comparative veterinary ophthalmology - cal > home
TRANSCRIPT

COMPARATIVE VETERINARY OPHTHALMOLOGY
QuickTimeª and aYUV420 codec decompressor
are needed to see this picture.

Recommended Texts
QuickTimeª and aTIFF (Uncompressed) decompressorare needed to see this picture.
Newest and Best Two Volume Set

Surgical Laboratory Videos
Surgical Videos
Download at
www.schostereye.org
PW = harley

Lights
QuickTimeª and aTIFF (LZW) decompressor
are needed to see this picture.
Pelican Lights
Pelican Lights Web Site WelchAllyn Web Site

Lenses
Home Made LensObtain Lens from Melles GriotWeb Site for Melles Griot where lens can be ordered
((585) 244-7220
01 LAG 011Plano-Convex Aspheric Lens; f = 42.0 mm, dia = 45 mm
Paraxial Focal Length: 42.0 mm Material : Crown glass
Unit Price: $28.00
Obtain Plastic Holder from Hardware Store
Plumbing Fitting $2.00
QuickTimeª and aTIFF (LZW) decompressor
are needed to see this picture.
WelchAllyn Web Site
VOLK
The Ophthalmic History and Examination
Clinical ProblemThe First Step in solving ANY Problem is to:
DEFINE THE PROBLEM
• Solving of a patients Clinical Problem– In ophthalmology, almost 99% of the
information collected and utilized in making the initial tentative diagnosis which will direct the subsequent diagnostic and therapeutic plan is based on:The clinicians OBSERVATIONS

THE OPHTHALMIC EXAMINATION FLOW CHART
GOAL = SOLVE THE PATIENT’S PROBLEM • *Signalment• *Primary complaint• *History• *Ophthalmic Examination• *Special Diagnostic Tests• Problem List• Differential Diagnosis• Diagnosis• Therapy• Prognosis• Re-examination plan
* Key Defining Information

Signalment
• Species• Breed• Age• Sex• Coat Color• Altered or not

Primary Complaint
HistoryWhat led you to believe your animal hasan eye problem?
* Loss of Vision* Eye discharge* Peculiar color of eye(s)* Veterinarian noted problem* Other, explain
HistoryHow long has this problem been present? Which eye(s) is (are) affected?
RIGHT LEFT BOTH
Has the character of the eye(s) changed sinceyou first noticed it? YES NO UNK
If yes, how?Have you treated the eye(s)? YES NO UNK
If yes, how, and with what?

HistoryHow well do you believe your animal sees?
* Excellent* Poor in regard to moving objects* Poor on all occasions* Poor in regard to stationary objects * Poor especially in dim light or dark* Poor when turning to the right* Poor especially in bright light* Poor when turning to the left * Poor in regard to near objects* Poor when jumping or climbing down * Poor in regard to far objects* Poor when jumping or climbing up
HistoryDo you think your animal sees well in familiarsurroundings?
YES NO UNK
Strange surroundings?YES NO UNK
Has your animal had any other eye problems?NO YES UNK
If YES, what type?

HistoryHas your animal experienced seizures, loss of balance,weakness, in coordination or personality change?
NO YES UNK Is your animal receiving medication?
NO YES UNKIf YES, what?
Do you have other animals?NO YESIf YES, do they have eye problems? NO YES
If YES, what type?
Do you know your animal's dam or sire?NO YES UNK
HistoryIf YES, do either of them have eye problems? NO YES
UNK13. Is your animal consuming water and food normally?
YES NO UNK14. Is you animal urinating more frequently than normal?
YES NO UNK15. Has your animal had previous or present illness? NO
YES UNK 16. Has your animal been exposed to house or farm
chemicals (cleaners, agricultural, industrial or automotive chemicals) or building supplies? NO YES UNK

Ophthalmic ExaminationKNOWING:
CHIEF COMPLAINTSIGNALMENT
andPERFORMANCE OF A GOOD
MEDICAL HISTORY
WILL GREATLY HELP DIRECT AND REFINE YOUR
OPHTHALMIC EXAMINATION THIS WILL RESULT IN AN
ACCURATEPROBLEM LIST and DIAGNOSIS
CHIEF COMPLAINT
SIGNALMENT
+
HISTORY
Focus
OPHTHALMIC EXAM
PROBLEM LIST
ACCURATE DIAGNOSIS

Examination Environment
The examination environment is important and can greatly influence the examination results. In an environment that is too distractive and bright, a complete careful examination can not be done; especially in an animal that is unruly. Small animals are best examined on a table with a non-slip surface. Unruly cats can be placed in a cat bag for the examination. For large animals, try to locate a non-confined area that is away from the general activity, which provides adequate lighting that can be reduced when necessary.
Vision Testing • Menace Response
• Cotton Balls
• Maze Testing
Menace Response
• This is a response and it is learned.
• The endpoint is a blink. QuickTimeª and a
YUV420 codec decompressorare needed to see this picture.
Cotton Balls
QuickTimeª and aYUV420 codec decompressor
are needed to see this picture.

