combination opportunities in immunotherapy with ... · hospital universitario reina sofía,...
TRANSCRIPT
Miguel F Sanmamed
María Rodriguez
Carlos Alfaro
Carmen Oñate
Inmaculada Rodriguez
José L Pérez Gracia
Bruno Sangro
Salvador Martin -Algarra
JM Lopez Picazo
Alfonso Gúrpide
Javier Rodriguez
Jesús San Miguel
Jesús Prieto
Alberto Benito
Ivan Peñuelas
Alvaro Gonzalez
Mercedes Iñarrairaegui
Aizea Morales
Arantza Azpilikueta
Elixabet Bolaños
Inmaculada Rodriguez
Sara Labiano
Eneko Elizalde
Alfonso Rodriguez
Angela Aznar
Maria Rodriguez-Ruiz
Pedro Berraondo
Luna Carneiro
Ines Guetgeman
Juan M Zapata
Manuel Rodriguez
Valerie Lang
Bettina Weigelin
Peter Friedl
Bristol Myers Squibb
Roche/Genentech
Pfizer
AstraZeneca
Boehringer Ingelheim

IGNORANT T CELL
Insufficient antigen/
lack of co-stimulatory signals
ANERGIC T CELL
Unsuccessful stimulation/
negative regulation
APOPTOTIC T CELL
(DELETED)
Programmed cell death
NAIVE T CELL PRIMED T CELL EFFECTOR T CELL MEMORY
T CELL:
Central memory cell
Effector memory cellCD27
CD28
HVEM
TCR
MHC
-peptide
CD27L
CD80/86
LIGHT
CTLA-4
B7-H4R
CD80/86
B7-H4
PD-1
B7-H4R
B7-H1
BTLA-4
B7-H1
B7-DC
B7-H4
BTLA-4R
CD137
OX40
ICOS
B7-H3R
CD137L
OX40L
B7h
B7-H3
IL-15
IL-7
CD-137
OX-40
others
IL-12
IFN-α

Schematic representation of the concept of immunostimulatory mAbs.
Melero I et al. Clin Cancer Res 2013;19:997-1008
©2013 by American Association for Cancer Research

Immune Checkpoint Blockade
against Malignancy
Blocking
Self-inflicted
Inhibitions?

CD80
CD86
CD28
CTLA-4
+
-

Anti-CTLA-4
Phase III clinical trials
Registered for metastatic melanoma.
Combines with vaccination preclinically.
10-20% sustained responses in phase II
30% incidence of moderate/severe autoimmunity
CTLA-4-/- dies because of multiorgan
lymphocyte infiltration
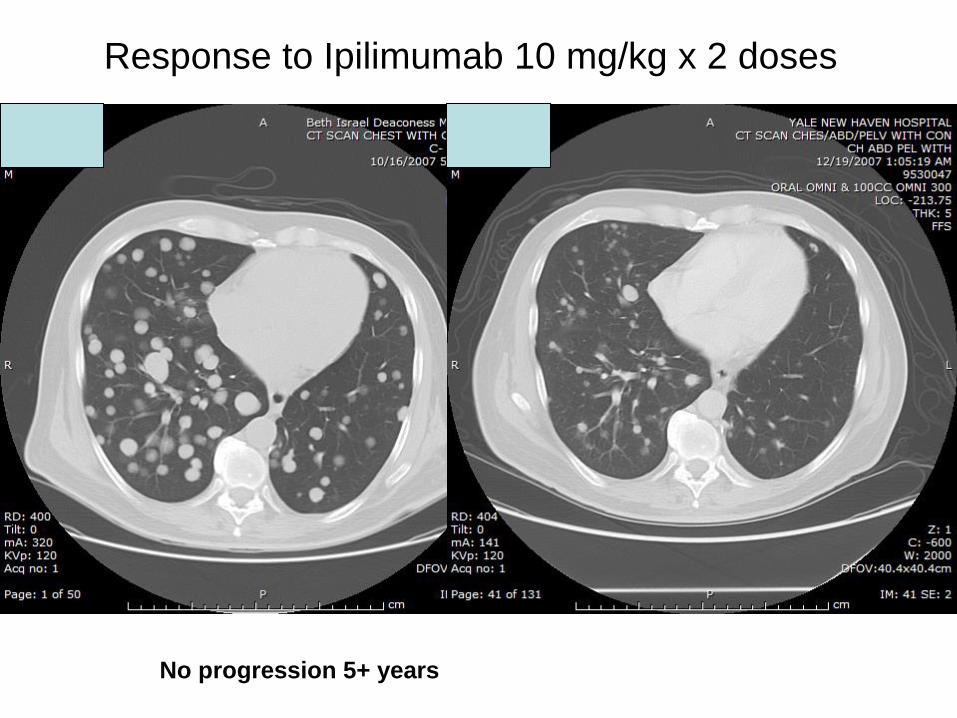
Response to Ipilimumab 10 mg/kg x 2 doses
No progression 5+ years

Survival Rate Ipilimumab + gp100 Ipilimumab alone gp100 alone
1-yr 44% 46% 25%
2-yr 22% 24% 14%

Hepatocellular carcinoma
A major target for immunotherapy
with checkpoint inhibitors.

Killing two birds with one stone

Phase II Trial of Anti-CTLA-4 Human Monoclonal
Antibody CP-675,206 in Patients With Advanced
HCC
Clinica Universidad de Navarra,
Pamplona
Hospital Universitario Reina Sofía,
Córdoba
Hospital Universitario 12 de Octubre,
Madrid
Protocol code CT-2007-01
EudraCT no. 2008-001177-15
NCT Identifier NCT01008358
Sponsor: University of Navarra, Pamplona, Spain

