resultant excess action of protease,
which leads on to the destruction.
EPIDEMIOLOGY25-28
PREVALENCE: Most data available on COPD statistics are from
developed countries, acquiring accurate epidemiological data on COPD is
very tough and costs much.
A meta-analysis in performed between 1990 and 2004 in 28
countries showed the prevalence was 11% in men and 5% in women and
3.9% in never smokers and 15.2% in smokers.
Halbert et al. reviewed 32 prevalence studies from 17 different countries
and concluded that prevalence of COPD ranged between 4 to 10%.
COPD IN INDIA29-31
The inference of the INDIAN STUDY INSEARCH phase II was
released and this studies show that the prevalence of COPD in India was
3.7% (4.5% males and 2.9% females).
Wig (1964) et al. showed prevalence of COPD to be 3.36% and
2.54% in men and women with 2:1 smoker non smoker ratio in rural Delhi.
Viswanathan (1966) et al. showed prevalence of 2.12% and 1.33%
in men and women respectively in a study in Patna.
In a pilot study in rural area of Mysore, prevalence of COPD was
7.1%, 11.1% in males and 4.5% in females.
Jindal (1993) et al. in a study in rural population of North India
showed Prevalence of 6.2% and 3.9% in males and females respectively.
In urban population of North India showed prevalence of 4.2% and 1.6%
in males and females respectively with smoker to nonsmoker ratio of 9.6.32
Ray (1995) et al. in a study in South India showed prevalence of
4.08% and 2.55% in males and females respectively with smoker to
nonsmoker ratio of 1.6.
Malik et al. (1986) in a study in rural population of North India
showed Prevalence of 9.4% and 4.9% in males and females respectively
with smoker to non smoker ratio of 5.5. In urban population of North India
showed prevalence of 3.7% and 1.6% in males and females respectively
with smoker to non smoker ratio of 3.7.
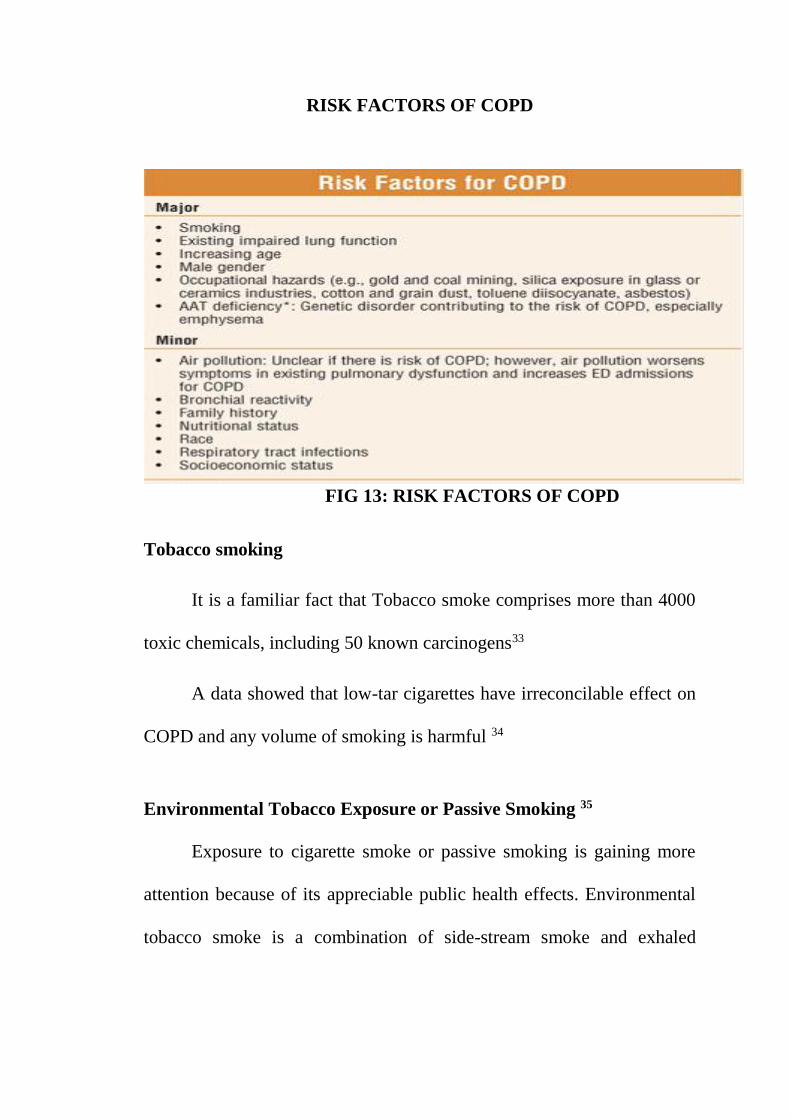
RISK FACTORS OF COPD
FIG 13: RISK FACTORS OF COPD
Tobacco smoking
It is a familiar fact that Tobacco smoke comprises more than 4000
toxic chemicals, including 50 known carcinogens33
A data showed that low-tar cigarettes have irreconcilable effect on
COPD and any volume of smoking is harmful 34
Environmental Tobacco Exposure or Passive Smoking 35
Exposure to cigarette smoke or passive smoking is gaining more
attention because of its appreciable public health effects. Environmental
tobacco smoke is a combination of side-stream smoke and exhaled
mainstream smoke. Owing to a lower temperature of combustion, side
stream smoke contains larger concentrations of
Ammonia,
Benzene,
Carbon-monoxide,
Nicotine,
and various carcinogens(2-naphthylamine, 4-aminobiphenyl,
n-nitrosamine, benza-anthracene, and benzopyrene) than the
mainstream smoke.
In enclosed spaces, smoke accumulates, and the concentration varies
with the number of smokers, with the type of smoking, and with the
characteristics of the room, especially the ventilation.
Gupta D et al. in a Multicentric Population Study from India
concluded that Passive smoking is associated with increased prevalence of
respiratory symptoms.
OCCUPATIONAL EXPOSURE 36
Epidemiological data by the Matheson et al. in their study of 1232
people concluded that occupational exposure to biological dust was
associated with elevated risk of COPD which was higher in women.
Bushra Iftikhar and his colleagues in Peshawar studied relationship
between silica exposure and COPD and concluded that people exposed to
silica dust for more than 10 years, and daily exposure of >8 hours had more
risk of developing COPD.
BIOMASS FUEL EXPOSURE 37-38
The combustion of biomass fuel releases several toxic gases and
causing respiratory problems.
Mrigendra Raj Pandey in his study in Nepal showed increased
prevalence in females exposed to biomass fuel exposure and the severity
of symptoms correlated with duration of exposure to smoke.
Orozco-Levi M et al in a case control study of 120 females in
Barcelona, Spain showed increased risk of COPD in exposure to wood or
charcoal smoke.
ALPHA-1 ANTITRYPSIN DEFICIENCY 39-40
The only known genetic cause of emphysema is Alpha-1 antitrypsin
(AAT) deficiency. An inherited deficiency of a protein in the blood called
the α1-antitrypsin (AAT). It is the only known genetic disorder that leads
to COPD. AAT deficiency accounts for less than 1 percent of COPD in
USA. This deficiency is an autosomal hereditary disorder in which there
are low levels of α1-antitrypsin in serum and lungs, with a high risk of
development of panlobular emphysema in the third to fifth decade. There
is an increased risk of development of liver disease in the childhood
associated with this condition.
AAT is a glycoprotein coded for by a single gene on chromosome
14. It is a serine protease inhibitor with primary function of inhibiting
neutrophil elastase. Emphysema results from an imbalance between the
neutrophil elastase in the lung and the anit-elastases.
This concept is known as the “elastase-antielastase balance
hypothesis of Emphysema.”
Many Indian studies have tried to examine the role of alpha-
1antitrypsin deficiency in the causation of COPD and is summarized by
Malik et al.The heterozygote state (intermediate) was found to be 10.3 to
23.3 percent and homozygous (severe) state in 2.8 to 20 percent of cases
of COPD.
Αlfa 1-Antitrypsin Deficiency Screening
In patients of Caucasian descent who develop COPD at a young age
(< 45 yr) or who have a strong family history of the disease, it may be
valuable to identify coexisting α1-antitrypsin deficiency. This could lead to
family screening or appropriate counseling.
Young patients with severe hereditary α1-antitrypsin with severe
hereditary α1-antitryspin augmentation therapy. However, this therapy is
very expensive, not available in most countries, and not recommended for
patients with COPD that is unrelated to α1-antitrypsin deficiency.
THE OVERLAP OF COPD AND ASTHMA
Active asthma patient have TEN fold risk of Chronic bronchitis
and SEVENTEEN fold risk of Emphysema.
FIG 14a : THE OVERLAP OF COPD AND ASTHMA
FIG 14b : THE OVERLAP OF COPD AND ASTHMA
Respiratory Infections: Childhood respiratory infections have been
assessed as potential predisposing factor for the eventual development of
COPD.
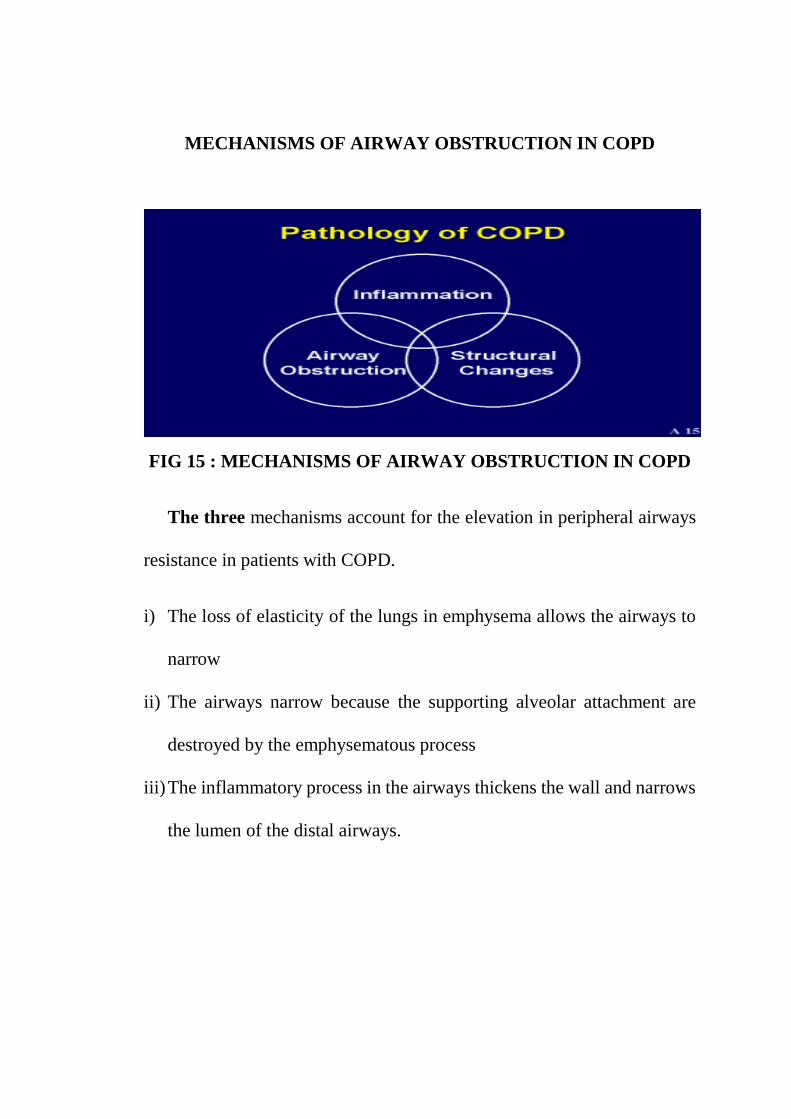
MECHANISMS OF AIRWAY OBSTRUCTION IN COPD
FIG 15 : MECHANISMS OF AIRWAY OBSTRUCTION IN COPD
The three mechanisms account for the elevation in peripheral airways
resistance in patients with COPD.
i) The loss of elasticity of the lungs in emphysema allows the airways to
narrow
ii) The airways narrow because the supporting alveolar attachment are
destroyed by the emphysematous process
iii) The inflammatory process in the airways thickens the wall and narrows
the lumen of the distal airways.
PATHOLOGY 41-43
Several of the abnormalities in chronic bronchitis and emphysema
occur in large bronchi (airways with cartilages in their walls and more than
2 mm in diameter), bronchioles (no cartilages in their walls and less than 2
mm internal diameter), and parenchyma. Since emphysema and chronic
bronchitis are invariably associated in the same patient, it is common to
find changes in all the above three components, although one or the other
change may predominate.
The important change in the large bronchi is the hypertrophy of the
mucus secreting glands in the sub epithelial layer that are enlarged and are
thought to secrete most of the mucus found in the airways. The hypertrophy
can be measured as the thickness of the gland layer in histological sections
and comparing it to that of the bronchial wall and is expressed as Reid
index. The mucous gland hypertrophy is largely seen in the larger bronchi
and is equally present throughout the lungs. The mucus secreting goblet
cells are also elevated in number in the large as well as in the bronchioli.
Bronchial muscle hyperplasia is present in patient with COPD.
The increasing amount of muscle may be responsible for the airway
hyper reactivity seen in this patient. Emphysema are classified as,
(a) Centriacinar Emphysema affects the respiratory brochioles . This is
probably secondary to bronchiolitis. It is commoner at the lung apices.
(b) Panacinar (or) Panlobular Emphysema. All components of the acinus
are involved about equally. usually related with ∝1 antiprotease
deficiency. It can also occur in bases of the lung.
(c) Distal Acinar Emphysema (or) Paraseptal emphysema predominantly
involvs the alveolar ducts and sacs.
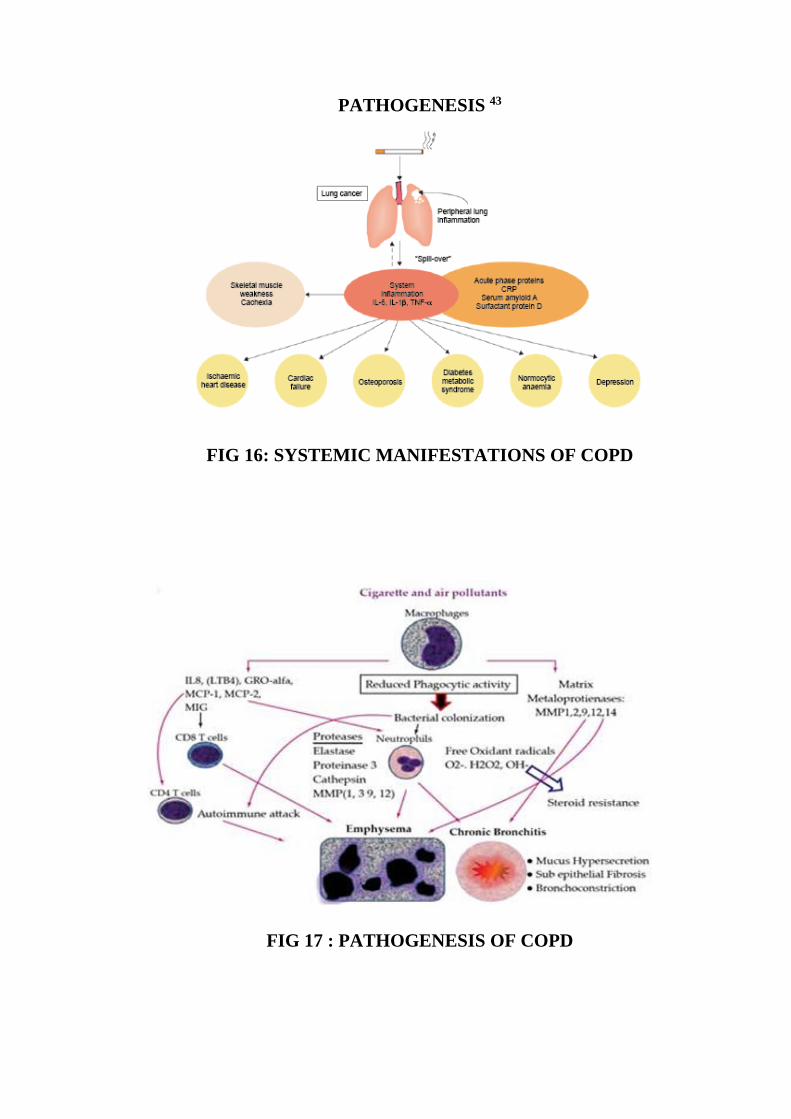
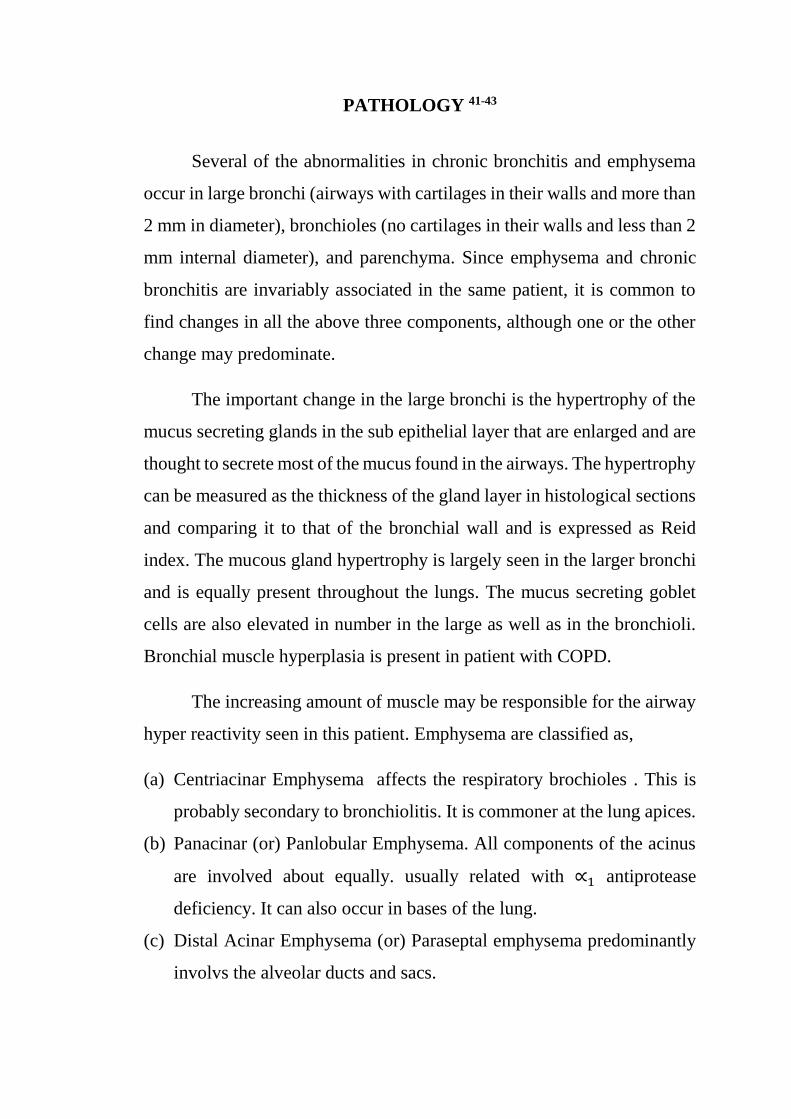
PATHOGENESIS 43
FIG 16: SYSTEMIC MANIFESTATIONS OF COPD
FIG 17 : PATHOGENESIS OF COPD
Inflammatory markers-Cytokines in COPD
Interleukin-6
TNFα
IL-1β
Chemokines- CXCL8 (IL-8) are released during the course of
illness and during acute exacerbations of COPD patients and these
cytokines are responsible for systemic inflammation and leads to
weight loss,cardiac failure ,normocytic anaemia etc.
CLINICAL FEATURES OF COPD 44-49
The usual presentation is at the fifth decade of life. The characteristic
symptoms of chronic bronchitis are cough with expectoration, wheeze, and
breathlessness. The cough and expectoration are usually exacerbated from
time to time particularly more during the winter.
Pure emphysema is mainly manifested as breathlessness and
wheezing, cough and expectoration are less important symptoms. The
patient gives a history of progressive dyspnea, sometimes starting
apparently after a mild infection and following exertion or exercise.
Airflow obstruction causes dyspnea and by the time this present, the FEV
is about 1 liter or less than 50 percent of the predicted value. The course
progresses over the next 5 year or more with further loss of FEV. The

patient will try to breathe with pursed lips to utilize the respiratory muscles
maximum.
Corpulmonale is more common in chronic bronchitis, this is less
common in emphysema except terminally. Respiratory failure is the
common mode of death of emphysema patients. The emphysema patient
maintains a near normal 𝑷𝒂𝑶𝟐 and normal 𝑷𝒂𝑪𝑶𝟐 by hyperventilation
until a late stage of the disease.
FIG 18: CAUSES OF EXACERBATION OF COPD
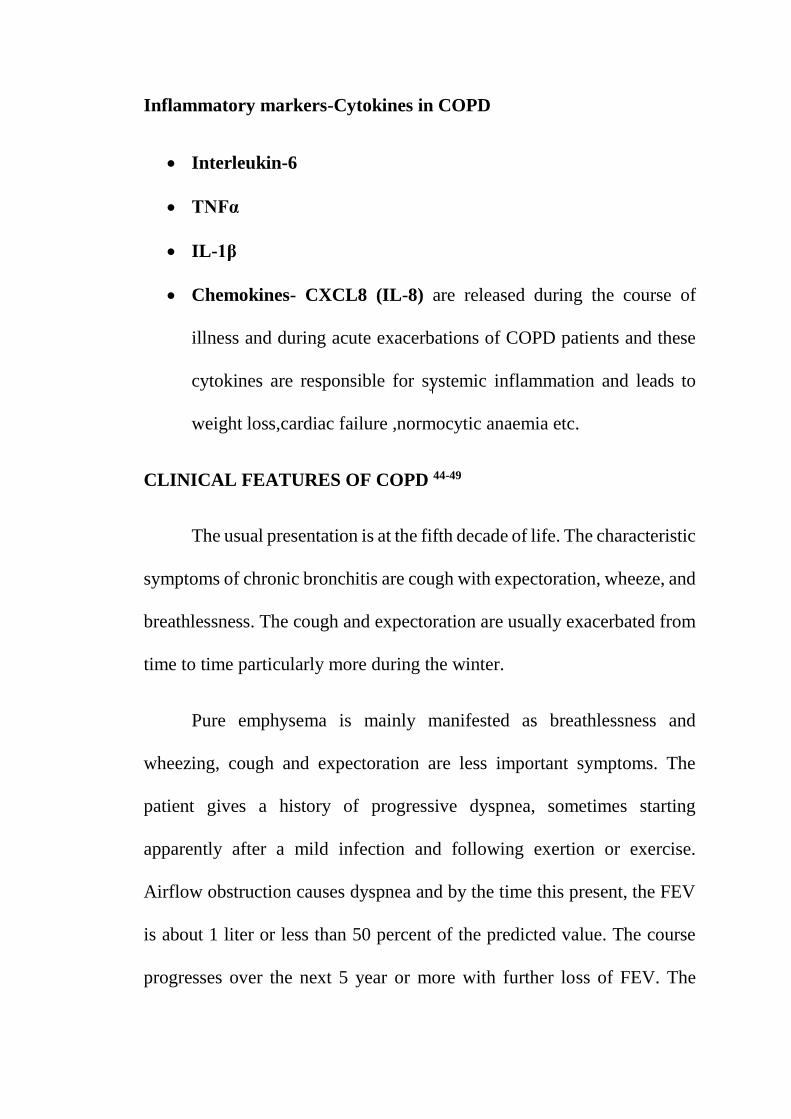
m MRC GRADING DYSPNOEA 50
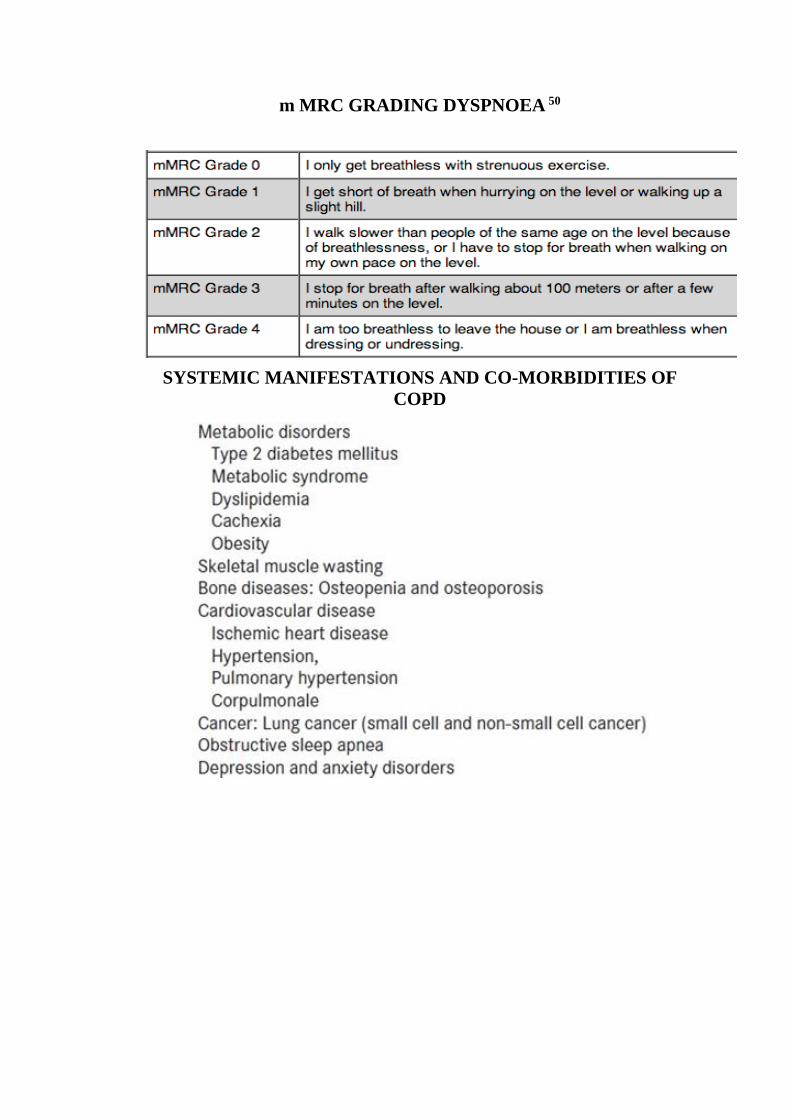
SYSTEMIC MANIFESTATIONS AND CO-MORBIDITIES OF
COPD
PHYSICAL SIGN 44-49
In early stage of the disease there may not be any findings on
examination. In later stages, there will be emaciation, cyanosis, anaemia,
edema, and raised jugular venous pressure, if there is associated
corpulmoale and heart failure.
The chest is barrel shaped with kyphosis, elevated anteroposterior
diameter, ribs being set more horizontal and these changes are permanent
and one may feel an inspiratory tracheal tug due to the contraction of low,
flat diaphragm. The movement of the chest wall is reduced with limited
expansion. The patient may use his accessory muscles of respiration.
JVP may be seen during expiration. In the more severe cases, the
costal margins will be drawn inwards on inspiration, paradoxically, due to
the pull of the low, flattened diaphragms. On percussion reveal
hyperresonant due to hyperinflation of lungs. On auscultation there is a
prolonged expiratory phase, wheeze and crepitations are heared.
Airflow obstruction is detected by placing the chest piece of the
stethoscope over the trachea and timing of a forced expiration. Normally it
is possible to empty the lungs in 4-5 seconds, but a patient with airflow
obstruction shows a prolonged expiratory time. Patients with end stage
COPD may adopt positions that relieve dyspnoea, by leaning forward with
neck extended called asTripod sign. The accessory respiratory muscle
helps in to keep the airway patent. Expiration often takes place through
pursed lips. Paradoxical in drawing of the lower intercostals space is often
evident (Hoover's sign), cyanosis may be present; clubbing is not
associated with COPD. If it present one should rule out bronchiectasis or
lung carcinoma. An enlarged, tender liver indicates heart failure due to
elevated intrathoracic pressure. Asterexis may be seen with severe
hypercapnia.
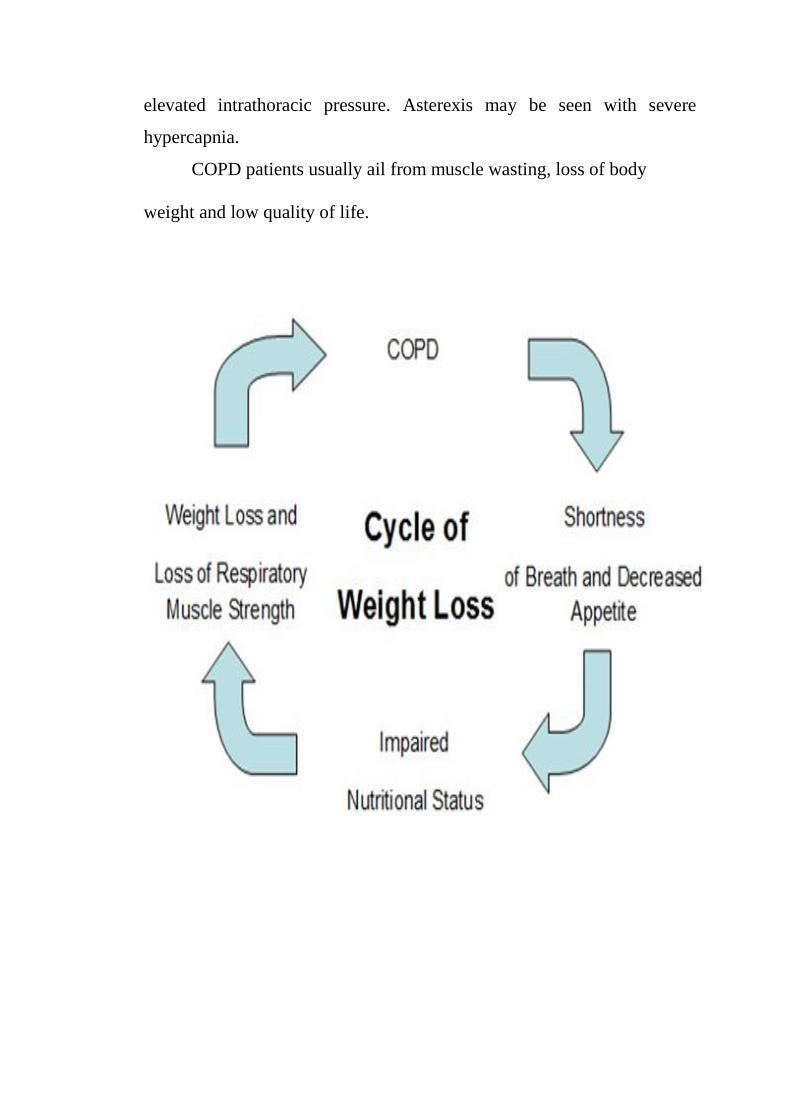
COPD patients usually ail from muscle wasting, loss of body
weight and low quality of life.

