community outreach: university of michigan brings … conference handout… · ·...
TRANSCRIPT

6/13/2011
1
Community Outreach:
University of Michigan Brings
New Partners Together
2011 Michigan Oral Health ConferenceJune 9, 2011 � 1:30 to 2:30 p.m.
THE ENERGY OF SYNERGISM
Primary Prosthodontic Care Pilot
OUTREACH CLINIC
Howard A. Hamerink DDS
Clinical Adjunct Associate Professor
University of Michigan School of Dentistry

6/13/2011
2
INERTIAINERTIA
WHOWHO WHATWHAT WHYWHY

6/13/2011
3
BUY-LINES
BY-LINES
DATA?DATA?
WHO?WHO?
WHERE?WHERE?
HOW?HOW?
BY-LINES

6/13/2011
4
Perhaps because there is no obvious
penalty for being wrong(or for not being as right as one might like),
decision-making in the face of
uncertainty (i.e., in the absence of data)
is a time-honored prosthodontic
tradition.
• PARTNER 4
• PARTNER 3
• PARTNER 2
• PARTNER 1
REFERING CLINIC
REFERING CLINIC
OUTREACH CLINIC
OUTREACH CLINIC
DONATION SOURCE
DONATION SOURCESCHOOL OF
DENTISTRY SCHOOL OF DENTISTRY
THE MODEL
6/13/2011
5
THE ENERGY OF SYNERGISM
– An Access to Care Educational
Opportunity Pilot
Linking the Public Health,
Educational and Private Sectors
BUY-LINES CDC PROSTHODONTIC
PILOT
CHECKLIST TEST CASE PHOTOS
RESEARCH
CHECKLIST TEST CASE PHOTOS
RESEARCH
FACULTYFACULTY
OFFSITE CLINIC
OFFSITE CLINIC
ACCEPTED EVALUATION
METHODS
ACCEPTED EVALUATION
METHODS
6/13/2011
6
BUY-IN
CEU
CLASSIFICATIONCLASSIFICATION
IMAGESIMAGESTEST CASETEST CASE
DATA
• Aim 1 Patients:
Patient recruitment by partnering with a community based non-profit organization with no
ability to provide prosthodontic service.
• Aim 2 Educational experience (An adult learning model):
Volunteer dental students were presented a defined logical protocol to accomplish patient care
over a series of four patient visits.
• Aim 3 Access to Care:
The community organization was able to identify, communicate with and provide
transportation for the referred patients.
• Aim 4 Financial Sustainability:
The Pilot recruited partners from four arenas the corporate sector to supply materials and
supplies, the dental school provided the faculty PI support and allowed volunteer dental
students the outreach experience at the pilot. A United Way grant to provided for laboratory
costs, transportation and the Community Dental Clinic provided clinic space, staff and supplies.
6/13/2011
7
• DENTSPLY• WARD LAB
• WHIPMIX CORP• IVOCAR/VIADENT
HOPE CLINICHOPE CLINIC
CDCCDC
UNITED WAY
UNITED WAY
U of M
SOD
U of M
SOD
THE CARE MODEL
PPC
MISSION STATEMENT
PREPARED
ACCURATE
REPRODUCABLE

6/13/2011
8
• 34 PATIENTS SEEN
• 30 PATIENTS TREATED
START
3/15/2010
START
3/15/2010
• 56 APPLIANCES
• 4.7 VISITS/PATIENT04/07/201104/07/2011
CD base $
RPD frame $
SET UP & TEETH
$
PROCESS
$
CD $230
RPD $287
Laboratory Costs

6/13/2011
9
PATIENT SURVEY FREQUENCY:Baseline1st visit Post delivery one weekOne month post delivery
IMAGING:Screening, impression, jaw relation, try-in and delivery visitsStudent check list for each visit evaluation
Documentation:Appointment Check List, Mi-Dent and Patient Treatment Record
STUDY DATA PROTOCAL
RESULTS TO DATE
BASELINE
• Average age: 50.6 years old
• 34 Responses
• Previous Appliances : Yes 15 No 19
• Previous Appliance Effectiveness Score 4.0
out of 5
• Expected Effectiveness 4.5 out of 5

