common pediatric rashes jfk pediatric core curriculum mgh center for global health pediatric global...
TRANSCRIPT
Common pediatric rashesJFK pediatric core curriculum
MGH Center for Global HealthPediatric Global Health Leadership Fellowship
Credits:Brett Nelson, MD, MPH
Sohil Patel, MD

Discussion outline
• Dermatology terminology
• Common benign newborn rashes
• Common infectious newborn rashes
• Newborn vascular lesions
• Various other pediatric rashes

Common dermatology terms• Macule: circumscribed change in skin color without elevation or
depression• Papule: solid elevated lesion usually <0.5 cm in diameter• Plaque: raised lesion >0.5cm in diameter• Wheal (hive): rounded or flat-topped elevated lesion formed by local
dermal edema• Purpura: non-blanching erythema or violaceous color due to
extravasation of blood• Nodule: palpable solid lesion of varying size• Vesicle: circumscribed elevated lesion which contains free fluid and
is <0.5 cm in diameter• Bulla (blister): same as vesicle but with diameter >0.5 cm• Cyst: sac containing liquid or semisolid material usually in the
dermis• Pustule: circumscribed elevated lesion which contains pus• Abscess: collection of pus in the dermis or subcutis
Benign newborn rashes
• Erythema toxicum neonatorum• Miliaria• Neonatal acne• Milia• Seborrheic dermatitis• Benign pustular melanosis of the newborn• Sucking blisters
Presented in random order….


Miliaria
• Due to obstruction and rupture of exocrine sweat duct
• Commonly seen secondary to thermal stress, particularly with crops of lesions over face, scalp, and trunk– Important to ensure infant is not over-wrapped– Once heat stress is removed, lesions usually
resolve quickly


Neonatal acne
• Can be present at birth or develop in first 2-4 weeks of life
• Consists of pustules over the cheeks primarily, but also involves other areas of face and scalp
• No comedones in neonatal form• Resolves spontaneously and without
scarring



Benign pustular melanosis of the newborn
• Lesions present at birth• Superficial pustules which rupture easily without
pus content, leaving spot of hyperpigmentation• Pustules last 1-2 days but pigmented spots may
persist for a while • Any area of the body may be involved• Smears from pustules reveal polymorphonuclear
leukocytes with absence of organisms


Seborrheic dermatitis
• Primarily affects scalp and intertriginous areas– Involvement of scalp is frequently termed "cradle cap“
and manifests as greasy, yellow plaques on scalp • Most common in first 6 weeks of life, but can
occur in children up to 12 months of age • Usually clears up without treatment in 3-4 weeks
– If needed, treatment can include mild tar shampoo, oatmeal baths, avoidance of soaps, and occasional use of mild topical steroid
– Involvement of skin creases can lead to secondary candidal infections
• Etiology unknown

Erythema toxicum neonatorum
• Onset on day 2-3 of life, mostly in term babies– Lesions wax and wane over ensuing 3-6 days– Lesions may intensify or coalesce particularly in
response to local heat
• Central white-yellow papule surrounded by a halo of erythema, mainly over trunk (but also on limbs and face)
• Scrapings of lesions would reveal eosinophils• Etiology unknown


Milia
• Tiny, white, usually discrete papules– Inclusion cysts that contain trapped keratinised stratum corneum
• Commonly occur on face and scalp• Usually resolve within a few months without treatment• Rarely associated with dermatologic syndromes
– Epidermolysis bullosa, oro-facial-digital syndrome (type 1)
• Similar lesions may occasionally be seen in mouth– When on hard palate, called Epstein's pearls– When on alveolar ridges, called alveolar cysts or Bohn's nodules


Sucking blisters
• Present at birth, most often over dorsal and lateral aspect of wrist – Either bilateral or unilateral
• May appear like well-demarcated bruises or vesicles
• Infant is noted to exhibit excessive sucking activity

Infectious newborn lesions
• Staphylococcal pustules• Herpes simplex• Generalized in utero infection• Paronychia• Bullous impetigo• Omphalitis• Congenital syphilis• Candida Dermatitis
Presented in random order….


