common reproductive concerns presented by: rahhegeh awni 1
TRANSCRIPT

Common Reproductive Concerns
Presented by: Rahhegeh Awni1

Pathophysiology of menstrual loss
-Immediately prior to menstruation intense spiral arteriole vasoconstriction occurs .
- -The spiral arterioles dilate and menstrual bleeding
occurs.
- Platelet adhesion in endometrial vessels is initially suppressed but with increased blood extravasation, damaged vessel ends are sealed by intravascular plugs of platelets and fibrin

-By 20 hours after the onset of menses, when most of the endometrial sheddinghas occurred, haemostasis occurs by intense spiral arteriole vasoconstriction.
-Endometrial regeneration begins within 36 hours of the onset of menses, while some shedding is still occurring.

The normal menstrual cycle.
Length 28 ± 7 daysDuration of menstrual flow 4 ± 2 daysMenstrual blood loss: 40 ± 20ml1
95% of normal women lose less than 60 ml of blood witheach menses .
Loss >80 ml is correlated with a lower meanhaemoglobin, haematocrit and serum iron level.


ASSOCIATED MENSTRUAL CONDITIONS
An abnormally short duration of menstrual flow is termed hypomenorrhea; an abnormally long one is called
hypermenorrhea. Excessive, profuse flow is calledmenorrhagia, and bleeding between periods is known
as metrorrhagia. Infrequent and too frequent menses are termed oligomenorrhea and polymenorrhea, respectively.

Definitions applied to abnormal uterine bleeding
1 -Dysfunctional uterine bleeding – abnormal uterine bleeding with nodemonstrable organic cause from the reproductive tract
2 -Menorrhagia – bleeding greater than 80ml occurring at regular intervals
3 -Metrorrhagia – irregular uterine bleeding at frequent intervals that is variable
4 -Menometrorrhagia – uterine bleeding that is prolonged and occurs at completely irregular intervals
5 -Polymenorrhoea – uterine bleeding occurring at regular intervals less than 21 days

6 -Intermenstrual bleeding – bleeding between periods of variable amounts
7 -Postmenopausal bleeding – bleeding occurring at more than 1 year after the last menses in a woman with ovarian failure
8 -Postcoital bleeding – bleeding occurring after intercourse
9 -Premenstrual spotting – scanty bleeding that occurs a few days to a week before menses

Menstrual Disorders
Women typically have menstrual cycles or approximately 40 years.
Once the predictable patterns is established, women may worry about any deviation from that patterns.
Menstrual disorders can be a source of severe distress & concerns for a woman as she wonder what is wrong.
9

The common menstrual problems
Amenorrhea Menorrhagia Dysmenorrhea metrorhgia Cyclic perimenstrual pain & discomfort.
Alterations in cyclic bleeding.
10

Amenorrrhea
Amenorrhea: is the absence or cessation of menstrual flow, is a clinical sign of a variety of disorders.
When amenorrhea is a clinical problem?1. The absence of both menarche & secondary sexual
characteristics by age 14.
2. The absence of menses by age of 16 regardless of presence of normal growth and development ( primary amenorrhea)
3. A 6-month cessation after a period of menstruation ( secondary
amenorrhea).
11

Cont..
Exercise –associated amenorrhea can occur in women undergoing vigorous physical & athletic training.
Stress-associated amenorrhea in the adolescent is likely similar to the disorder found in young reproductive-aged adults and is termed hypothalamic amenorrhea. The key defect is an abnormality in the secretion of GnRH
(James H & Arthur H. 2008)
Amenorrhea is one of the clinical signs of anorexia nervosa Calcium loss of bone as seen in postmenapausal women may
occur
12
Primary amenorrhea
-Primary amenorrhea: the absence of menstruation by age 16.
Prevalence: 1-2 % of girls in USA

Secondary amenorrhea
-Is the absence of menstruation for more than 6 months or for more than three cycles for a woman who had previously regular menstruation.
Prevalence: 2-5 % of women

causes
-Dysfunctional hypothalamus 35% caused by drugs, stress, diet and exercise.
2 -Polycystic ovarian dysfunctio 30%.
3 -Pituitary disease 20% like microadenomas
4 -Premature ovarian failure