PULMONARY FUNCTION TESTING.51-52
Pulmonary function evaluation not only establishes the diagnosis of COPD
but also assesses the progression and severity of COPD.
FIG 19: SPIROMETRY
Spirometry is performed in the following individuals
Unexplained dyspnea or suspicion of COPD
Screening of habitual smokers for early detection
Repeat spirometry after medications to detect the
reversibility.
Guidelines for rational therapy

FIG 20: CLASSIFICATION OF SEVERITY OF COPD
FIG: 21 DYNAMIC FLOW –VOLUME LOOPS
PROGNOSIS 53-54
Long term prospective studies in patients with severe COPD with
FEV of less than 1 liter have shows
5 yr survival rates - 69 %
10 yr survival rates - 40%
The presence of radiological evidence of emphysema or of bullae
in one study resulted in five-year mortalities of 53 percent and 70
percent respectively. Right ventricular failure carries a poor
prognosis with a five mortality of 60 to 80 percent reported in
different studies. Right ventricular systolic pressure of > 35 mm H,
FEV of < 30 percent of predicted and age > 70 years is other poor
prognostic factors.
Three risk factors have been useful in predicting the outcome of a
patient with COPD age, smoking status, and FEV. The studies of prognosis
in the National Institutes of Health Intermittent Positive Pressure Trial
confirmed the findings of earlier studies that age and initial FEV are
powerful predictors of outcome. The only consistent predictor of decline
in FEV besides the initial FEV is the bronchodilator response of the patient.
The larger the response the slower the decline in FEV and this relation is
not dependent on the initial FEV.
In persons with FEV < 0.75 L, mortality rate at
1 yr - 30 %
10 yr - 95%
However, some patients with severe airflow obstruction may survive
longer, and even up to 15 years. Some other data suggest that next to
cessation of smoking, a higher degree of reversibility of airflow obstruction
and a lower degree of airway reactivity are the two most important
predictors of a slower decline in FEV.
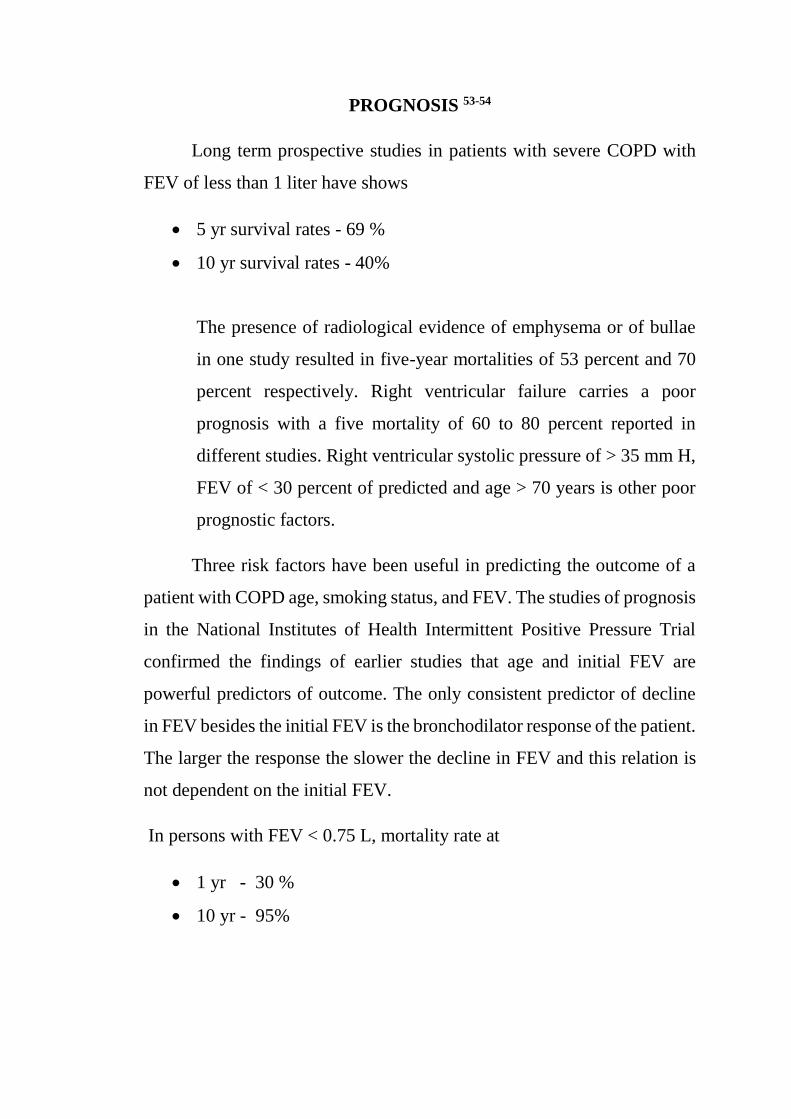
BODE INDEX FOR STAGING COPD 55
FIG 22: BODE INDEX FOR STAGING COPD
BODE INDEX PREDICTS
PROGNOSIS
DEATH AND HOSPITALIZATION BETTER THAN FEV1
ALONE
INVESTIGATIONS
Sputum Examination 56-58
Sputum Examination is done to all patients with cough of > two wks
as per RNTCP Guidelines because Smoking not only increases the risk of
COPD and tuberculosis (TB).
Pulse Oximetry 59-60
Pulse oximetry is to asses hypoxaemia during acute exacerbation of
COPD and in respiratory failure cases.
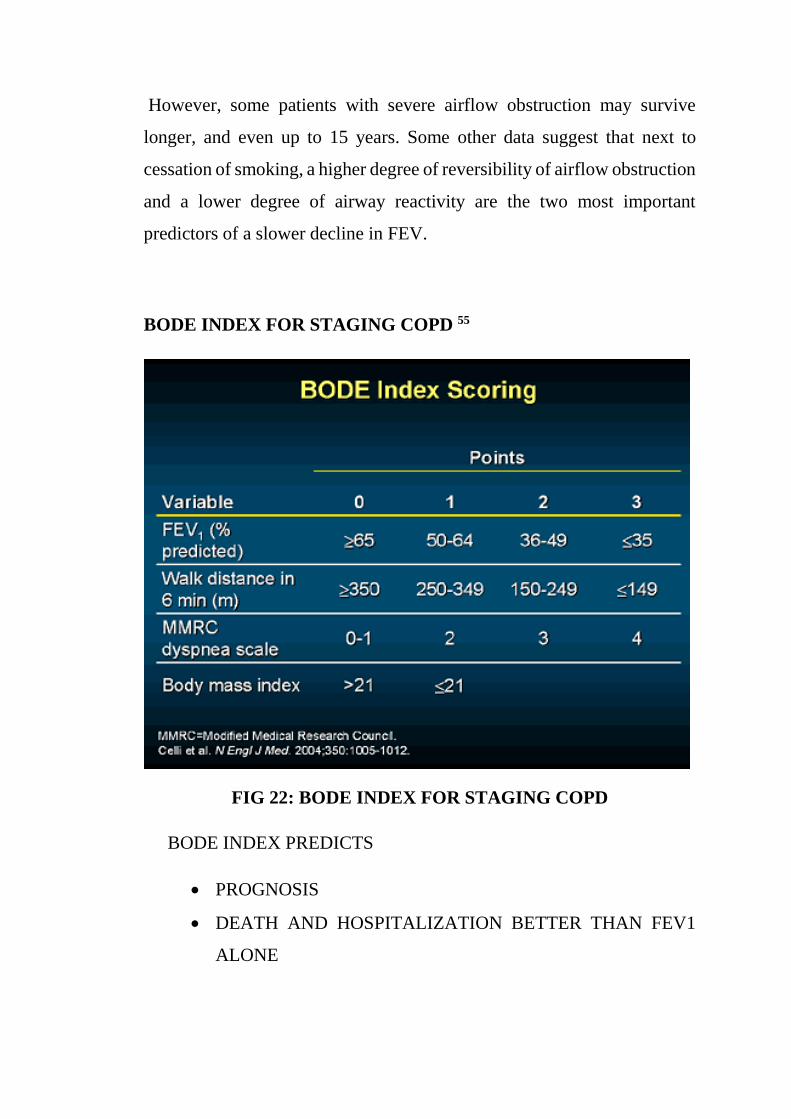
Chest X-Ray61-62
A plain Chest X-Ray in both posteroanterior and lateral view to be done.
FIG 23: CHEST X-RAY OF COPD
Five radiologic criteria have been described to diagnose
emphysema.
(i) A retrosternal space (greatest distance from the sternum to the
anterior heart silhouette) more than 2.54 cm(lateral radiograph)
(ii) Regular or irregular hyper-lucency of lung fields reflecting
attenuated pulmonary vessels
(iii) Low (mid diaphragm below tenth posterior intercostals space)
and flat diaphragm (for two thirds of their length) on lateral films
(iv) Low (mid diaphragm below tenth posterior intercostal space)
and flat (for two thirds of their length) on PA radiograph
(v) Bullae one or more clear walled lesions not considered to be a
cavity.
Radiologic emphysema is considered to be present when two criteria
are present.
CT CHEST 63-64
Even in normal study of chest xray, CT Scan identifys emphysema.
Computerized tomography is usually not necessary routinely in patients
with uncomplicated emphysema.
Early emphysema is identified and quantified by HRCT.
Detailed cardiopulmonary exercise testing (CPET) is helpful in
assessing65-66
Prognosis
Functional status for exercise restrictions
Impact of therapeutic interventions
6-minute walk test (6MWT) is the surrogate for CPET
Alpha -1 Antitrypsin Deficiency39
Western data shows that 3% of COPD patients have AAT
deficiency and there is no such data available in our country.
TREATMENT GOALS IN A PATIENT WITH STABLE CHRONIC
OBSTRUCTIVE PULMONARY DISEASE
NON-PHARMACOLOGICAL MANAGEMENT OF COPD 67
SMOKING CESSATION
PULMONARY REHABILITATION
OXYGEN THERAPY
NON-INVASIVE VENTILATION
SURGERY
SMOKING CESSATION 68-73
The most important method to prevent COPD and reduces the frequency
of exacerbations.
A variety of pharmacotherapies are available to quit smoking.
Nicotine replacement therapy:
Available in the form of
Chewing gums
Tablets
Patches
Nasal sprays
Lozenges
Inhalers
FIG 24 : NICOTINE PATCH FIG 25: NICOTINE INHALER
Bupropion:
It is the nicotine receptor antagonist; a weak norepinephrine -
dopamine reuptake inhibitor in the brain.
Carenicline:
Acts by partial agonist of the nicotinic receptor as well as
simultaneously blocks it.
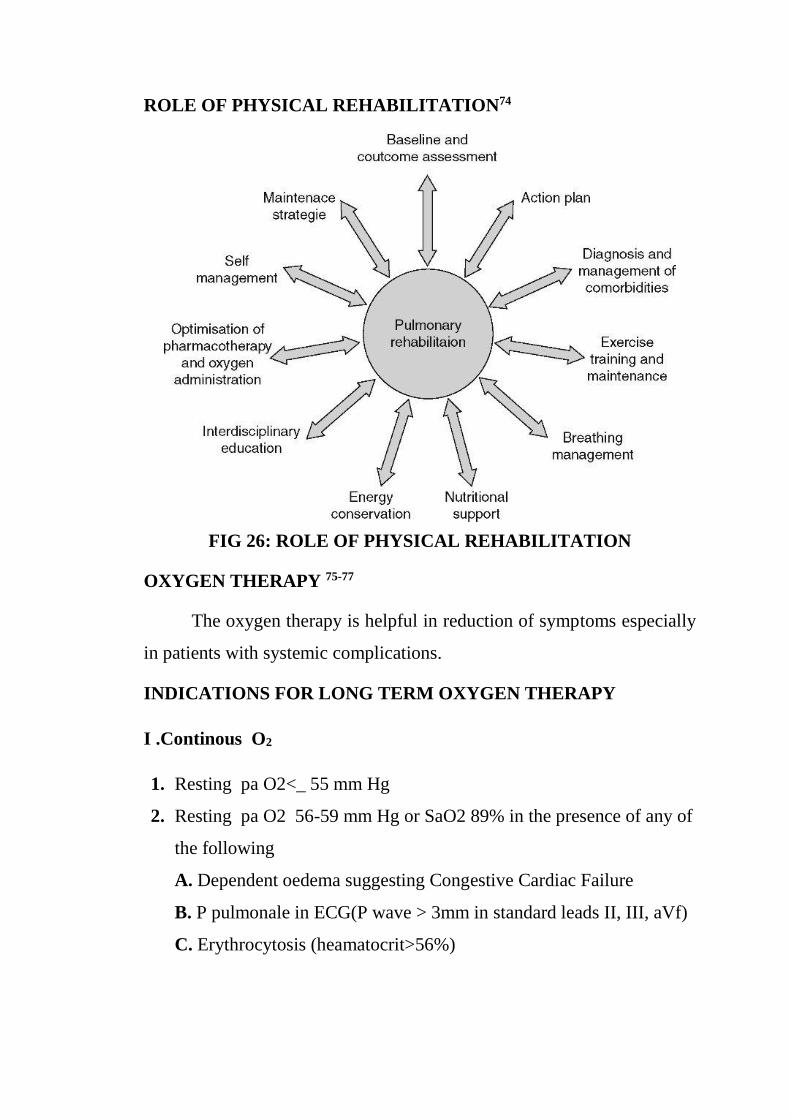
ROLE OF PHYSICAL REHABILITATION74
FIG 26: ROLE OF PHYSICAL REHABILITATION
OXYGEN THERAPY 75-77
The oxygen therapy is helpful in reduction of symptoms especially
in patients with systemic complications.
INDICATIONS FOR LONG TERM OXYGEN THERAPY
I .Continous O2
1. Resting pa O2<_ 55 mm Hg
2. Resting pa O2 56-59 mm Hg or SaO2 89% in the presence of any of
the following
A. Dependent oedema suggesting Congestive Cardiac Failure
B. P pulmonale in ECG(P wave > 3mm in standard leads II, III, aVf)
C. Erythrocytosis (heamatocrit>56%)
(a) Reimbursable only with additional documentation justifying O2
prescription and a summary of more conservative therapy that has
failed.
II. Non - Continous O2
1. O2 flow rate and number of hours per day must be specified.
2. During exercise Pa O2<55mmHg or Sa O2 <88% with associated
complications, such as pulmonary hypertension, daytime somnolence
or cardiac arrhythmias.
NON-INVASIVE VENTILATION 78-81
NIV is well established in the treatment of Acute Exacerbation of
COPD patients, and its controversial in stable COPD.
Benefits of NIV are
Maximum inspiratory pressure
Gas exchange
The indications for NIV in stable COPD are
1. Diagnosed case of COPD, optimization of other therapies and
exclusion of sleep apnoea if required.
2. Presence of both symptoms like fatigue, dysponea, morning
headache, etc.), and physiologic criteria (one of the following):
(a) PaCO2≥55 mmHg or PaCO2 of 50-54 mmHg and nocturnal
desaturation (oxygen saturation by pulse oximeter≤88% for five
continuous minutes while receiving oxygen therapy at 2L/min);
and
(b) PaCO2 of 50-54 mmHg and hospitalization related to recurrent
(≥2 in a 12-month period) episode of hypercapnic respiratory
failure.
ROLE OF VACCINATIONS81-82
Two vaccines are recommended
Influenza vaccine
Pneumococcal vaccine
These two vaccines are much beneficial in stage 3 and stage 4 COPD
Patients or Patients with recurrent exacerbations.
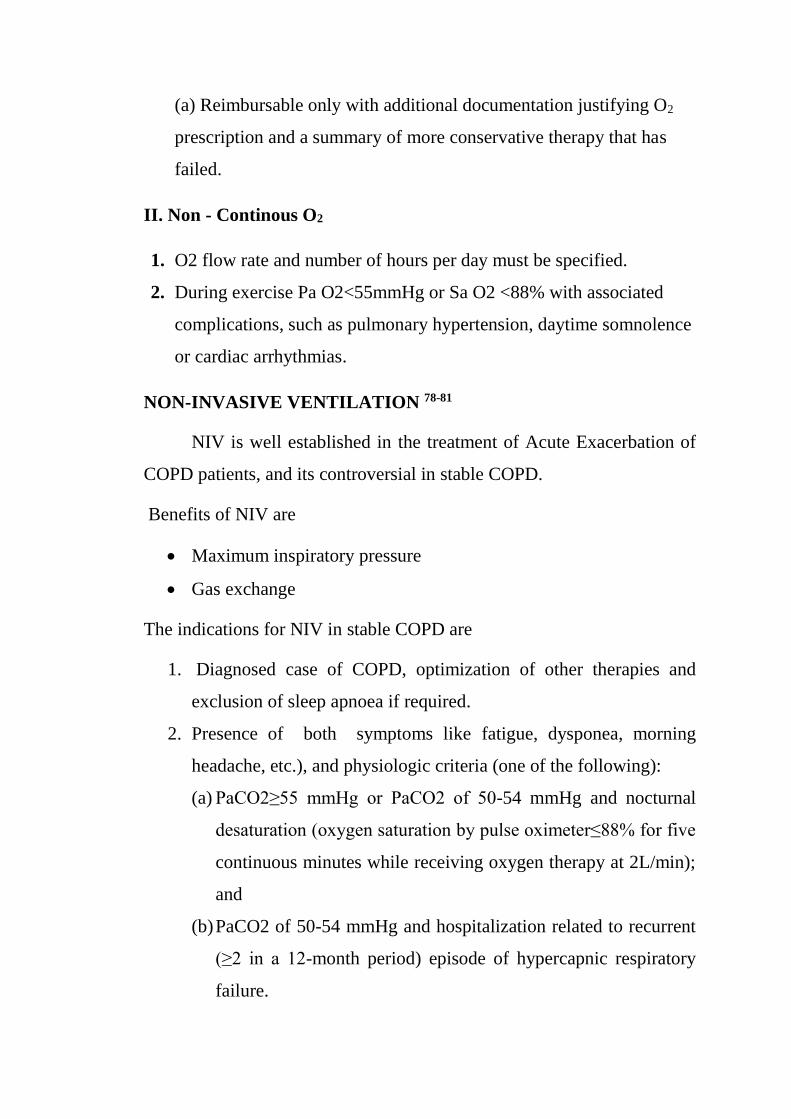
PHARMACOLOGICAL MANAGEMENT OF COPD 83
FIG 27: GOLD THERAPY AT EACH STAGE OF COPD
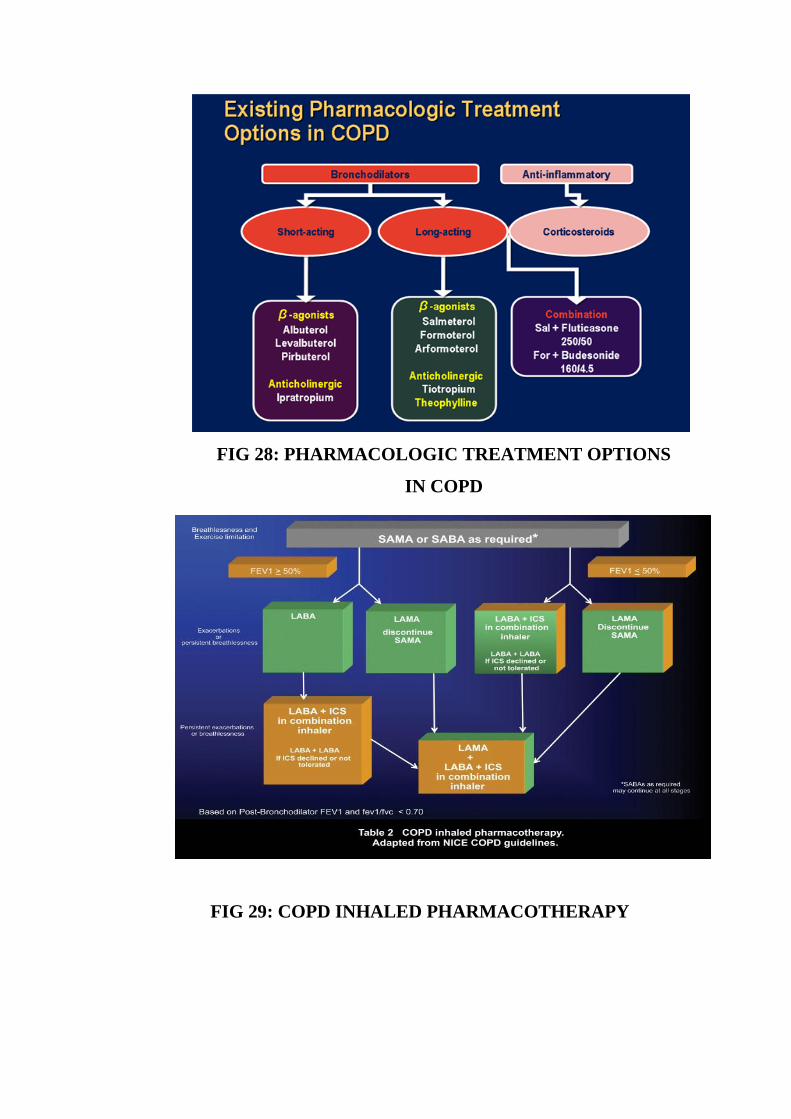
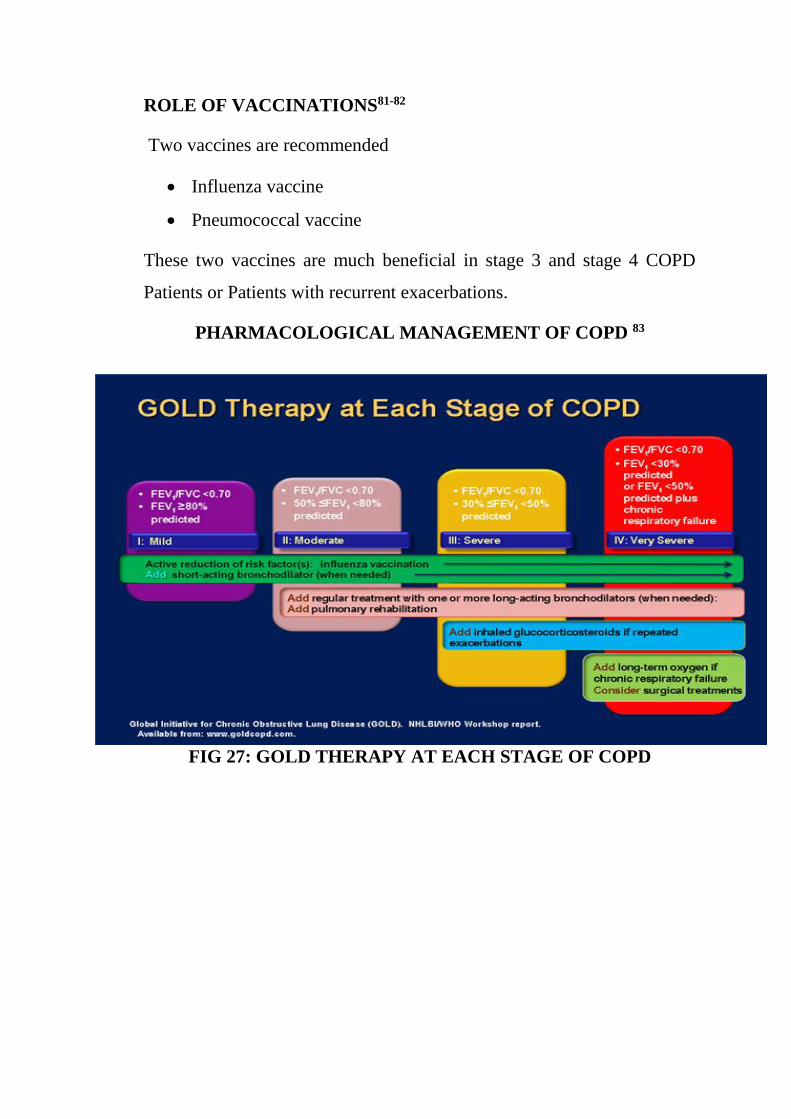
FIG 28: PHARMACOLOGIC TREATMENT OPTIONS
IN COPD
FIG 29: COPD INHALED PHARMACOTHERAPY