6/13/2011
10
Survey Results: Four Weeks Post Delivery
• Appliance Effectiveness Scores: out of 5
Overall 4.25Speaking 3.92Chewing 3.91Biting 4.0Looks 3.9
• Student Evaluation Scores:
Trust 4.55Knowledge 4.55Information 4.5Recommend 4.65
Comparison of Scores
BASELINE
Previous Appliance Effectiveness Score 4.0
Expected Appliance Effectiveness Score 4.5
FOUR WEEK FOLLOWUP
Overall Effectiveness Score New Prosthesis 4.25
Student overall Score 4.56

6/13/2011
11
University of Michigan School of Dentistry
Community and Outreach Program
Dental / Dental Hygiene Students
Wilhelm A. Piskorowski, DDS
Director for Community and Outreach Affairs
Outreach=Tradition
Photo courtesy of Dr. Jack Bates, Class of 1941
A Structured Way of Giving back to those less fortunate

6/13/2011
12
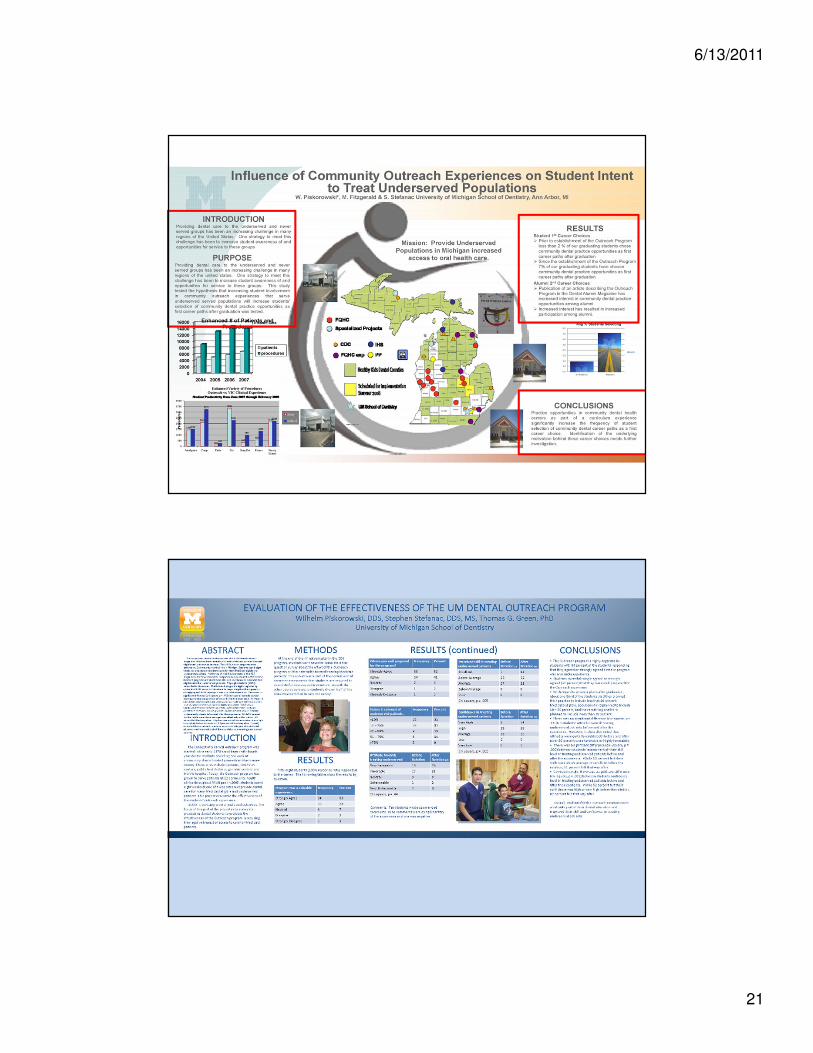
Mission:
Provide Underserved Populations in Michigan
increased access to oral health care.
Purpose:
Through community-based rotations our students will:
� Provide patient centered care that is both comprehensive and compassionate for a culturally diverse population
� Enhance their awareness to the disproportionate oral health concerns that are present in Michigan and elsewhere
� Develop a sense of civic responsibility which will enhance their future practices to include the underserved

