communicable disease outbreak and contact tracing for ... · measles (rubella) measles is an acute...
TRANSCRIPT
1 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
SH CP 156
Communicable Disease Outbreak and Contact Tracing for Staff Procedure
Version: 2
Summary:
The purpose of this document is to provide an agreed process for the stakeholders involved in the outbreak of any communicable disease affecting employees. In addition this document will provide an agreed process where mass screening or treatment is required for staff exposed to an infection, following advice from either the Infection Prevention and Control Team (IP&CT) or Public Health England (PHE). This involves the Southern Health NHS Foundation Trust, People Asset Management, and potentially, Public Health England.
Keywords (minimum of 5): (To assist policy search engine)
Outbreak, Communicable Disease, Staff Screening, Contact Tracing, Occupational Health
Target Audience:
All staff of all disciplines
Next Review Date: August 2021
Approved and ratified by:
IP&C Group Date of meeting: 12 May 2017
Date issued:
August 2017
Author:
Jacky Hunt – Lead Nurse Infection Prevention and Control
Sponsor:
Sara Courtney – Interim Chief Nurse
2 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
Version Control
Change Record
Date Author Version Page Reason for Change
01.05.14 Andy Nicoll & Theresa Lewis
1 New Procedure
22.02.16 1 Review date extended to May 2016
29.4.16 Theresa Lewis 1 Contact details updated, review date extended to April 2017 to allow for OH re-tendering process in Dec 2016/Jan 2017.
May 2017
Theresa Lewis Jacky Hunt
2 Throughout
Change of OH provider
Oct 2017
Jacky Hunt 2 Appendix 3 added: Process for obtaining treatment for staff following exposure to a communicable disease at work (relates to risk 1371)
Reviewers/contributors
Name Position Version Reviewed & Date
Angela Roberts IP&C Nurse March 2014
Mary Pilgrim IP&C Nurse March 2014
Louise Piper Assistant IP&C Nurse March 2014
IP&C Group Members 07.04.14
Clinical Directors and Professional Leads
07.04.14
Louise Jones Human Resources (HR) Manager 28.04.14
Nick Sargeant Acute Care Pathway Manager - AMH 22.04.14
Louise Jones HR Manager V2 11.5.17
IPC Group Members V2 12.5.17
Ross Taylor Regional Business Manager (PAM) V2 11.5.17
Janet O’Neil Head of Pam Academy V2 11.5.17
Vanessa Lawrence Deputy Chief Pharmacist V2 Sept 2017
Medicines Management Committtee (Appendix 3 only)
Sept 2017
3 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
Contents
Page
1. Purpose 4 2. Process flowchart 4 3. Process 5 3.1 Staff Member: Exposure to a Communicable Disease 5 3.2 Staff Member: Exposure to an Infection for Follow Up 6 3.3 Communication 6 3.4 Screening 6 3.5 Immunisation/Prophylactic Treatment 7 4. Examples of communicable disease outbreaks 7 4.1 Measles, Mumps and Rubella 7 4.2 Mumps 9 4.3 Rubella (German Measles) 9 4.4 Varicella 10 4.5 Tuberculosis 10 5. Other communicable diseases/exposure to a specific infection 12 Appendices A1 Proforma to be completed by manager detailing: Staff Exposure
to Communicable Disease 13
A2 Proforma to be completed by manager detailing: Staff Contact list for Screening and/or Treatment
15
A3 Process for obtaining treatment for staff following exposure to a communicable disease at work
17
A3a Staff template letter for GP’s – EXAMPLE Group A Strep 19
4 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
Communicable Disease Outbreak and Contact Tracing for Staff Procedure 1. Purpose
The purpose of this document is to provide an agreed process for the stakeholders involved in the outbreak of any communicable disease affecting employees. In addition this document will provide an agreed process where mass screening or treatment is required for staff exposed to an infection, following advice from either the Infection Prevention and Control Team (IP&CT) or Public Health England (PHE). This involves the Southern Health NHS Foundation Trust, People Asset Management (PAM) and potentially, Public Health England.
