community empowerment and technology - core group · india- 100% dots coverage by rntcp since 2006....
TRANSCRIPT

Community empowerment and Technology Building a cost effective, scalable & replicable model
April 2012
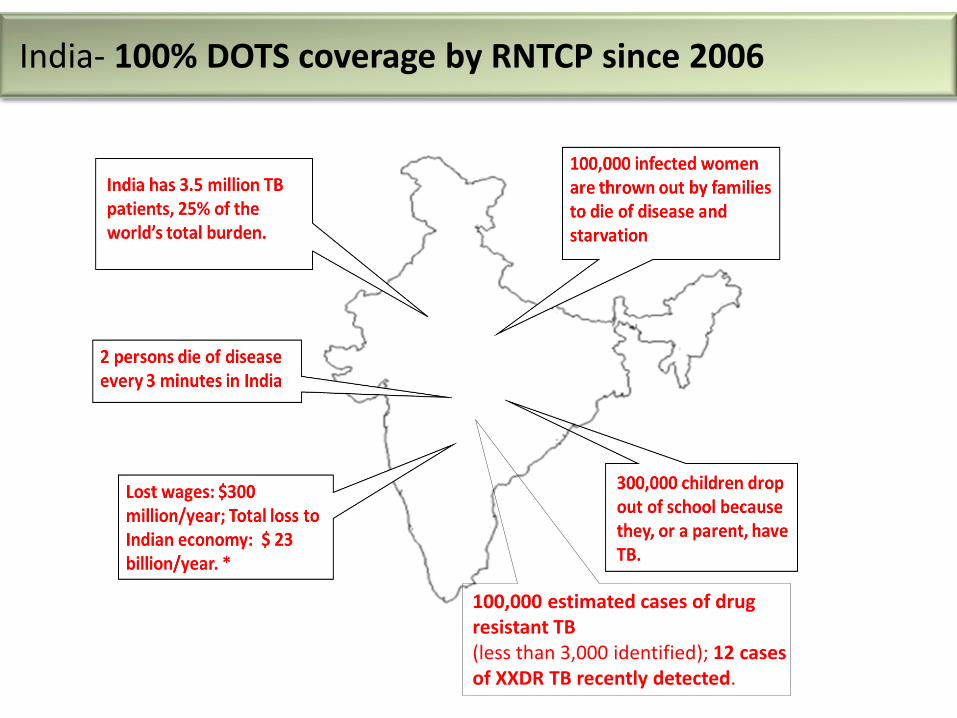
100,000 estimated cases of drug resistant TB (less than 3,000 identified); 12 cases of XXDR TB recently detected.
India- 100% DOTS coverage by RNTCP since 2006

4
India’s TB burden is more than double that of second-ranked China

“If you do not diagnose, you cannot treat”
1. Inaccessible Centers- Existing public infrastructure lacks the last mile connectivity - What to choose- wages or medicine? - who will pay the bus fare? 2. Social Stigma - patients go into denial or hide symptoms - Loss of jobs - Loss of families - Patients thrown out of homes by landlords if they have TB 3. Limited/ Ineffective Education or counseling 4. The Quacks - incomplete, irregular, inadequate treatment 5. Negligible follow-up of defaulting patients 6. High cost of implementation for most other NGOs 7. Program level – lack of electronic data, inaccuracy and human errors, most important - data fudging to show targets have been met
Challenges in TB Treatment: DOTS treatment requires 60 visits to a center over 6 months

MDR-TB
•Is not susceptible to first-line TB drugs
•5-10% of the total TB cases
•mortality rate of 80 percent
XDR-TB
•Develops when patients default on MDR-TB treatment
• 20-25% of the total MDR-TB cases
•Nearly 100% mortality,
XXDR-TB
•Is unresponsive to all known TB medicines
• was recently discovered in Mumbai, India.
•Twelve cases of this strain were identified, three have died
•There is currently no way to cure this disease
•l it can be directly transferred to anyone
1. Inaccessible centers • Open the usual business hours • What to choose? • Medicine or food • Who pays the bus fare?
2. The quacks • First point of contact for the disadvantaged • Late or no diagnosis • Insufficient duration, • Unscientific combinations ( Dharavi study)
5. Poor planning, lack of commitment of government, lack of funds
3. Social Stigma • disruption of family life • Loss of Job • I will lose the patch of land where I have made my
hut ! • Why take medicine when symptoms go away?
4. At DOTS centers- lack of surveillance • No counseling • No default tracking • No incentives for employees to give their best
Factors responsible for Drug Resistance
“DOTS alone is not sufficient to curb the TB epidemic in countries with high rates of MDR-TB.” –Stop TB Working Group
The New Idea….
“Electronic datasets are needed to facilitate accuracy and analysis of data.” - WHO (2011)