6/13/2011
13
Education for Citizenship Objectives
� Develope an ethic of caring for fellow
citizens
� Experience other ethnic groups &
cultures
� Reflect upon personal values and
ethics
A Diversified Portfolio
of Outreach Experiences
Outreach
Revenue
Sharing
Volunteerism
Local/State/Federally Supported• FQHC
• MCDC
• IHS
• Migrant programs
• School based
• Dental Hygiene programs
Private Sector• Generalist
• Specialists
• Hospitals
International• Alumni Sponsored
• Group/Organization
Sponsored
• School Partnership
Sponsored
Special Programs• Acute managed care
• Special needs
patients
• Veterans
• Homeless
Internal Rotations• Restorative dentistry
• Public health
• Oral surgery
• Periodontics
• Prosthodontics
• Orthodontics
• Research
• Hospital dentistry
Grant Supported
Pilot Programs
Affiliation Agreement�Same for all sites
�Describes:• Term
• Financial commitments
• Definition of responsibilities
• Service to communities

6/13/2011
14
Establishing your outreach program
• Do all partners have a mission to increase access to care?
• What community settings are available in your state for
developing a community-based dental education
program?
• What barriers do you expect to encounter in
implementing your plan?
• What resources are available to create and predictably
sustain the program long-term?
Valuable Partnerships
• 2 Dental schools /182 -first year students
• 9 Dental Assisting Schools-199 dental assts./year
• 13 Dental Hygiene Programs-346 dental hygiene students/year
• 26 Dental Component Societies
• PA161
• Volunteer Dental Service Programs
• 6459 dentists/8455 hygienists
6/13/2011
15
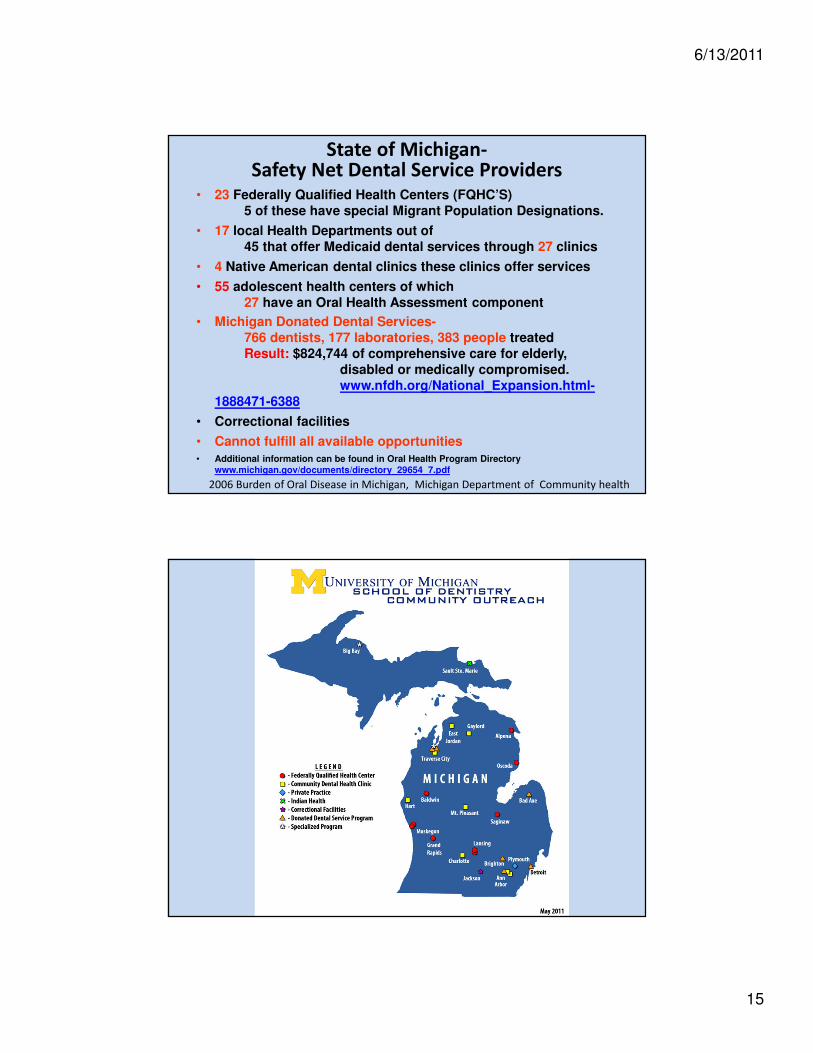
State of Michigan-Safety Net Dental Service Providers
• 23 Federally Qualified Health Centers (FQHC’S) 5 of these have special Migrant Population Designations.
• 17 local Health Departments out of45 that offer Medicaid dental services through 27 clinics
• 4 Native American dental clinics these clinics offer services
• 55 adolescent health centers of which 27 have an Oral Health Assessment component
• Michigan Donated Dental Services-766 dentists, 177 laboratories, 383 people treatedResult: $824,744 of comprehensive care for elderly,
disabled or medically compromised. www.nfdh.org/National_Expansion.html-
1888471-6388
• Correctional facilities
• Cannot fulfill all available opportunities • Additional information can be found in Oral Health Program Directory
www.michigan.gov/documents/directory_29654_7.pdf
2006 Burden of Oral Disease in Michigan, Michigan Department of Community health

