comparative study of functional outcome of lateral locking plate fixation and dual plating in...
TRANSCRIPT
D R . O M P A R S H U R A M P A T I L
D R . G . N . P U N D K A RM . S . O R T H O P A E D I C S ,P R O F E S S O R A N D H E A D , D E P A R T M E N T O F O R T H O P A E D I C S ,D R . P D M M C ,A M R A V A T I
Comparative study of functional outcome of lateral locking plate fixation and dual plating in closed fracture’s of Schatzker’s Grade V of tibial condyles in adults.
Introduction
Constitutes 1% of all fractures
8% of all elderly fractures.
Body weight transmission through knee joint and leg, it plays a vital role in knee function and stability
The incidence of malunion, non-union and infections are relatively high in many reported series, causing significant long term disability.
Hence ,Soft tissue friendly approaches and minimally invasive techniques have improved outcome.
Aims and Objectives
Early mobilization of knee joint.
To assess the union of fractures after fixation.
To assess functional outcome, range of motion of knee joint after surgical management.
Materials and Methods
Prospective two year study was conducted at our institute
40 Patients of closed Bicondylar tibial plateau fractures(Schatzkers grade V) aged 18 years and above were selected randomly and treated by lateral locking plate fixation and dual plating in alternate cases.
Patients with pathological proximal tibial fractures other than osteoporosis and Patients who were medically unfit for surgery were excluded in this study.
Materials and Methods
After obtaining detailed history, complete general physical and systemic examination patients were subjected to relevant investigations and surgery.
Follow-up clinical and radiological evaluation done at 6 weeks ,12 weeks and six months,
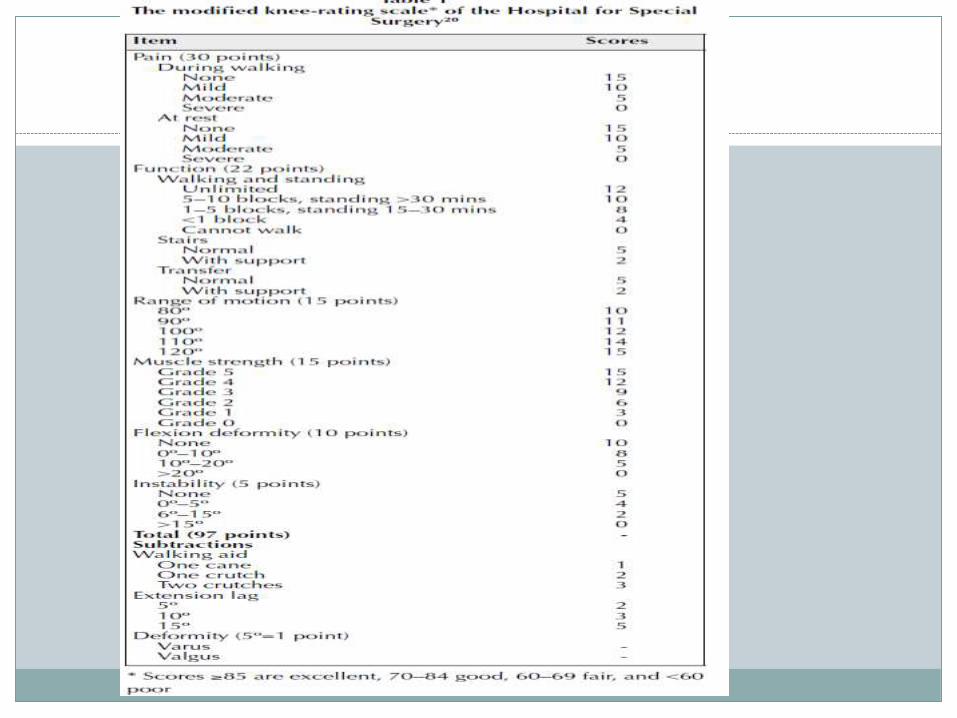
Post operatively patients were followed upto six months and evaluated with Rassmussen functional grading score and Hospital for special surgery knee score

Radiological Investigation
X- Ray of the Knee joint and upper half of tibia anteroposterior, lateral view and oblique views
Computerized tomography scan with 3D reconstruction of knee joint , as per requirement.
Early management
Immobilization
Strict limb elevation
Skin or skeletal traction till tissue oedema resolves
Ice fomentation
Enzymatic oral preparations chymoral, bromelainand rutoside and antibiotics if required.
Types Of Treatment
Lateral locking plate fixation
Single incision with minimally invasive technique was used.
