collection department team ward prince of wales hospital · prince of wales hospital date of...
TRANSCRIPT
M&M Data Collection FormDepartment of SurgeryPrince of Wales Hospital
Date of M&M meeting:
Team 4
(dd/mm/yyyy)
Ward
(
Type of case Particulars Discharge Summary (please include dates and name of procedures, clinicalcourses and causes of death)
c
t
l¿t-I
Name: Ld ,
Sex / Age. ¡rr\ | 6q,
HKID
Ward / Bed No..
For mortality cases:
Referred to Coroner?
/Y"t ì*' tloExpected deaSh?
l* Yes Ø no
For morbidity cases:
Complicationsnecessitatelnterventional Radiologyprocedures?
[- Yes í: No
Complicationsnecessitate ICUadmission?
[* Yes l* no
Complicationsnecessitatere-operation?
ñ Yes f'- t'lo
ls this case aincident?
+ r,¡ YESI
medical
No
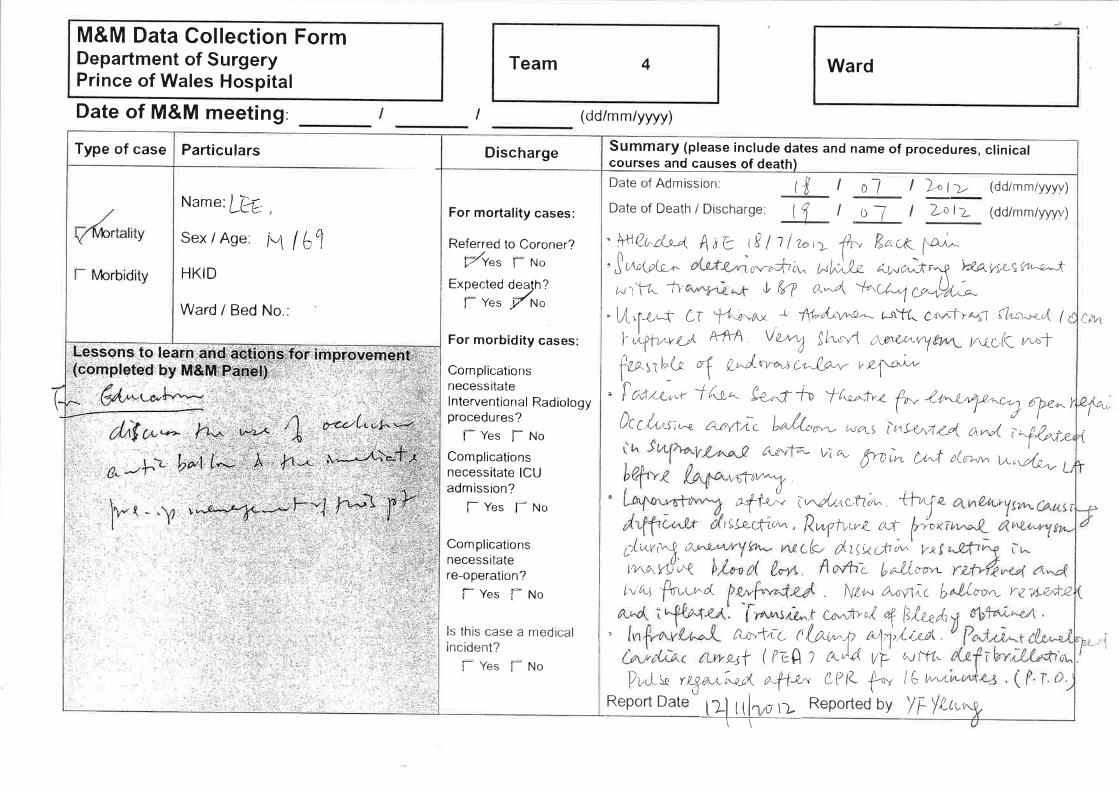
Date of Admission: l, I I o1 I )," t -¿. (dd/mm/yyyy)
DateofDeath/Discharge: ll I Ol I 'l,,pl> (dd/mm/yyyy)
" !48rc1"-t A¡e i8 I 1 lzo,> frn B"X ¡a"^,l¿n{7þ-,- c- lo.fi¿,u
^È"At ¿.r,.vr.ùc-.V YkLw(,St'r+ç,-*
¿.-,lV- t'r- I íç? o'.ø l¿'( ,/-*1 Lo.-vÒrL.t -
" L,{'f-¿q ti- 'f4.c-'.ao + l\t-a|*"'a,- þìTú. c¿v"1>¿*T flu¡r^.n"",( 1c
I J..yf^nrtt A-frA Vu1 !/.-o4 úuØùe+ty ¿,vc.K ru-t
føsal,-l-o \ l,^'J'nr",t, Òç'Lo-""' ,4*, ?ó"-L.u,"r ifa,-. 1et.ç-t-v 't[,e.Jv
þ Z4-,1-*y,L,c.t] ¿?z^)ÒtC.l-r-uç¡r* r^øvfic lraftr,r^- iu,,rs ì¡S<r,424 an
^L1^.t"'¡72- vì o- ffrtin t¿-t ,rr-, Urr',ffJi
@'*f^+f..- i-çLt<cüà^'tir.i
rllzcfic;vr , R,,,r,þ.rrL o-f- tlrÞ
¿l*vt\.o" .(<, d,tiççfiì,w' lrtLtno,ç{vj Z b^,L(m-*L^'u-5'þçv-¿1 N!,+-t \u¡|lìc b /.¿'¿'".- ).¿TLÊ,\,+j2
.t ce.^À>,.( q [|fu"Å,, /Lc*I,tc (Ur,* ,!1),,,¿r^ut (¿e û ? &Jd, vi: ¿";rrø.
