colorectal cancer diagnostic pathway wessex endoscopy ... · pdf filewessex endoscopy capacity...
TRANSCRIPT

Richard Guerrero L., Senior Research Assistant Centre of Implementation Science, University of Southampton Sally Rickard, Strategic Clinical Network Manager
September 2015
Colorectal cancer diagnostic pathway Wessex endoscopy capacity and demand

Introduction • Background
• Endoscopy activity in Wessex by provider and Clinical Commissioning Group (CCG)
• Five year projection of endoscopy demand across Wessex (from 2014 to 2019)
• Existing endoscopy capacity in Wessex by provider unit.
• Summary and conclusions

Background • This project builds on findings of the International Colorectal
Project, completed in 2012.
• This work was identified as a priority work-stream by the Strategic Clinical Network (SCN) and agreed as such by the Wessex CCGs through the Commissioning Assembly
• This project is part of a programme to increase early detection of cancer and thereby reduce premature mortality
• This project aims to support planning to meet future demand for endoscopy services.

• Endoscopy activity in Wessex by provider and Clinical Commissioning Group (CCG)
• Five year projection of endoscopy demand across Wessex (from 2014 to 2019)
• Existing endoscopy capacity in Wessex by provider unit.

Endoscopy units in Wessex included in the analysis
1 The number of endoscopy rooms by provider (current capacity) is shown in the circle next to each named hospital

Project approach
• A multi-disciplinary working group was established, chaired by Mr Tom Cecil (Consultant Colorectal Surgeon Hampshire Hospitals Foundation Trust), consisting of primary and secondary clinicians, health care managers and commissioners to oversee the undertaking of this project.
• The SCN Clinical Director, Mr Matthew Hayes, wrote to each Trust requesting their help with extracting endoscopy data.
• Professor Stephen Halloran at the Bowel Cancer Screening Southern Programme Hub provided published annual report screening data (uptake, positivity, clinical outcomes).
• Standard workload measures were taken from the British Society of Gastroenterology.
• Detailed assessment of working practices including utilisation rates were made at two Wessex NHS providers.

Endoscopy activity by Procedure in Wessex 2013/14 Procedure counts

• All significant providers contacted = 14 Units (12 NHS sites)
• Most recent activity data provided from April 2014 – March 2015
• Timetable of sessions planned
• Workload converted to units of time (20 minutes per point)
• Case-mix reflected in type of procedure (Colonoscopy = 2/3 points, Flexi-sig = 1/2 points, Gastroscopy = 1/2 points)
• Population demographic data obtained from ONS census
• Screening data extracted from 3 Local Screening Centre reports (October 2013 – October 2014)
• Flexible Sigmoidoscopy data from latest pilot programme (NHS Bowel Scope Screening http://www.cancerscreening.nhs.uk/bowel/bowel-scope-screening.html)
Activity data

• The British Society of Gastroenterology (BSG) specifies weightings for each GI endoscopic procedure, reflecting their average duration. 1 point typically equates to a 20 minute procedure. The national standard is 12 points per list.
• Due to the different time periods for which the data were provided by endoscopy units, activity and demand is shown per week.
• The analysis of activity by endoscopy unit, future demand and capacity is presented using Points as the standard measure.
Points
Diagnostic Therapeutic
Gastroscopy 1 2
Flexi-sigmoidoscopy 1 2
Colonoscopy 2 3
ERCP 2 3
Notes on data collected
It is important to distinguish between those procedures which are for diagnostic or therapeutic purposes due to the different time required. Whether the lists are used for training or service purposes is also an important distinction.

Wessex
Wessex
Activity by endoscopy unit in Wessex Number of procedures per week
• Total endoscopy activity in Wessex in 2013/14 was 3440 points per week
• Average endoscopy suit utilization in Wessex is 69%
• Average points by endoscopy list is 8.5
The total endoscopy activity in Wessex is based upon the providers’ actual scheduling. For example the smallest provider operates its endoscopy unit 2 sessions per week, the largest provider operates 3 sessions per day, five days per week plus some weekend sessions
The y axis displays the number of possible points in one session (morning, afternoon or evening period). The x-axis displays room utilisation where 100% equates to the total session time being booked by procedures.

