compartments, the stryker, & you
DESCRIPTION
Consensus is P compartment > 30 mm Hg likely requires intervention Δ P = (DBP – P compartment ) measure of P perfusion Pts w/ P compartment < 40 mm Hg can develop CS if Δ P elevated (i.e. > 30) Keeping extremity level w/ heart decreases limb MAP w/o increasing P compartment - PowerPoint PPT PresentationTRANSCRIPT
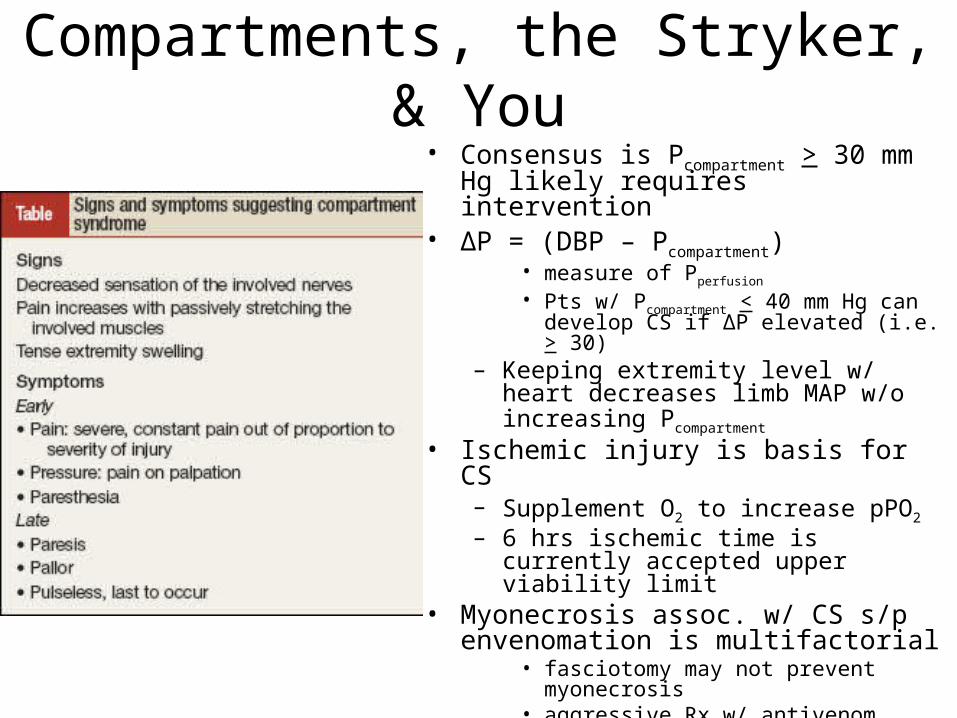
Compartments, the Stryker, & You• Consensus is Pcompartment > 30 mm Hg
likely requires intervention• ΔP = (DBP – Pcompartment)
• measure of Pperfusion
• Pts w/ Pcompartment < 40 mm Hg can develop CS if ΔP elevated (i.e. > 30)
– Keeping extremity level w/ heart decreases limb MAP w/o increasing Pcompartment
• Ischemic injury is basis for CS– Supplement O2 to increase pPO2 – 6 hrs ischemic time is currently accepted
upper viability limit• Myonecrosis assoc. w/ CS s/p
