compartment syndrome
TRANSCRIPT

DR HARDEV SINGHP.G IN ORTHOPAEDICS
BHMRCNEW DELHI
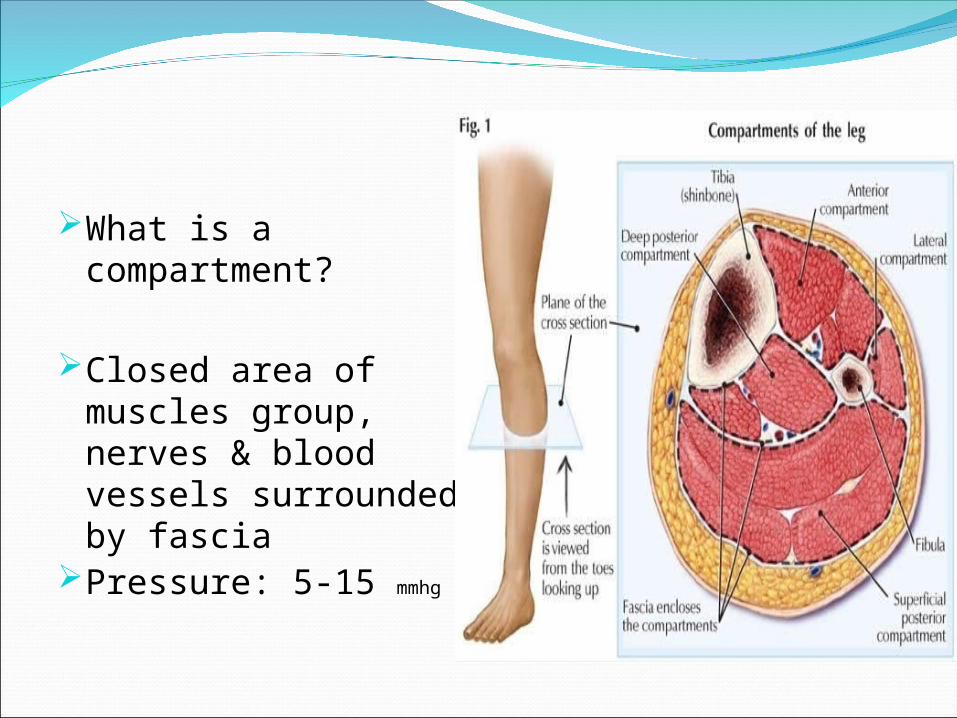
What is a compartment?
Closed area of muscles group, nerves & blood vessels surrounded by fascia
Pressure: 5-15 mmhg
Definition:An increased pressure within enclosed
osteofascial space that reduces capillary perfusion below level necessary for tissue viability; the underlying mechanism is:
- increased volume within space- decreased space for contents- combination of both
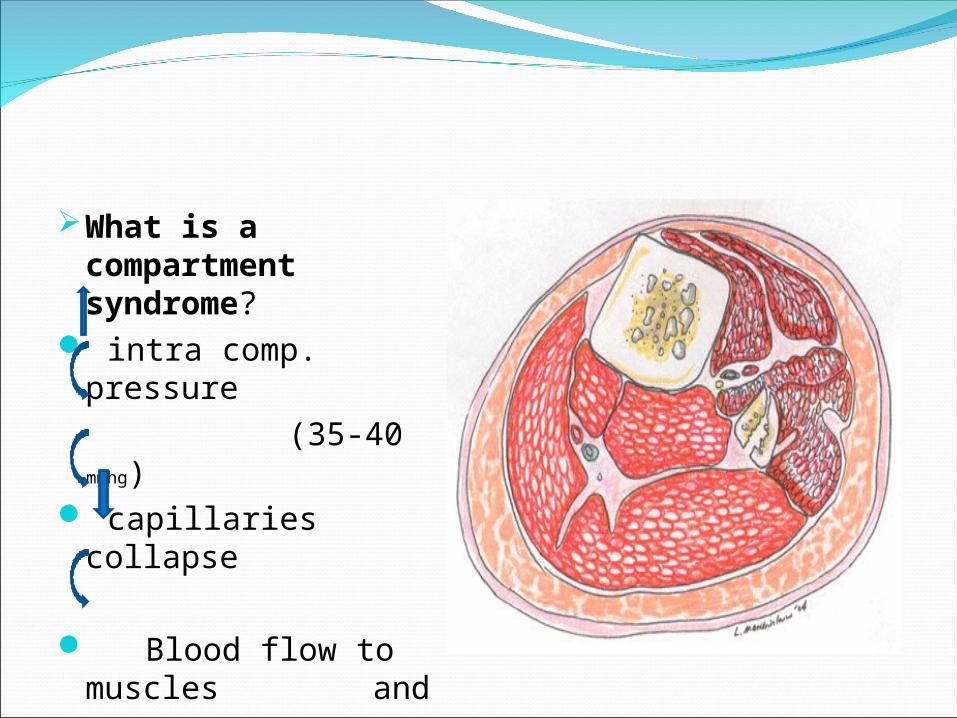
What is a compartment syndrome?
