comparison between mulligan bend leg raise technique and butler neural mobilization on pain and...
TRANSCRIPT
“COMPARISON BETWEEN MULLIGAN BEND LEG RAISE TECHNIQUE AND BUTLER
NEURAL MOBILIZATION ON PAIN AND STRAIGHT LEG RAISE IN LOW BACK PAIN
SUBJECTS.”
Introduction
Low back pain is the most prevalent of allmusculoskeletal conditions, afflicting everyone atsome time in their life.
In India incidence of low back pain has been reportedto be 23.09% and has a lifetime prevalence of 60-85%.
Low back pain is believed to involve 60% to 90% ofthe adult population at some point in their life time.It has been reported that 37% of health care costsassociated with low back pain are a direct result ofphysical therapy services.
Brian Mulligan pioneered the techniques of this concept in New Zealand in the 1970s. The concept has its foundation built on Kaltenborn’s (1989) principles of restoring the accessory component of physiological joint movement. Unique to this concept is the mobilization of the spine whilst the spine is in a weight bearing position and directing the mobilisation parallel to the spinal facet planes (Mulligan 1999). Passive oscillatory mobilisations called ‘NAGs’ (natural apophyseal glides) and sustained mobilisations with active movement ‘SNAGs’ (sustained natural apophyseal glides) are the mainstay of this concept’s spinal treatment (Mulligan 1999). The Mulligan concept of accessory gliding with active movement can be further expanded in our clinical practice to justify its place in the assessment of muscle dysfunction.
Neural mobilization is a method of conservativetreatment of disorders of neural tissue. Appropriate use of neural mobilization procedures
depends on excellent knowledge of normal and pathological
anatomy, differences between individual etiological factors,development of disease and symptom variability
Neurodynamics is an innovative management tools involve
conservative decompression of nerves, various neural
mobilizing techniques and patient education techniques
Neurodynamics offers a fresh understanding and
management strategies for common syndromes such as
plantar fasciitis, tennis elbow, nerve root disorders, carpal
tunnel syndromes and spinal pain.
.
To study the effect of Mulligan mobilization (bend leg raise technique) in patient with low back pain.
To study the effect of Butler Neural Mobilization in patient with low back pain.
The purpose of this study is to compare the outcomes between mulligan bent leg raise (BLR) and butler neural mobilization (NM) in straight leg raise (SLR)positive and low back pain (LBP) subjects .
Aim and objective of the study
Hypothesis
Null hypothesis (H0 ):
There will be no significant effect on pain and Rom in subjects treated with mulligan bend leg raise technique and butler neural mobilization with straight leg raise in low back pain subjects.
Experimental hypothesis (HA ):There will be significant effect on pain and Rom in subjects treated with mulligan bend leg raise technique and butler neural mobilization with straight leg raise in low back pain subjects.
ROL (review of literature)
Author’s Name Year Conclusion
Toby Hall 2005 There was a significant increase in the range by 7 degree in BLR group.
Toby Hall 2006 These results provide preliminary for the use of Mulligan’s TSLR technique in the management of LBP
L. Exelby 2002 It can also be incorporated with functional activities to assist in correcting joint positional faults within improved quality movement patterns.
ROL (review of literature)
Author’s Name Year Conclusion
David Butler 2005 neurodynamic mobilization techniques can be effective in addressing musculoskeletal presentations of peripheral neuropathic pain.
John D .Childs 2006 Slump stretching is beneficial for improving short-term disability, decreasing pain, and centralization of symptoms.

Methodology
Study design:
The study design used in this research will be randomized control trial.
Source of data:
Data will be taken from the the physiotherapy department of Doon P.G Paramedical college, dehradun.
Sample size:
The size of the sample will be forty(40).

Study sample:
Both male and female subjects with low back pain.
Sampling design:
Subjects will be randomly allocated into two groups i.e. group A and group B
Group A: mulligan’s bent leg raise (n=20).
Group B: butler’s neural mobilization (n=20).
Participants:
Participants with low back ache who will be referred to physiotherapy department and willing to take treatment for sessions will be recruit for study.
Method of data collection:
The method of data collection employed for the present study will be primary method.
Inclusion criteria:
Unilateral limitation of SLR more than 450.
Age group between 35 -60 years.
Refferd pain distal to buttocks.
No change of pain in lumber flexion and extension
Exclusion Criteria:
Patient with “Red flags” for a serious spinal conditions such as infection, tumors, osteoporosis, spinal fracture,
Pregnancy
History of spinal surgery
Diminished upper and lower extremity reflexes
Suggestive nerve root involvement
Presence of lower quarter neurological compromise
Materials:
Materials used for this study consisted of the following:
Consent Form – A signed consent form from the subjects to allow the subject to be included in the study.
Record or data collection sheet.
Variables:
Independent variable:
Mulligan’s bent leg raise technique
Butler’s neural mobilization
Dependent variable:
Pain (Visual analog scale)
Range of motion(SLR)
Instrumentation :
Bubble Goniometer- Used to measure Lumbar movements.
MAIN OUTCOME MEASURES Pain intensity:
By Visual analogue scale – A scale of 10 cm to evaluate intensity of pain where 0 represents no pain and 10 represent unbearable pain.
Range of motion:
Range of motion will be measured by Bubble Goniometer to measure Lumbar range of motions.
procedure All the subjects will be informed in detail about the type and
nature of the study and will be made to sign the informed
consent. Assessment of demographic data along with initial
assessment of visual analogue scale (VAS), range of motion
(ROM) will be measured pre-treatment and post-treatment of
the first session and last sessions.
GROUP A –
Will receive Mulligan’s Mobilization.
GROUP B –
Will receive Butler’s Neural Mobilization.