envenomation is multifactorial• fasciotomy may not prevent myonecrosis• aggressive Rx w/ antivenom decreases
limb hypoperfusion– consider delayed fasciotomy, if at all
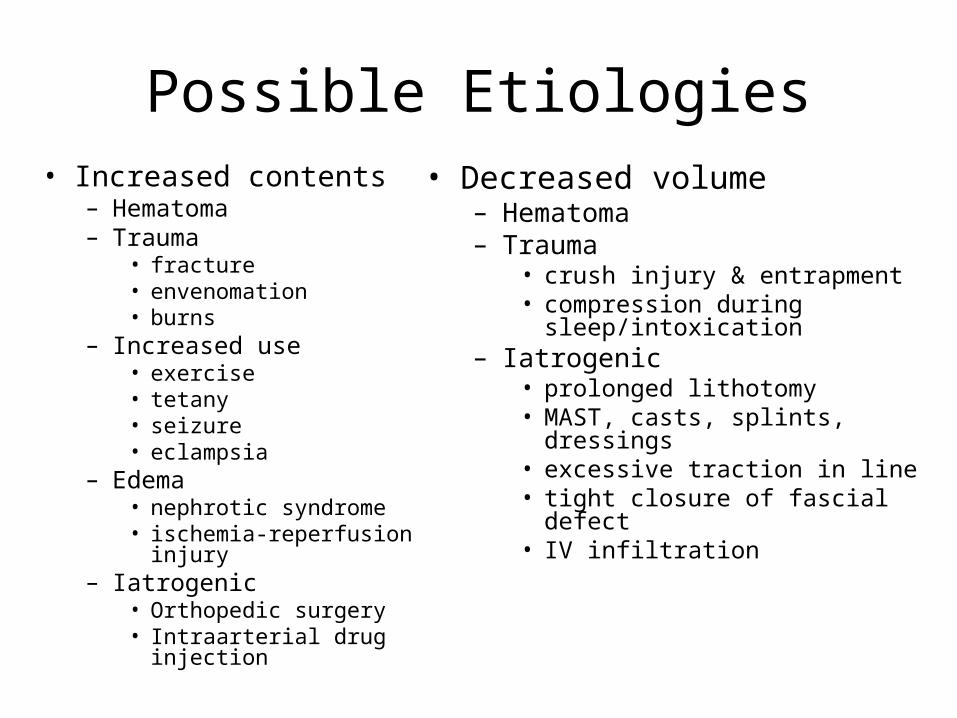
Possible Etiologies• Increased contents
– Hematoma– Trauma
• fracture• envenomation• burns
– Increased use• exercise• tetany• seizure• eclampsia
– Edema• nephrotic syndrome• ischemia-reperfusion injury
– Iatrogenic• Orthopedic surgery• Intraarterial drug injection
• Decreased volume– Hematoma– Trauma
• crush injury & entrapment• compression during sleep/intoxication
– Iatrogenic• prolonged lithotomy• MAST, casts, splints, dressings• excessive traction in line• tight closure of fascial defect• IV infiltration
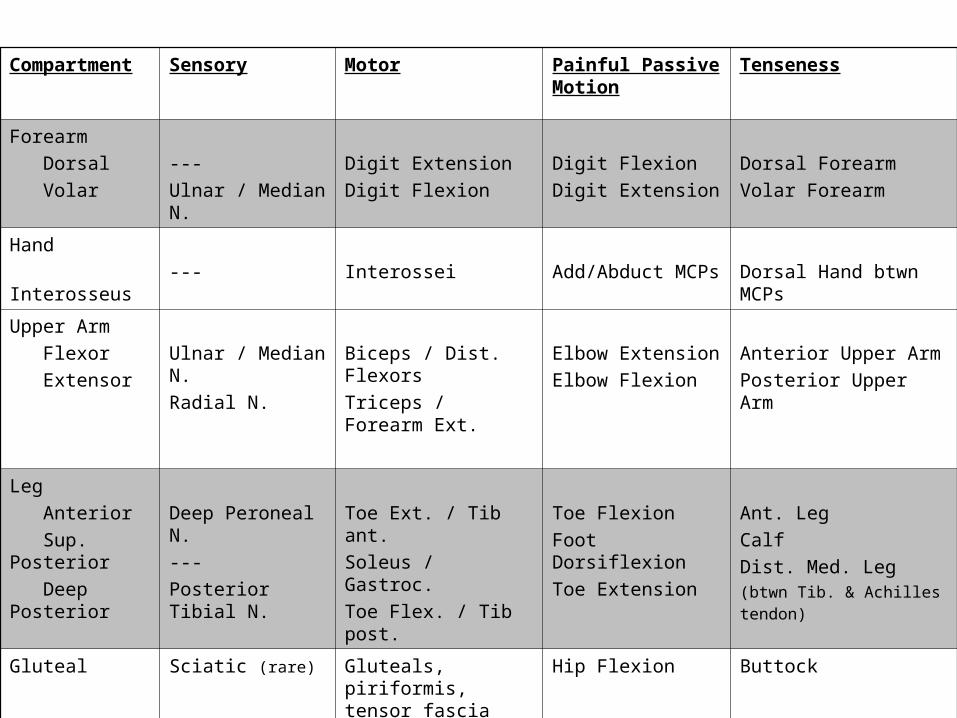
Compartment Sensory Motor Painful Passive Motion
Tenseness
Forearm Dorsal Volar
---Ulnar / Median N.