Paronychia
• Localized inflammation with infection of nail fold• Relatively common in infants• Treat most infections with oral antibiotics and
severe cases with IV antibiotics– First line treatment is usually flucloxacillin/floxacillin
for Staphylococcus aureus or Streptococcus pyogenes
– For chronic lesions, consider Gram-negative organisms or Candida as potential causes


Bullous impetigo
• Skin infection typically caused by Staphylococcus aureus
• Lesions tend to appear DOL 5-10• Any body site may be involved, with predilection
to diaper area• Bullae are flaccid, containing straw colored or
turbid fluid– Rupture easily leaving moist denuded area (“honey-
crusted lesions”)• Treatment with systemic antibiotics, particularly
for lesions around umbilicus


Staphylococcal pustule
• Typically seen first few days of life• Predilection to neck, axilla, and inguinal areas• Nearly always caused by Staphylococcus
aureus• If one lesion, may be treated "expectantly" with
application of chlorhexidine (mainly to prevent spread)– However, if more than one lesion, oral antibiotics are
indicated after culture is taken– For pustules in periumbilical area, consider systemic
antibiotics



Herpes simplex
• May involve skin, mouth, or eye• Lesions typically develop DOL 5-10• Grouped vesicles may be seen, often in linear
distribution if affecting limbs (1st slide)• If vesicle eroded, shallow ulcer with
erythematous base may be seen (2nd slide)• May have associated lesions on lips -- similar to
those of "cold sore" in an adult
Herpes Simplex: SEM
• HSV infection develops in one of three patterns, with roughly equal frequency– Localized to the skin, eyes, and mouth (SEM)– Localized CNS disease– Disseminated disease involving multiple organs
• Can develop anytime between birth and four weeks
• Patients with disseminated disease present earliest, often within the first week after delivery, although CNS symptoms usually occur during the second or third week
Discussion point:How do you differentiate HSV from impetigo from staph from
millia?


Omphalitis
• Infection of umbilical stump – Erythematous, edematous, +/- exudative
• Most commonly occurs after day 3• Infective organisms are variable, but
S.aureus, S.pyogenes, and Gram-negative organisms are common– If cultures available, swab affected area for
Gram-stain and culture to guide treatment– Initiate IV antibiotics

Congenital syphilis
• Dermatological findings quite variable– Classically involve palmar/plantar, perioral, and anogenital
regions
• Early lesions include petechiae, hemorrhagic vesicles, and bullae
• Lesions extremely infectious• May have extracutaneous findings
– Hepatomegaly, low birth weight, thrombocytopenia, anaemia, jaundice, respiratory distress, osteochondritis, hydrops fetalis, meningitis, chorioretinitis, and pseudoparalysis
– Older infants may present with "snuffles" (syphylitic rhinitis) which, in early stages, may be mistaken for URI
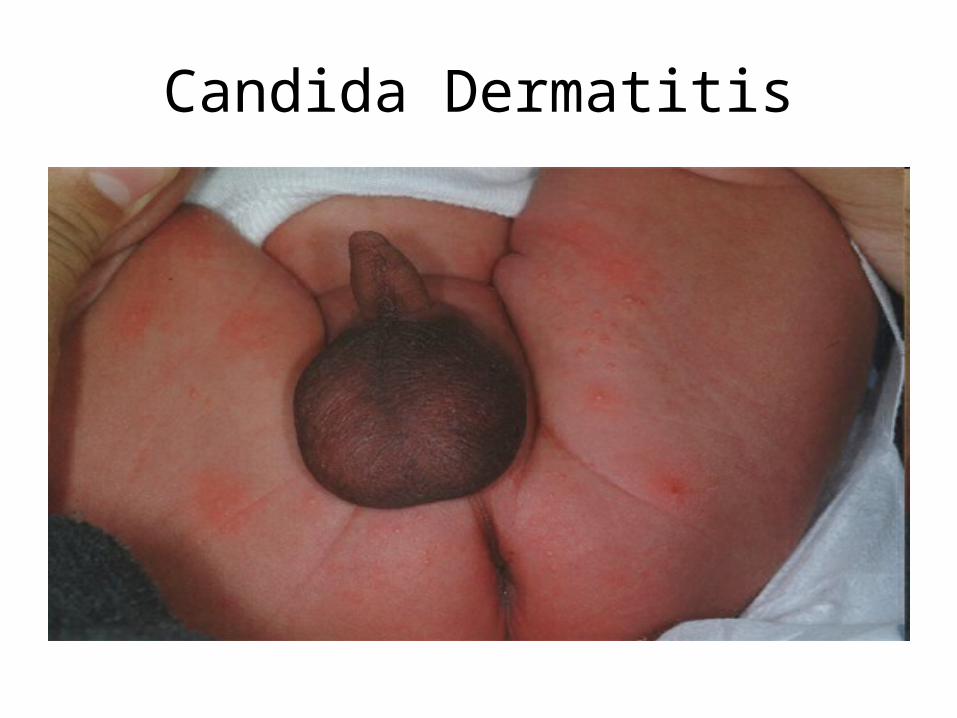
Candida Dermatitis
• A common condition of young infants• Most commonly caused by C. albicans• Characteristically appears as an erythematous
rash in the inguinal region• Classically has areas of confluent erythema with
discrete erythematous papules and plaques with superficial scales
• Satellite lesions are typically noted
Candida Dermatitis
Newborn vascular lesions
• Harlequin phenomenon
• Cutis marmorata


