complication o labor
DESCRIPTION
Complication o Labor. Psychologic Disorders. Alterations in thinking, mood or behavior Keep her well oriented and promote optimal functioning in labor. Focus on maintaining safe environment and ensuring fetal and maternal well-being. Dystocia r/t dysfunctional contractions. - PowerPoint PPT PresentationTRANSCRIPT

Complication o Labor
Psychologic Disorders
Alterations in thinking, mood or behavior
Keep her well oriented and promote optimal functioning in labor. Focus on maintaining safe environment and ensuring fetal and maternal well-being
Dystocia r/t dysfunctional contractions
Accounts for ~ 50% C/S for primips; <5% C/S for multips
Hypertonic: in 1st phase- poor quality U/Cs, become more frequent, but ineffective and changing dilatation or effacement prolonged latent phase
Tx: sedation, oxytocin, amniotomy
Hypotonic: irreg, low amplitude protracted labor and arrest of dilatation
Tx: oxytocin, amniotomy

Active Management of Labor
Standardized criteria for diagnosis of labor
Standardized method of labor management
One-to-one nursing care in labor
Prenatal education to teach re: this protocol
Method:Amniotomy right away
VE frequently
If change not as expected, oxytocin

Precipitous Labor and Birth
From beginning of regular contractions to delivery is 3 hours or lessRisks:
AbruptionCervical and perineal lacerationsFetal head trauma
Women with history may be scheduled for induction

Post-term Pregnancy> 42 completed weeks Cause of true post-term is unknown; often incorrect datesMaternal Risks:
Large baby and associationsPsychologic ills
Fetal-Neonatal Risks:Placental changes insufficienciesOligohydramniosmacrosomia birth trauma, glucose maintenance problemsMeconmium stained fluid (aspiration)
As pregnancy approached term, fetal well-being studies done

Fetal Malposition
OP position:Fetus must rotate 135° or occasionally born in OP position
If born OP, increased risk of 3rd or 4th degree laceration, broken symphysis
May use forceps or manual rotation
Positioning: knee chest, pelvic rocking

Fetal Malpresentation
Brow Usually C/S recommendedPerinatal morbidity and mortality:
Trauma: cerebral and neck compression; damage to trachea and larynx
Tx: pelvimetry, oxytocin?, C/S
FacePerinatal morbidity and mortality:
Risk of prolonged labor, fetal edema, swelling of neck and internal structures, petechiae, ecchymosis
Tx: C/S in no progress

Fetal Malpresentation
BreechMost common malpresentation
Frank breech most common
Risk of cord prolapse; fetal anomolies 3x higher
If vag del: head trauma, fetal entrapment
Tx: external version (50-60% success), if vag del: epidural, double set-up

Fetal Malpresentation
ShoulderVersion may be attempted
C/S
Compound presentation
Macrosomia
>4500 gObese 3-4x more likely to have macrosomic baby↑risk of perineal lacerations, infectionMost significant problem is shoulder dystocia
OB emergency permanent injury of brachial plexus, fx clavicle, asphyxia, neurologic damageTx:
Assessment of adequacy of pelvisSuprapubic pressureIntentional breaking of clavicle?C/S

Multiple Gestation
Mother at risk for:Hypertension or preeclampsia
Anemia
Hydramnios
PPROM, IUGR, incompetent cx
Malpresentation
More physical discomforts
Multiple Gestation
Tx:U/S to diagnose amnion/chorion, follow growth, observe for twin-twin transfusion
Frequent office visits to monitor for problems
Likely to deliver by C/S

Abruptio Placentae
Premature separation of normally implanted placenta from the uterine wallVery high mortalityCause unknown but r/t
Maternal hypertensionMaternal traumaCigarettes, cocaineShort umbilical cord, high parity
More common in Caucasian and African American than Asian or Latin American

Abruptio Placentae

Abruptio Placentae

Abruptio Placentae
http://video.about.com/pregnancy/Placenta-Abruptio.htm

Abruptio Placentae
ClassificationO=asymptomatic, diagnosed after birth
I=mild, most common
II=mod, both mom and baby show signs of distress
III=severe, maternal shock and fetal death likely