1.1 Scope
This guide is applicable to all PAM staff working on the Southern Health NHS Trust contract and to all SHFT staff
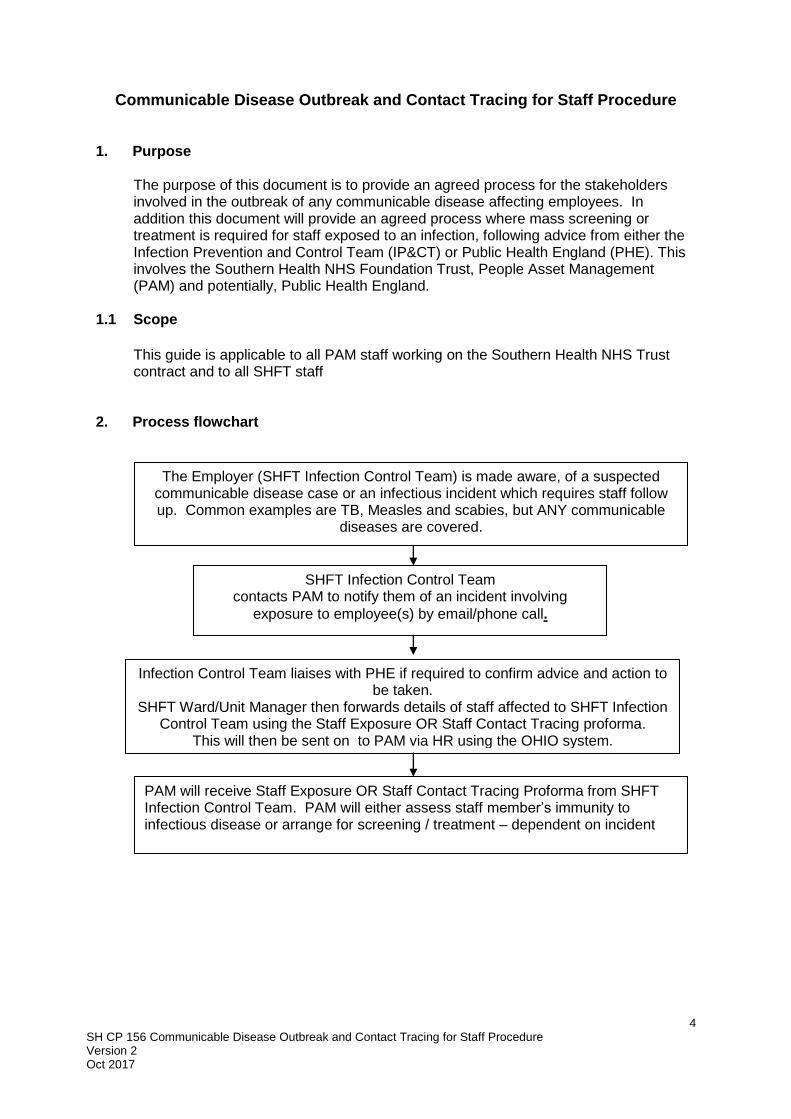
2. Process flowchart
The Employer (SHFT Infection Control Team) is made aware, of a suspected communicable disease case or an infectious incident which requires staff follow up. Common examples are TB, Measles and scabies, but ANY communicable
diseases are covered.
SHFT Infection Control Team contacts PAM to notify them of an incident involving
exposure to employee(s) by email/phone call.
Infection Control Team liaises with PHE if required to confirm advice and action to be taken.
SHFT Ward/Unit Manager then forwards details of staff affected to SHFT Infection Control Team using the Staff Exposure OR Staff Contact Tracing proforma.
This will then be sent on to PAM via HR using the OHIO system.
PAM will receive Staff Exposure OR Staff Contact Tracing Proforma from SHFT Infection Control Team. PAM will either assess staff member’s immunity to infectious disease or arrange for screening / treatment – dependent on incident
5 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
3. Process
When an employee is exposed to any communicable disease or there is an identified requirement for mass screening and/or treatment of SHFT staff, the following process will be adopted:
The Employer (Infection Control or the Manager) will be the first point of contact to advise of a suspected (index case), communicable disease case. Cases to consider include*: 1. Varicella Zoster (Chicken Pox) 2. Tuberculosis 3. Meningitis 4. Scabies 5. Measles 6. Mumps 7. Rubella 8. Food poisoning 9. Group A Streptococcus 10. Whooping cough *Please note this list is not exhaustive and if in doubt staff should contact a member of the IP&C team.
If PAM should become aware of a communicable disease outbreak of which the Infection Control Team has not notified them, they should contact the Infection Control Team to ensure they are aware of the outbreak.
All future communication from PAM regarding an outbreak should be to the Lead Nurse for Infection Prevention and Control Tel: 02380 874291, Fax: 02380 874275, Mob: 07500 975960 or nominated IP&CN in their absence.
3.1 Staff Member: Exposure to a Communicable Disease
Following exposure of staff to a communicable disease such as TB or Chicken Pox, there may be a need to draw up a list of contacts to follow up. Following consultation with PHE, the IP&C team will advise when/if this is necessary. The ward/unit manager is responsible for ensuring an accurate list of staff contacts is drawn up with the requested information to the questions below recorded - See Appendix 1. Confirmation of diagnosis should be sought with every case (exposed staff members) by following the questions as appropriate below:
When was the date of onset of first symptoms (of infected person/index case)?
Last day of contact with index case
Has a diagnosis been made?
How was a diagnosis made and by whom?