“…The data was being fudged.”
– Ghulam Nabi Azad, Union Health Minister (Times of India, Oct 31, 2011)
Independent evaluation by a WHO consultant
found default rate of 36% (6 times higher than
reported). Alarming: Is India an MDR factory?
World bank research- 44% absenteeism in govt school teachers A study on health care delivery found a 43% level of absenteeism.(a)
(a) Chaudhury, Hammer, Kremer, Muralidharan and Rogers, 2003
Sensational News Item in Times of India

* “Directly Observed Therapy - Short Course”
Treatment Centers: Inadequate in
slums
• Local “last mile” centers, distributing
medication and ensuring compliance
• 5 TCs required for every DC;
currently, only 1-4, with limited hours
of operation
• Scarcity of TCs results in high default
rates, causing relapse & drug-
resistance
The DOTS* model: network of three types of facilities
Hospital/ Warehouse
DC
DC
DC
DC
DC
DC
DC
DC
Diagnostic Centers: Adequate
• Sputum tests for initial/rapid diagnosis • 5 DCs required for every hospital ;
typically present
DC
TB Hospitals: Adequate
• Government facilities providing
comprehensive diagnostics and
treatment recommendation
• Warehouse for medicine supplies,
provided free by government &
donors
Hospital/
Warehouse
India’s TB Control program: The DOTS model- lacks Access and Availability

Specialized Training • For active case finding • Conduct health awareness programs • Provide counseling to ensure adherence and prevent MDR • To destigmatize TB
Local Community Members Hired as Counselors & Providers • Work- to treat TB, detect new patients, education camps, default tracking • Advantage - familiarity with local customs, geography, and
informal address systems • MUCH LESS cost than MD doctors! • PERFORMANCE BASED SALARIES to incentivize field workers
Strategically located TB Centers • In convenient, high-traffic areas • Centers open at convenient hours • No patient needs to miss work/wages to access treatment
OpASHA’s Solution: Fill the Gaps: Community
Empowerment & eCompliance