Activity by endoscopy unit in Wessex procedures per week
It can be seen from the graph above that the providers vary in scale enormously with four large acute hospitals and two very small community hospitals in terms of endoscopy activity. Data shows absolute values from the providers information.

Activity by endoscopy unit in Wessex procedures per room per week
It can be seen from the graph above that when the activity is divided across the numbers of rooms at each provider the range of activity falls between 23 and 65 procedures per room per week (excluding the two smallest units).

Proportion of procedure type by provider
The graph above shows that the proportions of procedure type by provider is fairly consistent, except for St Mary’s treatment centre, Lymington and Wimborne.

• Endoscopy activity in Wessex by provider and Clinical Commissioning Group (CCG)
• Five year projection of endoscopy demand across Wessex (from 2014 to 2019)
• Existing endoscopy capacity in Wessex by provider unit.

Demand for endoscopy is increasing due to a number of factors
• The ageing population (increase in both the number of older people and them living longer)
• The faecal occult blood testing (FOBT) screening programme including people aged 60-69 and aged 70-75
• The introduction in 2016 of the flexible sigmoidoscopy bowel screening programme for people when they reach the age of 55 which can be requested up to the age of 60
• The NHS Operating Framework expectation that less than 1% of patients should wait more than six weeks for diagnostic tests

Future endoscopy demand modelling for Wessex projecting five years: Results
The following five slides show the results for the 2 scenarios
Scenario 1: Increase in Faecal Occult Blood Test screening (FOBt) Scenario 2: FOBt (in Scenario 1) plus Bowel Scope FlexiSig (FS)
• total endoscopy demand in points per week
• Lower GI activity and future demand by CCG
• Total GI activity and future demand by CCG
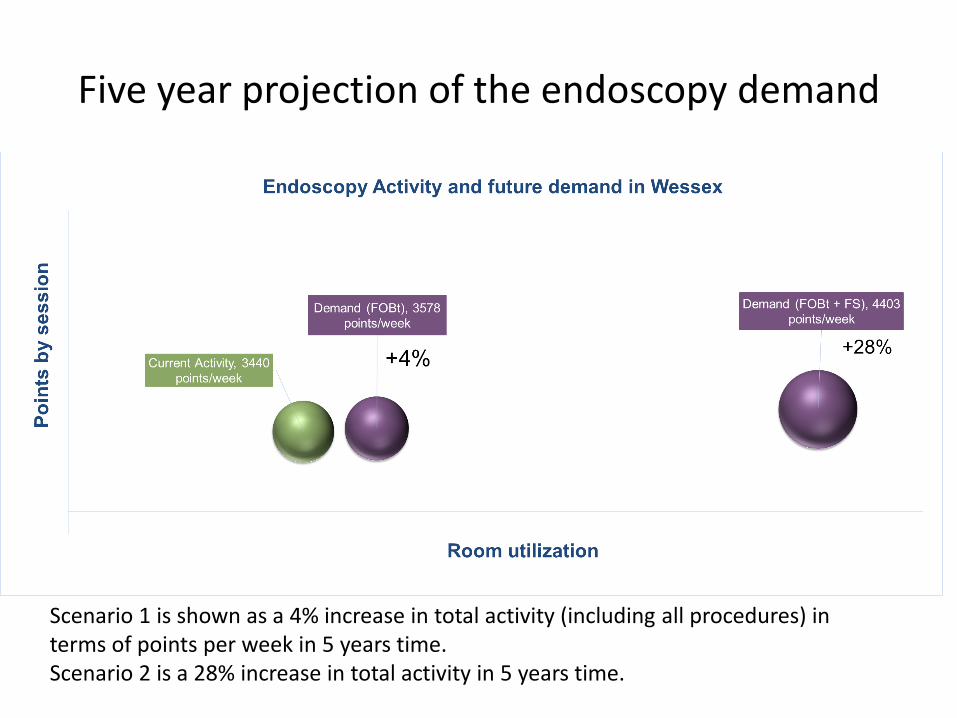
Five year projection of the endoscopy demand
Scenario 1 is shown as a 4% increase in total activity (including all procedures) in terms of points per week in 5 years time. Scenario 2 is a 28% increase in total activity in 5 years time.