Digit ExtensionDigit Flexion
Digit FlexionDigit Extension
Dorsal ForearmVolar Forearm
Hand Interosseus --- Interossei Add/Abduct MCPs Dorsal Hand btwn MCPs
Upper Arm Flexor Extensor
Ulnar / Median N.Radial N.
Biceps / Dist. FlexorsTriceps / Forearm Ext.
Elbow ExtensionElbow Flexion
Anterior Upper ArmPosterior Upper Arm
Leg Anterior Sup. Posterior Deep Posterior
Deep Peroneal N.---Posterior Tibial N.
Toe Ext. / Tib ant.Soleus / Gastroc.Toe Flex. / Tib post.
Toe FlexionFoot DorsiflexionToe Extension
Ant. LegCalfDist. Med. Leg(btwn Tib. & Achilles tendon)
Gluteal Sciatic (rare) Gluteals, piriformis, tensor fascia lata
Hip Flexion Buttock
Foot Digital Nerves Foot Intrinsics Toe Flex. / Ext. Dorsal / Plantar Foot
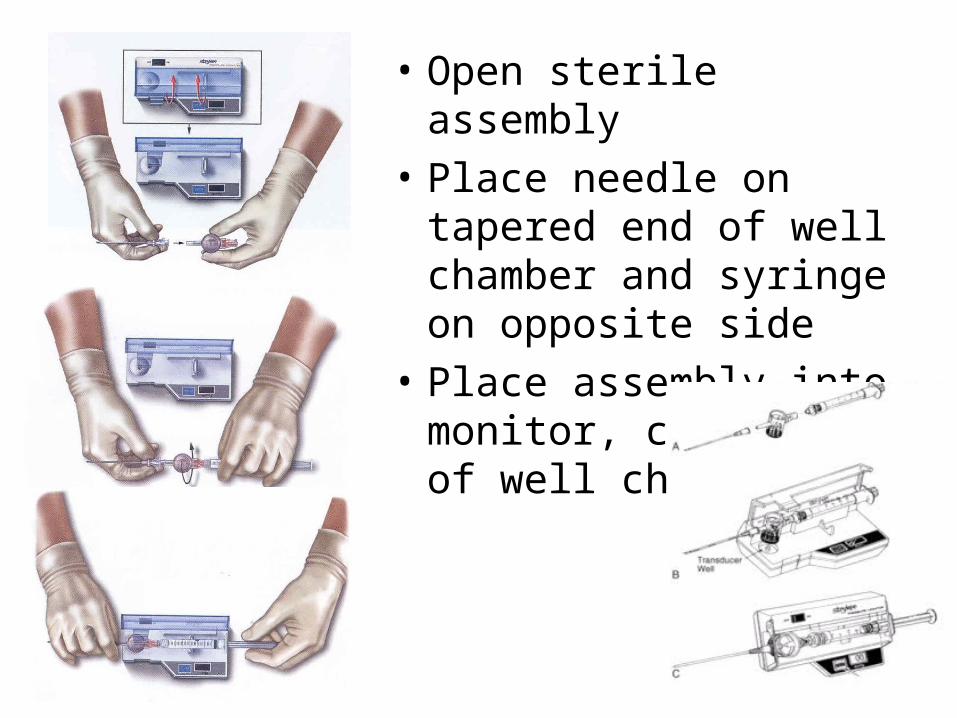
• Open sterile assembly• Place needle on tapered
end of well chamber and syringe on opposite side
• Place assembly into monitor, clear side of well chamber up
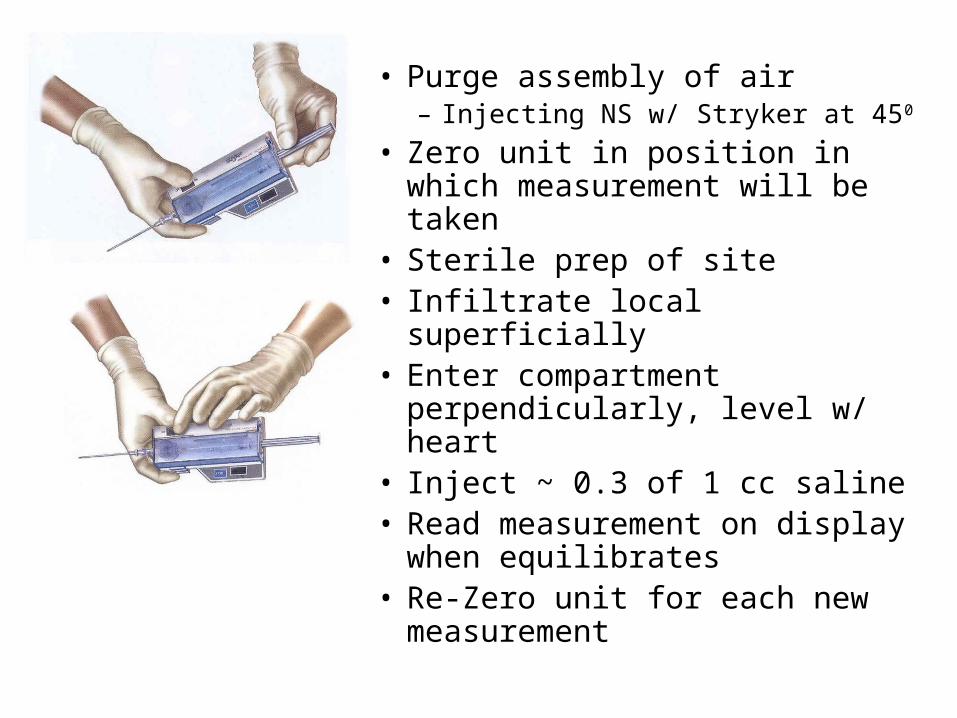
• Purge assembly of air – Injecting NS w/ Stryker at 450
• Zero unit in position in which measurement will be taken