OpASHA’s Innovative approach 1. Internationally accepted standard DOTS therapy prescribed by World Health Organization and followed by India all over the country. 2. Close coordination with Revised National TB Control Program.
– Hospitals & Diagnostic centers – TB medicines – Over-the-counter drugs like pain-killers and antacids to take care of the
side effects – NTP also provides the following
• Consumables and stationery like file covers and stock registers • Disposable plastic cups • Protein supplements • Tea and snacks for participants at awareness campaigns
– A grant two years after the patient is enrolled for treatment.
OpASHA’s Model for the “last mile”
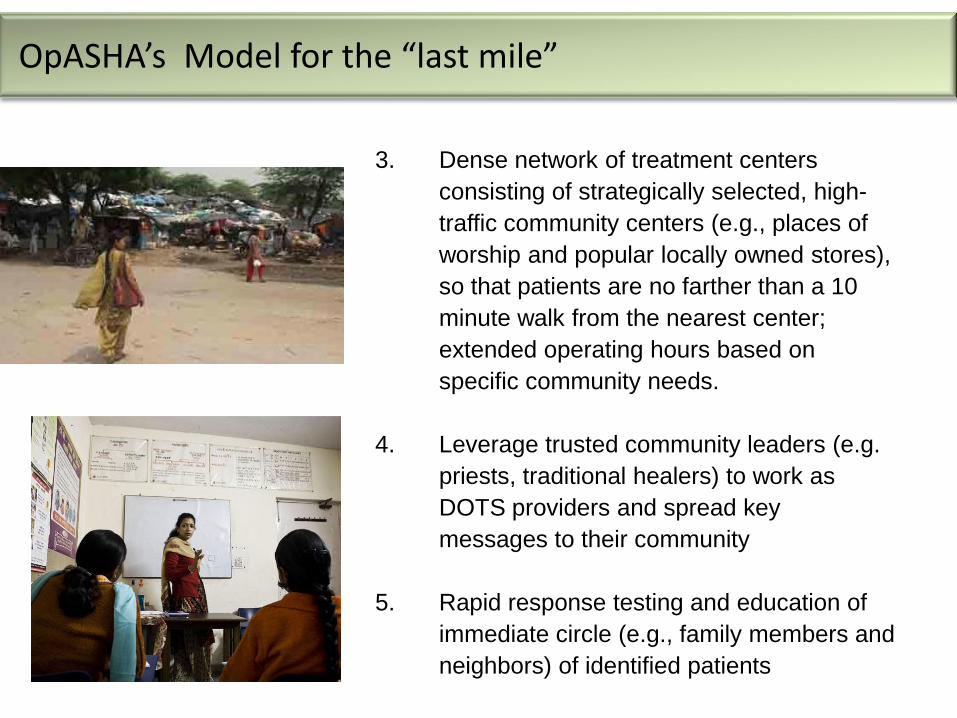
3. Dense network of treatment centers
consisting of strategically selected, high-
traffic community centers (e.g., places of
worship and popular locally owned stores),
so that patients are no farther than a 10
minute walk from the nearest center;
extended operating hours based on
specific community needs.
4. Leverage trusted community leaders (e.g.
priests, traditional healers) to work as
DOTS providers and spread key
messages to their community
5. Rapid response testing and education of
immediate circle (e.g., family members and
neighbors) of identified patients
OpASHA’s Model for the “last mile”
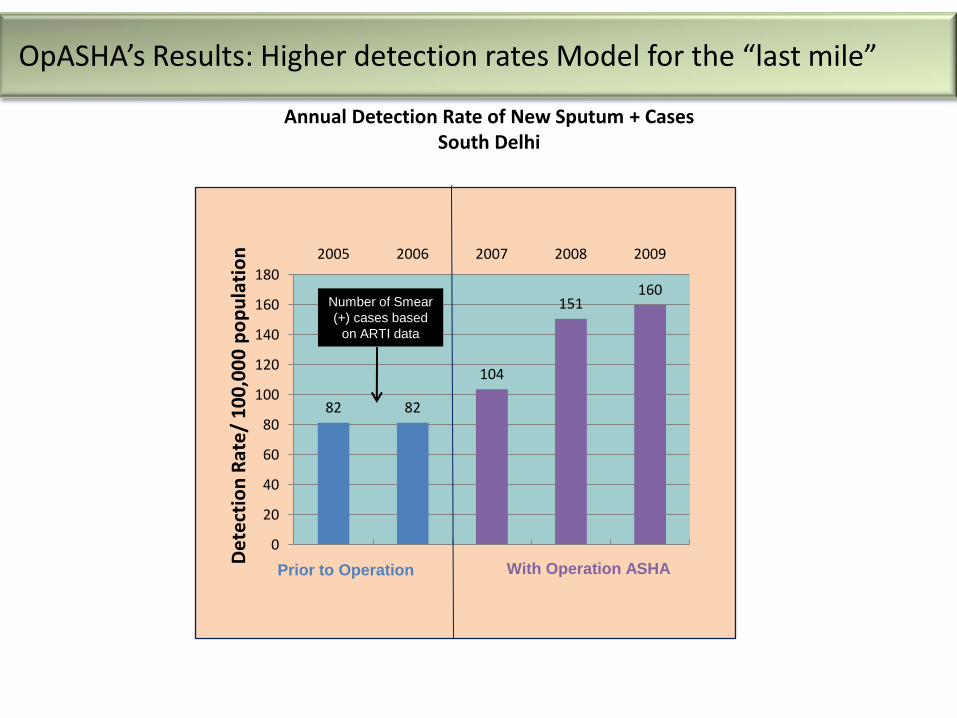
Annual Detection Rate of New Sputum + Cases South Delhi
82 82
104
151 160
0
20
40
60
80
100
120
140
160
180
2005 2006 2007 2008 2009
Prior to Operation With Operation ASHA
De
tect
ion
Rat
e/
10
0,0
00
po
pu
lati
on
Number of Smear
(+) cases based
on ARTI data
OpASHA’s Results: Higher detection rates Model for the “last mile”