INDIAN STRATEGY FOR THE MANAGEMENT OF COPD
SUGGESTED TREATMENT GUIDELINES FOR PATIENTS
WITH STABLE COPD
Indications for hospital assessment or admission for exacerbations of
COPD
Marked increase in intensity of symptoms, such as sudden
development of resting dyspnea, change in vital signs
Severe underlying COPD
Onset of new physical signs (e.g. cyanosis, peripheral edema)
Failure of exacerbation to respond to intial medical management
Significant comorbidities
Frequent exacerbations

Newly occurring arrhythmias
Diagnostic uncertainty
Older age
Insufficient home support
Indications for intensive care unit admission of patients with
exacerbations of COPD
Severe dyspnea that responds inadequately to initial emergency
therapy
Changes in mental status (confusion, lethargy, coma)
Persistent or worsening hypoxemia (Pao2 <5.3 kPa, 40mm Hg),
and/or severe/worsening hypercapnia (Paco2 >8.0 kPa, 60mm Hg,
and/or severe/worsening respiratory acidosis (pH < 7.25) despite
supplemental oxygen and noninvasive ventilation.
Need for invasive mechanical ventilation
Hemodynamic instability-need for vasopressors
Local resources need to be considered.
Management of severe but not life-threatening exacerbations of COPD
in the emergency department or the hospital
Assess severity of symptoms, blood gases, chest X-ray
Administer controlled oxygen therapy and repeat arterial blood gas
measurement after 30-60 min
Bronchodilators:
- Increase doses and/or frequency
- Combine2-agonists and anticholinergics
- Use spacers or air-driven nebulizers
- Consider adding intravenous methylxanthines, if needed
Add oral or intravenous glucocorticosteroids
Consider noninvasive mechanical ventilation
At all times:
- Monitor fluid balance and nutrition
- Consider subcutaneous heparin
- Identify and treat associated conditions (e.g., heart failure,
arthythmias)
- Closely monitor condition of the patient.
World COPD Day takes place each year on the second or third
Wednesday in November World COPD Day 2013 theme
“It’s Not Too Late”
This positive message was chosen to emphasize the meaningful actions
people can take to improve their respiratory health, at any stage before
or after a COPD diagnosis
WORLD COPD DAY 2014 LOGO
FIG 30: WORLD COPD DAY-2014 LOGO
MATERIALS AND METHODS
SOURCE OF DATA
All patients who presented with history of cough, sputum,
breathlessness or wheezing of more than 3 months duration to the Medical
Outpatient Department or admitted in the medical wards of Coimbatore
Medical College Hospital were subjected to pre and post-bronchodilator
Pulmonary Function Testing. Those patients whose post-bronchodilator
FEV1/FVC was less than 0.7 were included in this study. This study period
was from AUGUST 2013 to JULY 2014.
COLLABORATING DEPARTMENTS
Department of TB & Chest Medicine, Coimbatore Medical College
Hospital.
Design of Study : Observational Clinical study
Period : AUGUST 2013 to JULY 2014
Sample size : 60 Patients
Ethical Committee Approval : Obtained
Consent : Informed consent was obtained
INCLUSION CRITERIA
Both in-patients and out-patients were included in the study.
Both new and previously diagnosed cases were included in the
study.
Patients with post-bronchodilator FEV1 / FVC < 0.7.
EXCLUSION CRITERIA
Patients with systemic illness like Diabetes, Coronary artery heart
disease, Cardiac failure, renal failure, Liver diseases, Malignancy,
Collagen vascular disease.
Patients with history of present or past pulmonary tuberculosis
Patients with other lung diseases like interstitial lung disease,
Bronchiectasis, Pneumonia, Lung abscess.
Data was collected using a pretested Proforma meeting the
objectives of the study. Detailed history, physical examination and
necessary investigations were undertaken.
Pulmonary Function Testing was done using spirometer. Three
satisfactory efforts were recorded and the best effort was
considered. Bronchodilatation was done using 200 μg of inhaled
salbutamol using a metered dose inhaler and the test was repeated
after 15 min.
Patients were subjected to the following investigations:
Complete Haemogram
Peripheral smear
Blood urea, serum creatinine
Blood sugar
Spirometry (pre and post bronchodilator therapy)
Sputum for gram stain and AFB
Chest X-ray PA view
Urine: Albumin, Sugar
ECG in all leads
RESULTS
Sixty cases were studied and the following observation and analysis were
made.
TABLE 1: SEX DISTRIBUTION
SEX
NUMBER OF
PATIENTS
PERCENT
Male
48 80
Female
12 20
Total
60 100
CHART 1: SEX DISTRIBUTION
Out of the 60 cases studied, 48 Patients (80%) were Males and 12
Patients (20%)were Females.

TABLE 2: AGE DISTRIBUTION
AGE GROUP
NUMBER OF
PATIENTS
PERCENT
31 to 40 yrs 1 2
41 to 50 yrs 28 47
51 to 60 yrs 21 35
61 to 70 yrs 10 17
CHART 2: AGE DISTRIBUTION
Majority of the patients were in the age group of 41-50 years.
Minimum age being 38 years and Maximum age being 68 years.
TABLE 3.DURATION OF ILLNESS
DURATION OF
ILLNESS
NUMBER OF
PATIENTS
PERCENT
0-5 yrs 17 28
6 to 10 yrs 28 47
> 10 yrs 15 25
CHART 3. DURATION OF ILLNESS
Majority of patients, i.e. 28 patients (47 %) had duration of illness
6-10 years, 15 patients (25%) had duration of illness of >10 years
and 17 patients (28%) had duration of illness 0-5 years.
TABLE:4 PLACE OF LIVING
PLACE OF
LIVING
NUMBER OF
PATIENTS
PERCENT
Urban 48 80
Rural 12 20
CHART: 4 PLACE OF LIVING
48 Patients (80%) were living in urban areas whereas 12 Patients (20%)
were living in rural area.
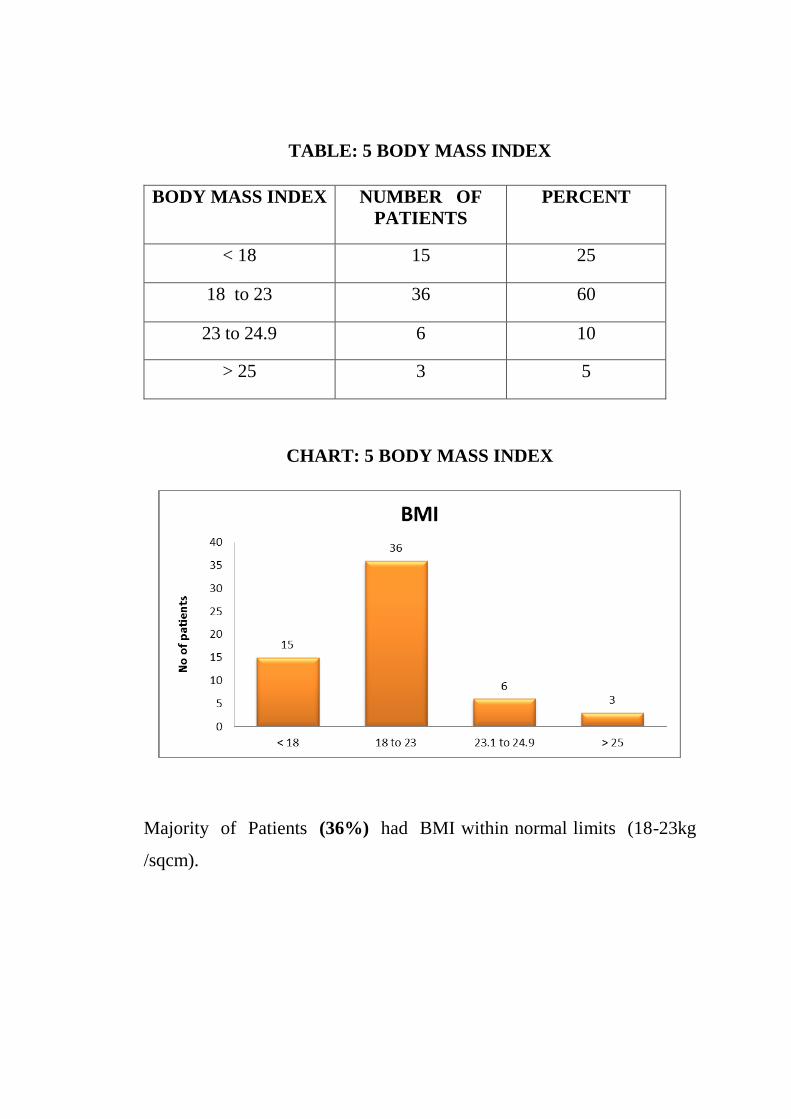
TABLE: 5 BODY MASS INDEX
BODY MASS INDEX
NUMBER OF
PATIENTS
PERCENT
< 18 15 25
18 to 23 36 60
23 to 24.9 6 10
> 25 3 5
CHART: 5 BODY MASS INDEX
Majority of Patients (36%) had BMI within normal limits (18-23kg
/sqcm).
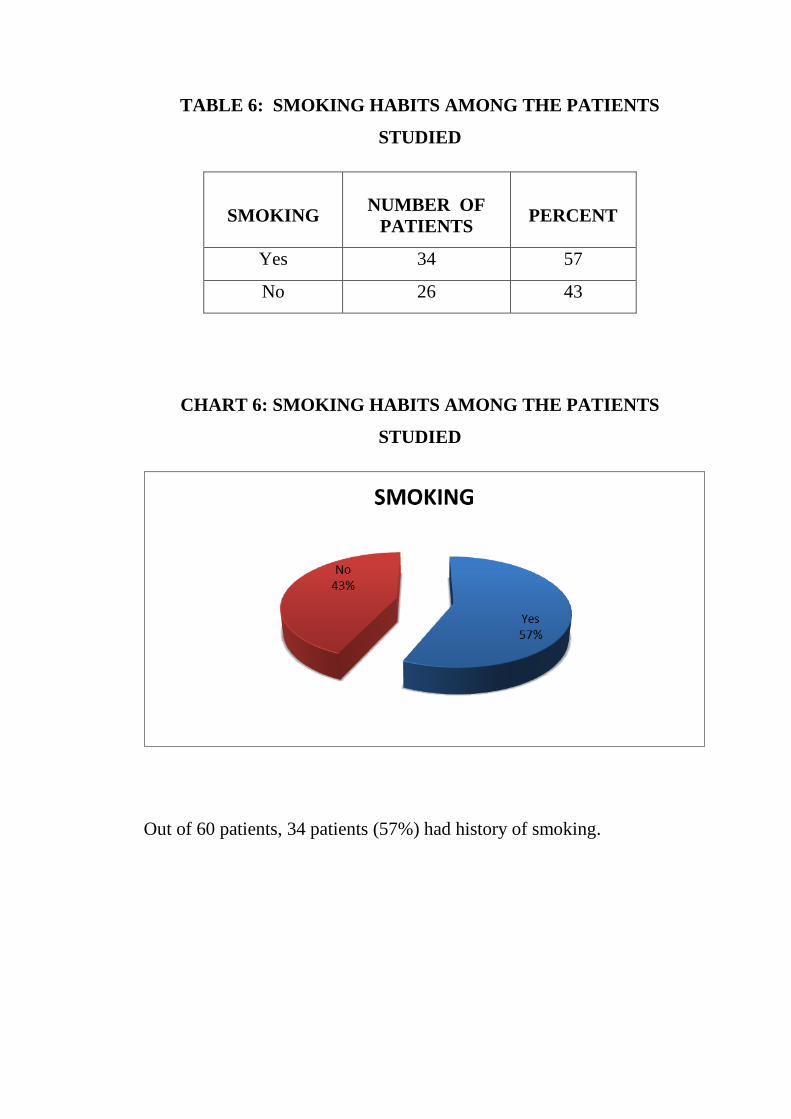
TABLE 6: SMOKING HABITS AMONG THE PATIENTS
STUDIED
SMOKING
NUMBER OF
PATIENTS
PERCENT
Yes 34 57
No 26 43
CHART 6: SMOKING HABITS AMONG THE PATIENTS
STUDIED
Out of 60 patients, 34 patients (57%) had history of smoking.
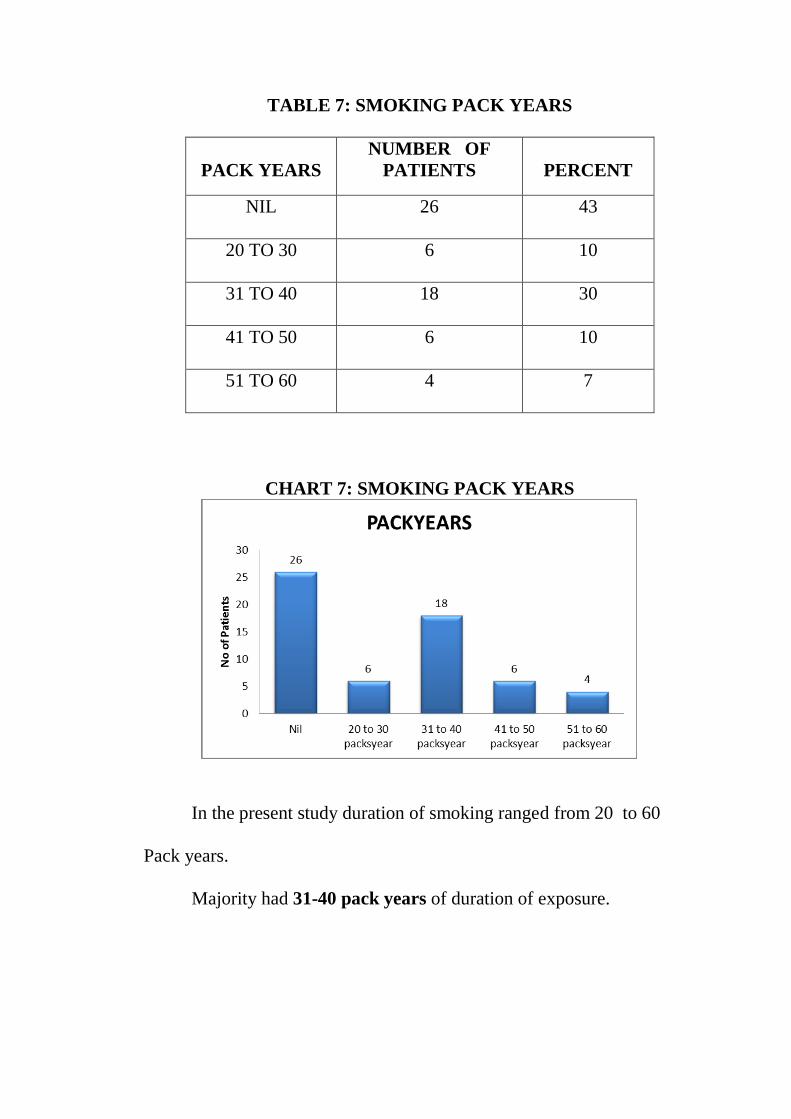
TABLE 7: SMOKING PACK YEARS
PACK YEARS
NUMBER OF
PATIENTS
PERCENT
NIL
26 43
20 TO 30
6 10
31 TO 40
18 30
41 TO 50
6 10
51 TO 60
4 7
CHART 7: SMOKING PACK YEARS
In the present study duration of smoking ranged from 20 to 60
Pack years.
Majority had 31-40 pack years of duration of exposure.
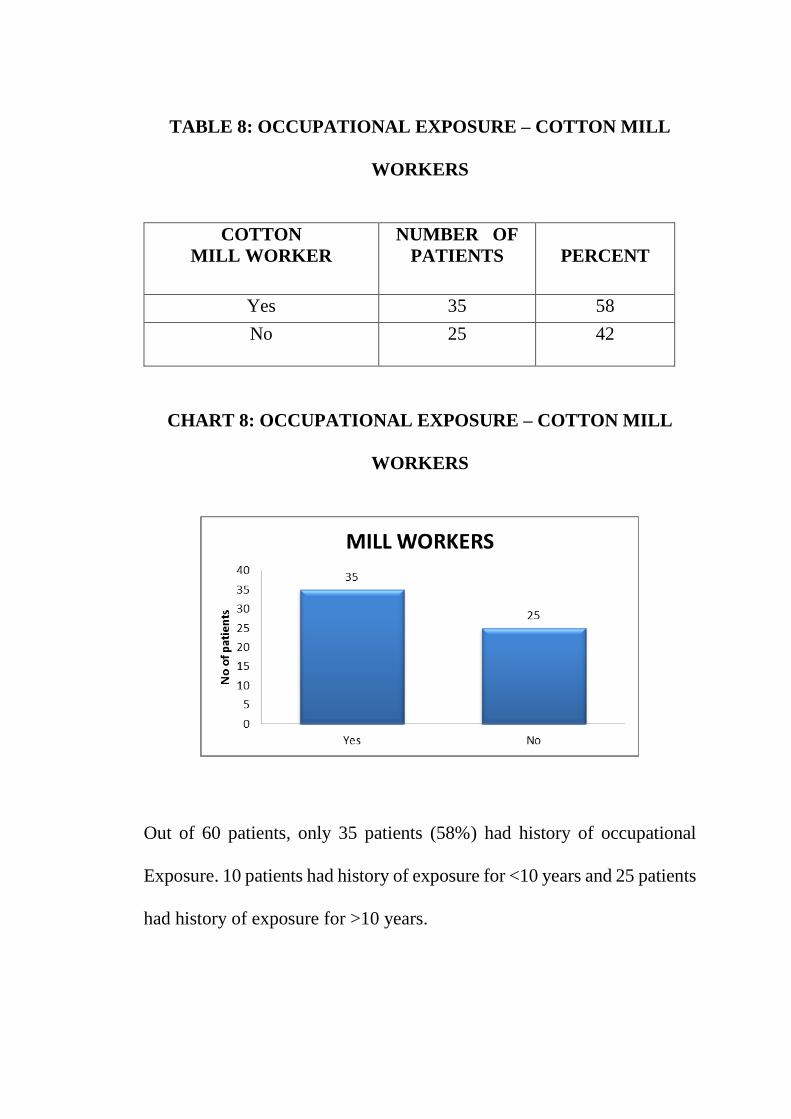
TABLE 8: OCCUPATIONAL EXPOSURE – COTTON MILL
WORKERS
COTTON
MILL WORKER
NUMBER OF
PATIENTS
PERCENT
Yes 35 58
No
25 42
CHART 8: OCCUPATIONAL EXPOSURE – COTTON MILL
WORKERS
Out of 60 patients, only 35 patients (58%) had history of occupational
Exposure. 10 patients had history of exposure for <10 years and 25 patients
had history of exposure for >10 years.
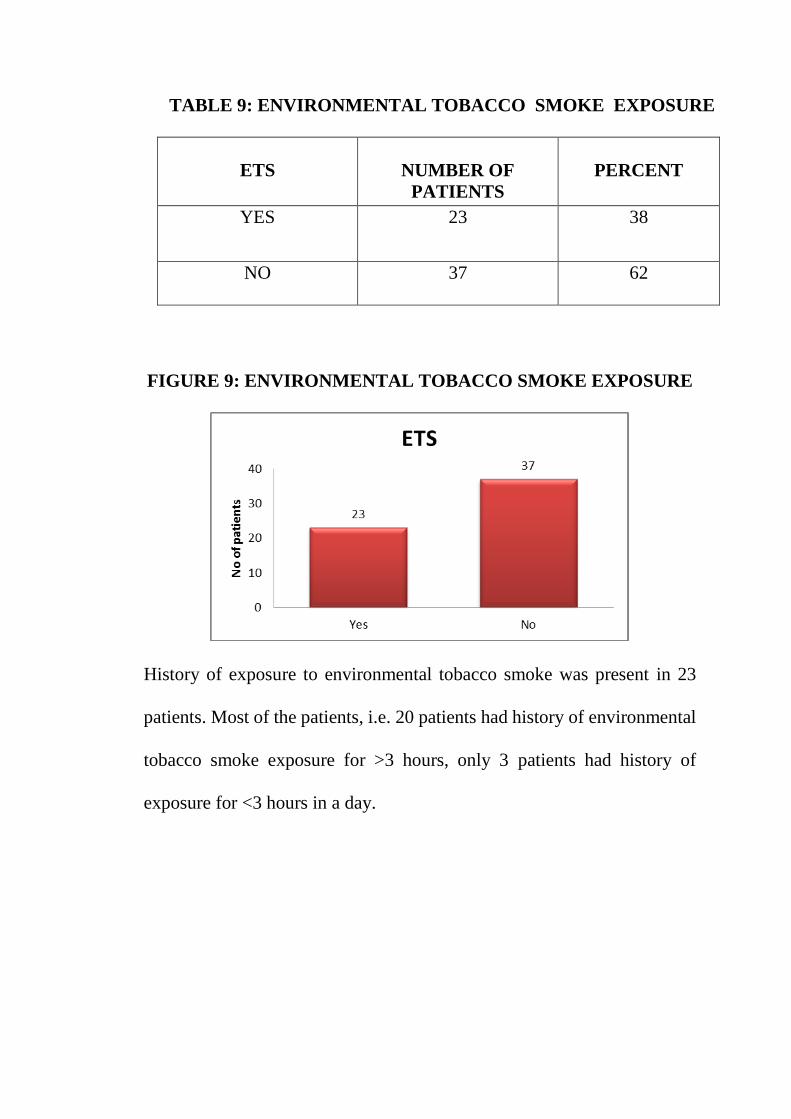
TABLE 9: ENVIRONMENTAL TOBACCO SMOKE EXPOSURE
ETS
NUMBER OF
PATIENTS
PERCENT
YES 23 38
NO
37 62
FIGURE 9: ENVIRONMENTAL TOBACCO SMOKE EXPOSURE
History of exposure to environmental tobacco smoke was present in 23
patients. Most of the patients, i.e. 20 patients had history of environmental
tobacco smoke exposure for >3 hours, only 3 patients had history of
exposure for <3 hours in a day.
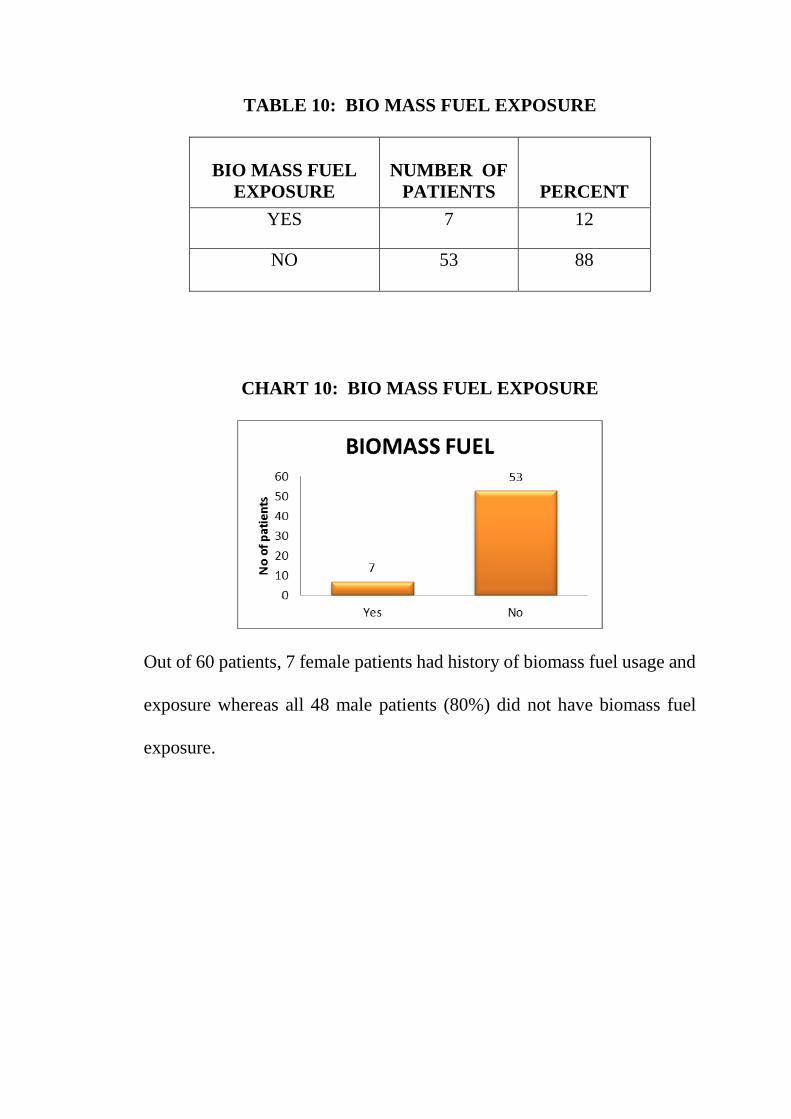
TABLE 10: BIO MASS FUEL EXPOSURE
BIO MASS FUEL
EXPOSURE
NUMBER OF
PATIENTS
PERCENT
YES 7 12
NO 53 88
CHART 10: BIO MASS FUEL EXPOSURE
Out of 60 patients, 7 female patients had history of biomass fuel usage and
exposure whereas all 48 male patients (80%) did not have biomass fuel
exposure.
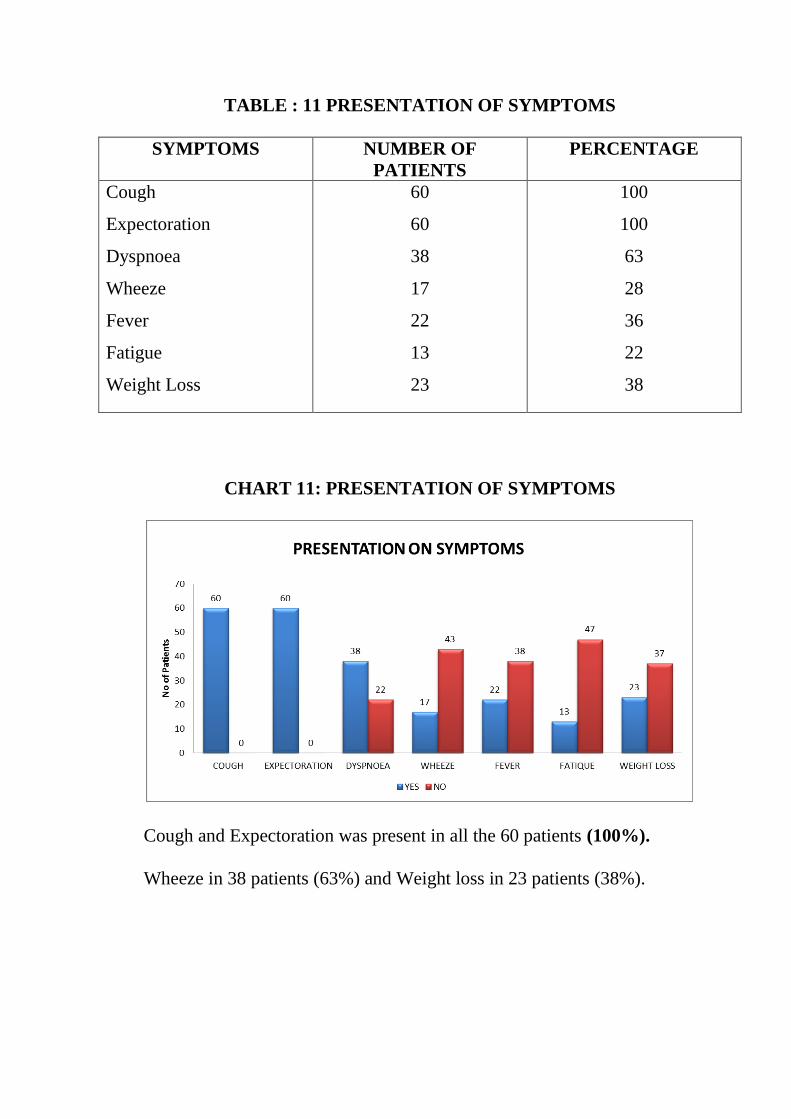
TABLE : 11 PRESENTATION OF SYMPTOMS
SYMPTOMS NUMBER OF
PATIENTS
PERCENTAGE
Cough
Expectoration
Dyspnoea
Wheeze
Fever
Fatigue
Weight Loss
60
60
38
17
22
13
23
100
100
63
28
36
22
38
CHART 11: PRESENTATION OF SYMPTOMS
Cough and Expectoration was present in all the 60 patients (100%).
Wheeze in 38 patients (63%) and Weight loss in 23 patients (38%).