6/13/2011
16
Outreach
PA161 Collaborative Practice
NW Michigan
Health Services, Inc.
Munson Healthcare
System
Donated Dental Services
Resort District Dental Society
Donated Dental Services
Other Charities
YOUR COMMUNITY
and
“SPECIALIZED PROJECT”COMMUNITY OUTREACH -- PRIVATE PRACTICE MODEL
FEBRUARY 4-5, 2011
Pilot Program Results / Lessons Learned
The

6/13/2011
17
Production from 14 hour pilot project:
26 restorations71 extractions1 core2 Impressions and records mounted
Many consultations, adjunctive radiographs
Production from Second 3 day
project:
37 Patients Treated14 Restorations129 Extractions5 Crown Preps
Delta Dental PPO Value of services rendered=$21,553.00

6/13/2011
18
Bad Axe Donated Service Project
Total production $15,611.00 for the 4 days equaling $3,902.75 production per day
Results: Win-Win Outcomes
• Relationships are Primary
• Win for the underserved communities who experienced increased access to care
• Win for the centers -increased and more consistent productivity
• Win for the students who increased their clinical skills and broadened their experience base
• Win for sites for they have noted a significant increase in recruitment of recent graduates as practitioners thus helping to solve a chronic manpower problem
•

6/13/2011
19
Patients & ProceduresUniversity of Michigan School of Dentistry
Community Outreach Program
Time Patients Seen Procedures Performed
5/2004-4/2005 7,332 21,5305/2005-4/2006 7,890 16,4885/2006-4/2007 5,790 12,0025/2007-4/2008 8,765 18,2475/2008-4/2009 13,806 25,4935/2009-4/2010 15,069 28,0095/2010-4/2011 15,758 31,662
TOTALS 74,410 153,431
In the past seven academic years, our students have treated more than 74,400 patients and have performed more than 153,400 procedures.
0
1000
2000
3000
4000
5000
6000EXT
ENDO
Surgical
EXT
Student Productivity2006-2010
Acad. Year Weeks at Sites
2006-2007 3 weeks
2007-2008 4 weeks
2008-2009 5 weeks
2009-2010 8 weeks
Exams
Emergency
Exams
Amalgams
Resins