Pi,rL.v yr-+€,,.4-r'!J/< afi-2,' ¿Pla t"v i3 t-.tReport Date t?ì tthr r> Reporred by y"l,f !-te'.y
ù4
/-,,
,'t
l?ì I tl1,r-r ìr.____1___r-
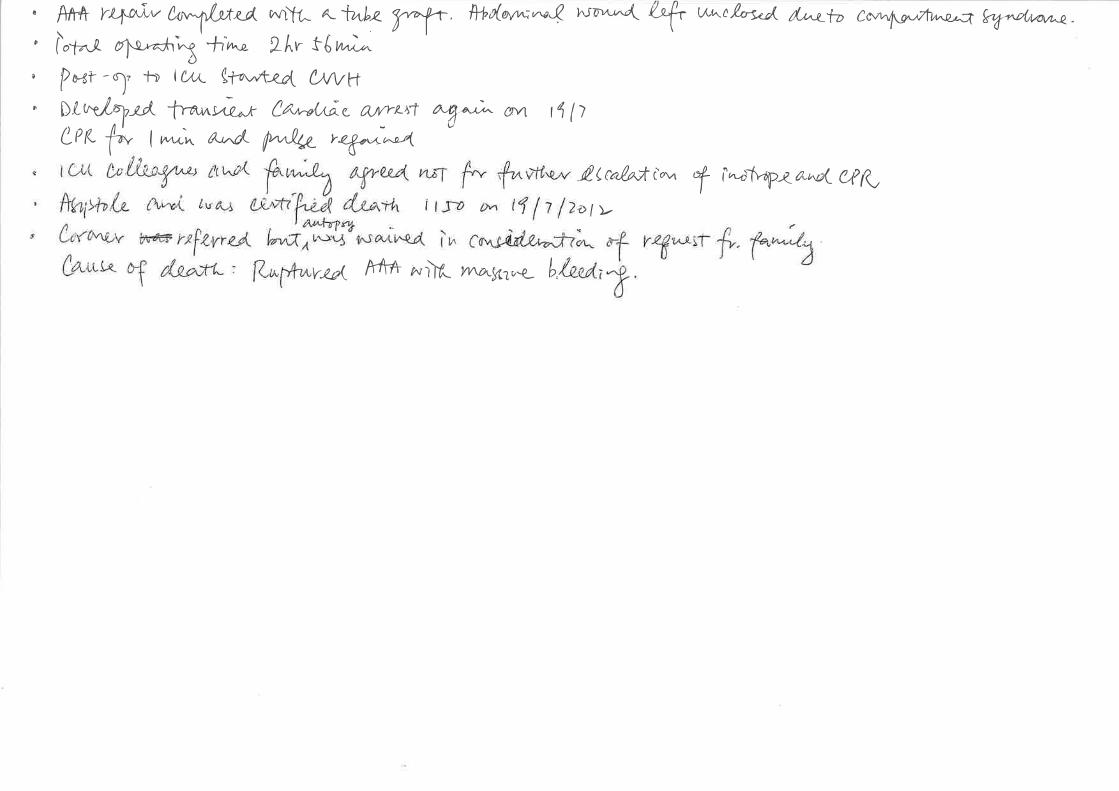
" Ê,T+ fr4o,i"v U,-"{-tt4i,0^rttL a-fwhz fY #Þt(ølt^,"-.Q rua''^,^,rl (+ u''^t,bço& ^.1"4--t-D
cav^l\E-,trwa}d e%.,,e(rrwa"
' lot^i. o}",-h\ 4-,"t^n 2/.,r t6 h";^
' P*r -I, t) tuu_ gflr,*¿^ cvvvi' DLÞ:e,lnij, -lmnu*-,r ¿^tu^s,('@s aLaftatJ "t"u;, eÌ\4 l4lì
Cerc þ I ^ìn a,*c/,- NA- r%¿'t^e4
de c"/.v,tt'- Y i"-f\-dp{ a-^d- e,pK
Ðl>.
uts( A-fff- zuùÂ /vwuf,1v*- b.