• Tremelimumab (CP 675,206) is a fullyhumanized IgG2 mAb that antagonizesbinding of CTLA-4 to B7 ligands.
– Antitumor activity has been demonstrated in a variety of murine tumor models
– It has shown efficacy on melanoma patients after single ormultiple doses. Similar drug Ipilimumab already approvedfor metastatic melanoma.
– It had not been tested against hepatocellular carcinoma
– Its antiviral effect had not been tested whatsoever
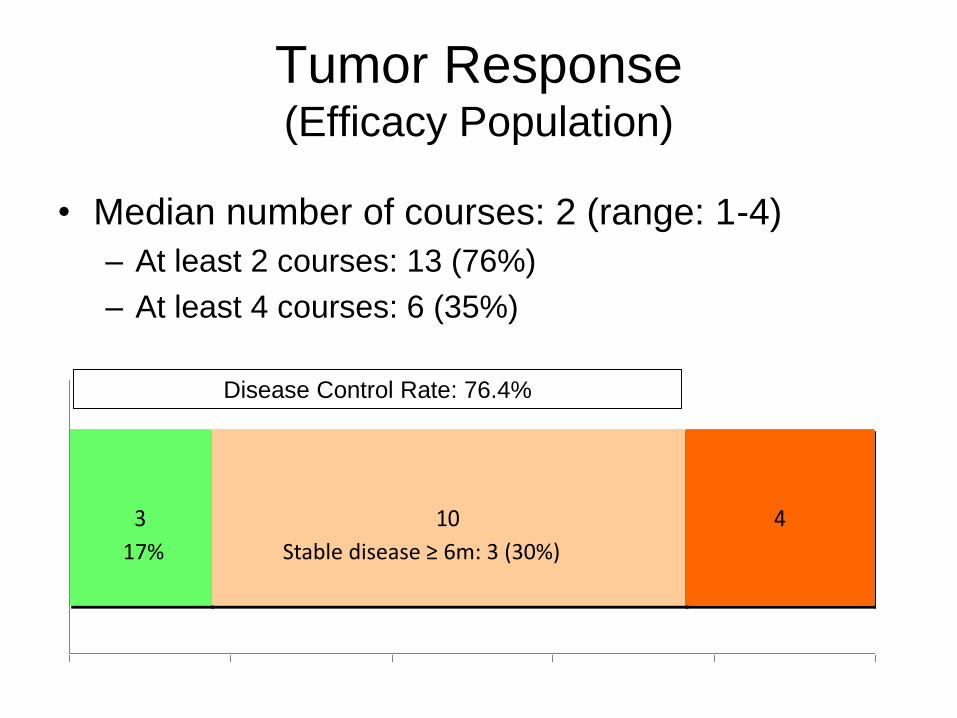
Tumor Response (Efficacy Population)
• Median number of courses: 2 (range: 1-4)
– At least 2 courses: 13 (76%)
– At least 4 courses: 6 (35%)
3 10 4
0% 20% 40% 60% 80% 100%
Disease Control Rate: 76.4%
Stable disease ≥ 6m: 3 (30%)17%

Tumor Response on Target
Lesions
-80
-60
-40
-20
0
20
40
60
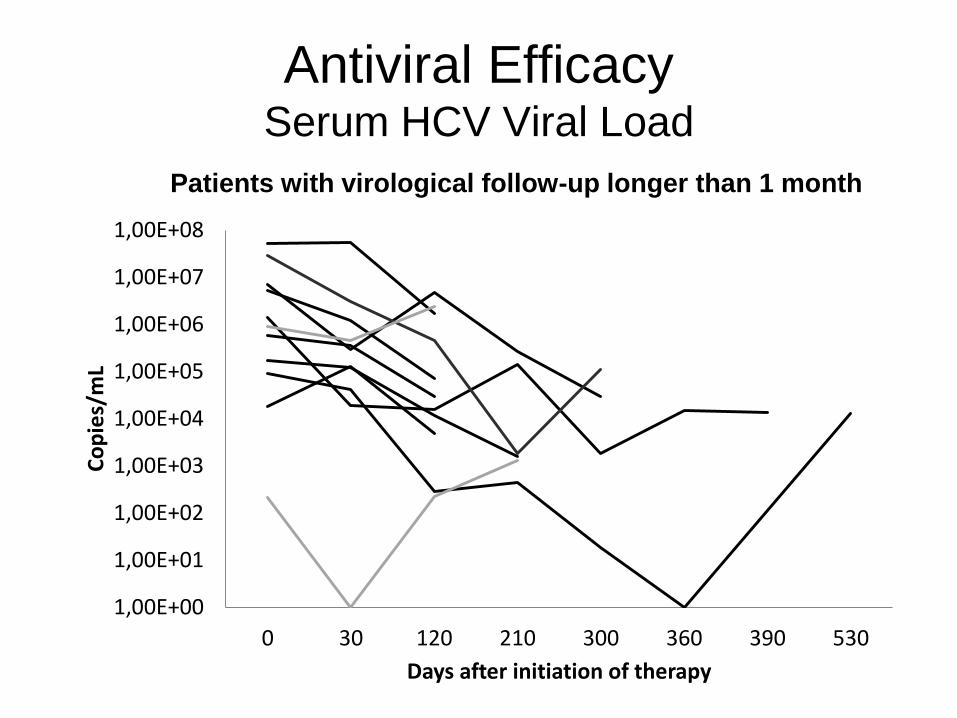
Antiviral EfficacySerum HCV Viral Load
1,00E+00
1,00E+01
1,00E+02
1,00E+03
1,00E+04
1,00E+05
1,00E+06
1,00E+07
1,00E+08
0 30 120 210 300 360 390 530
Co
pie
s/m
L
Days after initiation of therapy
Patients with virological follow-up longer than 1 month

rCore
0 30 120 210 300 3300
10
20
30
40
50
Days after treatment
SF
C
rNS3
0 30 120 210 300 3300
20
40
60
Days after treatmentS
FC
rNS4
0 30 120 210 300 3300
50
100
150
Days after treatment
SF
C
rNS5
0 30 120 210 300 3300
20
40
60
80
Days after treatment
SF
C
pepP7
0 30 120 210 300 3300
10
20
30
40
50
Days after treatment
SF
C
pepE2
0 30 120 210 300 3300
50
100
150
Days after treatment
SF
C
pepE1
0 30 120 210 300 3300
50
100
150
Days after treatment
SF
C
pepCore
0 30 120 210 300 3300
20
40
60
80
Days after treatment
SF
C
pepNS5
0 30 120 210 300 3300
100
200
300
400
500
Days after treatment
SF
C
pepNS4
0 30 120 210 300 3300
50
100
150
Days after treatment
SF
C
pepNS3
0 30 120 210 300 3300
50
100
150
200
Days after treatment
SF
C
pepNS2
0 30 120 210 300 3300
20
40
60
80
Days after treatment
SF
C
*
*
*
Immunological Outcomes
Global Changes in Anti-HCV Immune Response

Immune Checkpoint Blockade
against Malignancy
Blocking
Self-inflicted
Inhibitions?