TABLE 12: SIGNS ON PHYSICAL EXAMINATION
SIGNS NUMBER OF
PATIENTS
PERCENTAGE
Tachypnoea
Cyanosis
Clubbing
Accessory muscle
Pedel edema
JVP
Loud p2
Parasternal heave
Hepatomegaly
Crepitations
Rhonchi
42
25
9
30
14
13
12
4
3
42
42
70
42
15
50
23
22
20
7
5
70
70
CHART 12 :SIGNS ON PHYSICAL EXAMINATION
Tachypnea , Rhonchi, Crepitations were present in 42 patients (70%).
42
25
9
30
14 13 124 3
42 42
18
35
51
30
46 47 4856 57
18 18
0102030405060
No
of
pat
ien
ts
SIGNS ON PHYSICAL EXAMINATION
YES NO
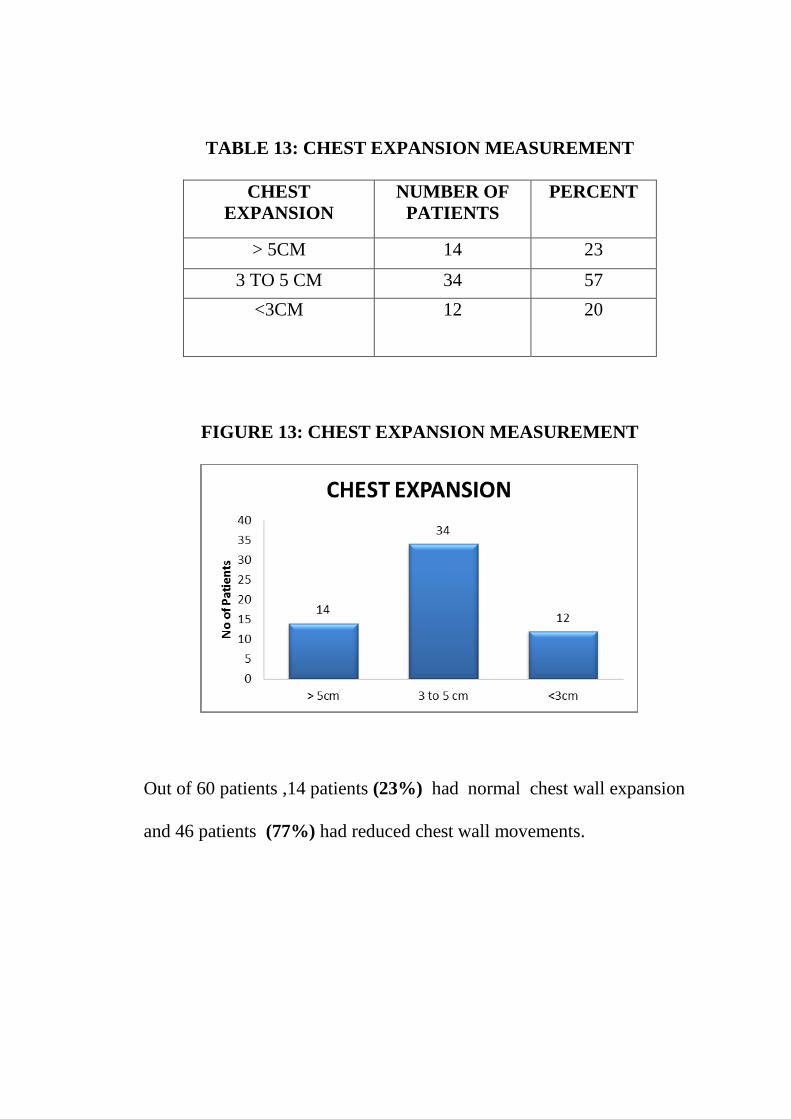
TABLE 13: CHEST EXPANSION MEASUREMENT
CHEST
EXPANSION
NUMBER OF
PATIENTS
PERCENT
> 5CM 14 23
3 TO 5 CM 34 57
<3CM
12 20
FIGURE 13: CHEST EXPANSION MEASUREMENT
Out of 60 patients ,14 patients (23%) had normal chest wall expansion
and 46 patients (77%) had reduced chest wall movements.
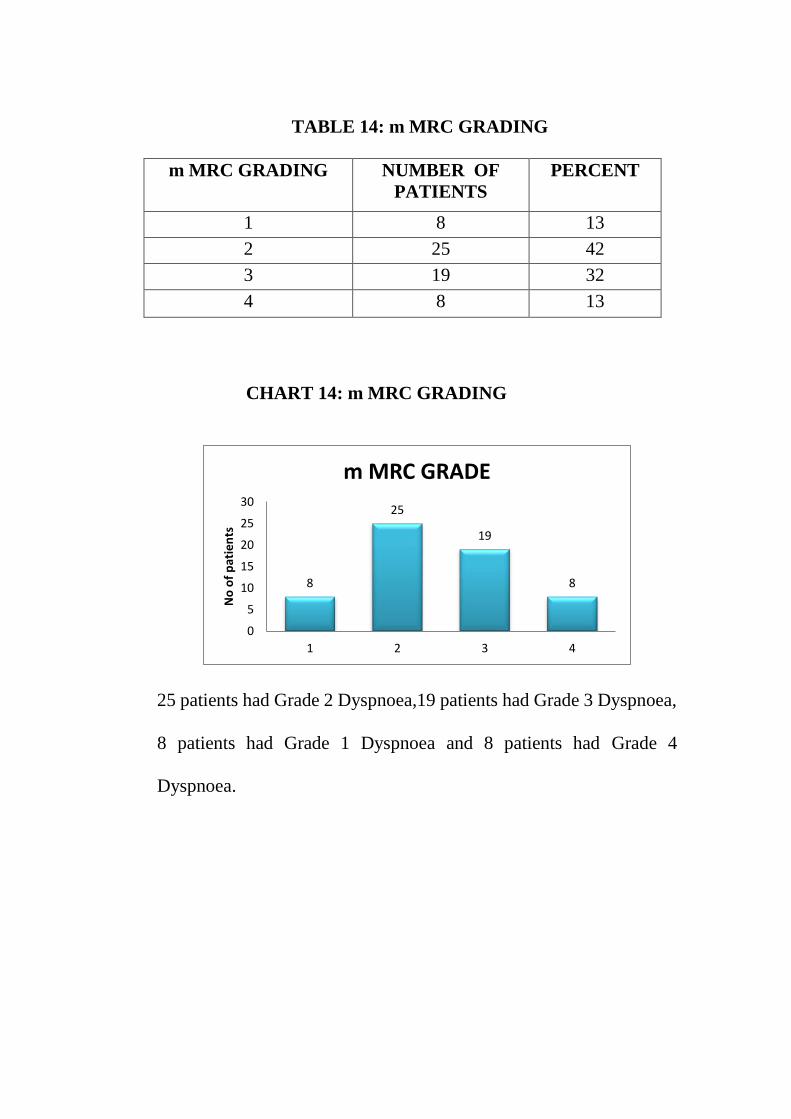
TABLE 14: m MRC GRADING
m MRC GRADING NUMBER OF
PATIENTS
PERCENT
1 8 13
2 25 42
3 19 32
4 8 13
CHART 14: m MRC GRADING
25 patients had Grade 2 Dyspnoea,19 patients had Grade 3 Dyspnoea,
8 patients had Grade 1 Dyspnoea and 8 patients had Grade 4
Dyspnoea.
8
25
19
8
0
5
10
15
20
25
30
1 2 3 4
No
of
pat
ien
ts
m MRC GRADE
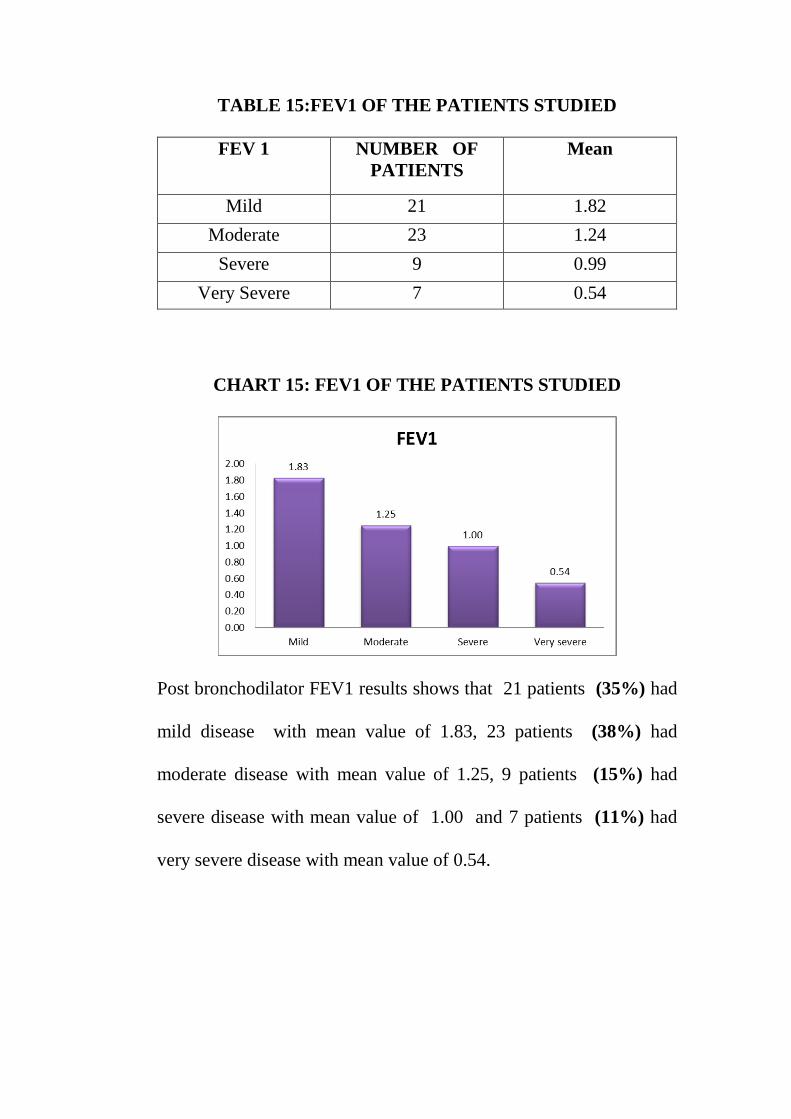
TABLE 15:FEV1 OF THE PATIENTS STUDIED
FEV 1 NUMBER OF
PATIENTS
Mean
Mild 21 1.82
Moderate 23 1.24
Severe 9 0.99
Very Severe 7 0.54
CHART 15: FEV1 OF THE PATIENTS STUDIED
Post bronchodilator FEV1 results shows that 21 patients (35%) had
mild disease with mean value of 1.83, 23 patients (38%) had
moderate disease with mean value of 1.25, 9 patients (15%) had
severe disease with mean value of 1.00 and 7 patients (11%) had
very severe disease with mean value of 0.54.
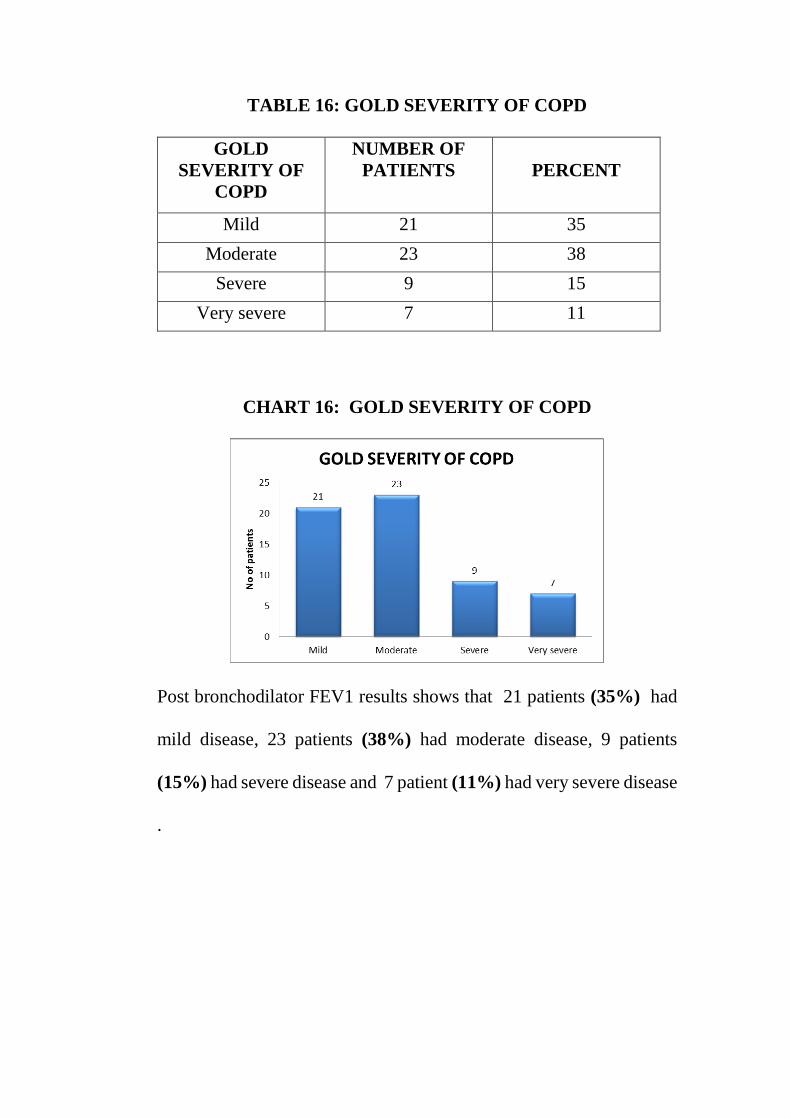
TABLE 16: GOLD SEVERITY OF COPD
GOLD
SEVERITY OF
COPD
NUMBER OF
PATIENTS
PERCENT
Mild 21 35
Moderate 23 38
Severe 9 15
Very severe 7 11
CHART 16: GOLD SEVERITY OF COPD
Post bronchodilator FEV1 results shows that 21 patients (35%) had
mild disease, 23 patients (38%) had moderate disease, 9 patients
(15%) had severe disease and 7 patient (11%) had very severe disease
.
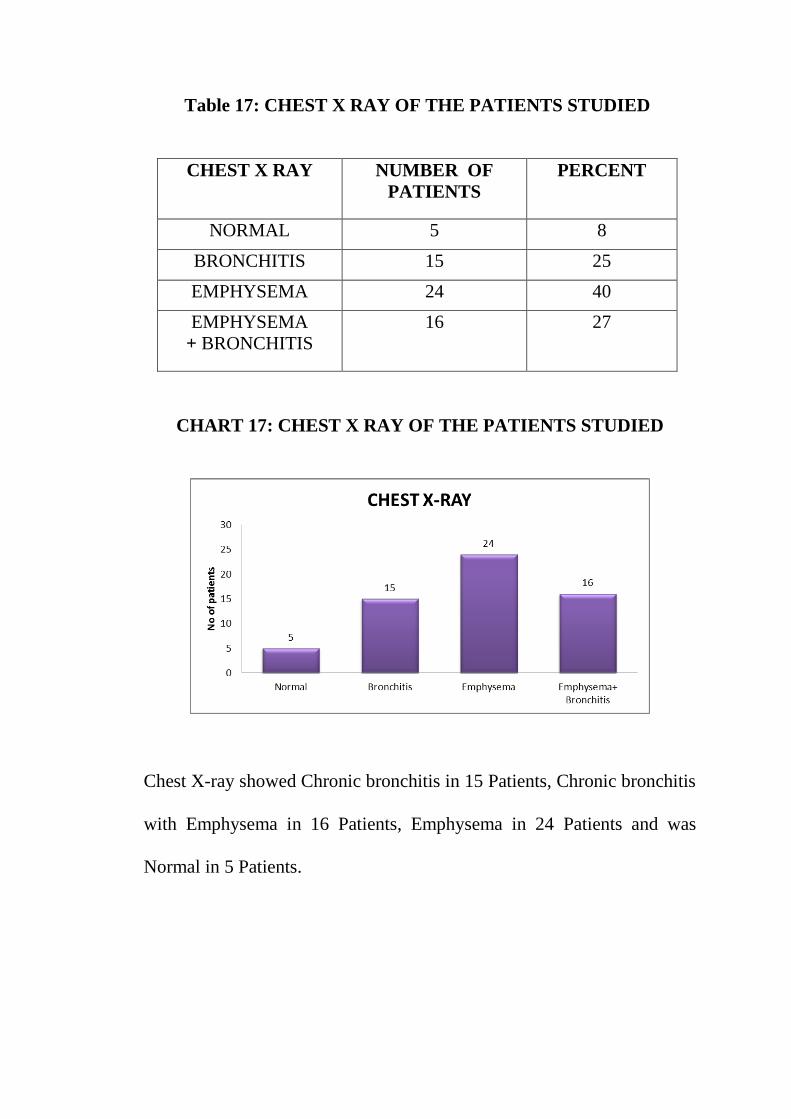
Table 17: CHEST X RAY OF THE PATIENTS STUDIED
CHEST X RAY
NUMBER OF
PATIENTS
PERCENT
NORMAL 5 8
BRONCHITIS 15 25
EMPHYSEMA 24 40
EMPHYSEMA
+ BRONCHITIS
16 27
CHART 17: CHEST X RAY OF THE PATIENTS STUDIED
Chest X-ray showed Chronic bronchitis in 15 Patients, Chronic bronchitis
with Emphysema in 16 Patients, Emphysema in 24 Patients and was
Normal in 5 Patients.
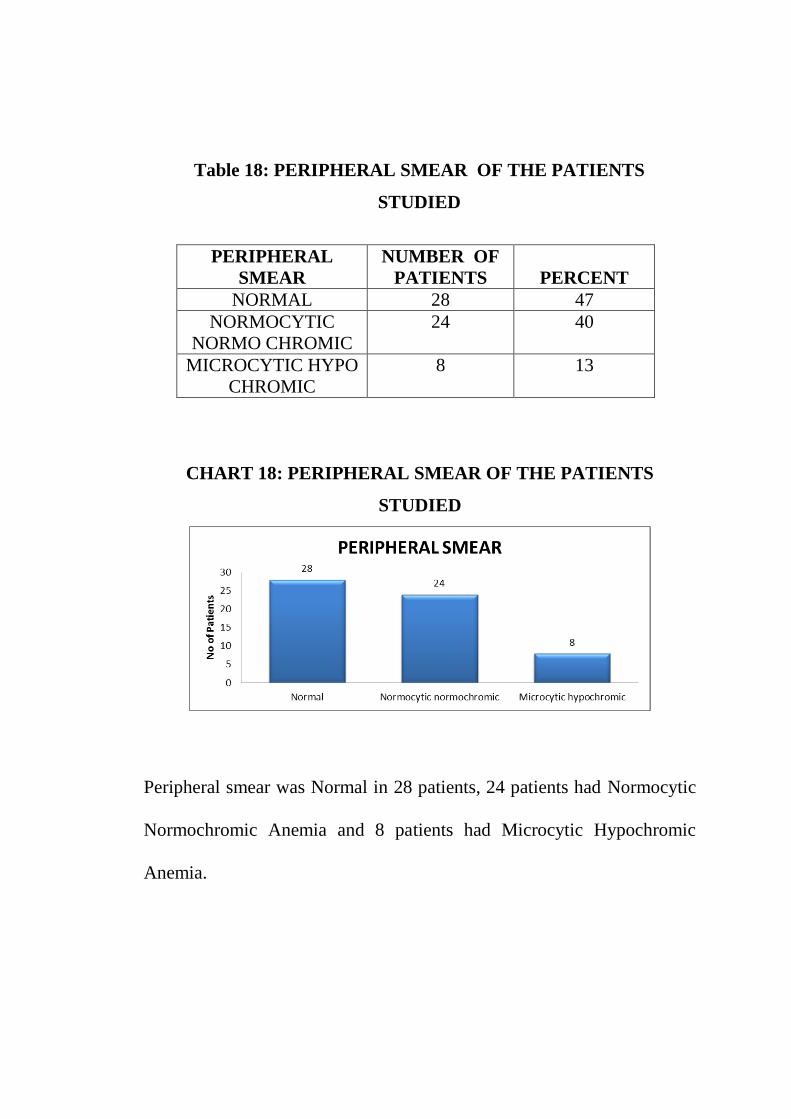
CHART 18: PERIPHERAL SMEAR OF THE PATIENTS
STUDIED
Peripheral smear was Normal in 28 patients, 24 patients had Normocytic
Normochromic Anemia and 8 patients had Microcytic Hypochromic
Anemia.
Table 18: PERIPHERAL SMEAR OF THE PATIENTS
STUDIED
PERIPHERAL
SMEAR
NUMBER OF
PATIENTS
PERCENT
NORMAL 28 47
NORMOCYTIC
NORMO CHROMIC
24 40
MICROCYTIC HYPO
CHROMIC
8 13
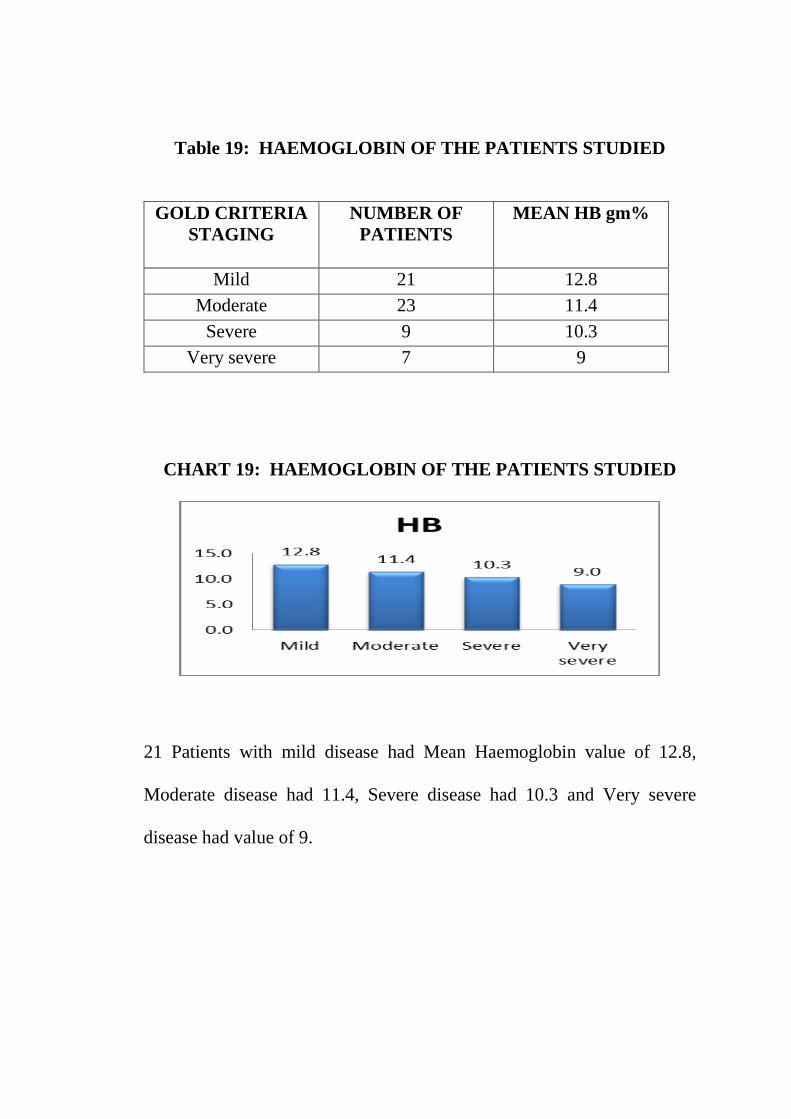
Table 19: HAEMOGLOBIN OF THE PATIENTS STUDIED
GOLD CRITERIA
STAGING
NUMBER OF
PATIENTS
MEAN HB gm%
Mild 21 12.8
Moderate 23 11.4
Severe 9 10.3
Very severe 7 9
CHART 19: HAEMOGLOBIN OF THE PATIENTS STUDIED
21 Patients with mild disease had Mean Haemoglobin value of 12.8,
Moderate disease had 11.4, Severe disease had 10.3 and Very severe
disease had value of 9.
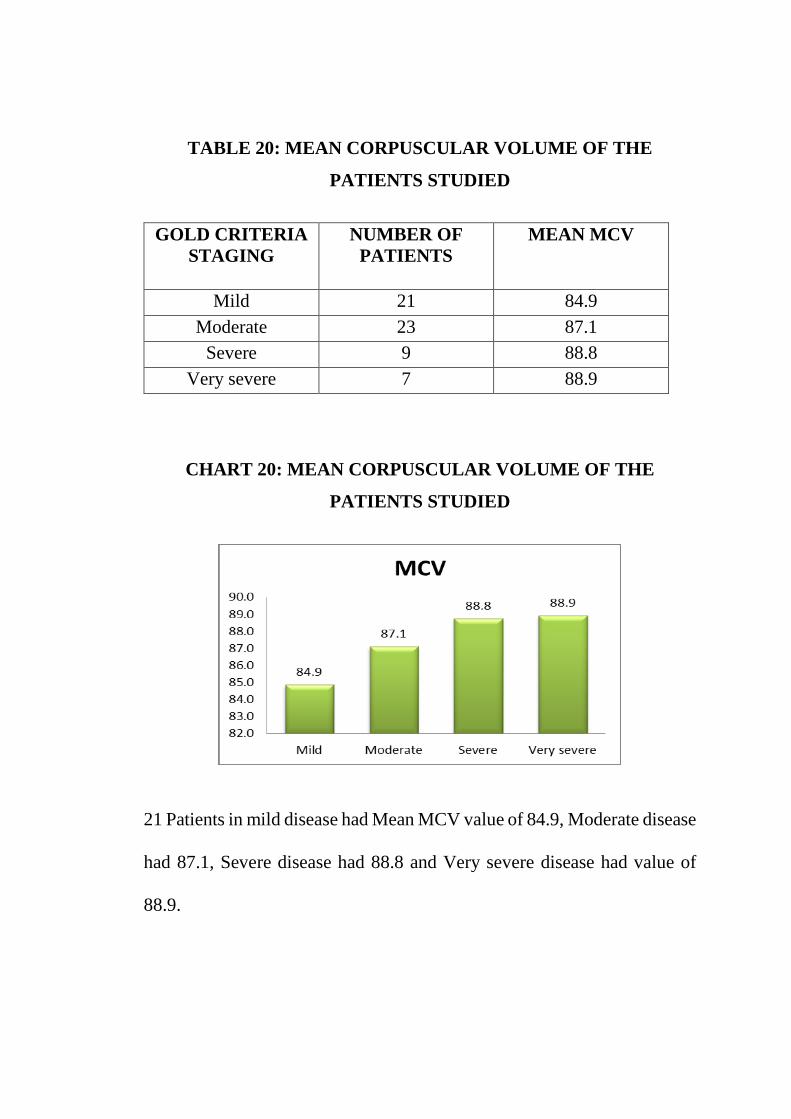
TABLE 20: MEAN CORPUSCULAR VOLUME OF THE
PATIENTS STUDIED
GOLD CRITERIA
STAGING
NUMBER OF
PATIENTS
MEAN MCV
Mild 21 84.9
Moderate 23 87.1
Severe 9 88.8
Very severe 7 88.9
CHART 20: MEAN CORPUSCULAR VOLUME OF THE
PATIENTS STUDIED
21 Patients in mild disease had Mean MCV value of 84.9, Moderate disease
had 87.1, Severe disease had 88.8 and Very severe disease had value of
88.9.