Maze Testing
Video provided by
Sinisa Grozdanic D.V.M., Ph.D. Iowa State University
QuickTimeª and aH.263 decompressor
are needed to see this picture.

Gross Evaluation of the Head
• Symmetry – Compare one side with the other

Gross Evaluation of the Head • Step back and compare the palpebral
fissures for their size, symmetry, position of the upper eyelid cilia and the general eyelid form, as well as characterization of any ocular discharge.
• Ocular discharge if present should be characterized as serous, mucoid, purulent, hemorrhagic, seromucoid, mucopurulent, or serosanguinous.
Gross Evaluation of the Head – The position of the upper eyelid cilia normally should be
directed nearly perpendicular -semivertical to the corneal surface. Subtle ptosis or drooping of the eyelid without noticeable narrowing of the fissure would be detected by observing more ventrally directed cilia. Horner's syndrome: sympathetic denervation (ptosis, miosis, enophthalmia, prolapsed third eyelid) can be due to pre or post ganglionic sympathetic denervation.

Pupillary symmetry
Pupillary symmetry can be evaluated by viewing the animal head on from about 6 feet through a direct ophthalmoscope set a 0 diopters and stimulating a tapetal reflection (eye shine).
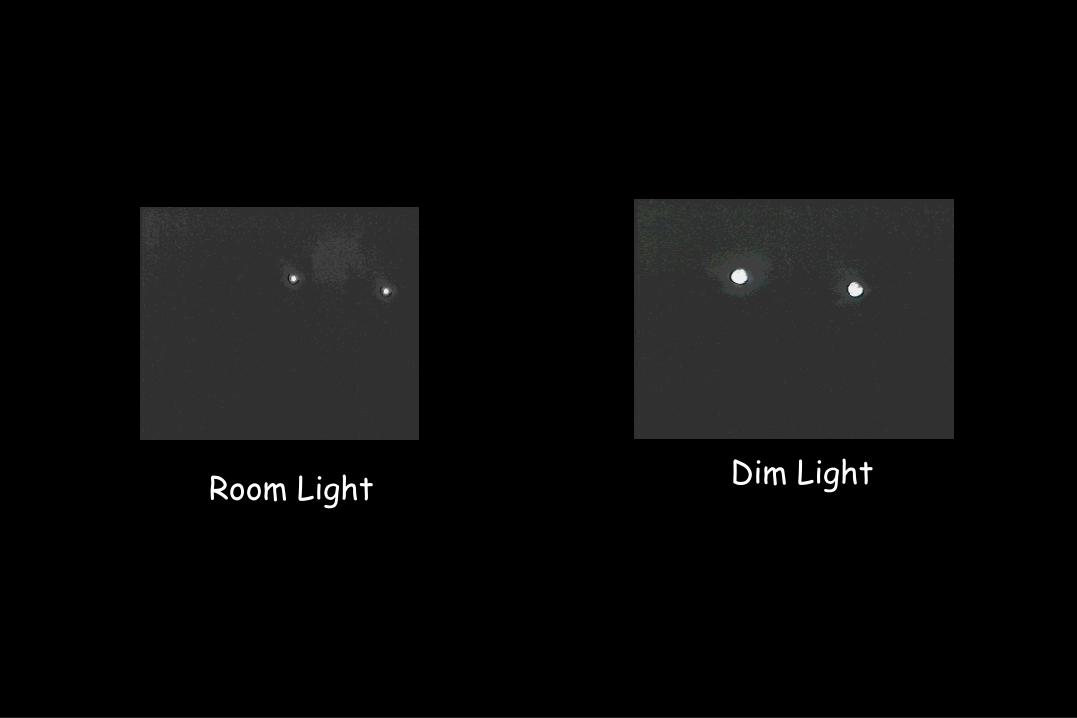
Room Light Dim Light