intra comp. pressure (35-40 mmhg) capillaries collapse
Blood flow to muscles and nerves
Bl.Vs collapse
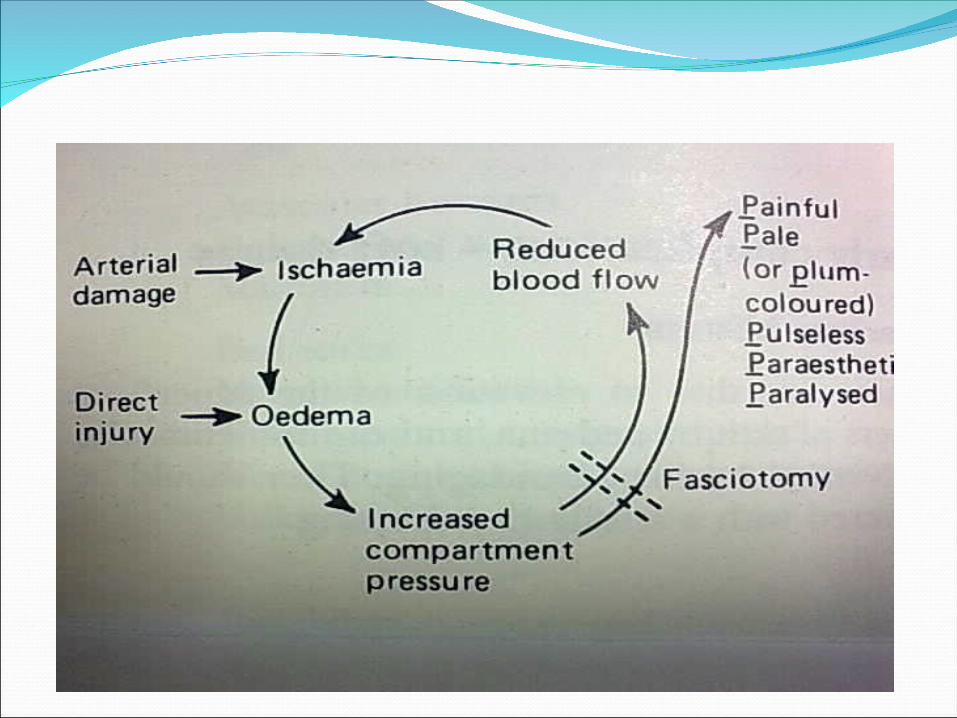
Pathophysiology:Increased compartment pressure
leads to increased venous pressure which decreases A-V gradient resulting in muscle and nerve ischemia.
Pathophysiology:Normal tissue pressure 0-4 mm Hg 8-10 with exertionAbsolute pressure theory30 mm Hg - Mubarak45 mm Hg - Matsen
Consequences –vicious cycle
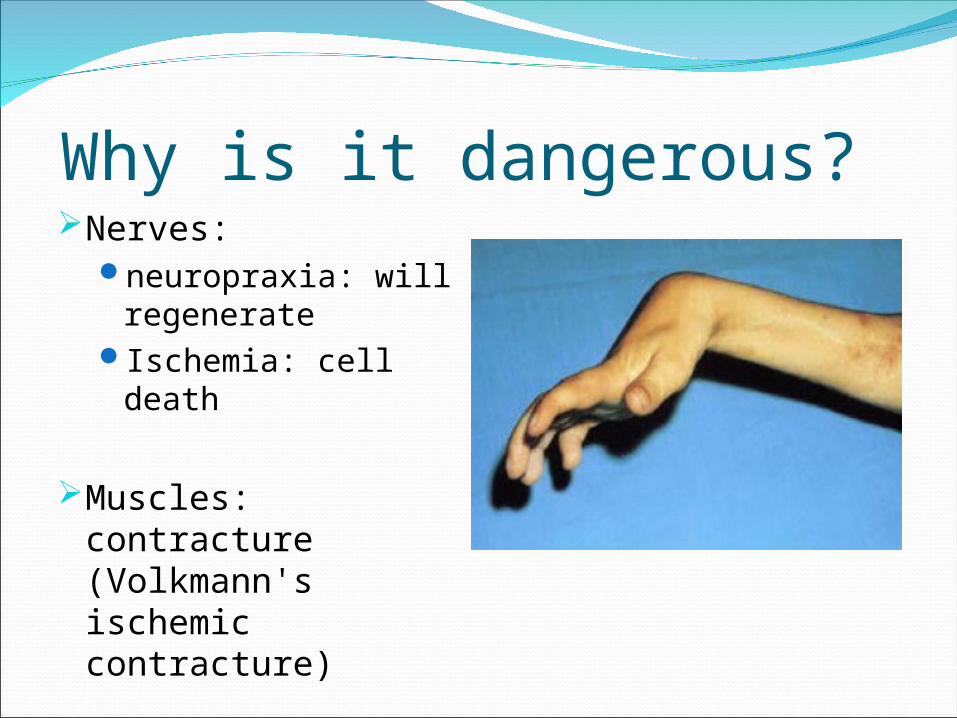
Why is it dangerous? Nerves:
neuropraxia: will regenerate
Ischemia: cell death
Muscles: contracture (Volkmann's ischemic contracture)
Gangrene
Compartment Syndrome- CAUSESCauses
Fractures Contusions Surgery Post Ischemic swelling after arterial occlusion Major vascular trauma Crush injuries Burns Prolonged limb compression