6. Corps of highly-trained, well-compensated, full-time counselors (equipped with motorcycles, as required)
7. Provision of Over-the-Counter drugs to treat side effects of TB drugs and provide camouflage.
8. Highly effective Performance-based remuneration. 9. Robust feedback loop involving government officers
Replicable Unit
Center/
Provider
Counsel
or Counsel
or
Counsel
or
Program
Manager
Center/
Provider
Replicable Unit
Counsel
or
Program
Manager
Counsel
or Counsel
or
Program
Manager
Center/
Provider
Center/
Provider
Center/
Provider
Counsel
or
Center/
Provider
Center/
Provider
Counsel
or
Counsel
or
Center/
Provider
Center/
Provider
Counsel
or
Counsel
or
Counsel
or
Center/
Provider
Center/
Provider
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
Counsel
or
Center/
Provider
Center/
Provider
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Center/
Provider
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Center/
Provider
Center/
Provider
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
Center/
Provider
Center/
Provider
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Counseo
r
Center/
Provider
Center/
Provider
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Center/
Provider
Center/
Provider
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Center/
Provider
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Center/
Provider
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Center/
Provider
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
Replicable Unit
Program
Manager
Counsel
or
Counsel
or
eplicable Unit
Counsel
or
Results: OpASHA
(2010)
Other
Organizations
Default Rate 2.75% Up to 60%
OpASHA’s Model for the “last mile”
Replicable Unit
Counselor Counselor Counselor Counselor
Provider
Program Manager
Provider

10. Stringent quality control with internal and external audit.
11. Low-cost, highly leveraged operating model
Cost of full treatment = $30 per patient
Results: Significantly lower cost per patient and higher “SROI”
OpASHA Other NGOs
Cost per patient
Leverage
USD
30
USD 300
4 0.08
SROI: On NGO’s
investment
3,500% 1,000%
SROI: on total investment
by all partners
850% 719%
Assumptions: TB treatment leads to increase in productivity, which in turn raises annual
income by USD $150*; it also saves USD $11,500 in indirect expenses to the economy*;
Discount rate = 8%
* Annual TB Report, Government of India, 2007 & 2011
OpASHA’s Model for the “last mile”

16
PROBLEM
• Unsupervised doses being given
• Missed doses and default
• Data fudged
• Missed doses are not tracked
• Inaccurate record keeping
• Inadequate follow-up
• Time lag between missed dose and follow-up
• Absenteeism among staff
SOLUTION
• Biometrics confirms a TB patient’s presence
• Patients/ staff scan their fingerprint at the treatment center
• This creates indisputable evidence of patient interaction, initial house visit and follow up of each missed dose
• One cannot ‘fudge’ a fingerprint!
PRIMARY OBJECTIVE - To ensure accuracy and adherence
A critical component: eCompliance- “What gets measured, gets done”

Biometric devices for automated compliance tracking deployed at all the South Delhi centers
Result: 1.5% default rate
USB Modem
for SMS
E-compliance- In collaboration with Microsoft Research & IIH

18
Patient Interaction with the Biometric Terminal

19
Electronic Reporting System
Online SMS Server
Health Worker & Program Manager
eDOTS Terminal
Fro
nt
End
B
ack
End
The Front End • Uses only off-the-shelf
components A fingerprint reader A netbook computer USB modem for SMS SMS Plan for 3yrs ($10)
The Back End • SMS Gateway • Central Reporting System • messages are downloaded
from the SMS server and imported into a centralized online database
SMS
How eCompliance Works
eCompliance terminals have been used in South Delhi since 2009
more terminals were installed in Jaipur in 2011
14
Implementation
26
Lessons Learned Our experience indicates that patients are not hesitant to give their fingerprints, and usually do so without difficulty
Patients have perceived the use of technology as a sign of the quality of treatment they are receiving
Results
• Default measured at 1.5% • Over 1,400 patient cured • Over 60,000 visits logged

21
PATIENT AND COMMUNITY LEVEL • Positive impact on the psyche • Improves motivation • Seen as dedication towards quality treatment • Interest generated by technology intervention in disadvantaged areas • Re-enforces belief in the government and DOTS • Indirect benefit- discussion of health issues
AT LEVEL OF FIELD STAFF • Ensures integrity of DOTS: eliminates unsupervised doses, which are
otherwise the norm across the world • Eliminates human errors in management of DOTS. For example, if a patient
comes on the wrong day, eCompliance automatically reminds the counselors and prevents such occurrences
• Improves skills • Makes counseling easy, ie. easier to convince patients • Accurate reporting and up-to-date intelligence
– Eliminates human error • Saves time spent in going thru paper records • Real-time records allows counselors to target counseling, which reduces
workload
The Key Benefits of Biometrics