Reflexes and Neurological Responses
• Palpebral Reflex • Corneal Reflex• Dazzle Reflex• Pupillary Light Reflex
Reflexes and Neurological Responses
• Palpebral Reflex Video on the left shows a clinical example of the technique as well as clinical patient with a CN 5 lesion.
Left eye Normal palpebral reflex
Right eye Abnormal
CN 5 Lesion
Notice that the lack of sensation is only in the temporal upper lid not nasal so if only the nasal area was stimulated the CN5 lesion would have been missed!!!Tests CN 5 and CN 7
QuickTimeª and aMotion JPEG OpenDML decompressor
are needed to see this picture.
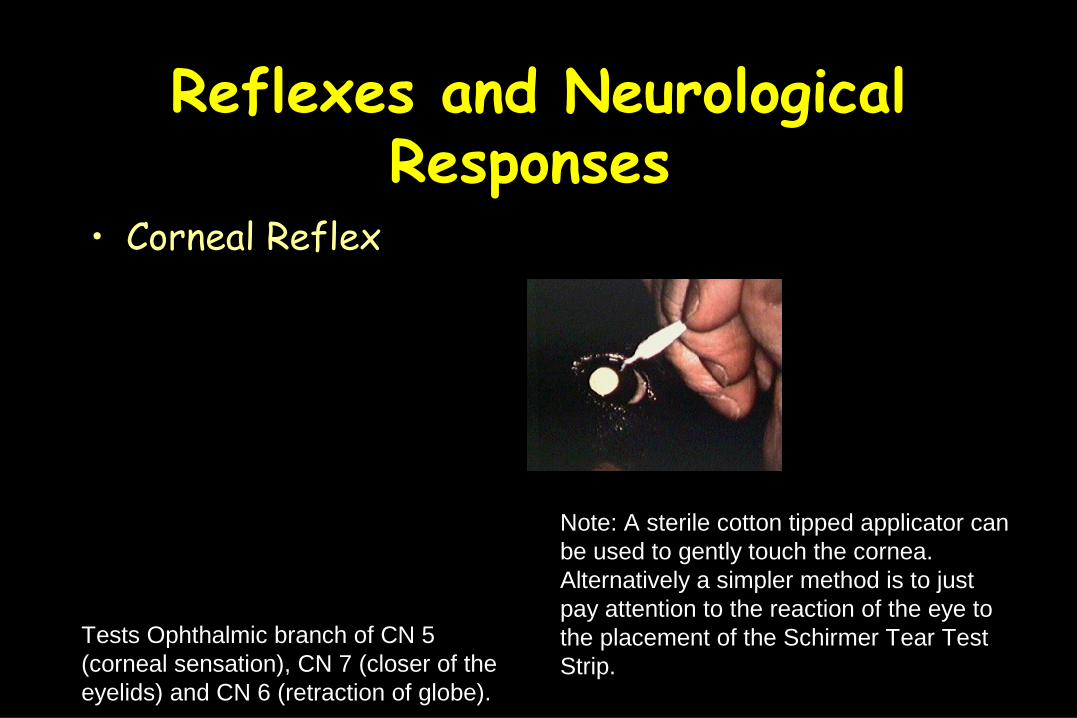
Reflexes and Neurological Responses
• Corneal Reflex
Note: A sterile cotton tipped applicator can be used to gently touch the cornea. Alternatively a simpler method is to just pay attention to the reaction of the eye to the placement of the Schirmer Tear Test Strip.
Tests Ophthalmic branch of CN 5 (corneal sensation), CN 7 (closer of the eyelids) and CN 6 (retraction of globe).
QuickTimeª and aYUV420 codec decompressor
are needed to see this picture.
Reflexes and Neurological Responses
Dazzle Reflex- not a vision test
- tests continuity of retina, optic nerve

Reflexes and Neurological Responses
The Pupillary Light Reflex is not a vision test.MUST USE A BRIGHT FOCAL LIGHT
CATARACTS WILL NOT BLOCK A PLR
Drawing by M. Wyman
QuickTimeª and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Representative PLR Diagram taken from Kathleen B. Digre, M.D. ハ ハ DEPARTMENTS OF NEUROLOGY AND OPHTHALMOLOGY UNIVERSITY OF UTAH MEDICAL CENTER
A bright light used to stimulate direct PLR and ideally a second person then observes the fellow pupil with a weak dim light in
most species, since it is hard to see the fellow pupil in just room light.