Dual plating
Dual incision technique
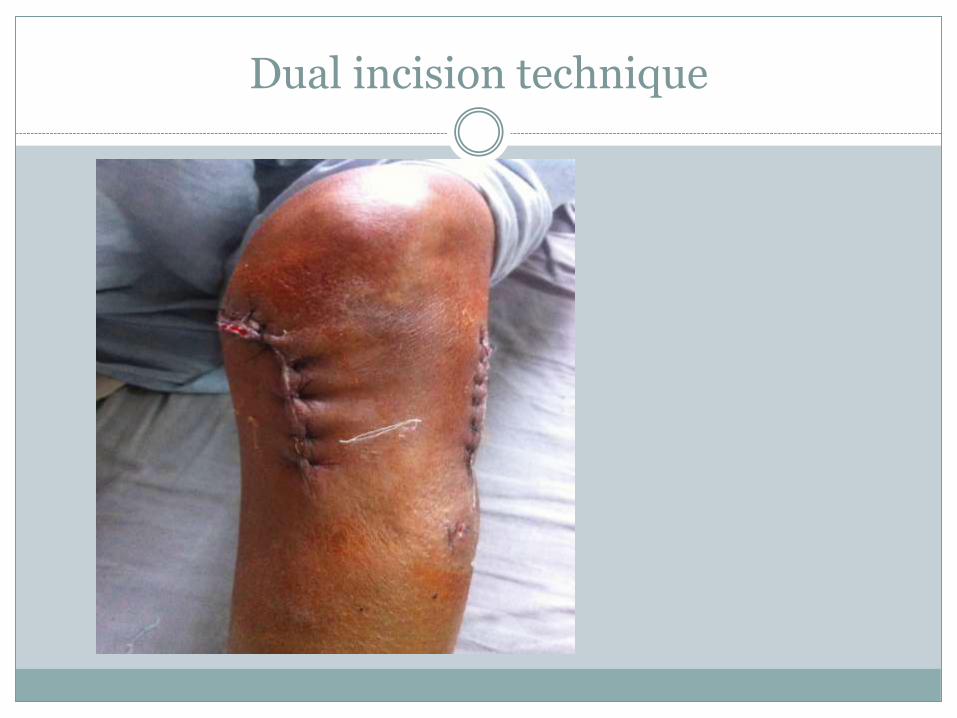
Dual incision technique

Dual Plating


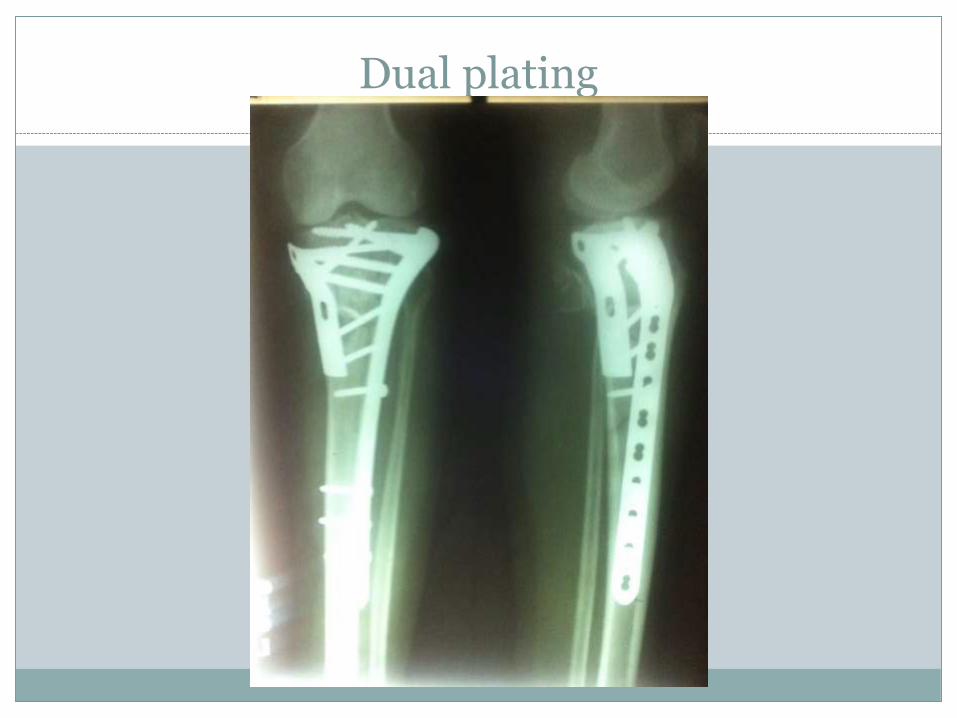
Dual plating
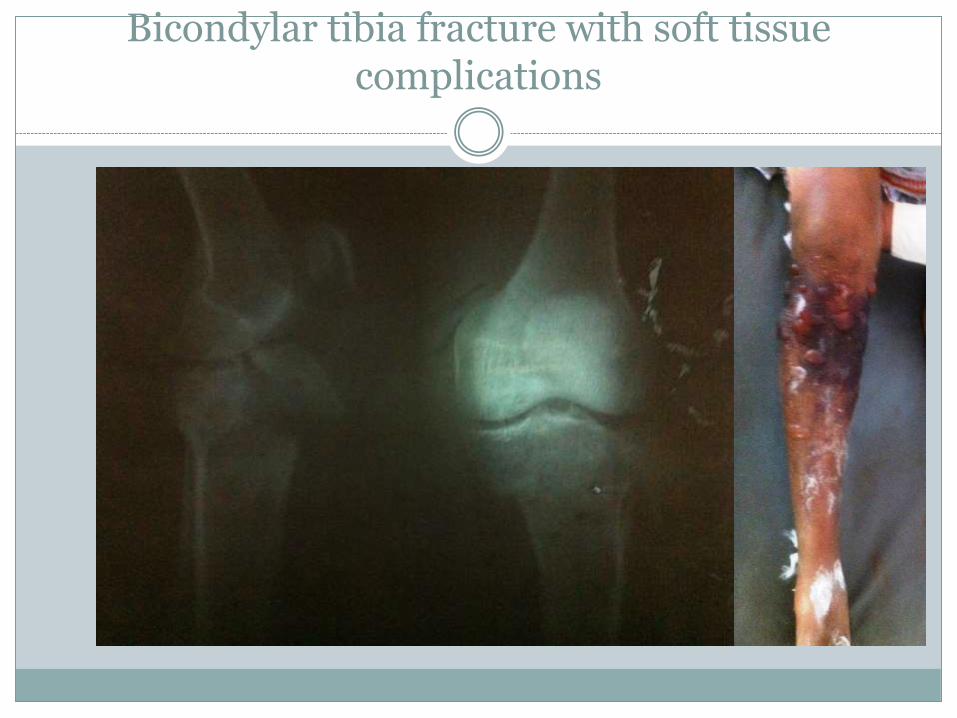
Bicondylar tibia fracture with soft tissue complications

Lateral locking plate fixation
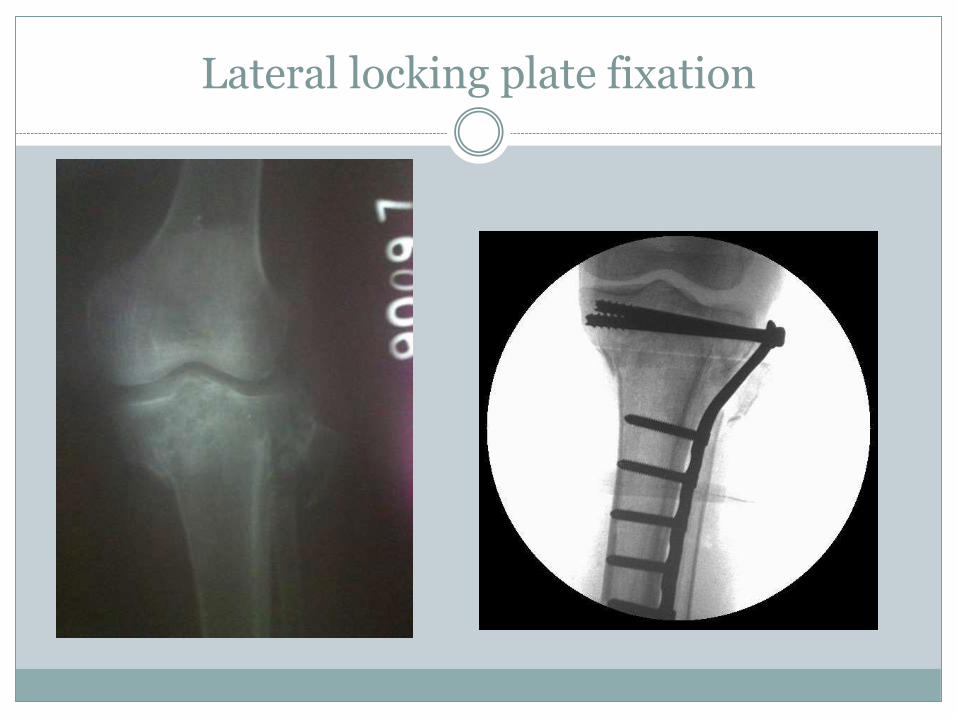
Lateral locking plate fixation

Post op three months
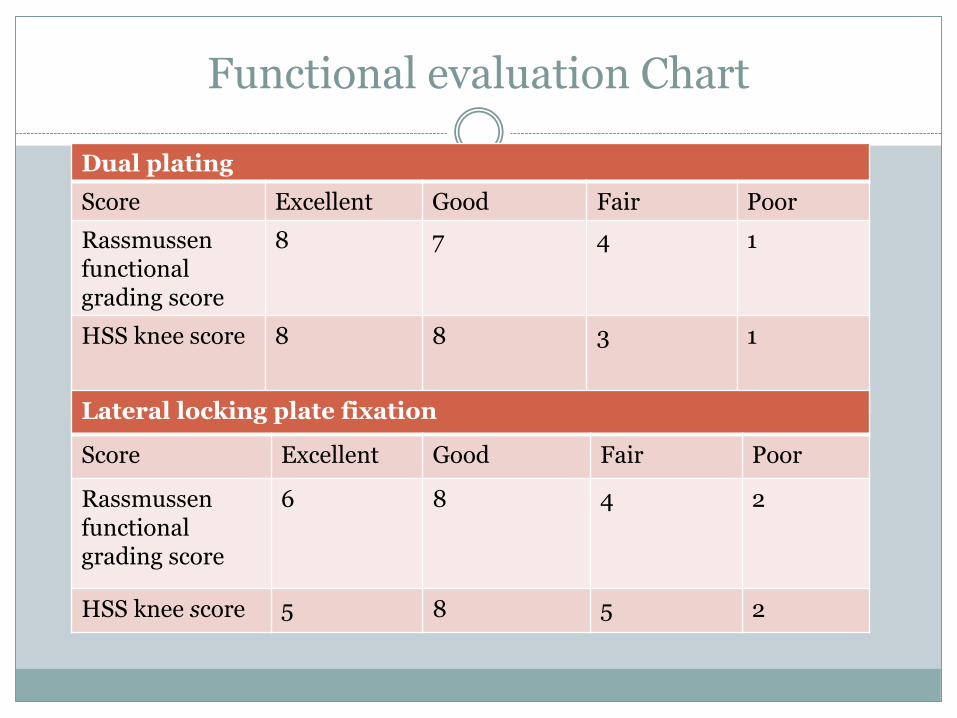
Functional evaluation Chart
Dual plating
Score Excellent Good Fair Poor