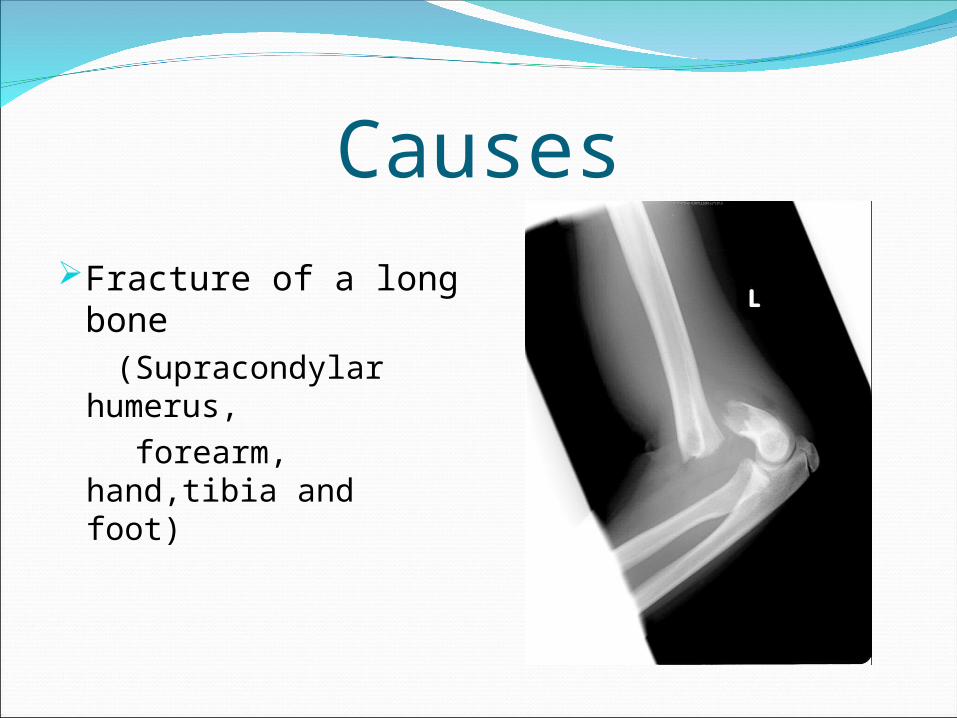
CausesFracture of a long
bone (Supracondylar
humerus, forearm, hand,tibia
and foot)


CAUSES
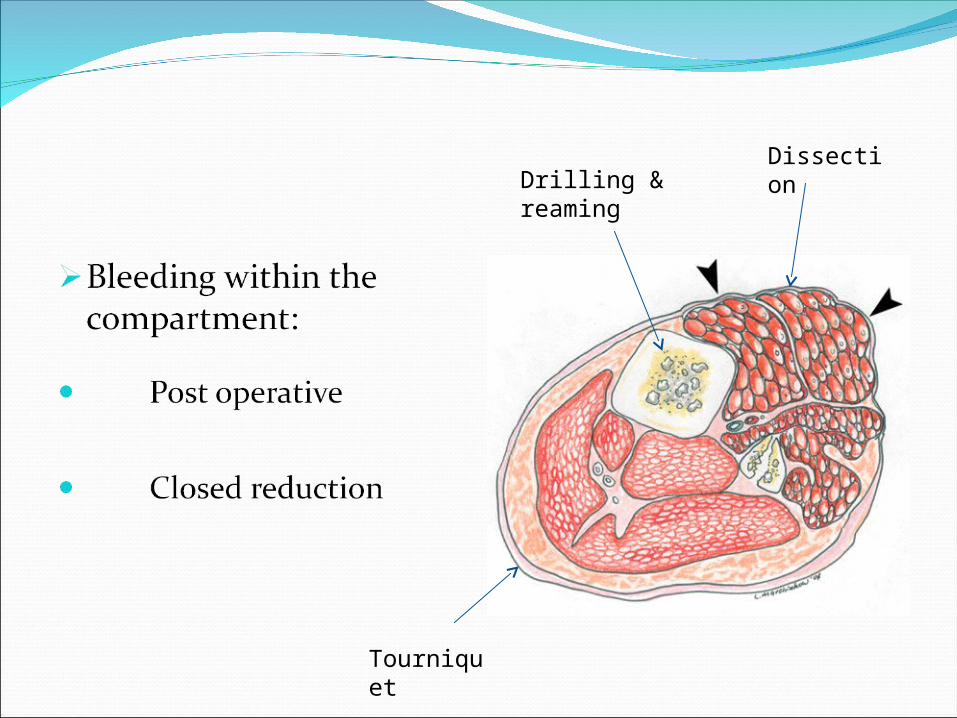
Drilling & reaming
Dissection
Tourniquet
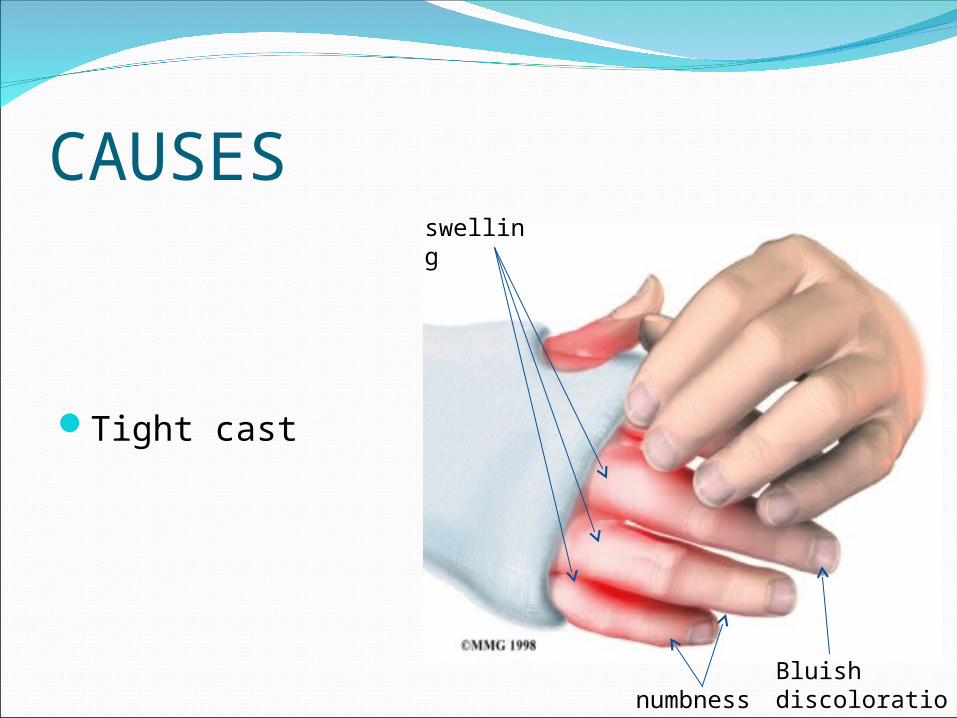
CAUSES
Tight cast
swelling
Bluish discolorationnumbness
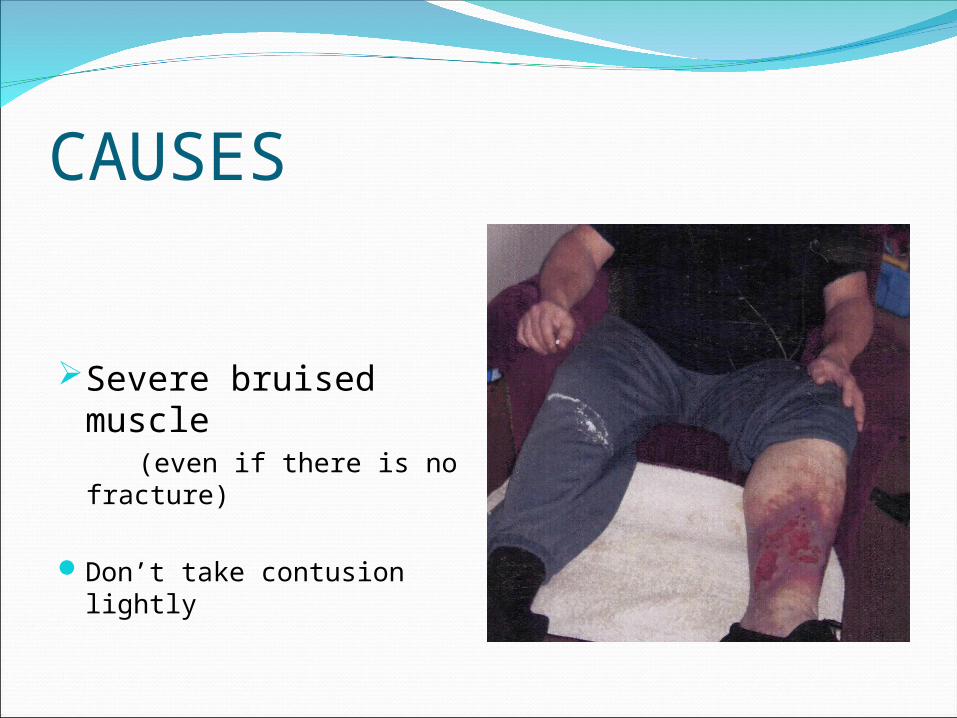
CAUSES
Severe bruised muscle
(even if there is no fracture)
Don’t take contusion lightly

COMPARTMENT SYNDROME
Signs and SymptomsIncreased Pressure and TightnessProgressive pain out of proportion to
initial injuryMarkedly swollen areaProgressive neurologic deficitSeven P’s
PainPressurePain with passive stretchParethesiaParesis/ ParalysisPulselessnessPallor
SYMPTOMS