PALPATION Orbital zone and Orbital rim
Feel for topographical changescharacterize them:
hard or soft, moveable or fixed, sensitive or insensitive and orbital or extra-orbital swellings/masses.
QuickTimeª and aYUV420 codec decompressor
are needed to see this picture.
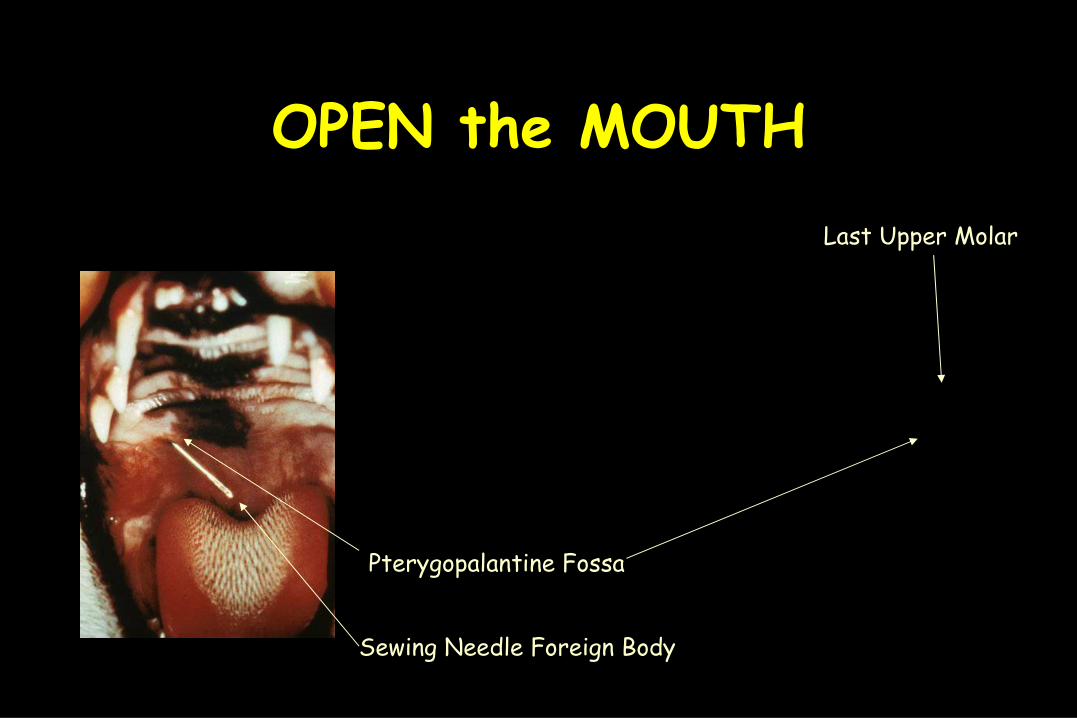
OPEN the MOUTH
Pterygopalantine Fossa
Sewing Needle Foreign Body
Last Upper Molar
Close Gross Evaluation EyelidsConjunctivaThird EyelidCorneaAnterior ChamberIrisLensVitreous and fundus:
Indirect and Direct ophthalmoscopic exam
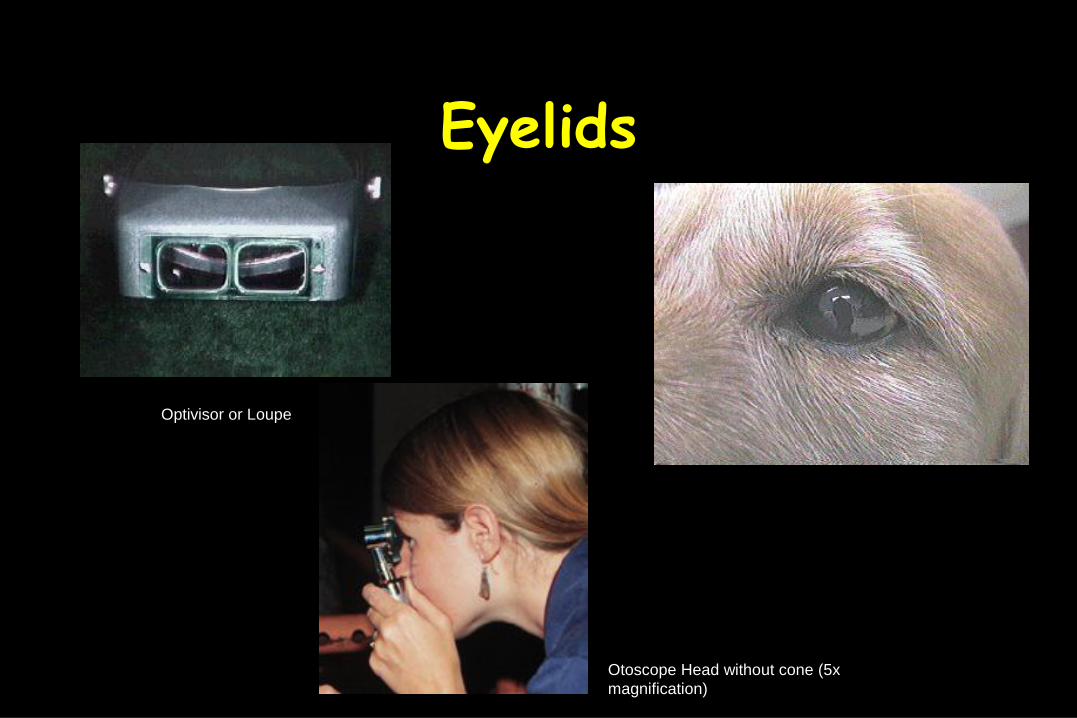
Eyelids
Optivisor or Loupe
Otoscope Head without cone (5x magnification)