Have you been in contact with the index case - include date of contact/exposure?
Have you had this communicable disease in the past? How was it confirmed?
Can you provide an Immunisation history?
6 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
3.2 Staff Member: Exposure to an Infection for Follow Up
There may be occasions when staff have been exposed to a specific infection eg scabies, Group A Streptococcus (as identified by either the IP&CT or PHE) which result in the need for either staff screening / treatment or both. When these situations have been identified, the IP&C team will request that the ward/unit manager completes a Staff Contact Screening form – see Appendix 2.
3.3 Communication
The Southern Health Infection Control Team will liaise directly with Public Health England (if necessary) to seek confirmation of how to manage staff that have been exposed. Any restrictions regarding work will be clarified directly with the Infection Control.
The Southern Health Infection Control Team will liaise with the manager of the team affected to identify any patients or colleagues who are potentially at risk.
If a ‘look back’ exercise is required to identify staff exposed to a communicable disease eg chicken pox or TB, the manager will complete Appendix 1 Staff Exposure to Communicable Disease
If screening and / or treatment is required eg scabies, the manager will complete Appendix 2 Staff Contact Screening form (Appendix 4)
The Ward/Unit Manager is responsible for collecting this information. Once completed the Ward/Unit Manager must send to the IPC team using secure nhs.net email. The Southern Health Infection Control Team will then contact the Regional Business Manager at PAM to advise them of the potentially exposed employees.
The Southern Health Infection Control Team will forward details of the staff contacts (obtained from the Ward/Unit Manager) to HR who will upload them onto OHIO so that they can be processed by PAM.
3.4 Screening
Where screening is required, the IPC team forward on a copy of the Staff Contact Screening form to PAM via secure email.
The IPC team will work with PAM to arrange for staff screening to take place at a convenient time and location
PAM will be responsible for collecting, processing and receiving the results of any screening required
On receipt of results from the laboratory PAM will communicate the screening results to the individual directly and update staff records accordingly
PAM will be responsible for keeping the IPC team updated of results and discussing any work restrictions required
7 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
3.5 Immunisation/Prophylactic Treatment
The SHFT IPC Team will provide PAM with the list of staff who have been exposed to the communicable disease. PAM will check the immunisation records for verification of immunity and update the Staff Exposure form and return the updated form to the IPC team.
If immunisations are required as a result of staff exposure, PAM will schedule the appointments for the staff identified. PAM will be responsible for contacting the individuals either directly or through their line manager to notify them of clinic venue, time slots and any other necessary advice.
Routine immunisation will be offered to all those employees found to be non–immune. PAM will ensure that all staff records updated accordingly
Any staff member wishing to decline vaccination will be required to sign a declaration confirming that they are aware of the risk of not accepting the vaccine. PAM will hold copies of this declaration form which will be forwarded to the generic Human Resources email inbox, for forwarding onto the relevant manager – see Staff Immunisation Policy for further details
PAM will inform IPC team re uptake of treatment / immunisation and any issues / problems that may have arisen
If mass treatment is required eg prophylactic antibiotics, scabicide treatment, PAM will work with the SHFT IPC Team to identify the most suitable method of obtaining supplies to staff with minimum disruption. PAM does not have prescribing capabilities. It is the Trust’s team leader/ward manger’s responsibility to send the staff list proforma to the Southern Health IPC Team, indicating who has received treatment, This will be forwarded to PAM staff can update the staff members records (by H.R. using the OHIO system)
4. Examples of communicable disease outbreaks 4.1 Measles, Mumps and Rubella
The protection of healthcare workers is especially important in the context of their ability to transmit Measles, Rubella or Mumps infections to vulnerable groups. Whilst they may need vaccination for their own benefit, on the grounds outlined above they should be immune to these infections for the protection of their patients. (Immunisation against Infectious Diseases 2006)
Measles (Rubella) Measles is an acute viral illness caused by a morbillivirus of the paramyxovirus family. The incubation period of measles is approximately 10-12 days from exposure to prodome, and 14 days from exposure to rash (range 7-18 days). The prodromal stage is characterised by the onset of fever, malaise, coryza, conjunctivitis and cough. The rash is erythematous and maculopapular, starting at the head and spreading to the trunk and limbs over three to four days. Measles is spread by airborne droplet transmission. Individuals are infectious from the beginning of the prodromal period (when first symptoms appear) to four days after the
8 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
appearance of the rash. It is one of the most highly communicable infectious diseases. Exclusion is advised for five days after the rash starts. Evidence of immunity Satisfactory evidence of protection against Measles infection should be sought on employment for all healthcare workers and laboratory staff (the ‘born before’ 1970 date is not accepted as evidence of immunity or vaccination). Satisfactory evidence of protection would include documentation of:
Having received two doses of MMR, or measles containing vaccine
Positive antibody test for measles.