Causes of Amenorrhea in general
1. Pregnancy.
2. Interruption in the hypothalamic-pituitary-ovarian-uterine axis.
3. Anatomic abnormalities.
4. Endocrine disorders (hypothyroidism or hyperthyroidism)
5. Chronic diseases (type 1 DM)
6. Medications ( phenytoin)
7. Eating disorders.
8. Strenuous exercise.
9. Emotional distress
10. Oral contraceptive use.
11. menapause
16

Research Findings
A qualitative study investigated Brazilian women's views regarding the suppression of menstruation using hormones.
Sixty-four women, 21–51 years old participated in the study.
Women see that menstruation associate with femaleness, youth, fertility and health.
Most women, although they would like to be free from menstruation, feared negative consequences of induced amenorrhea
(Amaral M et al. 2005)
17

Hypogonadtropic amenorrhea
Reflecta a problem in hypothalamic pitiutary axis.
CAUSES -Lesions or genetic inability to produce
FSH&LH. -Hypothalamic suppression as a result of
stress, body fat to lean ratio is inappropriate.

Assessment
-Assessment begins with thorough history and physical examination.
-Confirm that woman is not pregnant
-Assessment process depends on a woman’s age, and whether or not she has previously menstruated.

TREATMENT
- -Treatment for amenorrhea depends on the underlying cause .
- - Sometimes lifestyle changes can help if weight, stress, or physical activity is causing the amenorrhea .
- -Other times medications and oral contraceptives can help the problem .
-- contact of health care provider.

Management
Counseling & educating of pts are primary interventions Decrease or discontinue medications known to affect
menstruation. Many causes are reversible as weight loss and strss Correct weight loss Deal effectively with psychological stress Deep breath exercise & relaxation techniques Decrease the intensity or duration of vigorous exercise
21

Cont.
- -Adolescents may take promocripitine (paroldil) which can reduce high prolactin level by acting on the hypothalamus and initiating menstruation each month.
- -If menstrauation is delayed and pregnancy is suspected it should be stopped

Menorrhagia

Menorrhagia is an abnormally heavy and prolonged menstrual period at regular intervals.
-Depending upon the cause, it may be associated with abnormally painful periods) dysmenorrhea.(

-Menorrhagia affects approximately 20 per cent of otherwise healthy women (i.e. it adversely affects lifestyle) and approximately 5 percent of women of reproductive age will consult their general practitioner
with menstrual dysfunction .
-Up to 20 per cent of women have a hysterectomy by the age of 60 and in 50 per cent a normal uterus
is removed .

signs and symptoms
-Menstrual flow that soaks one or more sanitary pads or
tampons every hour for several consecutive hours -The need to use double sanitary protection to control your
menstrual flow -The need to change sanitary protection during the night
-Menstrual periods lasting longer than seven days -Menstrual flow that includes large blood clots
Heavy menstrual flow that interferes with regular lifestyle -Tiredness, fatigue or shortness of breath (symptoms of anemia)(

causes
-Anatomic lesion
-Inflammatory process
-Blood dyscarsias
-Systemic disease
-Carcinoma
-Hormonal change

CONT.
-Fibroids
-Endomeriosis
-Endometrial cancer
-Anticoagulant
-DUB
-Hyperthyroidism
-haemophilia

Medical conditions to be excluded asa cause of menorrhagia
1 -Hypothyroidism
-Hypothyroidism may be associated with abnormal uterine bleeding.
-With normalisation of the thyroid-stimulating hormone (TSH)
women become euthyroid and abnormal uterine bleeding resolves.

2 -Liver disease
Cirrhosis of the liver interferes with the ability to metabolise and conjugate oestrogens.
Thus the levels of free oestrogen are increased,
causing hyperstimulation of the endometrium and uterine bleeding.