Rassmussenfunctional grading score
8 7 4 1
HSS knee score 8 8 3 1
Lateral locking plate fixation
Score Excellent Good Fair Poor
Rassmussenfunctional grading score
6 8 4 2
HSS knee score 5 8 5 2
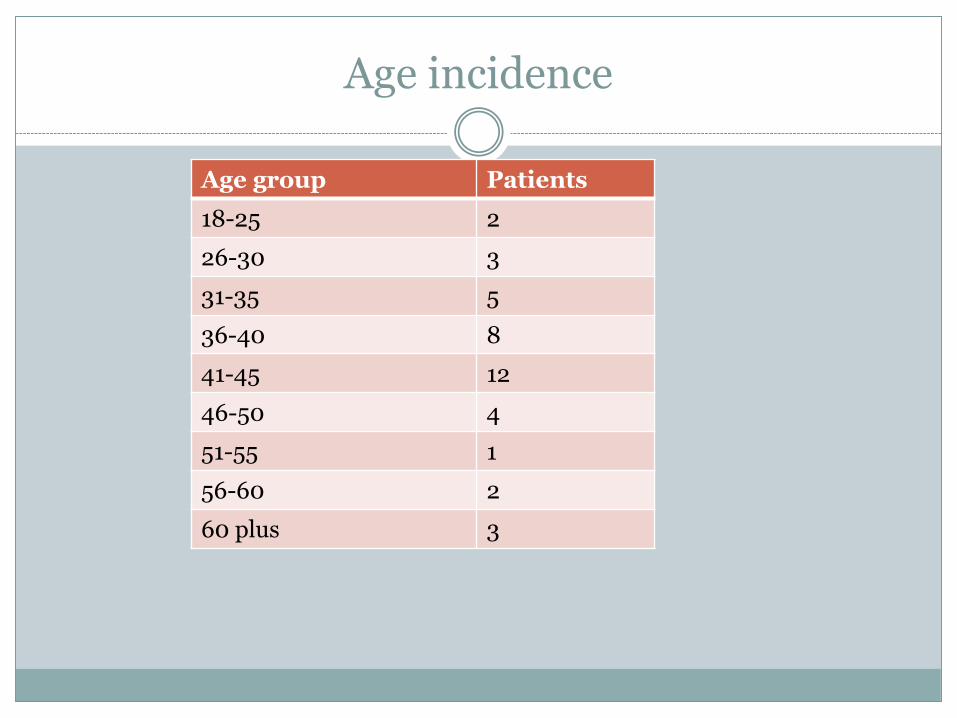
Age incidence
Age group Patients
18-25 2
26-30 3
31-35 5
36-40 8
41-45 12
46-50 4
51-55 1
56-60 2
60 plus 3

Range of motion
Lateral locking plate Dual plates
<70 0 0
71-80 1 1
81-90 2 1
91-100 6 4
101-110 7 9
111-120 2 3
121-130 1 1
131-140 1 1

Complications of surgery and fracture
Early complications
Compartment syndrome
Soft tissue complications and wound healing
Common Peroneal nerve injury
Anterior cruciate ligament tear in posteromedial fracture
Late complications
Post traumatic joint stiffness
Secondary osteoarthritis
Ligamentous instability
Results
Mean time of surgery was after 12 days (2 to 34 days),
Average knee mobilization was started in 7 days(2 to 16),
The average time to healing fractures was 16 weeks (minimum 13 weeks , maximum 6 months).