• Sterile prep of site• Infiltrate local superficially• Enter compartment
perpendicularly, level w/ heart• Inject ~ 0.3 of 1 cc saline • Read measurement on
display when equilibrates• Re-Zero unit for each new
measurement
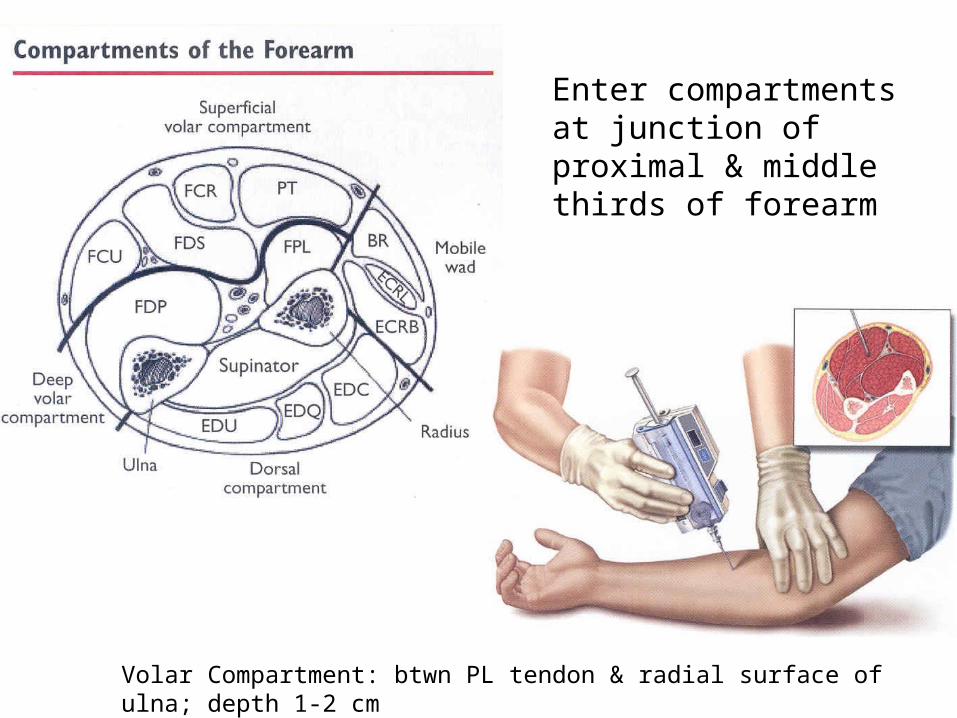
Volar Compartment: btwn PL tendon & radial surface of ulna; depth 1-2 cm
Enter compartments at junction of proximal & middle thirds of forearm
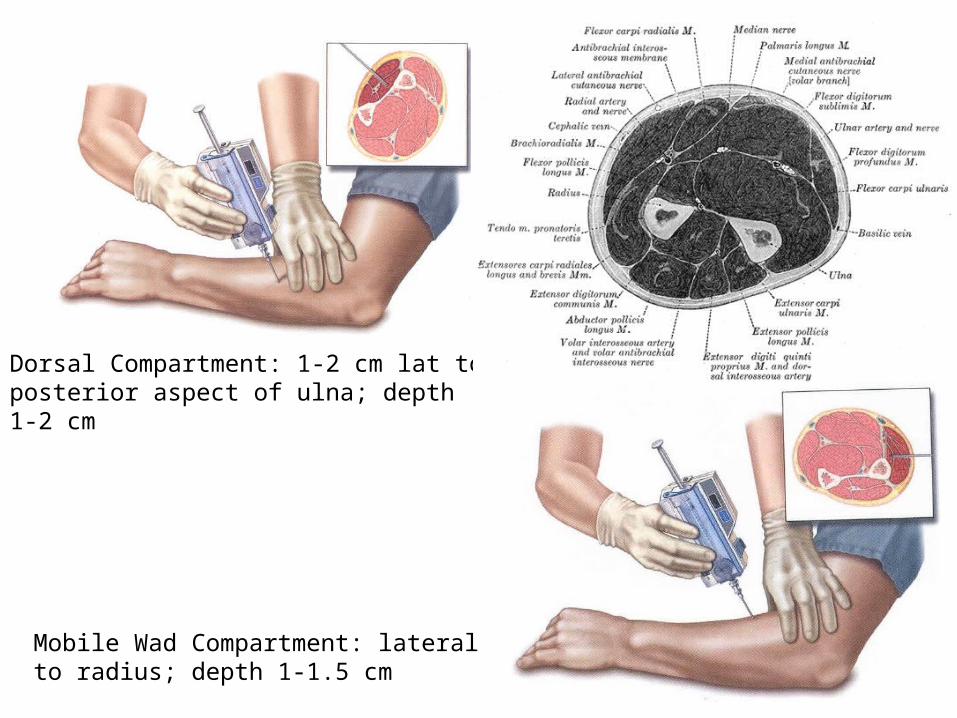
Dorsal Compartment: 1-2 cm lat to posterior aspect of ulna; depth 1-2 cm
Mobile Wad Compartment: lateral to radius; depth 1-1.5 cm