Severe pain inappropriate to the injury(not relieved even with morphia)
SYMPTOMSBurning of the affected limb
Tight muscle(rigid)tightness feeling
Numbness: bad sign
SIGNS & DIAGNOSIS
Passive stretching of fingers or toes (muscle stretch)will lead to severe pain (diagnostic sign)
Never wait for signs of ischemia (5 Ps):irreversible damage
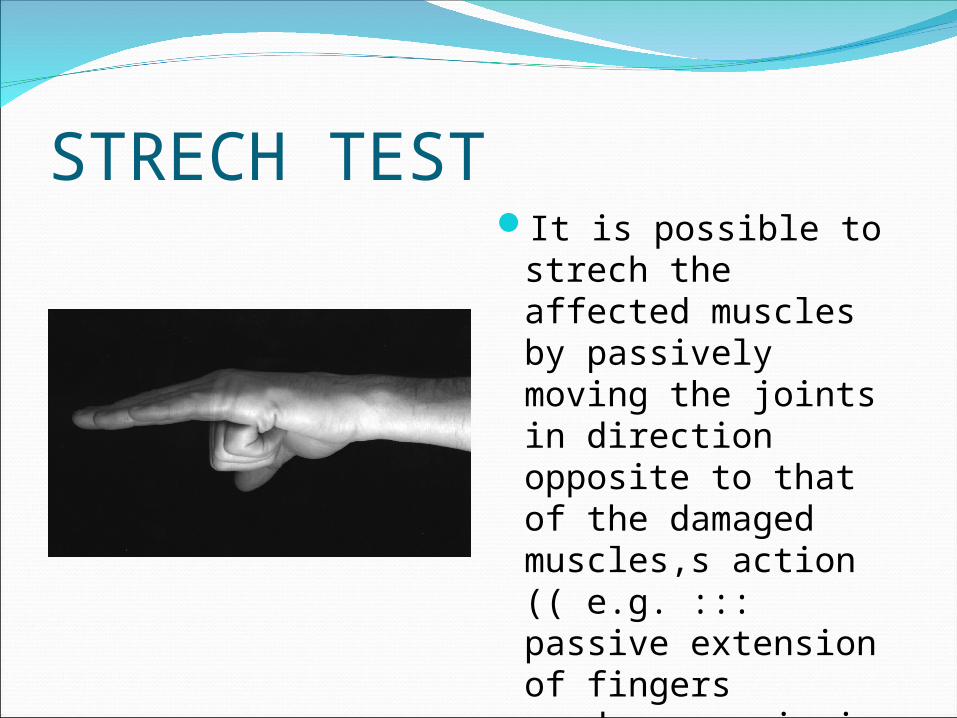
STRECH TESTIt is possible to
strech the affected muscles by passively moving the joints in direction opposite to that of the damaged muscles,s action (( e.g. ::: passive extension of fingers produces pain in flexor compartment of forearm
TechniqueSTRYKER
TECHNIQUEMERCURY
MANOMETERWick hand held
instrument
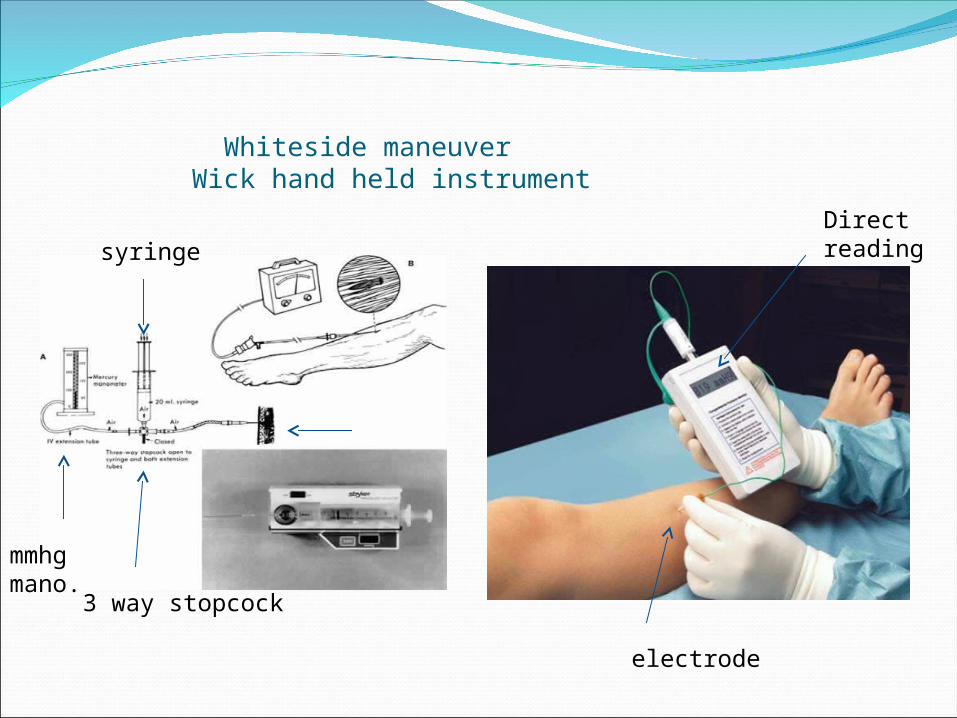
Whiteside maneuver Wick hand held instrument
syringe
3 way stopcock
mmhg mano.