Staff who are unable to provide the above should be given MMR vaccination. Combined measles-mumps-rubella (MMR) is not contra-indicated in those who may be immune to one or more components of the vaccine. MMR vaccine contains three live attenuated viruses – each vaccine virus will not replicate to a significant level in a host who has pre-existing immunity to that infection as a result of either vaccination or natural disease. MMR may therefore be safely given to people without other contra-indications regardless of prior vaccination status or a history of natural infection. (PHLS (now Public Health England) 2003. Commercial assays that measure IgG to measles and mumps are not recommended for testing prior to vaccination.
Refusal Healthcare workers who refuse to receive immunisation should have access to adequate information. They should be reminded of their legal duty of care to their patients which includes taking reasonable precautions to protect themselves from communicable diseases. If they still decline, the occupational health physician will assess the risk factors and give advice to the healthcare worker on fitness to work. N.B. If it is an outbreak situation, immunity testing (IgG) should be offered and arranged as soon as possible (see below).
Post Exposure advice and prophylaxis following exposure to Measles If there is satisfactory evidence of immunity to Measles the healthcare worker can continue working. The healthcare worker should be reminded of the symptoms and advised to cease working and promptly contact Occupational Health should they develop any of the following symptoms:
Rash for at least three days
Fever for at least one day, and
At least one of the following – cough, coryza or conjunctivitis
If the healthcare worker is not immune or there is no evidence of immunity, they should be excluded from clinical contact with patients after day 4 of the exposure
The healthcare worker can resume working if: they are asymptomatic after 18 (DoH Green book) days post exposure
Healthcare workers who develop symptoms can return to clinical contact 5 days after appearance of the rash
For healthcare workers who have no evidence of immunity to Measles following significant exposure (15 minutes in the same room, or direct face to face contact),
9 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
the MMR vaccination should be offered promptly (ideally within 3 days of the exposure) following discussion with an occupational health physician.
Human Normal Immunoglobulin (HNIG) should be offered promptly ideally within 6 days, if clinically indicated (pregnancy, immunocompromised) and following liaison with the Public Health England or microbiologist. The occupational health physician will prescribe the HNIG if indicated.
IgG screening may be advocated in certain circumstances (normally if there are a number of employees potentially exposed, who will be removed from the work environment if documented evidence of immunity cannot be provided).
4.2 Mumps
Persons with classical Mumps have bilateral or unilateral parotitis. The average incubation period is 16-18 days after exposure. Mumps can present as asymptomatic or mild respiratory symptoms. Most serious complications occur more commonly in adults. Exclusion is advised for five days after the swelling starts.
Evidence of Immunity Satisfactory evidence of protection against Mumps infection should be sought on employment for all healthcare workers and laboratory staff. Satisfactory evidence of protection would include documentation of:
Having received two doses of MMR, or mumps containing vaccine Staff who are unable to provide the above should be managed as follows:
MMR vaccination should be offered.
Post Exposure advice and prophylaxis following exposure to Mumps Mumps is transmitted by droplet transmission. It is considered low risk and healthcare workers who have no evidence of immunity to Mumps following significant exposure would not be removed from the workplace unless symptoms develop.
4.3 Rubella (German Measles)
Rubella is a mild disease caused by togavirus. There may be mild prodromal illness involving low-grade fever, malaise, coryza and mild conjunctivitis. The rash is mainly transitory, erythematous and mostly seen behind the ears on the face and neck. Rubella is spread by droplet transmission. The incubation period is 14 to 21 days. Individuals with Rubella are infectious from one week before symptoms appear to four days after the onset of rash. Exclusion is advised for five days after the rash starts.
Evidence of Immunity Satisfactory evidence of protection against Rubella infection should be sought on employment for all healthcare workers and laboratory staff. Satisfactory evidence of protection would include documentation of:
Having received two doses of MMR, or Rubella containing vaccine
Positive antibody test for Rubella.
Staff who are unable to provide the above should be managed as follows:
MMR vaccination should be given
Refusal Healthcare workers, who refuse MMR vaccine, should have a blood test. If the test result is negative indicating that the individual is not immune to Rubella, MMR should
10 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
be offered again. If they decline again they should have access to adequate information and be reminded of their legal duty to protect themselves and others and also their duty of care towards their patients which includes taking reasonable precautions to protect themselves from communicable diseases. The occupational health physician will assess the risk factors and give advice to the employer and healthcare worker on fitness to work.
Post exposure advice and prophylaxis following exposure to Rubella Antibody response following vaccination with MMR does not develop soon enough to provide effective prophylaxis after exposure. For those healthcare workers who have no immunity to Rubella, MMR vaccination should be given to prevent further infections. Healthcare workers should be advised that if Rubella like illness develops shortly after infection, it is likely to be due to natural infection. Human Normal Immunoglobulin is not normally given as there is no evidence that it is effective. It is not recommended for the protection of women who are pregnant. Pregnant healthcare workers who have been exposed to Rubella and have no immunity should be referred to the occupational health physician for appropriate advice.