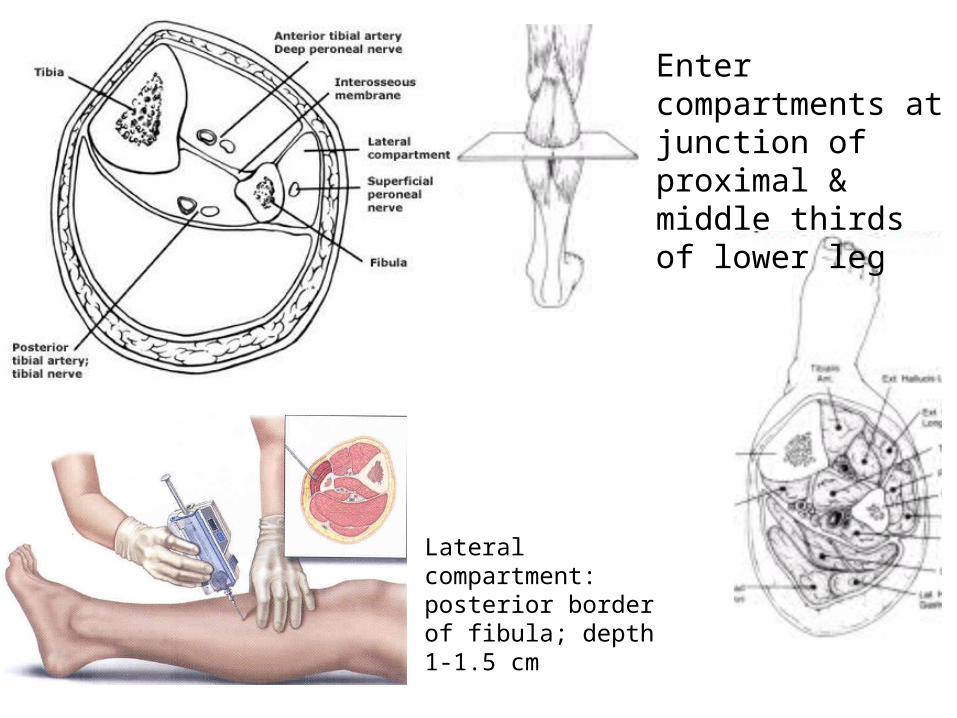
Enter compartments at junction of proximal & middle thirds of lower leg
Lateral compartment: posterior border of fibula; depth 1-1.5 cm
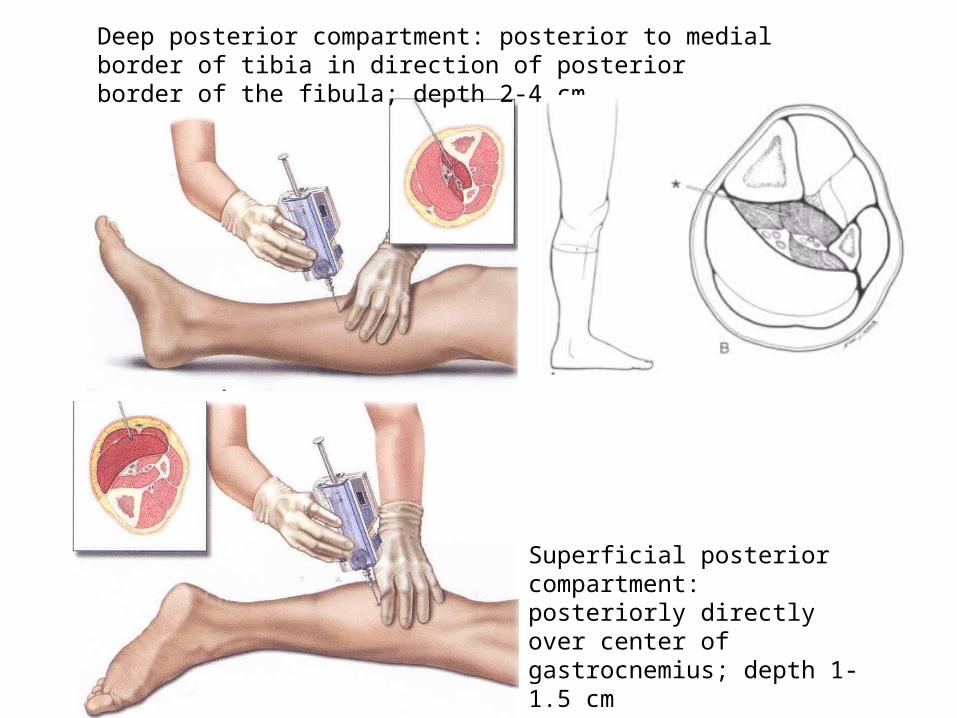
Deep posterior compartment: posterior to medial border of tibia in direction of posterior border of the fibula; depth 2-4 cm
Superficial posterior compartment: posteriorly directly over center of gastrocnemius; depth 1-1.5 cm
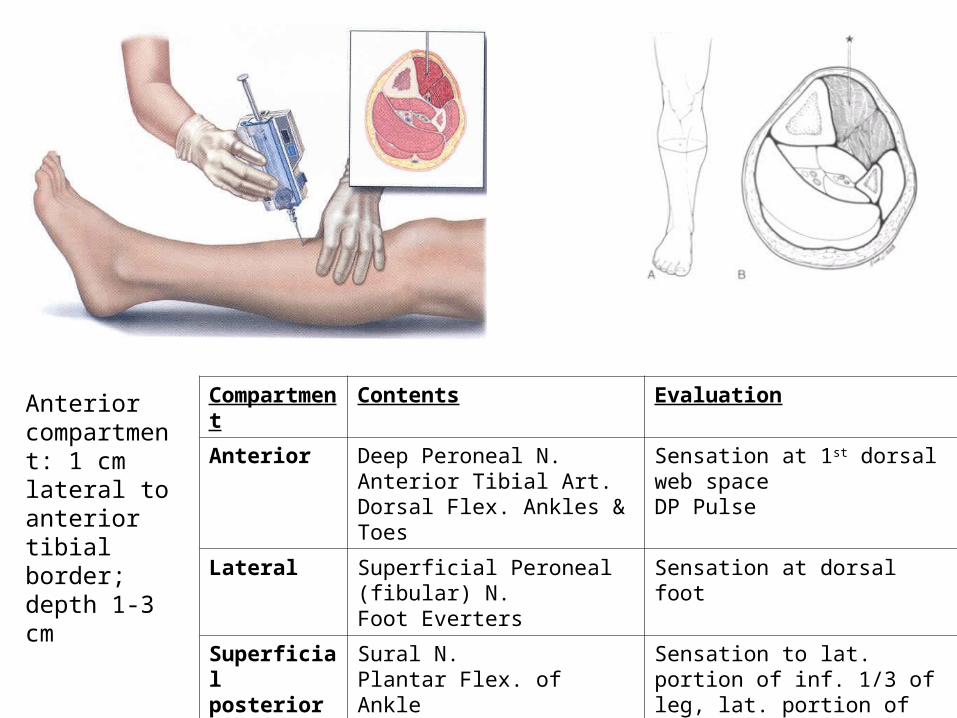
Anterior compartment: 1 cm lateral to anterior tibial border; depth 1-3 cm
Compartment Contents Evaluation
Anterior Deep Peroneal N.Anterior Tibial Art.Dorsal Flex. Ankles & Toes
Sensation at 1st dorsal web spaceDP Pulse
Lateral Superficial Peroneal (fibular) N.Foot Everters
Sensation at dorsal foot
Superficial posterior
Sural N.Plantar Flex. of Ankle
Sensation to lat. portion of inf. 1/3 of leg, lat. portion of 5th digit
Deep posterior
Tibial N.Posterior Tibial & Peroneal Art.Plantar Flex. of toes
Sensation to plantar footPT Pulse
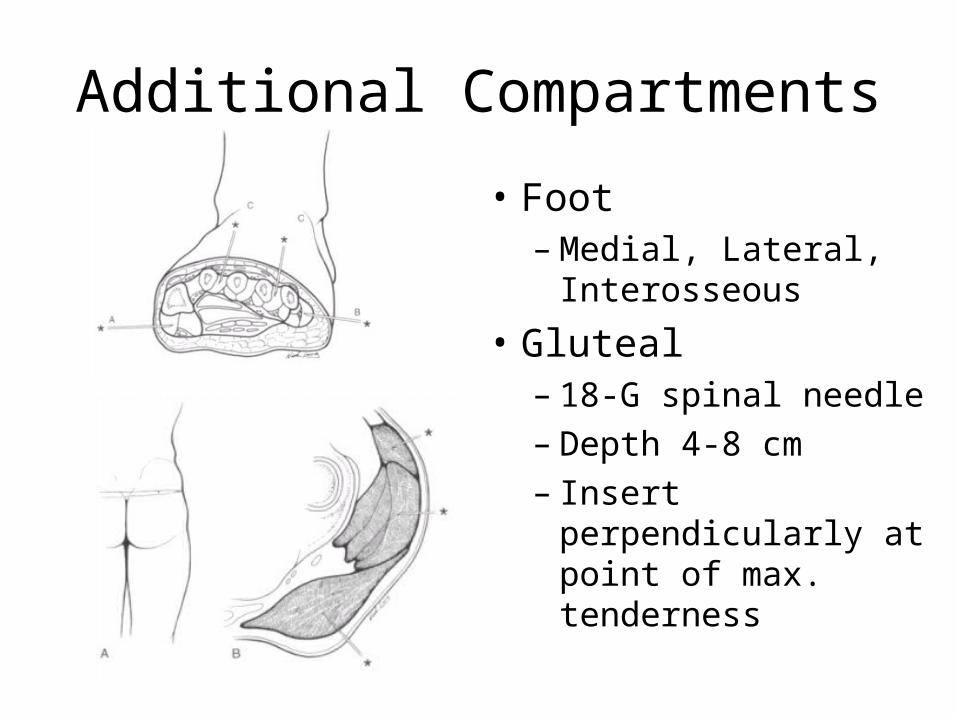