Conjunctiva
Third Eyelid
The third eyelid is covered with the palpebral conjunctiva which has bulbar and palpebral surfaces and the obvious gross feature is that the bulbar surface has a cluster of lymph follicles. Examine the anterior surface simply by retropulsing the globe.

CorneaEvaluate the cornea briefly for its clarity and surface characteristics (smooth, uniform and glistening normally).

Anterior Chamber
Slit Lights
Anterior Chamber
Lens
Click hereFor Info.About slit light
QuickTimeª and aYUV420 codec decompressor
are needed to see this picture.

Iris
Edilon Hand Held Slit Light - Excellent!!

Lens
EXAMINE AT AN ARMS LENGTH
LOOK FOR OPACITIES IN THE LENS
DIRECT OPHTHALMOSCOPE
SET AT 0 DIOPTERS
Step One
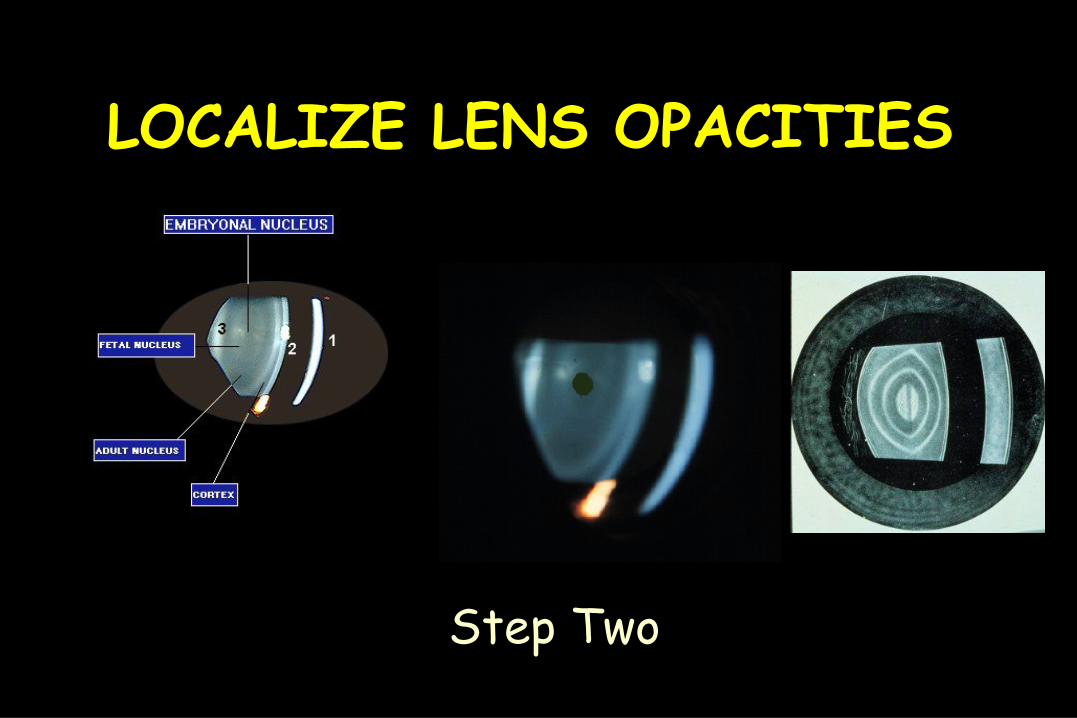
LOCALIZE LENS OPACITIES
Step Two

Vitreous and Fundus• Indirect Ophthalmoscopic Exam
• Direct Ophthalmoscopic Exam
QuickTimeª and aYUV420 codec decompressor
are needed to see this picture.
Direct Ophthalmoscope tid bits
• One diopter of change = movement of 0.2 mm in the cat, 0.3mm in the dog, 0.7 mm in the ox, and about 1.3 mm in the horse.
Special Diagnostic Tests
• Schirmer Tear Test• Culture• Fluorescein• Eyelid Eversion• Nasolacrimal Flush

Schirmer Tear TestSchirmer tear test
valuesNormal – 15 – 25 mm/60
secMarginal – 10 – 15 mm/60
secLow <10 mm/60 sec
QuickTimeª and aYUV420 codec decompressor
are needed to see this picture.
Culture
QuickTimeª and aYUV420 codec decompressor
are needed to see this picture.

