common medical procedures - weebly
TRANSCRIPT
Dr. Rodney Martinez
1

Hand washing is the single most important procedure for preventing the spread of infections.
Alcohol handrub should also be regularly used when entering or leaving a ward and before and after examining patients.
2
This is an important and routine procedure which is often carried out by nursing staff, although doctors may be asked to administer medication at times.
Good injection technique can make the experience for the patient relatively painless.
Three commonly used routes of administration are: ◦ subcutaneous (S/C), ◦ intramuscular (IM) and ◦ intradermal (ID).
3
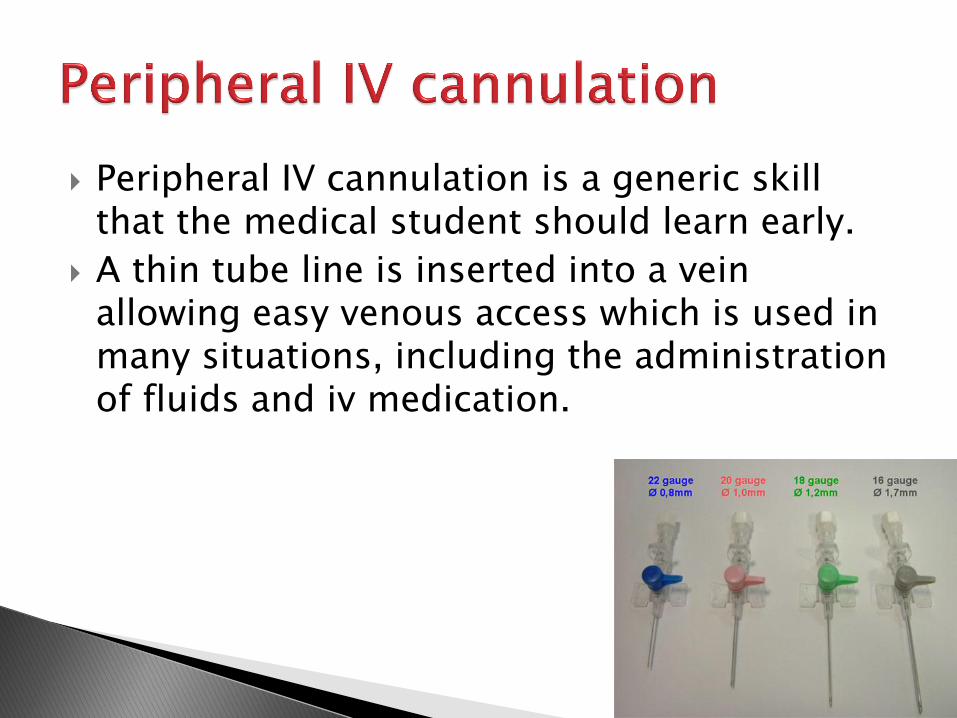
Peripheral IV cannulation is a generic skill that the medical student should learn early.
A thin tube line is inserted into a vein allowing easy venous access which is used in many situations, including the administration of fluids and iv medication.
4