Five year projection of the endoscopy demand by CCG (Scenario 1)

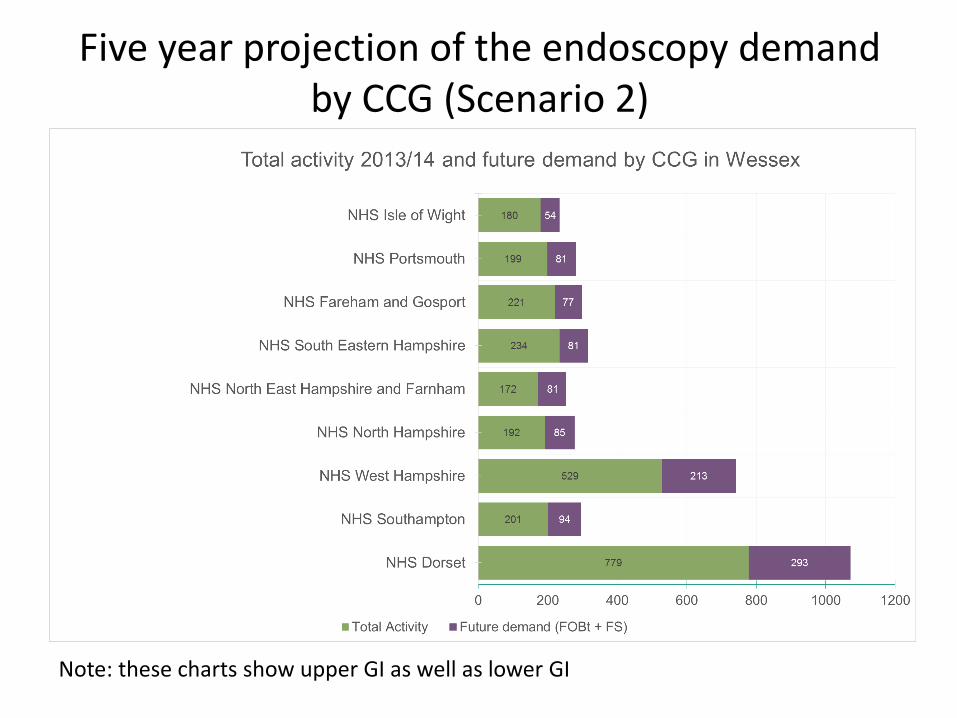
Five year projection of the endoscopy demand by CCG (Scenario 2)

Five year projection of the endoscopy demand by CCG (Scenario 1)
Note: these charts show upper GI as well as lower GI
Five year projection of the endoscopy demand by CCG (Scenario 2)
Note: these charts show upper GI as well as lower GI

• Endoscopy activity in Wessex by provider and Clinical Commissioning Group (CCG)
• Five year projection of endoscopy demand across Wessex (from 2014 to 2019)
• Existing endoscopy capacity in Wessex by provider unit.

Existing endoscopy capacity in Wessex
• Total points per week in Wessex is 3440 in the green bubble in the next chart
• The current system (without change to existing scheduling) but excluding DNA etc is 4473 points – the red bubble in the next chart
• Potential to increase capacity within existing resources
– increasing the number of points per session
– increasing room utilisation
• Any changes to staff resources are NOT considered

24
Endoscopy capacity in Wessex
Example: if 11 points every session and utilisation rate of 80% then capacity = 3872 points per week in Wessex, about 12.5% increase on current. Current system of 4473 when activity goes as planned ie all scheduled activity takes place, no change to staffing nor session time required.