22
MANAGEMENT LEVEL • Accuracy of records- retrieval for analysis and research
• Digitization of record increases productivity of staff
• Multi-level accountability and transparency
• An accurate platform for monitoring and evaluation of the core program
– Eliminates absenteeism, late coming of counselors
– Prevents tampering with patient data
– Synchronization of data at all levels of management
• Transparent treatment supervision
• Ensures accurate performance based incentives
THE PUBLIC HEALTH PERSPECTIVE • ENSURES DOTS is being delivered
• Halts the development of drug resistance due to default.
• Provides unlimited quality data for future research
The Key Benefits of eCompliance
STAFF Fear of micro-monitoring
Fear of losing jobs to computers
Initial increase in work load (hybrid system)
Fear of theft, breakages
PATIENTS Fear of electric shock!
TECH TEAM Recognition accuracy
Computational ability
- Maintenance
- Software hardware failure, viruses etc
- Need based ongoing system analysis
- Security measures needed to prevent tampering
- Reconciliation of data
Challenges and the solutions

Develop Software Further For
Daily dose regimen
Adherence for MDR-TB,
ART
Integration with MCH, midday meals etc
NCD, especially integration with DM
Zero literacy areas (use icons and audio tracks)
Migrate to inexpensive smart phones
LINKING eCompliance WITH ERP Developing Q&A/ FAQs for contact tracing
Showing educational videos on net-book/ Smart phone
Sending SMS reminders and medical information
AT NATIONAL LEVEL
Developing help lines for patients
Technology & Upgrades - Next steps

• Operation ASHA- started work in September2006
• Treated 18,000 patients so far, ( 5500 this year)
• Almost 2,070 patients were children( how many missed?)
• Challenges - Plenty!
• Diagnostic difficulties • Traditionally ignored because not infective • No gold standard • Late diagnosis-high morbidity and
mortality • Stigma, lack of schooling • Neglected by public health experts and
Policy makers alike!
TB in children =under-detected and under-reported
MDR- / XDR-TB rates in children reflect community transmission rates
Our experience with pediatric TB
Medicines- nobody thought of children? Crushing and breaking tablets- irregular treatment, bitter taste

Operation ASHA’s Exponential Growth (number of DOTs centers)

Replication of our model in 14 cities, 7 states of India, diverse regions, ethnicity, geography, demographics, social structure
REPLICATION IN CAMBODIA
Serving 6% of the population and 8% of the patients
Working in 4 ODs, in 2 provinces
34 staff, all local people except for one Technical advisor from India
Detection rate increased by 71% in Q4- 2011 in Phnom Penh
VIETNAM
Replication of the PPM & DOTS expansion
We have the seed funding, political commitment
Charismatic leadership- prospective country manager (KPMG background) 15 months in India in full time position
UGANDA
First step towards third party replication
eCompliance initiative to be replicated by a leading nonprofit, which works in 8many countries in Africa
OpASHA will be the resource centre, provide training and tech support, free software,
OTHER COUNTRIES
Ground work in progress in Ghana, Kenya and Morocco
Beyond India’s Borders: South-South Cooperation

Next Steps: To Develop Clarity and build partnerships
Establish best practices across the world by policy making – To become a resource centre – Training Nonprofits in high burden countries – Support educational activities, (text free videos, translation of training manual
etc)
Collaborate with World Bank, Government and other stake holders – Lobby with developing country govts for increased funding for PPM programs
(Stop TB grants $425 per DETECTION ALONE) – Persuade govts across the world to link grants to outcome metrics, not just
processes – Ensure that govt procedures are simplified and streamlined – Ensure that agreements with govt for TB control should include establishing
best practices

• Decentralize and de-stigmatize TB • eCompliance will remain open source • It will continue to use commercially available
hardware. • Can be quickly and freely adopted by other TB
institutions • OpASHA plans to develop capacity to help govts and
NGOs replicate its model • Grave concerns- MDR prevention and Pediatric TB • Advocacy – to express urgency, establish best
practices, and use eCompliance for best results in TB
Community empowerment &Technology together gives best results.
Conclusion