Plastic tube is inserted through the nose, down the back of the throat, oesophagus and into the stomach.
5
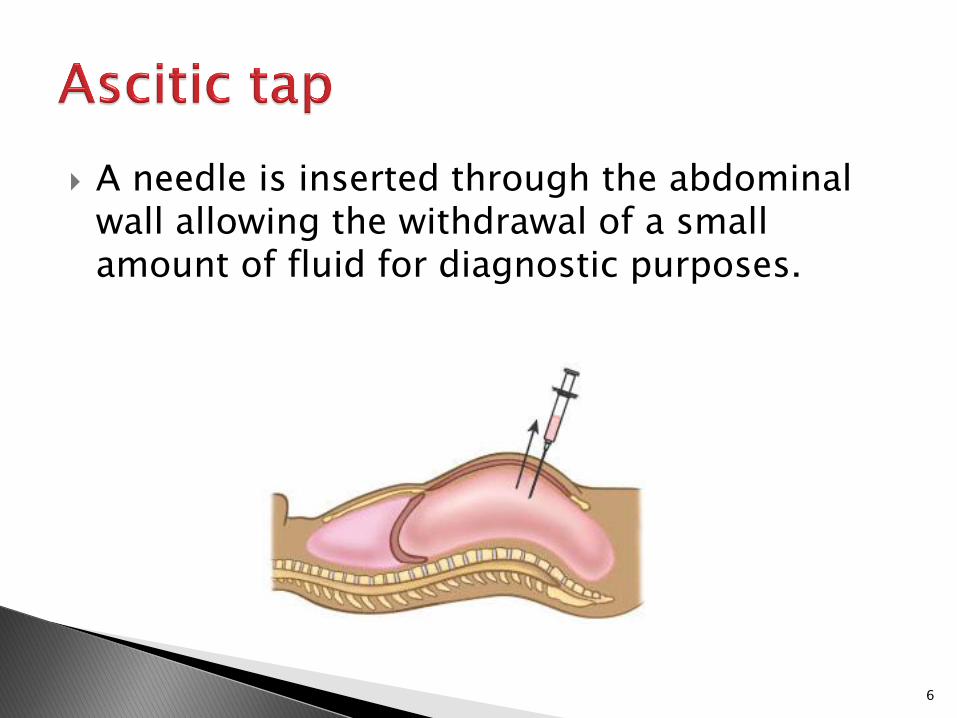
A needle is inserted through the abdominal wall allowing the withdrawal of a small amount of fluid for diagnostic purposes.
6
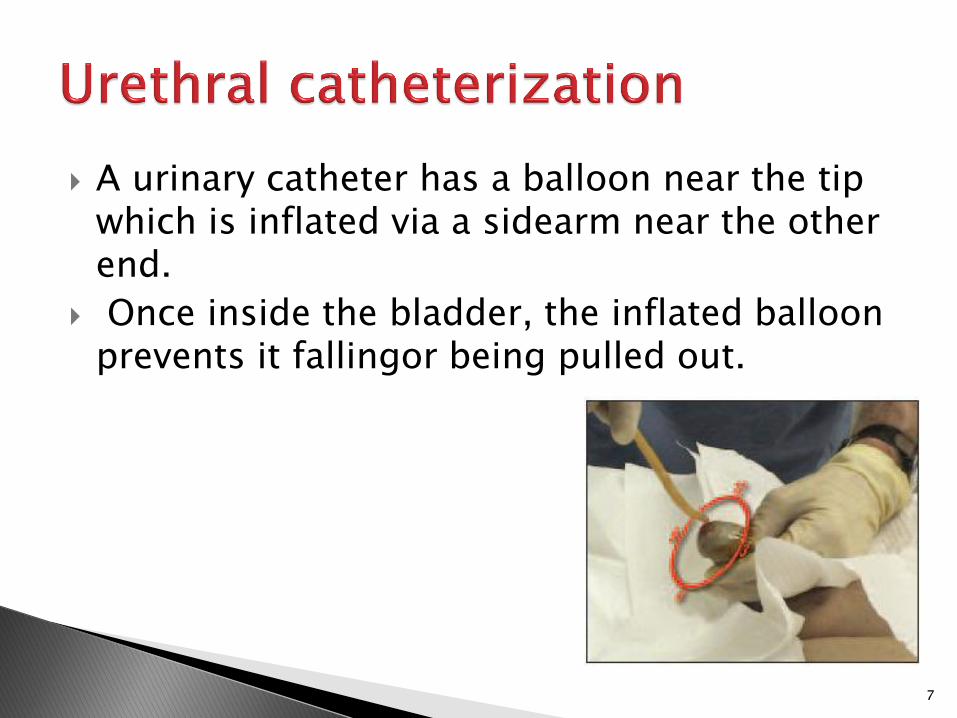
A urinary catheter has a balloon near the tip which is inflated via a sidearm near the other end.
Once inside the bladder, the inflated balloon prevents it fallingor being pulled out.
7
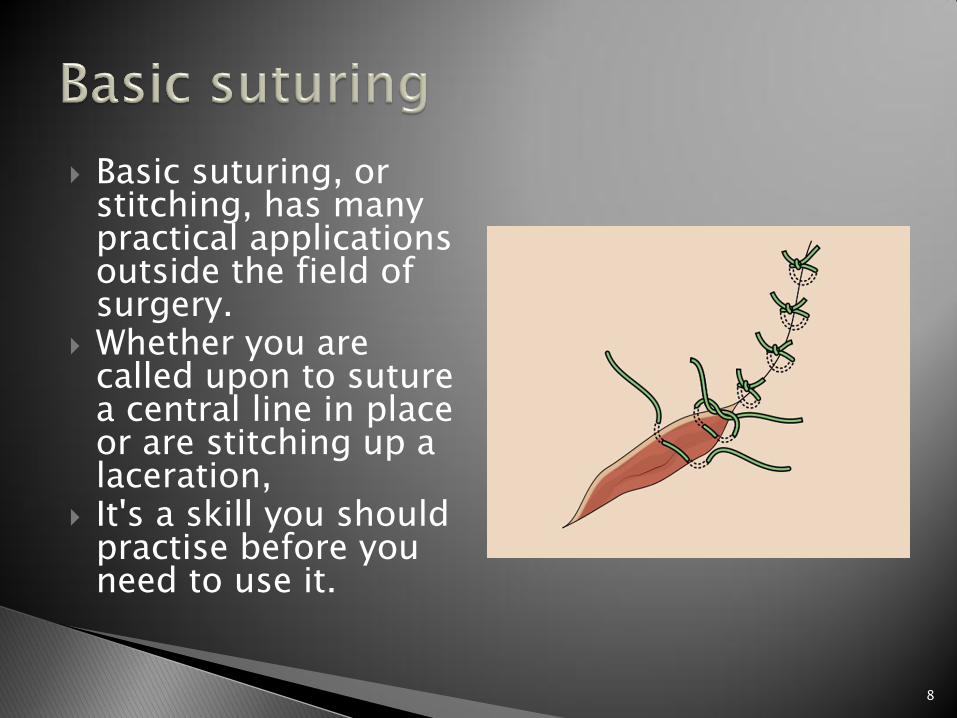
Basic suturing, or stitching, has many practical applications outside the field of surgery.
Whether you are called upon to suture a central line in place or are stitching up a laceration,
It's a skill you should practise before you need to use it.
8