Endoscopy activity and capacity in Wessex Current and maximum capacity (scenario A and B)

Current capacity and impact of increasing to 12 points per session, 2 sessions per day, 5 days per week
Some units are already operating beyond 10 sessions per week

Current capacity and impact of increasing to 12 points per session, 3 sessions per day, 7 days per week
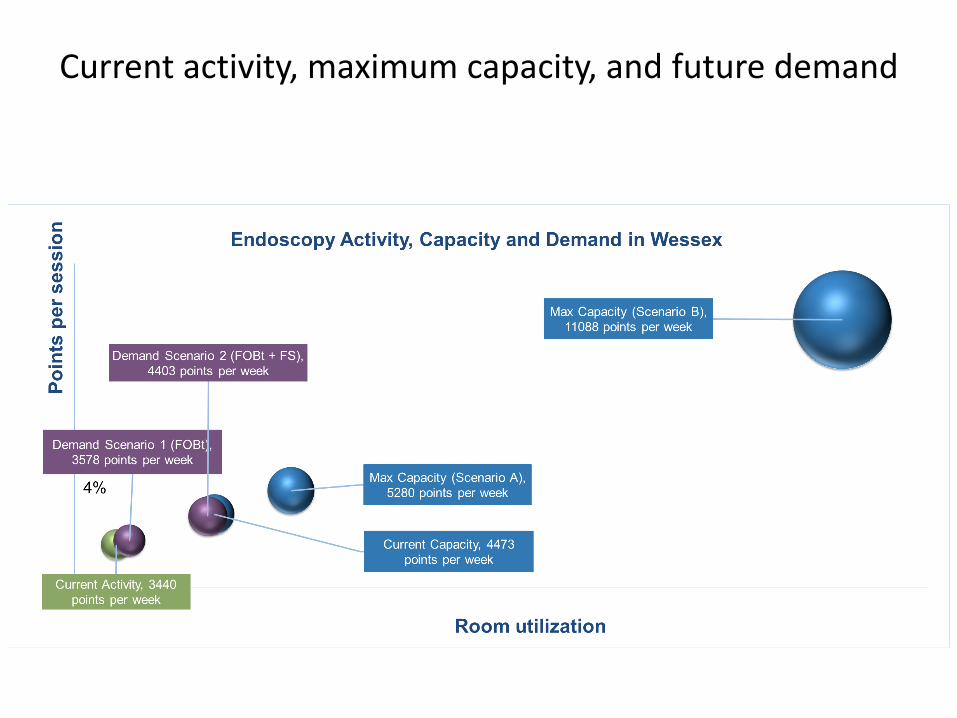
Current activity, maximum capacity, and future demand

Summary of the results of our work (1)
Our aim was to quantify existing capacity and activity for all Wessex (providers and CCGs)
• Theoretical maximum capacity in Wessex
- 5280 points per week [based on 2 sessions per day, 5 days per week, 12 points per list, 100% utilization]
- 11088 points per week [based on 3 sessions per day, 7 days per week, 12 points per list, 100% utilization]
• Current capacity in Wessex = 4473 points per week [based on existing working practices]
• Activity in Wessex = 3440 points per week
• Average utilization rate = 77% [based on Current capacity in Wessex] - Utilisation varies from 41% to 94%
• Potential capacity identified with different ‘working time’ scenarios.
29