Cutis marmorata
• Reticulated pattern of constricted capillaries and venules– Often called "mottling“
• Due to vasomotor instability in immature infants• Generally resolves with increasing age and for
most infants is of no significance– However, may reflect underlying poor perfusion– Infants who develop mottling and are unwell need to
be clinically evaluated for sepsis and other illnesses


Harlequin phenomenon
• Striking reddening of one side of body and blanching of other half
• Each episode may last from seconds to minutes
• Episodes occur most often during first few days of life
• Thought to be vascular manifestation of changes occurring in newborn’s autonomic system

Various other pediatric rashes
Adapted from:Paul Geltman, MD, MPH and
Johns Hopkins DermAtlas
The following are ~80 slides to be used as time permits – possibly during a second lecture session. Some
photos may contain nude anatomy and would not be appropriate for openly public display.
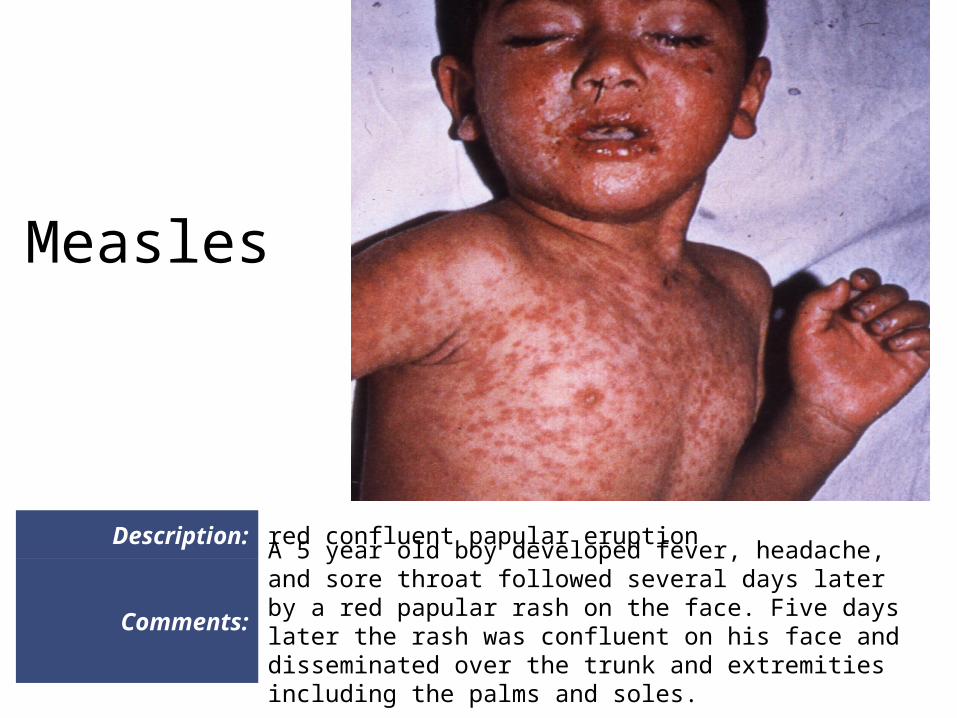
Description: red confluent papular eruption
Comments:
A 5 year old boy developed fever, headache, and sore throat followed several days later by a red papular rash on the face. Five days later the rash was confluent on his face and disseminated over the trunk and extremities including the palms and soles.
Measles

[The remainder of these ~80 slides have been temporarily removed from this
lecture due to space limitations. The full lecture (25MB) is available from