In the context of a swollen joint, a joint aspiration is performed for both:
Diagnostic (to identify infectious and crystal arthropathies) and
Therapeutic (to relieve tense effusions and haemarthroses) purposes.
9

10
Insertion of a spinal needle through the L3-L4 interspace into the lumbar subarachnoid
space to obtain cerebrospinal fluid,
measure CSF fluid or pressure, or instill air, dye, or medications.
11
DIAGNOSTIC Suspected meningitis Subarachnoid hemorrhage Hydrocephalus Benign Intracranial hypertension
THERAPEUTIC Spinal anesthesia Chemotherapy
12

CONTRAINDICATIONS
-coliosis -CP unidentified -oagulopathy -yphosis
S I C K
13

PRETEST orm of informed consent ree of urine bladder etal position
F F F
14

INTRATEST
hrimp or Fetal position
pecimens to be collected
terile vials- 4
trict asepsis
S S S S
15
POSTTEST lat 12-24 hrs or vital signs and LOC
monitoring orce fluid unless
contraindicated uncture site for bleeding,
CSF leakage erform CMS assessment
F F F p p
16

COMPLICATION
Spinal Headache
-lat
-luids
-ain Management
F F P
17

-valuates heart rate and the regularity of heartbeats.
-ardiac dysrhythmias, MI, and cardiac hypertrophy
- raph of the electrical impulses moving through the heart.
E C G
18
Consideration: -lectrical shock will not occur
-ardiac medications of the patient should be documented
-ive instructions to lie still, breathe normally, and refrain from talking during the test
E C G
19

PRECORDIAL LEADS
White: Right Arm Black: Left Arm Green: Right Leg Red: Left Leg
20