The overall knee range of motion averaged 105°(range 70–135°) at the latest follow-up of average 8 months in both the groups.
Conclusion
Dual plating is the best modality of treatment available for bicondylar tibia fracture
Dual plating has more stabilty as compared to lateral locking plate fixation alone,
Early union of fracture and weight bearing exercises.
Prolonged non weight bearing over the knee joint was adviced to prevent early varus deformities.
Limitations
Dual plating has its own limitations like
Soft tissue complications
More blood loss
More surgery time than lateral locking plate alone.
Discussion of the tibial Condyle fractures
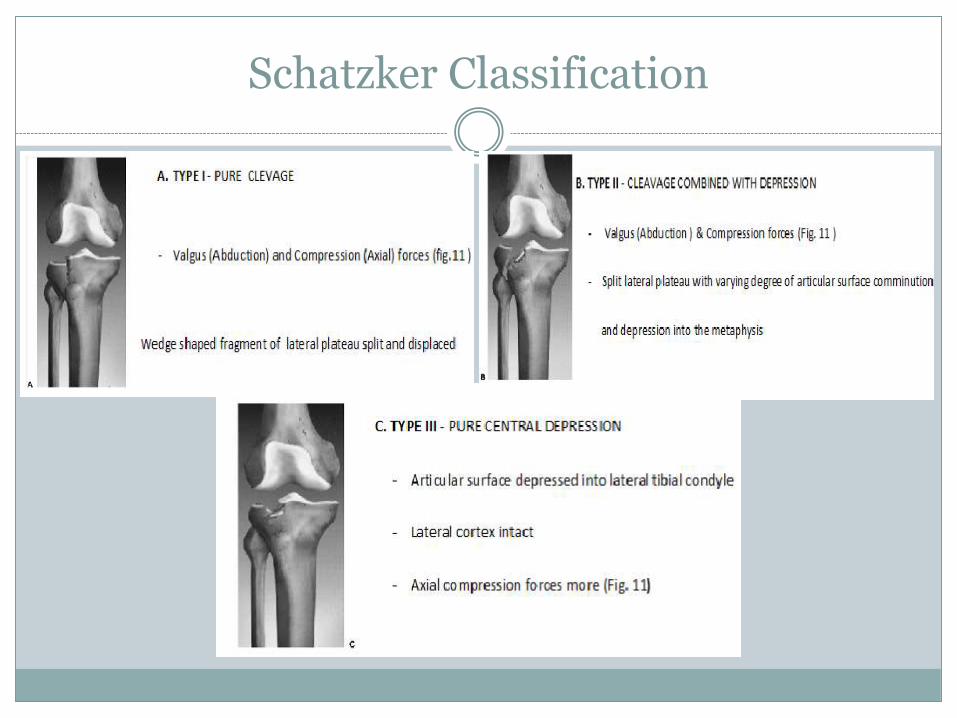
Schatzker Classification
Most widely used and familiar classification of tibialplateau fractures.
For instance, Hohl in 1969 classified split, split depression, and central depression fractures.
Many surgeons may not be familiar with the numbers of the six types, but most are familiar with the meaning of the verbal descriptions of each type and this is an important advantage of the Schatzker classification.
Because the six types are typically treated differently, the classification fufills some of the goals of an ideal classification.
Schatzkers classification is most widely used and familiar classification of tibial plateau fractures.