Mortality CaseLYF 67/M
Team 427/12/2012
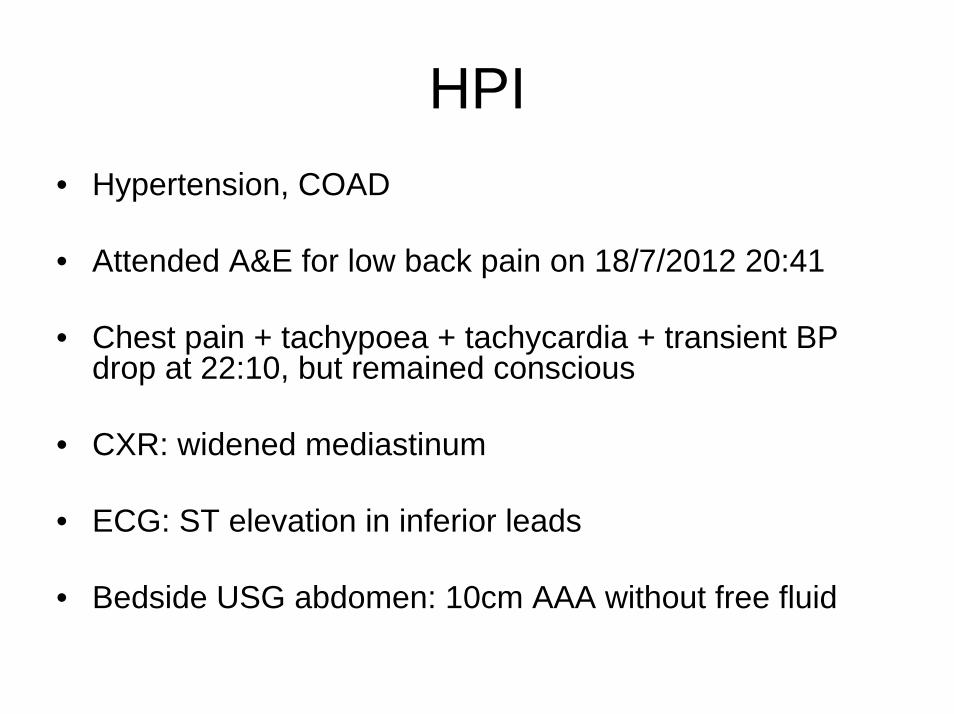
HPI• Hypertension, COAD
• Attended A&E for low back pain on 18/7/2012 20:41
• Chest pain + tachypoea + tachycardia + transient BP drop at 22:10, but remained conscious
• CXR: widened mediastinum
• ECG: ST elevation in inferior leads
• Bedside USG abdomen: 10cm AAA without free fluid
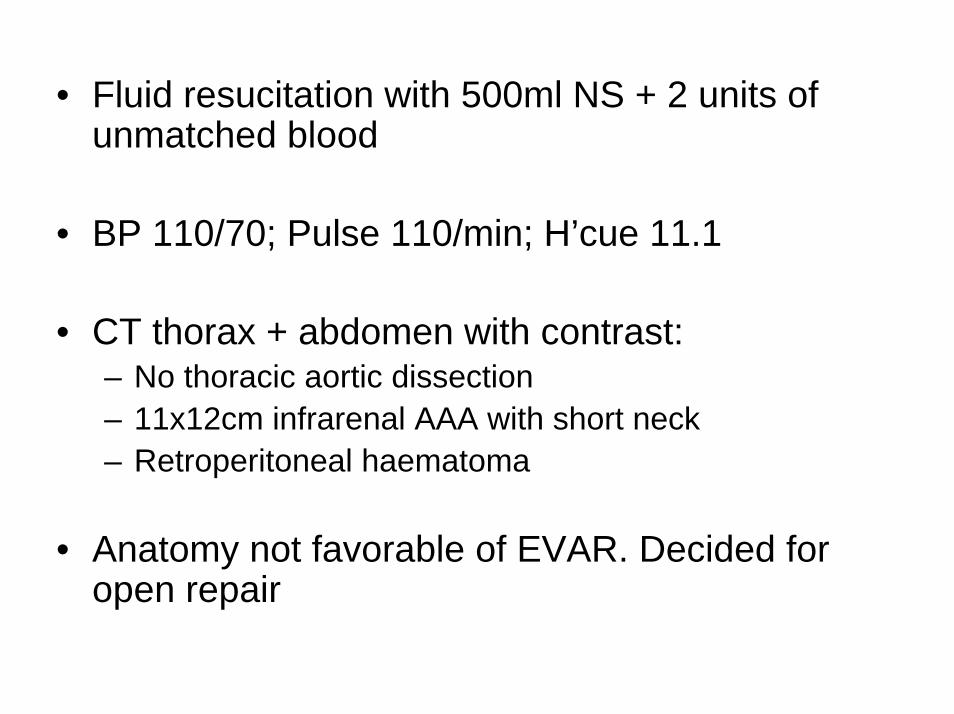
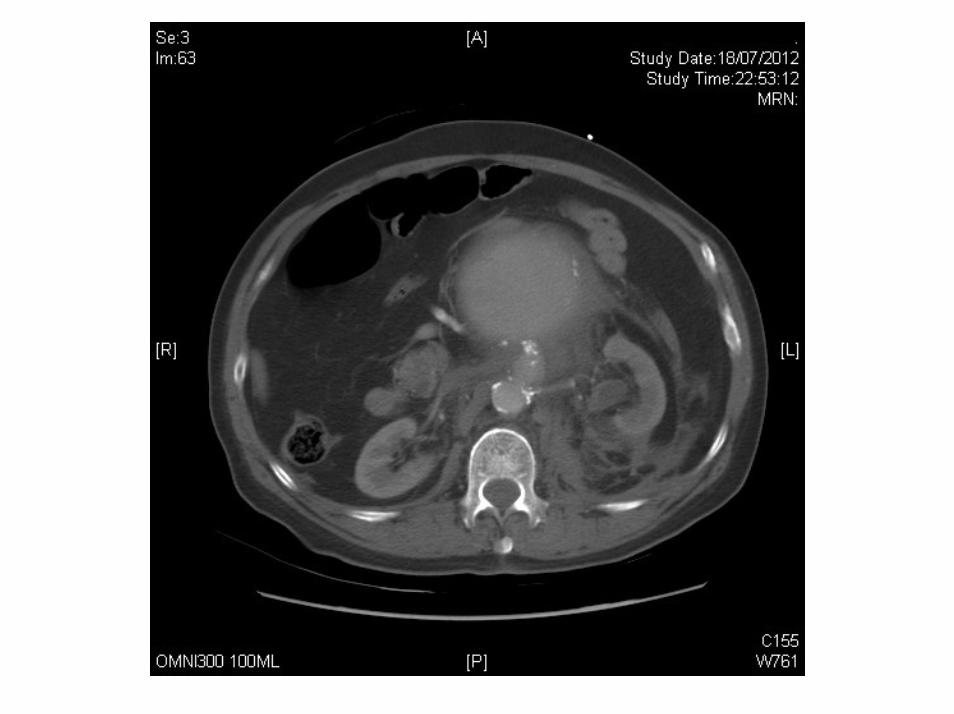
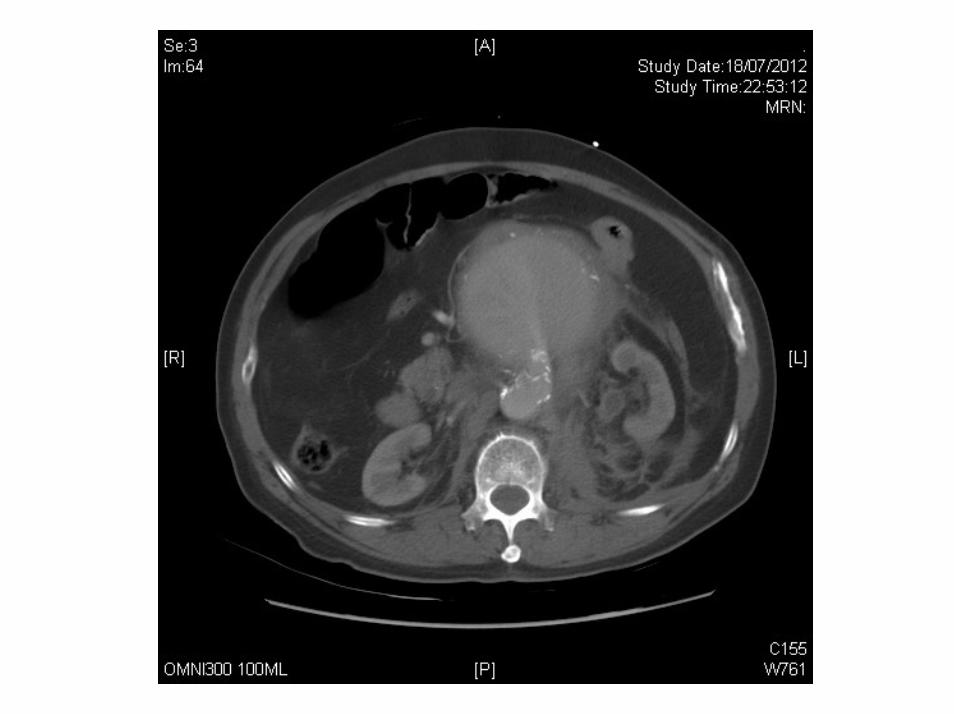
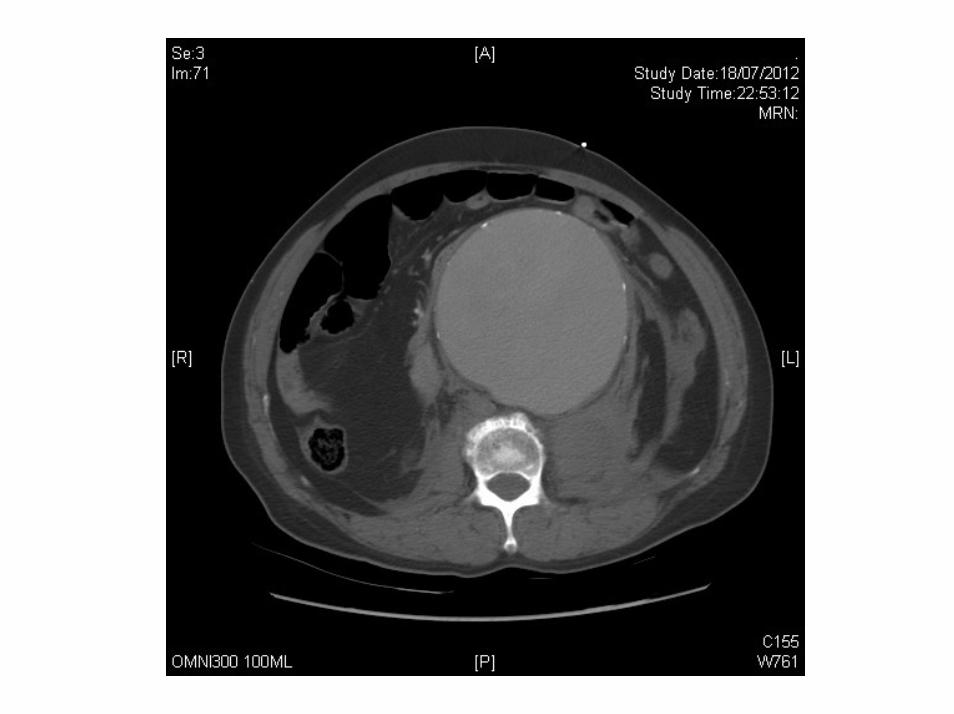
• Fluid resucitation with 500ml NS + 2 units of unmatched blood
• BP 110/70; Pulse 110/min; H’cue 11.1