PD-L1 and IDO-1 permit placentation across MHC barriers

Why might PD-L1 be important?
Anti-tumour immune
responses are turned off
Promoting anti-tumour immune
responses
T cell activationT cell inactivation
PD-1
PD-L1/PD-L2
TCR
MHC
PD-1TCR
MHC No PD-L1
Partner cell
T cell T cell
Partner cell
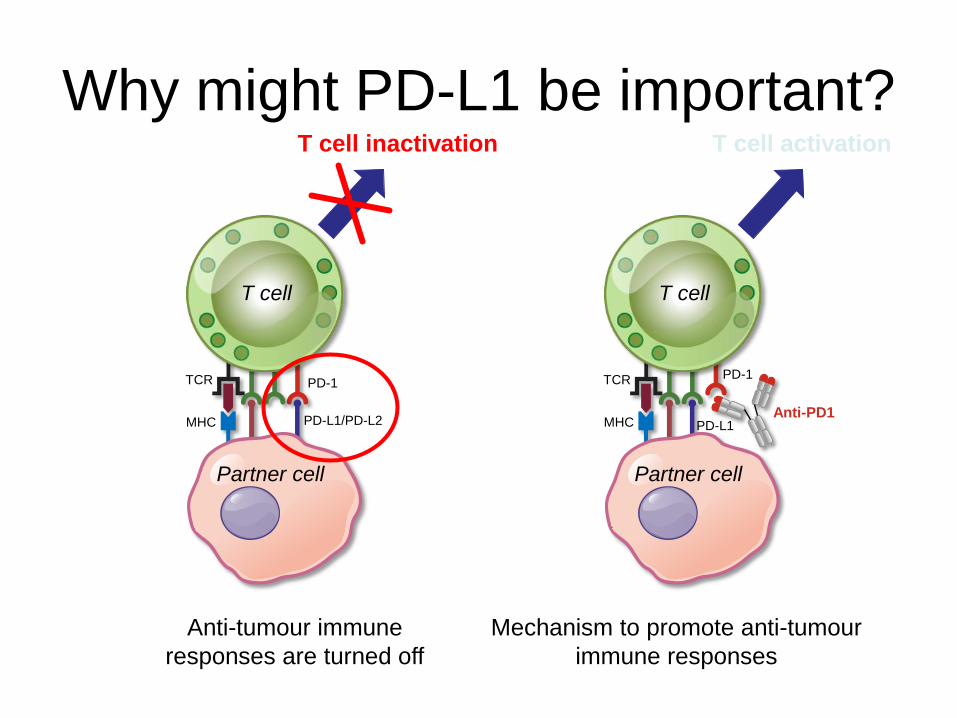
Why might PD-L1 be important?
Anti-tumour immune
responses are turned off
Mechanism to promote anti-tumour
immune responses
T cell activationT cell inactivation
PD-1
PD-L1/PD-L2
TCR
MHC
PD-1TCR
MHCAnti-PD1
PD-L1
Partner cell
T cell T cell
Partner cell

PD-L1 blockade PD-1 blockade
PD-1 blockade = PD-L1 blockade?
Keir, et al. Annu Rev Immunol 2008
TCRMHC
PD-L1
PD-L2
B7.1PD-L1
B7.1
PD-1
-
APC T cell
TCRMHC
PD-L1
PD-L2
B7.1PD-L1
B7.1
PD-1
-
APC T cell
-

PD-1/PD-L1 blockade: a simple
paradigm
MHC=major histocompatibility complex; TCR=T cell receptor
Hayden. Nature 2012
T cell receptor
recognises
tumour cell
PD-L1 binds
PD-1, inhibiting
T cell response
A separate
therapy uses
antibodies that
bind PD-L1 on the
tumour cell
Antibodies
block inhibitory
signal to PD-1
T cellTumour
cellT cell
Tumour
cell
PD-L1PD-1
TCR MHC
PD-L1
PD-1

PD-L1
PD-1
Truth is: many cell types can be PD-L1+
IFN-g=interferon gamma
Chen, et al. Clin Cancer Res 2012
PD-L1
PD-L1
B7.1
B7.1
MHC I
B7.1
PD-1
PD-L1
CD28
TCR
PD-L1
PD-1
MHC I
TCR
PD-L1 PD-1
PD-L1
PD-1
PD-1PD-L2
Tumour
cell
CD8+ cytotoxic
T lymphocyte (CTL)
Tumour-associated
fibroblast
M2 Macrophage
Dendritic
cell
Th2
T cell
Treg
cell
Priming and
activation of T cells
PD-L1/PD-1-mediated
inhibition of tumour
cell killing
IFN-g-mediated
upregulation of
tumour PD-L1
Immune cell
modulation of T cells
PD-L2-mediated
inhibition of TH2 T cells
Stromal PD-L1
modulation of T cells
IFN-g
IFN-gR
TGF-b
IL-4/IL-13
T cell polarisation
Other NFkB PI3K
Shp-2
Shp-2

CARs and PD-1 at tumor–T cell immune synapses.
Morales-Kastresana A et al. Clin Cancer Res 2013;19:5546-5548
©2013 by American Association for Cancer Research

MHC
PD-L1
PD-1
PD-1
T-cellreceptor
PD-L2
T cell
NFκB
Other
PI3K
Tumor cell
IFNγ
IFNγR
Shp-2
Nivolumab
Nivolumab and Immune
Checkpoint Inhibition
• Nivolumab is a fully human IgG4 anti-PD-1 monoclonal antibody that selectively
blocks the interaction between PD-1 and PD-L1/PD-L2,1 restoring T-cell immune
activity directed against the tumor cell
1. Topalian SL, et al. N Engl J Med. 2012;366:2443-2454
25
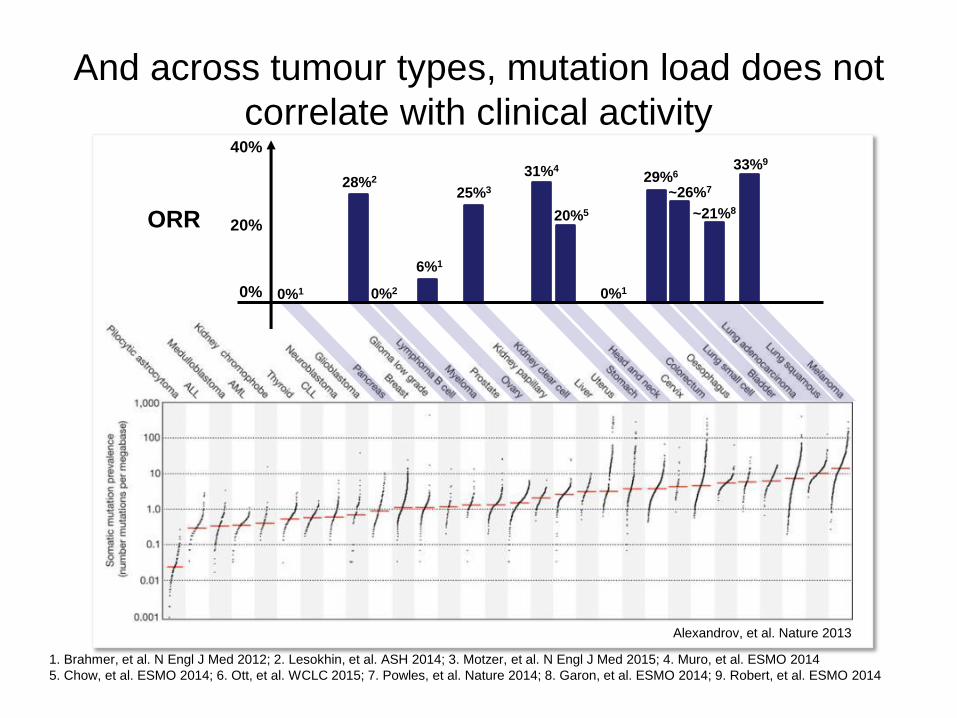
And across tumour types, mutation load does not
correlate with clinical activity40%
20%
0%
28%2
0%2
6%1
25%3
0%1
20%5
31%4
0%1
~26%7
~21%8
33%9
29%6
ORR
Alexandrov, et al. Nature 2013
1. Brahmer, et al. N Engl J Med 2012; 2. Lesokhin, et al. ASH 2014; 3. Motzer, et al. N Engl J Med 2015; 4. Muro, et al. ESMO 2014
5. Chow, et al. ESMO 2014; 6. Ott, et al. WCLC 2015; 7. Powles, et al. Nature 2014; 8. Garon, et al. ESMO 2014; 9. Robert, et al. ESMO 2014
27
HCC and Programmed Death-1
(PD-1)
• HCC is typically an inflammation-associated cancer and can be immunogenic1
• Association of hepatitis C and hepatitis B infection with upregulation of PD-12,3
• Upregulation of PD-1 and the PD-1 immune checkpoint ligand, PD-L1, in HCC is
associated with poor outcomes4
• Blockade of PD-1 with monoclonal antibodies combined with immunostimulatory
monoclonal antibodies extended survival in a mouse model of HCC5,6
• Immune checkpoint inhibition (anti-CTLA-4) has shown encouraging activity in an early
clinical trial in HCC7
• PD-1 blockade with nivolumab may boost host immunity against HCC and improve clinical
outcomes
1. Hato T, et al. Hepatol. 2014;60:1776-1782
2. Xu P, et al. Gut Liver. 2014;8:186-195
3. Barathan M, et al. Apoptosis. 2015;20:466-480
4. Zeng Z, et al. PLoS One. 2011;6:e23621
5. Chen Y, et al. Hepatology. 2015;61:1591-1602
6. Morales-Kastresana A, et al. Clin Cancer Res.
2013;19:6151-6162
7. Sangro B, et al. J Hepatol. 2013;59:81-88