LIMBS LEADS
21
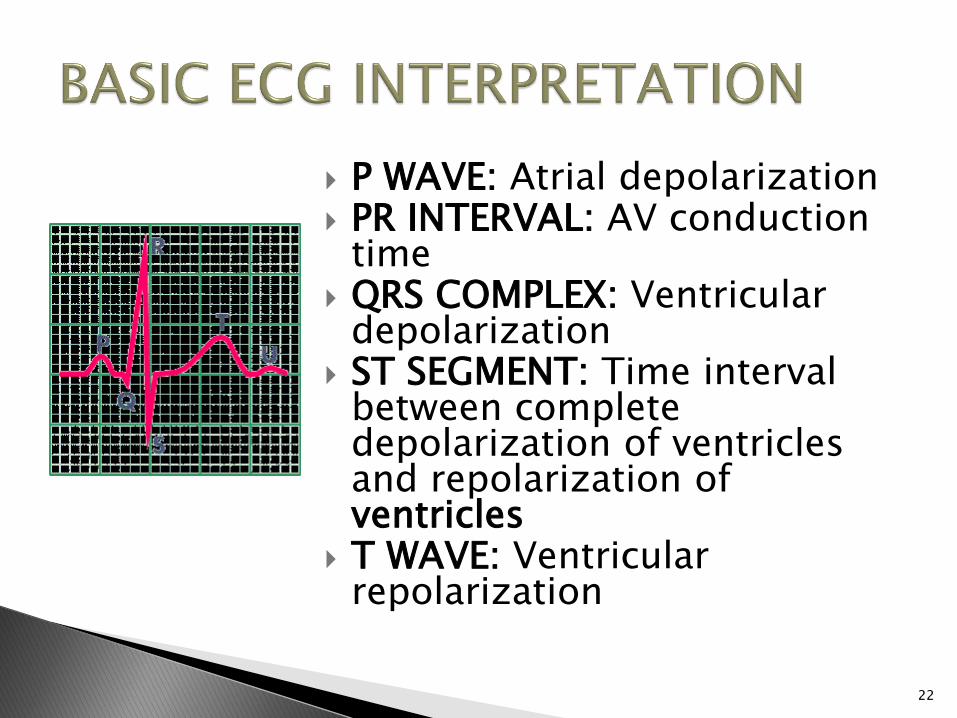
P WAVE: Atrial depolarization PR INTERVAL: AV conduction
time QRS COMPLEX: Ventricular
depolarization ST SEGMENT: Time interval
between complete depolarization of ventricles and repolarization of ventricles
T WAVE: Ventricular repolarization
22

NORMAL SINUS RHYTHM: 60 TO 100 bpm
SINUS BRADYCARDIA: <60 bpm
SINUS TACHYCARDIA: >100 bpm
QRS WIDTH: 0.08 to 0.12 sec PR INTERVAL: 0.12 to 0.20
sec QT INTERVAL: 0.30 to 0.40
sec
23
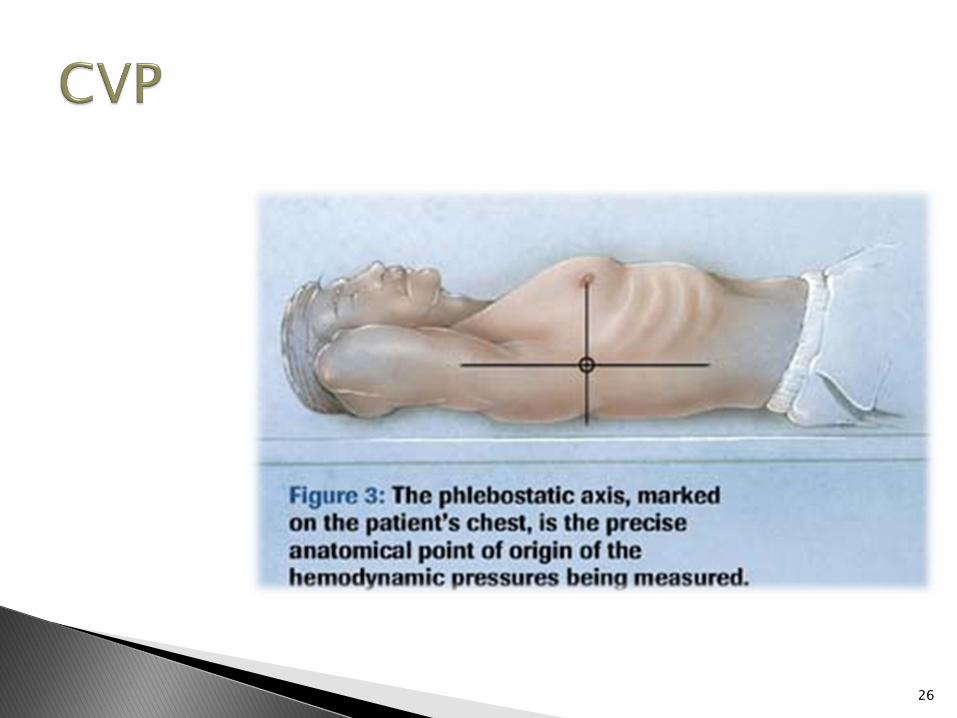
-atheter is attached to an IV infusion and H2O manometer by a three way stopcock
-eins external jugular, antecubital, or femoral
- ressure within the superior vena cava
C V P
24