4.4 Varicella
In the event of a Varicella outbreak, guidance may be taken from the Public Health England and from the Southern Health IPCT. Where there is uncertainty regarding immunity, blood testing will be carried out as soon as possible. Health care workers who have direct patient contact and have been exposed to chickenpox and do not have evidence of immunity to chickenpox may be required to refrain from work from day 10 to day 20 following exposure. The Southern Health IPCT and Human Resources will advise the Trust about work restrictions.
4.5 Tuberculosis
Introduction Human tuberculosis (TB) is caused by infection with bacteria of the Mycobacterium tuberculosis complex (M. tuberculosis, M. bovis or M. africanum) and may affect almost any part of the body. The most common form is pulmonary TB, which accounts for almost 60% of all cases in the UK. General symptoms may include:
fever
loss of appetite
weight loss
night sweats
lassitude
blood-streaked sputum or, more rarely,
frank haemoptysis.
Untreated, TB in most otherwise healthy adults is a slowly progressive disease that may eventually be fatal. Almost all cases of TB in the UK are acquired through the respiratory route, by breathing in infected respiratory droplets from a person with infectious respiratory TB. Transmission is most likely when the index case has sputum that is smear positive for the bacillus on microscopy, and often after prolonged close contact.
11 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
Sputum smear positive cases stop being infectious after approximately 2 weeks of treatment. Definition of Close Contact NICE do not provide a definition of prolonged contact with regard to occupational risk. In most occupational circumstances, close contact is considered to be 8 hours of cumulative contact with the index case. However, an individual risk assessment for each index case should be made by the Control of Infection team supported by advice from the TB Nurse and Public Health England as required.
Occupational Risk Casual contacts of people with TB, who will include the great majority of workplace contacts, should not normally be assessed following exposure to a sputum smear positive case. As outlined in the Green Book, there is not sufficient age-specific evidence to make recommendations on BCG vaccination for people older than 35. However, healthcare workers are considered to be at an increased risk of contracting TB if they remain unvaccinated. Therefore NICE state that BCG vaccination is recommended for healthcare workers of all ages. All healthcare workers should be reminded of the symptoms of TB annually and provided with one-off reminders after a TB incident on a ward.
BCG Vaccination BCG vaccination can offer some protection against TB but plays a limited role in TB control following a workplace exposure. All healthcare workers and other employees with a higher occupational risk e.g. prison officers should be offered BCG vaccination, irrespective of age in accordance with Immunisation policy.
Process following notification of sputum smear positive case of TB In the event of a staff member of patient testing positive for TB disease, the IPC Team will liaise directly with PHE for management advice When an enquiry is taken about a case of TB, the following information should be obtained: Is the case pulmonary TB? If not then no further action is usually necessary If it is a confirmed sputum smear positive case of pulmonary TB, the details of the infected person should be obtained, including:
Name
Date of birth
Hospital number (if appropriate)
Contact point and named contact (e.g. The ward, the prison, the practice)
Location of patient (i.e. At home, a prison inmate or in hospital)
Protection of staff caring for patients with sputum smear positive TB In most circumstances, healthcare workers caring for people with TB should not use masks, gowns or barrier nursing techniques unless:
multidrug-resistant (MDR) TB is suspected
aerosol generating procedures are being performed, e.g. bronchoscopy.
Each NHS Trust will take advice from their Control of Infection team and/or Public Health England.

12 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
5. Other communicable diseases/exposure to a specific infection
In the event of other communicable disease, such as Meningitis, or exposure to a specific infection, SHFT will liaise with Public Health England to determine the action required and liaise with PAM as necessary.