• CT thorax + abdomen with contrast: – No thoracic aortic dissection– 11x12cm infrarenal AAA with short neck– Retroperitoneal haematoma
• Anatomy not favorable of EVAR. Decided for open repair

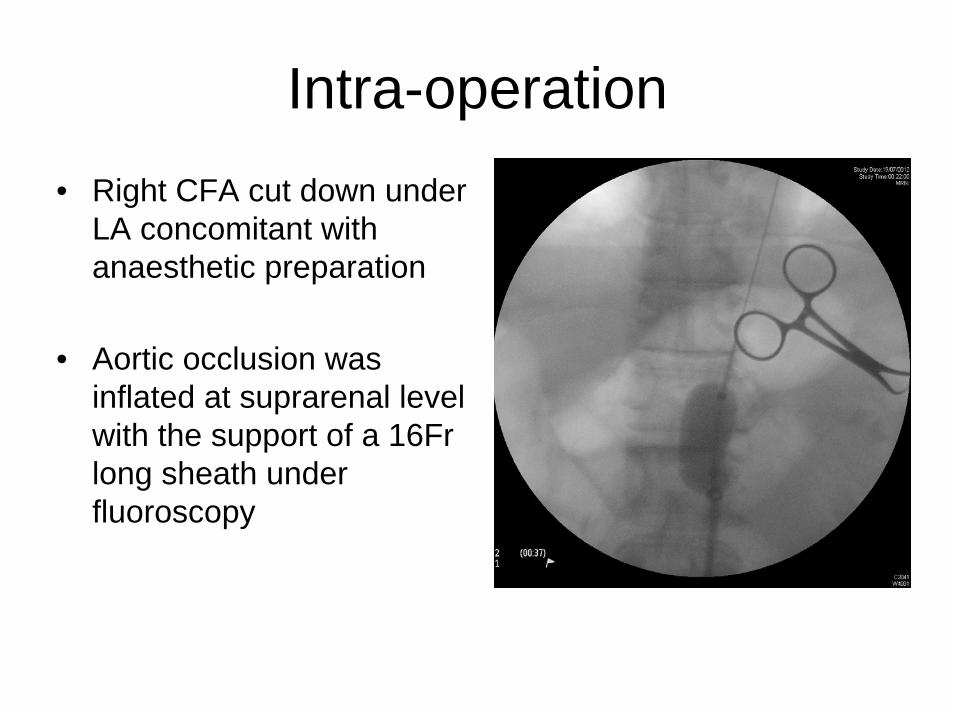
Intra-operation• Right CFA cut down under
LA concomitant with anaesthetic preparation
• Aortic occlusion was inflated at suprarenal level with the support of a 16Fr long sheath under fluoroscopy
Intra-operation• Midline laparotomy after induction
• Rupture at aneurysm neck during dissection resulting in massive bleeding
• Aortic balloon retrieved and was found burst
• Reinsertion of another aortic balloon with bleeding under control
• Developed VF and PEA. Regained pulses after cardioversion and CPR for 16 min
Intra-operation• Infrarenal aortic clamp on after further dissection of aortic
neck
• 16mm tube graft
• Difficult ventilation upon closure of fascia
• Transfer to ICU with laparostomy
• Operation time: 2hr 56min. Blood loss 4500ml
• 10 units of packed cell; 16 units of FFP; 16 units of platelet conc
Post-operation• Multi-organ failure. Started CVVH in ICU
• Developed transient cardiac arrest again on 19/7 required CPR for 1 minute
• ICU and family agreed not for escalation of treatment
• Succumbed at 1150 on 19/7/2012
• Coroner referred. Autopsy was waived.