electrode
Direct reading
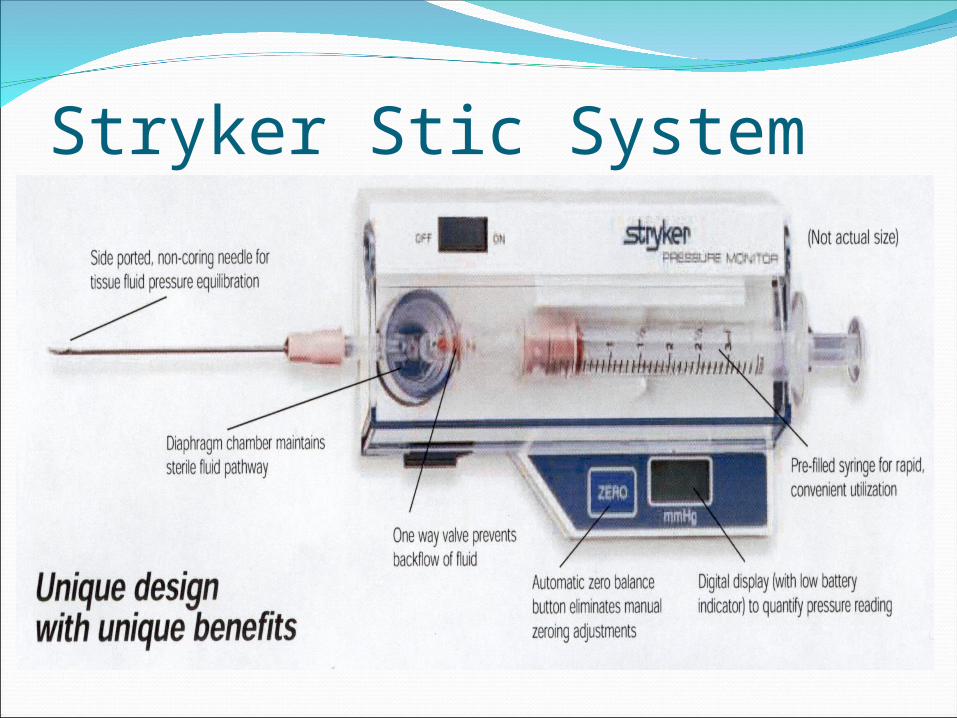
Stryker Stic SystemEasy to useCan check multiple compartmentsDifferent areas in one compartment
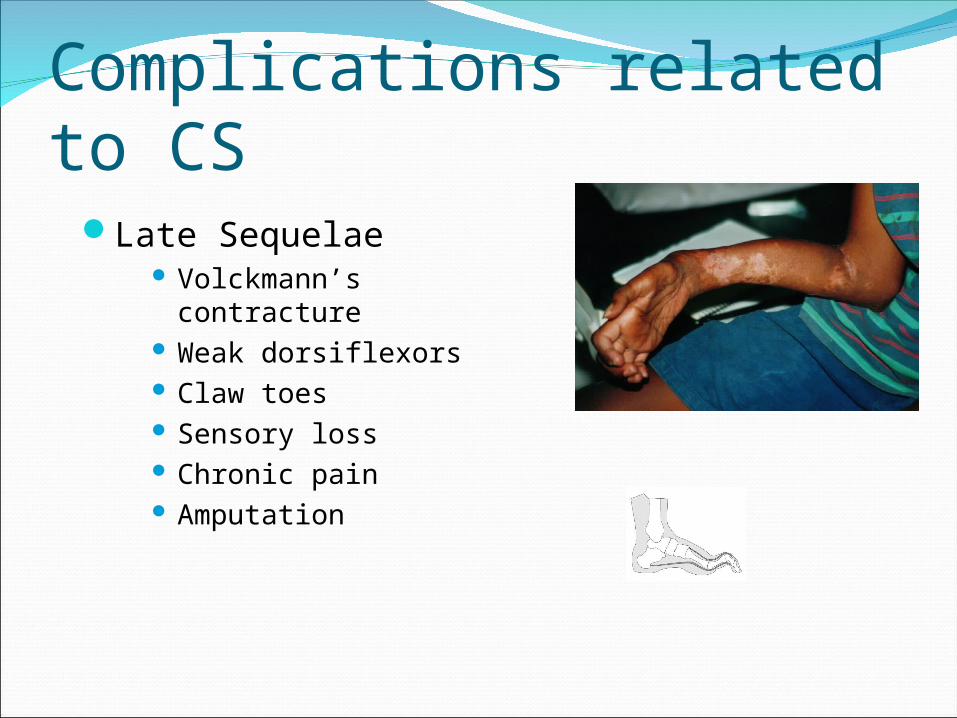
Complications related to CSLate Sequelae
Volckmann’s contracture Weak dorsiflexors Claw toes Sensory loss Chronic pain Amputation
Compartment SyndromeTissue Survival
• Muscle– 3-4 hours - reversible changes– 6 hours - variable damage– 8 hours - irreversible changes
• Nerve – 2 hours - looses nerve conduction– 4 hours - neuropraxia– 8 hours - irreversible changes

COMPARTMENT SYNDROME
ManagementNon surgical management:
Remove any tight bandage, soaked dressing
Cast should be removed completely
Elevation
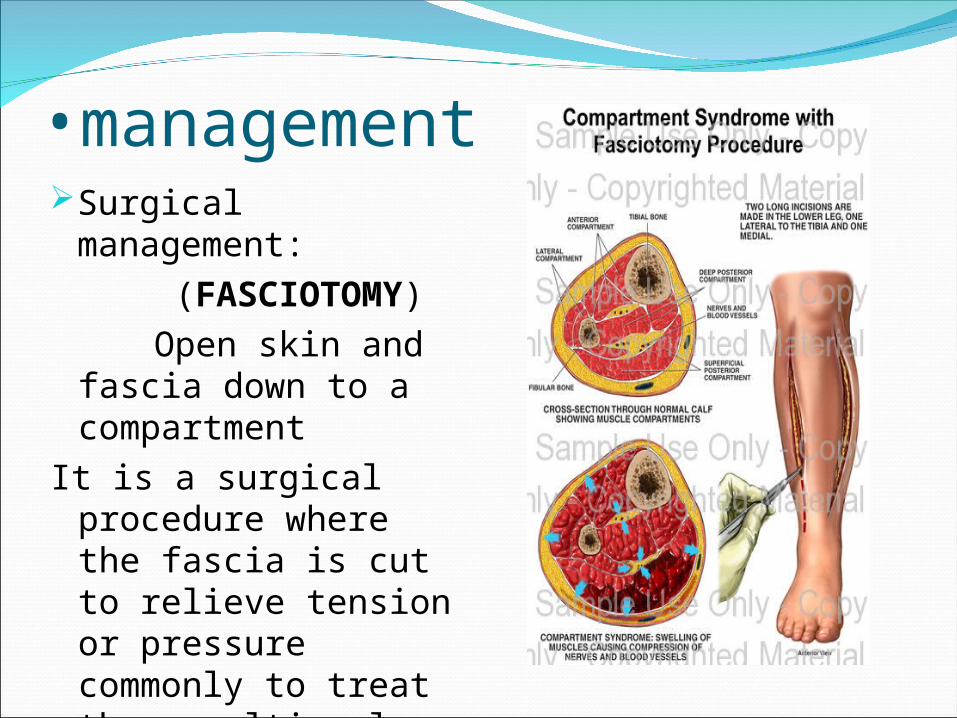
•managementSurgical
management: (FASCIOTOMY) Open skin and
fascia down to a compartment
It is a surgical procedure where the fascia is cut to relieve tension or pressure commonly to treat the resulting loss of circulation to the tissue