13 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
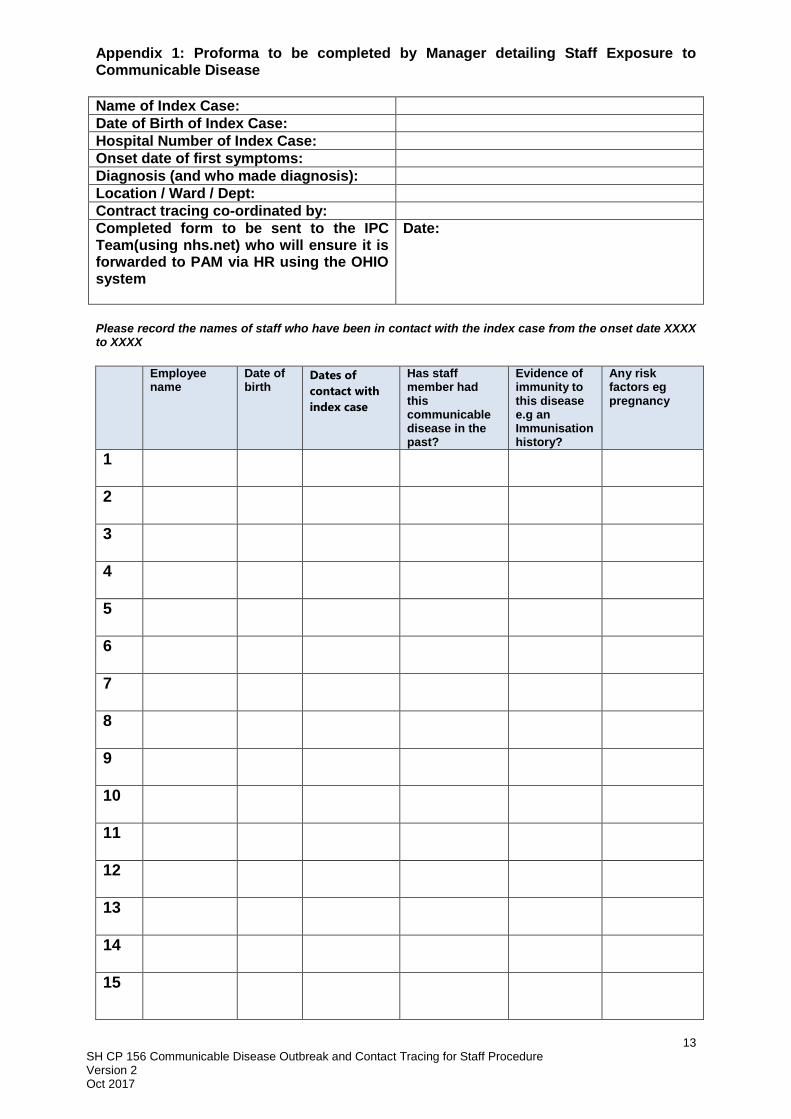
Appendix 1: Proforma to be completed by Manager detailing Staff Exposure to Communicable Disease
Name of Index Case:
Date of Birth of Index Case:
Hospital Number of Index Case:
Onset date of first symptoms:
Diagnosis (and who made diagnosis):
Location / Ward / Dept:
Contract tracing co-ordinated by:
Completed form to be sent to the IPC Team(using nhs.net) who will ensure it is forwarded to PAM via HR using the OHIO system
Date:
Please record the names of staff who have been in contact with the index case from the onset date XXXX to XXXX
Employee
name Date of birth
Dates of
contact with
index case
Has staff member had this communicable disease in the past?
Evidence of immunity to this disease e.g an Immunisation history?
Any risk factors eg pregnancy
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
14 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
16
17
18
19
20
15 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
Appendix 2: Proforma to be completed by Manager detailing Staff Contact list for Screening and/or Treatment Staff contact with Communicable Disease/ Infectious Organism
Name of Index Case:
Date of Birth of Index Case:
Hospital Number of Index Case:
Diagnosis / Infectious organism:
Location / Ward / Dept:
Contract tracing co-ordinated by:
Screening Required: eg throat swab
Any treatment recommended:
Completed form to be sent to the IPC Team (using nhs.net) who will ensure it is forwarded to PAM via HR using the Ohio system
Date:
Employee name Date of
birth Screening Treatment
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
16 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
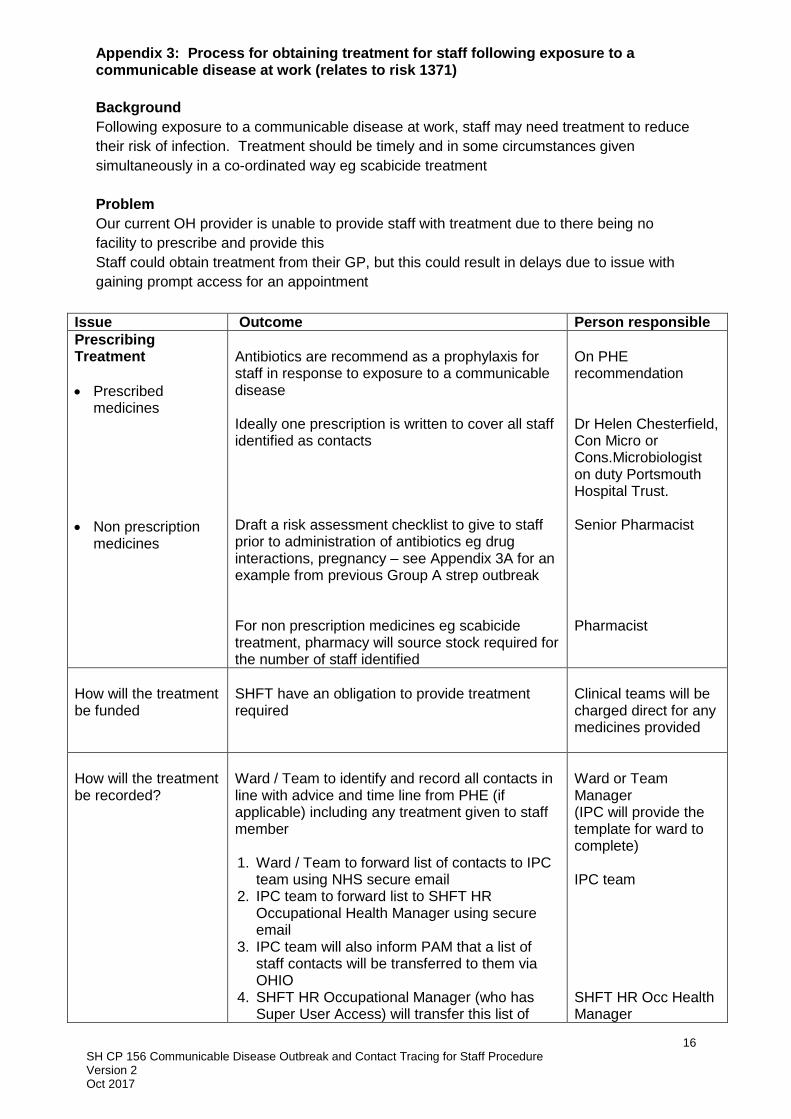
Appendix 3: Process for obtaining treatment for staff following exposure to a communicable disease at work (relates to risk 1371)
Background
Following exposure to a communicable disease at work, staff may need treatment to reduce
their risk of infection. Treatment should be timely and in some circumstances given
simultaneously in a co-ordinated way eg scabicide treatment
Problem
Our current OH provider is unable to provide staff with treatment due to there being no
facility to prescribe and provide this
Staff could obtain treatment from their GP, but this could result in delays due to issue with
gaining prompt access for an appointment
Issue Outcome Person responsible
Prescribing Treatment