• Cause of death: Ruptured AAA with massive bleeding
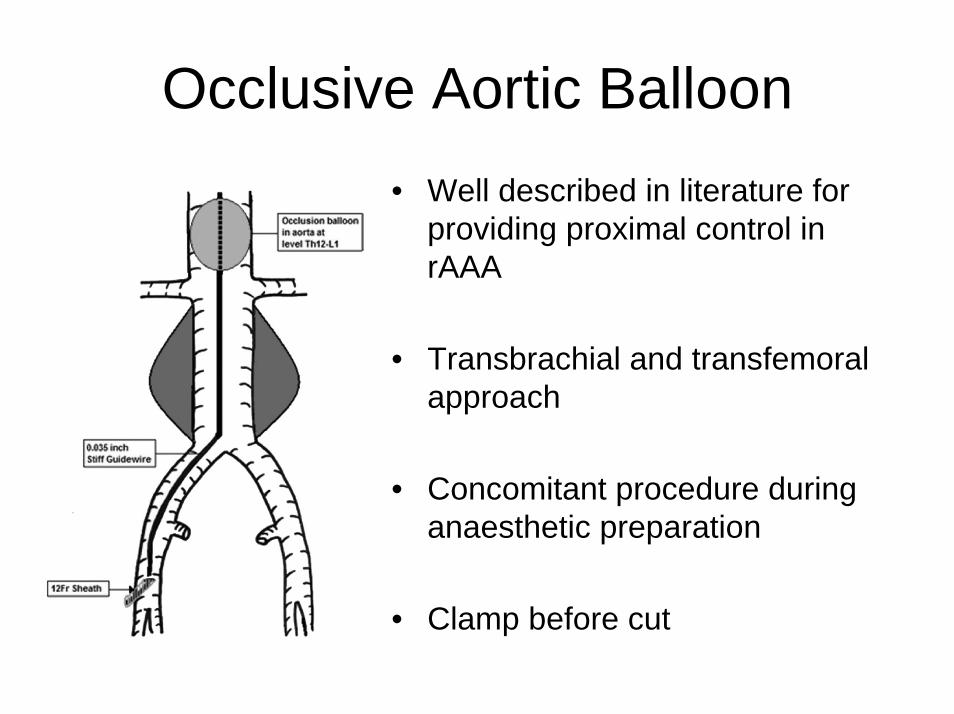
Occlusive Aortic Balloon• Well described in literature for
providing proximal control in rAAA
• Transbrachial and transfemoralapproach
• Concomitant procedure during anaesthetic preparation
• Clamp before cut
Occlusive Aortic Balloon• Bursting of balloon is one of the known
complication
• Related to disease in aortic wall e.g. calcified plaque, mural thrombus
• Associate with high mortality
• To prevent bursting:– Avoid inflation in diseased area– Avoid over-inflation
Date
Team
Presenter
Patient Name
Sex
M & M Meetinq
Thursday 27 December 2012
T4
DT YEUNG YING FUNE
First Name (initial): YF Last Name: LEE
MAge:69
Comments from Ghairperson
- i¡r , cÐ-AD
^ Þ¿tz* ¿-**.,t ¿¿-t l^-¿-t "
- iZ (* /?\ lt, v+ohw ¿-4-n*--¡\--'--\ t.o*--'-'\- --^-
. ¿¡(¡-"'ì-oG-\. b* f)watu- t\¿o-¡v
t( tr
. âor*-.¿ hq..\t U-n rr""pl*r-o\ . 'Y* nl-e*.J *"f \
2t í6 ** Vs-u¡ '---t h\m'-.{ t-" tr*ì -ty, 'u<tl]''1'\*'- +-J\^'-L
I
' -[-wtt l,nnc¡-*\*- ''t Ç-'+-üç ¿-*1P\'R'rfì\'- ; -|1u,v t'ø^'- I
Professor Paul B. S. LaiChairpersonDepartment of Surgery
Follow-up Action: M ruo
tJ Yes (please list the details)
t
o
o
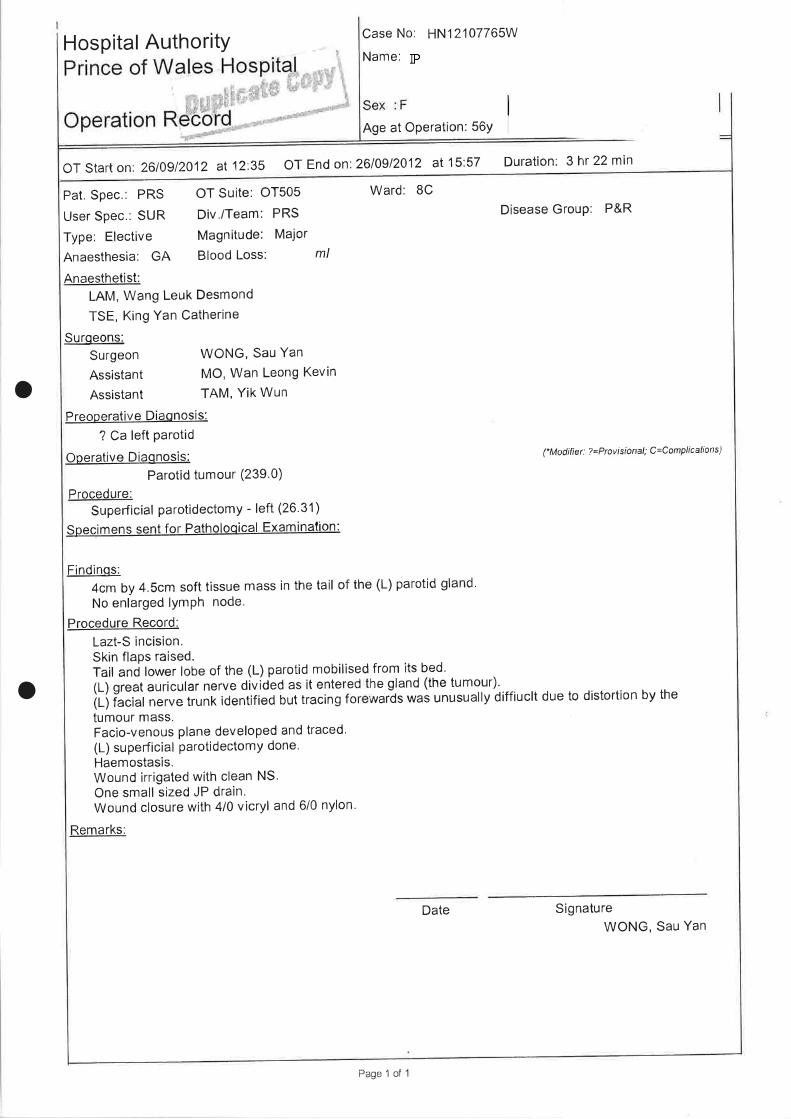
Hospital AuthoritY Case No: HN12'107765W
Name:
Age at Operation: 56Y
oT start on: 2610912012 at 12"35 0T End on 2610912012 al 15:57 Duration: 3hr 22 min
Pat. Spec.: PRS OT Suite: OT505 Ward: 8C
User Spec.: SUR Div./Team: PRS Disease Group: P&R
Type: Elective Magnitude: Major
Anaesthesia: GA Blood Loss: ml
Anaesthetist:LAM, Wang Leuk Desmond
TSE, King Yan Catherine
Surqeons:Surgeon WONG, Sau Yan
Assistant MO, Wan Leong Kevin
Assistant TAM, Yik Wun
Preoperative Diaonosis:
? Ca left Parotid