TABLE 21: MEAN CORPUSCULAR HAEMOGLOBIN OF THE
PATIENTS STUDIED
GOLD CRITERIA
STAGING
NUMBER OF
PATIENTS
MEAN MCH
Mild 21 29.1
Moderate 23 29.4
Severe 9 29.5
Very severe 7 29.1
CHART 21: MEAN CORPUSCULAR HAEMOGLOBIN OF THE
PATIENTS STUDIED
21 Patients in mild disease had Mean MCH value of 29.1, Moderate
disease had 29.4, Severe disease had 29.5, Very severe disease had
29.1.
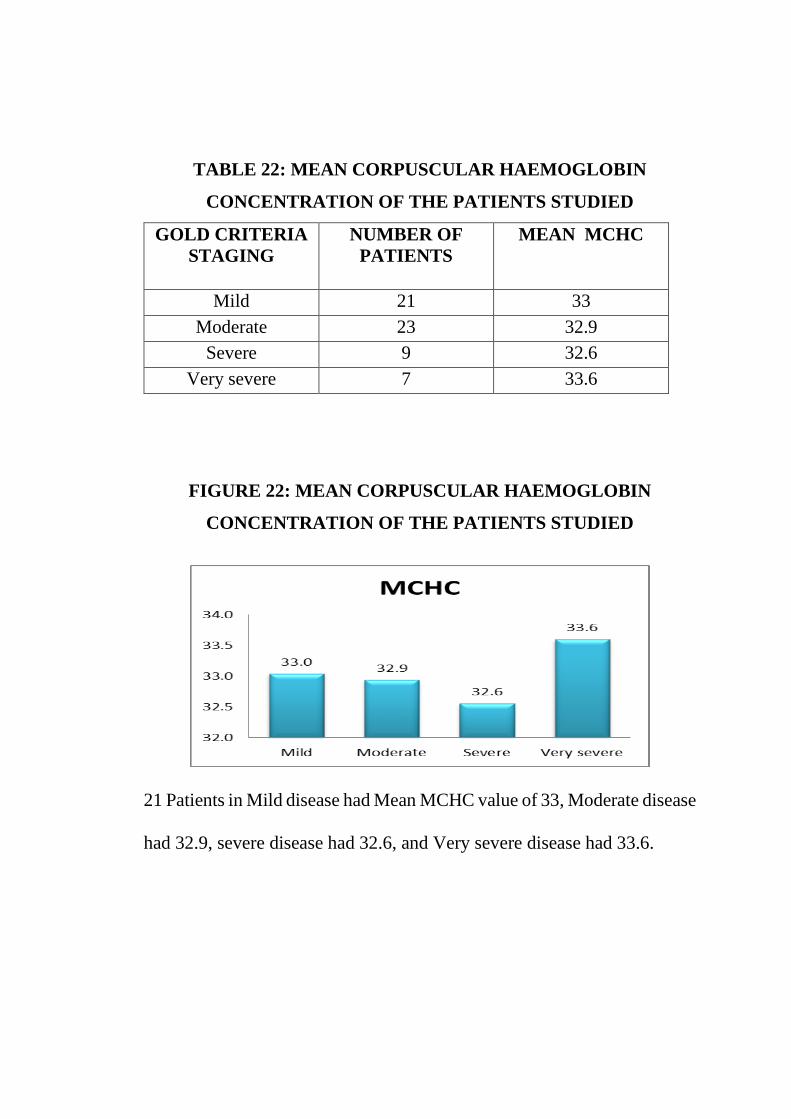
TABLE 22: MEAN CORPUSCULAR HAEMOGLOBIN
CONCENTRATION OF THE PATIENTS STUDIED
GOLD CRITERIA
STAGING
NUMBER OF
PATIENTS
MEAN MCHC
Mild 21 33
Moderate 23 32.9
Severe 9 32.6
Very severe 7 33.6
FIGURE 22: MEAN CORPUSCULAR HAEMOGLOBIN
CONCENTRATION OF THE PATIENTS STUDIED
21 Patients in Mild disease had Mean MCHC value of 33, Moderate disease
had 32.9, severe disease had 32.6, and Very severe disease had 33.6.

TABLE 23: HAEMATOCRIT OF THE PATIENTS STUDIED
GOLD CRITERIA
STAGING
NUMBER OF
PATIENTS
MEAN HCT
Mild 21 42.3
Moderate 23 43.5
Severe 9 44.2
Very severe 7 43.7
CHART 23: HAEMATOCRIT OF THE PATIENTS STUDIED
21 Patients in mild disease had Haematocrit value of 42.3, Moderate
disease had 43.5, Severe disease had 44.2, Very severe disease had 43.7.

TABLE 24: COMPARISON OF AGE vs HAEMOGLOBIN
AGE
HAEMOGLOBIN
ANEMIA NORMAL
31 to 40 yrs 0 1
41 to 50 yrs 19 9
51 to 60 yrs 15 6
61 to 70 yrs 7 3
CHART 24 :COMPARISON OF AGE vs HAEMOGLOBIN
Haemoglobin of the patient were compared with age of the patient.
Patient with age group ranged from 41-50 yrs had 68% chance for
development of anemia. . Patient with age group ranged from 51-60 yrs
had 71% chance for development of anemia. Patient with age group ranged
from 61-70 yrs had 70% chance for development of anemia.
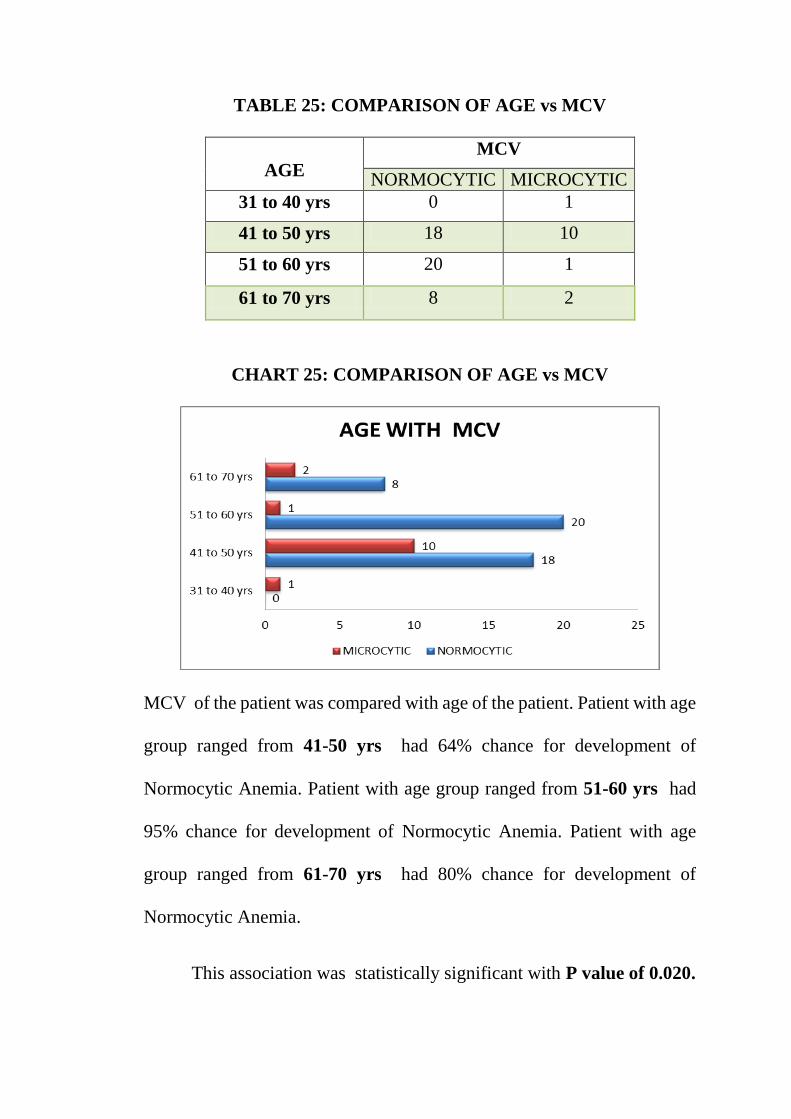
TABLE 25: COMPARISON OF AGE vs MCV
AGE
MCV
NORMOCYTIC MICROCYTIC
31 to 40 yrs 0 1
41 to 50 yrs 18 10
51 to 60 yrs 20 1
61 to 70 yrs 8 2
CHART 25: COMPARISON OF AGE vs MCV
MCV of the patient was compared with age of the patient. Patient with age
group ranged from 41-50 yrs had 64% chance for development of
Normocytic Anemia. Patient with age group ranged from 51-60 yrs had
95% chance for development of Normocytic Anemia. Patient with age
group ranged from 61-70 yrs had 80% chance for development of
Normocytic Anemia.
This association was statistically significant with P value of 0.020.

TABLE 26: COMPARISION OF AGE vs MCH
AGE
MCH
NORMOCHROMIC HYPOCHROMIC
31 to 40 yrs 1 0
41 to 50 yrs 21 7
51 to 60 yrs 19 2
61 to 70 yrs 9 1
CHART 26: COMPARISION OF AGE vs MCH
MCH of the patient was compared with age of the patient. Patient with age
group ranged from 41-50 yrs had 75% chance for development of
Normochromic. Patient with age group ranged from 51-60 yrs had 90%
chance for development of Normochromia. Patient with age group ranged
from 61-70 yrs had 90% chance for development of Normochromia.
This association was not statistically significant with P value of 0.442.
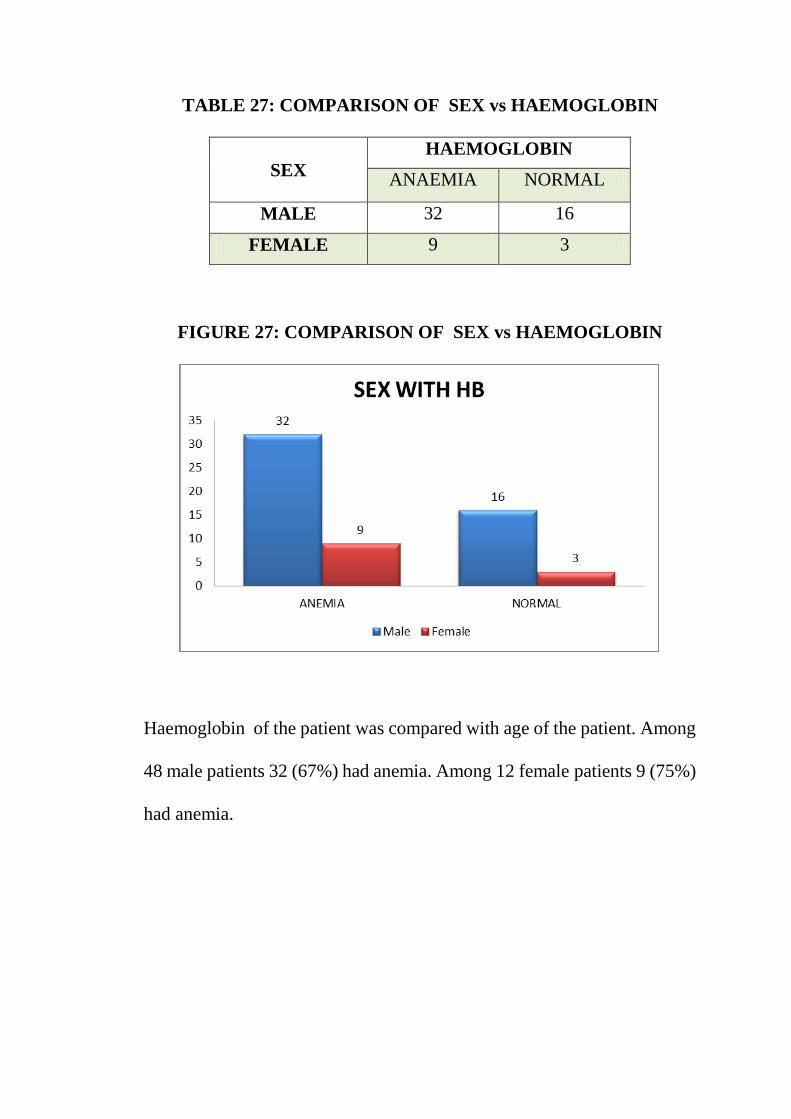
TABLE 27: COMPARISON OF SEX vs HAEMOGLOBIN
SEX
HAEMOGLOBIN
ANAEMIA NORMAL
MALE 32 16
FEMALE 9 3
FIGURE 27: COMPARISON OF SEX vs HAEMOGLOBIN
Haemoglobin of the patient was compared with age of the patient. Among
48 male patients 32 (67%) had anemia. Among 12 female patients 9 (75%)
had anemia.

TABLE 28 : COMPARISON OF SEX vs MCV
SEX
MCV
NORMOCYTIC MICROCYTIC
MALE 38 10
FEMALE 8 4
CHART 28: COMPARISON OF SEX vs MCV
MCV of the patient was compared with age of the patient. Among 48
male patients 38 (79%) had normocytic. Among 12 female patients 8
(67%) had normocytic.
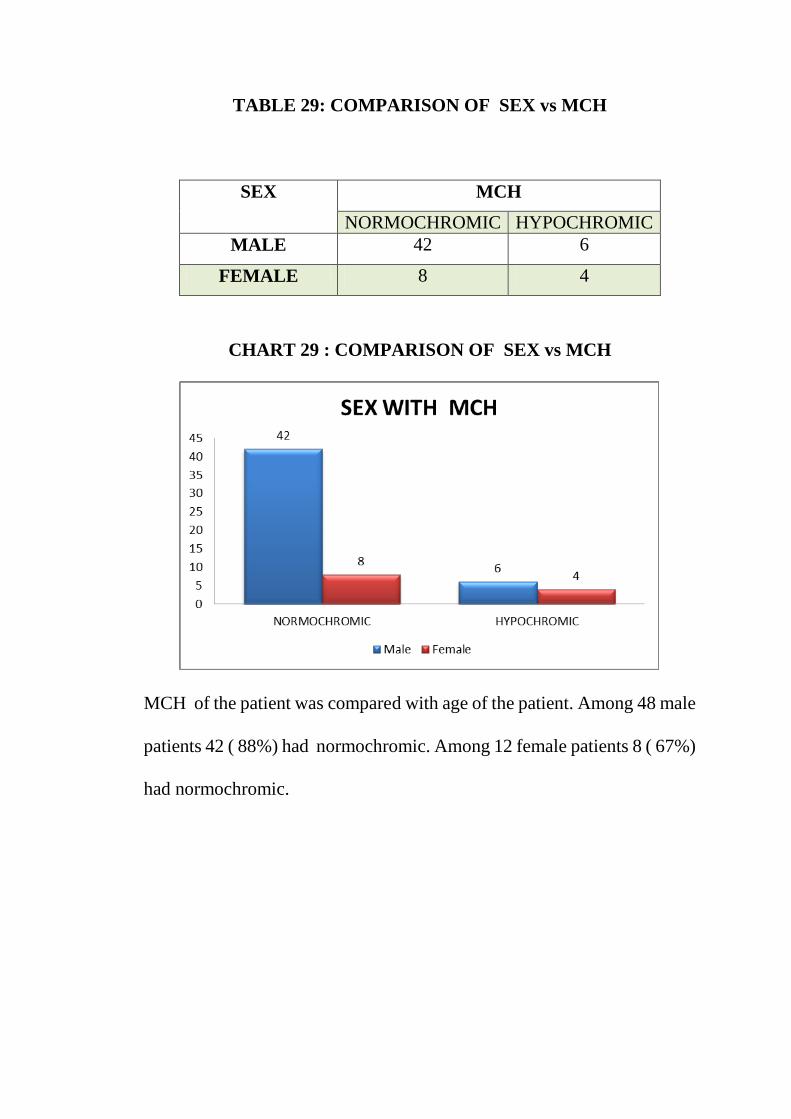
TABLE 29: COMPARISON OF SEX vs MCH
SEX
MCH
NORMOCHROMIC HYPOCHROMIC
MALE 42 6
FEMALE 8 4
CHART 29 : COMPARISON OF SEX vs MCH
MCH of the patient was compared with age of the patient. Among 48 male
patients 42 ( 88%) had normochromic. Among 12 female patients 8 ( 67%)
had normochromic.
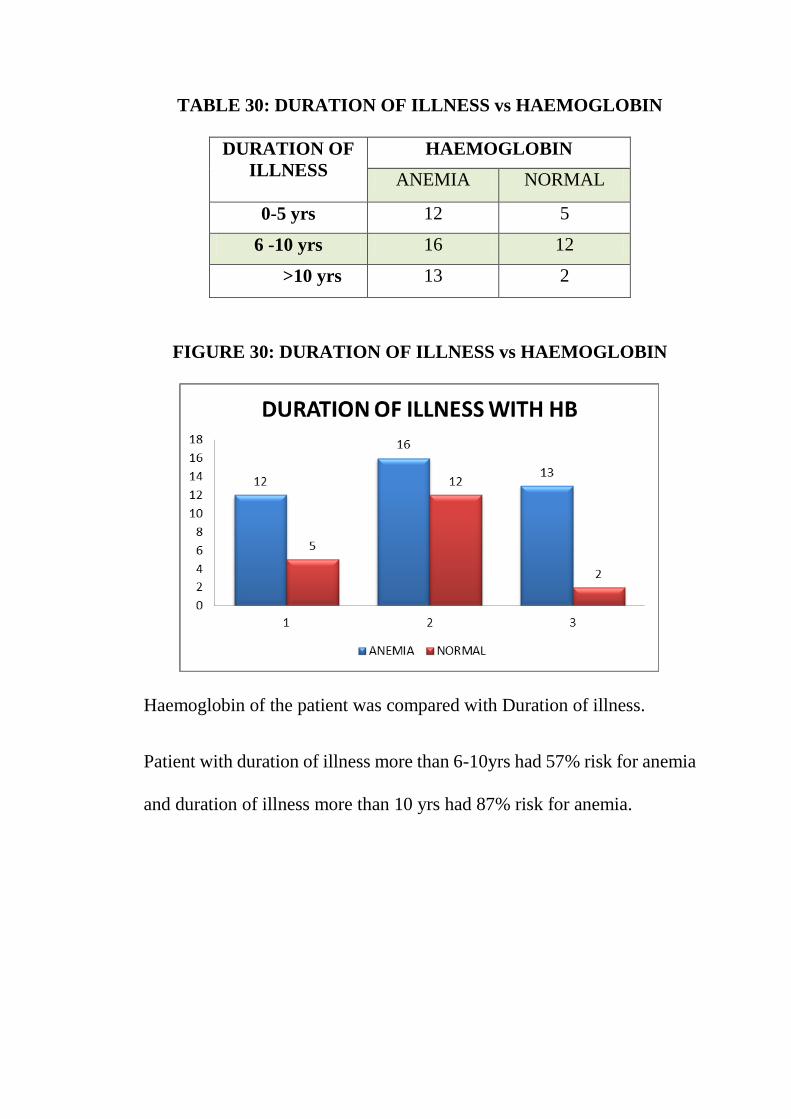
TABLE 30: DURATION OF ILLNESS vs HAEMOGLOBIN
DURATION OF
ILLNESS
HAEMOGLOBIN
ANEMIA NORMAL
0-5 yrs 12 5
6 -10 yrs 16 12
>10 yrs 13 2
FIGURE 30: DURATION OF ILLNESS vs HAEMOGLOBIN
Haemoglobin of the patient was compared with Duration of illness.
Patient with duration of illness more than 6-10yrs had 57% risk for anemia
and duration of illness more than 10 yrs had 87% risk for anemia.
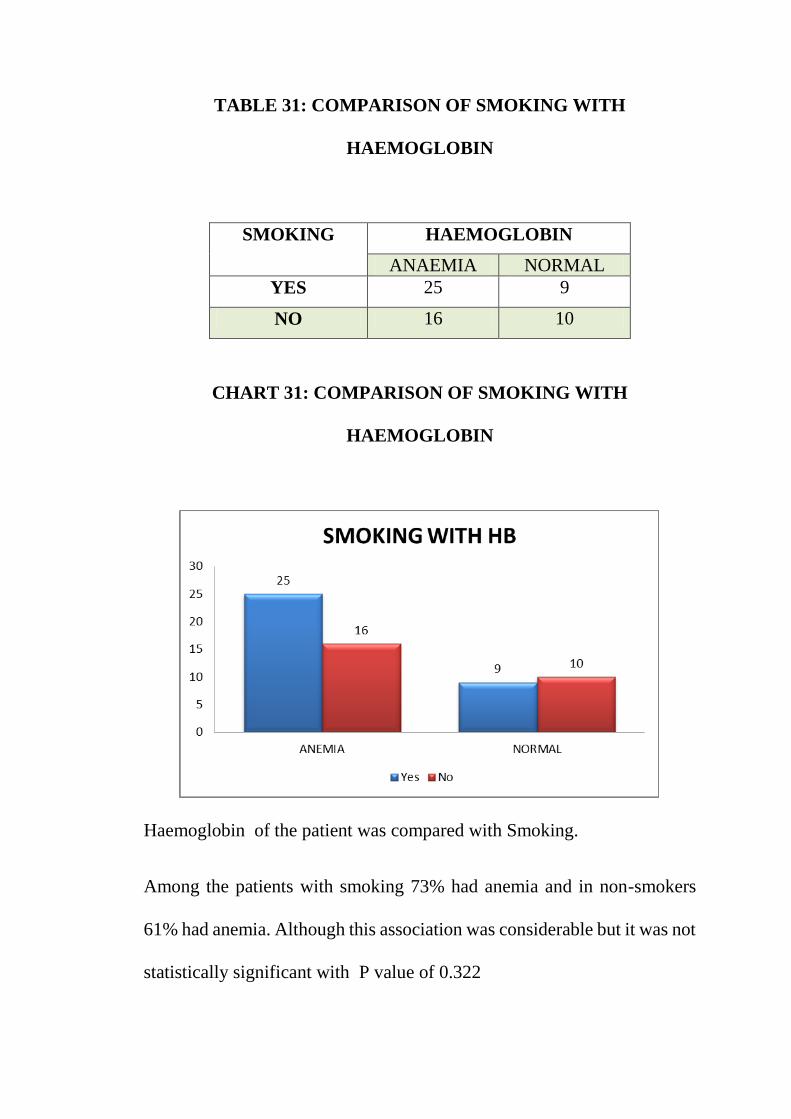
TABLE 31: COMPARISON OF SMOKING WITH
HAEMOGLOBIN
SMOKING
HAEMOGLOBIN
ANAEMIA NORMAL
YES 25 9
NO 16 10
CHART 31: COMPARISON OF SMOKING WITH
HAEMOGLOBIN
Haemoglobin of the patient was compared with Smoking.
Among the patients with smoking 73% had anemia and in non-smokers
61% had anemia. Although this association was considerable but it was not
statistically significant with P value of 0.322