Prescribed medicines
Non prescription medicines
Antibiotics are recommend as a prophylaxis for staff in response to exposure to a communicable disease Ideally one prescription is written to cover all staff identified as contacts Draft a risk assessment checklist to give to staff prior to administration of antibiotics eg drug interactions, pregnancy – see Appendix 3A for an example from previous Group A strep outbreak For non prescription medicines eg scabicide treatment, pharmacy will source stock required for the number of staff identified
On PHE recommendation Dr Helen Chesterfield, Con Micro or Cons.Microbiologist on duty Portsmouth Hospital Trust. Senior Pharmacist Pharmacist
How will the treatment be funded
SHFT have an obligation to provide treatment required
Clinical teams will be charged direct for any medicines provided
How will the treatment be recorded?
Ward / Team to identify and record all contacts in line with advice and time line from PHE (if applicable) including any treatment given to staff member 1. Ward / Team to forward list of contacts to IPC
team using NHS secure email 2. IPC team to forward list to SHFT HR
Occupational Health Manager using secure email
3. IPC team will also inform PAM that a list of staff contacts will be transferred to them via OHIO
4. SHFT HR Occupational Manager (who has Super User Access) will transfer this list of
Ward or Team Manager (IPC will provide the template for ward to complete) IPC team SHFT HR Occ Health Manager
17 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
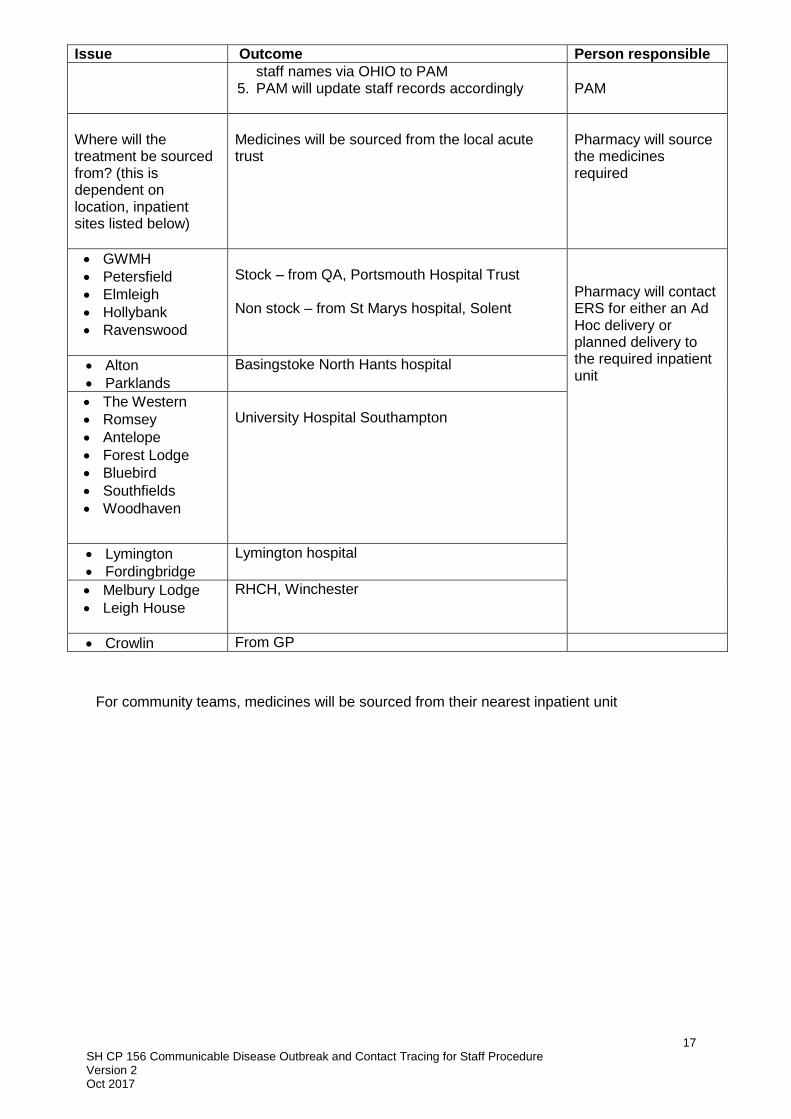
Issue Outcome Person responsible
staff names via OHIO to PAM 5. PAM will update staff records accordingly
PAM
Where will the treatment be sourced from? (this is dependent on location, inpatient sites listed below)
Medicines will be sourced from the local acute trust
Pharmacy will source the medicines required
GWMH
Petersfield
Elmleigh
Hollybank
Ravenswood
Stock – from QA, Portsmouth Hospital Trust Non stock – from St Marys hospital, Solent
Pharmacy will contact ERS for either an Ad Hoc delivery or planned delivery to the required inpatient unit
Alton
Parklands
Basingstoke North Hants hospital
The Western
Romsey
Antelope
Forest Lodge
Bluebird
Southfields
Woodhaven
University Hospital Southampton
Lymington
Fordingbridge
Lymington hospital
Melbury Lodge
Leigh House
RHCH, Winchester
Crowlin From GP
For community teams, medicines will be sourced from their nearest inpatient unit