Additional Compartments
• Foot– Medial, Lateral,
Interosseous• Gluteal
– 18-G spinal needle– Depth 4-8 cm– Insert perpendicularly
at point of max. tenderness
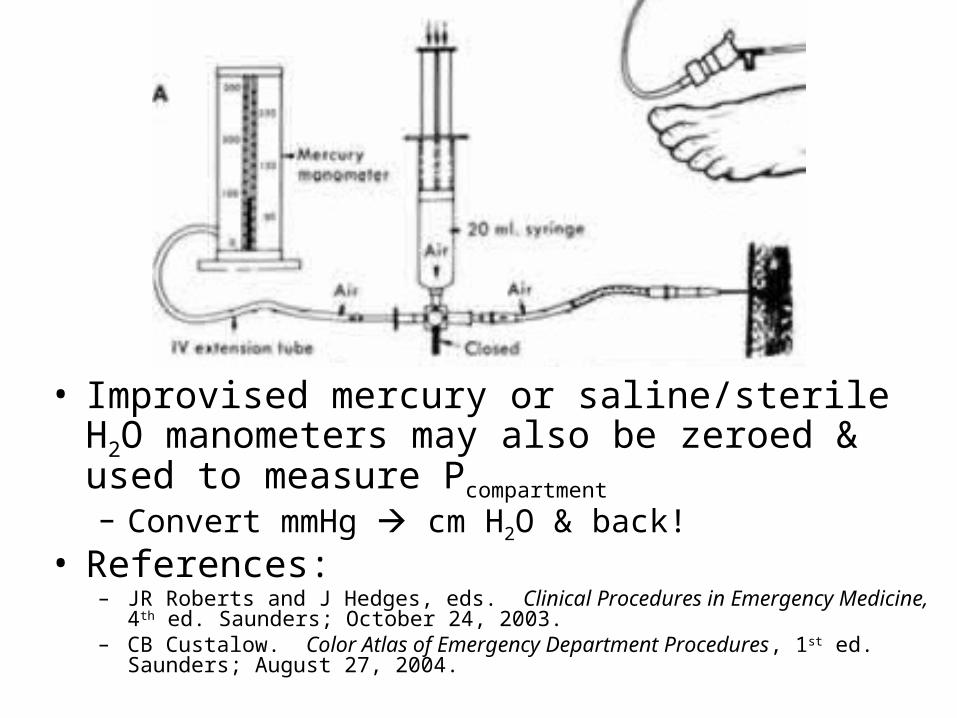
• Improvised mercury or saline/sterile H2O manometers may also be zeroed & used to measure Pcompartment – Convert mmHg cm H2O & back!
• References:– JR Roberts and J Hedges, eds. Clinical Procedures in Emergency Medicine, 4th ed.
Saunders; October 24, 2003.– CB Custalow. Color Atlas of Emergency Department Procedures, 1st ed. Saunders;
August 27, 2004.