Summary of the results of our work (2)
• 5 year projection of future activity and capacity needed
– Computer based modelling (Discrete event simulation approach) to estimate the future demand based on scenarios
• FOBt screening, the expected increase [(Colonoscopies + FlexiSig) / Total number of Endoscopies] is 4%
• FOBt + Bowel Scope (FlexiSig) [based on 100% of patients 55y invited to the Screening, and 50% uptake, the expected value is 28% [(Colonoscopies + FlexiSig) / Total number of Endoscopies]
– Detailed model of provider endoscopy unit
• Input actual patient demand, patients flows and existing working practices
• Developed for General Hospital and University Teaching site
• Incorporate ‘did not attend’ rate, delays, turnover time between patients
30

Recommendations
• Develop bespoke models for each provider unit
• Review session start and finish times against recommended standard
• Minimise patient re-scheduling (up to 25%)
• Reduce do not attendant rate (up to 15%)
• Look at ways to reduce delays (patient and clinician late arrival, medical clearance delays, patient dressing, DNA, endoscopy equipment failure, patient not checked, transport to endoscopy suite, delayed room turnover, anaesthesia related)
• Productive endoscopy box set (http://www.nhsiq.nhs.uk/7923.aspx)

Glossary
• Activity: All the work done. This does not necessarily reflect capacity or demand on a day to day basis. The activity or the work done on a Monday may be result of some of Monday’s demand (i.e. emergency) and the previous week’s demand. The capacity is the capacity available on the Monday but activity is often less than available capacity.[1]
• Capacity: Resources available to do work. For example, the number of pieces of equipment available multiplied by the hours of staff time available to run it.[1]
• Demand: All the requests / referrals coming in from all sources and how many resources they need (equipment time, staff time, room time) to deal with.[1]
• (Endoscopy) list: Many units allocate 12 points to a morning list and 10 to an afternoon list on the basis that a morning list lasts 3 hours (210 minutes) and an afternoon list 2.5 hours (180 minutes).
• Point: A point is a unit of time. For example some units assign 15 minutes to one point and allocate 1 point for and OGD, 2 for colonoscopy, etc.[2]
[1] Demand and Capacity – A Comprehensive Guide. NHS Institute for Innovation and Improvement. http://www.institute.nhs.uk/quality_and_service_improvement_tools/quality_and_service_improvement_tools/demand_and_capacity_-_a_comprehensive_guide.html [2] How many ‘points’ should there be on an endoscopy list? JAG Join Advisory Group on GI Endoscopy http://goo.gl/uXh1w2


Supplementary notes for review by providers

Number of points scheduled per list
• Point system: – Some units assign 15 minutes to one point (and some assign 20
minutes) – 12 points to a morning list (3.5 hours, 210 minutes) and 10 to an
afternoon list (3 hours, 180 minutes) – Training lists – assign less points
• 10 points per endoscopy list (session) as standard plus an additional 2 points per list to accommodate any emergencies/inpatients could be implemented.
• Training or nurse endoscopist lists usually carry 7 – 10 points depending upon experience.
• We recommend to review the booking templates across sites to understand the variation from the 12 point standard

Session utilisation and start and finish times
Session utilisation should be routinely monitored as low utilisation usually falls into 3 categories:
1. Insufficient backfilling of lists
2. High DNA rates
3. Under/over booking
Scheduled start and finish times should be reviewed on each of the sites.
• 9:00 hrs until 12:30 hrs and 13:30 hrs until 17:00 hrs – are these standard hours?
• Based on UK guidelines and Wessex practices
Patients scheduling
• We recommend scheduling options are analysed, for example – 1:1 endoscopist to room ratio vs 1:2 endoscopist to room (endoscopy
room turnover time vs endoscopist turnover time)
• Example of impact of patients scheduling on the performance: – If 6 minutes to turn a room round, and 12 point lists: – List 1: 12 Gastroscopies (1 point), 11 turnrounds room utilisation =
68%. – List 2: 6 Colonoscopies (2 points), 5 turnarounds room utilisation =
86%.
• Room utilisation: We recommend the focus on the patient’s time being scoped (vs patients’ time in the room/total list time) importance of the turnaround time, and delays (patients, clinicians, equipment).