OpefatiVe DiaOnOSiS: (Modifier: ?=Provisional; C=ComplicalÌons)
Parotid tumour (239.0)
Procedure:Superficial parotidectomy - left (26.31)
Spegimens sent for Patholoqical Examination:
Findinqs:4cmby4.Scmsofttissuemassinthetailofthe(L)parotidgland.No enlarged lYmPh node.
Procedure Record:
Lazt-S incision.Skin flaps raised.Tailandlowerlobeofthe(L)parotidmobilisedfromitsbed.(L) great auricular nerve divíded as it entered he gland (the tumour).
(L) facial nerve trunk identified but tracing for waids was unusually diffiuclt due to distortion by the
tumour mass.Facio-venous plane developed and traced'(L) super-ficial parotidectomy done'Haemostasis.Wound irrigated with clean NS.One small sized JP drain.Wound closure with 4/0 vicryl and 6/0 nylon'
Remarks:
Date Signature
WONG, Sau Yan
Page 1 of I
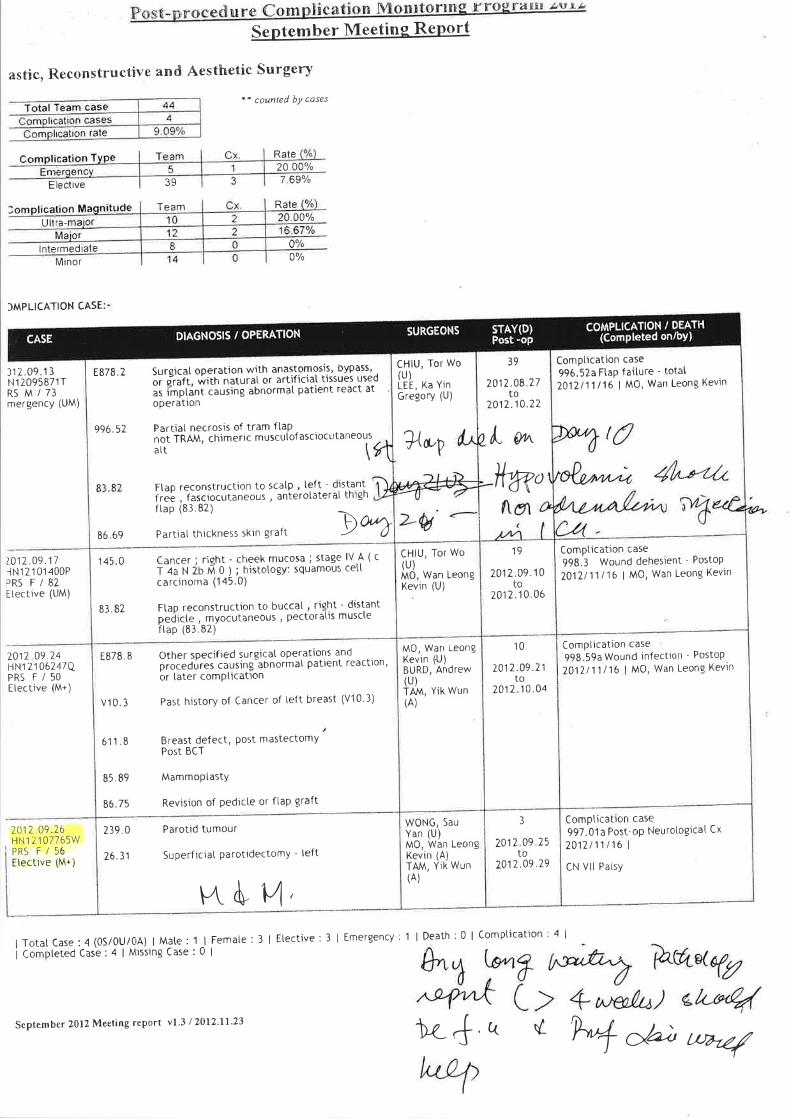
SePtember Meeting RePort
astic, Reconstructive and Aesthetic Surgery
Elective
Ultra-
lntermediateMinor
39
Team
a* coun.led bY coses
Rate20 00o/o
7 69%
Rate
0%
00%
)MPLICATION CASE:
Complication case
996.S?,aFtap failure - totat2017111/16 I MO, Wan Leong Kevìn
39
2012.08.27to
2012.10.22
l" g^
l(g,t
CHIU, Tor Wo(u)M0, Wan LeongKevìn (U)
19 | ComPtication case
998.3 Wound dehesjent - PostoP
2012.09.10 I ZOtZ¡t/ 16 I MO, Wan Leong Kevinto
2012.10,06
10 | ComPtication case
998 59a Wound infection - Postop
7012 09.71 | ZOtZl1 /16 I MO, Wan Leong Kevinto
7012 10.04
M0, Wan LeongKevìn (U)BURD, Andrew(u)TA,M, YiK WUN(Ä)
l1 2.09. 1 3N1 20958717R5 M/73mergency (UM)
¿017.09 111N12101400PPRS F/82ttectìve (UM)
2017,09.74HN1 21 06247QPRS F/50E[ective (M+)
7012.09 76HN1 21 07765WPRS F/56Etective (M+)
E878 .2
996.52
86.69
145 0
83, B2
Suroica[ ooeration with anastomosis, bypass' .