Mulligan’s bent leg raise technique Stand at the limited SLR side of the supine patient.
Place his flexed knee over shoulder and ask the patient to push the knee away with his leg and then relax, at this point therapist push patients bend knee up to as far as can in the direction of his shoulder, on the same side provided there is no pain.
If it is painful alter the direction by taking his leg more medially or laterally. Sustain this stretch for 5sec and repit it thrice in a session.
With the bend knee over the therapist's shoulder include a traction with this technique.

Butler’s neural mobilization 1. Patient was instructed to sit erect with knees in 900 of
flexion. The presence or absence of symptoms was recorded.
2. Patients were instructed to ‘‘slump’’ shoulders and lower back while maintaining the cervical spine in neutral. The presence or absence of symptoms was recorded.
3. While maintaining the position described in step 2 the patients was instructed to touch their chin to the chest and the clinician applied overpressure into cervical flexion. The presence or absence of symptoms was recorded.
4. While maintaining overpressure into cervical flexion the patient was instructed to extend the knee. The presence or absence of symptoms was recorded.
5. Position 4 was maintained while the patient was instructed to actively dorsiflex the ankle. The presence or absence of symptoms was recorded. This position was held for 30 sec,a total of 5 repetition.
6. Overpressure of the cervical spine was released and the patients were instructed to return the neck to a neutral position. The presence or absence of symptoms was recorded.
Both technique will be continue twice weekly for 3weeks total of 6 visit.
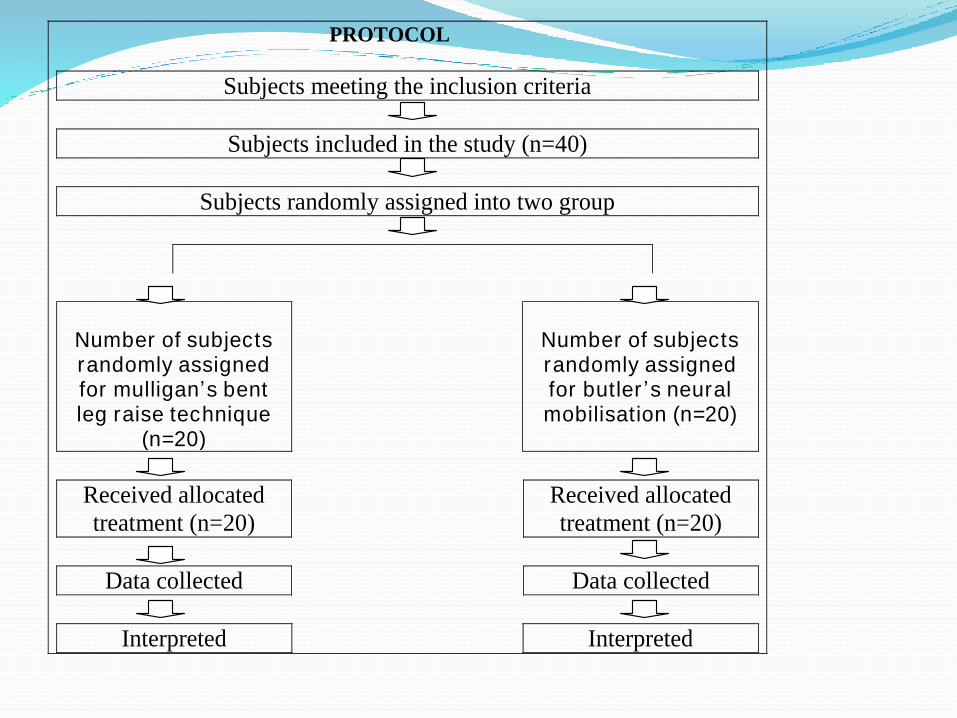
PROTOCOL
Subjects meeting the inclusion criteria
Subjects included in the study (n=40)
Subjects randomly assigned into two group
Number of subjects randomly assigned for mulligan’s bent leg raise technique
(n=20)
Number of subjects randomly assigned for butler ’s neural mobilisation (n=20)
Received allocated
treatment (n=20)
Received allocated
treatment (n=20)
Data collected Data collected
Interpreted Interpreted
`