6/13/2011
20
Staying NimbleThe community outreach endeavors are not static.
We always try to remember two important points.
First, since oral health care is a dynamic profession, nothing remains “as is” for very long. • We have to be nimble.
• Do our best to adapt to the needs of our outreach partners who, in turn, are doing their best to respond to the needs of patients in their communities.
• Our flexibility, conveys an important message to our students: they too will have to be adaptable as practitioners.
• Our partners reciprocate. When asked to accommodate one or two additional students from our School for a rotation, without hesitation they do.
Staying Nimble
Second, the reason the number of School-approved outreach sites changes is that we are always active looking for “the best” model.
– It’s interesting to see the approaches taken by our partners in communities across the state, and even at different clinics within the same community.
– The one size does not fit all approach helps our students become even more familiar with dentistry.
6/13/2011
21

6/13/2011
22
It is one of the most beautiful compensations of life that no person can
sincerely try to help another without helping themselves.
Ralf Waldo Emerson

6/13/2011
23
Thank You
Dental Access Program
Rene Louchart, B.S., R.D.H.Dental Health Director

6/13/2011
24
THE ENERGY OF SYNERGISM
– An Access to Care Educational
Opportunity Pilot
Linking the Public Health,
Educational and Private Sectors
Traverse Health Clinic = access to health care since 1975
Coalition Health Access Program (CHAP) = the income
qualifying program that gives patients a CHAP card to access
services
Dental Access Program (DAP) = from 2006 to 2010, urgent
dental needs were referred and oral health instruction was
given

6/13/2011
25
Local Population Living Below Poverty in 2010
“Path to Prevention” was born!By implementing Public Act 161, we were able to expand our DAP.
Typical Oral Condition

6/13/2011
26
Traverse Health Clinic Implements
Collaborative Practice Program• Public Act 161 was passed in 2005 to help solve the access to
oral health care dilemma. It allows Registered Dental Hygienists to provide preventive services to underserved populations without a dentist on site. It offers employment to Michigan’s 10,000 RDHs. It can ultimately decrease costs to taxpayers by increasing oral health and keeping citizens out of ER rooms.
• Before implemented: ER emergency/urgent care referrals to volunteer DDS or back to ER = patient receives limited problem focused treatment
• After implemented: oral evaluation by RDH includes x-rays, hard and soft tissue charting = patient receives preventive services (sc/rp, px, FL2 varnish, OHI, nutrition counseling, tobacco cessation counseling), dental referral for treatment and medical referral for evaluation (diabetes risk assessment, BP, etc.) The patient is now able to achieve more comprehensive, consistent care.
OPEN FOR BUSINESS!!! OPEN FOR BUSINESS!!! OPEN FOR BUSINESS!!! OPEN FOR BUSINESS!!!
1st pt on 1/11/11 at 1:00

6/13/2011
27
“Path to Prevention” Traverse Health Clinic Dental Access Program 2010
Enrolled in CHAP
DAP Intake Program
DAP Prevention Program
DAP Referral Program
Increasing Oral Health
DAP Referral Program
Patients are referred for restorative, surgical, and advanced
periodontal services using the DAP MAP, then return for preventive
re-care.
More than 36 community dentists volunteer their services for our
patients.
Dentists agree to see a certain number of patients for a certain
number of procedures
Our community dentists provided $200,00 worth of services in 2010
These services included extractions, root canals, SC/RP, dentures,
crowns, etc.
Traverse Health Clinic Dental Access Program sees 50 – 70 new
patients each month that need dental care, most with urgent needs
and our volunteer DDS’s have a limit.