Normal Value: 3 to 8 mmHg Position: Cardiac Disease: Semi
Fowler’s Dressing or Tubing Change:
Flat or Trendelenburg CVP Reading and Monitoring:
Flat, Supine, or Dorsal Recumbent
Air Embolism: Left Side Lying
25
26

Ericardial
effusion
uncture
ericardial sac
ericardial fluid
P P P P
27

PREPROCEDURE erform blood analysis CG estriction of food and water is recommended for six hours before the test.
V line for sedation
P E R I
28

INTRAPROCEDURE vail emergency resuscitative equipment at bedside
ed is elevated to 45 to 60 degrees
ardiac activity monitoring one in emergency room, ICU, or at the bedside
A B C D
29

POSTPROCEDURE
pical pulse monitoring lood pressure VP etect complications:
Ventricular or coronary artery puncture, dysrhythmias, pleural laceration, gastric puncture, myocardial trauma
A B C D
30

31

Purposes: -pply medications
-rush biopsy
-arefully remove foreign objects
-irect visualization
A B C D
32

PREPROCEDURE: tain informed consent emove dentures or eyeglasses btain vital signs PO postmidnight oagulation studies result must be
checked ave emergency resuscitation
equipment readily vailable give IVF and medication for
sedation uction equipment at bedside
B
O N
C
H
U
S
R
33

POSTPROCEDURE: ag reflex return ssess for bloody sputum ive instruction that sore throat is
common espiratory status must be monitored mesis basin at bedside owler’s semi position ook out for complications like
bronchospasm or bronchial perforation
levated temperature and DOB- Notify! amine vital signs
G A G R E F L E X
34

Insertion of a needle through the chest wall:
Obtain specimen
Remove pleural fluid accumulation
Instill medication
35

36

PREPROCEDURE: o obtain informed consent ealth teaching: not cough, breathe
deeply, or move during the test n doctor's office, in the X-ray
department, ER, OR or at bedside idden on bed: Sidelying towards the
unaffected side with HOB elevated mbulatory: Sit upright with arms and
shoulders supported by a table -ray or ultrasound before the
procedure
T H O R A X
37

POSTPROCEDURE: Monitor vital signs
Monitor respiratory status
Apply a pressure dressing
Assess the puncture site for bleeding and crepitus
Monitor for signs of pneumothorax, air embolism, and pulmonary edema
38

C-ulture
C-ytological
exam
P-ulmonary
lesion
P-leural
effusion
39
PREPROCEDURE: -et the patient signs informed consent
-se of local anesthesia, pressure during insertion of needle
-PO -ive analgesics and sedatives as prescribed
L U N G
40
POSTPROCEDURE: -ital signs must be monitored -nspect biopsy site for drainage
or bleeding -n biopsy site dressing must be
applied -neumothorax and air embolism -igns of respiratory distress must
be monitored -ou prepare the patient for chest
x-ray
B I
O P S Y
41

Measuremet Oxygen Carbon dioxide
Arterial blood
Acid base state
42

PREPROCEDURE: -llen’s test before drawing radial artery specimens
-efore specimen collection, client to rest for 30 minutes
-iving suction before drawing ABG sample is avoided
A B G
43