Fasciotomy PrinciplesMake early diagnosisLong extensile incisionsRelease all fascial compartmentsPreserve neurovascular structuresDebride necrotic tissuesCoverage within 7-10 days
Compartment SyndromeIndications for Fasciotomy
Unequivocal clinical findingsPressure within 15-20 mm hg of DBPRising tissue pressureSignificant tissue injury or high risk pt> 6 hours of total limb ischemiaInjury at high risk of compartment
syndrome
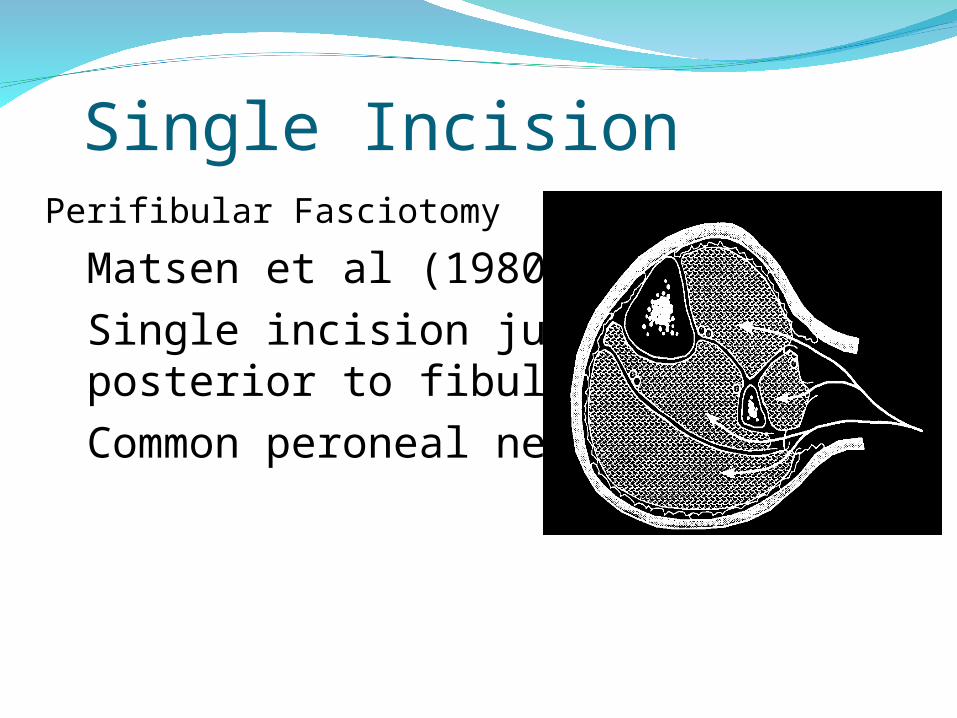
Single Incision• Perifibular Fasciotomy
– Matsen et al (1980)– Single incision just
posterior to fibula– Common peroneal nerve
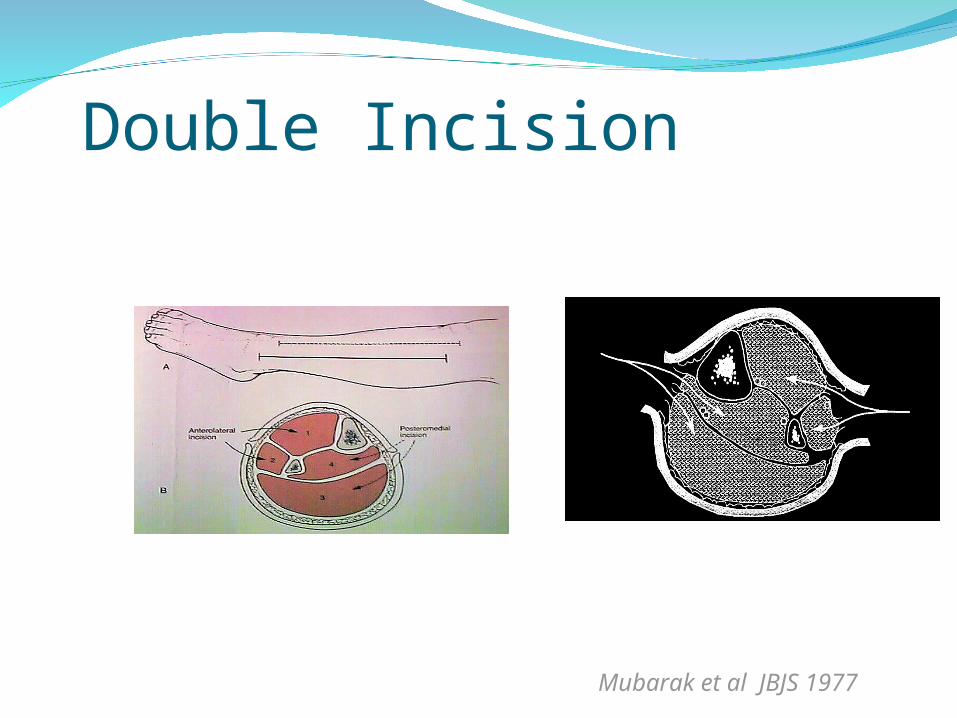
Double Incision
Mubarak et al JBJS 1977
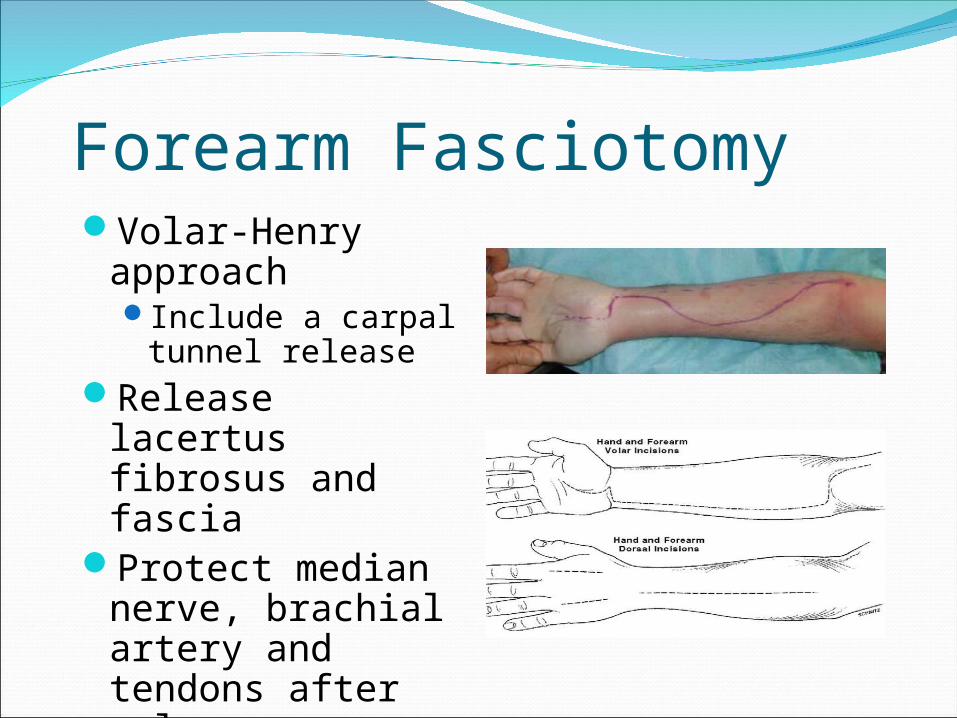
Forearm FasciotomyVolar-Henry
approachInclude a carpal
tunnel releaseRelease lacertus
fibrosus and fascia
Protect median nerve, brachial artery and tendons after release

Compartment syndrome foot9 compartments -medial superficial
lateral calcaneal interossei(4) adductor.