6/13/2011
28
referral program cont’d…
• Through efforts with University of Michigan School of
Dentistry, our patients are now able to be seen by
dental students three days a month.
• Our staff hygienists and local dentists have become
U of M Preceptors to oversee the students as they
provide valuable services to our patients, increasing
oral health together!
DAP MAP

6/13/2011
29
Traverse Health Clinic
Dental Access
Program
Government Grants
Donations
Volunteer Dental
Services
Traverse Health Clinic
Dental Access Program
Patients
4 hours volunteered for every $100 worth of services received
(C2 Program)
Volunteer Services at local non-profits
Commitment to Care Program
2010 = over 1,000 hours

6/13/2011
30
What does the future hold?
U of M Dental Hygiene Students ?
University of Detroit ?
Expanding to children ?
Expanding to include other populations ?
Follow us at www.traversehealthclinic.org
BUY-LINES TRAVERSE HEALTH CLINIC
PRETREATMENT ASSESSMENT
PRETREATMENT ASSESSMENT
FACULTY/PRECEPTORSFACULTY/PRECEPTORS
FULL SERVICE CLINIC FULL SERVICE CLINIC
ACCEPTED EVALUATION METHODS , REFERAL
AND FOLLOW - UP
ACCEPTED EVALUATION METHODS , REFERAL
AND FOLLOW - UP

6/13/2011
31
• DENTAL LABORATORIES
• SPECIALITY REFERAL BASE
• DONATED DDS SERVICES
• PRIVATE CLINIC SITE
REFERING CLINICS
REFERING CLINICS
TRAVERSE HEALTH CLINIC
TRAVERSE HEALTH CLINIC
DONATION SOURCE
DONATION SOURCESCHOOL OF
DENTISTRY SCHOOL OF DENTISTRY
TRAVERSE HEALTH CLINIC
Perhaps because there is an obvious
penalty for being wrong(or for not being as right as one might like),
decision-making in the face of
uncertainty (i.e., in the absence of data)
Should not be a time-honored
prosthodontic tradition.

6/13/2011
32
Thank You
DAP Intake ProgramAt Garfield Dental Group location, services include: � D0180 Comprehensive Periodontal Evaluation (New or Established Patient)
This procedure is indicated for patients showing signs or symptoms of periodontal disease and for patients with
risk factors such as smoking or diabetes. It includes evaluation of periodontal conditions, probing and charting, evaluation and recording of the patient’s dental and medical history and general health assessment. It may include the evaluation and recording of dental caries, missing or unerupted teeth, restorations, occlusalrelationships and oral cancer evaluation.
� D0140 Limited Oral Evaluation – Problem Focused
An evaluation limited to a specific oral health problem or complaint. This may require interpretation of
information acquired through additional diagnostic procedures. Report additional diagnostic procedures separately. Definitive procedures may be required on the same date as the evaluation. Typically, patients receiving this type of evaluation present with a specific problem and/or dental emergencies, trauma, acute infections, etc.
� D0210 Intraoral – Complete Series
� D0220 Intraoral – Periapical (initial)
� D0230 Intraoral – Periapical (each additional)
� D0272 Bitewing – Two Films
� D0274 Bitewing – Four Films
� D0330 Panoramic Film
� D0350 Oral/Facial Photographic Images (with intraoral or extraoral cameras)