Surgical management was advised for fractures with greater than 5mm displacement or greater than 5 degress of instability on varus valgus stress
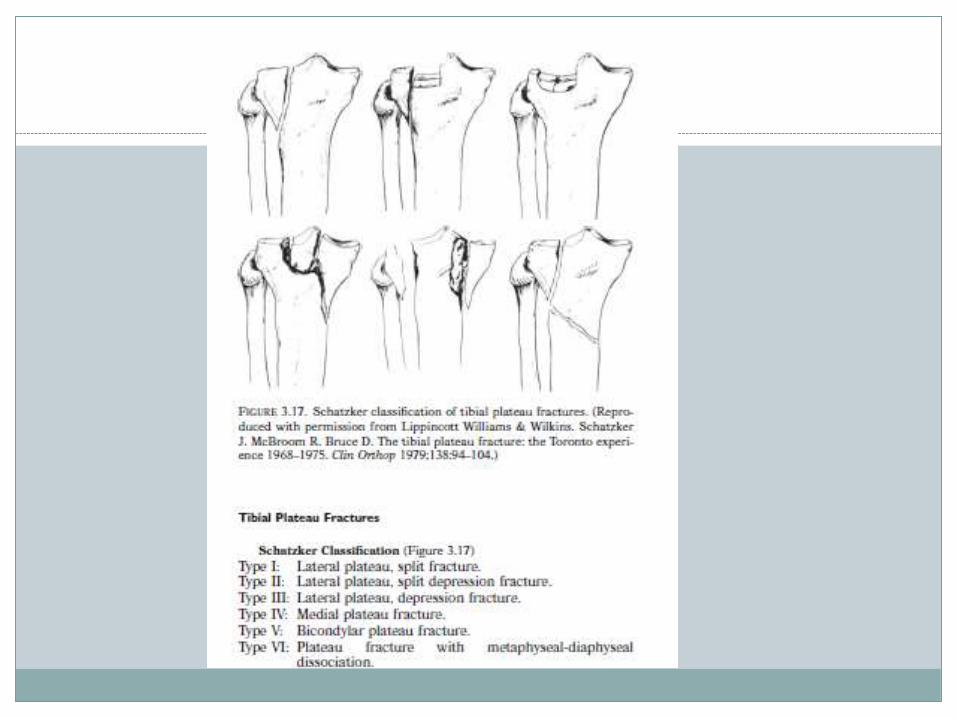
Schatzker Classification
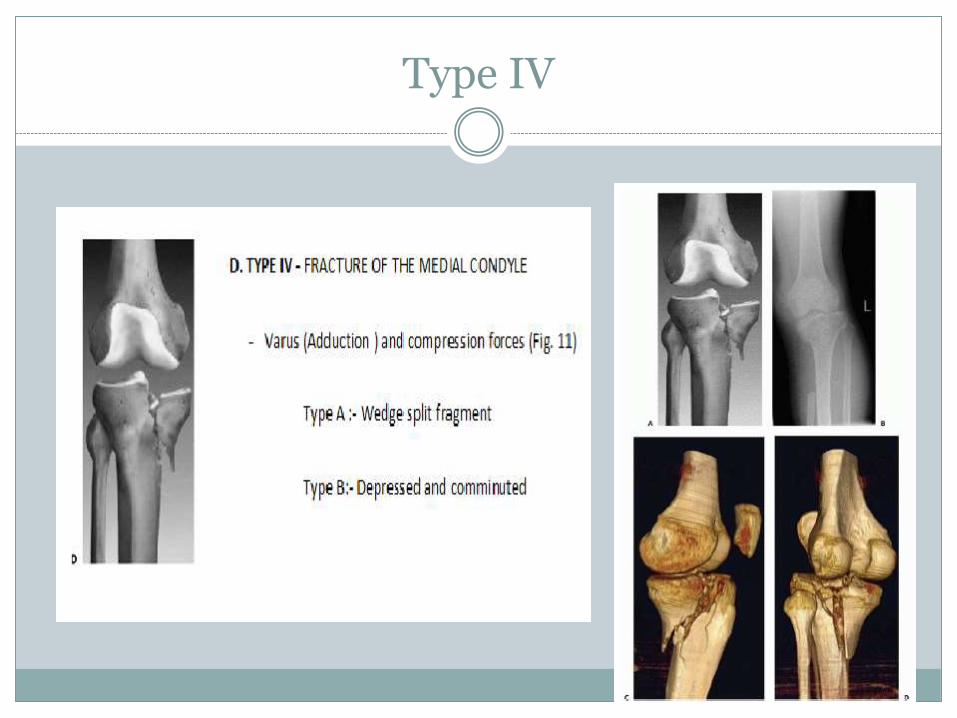
Type IV
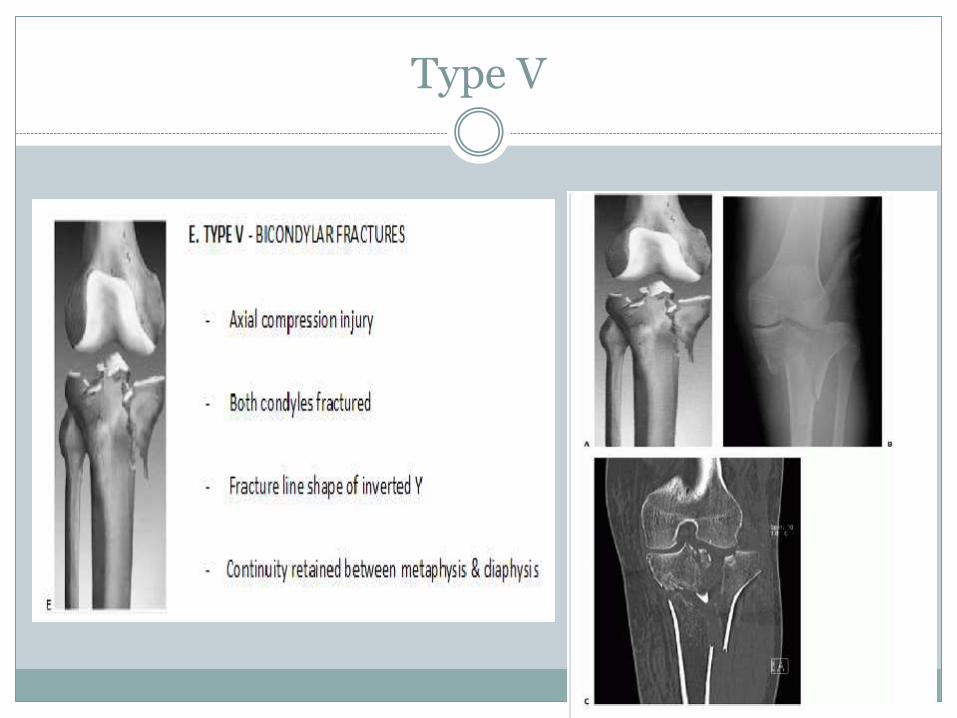
Type V
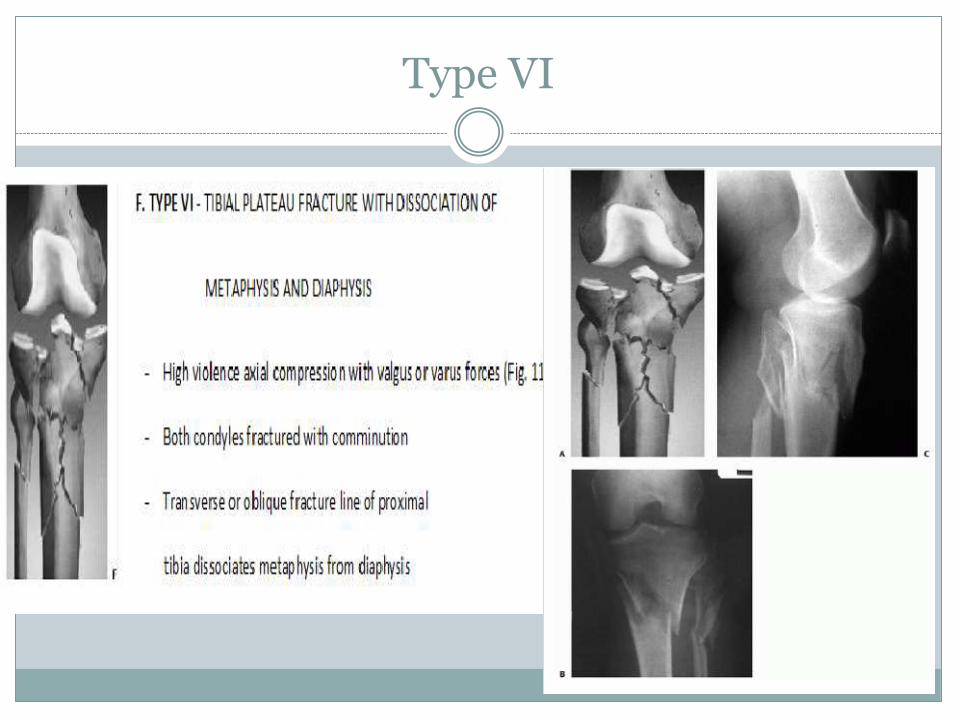
Type VI
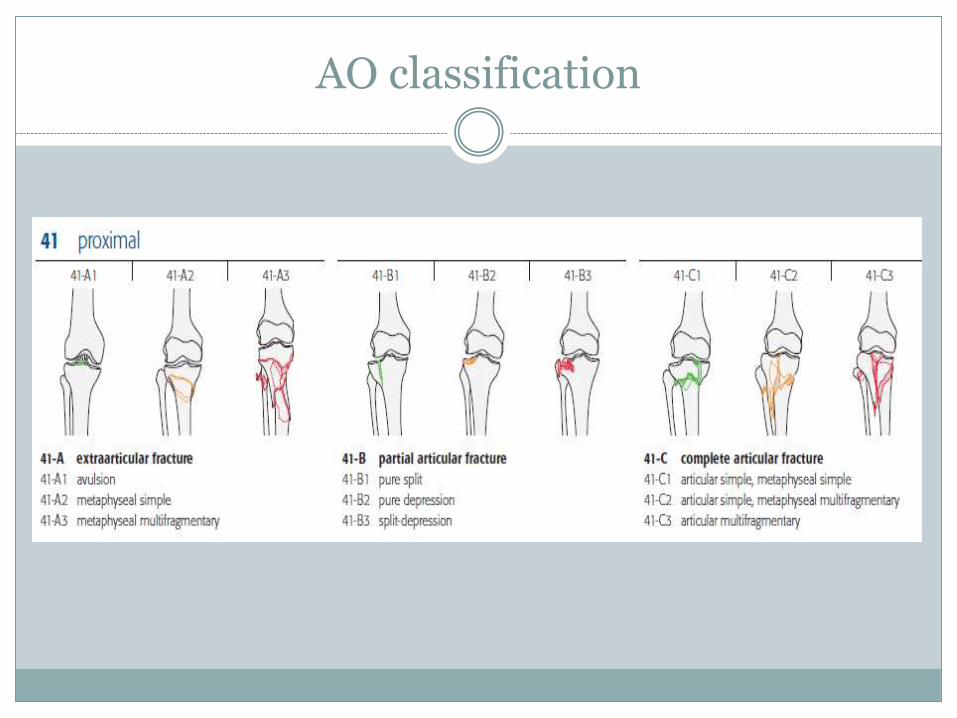
AO classification
References Rockwood and green page 1491Schatzkers classification of tibial condyle fractures. Kenneth. A. Egol and Kenneth J Koval , In: Fractures of proximal tibia : chapter 50 , Rockwood and
Green’s “Fractures in Adults”, Vol. 2, 6th edition, Lippincott Williams and Wilkins In: Fractures of tibia and fibula. chapter 52 , Rockwood and Green’s “Fractures in Adults”, Vol. 2, 7th
edition, Lippincott Williams and Wilkins Cole, Peter. MD*; Zlowodzke, Micheal MD+; Kregor, Philip J. MD+. Treatment of proximal tibial fractures
using the Less Invasive Stabilisation System: Surgical Experience And Early Clinical results in 77 fractures. Journal of orthopaedic trauma 18(8):528-535, September 2004.
Egol, Kenneth A. MD; Su, Edward MD; Tejwani, Nirmal C MD; Sims, Stephen H. MD; Kummer, Frederick J. PhD; Koval, Kenneth J. MD. Treatment of complex tibial plateau fractures using the less invasive stabilisation system plate: clinical experience and a laboratory comparison with double plating. Journal of trauma injury infection and critical care. 52(2):340-346 AUGUST 2004