Phase 1/2 Safety and Antitumor Activity
of Nivolumab in Patients With Advanced
Hepatocellular Carcinoma (HCC): CA209-
040
Anthony B. El-Khoueiry,1 Ignacio Melero,2 Todd S. Crocenzi,3
Theodore H. Welling III,4 Thomas Yau,5 Winnie Yeo,5 Akhil Chopra,6
Joseph F. Grosso,7 Lixin Lang,7 Jeffrey Anderson,7 Christine de la Cruz,7 Bruno
Sangro2
1University of Southern California Norris Comprehensive Cancer Center, Los Angeles,
CA, USA; 2Clinica Universidad de Navarra and CIBERehd, Pamplona, Spain; 3Providence Cancer Center, Portland, OR, USA; 4University of Michigan, Ann Arbor,
MI, USA; 5University of Hong Kong, China; 6Johns Hopkins Singapore International
Medical Centre, Singapore; 7Bristol-Myers Squibb, Princeton, NJ, USA
Abstract LBA 101

29
Study Design
• Patients received nivolumab Q2W for up to 2 years (maximum of 48 doses), depending on response
– Imaging for disease assessment performed every 6 weeks
• A 3+3 design was used in the phase 1 dose escalation phase
• Here, we report interim results from the ongoing dose escalation phase and part of the expansion phase
Dose Escalation Expansion
Uninfected sorafenibprogressors
3 mg/kg (n=50)
HCV-infected
Expand at 3 mg/kg
(n=50)
HBV-infected
Dose TBD
(n=50)
Uninfected 0.3 mg/kg 1 mg/kg 3 mg/kg 10 mg/kg0.1 mg/kg
HCV-infected 0.3 mg/kg 1 mg/kg 3 mg/kg 10 mg/kg
Uninfected sorafenib-naïve or intolerant
3 mg/kg (n=50)
HBV-infected 0.3 mg/kg0.1 mg/kg 1 mg/kg 3 mg/kg 10 mg/kg

Baseline Patient CharacteristicsUninfected
(n=24)
HCV
(n=12)
HBV
(n=11)
Total
(N=47)
Age (years), median
(range) 63.5 (22–79) 67 (55–83) 62 (41–68) 64 (22–83)
Male, n (%) 18 (75) 7 (58) 9 (82) 34 (72)
Race, n (%)
White 20 (83) 10 (83) 1 (9) 31 (66)
Asian 2 (8) 2 (16) 10 (91) 14 (30)
Black 2 (8) 0 0 2 (4)
Extrahepatic
metastases, n (%) 17 (71) 7 (58) 9 (82) 33 (70)
Vascular invasion, n (%) 3 (13) 2 (17) 1 (9) 6 (13)
Child-Pugh Score, n (%)
5 21 (88) 9 (75) 11 (100) 41 (87)
6 3 (13) 2 (17) 0 5 (11)
7 0 1 (8) 0 1 (2)
AFP >200 μg/L, n (%)* 8 (33) 2 (17) 7 (64) 17 (36)
*Baseline AFP values were missing for 5 patients 30

Prior Treatment History
Treatment Type, n (%) Uninfecte
d (n=24)
HCV
(n=12)
HBV
(n=11)
Total
(N=47)
Prior surgical resection 14 (58) 8 (67) 9 (82) 31 (66)
Prior radiotherapy 6 (25) 1 (8) 1 (9) 8 (17)
Local treatment for HCC 12 (50) 8 (67) 9 (82) 29 (62)
TACE, TAE, or
radioembolization 11 (46) 8 (67) 7 (64) 26 (55)
RFA or PEI 5 (21) 4 (33) 4 (36) 13 (28)
Other 1 (4) 0 1 (9) 2 (4)
Prior systemic therapy 17 (71) 7 (58) 11 (100) 35 (75)
Prior sorafenib 15 (63) 6 (50) 11 (100) 32 (68)
TACE, transcatheter arterial chemoembolization; TAE, transcatheter arterial embolization; RFA, radiofrequency ablation;
PEI, percutaneous ethanol injection
31