6/13/2011
33
DAP Prevention Program� D1110 Prophylaxis – Adult Removal of plaque, calculus and stains from the tooth structures in the permanent
and transitional dentition. It is intended to control local irritational factors. It may also be used for removal of plaque,
calculus and stains from partial or complete prosthetic appliances in partially or completely edentulous patients.
� D4910 Periodontal Maintenance This procedure is instituted following periodontal therapy and continues at
varying intervals, determined by the clinical evaluation of the dentist, for the life of the dentition or any implant
replacements. It includes removal of the bacterial plaque and calculus from supragingival and subgingival regions, site
specific scaling and root planing where indicated, and polishing the teeth. If new or recurring periodontal disease
appears, additional diagnostic and treatment procedures must be considered.
� D1206 Topical Fluoride Varnish Therapeutic application for moderate to high caries risk patients. Application
of topical fluoride varnish, delivered in a single visit and involving the entire oral cavity. Not to be used for
desensitization.
� D1310 Nutritional Counseling for Control of Dental Disease Counseling on food selection and dietary
habits as a part of treatment and control of periodontal disease and caries.
� D1320 Tobacco Counseling for the Control and Prevention of Oral Disease Tobacco prevention and
cessation services reduce patient risks of developing tobacco-related oral diseases and conditions and improves
prognosis for certain dental therapies.
� D1330 Oral Hygiene Instructions This may include instructions for home care. Examples include tooth
brushing technique, flossing, and use of special oral hygiene aids.
� D4341 Periodontal Scaling and Root Planing (four or more teeth per quadrant) This procedure involves instrumentation of the crown and root surfaces of the teeth to remove plaque and calculus from these surfaces. It is indicated for patients with periodontal disease and is therapeutic, not prophylactic, in nature. Root planing is the definitive procedure designed for the removal of cementum and dentin that is rough, and/or permeated by calculus or contaminated with toxins or microorganisms. Some soft tissue removal occurs. This procedure may be used as a definitive treatment in some stages of periodontal disease and/or as a part of pre-surgical procedures in others.
� D4342 Periodontal Scaling and Root Planing (one to three teeth per quadrant) This procedure involves instrumentation of the crown and root surfaces of the teeth to remove plaque and calculus from these surfaces. It is indicated for patients with periodontal disease and is therapeutic, not prophylactic, in nature. Root planing is the definitive procedure designed for the removal of cementum and dentin that is rough, and/or permeated by calculus or contaminated with toxins or microorganisms. Some soft tissue removal occurs. This procedure may be used as a definitive treatment in some stages of periodontal disease and/or as a part of pre-surgical procedures in others.
� D4910 Periodontal Maintenance This procedure is instituted following periodontal therapy and continues at varying intervals, determined by the clinical evaluation of the dentist, for the life of the dentition or any implant replacements. It includes removal of the bacterial plaque and calculus from supragingival and subgingival regions, site specific scaling and root planing where indicated, and polishing the teeth. If new or recurring periodontal disease appears, additional diagnostic and treatment procedures must be considered.
� D4999 Unspecified Periodontal Procedure, by Report Can be used for many things, including irrigation of chlorhexidine following scaling and root planing.
� D9910 Application of Desensitizing Medicament Includes in-office treatment for root sensitivity. Typically reported on a “per visit” basis for application of topical fluoride. This code is not to be used forbases, liners or adhesives used under restorations.

6/13/2011
34
Patient Referral Patients have been referred from Traverse Health Clinic using the DAP MAP form.
The top of this form has been filled out by the referring hygienist. It will include important patient information as well as draw your attention to some clinical findings for treatment.
More information can be found on the Baseline Report and Hygiene Sheet pages.
If you have any questions regarding a patient’s health history let us know. We can access more information for you or get a medical sign off as needed.
Preceptor OversightOne preceptor will be assigned to a maximum of two students.
The preceptor will be available to his or her students at all times. If the preceptor will not be available, a staff member should be notified for temporary coverage (i.e. bathroom breaks, etc).
Blood pressures greater than 165/95 require a consult to proceed.
The Preceptor Form will be filled out in its entirety by the preceptor and will include pt name, pt DOB, printed student name, printed preceptor name, if student reviewed the HHx and checked BP, and if the student requested/took films. The preceptor will also list the procedures performed by tooth number and sign off in the box for each procedure.

6/13/2011
35
Preceptor Sign Off Sheet