Sommer, C.H; Wullschleger, M; Walliser, M; Bereiter, H; Leutenneger, A experience with locking compression plate in fracture treatment of osteoporotic bones. British journal of surgery, Vol 91(7) july2004 page 912.
Lang G J, Cohen B E, Bosse M J et al . Proximal third tibial shaft fracture. Should they be nailed ? Clin. Orthop 1995; 315:64-74.
Kenneth Koval “Handbook of fractures” ch 37 tibial plateau “Comparison of unilateral locking plate fixation and dual plating in bicondylar tibia fracture” Meng Hsuan
lee,Chien , lee Kai JOSR 2014 9:62 Barei DP, Nork SE, Mills WJ, et al. Complications associated with internal fixation of high-energy
bicondylar tibial plateau fractures utilizing atwo-incision technique. J Orthop Trauma 2004;18:649-657 Boldin C, Fankhauser F, Hofer HP, et al. Three-year results of proximal tibia fractures treated with the
LISS. Clin Orthop Relat Res2006;445:222-229. Gosling T, Schandelmaier P, Muller M, et al. Single lateral locked screw plating of bicondylar tibial plateau
fractures. Clin Orthop Relat Res2005;439:207-214.
References
Haidukewych G, Sems SA, Huebner D, et al. Results of polyaxial locked-plate fixation of periarticular fractures of the knee. J Bone Joint SurgAm 2007;89A:614-620.67.