Uninfecte
d
(n=21)
HCV
(n=11)
HBV
(n=10)
Total
Evaluable
*
(n=42)
Objective response, n (%) 3 (14) 4 (36) 1 (10) 8 (19)
Complete response 2 (10) 0 0 2 (5)
Partial response 1 (5) 4 (36) 1 (10) 6 (14)
Stable disease 10 (48) 5 (45)† 5 (50) 20 (48)
Progressive disease 8 (38) 2 (18) 4 (40) 14 (33)
Ongoing response, n (%) 3/3 (100) 3/4 (75) 0 6/8 (75)
Responses assessed by RECIST 1.1
*5 patients not evaluable: first disease assessment not yet performed in 4 patients, 1 patient died from clinical
progression before disease assessment†Patient with resolved HCV infection
Investigator-Assessed Best Overall
Response
32

Maximal Change in Target Lesions
From Baseline120
100
80
60
40
20
0
-20
-40
-60
-80
-100
Patients (N = 40)†
Ch
an
ge
in
Ta
rge
t L
es
ion
Fro
m B
as
eli
ne
, %
Uninfected
HCV
HBV
Confirmed response
*
* *
* ** *
* *
†2 uninfected patients not shown: 1 had disease progression before the first assessment; 1 had a maximal change of +23%‡Patient with resolved HCV infection
‡
33

Response Kinetics
Time Since First Dose, Months
Ch
an
ge
in
Ta
rge
t L
es
ion
Fro
m B
as
eli
ne
, %
180
0 3 6 9 12 15 18 21
-100
-80
-60
-40
-20
0
20
40
60
80
100 Months,
range
Uninfected
(n=21)
HCV
(n=11)
HBV
(n=10)
Total
Evaluable
(n=42)
DOR7.2* –
12.5*1.4* – 8.3* 11.9 1.4* – 12.5*
Duration of SD1.1* –
17.3*2.9† – 14.0 2.7* – 6.9* 1.1* – 17.3*
*Censored†Patient with resolved HCV infection
First occurrence of new lesion
34
+
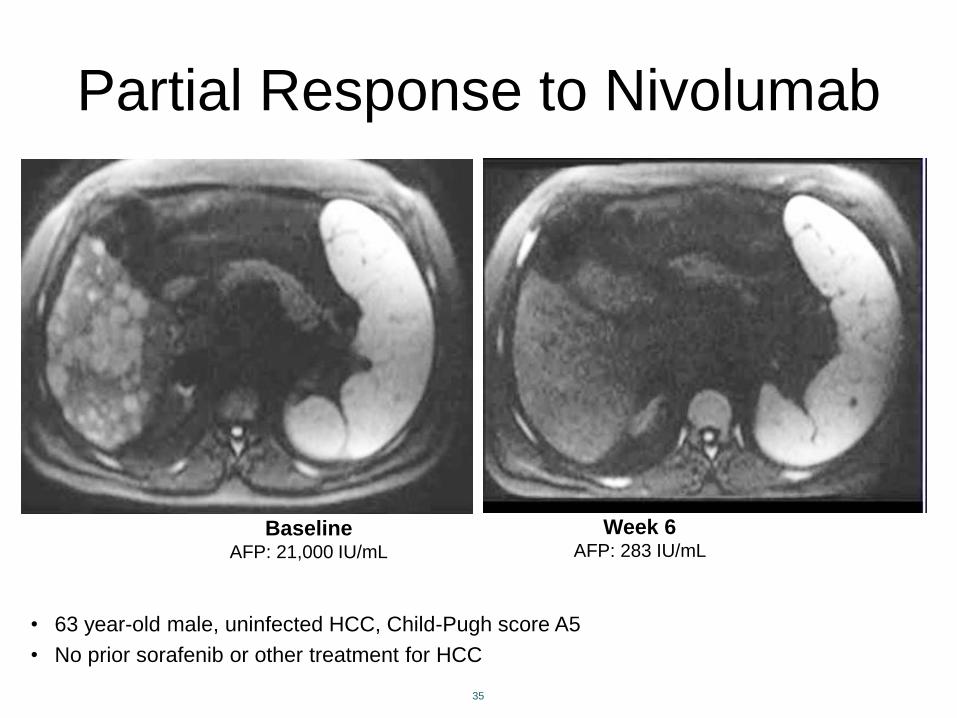
Partial Response to Nivolumab
• 63 year-old male, uninfected HCC, Child-Pugh score A5
• No prior sorafenib or other treatment for HCC
35
BaselineAFP: 21,000 IU/mL
Week 6AFP: 283 IU/mL

Remove inhibitions
Release the brakes Press the gas pedal to the metal
Enforce costimulation

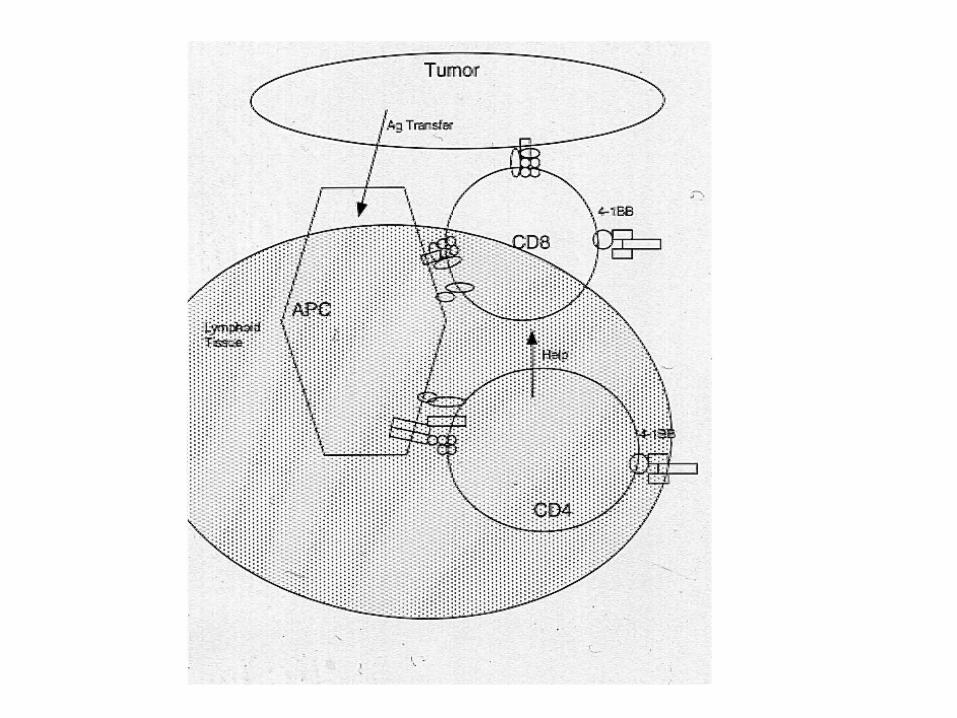
• CD137, also known as 4-1BB, is a surface glycoprotein involved in T cell costimulation
• Its cognate ligand is CD137L, which is expressed on APCs
• Functions: T cell proliferation, inhibition of apoptosis, enhances cytotoxic activity, cytokine production
• Therapeutic target: treatment with agonist anti-CD137 monoclonal antibodies can overcome tumour antigen tolerance
• Anti-human CD137 agonist monoclonal antibodies are undergoing phase I/II clinical trials
CD137 (4-1BB, TNFRSF9)
T cellAPC
4-1BBL 4-1BB
Melero, et al. Trends Pharmacol Sci 2008