TABLE 32: COMPARISON OF OCCUPATIONAL EXPOSURE –
COTTON MILL WORKERS WITH HAEMOGLOBIN
COTTON
MILL WORKER
HAEMOGLOBIN
ANAEMIA NORMAL
YES 25 10
NO 16 9
CHART 32: COMPARISON OF OCCUPATIONAL EXPOSURE –
COTTON MILL WORKERS WITH HAEMOGLOBIN
Haemoglobin of the patient was compared with Mill workers.Among the
mill workers 71% had anaemia and 64% in non –mill workers. Although
this association was considerable but it was not statistically significant.

TABLE 33: m MRC GRADING vs HAEMOGLOBIN
m MRC
GRADING
HAEMOGLOBIN
ANEMIC NORMAL
1 6 2
2 19 6
3 17 2
4 8 0
CHART 33: m MRC GRADING vs HAEMOGLOBIN
Haemoglobin of the patient was compared with m MRC GRADING.
Patients with increased Grades of Dyspnea had more risk for anemia and
vice versa.
6
19
17
8
2
6
2
00
2
4
6
8
10
12
14
16
18
20
1 2 3 4
mMRC GRADE WITH HAEMOGLOBIN

DISCUSSION
This clinical observational study was undertaken to investigate the
pattern and magnitude of Hematological parameters in the relationship
with the Severity of the disease. The study consisted of 60 subjects, among
them 21 Patients had mild COPD, 23 Patients with moderate COPD, 9
Patients had severe COPD and 7 Patients had very severe COPD.
All the individuals in different groups were subjected to detailed
History and Physical examination. Lung function parameters were
assessed with the help of spirometer. All patients underwent
Haematological parameters with particular reference to Hb%, MCV,
MCH, MCHC, HAEMATOCRIT, PERIPHERAL SMEAR along with
routine tests.
The aim of the present study was to assess the relationship between
Physical examination, Hematological parameters and the severity of
COPD.
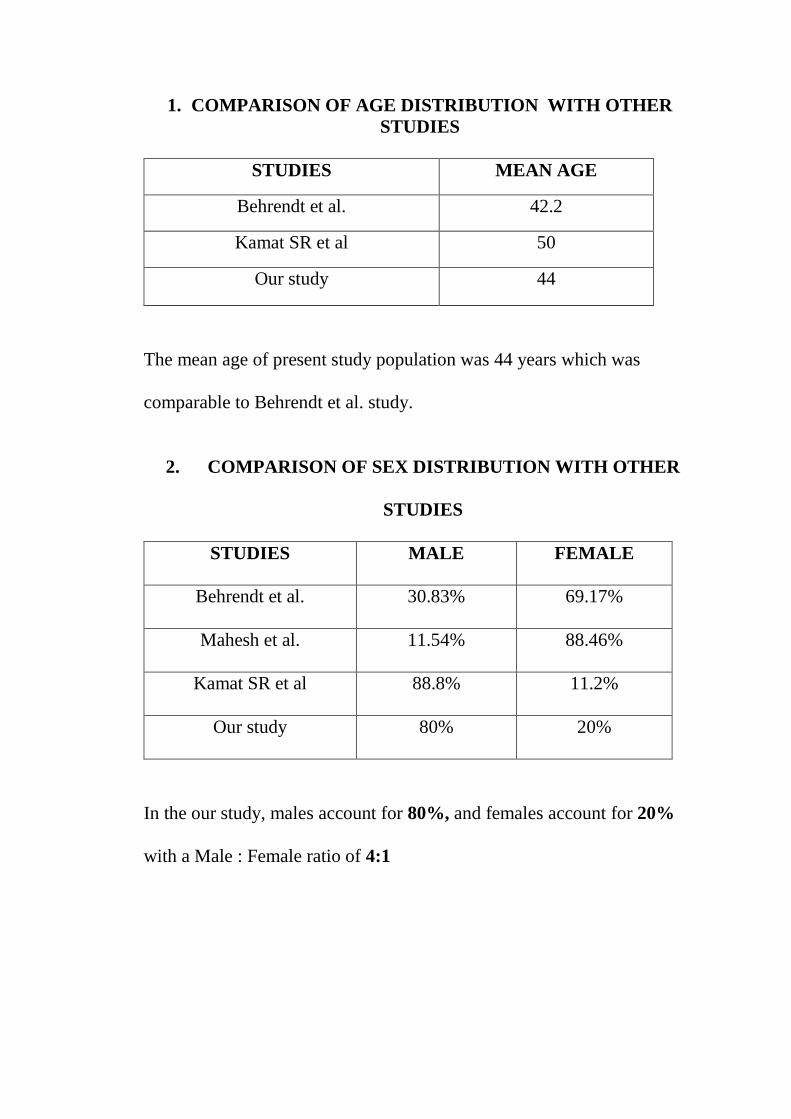
1. COMPARISON OF AGE DISTRIBUTION WITH OTHER
STUDIES
STUDIES MEAN AGE
Behrendt et al. 42.2
Kamat SR et al 50
Our study 44
The mean age of present study population was 44 years which was
comparable to Behrendt et al. study.
2. COMPARISON OF SEX DISTRIBUTION WITH OTHER
STUDIES
STUDIES MALE FEMALE
Behrendt et al. 30.83% 69.17%
Mahesh et al. 11.54% 88.46%
Kamat SR et al 88.8% 11.2%
Our study 80% 20%
In the our study, males account for 80%, and females account for 20%
with a Male : Female ratio of 4:1
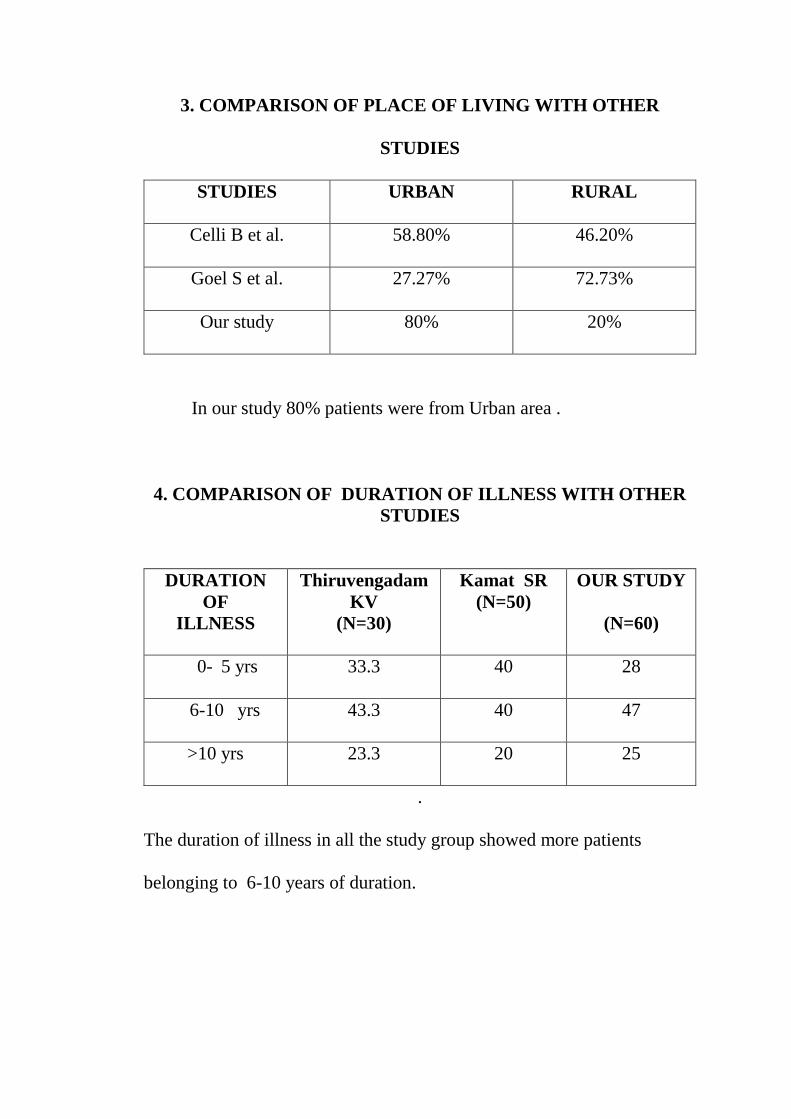
3. COMPARISON OF PLACE OF LIVING WITH OTHER
STUDIES
STUDIES URBAN RURAL
Celli B et al. 58.80% 46.20%
Goel S et al. 27.27% 72.73%
Our study 80% 20%
In our study 80% patients were from Urban area .
4. COMPARISON OF DURATION OF ILLNESS WITH OTHER
STUDIES
DURATION
OF
ILLNESS
Thiruvengadam
KV
(N=30)
Kamat SR
(N=50)
OUR STUDY
(N=60)
0- 5 yrs 33.3 40 28
6-10 yrs 43.3 40 47
>10 yrs 23.3 20 25
.
The duration of illness in all the study group showed more patients
belonging to 6-10 years of duration.
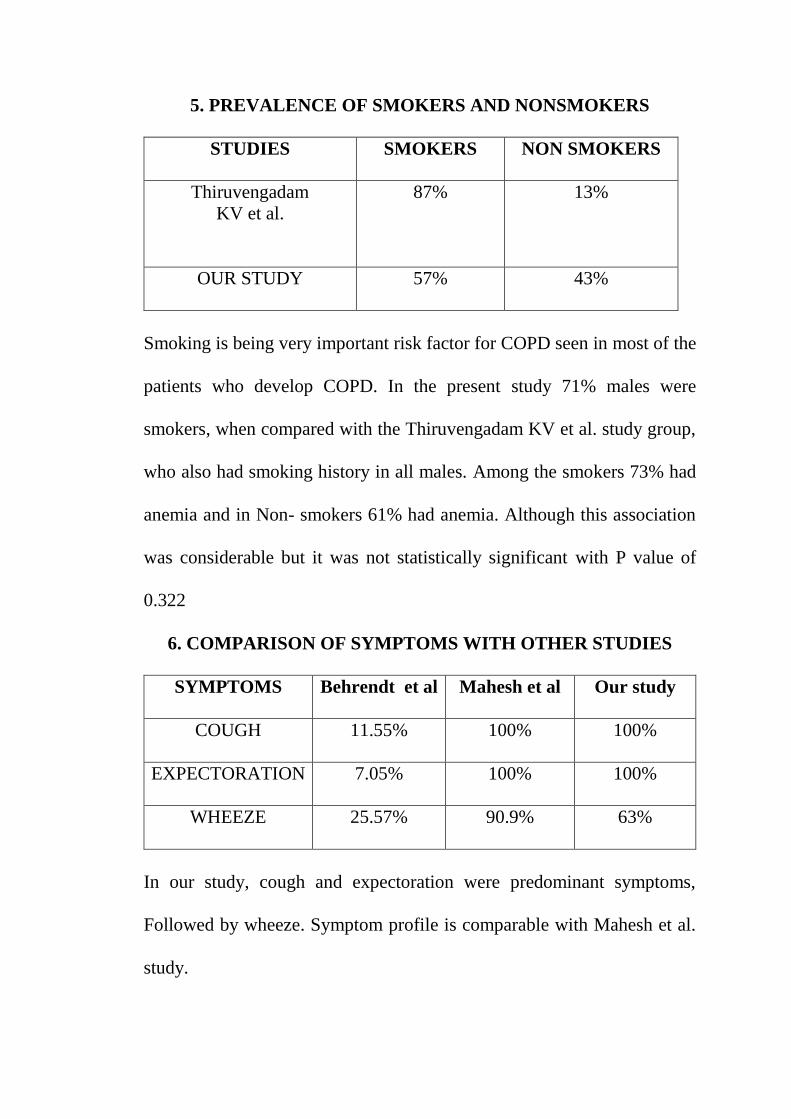
5. PREVALENCE OF SMOKERS AND NONSMOKERS
STUDIES SMOKERS NON SMOKERS
Thiruvengadam
KV et al.
87% 13%
OUR STUDY 57% 43%
Smoking is being very important risk factor for COPD seen in most of the
patients who develop COPD. In the present study 71% males were
smokers, when compared with the Thiruvengadam KV et al. study group,
who also had smoking history in all males. Among the smokers 73% had
anemia and in Non- smokers 61% had anemia. Although this association
was considerable but it was not statistically significant with P value of
0.322
6. COMPARISON OF SYMPTOMS WITH OTHER STUDIES
SYMPTOMS Behrendt et al Mahesh et al Our study
COUGH 11.55% 100% 100%
EXPECTORATION 7.05% 100% 100%
WHEEZE 25.57% 90.9% 63%
In our study, cough and expectoration were predominant symptoms,
Followed by wheeze. Symptom profile is comparable with Mahesh et al.
study.
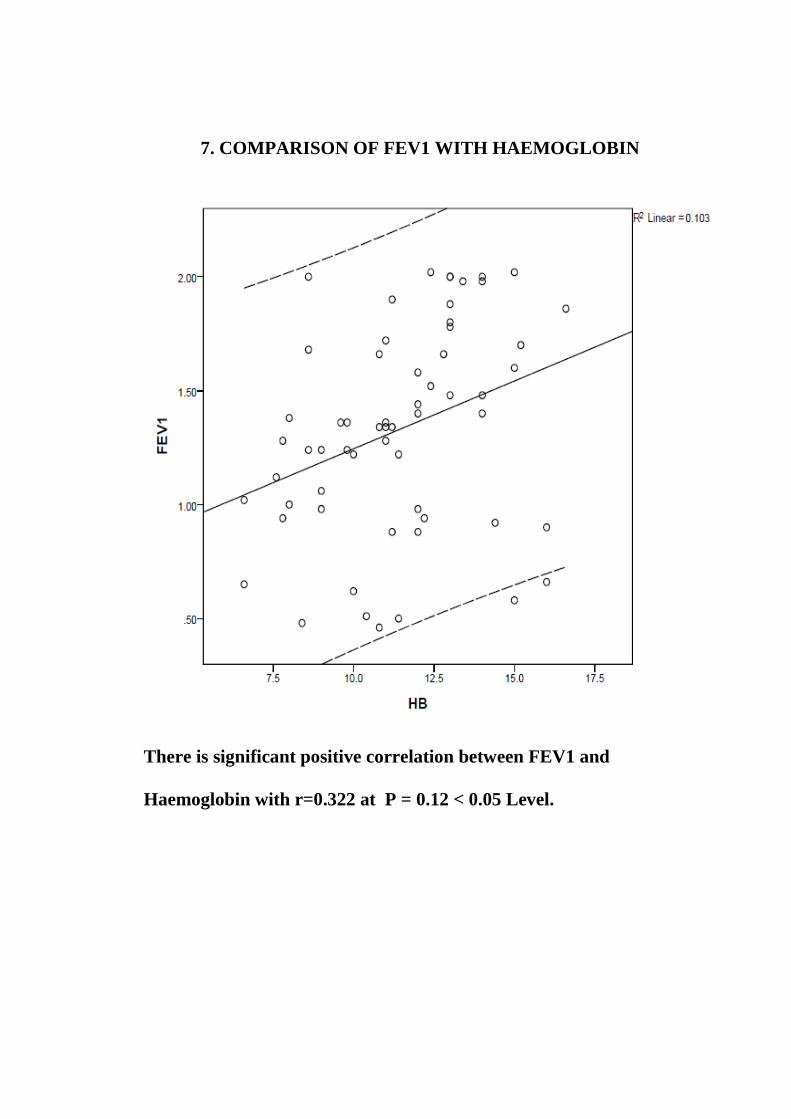
7. COMPARISON OF FEV1 WITH HAEMOGLOBIN
There is significant positive correlation between FEV1 and
Haemoglobin with r=0.322 at P = 0.12 < 0.05 Level.

8. Among the patients studied 58% had exposure to cotton mill
industry.Among them 71% had anemia.
9. Patient with increased levels of Dyspnea (m MRC Grading) had
more risk for anemia
Grade 2 Dyspnea - 76% had anemia
Grade 3 Dyspnea – 89% had anemia
Grade 4 Dyspnea - 100% had anemia.
CONCLUSION
1. The age of the patients being studied ranged between 30 yrs to 70 yrs
and the majority of the patients were in the age group of 41-50 years.
2. In our study, out of 60 patients 48 (80%) were males and 12 (20%)
were females. The Male:Female ratio of this study was 4:1.
3. In our study, the duration of illness was more in patients with severe
COPD as compared to the mild and moderate COPD group. This shows
that the severity of COPD increases with the duration of illness.
4. In our study Post bronchodilator FEV1 results showed that 21 patients
(35%) had GOLD CRITERIA of mild disease who had a mean of 1.82,
23 patients (38%) had moderate disease who had a mean of 1.24,
9 patients (15%) had severe disease who had a mean of 0.99 and
7 patient (11%) had very severe disease who had a mean of 0.54.
5. The most common symptoms were cough and expectoration , Present
in all the 60 patients (100%). The most common sign observed was
tachypnea in 42 (70%) patients.
6. In our study out of 60 (100%) patients studied chest x ray shows
Chronic bronchitis in 15 patients , Chronic bronchitis with Emphysema
in 16 patients , Emphysema in 24 patients and was Normal in 5 patients
7. Among the Patients 57% were smokers. 71% of male patients had a
history of smoking for 5yrs or more. Among smokers 73% had anemia
and in Non-smokers 61% had anemia.
8. In our study 56% of Patients had anemia.Among them 70% had
Normocytic Normochromic Anemia and the remaining 30% had
Microcytic Hypochromic Anemia.
9. The Prevalence of anemia was more common with increased duration
of illness.Duration of illness 6-10 yrs had 57% risk for anemia and > 10
yrs had 87% risk of anemia.
10. The prevalence of anemia was more common in Cottton mill workers
with 71% and 64% in non –mill workers.
11. The prevalence of anemia was more common in Patients with m MRC
grade 3 and 4 dyspnoea.
12. In our study the fall in FEV1 was associated with fall in Haemoglobin
percentage and vice versa.

SUMMARY
This study was conducted to detect the haematological
manifestations in relation to FEVI in COPD Patients.60 Patients were
included in this study.
Results from the study showed Patients with decreased FEV1,
having prolonged duration of illness and increasing grades of dyspnea had
high risk for anemia. Patients with exposure to Cotton Mill dust and with
the history of smoking had increased risk for anemia, but its association
was not statistically significant.
BIBILIOGRAPHY
1. Mannino DM, Thorn D, Holguin F.Prevalence and outcomes in
diabetes, hypertensionand cardiovascular disease in Chronic
obstructive pulmonary disease Eur Resp j 2008; 32;962-269
2. Foster TS Miller JD Assessment of economic burden of COPD IN
THE us;a review and synthesis of the literature in COPD
2006:3;211-218
3. Sevenoks MJ , STOCKLEY . Chronic obstructive pulmonary
disease and comorbidity Respir res 2006 7;70
4. John. M, Lange A, Hoernig S, Witt C, Anker SD. Prevalence of
anemia in chronic obstructive pulmonary disease; comparison to
other chronic diseases. Int I Cardiol 2006; 111: 365-370.
5. Cote C, Zilberberg MD, Mody SH, Dordelly LJ, Celli B.
Haemoglobin level and its clinical impact in a cohort of patients with
COPD. Eur Respir J 2007; 29: 923-929.
6. Shorr AF, Doyle J, Stern L, Dolgitser M, Zilberberg MD. Anemia in
chronic obstructive pulmonary disease: epidemiology and economic
implications. Curr Med Res Opin 2008; 24: 1123-1130.
7. Krishnan G, Grant BJ, Multi PC, et al. Association between anemia
and quality of life in a population sample of individuals with chronic
obstructive pulmonary disease. BMC Pulm Med 2006; 6: 23.
8. Similowski T, Agusti A, MacNee W, Schonhofer B. The potential
impact of anaemia of chronic disease in COPD. Eur Respir J 2006;
27: 390-396.
9. John M, Hoernig S, Doehner W, Okonko DD, Witt C, Anker SD.
Anemia and inflammation in COPD. Chest 2005; 127: 825-829.
10. Thomas L Petty. The history of COPD. International Journal of
COPD 2006;1(1):3-14.
11. Swash M, Glynn M. Hutchinson’s Clinical methods. 22nd ed.
Chapter 6. p.58.
12. Moore KL, Persavd Tvn: the respiratory system. In moore KL,
Persavd Tvn, editors: the developing human. Clinically oriented
embryology, ed7, Philadelphia, 2003, wb savnders.
13. Maeda Y, Dave.V, Whitsett JA: Transcritional control of lung
morphpoenesis. Physiol Rev 87: 219 – 244.2007.
14. De Langhes, Del moral P, Tefft D, ET at: The genetic molecular and
cellular basis of lung development. In fishman A, Ellas J, Fishman
J, et al, editors: Fishman’s pulmonary diseases and disorders, ed4,
Newyork, 2008, Mc Graw-Hill.
15. Morrisey EE, Hogan BLM: Preparing for the first birth: Genetic and
Cellular Mechanisms in lung development. Dev cell 18:8 – 23, 2010.
16. Langston C, Kida.K, Reed M, etal: Human lung growth in late
gestation end in the neonate, Am Rev Respir Dis 129:607-13, 1992.