Fluorescein
Note: If an Immunofluorescent Antibody Test (IFA for Herpes or Chlamydia) is planned in a cat, do not apply Fluorescein before doing the conjunctival scraping. Fluorescein will cause a false positive test result to occur. Fluorescein may affect the IFA result for up to 7 - 10 days.
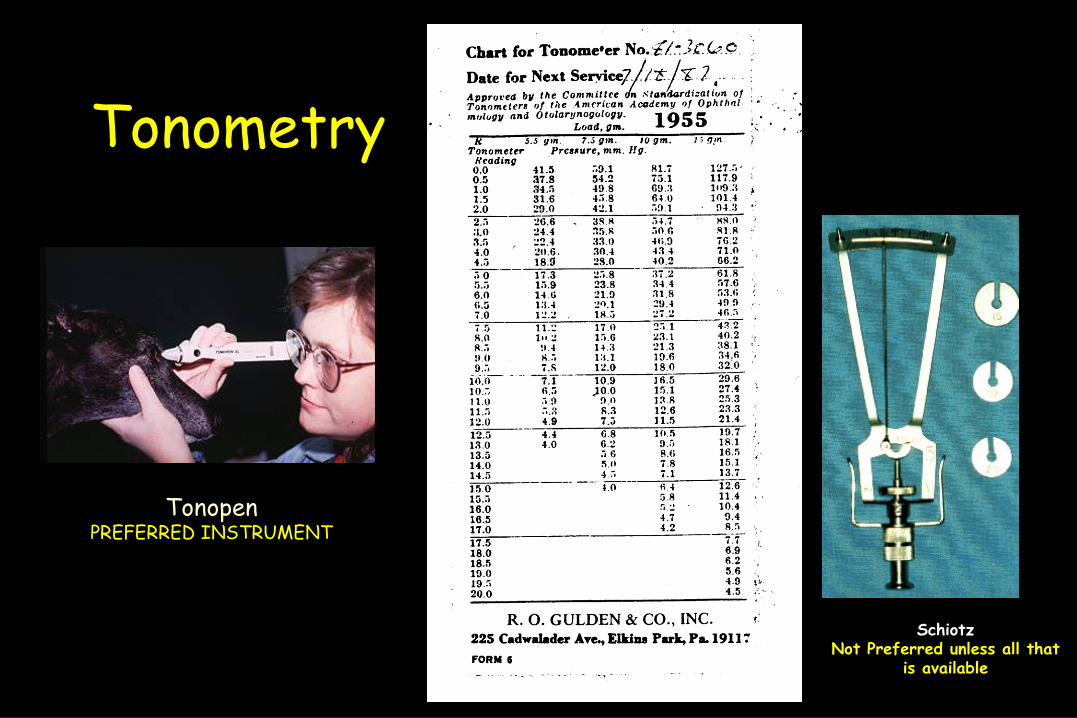
Tonometry
TonopenPREFERRED INSTRUMENT
SchiotzNot Preferred unless all that
is available