or p"raft. with naturaI or artificia[ tissues useo
ás imptãnt causing abnormaI patient react atoperation
Partiat necrosis of tram ftaPnot fRÄJv\, chimeric muscutof ascìocutaneous
CHIU, Tor Wo(u)LEE, Ka YinGregory (U)
Ftap reconstruction to scatp , teft dls-t:ä.11
freb , fasciocutaneous , anterotaterat thìgn
aIt
ftap (83.82)
Partìat thickness skìn graft
7@P
WONG, Sau
Yan (U)M0, Wan LeongKevin (A)TAM, Yik Wun(A)
Þ%Cancer; riqht - cheek mucosa; stage lV.A (cr lJtl io ú o I ; nistotogy: squamous cett
carcinoma (145.0)
Ftap reconstruction to buccat., riqft I dis-\1nt
pedicte , myocutaneous , pectoratis muscteftap (83.82)
EB78. 8
v10. 3
611 .8
85. 89
86.75
239.0
76.31
Other soecified surgicat operations andprocedures causing abnormal patlent reactlon,or later comPÌlcation
Pas[ history of Cancer of teft breast (V10'3)
Breast defect, Post mastectomyPost BCT
Mammoptasty
Revision of Pedicte or ftaP graft
Parotid tumour
Superficiat Parotidectomy - teft
3
7017.09.25to
2012.09.79
Compticatton case
997.01a Post-oP NeurologicaI Cx
2012/11116 I
CN Vll PatsY
F4. ù u,I Total Case : 4 (0S/0U/04) | Male : 1 | Femate :
i Compteted Casê : 4 | Missing Case : 0 I
3 | Etective:3 | Emergency:1 | Death:0 I Compucation:4 I
September 2012 Meeting report vl.3 12012'll'23 ì¿4 u ú ry d.; Øvzz/

PRAS Team
55yr old female
First seen in clinic 14/04/12
Left parotid swelling for several months
Asymptomatic
Firm mass
Left angle of mandible
6cm x 5cm x 4cm
No cervical lymph nodes
Facial nerve: intact
Multiple lobulated masses in bilateral parotid glands
Features suggest lipoma’s
MRI +/- FNAC arranged for further evaluation

Multiple lobulated massesBilateral parotid glandsInvolves superficial & deep lobes?Lymphoma ?salivary gland tumour
FNAC: Suspicious of low grade epitheial neoplasm – Need to rule out acinic carcinoma

Left superficial parotidectomy 4cm x 4.5cm tumour in tail of parotidLeft GAN dividedFacial nerve identifiedTracing of nerve difficult due to distortion by tumour massDuration: 3hrs 22mins

Noted complete left facial nerve palsy
Patient reassured this is likely temporary
Discharged home day 3 post op

Last seen in clinic 6/12/12Left facial nerve paralysisNo function/recovery
Pathology: Benign - Oncocytoma


Benign tumour
80% occur in the parotid glands
7% bilateral involvement
Represent 1% of all parotid tumours

Occurs in 6th decadeMale & females effected equallySimilar to Warthin’s tumour & pleomorphic adenomaSlow growingAsymptomatic

Surgery
Recurrence rate: 20%

Date
Team
Presenter
Patient Name
Sex
M & M Meetinq
Thursday 27 Ðecember 2012
PRAS
Dr MO WAN LEONG, KEVIN
First Name (initial): KC Last Name: lP
Age : 50
Comments from Ghairperson
( *1*).cnt-\
1*,Þ;\4,*Lïî*^
a^-r.ts-) t- à-_,. à*-. s
-) (-rn'r' t-.r-- a l-'*'* ¿'lv+-* "\ "9-*7"
Professor Paul B. S. LaiChairpersonDepartment of Surgery
Follow-up Action: M No
tr Yes (please list the details)