17. Merkus PJ, ten Have-opbroek AA, Ovanjer PH. Human Lung
growth: a review. Aed pulmonary 21:383-397, 1996.
18. Susan Standring. Grey’s Anatomy. Thorax: Overview and surface
anatomy.40th ed. p. 914.
19. Maria L Padilla. Pulmonary Circulation. Chest 2003;124:1183.
20. Comroe JH.Jr, Physiology of Respiratory 2nd ed. Chicago year
book 1974.
21. William F Ganong. Pulmonary function. Chapter 34. 22nd ed.
Review of
22. Medical Physiology. The McGraw-Hill Companies.
23. William Macnee. Chronic bronchitis and emphysema. 5th ed.
Chapter 23.
24. In: Crofton and Douglas’s respiratory disease, Anthony Seaton,
Douglas, eds. Oxford: Blackwell Science Publishers; 2000.
25. Viegi G, Pistelli F, Sherrill DL. Definition, epidemiology and
natural history of COPD. Eur Respir J 2007;30:993-1013.
26. Fletcher CM, Pride NB. Definitions of emphysema, chronic
bronchitis, asthma, and airflow obstruction: 25 years on from the
Ciba symposium. Thorax 1984;39:81-5.
27. GOLD 2004 executive summary page 1-21.
28. Halbert RJ, Natoli JL, Gano A, et al. Global burden of COPD:
systematic

29. review and meta-analysis. Eur Respir J 2006;28:523-32.
30. Shirtcliffe P, Weatherall M, Marsh S, et al. COPD prevalence in a
random population survey: a matter of definition. Eur Respir J
2007;30:232–9.
31. Halbert, Sharon Isonaka, Dorothy George, et al. What Is the True
Burden
32. Disease? Interpreting COPD Prevalence Estimates. Chest
2003;123:1684-92. World Health Organistion. Global Status Report
on Non communicable Diseases 2010. Geneva: WHO;2011.
33. Chhabra SK, Rajpal S, Gupta R. Patterns of smoking in Delhi and
comparison of chronic respiratory morbidity among beedi and
cigarette smokers. Indian J Chest Dis Allied Sci 2001;43:19-26.
34. Jindal SK, Aggarwal AN, Chaudhry K, Chhabra SK, D’Souza GA,
Gupta D, et al. Tobacco smoking in India: prevalence, quit-rates
and respiratory morbidity. Indian J Chest Dis Allied Sci
2006;48:37-42. .
35. Jindal SK, Aggarwal A N, A review of population studies from
India to estimate national burden of Chronic Obstructive Lung
Disease and its association with smoking. Indian J Chest Dis Allied
Sci 2001; 43:139-147
36. Foreman MG, Campos M, Celedon JC, Genes and chronic
obstructive pulmonary disease. Med Clin North Am 2012;96:699-
711.
37. Eisner MD, Anthonisen N, Coultas D, Kuenzli N, Perez-Padilla R,
Postma D, et al. An official American Thoracic Society public policy
statement: Novel risk factors and the global burden of chronic
obstructive pulmonary disease. Am J Respir Crit Care Med
2010;182:693-718.
38. Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-
smokers. Lancet 2009;374:33-43.
39. Balmes J, Becklake M, Blanc P, Hennebergere P, Kreiss K, Mapp
C, et al. American Thoracic Society Statement: Occupational
contribution to the burden of airway disease. Am J Respir Crit Care
Med 2003;167:787-97.
40. Semple S, Devakumar D, Fullerton DG, Thorne PS, Metwali N,
Costello A, et al. Airborne endotoxin concentrations in homes
burning biomass fuel. Environ Health Perspect 2010;118:988-91.
41. Qureshi KA. Domestic smoke pollution and prevalence of chronic
bronchitis/asthma I a rural area of Kashmir. Indian J Chest Dis
Allied Sci 1994;36:61-72.
42. Ray D, Kanagasabapthy As, Jairaj PS. Alpha 1 antitrypsin
deficiency in India patients with chronic obstructive airways and
other pulmonary diseases. Ceylon Med J 1994;39:77-81.
43. Alpha 1-antitrypsin deficiency: memorandum from a WHO
meeting. Bull World health Organ 1997;75:397-415.
44. Thomas L Petty. COPD in Perspective. Chest 2002;121:116S-120S.
45. William Macnee. Pathogenesis of COPD. Proc Am Thorac Soc
2005;
46. 2:258-66.
47. Steven R Rutgers, Dirkje S Postma, Nick Htten Hacken, et al.
Ongoing airway inflammation in patients with COPD who do not
currently smoke. Thorax 2000;55:12-8.
48. Bhatt SP, Guleria R, Lugman Arafath TK, et al. Effect of Tripod
Position on Objective Parameters of Respiratory Function in Stable
Chronic Obtructive Pulmonary Disease. Indian J Chest Dis Allied
Sci 2009;51:83-5.
49. Jadranka Spahija, Michel de Marchie, Alejandro Grassino. Effects
of Imposed Pursed-Lips Breathing on Respiratory Mechanics and
Dyspnea at Rest and During Exercise in COPD. Chest
2005;128:640-50.
50. Bestall JC, Paul EA, Garrod R, et al. Usefulness of the Medical
Research
51. Council (MRC) dyspnoea scale as a measure of disability in
patients with
52. chronic obstructive pulmonary disease. Thorax 1999;54:581-6.
53. Bohadana AB, Peslin R, Uffhottz H. Breath sounds in the clinical
assessment of airflow obstruction. Thorax 1978;33:345-51.
54. Brinnel Caszo, George A D’Souza. COPD and nutrition. Lung
India
55. 2006;23:78-81.
56. Stephen I Rennard, Jorgen Vestbo, et al. Natural Histories of
Chronic
57. Obstructive Pulmonary Disease. Proc Am Thorac Soc 2008;5:878-
83. 50.
58. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha
JA. Usefulness of the Medical Research Council (MRC) dyspnoea
scale as a measure of disability in patients with chronic obstructive
pulmonary disease Thorax 1990;54:581-6.
59. Om Prakash. Spirometric norms: A study from Karnataka. Lung
India 1990; 8(1):23-7.
60. Jindal SK. Spirometers. Lung India 1993;11(1&2):60-3.
61. Miller MR, Hankinson J, Burgos F, Casaburi R, Coates A, et al.
Standardisation of spirometry. Eur Respir J 2005;26:319-38.
62. American Thoracic Society Standardization of spirometry, 1994
update. Am J Respir Crit Care Med 1995; 152;1107-36.
63. Adapted from Celi BR, Cote.C, Martin JM, etal: The body mass
index, airflow obstruction, Dyspnoea, and exercise capacity index
in COPD. N Engl J med 350: 005-1012, 2004.
64. Gajalakshmi V, Peto R, Kanaka TS, Jha P.Smoking and mortality
from tuberculosis and other diseases in India: retrospective study of
43000 adult male deaths and 35000 controls. Lancet 2003;362:507-
15.
65. Dhamgaye TM. Tobacco smoking and pulmonary tuberculosis: a
case-control study. J Indian Med Assoc 2008;106:216-9.
66. Kolappan C, Gopi PG. Tobacco smoking and pulmonary
tuberculosis. Thorax 2002;57:964-6.
67. Guryay MS, Ceylan E, Gunay T, Karaduman S,Bengi F, Parlak I, et
al. Can spirometry, pulse oximetry and dyspnea scoring reflect
respiratory failure in patients with chronic obstructive pulmonary
disease exacerbation? Med Princ Pract 2007;16:378-83.
68. Kelly AM, McAlpine R, Kyle E. How accurate are pulse oximeters
in patients with acute exacerbations of chronic obstructive airways
disease? Respir Med 2001;95:336-40.
69. Simon G, Medvei VC. Chronic bronchitis: radiological aspects of a
five –year follow-up. Thorax 1962;17:5-8.

70. Thurlbeck WM, Winter JH, Winter JE, Taylor A, Taylor TW,
Cameron RC. Chest z-rays in COPD screening: are they
worthwhile? Respir Med 2009;103:1862-5.
71. Gevenois PA, De Vuyst P, de Maertelaer V, Zanan J, Jacobovitz D,
Cosio MG, et al. Comparison of Computed density and microscopic
morphometry in pulmonary emphysema. Am J Respir Crit Care Med
1996;154:187-92.
72. Gould GA, Macnee W, McLean A, Warren PM, Redpath A, Best JJ,
e al. CT measurements of lung density in life can quantitate distal
airspace enlargement an essential defining feature of human
emphysema. Am Rev Respir Dis 1988;137:380-92.
73. Bernstein ML, Despars JA, Singh NP, Aalos K, Stansbury DW,
Light RW, Reanalysis of the 12-minute walk in patients with chronic
obstructive pulmonary disease. Chest 1994;105:163-7.
74. Hajiro T, Nishmura K, Tsukino M, Ikeda A, Koyama H, Izumi T.
Analysis of clinincal methods used to evaluate dyspnea in patients
with chronic obstructive pulmonary disease. Am J Respir Crit Care
Med 1999;159:158-64.
75. Jindal SK, Gupta D, Aggarwal AN. Guidelines for management of
chronic obstructive pulmonary disease (COPD) in India: a guide for
physicians (2003). Indian J Chest Dis. Allied Sci 2004;46:137-53.
76. Au DH, Bryson CL, Chien JW, Sun H, Udris EM, Evans LE, et al.
The effects of smoking cessation on the risk of chronic obstructive
pulmonary disease exacerbations. J Gen Intern Med 2009;24:457-
63.
77. Ministry of Health and Family Welfare, (GOLD). Tobacco
Dependence Treatment Guidelines. National Tobacco Control
Programme, DHGS New Delhi, Ministry of Health and Family
Welfare, Government of India;2011.
78. Jindal SK. Quit Smoking: Why and How. New Delhi: Vikasta
Publishinig Pvt Ltd:2008.
79. Stead LF, Lancaster Combined pharmacotherapy and behavioural
intervention for smoking cessation. Cochrane Database Syst Rev
2012;10:CD008286.
80. Galanti LM. Tobacco smoking cession management integrating
varenicline in current practice. Vasc Health Risk Manag
2008;4:837-45.
81. Smoking cessation for patients with chronic obstructive pulmonary
disease (COPD): an evidence-based analysis. One Health Technical
Asses Ser 2012;12:1
82. Nici L, Donner C, Wouters E, Zuwallack R, Ambrosino N,
Bourbeau J, et al. American Thoracis Society/ Eropean Respiratory
Society statement on pulmonary rehabilitation. Am J Respir Crit
Care Med 2006;173:1390-413.
83. Is 12-hour oxygen as effective as 24-hour oxygen in advanced
chronic obstructive pulmonary disease with hypoxemia? (The
nocturnal oxygen therapy trial-NOTT). Chest 1980;78:419-20.
84. Nocturnal Oxygen Therapy Trial Group. Continuous or nocturnal
oxygen therapy in hypoxmic chronic obstructive lung disease: a
clinical trial. Ann Intern Med 1980;93:391-8.
85. Medical Research Council Working Party. Long term domiciliary
oxygen therapy in chronic hypoxic cor pulmonale complicating
chronic bronchitis and emphysema. Lancel 1981;1:681-6.
86. Khilnani GC, Banga Noninvasive ventilation in patients with
chronic obstructive airway disease. Int J Chron Obstruct Pulmon Dis
2008;3: 351-357.
87. Diaz-Lobato S, Alises SM, Rodriguez EP. Current status of
noninvasive ventilation in stable COPD patients. Int J Chron
Obstruct Pulmon Dis 2006 2006;1:129-35.
88. Nickol AH, Hart N, Hopkinson NS, Hamnegard CH, Moxham J,
Simonds A, et al. Mechanisms of improvement of respiratory failure
in patients with COPD treated with NIV. Int J Chronic Obsturct
Pulmon Dis 2008;3:453-62.

89. Moberley S, Holden, Tatham DP, Andrews RM. Vaccines for
preventing pneumococcal infection in adults. Cochrane Database
Syst Rev 2013;1:CD000422.
90. Expert Group of the Association of Physicians of India on Adult
Immunization in India. The Association of Physicians of India
evidence-based clinical practice practice guidelines on adult
immunization. J Assoc Physicians India 2009;57345-56.
91. Global Initiative for Chronic Obstructive Lung Disease (GOLD)
Global Strategy for the Diagnosis, Management and Prevention of
COPD, 2013. Available from: http;//www.goldcopd.org
PROFORMA
NAME OF THE PATIENT:
AGE: SEX:
OCCUPATION:
ADDRESS:
EDUCATION:
MARITAL STATUS:
INCOME:
DATE OF ADMISSION:
DATE OF EXAMINATION:
IP NUMBER: OP NUMBER:
PRESENTING COMPLAINTS: DURATION
1. Cough
2. Breathlessness
3. Sputum
4. Hemoptysis
5. Weight loss
6. Weakness and fatigue
9. Wheeze
10. Fever
11. Chest pain
12. Swelling of lower limbs
A) HISTORY OF PRESENTING COMPLAINTS:
1. Cough :
Duration
Dry/productive
Persistent/paroxysmal
Postural variation- Present/Absent
Diurnal variation - Present/Absent
Seasonal variation- Present/Absent
Progression- Increasing/decreasing/persisting
Any triggering factors- Smoke/cold/pollen/infection/dust
Relation to occupation- Increased at work/not
2. Breathlessness :
Duration
Onset- Sudden/insidious
Progression- increasing/deteriorating/static
Persistent/paroxysmal
Relation to exertion- present/absent
Seasonal variation- present/absent
Precipitating factors- present/absent
Any triggering factors- Smoke/cold/pollen/infection/dust
Orthopnoea/trepopnoea/platypnoea/PND
3. Sputum:
Colour
Quantity minimal/ moderate/ copious
Consistency
Postural variation Yes/ No
Diurnal variation Yes/ No
Foul smell-present/absent
4. Weight loss: Percentage of loss of weight:
Time period:
5. Chest pain :
Duration
Onset- Sudden/insidious
Location.
Nature of pain- pleuritic/anginal/other types
Radiationf.
Aggravating factors- deep inspiration/exertion/cough/any other
Relieving factors.
Duration of each episode
6. Wheezing :
Duration.
Precipitating factors.
Duration of attack
Seasonal variation- Present/Absent
7. Hemoptysis: Present/Absent
If present- Streaky/frank hemoptysis/pink frothy
8. Fever :
Onset- sudden/insidious
Type- continuous /intermittent/remittent
Accompanied by chills / rigors / sweating
9. Swelling of lower limbs:
Onset- sudden/insidious
Duration.
Pain- present/absent
Diurnal variation- present/absent
Postural variation- present/absent
10. Any other symptoms; Details:
B) Past history:
History of similar complaints
H/O tuberculosis/ asthma/ /allergy/epilepsy/nasal polyps/sinusitis/cardiac
illness/ diabetes mellitus/hypertension/ repeated respiratory infections
in childhood
History of exacerbations:
Number of exacerbations:
Hospitalization was required or not: Yes/ No
Duration of hospitalization:
C) Family history:
History of Asthma/tuberculosis/allergic disease.
No. of family members smoking.
Exposure to smoke (passive smoking) during infancy and childhood.
D) Personal history:
Diet: veg/ nonveg/ mixed
Sleep: Sound/ disturbed
Snoring- present/absent
Early morning headache- present/ absent
Appetite: Normal/decreased/increased
Bowel habits: regular habits/ constipated/loose stools
Habits:
Smoking: Yes/No
ETS or Passive Smoking exposure: Yes/ No
If Yes:
At Home/ work place
Duration of exposure: <3hrs/ >3hrs per day
Years of exposure:
Exposure to bio mass fuels at home or work place: yes/no
Duration of exposure: nature of fuel:
No. of years exposure:
Tobacco chewing: No. of times/day-
Duration
Snuff inhalation: yes/no
Alcohol: Quantity-
Duration- Type-
Occupational exposure to dust/fumes/vapors/smoke/chemicals.
Nature of exposure
Duration of exposure per day: hours per week
Place of living: urban/ rural
Exposure to atmospheric air pollution: present/ absent
E) Menstrual history: regular/irregular.
F) Treatment history: h/o taking any steroids, any beta 2 agonist or any
theophylline derivative.
2. A) GENERAL PHYSICAL EXAMINATION:
Comfortable/dyspnoeic
Built: well built/moderate built/poorly built
Nourishment: well nourished/moderate/poorly
Weight:
Height:
Body mass index:
B) Vital signs
Pulse:
Rate- / min
Rhythm-
Volume-
Condition of the Vessel wall:
Blood Pressure: mm/Hg
Respiration: Rate-
Rhythm
Type
Temperature: °C
Pallor: Present/absent
Cyanosis: Present/absent
Central/ peripheral/mixed
Clubbing: present/absent degree
Koilonychia/platynychia: Present/absent
Icterus: Present/absent
Lymphadenopathy: Present/absent
Oedema: Present/absent
Any other significant signs-
3. SYSTEMIC EXAMINATION:
RESPIRATORY SYSTEM
A) Upper respiratory system:
B) Lower respiratory tract
INSPECTION:
a. Position of the trachea: Central / left / right.
b. Shape of the chest: Normal/ barrel chest/ pigeon chest/ pectus
excavatum / kyphoscoliosis / Harrison’s sulcus /any other chest
deformity.
c. Asymmetry: Bulging/ retraction.
d. Respiratory movements: Normal
Diminished- bilateral / unilateral / localized
e. Respiratory sounds heard: respiratory stridor/ respiratory wheeze
f. Position of the apical impulse:
g.Visible veins over the chest: present/absent
h.Special features to be noted
i.Tracheal descent with inspiration
j.Excessive use of scalene and sternocleidomastoid muscle
PALPATION:
a. Position of the trachea: central/right/left.
b. Position of the apical impulse:
c. Movements of the chest wall- normal / decreased
d. Measurements: during Deep inspiration - cms
Deep expiration - cms
A P diameter - cms
Transverse diameter- cms
Chest expansion- cms
Hemithorax Right- cms
Left- cms
e. Any palpable rhonchi or rub –
f. Vocal fremitus- Normal / increased / decreased
Areasg.
Tenderness over the chest- areas
PERCUSSION:
a. Percussion note: Normal / impaired / hyper resonant / woody dullness/
stony dullness
b. Liver dullness:
c. Cardiac dullness- Normal/ obliterated.
d. Tidal percussion - Normal / diminished
AUSCULTATION:
a. Breath sound: type: NVBS / bronchial / vesicular breath sounds with
prolonged expiration.
b. Air entry: Normal / diminished / absent
c.Rhonchi: Present / absent
d.Crepitation: Present / absent
Inspiratory/expiratory
Fine/coarse
e.Pleural rub: Present / absent
f.Vocal resonance: Normal / increased /decreased
CARDIOVASCULAR SYSTEM:
ABDOMEN:
NERVOUS SYSTEM:
4. INVESTIGATION
BLOOD: Hb%-
TC DC
ESR FBS
PPBS Blood Urea
Serum creatinine
URINE: Albumin- Sugar-
Microscopy-
SPUTUM: Quantity per day-
Colour- Odour-
Blood: present/ absent
Microscopy: Gram stain
AFB stain
CHEST RADIOGRAPH: Report –
SPIROMETRIC PARAMETERS: Pre bronchodilator Post bronchodilator
FVC:
FEV1:
FEV1/FVC:
STATISTICAL METHODS
The collected data was analysed with SPSS 16.0 version. To describe
about the data descriptive statistics frequency analysis, percentage
analysis, mean and S.D were used. To associate the various clinical
variables Chi-Square test was done.In the above statistical tool the
probability value .05 is considered as significant level.
KEY TO MASTER CHART
S.NO-SERIAL NUMBER
ETS-ENVIRONMENTAL TOBACCO EXPOSURE
BMI-BODY MASS INDEX
JVP-JUGULAR VENOUS PULSE
m MRC-MODIFIED MEDICAL RESEARCH COUNCIL
HB –HAEMOGLOBIN
MCV-MEAN CORPUSCULAR VOLUME
MCH-MEAN CORPUSCULAR HAEMOGLOBIN
MCHC- MEAN CORPUSCULAR HAEMOGLOBIN
CONCENTRATION
SEX
1 = MALE
2= FEMALE
AGE
1= 21-30 YRS
2= 31- 40 YRS
3= 41-50YRS
4= 51-60 YRS
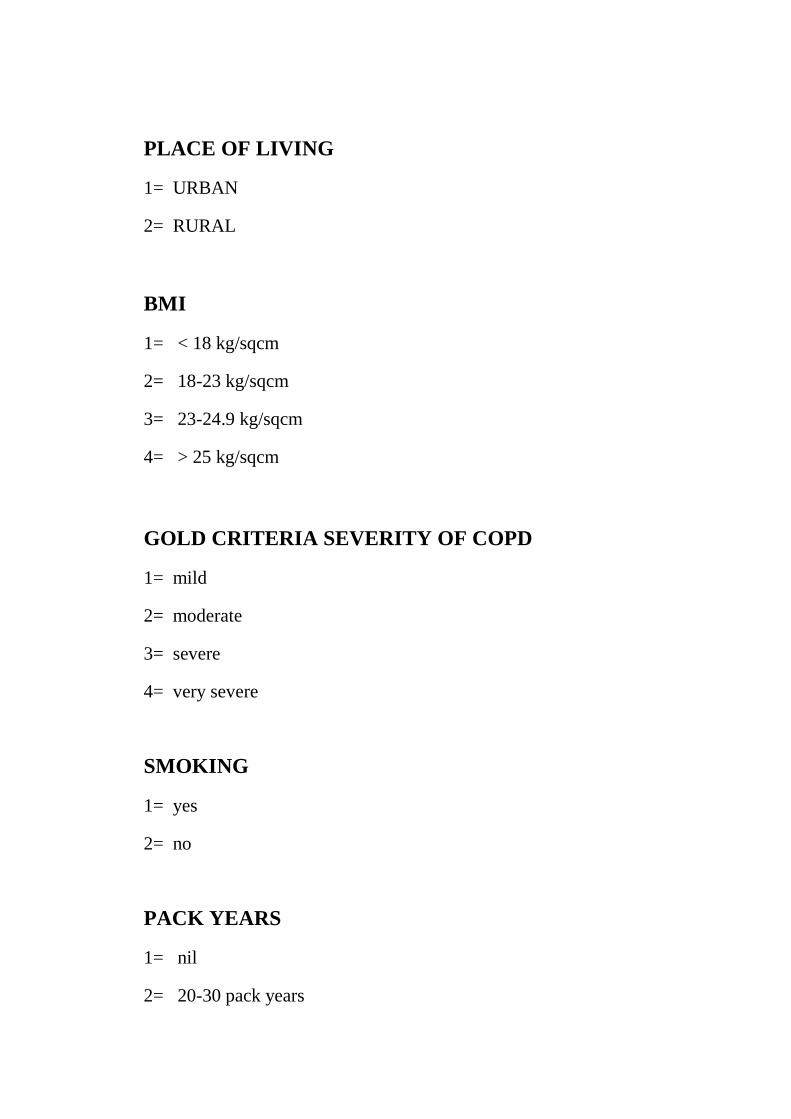
PLACE OF LIVING
1= URBAN
2= RURAL
BMI
1= < 18 kg/sqcm
2= 18-23 kg/sqcm
3= 23-24.9 kg/sqcm
4= > 25 kg/sqcm
GOLD CRITERIA SEVERITY OF COPD
1= mild
2= moderate
3= severe
4= very severe
SMOKING
1= yes
2= no
PACK YEARS
1= nil
2= 20-30 pack years
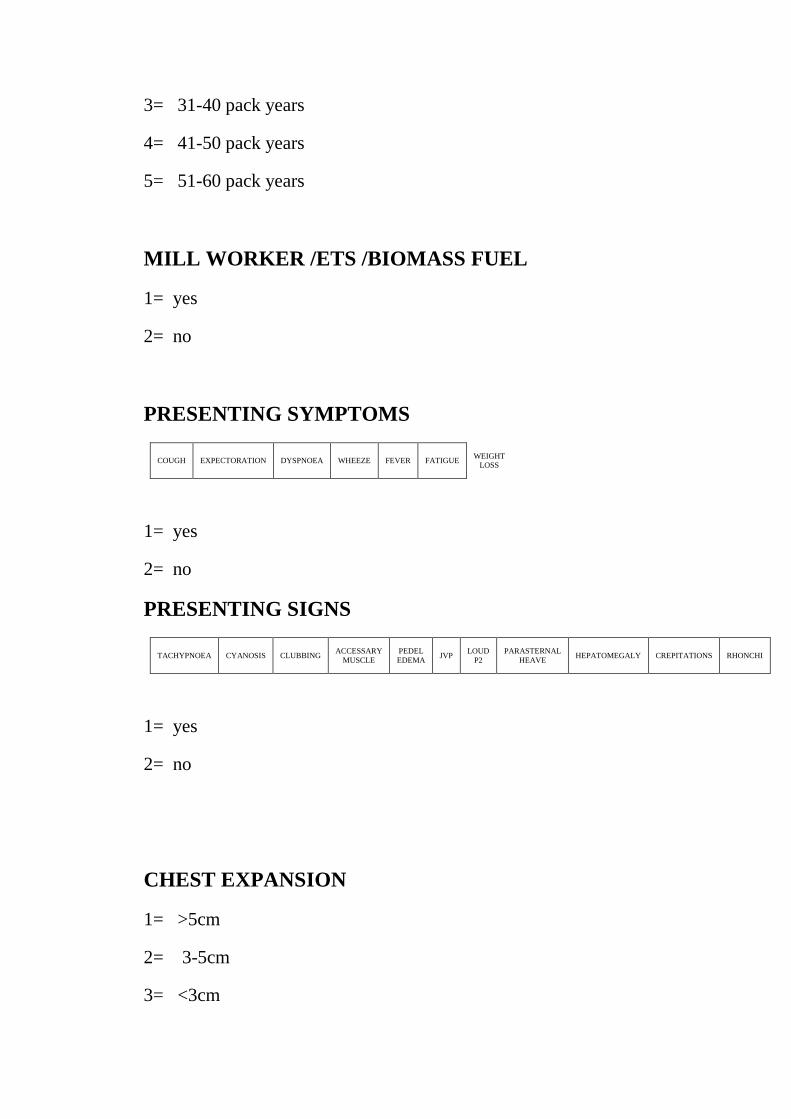
3= 31-40 pack years
4= 41-50 pack years
5= 51-60 pack years
MILL WORKER /ETS /BIOMASS FUEL
1= yes
2= no
PRESENTING SYMPTOMS
COUGH EXPECTORATION DYSPNOEA WHEEZE FEVER FATIGUE WEIGHT
LOSS
1= yes
2= no
PRESENTING SIGNS
TACHYPNOEA CYANOSIS CLUBBING ACCESSARY
MUSCLE
PEDEL
EDEMA JVP
LOUD
P2
PARASTERNAL
HEAVE HEPATOMEGALY CREPITATIONS RHONCHI
1= yes
2= no
CHEST EXPANSION
1= >5cm
2= 3-5cm
3= <3cm
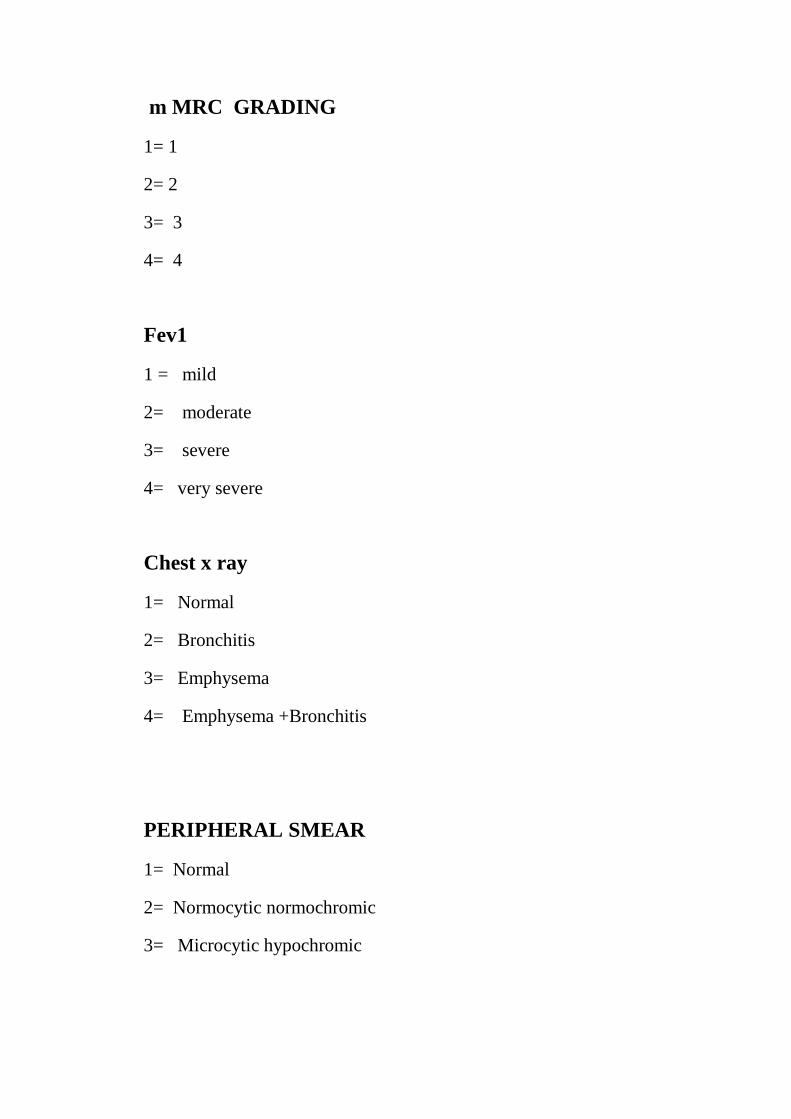
m MRC GRADING
1= 1
2= 2
3= 3
4= 4
Fev1
1 = mild
2= moderate
3= severe
4= very severe
Chest x ray
1= Normal
2= Bronchitis
3= Emphysema
4= Emphysema +Bronchitis
PERIPHERAL SMEAR
1= Normal
2= Normocytic normochromic
3= Microcytic hypochromic
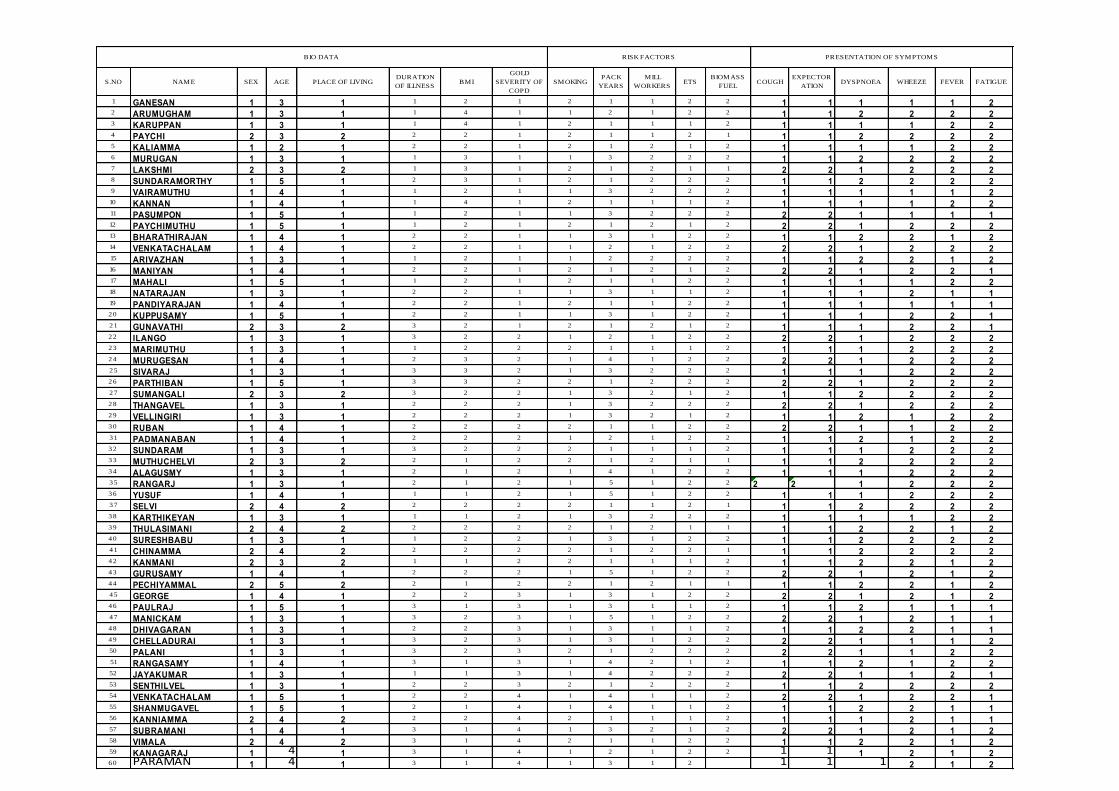
S.NO NAME SEX AGE PLACE OF LIVINGDURATION
OF ILLNESSBMI
GOLD
SEVERITY OF
COPD
SMOKINGPACK
YEARS
MILL
WORKERSETS
BIOMASS
FUELCOUGH
EXPECTOR
ATIONDYSPNOEA WHEEZE FEVER FATIGUE
1 GANESAN 1 3 1 1 2 1 2 1 1 2 2 1 1 1 1 1 22 ARUMUGHAM 1 3 1 1 4 1 1 2 1 2 2 1 1 2 2 2 23 KARUPPAN 1 3 1 1 4 1 2 1 1 1 2 1 1 1 1 2 24 PAYCHI 2 3 2 2 2 1 2 1 1 2 1 1 1 2 2 2 25 KALIAMMA 1 2 1 2 2 1 2 1 2 1 2 1 1 1 1 2 26 MURUGAN 1 3 1 1 3 1 1 3 2 2 2 1 1 2 2 2 27 LAKSHMI 2 3 2 1 3 1 2 1 2 1 1 2 2 1 2 2 28 SUNDARAMORTHY 1 5 1 2 3 1 2 1 2 2 2 1 1 2 2 2 29 VAIRAMUTHU 1 4 1 1 2 1 1 3 2 2 2 1 1 1 1 1 210 KANNAN 1 4 1 1 4 1 2 1 1 1 2 1 1 1 1 2 211 PASUMPON 1 5 1 1 2 1 1 3 2 2 2 2 2 1 1 1 112 PAYCHIMUTHU 1 5 1 1 2 1 2 1 2 1 2 2 2 1 2 2 213 BHARATHIRAJAN 1 4 1 2 2 1 1 3 1 2 2 1 1 2 2 1 214 VENKATACHALAM 1 4 1 2 2 1 1 2 1 2 2 2 2 1 2 2 215 ARIVAZHAN 1 3 1 1 2 1 1 2 2 2 2 1 1 2 2 1 216 MANIYAN 1 4 1 2 2 1 2 1 2 1 2 2 2 1 2 2 117 MAHALI 1 5 1 1 2 1 2 1 1 2 2 1 1 1 1 2 218 NATARAJAN 1 3 1 2 2 1 1 3 1 1 2 1 1 1 2 1 119 PANDIYARAJAN 1 4 1 2 2 1 2 1 1 2 2 1 1 1 1 1 120 KUPPUSAMY 1 5 1 2 2 1 1 3 1 2 2 1 1 1 2 2 121 GUNAVATHI 2 3 2 3 2 1 2 1 2 1 2 1 1 1 2 2 122 ILANGO 1 3 1 3 2 2 1 2 1 2 2 2 2 1 2 2 223 MARIMUTHU 1 3 1 1 2 2 2 1 1 1 2 1 1 1 2 2 224 MURUGESAN 1 4 1 2 3 2 1 4 1 2 2 2 2 1 2 2 225 SIVARAJ 1 3 1 3 3 2 1 3 2 2 2 1 1 1 2 2 226 PARTHIBAN 1 5 1 3 3 2 2 1 2 2 2 2 2 1 2 2 227 SUMANGALI 2 3 2 3 2 2 1 3 2 1 2 1 1 2 2 2 228 THANGAVEL 1 3 1 2 2 2 1 3 2 2 2 2 2 1 2 2 229 VELLINGIRI 1 3 1 2 2 2 1 3 2 1 2 1 1 2 1 2 230 RUBAN 1 4 1 2 2 2 2 1 1 2 2 2 2 1 1 2 231 PADMANABAN 1 4 1 2 2 2 1 2 1 2 2 1 1 2 1 2 232 SUNDARAM 1 3 1 3 2 2 2 1 1 1 2 1 1 1 2 2 233 MUTHUCHELVI 2 3 2 2 1 2 2 1 2 1 1 1 1 2 2 2 234 ALAGUSMY 1 3 1 2 1 2 1 4 1 2 2 1 1 1 2 2 235 RANGARJ 1 3 1 2 1 2 1 5 1 2 2 2 2 1 2 2 236 YUSUF 1 4 1 1 1 2 1 5 1 2 2 1 1 1 2 2 237 SELVI 2 4 2 2 2 2 2 1 1 2 1 1 1 2 2 2 238 KARTHIKEYAN 1 3 1 1 1 2 1 3 2 2 2 1 1 1 1 2 239 THULASIMANI 2 4 2 2 2 2 2 1 2 1 1 1 1 2 2 1 240 SURESHBABU 1 3 1 1 2 2 1 3 1 2 2 1 1 2 2 2 241 CHINAMMA 2 4 2 2 2 2 2 1 2 2 1 1 1 2 2 2 242 KANMANI 2 3 2 1 1 2 2 1 1 1 2 1 1 2 2 1 243 GURUSAMY 1 4 1 2 2 2 1 5 1 2 2 2 2 1 2 1 244 PECHIYAMMAL 2 5 2 2 1 2 2 1 2 1 1 1 1 2 2 1 245 GEORGE 1 4 1 2 2 3 1 3 1 2 2 2 2 1 2 1 246 PAULRAJ 1 5 1 3 1 3 1 3 1 1 2 1 1 2 1 1 147 MANICKAM 1 3 1 3 2 3 1 5 1 2 2 2 2 1 2 1 148 DHIVAGARAN 1 3 1 2 2 3 1 3 1 1 2 1 1 2 2 1 149 CHELLADURAI 1 3 1 3 2 3 1 3 1 2 2 2 2 1 1 1 250 PALANI 1 3 1 3 2 3 2 1 2 2 2 2 2 1 1 2 251 RANGASAMY 1 4 1 3 1 3 1 4 2 1 2 1 1 2 1 2 252 JAYAKUMAR 1 3 1 1 1 3 1 4 2 2 2 2 2 1 1 2 153 SENTHILVEL 1 3 1 2 2 3 2 1 2 2 2 1 1 2 2 2 254 VENKATACHALAM 1 5 1 2 2 4 1 4 1 1 2 2 2 1 2 2 155 SHANMUGAVEL 1 5 1 2 1 4 1 4 1 1 2 1 1 2 2 1 156 KANNIAMMA 2 4 2 2 2 4 2 1 1 1 2 1 1 1 2 1 157 SUBRAMANI 1 4 1 3 1 4 1 3 2 1 2 2 2 1 2 1 258 VIMALA 2 4 2 3 1 4 2 1 1 2 2 1 1 2 2 1 259 KANAGARAJ 1 4 1 3 1 4 1 2 1 2 2 1 1 1 2 1 260 PARAMAN 1 4 1 3 1 4 1 3 1 2 1 1 1 2 1 2
BIO DATA RISK FACTORS PRESENTATION OF SYMPTOMS