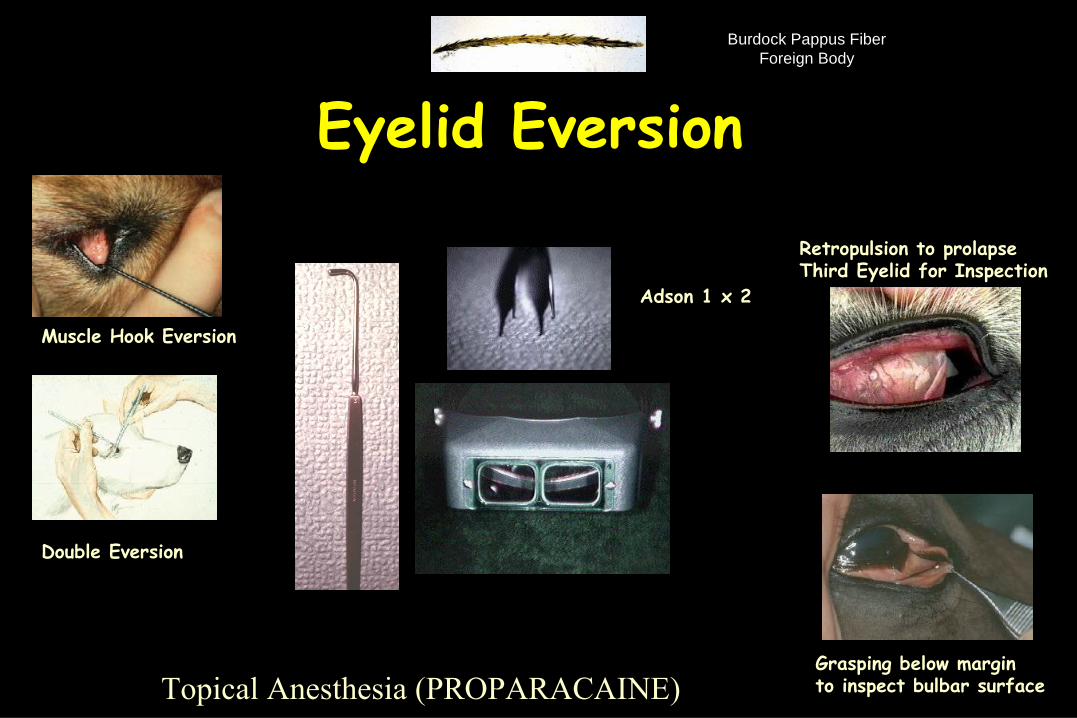
Eyelid Eversion
Muscle Hook
Adson 1 x 2
Retropulsion to prolapseThird Eyelid for Inspection
Grasping below marginto inspect bulbar surface
Double Eversion
Muscle Hook Eversion
Topical Anesthesia (PROPARACAINE)
Burdock Pappus FiberForeign Body

Conjunctival Scraping
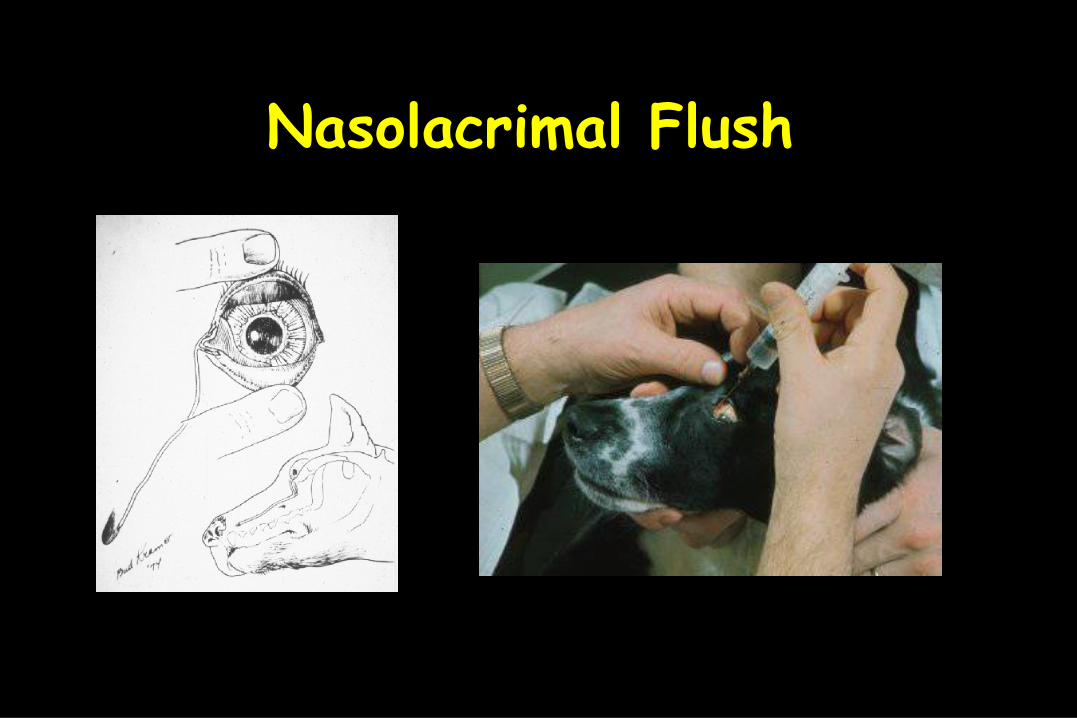
Nasolacrimal Flush