3 -Iatrogenic causesThese include steroids used for contraception, hormone replacement therapy, corticosteroids, anticoagulants, tranquillizers, antidepressants,digitalis, dilantin and intrauterine devices.
Medical management of menorrhagea
1 -Antifibrinolytic agentsTranexamic acid – an antifibrinolytic Dosage: 1–1.5 g orally three to four times daily for the period ofbleeding.This is the first line of therapy.
The action of tranexamic acid is via a strong inhibitory effect onthe activation of plasminogen, i.e. the conversion of plasminogen toplasmin in the fibrinolytic system .
It is excreted unchanged in theurine.
Maximal levels are achieved within 2–3 hours. It results in a 50 per cent reduction in menstrual blood loss (MBL).
Success is greatest in women with the greatest loss of menstrualblood.

2-Aminocaproic acid
Dosage: 3g four times a day .
It reduces menstrual blood loss by up to 60 per cent of women compared with pretreatment values.
-The reduction in menstrual loss does not persist after stopping RX.

3 -The combined oral contraceptive pill
Reduces average MBL by 40–50 per cent
70–80 per cent of patients benefit
Few side effects
Avoid in women aged >35 who are cigarette smokers
Avoid in those with a body mass index (BMI) of >30

4 - Non-steroidal anti-inflammatory drugs (NSAIDs)
are effective in reducing menstrual blood loss in women with menorrhagia.

SURGICAL TREATMENT
-Up to 50 per cent of hysterectomies are done for dysfunctionaluterine bleeding .
Mortality for hysterectomy is 6–11 per 10 000 proceduresand morbidity is 3–40 per cent .
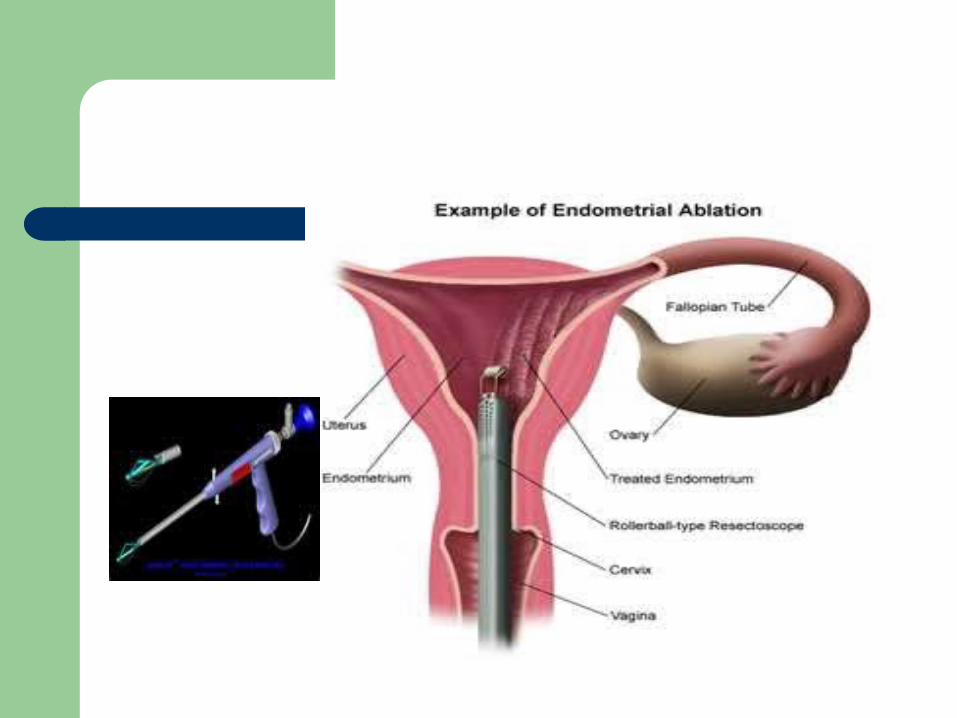
-Operative complications from ablation may occur in up to 6 per cent for first time procedures,and 15 per cent for repeat ablation .
-Patient satisfaction with endometrialablative techniques, including transcervical resection of theendometrium, is high-

Cyclic perimenstrual pain & discomfort
Cyclic perimenstrual pain & discomfort (CPPD): a new concept develop by nurse science team, it is a health problem can have a significant impact on the quality of life or a woman.
CPPD includes:
1. Dysmenorrhea
2. Premenstrual syndrome (PMS)
3. Premenstrual dysphoric disorders (PMDD)
38

Dysmenorrhea
Dysmenorrhea, or painful menstruation, occurs at or a day before the onset of menstruation
and disappears by the end of menses .
Dysmenorrhea is classified as primary or secondary.

Dysmenorrhea
Dysmenorrhea is the most common gynecologic problems in women
Many adolescents have dysmenorrhea in the first 3 years after menarche.
40

Cont..
Young adult women ages 17-24 years are most likely to report painful menses.
Symptoms usually begin with menstruation. The range and severity of symptoms are
different from woman to woman, and from cycle to cycle in the same woman.
Symptoms may last several hours to several days.
41

Cont..
Pain is usually located in the suprapubic area or lower abdomen.
Pain is described as sharp, cramping, or gripping, and it may radiate to the lower back or upper thigh.
42

Risk factors
Smoking Obesity Early menarche Nulliparity Stress
43

Cont..
Dysmenorrhea is differentiated as:
1. Primary dysmenorrhea
2. Secondary dysmenorrhea
44

Primary dysmenorrhea
-Primary dysmenorrhea is defined as cramps without underlying disease.
- -Prostaglandins F2 and E2, which are produced by the uterus in higher concentrations during menses, are the primary cause.
Primary dysmenorrhea
It is a condition associated with ovulatory cycles.
It has a biochemical basis& arise from the release of prostaglandins with menses.
It usually appears 6-12 months after menarche when ovulation is established.
The symptoms are definitely related to ovulation & don’t occur when ovulation is suppressed.
Dysmenorrhea typically disappears after a firstpregnancy and does not occur if cycles are anovulatory.
46

Signs & Symptoms
Lower abdominal cramps Backache Weakness Sweats Gastrointestinal symptoms( anorexia,nausea, vomiting,
& diarrhea). CNS symptoms ( dizziness, headache, & poor
concentration)NOTE( Pain begins at the onset of menstruation and lasts
8-48 hours).
47

Management
Important components of midwife care are information and support.
Offering of different alternatives to alleviate dysmenorrhea:
Heat (heating pad or hot bath) Massaging the lower back. Soft, rhythmic rubbing of the abdomen. Progressive relaxation, yoga, & acupuncture
48

Cont..
Exercise Maintaining good nutrition at all times Decrease salt & refined sugar intake 7-10 days
before expected menses may reduce fluid retention.
Decreasing red meat intake Medications (NSAIDs, combined OCPs) Herbal preparations (Ginger, black cohosh)
49

Secondary dysmenorrhea
It is acquired menstrual pain that develops later in life than primary dysmenorrhea, typically after age 25.
It is associated with pelvic pathology such as adenmyosis, endometriosis, pelvic inflammatory disease, endometrial polyps, uterine fibroid, or use of IUD.
50

Signs & Symptoms
Dull pain starts few days before menses, but it can be continue through the first days of menses.
Lower abdominal aching radiating to the back or thighs
Feelings of bloating or pelvic fullness.
51

Management
Treatment directed toward removal of the underlying pathology
Many measures described for primary dysmenorrhea can be helpful for women with secondary dysmenorrhea.
52

Cont.
Some nutritionists suggest that vitamins B and E helprelieve the discomforts associated with menstruation.
Heat is soothing and promotes increased blood flow.Regular exercise can ease menstrual discomfort andhelp prevent cramps and other menstrual complaints
Persistent discomfortshould be medically evaluated.

Premenstrual Syndrome (PMS)
PMS is a complex, poorly understood condition that includes one or more of a large number( more than 100) of physical & psychological symptoms.
It begins in the luteal phase of the menstrual cycle, and followed by a symptoms-free period.
It occurs to a such degree that lifestyle or work is affected.
54

Cont..
Premenstrual dysphoric disorders (PMDD) is amore severe variant of PMS in which women have marked irritability, mood lability, anxiety, fatigue, appetite changes, & sense of feeling overwhelmed
55

Signs & Symptoms of PMS
Physical symptoms 1. abdominal pain, headache, fatigue, & backache.2. Fluid retention ( abdominal bloating, pelvic fullness,
edema of the lower extremities ,breast tenderness,& weight gain)
Behavioral or emotional changes1. Depression, crying spells, irritability, panic attacks, &
impaired ability to concentrate)2. Premenstrual cravings (sweats, salt, & increased
appetite)
56

Research Findings
An observational study of 384 young girls was conducted to describe the severity of emotional, physical and behavioral symptoms.
Result A total of 64 girls (18.2%) met the DSM-IV criteria for severe
PMS or Premenstrual Dysphoric disorder (PMDD). The order of frequency of symptoms occurring in PMS was general body discomfort, anxiety, backache, fatigue and depression. Most frequently reported symptoms in PMDD group were anger, anxiety, stress, depression, fatigue and general body discomfort.
(Tabassum S et al. 2005)
57

Diagnosis of PMS
Diagnosis of PMS and PMDD should be based on clinical history and prospective charting of symptoms by the patient over two or three menstrual cycles.
A diagnosis of PMS is made only if the following criteria are met
Symptoms occur in the luteal phase & resolve within a few days of menses onset.
A symptom-free period occurs in the follicular phase. Symptoms are recurrent
58

Management
A careful, detailed history and daily log of symptoms may give direction to plan of management.
Diet & exercise changes1. Stop smoking & limit consumption of refined (sugar, salt, & red
meat).2. Three small to moderate- sized meals and three small snacks
per day rich in carbohydrates & fiber.3. Use of natural diuretics.4. Nutritional supplements (calcium, magnesium, vitamin B6)
Use of primrose oil to relieve o breast discomfort
59

Yoga, acupuncture, & massage therapy. Herbal therapy. Counseling, in form of support group or
individual counseling. Stress reduction techniques. If symptoms didn't relieve within 1-2 months,
medication is often begun (diuretics, progesterone, NSAIDs, & OCPs.
60

Dysfunctional Uterine Bleeding
Abnormal Uterine Bleeding (AUB) is any form of uterine bleeding that is irregular in amount, timing, or duration & not related to regular menstrual bleeding.
Dysfunctional Uterine Bleeding (DUB) is an excessive uterine bleeding with no demonstrable organic cause, genital, or extra-genital.
61

Possible Causes of AUB
Anovulation (hypothalamic dysfunction & polyscystic ovary syndrome).
Pregnancy related condition (miscarriage, ectopic pregnancy).
Lower reproductive tract infection (pelvic inflammatory disease).
Neoplasms ( CA of cervix & endometrium, leiomyomata) Trauma (genital injury, foreign body) Systemic diseases (DM,renal or liver failure). Iatrogenic causes (use of OCPs, herbal preparation (ginseng)
62

Endometriosis
It is characterized by presence & growth of endometrial tissues outside of the uterus.
The tissue may be implanted on the ovaries, uterine ligaments, sigmoid colon, cervix, or inguinal area.
It is a common gynecologic problem, affecting from 5% to 15% of women of reproductive age.
63


Dysmenorrhea Deep pelvic dyspareunia Chronic monocyclic pelvic pain Pelvic heaviness Pain radiated into the thighs Bowel symptoms ( diarrhea) Less common symptoms include abnormal bleeding Chronic fatigue syndrome
Symptoms
65

Research Findings
Data from over 7000 confirmed cases clearly show that delay in diagnosis (the average time to diagnosis is >9 years) is a major problem and that current treatments are far from satisfactory. In conclusion, the impact of endometriosis, a disease that already produces intense symptoms, is worsened by a current lack of understanding of the disease.
(M . Ballweg M. 2004)
66