• Resistance to apoptosis• Proliferation• Gain effector functions• Differentiation to memory cells
Early cytokine production
Early tumour cell killing
Provision of tumour cell debris for cross-priming
Tumour antigencross-presentation
Proinflammatory moleculeslymphocyte infiltration?
Inhibition/activationin vivo paradox
Antigen-independentactivation
Controversial effects
on regulatory function
CytokinesecretionIL-13 and
IFN-g
Anti-CD137mAb
Memory
CD8+ T cell
Dendritic
cell
Activated
NK cell
Activated
CD4+ T cell
T regs?
IKDC?
NKT
cell
Tumour endothelium
Activated
CTL
Melero, et al. Trends Pharmacol Sci.2008
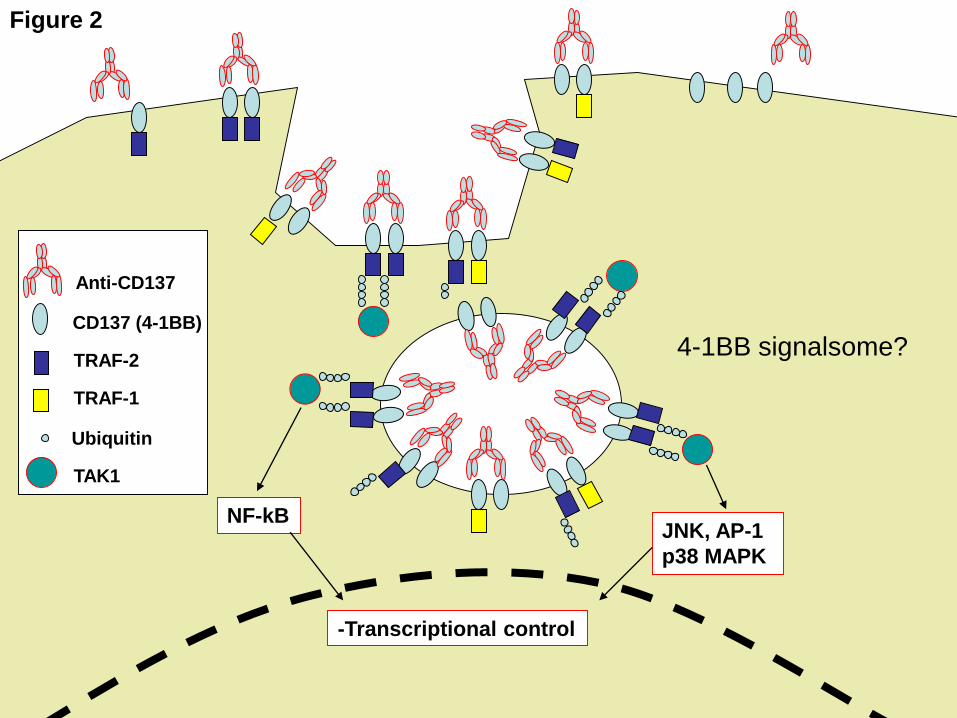
NF-kBJNK, AP-1
p38 MAPK
-Transcriptional control
Anti-CD137
CD137 (4-1BB)
TRAF-2
Ubiquitin
TAK1
4-1BB signalsome?
TRAF-1
Figure 2

Early signal transduction events from CD137.
Melero I et al. Clin Cancer Res 2013;19:1044-1053
©2013 by American Association for Cancer Research
SYNERGY
syn-ergos, συνεργός, meaning 'working
together'.

Strategies for immunotherapy combinations.
Melero I et al. Clin Cancer Res 2009;15:1507-1509
©2009 by American Association for Cancer Research

-OX40
Radiotherapy
Chemotherapy
Vaccination
T-reg depletion/
inactivation
Adoptive T-cell
immunotherapy
–Clinical Standard
–Clinical Trials
–Preclinical Studies
Antiangiogenic
therapy
-TIM-3
-LAG3
-CTLA-4
-CD137
-PD1
-PD-L1
-CD40
Virotherapy
or intratumoral
PAMPS

Spontaneous HCC (c-mycOVA75/tTALAP)
Ney et al, Hepatology 2009

HC
CLitte
rmate
Week 5
H&E OVA

Anti-CD137 + anti-PD-1 + anti-OX40

12/39
Combo3
d -21 d 0 d21
breeding Birth weaning
Dox
d25
TREATMENT
mAbs mAbs
Survival
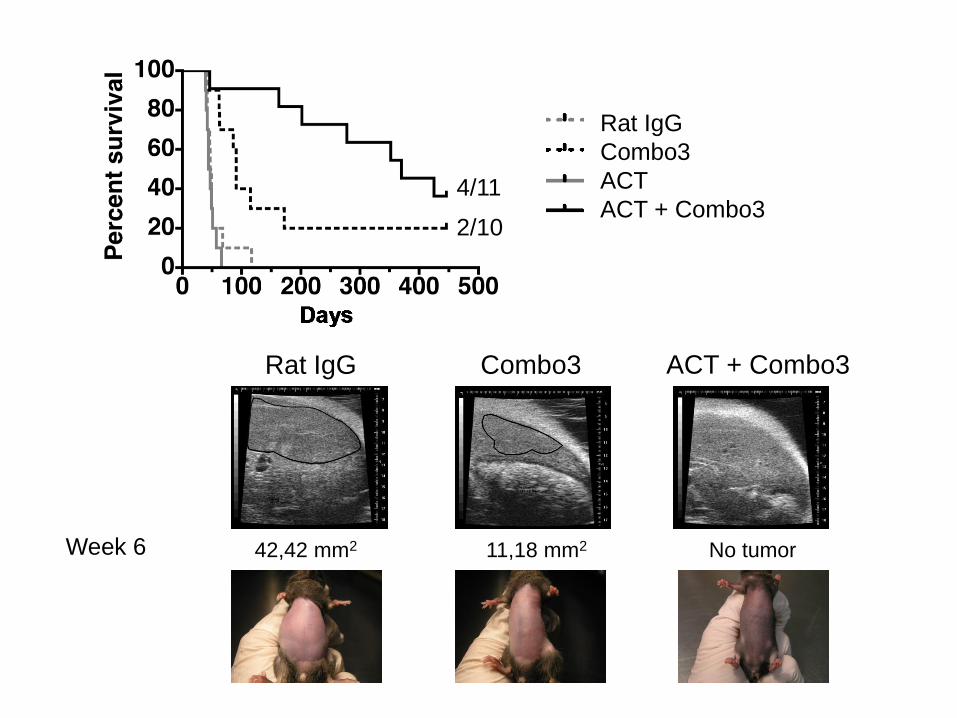
Rat IgG
Combo3
ACT
ACT + Combo3
Rat IgG ACT + Combo3Combo3
42,42 mm2 11,18 mm2 No tumor
4/11
2/10
Week 6