Gonioscopy
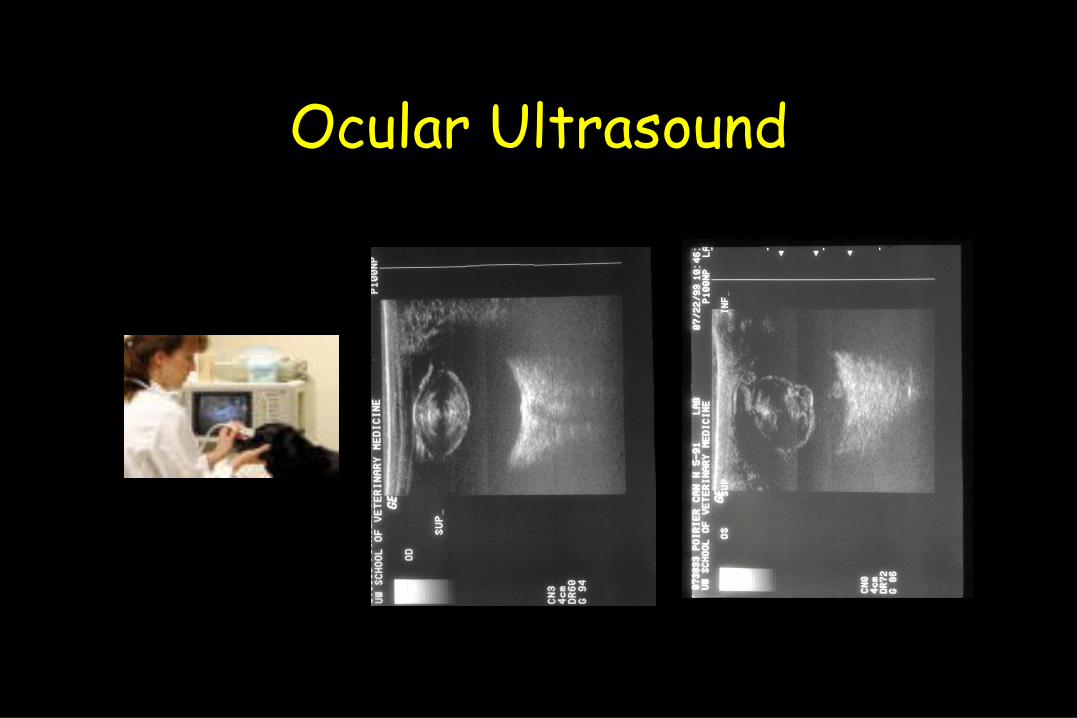
Ocular Ultrasound

Electroretinogram

At the completion of the exam:
• Make a list of all of the problems that were identified.
• This list can be as unrefined (red eye) or refined (anterior uveitis) as you can at this point.
• Create the Temporary Problem List

Temporary Problem List
5
4
3
2
1
Try to Group Problem“Refine” Problem List
• For Example:– Conjunctival hyperemia– Serous ocular discharge– Aqueous Flare– Miosis– Enophthalmia with prolapse of the third eyelid
• Group to: ANTERIOR UVEITIS

Initial Differential DiagnosisFor Each Problem
• For Example: There are at least twelve possible reasons for the Red Eye
• Blepharitis• Cherry Eye• Conjunctivitis• Corneal Hemorrhage• Episcleritis• Glaucoma• Hyphema• Iris Hemorrhage• Intraocular Neoplasia• Keratitis• Subconjunctival Hemorrhage• Uveitis

Clinical Diagnosis• The Tentative Clinical Diagnosis is based
upon the findings in the previous steps.– Combination of the
• Signalment• Primary Complaint• History• Ophthalmic Examination
• A Final Diagnosis can be made initially or after subsequent diagnostic tests have been performed.
Therapy• The therapy of course depends on the diagnosis
– Many times there are pending laboratory test or other diagnostic procedures and the exact clinical diagnosis can not be made yet. However the patient needs some form of therapy started immediately.
– The decision of what therapy to initially institute is based on the findings up to this point. One must be cautious and avoid therapies that could cause harm if given in the face of a condition where that therapy was contraindicated.

Prognosis
• Depends on severity of the problems.• Depends on accuracy of diagnosis.• Depends on the diagnosis; some disorders
are more serious than others.
Re-examination Plan
• Hospitalize• Send home on treatment
– Re-examine 24 hours to 7 days• Depending on the severity and what the diagnosis is.
Key Points to Consider During General Physical Examination
• SIGNALMENT• PRIMARY COMPLAINT• HISTORY• GROSS APPEARANCE OF THE HEAD
• SYMMETRY• RED EYE ?• CLARITY OF THE OCULAR MEDIA• MONOCULAR INDIRECT OPHTHALMIC EXAMINATION

COMPARATIVE VETERINARY OPHTHALMOLOGY