S.NO NAMEWEIGHT
LOSSTACHYPNOEA CYANOSIS CLUBBING
ACCESSARY
MUSCLE
PEDEL
EDEMAJVP
LOUD
P2
PARASTERNAL
HEAVE
HEPATO
MEGALY
CREPITA
TIONSRHONCHI
CHEST
EXPANSI
ON
mMRC
GRADEFEV1
CHEST X-
RAYHB % HCT MCV MCH MCHC
PERIPHERAL
SMEAR
1 GANESAN 1 1 2 2 2 2 2 2 2 2 1 1 1 1 2 .02 2 12 .4 45.9 81 28 32 .4 1
2 ARUMUGHAM 2 1 2 2 2 2 2 2 2 2 1 1 1 3 1.98 2 13 .4 43 .5 86 28 .6 34 .4 1
3 KARUPPAN 2 1 2 2 2 2 2 2 2 2 1 1 1 3 1.66 2 12 .8 40 .6 95 30 34 .6 1
4 PAYCHI 2 1 2 2 2 2 2 2 2 2 1 1 1 2 1.6 2 14 .4 43 .6 88 31 35.4 1
5 KALIAMMA 2 2 2 2 2 2 2 2 2 2 1 1 1 1 2 2 15 42 .2 96 32 32 1
6 MURUGAN 2 1 2 2 2 2 2 2 2 2 1 1 1 1 1.7 1 8 .6 43 56 25 28 .8 3
7 LAKSHMI 2 1 2 2 2 2 2 2 2 2 1 1 1 1 1.86 2 11.2 44 67 24 .6 27.8 3
8 SUNDARAMORTHY 2 2 2 2 2 2 2 2 2 2 1 1 1 1 1.72 3 15.2 45.2 90 30 36 1
9 VAIRAMUTHU 2 2 2 2 2 2 2 2 2 2 1 2 1 1 1.66 2 16 .6 43 .6 89 31 32 .4 1
10 KANNAN 2 2 2 2 2 2 2 2 2 2 2 2 1 2 1.8 2 11 40 .2 90 .4 29 .6 32 .8 1
11 PASUMPON 2 2 2 2 2 2 2 2 2 2 2 2 1 3 1.52 2 10 .8 40 .4 70 23 27.6 3
12 PAYCHIMUTHU 1 2 2 2 2 2 2 2 2 2 2 2 1 2 2 3 13 40 .6 89 29 .4 32 1
13 BHARATHIRAJAN 1 2 2 2 2 2 2 2 2 2 2 1 1 2 2 .02 2 12 .4 40 .8 89 30 .4 33 1
14 VENKATACHALAM 1 2 2 2 2 2 2 2 2 2 2 2 2 1 2 1 13 43 .4 88 30 .2 34 1
15 ARIVAZHAN 2 1 2 2 2 2 2 2 2 2 2 2 2 1 2 1 15 43 .8 92 .4 31.8 35.4 1
16 MANIYAN 2 1 2 2 1 2 2 2 2 2 2 2 2 3 1.98 2 14 44 93 28 .8 35.6 1
17 MAHALI 2 1 2 2 1 2 2 2 2 2 1 2 2 3 1.78 3 13 40 90 .2 29 .2 35.8 1
18 NATARAJAN 2 1 2 2 2 2 2 2 2 2 1 1 2 2 1.9 1 14 40 .6 93 32 34 .2 1
19 PANDIYARAJAN 2 1 2 2 2 2 2 2 2 2 1 1 2 3 1.88 3 13 40 .7 87.4 31.6 34 .6 1
2 0 KUPPUSAMY 2 1 2 2 2 2 2 2 2 2 2 1 2 2 1.68 1 11.2 40 .2 82 .7 32 34 .8 2
21 GUNAVATHI 2 1 2 2 1 2 2 2 2 2 2 1 2 2 1.58 4 9 42 .4 69 22 .8 30 .2 3
2 2 ILANGO 2 2 2 2 1 2 2 2 2 2 2 1 1 3 0 .9 3 13 43 .8 88 .8 32 34 .8 1
2 3 MARIMUTHU 2 2 2 2 1 2 2 2 2 2 2 1 2 3 1.22 3 8 .6 44 .4 74 24 .2 31.2 3
2 4 MURUGESAN 2 2 1 2 1 2 2 2 2 2 2 1 2 2 1.34 2 12 43 .2 92 .6 31.4 32 1
25 SIVARAJ 2 2 1 2 1 2 2 2 2 2 2 1 2 2 1.22 2 16 42 .5 88 32 32 .8 1
2 6 PARTHIBAN 2 2 2 2 1 2 2 2 2 2 1 1 2 2 1.4 2 11.4 42 .6 90 32 32 .8 2
27 SUMANGALI 2 1 2 2 1 2 2 2 2 2 1 1 2 2 1.36 4 8 42 .8 76 .8 20 .8 28 .8 3
2 8 THANGAVEL 2 1 2 2 1 2 2 2 2 2 1 2 2 2 1.38 3 11.2 42 .6 80 .4 32 .4 32 .4 2
2 9 VELLINGIRI 2 1 2 2 2 2 2 2 2 2 1 2 2 2 1.4 4 10 44 88 32 34 .2 2
3 0 RUBAN 1 1 1 2 1 2 2 2 2 2 2 2 2 2 1.48 3 12 43 .6 92 .5 32 34 .8 1
31 PADMANABAN 2 2 1 2 2 2 2 2 2 2 2 2 2 2 1.44 3 9 .8 42 .8 77 2O.4 29 .6 3
3 2 SUNDARAM 1 2 1 2 2 2 2 2 2 2 2 2 2 2 1.06 3 8 42 .7 88 .5 31 36 2
3 3 MUTHUCHELVI 2 2 2 2 1 2 2 2 2 2 1 2 2 2 0 .94 3 6 .6 44 75 23 .8 30 3
3 4 ALAGUSMY 2 1 1 2 1 2 2 2 2 2 1 2 2 2 0 .88 4 14 43 .4 90 .2 28 35.4 1
35 RANGARJ 2 1 2 2 1 2 2 2 2 2 1 2 2 2 0 .98 3 13 45 91.4 32 36 .2 2
3 6 YUSUF 2 1 1 2 2 2 2 2 2 2 1 1 2 2 1.28 3 12 44 .2 91 32 .4 34 .6 1
37 SELVI 1 1 2 2 2 2 2 2 2 2 1 1 2 3 1.36 4 16 44 .8 93 .6 28 .8 34 .6 1
3 8 KARTHIKEYAN 1 1 2 2 2 2 2 2 2 2 2 1 2 2 1.34 3 9 44 .2 86 .8 28 31.8 2
3 9 THULASIMANI 2 2 2 2 2 2 2 2 2 2 2 1 2 3 1.12 3 15 42 .2 95 28 34 .4 1
4 0 SURESHBABU 2 2 2 1 2 2 2 2 2 2 1 1 2 3 1.24 3 12 .2 43 .6 87.6 29 .4 34 .2 1
41 CHINAMMA 1 1 1 1 2 2 2 2 2 2 1 1 2 2 1.28 4 10 42 .6 86 .7 30 .4 28 .8 2
4 2 KANMANI 1 1 2 2 1 2 2 2 1 1 1 1 2 2 1.24 4 11.4 44 .4 89 .2 32 31.8 2
4 3 GURUSAMY 2 1 2 2 1 2 2 1 1 1 1 1 2 2 1.48 4 12 43 90 .6 32 35 1
4 4 PECHIYAMMAL 1 1 1 2 1 2 2 1 1 1 1 1 2 2 1.36 4 10 .8 43 .6 89 .6 31.4 31.4 2
45 GEORGE 1 1 1 1 2 2 2 1 2 2 1 2 3 3 1.34 4 12 43 .8 89 30 .4 34 1
4 6 PAULRAJ 1 1 1 1 2 2 2 1 2 2 1 2 3 4 1.24 3 11 43 .3 88 .8 30 .6 31.4 2
47 MANICKAM 1 1 1 1 1 1 2 2 2 2 1 1 3 3 1.02 4 11 43 .6 88 .4 30 .8 32 2
4 8 DHIVAGARAN 2 1 1 1 1 1 1 2 2 2 1 1 2 3 0 .94 3 10 .8 46 .8 84 29 .8 32 2
4 9 CHELLADURAI 1 1 1 2 1 1 1 1 2 2 1 1 3 3 0 .92 4 7.6 45 82 .2 28 .4 32 .8 2
50 PALANI 2 1 1 2 1 1 1 1 2 2 1 1 2 4 0 .88 3 9 .8 43 .8 88 28 .4 32 .4 2
51 RANGASAMY 1 1 1 2 1 1 1 1 1 2 1 1 3 4 0 .98 4 7.8 44 .8 92 28 .8 32 .4 2
52 JAYAKUMAR 2 1 1 1 2 1 1 2 2 2 1 1 2 3 1 3 8 .6 44 .2 92 .4 28 .8 32 2
53 SENTHILVEL 1 1 1 1 1 1 1 2 2 2 1 1 3 4 0 .65 3 14 42 .4 94 29 .6 34 I
54 VENKATACHALAM 2 1 1 1 1 1 1 2 2 2 1 1 3 4 0 .66 4 9 .6 43 86 .4 29 .8 34 .4 2
55 SHANMUGAVEL 1 1 1 2 1 1 1 2 2 2 1 1 3 3 0 .58 3 11 43 .4 88 29 .4 34 .8 2
56 KANNIAMMA 1 1 1 2 1 1 1 1 2 2 1 1 3 4 0 .62 2 10 .4 45.2 86 .2 28 .4 35 2
57 SUBRAMANI 1 1 1 2 1 1 1 1 2 2 1 1 3 3 0 .5 3 9 44 .2 89 .8 28 .4 34 2
58 VIMALA 1 1 1 2 1 1 1 1 2 2 1 1 3 4 0 .46 4 8 .4 44 .4 94 28 .4 32 .4 2
59 KANAGARAJ 1 1 1 2 1 1 1 1 2 2 1 1 2 4 0 .51 4 6 .6 43 .2 92 29 .4 32 .2 2
6 0 PARAMAN 1 1 1 2 1 1 1 1 2 2 1 1 3 3 0 .48 3 7.8 42 .2 86 29 .8 32 .4 2
HAEMATOLOGICALBIO DATA PRESENTATION OF SIGNS

INFORMED CONSENT
Department of General Medicine
COIMBATORE MEDICAL COLLEGE, COIMBATORE
Principal Investigator : Dr. M. Gowri Sankar
Research Guide : Dr.S.Usha.M.D
Organization : Department of General Medicine
Informed consent: I have been invited to participate in research project
titled “HAEMATOLOGICAL MANIFESTATIONS IN
CHRONIC OBSTRUCTIVE LUNG DISEASE IN
RELATION TO FEV1
IN COIMBATORE MEDICAL COLLEGE HOSPITAL”, I
understand, I will be answering a set of questionnaire, undergo physical
examination, investigation and appropriate treatment. I also give consent
to utilize my personal details for study purpose and can be contacted if
necessary.
I am aware that I have the right to withdraw at any time which will not
affect my medical care.
Name of the participant:
Signature:
Date:
xg;Gjy; gbtk;
ngah; :
ghypdk; : taJ:
Kfthp :
muR Nfhit kUj;Jtf; fy;Y}hpapy; nghJ kUj;Jtj; Jiwapy;
gl;l Nkw;gbg;G gapYk; khzth; Nkw;nfhs;Sk; “%r;Rf;Foy;fs;
milg;G fhuzkhf Kjy;; nehbapy; ntspj;js;Sk; %r;rpd; msitg;
nghWj;Jk; kw;Wk; EiuaPuypd; khWjypdhYk; ,uj;jj;jpy; Vw;gLk;
tpisTfs;” Fwpj;j Ma;tpy; nra;Kiw kw;Wk; midj;J
tptuq;fisAk; Nfl;Lf; nfhz;L vdJ re;Njfq;fis njspTgLj;jpf;
nfhz;Nld; vd;gij njhptpj;Jf; nfhs;fpNwd;.
ehd; ,e;j Ma;tpy; KO rk;kjj;JlDk;> Ra rpe;jidAlDk;
fye;J nfhs;s rk;kjpf;fpNwd;.
,e;j Ma;tpy; vd;Dila midj;J tpguq;fs;
ghJfhf;fg;gLtJld; ,jd; KbTfs; Ma;tpjopy; ntspaplg;gLtjpy;
Ml;Nrgid ,y;iy vd;gij njhptpj;Jf; nfhs;fpNwd;. ve;j
Neuj;jpYk; ,e;j Ma;tpypUe;J ehd; tpyfpf; nfhs;s vdf;F chpik
cz;L vd;gijAk; mwpNtd;.
,lk;: ifnahg;gk; / Nuif
ehs;: