common thyroid problems in women - beacon hospital€¦ · common thyroid problems in women tip and...
TRANSCRIPT
Internal use only by approved personnel. Unpublished Work © 2019 Beacon Hospital. All rights Reserved. In Strict Confidence.
Common Thyroid Problems in Women Tip and Tricks
Dr Carla MoranConsultant Endocrinologist
1. New Thyrotoxicosis – what to do
2. Hypothyroidism – Tips
3. Pregnancy issues
2
Topics
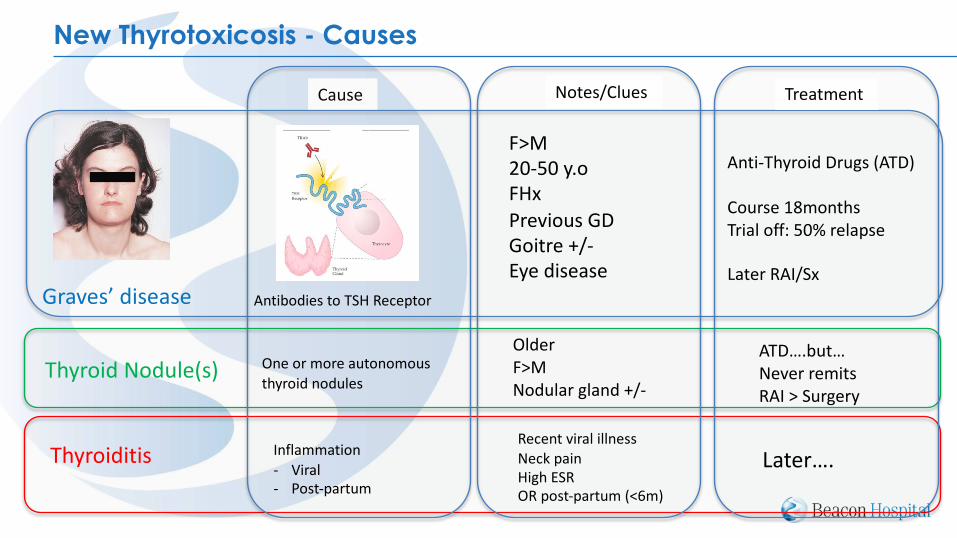
New Thyrotoxicosis - Causes
Graves’ disease
Cause Notes/Clues Treatment
Thyroid Nodule(s)
Thyroiditis
F>M20-50 y.oFHxPrevious GDGoitre +/-Eye disease
Antibodies to TSH Receptor
Anti-Thyroid Drugs (ATD)
Course 18monthsTrial off: 50% relapse
Later RAI/Sx
One or more autonomous thyroid nodules
OlderF>MNodular gland +/-
ATD….but…Never remitsRAI > Surgery
Inflammation - Viral - Post-partum
Recent viral illnessNeck pain High ESROR post-partum (<6m)
Later….

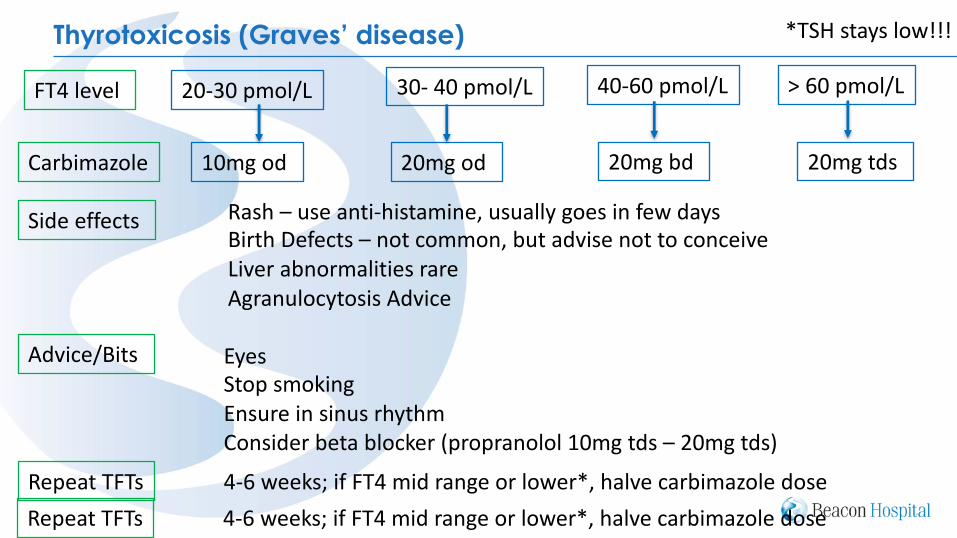
Thyrotoxicosis (Graves’ disease)
20-30 pmol/L 30- 40 pmol/L > 60 pmol/L
Carbimazole
40-60 pmol/L
10mg od
FT4 level
20mg od 20mg bd 20mg tds
Side effects Rash – use anti-histamine, usually goes in few days Birth Defects – not common, but advise not to conceiveLiver abnormalities rare Agranulocytosis –
STOP medication if:• Sore throat• Flu-like illness• Mouth ulcers• FeverHave FBC within 24 hours – if normal WCC, restart
Thyrotoxicosis (Graves’ disease)
20-30 pmol/L 30- 40 pmol/L > 60 pmol/L
Carbimazole
40-60 pmol/L
10mg od
FT4 level
20mg od 20mg bd 20mg tds
Side effects Rash – use anti-histamine, usually goes in few days Birth Defects – not common, but advise not to conceiveLiver abnormalities rare Agranulocytosis Advice
Advice/Bits EyesStop smokingEnsure in sinus rhythmConsider beta blocker (propranolol 10mg tds – 20mg tds)
Repeat TFTs 4-6 weeks; if FT4 mid range or lower*, halve carbimazole dose
Repeat TFTs 4-6 weeks; if FT4 mid range or lower*, halve carbimazole dose
*TSH stays low!!!

TSH remains high on thyroxine 1. Check administration is correct
• First thing in morning• On empty stomach• Do not eat or drink anything other than water for at least 30 mins• Some medications require further time spacing; calcium, iron, sevelamer,
cholestyramine (at least 2 hours) 2. Increase dose by 25mcg daily 3. Repeat TSH in 6-8 weeks 4. Consider anti-TTG (even if no symptoms) 5. If remains high, refer - we sometimes do a thyroxine absorption test
Hypothyroidism
Tips• No need to repeat TPO antibodies if previously positive (EVER!)• No need to reduce thyroxine dose if TSH normal and FT4 high• If misses dose, can take double next day
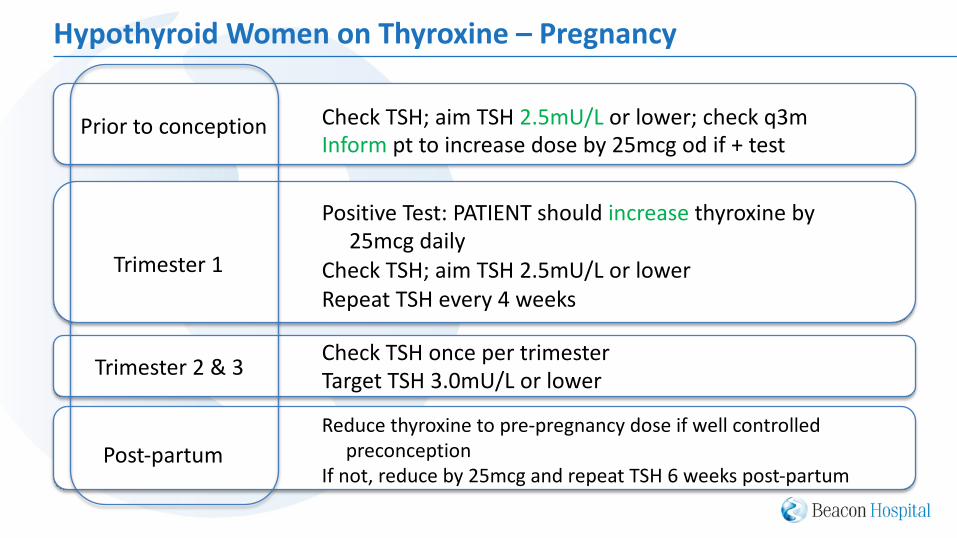
Hypothyroid Women on Thyroxine – Pregnancy
Prior to conception
Trimester 1
Trimester 2 & 3
Post-partum
Check TSH; aim TSH 2.5mU/L or lower; check q3mInform pt to increase dose by 25mcg od if + test
Positive Test: PATIENT should increase thyroxine by 25mcg daily
Check TSH; aim TSH 2.5mU/L or lower
Repeat TSH every 4 weeks
Check TSH once per trimesterTarget TSH 3.0mU/L or lower
Reduce thyroxine to pre-pregnancy dose if well controlled
preconception
If not, reduce by 25mcg and repeat TSH 6 weeks post-partum
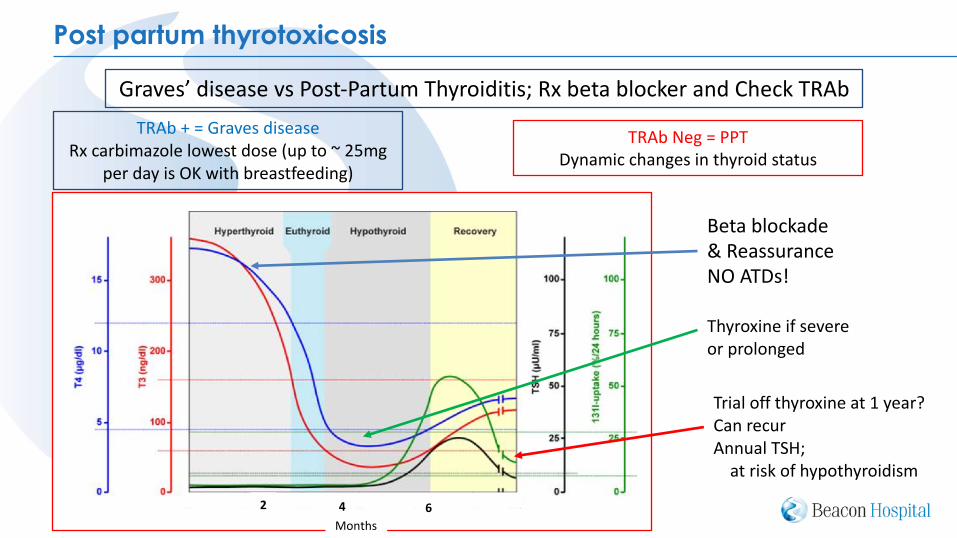
Post partum thyrotoxicosis
Beta blockade& ReassuranceNO ATDs!
Thyroxine if severeor prolonged
Trial off thyroxine at 1 year?Can recurAnnual TSH;
at risk of hypothyroidism
Graves’ disease vs Post-Partum Thyroiditis; Rx beta blocker and Check TRAbTRAb + = Graves disease
Rx carbimazole lowest dose (up to ~ 25mg per day is OK with breastfeeding)
TRAb Neg = PPTDynamic changes in thyroid status
Months62 4
Key points
Thyrotoxicosis:• Most likely to be Graves disease• Patients should be seen within 2 weeks • Don’t be concerned about starting carbimazole; just remember about agranulocytosis &
Repeat thyroid function in 4-6 weeks and adjust meds
Useful website: Hypothyroidism • Administration of thyroxine important • When planning pregnancy, or during pregnancy, aim
for TSH </=2.5mU/L & check q4 weeks in T1
• If checking any antibody; check TRAb
Post-Partum Thyrotoxicosis • TRAb helpful • Likely to be PPT; treat symptomatically • PPT patients at risk of later hypothyroidism

Referral Information Beacon Outpatients Phone (01) 293 8669Fax (01) 293 8654
[email protected]@beaconhospital.ie
10