18 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
Appendix 3a: Staff template letter– EXAMPLE Group A Streptococcus
We are investigating a cluster of Group A Strep infections on XXX ward. As a precaution we are advising that all clinical staff (direct patient contact) obtain an individual throat swab and then commence a course of antibiotic treatment. This will ensure that all staff are protected and will reduce the possibility of further cross infection and/or carriage. Patients will also be given appropriate prophylaxis Plan
All consenting clinical staff to have a throat swab taken. If you have any wounds
please ensure a wound swab is also taken and wound is kept covered.
Clinical swabs will be taken and followed up by PAM – Occupational Health.
Please ensure “XXX Staff screening” is written on the request form
Complete a risk assessment check list to inform of any allergies especially
erythromycin and clarithromycin. If any known allergies please advise to type of
reaction eg rash, breathing difficulties and urticaria and contact on call microbiologist
at Portsmouth Health Trust ( 02392 286000) to discuss. (see below)
If you are currently prescribed a statin please discontinue these for the duration of
the antibiotic course and restart once the antibiotics are completed.
If you may be pregnant please contact XXX or the on call Microbiologist (02392
286000) to discuss treatment options.
Staff Consent Print Name ……………………………… Date …………………………. Signature ………………………………………………………………………….
Consent to throat swab (+ wounds if applicable) Yes / No
Microbiology form completed and swab sent Yes / No
Consent for antibiotic treatment
Yes / No
List known allergies /contra-indications (including erythromycin and clarithromycin) Include any known reaction to previous antibiotics eg rash, urticaria, breathing difficulties or anaphylaxis
Pregnant Yes / No
Antibiotics received and commenced Date:
Staff members should inform their own GP of any treatment they have received.
19 SH CP 156 Communicable Disease Outbreak and Contact Tracing for Staff Procedure Version 2 Oct 2017
For any further information please contact the Infection Control team on 02380 874291 EXAMPLE PRESCRIPTION: This prescription is for all members of staff (detailed below) who have been exposed to
XXXXXXXXXXXXXXXXXX infection
Name of Treatment
Name of Prescribing Doctor
Signature
Date
Staff Name DOB Address Date Issued
Issued by (sig)
Checked by (sig)