POSTPROCEDURE:
Place the specimen on ice
Note the client’s temperature on the laboratory form
Note the oxygen and type of ventilation that the client is receiving on the laboratory form
44

POSTPROCEDURE: Apply pressure to the puncture site for 5 to 10 minutes or longer if the client is taking anticoagulant therapy or has a bleeding disorder
Transport the specimen to the laboratory within 15 minutes
45
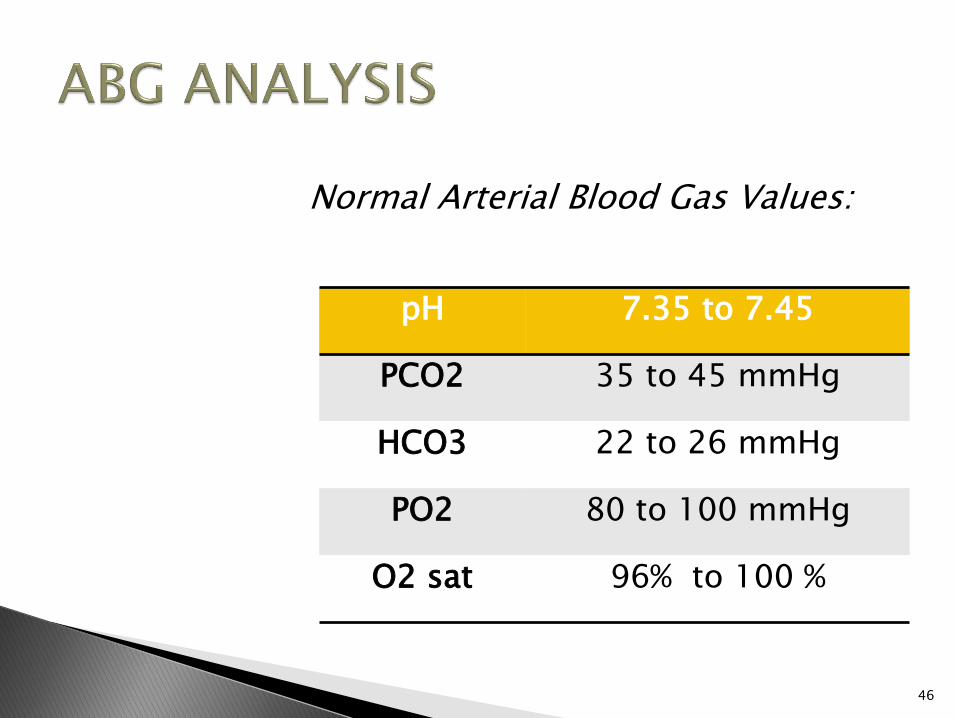
Normal Arterial Blood Gas Values:
pH 7.35 to 7.45
PCO2 35 to 45 mmHg
HCO3 22 to 26 mmHg
PO2 80 to 100 mmHg
O2 sat 96% to 100 %
46
R-espiratory
O-pposite
M-etabolic
E-qual
47

Sustained
Maximal
Inspiration
48

49

INDICATIONS:
Upper-abdominal surgery
Thoracic surgery
Surgery in patients with chronic obstructive pulmonary disease
Pulmonary atelectasis
Presence of a restrictive lung defect associated with quadraplegia and/or dysfunctional diaphragm.
50
Considerations PREPROCEDURE -void smoking or eating heavy meal
for 4 to 6 hours before the test -e sure to remove dentures -onsult with the physician regarding
holding bronchodilators before testing
-etermine whether analgesic that may depress the respiratory function is being administered
-ncourage to void and wear loose clothing
A B C D E
51

Considerations
POSTPROCEDURE
Resume:
Diet
Bronchodilators
Respiratory treatments
52

determines the effectivity of bronchodilator for asthmatic patients
53
Management: 1. Diary 2. Weeks period that the child
is well 3. Blows Results: GREEN: 80 to 100%... Very
Good YELLOW: 50 to 80%...
Beginning Attack RED: <50%... Bring to ER
54