TILs
CD8+

alive/total
Combo3 efficacy is dependent on CD8+ T cells

GzmB Perforin FasL
Rat IgG
Combo3
17,8% 12,7
462 185
15% 4,5
143 23
1,4% 0,1
12 1
69,4% 6
2083 225
63,5% 0,4
371 7
3,1% 0,6
39 7
Effector machinery is enhanced upon Combo3 Tx
Gated on CD8 TILs
Synergy with adoptive T cell therapy

0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0
0
1 0 0
2 0 0
3 0 0
4 0 0
B 1 6 -O V A w /o T x
O T 1 + R a t Ig G
O T 1 w /o a b
0 /50 /50 /5
T im e (D a y s )
Tu
mo
r a
re
a (
mm
2)
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0
0
1 0 0
2 0 0
3 0 0
4 0 0
0 /6
T im e (D a y s )
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0
0
1 0 0
2 0 0
3 0 0
4 0 0
1 1 /1 1
T im e (D a y s )
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0
0
1 0 0
2 0 0
3 0 0
4 0 0
0 /5
T im e (D a y s )
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0
0
1 0 0
2 0 0
3 0 0
4 0 0
5 /6
T im e (D a y s )
Tu
mo
r a
re
a (
mm
2)
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0
0
1 0 0
2 0 0
3 0 0
4 0 0
0 /6
T im e (D a y s )
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0
0
1 0 0
2 0 0
3 0 0
4 0 0
0 /1 1
T im e (D a y s )
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0
0
1 0 0
2 0 0
3 0 0
4 0 0
1 /7
T im e (D a y s )
C o n tr o lsN o n -T C R tr a n s g e n ic
a c t iv a t e d T c e l ls + C D 1 3 7
O T -1 + C D 1 3 7
(T r e a te d o n d a y + 3 )
O T -1 + C D 1 3 7
(T r e a te d o n d a y + 7 )
O T -1 + C D 1 3 7
(C D 4 d e p le t io n )
O T -1 (C D 1 3 7 K O )
+ C D 1 3 7
O T -1 + C D 1 3 7
in C D 1 3 7 K O
O T -1 + C D 1 3 7
in R A G 1 K O
A B C D
E F G H

Figure 2.

0
5 0 0
1 0 0 0
1 5 0 0
2 0 0 0
M o u s e :
O T -1 :
A b :
W T C D 1 3 7 K O
1 D 8 R a t Ig G
2 3 7 ,5
0 ,0 0 69 ,5 0 5 4 2 7
p = 0 ,0 0 6 3
W T
W T W T W T
1 D 8
C D 1 3 7 K O
W T
1 D 8
MF
I
0
3 5 0
7 0 0
1 0 5 0
1 4 0 0
1 9 9 ,5
p = 0 ,0 0 2
p = 0 ,0 1 0 9
1 4 4
M o u s e :
O T -1 :
A b :
W T C D 1 3 7 K O
1 D 8 R a t Ig G
W T
W T W T W T
1 D 8
C D 1 3 7 K O
W T
1 D 8
0 ,0
1 6 ,5
MF
I
0
2 0 0
4 0 0
6 0 0
8 0 0
2 1 2
2 8 ,5 0 ,0
1 4 8
p = 0 ,0 2 6 7
M o u s e :
O T -1 :
A b :
W T C D 1 3 7 K O
1 D 8 R a t Ig G
W T
W T W T W T
1 D 8
C D 1 3 7 K O
W T
1 D 8
MF
I
0
1 6 0 0
3 2 0 0
4 8 0 0
6 4 0 0
1 3 7 2
p = 0 ,0 0 1 8
p < 0 ,0 0 0 1
p = 0 ,0 0 0 3
p = 0 ,0 3 1 1
1 8 2 4
2 7 4 ,5
M o u s e :
O T -1 :
A b :
W T C D 1 3 7 K O
1 D 8 R a t Ig G
W T
W T W T W T
1 D 8
C D 1 3 7 K O
W T
1 D 8M
FI
0
6 5 0 0
1 3 0 0 0
1 9 5 0 0
2 6 0 0 0 n s
5 2 32 5 2 0 ,5 1 7 1
M o u s e :
O T -1 :
A b :
W T C D 1 3 7 K O
1 D 8 R a t Ig G
W T
W T W T W T
1 D 8
C D 1 3 7 K O
W T
1 D 8
MF
I
0
3 0 0 0
6 0 0 0
9 0 0 0
1 2 0 0 0n s
2 0 0 ,00 ,0 1 5
M o u s e :
O T -1 :
A b :
W T C D 1 3 7 K O
1 D 8 R a t Ig G
W T
W T W T W T
1 D 8
C D 1 3 7 K O
W T
1 D 8
MF
I
S u r fa c e C D 1 0 7 a
S u r fa c e K L R G 1
In tra c e llu la r IF N g
T ra n s fe r re d C D 8+
E n d o g e n o u s C D 8+
A
B
C
Figure 3.


MS
D(µ
m2)
A B C
D
Unconfined tracks, low dwell time per tumour cell
α-CD137
Confined tracks, concentrated Dwell timehigh dwell time per tumour cell
Ctrl
0h 1h
0
50
100
150
200
CT
L :
tu
mo
ur
ce
llco
nta
ctd
ura
tio
n(m
in)
0
Tumour: F10 F10/OVA
2
4
8
6
10
12
Sp
ee
d(µ
m/m
in)
OT1OT1 + αCD137
OT1OT1 + αCD137
OT1OT1 + αCD137
0 20 40 60 80
dt (min)
0
1000
2000
3000
Weigelin, et al. PNAS in press



Tumor
Proliferation
Blood
vessel
Activation of
endothelial cells
Enhanced CTL effector
functions
Costimulation
Killing
A B
C
00:00 h 00:40 h 01:06 h
CTL mitosis00:00 h 00:14 h 00:32 h
Tumor cell apoptosis
OT1 CD8 T cells Blood vessels
B16F10/OVA melanoma cell nuclei
CD8 T cells B16F10/OVA melanoma cells
Autofluorescent tissue
Hot spots for extravasationOverview tumor lesion
500 µm
CTL migration tracks
Enrichment of potent
effector cells
Costimulation during
activation
Chimeric receptors
containing CD137cyt
Ligand binding
Transmembrane
Costimulatory
Signaling
CD137 -derived
Dendritic cell Migration track
CD8 T cellTumor cellα-CD137 mAb
TILAPC
Proliferation
Effector function
Cell culture flaskDomains:
Imm
uno
-magnetic
cell
sort
ing
Undesired cells
TIL
CD137 and adoptive T cell transfer. A perfect marriage?