Jiang R, Luo CF, Wang MC, et al. A comparative study of Less Invasive Stabilization System (LISS) fixation and two-incision double plating forthe treatment of bicondylar tibial plateau fractures. Knee 2008;15:139-143.
Marsh JL, Buckwalter J, Gelberman R, et al. Articular fractures: does an anatomic reduction really change the result? J Bone Joint Surg Am2002;84A:1259-1271.
Mueller KL, Karunakar MA, Frankenburg EP, et al. Bicondylar tibial plateau fractures: a biomechanical study. Clin Orthop Relat Res2003:189-195
Phisitkul P, McKinley TO, Nepola JV, et al. Complications of locking plate fixation in complex proximal tibia injuries. J Orthop Trauma2007;21:83-91
Ricci WM, Rudzki JR, Borrelli J Jr. Treatment of complex proximal tibia fractures with the less invasive skeletal stabilization system. J OrthopTrauma 2004;18:521-527
Watson JT, Phillips M, Karges D, et al. Lateral locking plates for the treatment of bicondylartibial plateau fractures: treatment protocol,indications, and results. Presented at the 23rd Annual Meeting OTA 2007, October 19, 2007, Boston, MA.
Sommer, C.H; Wullschleger, M; Walliser, M; Bereiter, H; Leutenneger, A experience with locking compression plate in fracture treatment of osteoporotic bones. British journal of surgery, Vol 91(7) july 2004 p. 912.

Thank you