Abruptio Placentae
TypesMarginal-blood passes between fetal membranes and uterine wall and escapes vaginally; separation at periphery of placenta
Central-separates centrally, blood trapped between placenta and uterine wall. No overt bleeding
Complete-massive vaginal bleeding in presence of almost total separation

Abruptio Placentae

Abruptio Placentae
Blood invades myometrial tissue pain and uterine irritability.
May necessitate hysterectomy after delivery secondary to inability to uterus to contract.
May lead to coagulation defects

Abruptio Placentae
Maternal RisksBlood coagulation problemsShockRenal failure (r/t hemorrhage)Possible hysterectomy
Fetal-Neonatal RisksIf separation ~50% 100% demiseDepending upon separation, time before delivery, maturity of baby neurologic damage

Abruptio Placentae
TxContinuous EFM (if baby alive)
Develop plan for birth
Maintain CV status/tx hypovolemic shock
Follow blood coag studies/have blood factors available

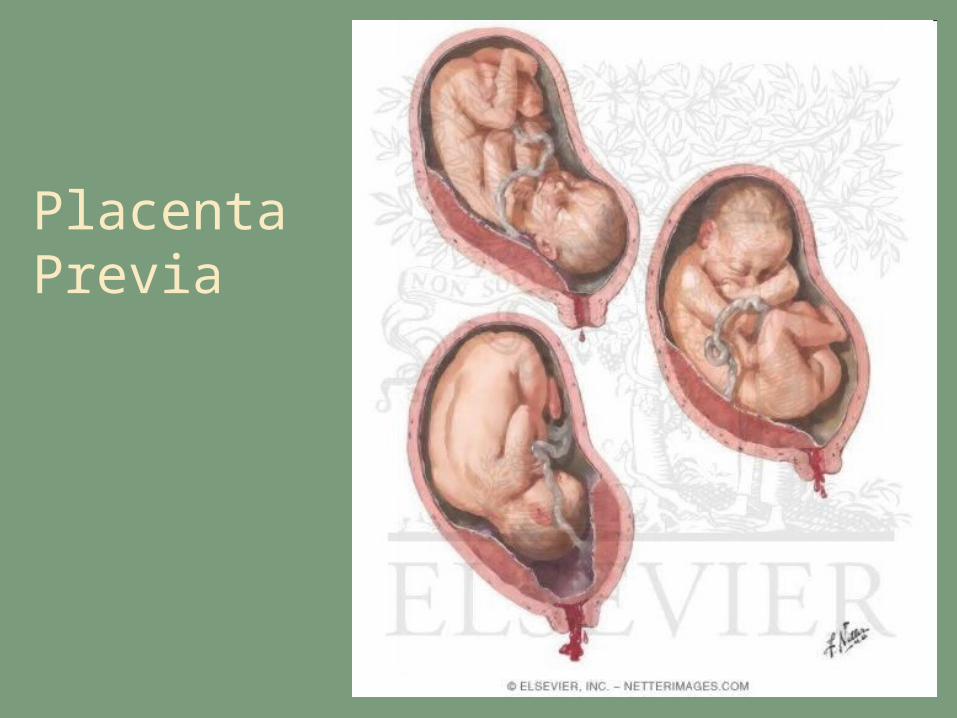
Placenta Previa
Improperly implanted in lower uterine segment
TypesLow lying: close proximity to os, but doesn’t reach it
Marginal: edge of placenta at margin of the os
Partial: internal os is partially covered by placenta
Total: internal os completely covered

Placenta Previa

Placenta Previa

Placenta Previa
Placenta Previa
Placenta Previa
Cause unknown, but associated withMultiparityIncreased ageDefective development of blood vessels in deciduaDefective implantation of the placentaPrior C/SSmokingLarge placenta

Placenta Previa
TxContinuous EFM
Differential diagnosis
☺No vag exam until previa r/o (U/S, other assessments)
Care depends on amt bleeding, gestational age, assessment of fetus