PROFESSIONALCROSSPRIMING DENDRITIC CELLS


0 2 0 4 0 6 0
0
1 0 0
2 0 0
3 0 0
4 0 0
0 / 2 8
0 2 0 4 0 6 0
4 / 2 3
0 2 0 4 0 6 0
1 6 /2 3
0 2 0 4 0 6 0
8 / 9
0 2 0 4 0 6 0
0 / 1 6
0 2 0 4 0 6 0
0
1 0 0
2 0 0
3 0 0
4 0 0
0 / 2 4
0 2 0 4 0 6 0
0 / 1 6
0 2 0 4 0 6 0
0 / 9
Untreated αCD137 αPD-1 αCD137 + αPD-1
WT
Batf3-/-
Days post-inoculation
Tu
mo
r si
ze (
mm
2)
0 2 0 4 0 6 0 8 0
0
2 0
4 0
6 0
8 0
1 0 0 8/9
16/23
4 /23
W T C D 1 3 7 + P D - 1
W T C D 1 3 7
W T P D - 1
W T c o n tro l
***
0 2 0 4 0 6 0 8 0
0
2 0
4 0
6 0
8 0
1 0 0
B a t f3- / -
C D 1 3 7 + P D - 1
B a t f3- / -
C D 1 3 7
B a t f3- / -
P D - 1
B a t f3- / -
c o n t r o l
**
WT Batf3-/-
Per
cent su
rviv
al
Days post-inoculation Days post-inoculation
Crosspriming DC absolutely needed!

0 10 20 300
50
100
150
200
Control mAb
13%
CD137
Avera
ge t
um
or
siz
e (
mm
2)
0 10 20 300
50
100
150
200
250
Batf3-/-
Days post-inoculation
Avera
ge t
um
or
siz
e (
mm
2)
0 10 20 300
50
100
150
200
Batf3-/-
Days post-inoculation
Avera
ge t
um
or
siz
e (
mm
2)
0 10 20 300
50
100
150
200
33%
FLT3L+PolyIC FLT3L+PolyIC + mAb
-PD-1
Avera
ge t
um
or
siz
e (
mm
2)

IMMUNOAVATAR
MICE PROJECTS
0
50
100
150
hPBMCs
hIgG4hCD137
hPD-1
4 7 21Time (Days) 4 7 21 4 7 21 4 7 21
+ + ++ + + + + ++ + +- - -- + +- + +
- - -- - -- + +
- - -- + +- - -
- - -- - -
- + +
h-I
FNg
(pg
/mL
)
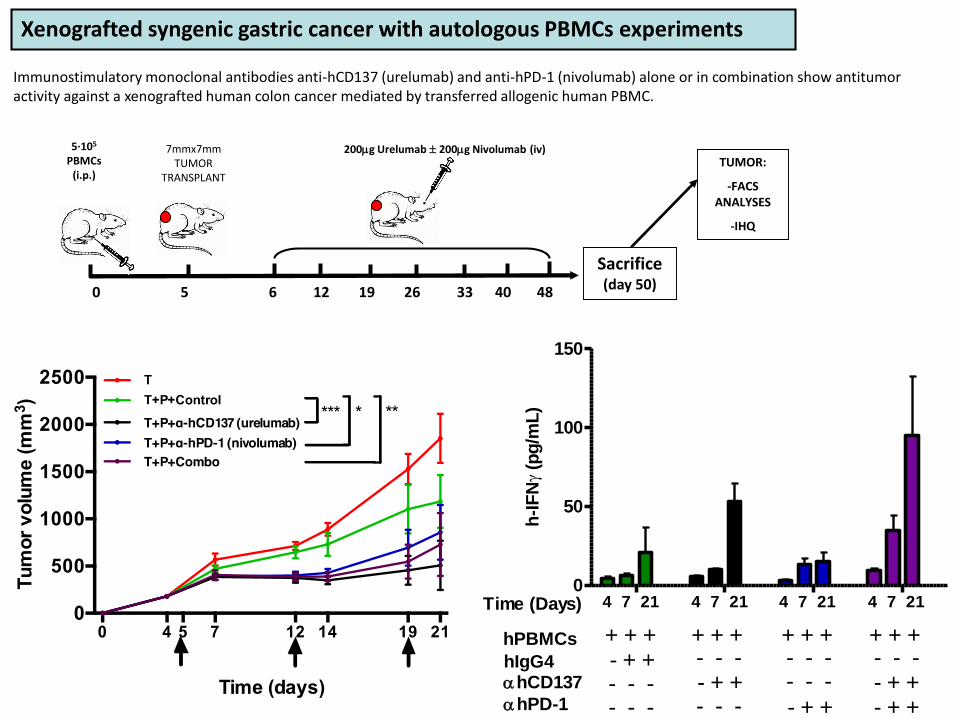
Xenografted syngenic gastric cancer with autologous PBMCs experiments
Sacrifice(day 50)
5·105
PBMCs(i.p.)
7mmx7mmTUMOR
TRANSPLANT
0 5 6 12 19 26 33 40 48
200g Urelumab 200g Nivolumab (iv)TUMOR:
-FACS ANALYSES
-IHQ
Immunostimulatory monoclonal antibodies anti-hCD137 (urelumab) and anti-hPD-1 (nivolumab) alone or in combination show antitumoractivity against a xenografted human colon cancer mediated by transferred allogenic human PBMC.

Xenografted syngenic gastric cancer with autologous PBMCs experiments
Co
mb
oα
-hC
D1
37
α-h
PD
-1C
on
tro
l
CD3/CD8/CD20/CK/DAPI
CD3/CD8/CD20/CK/DAPI
CD3/CD8/CD20/CK/DAPI
CD3/CD8/CD20/CK/DAPI
IgG4
-hCD13
7
-h
PD-1
Com
bo0.00
0.01
0.02
0.03
0.04
Tumor compartment
*
rati
o h
CD
3/t
ota
l p
are
cn
ch
ima c
ells
IgG4
-hCD13
7
-h
PD-1
Com
bo0.0
0.2
0.4
0.6
0.8Stromal compartment
rati
o h
CD
3/ to
tal str
om
a c
ells
Multiplexed immunofluorescence microphotographs showing the architecture of tumor xenografts

MINECO
Gob Navarra
EU FP7 & H2020
AECC
AICR
Fundación BBVA
Fundación CAN
OUR GRATITUDE GOES TO:
Patients and
their families
Central facilities at
CIMA and CUN