Suspicion with-lisfranc fracture -calcaneal fracture
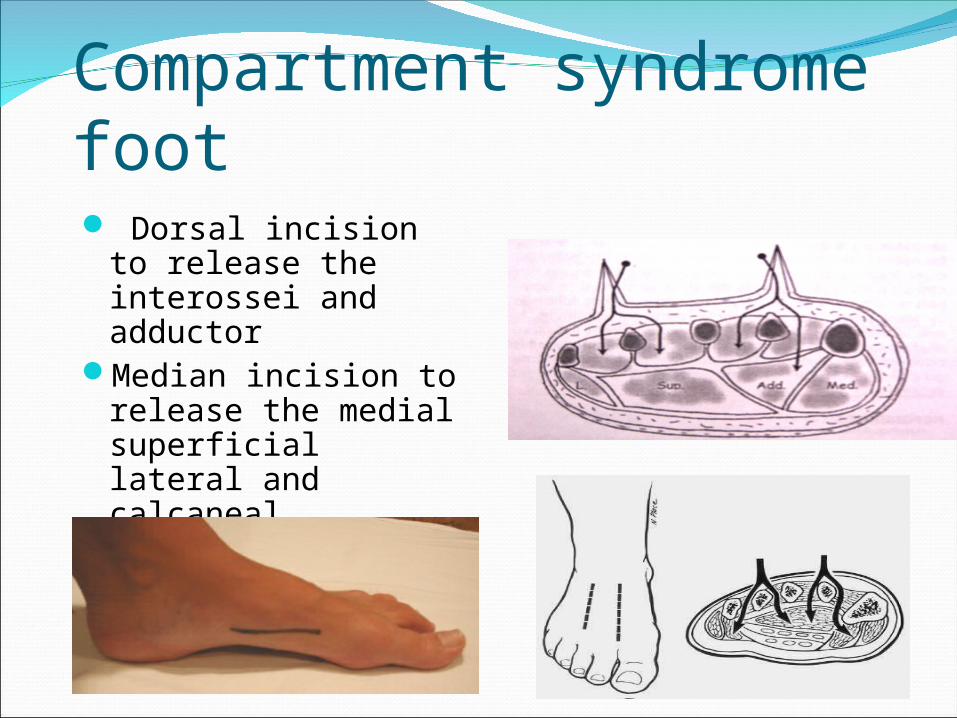
Compartment syndrome foot Dorsal incision to
release the interossei and adductor
Median incision to release the medial superficial lateral and calcaneal compartment
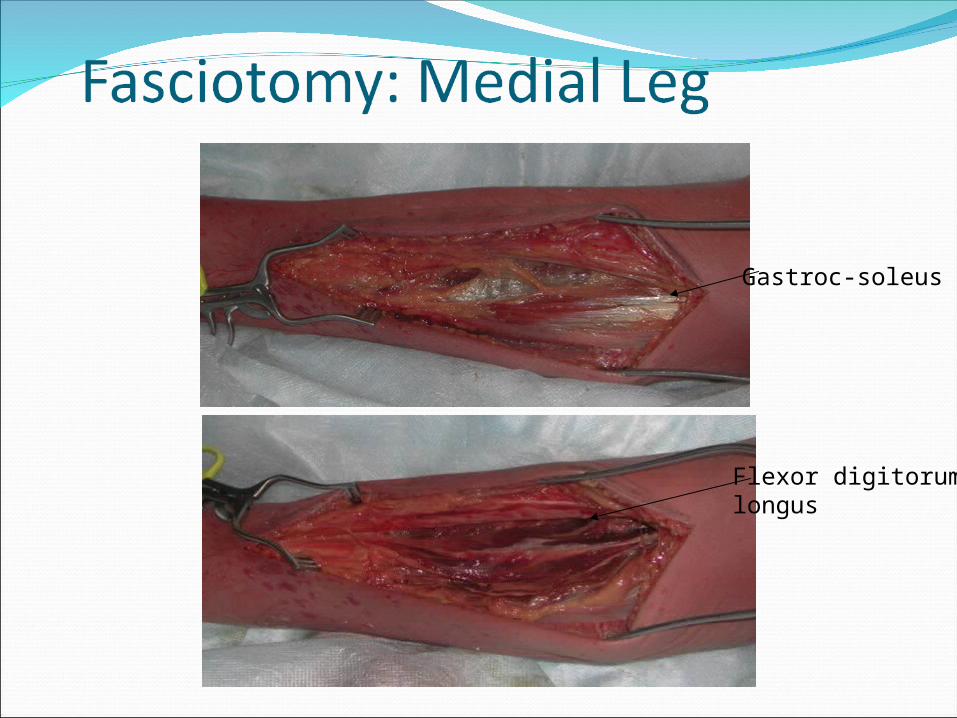
Flexor digitorum longus
Gastroc-soleus

Superficial peroneal nerve
Intermuscular septum
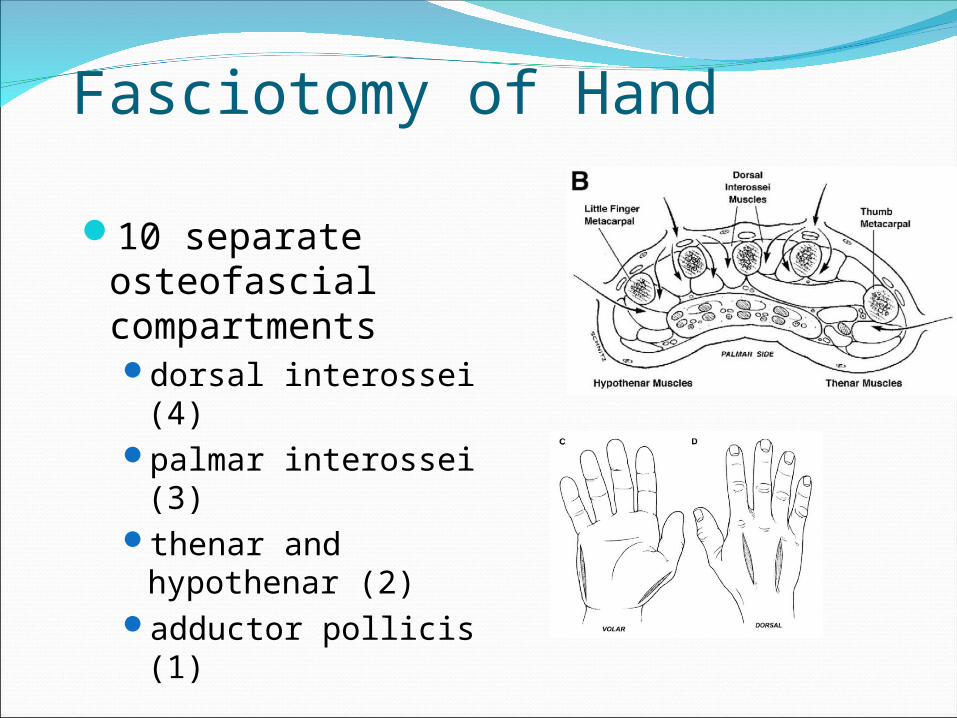
Fasciotomy of Hand
10 separate osteofascial compartmentsdorsal interossei (4) palmar interossei (3)thenar and
hypothenar (2)adductor pollicis (1)
Close skin by 2ry sutures after oedema subsides

It may need skin graft
Wound ManagementWound is not closed at initial surgerySecond look debridement with
consideration for coverage after 48-72 hrsLimb should not be at risk for further
swellingPt should be adequately stabilized Usually requires skin graft DPC possible if residual swelling is minimalFlap coverage needed if nerves, vessels, or
bone exposedGoal is to obtain definitive coverage
within 7-10 days
Wound ManagementAfter the fasciotomy, a bulky compression
dressing and a splint are applied.“VAC” (Vacuum Assisted Closure) can be used Foot should be placed in neutral to prevent
equinus contracture. Incision for the fasciotomy usually can be
closed after three to five days
Complications Related to Fasciotomies
Altered sensation within the margins of the wound (77%)
Dry, scaly skin (40%) Pruritus (33%) Discolored wounds (30%) Swollen limbs (25%) Tethered scars (26%) Recurrent ulceration (13%) Muscle herniation (13%) Pain related to the wound (10%) Tethered tendons (7%)
Fitzgerald, McQueen Br J Plast Surg 2000Fitzgerald, McQueen Br J Plast Surg 2000
Compartment syndrome is a serious syndrome, Which needs to be diagnosed early.Palpable pulse doesn’t exclude compartment syndromeIf diagnosis and fasciotomy were done within 24 hrs, the prognosis is good.If delayed, complications will develop.
The earlier you diagnose, the safer you are